User login
Port‐A‐Cath Embolization
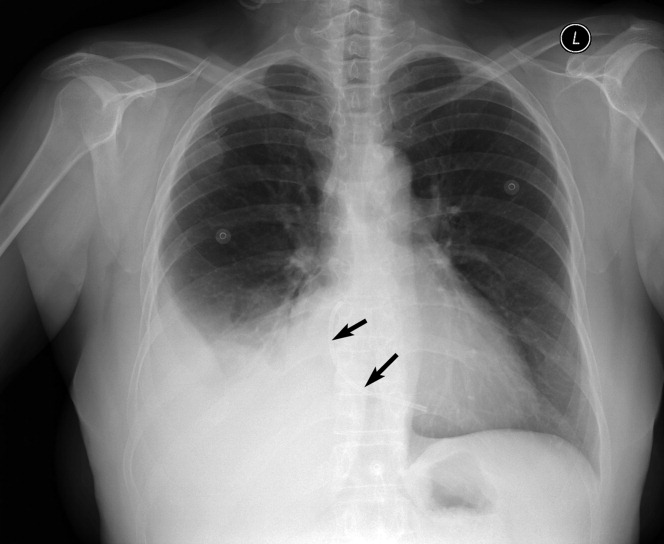
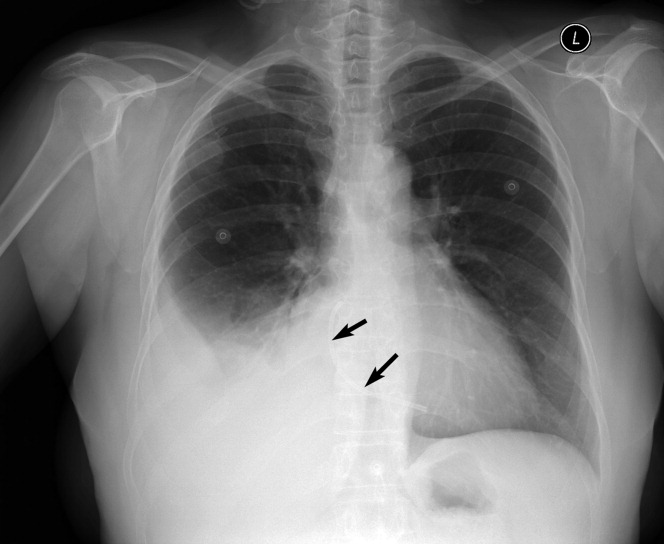
A 59‐year‐old white female, with a 3‐year history of Port‐A‐Cath (PAC) placement for abdominal mesothelioma, presented with 2 episodes of cardiac palpitations. The onset of palpitations occurred 2 days prior to admission, following 15 minutes of vigorous but failed attempts to access the PAC with normal saline and tissue plasminogen activator at her oncologist's office. Although asymptomatic at the time of manipulation, each episode was triggered by subsequent exertion, lasting for about 1 minute, and not associated with chest pain. Electrocardiogram showed normal sinus rhythm and occasional premature ventricular contractions. A chest x‐ray showed a catheter fragment spanning the right atrium and ventricle (Figure 1). Computed tomography (CT) scan confirmed a 10‐cm dislodged catheter (Figure 2). Following emergent catheter retrieval via right‐sided heart catheterization, the patient's symptoms resolved. At least 42 cases of catheter embolization have been reported in the recent literature.1 Of these cases, only 7% had palpitations. Although rare, catheter fracture should be considered in patients with palpitations and history of indwelling venous catheter.

- ,.Ventricular tachycardia secondary to Port‐A‐Cath fracture and embolization.J Emerg Med.2003;24:29–34.
A 59‐year‐old white female, with a 3‐year history of Port‐A‐Cath (PAC) placement for abdominal mesothelioma, presented with 2 episodes of cardiac palpitations. The onset of palpitations occurred 2 days prior to admission, following 15 minutes of vigorous but failed attempts to access the PAC with normal saline and tissue plasminogen activator at her oncologist's office. Although asymptomatic at the time of manipulation, each episode was triggered by subsequent exertion, lasting for about 1 minute, and not associated with chest pain. Electrocardiogram showed normal sinus rhythm and occasional premature ventricular contractions. A chest x‐ray showed a catheter fragment spanning the right atrium and ventricle (Figure 1). Computed tomography (CT) scan confirmed a 10‐cm dislodged catheter (Figure 2). Following emergent catheter retrieval via right‐sided heart catheterization, the patient's symptoms resolved. At least 42 cases of catheter embolization have been reported in the recent literature.1 Of these cases, only 7% had palpitations. Although rare, catheter fracture should be considered in patients with palpitations and history of indwelling venous catheter.
A 59‐year‐old white female, with a 3‐year history of Port‐A‐Cath (PAC) placement for abdominal mesothelioma, presented with 2 episodes of cardiac palpitations. The onset of palpitations occurred 2 days prior to admission, following 15 minutes of vigorous but failed attempts to access the PAC with normal saline and tissue plasminogen activator at her oncologist's office. Although asymptomatic at the time of manipulation, each episode was triggered by subsequent exertion, lasting for about 1 minute, and not associated with chest pain. Electrocardiogram showed normal sinus rhythm and occasional premature ventricular contractions. A chest x‐ray showed a catheter fragment spanning the right atrium and ventricle (Figure 1). Computed tomography (CT) scan confirmed a 10‐cm dislodged catheter (Figure 2). Following emergent catheter retrieval via right‐sided heart catheterization, the patient's symptoms resolved. At least 42 cases of catheter embolization have been reported in the recent literature.1 Of these cases, only 7% had palpitations. Although rare, catheter fracture should be considered in patients with palpitations and history of indwelling venous catheter.
- ,.Ventricular tachycardia secondary to Port‐A‐Cath fracture and embolization.J Emerg Med.2003;24:29–34.
- ,.Ventricular tachycardia secondary to Port‐A‐Cath fracture and embolization.J Emerg Med.2003;24:29–34.