User login
Disseminated Sporotrichosis
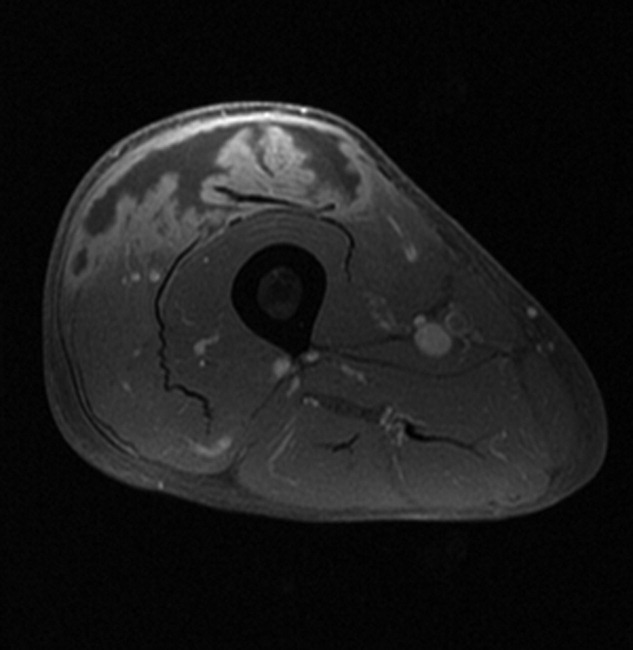
A 61‐year‐old healthy man presented with recurrent right wrist pain. The patient underwent unsuccessful carpal tunnel surgery and pathology revealed granulomatous inflammation. With worsening pain and new nodular inflammation, prednisone and azathioprine were prescribed for presumed sarcoidosis. Subsequently, right arm ulceration developed (Figure 1), and wound and blood cultures revealed Sporothrix schenkii. Immunosuppressive medications were stopped, but the ulceration progressed and ultimately involved the entire arm (Figure 2). New lower‐extremity fluid collections seen on the magnetic resonance imaging (MRI) MRI (Figures 3, 4) prompted several surgical debridements. Multiple abscesses formed in all extremities despite amphotericin and itraconazole therapy. The patient was eventually discharged with ongoing amphotericin and plans for surveillance imaging and repeated debridements.



Sporothrix schenckii is a dimorphic fungus often associated with cutaneous infections of the extremities in gardeners. These infections are definitively treated with oral azole medications or topical potassium iodide. Disseminated sporotrichosis is almost exclusively seen in immunosuppressed patients including those with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)1 and hematologic malignancies.2 Iatrogenic immunosuppression from chemotherapy or corticosteroids can also place a patient at risk for disseminated disease. Disseminated sporotrichosis is extremely difficult to manage with significant morbidity and mortality; fatal cases are commonly reported in the literature.3
- ,,,.Cutaneous and meningeal sporotrichosis in a HIV patient.Rev Iberoam Micol.2007;24(2):161–163.
- ,,.Systemic sporotrichosis.Ann Intern Med.1970;73(1):23–30.
- ,,,,.Fatal sporotrichosis.Cutis.2006;78(4):253–256.
A 61‐year‐old healthy man presented with recurrent right wrist pain. The patient underwent unsuccessful carpal tunnel surgery and pathology revealed granulomatous inflammation. With worsening pain and new nodular inflammation, prednisone and azathioprine were prescribed for presumed sarcoidosis. Subsequently, right arm ulceration developed (Figure 1), and wound and blood cultures revealed Sporothrix schenkii. Immunosuppressive medications were stopped, but the ulceration progressed and ultimately involved the entire arm (Figure 2). New lower‐extremity fluid collections seen on the magnetic resonance imaging (MRI) MRI (Figures 3, 4) prompted several surgical debridements. Multiple abscesses formed in all extremities despite amphotericin and itraconazole therapy. The patient was eventually discharged with ongoing amphotericin and plans for surveillance imaging and repeated debridements.
Sporothrix schenckii is a dimorphic fungus often associated with cutaneous infections of the extremities in gardeners. These infections are definitively treated with oral azole medications or topical potassium iodide. Disseminated sporotrichosis is almost exclusively seen in immunosuppressed patients including those with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)1 and hematologic malignancies.2 Iatrogenic immunosuppression from chemotherapy or corticosteroids can also place a patient at risk for disseminated disease. Disseminated sporotrichosis is extremely difficult to manage with significant morbidity and mortality; fatal cases are commonly reported in the literature.3
A 61‐year‐old healthy man presented with recurrent right wrist pain. The patient underwent unsuccessful carpal tunnel surgery and pathology revealed granulomatous inflammation. With worsening pain and new nodular inflammation, prednisone and azathioprine were prescribed for presumed sarcoidosis. Subsequently, right arm ulceration developed (Figure 1), and wound and blood cultures revealed Sporothrix schenkii. Immunosuppressive medications were stopped, but the ulceration progressed and ultimately involved the entire arm (Figure 2). New lower‐extremity fluid collections seen on the magnetic resonance imaging (MRI) MRI (Figures 3, 4) prompted several surgical debridements. Multiple abscesses formed in all extremities despite amphotericin and itraconazole therapy. The patient was eventually discharged with ongoing amphotericin and plans for surveillance imaging and repeated debridements.
Sporothrix schenckii is a dimorphic fungus often associated with cutaneous infections of the extremities in gardeners. These infections are definitively treated with oral azole medications or topical potassium iodide. Disseminated sporotrichosis is almost exclusively seen in immunosuppressed patients including those with human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS)1 and hematologic malignancies.2 Iatrogenic immunosuppression from chemotherapy or corticosteroids can also place a patient at risk for disseminated disease. Disseminated sporotrichosis is extremely difficult to manage with significant morbidity and mortality; fatal cases are commonly reported in the literature.3
- ,,,.Cutaneous and meningeal sporotrichosis in a HIV patient.Rev Iberoam Micol.2007;24(2):161–163.
- ,,.Systemic sporotrichosis.Ann Intern Med.1970;73(1):23–30.
- ,,,,.Fatal sporotrichosis.Cutis.2006;78(4):253–256.
- ,,,.Cutaneous and meningeal sporotrichosis in a HIV patient.Rev Iberoam Micol.2007;24(2):161–163.
- ,,.Systemic sporotrichosis.Ann Intern Med.1970;73(1):23–30.
- ,,,,.Fatal sporotrichosis.Cutis.2006;78(4):253–256.
