User login
Abnormal uterine bleeding: Avoid the rush to hysterectomy
- The levonorgestrel-IUS is the most effective treatment for heavy menstrual bleeding, reducing blood loss by close to 100% (A).
- Endometrial ablation is an effective treatment for women who want to avoid major surgery and preserve their uterus, but have no wish to become pregnant in the future (A).
- Endometrial biopsy should be part of the evaluation of abnormal uterine bleeding in all women over age 35 (B).
Strength of recommendation (SOR)
A. Good-quality patient-oriented evidence
B. Inconsistent or limited-quality patient-oriented evidence
C. Consensus, usual practice, opinion, disease-oriented evidence, case series
Ms. M, a 39-year-old mother of 3, runs a busy day-care center, cares for her sick mother, and shuttles her children among their myriad activities. During today’s office visit, she seems anxious. She says her periods are regular, but have become increasingly heavy in recent years and may last as long as 9 days. The bleeding is very heavy, with a lot of clots and some cramps during the first few days. In the past year, painful periods have caused her to miss work on several occasions. She says she often feels tired, and worries that she may be anemic. Preserving fertility is not a concern; her husband has had a vasectomy.
On exam she is without orthostasis and appears well. Her uterus is top-normal size, nontender, and there are no adnexal masses or cervical or vaginal abnormalities. You note a normal Pap at your office 5 months ago. Her office hemoglobin is 9.8 mg/dL.
She asks you to refer her to a gynecologist for a hysterectomy because she “just can’t take it anymore.” Her heavy menses are disrupting her life. Since she does not want any more children, she feels that if someone could “just take it out,” her problem would be solved. But she isn’t really enthusiastic about a hysterectomy because her life is too busy to allow time for a lengthy recovery.
You explain that there are a number of options you’d like her to consider first. Then you review the options and some of the research behind them, having recently read an article on evidence-based therapy for abnormal uterine bleeding.
A common complaint in primary care
Abnormal uterine bleeding is a common reason for women to visit their primary care clinician, accounting for about 20% of gynecologic primary care visits.1 Women are understandably concerned about any disruption of their normal bleeding pattern. Many, however, are unaware of common causes of abnormal bleeding and available treatment options.
Most cases of chronic abnormal bleeding can be classified as either heavy and regular (menorrhagia) or heavy and irregular (menometrorrhagia). A rule of thumb to help guide diagnostic testing is that menorrhagia often results from anatomic problems of the uterus or endometrium, such as polyps. Menometrorrhagia is more likely to result from hormonal abnormalities, such as polycystic ovarian syndrome (PCOS). This review will focus on medical and minimally invasive surgical therapy for chronic abnormal bleeding.

First step: Pregnancy test
Many conditions can cause abnormal uterine bleeding (TABLE 1). In women of reproductive age, the first step in the diagnostic process should be a urine or serum pregnancy test. Urine pregnancy tests have a sensitivity of 90% one day after a missed period and approximately 97% after one week.2 In addition to a pregnancy test, consider testing for thyroid dysfunction and obtaining serum prolactin levels for women presenting with anovulatory bleeding.3 If anemia is suspected, a hematocrit or hemogram is indicated. All patients over the age of 35 who present with abnormal uterine bleeding should have an office endometrial biopsy to rule out endometrial hyperplasia or cancer.4
Is she ovulating? Most cases of heavy bleeding with irregular periods are the result of anovulation, which is common soon after menarche and at the approach of menopause. Other causes of anovulatory bleeding include PCOS, hypothyroidism, and elevated prolactin levels. Chronic, irregular bleeding without a known anatomic cause is termed “dysfunctional uterine bleeding,” or DUB.5
Are periods regular? Heavy bleeding with a regular menstrual cycle (ovulatory bleeding) usually has a different etiology. It most often occurs because of anatomic abnormalities such as endometrial polyps, fibroids, and adenomyosis (pockets of endometrium found within the uterine myometrium). Heavy menstrual bleeding that occurs at the onset of or shortly after menarche may be due to a coagulopathy, such as von Willebrand disease. Therefore, consider platelet function analysis for adolescents who present with heavy menses, particularly if they require blood transfusion.
What else do you observe? When evaluating patients with abnormal uterine bleeding, don’t let the obvious focus on the gynecologic organs cause you to overlook other possibly significant findings. Look for acanthosis nigrican and an elevated body mass index (BMI), signs of PCOS, and also check for evidence of hyperthyroidism or galactorrhea. The bimanual exam should determine if the patient has an enlarged uterus, suggesting fibroids or adenomyosis.
TABLE 1
Abnormal uterine bleeding: 4 categories, many causes
| CATEGORY | MOST COMMON TYPE OF BLEEDING | SELECTED CAUSES |
|---|---|---|
| Bleeding associated with uterine pathology | Heavy bleeding, regular cycle (menorrhagia) | Endometrial polyps Adenomyosis Uterine fibroids Endometrial hyperplasia Uterine cancer |
| Dysfunctional uterine bleeding (DUB) without anatomic abnormalities | Heavy bleeding, irregular cycle (menometrorrhagia) | Polycystic ovarian syndrome Hypothalamic dysfunction
|
| Bleeding with a systemic illness | Usually menometrorrhagia | Thyroid dysfunction Elevated prolactin levels Liver or renal disease Coagulopathy Leukemia |
| Iatrogenic bleeding | Usually menometrorrhagia | Oral contraceptives Depot medroxyprogesterone acetate Postmenopausal hormone therapy Anticoagulants Herbal supplements |
Refer for a look inside the uterus
Patients with a pelvic exam that is inconclusive or suggests an enlarged uterus will likely benefit from referral for transvaginal sonography. This procedure is considered by many to be the test of choice for abnormal uterine bleeding.6 Saline infusion vaginal sonography, however, is considered a more sensitive test by some authorities.7 In saline infusion sonography, the clinician infuses a small amount of sterile saline into the uterus via a small catheter, which distends the normally compressed uterine walls and allows visualization of any endometrial cavity abnormalities, such as polyps or fibroids (FIGURE).
Office or outpatient hysteroscopy can also help visualize the endometrial cavity to diagnose cavity defects. Although hysteroscopy is an excellent and usually well-tolerated technique for visualizing the endometrial cavity, it cannot visualize the myometrium or ovaries as saline infusion sonography can. (TABLE 2) details the pros and cons of these diagnostic procedures.
FIGURE
What a difference saline can make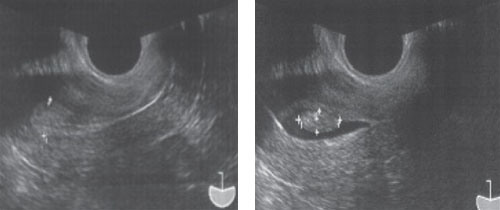
Routine transvaginal sonography shows the endometrium (calipers) without apparent abnormality. A previously undiagnosed endometrial polyp (calipers) in the same patient, revealed after saline infusion.
TABLE 2
Diagnostic studies: The pros, the cons
| STUDY | BENEFITS | POTENTIAL DRAWBACKS |
|---|---|---|
| Transvaginal sonography |
| May miss small or flaccid lesions (polyps) |
| Saline infusion vaginal sonography |
|
|
| Hysteroscopy |
|
|
What’s to be done?
In many cases clinicians can direct a plan of care on the basis of an accurate diagnosis. For example, patients with endometrial polyps or submucous uterine fibroids will benefit from referral to a gynecologist for outpatient surgical intervention. Otherwise, a variety of medical or minimally invasive surgical options are available.
Patients unaware of other options may come in asking about a hysterectomy, the second most common surgical procedure in the United States.8 Although this procedure is the definitive treatment for abnormal uterine bleeding, it carries the risk of surgical bleeding, ureteral or intestinal damage, incision breakdown, venous thromboembolism, and other intra- and postoperative problems.
While it is certainly appropriate to counsel the patient that hysterectomy is an option, there are many other options to consider. We now have a number of randomized trials that provide evidence-based guidance for the management of chronic abnormal uterine bleeding without hysterectomy (TABLE 3). These options can allow the patient to avoid the risks of major surgery and return to work and normal activities more rapidly.
TABLE 3
Beyond hysterectomy: Other treatment options to consider
| TREATMENT | COMMON REGIMENS | SOR | COMMENTS |
|---|---|---|---|
| Combined oral contraceptives9,12 | Cyclic or daily | A, B |
|
| Cyclic progestins9 |
| A | Side effects include spotting, weight gain, nausea, edema, and exacerbation of depression |
| NSAIDs14 | Mefenamic acid (Ponstel) 500 mg orally TID during menses; ibuprofen 800 mg orally TID during menses | A |
|
| Levonorgestrel IUS9,10 | Device provides 20 mcg/24 hours continuously for 5 years | A |
|
| Global endometrial ablation15,16 | Office or outpatient procedure | A |
|
| IUS, intrauterine system; NSAID, nonsteroidal anti-inflammatory drug. | |||
| Strength of recommendation (SOR) A. Good-quality patient-oriented evidence | |||
First choice: LNG-IUS
The levonorgestrel intrauterine system (LNG-IUS) appears to be the most effective medical therapy for treating menorrhagia, with studies showing a 94% reduction in menstrual blood loss.9 The LNG-IUS secretes a small amount of levonorgestrel, which acts locally to keep the endometrium from proliferating. The IUS has not been compared with placebo or no treatment, but it has been found to be more successful than 21-day progestin therapy and somewhat less successful than balloon endometrial ablation.10
An interesting study suggested that women given the choice between an LNG-IUS and hysterectomy will choose the intrauterine system rather than undergo invasive surgery. In this study, researchers randomized 56 women waiting to undergo hysterectomy for heavy menstrual bleeding to either continuation of their existing medical treatment or an LNG-IUS. At 6 months, 64% of the women in the IUS group canceled their hysterectomy, whereas only 14% in the medical therapy group did so.11
IUS candidates should have a uterus free of congenital abnormalities that measures between 6 and 9 centimeters by uterine sound, and be at low risk for sexually transmitted infections. Patients who have never been pregnant may use the LNG-IUS. Side effects of the LNGIUS may include irregular menses, amenorrhea, pelvic inflammatory disease, and uterine perforation at insertion.
Hormonal therapy is another option
Various types of hormonal therapy are also effective options for treating abnormal menstrual bleeding.
Combined oral contraceptives (COCs). Although many clinicians use COCs to treat menorrhagia, data supporting this indication are actually limited.12 COCs are proven to reduce mean menstrual blood loss but have not been well evaluated for patients who complain of heavy menstrual bleeding.9
All COCs contain relatively more progestin than estrogen, which benefits patients with abnormal uterine bleeding by thinning the uterine lining, leading to less menstrual blood loss. Newer types of oral contraceptives, such as lower dose pills or extended cycle formulations where patients take 3 months of pills before having a menstrual cycle, have not been studied for treatment of heavy menstrual bleeding.
Progestin alone. There are several formulations of progestins, including intramuscular injections, oral preparations, vaginal suppositories, creams, and the LNG-IUS. Although there are many potential oral progestin regimens—for example, a 10-day course vs a 21-day course—it appears that the 21-day regimen is most effective. Analysis of several trials shows that bleeding was reduced in 86% of women using a 21-day course of oral progestins.9
Possible side effects include spotting, weight gain, peripheral edema, and exacerbation of depression. Depot-medroxyprogesterone acetate is an injectable progestin that may cause abnormal bleeding or amenorrhea. It has not been studied as a treatment for heavy menstrual bleeding.
Danazol therapy. Danazol is a synthetic steroid that opposes progesterone and estrogen, leading to endometrial atrophy. Although possibly effective for reducing blood loss, danazol has lost favor due to androgenic side effects such as acne, weight gain, and voice deepening.13
NSAIDs reduce bleeding
Although NSAIDs are associated with gastrointestinal bleeding, their effect on uterine bleeding is different. At pharmacologic doses, NSAIDs reduce uterine bleeding. These drugs appear to slow uterine bleeding by helping to constrict the uterine vasculature, reduce prostaglandins, and improve platelet aggregation.14 Several studies show successful use of NSAIDs for abnormal uterine bleeding. A meta-analysis of NSAID therapy concluded that about half of the menorrhagia patients studied benefitted, and these patients had about a 30% reduction in blood loss.9 Mefenamic acid (Ponstel) is the only NSAID currently approved by the US Food and Drug Administration for treating menorrhagia, although all NSAIDs are likely effective.
Consider minimally invasive surgery
The term global endometrial ablation refers to a group of minimally invasive, outpatient procedures designed to destroy the endometrial lining, leading to either reduced bleeding or amenorrhea. These procedures are less invasive than hysterectomy and are best suited for patients with abnormal uterine bleeding who do not have other uterine abnormalities, such as prolapse, dyspareunia, or painful fibroids.
Examples of global ablation procedures include microwave ablation, cryotherapy, thermal balloon ablation, bipolar radiofrequency ablation, and hydrothermal ablation. Some OB/GYNs perform these procedures in the office.
Ablation procedures have some drawbacks. None of the ablation procedures can guarantee complete amenorrhea. Published amenorrhea rates range from 14% to 55%.15 Outpatient ablation procedures are relatively fast (usually under 1 hour) and allow the patient to return to normal activity quickly. There is also a cost advantage: endometrial ablation may be 80% less expensive than hysterectomy.
Not all patients who undergo these procedures remain satisfied with the outcome, however. One study concluded that some patients undergoing hysterectomy were more satisfied after 4 years than those who had an endometrial ablation. Thus, you should counsel patients that they may need to return later for more definitive therapy.16 In addition, because the uterine environment after ablation is not hospitable to fetal development, you’ll want to caution patients that future childbearing is contraindicated and advise them to undergo some type of permanent sterilization procedure.
Uterine artery embolization (UAE). This interventional radiology technique uses embolic particles placed via the femoral artery to occlude the blood supply to the uterine arteries. The procedure is most commonly used to treat heavy bleeding from uterine fibroids, gynecologic malignancies, or postpartum hemorrhage. Although useful for treating heavy menstrual bleeding from uterine fibroids, this technique has not been fully evaluated as a treatment option for heavy menstrual bleeding caused by other disorders.17
Ms. M keeps her uterus
Because Ms. M is older than 35, your first step is a brief, office endometrial pipelle biopsy. The results indicate a benign, proliferative endometrium. You discuss the various treatment options with your patient, and she decides on an LNG-IUS. Her urine pregnancy test is negative, and you place the IUS uneventfully on the last day of her next menses.
Five months later she has amenorrhea, except for rare spotting, and is symptom-free. Her hemoglobin returns to normal levels using oral iron therapy. She is extremely pleased that she was finally able to get some relief without disrupting her busy schedule or undergoing major surgery.
Correspondence
D. Ashley Hill, MD, Associate Director, Dept. of Obstetrics and Gynecology, Florida Hospital Orlando & Loch Haven OB/Gyn Group, 235 Princeton Street, Suite 200, Orlando, FL 32804; d.ashley.hill.md.flhosp.org
1. Nicholson WK, Ellison SA, Grason H, et al. Patterns of ambulatory care use for gynecologic conditions: a national study. Am J Obstet Gynecol. 2001;184:523-530.
2. Wilcox A, Baird DD, Dunson D, et al. Natural limits of pregnancy testing in relation to the expected menstrual period. JAMA. 2001;286:1759-1761.
3. Ely JW, Kennedy CM, Clark EC, et al. Abnormal uterine bleeding: a management algorithm. J Am Board Fam Med. 2006;19:590-602.
4. Dijkhuizen F, Mol B, Brölmann H, et al. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia—a meta-analysis. Cancer. 2000;89:1765-1762.
5. Bayer SR, DeCherney AH. Clinical manifestations and treatment of dysfunctional uterine bleeding. JAMA. 1993;269:1823-1828.
6. Oehler MK, Rees MC. Menorrhagia: an update. Acta Obstet Gynecol Scand. 2003;82:405-422.
7. Hill DA. Abnormal uterine bleeding. In: Henningsen C, ed. Clinical Guide to Ultrasonography. St. Louis, Mo: Mosby; 2004:173-196.
8. Keshavarz H, Hillis SD, Kieke BA, et al. Hysterectomy surveillance—United States, 1994–1999. MMWR CDC Surveill Summ. 2002;51(SS-5):1-8.
9. Working Party for Guidelines for the Management of Heavy Menstrual Bleeding. An evidence-based guideline for the management of heavy menstrual bleeding. N Z Med J. 1999;112:174-177.
10. Lethaby AE, Cooke I, Rees M. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev. 2005;(4):CD002126.-
11. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of levonorgestrel releasing intrauterine system as alternative to hysterectomy. BMJ. 1998;316:1122-1126.
12. American College of Obstetricians and Gynecologists (ACOG). Management of anovulatory bleeding. Washington, DC: ACOG; 2000 Mar. 9. ACOG practice bulletin; no. 14.
13. Beaumont H, Augood C, Duckitt K, et al. Danazol for heavy menstrual bleeding. Cochrane Database Syst Rev. 2007;(3):CD001017.-
14. Dawood MY. Nonsteroidal antiinflammatory drugs and reproduction. Am J Obstet Gynecol. 1993;169:1255-1265.
15. Sharp HT. Assessment of new technology in the treatment of idiopathic menorrhagia and uterine leiomyomata. Obstet Gynecol. 2006;108:990-1003.
16. Lethaby A, Shepperd S, Cooke I, et al. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev. 2000;(2):CD000329.-
17. Pron G, Bennett J, Common A, et al. The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril. 2003;79:120-127.
- The levonorgestrel-IUS is the most effective treatment for heavy menstrual bleeding, reducing blood loss by close to 100% (A).
- Endometrial ablation is an effective treatment for women who want to avoid major surgery and preserve their uterus, but have no wish to become pregnant in the future (A).
- Endometrial biopsy should be part of the evaluation of abnormal uterine bleeding in all women over age 35 (B).
Strength of recommendation (SOR)
A. Good-quality patient-oriented evidence
B. Inconsistent or limited-quality patient-oriented evidence
C. Consensus, usual practice, opinion, disease-oriented evidence, case series
Ms. M, a 39-year-old mother of 3, runs a busy day-care center, cares for her sick mother, and shuttles her children among their myriad activities. During today’s office visit, she seems anxious. She says her periods are regular, but have become increasingly heavy in recent years and may last as long as 9 days. The bleeding is very heavy, with a lot of clots and some cramps during the first few days. In the past year, painful periods have caused her to miss work on several occasions. She says she often feels tired, and worries that she may be anemic. Preserving fertility is not a concern; her husband has had a vasectomy.
On exam she is without orthostasis and appears well. Her uterus is top-normal size, nontender, and there are no adnexal masses or cervical or vaginal abnormalities. You note a normal Pap at your office 5 months ago. Her office hemoglobin is 9.8 mg/dL.
She asks you to refer her to a gynecologist for a hysterectomy because she “just can’t take it anymore.” Her heavy menses are disrupting her life. Since she does not want any more children, she feels that if someone could “just take it out,” her problem would be solved. But she isn’t really enthusiastic about a hysterectomy because her life is too busy to allow time for a lengthy recovery.
You explain that there are a number of options you’d like her to consider first. Then you review the options and some of the research behind them, having recently read an article on evidence-based therapy for abnormal uterine bleeding.
A common complaint in primary care
Abnormal uterine bleeding is a common reason for women to visit their primary care clinician, accounting for about 20% of gynecologic primary care visits.1 Women are understandably concerned about any disruption of their normal bleeding pattern. Many, however, are unaware of common causes of abnormal bleeding and available treatment options.
Most cases of chronic abnormal bleeding can be classified as either heavy and regular (menorrhagia) or heavy and irregular (menometrorrhagia). A rule of thumb to help guide diagnostic testing is that menorrhagia often results from anatomic problems of the uterus or endometrium, such as polyps. Menometrorrhagia is more likely to result from hormonal abnormalities, such as polycystic ovarian syndrome (PCOS). This review will focus on medical and minimally invasive surgical therapy for chronic abnormal bleeding.
First step: Pregnancy test
Many conditions can cause abnormal uterine bleeding (TABLE 1). In women of reproductive age, the first step in the diagnostic process should be a urine or serum pregnancy test. Urine pregnancy tests have a sensitivity of 90% one day after a missed period and approximately 97% after one week.2 In addition to a pregnancy test, consider testing for thyroid dysfunction and obtaining serum prolactin levels for women presenting with anovulatory bleeding.3 If anemia is suspected, a hematocrit or hemogram is indicated. All patients over the age of 35 who present with abnormal uterine bleeding should have an office endometrial biopsy to rule out endometrial hyperplasia or cancer.4
Is she ovulating? Most cases of heavy bleeding with irregular periods are the result of anovulation, which is common soon after menarche and at the approach of menopause. Other causes of anovulatory bleeding include PCOS, hypothyroidism, and elevated prolactin levels. Chronic, irregular bleeding without a known anatomic cause is termed “dysfunctional uterine bleeding,” or DUB.5
Are periods regular? Heavy bleeding with a regular menstrual cycle (ovulatory bleeding) usually has a different etiology. It most often occurs because of anatomic abnormalities such as endometrial polyps, fibroids, and adenomyosis (pockets of endometrium found within the uterine myometrium). Heavy menstrual bleeding that occurs at the onset of or shortly after menarche may be due to a coagulopathy, such as von Willebrand disease. Therefore, consider platelet function analysis for adolescents who present with heavy menses, particularly if they require blood transfusion.
What else do you observe? When evaluating patients with abnormal uterine bleeding, don’t let the obvious focus on the gynecologic organs cause you to overlook other possibly significant findings. Look for acanthosis nigrican and an elevated body mass index (BMI), signs of PCOS, and also check for evidence of hyperthyroidism or galactorrhea. The bimanual exam should determine if the patient has an enlarged uterus, suggesting fibroids or adenomyosis.
TABLE 1
Abnormal uterine bleeding: 4 categories, many causes
| CATEGORY | MOST COMMON TYPE OF BLEEDING | SELECTED CAUSES |
|---|---|---|
| Bleeding associated with uterine pathology | Heavy bleeding, regular cycle (menorrhagia) | Endometrial polyps Adenomyosis Uterine fibroids Endometrial hyperplasia Uterine cancer |
| Dysfunctional uterine bleeding (DUB) without anatomic abnormalities | Heavy bleeding, irregular cycle (menometrorrhagia) | Polycystic ovarian syndrome Hypothalamic dysfunction
|
| Bleeding with a systemic illness | Usually menometrorrhagia | Thyroid dysfunction Elevated prolactin levels Liver or renal disease Coagulopathy Leukemia |
| Iatrogenic bleeding | Usually menometrorrhagia | Oral contraceptives Depot medroxyprogesterone acetate Postmenopausal hormone therapy Anticoagulants Herbal supplements |
Refer for a look inside the uterus
Patients with a pelvic exam that is inconclusive or suggests an enlarged uterus will likely benefit from referral for transvaginal sonography. This procedure is considered by many to be the test of choice for abnormal uterine bleeding.6 Saline infusion vaginal sonography, however, is considered a more sensitive test by some authorities.7 In saline infusion sonography, the clinician infuses a small amount of sterile saline into the uterus via a small catheter, which distends the normally compressed uterine walls and allows visualization of any endometrial cavity abnormalities, such as polyps or fibroids (FIGURE).
Office or outpatient hysteroscopy can also help visualize the endometrial cavity to diagnose cavity defects. Although hysteroscopy is an excellent and usually well-tolerated technique for visualizing the endometrial cavity, it cannot visualize the myometrium or ovaries as saline infusion sonography can. (TABLE 2) details the pros and cons of these diagnostic procedures.
FIGURE
What a difference saline can make
Routine transvaginal sonography shows the endometrium (calipers) without apparent abnormality. A previously undiagnosed endometrial polyp (calipers) in the same patient, revealed after saline infusion.
TABLE 2
Diagnostic studies: The pros, the cons
| STUDY | BENEFITS | POTENTIAL DRAWBACKS |
|---|---|---|
| Transvaginal sonography |
| May miss small or flaccid lesions (polyps) |
| Saline infusion vaginal sonography |
|
|
| Hysteroscopy |
|
|
What’s to be done?
In many cases clinicians can direct a plan of care on the basis of an accurate diagnosis. For example, patients with endometrial polyps or submucous uterine fibroids will benefit from referral to a gynecologist for outpatient surgical intervention. Otherwise, a variety of medical or minimally invasive surgical options are available.
Patients unaware of other options may come in asking about a hysterectomy, the second most common surgical procedure in the United States.8 Although this procedure is the definitive treatment for abnormal uterine bleeding, it carries the risk of surgical bleeding, ureteral or intestinal damage, incision breakdown, venous thromboembolism, and other intra- and postoperative problems.
While it is certainly appropriate to counsel the patient that hysterectomy is an option, there are many other options to consider. We now have a number of randomized trials that provide evidence-based guidance for the management of chronic abnormal uterine bleeding without hysterectomy (TABLE 3). These options can allow the patient to avoid the risks of major surgery and return to work and normal activities more rapidly.
TABLE 3
Beyond hysterectomy: Other treatment options to consider
| TREATMENT | COMMON REGIMENS | SOR | COMMENTS |
|---|---|---|---|
| Combined oral contraceptives9,12 | Cyclic or daily | A, B |
|
| Cyclic progestins9 |
| A | Side effects include spotting, weight gain, nausea, edema, and exacerbation of depression |
| NSAIDs14 | Mefenamic acid (Ponstel) 500 mg orally TID during menses; ibuprofen 800 mg orally TID during menses | A |
|
| Levonorgestrel IUS9,10 | Device provides 20 mcg/24 hours continuously for 5 years | A |
|
| Global endometrial ablation15,16 | Office or outpatient procedure | A |
|
| IUS, intrauterine system; NSAID, nonsteroidal anti-inflammatory drug. | |||
| Strength of recommendation (SOR) A. Good-quality patient-oriented evidence | |||
First choice: LNG-IUS
The levonorgestrel intrauterine system (LNG-IUS) appears to be the most effective medical therapy for treating menorrhagia, with studies showing a 94% reduction in menstrual blood loss.9 The LNG-IUS secretes a small amount of levonorgestrel, which acts locally to keep the endometrium from proliferating. The IUS has not been compared with placebo or no treatment, but it has been found to be more successful than 21-day progestin therapy and somewhat less successful than balloon endometrial ablation.10
An interesting study suggested that women given the choice between an LNG-IUS and hysterectomy will choose the intrauterine system rather than undergo invasive surgery. In this study, researchers randomized 56 women waiting to undergo hysterectomy for heavy menstrual bleeding to either continuation of their existing medical treatment or an LNG-IUS. At 6 months, 64% of the women in the IUS group canceled their hysterectomy, whereas only 14% in the medical therapy group did so.11
IUS candidates should have a uterus free of congenital abnormalities that measures between 6 and 9 centimeters by uterine sound, and be at low risk for sexually transmitted infections. Patients who have never been pregnant may use the LNG-IUS. Side effects of the LNGIUS may include irregular menses, amenorrhea, pelvic inflammatory disease, and uterine perforation at insertion.
Hormonal therapy is another option
Various types of hormonal therapy are also effective options for treating abnormal menstrual bleeding.
Combined oral contraceptives (COCs). Although many clinicians use COCs to treat menorrhagia, data supporting this indication are actually limited.12 COCs are proven to reduce mean menstrual blood loss but have not been well evaluated for patients who complain of heavy menstrual bleeding.9
All COCs contain relatively more progestin than estrogen, which benefits patients with abnormal uterine bleeding by thinning the uterine lining, leading to less menstrual blood loss. Newer types of oral contraceptives, such as lower dose pills or extended cycle formulations where patients take 3 months of pills before having a menstrual cycle, have not been studied for treatment of heavy menstrual bleeding.
Progestin alone. There are several formulations of progestins, including intramuscular injections, oral preparations, vaginal suppositories, creams, and the LNG-IUS. Although there are many potential oral progestin regimens—for example, a 10-day course vs a 21-day course—it appears that the 21-day regimen is most effective. Analysis of several trials shows that bleeding was reduced in 86% of women using a 21-day course of oral progestins.9
Possible side effects include spotting, weight gain, peripheral edema, and exacerbation of depression. Depot-medroxyprogesterone acetate is an injectable progestin that may cause abnormal bleeding or amenorrhea. It has not been studied as a treatment for heavy menstrual bleeding.
Danazol therapy. Danazol is a synthetic steroid that opposes progesterone and estrogen, leading to endometrial atrophy. Although possibly effective for reducing blood loss, danazol has lost favor due to androgenic side effects such as acne, weight gain, and voice deepening.13
NSAIDs reduce bleeding
Although NSAIDs are associated with gastrointestinal bleeding, their effect on uterine bleeding is different. At pharmacologic doses, NSAIDs reduce uterine bleeding. These drugs appear to slow uterine bleeding by helping to constrict the uterine vasculature, reduce prostaglandins, and improve platelet aggregation.14 Several studies show successful use of NSAIDs for abnormal uterine bleeding. A meta-analysis of NSAID therapy concluded that about half of the menorrhagia patients studied benefitted, and these patients had about a 30% reduction in blood loss.9 Mefenamic acid (Ponstel) is the only NSAID currently approved by the US Food and Drug Administration for treating menorrhagia, although all NSAIDs are likely effective.
Consider minimally invasive surgery
The term global endometrial ablation refers to a group of minimally invasive, outpatient procedures designed to destroy the endometrial lining, leading to either reduced bleeding or amenorrhea. These procedures are less invasive than hysterectomy and are best suited for patients with abnormal uterine bleeding who do not have other uterine abnormalities, such as prolapse, dyspareunia, or painful fibroids.
Examples of global ablation procedures include microwave ablation, cryotherapy, thermal balloon ablation, bipolar radiofrequency ablation, and hydrothermal ablation. Some OB/GYNs perform these procedures in the office.
Ablation procedures have some drawbacks. None of the ablation procedures can guarantee complete amenorrhea. Published amenorrhea rates range from 14% to 55%.15 Outpatient ablation procedures are relatively fast (usually under 1 hour) and allow the patient to return to normal activity quickly. There is also a cost advantage: endometrial ablation may be 80% less expensive than hysterectomy.
Not all patients who undergo these procedures remain satisfied with the outcome, however. One study concluded that some patients undergoing hysterectomy were more satisfied after 4 years than those who had an endometrial ablation. Thus, you should counsel patients that they may need to return later for more definitive therapy.16 In addition, because the uterine environment after ablation is not hospitable to fetal development, you’ll want to caution patients that future childbearing is contraindicated and advise them to undergo some type of permanent sterilization procedure.
Uterine artery embolization (UAE). This interventional radiology technique uses embolic particles placed via the femoral artery to occlude the blood supply to the uterine arteries. The procedure is most commonly used to treat heavy bleeding from uterine fibroids, gynecologic malignancies, or postpartum hemorrhage. Although useful for treating heavy menstrual bleeding from uterine fibroids, this technique has not been fully evaluated as a treatment option for heavy menstrual bleeding caused by other disorders.17
Ms. M keeps her uterus
Because Ms. M is older than 35, your first step is a brief, office endometrial pipelle biopsy. The results indicate a benign, proliferative endometrium. You discuss the various treatment options with your patient, and she decides on an LNG-IUS. Her urine pregnancy test is negative, and you place the IUS uneventfully on the last day of her next menses.
Five months later she has amenorrhea, except for rare spotting, and is symptom-free. Her hemoglobin returns to normal levels using oral iron therapy. She is extremely pleased that she was finally able to get some relief without disrupting her busy schedule or undergoing major surgery.
Correspondence
D. Ashley Hill, MD, Associate Director, Dept. of Obstetrics and Gynecology, Florida Hospital Orlando & Loch Haven OB/Gyn Group, 235 Princeton Street, Suite 200, Orlando, FL 32804; d.ashley.hill.md.flhosp.org
- The levonorgestrel-IUS is the most effective treatment for heavy menstrual bleeding, reducing blood loss by close to 100% (A).
- Endometrial ablation is an effective treatment for women who want to avoid major surgery and preserve their uterus, but have no wish to become pregnant in the future (A).
- Endometrial biopsy should be part of the evaluation of abnormal uterine bleeding in all women over age 35 (B).
Strength of recommendation (SOR)
A. Good-quality patient-oriented evidence
B. Inconsistent or limited-quality patient-oriented evidence
C. Consensus, usual practice, opinion, disease-oriented evidence, case series
Ms. M, a 39-year-old mother of 3, runs a busy day-care center, cares for her sick mother, and shuttles her children among their myriad activities. During today’s office visit, she seems anxious. She says her periods are regular, but have become increasingly heavy in recent years and may last as long as 9 days. The bleeding is very heavy, with a lot of clots and some cramps during the first few days. In the past year, painful periods have caused her to miss work on several occasions. She says she often feels tired, and worries that she may be anemic. Preserving fertility is not a concern; her husband has had a vasectomy.
On exam she is without orthostasis and appears well. Her uterus is top-normal size, nontender, and there are no adnexal masses or cervical or vaginal abnormalities. You note a normal Pap at your office 5 months ago. Her office hemoglobin is 9.8 mg/dL.
She asks you to refer her to a gynecologist for a hysterectomy because she “just can’t take it anymore.” Her heavy menses are disrupting her life. Since she does not want any more children, she feels that if someone could “just take it out,” her problem would be solved. But she isn’t really enthusiastic about a hysterectomy because her life is too busy to allow time for a lengthy recovery.
You explain that there are a number of options you’d like her to consider first. Then you review the options and some of the research behind them, having recently read an article on evidence-based therapy for abnormal uterine bleeding.
A common complaint in primary care
Abnormal uterine bleeding is a common reason for women to visit their primary care clinician, accounting for about 20% of gynecologic primary care visits.1 Women are understandably concerned about any disruption of their normal bleeding pattern. Many, however, are unaware of common causes of abnormal bleeding and available treatment options.
Most cases of chronic abnormal bleeding can be classified as either heavy and regular (menorrhagia) or heavy and irregular (menometrorrhagia). A rule of thumb to help guide diagnostic testing is that menorrhagia often results from anatomic problems of the uterus or endometrium, such as polyps. Menometrorrhagia is more likely to result from hormonal abnormalities, such as polycystic ovarian syndrome (PCOS). This review will focus on medical and minimally invasive surgical therapy for chronic abnormal bleeding.
First step: Pregnancy test
Many conditions can cause abnormal uterine bleeding (TABLE 1). In women of reproductive age, the first step in the diagnostic process should be a urine or serum pregnancy test. Urine pregnancy tests have a sensitivity of 90% one day after a missed period and approximately 97% after one week.2 In addition to a pregnancy test, consider testing for thyroid dysfunction and obtaining serum prolactin levels for women presenting with anovulatory bleeding.3 If anemia is suspected, a hematocrit or hemogram is indicated. All patients over the age of 35 who present with abnormal uterine bleeding should have an office endometrial biopsy to rule out endometrial hyperplasia or cancer.4
Is she ovulating? Most cases of heavy bleeding with irregular periods are the result of anovulation, which is common soon after menarche and at the approach of menopause. Other causes of anovulatory bleeding include PCOS, hypothyroidism, and elevated prolactin levels. Chronic, irregular bleeding without a known anatomic cause is termed “dysfunctional uterine bleeding,” or DUB.5
Are periods regular? Heavy bleeding with a regular menstrual cycle (ovulatory bleeding) usually has a different etiology. It most often occurs because of anatomic abnormalities such as endometrial polyps, fibroids, and adenomyosis (pockets of endometrium found within the uterine myometrium). Heavy menstrual bleeding that occurs at the onset of or shortly after menarche may be due to a coagulopathy, such as von Willebrand disease. Therefore, consider platelet function analysis for adolescents who present with heavy menses, particularly if they require blood transfusion.
What else do you observe? When evaluating patients with abnormal uterine bleeding, don’t let the obvious focus on the gynecologic organs cause you to overlook other possibly significant findings. Look for acanthosis nigrican and an elevated body mass index (BMI), signs of PCOS, and also check for evidence of hyperthyroidism or galactorrhea. The bimanual exam should determine if the patient has an enlarged uterus, suggesting fibroids or adenomyosis.
TABLE 1
Abnormal uterine bleeding: 4 categories, many causes
| CATEGORY | MOST COMMON TYPE OF BLEEDING | SELECTED CAUSES |
|---|---|---|
| Bleeding associated with uterine pathology | Heavy bleeding, regular cycle (menorrhagia) | Endometrial polyps Adenomyosis Uterine fibroids Endometrial hyperplasia Uterine cancer |
| Dysfunctional uterine bleeding (DUB) without anatomic abnormalities | Heavy bleeding, irregular cycle (menometrorrhagia) | Polycystic ovarian syndrome Hypothalamic dysfunction
|
| Bleeding with a systemic illness | Usually menometrorrhagia | Thyroid dysfunction Elevated prolactin levels Liver or renal disease Coagulopathy Leukemia |
| Iatrogenic bleeding | Usually menometrorrhagia | Oral contraceptives Depot medroxyprogesterone acetate Postmenopausal hormone therapy Anticoagulants Herbal supplements |
Refer for a look inside the uterus
Patients with a pelvic exam that is inconclusive or suggests an enlarged uterus will likely benefit from referral for transvaginal sonography. This procedure is considered by many to be the test of choice for abnormal uterine bleeding.6 Saline infusion vaginal sonography, however, is considered a more sensitive test by some authorities.7 In saline infusion sonography, the clinician infuses a small amount of sterile saline into the uterus via a small catheter, which distends the normally compressed uterine walls and allows visualization of any endometrial cavity abnormalities, such as polyps or fibroids (FIGURE).
Office or outpatient hysteroscopy can also help visualize the endometrial cavity to diagnose cavity defects. Although hysteroscopy is an excellent and usually well-tolerated technique for visualizing the endometrial cavity, it cannot visualize the myometrium or ovaries as saline infusion sonography can. (TABLE 2) details the pros and cons of these diagnostic procedures.
FIGURE
What a difference saline can make
Routine transvaginal sonography shows the endometrium (calipers) without apparent abnormality. A previously undiagnosed endometrial polyp (calipers) in the same patient, revealed after saline infusion.
TABLE 2
Diagnostic studies: The pros, the cons
| STUDY | BENEFITS | POTENTIAL DRAWBACKS |
|---|---|---|
| Transvaginal sonography |
| May miss small or flaccid lesions (polyps) |
| Saline infusion vaginal sonography |
|
|
| Hysteroscopy |
|
|
What’s to be done?
In many cases clinicians can direct a plan of care on the basis of an accurate diagnosis. For example, patients with endometrial polyps or submucous uterine fibroids will benefit from referral to a gynecologist for outpatient surgical intervention. Otherwise, a variety of medical or minimally invasive surgical options are available.
Patients unaware of other options may come in asking about a hysterectomy, the second most common surgical procedure in the United States.8 Although this procedure is the definitive treatment for abnormal uterine bleeding, it carries the risk of surgical bleeding, ureteral or intestinal damage, incision breakdown, venous thromboembolism, and other intra- and postoperative problems.
While it is certainly appropriate to counsel the patient that hysterectomy is an option, there are many other options to consider. We now have a number of randomized trials that provide evidence-based guidance for the management of chronic abnormal uterine bleeding without hysterectomy (TABLE 3). These options can allow the patient to avoid the risks of major surgery and return to work and normal activities more rapidly.
TABLE 3
Beyond hysterectomy: Other treatment options to consider
| TREATMENT | COMMON REGIMENS | SOR | COMMENTS |
|---|---|---|---|
| Combined oral contraceptives9,12 | Cyclic or daily | A, B |
|
| Cyclic progestins9 |
| A | Side effects include spotting, weight gain, nausea, edema, and exacerbation of depression |
| NSAIDs14 | Mefenamic acid (Ponstel) 500 mg orally TID during menses; ibuprofen 800 mg orally TID during menses | A |
|
| Levonorgestrel IUS9,10 | Device provides 20 mcg/24 hours continuously for 5 years | A |
|
| Global endometrial ablation15,16 | Office or outpatient procedure | A |
|
| IUS, intrauterine system; NSAID, nonsteroidal anti-inflammatory drug. | |||
| Strength of recommendation (SOR) A. Good-quality patient-oriented evidence | |||
First choice: LNG-IUS
The levonorgestrel intrauterine system (LNG-IUS) appears to be the most effective medical therapy for treating menorrhagia, with studies showing a 94% reduction in menstrual blood loss.9 The LNG-IUS secretes a small amount of levonorgestrel, which acts locally to keep the endometrium from proliferating. The IUS has not been compared with placebo or no treatment, but it has been found to be more successful than 21-day progestin therapy and somewhat less successful than balloon endometrial ablation.10
An interesting study suggested that women given the choice between an LNG-IUS and hysterectomy will choose the intrauterine system rather than undergo invasive surgery. In this study, researchers randomized 56 women waiting to undergo hysterectomy for heavy menstrual bleeding to either continuation of their existing medical treatment or an LNG-IUS. At 6 months, 64% of the women in the IUS group canceled their hysterectomy, whereas only 14% in the medical therapy group did so.11
IUS candidates should have a uterus free of congenital abnormalities that measures between 6 and 9 centimeters by uterine sound, and be at low risk for sexually transmitted infections. Patients who have never been pregnant may use the LNG-IUS. Side effects of the LNGIUS may include irregular menses, amenorrhea, pelvic inflammatory disease, and uterine perforation at insertion.
Hormonal therapy is another option
Various types of hormonal therapy are also effective options for treating abnormal menstrual bleeding.
Combined oral contraceptives (COCs). Although many clinicians use COCs to treat menorrhagia, data supporting this indication are actually limited.12 COCs are proven to reduce mean menstrual blood loss but have not been well evaluated for patients who complain of heavy menstrual bleeding.9
All COCs contain relatively more progestin than estrogen, which benefits patients with abnormal uterine bleeding by thinning the uterine lining, leading to less menstrual blood loss. Newer types of oral contraceptives, such as lower dose pills or extended cycle formulations where patients take 3 months of pills before having a menstrual cycle, have not been studied for treatment of heavy menstrual bleeding.
Progestin alone. There are several formulations of progestins, including intramuscular injections, oral preparations, vaginal suppositories, creams, and the LNG-IUS. Although there are many potential oral progestin regimens—for example, a 10-day course vs a 21-day course—it appears that the 21-day regimen is most effective. Analysis of several trials shows that bleeding was reduced in 86% of women using a 21-day course of oral progestins.9
Possible side effects include spotting, weight gain, peripheral edema, and exacerbation of depression. Depot-medroxyprogesterone acetate is an injectable progestin that may cause abnormal bleeding or amenorrhea. It has not been studied as a treatment for heavy menstrual bleeding.
Danazol therapy. Danazol is a synthetic steroid that opposes progesterone and estrogen, leading to endometrial atrophy. Although possibly effective for reducing blood loss, danazol has lost favor due to androgenic side effects such as acne, weight gain, and voice deepening.13
NSAIDs reduce bleeding
Although NSAIDs are associated with gastrointestinal bleeding, their effect on uterine bleeding is different. At pharmacologic doses, NSAIDs reduce uterine bleeding. These drugs appear to slow uterine bleeding by helping to constrict the uterine vasculature, reduce prostaglandins, and improve platelet aggregation.14 Several studies show successful use of NSAIDs for abnormal uterine bleeding. A meta-analysis of NSAID therapy concluded that about half of the menorrhagia patients studied benefitted, and these patients had about a 30% reduction in blood loss.9 Mefenamic acid (Ponstel) is the only NSAID currently approved by the US Food and Drug Administration for treating menorrhagia, although all NSAIDs are likely effective.
Consider minimally invasive surgery
The term global endometrial ablation refers to a group of minimally invasive, outpatient procedures designed to destroy the endometrial lining, leading to either reduced bleeding or amenorrhea. These procedures are less invasive than hysterectomy and are best suited for patients with abnormal uterine bleeding who do not have other uterine abnormalities, such as prolapse, dyspareunia, or painful fibroids.
Examples of global ablation procedures include microwave ablation, cryotherapy, thermal balloon ablation, bipolar radiofrequency ablation, and hydrothermal ablation. Some OB/GYNs perform these procedures in the office.
Ablation procedures have some drawbacks. None of the ablation procedures can guarantee complete amenorrhea. Published amenorrhea rates range from 14% to 55%.15 Outpatient ablation procedures are relatively fast (usually under 1 hour) and allow the patient to return to normal activity quickly. There is also a cost advantage: endometrial ablation may be 80% less expensive than hysterectomy.
Not all patients who undergo these procedures remain satisfied with the outcome, however. One study concluded that some patients undergoing hysterectomy were more satisfied after 4 years than those who had an endometrial ablation. Thus, you should counsel patients that they may need to return later for more definitive therapy.16 In addition, because the uterine environment after ablation is not hospitable to fetal development, you’ll want to caution patients that future childbearing is contraindicated and advise them to undergo some type of permanent sterilization procedure.
Uterine artery embolization (UAE). This interventional radiology technique uses embolic particles placed via the femoral artery to occlude the blood supply to the uterine arteries. The procedure is most commonly used to treat heavy bleeding from uterine fibroids, gynecologic malignancies, or postpartum hemorrhage. Although useful for treating heavy menstrual bleeding from uterine fibroids, this technique has not been fully evaluated as a treatment option for heavy menstrual bleeding caused by other disorders.17
Ms. M keeps her uterus
Because Ms. M is older than 35, your first step is a brief, office endometrial pipelle biopsy. The results indicate a benign, proliferative endometrium. You discuss the various treatment options with your patient, and she decides on an LNG-IUS. Her urine pregnancy test is negative, and you place the IUS uneventfully on the last day of her next menses.
Five months later she has amenorrhea, except for rare spotting, and is symptom-free. Her hemoglobin returns to normal levels using oral iron therapy. She is extremely pleased that she was finally able to get some relief without disrupting her busy schedule or undergoing major surgery.
Correspondence
D. Ashley Hill, MD, Associate Director, Dept. of Obstetrics and Gynecology, Florida Hospital Orlando & Loch Haven OB/Gyn Group, 235 Princeton Street, Suite 200, Orlando, FL 32804; d.ashley.hill.md.flhosp.org
1. Nicholson WK, Ellison SA, Grason H, et al. Patterns of ambulatory care use for gynecologic conditions: a national study. Am J Obstet Gynecol. 2001;184:523-530.
2. Wilcox A, Baird DD, Dunson D, et al. Natural limits of pregnancy testing in relation to the expected menstrual period. JAMA. 2001;286:1759-1761.
3. Ely JW, Kennedy CM, Clark EC, et al. Abnormal uterine bleeding: a management algorithm. J Am Board Fam Med. 2006;19:590-602.
4. Dijkhuizen F, Mol B, Brölmann H, et al. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia—a meta-analysis. Cancer. 2000;89:1765-1762.
5. Bayer SR, DeCherney AH. Clinical manifestations and treatment of dysfunctional uterine bleeding. JAMA. 1993;269:1823-1828.
6. Oehler MK, Rees MC. Menorrhagia: an update. Acta Obstet Gynecol Scand. 2003;82:405-422.
7. Hill DA. Abnormal uterine bleeding. In: Henningsen C, ed. Clinical Guide to Ultrasonography. St. Louis, Mo: Mosby; 2004:173-196.
8. Keshavarz H, Hillis SD, Kieke BA, et al. Hysterectomy surveillance—United States, 1994–1999. MMWR CDC Surveill Summ. 2002;51(SS-5):1-8.
9. Working Party for Guidelines for the Management of Heavy Menstrual Bleeding. An evidence-based guideline for the management of heavy menstrual bleeding. N Z Med J. 1999;112:174-177.
10. Lethaby AE, Cooke I, Rees M. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev. 2005;(4):CD002126.-
11. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of levonorgestrel releasing intrauterine system as alternative to hysterectomy. BMJ. 1998;316:1122-1126.
12. American College of Obstetricians and Gynecologists (ACOG). Management of anovulatory bleeding. Washington, DC: ACOG; 2000 Mar. 9. ACOG practice bulletin; no. 14.
13. Beaumont H, Augood C, Duckitt K, et al. Danazol for heavy menstrual bleeding. Cochrane Database Syst Rev. 2007;(3):CD001017.-
14. Dawood MY. Nonsteroidal antiinflammatory drugs and reproduction. Am J Obstet Gynecol. 1993;169:1255-1265.
15. Sharp HT. Assessment of new technology in the treatment of idiopathic menorrhagia and uterine leiomyomata. Obstet Gynecol. 2006;108:990-1003.
16. Lethaby A, Shepperd S, Cooke I, et al. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev. 2000;(2):CD000329.-
17. Pron G, Bennett J, Common A, et al. The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril. 2003;79:120-127.
1. Nicholson WK, Ellison SA, Grason H, et al. Patterns of ambulatory care use for gynecologic conditions: a national study. Am J Obstet Gynecol. 2001;184:523-530.
2. Wilcox A, Baird DD, Dunson D, et al. Natural limits of pregnancy testing in relation to the expected menstrual period. JAMA. 2001;286:1759-1761.
3. Ely JW, Kennedy CM, Clark EC, et al. Abnormal uterine bleeding: a management algorithm. J Am Board Fam Med. 2006;19:590-602.
4. Dijkhuizen F, Mol B, Brölmann H, et al. The accuracy of endometrial sampling in the diagnosis of patients with endometrial carcinoma and hyperplasia—a meta-analysis. Cancer. 2000;89:1765-1762.
5. Bayer SR, DeCherney AH. Clinical manifestations and treatment of dysfunctional uterine bleeding. JAMA. 1993;269:1823-1828.
6. Oehler MK, Rees MC. Menorrhagia: an update. Acta Obstet Gynecol Scand. 2003;82:405-422.
7. Hill DA. Abnormal uterine bleeding. In: Henningsen C, ed. Clinical Guide to Ultrasonography. St. Louis, Mo: Mosby; 2004:173-196.
8. Keshavarz H, Hillis SD, Kieke BA, et al. Hysterectomy surveillance—United States, 1994–1999. MMWR CDC Surveill Summ. 2002;51(SS-5):1-8.
9. Working Party for Guidelines for the Management of Heavy Menstrual Bleeding. An evidence-based guideline for the management of heavy menstrual bleeding. N Z Med J. 1999;112:174-177.
10. Lethaby AE, Cooke I, Rees M. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev. 2005;(4):CD002126.-
11. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of levonorgestrel releasing intrauterine system as alternative to hysterectomy. BMJ. 1998;316:1122-1126.
12. American College of Obstetricians and Gynecologists (ACOG). Management of anovulatory bleeding. Washington, DC: ACOG; 2000 Mar. 9. ACOG practice bulletin; no. 14.
13. Beaumont H, Augood C, Duckitt K, et al. Danazol for heavy menstrual bleeding. Cochrane Database Syst Rev. 2007;(3):CD001017.-
14. Dawood MY. Nonsteroidal antiinflammatory drugs and reproduction. Am J Obstet Gynecol. 1993;169:1255-1265.
15. Sharp HT. Assessment of new technology in the treatment of idiopathic menorrhagia and uterine leiomyomata. Obstet Gynecol. 2006;108:990-1003.
16. Lethaby A, Shepperd S, Cooke I, et al. Endometrial resection and ablation versus hysterectomy for heavy menstrual bleeding. Cochrane Database Syst Rev. 2000;(2):CD000329.-
17. Pron G, Bennett J, Common A, et al. The Ontario Uterine Fibroid Embolization Trial. Part 2. Uterine fibroid reduction and symptom relief after uterine artery embolization for fibroids. Fertil Steril. 2003;79:120-127.