User login
3 alternatives to standard varicose vein treatment
• Discuss minimally invasive procedures with patients considering surgery for treatment of chronic venous insufficiency. Thermal ablation, in particular, has higher success rates than vein stripping. A
• Consider endovenous chemical ablation for treatment of tortuous saphenous tributary varicosities that cannot be treated with thermal ablation. Foamed sclerosant, injected under ultrasound guidance, allows for direct visualization and has equivalent efficacy rates when compared to venous stripping. A
• Pregnancy, active deep vein thrombosis, poor health with limited mobility, and severe peripheral vascular disease are contraindications for both thermal and chemical ablation. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE
Kevin M., a 35-year-old researcher who often works 12- to 14-hour days, is in your office again, following his second trip to the emergency room for bleeding from a protruding varicose vein proximal to his left ankle. He has complained of leg aching and ankle swelling in the past, usually after he’s been on his feet for hours.
A previous ultrasound showed no evidence of deep vein thrombosis (DVT), but did reveal reflux along the left great saphenous vein from the saphenofemoral junction to the ankle. On examination, Kevin’s lower extremity pulses are intact bilaterally, but there are multiple tortuous varicosities branching from the medial thigh to the left medial malleolus, with evidence of hemosiderin hyperpigmentation and dermatitis on the left lower leg. Previous lab studies have been normal, and Kevin has no other chronic conditions. Kevin’s main concern is to minimize “down time” from work, and he asks you about the newer, minimally invasive vein treatments he’s read about on the Internet.
What should you tell him?
Chronic venous insufficiency is a common and costly condition, affecting nearly one-third of the US population.1 While many people mistakenly think of varicose veins primarily as a cosmetic issue, venous insufficiency often results in painful, even debilitating, signs and symptoms—from swelling and aching legs to skin changes that range from stasis dermatitis to open ulceration.
Venous stripping and ambulatory phlebectomy were long considered the primary means of addressing saphenous venous insufficiency,2 and compression therapy with gradient stockings, short stretch bandages, and Unna’s dressings remains a therapeutic cornerstone for every stage of chronic venous disease. Compression has also been shown to dramatically decrease the risk of post-thrombotic syndrome following DVT3 and, when combined with anticoagulation, to prevent DVT after surgery.4
Outcomes of surgical treatment of large varicose veins arising from saphenous truncal vein reflux, however, have historically been poor.5 This is primarily because of neovascularization and residual refluxing veins. Average failure rates of 25% for saphenous vein stripping and 43% for saphenofemoral junction ligation have been reported.6 A subsequent study of 140 patients who underwent saphenous vein stripping found that 20% experienced neovascularization.7
In the last decade, a number of minimally invasive procedures have been developed and tested, giving physicians and their patients more choices for medical management of venous insufficiency. A closer look at 3 procedures, which include 2 types of thermal ablation, will help you direct patients like Kevin to the best possible treatment.
2 thermal ablation procedures use only local anesthesia
Collectively termed endovenous thermal ablation (EVTA), radiofrequency ablation (RFA) and endovenous laser treatment (ELT) are similar. Performed under duplex ultrasound visualization, both offer a number of benefits.
Outpatient treatment. EVTA procedures are typically done on an outpatient basis, with only local anesthesia—0.05% to 0.1% lidocaine, injected as a perivenous tumescent solution under ultrasound guidance.8,9 The physician places and advances an endovenous catheter (for RFA) or a laser fiber (for ELT) into the vein (FIGURE 1). When the catheter or laser is in proper position, the RF generator or laser is activated. Heat, delivered through the tip of the catheter or fiber, ablates the lumen of the vein as the physician withdraws the catheter.
Mild side effects. Temporary discomfort is common with EVTA. Mild bruising, swelling, and nodularity of the treated veins are the most frequent side effects. More serious adverse effects, including skin burns, paresthesias, DVT, and pulmonary embolism, are rare.10-12
High success rates. Successful treatment of both the great and small saphenous veins and long-term maintenance of vein closure are the norm, with rates ranging from 88% to 100% for both RFA13,14 and ELT, regardless of vein size.15-19 Thermal ablation has been shown to be superior to surgery in other ways as well, eliminating the need for general anesthesia and inpatient treatment and resulting in less postoperative pain, a shorter recovery period, an improved quality of life, and lower costs (TABLE).20-23
TABLE
Endovenous thermal ablation vs standard surgery
| Outcomes | |||||
|---|---|---|---|---|---|
| Study | Type | Modalities studied | Follow-up | Return to work | Pain |
| Rautio et al20 | RCT | RFA vs stripping | 8 weeks | Earlier with RFA | Less with RFA |
| Lurie et al21 | RCT | RFA vs stripping | 2 years | N/A | Less with RFA |
| Hinchcliffe et al22 | RCT | RFA vs stripping | 1 year | N/A | Less with RFA |
| Darwood et al23 | RCT | ELT vs stripping | 3 months | Earlier with ELT | Less with ELT |
| ELT, endovenous laser treatment; NA, not available; RCT, randomized controlled trial; RFA, radiofrequency ablation. | |||||
FIGURE 1
Endovenous laser treatment
In preparation for thermal ablation, the physician (A) places a laser catheter tip into the vein and (B) injects perivenous tumescent anesthesia, guided by duplex ultrasound. The laser tip shown here (C) is in the region of the saphenofemoral junction.
Not for every patient
Despite the usefulness of these minimally invasive procedures, RFA and ELT are not always possible. Veins that are tortuous, too small, or too close to the surface of the skin are not well suited for thermal ablation; in some cases, chemical ablation, discussed below, is the only option. However, some conditions—including pregnancy, active DVT, poor health status with limited mobility, and severe peripheral vascular disease—are contraindications for both thermal and chemical ablation.24
Thermal won’t work? Consider chemical ablation
Endovenous chemoablation (ECA), like thermal ablation, is performed on an outpatient basis without sedation. Hypertonic saline, an osmotic agent, has been used for decades in treating small-caliber varicose veins, or “spider veins.” Detergenttype sclerosants, which we’ll discuss here, are now widely used to treat larger veins, including the great and small saphenous vein trunks and their affected tributaries.
Better suited for tortuous veins. Patients who have had prior stripping often have branches that are too tortuous to access with thermal ablation. In such cases, ECA is the only option. Those who have never undergone vein stripping often need a combination of thermal and chemical ablation, as well, with ECA reserved for saphenous veins that are inaccessible by RFA or laser.
Foamed sclerosants allow visualization. When mixed through a 3-way stopcock with an inert gas such as room air or carbon dioxide, the detergent-type sclerosants produce a micro-foamed preparation that is echogenic, and allows direct visualization with ultrasound (FIGURE 2). The foam displaces blood from within the vein and promotes contact with the venous endothelium, and intense vasospasm results. The sclerosant foam mixture, which makes it possible to watch the effect (and extent) of the foam as it disperses throughout the target vessel, has enhanced the treatment of larger viscosities.25-26 Pretreatment venous ultrasound mapping—a process in which the patient stands upright while compression is applied to the saphenous veins and their tributaries to test the valves for normal flow—combined with realtime duplex imaging, minimizes the chance of arterial injection, extravasation, and tissue necrosis.25
Serious adverse effects are rare. Hemosiderin hyperpigmentation and pain at the injection site are among the most common side effects of ultrasound-guided sclerotherapy. Serious adverse events, including anaphylaxis, DVT/pulmonary embolus, cutaneous necrosis, transient ischemic attack, and arterial injection, are rare.27
To date, there is only 1 published prospective, randomized study that directly compares foam sclerotherapy with stripping/ligation surgery. The researchers found the results of both treatments to be comparable, but reported that surgery was more expensive than foam sclerotherapy and produced less improvement in quality of life.28 A meta-analysis of treatment for 12,000 limbs concluded that foam sclerotherapy and EVTA were as effective as surgical stripping.29 There are no prospective, randomized studies comparing foam sclerotherapy with thermal ablation.
FIGURE 2
Endovenous chemoablation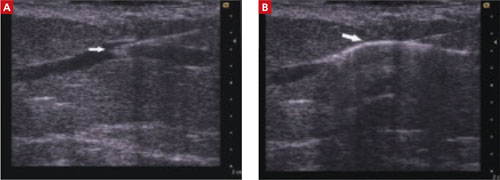
ECA is also conducted under ultrasound guidance: The image at left (A) shows the needle tip inside a refluxing saphenous tributary vein; in the image at right (B), the arrow points to the vein injected with foamed sclerosant.
Advising Kevin M.: What’s his best bet?
You’ve talked to your patient in the past about vein stripping, but he’s been reluctant to undergo surgery. When you describe the minimally invasive approaches to chronic venous insufficiency with him, however, he asks to see a specialist—and to undergo ultrasound mapping.
You give him a prescription for graduated compression stockings for immediate use and a referral to a phlebologist. Soon after, you receive a report from the specialist, indicating that your patient had a combination of ELT of the refluxing left great saphenous vein and subsequent ultrasound-guided ECA of the saphenous tributaries.
The next time you see Kevin, he reports that his leg no longer aches—and you can see that the bulging, tortuous varicosities and swelling have improved significantly.
Acknowledgments
The authors thank John Hickner, MD, MSc, for his input during the manuscript process.
CORRESPONDENCE
Jeffery P. Schoonover, MD, FAAFP, Vein Clinics of America, 9000 Keystone Crossing, Suite 960, Indianapolis, IN 46240; [email protected]
1. McLafferty R, Lohr J, Caprini J, et al. Results of the national pilot screening program for venous disease by the American Venous Forum. J Vasc Surg. 2007;45:142-148.
2. Hagen MD, Johnson ED, Adelman A. What treatments are effective for varicose veins? J Fam Pract. 2003;52:329-331.
3. Partsch H, Flour M, Smith PC. Indications for compression therapy in venous and disease consensus based on experimental data and scientific evidence. Under the auspices of the IUP. Int Angiol. 2008;27:193-219.
4. Partsch H. ed. Evidence-based compression therapy. VASA. 2003;32(suppl 63):S3-S39.
5. Fischer R, Chandler JG, de Maeseneer MG, et al. The unresolved problem of recurrent saphenofemoral reflux. J Am Coll Surg. 2002;195:80-94.
6. Perrin MR. Recurrent varices after surgery (REVAS), a consensus document. Cardiovasc Surg. 2000;8:233-245.
7. Perrin MR, Labropoulos M, Leon L. Presentation of the patient with recurrent varices after surgery (REVAS). J Vasc Surg. 2006;43:327-334.
8. Navarro L, Min R, Boné C. Endovenous laser: a new minimally invasive method of treatment for varicose veins—preliminary observations using an 810 nm diode laser. Dermatol Surg. 2001;27:117-122.
9. Min R, Zimmet S, Isaacs M, et al. Endovenous laser treatment of the incompetent greater saphenous vein. J Vasc Interv Radiol. 2001;12:1167-1171.
10. Mundy L, Merlin TL, Fitridge RA, et al. Systematic review of endovenous laser treatment for varicose veins. Br J Surg. 2005;92:1189-1194.
11. van den Bos RR, Kockaert MA, Neumann HAM, et al. Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008;35:88-95.
12. Proebstle TM, Moehler T, Gul D, et al. Endovenous treatment of the great saphenous vein using a 1320 nm Nd:YAG laser causes fewer side effects than using a 940 nm diode laser. Dermatol Surg. 2005;31:1380-1385.
13. Pichot O, Kabnick LS, Creton D, et al. Duplex ultrasound scan findings two years after great saphenous vein radiofrequency endovenous obliteration. J Vasc Surg. 2004;39:189-195.
14. Merchant RF, Pichot O, Myers KA. Four-year follow-up on endovascular radiofrequency obliteration of great saphenous reflux. Dermatol Surg. 2005;31:129-134.
15. Kabnick LS. Outcome of different endovenous laser wavelengths for great saphenous vein ablation. J Vasc Surg. 2006;43:88-93.
16. Min RJ, Khilnani N, Zimmet SE. Endovenous laser treatment of saphenous vein reflux: long-term results. J Vasc Interv Radiol. 2003;14:991-996.
17. Proebstle TM, Gul D, Kargl A, et al. Endovenous laser treatment of the lesser saphenous vein with a 940-nm diode laser: early results. Dermatol Surg. 2003;29:357-361.
18. Theivacumar NS, Beale RJ, Mavor AID, et al. Initial experience in endovenous laser ablation (EVLA) of varicose veins due to small saphenous vein reflux. Eur J Vasc Endovasc Surg. 2007;33:614-618.
19. Gibson KD, Ferris BL, Polissar N, et al. Endovenous laser treatment of the short saphenous vein: efficacy and complications. J Vasc Surg. 2007;45:795-803.
20. Rautio T, Ohinmaa A, Perala J, et al. Endovenous obliteration versus conventional stripping operation in the treatment of primary varicose veins: a randomized controlled trial with comparison of the costs. J Vasc Surg. 2002;35:958-965.
21. Lurie F, Creton D, Eklof B, et al. Prospective randomised study of endovenous radiofrequency obliteration (closure) versus ligation and vein stripping (EVOLVeS): two-year follow-up. Eur J Vasc Endovasc Surg. 2005;29:67-73.
22. Hinchcliffe RJ, Ubhi J, Beech A, et al. A prospective randomized controlled trial of VNUS closure versus surgery for the treatment of recurrent long saphenous varicose veins. Eur J Vasc Endovasc Surg. 2006;31:212-218.
23. Darwood RJ, Theivacumar N, Dellagrammaticas D, et al. Randomized clinical trial comparing endovenous laser ablation with surgery for the treatment of primary great saphenous varicose veins. Br J Surg. 2008;95:294-301.
24. Sadick NS. Advances in the treatment of varicose veins: ambulatory phlebectomy, foam sclerotherapy, endovascular laser, and radiofrequency closure. Dermatol Clin. 2005;23:443-455.
25. Kakkos SK, Bountouroglou DG, Azzam M, et al. Effectiveness and safety of ultrasound-guided foam sclerotherapy for recurrent varicose veins: immediate results. J Endovasc Ther. 2006;13:357-364.
26. Cabrera J, Cabrera A, Jr, Garcia-Olmedo A. Treatment of varicose long saphenous veins with sclerosant in microfoam form: long-term outcomes. Phlebology. 2000;15:19-23.
27. Jia X, Mowatt G, Burr JM, et al. Systematic review of foam sclerotherapy for varicose veins. Br J Surg. 2007;10:307-1308.
28. Belcaro G, Cesarone MR, Di Renzo A, et al. Foam-sclerotherapy, surgery, sclerotherapy, and combined treatment for varicose veins: a 10-year, prospective, randomized, controlled, trial (VEDICO trial). Angiology. 2003;54:307-315.
29. van den Bos R, Arends L, Kockaert M, et al. Endovenous therapies of lower extremity varicosities: a meta-analysis. J Vasc Surg. 2009;49:230-239.
• Discuss minimally invasive procedures with patients considering surgery for treatment of chronic venous insufficiency. Thermal ablation, in particular, has higher success rates than vein stripping. A
• Consider endovenous chemical ablation for treatment of tortuous saphenous tributary varicosities that cannot be treated with thermal ablation. Foamed sclerosant, injected under ultrasound guidance, allows for direct visualization and has equivalent efficacy rates when compared to venous stripping. A
• Pregnancy, active deep vein thrombosis, poor health with limited mobility, and severe peripheral vascular disease are contraindications for both thermal and chemical ablation. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE
Kevin M., a 35-year-old researcher who often works 12- to 14-hour days, is in your office again, following his second trip to the emergency room for bleeding from a protruding varicose vein proximal to his left ankle. He has complained of leg aching and ankle swelling in the past, usually after he’s been on his feet for hours.
A previous ultrasound showed no evidence of deep vein thrombosis (DVT), but did reveal reflux along the left great saphenous vein from the saphenofemoral junction to the ankle. On examination, Kevin’s lower extremity pulses are intact bilaterally, but there are multiple tortuous varicosities branching from the medial thigh to the left medial malleolus, with evidence of hemosiderin hyperpigmentation and dermatitis on the left lower leg. Previous lab studies have been normal, and Kevin has no other chronic conditions. Kevin’s main concern is to minimize “down time” from work, and he asks you about the newer, minimally invasive vein treatments he’s read about on the Internet.
What should you tell him?
Chronic venous insufficiency is a common and costly condition, affecting nearly one-third of the US population.1 While many people mistakenly think of varicose veins primarily as a cosmetic issue, venous insufficiency often results in painful, even debilitating, signs and symptoms—from swelling and aching legs to skin changes that range from stasis dermatitis to open ulceration.
Venous stripping and ambulatory phlebectomy were long considered the primary means of addressing saphenous venous insufficiency,2 and compression therapy with gradient stockings, short stretch bandages, and Unna’s dressings remains a therapeutic cornerstone for every stage of chronic venous disease. Compression has also been shown to dramatically decrease the risk of post-thrombotic syndrome following DVT3 and, when combined with anticoagulation, to prevent DVT after surgery.4
Outcomes of surgical treatment of large varicose veins arising from saphenous truncal vein reflux, however, have historically been poor.5 This is primarily because of neovascularization and residual refluxing veins. Average failure rates of 25% for saphenous vein stripping and 43% for saphenofemoral junction ligation have been reported.6 A subsequent study of 140 patients who underwent saphenous vein stripping found that 20% experienced neovascularization.7
In the last decade, a number of minimally invasive procedures have been developed and tested, giving physicians and their patients more choices for medical management of venous insufficiency. A closer look at 3 procedures, which include 2 types of thermal ablation, will help you direct patients like Kevin to the best possible treatment.
2 thermal ablation procedures use only local anesthesia
Collectively termed endovenous thermal ablation (EVTA), radiofrequency ablation (RFA) and endovenous laser treatment (ELT) are similar. Performed under duplex ultrasound visualization, both offer a number of benefits.
Outpatient treatment. EVTA procedures are typically done on an outpatient basis, with only local anesthesia—0.05% to 0.1% lidocaine, injected as a perivenous tumescent solution under ultrasound guidance.8,9 The physician places and advances an endovenous catheter (for RFA) or a laser fiber (for ELT) into the vein (FIGURE 1). When the catheter or laser is in proper position, the RF generator or laser is activated. Heat, delivered through the tip of the catheter or fiber, ablates the lumen of the vein as the physician withdraws the catheter.
Mild side effects. Temporary discomfort is common with EVTA. Mild bruising, swelling, and nodularity of the treated veins are the most frequent side effects. More serious adverse effects, including skin burns, paresthesias, DVT, and pulmonary embolism, are rare.10-12
High success rates. Successful treatment of both the great and small saphenous veins and long-term maintenance of vein closure are the norm, with rates ranging from 88% to 100% for both RFA13,14 and ELT, regardless of vein size.15-19 Thermal ablation has been shown to be superior to surgery in other ways as well, eliminating the need for general anesthesia and inpatient treatment and resulting in less postoperative pain, a shorter recovery period, an improved quality of life, and lower costs (TABLE).20-23
TABLE
Endovenous thermal ablation vs standard surgery
| Outcomes | |||||
|---|---|---|---|---|---|
| Study | Type | Modalities studied | Follow-up | Return to work | Pain |
| Rautio et al20 | RCT | RFA vs stripping | 8 weeks | Earlier with RFA | Less with RFA |
| Lurie et al21 | RCT | RFA vs stripping | 2 years | N/A | Less with RFA |
| Hinchcliffe et al22 | RCT | RFA vs stripping | 1 year | N/A | Less with RFA |
| Darwood et al23 | RCT | ELT vs stripping | 3 months | Earlier with ELT | Less with ELT |
| ELT, endovenous laser treatment; NA, not available; RCT, randomized controlled trial; RFA, radiofrequency ablation. | |||||
FIGURE 1
Endovenous laser treatment
In preparation for thermal ablation, the physician (A) places a laser catheter tip into the vein and (B) injects perivenous tumescent anesthesia, guided by duplex ultrasound. The laser tip shown here (C) is in the region of the saphenofemoral junction.
Not for every patient
Despite the usefulness of these minimally invasive procedures, RFA and ELT are not always possible. Veins that are tortuous, too small, or too close to the surface of the skin are not well suited for thermal ablation; in some cases, chemical ablation, discussed below, is the only option. However, some conditions—including pregnancy, active DVT, poor health status with limited mobility, and severe peripheral vascular disease—are contraindications for both thermal and chemical ablation.24
Thermal won’t work? Consider chemical ablation
Endovenous chemoablation (ECA), like thermal ablation, is performed on an outpatient basis without sedation. Hypertonic saline, an osmotic agent, has been used for decades in treating small-caliber varicose veins, or “spider veins.” Detergenttype sclerosants, which we’ll discuss here, are now widely used to treat larger veins, including the great and small saphenous vein trunks and their affected tributaries.
Better suited for tortuous veins. Patients who have had prior stripping often have branches that are too tortuous to access with thermal ablation. In such cases, ECA is the only option. Those who have never undergone vein stripping often need a combination of thermal and chemical ablation, as well, with ECA reserved for saphenous veins that are inaccessible by RFA or laser.
Foamed sclerosants allow visualization. When mixed through a 3-way stopcock with an inert gas such as room air or carbon dioxide, the detergent-type sclerosants produce a micro-foamed preparation that is echogenic, and allows direct visualization with ultrasound (FIGURE 2). The foam displaces blood from within the vein and promotes contact with the venous endothelium, and intense vasospasm results. The sclerosant foam mixture, which makes it possible to watch the effect (and extent) of the foam as it disperses throughout the target vessel, has enhanced the treatment of larger viscosities.25-26 Pretreatment venous ultrasound mapping—a process in which the patient stands upright while compression is applied to the saphenous veins and their tributaries to test the valves for normal flow—combined with realtime duplex imaging, minimizes the chance of arterial injection, extravasation, and tissue necrosis.25
Serious adverse effects are rare. Hemosiderin hyperpigmentation and pain at the injection site are among the most common side effects of ultrasound-guided sclerotherapy. Serious adverse events, including anaphylaxis, DVT/pulmonary embolus, cutaneous necrosis, transient ischemic attack, and arterial injection, are rare.27
To date, there is only 1 published prospective, randomized study that directly compares foam sclerotherapy with stripping/ligation surgery. The researchers found the results of both treatments to be comparable, but reported that surgery was more expensive than foam sclerotherapy and produced less improvement in quality of life.28 A meta-analysis of treatment for 12,000 limbs concluded that foam sclerotherapy and EVTA were as effective as surgical stripping.29 There are no prospective, randomized studies comparing foam sclerotherapy with thermal ablation.
FIGURE 2
Endovenous chemoablation
ECA is also conducted under ultrasound guidance: The image at left (A) shows the needle tip inside a refluxing saphenous tributary vein; in the image at right (B), the arrow points to the vein injected with foamed sclerosant.
Advising Kevin M.: What’s his best bet?
You’ve talked to your patient in the past about vein stripping, but he’s been reluctant to undergo surgery. When you describe the minimally invasive approaches to chronic venous insufficiency with him, however, he asks to see a specialist—and to undergo ultrasound mapping.
You give him a prescription for graduated compression stockings for immediate use and a referral to a phlebologist. Soon after, you receive a report from the specialist, indicating that your patient had a combination of ELT of the refluxing left great saphenous vein and subsequent ultrasound-guided ECA of the saphenous tributaries.
The next time you see Kevin, he reports that his leg no longer aches—and you can see that the bulging, tortuous varicosities and swelling have improved significantly.
Acknowledgments
The authors thank John Hickner, MD, MSc, for his input during the manuscript process.
CORRESPONDENCE
Jeffery P. Schoonover, MD, FAAFP, Vein Clinics of America, 9000 Keystone Crossing, Suite 960, Indianapolis, IN 46240; [email protected]
• Discuss minimally invasive procedures with patients considering surgery for treatment of chronic venous insufficiency. Thermal ablation, in particular, has higher success rates than vein stripping. A
• Consider endovenous chemical ablation for treatment of tortuous saphenous tributary varicosities that cannot be treated with thermal ablation. Foamed sclerosant, injected under ultrasound guidance, allows for direct visualization and has equivalent efficacy rates when compared to venous stripping. A
• Pregnancy, active deep vein thrombosis, poor health with limited mobility, and severe peripheral vascular disease are contraindications for both thermal and chemical ablation. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE
Kevin M., a 35-year-old researcher who often works 12- to 14-hour days, is in your office again, following his second trip to the emergency room for bleeding from a protruding varicose vein proximal to his left ankle. He has complained of leg aching and ankle swelling in the past, usually after he’s been on his feet for hours.
A previous ultrasound showed no evidence of deep vein thrombosis (DVT), but did reveal reflux along the left great saphenous vein from the saphenofemoral junction to the ankle. On examination, Kevin’s lower extremity pulses are intact bilaterally, but there are multiple tortuous varicosities branching from the medial thigh to the left medial malleolus, with evidence of hemosiderin hyperpigmentation and dermatitis on the left lower leg. Previous lab studies have been normal, and Kevin has no other chronic conditions. Kevin’s main concern is to minimize “down time” from work, and he asks you about the newer, minimally invasive vein treatments he’s read about on the Internet.
What should you tell him?
Chronic venous insufficiency is a common and costly condition, affecting nearly one-third of the US population.1 While many people mistakenly think of varicose veins primarily as a cosmetic issue, venous insufficiency often results in painful, even debilitating, signs and symptoms—from swelling and aching legs to skin changes that range from stasis dermatitis to open ulceration.
Venous stripping and ambulatory phlebectomy were long considered the primary means of addressing saphenous venous insufficiency,2 and compression therapy with gradient stockings, short stretch bandages, and Unna’s dressings remains a therapeutic cornerstone for every stage of chronic venous disease. Compression has also been shown to dramatically decrease the risk of post-thrombotic syndrome following DVT3 and, when combined with anticoagulation, to prevent DVT after surgery.4
Outcomes of surgical treatment of large varicose veins arising from saphenous truncal vein reflux, however, have historically been poor.5 This is primarily because of neovascularization and residual refluxing veins. Average failure rates of 25% for saphenous vein stripping and 43% for saphenofemoral junction ligation have been reported.6 A subsequent study of 140 patients who underwent saphenous vein stripping found that 20% experienced neovascularization.7
In the last decade, a number of minimally invasive procedures have been developed and tested, giving physicians and their patients more choices for medical management of venous insufficiency. A closer look at 3 procedures, which include 2 types of thermal ablation, will help you direct patients like Kevin to the best possible treatment.
2 thermal ablation procedures use only local anesthesia
Collectively termed endovenous thermal ablation (EVTA), radiofrequency ablation (RFA) and endovenous laser treatment (ELT) are similar. Performed under duplex ultrasound visualization, both offer a number of benefits.
Outpatient treatment. EVTA procedures are typically done on an outpatient basis, with only local anesthesia—0.05% to 0.1% lidocaine, injected as a perivenous tumescent solution under ultrasound guidance.8,9 The physician places and advances an endovenous catheter (for RFA) or a laser fiber (for ELT) into the vein (FIGURE 1). When the catheter or laser is in proper position, the RF generator or laser is activated. Heat, delivered through the tip of the catheter or fiber, ablates the lumen of the vein as the physician withdraws the catheter.
Mild side effects. Temporary discomfort is common with EVTA. Mild bruising, swelling, and nodularity of the treated veins are the most frequent side effects. More serious adverse effects, including skin burns, paresthesias, DVT, and pulmonary embolism, are rare.10-12
High success rates. Successful treatment of both the great and small saphenous veins and long-term maintenance of vein closure are the norm, with rates ranging from 88% to 100% for both RFA13,14 and ELT, regardless of vein size.15-19 Thermal ablation has been shown to be superior to surgery in other ways as well, eliminating the need for general anesthesia and inpatient treatment and resulting in less postoperative pain, a shorter recovery period, an improved quality of life, and lower costs (TABLE).20-23
TABLE
Endovenous thermal ablation vs standard surgery
| Outcomes | |||||
|---|---|---|---|---|---|
| Study | Type | Modalities studied | Follow-up | Return to work | Pain |
| Rautio et al20 | RCT | RFA vs stripping | 8 weeks | Earlier with RFA | Less with RFA |
| Lurie et al21 | RCT | RFA vs stripping | 2 years | N/A | Less with RFA |
| Hinchcliffe et al22 | RCT | RFA vs stripping | 1 year | N/A | Less with RFA |
| Darwood et al23 | RCT | ELT vs stripping | 3 months | Earlier with ELT | Less with ELT |
| ELT, endovenous laser treatment; NA, not available; RCT, randomized controlled trial; RFA, radiofrequency ablation. | |||||
FIGURE 1
Endovenous laser treatment
In preparation for thermal ablation, the physician (A) places a laser catheter tip into the vein and (B) injects perivenous tumescent anesthesia, guided by duplex ultrasound. The laser tip shown here (C) is in the region of the saphenofemoral junction.
Not for every patient
Despite the usefulness of these minimally invasive procedures, RFA and ELT are not always possible. Veins that are tortuous, too small, or too close to the surface of the skin are not well suited for thermal ablation; in some cases, chemical ablation, discussed below, is the only option. However, some conditions—including pregnancy, active DVT, poor health status with limited mobility, and severe peripheral vascular disease—are contraindications for both thermal and chemical ablation.24
Thermal won’t work? Consider chemical ablation
Endovenous chemoablation (ECA), like thermal ablation, is performed on an outpatient basis without sedation. Hypertonic saline, an osmotic agent, has been used for decades in treating small-caliber varicose veins, or “spider veins.” Detergenttype sclerosants, which we’ll discuss here, are now widely used to treat larger veins, including the great and small saphenous vein trunks and their affected tributaries.
Better suited for tortuous veins. Patients who have had prior stripping often have branches that are too tortuous to access with thermal ablation. In such cases, ECA is the only option. Those who have never undergone vein stripping often need a combination of thermal and chemical ablation, as well, with ECA reserved for saphenous veins that are inaccessible by RFA or laser.
Foamed sclerosants allow visualization. When mixed through a 3-way stopcock with an inert gas such as room air or carbon dioxide, the detergent-type sclerosants produce a micro-foamed preparation that is echogenic, and allows direct visualization with ultrasound (FIGURE 2). The foam displaces blood from within the vein and promotes contact with the venous endothelium, and intense vasospasm results. The sclerosant foam mixture, which makes it possible to watch the effect (and extent) of the foam as it disperses throughout the target vessel, has enhanced the treatment of larger viscosities.25-26 Pretreatment venous ultrasound mapping—a process in which the patient stands upright while compression is applied to the saphenous veins and their tributaries to test the valves for normal flow—combined with realtime duplex imaging, minimizes the chance of arterial injection, extravasation, and tissue necrosis.25
Serious adverse effects are rare. Hemosiderin hyperpigmentation and pain at the injection site are among the most common side effects of ultrasound-guided sclerotherapy. Serious adverse events, including anaphylaxis, DVT/pulmonary embolus, cutaneous necrosis, transient ischemic attack, and arterial injection, are rare.27
To date, there is only 1 published prospective, randomized study that directly compares foam sclerotherapy with stripping/ligation surgery. The researchers found the results of both treatments to be comparable, but reported that surgery was more expensive than foam sclerotherapy and produced less improvement in quality of life.28 A meta-analysis of treatment for 12,000 limbs concluded that foam sclerotherapy and EVTA were as effective as surgical stripping.29 There are no prospective, randomized studies comparing foam sclerotherapy with thermal ablation.
FIGURE 2
Endovenous chemoablation
ECA is also conducted under ultrasound guidance: The image at left (A) shows the needle tip inside a refluxing saphenous tributary vein; in the image at right (B), the arrow points to the vein injected with foamed sclerosant.
Advising Kevin M.: What’s his best bet?
You’ve talked to your patient in the past about vein stripping, but he’s been reluctant to undergo surgery. When you describe the minimally invasive approaches to chronic venous insufficiency with him, however, he asks to see a specialist—and to undergo ultrasound mapping.
You give him a prescription for graduated compression stockings for immediate use and a referral to a phlebologist. Soon after, you receive a report from the specialist, indicating that your patient had a combination of ELT of the refluxing left great saphenous vein and subsequent ultrasound-guided ECA of the saphenous tributaries.
The next time you see Kevin, he reports that his leg no longer aches—and you can see that the bulging, tortuous varicosities and swelling have improved significantly.
Acknowledgments
The authors thank John Hickner, MD, MSc, for his input during the manuscript process.
CORRESPONDENCE
Jeffery P. Schoonover, MD, FAAFP, Vein Clinics of America, 9000 Keystone Crossing, Suite 960, Indianapolis, IN 46240; [email protected]
1. McLafferty R, Lohr J, Caprini J, et al. Results of the national pilot screening program for venous disease by the American Venous Forum. J Vasc Surg. 2007;45:142-148.
2. Hagen MD, Johnson ED, Adelman A. What treatments are effective for varicose veins? J Fam Pract. 2003;52:329-331.
3. Partsch H, Flour M, Smith PC. Indications for compression therapy in venous and disease consensus based on experimental data and scientific evidence. Under the auspices of the IUP. Int Angiol. 2008;27:193-219.
4. Partsch H. ed. Evidence-based compression therapy. VASA. 2003;32(suppl 63):S3-S39.
5. Fischer R, Chandler JG, de Maeseneer MG, et al. The unresolved problem of recurrent saphenofemoral reflux. J Am Coll Surg. 2002;195:80-94.
6. Perrin MR. Recurrent varices after surgery (REVAS), a consensus document. Cardiovasc Surg. 2000;8:233-245.
7. Perrin MR, Labropoulos M, Leon L. Presentation of the patient with recurrent varices after surgery (REVAS). J Vasc Surg. 2006;43:327-334.
8. Navarro L, Min R, Boné C. Endovenous laser: a new minimally invasive method of treatment for varicose veins—preliminary observations using an 810 nm diode laser. Dermatol Surg. 2001;27:117-122.
9. Min R, Zimmet S, Isaacs M, et al. Endovenous laser treatment of the incompetent greater saphenous vein. J Vasc Interv Radiol. 2001;12:1167-1171.
10. Mundy L, Merlin TL, Fitridge RA, et al. Systematic review of endovenous laser treatment for varicose veins. Br J Surg. 2005;92:1189-1194.
11. van den Bos RR, Kockaert MA, Neumann HAM, et al. Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008;35:88-95.
12. Proebstle TM, Moehler T, Gul D, et al. Endovenous treatment of the great saphenous vein using a 1320 nm Nd:YAG laser causes fewer side effects than using a 940 nm diode laser. Dermatol Surg. 2005;31:1380-1385.
13. Pichot O, Kabnick LS, Creton D, et al. Duplex ultrasound scan findings two years after great saphenous vein radiofrequency endovenous obliteration. J Vasc Surg. 2004;39:189-195.
14. Merchant RF, Pichot O, Myers KA. Four-year follow-up on endovascular radiofrequency obliteration of great saphenous reflux. Dermatol Surg. 2005;31:129-134.
15. Kabnick LS. Outcome of different endovenous laser wavelengths for great saphenous vein ablation. J Vasc Surg. 2006;43:88-93.
16. Min RJ, Khilnani N, Zimmet SE. Endovenous laser treatment of saphenous vein reflux: long-term results. J Vasc Interv Radiol. 2003;14:991-996.
17. Proebstle TM, Gul D, Kargl A, et al. Endovenous laser treatment of the lesser saphenous vein with a 940-nm diode laser: early results. Dermatol Surg. 2003;29:357-361.
18. Theivacumar NS, Beale RJ, Mavor AID, et al. Initial experience in endovenous laser ablation (EVLA) of varicose veins due to small saphenous vein reflux. Eur J Vasc Endovasc Surg. 2007;33:614-618.
19. Gibson KD, Ferris BL, Polissar N, et al. Endovenous laser treatment of the short saphenous vein: efficacy and complications. J Vasc Surg. 2007;45:795-803.
20. Rautio T, Ohinmaa A, Perala J, et al. Endovenous obliteration versus conventional stripping operation in the treatment of primary varicose veins: a randomized controlled trial with comparison of the costs. J Vasc Surg. 2002;35:958-965.
21. Lurie F, Creton D, Eklof B, et al. Prospective randomised study of endovenous radiofrequency obliteration (closure) versus ligation and vein stripping (EVOLVeS): two-year follow-up. Eur J Vasc Endovasc Surg. 2005;29:67-73.
22. Hinchcliffe RJ, Ubhi J, Beech A, et al. A prospective randomized controlled trial of VNUS closure versus surgery for the treatment of recurrent long saphenous varicose veins. Eur J Vasc Endovasc Surg. 2006;31:212-218.
23. Darwood RJ, Theivacumar N, Dellagrammaticas D, et al. Randomized clinical trial comparing endovenous laser ablation with surgery for the treatment of primary great saphenous varicose veins. Br J Surg. 2008;95:294-301.
24. Sadick NS. Advances in the treatment of varicose veins: ambulatory phlebectomy, foam sclerotherapy, endovascular laser, and radiofrequency closure. Dermatol Clin. 2005;23:443-455.
25. Kakkos SK, Bountouroglou DG, Azzam M, et al. Effectiveness and safety of ultrasound-guided foam sclerotherapy for recurrent varicose veins: immediate results. J Endovasc Ther. 2006;13:357-364.
26. Cabrera J, Cabrera A, Jr, Garcia-Olmedo A. Treatment of varicose long saphenous veins with sclerosant in microfoam form: long-term outcomes. Phlebology. 2000;15:19-23.
27. Jia X, Mowatt G, Burr JM, et al. Systematic review of foam sclerotherapy for varicose veins. Br J Surg. 2007;10:307-1308.
28. Belcaro G, Cesarone MR, Di Renzo A, et al. Foam-sclerotherapy, surgery, sclerotherapy, and combined treatment for varicose veins: a 10-year, prospective, randomized, controlled, trial (VEDICO trial). Angiology. 2003;54:307-315.
29. van den Bos R, Arends L, Kockaert M, et al. Endovenous therapies of lower extremity varicosities: a meta-analysis. J Vasc Surg. 2009;49:230-239.
1. McLafferty R, Lohr J, Caprini J, et al. Results of the national pilot screening program for venous disease by the American Venous Forum. J Vasc Surg. 2007;45:142-148.
2. Hagen MD, Johnson ED, Adelman A. What treatments are effective for varicose veins? J Fam Pract. 2003;52:329-331.
3. Partsch H, Flour M, Smith PC. Indications for compression therapy in venous and disease consensus based on experimental data and scientific evidence. Under the auspices of the IUP. Int Angiol. 2008;27:193-219.
4. Partsch H. ed. Evidence-based compression therapy. VASA. 2003;32(suppl 63):S3-S39.
5. Fischer R, Chandler JG, de Maeseneer MG, et al. The unresolved problem of recurrent saphenofemoral reflux. J Am Coll Surg. 2002;195:80-94.
6. Perrin MR. Recurrent varices after surgery (REVAS), a consensus document. Cardiovasc Surg. 2000;8:233-245.
7. Perrin MR, Labropoulos M, Leon L. Presentation of the patient with recurrent varices after surgery (REVAS). J Vasc Surg. 2006;43:327-334.
8. Navarro L, Min R, Boné C. Endovenous laser: a new minimally invasive method of treatment for varicose veins—preliminary observations using an 810 nm diode laser. Dermatol Surg. 2001;27:117-122.
9. Min R, Zimmet S, Isaacs M, et al. Endovenous laser treatment of the incompetent greater saphenous vein. J Vasc Interv Radiol. 2001;12:1167-1171.
10. Mundy L, Merlin TL, Fitridge RA, et al. Systematic review of endovenous laser treatment for varicose veins. Br J Surg. 2005;92:1189-1194.
11. van den Bos RR, Kockaert MA, Neumann HAM, et al. Technical review of endovenous laser therapy for varicose veins. Eur J Vasc Endovasc Surg. 2008;35:88-95.
12. Proebstle TM, Moehler T, Gul D, et al. Endovenous treatment of the great saphenous vein using a 1320 nm Nd:YAG laser causes fewer side effects than using a 940 nm diode laser. Dermatol Surg. 2005;31:1380-1385.
13. Pichot O, Kabnick LS, Creton D, et al. Duplex ultrasound scan findings two years after great saphenous vein radiofrequency endovenous obliteration. J Vasc Surg. 2004;39:189-195.
14. Merchant RF, Pichot O, Myers KA. Four-year follow-up on endovascular radiofrequency obliteration of great saphenous reflux. Dermatol Surg. 2005;31:129-134.
15. Kabnick LS. Outcome of different endovenous laser wavelengths for great saphenous vein ablation. J Vasc Surg. 2006;43:88-93.
16. Min RJ, Khilnani N, Zimmet SE. Endovenous laser treatment of saphenous vein reflux: long-term results. J Vasc Interv Radiol. 2003;14:991-996.
17. Proebstle TM, Gul D, Kargl A, et al. Endovenous laser treatment of the lesser saphenous vein with a 940-nm diode laser: early results. Dermatol Surg. 2003;29:357-361.
18. Theivacumar NS, Beale RJ, Mavor AID, et al. Initial experience in endovenous laser ablation (EVLA) of varicose veins due to small saphenous vein reflux. Eur J Vasc Endovasc Surg. 2007;33:614-618.
19. Gibson KD, Ferris BL, Polissar N, et al. Endovenous laser treatment of the short saphenous vein: efficacy and complications. J Vasc Surg. 2007;45:795-803.
20. Rautio T, Ohinmaa A, Perala J, et al. Endovenous obliteration versus conventional stripping operation in the treatment of primary varicose veins: a randomized controlled trial with comparison of the costs. J Vasc Surg. 2002;35:958-965.
21. Lurie F, Creton D, Eklof B, et al. Prospective randomised study of endovenous radiofrequency obliteration (closure) versus ligation and vein stripping (EVOLVeS): two-year follow-up. Eur J Vasc Endovasc Surg. 2005;29:67-73.
22. Hinchcliffe RJ, Ubhi J, Beech A, et al. A prospective randomized controlled trial of VNUS closure versus surgery for the treatment of recurrent long saphenous varicose veins. Eur J Vasc Endovasc Surg. 2006;31:212-218.
23. Darwood RJ, Theivacumar N, Dellagrammaticas D, et al. Randomized clinical trial comparing endovenous laser ablation with surgery for the treatment of primary great saphenous varicose veins. Br J Surg. 2008;95:294-301.
24. Sadick NS. Advances in the treatment of varicose veins: ambulatory phlebectomy, foam sclerotherapy, endovascular laser, and radiofrequency closure. Dermatol Clin. 2005;23:443-455.
25. Kakkos SK, Bountouroglou DG, Azzam M, et al. Effectiveness and safety of ultrasound-guided foam sclerotherapy for recurrent varicose veins: immediate results. J Endovasc Ther. 2006;13:357-364.
26. Cabrera J, Cabrera A, Jr, Garcia-Olmedo A. Treatment of varicose long saphenous veins with sclerosant in microfoam form: long-term outcomes. Phlebology. 2000;15:19-23.
27. Jia X, Mowatt G, Burr JM, et al. Systematic review of foam sclerotherapy for varicose veins. Br J Surg. 2007;10:307-1308.
28. Belcaro G, Cesarone MR, Di Renzo A, et al. Foam-sclerotherapy, surgery, sclerotherapy, and combined treatment for varicose veins: a 10-year, prospective, randomized, controlled, trial (VEDICO trial). Angiology. 2003;54:307-315.
29. van den Bos R, Arends L, Kockaert M, et al. Endovenous therapies of lower extremity varicosities: a meta-analysis. J Vasc Surg. 2009;49:230-239.