User login
Which tympanometer is optimal for an outpatient primary care setting?
- Four tympanometers are suitable for outpatient primary care, and each has positive and negative attributes. The Earscan was rated easiest to use and provided the most consistent data.
In a primary care setting where patient volume, time constraints, and provider turnover are on the increase, you need dependable biomedical equipment that produces quality data and is easy to use, ergonomic, and affordable. This is certainly true of the tympanometer, which is used to measure mobility and impedance of the tympanic membrane and ossicles, provide an objective measurement of the middle ear, augment visual and pneumatic otoscopy, and confirm and document otitis media with effusion (OME) and acute otitis media (AOM).1-3 Our study aimed to determine which tympanometer is optimal in the outpatient primary care setting.
Based on objective and subjective analysis, the Earscan appears to be an excellent choice for outpatient primary care, though users also liked the MT 10 and GSI 37.
Four units made initial cut
Of 16 tympanometers we found through a review of market literature, an Internet search, and audiology recommendations, 4 met the minimum requirements (TABLE 1)—Earscan (www.microaud.com), GSI 37 (www.viasyshealthcare.com), MicroTymp 2 (www.welchallyn.com) and MT 10 (www.interacoustics-us.com).
TABLE 1
Tympanometers had to meet these minimum requirements to be considered
| 1. COMPLIANCE |
| Pressure measurement: +200 to –300 daPa |
| Sound frequency: 226 Hz ±3% |
| Sound amplitude: 85 dB SPL ±3dB |
| 2. PRESSURE PUMP |
| Accuracy: ±15% or 10 daPa (or better) |
| Positive to negative pressure sweep |
| 3. DATA DISPLAY |
| Screen size: 2.5 cm × 2.5 cm |
| Horizontal axis (pressure): +200 to –300 daPa |
| Vertical axis (volume): 1.0 to 2.5 cm3 displayed |
| 4. PRICE |
| <$3000 list price per unit |
| 5. SIZE AND ERGONOMICS |
| Main box or docking station: dimensions < 30 cm × 23 cm × 10 cm; weight <2.7 kg |
| Handheld component: dimensions < 10 cm × 25 cm × 13 cm; weight <500 g |
What we looked for in our in-depth evaluation
We evaluated the tympanometers with formal objective testing, clinical use, subjective user rating, and feature comparison.
We assessed reproducibility with a volume calibration tool (in vitro), and with intra- and inter-device testing (in vivo) on volunteers. The tympanometers were also compared side by side in a clinical setting on adults and children with and without ear disease.
Eight evaluators with various clinical and technical backgrounds were our subjective raters. They used a Likert scale survey to rate the following tympanometer attributes: appearance, size, safety, durability, capabilities, ergonomics of physical design, ease of use (overall operations, specific control features), screen information layout, LCD screen/monitor, printing, maintenance, software interface, data quality and reliability, and accessories. Participants independently reviewed the tympanometers and were blinded to others’ evaluations.
We prioritized categories as high, medium, or low importance. Finally, important features of each unit were identified and verified.
Our rankings
Earscan comes out on top
Formal testing, clinical use, and feature comparison suggest the Earscan is the tympanometer best suited for primary care (see “How the units compared”).
The Earscan delivered high-quality data with excellent results in reproducibility testing for volume, pressure, and compliance. It proved reliable in the clinical setting with positive comments from participants.
Ergonomics. The Earscan was rated the easiest to use and the simplest to obtain a probe tip-ear seal. The Earscan has a small cylindrical probe affixed to a pressure/sound tube that attaches to the control unit. Anecdotally, these kinds of box-and-tube tympanometers provide the best seal and true readings. The probe is small, lightweight, and well suited for the clinician’s hand and patient’s ear so the tip-ear seal is easily viewed during the procedure. The tips are malleable, beveled, and tapered to provide an excellent fit in the ear canal.
The control unit is a reasonable size with finger-sized buttons and a viewable screen. It is simple to turn the unit on, press the Impedance button and perform the exam. The unit displays understandable feedback as to status.
Construction. The air pump, tone inducer, tubing, probe, and compliance pressure sensor are sturdy and yield consistent results. The unit is rugged and portable making it popular for occupational health.
Features. The Earscan is affordable and comes with additional functionality of audiometry and acoustic reflex testing. It has RS232 serial port capability to facilitate printer and limited computer integration.
Drawbacks. The unit is powered by a 120-volt adapter, making it less convenient than a handheld tympanometer. It may not be reasonable to carry the Earscan from one exam room to another. The Earscan has an older appearance with sealed buttons that are encased and provide little tactile feedback.
When other units may be preferable
If a handheld tympanometer with a docking station is necessary, then the MT10 or GSI 37 would be an appropriate choice.
MT10. This unit received the highest overall user ratings, slightly higher than the Earscan. The MT10 has a larger monitor and better control features than the GSI 37. It also has the capability for computer integration. However, the MT 10 gave less consistent readings for same-ear measurements when compared with the Earscan and GSI 37.
GSI 37. This unit provided more consistent pressure and compliance readings than the MT 10, and had no glare on its screen. It also has a longer track record in the field than does the newer MT10. It has an excellent operation manual.
In vitro testing for volume using a fixed object (calibration tube) demonstrated excellent reproducibility. There was little to no variation for 10 consecutive measurements for each tympanometer. In vivo reproducibility testing was performed taking 3 consecutive readings on each of 5 different ears using the tympanometers. For Compliance and Pressure readings the Earscan showed the most consistency while the MT 10 showed the least (TABLE 2).
Compliance data is graphed from 1 left ear to portray the range of values obtained from 4 tympanometers (FIGURE 1). While all tympanometers gave normal compliance readings, some units were less consistent than others. The MT10 showed the widest range of readings (least consistency). For this patient’s right ear (not shown), 3 tympanometers identified an overly compliant ear drum, while the MT10 gave normal and close to normal values. The MicroTymp 2 did not provide a compliance reading for the right ear.
Middle ear pressure data is graphed from the same left ear to portray the range of values obtained from 4 tympanometers (FIGURE 2). Overall, the units gave values that were within the clinically acceptable range of normal. However, there was a wide range of readings from the MT10 and MicroTymp 2. Assuming the participants’ middle ear pressure was truly close to zero, the outlier values reported by the MT10 and MicroTymp 2 might have clinical significance.
More than 100 tympanograms were obtained on children and adults; observations were noted. The Earscan, GSI 37 and MT 10 were easier to use and to obtain a good seal. The MicroTymp 2 proved more difficult to obtain a seal with and at times presented a falsely positive flat tympanogram. Earscan and MT10 gave similar readings on several occasions. On several occasions, the MicroTymp 2 and GSI 37 values significantly disagreed with each other. At times the MicroTymp 2 provided a graphical tympanogram but did not provide the numerical data. It was also easy to inadvertently combine previous data from one ear with new data from contralateral ear when using the MicroTymp 2.
Earscan tympanograms and corresponding video otoscope images are shown in FIGURE 3. The right tympanogram (bottom) is consistent with the video otoscope findings of otitis media. Observe the low compliance, elevated middle ear pressure, and low physical volume. The normal left tympanogram and otoscopy are concordant.
User ratings are shown in TABLE 3. Overall, participants ranked the MT10 highest (56.3) with the Earscan second (54.9), GSI 37 third (50.4), and MicroTymp 2 fourth (46.0). The MT10 rated highest in Ergonomics, Ease of Use of Control Features, Screen, Accessories, Appearance, Size and Information Layout. The Earscan rated highest in Overall Ease of Use and Perceived Durability. The MT10 and Earscan were tied for Capabilities and Interfacing. The MT10, GSI 37 and Earscan were tied for Perceived Data Quality. The GSI 37 was rated highest in Perceived Maintenance. Seven out of 8 reviewers (2 ties with the MT10) selected the Earscan as easiest to use. Eight out of eight (2 ties with MT10) selected the Earscan as the most simple to obtain a good seal.
The features representing the main differences between the 4 tympanometers are listed on pages 951 and 952. Features are identified as positive or negative and ranked according to how they impacted the final selection from most influential to least.
FIGURE 1
Compliance data obtained from 4 tympanometers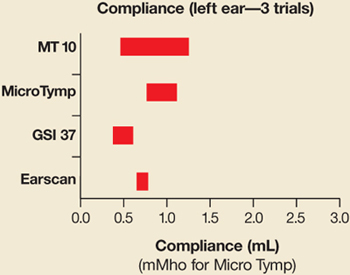
While all 4 gave normal readings, the MT10 showed the least consistency.
FIGURE 2
Middle ear pressure data obtained from 4 tympanometers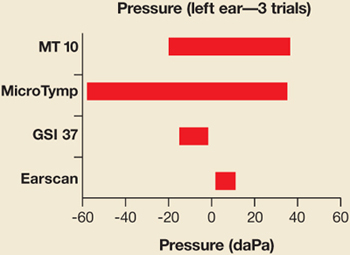
All 4 units gave values within normal range; there was a wide range from the MT10 and MicroTymp2.
FIGURE 3
Earscan tympanograms agree with corresponding video otoscope images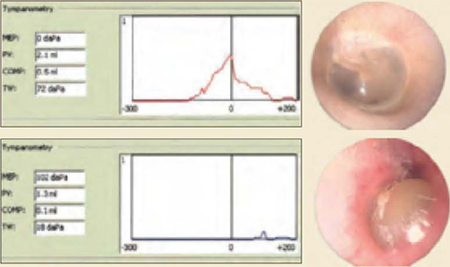
Top: Earscan demonstrating a normal left tympanogram and corresponding video otoscope image.
Bottom: Earscan demonstrating an abnormal right tympanogram with elevated middle ear pressure, reduced compliance and reduced physical volume. The video otoscope image is consistent with otitis media.
TABLE 2
For compliance and pressure readings, the Earscan showed the most consistency while the MT10 showed the least
| EAR A | EAR B | EAR C | EAR D | EAR E | |
|---|---|---|---|---|---|
| Range of readings (variance) for compliance in mL | |||||
| Earscan | 0.2 | 0.1 | 0.2 | 0.1 | 0.4 |
| MT 10 | 0.8 | 0.65 | 0.64 | 0.12 | 0.62 |
| Range of readings (variance) for pressure in daPa | |||||
| Earscan | 0 | 6 | 0 | 0 | 6 |
| MT10 | 30 | 53 | 31 | 16 | 82 |
TABLE 3
User ratings of 4 tympanometers (Likert scale 1 to 5)
| CATEGORY | EARSCAN | GSI 37 | MICROTYMP 2 | MT10 |
|---|---|---|---|---|
| Categories deemed highest importance | ||||
| Ease of use: overall | 4.1 | 3.8 | 3.0 | 3.8 |
| Data quality | 4.4 | 4.4 | 4.0 | 4.4 |
| Ergonomics | 4.5 | 4.6 | 4.4 | 4.0 |
| Durability | 4.9 | 4.3 | 4.4 | 4.6 |
| Maintenance | 4.7 | 4.8 | 3.7 | 4.4 |
| Categories deemed medium importance | ||||
| Ease of use: controls | 3.8 | 3.7 | 4.2 | 4.5 |
| Screen | 4.3 | 4.5 | 3.1 | 4.7 |
| Accessories | 4.2 | 3.9 | 3.8 | 4.3 |
| Categories deemed lowest importance | ||||
| Appearance | 4.0 | 3.8 | 3.7 | 4.1 |
| Size | 4.1 | 3.8 | 4.2 | 4.4 |
| Capabilities | 4.0 | 2.0 | 1.0 | 4.0 |
| Info layout | 4.2 | 4.2 | 4.1 | 4.7 |
| Interface | 3.7 | 2.6 | 2.4 | 3.7 |
| Total | 54.9 | 50.4 | 46.0 | 56.3 |
CORRESPONDENCE
Chris Patricoski, MD, Alaska Federal Health Care Access Network, 4000 Ambassador Drive, Anchorage, AK 99508. E-mail: [email protected]
1. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Otitis Media with Effusion. Pediatrics 2004;113:1412-1429.
2. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Acute Otitis Media Pediatrics 2004;113:1451-1465.
3. Onusko E. Tympanometry. Am Fam Physician 2004;7:1713-1720.
- Four tympanometers are suitable for outpatient primary care, and each has positive and negative attributes. The Earscan was rated easiest to use and provided the most consistent data.
In a primary care setting where patient volume, time constraints, and provider turnover are on the increase, you need dependable biomedical equipment that produces quality data and is easy to use, ergonomic, and affordable. This is certainly true of the tympanometer, which is used to measure mobility and impedance of the tympanic membrane and ossicles, provide an objective measurement of the middle ear, augment visual and pneumatic otoscopy, and confirm and document otitis media with effusion (OME) and acute otitis media (AOM).1-3 Our study aimed to determine which tympanometer is optimal in the outpatient primary care setting.
Based on objective and subjective analysis, the Earscan appears to be an excellent choice for outpatient primary care, though users also liked the MT 10 and GSI 37.
Four units made initial cut
Of 16 tympanometers we found through a review of market literature, an Internet search, and audiology recommendations, 4 met the minimum requirements (TABLE 1)—Earscan (www.microaud.com), GSI 37 (www.viasyshealthcare.com), MicroTymp 2 (www.welchallyn.com) and MT 10 (www.interacoustics-us.com).
TABLE 1
Tympanometers had to meet these minimum requirements to be considered
| 1. COMPLIANCE |
| Pressure measurement: +200 to –300 daPa |
| Sound frequency: 226 Hz ±3% |
| Sound amplitude: 85 dB SPL ±3dB |
| 2. PRESSURE PUMP |
| Accuracy: ±15% or 10 daPa (or better) |
| Positive to negative pressure sweep |
| 3. DATA DISPLAY |
| Screen size: 2.5 cm × 2.5 cm |
| Horizontal axis (pressure): +200 to –300 daPa |
| Vertical axis (volume): 1.0 to 2.5 cm3 displayed |
| 4. PRICE |
| <$3000 list price per unit |
| 5. SIZE AND ERGONOMICS |
| Main box or docking station: dimensions < 30 cm × 23 cm × 10 cm; weight <2.7 kg |
| Handheld component: dimensions < 10 cm × 25 cm × 13 cm; weight <500 g |
What we looked for in our in-depth evaluation
We evaluated the tympanometers with formal objective testing, clinical use, subjective user rating, and feature comparison.
We assessed reproducibility with a volume calibration tool (in vitro), and with intra- and inter-device testing (in vivo) on volunteers. The tympanometers were also compared side by side in a clinical setting on adults and children with and without ear disease.
Eight evaluators with various clinical and technical backgrounds were our subjective raters. They used a Likert scale survey to rate the following tympanometer attributes: appearance, size, safety, durability, capabilities, ergonomics of physical design, ease of use (overall operations, specific control features), screen information layout, LCD screen/monitor, printing, maintenance, software interface, data quality and reliability, and accessories. Participants independently reviewed the tympanometers and were blinded to others’ evaluations.
We prioritized categories as high, medium, or low importance. Finally, important features of each unit were identified and verified.
Our rankings
Earscan comes out on top
Formal testing, clinical use, and feature comparison suggest the Earscan is the tympanometer best suited for primary care (see “How the units compared”).
The Earscan delivered high-quality data with excellent results in reproducibility testing for volume, pressure, and compliance. It proved reliable in the clinical setting with positive comments from participants.
Ergonomics. The Earscan was rated the easiest to use and the simplest to obtain a probe tip-ear seal. The Earscan has a small cylindrical probe affixed to a pressure/sound tube that attaches to the control unit. Anecdotally, these kinds of box-and-tube tympanometers provide the best seal and true readings. The probe is small, lightweight, and well suited for the clinician’s hand and patient’s ear so the tip-ear seal is easily viewed during the procedure. The tips are malleable, beveled, and tapered to provide an excellent fit in the ear canal.
The control unit is a reasonable size with finger-sized buttons and a viewable screen. It is simple to turn the unit on, press the Impedance button and perform the exam. The unit displays understandable feedback as to status.
Construction. The air pump, tone inducer, tubing, probe, and compliance pressure sensor are sturdy and yield consistent results. The unit is rugged and portable making it popular for occupational health.
Features. The Earscan is affordable and comes with additional functionality of audiometry and acoustic reflex testing. It has RS232 serial port capability to facilitate printer and limited computer integration.
Drawbacks. The unit is powered by a 120-volt adapter, making it less convenient than a handheld tympanometer. It may not be reasonable to carry the Earscan from one exam room to another. The Earscan has an older appearance with sealed buttons that are encased and provide little tactile feedback.
When other units may be preferable
If a handheld tympanometer with a docking station is necessary, then the MT10 or GSI 37 would be an appropriate choice.
MT10. This unit received the highest overall user ratings, slightly higher than the Earscan. The MT10 has a larger monitor and better control features than the GSI 37. It also has the capability for computer integration. However, the MT 10 gave less consistent readings for same-ear measurements when compared with the Earscan and GSI 37.
GSI 37. This unit provided more consistent pressure and compliance readings than the MT 10, and had no glare on its screen. It also has a longer track record in the field than does the newer MT10. It has an excellent operation manual.
In vitro testing for volume using a fixed object (calibration tube) demonstrated excellent reproducibility. There was little to no variation for 10 consecutive measurements for each tympanometer. In vivo reproducibility testing was performed taking 3 consecutive readings on each of 5 different ears using the tympanometers. For Compliance and Pressure readings the Earscan showed the most consistency while the MT 10 showed the least (TABLE 2).
Compliance data is graphed from 1 left ear to portray the range of values obtained from 4 tympanometers (FIGURE 1). While all tympanometers gave normal compliance readings, some units were less consistent than others. The MT10 showed the widest range of readings (least consistency). For this patient’s right ear (not shown), 3 tympanometers identified an overly compliant ear drum, while the MT10 gave normal and close to normal values. The MicroTymp 2 did not provide a compliance reading for the right ear.
Middle ear pressure data is graphed from the same left ear to portray the range of values obtained from 4 tympanometers (FIGURE 2). Overall, the units gave values that were within the clinically acceptable range of normal. However, there was a wide range of readings from the MT10 and MicroTymp 2. Assuming the participants’ middle ear pressure was truly close to zero, the outlier values reported by the MT10 and MicroTymp 2 might have clinical significance.
More than 100 tympanograms were obtained on children and adults; observations were noted. The Earscan, GSI 37 and MT 10 were easier to use and to obtain a good seal. The MicroTymp 2 proved more difficult to obtain a seal with and at times presented a falsely positive flat tympanogram. Earscan and MT10 gave similar readings on several occasions. On several occasions, the MicroTymp 2 and GSI 37 values significantly disagreed with each other. At times the MicroTymp 2 provided a graphical tympanogram but did not provide the numerical data. It was also easy to inadvertently combine previous data from one ear with new data from contralateral ear when using the MicroTymp 2.
Earscan tympanograms and corresponding video otoscope images are shown in FIGURE 3. The right tympanogram (bottom) is consistent with the video otoscope findings of otitis media. Observe the low compliance, elevated middle ear pressure, and low physical volume. The normal left tympanogram and otoscopy are concordant.
User ratings are shown in TABLE 3. Overall, participants ranked the MT10 highest (56.3) with the Earscan second (54.9), GSI 37 third (50.4), and MicroTymp 2 fourth (46.0). The MT10 rated highest in Ergonomics, Ease of Use of Control Features, Screen, Accessories, Appearance, Size and Information Layout. The Earscan rated highest in Overall Ease of Use and Perceived Durability. The MT10 and Earscan were tied for Capabilities and Interfacing. The MT10, GSI 37 and Earscan were tied for Perceived Data Quality. The GSI 37 was rated highest in Perceived Maintenance. Seven out of 8 reviewers (2 ties with the MT10) selected the Earscan as easiest to use. Eight out of eight (2 ties with MT10) selected the Earscan as the most simple to obtain a good seal.
The features representing the main differences between the 4 tympanometers are listed on pages 951 and 952. Features are identified as positive or negative and ranked according to how they impacted the final selection from most influential to least.
FIGURE 1
Compliance data obtained from 4 tympanometers
While all 4 gave normal readings, the MT10 showed the least consistency.
FIGURE 2
Middle ear pressure data obtained from 4 tympanometers
All 4 units gave values within normal range; there was a wide range from the MT10 and MicroTymp2.
FIGURE 3
Earscan tympanograms agree with corresponding video otoscope images
Top: Earscan demonstrating a normal left tympanogram and corresponding video otoscope image.
Bottom: Earscan demonstrating an abnormal right tympanogram with elevated middle ear pressure, reduced compliance and reduced physical volume. The video otoscope image is consistent with otitis media.
TABLE 2
For compliance and pressure readings, the Earscan showed the most consistency while the MT10 showed the least
| EAR A | EAR B | EAR C | EAR D | EAR E | |
|---|---|---|---|---|---|
| Range of readings (variance) for compliance in mL | |||||
| Earscan | 0.2 | 0.1 | 0.2 | 0.1 | 0.4 |
| MT 10 | 0.8 | 0.65 | 0.64 | 0.12 | 0.62 |
| Range of readings (variance) for pressure in daPa | |||||
| Earscan | 0 | 6 | 0 | 0 | 6 |
| MT10 | 30 | 53 | 31 | 16 | 82 |
TABLE 3
User ratings of 4 tympanometers (Likert scale 1 to 5)
| CATEGORY | EARSCAN | GSI 37 | MICROTYMP 2 | MT10 |
|---|---|---|---|---|
| Categories deemed highest importance | ||||
| Ease of use: overall | 4.1 | 3.8 | 3.0 | 3.8 |
| Data quality | 4.4 | 4.4 | 4.0 | 4.4 |
| Ergonomics | 4.5 | 4.6 | 4.4 | 4.0 |
| Durability | 4.9 | 4.3 | 4.4 | 4.6 |
| Maintenance | 4.7 | 4.8 | 3.7 | 4.4 |
| Categories deemed medium importance | ||||
| Ease of use: controls | 3.8 | 3.7 | 4.2 | 4.5 |
| Screen | 4.3 | 4.5 | 3.1 | 4.7 |
| Accessories | 4.2 | 3.9 | 3.8 | 4.3 |
| Categories deemed lowest importance | ||||
| Appearance | 4.0 | 3.8 | 3.7 | 4.1 |
| Size | 4.1 | 3.8 | 4.2 | 4.4 |
| Capabilities | 4.0 | 2.0 | 1.0 | 4.0 |
| Info layout | 4.2 | 4.2 | 4.1 | 4.7 |
| Interface | 3.7 | 2.6 | 2.4 | 3.7 |
| Total | 54.9 | 50.4 | 46.0 | 56.3 |
CORRESPONDENCE
Chris Patricoski, MD, Alaska Federal Health Care Access Network, 4000 Ambassador Drive, Anchorage, AK 99508. E-mail: [email protected]
- Four tympanometers are suitable for outpatient primary care, and each has positive and negative attributes. The Earscan was rated easiest to use and provided the most consistent data.
In a primary care setting where patient volume, time constraints, and provider turnover are on the increase, you need dependable biomedical equipment that produces quality data and is easy to use, ergonomic, and affordable. This is certainly true of the tympanometer, which is used to measure mobility and impedance of the tympanic membrane and ossicles, provide an objective measurement of the middle ear, augment visual and pneumatic otoscopy, and confirm and document otitis media with effusion (OME) and acute otitis media (AOM).1-3 Our study aimed to determine which tympanometer is optimal in the outpatient primary care setting.
Based on objective and subjective analysis, the Earscan appears to be an excellent choice for outpatient primary care, though users also liked the MT 10 and GSI 37.
Four units made initial cut
Of 16 tympanometers we found through a review of market literature, an Internet search, and audiology recommendations, 4 met the minimum requirements (TABLE 1)—Earscan (www.microaud.com), GSI 37 (www.viasyshealthcare.com), MicroTymp 2 (www.welchallyn.com) and MT 10 (www.interacoustics-us.com).
TABLE 1
Tympanometers had to meet these minimum requirements to be considered
| 1. COMPLIANCE |
| Pressure measurement: +200 to –300 daPa |
| Sound frequency: 226 Hz ±3% |
| Sound amplitude: 85 dB SPL ±3dB |
| 2. PRESSURE PUMP |
| Accuracy: ±15% or 10 daPa (or better) |
| Positive to negative pressure sweep |
| 3. DATA DISPLAY |
| Screen size: 2.5 cm × 2.5 cm |
| Horizontal axis (pressure): +200 to –300 daPa |
| Vertical axis (volume): 1.0 to 2.5 cm3 displayed |
| 4. PRICE |
| <$3000 list price per unit |
| 5. SIZE AND ERGONOMICS |
| Main box or docking station: dimensions < 30 cm × 23 cm × 10 cm; weight <2.7 kg |
| Handheld component: dimensions < 10 cm × 25 cm × 13 cm; weight <500 g |
What we looked for in our in-depth evaluation
We evaluated the tympanometers with formal objective testing, clinical use, subjective user rating, and feature comparison.
We assessed reproducibility with a volume calibration tool (in vitro), and with intra- and inter-device testing (in vivo) on volunteers. The tympanometers were also compared side by side in a clinical setting on adults and children with and without ear disease.
Eight evaluators with various clinical and technical backgrounds were our subjective raters. They used a Likert scale survey to rate the following tympanometer attributes: appearance, size, safety, durability, capabilities, ergonomics of physical design, ease of use (overall operations, specific control features), screen information layout, LCD screen/monitor, printing, maintenance, software interface, data quality and reliability, and accessories. Participants independently reviewed the tympanometers and were blinded to others’ evaluations.
We prioritized categories as high, medium, or low importance. Finally, important features of each unit were identified and verified.
Our rankings
Earscan comes out on top
Formal testing, clinical use, and feature comparison suggest the Earscan is the tympanometer best suited for primary care (see “How the units compared”).
The Earscan delivered high-quality data with excellent results in reproducibility testing for volume, pressure, and compliance. It proved reliable in the clinical setting with positive comments from participants.
Ergonomics. The Earscan was rated the easiest to use and the simplest to obtain a probe tip-ear seal. The Earscan has a small cylindrical probe affixed to a pressure/sound tube that attaches to the control unit. Anecdotally, these kinds of box-and-tube tympanometers provide the best seal and true readings. The probe is small, lightweight, and well suited for the clinician’s hand and patient’s ear so the tip-ear seal is easily viewed during the procedure. The tips are malleable, beveled, and tapered to provide an excellent fit in the ear canal.
The control unit is a reasonable size with finger-sized buttons and a viewable screen. It is simple to turn the unit on, press the Impedance button and perform the exam. The unit displays understandable feedback as to status.
Construction. The air pump, tone inducer, tubing, probe, and compliance pressure sensor are sturdy and yield consistent results. The unit is rugged and portable making it popular for occupational health.
Features. The Earscan is affordable and comes with additional functionality of audiometry and acoustic reflex testing. It has RS232 serial port capability to facilitate printer and limited computer integration.
Drawbacks. The unit is powered by a 120-volt adapter, making it less convenient than a handheld tympanometer. It may not be reasonable to carry the Earscan from one exam room to another. The Earscan has an older appearance with sealed buttons that are encased and provide little tactile feedback.
When other units may be preferable
If a handheld tympanometer with a docking station is necessary, then the MT10 or GSI 37 would be an appropriate choice.
MT10. This unit received the highest overall user ratings, slightly higher than the Earscan. The MT10 has a larger monitor and better control features than the GSI 37. It also has the capability for computer integration. However, the MT 10 gave less consistent readings for same-ear measurements when compared with the Earscan and GSI 37.
GSI 37. This unit provided more consistent pressure and compliance readings than the MT 10, and had no glare on its screen. It also has a longer track record in the field than does the newer MT10. It has an excellent operation manual.
In vitro testing for volume using a fixed object (calibration tube) demonstrated excellent reproducibility. There was little to no variation for 10 consecutive measurements for each tympanometer. In vivo reproducibility testing was performed taking 3 consecutive readings on each of 5 different ears using the tympanometers. For Compliance and Pressure readings the Earscan showed the most consistency while the MT 10 showed the least (TABLE 2).
Compliance data is graphed from 1 left ear to portray the range of values obtained from 4 tympanometers (FIGURE 1). While all tympanometers gave normal compliance readings, some units were less consistent than others. The MT10 showed the widest range of readings (least consistency). For this patient’s right ear (not shown), 3 tympanometers identified an overly compliant ear drum, while the MT10 gave normal and close to normal values. The MicroTymp 2 did not provide a compliance reading for the right ear.
Middle ear pressure data is graphed from the same left ear to portray the range of values obtained from 4 tympanometers (FIGURE 2). Overall, the units gave values that were within the clinically acceptable range of normal. However, there was a wide range of readings from the MT10 and MicroTymp 2. Assuming the participants’ middle ear pressure was truly close to zero, the outlier values reported by the MT10 and MicroTymp 2 might have clinical significance.
More than 100 tympanograms were obtained on children and adults; observations were noted. The Earscan, GSI 37 and MT 10 were easier to use and to obtain a good seal. The MicroTymp 2 proved more difficult to obtain a seal with and at times presented a falsely positive flat tympanogram. Earscan and MT10 gave similar readings on several occasions. On several occasions, the MicroTymp 2 and GSI 37 values significantly disagreed with each other. At times the MicroTymp 2 provided a graphical tympanogram but did not provide the numerical data. It was also easy to inadvertently combine previous data from one ear with new data from contralateral ear when using the MicroTymp 2.
Earscan tympanograms and corresponding video otoscope images are shown in FIGURE 3. The right tympanogram (bottom) is consistent with the video otoscope findings of otitis media. Observe the low compliance, elevated middle ear pressure, and low physical volume. The normal left tympanogram and otoscopy are concordant.
User ratings are shown in TABLE 3. Overall, participants ranked the MT10 highest (56.3) with the Earscan second (54.9), GSI 37 third (50.4), and MicroTymp 2 fourth (46.0). The MT10 rated highest in Ergonomics, Ease of Use of Control Features, Screen, Accessories, Appearance, Size and Information Layout. The Earscan rated highest in Overall Ease of Use and Perceived Durability. The MT10 and Earscan were tied for Capabilities and Interfacing. The MT10, GSI 37 and Earscan were tied for Perceived Data Quality. The GSI 37 was rated highest in Perceived Maintenance. Seven out of 8 reviewers (2 ties with the MT10) selected the Earscan as easiest to use. Eight out of eight (2 ties with MT10) selected the Earscan as the most simple to obtain a good seal.
The features representing the main differences between the 4 tympanometers are listed on pages 951 and 952. Features are identified as positive or negative and ranked according to how they impacted the final selection from most influential to least.
FIGURE 1
Compliance data obtained from 4 tympanometers
While all 4 gave normal readings, the MT10 showed the least consistency.
FIGURE 2
Middle ear pressure data obtained from 4 tympanometers
All 4 units gave values within normal range; there was a wide range from the MT10 and MicroTymp2.
FIGURE 3
Earscan tympanograms agree with corresponding video otoscope images
Top: Earscan demonstrating a normal left tympanogram and corresponding video otoscope image.
Bottom: Earscan demonstrating an abnormal right tympanogram with elevated middle ear pressure, reduced compliance and reduced physical volume. The video otoscope image is consistent with otitis media.
TABLE 2
For compliance and pressure readings, the Earscan showed the most consistency while the MT10 showed the least
| EAR A | EAR B | EAR C | EAR D | EAR E | |
|---|---|---|---|---|---|
| Range of readings (variance) for compliance in mL | |||||
| Earscan | 0.2 | 0.1 | 0.2 | 0.1 | 0.4 |
| MT 10 | 0.8 | 0.65 | 0.64 | 0.12 | 0.62 |
| Range of readings (variance) for pressure in daPa | |||||
| Earscan | 0 | 6 | 0 | 0 | 6 |
| MT10 | 30 | 53 | 31 | 16 | 82 |
TABLE 3
User ratings of 4 tympanometers (Likert scale 1 to 5)
| CATEGORY | EARSCAN | GSI 37 | MICROTYMP 2 | MT10 |
|---|---|---|---|---|
| Categories deemed highest importance | ||||
| Ease of use: overall | 4.1 | 3.8 | 3.0 | 3.8 |
| Data quality | 4.4 | 4.4 | 4.0 | 4.4 |
| Ergonomics | 4.5 | 4.6 | 4.4 | 4.0 |
| Durability | 4.9 | 4.3 | 4.4 | 4.6 |
| Maintenance | 4.7 | 4.8 | 3.7 | 4.4 |
| Categories deemed medium importance | ||||
| Ease of use: controls | 3.8 | 3.7 | 4.2 | 4.5 |
| Screen | 4.3 | 4.5 | 3.1 | 4.7 |
| Accessories | 4.2 | 3.9 | 3.8 | 4.3 |
| Categories deemed lowest importance | ||||
| Appearance | 4.0 | 3.8 | 3.7 | 4.1 |
| Size | 4.1 | 3.8 | 4.2 | 4.4 |
| Capabilities | 4.0 | 2.0 | 1.0 | 4.0 |
| Info layout | 4.2 | 4.2 | 4.1 | 4.7 |
| Interface | 3.7 | 2.6 | 2.4 | 3.7 |
| Total | 54.9 | 50.4 | 46.0 | 56.3 |
CORRESPONDENCE
Chris Patricoski, MD, Alaska Federal Health Care Access Network, 4000 Ambassador Drive, Anchorage, AK 99508. E-mail: [email protected]
1. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Otitis Media with Effusion. Pediatrics 2004;113:1412-1429.
2. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Acute Otitis Media Pediatrics 2004;113:1451-1465.
3. Onusko E. Tympanometry. Am Fam Physician 2004;7:1713-1720.
1. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Otitis Media with Effusion. Pediatrics 2004;113:1412-1429.
2. American Academy of Family Physicians; American Academy of Otolaryngology-Head and Neck Surgery; American Academy of Pediatrics Subcommittee on Acute Otitis Media Pediatrics 2004;113:1451-1465.
3. Onusko E. Tympanometry. Am Fam Physician 2004;7:1713-1720.