User login
Fever, wet cough, rash—Dx?
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
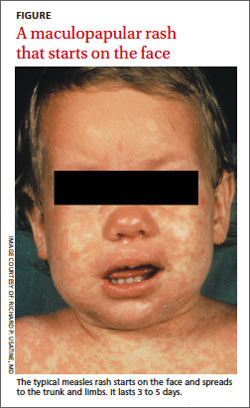
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
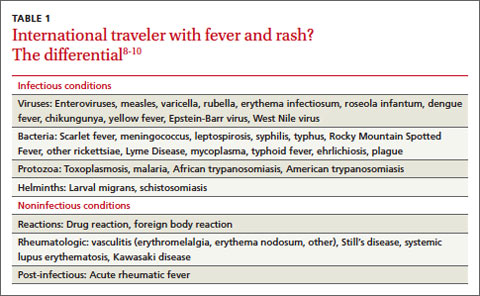
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness

Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness
Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
THE CASE
An 8-month-old Afghan-American girl was brought to the emergency department (ED) for evaluation of a fever and cough. She had been a full-term newborn and was otherwise healthy and up-to-date on routine immunizations. The patient was alert and crying, but consolable. The patient’s pulse was 140 beats/min, axillary temperature was 100.3°F, and respiratory rate was 25 breaths/min. She had rhinorrhea and scattered rhonchi on lung examination; no abnormal skin findings were reported. A chest x-ray showed nonspecific perihilar streaking without consolidation, which the ED physician interpreted as likely reflecting a viral or reactive airway disease. The patient was diagnosed with possible atypical pneumonia and prescribed a course of oral azithromycin (5 mg/kg/d for 7 days).
Two days later, the baby’s parents brought her to our outpatient office because she still had a fever and had developed a rash that had moved from her face to her trunk to her upper arms. The girl also had a wet cough, rhinorrhea, pharyngitis, emesis, nonbloody diarrhea, and poor fluid intake with low urine output. She was fussy and unable to produce tears while crying.
She had an axillary temperature of 100.5°F and a respiratory rate of 60 breaths/min. She also had mild facial edema, copious nasal discharge, erythematous ear canals with opaque, bulging tympanic membranes, right eye discharge, tachycardia, and tachypnea. The patient had pink to violaceous blanching papules and plaques of varied size and shape on her face, chest, abdomen, back, genitals, and upper arms. The plaques were surrounded by halos. She had no lesions on her oral mucosa, palms, or soles.
The parents indicated that the baby’s fever and accompanying symptoms had started 5 days after she and her mother had returned from a 6-week trip to Kabul, Afghanistan to visit family. They stayed in air-conditioned housing, didn’t travel rurally, and had no known exposure to illness. The patient had taken malaria prophylaxis as prescribed.
Due to the appearance of the patient’s rash and the fact that it had appeared soon after she started an antibiotic, we suspected she had a drug allergy that was complicating an upper respiratory viral syndrome with moderate (7%-10% loss of body weight) dehydration. However, given the history of travel along with the presence of cough, rhinorrhea, diarrhea, and a descending rash beginning on the face, we also considered measles.
We instructed the parents to immediately take their daughter to the regional children’s medical center for intravenous fluids and further evaluation. However, possibly due to miscommunication or cultural barriers, they did not go to the children’s hospital ED.
THE DIAGNOSIS
The next day, the Centers for Disease Control and Prevention (CDC) notified us that there had been a case of measles in a child who had been on the same return flight from Afghanistan as our patient. The CDC also confirmed a recent measles outbreak in Kabul.
The local public health department immediately reached out to the patient’s parents, tested the infant, and quarantined the family. Subsequent serologic and polymerase chain reaction (PCR) testing confirmed measles.
DISCUSSION
Measles (English measles/rubeola) is a highly contagious morbillivirus in the paramyxovirus family that spreads quickly through respiratory droplets and remains suspended in nonventilated waiting rooms after an infected patient has left.1
Measles is a leading cause of vaccine-preventable childhood mortality in the world, accounting for an estimated 46% of 1.7 million deaths in 2000.2 Measles disproportionately affects poorer communities, where vaccines may not be available. If just 10% of the population is not immunized, outbreaks can occur.3
Fortunately, thanks to increased immunization, the number of deaths due to measles worldwide has been on the decline, from approximately 733,000 in 2001 to 164,000 in 2008.3,4 Measles is no longer endemic in the United States and is near elimination in the Western Hemisphere if vaccination coverage remains high.
Vaccination. If not traveling internationally, children should receive measles-mumps-rubella (MMR) vaccination between 12 and 15 months and the second dose should be given before they reach age 4.5 However, the CDC reported that in 2014, the number of measles cases in the United States had reached a 20-year high, with 593 cases reported as of August 8.6 Many of these cases involved Americans who were not vaccinated before traveling to countries where the disease was prevalent.4
Before traveling internationally, infants ages 6 to 11 months should receive one MMR vaccination and children >12 months should receive 2 doses before leaving the United States.5
Look for fever, rash, and “the 3 Cs”
During its incubation period, the measles virus replicates in the epithelial cells and spreads first to the local lymphatics and then hematogenously to multiple organs.4 A fever typically develops 10 days after exposure; the rash develops about 4 days later.4
The measles rash is maculopapular and starts on the face, progresses to the trunk and then limbs, and coalesces (FIGURE). The rash typically lasts 3 to 5 days and clears in the same distribution that it appeared.3 The rash is part of a classic clinical presentation that also includes the “3 Cs” (cough, coryza [rhinorrhea], and conjunctivitis). In addition, patients may develop diarrhea and/or Koplik spots, an enanthem of small blue-white haloed lesions on the buccal mucosa (not palate) that are an early manifestation of illness.
Complications occur in around 40% of patients.7 Pneumonia is most common; other complications include croup and otitis media. Stomatitis may hinder children from eating. Rare but serious complications include late central nervous system manifestations such as encephalomyelitis, which affects 1/1000 people with measles.7 Measles inclusion body encephalitis and subacute sclerosing panencephalitis may emerge months to years after the acute infection and can cause progressive cognitive deterioration and death.7
Timing of fever helps narrow the diagnosis
The differential diagnosis for fever and rash in a returning traveler is broad (TABLE 1)8-10 and can be narrowed by a thorough history and exam (TABLE 2).10,11 Reportable public health conditions must be considered in all returning travelers who present with fever, particularly malaria, due to the possibility of acute deterioration.12,13 The timing of fever in relation to travel helps narrow the differential diagnosis. If the incubation period is <21 days, many viral infections (including measles, dengue fever, and chikungunya), malaria (especially falciparum), typhoid fever, leptospirosis, and rickettsial diseases should receive top consideration. If the period is >21 days, other causes are more likely.14
TABLE 2
Taking a returning traveler's history: What to ask10,11
Personal history
Travel history
|
The diagnosis of measles can be confirmed by serologic testing for measles-specific immunoglobulin M (IgM) antibodies (which may not be detected until 4 or more days after the onset of rash) or a 4-fold rise in immunoglobulin G. Detection of measles ribonucleic acid by PCR assay also can provide confirmation.3
Vitamin A can lower risk of mortality, blindness
Treatment of measles consists of supportive care and administration of vitamin A—regardless of the patient’s nutritional status. Vitamin A reduces mortality, decreases the risk of corneal damage, and promotes more rapid recovery and shortened hospital stays.1,15 World Health Organization guidelines recommend administering specific dosages of vitamin A on 2 consecutive days based on the patient’s age (TABLE 3).16 For patients with an underlying vitamin A deficiency, a third dose 2 to 4 weeks later is recommended.17
Our patient
We prescribed vitamin A for our patient but did not administer it. The patient did not follow up and we were not able to confirm the outcome.
THE TAKEAWAY
Before patients travel, counsel them on the need for appropriate immunizations. The MMR vaccine should be given to any child older than age 6 months who will be traveling to a high-risk setting. Health-related information for people who plan to travel is available from the CDC at http://wwwnc.cdc.gov/travel and the US Department of State at http://travel.state.gov/content/passports/english/country.html.
To evaluate fever and rash in an individual returning from travel, take a thorough personal and travel history. Suspect measles in patients who present with cough, rhinorrhea, conjunctivitis, diarrhea, and a descending rash that began on the face. The diagnosis can be confirmed with serologic or PCR testing. Treatment should include supportive measures and vitamin A, regardless of the patient’s nutritional status.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
1. Centers for Disease Control and Prevention (CDC). Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR Morb Mortal Wkly Rep. 2003;52:471-475.
2. Moss WJ, Griffin DE. Measles. Lancet. 2012;379:153-164.
3. Centers for Disease Control and Prevention. Measles. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/meas.pdf. Accessed July 24, 2014.
4. Mackell SM. Vaccine recommendations for infants & children. Centers for Disease Control and Prevention Website. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-7-international-travel-infants-children/vaccine-recommendations-for-infants-and-children. Accessed August 8, 2014.
5. Centers for Disease Control and Prevention. Measles cases and outbreaks. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/measles/cases-outbreaks.html. Accessed August 11, 2014.
6. Habif TP. Clinical Dermatology: A Color Guide to Diagnosis and Therapy. 5th ed. Philadelphia, PA: Mosby; 2009.
7. Moss WJ. Measles. Magill AJ, Ryan ET, Solomon T, et al. Hunter’s Tropical Medicine and Emerging Infectious Disease. 9th ed. Philadelphia, PA: Saunders Elsevier Inc; 2012.
8. McKinnon HD, Howard T. Evaluating the febrile patient with a rash. [published correction appears in American Academy of Family Physicians Web site. Available at: http://www.aafp.org/afp/2000/0815/p804.html]. Am Fam Physician. 2000;62:804-816.
9. Wilson ME. Fever in returned travelers. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2012/chapter-5-post-travel-evaluation/fever-in-returned-travelers.htm. Updated August 1, 2013. Accessed July 24, 2014.
10. Lopez FA, Sanders CV. Fever and rash in the immunocompetent patient. UpToDate Web site. Available at: http://www.uptodate. com/contents/fever-and-rash-in-the-immunocompetent-patient. Updated June 23, 2014. Accessed July 24, 2014.
11. Feder HM Jr, Mansilla-River K. Fever in returning travelers: a case-based approach. Am Fam Physician. 2013;88:524-530.
12. Centers for Disease Control and Prevention (CDC). Malaria deaths following inappropriate malaria chemoprophylaxis— United States, 2001. MMWR Morb Mortal Wkly Rep. 2001;50: 597-599.
13. Centers for Disease Control and Prevention. MMWR: Summary of notifiable diseases. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/mmwr/mmwr_ nd/index.html. Accessed July 24, 2014.
14. Lo Re V 3rd, Gluckman SJ. Fever in the returned traveler. Am Fam Physician. 2003;68:1343-1350.
15. Huiming Y, Chaomin W, Meng M. Vitamin A for treating measles in children. Cochrane Database Syst Rev. 2005;(4):CD001479.
16. World Health Organization. WHO guidelines for epidemic preparedness and response to measles outbreaks. World Health Organization Web site. Available at: http://www.who.int/csr/ resources/publications/measles/whocdscsrisr991.pdf. Accessed July 24, 2014.
17. Fiebelkorn AP, Goodson JL. Infectious diseases related to travel. Centers for Disease Control and Prevention Web site. Available at: http://wwwnc.cdc.gov/travel/yellowbook/2014/chapter-3-infectious-diseases-related-to-travel/measles-rubeola. Accessed August 19, 2014.
MANAGING CAP: An evidence-based algorithm
The 2007 guidelines from the Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS)1 are a blend of level-of-evidence strength and consensus opinion—a unified, evidence-based document. these new recommendations address prior discrepancies between the 2 specialties. We developed a CAP treatment algorithm based on the new advisory. (The following text includes levels of evidence.)
Site-of-care decisions
1. Let severity score be your guide
Based on evidence that physicians often hospitalize patients for CAP who could be managed as outpatients, the new guidelines recommend that we use an illness severity score (strong recommendation, level I evidence).
Previous guidelines advised only that we consider using a severity score.
- Use the validated Pneumonia Severity Index or the easier-to-use CURB-65. Patients with a CURB-65 score of 2 or more generally require hospitalization (moderate recommendation, level III evidence).
- Ability to reliably and safely take medications at home must also be taken into account (strong recommendation, level II evidence.)
2. Admit to ICU promptly if needed
The criteria for admission to the ICU is similar to the previous ATS guidelines, but the list of minor criteria is more extensive. This change reflects evidence demonstrating worse outcomes in patients whose transfer to the ICU was delayed. This new criteria has not been validated.
- Patients requiring vasopressors for blood pressure support or with hypoxemic respiratory failure should be admitted to the ICU—these are major criteria (strong recommendation, level II evidence).
- Patients with 3 or more minor criteria should also be directly admitted to the ICU (moderate recommendation, level II evidence).
3. Identify who needs more tests
In the wake of controversy about diagnostic testing recommendations, the new guidelines attempt to better identify patients who would benefit from further testing (TABLE).
- 12 indications. Prior ATS guidelines lacked specifics on required additional testing, but the new guidelines give 12 clinical indications for more extensive evaluation, and identify which tests are recommended for each indication (strong recommendation, level II evidence).
- Routine testing to identify the cause of CAP in outpatients is optional (moderate recommendation, level III evidence).
TABLE
Clinical indications for more extensive diagnostic testing
| CLINICAL INDICATION | RECOMMENDED DIAGNOSTIC TESTS | |||
|---|---|---|---|---|
| BLOOD CULTURE | SPUTUM CULTURE | LEGIONELLA URINARY ANTIGEN TEST | PNEUMOCOCCAL URINARY ANTIGEN TEST | |
| ICU admission* | ||||
| Failed outpatient therapy | ||||
| Cavitary infiltrates† | ||||
| Leukopenia | ||||
| Active alcohol abuse | ||||
| Chronic severe liver disease | ||||
| Severe lung disease | ||||
| Asplenia | ||||
| Anatomic or functional | ||||
| Recent travel‡ | ||||
| Within past 2 weeks | ||||
| Positive Legionella urinary antigen test | N/A | |||
| Positive Pneumococcal urinary antigen test | N/A | |||
| Pleural effusion** | ||||
| Additional tests: | ||||
| * Endotracheal aspirate if intubated, possibly bronchoscopy or nonbronchoscopic bronchoalveolar lavage. | ||||
| † Fungal and tuberculosis cultures. | ||||
| ‡ Region/type of travel related to Legionella, Coccidioides, Hantavirus, B pseudomallei, avian influenza, SARS. | ||||
| ** Thoracentesis and pleural fluid cultures. | ||||
| Adapted from Mandell et al.1 | ||||
Empiric antibiotics
The recommendations of IDSA/ATS are generally for a class of antibiotics rather than a specific drug, unless noted.
4. Assess DRSP risk factors
Growth of drug-resistant Streptococcus pneumoniae (DRSP) necessitated a more extensive list of risk factors for DRSP. Other recommendations did not change.
Outpatient treatment
- Adults who were previously healthy and who do not have risk factors for DRSP CAP should be treated with either a macrolide (azithromycin, clarithromycin, or erythromycin) (strong recommendation, level I evidence) or doxycycline (weak recommendation; level III evidence).
- In the presence of comorbidities that increase the risk for DRSP, these antibiotics are appropriate: a respiratory fluoroquinolone (moxifloxacin, gemifloxacin, or levofloxacin [750 mg/day dose]) (strong recommendation, level I evidence); or β-lactam plus a macrolide: (high-dose amoxicillin [eg, 1 g 3x daily] [strong recommendation, level I evidence] or amoxicillin-clavulanate [2 g twice daily] is preferred; but alternatives include ceftriaxone, cefpodoxime, and cefuroxime [500 mg twice daily]. Doxycycline [level II evidence] is an alternative to the macrolide.)
Inpatient non-ICU treatment
- β-lactam plus a macrolide (strong recommendation, level I evidence) (cefotaxime, ceftriaxone, and ampicillin; ertapenem for selected patients; doxycycline [level III evidence] is an alternative to the macrolide.).
- A respiratory fluoroquinolone (strong recommendation, level I evidence) is the treatment of choice for penicillin-allergic patients.
5. Assess MRSA risk factors
Although similar to the prior ATS guidelines, the new guidelines have added specific risk factors for community-acquired methicillin-resistant S aureus (MRSA). This change reflects the increasing prevalence of community-acquired MRSA as an etiology for CAP.
The new guidelines state that the overwhelming majority of CAP pathogens will be adequately treated with the recommended empiric regimens. Exceptions are infections due to community-acquired methicillin-resistant S aureus and Pseudomonas aeruginosa.
ICU treatment
- A β-lactam (cefotaxime, ceftriaxone, or ampicillin-sulbactam) plus either azithromycin (strong recommendation, level II evidence) or a respiratory fluoroquinolone (strong recommendation, level I evidence).
- For penicillin-allergic patients, a respiratory fluoroquinolone and aztreonam are recommended.
- For Pseudomonas infection (see FIGURE for risk factors), use an anti-pneumococcal, antipseudomonal β-lactam (piperacillin-tazobactam, cefepime, imipenem, or meropenem) plus either ciprofloxacin or levofloxacin (750-mg dose) or the above β-lactam plus an aminoglycoside and azithromycin or the above β-lactam plus aminoglycoside and a respiratory fluoroquinolone (moderate recommendation, level II evidence). Fifteen days of therapy may be more effective in Pseudomonas CAP based on nosocomial infection data.
- For community-acquired methicillin-resistant S aureus infection (see FIGURE for risk factors), add vancomycin or linezolid (moderate recommendation, level III evidence).
Diagnostic testing is of high yield for patients with severe CAP requiring ICU admission, allowing for early de-escalation of empirical treatment if results are negative.
FIGURE
Treatment of community-acquired pneumonia*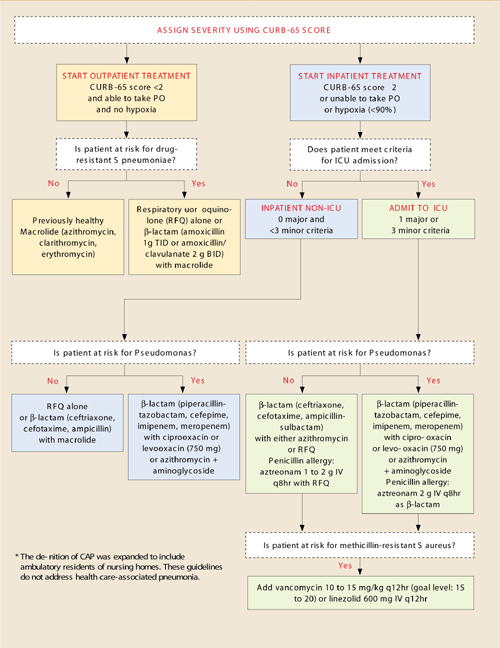
Adapted from: Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44(Suppl 2):S27–S72.
CURB-65 score for assessing severity of illness
Confusion
Uremia BUN >20
Respiration ≥30
BP <90/≤60 mm Hg
≥65 years of age
| TOTAL POINTS | MORTALITY RATE |
|---|---|
| 0 | 0.7% |
| 1 | 2.1% |
| 2 | 9.2% |
| 3 | 14.5% |
| 4 | 40.0% |
| 5 | 57.0% |
Criteria for ICU admission
Major
Invasive mechanical ventilation
Septic shock with need for vasopressors
Minor
- Respiration ≥30
- PaO2/FiO2 ≤250
- Multilobar infiltrates
- Disorientation
- BUN ≥20
- Hypotension requiring aggressive fluids
- Temperature <36°C
- Platelets <100,000
- WBC<4000
Risk factors
Drug-resistant S pneumoniae
- Any antibiotics within 3 months
- Comorbidities: Cardiac disease, diabetes mellitus, alcoholism, pulmonary disease, renal disease, liver disease, asplenia, malignancy, immunosuppressed.
- age >65 years
Pseudomonal infection
- Structural lung disease (bronchiectasis)
- Severe COPD with frequent admissions, recent antibiotic and steroid use
Methicillin-resistant S aureus
Pulmonary abscess
End-stage renal disease
IV drug abuse
Recent influenza
Recent fluroquinolone use
Duration of antibiotic treatment
- At least 5 days
- After 5 days, antibiotics may be discontinued when patient is afebrile 72 hours and has no more than 1 criteria for instability: temperature ≥37.8°C, heart rate ≥100, respiration ≥24, systolic BP ≤90 mm Hg, O2 saturation ≤90%, inability to maintain oral intake, altered mental status
- 15 days for CAP due to Pseudomonas
Criteria for discharge
Temperature ≤37.8°C, heart rate ≤100, respiration ≤24, systolic BP ≥ 90 mm Hg,O2 saturation ≥90%, ability to maintain oral intake, normal mental status
Pathogen-directed therapy
6. Identify the pathogen
New guidelines recommend that, once the pathogen is identified by reliable microbiological methods, therapy should be directed towards that specific pathogen to prevent increased resistance in the community (moderate recommendation, level III evidence).
Influenza. Treatment within 48 hours of symptom onset with oseltamivir or zanamivir is recommended for influenza A (strong recommendation, level I evidence).
While these antimicrobials should not be used in uncomplicated influenza with symptoms for >48 hours (level I evidence), they may be used in hospitalized patients or influenza pneumonia to reduce viral shedding (moderate recommendation, level III evidence).
LEVEL I HIGH
Well-conducted, randomized controlled trials
LEVEL II MODERATE
Well-designed, controlled trials without randomization (including cohort, patient series, and case-controlled studies); large case series in which systematic analysis of disease patterns and/or microbial etiology was conducted; and reports of data on new therapies that were not collected in a randomized fashion.
LEVEL III LOW
Case studies and expert opinion. In some instances, therapy recommendations may come from antibiotic susceptibility data without clinical observations.
Adapted from: Mandell et al.1
Time to first dose
7. Start treatment in the ED
Rather than designating a time window for starting treatment, the IDSA/ATS committee recommended that patients receive the first antibiotic dose in the Emergency Department (moderate recommendation, level III evidence).
This newly added statement contrasts with some current quality measures that grade hospitals according to whether antibiotics are started within a specific time frame.
Duration of antibiotics
8. Base duration on specific criteria
Reflecting evidence that shorter courses appear to be as effective as longer courses, the newer guidelines recommend discontinuation when the patient meets specific clinical criteria. Before discontinuing antibiotics, all patients with CAP should:
- Be treated for at least 5 days (level I evidence),
- Be afebrile for 48 to 72 hours, and
- Have no more than 1 of these criteria for clinical instability (moderate recommendation, level II evidence): temperature ≥37.8°C; heart rate ≥100 beats/min; respiratory rate ≥24 breaths/min; systolic blood pressure ≤90 mm Hg; arterial oxygen saturation ≤90% or pO2 ≤60 mm Hg on room air; inability to maintain oral intake; altered mental status.
Switching from IV to oral
The guidelines, similar to the prior guidelines, recommend switching to oral therapy for hemodynamically stable patients who are clinically improving, able to ingest medications, and have a normally functioning gastrointestinal tract (strong recommendation, level II evidence).
Hospital discharge
The guidelines recommend that patients be discharged as soon as they are clinically stable and have a safe environment for continued care. Patients receiving oral therapy do not require inpatient observation (moderate recommendation, level II evidence). This is unchanged from prior recommendations.
1. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell D, Dean NC, et al. IDSA/ATS consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44:(Suppl 2) S27-S72.
The 2007 guidelines from the Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS)1 are a blend of level-of-evidence strength and consensus opinion—a unified, evidence-based document. these new recommendations address prior discrepancies between the 2 specialties. We developed a CAP treatment algorithm based on the new advisory. (The following text includes levels of evidence.)
Site-of-care decisions
1. Let severity score be your guide
Based on evidence that physicians often hospitalize patients for CAP who could be managed as outpatients, the new guidelines recommend that we use an illness severity score (strong recommendation, level I evidence).
Previous guidelines advised only that we consider using a severity score.
- Use the validated Pneumonia Severity Index or the easier-to-use CURB-65. Patients with a CURB-65 score of 2 or more generally require hospitalization (moderate recommendation, level III evidence).
- Ability to reliably and safely take medications at home must also be taken into account (strong recommendation, level II evidence.)
2. Admit to ICU promptly if needed
The criteria for admission to the ICU is similar to the previous ATS guidelines, but the list of minor criteria is more extensive. This change reflects evidence demonstrating worse outcomes in patients whose transfer to the ICU was delayed. This new criteria has not been validated.
- Patients requiring vasopressors for blood pressure support or with hypoxemic respiratory failure should be admitted to the ICU—these are major criteria (strong recommendation, level II evidence).
- Patients with 3 or more minor criteria should also be directly admitted to the ICU (moderate recommendation, level II evidence).
3. Identify who needs more tests
In the wake of controversy about diagnostic testing recommendations, the new guidelines attempt to better identify patients who would benefit from further testing (TABLE).
- 12 indications. Prior ATS guidelines lacked specifics on required additional testing, but the new guidelines give 12 clinical indications for more extensive evaluation, and identify which tests are recommended for each indication (strong recommendation, level II evidence).
- Routine testing to identify the cause of CAP in outpatients is optional (moderate recommendation, level III evidence).
TABLE
Clinical indications for more extensive diagnostic testing
| CLINICAL INDICATION | RECOMMENDED DIAGNOSTIC TESTS | |||
|---|---|---|---|---|
| BLOOD CULTURE | SPUTUM CULTURE | LEGIONELLA URINARY ANTIGEN TEST | PNEUMOCOCCAL URINARY ANTIGEN TEST | |
| ICU admission* | ||||
| Failed outpatient therapy | ||||
| Cavitary infiltrates† | ||||
| Leukopenia | ||||
| Active alcohol abuse | ||||
| Chronic severe liver disease | ||||
| Severe lung disease | ||||
| Asplenia | ||||
| Anatomic or functional | ||||
| Recent travel‡ | ||||
| Within past 2 weeks | ||||
| Positive Legionella urinary antigen test | N/A | |||
| Positive Pneumococcal urinary antigen test | N/A | |||
| Pleural effusion** | ||||
| Additional tests: | ||||
| * Endotracheal aspirate if intubated, possibly bronchoscopy or nonbronchoscopic bronchoalveolar lavage. | ||||
| † Fungal and tuberculosis cultures. | ||||
| ‡ Region/type of travel related to Legionella, Coccidioides, Hantavirus, B pseudomallei, avian influenza, SARS. | ||||
| ** Thoracentesis and pleural fluid cultures. | ||||
| Adapted from Mandell et al.1 | ||||
Empiric antibiotics
The recommendations of IDSA/ATS are generally for a class of antibiotics rather than a specific drug, unless noted.
4. Assess DRSP risk factors
Growth of drug-resistant Streptococcus pneumoniae (DRSP) necessitated a more extensive list of risk factors for DRSP. Other recommendations did not change.
Outpatient treatment
- Adults who were previously healthy and who do not have risk factors for DRSP CAP should be treated with either a macrolide (azithromycin, clarithromycin, or erythromycin) (strong recommendation, level I evidence) or doxycycline (weak recommendation; level III evidence).
- In the presence of comorbidities that increase the risk for DRSP, these antibiotics are appropriate: a respiratory fluoroquinolone (moxifloxacin, gemifloxacin, or levofloxacin [750 mg/day dose]) (strong recommendation, level I evidence); or β-lactam plus a macrolide: (high-dose amoxicillin [eg, 1 g 3x daily] [strong recommendation, level I evidence] or amoxicillin-clavulanate [2 g twice daily] is preferred; but alternatives include ceftriaxone, cefpodoxime, and cefuroxime [500 mg twice daily]. Doxycycline [level II evidence] is an alternative to the macrolide.)
Inpatient non-ICU treatment
- β-lactam plus a macrolide (strong recommendation, level I evidence) (cefotaxime, ceftriaxone, and ampicillin; ertapenem for selected patients; doxycycline [level III evidence] is an alternative to the macrolide.).
- A respiratory fluoroquinolone (strong recommendation, level I evidence) is the treatment of choice for penicillin-allergic patients.
5. Assess MRSA risk factors
Although similar to the prior ATS guidelines, the new guidelines have added specific risk factors for community-acquired methicillin-resistant S aureus (MRSA). This change reflects the increasing prevalence of community-acquired MRSA as an etiology for CAP.
The new guidelines state that the overwhelming majority of CAP pathogens will be adequately treated with the recommended empiric regimens. Exceptions are infections due to community-acquired methicillin-resistant S aureus and Pseudomonas aeruginosa.
ICU treatment
- A β-lactam (cefotaxime, ceftriaxone, or ampicillin-sulbactam) plus either azithromycin (strong recommendation, level II evidence) or a respiratory fluoroquinolone (strong recommendation, level I evidence).
- For penicillin-allergic patients, a respiratory fluoroquinolone and aztreonam are recommended.
- For Pseudomonas infection (see FIGURE for risk factors), use an anti-pneumococcal, antipseudomonal β-lactam (piperacillin-tazobactam, cefepime, imipenem, or meropenem) plus either ciprofloxacin or levofloxacin (750-mg dose) or the above β-lactam plus an aminoglycoside and azithromycin or the above β-lactam plus aminoglycoside and a respiratory fluoroquinolone (moderate recommendation, level II evidence). Fifteen days of therapy may be more effective in Pseudomonas CAP based on nosocomial infection data.
- For community-acquired methicillin-resistant S aureus infection (see FIGURE for risk factors), add vancomycin or linezolid (moderate recommendation, level III evidence).
Diagnostic testing is of high yield for patients with severe CAP requiring ICU admission, allowing for early de-escalation of empirical treatment if results are negative.
FIGURE
Treatment of community-acquired pneumonia*
Adapted from: Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44(Suppl 2):S27–S72.
CURB-65 score for assessing severity of illness
Confusion
Uremia BUN >20
Respiration ≥30
BP <90/≤60 mm Hg
≥65 years of age
| TOTAL POINTS | MORTALITY RATE |
|---|---|
| 0 | 0.7% |
| 1 | 2.1% |
| 2 | 9.2% |
| 3 | 14.5% |
| 4 | 40.0% |
| 5 | 57.0% |
Criteria for ICU admission
Major
Invasive mechanical ventilation
Septic shock with need for vasopressors
Minor
- Respiration ≥30
- PaO2/FiO2 ≤250
- Multilobar infiltrates
- Disorientation
- BUN ≥20
- Hypotension requiring aggressive fluids
- Temperature <36°C
- Platelets <100,000
- WBC<4000
Risk factors
Drug-resistant S pneumoniae
- Any antibiotics within 3 months
- Comorbidities: Cardiac disease, diabetes mellitus, alcoholism, pulmonary disease, renal disease, liver disease, asplenia, malignancy, immunosuppressed.
- age >65 years
Pseudomonal infection
- Structural lung disease (bronchiectasis)
- Severe COPD with frequent admissions, recent antibiotic and steroid use
Methicillin-resistant S aureus
Pulmonary abscess
End-stage renal disease
IV drug abuse
Recent influenza
Recent fluroquinolone use
Duration of antibiotic treatment
- At least 5 days
- After 5 days, antibiotics may be discontinued when patient is afebrile 72 hours and has no more than 1 criteria for instability: temperature ≥37.8°C, heart rate ≥100, respiration ≥24, systolic BP ≤90 mm Hg, O2 saturation ≤90%, inability to maintain oral intake, altered mental status
- 15 days for CAP due to Pseudomonas
Criteria for discharge
Temperature ≤37.8°C, heart rate ≤100, respiration ≤24, systolic BP ≥ 90 mm Hg,O2 saturation ≥90%, ability to maintain oral intake, normal mental status
Pathogen-directed therapy
6. Identify the pathogen
New guidelines recommend that, once the pathogen is identified by reliable microbiological methods, therapy should be directed towards that specific pathogen to prevent increased resistance in the community (moderate recommendation, level III evidence).
Influenza. Treatment within 48 hours of symptom onset with oseltamivir or zanamivir is recommended for influenza A (strong recommendation, level I evidence).
While these antimicrobials should not be used in uncomplicated influenza with symptoms for >48 hours (level I evidence), they may be used in hospitalized patients or influenza pneumonia to reduce viral shedding (moderate recommendation, level III evidence).
LEVEL I HIGH
Well-conducted, randomized controlled trials
LEVEL II MODERATE
Well-designed, controlled trials without randomization (including cohort, patient series, and case-controlled studies); large case series in which systematic analysis of disease patterns and/or microbial etiology was conducted; and reports of data on new therapies that were not collected in a randomized fashion.
LEVEL III LOW
Case studies and expert opinion. In some instances, therapy recommendations may come from antibiotic susceptibility data without clinical observations.
Adapted from: Mandell et al.1
Time to first dose
7. Start treatment in the ED
Rather than designating a time window for starting treatment, the IDSA/ATS committee recommended that patients receive the first antibiotic dose in the Emergency Department (moderate recommendation, level III evidence).
This newly added statement contrasts with some current quality measures that grade hospitals according to whether antibiotics are started within a specific time frame.
Duration of antibiotics
8. Base duration on specific criteria
Reflecting evidence that shorter courses appear to be as effective as longer courses, the newer guidelines recommend discontinuation when the patient meets specific clinical criteria. Before discontinuing antibiotics, all patients with CAP should:
- Be treated for at least 5 days (level I evidence),
- Be afebrile for 48 to 72 hours, and
- Have no more than 1 of these criteria for clinical instability (moderate recommendation, level II evidence): temperature ≥37.8°C; heart rate ≥100 beats/min; respiratory rate ≥24 breaths/min; systolic blood pressure ≤90 mm Hg; arterial oxygen saturation ≤90% or pO2 ≤60 mm Hg on room air; inability to maintain oral intake; altered mental status.
Switching from IV to oral
The guidelines, similar to the prior guidelines, recommend switching to oral therapy for hemodynamically stable patients who are clinically improving, able to ingest medications, and have a normally functioning gastrointestinal tract (strong recommendation, level II evidence).
Hospital discharge
The guidelines recommend that patients be discharged as soon as they are clinically stable and have a safe environment for continued care. Patients receiving oral therapy do not require inpatient observation (moderate recommendation, level II evidence). This is unchanged from prior recommendations.
The 2007 guidelines from the Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS)1 are a blend of level-of-evidence strength and consensus opinion—a unified, evidence-based document. these new recommendations address prior discrepancies between the 2 specialties. We developed a CAP treatment algorithm based on the new advisory. (The following text includes levels of evidence.)
Site-of-care decisions
1. Let severity score be your guide
Based on evidence that physicians often hospitalize patients for CAP who could be managed as outpatients, the new guidelines recommend that we use an illness severity score (strong recommendation, level I evidence).
Previous guidelines advised only that we consider using a severity score.
- Use the validated Pneumonia Severity Index or the easier-to-use CURB-65. Patients with a CURB-65 score of 2 or more generally require hospitalization (moderate recommendation, level III evidence).
- Ability to reliably and safely take medications at home must also be taken into account (strong recommendation, level II evidence.)
2. Admit to ICU promptly if needed
The criteria for admission to the ICU is similar to the previous ATS guidelines, but the list of minor criteria is more extensive. This change reflects evidence demonstrating worse outcomes in patients whose transfer to the ICU was delayed. This new criteria has not been validated.
- Patients requiring vasopressors for blood pressure support or with hypoxemic respiratory failure should be admitted to the ICU—these are major criteria (strong recommendation, level II evidence).
- Patients with 3 or more minor criteria should also be directly admitted to the ICU (moderate recommendation, level II evidence).
3. Identify who needs more tests
In the wake of controversy about diagnostic testing recommendations, the new guidelines attempt to better identify patients who would benefit from further testing (TABLE).
- 12 indications. Prior ATS guidelines lacked specifics on required additional testing, but the new guidelines give 12 clinical indications for more extensive evaluation, and identify which tests are recommended for each indication (strong recommendation, level II evidence).
- Routine testing to identify the cause of CAP in outpatients is optional (moderate recommendation, level III evidence).
TABLE
Clinical indications for more extensive diagnostic testing
| CLINICAL INDICATION | RECOMMENDED DIAGNOSTIC TESTS | |||
|---|---|---|---|---|
| BLOOD CULTURE | SPUTUM CULTURE | LEGIONELLA URINARY ANTIGEN TEST | PNEUMOCOCCAL URINARY ANTIGEN TEST | |
| ICU admission* | ||||
| Failed outpatient therapy | ||||
| Cavitary infiltrates† | ||||
| Leukopenia | ||||
| Active alcohol abuse | ||||
| Chronic severe liver disease | ||||
| Severe lung disease | ||||
| Asplenia | ||||
| Anatomic or functional | ||||
| Recent travel‡ | ||||
| Within past 2 weeks | ||||
| Positive Legionella urinary antigen test | N/A | |||
| Positive Pneumococcal urinary antigen test | N/A | |||
| Pleural effusion** | ||||
| Additional tests: | ||||
| * Endotracheal aspirate if intubated, possibly bronchoscopy or nonbronchoscopic bronchoalveolar lavage. | ||||
| † Fungal and tuberculosis cultures. | ||||
| ‡ Region/type of travel related to Legionella, Coccidioides, Hantavirus, B pseudomallei, avian influenza, SARS. | ||||
| ** Thoracentesis and pleural fluid cultures. | ||||
| Adapted from Mandell et al.1 | ||||
Empiric antibiotics
The recommendations of IDSA/ATS are generally for a class of antibiotics rather than a specific drug, unless noted.
4. Assess DRSP risk factors
Growth of drug-resistant Streptococcus pneumoniae (DRSP) necessitated a more extensive list of risk factors for DRSP. Other recommendations did not change.
Outpatient treatment
- Adults who were previously healthy and who do not have risk factors for DRSP CAP should be treated with either a macrolide (azithromycin, clarithromycin, or erythromycin) (strong recommendation, level I evidence) or doxycycline (weak recommendation; level III evidence).
- In the presence of comorbidities that increase the risk for DRSP, these antibiotics are appropriate: a respiratory fluoroquinolone (moxifloxacin, gemifloxacin, or levofloxacin [750 mg/day dose]) (strong recommendation, level I evidence); or β-lactam plus a macrolide: (high-dose amoxicillin [eg, 1 g 3x daily] [strong recommendation, level I evidence] or amoxicillin-clavulanate [2 g twice daily] is preferred; but alternatives include ceftriaxone, cefpodoxime, and cefuroxime [500 mg twice daily]. Doxycycline [level II evidence] is an alternative to the macrolide.)
Inpatient non-ICU treatment
- β-lactam plus a macrolide (strong recommendation, level I evidence) (cefotaxime, ceftriaxone, and ampicillin; ertapenem for selected patients; doxycycline [level III evidence] is an alternative to the macrolide.).
- A respiratory fluoroquinolone (strong recommendation, level I evidence) is the treatment of choice for penicillin-allergic patients.
5. Assess MRSA risk factors
Although similar to the prior ATS guidelines, the new guidelines have added specific risk factors for community-acquired methicillin-resistant S aureus (MRSA). This change reflects the increasing prevalence of community-acquired MRSA as an etiology for CAP.
The new guidelines state that the overwhelming majority of CAP pathogens will be adequately treated with the recommended empiric regimens. Exceptions are infections due to community-acquired methicillin-resistant S aureus and Pseudomonas aeruginosa.
ICU treatment
- A β-lactam (cefotaxime, ceftriaxone, or ampicillin-sulbactam) plus either azithromycin (strong recommendation, level II evidence) or a respiratory fluoroquinolone (strong recommendation, level I evidence).
- For penicillin-allergic patients, a respiratory fluoroquinolone and aztreonam are recommended.
- For Pseudomonas infection (see FIGURE for risk factors), use an anti-pneumococcal, antipseudomonal β-lactam (piperacillin-tazobactam, cefepime, imipenem, or meropenem) plus either ciprofloxacin or levofloxacin (750-mg dose) or the above β-lactam plus an aminoglycoside and azithromycin or the above β-lactam plus aminoglycoside and a respiratory fluoroquinolone (moderate recommendation, level II evidence). Fifteen days of therapy may be more effective in Pseudomonas CAP based on nosocomial infection data.
- For community-acquired methicillin-resistant S aureus infection (see FIGURE for risk factors), add vancomycin or linezolid (moderate recommendation, level III evidence).
Diagnostic testing is of high yield for patients with severe CAP requiring ICU admission, allowing for early de-escalation of empirical treatment if results are negative.
FIGURE
Treatment of community-acquired pneumonia*
Adapted from: Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44(Suppl 2):S27–S72.
CURB-65 score for assessing severity of illness
Confusion
Uremia BUN >20
Respiration ≥30
BP <90/≤60 mm Hg
≥65 years of age
| TOTAL POINTS | MORTALITY RATE |
|---|---|
| 0 | 0.7% |
| 1 | 2.1% |
| 2 | 9.2% |
| 3 | 14.5% |
| 4 | 40.0% |
| 5 | 57.0% |
Criteria for ICU admission
Major
Invasive mechanical ventilation
Septic shock with need for vasopressors
Minor
- Respiration ≥30
- PaO2/FiO2 ≤250
- Multilobar infiltrates
- Disorientation
- BUN ≥20
- Hypotension requiring aggressive fluids
- Temperature <36°C
- Platelets <100,000
- WBC<4000
Risk factors
Drug-resistant S pneumoniae
- Any antibiotics within 3 months
- Comorbidities: Cardiac disease, diabetes mellitus, alcoholism, pulmonary disease, renal disease, liver disease, asplenia, malignancy, immunosuppressed.
- age >65 years
Pseudomonal infection
- Structural lung disease (bronchiectasis)
- Severe COPD with frequent admissions, recent antibiotic and steroid use
Methicillin-resistant S aureus
Pulmonary abscess
End-stage renal disease
IV drug abuse
Recent influenza
Recent fluroquinolone use
Duration of antibiotic treatment
- At least 5 days
- After 5 days, antibiotics may be discontinued when patient is afebrile 72 hours and has no more than 1 criteria for instability: temperature ≥37.8°C, heart rate ≥100, respiration ≥24, systolic BP ≤90 mm Hg, O2 saturation ≤90%, inability to maintain oral intake, altered mental status
- 15 days for CAP due to Pseudomonas
Criteria for discharge
Temperature ≤37.8°C, heart rate ≤100, respiration ≤24, systolic BP ≥ 90 mm Hg,O2 saturation ≥90%, ability to maintain oral intake, normal mental status
Pathogen-directed therapy
6. Identify the pathogen
New guidelines recommend that, once the pathogen is identified by reliable microbiological methods, therapy should be directed towards that specific pathogen to prevent increased resistance in the community (moderate recommendation, level III evidence).
Influenza. Treatment within 48 hours of symptom onset with oseltamivir or zanamivir is recommended for influenza A (strong recommendation, level I evidence).
While these antimicrobials should not be used in uncomplicated influenza with symptoms for >48 hours (level I evidence), they may be used in hospitalized patients or influenza pneumonia to reduce viral shedding (moderate recommendation, level III evidence).
LEVEL I HIGH
Well-conducted, randomized controlled trials
LEVEL II MODERATE
Well-designed, controlled trials without randomization (including cohort, patient series, and case-controlled studies); large case series in which systematic analysis of disease patterns and/or microbial etiology was conducted; and reports of data on new therapies that were not collected in a randomized fashion.
LEVEL III LOW
Case studies and expert opinion. In some instances, therapy recommendations may come from antibiotic susceptibility data without clinical observations.
Adapted from: Mandell et al.1
Time to first dose
7. Start treatment in the ED
Rather than designating a time window for starting treatment, the IDSA/ATS committee recommended that patients receive the first antibiotic dose in the Emergency Department (moderate recommendation, level III evidence).
This newly added statement contrasts with some current quality measures that grade hospitals according to whether antibiotics are started within a specific time frame.
Duration of antibiotics
8. Base duration on specific criteria
Reflecting evidence that shorter courses appear to be as effective as longer courses, the newer guidelines recommend discontinuation when the patient meets specific clinical criteria. Before discontinuing antibiotics, all patients with CAP should:
- Be treated for at least 5 days (level I evidence),
- Be afebrile for 48 to 72 hours, and
- Have no more than 1 of these criteria for clinical instability (moderate recommendation, level II evidence): temperature ≥37.8°C; heart rate ≥100 beats/min; respiratory rate ≥24 breaths/min; systolic blood pressure ≤90 mm Hg; arterial oxygen saturation ≤90% or pO2 ≤60 mm Hg on room air; inability to maintain oral intake; altered mental status.
Switching from IV to oral
The guidelines, similar to the prior guidelines, recommend switching to oral therapy for hemodynamically stable patients who are clinically improving, able to ingest medications, and have a normally functioning gastrointestinal tract (strong recommendation, level II evidence).
Hospital discharge
The guidelines recommend that patients be discharged as soon as they are clinically stable and have a safe environment for continued care. Patients receiving oral therapy do not require inpatient observation (moderate recommendation, level II evidence). This is unchanged from prior recommendations.
1. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell D, Dean NC, et al. IDSA/ATS consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44:(Suppl 2) S27-S72.
1. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell D, Dean NC, et al. IDSA/ATS consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44:(Suppl 2) S27-S72.