User login
Herbal medicine can reduce pain, fatigue in SCD patients

Convention Center, site of
the 2016 ASH Annual Meeting
SAN DIEGO—Results of a phase 1 study suggest that SCD-101, a botanical extract based on an herbal medicine used in Nigeria to treat sickle cell disease (SCD), can reduce pain and fatigue in people with SCD.
The anti-sickling drug also improves the shape of red blood cells but doesn’t produce a change in hemoglobin, according to researchers.
Peter Gillette, MD, of SUNY Downstate in Brooklyn, New York, reported these results at the 2016 ASH Annual Meeting (abstract 121*).
A 6-month phase 2b study conducted previously in Nigeria showed that the herbal medicine Niprisan reduced pain crises and school absenteeism and raised hemoglobin levels compared to placebo.
Based on this study and positive preclinical activity, Dr Gillette and his colleagues undertook a phase 1 study to determine the safety of escalating doses of SCD-101.
Dr Gillette pointed out that Niprisan had been produced commercially in Nigeria but was later removed by the government from the commercial market because of production problems.
The researchers evaluated 23 patients with homozygous SCD or S/beta0 thalassemia.
Patients were aged 18 to 55 years with hemoglobin F of 15% or less and hemoglobin levels between 6.0 and 9.5 g/dL.
Patients could not have had hydroxyurea treatment within 6 months of enrollment, red blood cell transfusion within 3 months, or hospitalization within 4 weeks.
Patients received SCD-101 orally for 28 days administered 2 times daily (BID) or 3 times daily (TID). Doses were 550 mg BID, 1100 mg BID, 2200 mg BID, 4400 mg BID, and 2750 mg TID.
Dr Gillette explained that by distributing the highest dose 3 times over the course of a day, the researchers were able to decrease the side effects of bloating and flatulence on the highest dose.
“Interestingly, with the dose-distributed TID, we found that the hemoglobin had increased by 10%,” he said. “In other words, it appears that the effects are very short-acting, and that by going from a Q12 to a Q8 dosage, the hemoglobin suddenly looks like it might be significant, although this is not a significant change.”
Laboratory outcomes included hemoglobin and hemolysis (LDH, bilirubin, and reticulocyte measurements). Patient-reported outcomes included pain and fatigue.
The most common adverse events (AEs) were pain, flatulence, bloating, diarrhea, constipation, nausea, and headache.
Seven patients in the 2200 mg BID and 4400 mg BID cohorts had dose-related bloating, gas, flatulence or diarrhea, which subsided in a few days.
Patients in the 2750 mg TID cohort did not experience gas side effects.
The gastrointestinal symptoms were most likely dose-related from an excipient of SCD-101, Dr Gillette said.
He and his colleagues found no significant side effects after 28 days of dosing, and there were no dose reductions or interruptions due to drug-related AEs.
There were also no laboratory or electrocardiogram abnormalities.
“Almost all pain AEs stopped by day 13 in 22 of 23 patients,” Dr Gillette said.
“And unexpectedly, patients began to report that they slept better and had improved energy and cognition,” he noted.
Six patients in the 2200 and 4400 mg BID cohorts reported reduced fatigue as measured by the PROMIS fatigue questionnaire.
And 2 patients with ankle ulcers in the 2 highest dose cohorts reported improved healing.
Two weeks after treatment stopped, patients were almost back to baseline in terms of their chronic pain and fatigue levels, Dr Gillette said.
A parallel design, double-blind, placebo-controlled pilot study of the 2750 mg TID dose is ongoing.
Future studies include a crossover-design, exploratory study of the 2750 mg TID dose and a phase 2 parallel design study of the 2200 mg BID and 2750 mg TID doses.
While the researchers are uncertain about the mechanism of action of SCD-101, they hypothesize that its effects could be due to increased vascular flow, increased oxygen delivery, or a reduction in inflammation.
“This is a promising drug potentially for low-income countries or middle-income countries elsewhere in the world where gene therapy and transplant are really not that feasible,” Dr Gillette said.
Research for this study was supported in part by the National Heart, Lung, and Blood Institute and National Center for Complementary and Integrative Health of the National Institutes of Health. ![]()
*Information presented at the meeting differs from the abstract.
Convention Center, site of
the 2016 ASH Annual Meeting
SAN DIEGO—Results of a phase 1 study suggest that SCD-101, a botanical extract based on an herbal medicine used in Nigeria to treat sickle cell disease (SCD), can reduce pain and fatigue in people with SCD.
The anti-sickling drug also improves the shape of red blood cells but doesn’t produce a change in hemoglobin, according to researchers.
Peter Gillette, MD, of SUNY Downstate in Brooklyn, New York, reported these results at the 2016 ASH Annual Meeting (abstract 121*).
A 6-month phase 2b study conducted previously in Nigeria showed that the herbal medicine Niprisan reduced pain crises and school absenteeism and raised hemoglobin levels compared to placebo.
Based on this study and positive preclinical activity, Dr Gillette and his colleagues undertook a phase 1 study to determine the safety of escalating doses of SCD-101.
Dr Gillette pointed out that Niprisan had been produced commercially in Nigeria but was later removed by the government from the commercial market because of production problems.
The researchers evaluated 23 patients with homozygous SCD or S/beta0 thalassemia.
Patients were aged 18 to 55 years with hemoglobin F of 15% or less and hemoglobin levels between 6.0 and 9.5 g/dL.
Patients could not have had hydroxyurea treatment within 6 months of enrollment, red blood cell transfusion within 3 months, or hospitalization within 4 weeks.
Patients received SCD-101 orally for 28 days administered 2 times daily (BID) or 3 times daily (TID). Doses were 550 mg BID, 1100 mg BID, 2200 mg BID, 4400 mg BID, and 2750 mg TID.
Dr Gillette explained that by distributing the highest dose 3 times over the course of a day, the researchers were able to decrease the side effects of bloating and flatulence on the highest dose.
“Interestingly, with the dose-distributed TID, we found that the hemoglobin had increased by 10%,” he said. “In other words, it appears that the effects are very short-acting, and that by going from a Q12 to a Q8 dosage, the hemoglobin suddenly looks like it might be significant, although this is not a significant change.”
Laboratory outcomes included hemoglobin and hemolysis (LDH, bilirubin, and reticulocyte measurements). Patient-reported outcomes included pain and fatigue.
The most common adverse events (AEs) were pain, flatulence, bloating, diarrhea, constipation, nausea, and headache.
Seven patients in the 2200 mg BID and 4400 mg BID cohorts had dose-related bloating, gas, flatulence or diarrhea, which subsided in a few days.
Patients in the 2750 mg TID cohort did not experience gas side effects.
The gastrointestinal symptoms were most likely dose-related from an excipient of SCD-101, Dr Gillette said.
He and his colleagues found no significant side effects after 28 days of dosing, and there were no dose reductions or interruptions due to drug-related AEs.
There were also no laboratory or electrocardiogram abnormalities.
“Almost all pain AEs stopped by day 13 in 22 of 23 patients,” Dr Gillette said.
“And unexpectedly, patients began to report that they slept better and had improved energy and cognition,” he noted.
Six patients in the 2200 and 4400 mg BID cohorts reported reduced fatigue as measured by the PROMIS fatigue questionnaire.
And 2 patients with ankle ulcers in the 2 highest dose cohorts reported improved healing.
Two weeks after treatment stopped, patients were almost back to baseline in terms of their chronic pain and fatigue levels, Dr Gillette said.
A parallel design, double-blind, placebo-controlled pilot study of the 2750 mg TID dose is ongoing.
Future studies include a crossover-design, exploratory study of the 2750 mg TID dose and a phase 2 parallel design study of the 2200 mg BID and 2750 mg TID doses.
While the researchers are uncertain about the mechanism of action of SCD-101, they hypothesize that its effects could be due to increased vascular flow, increased oxygen delivery, or a reduction in inflammation.
“This is a promising drug potentially for low-income countries or middle-income countries elsewhere in the world where gene therapy and transplant are really not that feasible,” Dr Gillette said.
Research for this study was supported in part by the National Heart, Lung, and Blood Institute and National Center for Complementary and Integrative Health of the National Institutes of Health. ![]()
*Information presented at the meeting differs from the abstract.
Convention Center, site of
the 2016 ASH Annual Meeting
SAN DIEGO—Results of a phase 1 study suggest that SCD-101, a botanical extract based on an herbal medicine used in Nigeria to treat sickle cell disease (SCD), can reduce pain and fatigue in people with SCD.
The anti-sickling drug also improves the shape of red blood cells but doesn’t produce a change in hemoglobin, according to researchers.
Peter Gillette, MD, of SUNY Downstate in Brooklyn, New York, reported these results at the 2016 ASH Annual Meeting (abstract 121*).
A 6-month phase 2b study conducted previously in Nigeria showed that the herbal medicine Niprisan reduced pain crises and school absenteeism and raised hemoglobin levels compared to placebo.
Based on this study and positive preclinical activity, Dr Gillette and his colleagues undertook a phase 1 study to determine the safety of escalating doses of SCD-101.
Dr Gillette pointed out that Niprisan had been produced commercially in Nigeria but was later removed by the government from the commercial market because of production problems.
The researchers evaluated 23 patients with homozygous SCD or S/beta0 thalassemia.
Patients were aged 18 to 55 years with hemoglobin F of 15% or less and hemoglobin levels between 6.0 and 9.5 g/dL.
Patients could not have had hydroxyurea treatment within 6 months of enrollment, red blood cell transfusion within 3 months, or hospitalization within 4 weeks.
Patients received SCD-101 orally for 28 days administered 2 times daily (BID) or 3 times daily (TID). Doses were 550 mg BID, 1100 mg BID, 2200 mg BID, 4400 mg BID, and 2750 mg TID.
Dr Gillette explained that by distributing the highest dose 3 times over the course of a day, the researchers were able to decrease the side effects of bloating and flatulence on the highest dose.
“Interestingly, with the dose-distributed TID, we found that the hemoglobin had increased by 10%,” he said. “In other words, it appears that the effects are very short-acting, and that by going from a Q12 to a Q8 dosage, the hemoglobin suddenly looks like it might be significant, although this is not a significant change.”
Laboratory outcomes included hemoglobin and hemolysis (LDH, bilirubin, and reticulocyte measurements). Patient-reported outcomes included pain and fatigue.
The most common adverse events (AEs) were pain, flatulence, bloating, diarrhea, constipation, nausea, and headache.
Seven patients in the 2200 mg BID and 4400 mg BID cohorts had dose-related bloating, gas, flatulence or diarrhea, which subsided in a few days.
Patients in the 2750 mg TID cohort did not experience gas side effects.
The gastrointestinal symptoms were most likely dose-related from an excipient of SCD-101, Dr Gillette said.
He and his colleagues found no significant side effects after 28 days of dosing, and there were no dose reductions or interruptions due to drug-related AEs.
There were also no laboratory or electrocardiogram abnormalities.
“Almost all pain AEs stopped by day 13 in 22 of 23 patients,” Dr Gillette said.
“And unexpectedly, patients began to report that they slept better and had improved energy and cognition,” he noted.
Six patients in the 2200 and 4400 mg BID cohorts reported reduced fatigue as measured by the PROMIS fatigue questionnaire.
And 2 patients with ankle ulcers in the 2 highest dose cohorts reported improved healing.
Two weeks after treatment stopped, patients were almost back to baseline in terms of their chronic pain and fatigue levels, Dr Gillette said.
A parallel design, double-blind, placebo-controlled pilot study of the 2750 mg TID dose is ongoing.
Future studies include a crossover-design, exploratory study of the 2750 mg TID dose and a phase 2 parallel design study of the 2200 mg BID and 2750 mg TID doses.
While the researchers are uncertain about the mechanism of action of SCD-101, they hypothesize that its effects could be due to increased vascular flow, increased oxygen delivery, or a reduction in inflammation.
“This is a promising drug potentially for low-income countries or middle-income countries elsewhere in the world where gene therapy and transplant are really not that feasible,” Dr Gillette said.
Research for this study was supported in part by the National Heart, Lung, and Blood Institute and National Center for Complementary and Integrative Health of the National Institutes of Health. ![]()
*Information presented at the meeting differs from the abstract.
Combine flow and HTS for sensitive MRD detection in CLL, speaker says

laser beam
Photo courtesy of NIH
NEW YORK—Combining 2 technologies—flow cytometry and high-throughput sequencing (HTS)—produces a very sensitive approach to detecting minimal residual disease (MRD) in chronic lymphocytic leukemia (CLL), according to a speaker at Lymphoma & Myeloma 2016.
The approach is both reproducible and widely accessible, added the speaker, Peter Hillmen, MB ChB, PhD, of St James’s University Hospital in Leeds, UK.
“PCR [polymerase chain reaction] is more sensitive than flow cytometry,” he noted, “but it is probably not necessary to assess response by that criteria.”
Features to consider when choosing a technology for detecting MRD include sensitivity, specificity for the patient and/or the disease, applicability to all patients or to an individual, the platform—flow cytometry, conventional molecular PCR, or next-generation sequencing—and which tissue to use, blood or bone marrow.
In the era of immunotherapy, Dr Hillmen said, assessment should be performed at least 2 months after completion of immunotherapy to get a reliable assessment of MRD, particularly after treatment with alemtuzumab, rituximab, and other antibodies targeting CLL.
History of MRD analysis
The definition of MRD hasn’t changed since 2008, when the International Workshop on CLL updated National Cancer Institute guidelines. It is still 1 single cell in 10,000 (10-4) leukocytes, regardless of the tissue used.
Prior to the mid-1990s, there were limited options for assessing MRD, Dr Hillmen said.
Based on the profound remissions patients experienced with alemtuzumab, investigators began to develop assays to assess MRD.
“[W]e started standardizing these assays around 2007,” Dr Hillmen said, and a standardized assay was used prospectively in clinical trials beginning in 2012.
Technologies
Several technologies can be used to assess MRD.
Flow cytometry using 6 colors or 8 colors—to simplify the assay and to make it more sensitive—is a multiparameter assessment of CLL phenotype that is not clonality-based.
Allele-specific oligonucleotide PCR (ASO-PCR) is laborious to perform, Dr Hillmen said, but it’s very sensitive.
“[I]t probably shouldn’t be considered as an MRD test,” he said, since it uses patient-specific primers, not consensus primers.
HTS provides an increasing amount of information on B-cell sequences and enumeration of the CLL-specific immunoglobulin gene, “and I would move it towards being approved as a regulatory endpoint,” Dr Hillmen asserted.
Flow cytometry and HTS
A consensus document by the European Research Initiative on CLL (ERIC) identified and validated a flow cytometric approach to MRD assessment in parallel with HTS.
According to the ERIC investigators, flow cytometry had to utilize a core panel of 6 antigens used by most labs—CD19, CD20, CD5, CD43, CD79b, and CD81. And the markers used had to quantitate cells to a level of 0.01% (10-4).
Assays had to be independent and compatible with older, established therapies as well as newer treatments.
For example, 6-color flow had to be effective with fludarabine, cyclophosphamide, and rituximab (FCR) regimens, as well as effective with the novel agents ibrutinib and venetoclax (ABT-199).
Compared to PCR, multiparameter flow cytometry is more convenient, Dr Hillmen noted.
And while PCR is more sensitive than flow cytometry (sensitive to 10-5 to 10-6), it is more difficult to apply to large clinical trials because the assay must be validated for each patient.
The investigators validated the flow cytometric approach in 450 patients on FCR-type therapy enrolled in the ADMIRE and ARCTIC trials.
They assessed MRD in patients’ bone marrow 3 months after the last course of treatment and presented the data at EHA 2015 (Rawstron AC, abstract S794).
They found that all patients who were MRD negative, including 9 patients with partial responses, achieved a significantly better progression-free survival (PFS) than patients who had achieved a complete response but were still MRD positive.
The parallel analysis of HTS showed good concordance with flow cytometry at the 0.01% (10-4) level.
Peripheral blood or bone marrow?
“[T]he blood is a tissue which can be used, but it’s certainly not as sensitive as the bone marrow,” Dr Hillmen said. “And depending upon what we are using MRD for, the marrow is probably a better tissue, with some exceptions.”
Data from the ADMIRE and ARCTIC trials confirmed that 177 patients on FCR-based therapy who were negative in the bone marrow were always negative in the blood. However, a quarter of patients negative in the blood were positive in the bone marrow.
Investigators followed the same patients on FCR-based therapy for 3 years and found no difference in outcome in terms of PFS for patients negative in peripheral blood and positive in the bone marrow (PB-/BM+) and those negative in peripheral blood and negative in the bone marrow (PB-/BM-) (Rawstron abstract S794).
But for patients on alemtuzumab, with the same analysis, those who were PB-/BM+ did less well and had similar PFS to those who were PB+/BM+.
And at a follow-up of 4 years or longer, patients on FCR-based therapy who were PB-/BM- had superior outcomes than those who were PB-/BM+.
“So as a predictive marker, the bone marrow is a better tissue to look at, but peripheral blood negativity also can predict with FCR but not with agents such as alemtuzumab,” Dr Hillmen summarized.
Prognostic value of MRD assessment
Multivariate analysis of a 10-year follow-up of 133 CLL patients revealed that MRD level and adverse cytogenetics were the only significant parameters in terms of PFS.
And in terms of overall survival (OS), MRD level, prior treatment, Binet stage, and age were significant.
Sixty-seven of these patients had been treated with chemoimmunotherapy, 31 with single-agent chemotherapy, 7 had autologous stem cell transplants, and 28 had prior exposure to alemtuzumab.
In terms of survival beyond 10 or 15 years, previously untreated patients who were MRD negative after their first therapy had significantly better PFS and OS than previously treated patients who were MRD negative and patients with or without prior treatment who were MRD positive (P<0.001).
“Consistently, MRD, regardless of therapy, is the most important prognostic marker,” Dr Hillmen said.
Data from MD Anderson Cancer Center showed that 75% of patients treated first-line with FCR who achieved a complete response were MRD negative.
And patients who achieved MRD negativity had significantly better PFS (P<0.001) and OS (P=0.006) than patients who remained MRD positive.
In the ADMIRE and ARCTIC trials mentioned earlier, patients who achieved MRD negativity in the marrow at 3 months post-therapy also had significantly better PFS (P<0.0001) and OS (P=0.0002) than those who were MRD positive.
For every log of positivity, Dr Hillmen said, patients have a worse survival. Conversely, for every log reduction in MRD level, there is a 33% reduction in risk for disease progression.
“MRD is probably the most important prognostic marker we have,” he said. “We need to look at MRD levels with novel agents and use it to define duration of therapy, maybe use it to define additional therapy if patients are stalled in their response.” ![]()
laser beam
Photo courtesy of NIH
NEW YORK—Combining 2 technologies—flow cytometry and high-throughput sequencing (HTS)—produces a very sensitive approach to detecting minimal residual disease (MRD) in chronic lymphocytic leukemia (CLL), according to a speaker at Lymphoma & Myeloma 2016.
The approach is both reproducible and widely accessible, added the speaker, Peter Hillmen, MB ChB, PhD, of St James’s University Hospital in Leeds, UK.
“PCR [polymerase chain reaction] is more sensitive than flow cytometry,” he noted, “but it is probably not necessary to assess response by that criteria.”
Features to consider when choosing a technology for detecting MRD include sensitivity, specificity for the patient and/or the disease, applicability to all patients or to an individual, the platform—flow cytometry, conventional molecular PCR, or next-generation sequencing—and which tissue to use, blood or bone marrow.
In the era of immunotherapy, Dr Hillmen said, assessment should be performed at least 2 months after completion of immunotherapy to get a reliable assessment of MRD, particularly after treatment with alemtuzumab, rituximab, and other antibodies targeting CLL.
History of MRD analysis
The definition of MRD hasn’t changed since 2008, when the International Workshop on CLL updated National Cancer Institute guidelines. It is still 1 single cell in 10,000 (10-4) leukocytes, regardless of the tissue used.
Prior to the mid-1990s, there were limited options for assessing MRD, Dr Hillmen said.
Based on the profound remissions patients experienced with alemtuzumab, investigators began to develop assays to assess MRD.
“[W]e started standardizing these assays around 2007,” Dr Hillmen said, and a standardized assay was used prospectively in clinical trials beginning in 2012.
Technologies
Several technologies can be used to assess MRD.
Flow cytometry using 6 colors or 8 colors—to simplify the assay and to make it more sensitive—is a multiparameter assessment of CLL phenotype that is not clonality-based.
Allele-specific oligonucleotide PCR (ASO-PCR) is laborious to perform, Dr Hillmen said, but it’s very sensitive.
“[I]t probably shouldn’t be considered as an MRD test,” he said, since it uses patient-specific primers, not consensus primers.
HTS provides an increasing amount of information on B-cell sequences and enumeration of the CLL-specific immunoglobulin gene, “and I would move it towards being approved as a regulatory endpoint,” Dr Hillmen asserted.
Flow cytometry and HTS
A consensus document by the European Research Initiative on CLL (ERIC) identified and validated a flow cytometric approach to MRD assessment in parallel with HTS.
According to the ERIC investigators, flow cytometry had to utilize a core panel of 6 antigens used by most labs—CD19, CD20, CD5, CD43, CD79b, and CD81. And the markers used had to quantitate cells to a level of 0.01% (10-4).
Assays had to be independent and compatible with older, established therapies as well as newer treatments.
For example, 6-color flow had to be effective with fludarabine, cyclophosphamide, and rituximab (FCR) regimens, as well as effective with the novel agents ibrutinib and venetoclax (ABT-199).
Compared to PCR, multiparameter flow cytometry is more convenient, Dr Hillmen noted.
And while PCR is more sensitive than flow cytometry (sensitive to 10-5 to 10-6), it is more difficult to apply to large clinical trials because the assay must be validated for each patient.
The investigators validated the flow cytometric approach in 450 patients on FCR-type therapy enrolled in the ADMIRE and ARCTIC trials.
They assessed MRD in patients’ bone marrow 3 months after the last course of treatment and presented the data at EHA 2015 (Rawstron AC, abstract S794).
They found that all patients who were MRD negative, including 9 patients with partial responses, achieved a significantly better progression-free survival (PFS) than patients who had achieved a complete response but were still MRD positive.
The parallel analysis of HTS showed good concordance with flow cytometry at the 0.01% (10-4) level.
Peripheral blood or bone marrow?
“[T]he blood is a tissue which can be used, but it’s certainly not as sensitive as the bone marrow,” Dr Hillmen said. “And depending upon what we are using MRD for, the marrow is probably a better tissue, with some exceptions.”
Data from the ADMIRE and ARCTIC trials confirmed that 177 patients on FCR-based therapy who were negative in the bone marrow were always negative in the blood. However, a quarter of patients negative in the blood were positive in the bone marrow.
Investigators followed the same patients on FCR-based therapy for 3 years and found no difference in outcome in terms of PFS for patients negative in peripheral blood and positive in the bone marrow (PB-/BM+) and those negative in peripheral blood and negative in the bone marrow (PB-/BM-) (Rawstron abstract S794).
But for patients on alemtuzumab, with the same analysis, those who were PB-/BM+ did less well and had similar PFS to those who were PB+/BM+.
And at a follow-up of 4 years or longer, patients on FCR-based therapy who were PB-/BM- had superior outcomes than those who were PB-/BM+.
“So as a predictive marker, the bone marrow is a better tissue to look at, but peripheral blood negativity also can predict with FCR but not with agents such as alemtuzumab,” Dr Hillmen summarized.
Prognostic value of MRD assessment
Multivariate analysis of a 10-year follow-up of 133 CLL patients revealed that MRD level and adverse cytogenetics were the only significant parameters in terms of PFS.
And in terms of overall survival (OS), MRD level, prior treatment, Binet stage, and age were significant.
Sixty-seven of these patients had been treated with chemoimmunotherapy, 31 with single-agent chemotherapy, 7 had autologous stem cell transplants, and 28 had prior exposure to alemtuzumab.
In terms of survival beyond 10 or 15 years, previously untreated patients who were MRD negative after their first therapy had significantly better PFS and OS than previously treated patients who were MRD negative and patients with or without prior treatment who were MRD positive (P<0.001).
“Consistently, MRD, regardless of therapy, is the most important prognostic marker,” Dr Hillmen said.
Data from MD Anderson Cancer Center showed that 75% of patients treated first-line with FCR who achieved a complete response were MRD negative.
And patients who achieved MRD negativity had significantly better PFS (P<0.001) and OS (P=0.006) than patients who remained MRD positive.
In the ADMIRE and ARCTIC trials mentioned earlier, patients who achieved MRD negativity in the marrow at 3 months post-therapy also had significantly better PFS (P<0.0001) and OS (P=0.0002) than those who were MRD positive.
For every log of positivity, Dr Hillmen said, patients have a worse survival. Conversely, for every log reduction in MRD level, there is a 33% reduction in risk for disease progression.
“MRD is probably the most important prognostic marker we have,” he said. “We need to look at MRD levels with novel agents and use it to define duration of therapy, maybe use it to define additional therapy if patients are stalled in their response.” ![]()
laser beam
Photo courtesy of NIH
NEW YORK—Combining 2 technologies—flow cytometry and high-throughput sequencing (HTS)—produces a very sensitive approach to detecting minimal residual disease (MRD) in chronic lymphocytic leukemia (CLL), according to a speaker at Lymphoma & Myeloma 2016.
The approach is both reproducible and widely accessible, added the speaker, Peter Hillmen, MB ChB, PhD, of St James’s University Hospital in Leeds, UK.
“PCR [polymerase chain reaction] is more sensitive than flow cytometry,” he noted, “but it is probably not necessary to assess response by that criteria.”
Features to consider when choosing a technology for detecting MRD include sensitivity, specificity for the patient and/or the disease, applicability to all patients or to an individual, the platform—flow cytometry, conventional molecular PCR, or next-generation sequencing—and which tissue to use, blood or bone marrow.
In the era of immunotherapy, Dr Hillmen said, assessment should be performed at least 2 months after completion of immunotherapy to get a reliable assessment of MRD, particularly after treatment with alemtuzumab, rituximab, and other antibodies targeting CLL.
History of MRD analysis
The definition of MRD hasn’t changed since 2008, when the International Workshop on CLL updated National Cancer Institute guidelines. It is still 1 single cell in 10,000 (10-4) leukocytes, regardless of the tissue used.
Prior to the mid-1990s, there were limited options for assessing MRD, Dr Hillmen said.
Based on the profound remissions patients experienced with alemtuzumab, investigators began to develop assays to assess MRD.
“[W]e started standardizing these assays around 2007,” Dr Hillmen said, and a standardized assay was used prospectively in clinical trials beginning in 2012.
Technologies
Several technologies can be used to assess MRD.
Flow cytometry using 6 colors or 8 colors—to simplify the assay and to make it more sensitive—is a multiparameter assessment of CLL phenotype that is not clonality-based.
Allele-specific oligonucleotide PCR (ASO-PCR) is laborious to perform, Dr Hillmen said, but it’s very sensitive.
“[I]t probably shouldn’t be considered as an MRD test,” he said, since it uses patient-specific primers, not consensus primers.
HTS provides an increasing amount of information on B-cell sequences and enumeration of the CLL-specific immunoglobulin gene, “and I would move it towards being approved as a regulatory endpoint,” Dr Hillmen asserted.
Flow cytometry and HTS
A consensus document by the European Research Initiative on CLL (ERIC) identified and validated a flow cytometric approach to MRD assessment in parallel with HTS.
According to the ERIC investigators, flow cytometry had to utilize a core panel of 6 antigens used by most labs—CD19, CD20, CD5, CD43, CD79b, and CD81. And the markers used had to quantitate cells to a level of 0.01% (10-4).
Assays had to be independent and compatible with older, established therapies as well as newer treatments.
For example, 6-color flow had to be effective with fludarabine, cyclophosphamide, and rituximab (FCR) regimens, as well as effective with the novel agents ibrutinib and venetoclax (ABT-199).
Compared to PCR, multiparameter flow cytometry is more convenient, Dr Hillmen noted.
And while PCR is more sensitive than flow cytometry (sensitive to 10-5 to 10-6), it is more difficult to apply to large clinical trials because the assay must be validated for each patient.
The investigators validated the flow cytometric approach in 450 patients on FCR-type therapy enrolled in the ADMIRE and ARCTIC trials.
They assessed MRD in patients’ bone marrow 3 months after the last course of treatment and presented the data at EHA 2015 (Rawstron AC, abstract S794).
They found that all patients who were MRD negative, including 9 patients with partial responses, achieved a significantly better progression-free survival (PFS) than patients who had achieved a complete response but were still MRD positive.
The parallel analysis of HTS showed good concordance with flow cytometry at the 0.01% (10-4) level.
Peripheral blood or bone marrow?
“[T]he blood is a tissue which can be used, but it’s certainly not as sensitive as the bone marrow,” Dr Hillmen said. “And depending upon what we are using MRD for, the marrow is probably a better tissue, with some exceptions.”
Data from the ADMIRE and ARCTIC trials confirmed that 177 patients on FCR-based therapy who were negative in the bone marrow were always negative in the blood. However, a quarter of patients negative in the blood were positive in the bone marrow.
Investigators followed the same patients on FCR-based therapy for 3 years and found no difference in outcome in terms of PFS for patients negative in peripheral blood and positive in the bone marrow (PB-/BM+) and those negative in peripheral blood and negative in the bone marrow (PB-/BM-) (Rawstron abstract S794).
But for patients on alemtuzumab, with the same analysis, those who were PB-/BM+ did less well and had similar PFS to those who were PB+/BM+.
And at a follow-up of 4 years or longer, patients on FCR-based therapy who were PB-/BM- had superior outcomes than those who were PB-/BM+.
“So as a predictive marker, the bone marrow is a better tissue to look at, but peripheral blood negativity also can predict with FCR but not with agents such as alemtuzumab,” Dr Hillmen summarized.
Prognostic value of MRD assessment
Multivariate analysis of a 10-year follow-up of 133 CLL patients revealed that MRD level and adverse cytogenetics were the only significant parameters in terms of PFS.
And in terms of overall survival (OS), MRD level, prior treatment, Binet stage, and age were significant.
Sixty-seven of these patients had been treated with chemoimmunotherapy, 31 with single-agent chemotherapy, 7 had autologous stem cell transplants, and 28 had prior exposure to alemtuzumab.
In terms of survival beyond 10 or 15 years, previously untreated patients who were MRD negative after their first therapy had significantly better PFS and OS than previously treated patients who were MRD negative and patients with or without prior treatment who were MRD positive (P<0.001).
“Consistently, MRD, regardless of therapy, is the most important prognostic marker,” Dr Hillmen said.
Data from MD Anderson Cancer Center showed that 75% of patients treated first-line with FCR who achieved a complete response were MRD negative.
And patients who achieved MRD negativity had significantly better PFS (P<0.001) and OS (P=0.006) than patients who remained MRD positive.
In the ADMIRE and ARCTIC trials mentioned earlier, patients who achieved MRD negativity in the marrow at 3 months post-therapy also had significantly better PFS (P<0.0001) and OS (P=0.0002) than those who were MRD positive.
For every log of positivity, Dr Hillmen said, patients have a worse survival. Conversely, for every log reduction in MRD level, there is a 33% reduction in risk for disease progression.
“MRD is probably the most important prognostic marker we have,” he said. “We need to look at MRD levels with novel agents and use it to define duration of therapy, maybe use it to define additional therapy if patients are stalled in their response.” ![]()
Rethinking testing in multiple myeloma
NEW YORK—As the number of therapeutic options for multiple myeloma (MM) increases, so too does the need to reassess prognostic markers for the disease, according to a speaker at Lymphoma & Myeloma 2016.
“A good prognosticator for one patient may have little meaning for another patient,” said Scott Ely, MD, of Weill Cornell Medicine in New York, New York.
“It’s really important before doing any testing to ask, ‘Will the result of this test affect patient care?’”
To answer this question, Dr Ely reviewed the different testing methods used in MM patients and explained the advantages of each.
“[I]t’s really important to understand that a lot of methods are really great for research but don’t work or are not feasible for real-life diagnostic purposes,” he added.
Dr Ely also said it’s important to consider who wants the data, how much the test costs, and who will pay for it, keeping in mind that, these days, the patient’s share of the bill is increasing.
Dr Ely stressed that, until more precise targets or a better understanding of drug mechanisms exist, clinical features—patient age, performance status or frailty, renal function, and disease stage—remain the most important prognosticators.
“But still, 2 patients in the same box based on clinical features will often have very different outcomes,” he said. “So in addition to clinical factors, we need prognosticators for tumor cell behavior. We need to know how fast they are growing and how they will respond to treatment.”
Methods to assess myeloma cell proliferation
Cytogenetics (FISH), gene array technology, and genomics using next-generation sequencing can provide some information, but they are not necessarily good methods to assess proliferation, Dr Ely explained.
To determine the proliferation rate of a patient’s cancer, you can look at tens of thousands of genes by gene array, he said, “or you can just look at one thing, which is Ki67.”
If the cell has Ki67, it’s proliferating, and if it doesn’t have Ki67, it’s not.
“Often, looking at all the other upstream molecules can be confusing and even misleading,” he noted. “So Ki67 is the best way to look for proliferation when it comes to myeloma.”
Other methods include the plasma cell labeling index (PCLI), gene expression profiling, flow cytometry, and multiplex immunohistochemistry (mIHC).
Dr Ely, as a hematopathologist, has found IHC to be the best method to determine proliferation, most likely because the other methods use bone marrow aspirate and IHC uses core biopsy of histologic sections.
It’s the gold standard, he said, for determining the percentage of plasma cells because core biopsy takes a “complete, intact piece of marrow that’s truly representative of what’s going on in the patient.”
In a study of more than 350 bone marrow samples comparing core biopsy with aspirate smears, plasma cells were under-represented in approximately half the aspirate specimens by about 20%.
In addition, Dr Ely noted that myeloma cells die very quickly once they are removed from the stroma.
“So if you take myeloma cells out as an aspirate,” he said, “myeloma cells die and others survive.”
And if the aspirate is sent overnight to the lab, the number of plasma cells in the specimen will already be reduced when the lab gets it.
Aspirates are best for leukemia and myelodysplastic syndromes, Dr Ely said, while core biopsies are best for lymphoma and myeloma.
Plasma cell proliferation indices
Proliferation is a myeloma-defining criterion, Dr Ely said. It predicts an 80% probability of progression in 2 years.
And PCLI has shown conclusively that plasma cell proliferation is a good prognosticator in all types of myeloma patients. However, it is not really feasible to use or easy to perform.
On the other hand, core biopsy combined with IHC is a feasible way of measuring plasma cell proliferation for routine clinical use.
Using standard IHC, it’s difficult to distinguish proliferating from non-proliferating cells, Dr Ely said.
“The solution to this problem is multiplex IHC,” he said, using 3 stains—red for CD138 (the plasma cell marker), brown for Ki67 (the proliferation marker), and blue as a negative nuclear counter stain.
A red membrane around the stained cell indicates a myeloma cell. Non-proliferating MM cells have blue nuclei, and proliferating MM cells have brown nuclei.
This assay is called the plasma cell proliferation index (PCPI).
“[A]ny lab that can do standard IHC can do multiplex IHC,” Dr Ely added.
It uses the same machines, the same reagents, the same expertise, and it’s easy to set up.
Validation studies
Dr Ely and his colleagues performed extensive laboratory validation to make sure the new PCPI correlated with the old PCLI.
They also performed 3 clinical validation studies, the first in bone marrow transplant patients. The investigators followed the patients for 12 years and found the PCPI correlated with survival.
The investigators performed a second clinical validation in 151 newly diagnosed patients. On multivariate analysis, the team found PCPI to be an independent prognostic indicator.
Each 1% increase in PCPI was associated with a 3% increased risk of disease progression (hazard ratio=1.03, 95% CI, 1.01-1.05, P=0.02).
The third clinical validation the investigators conducted was a retrospective cohort study in which they evaluated the effect of rising PCPI at relapse in 37 patients. The team defined rising PCPI as a 5% or greater increase in plasma cells.
Nineteen patients had a rising PCPI, and 17 patients had stable or decreased PCPI.
Patients with a rising PCPI at relapse had a shorter median overall survival than patients with stable or decreased PCPI—72 months and not reached, respectively (P=0.0069).
Patients with a rising PCPI also had a shorter median progression-free survival on first post-relapse treatment compared to patients with stable or decreased PCPI—25 months and 47 months, respectively (P=0.036).
“It’s also important to note that if you’re getting high-risk by PCPI plus β2-microglobulin albumin, I’d advise that, for all high-risk patients, getting the cytogenetics doesn’t really help,” Dr Ely said
Three patients considered high-risk by cytogenetics were standard-risk by PCPI plus β2 microglobulin.
“So we found that cytogenetics isn’t really adding anything except the cost,” Dr Ely asserted.
Other labs are now using PCPI for prognostication, he noted, adding, “We hope PCPI will be incorporated into the International Myeloma Working Group diagnosis of MM.” ![]()
NEW YORK—As the number of therapeutic options for multiple myeloma (MM) increases, so too does the need to reassess prognostic markers for the disease, according to a speaker at Lymphoma & Myeloma 2016.
“A good prognosticator for one patient may have little meaning for another patient,” said Scott Ely, MD, of Weill Cornell Medicine in New York, New York.
“It’s really important before doing any testing to ask, ‘Will the result of this test affect patient care?’”
To answer this question, Dr Ely reviewed the different testing methods used in MM patients and explained the advantages of each.
“[I]t’s really important to understand that a lot of methods are really great for research but don’t work or are not feasible for real-life diagnostic purposes,” he added.
Dr Ely also said it’s important to consider who wants the data, how much the test costs, and who will pay for it, keeping in mind that, these days, the patient’s share of the bill is increasing.
Dr Ely stressed that, until more precise targets or a better understanding of drug mechanisms exist, clinical features—patient age, performance status or frailty, renal function, and disease stage—remain the most important prognosticators.
“But still, 2 patients in the same box based on clinical features will often have very different outcomes,” he said. “So in addition to clinical factors, we need prognosticators for tumor cell behavior. We need to know how fast they are growing and how they will respond to treatment.”
Methods to assess myeloma cell proliferation
Cytogenetics (FISH), gene array technology, and genomics using next-generation sequencing can provide some information, but they are not necessarily good methods to assess proliferation, Dr Ely explained.
To determine the proliferation rate of a patient’s cancer, you can look at tens of thousands of genes by gene array, he said, “or you can just look at one thing, which is Ki67.”
If the cell has Ki67, it’s proliferating, and if it doesn’t have Ki67, it’s not.
“Often, looking at all the other upstream molecules can be confusing and even misleading,” he noted. “So Ki67 is the best way to look for proliferation when it comes to myeloma.”
Other methods include the plasma cell labeling index (PCLI), gene expression profiling, flow cytometry, and multiplex immunohistochemistry (mIHC).
Dr Ely, as a hematopathologist, has found IHC to be the best method to determine proliferation, most likely because the other methods use bone marrow aspirate and IHC uses core biopsy of histologic sections.
It’s the gold standard, he said, for determining the percentage of plasma cells because core biopsy takes a “complete, intact piece of marrow that’s truly representative of what’s going on in the patient.”
In a study of more than 350 bone marrow samples comparing core biopsy with aspirate smears, plasma cells were under-represented in approximately half the aspirate specimens by about 20%.
In addition, Dr Ely noted that myeloma cells die very quickly once they are removed from the stroma.
“So if you take myeloma cells out as an aspirate,” he said, “myeloma cells die and others survive.”
And if the aspirate is sent overnight to the lab, the number of plasma cells in the specimen will already be reduced when the lab gets it.
Aspirates are best for leukemia and myelodysplastic syndromes, Dr Ely said, while core biopsies are best for lymphoma and myeloma.
Plasma cell proliferation indices
Proliferation is a myeloma-defining criterion, Dr Ely said. It predicts an 80% probability of progression in 2 years.
And PCLI has shown conclusively that plasma cell proliferation is a good prognosticator in all types of myeloma patients. However, it is not really feasible to use or easy to perform.
On the other hand, core biopsy combined with IHC is a feasible way of measuring plasma cell proliferation for routine clinical use.
Using standard IHC, it’s difficult to distinguish proliferating from non-proliferating cells, Dr Ely said.
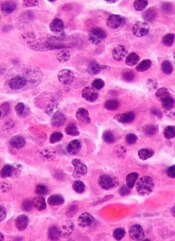
“The solution to this problem is multiplex IHC,” he said, using 3 stains—red for CD138 (the plasma cell marker), brown for Ki67 (the proliferation marker), and blue as a negative nuclear counter stain.
A red membrane around the stained cell indicates a myeloma cell. Non-proliferating MM cells have blue nuclei, and proliferating MM cells have brown nuclei.
This assay is called the plasma cell proliferation index (PCPI).
“[A]ny lab that can do standard IHC can do multiplex IHC,” Dr Ely added.
It uses the same machines, the same reagents, the same expertise, and it’s easy to set up.
Validation studies
Dr Ely and his colleagues performed extensive laboratory validation to make sure the new PCPI correlated with the old PCLI.
They also performed 3 clinical validation studies, the first in bone marrow transplant patients. The investigators followed the patients for 12 years and found the PCPI correlated with survival.
The investigators performed a second clinical validation in 151 newly diagnosed patients. On multivariate analysis, the team found PCPI to be an independent prognostic indicator.
Each 1% increase in PCPI was associated with a 3% increased risk of disease progression (hazard ratio=1.03, 95% CI, 1.01-1.05, P=0.02).
The third clinical validation the investigators conducted was a retrospective cohort study in which they evaluated the effect of rising PCPI at relapse in 37 patients. The team defined rising PCPI as a 5% or greater increase in plasma cells.
Nineteen patients had a rising PCPI, and 17 patients had stable or decreased PCPI.
Patients with a rising PCPI at relapse had a shorter median overall survival than patients with stable or decreased PCPI—72 months and not reached, respectively (P=0.0069).
Patients with a rising PCPI also had a shorter median progression-free survival on first post-relapse treatment compared to patients with stable or decreased PCPI—25 months and 47 months, respectively (P=0.036).
“It’s also important to note that if you’re getting high-risk by PCPI plus β2-microglobulin albumin, I’d advise that, for all high-risk patients, getting the cytogenetics doesn’t really help,” Dr Ely said
Three patients considered high-risk by cytogenetics were standard-risk by PCPI plus β2 microglobulin.
“So we found that cytogenetics isn’t really adding anything except the cost,” Dr Ely asserted.
Other labs are now using PCPI for prognostication, he noted, adding, “We hope PCPI will be incorporated into the International Myeloma Working Group diagnosis of MM.” ![]()
NEW YORK—As the number of therapeutic options for multiple myeloma (MM) increases, so too does the need to reassess prognostic markers for the disease, according to a speaker at Lymphoma & Myeloma 2016.
“A good prognosticator for one patient may have little meaning for another patient,” said Scott Ely, MD, of Weill Cornell Medicine in New York, New York.
“It’s really important before doing any testing to ask, ‘Will the result of this test affect patient care?’”
To answer this question, Dr Ely reviewed the different testing methods used in MM patients and explained the advantages of each.
“[I]t’s really important to understand that a lot of methods are really great for research but don’t work or are not feasible for real-life diagnostic purposes,” he added.
Dr Ely also said it’s important to consider who wants the data, how much the test costs, and who will pay for it, keeping in mind that, these days, the patient’s share of the bill is increasing.
Dr Ely stressed that, until more precise targets or a better understanding of drug mechanisms exist, clinical features—patient age, performance status or frailty, renal function, and disease stage—remain the most important prognosticators.
“But still, 2 patients in the same box based on clinical features will often have very different outcomes,” he said. “So in addition to clinical factors, we need prognosticators for tumor cell behavior. We need to know how fast they are growing and how they will respond to treatment.”
Methods to assess myeloma cell proliferation
Cytogenetics (FISH), gene array technology, and genomics using next-generation sequencing can provide some information, but they are not necessarily good methods to assess proliferation, Dr Ely explained.
To determine the proliferation rate of a patient’s cancer, you can look at tens of thousands of genes by gene array, he said, “or you can just look at one thing, which is Ki67.”
If the cell has Ki67, it’s proliferating, and if it doesn’t have Ki67, it’s not.
“Often, looking at all the other upstream molecules can be confusing and even misleading,” he noted. “So Ki67 is the best way to look for proliferation when it comes to myeloma.”
Other methods include the plasma cell labeling index (PCLI), gene expression profiling, flow cytometry, and multiplex immunohistochemistry (mIHC).
Dr Ely, as a hematopathologist, has found IHC to be the best method to determine proliferation, most likely because the other methods use bone marrow aspirate and IHC uses core biopsy of histologic sections.
It’s the gold standard, he said, for determining the percentage of plasma cells because core biopsy takes a “complete, intact piece of marrow that’s truly representative of what’s going on in the patient.”
In a study of more than 350 bone marrow samples comparing core biopsy with aspirate smears, plasma cells were under-represented in approximately half the aspirate specimens by about 20%.
In addition, Dr Ely noted that myeloma cells die very quickly once they are removed from the stroma.
“So if you take myeloma cells out as an aspirate,” he said, “myeloma cells die and others survive.”
And if the aspirate is sent overnight to the lab, the number of plasma cells in the specimen will already be reduced when the lab gets it.
Aspirates are best for leukemia and myelodysplastic syndromes, Dr Ely said, while core biopsies are best for lymphoma and myeloma.
Plasma cell proliferation indices
Proliferation is a myeloma-defining criterion, Dr Ely said. It predicts an 80% probability of progression in 2 years.
And PCLI has shown conclusively that plasma cell proliferation is a good prognosticator in all types of myeloma patients. However, it is not really feasible to use or easy to perform.
On the other hand, core biopsy combined with IHC is a feasible way of measuring plasma cell proliferation for routine clinical use.
Using standard IHC, it’s difficult to distinguish proliferating from non-proliferating cells, Dr Ely said.
“The solution to this problem is multiplex IHC,” he said, using 3 stains—red for CD138 (the plasma cell marker), brown for Ki67 (the proliferation marker), and blue as a negative nuclear counter stain.
A red membrane around the stained cell indicates a myeloma cell. Non-proliferating MM cells have blue nuclei, and proliferating MM cells have brown nuclei.
This assay is called the plasma cell proliferation index (PCPI).
“[A]ny lab that can do standard IHC can do multiplex IHC,” Dr Ely added.
It uses the same machines, the same reagents, the same expertise, and it’s easy to set up.
Validation studies
Dr Ely and his colleagues performed extensive laboratory validation to make sure the new PCPI correlated with the old PCLI.
They also performed 3 clinical validation studies, the first in bone marrow transplant patients. The investigators followed the patients for 12 years and found the PCPI correlated with survival.
The investigators performed a second clinical validation in 151 newly diagnosed patients. On multivariate analysis, the team found PCPI to be an independent prognostic indicator.
Each 1% increase in PCPI was associated with a 3% increased risk of disease progression (hazard ratio=1.03, 95% CI, 1.01-1.05, P=0.02).
The third clinical validation the investigators conducted was a retrospective cohort study in which they evaluated the effect of rising PCPI at relapse in 37 patients. The team defined rising PCPI as a 5% or greater increase in plasma cells.
Nineteen patients had a rising PCPI, and 17 patients had stable or decreased PCPI.
Patients with a rising PCPI at relapse had a shorter median overall survival than patients with stable or decreased PCPI—72 months and not reached, respectively (P=0.0069).
Patients with a rising PCPI also had a shorter median progression-free survival on first post-relapse treatment compared to patients with stable or decreased PCPI—25 months and 47 months, respectively (P=0.036).
“It’s also important to note that if you’re getting high-risk by PCPI plus β2-microglobulin albumin, I’d advise that, for all high-risk patients, getting the cytogenetics doesn’t really help,” Dr Ely said
Three patients considered high-risk by cytogenetics were standard-risk by PCPI plus β2 microglobulin.
“So we found that cytogenetics isn’t really adding anything except the cost,” Dr Ely asserted.
Other labs are now using PCPI for prognostication, he noted, adding, “We hope PCPI will be incorporated into the International Myeloma Working Group diagnosis of MM.” ![]()
Genetic screening for CLL premature, speaker says

Photo courtesy of the
National Institute
of General Medical Science
NEW YORK—Research has shown that family history is a strong risk factor for developing chronic lymphocytic leukemia (CLL).
First-degree relatives have an 8.5-fold risk of getting CLL and an increased risk of other lymphoproliferative disorders, according to a study published in 2009.
However, despite the strong evidence of a genetic contribution, one expert believes it’s premature to bring genetic testing into the clinic for screening in CLL.
“At this time, we do not recommend genetic screening,” said Susan Slager, PhD, of the Mayo Clinic in Rochester, Minnesota.
“There’s no known relationship between the inherited variants and treatment response,” she explained, and the relatively low incidence of CLL argues against active screening in affected families at present.
Dr Slager discussed genetic and non-genetic factors associated with CLL and the clinical implications of these factors at Lymphoma & Myeloma 2016.
Demographic risk factors
Dr Slager noted that age, gender, and race are risk factors for CLL.
Individuals aged 65 to 74 have the highest incidence of CLL, at 28%, while the risk is almost non-existent for those under age 20, she said.
There is a higher incidence of CLL in males than in females, and the reason for this gender disparity is unknown.
There is a higher incidence of CLL in Caucasians than Asians, for both males and females.
“Again, it’s unknown why there’s this variability in incidence in CLL,” Dr Slager said. “Obviously, age, sex, and race—these are things you can’t modify. You’re stuck with them.”
However, several studies have been undertaken to look at some of the potentially modifiable factors associated with CLL.
Beyond demographic factors
The International Lymphoma Epidemiology Consortium, known as InterLymph, was initiated in 2001 to evaluate the association of risk factors in CLL. Study centers are located primarily in North America and Europe, with one in Australia.
In one of the larger InterLymph studies, investigators evaluated risk factors—lifestyle exposure, reproductive history, medical history, occupational exposures, farming exposure, and family history—in 2440 CLL patients and 15,186 controls.
The investigators found that sun exposure and atopy—allergies, asthma, eczema, and hay fever—have a protective effect in CLL, while serological hepatitis C virus (HCV) infections, farming exposure, and family history carry an increased risk of CLL.
This confirmed an earlier study conducted in New South Wales, Australia, that had uncovered an inverse association between sun exposure and non-Hodgkin lymphoma (NHL) risk, which fell significantly with increasing recreational sun exposure.
Medical history
Another earlier study from New South Wales revealed a 20% reduction in the risk of NHL for any specific allergy.
However, the investigators of the large, more recent study observed little to no evidence of reduced risk for asthma and eczema.
The underlying biology for atopy or allergies is a hyper-immune system, Dr Slager explained.
“So if you have a hyper-immune system, then we hypothesize that you have protection against CLL,” she said.
Another medical exposure investigators analyzed that impacts CLL risk is HCV. People infected with HCV have an increased risk of CLL, perhaps due to chronic antigen stimulation or possibly disruption of the T-cell function.
Height is also associated with CLL. CLL risk increases with greater height. The concept is that taller individuals have increased exposure to growth hormones that possibly result in cell proliferation.
Another hypothesis supporting the height association is that people of shorter stature experience more infections, which could result in a stronger immune system. And a stronger immune system perhaps protects against NHL.
Occupational exposures
Investigators consistently observed a 20% increased risk of CLL for people living or working on a farm.
Animal farmers, as opposed to crop farmers, experienced some protection. However, the sample size was too small to be conclusive, with only 29 people across all studies being animal farmers.
Among other occupations evaluated, hairdressers also had an increased risk of CLL, although this too was based on a small sample size.
Family history
One of the strongest risk factors for CLL is family history.
Using population-based registry data from Sweden, investigators found that people with a first-degree relative with CLL have an 8.5-fold risk of CLL.
They also have an elevated risk of other lymphoproliferative disorders, including NHL (1.9-fold risk), Waldenström’s macroglobulinemia (4.0-fold risk), hairy cell leukemia (3.3-fold risk), and follicular lymphoma (1.6-fold risk).
GWAS in CLL
Investigators conducted genome-wide association studies (GWAS) to determine what is driving the familial risk.
Dr Slager described these studies as an agnostic approach that looks across the entire genome to determine which regions are associated with a trait of interest.
Typically, many markers are genotyped—somewhere between half a million to 5 million markers—and each is looked at individually with respect to CLL, she said.
Unrelated cases and controls are included in the studies.
The first GWAS study identifying susceptibility loci for CLL was published in 2008. Subsequently, more studies were published with increasing sample sizes—more cases, more controls, and more genetic variants identified.
In the largest meta-analysis for CLL to date (Slager and Houlston et al, not yet published), investigators analyzed 4400 CLL cases and 13,000 controls.
They identified 9 more inherited variances with CLL, for a total of 43 identified to date.
The genes involved follow an apoptosis pathway, the telomere length pathway, and the B-cell lymphocyte development pathway.
“We have to remember, though, that these are non-causal,” Dr Slager cautioned. “We are just identifying the region in the genome that’s associated with CLL . . . . So now we have to dig deeper in these relationships to understand what’s going on.”
Using the identified CLL single-nucleotide polymorphisms, the investigators computed a polygenic risk score. CLL cases in the highest quintile had 2.7-fold increased risk of CLL.
However, the most common GWAS variants explain only 17% of the genetic heritability of CLL, which suggests that more loci are yet to be identified, Dr Slager clarified.
She went on to say that CLL incidence varies by ethnicity. Caucasians have a very high rate of CLL, while Asians have a very low rate. And African Americans have an incidence rate between those of Caucasians and Asians.
Investigators have hypothesized that the differences in incidence are based on the distinct genetic variants that are associated with the ethnicities.
For example, 4 of the variants with more than 20% frequency in Caucasians are quite rare in Chinese individuals and are also quite uncommon in African Americans, with frequencies less than 10%.
Dr Slager suggested that conducting these kinds of studies in Asians and African Americans will take a large sample size and most likely require an international consortium to bring enough CLL cases together.
Impact on clinical practice
Because of the strong genetic risk, patients with CLL naturally want to know about their offspring and their siblings, Dr Slager has found.
Patients who have monoclonal B-cell lymphocytosis (MBL), which is a precursor to CLL, pose the biggest quandary.
MBL is detected in about 5% of people over age 40. However, it’s detected in about 15% to 18% of people with a first-degree relative with CLL.
“These are individuals who have lymphocytosis,” Dr Slager said. “They come to your clinic and have an elevated blood cell count, flow cytometry. [So] you screen them for MBL, and these individuals who have more than 500 cells per microliter, they are the ones who progress to CLL, at 1% per year.”
Individuals who don’t have the elevated blood counts do have the clonal cells, Dr Slager noted.
“They just don’t have the expansion,” she said. “The progression of these individuals to CLL is still yet to be determined.”
For these reasons, Dr Slager believes “it’s still premature to bring genetic testing into clinical practice.”
Future directions include bringing together the non-environmental issues and the inherited issues to create a model that will accurately predict the risk of CLL. ![]()
Photo courtesy of the
National Institute
of General Medical Science
NEW YORK—Research has shown that family history is a strong risk factor for developing chronic lymphocytic leukemia (CLL).
First-degree relatives have an 8.5-fold risk of getting CLL and an increased risk of other lymphoproliferative disorders, according to a study published in 2009.
However, despite the strong evidence of a genetic contribution, one expert believes it’s premature to bring genetic testing into the clinic for screening in CLL.
“At this time, we do not recommend genetic screening,” said Susan Slager, PhD, of the Mayo Clinic in Rochester, Minnesota.
“There’s no known relationship between the inherited variants and treatment response,” she explained, and the relatively low incidence of CLL argues against active screening in affected families at present.
Dr Slager discussed genetic and non-genetic factors associated with CLL and the clinical implications of these factors at Lymphoma & Myeloma 2016.
Demographic risk factors
Dr Slager noted that age, gender, and race are risk factors for CLL.
Individuals aged 65 to 74 have the highest incidence of CLL, at 28%, while the risk is almost non-existent for those under age 20, she said.
There is a higher incidence of CLL in males than in females, and the reason for this gender disparity is unknown.
There is a higher incidence of CLL in Caucasians than Asians, for both males and females.
“Again, it’s unknown why there’s this variability in incidence in CLL,” Dr Slager said. “Obviously, age, sex, and race—these are things you can’t modify. You’re stuck with them.”
However, several studies have been undertaken to look at some of the potentially modifiable factors associated with CLL.
Beyond demographic factors
The International Lymphoma Epidemiology Consortium, known as InterLymph, was initiated in 2001 to evaluate the association of risk factors in CLL. Study centers are located primarily in North America and Europe, with one in Australia.
In one of the larger InterLymph studies, investigators evaluated risk factors—lifestyle exposure, reproductive history, medical history, occupational exposures, farming exposure, and family history—in 2440 CLL patients and 15,186 controls.
The investigators found that sun exposure and atopy—allergies, asthma, eczema, and hay fever—have a protective effect in CLL, while serological hepatitis C virus (HCV) infections, farming exposure, and family history carry an increased risk of CLL.
This confirmed an earlier study conducted in New South Wales, Australia, that had uncovered an inverse association between sun exposure and non-Hodgkin lymphoma (NHL) risk, which fell significantly with increasing recreational sun exposure.
Medical history
Another earlier study from New South Wales revealed a 20% reduction in the risk of NHL for any specific allergy.
However, the investigators of the large, more recent study observed little to no evidence of reduced risk for asthma and eczema.
The underlying biology for atopy or allergies is a hyper-immune system, Dr Slager explained.
“So if you have a hyper-immune system, then we hypothesize that you have protection against CLL,” she said.
Another medical exposure investigators analyzed that impacts CLL risk is HCV. People infected with HCV have an increased risk of CLL, perhaps due to chronic antigen stimulation or possibly disruption of the T-cell function.
Height is also associated with CLL. CLL risk increases with greater height. The concept is that taller individuals have increased exposure to growth hormones that possibly result in cell proliferation.
Another hypothesis supporting the height association is that people of shorter stature experience more infections, which could result in a stronger immune system. And a stronger immune system perhaps protects against NHL.
Occupational exposures
Investigators consistently observed a 20% increased risk of CLL for people living or working on a farm.
Animal farmers, as opposed to crop farmers, experienced some protection. However, the sample size was too small to be conclusive, with only 29 people across all studies being animal farmers.
Among other occupations evaluated, hairdressers also had an increased risk of CLL, although this too was based on a small sample size.
Family history
One of the strongest risk factors for CLL is family history.
Using population-based registry data from Sweden, investigators found that people with a first-degree relative with CLL have an 8.5-fold risk of CLL.
They also have an elevated risk of other lymphoproliferative disorders, including NHL (1.9-fold risk), Waldenström’s macroglobulinemia (4.0-fold risk), hairy cell leukemia (3.3-fold risk), and follicular lymphoma (1.6-fold risk).
GWAS in CLL
Investigators conducted genome-wide association studies (GWAS) to determine what is driving the familial risk.
Dr Slager described these studies as an agnostic approach that looks across the entire genome to determine which regions are associated with a trait of interest.
Typically, many markers are genotyped—somewhere between half a million to 5 million markers—and each is looked at individually with respect to CLL, she said.
Unrelated cases and controls are included in the studies.
The first GWAS study identifying susceptibility loci for CLL was published in 2008. Subsequently, more studies were published with increasing sample sizes—more cases, more controls, and more genetic variants identified.
In the largest meta-analysis for CLL to date (Slager and Houlston et al, not yet published), investigators analyzed 4400 CLL cases and 13,000 controls.
They identified 9 more inherited variances with CLL, for a total of 43 identified to date.
The genes involved follow an apoptosis pathway, the telomere length pathway, and the B-cell lymphocyte development pathway.
“We have to remember, though, that these are non-causal,” Dr Slager cautioned. “We are just identifying the region in the genome that’s associated with CLL . . . . So now we have to dig deeper in these relationships to understand what’s going on.”
Using the identified CLL single-nucleotide polymorphisms, the investigators computed a polygenic risk score. CLL cases in the highest quintile had 2.7-fold increased risk of CLL.
However, the most common GWAS variants explain only 17% of the genetic heritability of CLL, which suggests that more loci are yet to be identified, Dr Slager clarified.
She went on to say that CLL incidence varies by ethnicity. Caucasians have a very high rate of CLL, while Asians have a very low rate. And African Americans have an incidence rate between those of Caucasians and Asians.
Investigators have hypothesized that the differences in incidence are based on the distinct genetic variants that are associated with the ethnicities.
For example, 4 of the variants with more than 20% frequency in Caucasians are quite rare in Chinese individuals and are also quite uncommon in African Americans, with frequencies less than 10%.
Dr Slager suggested that conducting these kinds of studies in Asians and African Americans will take a large sample size and most likely require an international consortium to bring enough CLL cases together.
Impact on clinical practice
Because of the strong genetic risk, patients with CLL naturally want to know about their offspring and their siblings, Dr Slager has found.
Patients who have monoclonal B-cell lymphocytosis (MBL), which is a precursor to CLL, pose the biggest quandary.
MBL is detected in about 5% of people over age 40. However, it’s detected in about 15% to 18% of people with a first-degree relative with CLL.
“These are individuals who have lymphocytosis,” Dr Slager said. “They come to your clinic and have an elevated blood cell count, flow cytometry. [So] you screen them for MBL, and these individuals who have more than 500 cells per microliter, they are the ones who progress to CLL, at 1% per year.”
Individuals who don’t have the elevated blood counts do have the clonal cells, Dr Slager noted.
“They just don’t have the expansion,” she said. “The progression of these individuals to CLL is still yet to be determined.”
For these reasons, Dr Slager believes “it’s still premature to bring genetic testing into clinical practice.”
Future directions include bringing together the non-environmental issues and the inherited issues to create a model that will accurately predict the risk of CLL. ![]()
Photo courtesy of the
National Institute
of General Medical Science
NEW YORK—Research has shown that family history is a strong risk factor for developing chronic lymphocytic leukemia (CLL).
First-degree relatives have an 8.5-fold risk of getting CLL and an increased risk of other lymphoproliferative disorders, according to a study published in 2009.
However, despite the strong evidence of a genetic contribution, one expert believes it’s premature to bring genetic testing into the clinic for screening in CLL.
“At this time, we do not recommend genetic screening,” said Susan Slager, PhD, of the Mayo Clinic in Rochester, Minnesota.
“There’s no known relationship between the inherited variants and treatment response,” she explained, and the relatively low incidence of CLL argues against active screening in affected families at present.
Dr Slager discussed genetic and non-genetic factors associated with CLL and the clinical implications of these factors at Lymphoma & Myeloma 2016.
Demographic risk factors
Dr Slager noted that age, gender, and race are risk factors for CLL.
Individuals aged 65 to 74 have the highest incidence of CLL, at 28%, while the risk is almost non-existent for those under age 20, she said.
There is a higher incidence of CLL in males than in females, and the reason for this gender disparity is unknown.
There is a higher incidence of CLL in Caucasians than Asians, for both males and females.
“Again, it’s unknown why there’s this variability in incidence in CLL,” Dr Slager said. “Obviously, age, sex, and race—these are things you can’t modify. You’re stuck with them.”
However, several studies have been undertaken to look at some of the potentially modifiable factors associated with CLL.
Beyond demographic factors
The International Lymphoma Epidemiology Consortium, known as InterLymph, was initiated in 2001 to evaluate the association of risk factors in CLL. Study centers are located primarily in North America and Europe, with one in Australia.
In one of the larger InterLymph studies, investigators evaluated risk factors—lifestyle exposure, reproductive history, medical history, occupational exposures, farming exposure, and family history—in 2440 CLL patients and 15,186 controls.
The investigators found that sun exposure and atopy—allergies, asthma, eczema, and hay fever—have a protective effect in CLL, while serological hepatitis C virus (HCV) infections, farming exposure, and family history carry an increased risk of CLL.
This confirmed an earlier study conducted in New South Wales, Australia, that had uncovered an inverse association between sun exposure and non-Hodgkin lymphoma (NHL) risk, which fell significantly with increasing recreational sun exposure.
Medical history
Another earlier study from New South Wales revealed a 20% reduction in the risk of NHL for any specific allergy.
However, the investigators of the large, more recent study observed little to no evidence of reduced risk for asthma and eczema.
The underlying biology for atopy or allergies is a hyper-immune system, Dr Slager explained.
“So if you have a hyper-immune system, then we hypothesize that you have protection against CLL,” she said.
Another medical exposure investigators analyzed that impacts CLL risk is HCV. People infected with HCV have an increased risk of CLL, perhaps due to chronic antigen stimulation or possibly disruption of the T-cell function.
Height is also associated with CLL. CLL risk increases with greater height. The concept is that taller individuals have increased exposure to growth hormones that possibly result in cell proliferation.
Another hypothesis supporting the height association is that people of shorter stature experience more infections, which could result in a stronger immune system. And a stronger immune system perhaps protects against NHL.
Occupational exposures
Investigators consistently observed a 20% increased risk of CLL for people living or working on a farm.
Animal farmers, as opposed to crop farmers, experienced some protection. However, the sample size was too small to be conclusive, with only 29 people across all studies being animal farmers.
Among other occupations evaluated, hairdressers also had an increased risk of CLL, although this too was based on a small sample size.
Family history
One of the strongest risk factors for CLL is family history.
Using population-based registry data from Sweden, investigators found that people with a first-degree relative with CLL have an 8.5-fold risk of CLL.
They also have an elevated risk of other lymphoproliferative disorders, including NHL (1.9-fold risk), Waldenström’s macroglobulinemia (4.0-fold risk), hairy cell leukemia (3.3-fold risk), and follicular lymphoma (1.6-fold risk).
GWAS in CLL
Investigators conducted genome-wide association studies (GWAS) to determine what is driving the familial risk.
Dr Slager described these studies as an agnostic approach that looks across the entire genome to determine which regions are associated with a trait of interest.
Typically, many markers are genotyped—somewhere between half a million to 5 million markers—and each is looked at individually with respect to CLL, she said.
Unrelated cases and controls are included in the studies.
The first GWAS study identifying susceptibility loci for CLL was published in 2008. Subsequently, more studies were published with increasing sample sizes—more cases, more controls, and more genetic variants identified.
In the largest meta-analysis for CLL to date (Slager and Houlston et al, not yet published), investigators analyzed 4400 CLL cases and 13,000 controls.
They identified 9 more inherited variances with CLL, for a total of 43 identified to date.
The genes involved follow an apoptosis pathway, the telomere length pathway, and the B-cell lymphocyte development pathway.
“We have to remember, though, that these are non-causal,” Dr Slager cautioned. “We are just identifying the region in the genome that’s associated with CLL . . . . So now we have to dig deeper in these relationships to understand what’s going on.”
Using the identified CLL single-nucleotide polymorphisms, the investigators computed a polygenic risk score. CLL cases in the highest quintile had 2.7-fold increased risk of CLL.
However, the most common GWAS variants explain only 17% of the genetic heritability of CLL, which suggests that more loci are yet to be identified, Dr Slager clarified.
She went on to say that CLL incidence varies by ethnicity. Caucasians have a very high rate of CLL, while Asians have a very low rate. And African Americans have an incidence rate between those of Caucasians and Asians.
Investigators have hypothesized that the differences in incidence are based on the distinct genetic variants that are associated with the ethnicities.
For example, 4 of the variants with more than 20% frequency in Caucasians are quite rare in Chinese individuals and are also quite uncommon in African Americans, with frequencies less than 10%.
Dr Slager suggested that conducting these kinds of studies in Asians and African Americans will take a large sample size and most likely require an international consortium to bring enough CLL cases together.
Impact on clinical practice
Because of the strong genetic risk, patients with CLL naturally want to know about their offspring and their siblings, Dr Slager has found.
Patients who have monoclonal B-cell lymphocytosis (MBL), which is a precursor to CLL, pose the biggest quandary.
MBL is detected in about 5% of people over age 40. However, it’s detected in about 15% to 18% of people with a first-degree relative with CLL.
“These are individuals who have lymphocytosis,” Dr Slager said. “They come to your clinic and have an elevated blood cell count, flow cytometry. [So] you screen them for MBL, and these individuals who have more than 500 cells per microliter, they are the ones who progress to CLL, at 1% per year.”
Individuals who don’t have the elevated blood counts do have the clonal cells, Dr Slager noted.
“They just don’t have the expansion,” she said. “The progression of these individuals to CLL is still yet to be determined.”
For these reasons, Dr Slager believes “it’s still premature to bring genetic testing into clinical practice.”
Future directions include bringing together the non-environmental issues and the inherited issues to create a model that will accurately predict the risk of CLL. ![]()
No longer a hand-me-down approach to WM

Photo courtesy of DFCI
NEW YORK—Whole-genome sequencing has changed the entire approach to drug development for Waldenström’s macroglobulinemia (WM), according to a speaker at Lymphoma & Myeloma 2016.
The strategy has changed from a hand-me-down one, relying on drugs developed first for other diseases, to a rational plan designed specifically to treat WM patients.
“We would wait for our colleagues in the myeloma world or lymphoma world, CLL world, anywhere we could find them, to help us with the development of drugs,” said Steven Treon, MD, PhD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“And, sometimes, this resulted in delays of many, many years before those therapeutics could be vetted out and eventually be handed down to the Waldenström investigators.”
At Lymphoma & Myeloma 2016, Dr Treon described the current therapy of WM and the impact of the discovery of MYD88 and CXCR4 on drug development and treatment choices in WM.
Rituximab-based therapy
WM is a disease that strongly expresses CD20, even though it’s a lymphoplasmacytic disease. So rituximab, given alone and in combination, has been, to date, the most common approach to treating WM.
As a single agent, rituximab produces a response in 25% to 40% of WM patients, but these are very seldom deep responses, Dr Treon noted.
So investigators combined rituximab with cyclophosphamide, nucleoside analogues, proteasome inhibitors, and bendamustine, which increased the overall response rate and depth of response.
This translated into improvement in time to progression, which is now 4 to 5 years with these combination therapies.
“Now, the problem is, when you borrow things from other people, you sometimes end up with problems you didn’t anticipate,” Dr Treon said.
One of the unanticipated side effects with rituximab in WM patients is the IgM flare, which occurs in 40% to 60% of WM patients.
Rituximab can also cause hypogammaglobulinema, leading to infections, and results in a high intolerance rate, which tends to occur a few cycles into induction or maintenance therapy.
“In some cases,” Dr Treon advised, “a switch to ofatumumab, a fully human CD20 molecule, overcomes this intolerance.”
Nucleoside analogues, which used to be the mainstay of WM, have a high rate of transformation into a more aggressive lymphoma or acute myeloid leukemia.
Immunomodulatory drugs, particularly thalidomide, cause peripheral neuropathy greater than grade 2 in 60% of patients.
And a greater incidence of peripheral neuropathy is also observed with proteasome inhibitors, particularly bortezomib, in WM patients than in myeloma or mantle cell lymphoma patients.
“So this was at least the impetus for why we needed to develop novel approaches to treating this disease,” Dr Treon said.
MYD88 mutations
With whole-genome sequencing, investigators discovered that mutations in the MYD88 gene were highly prevalent in WM patients.
About 93% to 95% of WM patients have the L265P MYD88 mutation, and about 2% have the non-L265P MYD88 mutation.
MYD88 has prognostic significance in WM. Mutated MYD88 confers a better prognosis than unmutated MYD88.
MYD88 may also be important in predicting who will respond to drugs like ibrutinib.
CXCR4 mutations
Mutations in CXCR4 are the second most common mutation in WM.
Between 30% and 40% of WM patients have the WHIM-like CXCR4 C-tail mutations, which traffic the Waldenström’s cells to the bone marrow.
This mutation promotes drug resistance, including resistance to ibrutinib because of the enhanced AKT/ERK signaling.
Ibrutinib therapy
With this in mind, investigators set out to evaluate the potential of using a BTK inhibitor in relapsed/refractory WM patients and at the same time observe the genomics that might predict for response and resistance.
They enrolled 63 patients in the multicenter study. Patients had a median of 2 prior therapies (range, 1–9), and 60% had bone marrow involvement.
Patients received single-agent ibrutinib at a dose of 420 mg orally each day until disease progression or the development of unacceptable toxic side effects.
“By the time they came back 4 weeks later to be evaluated, many of them were already in a response,” Dr Treon said. “And what we saw, in fact, was almost immediate improvement in hemoglobin, something that we didn’t see with many of our trials before that.”
The best IgM response reduced levels from 3520 to 880 mg/dL (P<0.001) for the entire cohort.
The best hemoglobin response increased hemoglobin levels 3 points, from 10.5 to 13.8 g/dL (P<0.001).
The progression-free survival at 2 years was 69% and overall survival was 95%.
At 37 months, most patients who achieve a response experience a durable, ongoing response, according to an update presented at the IX International Workshop on Waldenstrom’s Macroglobulinemia.
And toxicities were “very much in line with what our colleagues have seen in other disease groups,” Dr Treon stated.
Response to ibrutinib by mutation status
The overall response rate was 90% for all patients, but there were differences according to mutation status.
Patients with no MYD88 mutation and no CXCR4 mutation had absolutely no major response.
Patients with a MYD88 mutation responded at an overall rate of 100% and had a major response rate of 91.7% if they did not have a CXCR4 mutation as well.
If they also had a CXCR4WHIM mutation, the overall response rate was lower, at 85.7%, and the major response rate was 61.9%.
“It’s still something to be incredibly excited about—61.9% single-agent activity,” Dr Treon said.
Patients with a CXCR4 mutation also respond more slowly than those without the mutation.
This investigator-sponsored study led to the approval of ibrutinib in WM in the US as well as in Europe and Canada.
“And the point to make about this is that investigators can bring their data to the FDA, the EMA, even Canada, and it can make a difference,” Dr Treon said.
“We don’t always have to have company-sponsored registration studies to be able to make these kinds of advances.”
Ibrutinib in rituximab-refractory patients
A multicenter, phase 3 study of ibrutinib in rituximab-refractory patients was “almost a photocopy of our study,” Dr Treon said.
The main difference was that the patients were even sicker, having failed a median of 4 prior therapies.
Patients experienced rapid improvements in hemoglobin and IgM levels and had an overall response rate of 90%.
Patients with a CXCR4 mutation also tended to lag in terms of pace of hemoglobin improvement and reduction in IgM.
The study was just accepted for publication in Lancet Oncology.
IRAK inhibition
Investigators were puzzled by the paucity of complete responses with ibrutinib, and they found the IRAK pathway remained turned on in patients treated with ibrutinib.
So they took cells of patients treated for 6 months with ibrutinib and co-cultured them with ibrutinib and an IRAK inhibitor. They observed the induction of apoptosis.
Based on this finding, the investigators are manufacturing a very potent IRAK1 inhibitor (JH-X-119), which, when combined with ibrutinib, synergistically increases tumor-cell killing.
“And so one of the strategies we have going forward,” Dr Treon said, “is the ability to advance ibrutinib therapy in MYD88-mutated tumors by the addition of the IRAK inhibitor.”
Resistance to ibrutinib
Investigators have found multiple mutations in the C481 site in individual WM patients, which is where ibrutinib binds.
These mutations represent a minority of the clone, but they exert almost a fully clonal signature. The few patients with these mutations also have a CXCR4 mutation.
C481 mutations shift the signaling of cells in the presence of ibrutinib toward ERK, which is a very powerful survival pathway.
So investigators are examining whether an ERK inhibitor combined with ibrutinib can elicit synergistic killing of BTK-resistant cells.
Investigators have also been synthesizing potent HCK inhibitors, which might overcome BTK mutations by shutting down the ability to activate Bruton’s tyrosine kinase.
Other drugs being developed for WM include:
- Combinations with a proteasome inhibitor, such as ixazomib, dexamethasone, and rituximab
- Agents that target MYD88 signaling, such as the BTK inhibitors acalabrutinib and BGB-3111
- Agents that block CXCR4 receptor signaling, such as ulocuplomab
- The BCL2 inhibitor venetoclax
- The CD38-targeted agent daratumumab.
Current treatment strategies
Knowing a patient’s MYD88 and CXCR4 mutation status provides an opportunity to take a rational approach to treating individuals with WM, Dr Treon said.
For patients with mutated MYD88 and no CXCR4 mutation:
- If patients do not have bulky disease or contraindications, ibrutinib may be used if available.
- If patients have bulky disease, a combination of bendamustine and rituximab may be used.
- If patients have amyloidosis, a combination of bortezomib, dexamethasone, and rituximab is possible.
- If patients have IgM peripheral neuropathy, then rituximab with or without an alkylator is recommended.
For patients with mutated MYD88 and mutated CXCR4, the same treatments can be used as for patients with mutated MYD88 and unmutated CXCR4 with the same restrictions.
To achieve an immediate response for patients with a CXCR4 mutation, an alternative therapy to ibrutinib—such as the bendamustine, dexamethasone, rituximab combination—may be the best choice, because CXCR4-mutated individuals have a slower response to ibrutinib.
The problem arises with the MYD88-wild-type patients, because their survival is poorer than the MYD88-mutated patients.
“We still don’t know what’s wrong with these individuals,” Dr Treon said. “We don’t have any idea about what their basic genomic problems are.”
Bendamustine- or bortezomib-based therapy is effective in this population and can be considered.
In terms of salvage therapy, “the only thing to keep in mind is that if something worked the first time and you got at least a 2-year response with it, you can go back and consider it,” Dr Treon said. ![]()
Photo courtesy of DFCI
NEW YORK—Whole-genome sequencing has changed the entire approach to drug development for Waldenström’s macroglobulinemia (WM), according to a speaker at Lymphoma & Myeloma 2016.
The strategy has changed from a hand-me-down one, relying on drugs developed first for other diseases, to a rational plan designed specifically to treat WM patients.
“We would wait for our colleagues in the myeloma world or lymphoma world, CLL world, anywhere we could find them, to help us with the development of drugs,” said Steven Treon, MD, PhD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“And, sometimes, this resulted in delays of many, many years before those therapeutics could be vetted out and eventually be handed down to the Waldenström investigators.”
At Lymphoma & Myeloma 2016, Dr Treon described the current therapy of WM and the impact of the discovery of MYD88 and CXCR4 on drug development and treatment choices in WM.
Rituximab-based therapy
WM is a disease that strongly expresses CD20, even though it’s a lymphoplasmacytic disease. So rituximab, given alone and in combination, has been, to date, the most common approach to treating WM.
As a single agent, rituximab produces a response in 25% to 40% of WM patients, but these are very seldom deep responses, Dr Treon noted.
So investigators combined rituximab with cyclophosphamide, nucleoside analogues, proteasome inhibitors, and bendamustine, which increased the overall response rate and depth of response.
This translated into improvement in time to progression, which is now 4 to 5 years with these combination therapies.
“Now, the problem is, when you borrow things from other people, you sometimes end up with problems you didn’t anticipate,” Dr Treon said.
One of the unanticipated side effects with rituximab in WM patients is the IgM flare, which occurs in 40% to 60% of WM patients.
Rituximab can also cause hypogammaglobulinema, leading to infections, and results in a high intolerance rate, which tends to occur a few cycles into induction or maintenance therapy.
“In some cases,” Dr Treon advised, “a switch to ofatumumab, a fully human CD20 molecule, overcomes this intolerance.”
Nucleoside analogues, which used to be the mainstay of WM, have a high rate of transformation into a more aggressive lymphoma or acute myeloid leukemia.
Immunomodulatory drugs, particularly thalidomide, cause peripheral neuropathy greater than grade 2 in 60% of patients.
And a greater incidence of peripheral neuropathy is also observed with proteasome inhibitors, particularly bortezomib, in WM patients than in myeloma or mantle cell lymphoma patients.
“So this was at least the impetus for why we needed to develop novel approaches to treating this disease,” Dr Treon said.
MYD88 mutations
With whole-genome sequencing, investigators discovered that mutations in the MYD88 gene were highly prevalent in WM patients.
About 93% to 95% of WM patients have the L265P MYD88 mutation, and about 2% have the non-L265P MYD88 mutation.
MYD88 has prognostic significance in WM. Mutated MYD88 confers a better prognosis than unmutated MYD88.
MYD88 may also be important in predicting who will respond to drugs like ibrutinib.
CXCR4 mutations
Mutations in CXCR4 are the second most common mutation in WM.
Between 30% and 40% of WM patients have the WHIM-like CXCR4 C-tail mutations, which traffic the Waldenström’s cells to the bone marrow.
This mutation promotes drug resistance, including resistance to ibrutinib because of the enhanced AKT/ERK signaling.
Ibrutinib therapy
With this in mind, investigators set out to evaluate the potential of using a BTK inhibitor in relapsed/refractory WM patients and at the same time observe the genomics that might predict for response and resistance.
They enrolled 63 patients in the multicenter study. Patients had a median of 2 prior therapies (range, 1–9), and 60% had bone marrow involvement.
Patients received single-agent ibrutinib at a dose of 420 mg orally each day until disease progression or the development of unacceptable toxic side effects.
“By the time they came back 4 weeks later to be evaluated, many of them were already in a response,” Dr Treon said. “And what we saw, in fact, was almost immediate improvement in hemoglobin, something that we didn’t see with many of our trials before that.”
The best IgM response reduced levels from 3520 to 880 mg/dL (P<0.001) for the entire cohort.
The best hemoglobin response increased hemoglobin levels 3 points, from 10.5 to 13.8 g/dL (P<0.001).
The progression-free survival at 2 years was 69% and overall survival was 95%.
At 37 months, most patients who achieve a response experience a durable, ongoing response, according to an update presented at the IX International Workshop on Waldenstrom’s Macroglobulinemia.
And toxicities were “very much in line with what our colleagues have seen in other disease groups,” Dr Treon stated.
Response to ibrutinib by mutation status
The overall response rate was 90% for all patients, but there were differences according to mutation status.
Patients with no MYD88 mutation and no CXCR4 mutation had absolutely no major response.
Patients with a MYD88 mutation responded at an overall rate of 100% and had a major response rate of 91.7% if they did not have a CXCR4 mutation as well.
If they also had a CXCR4WHIM mutation, the overall response rate was lower, at 85.7%, and the major response rate was 61.9%.
“It’s still something to be incredibly excited about—61.9% single-agent activity,” Dr Treon said.
Patients with a CXCR4 mutation also respond more slowly than those without the mutation.
This investigator-sponsored study led to the approval of ibrutinib in WM in the US as well as in Europe and Canada.
“And the point to make about this is that investigators can bring their data to the FDA, the EMA, even Canada, and it can make a difference,” Dr Treon said.
“We don’t always have to have company-sponsored registration studies to be able to make these kinds of advances.”
Ibrutinib in rituximab-refractory patients
A multicenter, phase 3 study of ibrutinib in rituximab-refractory patients was “almost a photocopy of our study,” Dr Treon said.
The main difference was that the patients were even sicker, having failed a median of 4 prior therapies.
Patients experienced rapid improvements in hemoglobin and IgM levels and had an overall response rate of 90%.
Patients with a CXCR4 mutation also tended to lag in terms of pace of hemoglobin improvement and reduction in IgM.
The study was just accepted for publication in Lancet Oncology.
IRAK inhibition
Investigators were puzzled by the paucity of complete responses with ibrutinib, and they found the IRAK pathway remained turned on in patients treated with ibrutinib.
So they took cells of patients treated for 6 months with ibrutinib and co-cultured them with ibrutinib and an IRAK inhibitor. They observed the induction of apoptosis.
Based on this finding, the investigators are manufacturing a very potent IRAK1 inhibitor (JH-X-119), which, when combined with ibrutinib, synergistically increases tumor-cell killing.
“And so one of the strategies we have going forward,” Dr Treon said, “is the ability to advance ibrutinib therapy in MYD88-mutated tumors by the addition of the IRAK inhibitor.”
Resistance to ibrutinib
Investigators have found multiple mutations in the C481 site in individual WM patients, which is where ibrutinib binds.
These mutations represent a minority of the clone, but they exert almost a fully clonal signature. The few patients with these mutations also have a CXCR4 mutation.
C481 mutations shift the signaling of cells in the presence of ibrutinib toward ERK, which is a very powerful survival pathway.
So investigators are examining whether an ERK inhibitor combined with ibrutinib can elicit synergistic killing of BTK-resistant cells.
Investigators have also been synthesizing potent HCK inhibitors, which might overcome BTK mutations by shutting down the ability to activate Bruton’s tyrosine kinase.
Other drugs being developed for WM include:
- Combinations with a proteasome inhibitor, such as ixazomib, dexamethasone, and rituximab
- Agents that target MYD88 signaling, such as the BTK inhibitors acalabrutinib and BGB-3111
- Agents that block CXCR4 receptor signaling, such as ulocuplomab
- The BCL2 inhibitor venetoclax
- The CD38-targeted agent daratumumab.
Current treatment strategies
Knowing a patient’s MYD88 and CXCR4 mutation status provides an opportunity to take a rational approach to treating individuals with WM, Dr Treon said.
For patients with mutated MYD88 and no CXCR4 mutation:
- If patients do not have bulky disease or contraindications, ibrutinib may be used if available.
- If patients have bulky disease, a combination of bendamustine and rituximab may be used.
- If patients have amyloidosis, a combination of bortezomib, dexamethasone, and rituximab is possible.
- If patients have IgM peripheral neuropathy, then rituximab with or without an alkylator is recommended.
For patients with mutated MYD88 and mutated CXCR4, the same treatments can be used as for patients with mutated MYD88 and unmutated CXCR4 with the same restrictions.
To achieve an immediate response for patients with a CXCR4 mutation, an alternative therapy to ibrutinib—such as the bendamustine, dexamethasone, rituximab combination—may be the best choice, because CXCR4-mutated individuals have a slower response to ibrutinib.
The problem arises with the MYD88-wild-type patients, because their survival is poorer than the MYD88-mutated patients.
“We still don’t know what’s wrong with these individuals,” Dr Treon said. “We don’t have any idea about what their basic genomic problems are.”
Bendamustine- or bortezomib-based therapy is effective in this population and can be considered.
In terms of salvage therapy, “the only thing to keep in mind is that if something worked the first time and you got at least a 2-year response with it, you can go back and consider it,” Dr Treon said. ![]()
Photo courtesy of DFCI
NEW YORK—Whole-genome sequencing has changed the entire approach to drug development for Waldenström’s macroglobulinemia (WM), according to a speaker at Lymphoma & Myeloma 2016.
The strategy has changed from a hand-me-down one, relying on drugs developed first for other diseases, to a rational plan designed specifically to treat WM patients.
“We would wait for our colleagues in the myeloma world or lymphoma world, CLL world, anywhere we could find them, to help us with the development of drugs,” said Steven Treon, MD, PhD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“And, sometimes, this resulted in delays of many, many years before those therapeutics could be vetted out and eventually be handed down to the Waldenström investigators.”
At Lymphoma & Myeloma 2016, Dr Treon described the current therapy of WM and the impact of the discovery of MYD88 and CXCR4 on drug development and treatment choices in WM.
Rituximab-based therapy
WM is a disease that strongly expresses CD20, even though it’s a lymphoplasmacytic disease. So rituximab, given alone and in combination, has been, to date, the most common approach to treating WM.
As a single agent, rituximab produces a response in 25% to 40% of WM patients, but these are very seldom deep responses, Dr Treon noted.
So investigators combined rituximab with cyclophosphamide, nucleoside analogues, proteasome inhibitors, and bendamustine, which increased the overall response rate and depth of response.
This translated into improvement in time to progression, which is now 4 to 5 years with these combination therapies.
“Now, the problem is, when you borrow things from other people, you sometimes end up with problems you didn’t anticipate,” Dr Treon said.
One of the unanticipated side effects with rituximab in WM patients is the IgM flare, which occurs in 40% to 60% of WM patients.
Rituximab can also cause hypogammaglobulinema, leading to infections, and results in a high intolerance rate, which tends to occur a few cycles into induction or maintenance therapy.
“In some cases,” Dr Treon advised, “a switch to ofatumumab, a fully human CD20 molecule, overcomes this intolerance.”
Nucleoside analogues, which used to be the mainstay of WM, have a high rate of transformation into a more aggressive lymphoma or acute myeloid leukemia.
Immunomodulatory drugs, particularly thalidomide, cause peripheral neuropathy greater than grade 2 in 60% of patients.
And a greater incidence of peripheral neuropathy is also observed with proteasome inhibitors, particularly bortezomib, in WM patients than in myeloma or mantle cell lymphoma patients.
“So this was at least the impetus for why we needed to develop novel approaches to treating this disease,” Dr Treon said.
MYD88 mutations
With whole-genome sequencing, investigators discovered that mutations in the MYD88 gene were highly prevalent in WM patients.
About 93% to 95% of WM patients have the L265P MYD88 mutation, and about 2% have the non-L265P MYD88 mutation.
MYD88 has prognostic significance in WM. Mutated MYD88 confers a better prognosis than unmutated MYD88.
MYD88 may also be important in predicting who will respond to drugs like ibrutinib.
CXCR4 mutations
Mutations in CXCR4 are the second most common mutation in WM.
Between 30% and 40% of WM patients have the WHIM-like CXCR4 C-tail mutations, which traffic the Waldenström’s cells to the bone marrow.
This mutation promotes drug resistance, including resistance to ibrutinib because of the enhanced AKT/ERK signaling.
Ibrutinib therapy
With this in mind, investigators set out to evaluate the potential of using a BTK inhibitor in relapsed/refractory WM patients and at the same time observe the genomics that might predict for response and resistance.
They enrolled 63 patients in the multicenter study. Patients had a median of 2 prior therapies (range, 1–9), and 60% had bone marrow involvement.
Patients received single-agent ibrutinib at a dose of 420 mg orally each day until disease progression or the development of unacceptable toxic side effects.
“By the time they came back 4 weeks later to be evaluated, many of them were already in a response,” Dr Treon said. “And what we saw, in fact, was almost immediate improvement in hemoglobin, something that we didn’t see with many of our trials before that.”
The best IgM response reduced levels from 3520 to 880 mg/dL (P<0.001) for the entire cohort.
The best hemoglobin response increased hemoglobin levels 3 points, from 10.5 to 13.8 g/dL (P<0.001).
The progression-free survival at 2 years was 69% and overall survival was 95%.
At 37 months, most patients who achieve a response experience a durable, ongoing response, according to an update presented at the IX International Workshop on Waldenstrom’s Macroglobulinemia.
And toxicities were “very much in line with what our colleagues have seen in other disease groups,” Dr Treon stated.
Response to ibrutinib by mutation status
The overall response rate was 90% for all patients, but there were differences according to mutation status.
Patients with no MYD88 mutation and no CXCR4 mutation had absolutely no major response.
Patients with a MYD88 mutation responded at an overall rate of 100% and had a major response rate of 91.7% if they did not have a CXCR4 mutation as well.
If they also had a CXCR4WHIM mutation, the overall response rate was lower, at 85.7%, and the major response rate was 61.9%.
“It’s still something to be incredibly excited about—61.9% single-agent activity,” Dr Treon said.
Patients with a CXCR4 mutation also respond more slowly than those without the mutation.
This investigator-sponsored study led to the approval of ibrutinib in WM in the US as well as in Europe and Canada.
“And the point to make about this is that investigators can bring their data to the FDA, the EMA, even Canada, and it can make a difference,” Dr Treon said.
“We don’t always have to have company-sponsored registration studies to be able to make these kinds of advances.”
Ibrutinib in rituximab-refractory patients
A multicenter, phase 3 study of ibrutinib in rituximab-refractory patients was “almost a photocopy of our study,” Dr Treon said.
The main difference was that the patients were even sicker, having failed a median of 4 prior therapies.
Patients experienced rapid improvements in hemoglobin and IgM levels and had an overall response rate of 90%.
Patients with a CXCR4 mutation also tended to lag in terms of pace of hemoglobin improvement and reduction in IgM.
The study was just accepted for publication in Lancet Oncology.
IRAK inhibition
Investigators were puzzled by the paucity of complete responses with ibrutinib, and they found the IRAK pathway remained turned on in patients treated with ibrutinib.
So they took cells of patients treated for 6 months with ibrutinib and co-cultured them with ibrutinib and an IRAK inhibitor. They observed the induction of apoptosis.
Based on this finding, the investigators are manufacturing a very potent IRAK1 inhibitor (JH-X-119), which, when combined with ibrutinib, synergistically increases tumor-cell killing.
“And so one of the strategies we have going forward,” Dr Treon said, “is the ability to advance ibrutinib therapy in MYD88-mutated tumors by the addition of the IRAK inhibitor.”
Resistance to ibrutinib
Investigators have found multiple mutations in the C481 site in individual WM patients, which is where ibrutinib binds.
These mutations represent a minority of the clone, but they exert almost a fully clonal signature. The few patients with these mutations also have a CXCR4 mutation.
C481 mutations shift the signaling of cells in the presence of ibrutinib toward ERK, which is a very powerful survival pathway.
So investigators are examining whether an ERK inhibitor combined with ibrutinib can elicit synergistic killing of BTK-resistant cells.
Investigators have also been synthesizing potent HCK inhibitors, which might overcome BTK mutations by shutting down the ability to activate Bruton’s tyrosine kinase.
Other drugs being developed for WM include:
- Combinations with a proteasome inhibitor, such as ixazomib, dexamethasone, and rituximab
- Agents that target MYD88 signaling, such as the BTK inhibitors acalabrutinib and BGB-3111
- Agents that block CXCR4 receptor signaling, such as ulocuplomab
- The BCL2 inhibitor venetoclax
- The CD38-targeted agent daratumumab.
Current treatment strategies
Knowing a patient’s MYD88 and CXCR4 mutation status provides an opportunity to take a rational approach to treating individuals with WM, Dr Treon said.
For patients with mutated MYD88 and no CXCR4 mutation:
- If patients do not have bulky disease or contraindications, ibrutinib may be used if available.
- If patients have bulky disease, a combination of bendamustine and rituximab may be used.
- If patients have amyloidosis, a combination of bortezomib, dexamethasone, and rituximab is possible.
- If patients have IgM peripheral neuropathy, then rituximab with or without an alkylator is recommended.
For patients with mutated MYD88 and mutated CXCR4, the same treatments can be used as for patients with mutated MYD88 and unmutated CXCR4 with the same restrictions.
To achieve an immediate response for patients with a CXCR4 mutation, an alternative therapy to ibrutinib—such as the bendamustine, dexamethasone, rituximab combination—may be the best choice, because CXCR4-mutated individuals have a slower response to ibrutinib.
The problem arises with the MYD88-wild-type patients, because their survival is poorer than the MYD88-mutated patients.
“We still don’t know what’s wrong with these individuals,” Dr Treon said. “We don’t have any idea about what their basic genomic problems are.”
Bendamustine- or bortezomib-based therapy is effective in this population and can be considered.
In terms of salvage therapy, “the only thing to keep in mind is that if something worked the first time and you got at least a 2-year response with it, you can go back and consider it,” Dr Treon said. ![]()
Speaker says use the best regimen ASAP in MM

NEW YORK—It’s important to use the best possible regimen as soon as possible when treating patients with multiple myeloma (MM), according to a speaker at Lymphoma & Myeloma 2016.
Antonio Palumbo, MD, of the University of Torino in Italy, explained that the urgency, from a biological point of view, is because myeloma accumulates genetic mutations that change the disease in a “dramatic way.”
“At diagnosis, you might have 5000 mutations, and, at first relapse, there are 12,000 mutations,” he said. “They are completely different tumors. So the first thing that we have to recognize is that, with time, myeloma is not the same. It’s becoming different tumors.”
Dr Palumbo noted that early intervention is important because genetic and epigenetic abnormalities increase as the disease progresses and becomes more resistant.
For example, if 100 patients receive first-line treatment, 40 of them will not reach the second line. Only 60 patients will receive second-line therapy, and only 35 patients will receive third-line treatment. By the fifth line, only 10 patients, or 10%, will receive it.
“If you have very good genomic stability, you can become sensitive to different treatments,” Dr Palumbo said. “But if you become a different disease, you will not be able to receive the next therapy. That’s why it’s so important . . . to use the best possible regimen as soon as possible.”
Best regimens
The triplet bortezomib-lenalidomide-dexamethasone is the “best possible regimen today,” Dr Palumbo said, “followed by continuous therapy.”
The 2-drug combination of lenalidomide and dexamethasone is probably more suitable for the elderly and the frail.
Alternative regimens include carfilzomib-cyclophosphamide-dexamethasone and ixazomib-lenalidomide-dexamethasone.
Continuous therapy
Continuous therapy has been “one of the major achievements” in the treatment of MM, Dr Palumbo said. Without continuous therapy, patients in complete response remain so for about 1 year when treated with conventional chemotherapy.
Investigators found that maintenance therapy significantly prolongs progression-free survival and overall survival (P=0.02). They recommend intensification with maintenance to optimize treatment efficacy and prolong survival.
Immunomodulatory drugs such as lenalidomide are the backbone of continuous therapy today.
However, ixazomib represents another option. Ixazomib maintenance has been shown to produce durable responses for a median of more than 2 years in previously untreated patients not undergoing autologous stem cell transplant.
Salvage therapy
Seven combinations are now available for salvage therapy, including those with proteasome inhibitors, monoclonal antibodies, pomalidomide, and histone deacetylase inhibitors.
Included in some of these combinations are the newer agents ixazomib, elotuzumab, and daratumumab, “which many might consider the new rituximab,” Dr Palumbo said.
Risk stratification
Dr Palumbo stressed the importance of risk stratification—both in clinical trials and in practice.
“[T]he moment you under-treat a patient, you transform a good-risk patient into a high-risk patient . . . ,” he said.
And if trials comparing treatments are not conducted within risk categories, researchers are comparing apples to oranges—good risk with high risk
The Revised International Staging System (R-ISS) for MM effectively stratifies newly diagnosed patients by combining the original ISS, chromosomal abnormalities, and serum lactate dehydrogenase levels to evaluate prognosis.
The R-ISS defines 3 new, distinct categories that researchers believe effectively define patients’ relative risk with respect to their survival.
Age and frailty
MM patients generally fall into 3 age categories: 25-64, 65-74, and 75-101.
The youngest group can receive autologous transplant, the fit patients ages 65 to 74 can receive full-dose chemotherapy, and the oldest, frailer patients should receive reduced-dose chemotherapy.
“It’s important to differentiate fit from frail,” Dr Palumbo said, “because we cannot give the same treatment schema to a 55-year-old versus 65 or 85. At 85, that schema would create a lot of toxicities.”
In frail patients, it’s always important to check which comorbidities are present using the Charlson comorbidity scale, Dr Palumbo said.
“Remember, when we put together age, chromosome abnormalities, and frailty, frailty is the most relevant prognostic factor when you add everything together,” he said.
“Two drugs versus 3 drugs doesn’t make much difference when you are starting to introduce treatment to these very frail patients with comorbidities.”
Minimal residual disease
Dr Palumbo indicated that a combination of MRI and PET-CT should be used for a more accurate indication of minimal residual disease.
“[W]e hope to have cure, [but] I don’t think, today, myeloma is a curable disease,” he said.
He clarified this by saying that patients who are in complete response and minimal residual disease-negative at 3 years do well, but, by 7 years, “something is happening.”
And at 10 years, progression-free survival has dropped off significantly, “telling us that cure is probably not yet there.” ![]()
NEW YORK—It’s important to use the best possible regimen as soon as possible when treating patients with multiple myeloma (MM), according to a speaker at Lymphoma & Myeloma 2016.
Antonio Palumbo, MD, of the University of Torino in Italy, explained that the urgency, from a biological point of view, is because myeloma accumulates genetic mutations that change the disease in a “dramatic way.”
“At diagnosis, you might have 5000 mutations, and, at first relapse, there are 12,000 mutations,” he said. “They are completely different tumors. So the first thing that we have to recognize is that, with time, myeloma is not the same. It’s becoming different tumors.”
Dr Palumbo noted that early intervention is important because genetic and epigenetic abnormalities increase as the disease progresses and becomes more resistant.
For example, if 100 patients receive first-line treatment, 40 of them will not reach the second line. Only 60 patients will receive second-line therapy, and only 35 patients will receive third-line treatment. By the fifth line, only 10 patients, or 10%, will receive it.
“If you have very good genomic stability, you can become sensitive to different treatments,” Dr Palumbo said. “But if you become a different disease, you will not be able to receive the next therapy. That’s why it’s so important . . . to use the best possible regimen as soon as possible.”
Best regimens
The triplet bortezomib-lenalidomide-dexamethasone is the “best possible regimen today,” Dr Palumbo said, “followed by continuous therapy.”
The 2-drug combination of lenalidomide and dexamethasone is probably more suitable for the elderly and the frail.
Alternative regimens include carfilzomib-cyclophosphamide-dexamethasone and ixazomib-lenalidomide-dexamethasone.
Continuous therapy
Continuous therapy has been “one of the major achievements” in the treatment of MM, Dr Palumbo said. Without continuous therapy, patients in complete response remain so for about 1 year when treated with conventional chemotherapy.
Investigators found that maintenance therapy significantly prolongs progression-free survival and overall survival (P=0.02). They recommend intensification with maintenance to optimize treatment efficacy and prolong survival.
Immunomodulatory drugs such as lenalidomide are the backbone of continuous therapy today.
However, ixazomib represents another option. Ixazomib maintenance has been shown to produce durable responses for a median of more than 2 years in previously untreated patients not undergoing autologous stem cell transplant.
Salvage therapy
Seven combinations are now available for salvage therapy, including those with proteasome inhibitors, monoclonal antibodies, pomalidomide, and histone deacetylase inhibitors.
Included in some of these combinations are the newer agents ixazomib, elotuzumab, and daratumumab, “which many might consider the new rituximab,” Dr Palumbo said.
Risk stratification
Dr Palumbo stressed the importance of risk stratification—both in clinical trials and in practice.
“[T]he moment you under-treat a patient, you transform a good-risk patient into a high-risk patient . . . ,” he said.
And if trials comparing treatments are not conducted within risk categories, researchers are comparing apples to oranges—good risk with high risk
The Revised International Staging System (R-ISS) for MM effectively stratifies newly diagnosed patients by combining the original ISS, chromosomal abnormalities, and serum lactate dehydrogenase levels to evaluate prognosis.
The R-ISS defines 3 new, distinct categories that researchers believe effectively define patients’ relative risk with respect to their survival.
Age and frailty
MM patients generally fall into 3 age categories: 25-64, 65-74, and 75-101.
The youngest group can receive autologous transplant, the fit patients ages 65 to 74 can receive full-dose chemotherapy, and the oldest, frailer patients should receive reduced-dose chemotherapy.
“It’s important to differentiate fit from frail,” Dr Palumbo said, “because we cannot give the same treatment schema to a 55-year-old versus 65 or 85. At 85, that schema would create a lot of toxicities.”
In frail patients, it’s always important to check which comorbidities are present using the Charlson comorbidity scale, Dr Palumbo said.
“Remember, when we put together age, chromosome abnormalities, and frailty, frailty is the most relevant prognostic factor when you add everything together,” he said.
“Two drugs versus 3 drugs doesn’t make much difference when you are starting to introduce treatment to these very frail patients with comorbidities.”
Minimal residual disease
Dr Palumbo indicated that a combination of MRI and PET-CT should be used for a more accurate indication of minimal residual disease.
“[W]e hope to have cure, [but] I don’t think, today, myeloma is a curable disease,” he said.
He clarified this by saying that patients who are in complete response and minimal residual disease-negative at 3 years do well, but, by 7 years, “something is happening.”
And at 10 years, progression-free survival has dropped off significantly, “telling us that cure is probably not yet there.” ![]()
NEW YORK—It’s important to use the best possible regimen as soon as possible when treating patients with multiple myeloma (MM), according to a speaker at Lymphoma & Myeloma 2016.
Antonio Palumbo, MD, of the University of Torino in Italy, explained that the urgency, from a biological point of view, is because myeloma accumulates genetic mutations that change the disease in a “dramatic way.”
“At diagnosis, you might have 5000 mutations, and, at first relapse, there are 12,000 mutations,” he said. “They are completely different tumors. So the first thing that we have to recognize is that, with time, myeloma is not the same. It’s becoming different tumors.”
Dr Palumbo noted that early intervention is important because genetic and epigenetic abnormalities increase as the disease progresses and becomes more resistant.
For example, if 100 patients receive first-line treatment, 40 of them will not reach the second line. Only 60 patients will receive second-line therapy, and only 35 patients will receive third-line treatment. By the fifth line, only 10 patients, or 10%, will receive it.
“If you have very good genomic stability, you can become sensitive to different treatments,” Dr Palumbo said. “But if you become a different disease, you will not be able to receive the next therapy. That’s why it’s so important . . . to use the best possible regimen as soon as possible.”
Best regimens
The triplet bortezomib-lenalidomide-dexamethasone is the “best possible regimen today,” Dr Palumbo said, “followed by continuous therapy.”
The 2-drug combination of lenalidomide and dexamethasone is probably more suitable for the elderly and the frail.
Alternative regimens include carfilzomib-cyclophosphamide-dexamethasone and ixazomib-lenalidomide-dexamethasone.
Continuous therapy
Continuous therapy has been “one of the major achievements” in the treatment of MM, Dr Palumbo said. Without continuous therapy, patients in complete response remain so for about 1 year when treated with conventional chemotherapy.
Investigators found that maintenance therapy significantly prolongs progression-free survival and overall survival (P=0.02). They recommend intensification with maintenance to optimize treatment efficacy and prolong survival.
Immunomodulatory drugs such as lenalidomide are the backbone of continuous therapy today.
However, ixazomib represents another option. Ixazomib maintenance has been shown to produce durable responses for a median of more than 2 years in previously untreated patients not undergoing autologous stem cell transplant.
Salvage therapy
Seven combinations are now available for salvage therapy, including those with proteasome inhibitors, monoclonal antibodies, pomalidomide, and histone deacetylase inhibitors.
Included in some of these combinations are the newer agents ixazomib, elotuzumab, and daratumumab, “which many might consider the new rituximab,” Dr Palumbo said.
Risk stratification
Dr Palumbo stressed the importance of risk stratification—both in clinical trials and in practice.
“[T]he moment you under-treat a patient, you transform a good-risk patient into a high-risk patient . . . ,” he said.
And if trials comparing treatments are not conducted within risk categories, researchers are comparing apples to oranges—good risk with high risk
The Revised International Staging System (R-ISS) for MM effectively stratifies newly diagnosed patients by combining the original ISS, chromosomal abnormalities, and serum lactate dehydrogenase levels to evaluate prognosis.
The R-ISS defines 3 new, distinct categories that researchers believe effectively define patients’ relative risk with respect to their survival.
Age and frailty
MM patients generally fall into 3 age categories: 25-64, 65-74, and 75-101.
The youngest group can receive autologous transplant, the fit patients ages 65 to 74 can receive full-dose chemotherapy, and the oldest, frailer patients should receive reduced-dose chemotherapy.
“It’s important to differentiate fit from frail,” Dr Palumbo said, “because we cannot give the same treatment schema to a 55-year-old versus 65 or 85. At 85, that schema would create a lot of toxicities.”
In frail patients, it’s always important to check which comorbidities are present using the Charlson comorbidity scale, Dr Palumbo said.
“Remember, when we put together age, chromosome abnormalities, and frailty, frailty is the most relevant prognostic factor when you add everything together,” he said.
“Two drugs versus 3 drugs doesn’t make much difference when you are starting to introduce treatment to these very frail patients with comorbidities.”
Minimal residual disease
Dr Palumbo indicated that a combination of MRI and PET-CT should be used for a more accurate indication of minimal residual disease.
“[W]e hope to have cure, [but] I don’t think, today, myeloma is a curable disease,” he said.
He clarified this by saying that patients who are in complete response and minimal residual disease-negative at 3 years do well, but, by 7 years, “something is happening.”
And at 10 years, progression-free survival has dropped off significantly, “telling us that cure is probably not yet there.” ![]()
Doc provides perspective on CAR T-cell therapy in CLL

Photo from Penn Medicine
NEW YORK—Trial data on the use of chimeric antigen receptor (CAR) T cells in chronic lymphocytic leukemia (CLL) are maturing, and a speaker at Lymphoma & Myeloma 2016 provided some perspective on the therapy as it now stands.
Stephen J. Schuster, MD, of the University of Pennsylvania in Philadelphia, noted that some CLL patients treated with CAR T cells remain in complete remission (CR) for more than 5 years.
Therefore, CAR T cells may be a consideration for patients who are resistant to chemotherapy.
“[I]mportantly, this immunologic approach, like other immunologic approaches . . ., tends to be non-cross-resistant to chemotherapy,” Dr Schuster said.
He made these and other observations while discussing trials of CAR T-cell therapy (particularly CTL019) in CLL.
Pilot study of CTL019 in CLL
CTL019, which is the CAR T-cell therapy used by investigators at the University of Pennsylvania, is licensed to Novartis.
The pilot study of CTL019, begun in 2009, enrolled 14 patients who had failed at least 2 prior therapies and progressed within 2 years of their last treatment.
Four patients (29%) achieved a CR, and 4 (29%) achieved a partial response (PR), for an overall response rate of 57%. Detailed results from this trial were reported earlier in HematologyTimes.
Two patients in this trial are still in CR beyond 5 years.
When investigators analyzed the different variables that might affect response—including age, number of prior therapies, p53 status, CAR T-cell dose, and the presence of cytokine release syndrome (CRS)—2 things became apparent.
First, patients who responded tended to have greater in vivo expansion of the CAR T cells than non-responders. And second, the responders had a greater incidence of CRS than non-responders.
Additionally, complete responders were negative for minimal residual disease (MRD) and had durable responses.
“This actually is different from the data you see in lymphoma with CAR cells,” Dr Schuster said. “[However,] it’s what we see in ALL [acute lymphoblastic leukemia] as well.”
Investigators also discovered that persistence of CAR T cells correlates with B-cell aplasia. In this trial, persistence of CAR T cells and B-cell aplasia were apparent at 12 and 18 months, and, in some cases, even longer.
“This is in distinction to what we are observing in trials with the lymphomas,” Dr Schuster said. “So what’s going to emerge is that the different diseases will have different response rates, different degrees of persistence of CAR cells and different toxicities.”
“When we compare B-cell ALL, B-cell non-Hodgkin lymphomas, you’ll get different responses across the subtypes of lymphomas, some unique toxicities, and differences in CLL. So these are all different diseases.”
Dose-finding trial of CTL019 in CLL
The second trial of CTL019 in relapsed/refractory CLL patients was a dose-finding study. Updated results from this study were presented at ASCO 2016.
The high-dose arm (5x108 CTL019) had a 10 times higher dose of CAR T cells than the low-dose arm (5x107 CTL019).
Investigators treated 12 patients in each arm in the first phase of the study, and then expanded the trial to include another 8 patients at the recommended dose. The phase 2 trial was powered for response rates but not duration of response.
Twenty-eight patients were enrolled, with 24 evaluable, 11 in the high-dose arm and 13 in the low-dose arm.
Their median age was 62 (range, 51-75), the median number of prior therapies was 4 (range, 2–7), 38% had p53 deletion, and 12% had received prior ibrutinib therapy.
With the 2 arms pooled together, 25% of patients achieved a CR, and 17% achieved a PR, for an overall response rate of 42%.
“Toxicities were identical in each group,” Dr Schuster said.
He noted that the CRS rate was “fairly high.” The incidence was 55% in the high-dose arm and 54% in the low-dose arm.
There was a tendency, although not statistically significant, for the higher-dose patients to have a greater response rate than the lower-dose group—54% and 31%, respectively.
So the investigators decided the expansion cohort should be conducted with the higher dose, “even though we weren’t sure there really was a difference,” Dr Schuster said.
Seventeen evaluable patients received the higher dose in the expansion cohort. Six (35%) achieved a CR, and 3 (18%) achieved a PR, for an overall response rate of 53%.
“Most [adverse] events happen in the first 3 months,” after infusion, Dr Schuster said. “And then nothing much happens. That’s because the patients that are responsive to this therapy have durable responses.”
Of all the patients who achieved a CR, only 2 have relapsed, he said, “and now many of these patients have passed the 5-year mark for complete remissions.”
Toxicity of CTL019 in CLL
“When you give the cells, there’s not much toxicity,” Dr Schuster said. “These are the patients’ own cells; they’re not reacting adversely to that. It’s what happens afterwards that you have to be on the lookout for as the cells begin to expand in vivo.”
Patients experience some reversible renal toxicity, mostly hypertension-related, and some tumor lysis syndrome (TLS). No deaths occurred from TLS in CLL.
B-cell aplasia and hypogammaglobulinema occur in responding patients. They receive gamma globulin replacement as supportive therapy and generally experience no excessive or unusual infections.
“Cytokine release syndrome is the real thing to look at,” Dr Schuster said, “and that’s where early recognition and management will be life-saving.”
In both CLL and ALL, almost all responding patients develop CRS, which can be rapidly reversed with tocilizumab, the IL-6 receptor blocker.
Other CAR T-cell trials in CLL
Institutions other than the University of Pennsylvania have conducted trials of CAR T-cell therapies other than CTL019, and response rates in CLL patients have ranged from 25% (MSKCC) to 46% (Seattle), as reported at ASCO this year.
“But what’s really important to keep in mind is almost all patients who achieve complete response to date have stayed in complete response,” Dr Schuster said.
Combination trials with ibrutinib
Dr Schuster noted that patients in CAR T-cell trials who had been on ibrutinib for more than 5 months “had really robust T-cell expansion.”
So investigators believe treatment with ibrutinib may be a way of enhancing T-cell function.
A combination trial of ibrutinib and CTL019 is underway (NCT02640209). Six patients have been treated thus far, and although the follow-up is short, all 6 achieved CR at the 3-month assessment.
“So the hope is that this is going to be a partner [therapy],” Dr Schuster said. “And maybe these complete responses will be very durable, like the responses in earlier trials of CAR therapy in patients with CLL.” ![]()
Photo from Penn Medicine
NEW YORK—Trial data on the use of chimeric antigen receptor (CAR) T cells in chronic lymphocytic leukemia (CLL) are maturing, and a speaker at Lymphoma & Myeloma 2016 provided some perspective on the therapy as it now stands.
Stephen J. Schuster, MD, of the University of Pennsylvania in Philadelphia, noted that some CLL patients treated with CAR T cells remain in complete remission (CR) for more than 5 years.
Therefore, CAR T cells may be a consideration for patients who are resistant to chemotherapy.
“[I]mportantly, this immunologic approach, like other immunologic approaches . . ., tends to be non-cross-resistant to chemotherapy,” Dr Schuster said.
He made these and other observations while discussing trials of CAR T-cell therapy (particularly CTL019) in CLL.
Pilot study of CTL019 in CLL
CTL019, which is the CAR T-cell therapy used by investigators at the University of Pennsylvania, is licensed to Novartis.
The pilot study of CTL019, begun in 2009, enrolled 14 patients who had failed at least 2 prior therapies and progressed within 2 years of their last treatment.
Four patients (29%) achieved a CR, and 4 (29%) achieved a partial response (PR), for an overall response rate of 57%. Detailed results from this trial were reported earlier in HematologyTimes.
Two patients in this trial are still in CR beyond 5 years.
When investigators analyzed the different variables that might affect response—including age, number of prior therapies, p53 status, CAR T-cell dose, and the presence of cytokine release syndrome (CRS)—2 things became apparent.
First, patients who responded tended to have greater in vivo expansion of the CAR T cells than non-responders. And second, the responders had a greater incidence of CRS than non-responders.
Additionally, complete responders were negative for minimal residual disease (MRD) and had durable responses.
“This actually is different from the data you see in lymphoma with CAR cells,” Dr Schuster said. “[However,] it’s what we see in ALL [acute lymphoblastic leukemia] as well.”
Investigators also discovered that persistence of CAR T cells correlates with B-cell aplasia. In this trial, persistence of CAR T cells and B-cell aplasia were apparent at 12 and 18 months, and, in some cases, even longer.
“This is in distinction to what we are observing in trials with the lymphomas,” Dr Schuster said. “So what’s going to emerge is that the different diseases will have different response rates, different degrees of persistence of CAR cells and different toxicities.”
“When we compare B-cell ALL, B-cell non-Hodgkin lymphomas, you’ll get different responses across the subtypes of lymphomas, some unique toxicities, and differences in CLL. So these are all different diseases.”
Dose-finding trial of CTL019 in CLL
The second trial of CTL019 in relapsed/refractory CLL patients was a dose-finding study. Updated results from this study were presented at ASCO 2016.
The high-dose arm (5x108 CTL019) had a 10 times higher dose of CAR T cells than the low-dose arm (5x107 CTL019).
Investigators treated 12 patients in each arm in the first phase of the study, and then expanded the trial to include another 8 patients at the recommended dose. The phase 2 trial was powered for response rates but not duration of response.
Twenty-eight patients were enrolled, with 24 evaluable, 11 in the high-dose arm and 13 in the low-dose arm.
Their median age was 62 (range, 51-75), the median number of prior therapies was 4 (range, 2–7), 38% had p53 deletion, and 12% had received prior ibrutinib therapy.
With the 2 arms pooled together, 25% of patients achieved a CR, and 17% achieved a PR, for an overall response rate of 42%.
“Toxicities were identical in each group,” Dr Schuster said.
He noted that the CRS rate was “fairly high.” The incidence was 55% in the high-dose arm and 54% in the low-dose arm.
There was a tendency, although not statistically significant, for the higher-dose patients to have a greater response rate than the lower-dose group—54% and 31%, respectively.
So the investigators decided the expansion cohort should be conducted with the higher dose, “even though we weren’t sure there really was a difference,” Dr Schuster said.
Seventeen evaluable patients received the higher dose in the expansion cohort. Six (35%) achieved a CR, and 3 (18%) achieved a PR, for an overall response rate of 53%.
“Most [adverse] events happen in the first 3 months,” after infusion, Dr Schuster said. “And then nothing much happens. That’s because the patients that are responsive to this therapy have durable responses.”
Of all the patients who achieved a CR, only 2 have relapsed, he said, “and now many of these patients have passed the 5-year mark for complete remissions.”
Toxicity of CTL019 in CLL
“When you give the cells, there’s not much toxicity,” Dr Schuster said. “These are the patients’ own cells; they’re not reacting adversely to that. It’s what happens afterwards that you have to be on the lookout for as the cells begin to expand in vivo.”
Patients experience some reversible renal toxicity, mostly hypertension-related, and some tumor lysis syndrome (TLS). No deaths occurred from TLS in CLL.
B-cell aplasia and hypogammaglobulinema occur in responding patients. They receive gamma globulin replacement as supportive therapy and generally experience no excessive or unusual infections.
“Cytokine release syndrome is the real thing to look at,” Dr Schuster said, “and that’s where early recognition and management will be life-saving.”
In both CLL and ALL, almost all responding patients develop CRS, which can be rapidly reversed with tocilizumab, the IL-6 receptor blocker.
Other CAR T-cell trials in CLL
Institutions other than the University of Pennsylvania have conducted trials of CAR T-cell therapies other than CTL019, and response rates in CLL patients have ranged from 25% (MSKCC) to 46% (Seattle), as reported at ASCO this year.
“But what’s really important to keep in mind is almost all patients who achieve complete response to date have stayed in complete response,” Dr Schuster said.
Combination trials with ibrutinib
Dr Schuster noted that patients in CAR T-cell trials who had been on ibrutinib for more than 5 months “had really robust T-cell expansion.”
So investigators believe treatment with ibrutinib may be a way of enhancing T-cell function.
A combination trial of ibrutinib and CTL019 is underway (NCT02640209). Six patients have been treated thus far, and although the follow-up is short, all 6 achieved CR at the 3-month assessment.
“So the hope is that this is going to be a partner [therapy],” Dr Schuster said. “And maybe these complete responses will be very durable, like the responses in earlier trials of CAR therapy in patients with CLL.” ![]()
Photo from Penn Medicine
NEW YORK—Trial data on the use of chimeric antigen receptor (CAR) T cells in chronic lymphocytic leukemia (CLL) are maturing, and a speaker at Lymphoma & Myeloma 2016 provided some perspective on the therapy as it now stands.
Stephen J. Schuster, MD, of the University of Pennsylvania in Philadelphia, noted that some CLL patients treated with CAR T cells remain in complete remission (CR) for more than 5 years.
Therefore, CAR T cells may be a consideration for patients who are resistant to chemotherapy.
“[I]mportantly, this immunologic approach, like other immunologic approaches . . ., tends to be non-cross-resistant to chemotherapy,” Dr Schuster said.
He made these and other observations while discussing trials of CAR T-cell therapy (particularly CTL019) in CLL.
Pilot study of CTL019 in CLL
CTL019, which is the CAR T-cell therapy used by investigators at the University of Pennsylvania, is licensed to Novartis.
The pilot study of CTL019, begun in 2009, enrolled 14 patients who had failed at least 2 prior therapies and progressed within 2 years of their last treatment.
Four patients (29%) achieved a CR, and 4 (29%) achieved a partial response (PR), for an overall response rate of 57%. Detailed results from this trial were reported earlier in HematologyTimes.
Two patients in this trial are still in CR beyond 5 years.
When investigators analyzed the different variables that might affect response—including age, number of prior therapies, p53 status, CAR T-cell dose, and the presence of cytokine release syndrome (CRS)—2 things became apparent.
First, patients who responded tended to have greater in vivo expansion of the CAR T cells than non-responders. And second, the responders had a greater incidence of CRS than non-responders.
Additionally, complete responders were negative for minimal residual disease (MRD) and had durable responses.
“This actually is different from the data you see in lymphoma with CAR cells,” Dr Schuster said. “[However,] it’s what we see in ALL [acute lymphoblastic leukemia] as well.”
Investigators also discovered that persistence of CAR T cells correlates with B-cell aplasia. In this trial, persistence of CAR T cells and B-cell aplasia were apparent at 12 and 18 months, and, in some cases, even longer.
“This is in distinction to what we are observing in trials with the lymphomas,” Dr Schuster said. “So what’s going to emerge is that the different diseases will have different response rates, different degrees of persistence of CAR cells and different toxicities.”
“When we compare B-cell ALL, B-cell non-Hodgkin lymphomas, you’ll get different responses across the subtypes of lymphomas, some unique toxicities, and differences in CLL. So these are all different diseases.”
Dose-finding trial of CTL019 in CLL
The second trial of CTL019 in relapsed/refractory CLL patients was a dose-finding study. Updated results from this study were presented at ASCO 2016.
The high-dose arm (5x108 CTL019) had a 10 times higher dose of CAR T cells than the low-dose arm (5x107 CTL019).
Investigators treated 12 patients in each arm in the first phase of the study, and then expanded the trial to include another 8 patients at the recommended dose. The phase 2 trial was powered for response rates but not duration of response.
Twenty-eight patients were enrolled, with 24 evaluable, 11 in the high-dose arm and 13 in the low-dose arm.
Their median age was 62 (range, 51-75), the median number of prior therapies was 4 (range, 2–7), 38% had p53 deletion, and 12% had received prior ibrutinib therapy.
With the 2 arms pooled together, 25% of patients achieved a CR, and 17% achieved a PR, for an overall response rate of 42%.
“Toxicities were identical in each group,” Dr Schuster said.
He noted that the CRS rate was “fairly high.” The incidence was 55% in the high-dose arm and 54% in the low-dose arm.
There was a tendency, although not statistically significant, for the higher-dose patients to have a greater response rate than the lower-dose group—54% and 31%, respectively.
So the investigators decided the expansion cohort should be conducted with the higher dose, “even though we weren’t sure there really was a difference,” Dr Schuster said.
Seventeen evaluable patients received the higher dose in the expansion cohort. Six (35%) achieved a CR, and 3 (18%) achieved a PR, for an overall response rate of 53%.
“Most [adverse] events happen in the first 3 months,” after infusion, Dr Schuster said. “And then nothing much happens. That’s because the patients that are responsive to this therapy have durable responses.”
Of all the patients who achieved a CR, only 2 have relapsed, he said, “and now many of these patients have passed the 5-year mark for complete remissions.”
Toxicity of CTL019 in CLL
“When you give the cells, there’s not much toxicity,” Dr Schuster said. “These are the patients’ own cells; they’re not reacting adversely to that. It’s what happens afterwards that you have to be on the lookout for as the cells begin to expand in vivo.”
Patients experience some reversible renal toxicity, mostly hypertension-related, and some tumor lysis syndrome (TLS). No deaths occurred from TLS in CLL.
B-cell aplasia and hypogammaglobulinema occur in responding patients. They receive gamma globulin replacement as supportive therapy and generally experience no excessive or unusual infections.
“Cytokine release syndrome is the real thing to look at,” Dr Schuster said, “and that’s where early recognition and management will be life-saving.”
In both CLL and ALL, almost all responding patients develop CRS, which can be rapidly reversed with tocilizumab, the IL-6 receptor blocker.
Other CAR T-cell trials in CLL
Institutions other than the University of Pennsylvania have conducted trials of CAR T-cell therapies other than CTL019, and response rates in CLL patients have ranged from 25% (MSKCC) to 46% (Seattle), as reported at ASCO this year.
“But what’s really important to keep in mind is almost all patients who achieve complete response to date have stayed in complete response,” Dr Schuster said.
Combination trials with ibrutinib
Dr Schuster noted that patients in CAR T-cell trials who had been on ibrutinib for more than 5 months “had really robust T-cell expansion.”
So investigators believe treatment with ibrutinib may be a way of enhancing T-cell function.
A combination trial of ibrutinib and CTL019 is underway (NCT02640209). Six patients have been treated thus far, and although the follow-up is short, all 6 achieved CR at the 3-month assessment.
“So the hope is that this is going to be a partner [therapy],” Dr Schuster said. “And maybe these complete responses will be very durable, like the responses in earlier trials of CAR therapy in patients with CLL.”
MF assessment and treatment an ‘evolution’ from the past

© ASCO/Zach Boyden-Holmes
NEW YORK—The 11th NCCN Congress: Hematologic Malignancies coincided with the release of the inaugural edition of the NCCN treatment guideline on myeloproliferative neoplasms (MPNs), and Ruben A. Mesa, MD, took the opportunity to discuss the framework of the document and the evolving management of MPNs.
Dr Mesa, of the Mayo Clinic Cancer Center in Arizona, is the chair of the MPN guideline committee.
This initial version of the guideline focuses on the workup and diagnosis of primary myelofibrosis (MF), post-polycythemia vera MF, and post-essential thrombocythemia MF, and treatment guidelines for MF.
The committee decided to first tackle the treatment guidelines in MF because, as Dr Mesa explained, MF is “the most severe of the MPNs with the most unmet needs in terms of guidance.”
Treatment guidelines for polycythemia vera (PV) and essential thrombocythemia (ET) will be forthcoming in 2017, he said, as well as diagnosis and treatment of atypical MPNs, such as hypereosinophilic syndrome and systemic mast cell disease.
Workup of an MPN
The guideline committee focused on information regarding diagnosis—the time and place to consider bone marrow biopsies, when to use cytogenetics, and when to perform next-generation sequencing.
They stressed the importance of quantifying disease burden and utilizing the now-validated symptom assessment tools, particularly in MF.
“Finally, we leveraged the many prognostic scoring systems that have been developed for these diseases, particularly IPSS for myelofibrosis at diagnosis or the DIPSS and DIPSS-plus at subsequent time points,” Dr Mesa said.
In addition to clinical-based prognostic scoring systems, information regarding molecular features and their impact is evolving, he said.
The guideline provides a table of mutations with prognostic significance. JAK2, MPL, or CALR mutations are “brighter mutations,” he said, while adverse prognostic markers include ASXL1, EZH2, IDH1/2, SRSF2, and TP53.
“All of these have some significant prognostic implications in primary myelofibrosis, specifically,” he said.
Assessing MPN burden
“When treating these patients, it’s important to be mindful of the overall burden of the disease,” Dr Mesa said.
He called this emphasis on disease burden “an evolution from the past, where therapy was either supportive or primarily focused on prevention of thrombosis with ET or PV.”
Practitioners need to be additionally mindful of the risk of vascular events, progression, the impact of cytopenias, splenomegaly, the burden of symptoms, and the baseline degree of comorbidities.
“[W]e encourage the use of validated symptom tools that have been used now in the majority of clinical trials in this setting,” Dr Mesa added.
The MPN-10 assessment tool, included in the guideline, evaluates 10 symptoms—early satiety, abdominal discomfort, inactivity, problems concentrating, numbness/tingling, night sweats, itching, bone pain, fever, and unintentional weight loss—on a scale of 0 to 10.
Patients with MF are the most symptomatic, Dr Mesa commented, although “it is notable how frequent symptoms are present in patients with PV and ET.”
Response criteria
For a complete response, individuals must have marked improvement to near normalization in both bone marrow and peripheral blood in addition to resolution of their disease symptoms.
Partial response is basically “just shy” of the complete response level, Dr Mesa said, with bone marrow resolution not being required.
The guideline also outlines response criteria for progressive, stable, and relapsed disease, clinical improvement, and anemia, spleen, and symptom response.
“But I’ll highlight that the majority of the responses that are received currently with medical therapy are in the area of clinical improvement,” Dr Mesa said.
Treatment guidance
Specific treatment guidelines for low-risk, intermediate-1 risk, intermediate-2- or high-risk MF from the new guideline have been described in an earlier article and will not be discussed here.
Of note, however, Dr Mesa explained that ruxolitinib is a very important part of the treatment guideline because it is the only therapy approved by the US Food and Drug Administration (FDA) to treat MF.
“Over time, it’s been shown that there is an improvement in survival [with ruxolitinib],” Dr Mesa said, perhaps because of a decrease with treatment in the morbidity and the debilitation of patients.
Investigators presented the 5-year update of this information at ASCO 2016 and reported that patients maintained reduction in splenomegaly up through 5 years, both in those randomized to ruxolitinib and those crossing over from placebo.
“Long-term, we clearly looked to see whether there was a signal of new onset or late onset toxicities,” Dr Mesa said, which largely was not the case. "Toxicities have been well described in earlier studies, primarily around anemia, thrombocytopenia, and mild constitutional symptoms.”
However, long-term therapy increases the rate of development of shingles and non-melanoma skin cancer. Rates of transformation to acute myeloid leukemia were consistent with those published for similar patient populations with MF.
“If I see a patient stable on ruxolitinib who has a marked drop in their counts later on in the course of their disease,” Dr Mesa added, “I’m certainly suspicious of progression.”
He also works them up for other causes of anemia if it evolves out of the blue.
Support in MF-related anemia
“With anemia, we’re mindful of iron stores, EPO level, and being certain there’s not the presence of hemolysis or other contributors,” Dr Mesa said.
The guideline recommends stratifying patients based on serum EPO levels—those with less than 500 mU/mL and those with 500 mU/mL and higher.
“If we lower the EPO level, the greater the likelihood of response,” Dr Mesa said. “In my experience, the lower the transfusion burden, the greater the likelihood of response.”
Other than erythropoiesis-stimulating agents for individuals with lower serum levels, androgens and immunomodulatory drugs for those with higher levels have some benefit.
But “they all have their limitations,” Dr Mesa said, and “they tend to range in benefit from 20% to 30%.”
The future
Dr Mesa discussed a few agents in the pipeline that “might impact these guidelines,” such as the JAK2/FLT3 inhibitor pacritinib and the JAK1/JAK2 inhibitor momelotinib.
Pacritinib had a positive phase 3 study, but the mortality rate was higher than expected, and it was put on an FDA hold.
Data from a second phase 3 study (PERSIST-1) will be reviewed in the aggregate to evaluate the benefit of pacritinib and whether the mortality rate was associated with drug-related side effects or adverse patient selection, “which we suspect might be the case,” Dr Mesa said.
“This agent may come off hold, depending upon the data of that second phase 3 study,” he added.
Momelotinib is also in an advanced phase 3 program with 2 trials underway. Both trials have completed accrual.
One is an upfront study of momelotinib versus ruxolitinib (NCT01969838). The goal is to reduce anemia without inferiority of splenomegaly and MPN symptoms.
The other phase 3 momelotinib trial is a second-line study versus best alternative therapy, including ruxoltinib (NCT02101268).
Combination studies are ongoing with a ruxolitinib base and a variety of secondary agents, including danazol, pomalidomide, PEG IFN α2a, 5-AZA, panobinostat, BKM-120, and LDE-225. All agents appear to achieve improvement in splenomegaly and symptoms.
But “incremental benefit over ruxolitinib alone is not yet clear,” Dr Mesa said. “I would say there’s not yet a recommended off-label combination which is widely being used.”
Dr Mesa also highlighted PRM-151, an antifibrosing drug that had a favorable early stage study with several doses, and the telomerase inhibitor imetelstat, which had a deep set of molecular responses in about a third of patients with MF. Imetelstat is currently being evaluated in the second-line setting (NCT02426086).
Regarding the possible positioning of new therapies, Dr Mesa believes “momelotinib and pacritinib may play a role in front-line, depending on the final data from those studies.”
“In second-line for MF—this is where most of the activity is in the trials,” he said. “Momelotinib, pacritinib, PRM-151, and imetelstat have possibilities.”
© ASCO/Zach Boyden-Holmes
NEW YORK—The 11th NCCN Congress: Hematologic Malignancies coincided with the release of the inaugural edition of the NCCN treatment guideline on myeloproliferative neoplasms (MPNs), and Ruben A. Mesa, MD, took the opportunity to discuss the framework of the document and the evolving management of MPNs.
Dr Mesa, of the Mayo Clinic Cancer Center in Arizona, is the chair of the MPN guideline committee.
This initial version of the guideline focuses on the workup and diagnosis of primary myelofibrosis (MF), post-polycythemia vera MF, and post-essential thrombocythemia MF, and treatment guidelines for MF.
The committee decided to first tackle the treatment guidelines in MF because, as Dr Mesa explained, MF is “the most severe of the MPNs with the most unmet needs in terms of guidance.”
Treatment guidelines for polycythemia vera (PV) and essential thrombocythemia (ET) will be forthcoming in 2017, he said, as well as diagnosis and treatment of atypical MPNs, such as hypereosinophilic syndrome and systemic mast cell disease.
Workup of an MPN
The guideline committee focused on information regarding diagnosis—the time and place to consider bone marrow biopsies, when to use cytogenetics, and when to perform next-generation sequencing.
They stressed the importance of quantifying disease burden and utilizing the now-validated symptom assessment tools, particularly in MF.
“Finally, we leveraged the many prognostic scoring systems that have been developed for these diseases, particularly IPSS for myelofibrosis at diagnosis or the DIPSS and DIPSS-plus at subsequent time points,” Dr Mesa said.
In addition to clinical-based prognostic scoring systems, information regarding molecular features and their impact is evolving, he said.
The guideline provides a table of mutations with prognostic significance. JAK2, MPL, or CALR mutations are “brighter mutations,” he said, while adverse prognostic markers include ASXL1, EZH2, IDH1/2, SRSF2, and TP53.
“All of these have some significant prognostic implications in primary myelofibrosis, specifically,” he said.
Assessing MPN burden
“When treating these patients, it’s important to be mindful of the overall burden of the disease,” Dr Mesa said.
He called this emphasis on disease burden “an evolution from the past, where therapy was either supportive or primarily focused on prevention of thrombosis with ET or PV.”
Practitioners need to be additionally mindful of the risk of vascular events, progression, the impact of cytopenias, splenomegaly, the burden of symptoms, and the baseline degree of comorbidities.
“[W]e encourage the use of validated symptom tools that have been used now in the majority of clinical trials in this setting,” Dr Mesa added.
The MPN-10 assessment tool, included in the guideline, evaluates 10 symptoms—early satiety, abdominal discomfort, inactivity, problems concentrating, numbness/tingling, night sweats, itching, bone pain, fever, and unintentional weight loss—on a scale of 0 to 10.
Patients with MF are the most symptomatic, Dr Mesa commented, although “it is notable how frequent symptoms are present in patients with PV and ET.”
Response criteria
For a complete response, individuals must have marked improvement to near normalization in both bone marrow and peripheral blood in addition to resolution of their disease symptoms.
Partial response is basically “just shy” of the complete response level, Dr Mesa said, with bone marrow resolution not being required.
The guideline also outlines response criteria for progressive, stable, and relapsed disease, clinical improvement, and anemia, spleen, and symptom response.
“But I’ll highlight that the majority of the responses that are received currently with medical therapy are in the area of clinical improvement,” Dr Mesa said.
Treatment guidance
Specific treatment guidelines for low-risk, intermediate-1 risk, intermediate-2- or high-risk MF from the new guideline have been described in an earlier article and will not be discussed here.
Of note, however, Dr Mesa explained that ruxolitinib is a very important part of the treatment guideline because it is the only therapy approved by the US Food and Drug Administration (FDA) to treat MF.
“Over time, it’s been shown that there is an improvement in survival [with ruxolitinib],” Dr Mesa said, perhaps because of a decrease with treatment in the morbidity and the debilitation of patients.
Investigators presented the 5-year update of this information at ASCO 2016 and reported that patients maintained reduction in splenomegaly up through 5 years, both in those randomized to ruxolitinib and those crossing over from placebo.
“Long-term, we clearly looked to see whether there was a signal of new onset or late onset toxicities,” Dr Mesa said, which largely was not the case. "Toxicities have been well described in earlier studies, primarily around anemia, thrombocytopenia, and mild constitutional symptoms.”
However, long-term therapy increases the rate of development of shingles and non-melanoma skin cancer. Rates of transformation to acute myeloid leukemia were consistent with those published for similar patient populations with MF.
“If I see a patient stable on ruxolitinib who has a marked drop in their counts later on in the course of their disease,” Dr Mesa added, “I’m certainly suspicious of progression.”
He also works them up for other causes of anemia if it evolves out of the blue.
Support in MF-related anemia
“With anemia, we’re mindful of iron stores, EPO level, and being certain there’s not the presence of hemolysis or other contributors,” Dr Mesa said.
The guideline recommends stratifying patients based on serum EPO levels—those with less than 500 mU/mL and those with 500 mU/mL and higher.
“If we lower the EPO level, the greater the likelihood of response,” Dr Mesa said. “In my experience, the lower the transfusion burden, the greater the likelihood of response.”
Other than erythropoiesis-stimulating agents for individuals with lower serum levels, androgens and immunomodulatory drugs for those with higher levels have some benefit.
But “they all have their limitations,” Dr Mesa said, and “they tend to range in benefit from 20% to 30%.”
The future
Dr Mesa discussed a few agents in the pipeline that “might impact these guidelines,” such as the JAK2/FLT3 inhibitor pacritinib and the JAK1/JAK2 inhibitor momelotinib.
Pacritinib had a positive phase 3 study, but the mortality rate was higher than expected, and it was put on an FDA hold.
Data from a second phase 3 study (PERSIST-1) will be reviewed in the aggregate to evaluate the benefit of pacritinib and whether the mortality rate was associated with drug-related side effects or adverse patient selection, “which we suspect might be the case,” Dr Mesa said.
“This agent may come off hold, depending upon the data of that second phase 3 study,” he added.
Momelotinib is also in an advanced phase 3 program with 2 trials underway. Both trials have completed accrual.
One is an upfront study of momelotinib versus ruxolitinib (NCT01969838). The goal is to reduce anemia without inferiority of splenomegaly and MPN symptoms.
The other phase 3 momelotinib trial is a second-line study versus best alternative therapy, including ruxoltinib (NCT02101268).
Combination studies are ongoing with a ruxolitinib base and a variety of secondary agents, including danazol, pomalidomide, PEG IFN α2a, 5-AZA, panobinostat, BKM-120, and LDE-225. All agents appear to achieve improvement in splenomegaly and symptoms.
But “incremental benefit over ruxolitinib alone is not yet clear,” Dr Mesa said. “I would say there’s not yet a recommended off-label combination which is widely being used.”
Dr Mesa also highlighted PRM-151, an antifibrosing drug that had a favorable early stage study with several doses, and the telomerase inhibitor imetelstat, which had a deep set of molecular responses in about a third of patients with MF. Imetelstat is currently being evaluated in the second-line setting (NCT02426086).
Regarding the possible positioning of new therapies, Dr Mesa believes “momelotinib and pacritinib may play a role in front-line, depending on the final data from those studies.”
“In second-line for MF—this is where most of the activity is in the trials,” he said. “Momelotinib, pacritinib, PRM-151, and imetelstat have possibilities.”
© ASCO/Zach Boyden-Holmes
NEW YORK—The 11th NCCN Congress: Hematologic Malignancies coincided with the release of the inaugural edition of the NCCN treatment guideline on myeloproliferative neoplasms (MPNs), and Ruben A. Mesa, MD, took the opportunity to discuss the framework of the document and the evolving management of MPNs.
Dr Mesa, of the Mayo Clinic Cancer Center in Arizona, is the chair of the MPN guideline committee.
This initial version of the guideline focuses on the workup and diagnosis of primary myelofibrosis (MF), post-polycythemia vera MF, and post-essential thrombocythemia MF, and treatment guidelines for MF.
The committee decided to first tackle the treatment guidelines in MF because, as Dr Mesa explained, MF is “the most severe of the MPNs with the most unmet needs in terms of guidance.”
Treatment guidelines for polycythemia vera (PV) and essential thrombocythemia (ET) will be forthcoming in 2017, he said, as well as diagnosis and treatment of atypical MPNs, such as hypereosinophilic syndrome and systemic mast cell disease.
Workup of an MPN
The guideline committee focused on information regarding diagnosis—the time and place to consider bone marrow biopsies, when to use cytogenetics, and when to perform next-generation sequencing.
They stressed the importance of quantifying disease burden and utilizing the now-validated symptom assessment tools, particularly in MF.
“Finally, we leveraged the many prognostic scoring systems that have been developed for these diseases, particularly IPSS for myelofibrosis at diagnosis or the DIPSS and DIPSS-plus at subsequent time points,” Dr Mesa said.
In addition to clinical-based prognostic scoring systems, information regarding molecular features and their impact is evolving, he said.
The guideline provides a table of mutations with prognostic significance. JAK2, MPL, or CALR mutations are “brighter mutations,” he said, while adverse prognostic markers include ASXL1, EZH2, IDH1/2, SRSF2, and TP53.
“All of these have some significant prognostic implications in primary myelofibrosis, specifically,” he said.
Assessing MPN burden
“When treating these patients, it’s important to be mindful of the overall burden of the disease,” Dr Mesa said.
He called this emphasis on disease burden “an evolution from the past, where therapy was either supportive or primarily focused on prevention of thrombosis with ET or PV.”
Practitioners need to be additionally mindful of the risk of vascular events, progression, the impact of cytopenias, splenomegaly, the burden of symptoms, and the baseline degree of comorbidities.
“[W]e encourage the use of validated symptom tools that have been used now in the majority of clinical trials in this setting,” Dr Mesa added.
The MPN-10 assessment tool, included in the guideline, evaluates 10 symptoms—early satiety, abdominal discomfort, inactivity, problems concentrating, numbness/tingling, night sweats, itching, bone pain, fever, and unintentional weight loss—on a scale of 0 to 10.
Patients with MF are the most symptomatic, Dr Mesa commented, although “it is notable how frequent symptoms are present in patients with PV and ET.”
Response criteria
For a complete response, individuals must have marked improvement to near normalization in both bone marrow and peripheral blood in addition to resolution of their disease symptoms.
Partial response is basically “just shy” of the complete response level, Dr Mesa said, with bone marrow resolution not being required.
The guideline also outlines response criteria for progressive, stable, and relapsed disease, clinical improvement, and anemia, spleen, and symptom response.
“But I’ll highlight that the majority of the responses that are received currently with medical therapy are in the area of clinical improvement,” Dr Mesa said.
Treatment guidance
Specific treatment guidelines for low-risk, intermediate-1 risk, intermediate-2- or high-risk MF from the new guideline have been described in an earlier article and will not be discussed here.
Of note, however, Dr Mesa explained that ruxolitinib is a very important part of the treatment guideline because it is the only therapy approved by the US Food and Drug Administration (FDA) to treat MF.
“Over time, it’s been shown that there is an improvement in survival [with ruxolitinib],” Dr Mesa said, perhaps because of a decrease with treatment in the morbidity and the debilitation of patients.
Investigators presented the 5-year update of this information at ASCO 2016 and reported that patients maintained reduction in splenomegaly up through 5 years, both in those randomized to ruxolitinib and those crossing over from placebo.
“Long-term, we clearly looked to see whether there was a signal of new onset or late onset toxicities,” Dr Mesa said, which largely was not the case. "Toxicities have been well described in earlier studies, primarily around anemia, thrombocytopenia, and mild constitutional symptoms.”
However, long-term therapy increases the rate of development of shingles and non-melanoma skin cancer. Rates of transformation to acute myeloid leukemia were consistent with those published for similar patient populations with MF.
“If I see a patient stable on ruxolitinib who has a marked drop in their counts later on in the course of their disease,” Dr Mesa added, “I’m certainly suspicious of progression.”
He also works them up for other causes of anemia if it evolves out of the blue.
Support in MF-related anemia
“With anemia, we’re mindful of iron stores, EPO level, and being certain there’s not the presence of hemolysis or other contributors,” Dr Mesa said.
The guideline recommends stratifying patients based on serum EPO levels—those with less than 500 mU/mL and those with 500 mU/mL and higher.
“If we lower the EPO level, the greater the likelihood of response,” Dr Mesa said. “In my experience, the lower the transfusion burden, the greater the likelihood of response.”
Other than erythropoiesis-stimulating agents for individuals with lower serum levels, androgens and immunomodulatory drugs for those with higher levels have some benefit.
But “they all have their limitations,” Dr Mesa said, and “they tend to range in benefit from 20% to 30%.”
The future
Dr Mesa discussed a few agents in the pipeline that “might impact these guidelines,” such as the JAK2/FLT3 inhibitor pacritinib and the JAK1/JAK2 inhibitor momelotinib.
Pacritinib had a positive phase 3 study, but the mortality rate was higher than expected, and it was put on an FDA hold.
Data from a second phase 3 study (PERSIST-1) will be reviewed in the aggregate to evaluate the benefit of pacritinib and whether the mortality rate was associated with drug-related side effects or adverse patient selection, “which we suspect might be the case,” Dr Mesa said.
“This agent may come off hold, depending upon the data of that second phase 3 study,” he added.
Momelotinib is also in an advanced phase 3 program with 2 trials underway. Both trials have completed accrual.
One is an upfront study of momelotinib versus ruxolitinib (NCT01969838). The goal is to reduce anemia without inferiority of splenomegaly and MPN symptoms.
The other phase 3 momelotinib trial is a second-line study versus best alternative therapy, including ruxoltinib (NCT02101268).
Combination studies are ongoing with a ruxolitinib base and a variety of secondary agents, including danazol, pomalidomide, PEG IFN α2a, 5-AZA, panobinostat, BKM-120, and LDE-225. All agents appear to achieve improvement in splenomegaly and symptoms.
But “incremental benefit over ruxolitinib alone is not yet clear,” Dr Mesa said. “I would say there’s not yet a recommended off-label combination which is widely being used.”
Dr Mesa also highlighted PRM-151, an antifibrosing drug that had a favorable early stage study with several doses, and the telomerase inhibitor imetelstat, which had a deep set of molecular responses in about a third of patients with MF. Imetelstat is currently being evaluated in the second-line setting (NCT02426086).
Regarding the possible positioning of new therapies, Dr Mesa believes “momelotinib and pacritinib may play a role in front-line, depending on the final data from those studies.”
“In second-line for MF—this is where most of the activity is in the trials,” he said. “Momelotinib, pacritinib, PRM-151, and imetelstat have possibilities.”
Supportive care isn’t palliative care, speaker says

Photo courtesy of NCI
NEW YORK—Two presentations at the NCCN 11th Annual Congress: Hematologic Malignancies addressed the importance of supportive care in the treatment of patients with T-cell lymphomas and multiple myeloma.
Erin Kopp, ACNP-BC, of City of Hope Comprehensive Cancer Center in Duarte, California, reminded the audience that supportive care is not palliative care.
Supportive care “complements critical care so that the patient doesn’t have to stop treatment,” she said.
Kopp focused primarily on cutaneous T-cell lymphoma (CTCL) in her presentation, with some recommendations for managing tumor lysis syndrome in patients undergoing therapy for peripheral T-cell lymphoma (PTCL).
And Kathleen Colson, RN, of the Dana-Farber Cancer Institute in Boston, Massachusetts, discussed supportive care for patients with multiple myeloma (MM).
T-cell lymphomas
Most T-cell lymphoma patients will require multiple treatment regimens over their lifetimes, Kopp said. And each type of therapy brings different treatment-related toxicities, which in turn require distinct supportive care measures to manage them.
Topical steroids, for example, may cause skin-thinning, stretch marks, skin irritation, and may be absorbed systemically when a high-potency formulation is used. So the lowest potency steroid that provides the maximum efficacy should be utilized. Practitioners should assess systemic effects if high-potency steroids are utilized.
Topical nitrogen mustard can darken the skin, which often occurs as the lesions resolve, Kopp said. She cautioned that patients experiencing hyperpigmentation often stop treatment without telling their physicians.
So Kopp recommends appropriate patient education to go along with the treatment. With nitrogen mustard, this includes applying a thin layer only to the affected areas and refrigerating the topical ointment to increase soothing.
Topical retinoids may cause redness, itching, warmth, swelling, burning, scaling or other irritation. They also increase the patients’ sensitivity to light. Kopp indicated that for the first week, topical retinoids should be applied once every other day and then titrated as tolerated.
Phototherapy with PUVA or narrowband-UVB may also cause itching, in addition to skin burn, nausea, and other side effects.
“Do not underestimate emollients,” Kopp said, for relief of pruritus. And skin baths with bleach significantly decrease infections that may result from treatment.
Systemic therapy with retinoids, interferon, cytotoxic agents, monoclonal antibodies, and HDAC inhibitors may also cause distinct reactions. For example, the retinoid bexarotene may cause primary hypothyroidism and major lipid abnormalities. Therefore, TSH, free T4, and triglycerides should be monitored every 8 weeks.
Cytotoxic agents such as pralatrexate and methotrexate significantly increase the risk for infection.
Monoclonal antibodies can reactivate previous viral infection, induce tumor lysis syndrome (TLS), and cause progressive multifocal leukoencephalopathy.
HDAC inhibitors such as vorinostat and romidepsin may cause QT prolongation and myelosuppression, among other side effects.
Practitioners need to assess symptoms and side effects thoroughly and often and provide options for supportive care management.
PTCL is an under recognized risk for TLS, Kopp said.
“It should be addressed aggressively,” she added, with monitoring and correction of electrolyte imbalance.
Patients should be rigorously hydrated, and allopurinol should be administered 2-3 days prior to treatment and adjusted based on the patient response and uric acid level.
Multiple myeloma
Colson described supportive care as “keeping all the pieces together.” MM itself can result in a broad spectrum of clinical manifestations, including renal compromise, neuropathy, infection, hypercalcemia, bone pain, lytic lesions, and anemia.
To preserve renal health, patients should drink plenty of water and avoid certain medications, such as IV contrast and nonsteroidal anti-inflammatory drugs.
Peripheral neuropathy can be a side effect of treatment or be caused by the disease itself. Bortezomib-related neuropathy can be reduced with weekly instead of twice weekly dosing and with subcutaneous administration.
Duration of higher doses of thalidomide treatment also impacts neuropathy. Carfilzomib and pomalidomide have a lower incidence of neuropathy.
Myeloma patients have a 15-fold increased risk of recurrent infection because white blood cell production is decreased and the normal immune role of plasma cells is lost.
Supportive therapy includes antibiotics and IVIG therapy. In addition, Colson said pneumonia and influenza vaccines should be considered, as well as prophylaxis for Pneumocystis carinii, herpes zoster, and fungal infections.
Hypercalcemia results from increased bone deterioration. Symptoms include loss of appetite, fatigue, vomiting, muscle weakness, confusion, constipation, increased thirst, and increased urine output. Supportive measures are adequate hydration, furosemide, bisphosphonates, and steroids.
Supportive therapy for bone pain includes bisphosphonates, radiation, pain medication, kyphoplasty, and vertebroplasty. Bisphosphonates, such as pamidronate and zoledronic acid, inhibit bone destruction and are recommended for all myeloma patients with bone disease. However, patients should be monitored for renal dysfunction and osteonecrosis of the jaw when taking bisphosphonates.
And Colson advises, “Hold bisphosphonate therapy if the patient needs a root canal or extraction.” Additionally, dental implants are not recommended for MM patients.
Anemia is another common presenting symptom of myeloma and may also be a result of decreased kidney function. Colson said the use of red blood cell supplements may be used with caution to ameliorate the symptom. Red blood cell transfusion may be considered and a reduction in the medication dose may be required.
MM is a hypercoagulable disease, and measures should be taken to avoid deep vein thrombosis (DVT) and pulmonary embolism (PE). Patients should wear anti-embolism stockings, exercise regularly, take low-dose aspirin, and move about frequently instead of sitting for long periods. Immunomodulatory medications may be adjusted to reduce the risk of a blot clot forming.
Infusion-related reactions are also a risk of therapy, and symptoms of a reaction need to be managed immediately and appropriately, with antihistamines, corticosteroids, interruption of the infusion, slowing of the infusion rate after symptom resolution, and permanent discontinuation in the case of grade 4 reactions.
The potential for longer survival exists, Colson said, due to appropriate supportive care measures.
Photo courtesy of NCI
NEW YORK—Two presentations at the NCCN 11th Annual Congress: Hematologic Malignancies addressed the importance of supportive care in the treatment of patients with T-cell lymphomas and multiple myeloma.
Erin Kopp, ACNP-BC, of City of Hope Comprehensive Cancer Center in Duarte, California, reminded the audience that supportive care is not palliative care.
Supportive care “complements critical care so that the patient doesn’t have to stop treatment,” she said.
Kopp focused primarily on cutaneous T-cell lymphoma (CTCL) in her presentation, with some recommendations for managing tumor lysis syndrome in patients undergoing therapy for peripheral T-cell lymphoma (PTCL).
And Kathleen Colson, RN, of the Dana-Farber Cancer Institute in Boston, Massachusetts, discussed supportive care for patients with multiple myeloma (MM).
T-cell lymphomas
Most T-cell lymphoma patients will require multiple treatment regimens over their lifetimes, Kopp said. And each type of therapy brings different treatment-related toxicities, which in turn require distinct supportive care measures to manage them.
Topical steroids, for example, may cause skin-thinning, stretch marks, skin irritation, and may be absorbed systemically when a high-potency formulation is used. So the lowest potency steroid that provides the maximum efficacy should be utilized. Practitioners should assess systemic effects if high-potency steroids are utilized.
Topical nitrogen mustard can darken the skin, which often occurs as the lesions resolve, Kopp said. She cautioned that patients experiencing hyperpigmentation often stop treatment without telling their physicians.
So Kopp recommends appropriate patient education to go along with the treatment. With nitrogen mustard, this includes applying a thin layer only to the affected areas and refrigerating the topical ointment to increase soothing.
Topical retinoids may cause redness, itching, warmth, swelling, burning, scaling or other irritation. They also increase the patients’ sensitivity to light. Kopp indicated that for the first week, topical retinoids should be applied once every other day and then titrated as tolerated.
Phototherapy with PUVA or narrowband-UVB may also cause itching, in addition to skin burn, nausea, and other side effects.
“Do not underestimate emollients,” Kopp said, for relief of pruritus. And skin baths with bleach significantly decrease infections that may result from treatment.
Systemic therapy with retinoids, interferon, cytotoxic agents, monoclonal antibodies, and HDAC inhibitors may also cause distinct reactions. For example, the retinoid bexarotene may cause primary hypothyroidism and major lipid abnormalities. Therefore, TSH, free T4, and triglycerides should be monitored every 8 weeks.
Cytotoxic agents such as pralatrexate and methotrexate significantly increase the risk for infection.
Monoclonal antibodies can reactivate previous viral infection, induce tumor lysis syndrome (TLS), and cause progressive multifocal leukoencephalopathy.
HDAC inhibitors such as vorinostat and romidepsin may cause QT prolongation and myelosuppression, among other side effects.
Practitioners need to assess symptoms and side effects thoroughly and often and provide options for supportive care management.
PTCL is an under recognized risk for TLS, Kopp said.
“It should be addressed aggressively,” she added, with monitoring and correction of electrolyte imbalance.
Patients should be rigorously hydrated, and allopurinol should be administered 2-3 days prior to treatment and adjusted based on the patient response and uric acid level.
Multiple myeloma
Colson described supportive care as “keeping all the pieces together.” MM itself can result in a broad spectrum of clinical manifestations, including renal compromise, neuropathy, infection, hypercalcemia, bone pain, lytic lesions, and anemia.
To preserve renal health, patients should drink plenty of water and avoid certain medications, such as IV contrast and nonsteroidal anti-inflammatory drugs.
Peripheral neuropathy can be a side effect of treatment or be caused by the disease itself. Bortezomib-related neuropathy can be reduced with weekly instead of twice weekly dosing and with subcutaneous administration.
Duration of higher doses of thalidomide treatment also impacts neuropathy. Carfilzomib and pomalidomide have a lower incidence of neuropathy.
Myeloma patients have a 15-fold increased risk of recurrent infection because white blood cell production is decreased and the normal immune role of plasma cells is lost.
Supportive therapy includes antibiotics and IVIG therapy. In addition, Colson said pneumonia and influenza vaccines should be considered, as well as prophylaxis for Pneumocystis carinii, herpes zoster, and fungal infections.
Hypercalcemia results from increased bone deterioration. Symptoms include loss of appetite, fatigue, vomiting, muscle weakness, confusion, constipation, increased thirst, and increased urine output. Supportive measures are adequate hydration, furosemide, bisphosphonates, and steroids.
Supportive therapy for bone pain includes bisphosphonates, radiation, pain medication, kyphoplasty, and vertebroplasty. Bisphosphonates, such as pamidronate and zoledronic acid, inhibit bone destruction and are recommended for all myeloma patients with bone disease. However, patients should be monitored for renal dysfunction and osteonecrosis of the jaw when taking bisphosphonates.
And Colson advises, “Hold bisphosphonate therapy if the patient needs a root canal or extraction.” Additionally, dental implants are not recommended for MM patients.
Anemia is another common presenting symptom of myeloma and may also be a result of decreased kidney function. Colson said the use of red blood cell supplements may be used with caution to ameliorate the symptom. Red blood cell transfusion may be considered and a reduction in the medication dose may be required.
MM is a hypercoagulable disease, and measures should be taken to avoid deep vein thrombosis (DVT) and pulmonary embolism (PE). Patients should wear anti-embolism stockings, exercise regularly, take low-dose aspirin, and move about frequently instead of sitting for long periods. Immunomodulatory medications may be adjusted to reduce the risk of a blot clot forming.
Infusion-related reactions are also a risk of therapy, and symptoms of a reaction need to be managed immediately and appropriately, with antihistamines, corticosteroids, interruption of the infusion, slowing of the infusion rate after symptom resolution, and permanent discontinuation in the case of grade 4 reactions.
The potential for longer survival exists, Colson said, due to appropriate supportive care measures.
Photo courtesy of NCI
NEW YORK—Two presentations at the NCCN 11th Annual Congress: Hematologic Malignancies addressed the importance of supportive care in the treatment of patients with T-cell lymphomas and multiple myeloma.
Erin Kopp, ACNP-BC, of City of Hope Comprehensive Cancer Center in Duarte, California, reminded the audience that supportive care is not palliative care.
Supportive care “complements critical care so that the patient doesn’t have to stop treatment,” she said.
Kopp focused primarily on cutaneous T-cell lymphoma (CTCL) in her presentation, with some recommendations for managing tumor lysis syndrome in patients undergoing therapy for peripheral T-cell lymphoma (PTCL).
And Kathleen Colson, RN, of the Dana-Farber Cancer Institute in Boston, Massachusetts, discussed supportive care for patients with multiple myeloma (MM).
T-cell lymphomas
Most T-cell lymphoma patients will require multiple treatment regimens over their lifetimes, Kopp said. And each type of therapy brings different treatment-related toxicities, which in turn require distinct supportive care measures to manage them.
Topical steroids, for example, may cause skin-thinning, stretch marks, skin irritation, and may be absorbed systemically when a high-potency formulation is used. So the lowest potency steroid that provides the maximum efficacy should be utilized. Practitioners should assess systemic effects if high-potency steroids are utilized.
Topical nitrogen mustard can darken the skin, which often occurs as the lesions resolve, Kopp said. She cautioned that patients experiencing hyperpigmentation often stop treatment without telling their physicians.
So Kopp recommends appropriate patient education to go along with the treatment. With nitrogen mustard, this includes applying a thin layer only to the affected areas and refrigerating the topical ointment to increase soothing.
Topical retinoids may cause redness, itching, warmth, swelling, burning, scaling or other irritation. They also increase the patients’ sensitivity to light. Kopp indicated that for the first week, topical retinoids should be applied once every other day and then titrated as tolerated.
Phototherapy with PUVA or narrowband-UVB may also cause itching, in addition to skin burn, nausea, and other side effects.
“Do not underestimate emollients,” Kopp said, for relief of pruritus. And skin baths with bleach significantly decrease infections that may result from treatment.
Systemic therapy with retinoids, interferon, cytotoxic agents, monoclonal antibodies, and HDAC inhibitors may also cause distinct reactions. For example, the retinoid bexarotene may cause primary hypothyroidism and major lipid abnormalities. Therefore, TSH, free T4, and triglycerides should be monitored every 8 weeks.
Cytotoxic agents such as pralatrexate and methotrexate significantly increase the risk for infection.
Monoclonal antibodies can reactivate previous viral infection, induce tumor lysis syndrome (TLS), and cause progressive multifocal leukoencephalopathy.
HDAC inhibitors such as vorinostat and romidepsin may cause QT prolongation and myelosuppression, among other side effects.
Practitioners need to assess symptoms and side effects thoroughly and often and provide options for supportive care management.
PTCL is an under recognized risk for TLS, Kopp said.
“It should be addressed aggressively,” she added, with monitoring and correction of electrolyte imbalance.
Patients should be rigorously hydrated, and allopurinol should be administered 2-3 days prior to treatment and adjusted based on the patient response and uric acid level.
Multiple myeloma
Colson described supportive care as “keeping all the pieces together.” MM itself can result in a broad spectrum of clinical manifestations, including renal compromise, neuropathy, infection, hypercalcemia, bone pain, lytic lesions, and anemia.
To preserve renal health, patients should drink plenty of water and avoid certain medications, such as IV contrast and nonsteroidal anti-inflammatory drugs.
Peripheral neuropathy can be a side effect of treatment or be caused by the disease itself. Bortezomib-related neuropathy can be reduced with weekly instead of twice weekly dosing and with subcutaneous administration.
Duration of higher doses of thalidomide treatment also impacts neuropathy. Carfilzomib and pomalidomide have a lower incidence of neuropathy.
Myeloma patients have a 15-fold increased risk of recurrent infection because white blood cell production is decreased and the normal immune role of plasma cells is lost.
Supportive therapy includes antibiotics and IVIG therapy. In addition, Colson said pneumonia and influenza vaccines should be considered, as well as prophylaxis for Pneumocystis carinii, herpes zoster, and fungal infections.
Hypercalcemia results from increased bone deterioration. Symptoms include loss of appetite, fatigue, vomiting, muscle weakness, confusion, constipation, increased thirst, and increased urine output. Supportive measures are adequate hydration, furosemide, bisphosphonates, and steroids.
Supportive therapy for bone pain includes bisphosphonates, radiation, pain medication, kyphoplasty, and vertebroplasty. Bisphosphonates, such as pamidronate and zoledronic acid, inhibit bone destruction and are recommended for all myeloma patients with bone disease. However, patients should be monitored for renal dysfunction and osteonecrosis of the jaw when taking bisphosphonates.
And Colson advises, “Hold bisphosphonate therapy if the patient needs a root canal or extraction.” Additionally, dental implants are not recommended for MM patients.
Anemia is another common presenting symptom of myeloma and may also be a result of decreased kidney function. Colson said the use of red blood cell supplements may be used with caution to ameliorate the symptom. Red blood cell transfusion may be considered and a reduction in the medication dose may be required.
MM is a hypercoagulable disease, and measures should be taken to avoid deep vein thrombosis (DVT) and pulmonary embolism (PE). Patients should wear anti-embolism stockings, exercise regularly, take low-dose aspirin, and move about frequently instead of sitting for long periods. Immunomodulatory medications may be adjusted to reduce the risk of a blot clot forming.
Infusion-related reactions are also a risk of therapy, and symptoms of a reaction need to be managed immediately and appropriately, with antihistamines, corticosteroids, interruption of the infusion, slowing of the infusion rate after symptom resolution, and permanent discontinuation in the case of grade 4 reactions.
The potential for longer survival exists, Colson said, due to appropriate supportive care measures.
Speaker outlines importance of cell of origin in DLBCL

NEW YORK—The importance of cell of origin in choosing a treatment for diffuse large B-cell lymphoma (DLBCL) is a topic “that has been kicking around for 16 years,” according to a speaker at the NCCN 11th Annual Congress: Hematologic Malignancies.
Cell of origin was first described in the year 2000 as a distinguishing factor in large-cell lymphoma, said the speaker, Andrew Zelenetz, MD, PhD, of Memorial Sloan Kettering Cancer Center in New York, New York.
The cell of origin in DLBCL—whether it’s germinal center B cell (GCB), activated B cell (ABC), or unclassified—contributes to biological and clinical heterogeneity of the disease.
“And more importantly, activated B-cell diffuse large B-cell lymphoma and germinal center diffuse large B-cell lymphoma are simply different diseases,” Dr Zelenetz said.
He then elaborated on the importance of cell of origin in treating DLBCL.
Biology
Dr Zelenetz noted that ABC and GCB lymphomas have different molecular pathways. ABC lymphomas are very dependent on the NF-kB pathway and have more active signaling through the B-cell receptor.
The GCB lymphomas tend to have more tonic regulation, and the PI3 kinase/mTOR pathway is more critical. GCB lymphomas have more genomic instability.
“So cell of origin determination identifies tumors with distinct biology, may provide prognostic information, and may be predictive for treatment selection,” Dr Zelenetz said. “Unfortunately, cell of origin is not the whole story.”
Gene mutations occur in large-cell lymphoma “just like every other cancer,” Dr Zelenetz said. And the vast majority occur in both lymphoma subtypes, he added, further complicating our understanding of the biology of these tumors.
Some of these mutations predict for sensitivity to treatment, while others predict for resistance. For example, CARD11 predicts for resistance to ibrutinib, while CD79b predicts for sensitivity.
Determining the cell of origin
Gene-expression profiling on fresh tissue is considered the gold standard, but “it is clearly not a clinical tool,” Dr Zelenetz said. It requires the Wright classifier, a statistical method based on Bayes’ rule, to make patient-level assignments to 1 of the 3 subgroups.
Immunohistochemistry is widely available, but reproducibility may be difficult. Many assays exist, such as the Hans, Choi, and Muris assays, but, in many studies, there may be a lack of correlation with gene-expression profiling.
In the last few years, gene-expression profiling of formalin‐fixed paraffin‐embedded (FFPE) tissue has emerged as a reliable method. The assay is reproducible between laboratories, and it’s reproducible between different sets of reagents.
“[T]here is tremendous correlation between the Lymph2Cx assay and the gold standard,” Dr Zelenetz added.
“So here we have a robust assay,” he said, which allows investigators to explore whether the cell of origin is prognostic in large-cell lymphoma.
Prognosis
In a data set of 339 patients with de novo DLBCL treated with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), the Lymph2Cx assay showing cell of origin was predictive of overall and progression-free survival.
However, the same exact assay applied to the RICOVER-60 data from the German High-Grade Non-Hodgkin Lymphoma Study group was not predictive, Dr Zelenetz reported, based on a personal communication from one of the investigators. There was a slight trend in favor of GCB tumors, but it was not statistically significant.
And the REMoDL-B study, using gene-expression profiling of FFPE tissue with the DASL assay, also didn’t show any difference in outcome between ABC or GCB tumors.
So gene-expression profiling of FFPE tissue does not universally show a prognostic difference, Dr Zelenetz said.
Influence of chemotherapy by cell of origin
CALGB 59910 showed that GCB tumors had a superior event-free, progression-free, and overall survival with dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) compared to ABC tumors.
“However, this is a phase 2, hypothesis-generating experiment,” Dr Zelenetz pointed out, and the results of the confirmatory study comparing dose-adjusted EPOCH-R and R-CHOP21 (CALGB 50303) will be presented later this year at the ASH Annual Meeting.
Sequential, non-cross-resistant chemotherapy
Data from the Memorial Sloan Kettering study (MSKCC 01-142/08-146; NCT00712582) of sequential therapy with R-CHOP followed by ICE (ifosfamide, carboplatin, and etoposide) demonstrate “excellent” progression-free and overall survival, Dr Zelenetz said.
“When we analyzed the outcome by cell of origin, there was a suggestion that the patients with the non-germinal center tumors were actually doing better than the germinal center tumors,” he added.
He pointed out one of the limitations of the study is that the cell of origin was determined by the Hans model. Nevertheless, the study raised another testable hypothesis: sequential therapy might overcome the adverse impact of the non-germinal center tumors.
Cell of origin analysis of the prospective, randomized study (LNH 03-2B) comparing R-ACVBP (rituximab, doxorubicin, cyclophosphamide, vindesine, bleomycin, and prednisone) to R-CHOP showed that whether patients with GCB tumors received CHOP or ACVBP didn’t make “a whit of difference,” Dr Zelenetz said, in terms of progression-free and overall survival.
However, patients with ABC tumors demonstrated an “enormous difference in favor of R-ACVBP,” he said.
“Again, evidence that you can overcome the adverse effect of the ABC tumors with chemotherapy.”
Dr Zelenetz pointed out that R-ACVBP and R-CHOP followed by ICE are “actually remarkably similar regimens.” Both are sequential, both include consolidation, and both incorporate high-dose ifosfamide and etoposide.
“[S]o they actually reinforce each other,” he said, “demonstrating a similar result.”
Lenalidomide
Lenalidomide in the relapsed/refractory setting has modest activity in DLBCL, with most of the benefit accruing to patients with non-germinal center tumors.
Two clinical studies evaluated the impact of adding lenalidomide to standard chemotherapy.
In an Italian series using lenalidomide (L) plus R-CHOP21 in elderly untreated patients, the combination produced outstanding progression-free and event-free survival, but with no significant differences between the subtypes.
A US study of RL-CHOP versus R-CHOP included 87 matched historical controls treated with R-CHOP and 64 patients treated with RL-CHOP. Patients with non-germinal center tumors treated with RL-CHOP fared much better than historical controls treated with R-CHOP.
However, among germinal center tumors, “there was not a hint of any difference,” Dr Zelenetz noted.
Two studies—E1412, using an unselected population, and the international ROBUST study, selecting for patients with ABC tumors—are underway to confirm that the benefit with lenalidomide is in patients with activated B-cell tumors.
Ibrutinib
Ibrutinib, a Bruton’s tyrosine kinase inhibitor, also has modest activity as a single agent in an unselected patient population with relapsed/refractory DLBCL. And most of the patients who demonstrated benefit had activated B-cell tumors.
Upon further analysis, investigators found that response was enhanced by the CD79b mutation, but it was not necessary for a response. And patients with CARD11 had no response.
MYD88 mutations seemed to cause resistance to ibrutinib, unless the mutation was associated with the CD79b mutation, and then patients had a “great” response, Dr Zelenetz explained.
In the upfront setting, a phase 1b study of R-CHOP plus ibrutinib demonstrated the safety of the combination, which had an overall survival rate of 100% and a complete response rate of 91%.
The prospective, randomized, phase 3 PHOENIX trial (NCT01855750) evaluating the combination in newly diagnosed non-germinal center DLBCL has completed accrual, but analysis is still pending.
Conclusion
“The prognostic significance of cell of origin is still controversial,” Dr Zelenetz wrapped up, “although I actually believe there is a prognostic difference in unselected registry patients.”
Sequential chemotherapy with ifosfamide and etoposide consolidation does very well in activated B-cell tumors, both in phase 2 and phase 3 studies.
“Importantly, small molecules seem to have differential effects totally predictable based on the biology of the difference between activated B-cell and germinal center tumors,” Dr Zelenetz said.
“But the big wild card here is somatic mutations further complicate things and will have to be incorporated into our understanding in the selection of patients.”
NEW YORK—The importance of cell of origin in choosing a treatment for diffuse large B-cell lymphoma (DLBCL) is a topic “that has been kicking around for 16 years,” according to a speaker at the NCCN 11th Annual Congress: Hematologic Malignancies.
Cell of origin was first described in the year 2000 as a distinguishing factor in large-cell lymphoma, said the speaker, Andrew Zelenetz, MD, PhD, of Memorial Sloan Kettering Cancer Center in New York, New York.
The cell of origin in DLBCL—whether it’s germinal center B cell (GCB), activated B cell (ABC), or unclassified—contributes to biological and clinical heterogeneity of the disease.
“And more importantly, activated B-cell diffuse large B-cell lymphoma and germinal center diffuse large B-cell lymphoma are simply different diseases,” Dr Zelenetz said.
He then elaborated on the importance of cell of origin in treating DLBCL.
Biology
Dr Zelenetz noted that ABC and GCB lymphomas have different molecular pathways. ABC lymphomas are very dependent on the NF-kB pathway and have more active signaling through the B-cell receptor.
The GCB lymphomas tend to have more tonic regulation, and the PI3 kinase/mTOR pathway is more critical. GCB lymphomas have more genomic instability.
“So cell of origin determination identifies tumors with distinct biology, may provide prognostic information, and may be predictive for treatment selection,” Dr Zelenetz said. “Unfortunately, cell of origin is not the whole story.”
Gene mutations occur in large-cell lymphoma “just like every other cancer,” Dr Zelenetz said. And the vast majority occur in both lymphoma subtypes, he added, further complicating our understanding of the biology of these tumors.
Some of these mutations predict for sensitivity to treatment, while others predict for resistance. For example, CARD11 predicts for resistance to ibrutinib, while CD79b predicts for sensitivity.
Determining the cell of origin
Gene-expression profiling on fresh tissue is considered the gold standard, but “it is clearly not a clinical tool,” Dr Zelenetz said. It requires the Wright classifier, a statistical method based on Bayes’ rule, to make patient-level assignments to 1 of the 3 subgroups.
Immunohistochemistry is widely available, but reproducibility may be difficult. Many assays exist, such as the Hans, Choi, and Muris assays, but, in many studies, there may be a lack of correlation with gene-expression profiling.
In the last few years, gene-expression profiling of formalin‐fixed paraffin‐embedded (FFPE) tissue has emerged as a reliable method. The assay is reproducible between laboratories, and it’s reproducible between different sets of reagents.
“[T]here is tremendous correlation between the Lymph2Cx assay and the gold standard,” Dr Zelenetz added.
“So here we have a robust assay,” he said, which allows investigators to explore whether the cell of origin is prognostic in large-cell lymphoma.
Prognosis
In a data set of 339 patients with de novo DLBCL treated with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), the Lymph2Cx assay showing cell of origin was predictive of overall and progression-free survival.
However, the same exact assay applied to the RICOVER-60 data from the German High-Grade Non-Hodgkin Lymphoma Study group was not predictive, Dr Zelenetz reported, based on a personal communication from one of the investigators. There was a slight trend in favor of GCB tumors, but it was not statistically significant.
And the REMoDL-B study, using gene-expression profiling of FFPE tissue with the DASL assay, also didn’t show any difference in outcome between ABC or GCB tumors.
So gene-expression profiling of FFPE tissue does not universally show a prognostic difference, Dr Zelenetz said.
Influence of chemotherapy by cell of origin
CALGB 59910 showed that GCB tumors had a superior event-free, progression-free, and overall survival with dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) compared to ABC tumors.
“However, this is a phase 2, hypothesis-generating experiment,” Dr Zelenetz pointed out, and the results of the confirmatory study comparing dose-adjusted EPOCH-R and R-CHOP21 (CALGB 50303) will be presented later this year at the ASH Annual Meeting.
Sequential, non-cross-resistant chemotherapy
Data from the Memorial Sloan Kettering study (MSKCC 01-142/08-146; NCT00712582) of sequential therapy with R-CHOP followed by ICE (ifosfamide, carboplatin, and etoposide) demonstrate “excellent” progression-free and overall survival, Dr Zelenetz said.
“When we analyzed the outcome by cell of origin, there was a suggestion that the patients with the non-germinal center tumors were actually doing better than the germinal center tumors,” he added.
He pointed out one of the limitations of the study is that the cell of origin was determined by the Hans model. Nevertheless, the study raised another testable hypothesis: sequential therapy might overcome the adverse impact of the non-germinal center tumors.
Cell of origin analysis of the prospective, randomized study (LNH 03-2B) comparing R-ACVBP (rituximab, doxorubicin, cyclophosphamide, vindesine, bleomycin, and prednisone) to R-CHOP showed that whether patients with GCB tumors received CHOP or ACVBP didn’t make “a whit of difference,” Dr Zelenetz said, in terms of progression-free and overall survival.
However, patients with ABC tumors demonstrated an “enormous difference in favor of R-ACVBP,” he said.
“Again, evidence that you can overcome the adverse effect of the ABC tumors with chemotherapy.”
Dr Zelenetz pointed out that R-ACVBP and R-CHOP followed by ICE are “actually remarkably similar regimens.” Both are sequential, both include consolidation, and both incorporate high-dose ifosfamide and etoposide.
“[S]o they actually reinforce each other,” he said, “demonstrating a similar result.”
Lenalidomide
Lenalidomide in the relapsed/refractory setting has modest activity in DLBCL, with most of the benefit accruing to patients with non-germinal center tumors.
Two clinical studies evaluated the impact of adding lenalidomide to standard chemotherapy.
In an Italian series using lenalidomide (L) plus R-CHOP21 in elderly untreated patients, the combination produced outstanding progression-free and event-free survival, but with no significant differences between the subtypes.
A US study of RL-CHOP versus R-CHOP included 87 matched historical controls treated with R-CHOP and 64 patients treated with RL-CHOP. Patients with non-germinal center tumors treated with RL-CHOP fared much better than historical controls treated with R-CHOP.
However, among germinal center tumors, “there was not a hint of any difference,” Dr Zelenetz noted.
Two studies—E1412, using an unselected population, and the international ROBUST study, selecting for patients with ABC tumors—are underway to confirm that the benefit with lenalidomide is in patients with activated B-cell tumors.
Ibrutinib
Ibrutinib, a Bruton’s tyrosine kinase inhibitor, also has modest activity as a single agent in an unselected patient population with relapsed/refractory DLBCL. And most of the patients who demonstrated benefit had activated B-cell tumors.
Upon further analysis, investigators found that response was enhanced by the CD79b mutation, but it was not necessary for a response. And patients with CARD11 had no response.
MYD88 mutations seemed to cause resistance to ibrutinib, unless the mutation was associated with the CD79b mutation, and then patients had a “great” response, Dr Zelenetz explained.
In the upfront setting, a phase 1b study of R-CHOP plus ibrutinib demonstrated the safety of the combination, which had an overall survival rate of 100% and a complete response rate of 91%.
The prospective, randomized, phase 3 PHOENIX trial (NCT01855750) evaluating the combination in newly diagnosed non-germinal center DLBCL has completed accrual, but analysis is still pending.
Conclusion
“The prognostic significance of cell of origin is still controversial,” Dr Zelenetz wrapped up, “although I actually believe there is a prognostic difference in unselected registry patients.”
Sequential chemotherapy with ifosfamide and etoposide consolidation does very well in activated B-cell tumors, both in phase 2 and phase 3 studies.
“Importantly, small molecules seem to have differential effects totally predictable based on the biology of the difference between activated B-cell and germinal center tumors,” Dr Zelenetz said.
“But the big wild card here is somatic mutations further complicate things and will have to be incorporated into our understanding in the selection of patients.”
NEW YORK—The importance of cell of origin in choosing a treatment for diffuse large B-cell lymphoma (DLBCL) is a topic “that has been kicking around for 16 years,” according to a speaker at the NCCN 11th Annual Congress: Hematologic Malignancies.
Cell of origin was first described in the year 2000 as a distinguishing factor in large-cell lymphoma, said the speaker, Andrew Zelenetz, MD, PhD, of Memorial Sloan Kettering Cancer Center in New York, New York.
The cell of origin in DLBCL—whether it’s germinal center B cell (GCB), activated B cell (ABC), or unclassified—contributes to biological and clinical heterogeneity of the disease.
“And more importantly, activated B-cell diffuse large B-cell lymphoma and germinal center diffuse large B-cell lymphoma are simply different diseases,” Dr Zelenetz said.
He then elaborated on the importance of cell of origin in treating DLBCL.
Biology
Dr Zelenetz noted that ABC and GCB lymphomas have different molecular pathways. ABC lymphomas are very dependent on the NF-kB pathway and have more active signaling through the B-cell receptor.
The GCB lymphomas tend to have more tonic regulation, and the PI3 kinase/mTOR pathway is more critical. GCB lymphomas have more genomic instability.
“So cell of origin determination identifies tumors with distinct biology, may provide prognostic information, and may be predictive for treatment selection,” Dr Zelenetz said. “Unfortunately, cell of origin is not the whole story.”
Gene mutations occur in large-cell lymphoma “just like every other cancer,” Dr Zelenetz said. And the vast majority occur in both lymphoma subtypes, he added, further complicating our understanding of the biology of these tumors.
Some of these mutations predict for sensitivity to treatment, while others predict for resistance. For example, CARD11 predicts for resistance to ibrutinib, while CD79b predicts for sensitivity.
Determining the cell of origin
Gene-expression profiling on fresh tissue is considered the gold standard, but “it is clearly not a clinical tool,” Dr Zelenetz said. It requires the Wright classifier, a statistical method based on Bayes’ rule, to make patient-level assignments to 1 of the 3 subgroups.
Immunohistochemistry is widely available, but reproducibility may be difficult. Many assays exist, such as the Hans, Choi, and Muris assays, but, in many studies, there may be a lack of correlation with gene-expression profiling.
In the last few years, gene-expression profiling of formalin‐fixed paraffin‐embedded (FFPE) tissue has emerged as a reliable method. The assay is reproducible between laboratories, and it’s reproducible between different sets of reagents.
“[T]here is tremendous correlation between the Lymph2Cx assay and the gold standard,” Dr Zelenetz added.
“So here we have a robust assay,” he said, which allows investigators to explore whether the cell of origin is prognostic in large-cell lymphoma.
Prognosis
In a data set of 339 patients with de novo DLBCL treated with R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone), the Lymph2Cx assay showing cell of origin was predictive of overall and progression-free survival.
However, the same exact assay applied to the RICOVER-60 data from the German High-Grade Non-Hodgkin Lymphoma Study group was not predictive, Dr Zelenetz reported, based on a personal communication from one of the investigators. There was a slight trend in favor of GCB tumors, but it was not statistically significant.
And the REMoDL-B study, using gene-expression profiling of FFPE tissue with the DASL assay, also didn’t show any difference in outcome between ABC or GCB tumors.
So gene-expression profiling of FFPE tissue does not universally show a prognostic difference, Dr Zelenetz said.
Influence of chemotherapy by cell of origin
CALGB 59910 showed that GCB tumors had a superior event-free, progression-free, and overall survival with dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) compared to ABC tumors.
“However, this is a phase 2, hypothesis-generating experiment,” Dr Zelenetz pointed out, and the results of the confirmatory study comparing dose-adjusted EPOCH-R and R-CHOP21 (CALGB 50303) will be presented later this year at the ASH Annual Meeting.
Sequential, non-cross-resistant chemotherapy
Data from the Memorial Sloan Kettering study (MSKCC 01-142/08-146; NCT00712582) of sequential therapy with R-CHOP followed by ICE (ifosfamide, carboplatin, and etoposide) demonstrate “excellent” progression-free and overall survival, Dr Zelenetz said.
“When we analyzed the outcome by cell of origin, there was a suggestion that the patients with the non-germinal center tumors were actually doing better than the germinal center tumors,” he added.
He pointed out one of the limitations of the study is that the cell of origin was determined by the Hans model. Nevertheless, the study raised another testable hypothesis: sequential therapy might overcome the adverse impact of the non-germinal center tumors.
Cell of origin analysis of the prospective, randomized study (LNH 03-2B) comparing R-ACVBP (rituximab, doxorubicin, cyclophosphamide, vindesine, bleomycin, and prednisone) to R-CHOP showed that whether patients with GCB tumors received CHOP or ACVBP didn’t make “a whit of difference,” Dr Zelenetz said, in terms of progression-free and overall survival.
However, patients with ABC tumors demonstrated an “enormous difference in favor of R-ACVBP,” he said.
“Again, evidence that you can overcome the adverse effect of the ABC tumors with chemotherapy.”
Dr Zelenetz pointed out that R-ACVBP and R-CHOP followed by ICE are “actually remarkably similar regimens.” Both are sequential, both include consolidation, and both incorporate high-dose ifosfamide and etoposide.
“[S]o they actually reinforce each other,” he said, “demonstrating a similar result.”
Lenalidomide
Lenalidomide in the relapsed/refractory setting has modest activity in DLBCL, with most of the benefit accruing to patients with non-germinal center tumors.
Two clinical studies evaluated the impact of adding lenalidomide to standard chemotherapy.
In an Italian series using lenalidomide (L) plus R-CHOP21 in elderly untreated patients, the combination produced outstanding progression-free and event-free survival, but with no significant differences between the subtypes.
A US study of RL-CHOP versus R-CHOP included 87 matched historical controls treated with R-CHOP and 64 patients treated with RL-CHOP. Patients with non-germinal center tumors treated with RL-CHOP fared much better than historical controls treated with R-CHOP.
However, among germinal center tumors, “there was not a hint of any difference,” Dr Zelenetz noted.
Two studies—E1412, using an unselected population, and the international ROBUST study, selecting for patients with ABC tumors—are underway to confirm that the benefit with lenalidomide is in patients with activated B-cell tumors.
Ibrutinib
Ibrutinib, a Bruton’s tyrosine kinase inhibitor, also has modest activity as a single agent in an unselected patient population with relapsed/refractory DLBCL. And most of the patients who demonstrated benefit had activated B-cell tumors.
Upon further analysis, investigators found that response was enhanced by the CD79b mutation, but it was not necessary for a response. And patients with CARD11 had no response.
MYD88 mutations seemed to cause resistance to ibrutinib, unless the mutation was associated with the CD79b mutation, and then patients had a “great” response, Dr Zelenetz explained.
In the upfront setting, a phase 1b study of R-CHOP plus ibrutinib demonstrated the safety of the combination, which had an overall survival rate of 100% and a complete response rate of 91%.
The prospective, randomized, phase 3 PHOENIX trial (NCT01855750) evaluating the combination in newly diagnosed non-germinal center DLBCL has completed accrual, but analysis is still pending.
Conclusion
“The prognostic significance of cell of origin is still controversial,” Dr Zelenetz wrapped up, “although I actually believe there is a prognostic difference in unselected registry patients.”
Sequential chemotherapy with ifosfamide and etoposide consolidation does very well in activated B-cell tumors, both in phase 2 and phase 3 studies.
“Importantly, small molecules seem to have differential effects totally predictable based on the biology of the difference between activated B-cell and germinal center tumors,” Dr Zelenetz said.
“But the big wild card here is somatic mutations further complicate things and will have to be incorporated into our understanding in the selection of patients.”