User login
Organic Erectile Dysfunction
Erectile dysfunction (ED) is defined as the recurrent inability, of three months’ duration or longer, to attain or maintain an erection sufficient for satisfactory sexual performance.1,2 It is classified as either psychogenic or organic; organic ED will be addressed here. Up to 80% of cases of organic ED can be further categorized into vascular, neurogenic, anatomic, or hormonal subtypes,2,3 with many affected patients vulnerable to potentially serious comorbidities and risk factors.
In the early 1990s, the NIH reported that nearly 30 million US men were affected by ED.2 However, increased public awareness of the condition, beginning with the availability of effective oral medications in the late 1990s, may have led to increased numbers of reported cases—and of men seeking treatment.
COMMON CONDITION, COMMONLY UNTREATED
According to results from the 2001-2002 National Health and Nutrition Examination Survey,4,5 ED affects about 8% of US men: 4% of those in their 50s, 17% of those in their 60s, 47% of men older than 65, and 78% of men 75 or older. More than 27,000 men from Europe and North and South America (ages 20 to 75) were interviewed for the 2004 Men’s Attitudes to Life Events and Sexuality (MALES) study; findings included an overall prevalence for ED of 16%, and 22% among men from the United States.6 See information regarding self-reported ED prevalence in Table 1.7
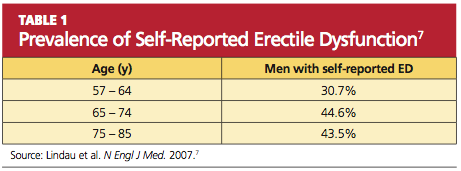
An important finding from the MALES study was that only 58% of respondents with self-reported ED had sought medical treatment for the condition.6 Some men may be reluctant to broach the subject with a health care provider because they consider ED a purely sexual problem—whereas the etiology is most commonly vascular.8 Thus, it is important for health care providers to include the sexual history as a routine component in the wellness exam for all patients, and to be aware of the potential presentation in patients with organic ED, appropriate work-up, and physical examination.
Additionally, ED can be a wake-up call for men at risk for cardiovascular disease (CVD); ED occurs at a mean time of five years before a cardiovascular event.9 Therefore, in addition to counseling patients with ED regarding treatment and prevention strategies, clinicians should be prepared to identify and address the risk factors and medical comorbidities associated with ED.
The Mechanisms of Erection
When sexual stimulation occurs, parasympathetic activity increases production of the nucleotide cyclic guanosine monophosphate (cGMP), resulting in relaxation of cavernosal smooth muscle and an influx of blood into the penis. This filling action produces expansion of the sinusoidal spaces in the penis, compressing venous channels and thereby preventing outflow of blood to allow maintenance of a rigid erection.10,11
Nitric oxide is needed for vasodilation of the corpora cavernosa. Inhibition of the enzyme phosphodiesterase type 5 (PDE-5) allows increased production and accumulation of penile cGMP. This results in relaxation of the smooth-muscle cells and improved erectile function.1,10,11
PRESENTATION, HISTORY, AND TYPES OF ORGANIC ED
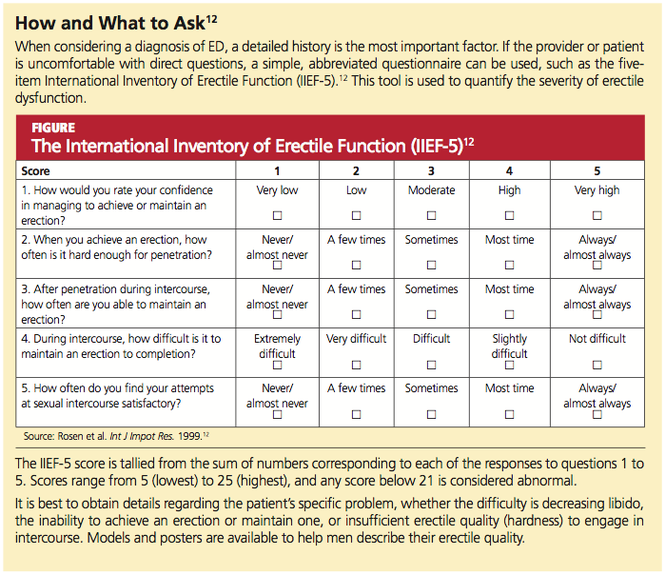
In the primary care setting, the opportunity to assess for and address erectile function generally presents itself at the patient’s annual wellness visit—but could easily go unmentioned if the health care provider does not initiate the discussion. Direct questioning during the review of systems may ease any anxiety for the patient and open up a dialogue regarding other problems or medical conditions. (See box, “How and What To Ask,”12)
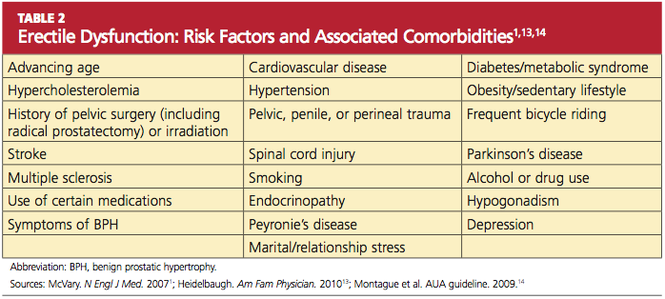
Providers can also assess the patient’s risk factors for ED and its associated comorbid conditions (see Table 21,13,14). The patient’s medical history may hold important clues to a diagnosis of organic ED.
Because certain vasculopathies, including diabetes, are known to accelerate the process of endothelial dysfunction, inquiries should be made into the sexual history of men with these disorders, regardless of age.10 Marked hyperlipidemia, uncontrolled hypertension, atherosclerosis, and other manifestations of CVD can impair erectile as well as endothelial function, leading to vascular ED.
The potential for atherosclerosis in the penile arteries (which are significantly narrower than the carotid, coronary, or femoral arteries) should prompt the primary care provider to evaluate the patient’s risk for vascular disease and its sequelae in the heart as well.8 (Of note, in one study of metabolic syndrome and ED, ED was found to be a predictor for impaired elasticity in the large arteries, independent of cardiovascular risk factors.15) In addition to damaging the small blood vessels and the endothelium, diabetes and other components of the metabolic syndrome contribute to ED by affecting cavernous nerve terminals and smooth muscle.1,14
Lifestyle factors, such as overconsumption of alcohol, smoking, recreational drug use, obesity, and inactivity can contribute to decreased libido and ED.14 Cigarette smoking can cause vasoconstriction and penile venous leak, resulting in poor erectile quality or even loss of erection. While small amounts of alcohol can improve libido and erection due to its anti-anxiety and vasodilatory effects, “more is not better” in this case, as higher doses result in sedation and decreased libido. Chronic alcoholism results in hypogonadism and polyneuropathy.16
Neurogenic ED can result from abnormalities at the level of the brain, the spinal cord, or the pelvis. Previous pelvic surgery, such as prostatectomy or colectomy, can disrupt the cavernous or pudendal nerves. Spinal cord injury, Parkinson’s disease, multiple sclerosis, diabetes with peripheral neuropathy, or a history of trauma can all result in neurogenic ED.16
Additionally, there is evidence of perineal compression from frequent bicycle riding leading to vascular, endothelial, and neurogenic dysfunction in men, with increased incidence of ED.17
Age alone is a risk factor for ED,7,18 as sexual function declines even in healthy men as they age. Penile sensitivity decreases, and there is increased latency between sexual stimulation and resulting erection, as well as between ejaculations. Ejaculations are less forceful, with less ejaculatory volume.16 Other factors that may affect the degree of ED include a history of stroke or pelvic surgery, especially in high-risk cardiac patients.19
Though not the focus of this article, the potential for psychogenic ED should be mentioned, as it warrants screening with a complete psychosocial history to rule out this etiology. The interview should allow time for the patient to discuss current or past relationship difficulties, marital conflict, life stressors, depression, and anxiety. Whatever the etiology of ED, the primary care provider should always elicit a sexual history, including number of sexual partners, current relationship status (ie, committed or casual), and incidence of ED with specific partners.20 The effects of ED on these relationships should be discussed.
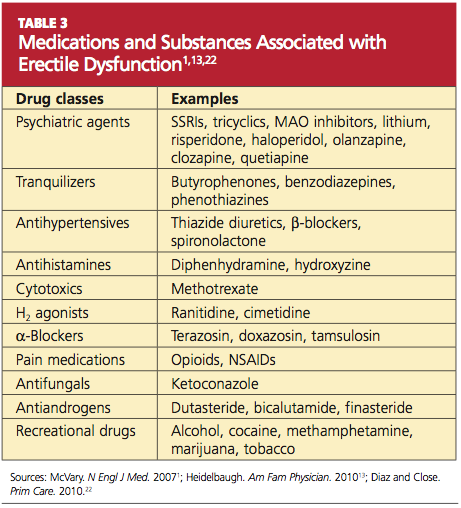
A medication history is important for the ED workup. Antidepressants, especially the SSRIs, and certain hypertensives can affect the libido, arousal, and orgasm.21 See Table 31,13,22 for commonly used agents that can affect erectile function and sexual satisfaction.
Previous Medical History
The patient should be asked whether he has had any previous testing or treatment for ED. Was any therapy used effective? Did he experience any adverse effects during treatment? If treatment results were unsatisfactory, he should be questioned to ensure that he was using treatment correctly. Commonly, patients do not understand that sexual stimulation is necessary to achieve an erection when they are being treated with an oral PDE-5 inhibitor.23
PHYSICAL EXAMINATION
The clinician who performs the physical examination should take into account the psychogenic, neurogenic, and vasculogenic causes of ED. The genitourinary examination alone is not sufficient; abdominal, vascular, and neurologic exams must be included. The patient should be assessed for body habitus, secondary sex characteristics (including ruling out gynecomastia), and lower extremity pulses.22
The genitourinary exam should include testicular, rectal, and penile examination to rule out physical abnormalities. Small testicles (< 5 mL) or testicular atrophy on palpation should lead the examiner to consider testosterone testing24,25 (see “Diagnostic Testing,” below). A digital rectal examination may reveal an enlarged prostate (this finding, in the presence of lower urinary tract symptoms, has been associated with ED26). Palpation of the penis for plaques and questioning about pain with erection or deviation of the erect penis can lead to a diagnosis of Peyronie’s disease27; if this is the case, the patient can be referred to urology for treatment.
The vascular system should be assessed by listening for abdominal or femoral bruits and the lower extremities checked for appropriate hair growth, skin color, and distal pulses. The examiner should note any scars indicating a history of bypass surgery, which may have been overlooked during the surgical history.
DIAGNOSTIC TESTING
A fasting glucose level and a lipid profile should be routinely obtained because of the links between ED and diabetes and CVD.28,29 A chemistry panel and complete blood count, if one has not been performed recently, can be used to assess the patient’s general health, with a thyroid-stimulating hormone (TSH) level tested in men who report fatigue or weakness.
Men who are older than 50 should be considered for prostate-specific antigen (PSA) testing. Testosterone levels (free and total) are generally reserved for patients with small or atrophic testicles25 or for those who report decreased libido with fatigue or other symptoms of hypogonadism, including depression and decreased muscle strength, muscle mass, or vitality.22,24,25,30 If testosterone levels are ordered, the patient should be counseled to have samples drawn in the early morning to avoid the influence of daily hormonal fluctuations. In patients found to have low testosterone levels (ie, < 300 ng/dL,13 occurring in 12.5% to 35% of men with ED24), prolactin testing may be considered next; in patients with ED, hypoprolactinemia is associated with dyslipidemia, metabolic syndrome, and other risk factors for cardiovascular events.29,31,32
Imaging Studies
A number of imaging studies, once frequently used in evaluation for ED, are considered outdated and are no longer performed. However, Doppler blood flow analysis or ultrasonographic penile blood flow studies can be useful for identifying and evaluating the specific causes of vasculogenic ED, including arterial insufficiency and veno-occlusive disease.33,34 Other conditions associated with ED, such as Peyronie’s disease and priapism, can also be identified through these modalities.33
TREATMENT
The PDE-5 Inhibitors
While historically not the first treatment available for ED, medical therapy is certainly the most popular option for men with ED. The oral PDE-5 inhibitors first became available in the 1990s. All three such agents currently available in the US—sildenafil, tadalafil, and vardenafil—have been demonstrated effective in improving and maintaining erections,35-38 but their pharmacokinetics differ,39 and few head-to-head studies have been conducted that demonstrate greater efficacy of one agent over another.39,40 It has been suggested that patients try all three medications to determine preference and satisfaction.39
Qaseem et al24 report that PDE-5 inhibitors demonstrated clinical benefit regardless of baseline severity of dysfunction or ED cause, including diabetes and depression. These medications require sexual stimulation to be effective and typically are effective about one hour after dosing.23 Tadalafil is remarkable for the length of its half-life, which makes it appropriate at 2.5- or 5.0-mg doses for once-daily dosing41; it is also noted for a relatively low incidence of associated flushing,42 but back pain is more common among tadalafil users than among men using sildenafil or vardenafil.11,39,43
In addition to back pain and myalgia, the most common adverse effects associated with PDE-5 inhibitor use are dyspepsia, flushing, headache, and nasal congestion.42 Because absorption of sildenafil is reduced by food intake, and vardenafil44 to a lesser extent, these agents are best avoided in close proximity to meals. Absorption of tadalafil is not affected by food.45 Higher doses of sildenafil and vardenafil were associated with greater benefit in treating ED.24,46
Note: All three PDE-5 inhibitors are contraindicated in men taking long-acting nitrates or nitroglycerin.24 Their effectiveness may be potentiated by use of erythromycin, ketoconazole, and HIV protease inhibitors.39 Information about dosing options and adverse effects can be found in Table 411.

Testosterone
Hypogonadism, though found in only 5% of men with ED,47 may be an indication for testosterone replacement therapy, and testosterone use has been found to improve libido in men with sexual dysfunction.48 However, the authors of the American College of Physicians clinical practice guidelines24 found insufficient evidence that testosterone replacement improved erections or quality of sexual intercourse. There was also insufficient evidence that testosterone plus sildenafil was more effective than sildenafil alone.24,49,50
Additional Pharmacologic Considerations
A careful review of the medication history for the patient with ED may lead the astute clinician to consider whether a change in current prescriptions might improve the man’s sexual function. Among the commonly used agents listed in Table 3, those with the greatest apparent impact on erections are thiazide diuretics and β-blockers, SSRIs, and tricyclic antidepressants.1,4
For a man who is interested in preserving potency, the clinician should select medications with the least effect on erectile function—for instance, an ACE inhibitor1 rather than a thiazide or β-blocker for the patient with hypertension. In the patient affected by depression, a trial of bupropion, substituted for or added to his current antidepressant, may be helpful.51 Medical therapies for hyperglycemia, hyperlipidemia, and hypertension should be considered if warranted, as should cardiovascular screening with exercise stress testing. (See box, “ED, CAD, and PDE-5 Inhibitors”52)

Alternative and Nonpharmacologic Options
A number of herbal products have been touted to improve sexual function. The FDA53 has issued press releases warning consumers about these and other alternatives to prescription medications. According to the FDA, many “sexual enhancement” products have been found to contain active ingredients resembling those found in one or more PDE-5 inhibitors. These products are in violation of federal law, and consumers are advised to avoid supplements that claim to produce effects similar to those of prescription drugs.53
By contrast, one potentially beneficial supplement currently under study is L-citrulline. As the body converts oral L-citrulline to L-arginine, vasodilation and endothelial function improve, often leading to resolution of mild ED. In a small, single-blind placebo-controlled study, patients who took L-citrulline (1.5 g/d in divided doses) reported improvement in hardness scale grading and increased satisfaction regarding sexual function. No adverse effects were reported, making L-citrulline a possible option for patients who hesitate to use a PDE-5 inhibitor.54
For patients with lack of response or contraindications to accepted medical therapy, other options include alprostadil intraurethral suppositories, penile prosthetic implants, vacuum erection devices, vascular surgery, yohimbine and other herbal therapies, and trazodone.1,14,55-59 These methods may require detailed counseling. Primary care providers who are unfamiliar with these modalities or reluctant to introduce them may wish to refer patients to urology.
PATIENT EDUCATION
Aggressive reduction in cardiovascular risks with smoking cessation, weight loss, and physical activity should be encouraged. In a study of obese men with ED (but without diabetes, hypertension, or hyperlipidemia), Esposito et al60 found that reducing caloric intake and increasing physical activity was associated with improved sexual function in about one-third of the subjects. Bicycle riders can decrease risks of perineal compression with newer seat designs.17
Smoking cessation alone has been shown to improve erectile function at one-year follow-up in at least 25% of men who stopped smoking, compared with none of the men who continued to smoke.61 Patients can help preserve endothelial function with efforts to maintain normal blood pressure and glycemic control.
Researchers are currently looking at occupational exposures as a cause of ED. Exposure to plastics containing bisphenol-A, for example, has been linked to decreased libido.62
CONCLUSION
In addition to addressing erectile dysfunction as a sexual problem, the health care provider should recognize its association with CVD, diabetes, depression, and other serious illnesses. However, it is also important to open a dialogue about sexual function to encourage the patient to discuss the problem of ED. Timely diagnosis and treatment of these conditions may be of even greater benefit to the patient than the effective therapies available for ED itself.
REFERENCES
1. McVary KT. Clinical practice: erectile dysfunction. N Engl J Med. 2007;357(24):2472-2481.
2. NIH Consensus Conference. Impotence: NIH Consensus Development Panel on Impotence. JAMA. 1993;270(1):83-90.
3. Hafez ES, Hafez SD. Erectile dysfunction: anatomical parameters, etiology, diagnosis, and therapy. Arch Androl. 2005;51(1):15-31.
4. Francis ME, Kusek JW, Nyberg LM, Eggers PW. The contribution of common medical conditions and drug exposures to erectile dysfunction in adult males. J Urol. 2007;178(2):591-596.
5. Saigal CS, Wessells H, Pace J, et al. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166 (2):207-212.
6. Rosen RC, Fisher WA, Eardley I, et al. The multinational Men’s Attitudes to Life Events and Sexuality (MALES) study. I. Prevalence of erectile dysfunction and related health concerns in the general population. Curr Med Res Opin. 2004;20 (5):607-617.
7. Lindau ST, Schumm LP, Laumann EO, et al. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357(8): 762-774.
8. Batty GD, Li Q, Czernichow S, et al. Erectile dysfunction and later cardiovascular disease in men with type 2 diabetes: prospective cohort study based on the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified-Release Controlled Evaluation) trial. J Am Coll Cardiol. 2010;56(23): 1908-1913.
9. Hodges LD, Kirby M, Solanki J, et al. The temporal relationship between erectile dysfunction and cardiovascular disease. Int J Clin Pract. 2007; 61(12):2019-2025.
10. Miner MM, Kuritzky L. Erectile dysfunction: a sentinel marker for cardiovascular disease in primary care. Cleve Clin J Med. 2007;74 suppl 3: S30-S37.
11. McCullough AR. An update on the PDE-5 inhibitors (PDE-5i). J Androl. 2003;24(6 suppl): S52-S58.
12. Rosen RC, Cappelleri JC, Smith MD, et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):
319-326.
13. Heidelbaugh JJ. Management of erectile dysfunction. Am Fam Physician. 2010;81(3):305-312.
14. Montague DK, Jarow JP, Broderick GA, et al; Erectile Dysfunction Guideline Update Panel. AUA guideline on the management of erectile dysfunction: an update (2006). American Urological Association Education and Research, Inc. www.auanet.org/content/guidelines-and-quality- care/clinical-guidelines.cfm?sub=ed. Accessed August 8, 2011.
15. Pohjantahti-Maaroos H, Palomäki A. Comparison of metabolic syndrome subjects with and without erectile dysfunction: levels of circulating oxidised LDL and arterial elasticity. Int J Clin Pract. 2011;65(3):274-280.
16. Lue TF. Male sexual dysfunction. In: Tanagho EA, McAninch JW, eds. Smith’s General Urology. 16th ed. San Francisco, CA: McGraw-Hill; 2004: 592-596.
17. Sommer F, Goldstein I, Korda JB. Bicycle riding and erectile dysfunction: a review. J Sex Med. 2010;7(7):2346-2358.
18. Feldman HA, Johannes CB, Derby CA, et al. Erectile dysfunction and coronary risk factors: prospective results from the Massachusetts male aging study. Prev Med. 2000;30(4):328-338.
19. Böhm M, Baumhäkel M, Probstfield JL, et al. Sexual function, satisfaction, and association of erectile dysfunction with cardiovascular disease and risk factors in cardiovascular high-risk patients: substudy of the ONgoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial/Telmisartan Randomized AssessmeNT Study in ACE-INtolerant Subjects with Cardiovascular Disease (ONTARGET/TRANSCEND). Am Heart J. 2007;154(1):94-101.
20. Athanasiadis L, Papaharitou S, Salpiggidis G, et al. Educating physicians to treat erectile dysfunction patients: development and evaluation of a course on communication and management strategies. J Sex Med. 2006;3(1):47-55.
21. Kennedy SH, Rizvi S. Sexual dysfunction, depression, and the impact of antidepressants.
J Clin Psychopharmacol. 2009;29(2):157-164.
22. Diaz VA Jr, Close JD. Male sexual dysfunction. Prim Care. 2010;37(3):473-489, vii-viii.
23. Carson CC, Lue TF. Phosphodiesterase type 5 inhibitors for erectile dysfunction. BJU Int. 2005; 96(3):257-280.
24. Qaseem A, Snow V, Denberg TD, et al. Hormonal testing and pharmacologic treatment of erectile dysfunction: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2009;151(9):630-649.
25. Dandona P, Rosenberg MT. A practical guide to male hypogonadism in the primary care setting. Int J Clin Pract. 2010;64(6):682-696.
26. Paick SH, Meehan A, Lee M, et al. The relationship among lower urinary tract symptoms, prostate specific antigen and erectile dysfunction in men with benign prostatic hyperplasia: results from the Proscar Long-Term Efficacy and Safety Study. J Urol. 2005;173(3):903-907.
27. Smith JF, Walsh TJ, Lue TF. Peyronie’s disease: a critical appraisal of current diagnosis and treatment. Int J Impot Res. 2008;20(5):445-459.
28. Gazzaruso C, Coppola A, Giustina A. Erectile dysfunction and coronary artery disease in patients with diabetes. Curr Diabetes Rev. 2011; 7(2):143-147.
29. Vlachopoulos C, Ioakeimidis N, Terentes-Printzios D, Stefanidis C. The triad: erectile dysfunction—endothelial dysfunction—cardiovascular disease. Curr Pharm Des. 2008;14(35): 3700-3704.
30. Makhlouf AA, Mohamed MA, Seftel AD, Niedergerger C. Hypogonadism is associated with overt depression symptoms in men with erectile dysfunction. Int J Impot Res. 2008;20(2): 157-161.
31. Corona G, Rastrelli G, Boddi V, et al. Prolactin levels independently predict major cardiovascular events in patients with erectile dysfunction. Int J Androl. 2011;34(3):217-224.
32. Vlachopoulos C, Rokkas K, Ioakeimidis N, Stefanadis C. Inflammation, metabolic syndrome, erectile dysfunction, and coronary artery disease: common links. Eur Urol. 2007;52(6):1590-1600.
33. LeRoy TJ, Broderick GA. Doppler blood flow analysis of erectile function: who, when, and how. Urol Clin North Am. 2011;38(2):147-154.
34. Aversa A, Sarteschi LM. J Sex Med. The role of penile color-duplex ultrasound for the evaluation of erectile dysfunction. J Sex Med. 2007;4(5): 1437-1447.
35. Fink HA, MacDonald R, Rutks IR, et al. Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med. 2002; 16(12):1349-1360.
36. Perimenis P, Roumeguere T, Heidler H, et al. Evaluation of patient expectations and treatment satisfaction after 1-year tadalafil therapy for erectile dysfunction: the DETECT study. J Sex Med. 2009;6(1):257-267.
37. Goldstein I, Kim E, Steers WD, et al. Efficacy and safety of tadalafil in men with erectile dysfunction with a high prevalence of comorbid conditions: results from MOMENTUS: multiple observations in men with erectile dysfunction in National Tadalafil Study in the US. J Sex Med. 2007;4(1):166-175.
38. Van Ahlen H, Zumbé J, Stauch K, Hanisch JU. The Real-Life Safety and Efficacy of vardenafil (REALISE) study: results in men from Europe and overseas with erectile dysfunction and cardiovascular or metabolic conditions. J Sex Med. 2010; 7(9):3161-3169.
39. Raheem AA, Kell P. Patient preference and satisfaction in erectile dysfunction therapy: a comparison of the three phosphodiesterase-5 inhibitors sildenafil, vardenafil and tadalafil. Patient Prefer Adherence. 2009;3:99-104.
40. Jannini EA, Isidori AM, Gravina GL, et al. The ENDOTRIAL study: a spontaneous, open-label, randomized, multicenter, crossover study on the efficacy of sildenafil, tadalafil, and vardenafil in the treatment of erectile dysfunction. J Sex Med. 2009;6(9):2547-2560.
41. Washington SL 3rd, Shindel AW. A once-daily dose of tadalafil for erectile dysfunction: compliance and efficacy. Drug Des Devel Ther. 2010 Sep 7;4:159-171.
42. Brock G, Glina S, Moncada I, et al. Likelihood of tadalafil-associated adverse events in integrated multiclinical trial database: classification tree analysis in men with erectile dysfunction. Urology. 2009;73(4):756-761.
43. Montorsi F, Avera A, Mocada I, et al. A randomized, double-blind, placebo-controlled, parallel study to assess the efficacy and safety of once-a-day tadalafil in men with erectile dysfunction who are naïve to PDE5 inhibitors. J Sex Med. 2011 Jun 27 [Epub ahead of print].
44. Rajagopalan P, Mazzu A, Xia C, et al. Effect of high-fat breakfast and moderate-fat evening meal on the pharmacokinetics of vardenafil, an oral phosphodiesterase-5 inhibitor for the treatment of erectile dysfunction. J Clin Pharmacol. 2003;43 (3):260-267.
45. Eardley I, Donatucci C, Corbin J, et al. Pharmacotherapy for erectile dysfunction. J Sex Med. 2010;7(1 pt 2):524-540.
46. Loran OB, Ströberg P, Lee SW, et al. Sildenafil citrate 100 mg starting dose in men with erectile dysfunction in an international, double-blind, placebo-controlled study: effect on the sexual experience and reducing feelings of anxiety about the next intercourse attempt. J Sex Med. 2009; 6(10):2826-2835.
47. Mihkail N. Does testosterone have a role in erectile function? Am J Med. 2006;119(5):373-382.
48. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82(1):20-28.
49. Shabsigh R, Kaufman JM, Steidle C, Padma-Nathan H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J Urol. 2004;172(2): 658-663.
50. Aversa A, Isidori AM, Spera G, et al. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin Endocrinol (Oxf). 2003;58(5):632-638.
51. Safarinejad MR. The effects of the adjunctive bupropion on male sexual dysfunction induced by a selective serotonin reuptake inhibitor: a double-blind placebo-controlled and randomized study. BJU Int. 2010;106(6):840-847.
52. Gazzaruso C, Solerte SB, Pujia A, et al. Erectile dysfunction as a predictor of cardiovascular events and death in diabetic patients with angiographically proven asymptomatic coronary artery disease: a potential protective role for statins and 5-phosphodiesterase inhibitors. J Am Coll Cardiol. 2008;51(21):2040-2044.
53. FDA. Tainted sexual enhancement products. www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsing MedicineSafely/MedicationHealthFraud/ucm234539.htm. Accessed August 8, 2011.
54. Cormio L, De Siati M, Lorusso F, et al. Oral L-citrulline supplementation improves erection hardness in men with mild erectile dysfunction. Urology. 2011;77(1):119-122.
55. Padma-Nathan H, Hellstrom WJ, Kaiser FE, et al. Treatment of men with erectile dysfunction with transurethral alprostadil: Medicated Urethral System for Erection (MUSE) Study Group. N Engl J Med. 1997;33(1)6:1-17.
56. Wolter CE, Hellstrom JG. The hydrophilic-coated penile prosthesis: 1-year experience. J Sex Med. 2004:1(2):221-224.
57. Yuan J, Hoang AN, Romero CA, et al. Vacuum therapy in erectile dysfunction: science and clinical evidence. Int J Impot Res. 2010;22(4):211-219.
58. Lebret T, Hervé JM, Gorny P, et al. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. Eur Urol. 2002; 41(6):608-613.
59. Fink HA, MacDonald R, Rutks IR, Wilt TJ. Trazodone for erectile dysfunction: a systematic review and meta-analysis. BJU Int. 2003;92(4): 441-446.
60. Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004;291(24):2978-2984.
61. Pourmand G, Alidaee M, Rasuli S, et al. Do cigarette smokers with erectile dysfunction benefit from stopping? A prospective study. BJU Int. 2004;94(9):1310-1313.
62. Li D, Zhou Z, Qing D, et al. Occupational exposure to bisphenol-A (BPA) and the risk of self-reported male sexual dysfunction. Hum Reprod. 2010;25(2):519-527.
Erectile dysfunction (ED) is defined as the recurrent inability, of three months’ duration or longer, to attain or maintain an erection sufficient for satisfactory sexual performance.1,2 It is classified as either psychogenic or organic; organic ED will be addressed here. Up to 80% of cases of organic ED can be further categorized into vascular, neurogenic, anatomic, or hormonal subtypes,2,3 with many affected patients vulnerable to potentially serious comorbidities and risk factors.
In the early 1990s, the NIH reported that nearly 30 million US men were affected by ED.2 However, increased public awareness of the condition, beginning with the availability of effective oral medications in the late 1990s, may have led to increased numbers of reported cases—and of men seeking treatment.
COMMON CONDITION, COMMONLY UNTREATED
According to results from the 2001-2002 National Health and Nutrition Examination Survey,4,5 ED affects about 8% of US men: 4% of those in their 50s, 17% of those in their 60s, 47% of men older than 65, and 78% of men 75 or older. More than 27,000 men from Europe and North and South America (ages 20 to 75) were interviewed for the 2004 Men’s Attitudes to Life Events and Sexuality (MALES) study; findings included an overall prevalence for ED of 16%, and 22% among men from the United States.6 See information regarding self-reported ED prevalence in Table 1.7
An important finding from the MALES study was that only 58% of respondents with self-reported ED had sought medical treatment for the condition.6 Some men may be reluctant to broach the subject with a health care provider because they consider ED a purely sexual problem—whereas the etiology is most commonly vascular.8 Thus, it is important for health care providers to include the sexual history as a routine component in the wellness exam for all patients, and to be aware of the potential presentation in patients with organic ED, appropriate work-up, and physical examination.
Additionally, ED can be a wake-up call for men at risk for cardiovascular disease (CVD); ED occurs at a mean time of five years before a cardiovascular event.9 Therefore, in addition to counseling patients with ED regarding treatment and prevention strategies, clinicians should be prepared to identify and address the risk factors and medical comorbidities associated with ED.
The Mechanisms of Erection
When sexual stimulation occurs, parasympathetic activity increases production of the nucleotide cyclic guanosine monophosphate (cGMP), resulting in relaxation of cavernosal smooth muscle and an influx of blood into the penis. This filling action produces expansion of the sinusoidal spaces in the penis, compressing venous channels and thereby preventing outflow of blood to allow maintenance of a rigid erection.10,11
Nitric oxide is needed for vasodilation of the corpora cavernosa. Inhibition of the enzyme phosphodiesterase type 5 (PDE-5) allows increased production and accumulation of penile cGMP. This results in relaxation of the smooth-muscle cells and improved erectile function.1,10,11
PRESENTATION, HISTORY, AND TYPES OF ORGANIC ED
In the primary care setting, the opportunity to assess for and address erectile function generally presents itself at the patient’s annual wellness visit—but could easily go unmentioned if the health care provider does not initiate the discussion. Direct questioning during the review of systems may ease any anxiety for the patient and open up a dialogue regarding other problems or medical conditions. (See box, “How and What To Ask,”12)
Providers can also assess the patient’s risk factors for ED and its associated comorbid conditions (see Table 21,13,14). The patient’s medical history may hold important clues to a diagnosis of organic ED.
Because certain vasculopathies, including diabetes, are known to accelerate the process of endothelial dysfunction, inquiries should be made into the sexual history of men with these disorders, regardless of age.10 Marked hyperlipidemia, uncontrolled hypertension, atherosclerosis, and other manifestations of CVD can impair erectile as well as endothelial function, leading to vascular ED.
The potential for atherosclerosis in the penile arteries (which are significantly narrower than the carotid, coronary, or femoral arteries) should prompt the primary care provider to evaluate the patient’s risk for vascular disease and its sequelae in the heart as well.8 (Of note, in one study of metabolic syndrome and ED, ED was found to be a predictor for impaired elasticity in the large arteries, independent of cardiovascular risk factors.15) In addition to damaging the small blood vessels and the endothelium, diabetes and other components of the metabolic syndrome contribute to ED by affecting cavernous nerve terminals and smooth muscle.1,14
Lifestyle factors, such as overconsumption of alcohol, smoking, recreational drug use, obesity, and inactivity can contribute to decreased libido and ED.14 Cigarette smoking can cause vasoconstriction and penile venous leak, resulting in poor erectile quality or even loss of erection. While small amounts of alcohol can improve libido and erection due to its anti-anxiety and vasodilatory effects, “more is not better” in this case, as higher doses result in sedation and decreased libido. Chronic alcoholism results in hypogonadism and polyneuropathy.16
Neurogenic ED can result from abnormalities at the level of the brain, the spinal cord, or the pelvis. Previous pelvic surgery, such as prostatectomy or colectomy, can disrupt the cavernous or pudendal nerves. Spinal cord injury, Parkinson’s disease, multiple sclerosis, diabetes with peripheral neuropathy, or a history of trauma can all result in neurogenic ED.16
Additionally, there is evidence of perineal compression from frequent bicycle riding leading to vascular, endothelial, and neurogenic dysfunction in men, with increased incidence of ED.17
Age alone is a risk factor for ED,7,18 as sexual function declines even in healthy men as they age. Penile sensitivity decreases, and there is increased latency between sexual stimulation and resulting erection, as well as between ejaculations. Ejaculations are less forceful, with less ejaculatory volume.16 Other factors that may affect the degree of ED include a history of stroke or pelvic surgery, especially in high-risk cardiac patients.19
Though not the focus of this article, the potential for psychogenic ED should be mentioned, as it warrants screening with a complete psychosocial history to rule out this etiology. The interview should allow time for the patient to discuss current or past relationship difficulties, marital conflict, life stressors, depression, and anxiety. Whatever the etiology of ED, the primary care provider should always elicit a sexual history, including number of sexual partners, current relationship status (ie, committed or casual), and incidence of ED with specific partners.20 The effects of ED on these relationships should be discussed.
A medication history is important for the ED workup. Antidepressants, especially the SSRIs, and certain hypertensives can affect the libido, arousal, and orgasm.21 See Table 31,13,22 for commonly used agents that can affect erectile function and sexual satisfaction.
Previous Medical History
The patient should be asked whether he has had any previous testing or treatment for ED. Was any therapy used effective? Did he experience any adverse effects during treatment? If treatment results were unsatisfactory, he should be questioned to ensure that he was using treatment correctly. Commonly, patients do not understand that sexual stimulation is necessary to achieve an erection when they are being treated with an oral PDE-5 inhibitor.23
PHYSICAL EXAMINATION
The clinician who performs the physical examination should take into account the psychogenic, neurogenic, and vasculogenic causes of ED. The genitourinary examination alone is not sufficient; abdominal, vascular, and neurologic exams must be included. The patient should be assessed for body habitus, secondary sex characteristics (including ruling out gynecomastia), and lower extremity pulses.22
The genitourinary exam should include testicular, rectal, and penile examination to rule out physical abnormalities. Small testicles (< 5 mL) or testicular atrophy on palpation should lead the examiner to consider testosterone testing24,25 (see “Diagnostic Testing,” below). A digital rectal examination may reveal an enlarged prostate (this finding, in the presence of lower urinary tract symptoms, has been associated with ED26). Palpation of the penis for plaques and questioning about pain with erection or deviation of the erect penis can lead to a diagnosis of Peyronie’s disease27; if this is the case, the patient can be referred to urology for treatment.
The vascular system should be assessed by listening for abdominal or femoral bruits and the lower extremities checked for appropriate hair growth, skin color, and distal pulses. The examiner should note any scars indicating a history of bypass surgery, which may have been overlooked during the surgical history.
DIAGNOSTIC TESTING
A fasting glucose level and a lipid profile should be routinely obtained because of the links between ED and diabetes and CVD.28,29 A chemistry panel and complete blood count, if one has not been performed recently, can be used to assess the patient’s general health, with a thyroid-stimulating hormone (TSH) level tested in men who report fatigue or weakness.
Men who are older than 50 should be considered for prostate-specific antigen (PSA) testing. Testosterone levels (free and total) are generally reserved for patients with small or atrophic testicles25 or for those who report decreased libido with fatigue or other symptoms of hypogonadism, including depression and decreased muscle strength, muscle mass, or vitality.22,24,25,30 If testosterone levels are ordered, the patient should be counseled to have samples drawn in the early morning to avoid the influence of daily hormonal fluctuations. In patients found to have low testosterone levels (ie, < 300 ng/dL,13 occurring in 12.5% to 35% of men with ED24), prolactin testing may be considered next; in patients with ED, hypoprolactinemia is associated with dyslipidemia, metabolic syndrome, and other risk factors for cardiovascular events.29,31,32
Imaging Studies
A number of imaging studies, once frequently used in evaluation for ED, are considered outdated and are no longer performed. However, Doppler blood flow analysis or ultrasonographic penile blood flow studies can be useful for identifying and evaluating the specific causes of vasculogenic ED, including arterial insufficiency and veno-occlusive disease.33,34 Other conditions associated with ED, such as Peyronie’s disease and priapism, can also be identified through these modalities.33
TREATMENT
The PDE-5 Inhibitors
While historically not the first treatment available for ED, medical therapy is certainly the most popular option for men with ED. The oral PDE-5 inhibitors first became available in the 1990s. All three such agents currently available in the US—sildenafil, tadalafil, and vardenafil—have been demonstrated effective in improving and maintaining erections,35-38 but their pharmacokinetics differ,39 and few head-to-head studies have been conducted that demonstrate greater efficacy of one agent over another.39,40 It has been suggested that patients try all three medications to determine preference and satisfaction.39
Qaseem et al24 report that PDE-5 inhibitors demonstrated clinical benefit regardless of baseline severity of dysfunction or ED cause, including diabetes and depression. These medications require sexual stimulation to be effective and typically are effective about one hour after dosing.23 Tadalafil is remarkable for the length of its half-life, which makes it appropriate at 2.5- or 5.0-mg doses for once-daily dosing41; it is also noted for a relatively low incidence of associated flushing,42 but back pain is more common among tadalafil users than among men using sildenafil or vardenafil.11,39,43
In addition to back pain and myalgia, the most common adverse effects associated with PDE-5 inhibitor use are dyspepsia, flushing, headache, and nasal congestion.42 Because absorption of sildenafil is reduced by food intake, and vardenafil44 to a lesser extent, these agents are best avoided in close proximity to meals. Absorption of tadalafil is not affected by food.45 Higher doses of sildenafil and vardenafil were associated with greater benefit in treating ED.24,46
Note: All three PDE-5 inhibitors are contraindicated in men taking long-acting nitrates or nitroglycerin.24 Their effectiveness may be potentiated by use of erythromycin, ketoconazole, and HIV protease inhibitors.39 Information about dosing options and adverse effects can be found in Table 411.
Testosterone
Hypogonadism, though found in only 5% of men with ED,47 may be an indication for testosterone replacement therapy, and testosterone use has been found to improve libido in men with sexual dysfunction.48 However, the authors of the American College of Physicians clinical practice guidelines24 found insufficient evidence that testosterone replacement improved erections or quality of sexual intercourse. There was also insufficient evidence that testosterone plus sildenafil was more effective than sildenafil alone.24,49,50
Additional Pharmacologic Considerations
A careful review of the medication history for the patient with ED may lead the astute clinician to consider whether a change in current prescriptions might improve the man’s sexual function. Among the commonly used agents listed in Table 3, those with the greatest apparent impact on erections are thiazide diuretics and β-blockers, SSRIs, and tricyclic antidepressants.1,4
For a man who is interested in preserving potency, the clinician should select medications with the least effect on erectile function—for instance, an ACE inhibitor1 rather than a thiazide or β-blocker for the patient with hypertension. In the patient affected by depression, a trial of bupropion, substituted for or added to his current antidepressant, may be helpful.51 Medical therapies for hyperglycemia, hyperlipidemia, and hypertension should be considered if warranted, as should cardiovascular screening with exercise stress testing. (See box, “ED, CAD, and PDE-5 Inhibitors”52)
Alternative and Nonpharmacologic Options
A number of herbal products have been touted to improve sexual function. The FDA53 has issued press releases warning consumers about these and other alternatives to prescription medications. According to the FDA, many “sexual enhancement” products have been found to contain active ingredients resembling those found in one or more PDE-5 inhibitors. These products are in violation of federal law, and consumers are advised to avoid supplements that claim to produce effects similar to those of prescription drugs.53
By contrast, one potentially beneficial supplement currently under study is L-citrulline. As the body converts oral L-citrulline to L-arginine, vasodilation and endothelial function improve, often leading to resolution of mild ED. In a small, single-blind placebo-controlled study, patients who took L-citrulline (1.5 g/d in divided doses) reported improvement in hardness scale grading and increased satisfaction regarding sexual function. No adverse effects were reported, making L-citrulline a possible option for patients who hesitate to use a PDE-5 inhibitor.54
For patients with lack of response or contraindications to accepted medical therapy, other options include alprostadil intraurethral suppositories, penile prosthetic implants, vacuum erection devices, vascular surgery, yohimbine and other herbal therapies, and trazodone.1,14,55-59 These methods may require detailed counseling. Primary care providers who are unfamiliar with these modalities or reluctant to introduce them may wish to refer patients to urology.
PATIENT EDUCATION
Aggressive reduction in cardiovascular risks with smoking cessation, weight loss, and physical activity should be encouraged. In a study of obese men with ED (but without diabetes, hypertension, or hyperlipidemia), Esposito et al60 found that reducing caloric intake and increasing physical activity was associated with improved sexual function in about one-third of the subjects. Bicycle riders can decrease risks of perineal compression with newer seat designs.17
Smoking cessation alone has been shown to improve erectile function at one-year follow-up in at least 25% of men who stopped smoking, compared with none of the men who continued to smoke.61 Patients can help preserve endothelial function with efforts to maintain normal blood pressure and glycemic control.
Researchers are currently looking at occupational exposures as a cause of ED. Exposure to plastics containing bisphenol-A, for example, has been linked to decreased libido.62
CONCLUSION
In addition to addressing erectile dysfunction as a sexual problem, the health care provider should recognize its association with CVD, diabetes, depression, and other serious illnesses. However, it is also important to open a dialogue about sexual function to encourage the patient to discuss the problem of ED. Timely diagnosis and treatment of these conditions may be of even greater benefit to the patient than the effective therapies available for ED itself.
REFERENCES
1. McVary KT. Clinical practice: erectile dysfunction. N Engl J Med. 2007;357(24):2472-2481.
2. NIH Consensus Conference. Impotence: NIH Consensus Development Panel on Impotence. JAMA. 1993;270(1):83-90.
3. Hafez ES, Hafez SD. Erectile dysfunction: anatomical parameters, etiology, diagnosis, and therapy. Arch Androl. 2005;51(1):15-31.
4. Francis ME, Kusek JW, Nyberg LM, Eggers PW. The contribution of common medical conditions and drug exposures to erectile dysfunction in adult males. J Urol. 2007;178(2):591-596.
5. Saigal CS, Wessells H, Pace J, et al. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166 (2):207-212.
6. Rosen RC, Fisher WA, Eardley I, et al. The multinational Men’s Attitudes to Life Events and Sexuality (MALES) study. I. Prevalence of erectile dysfunction and related health concerns in the general population. Curr Med Res Opin. 2004;20 (5):607-617.
7. Lindau ST, Schumm LP, Laumann EO, et al. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357(8): 762-774.
8. Batty GD, Li Q, Czernichow S, et al. Erectile dysfunction and later cardiovascular disease in men with type 2 diabetes: prospective cohort study based on the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified-Release Controlled Evaluation) trial. J Am Coll Cardiol. 2010;56(23): 1908-1913.
9. Hodges LD, Kirby M, Solanki J, et al. The temporal relationship between erectile dysfunction and cardiovascular disease. Int J Clin Pract. 2007; 61(12):2019-2025.
10. Miner MM, Kuritzky L. Erectile dysfunction: a sentinel marker for cardiovascular disease in primary care. Cleve Clin J Med. 2007;74 suppl 3: S30-S37.
11. McCullough AR. An update on the PDE-5 inhibitors (PDE-5i). J Androl. 2003;24(6 suppl): S52-S58.
12. Rosen RC, Cappelleri JC, Smith MD, et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):
319-326.
13. Heidelbaugh JJ. Management of erectile dysfunction. Am Fam Physician. 2010;81(3):305-312.
14. Montague DK, Jarow JP, Broderick GA, et al; Erectile Dysfunction Guideline Update Panel. AUA guideline on the management of erectile dysfunction: an update (2006). American Urological Association Education and Research, Inc. www.auanet.org/content/guidelines-and-quality- care/clinical-guidelines.cfm?sub=ed. Accessed August 8, 2011.
15. Pohjantahti-Maaroos H, Palomäki A. Comparison of metabolic syndrome subjects with and without erectile dysfunction: levels of circulating oxidised LDL and arterial elasticity. Int J Clin Pract. 2011;65(3):274-280.
16. Lue TF. Male sexual dysfunction. In: Tanagho EA, McAninch JW, eds. Smith’s General Urology. 16th ed. San Francisco, CA: McGraw-Hill; 2004: 592-596.
17. Sommer F, Goldstein I, Korda JB. Bicycle riding and erectile dysfunction: a review. J Sex Med. 2010;7(7):2346-2358.
18. Feldman HA, Johannes CB, Derby CA, et al. Erectile dysfunction and coronary risk factors: prospective results from the Massachusetts male aging study. Prev Med. 2000;30(4):328-338.
19. Böhm M, Baumhäkel M, Probstfield JL, et al. Sexual function, satisfaction, and association of erectile dysfunction with cardiovascular disease and risk factors in cardiovascular high-risk patients: substudy of the ONgoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial/Telmisartan Randomized AssessmeNT Study in ACE-INtolerant Subjects with Cardiovascular Disease (ONTARGET/TRANSCEND). Am Heart J. 2007;154(1):94-101.
20. Athanasiadis L, Papaharitou S, Salpiggidis G, et al. Educating physicians to treat erectile dysfunction patients: development and evaluation of a course on communication and management strategies. J Sex Med. 2006;3(1):47-55.
21. Kennedy SH, Rizvi S. Sexual dysfunction, depression, and the impact of antidepressants.
J Clin Psychopharmacol. 2009;29(2):157-164.
22. Diaz VA Jr, Close JD. Male sexual dysfunction. Prim Care. 2010;37(3):473-489, vii-viii.
23. Carson CC, Lue TF. Phosphodiesterase type 5 inhibitors for erectile dysfunction. BJU Int. 2005; 96(3):257-280.
24. Qaseem A, Snow V, Denberg TD, et al. Hormonal testing and pharmacologic treatment of erectile dysfunction: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2009;151(9):630-649.
25. Dandona P, Rosenberg MT. A practical guide to male hypogonadism in the primary care setting. Int J Clin Pract. 2010;64(6):682-696.
26. Paick SH, Meehan A, Lee M, et al. The relationship among lower urinary tract symptoms, prostate specific antigen and erectile dysfunction in men with benign prostatic hyperplasia: results from the Proscar Long-Term Efficacy and Safety Study. J Urol. 2005;173(3):903-907.
27. Smith JF, Walsh TJ, Lue TF. Peyronie’s disease: a critical appraisal of current diagnosis and treatment. Int J Impot Res. 2008;20(5):445-459.
28. Gazzaruso C, Coppola A, Giustina A. Erectile dysfunction and coronary artery disease in patients with diabetes. Curr Diabetes Rev. 2011; 7(2):143-147.
29. Vlachopoulos C, Ioakeimidis N, Terentes-Printzios D, Stefanidis C. The triad: erectile dysfunction—endothelial dysfunction—cardiovascular disease. Curr Pharm Des. 2008;14(35): 3700-3704.
30. Makhlouf AA, Mohamed MA, Seftel AD, Niedergerger C. Hypogonadism is associated with overt depression symptoms in men with erectile dysfunction. Int J Impot Res. 2008;20(2): 157-161.
31. Corona G, Rastrelli G, Boddi V, et al. Prolactin levels independently predict major cardiovascular events in patients with erectile dysfunction. Int J Androl. 2011;34(3):217-224.
32. Vlachopoulos C, Rokkas K, Ioakeimidis N, Stefanadis C. Inflammation, metabolic syndrome, erectile dysfunction, and coronary artery disease: common links. Eur Urol. 2007;52(6):1590-1600.
33. LeRoy TJ, Broderick GA. Doppler blood flow analysis of erectile function: who, when, and how. Urol Clin North Am. 2011;38(2):147-154.
34. Aversa A, Sarteschi LM. J Sex Med. The role of penile color-duplex ultrasound for the evaluation of erectile dysfunction. J Sex Med. 2007;4(5): 1437-1447.
35. Fink HA, MacDonald R, Rutks IR, et al. Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med. 2002; 16(12):1349-1360.
36. Perimenis P, Roumeguere T, Heidler H, et al. Evaluation of patient expectations and treatment satisfaction after 1-year tadalafil therapy for erectile dysfunction: the DETECT study. J Sex Med. 2009;6(1):257-267.
37. Goldstein I, Kim E, Steers WD, et al. Efficacy and safety of tadalafil in men with erectile dysfunction with a high prevalence of comorbid conditions: results from MOMENTUS: multiple observations in men with erectile dysfunction in National Tadalafil Study in the US. J Sex Med. 2007;4(1):166-175.
38. Van Ahlen H, Zumbé J, Stauch K, Hanisch JU. The Real-Life Safety and Efficacy of vardenafil (REALISE) study: results in men from Europe and overseas with erectile dysfunction and cardiovascular or metabolic conditions. J Sex Med. 2010; 7(9):3161-3169.
39. Raheem AA, Kell P. Patient preference and satisfaction in erectile dysfunction therapy: a comparison of the three phosphodiesterase-5 inhibitors sildenafil, vardenafil and tadalafil. Patient Prefer Adherence. 2009;3:99-104.
40. Jannini EA, Isidori AM, Gravina GL, et al. The ENDOTRIAL study: a spontaneous, open-label, randomized, multicenter, crossover study on the efficacy of sildenafil, tadalafil, and vardenafil in the treatment of erectile dysfunction. J Sex Med. 2009;6(9):2547-2560.
41. Washington SL 3rd, Shindel AW. A once-daily dose of tadalafil for erectile dysfunction: compliance and efficacy. Drug Des Devel Ther. 2010 Sep 7;4:159-171.
42. Brock G, Glina S, Moncada I, et al. Likelihood of tadalafil-associated adverse events in integrated multiclinical trial database: classification tree analysis in men with erectile dysfunction. Urology. 2009;73(4):756-761.
43. Montorsi F, Avera A, Mocada I, et al. A randomized, double-blind, placebo-controlled, parallel study to assess the efficacy and safety of once-a-day tadalafil in men with erectile dysfunction who are naïve to PDE5 inhibitors. J Sex Med. 2011 Jun 27 [Epub ahead of print].
44. Rajagopalan P, Mazzu A, Xia C, et al. Effect of high-fat breakfast and moderate-fat evening meal on the pharmacokinetics of vardenafil, an oral phosphodiesterase-5 inhibitor for the treatment of erectile dysfunction. J Clin Pharmacol. 2003;43 (3):260-267.
45. Eardley I, Donatucci C, Corbin J, et al. Pharmacotherapy for erectile dysfunction. J Sex Med. 2010;7(1 pt 2):524-540.
46. Loran OB, Ströberg P, Lee SW, et al. Sildenafil citrate 100 mg starting dose in men with erectile dysfunction in an international, double-blind, placebo-controlled study: effect on the sexual experience and reducing feelings of anxiety about the next intercourse attempt. J Sex Med. 2009; 6(10):2826-2835.
47. Mihkail N. Does testosterone have a role in erectile function? Am J Med. 2006;119(5):373-382.
48. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82(1):20-28.
49. Shabsigh R, Kaufman JM, Steidle C, Padma-Nathan H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J Urol. 2004;172(2): 658-663.
50. Aversa A, Isidori AM, Spera G, et al. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin Endocrinol (Oxf). 2003;58(5):632-638.
51. Safarinejad MR. The effects of the adjunctive bupropion on male sexual dysfunction induced by a selective serotonin reuptake inhibitor: a double-blind placebo-controlled and randomized study. BJU Int. 2010;106(6):840-847.
52. Gazzaruso C, Solerte SB, Pujia A, et al. Erectile dysfunction as a predictor of cardiovascular events and death in diabetic patients with angiographically proven asymptomatic coronary artery disease: a potential protective role for statins and 5-phosphodiesterase inhibitors. J Am Coll Cardiol. 2008;51(21):2040-2044.
53. FDA. Tainted sexual enhancement products. www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsing MedicineSafely/MedicationHealthFraud/ucm234539.htm. Accessed August 8, 2011.
54. Cormio L, De Siati M, Lorusso F, et al. Oral L-citrulline supplementation improves erection hardness in men with mild erectile dysfunction. Urology. 2011;77(1):119-122.
55. Padma-Nathan H, Hellstrom WJ, Kaiser FE, et al. Treatment of men with erectile dysfunction with transurethral alprostadil: Medicated Urethral System for Erection (MUSE) Study Group. N Engl J Med. 1997;33(1)6:1-17.
56. Wolter CE, Hellstrom JG. The hydrophilic-coated penile prosthesis: 1-year experience. J Sex Med. 2004:1(2):221-224.
57. Yuan J, Hoang AN, Romero CA, et al. Vacuum therapy in erectile dysfunction: science and clinical evidence. Int J Impot Res. 2010;22(4):211-219.
58. Lebret T, Hervé JM, Gorny P, et al. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. Eur Urol. 2002; 41(6):608-613.
59. Fink HA, MacDonald R, Rutks IR, Wilt TJ. Trazodone for erectile dysfunction: a systematic review and meta-analysis. BJU Int. 2003;92(4): 441-446.
60. Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004;291(24):2978-2984.
61. Pourmand G, Alidaee M, Rasuli S, et al. Do cigarette smokers with erectile dysfunction benefit from stopping? A prospective study. BJU Int. 2004;94(9):1310-1313.
62. Li D, Zhou Z, Qing D, et al. Occupational exposure to bisphenol-A (BPA) and the risk of self-reported male sexual dysfunction. Hum Reprod. 2010;25(2):519-527.
Erectile dysfunction (ED) is defined as the recurrent inability, of three months’ duration or longer, to attain or maintain an erection sufficient for satisfactory sexual performance.1,2 It is classified as either psychogenic or organic; organic ED will be addressed here. Up to 80% of cases of organic ED can be further categorized into vascular, neurogenic, anatomic, or hormonal subtypes,2,3 with many affected patients vulnerable to potentially serious comorbidities and risk factors.
In the early 1990s, the NIH reported that nearly 30 million US men were affected by ED.2 However, increased public awareness of the condition, beginning with the availability of effective oral medications in the late 1990s, may have led to increased numbers of reported cases—and of men seeking treatment.
COMMON CONDITION, COMMONLY UNTREATED
According to results from the 2001-2002 National Health and Nutrition Examination Survey,4,5 ED affects about 8% of US men: 4% of those in their 50s, 17% of those in their 60s, 47% of men older than 65, and 78% of men 75 or older. More than 27,000 men from Europe and North and South America (ages 20 to 75) were interviewed for the 2004 Men’s Attitudes to Life Events and Sexuality (MALES) study; findings included an overall prevalence for ED of 16%, and 22% among men from the United States.6 See information regarding self-reported ED prevalence in Table 1.7
An important finding from the MALES study was that only 58% of respondents with self-reported ED had sought medical treatment for the condition.6 Some men may be reluctant to broach the subject with a health care provider because they consider ED a purely sexual problem—whereas the etiology is most commonly vascular.8 Thus, it is important for health care providers to include the sexual history as a routine component in the wellness exam for all patients, and to be aware of the potential presentation in patients with organic ED, appropriate work-up, and physical examination.
Additionally, ED can be a wake-up call for men at risk for cardiovascular disease (CVD); ED occurs at a mean time of five years before a cardiovascular event.9 Therefore, in addition to counseling patients with ED regarding treatment and prevention strategies, clinicians should be prepared to identify and address the risk factors and medical comorbidities associated with ED.
The Mechanisms of Erection
When sexual stimulation occurs, parasympathetic activity increases production of the nucleotide cyclic guanosine monophosphate (cGMP), resulting in relaxation of cavernosal smooth muscle and an influx of blood into the penis. This filling action produces expansion of the sinusoidal spaces in the penis, compressing venous channels and thereby preventing outflow of blood to allow maintenance of a rigid erection.10,11
Nitric oxide is needed for vasodilation of the corpora cavernosa. Inhibition of the enzyme phosphodiesterase type 5 (PDE-5) allows increased production and accumulation of penile cGMP. This results in relaxation of the smooth-muscle cells and improved erectile function.1,10,11
PRESENTATION, HISTORY, AND TYPES OF ORGANIC ED
In the primary care setting, the opportunity to assess for and address erectile function generally presents itself at the patient’s annual wellness visit—but could easily go unmentioned if the health care provider does not initiate the discussion. Direct questioning during the review of systems may ease any anxiety for the patient and open up a dialogue regarding other problems or medical conditions. (See box, “How and What To Ask,”12)
Providers can also assess the patient’s risk factors for ED and its associated comorbid conditions (see Table 21,13,14). The patient’s medical history may hold important clues to a diagnosis of organic ED.
Because certain vasculopathies, including diabetes, are known to accelerate the process of endothelial dysfunction, inquiries should be made into the sexual history of men with these disorders, regardless of age.10 Marked hyperlipidemia, uncontrolled hypertension, atherosclerosis, and other manifestations of CVD can impair erectile as well as endothelial function, leading to vascular ED.
The potential for atherosclerosis in the penile arteries (which are significantly narrower than the carotid, coronary, or femoral arteries) should prompt the primary care provider to evaluate the patient’s risk for vascular disease and its sequelae in the heart as well.8 (Of note, in one study of metabolic syndrome and ED, ED was found to be a predictor for impaired elasticity in the large arteries, independent of cardiovascular risk factors.15) In addition to damaging the small blood vessels and the endothelium, diabetes and other components of the metabolic syndrome contribute to ED by affecting cavernous nerve terminals and smooth muscle.1,14
Lifestyle factors, such as overconsumption of alcohol, smoking, recreational drug use, obesity, and inactivity can contribute to decreased libido and ED.14 Cigarette smoking can cause vasoconstriction and penile venous leak, resulting in poor erectile quality or even loss of erection. While small amounts of alcohol can improve libido and erection due to its anti-anxiety and vasodilatory effects, “more is not better” in this case, as higher doses result in sedation and decreased libido. Chronic alcoholism results in hypogonadism and polyneuropathy.16
Neurogenic ED can result from abnormalities at the level of the brain, the spinal cord, or the pelvis. Previous pelvic surgery, such as prostatectomy or colectomy, can disrupt the cavernous or pudendal nerves. Spinal cord injury, Parkinson’s disease, multiple sclerosis, diabetes with peripheral neuropathy, or a history of trauma can all result in neurogenic ED.16
Additionally, there is evidence of perineal compression from frequent bicycle riding leading to vascular, endothelial, and neurogenic dysfunction in men, with increased incidence of ED.17
Age alone is a risk factor for ED,7,18 as sexual function declines even in healthy men as they age. Penile sensitivity decreases, and there is increased latency between sexual stimulation and resulting erection, as well as between ejaculations. Ejaculations are less forceful, with less ejaculatory volume.16 Other factors that may affect the degree of ED include a history of stroke or pelvic surgery, especially in high-risk cardiac patients.19
Though not the focus of this article, the potential for psychogenic ED should be mentioned, as it warrants screening with a complete psychosocial history to rule out this etiology. The interview should allow time for the patient to discuss current or past relationship difficulties, marital conflict, life stressors, depression, and anxiety. Whatever the etiology of ED, the primary care provider should always elicit a sexual history, including number of sexual partners, current relationship status (ie, committed or casual), and incidence of ED with specific partners.20 The effects of ED on these relationships should be discussed.
A medication history is important for the ED workup. Antidepressants, especially the SSRIs, and certain hypertensives can affect the libido, arousal, and orgasm.21 See Table 31,13,22 for commonly used agents that can affect erectile function and sexual satisfaction.
Previous Medical History
The patient should be asked whether he has had any previous testing or treatment for ED. Was any therapy used effective? Did he experience any adverse effects during treatment? If treatment results were unsatisfactory, he should be questioned to ensure that he was using treatment correctly. Commonly, patients do not understand that sexual stimulation is necessary to achieve an erection when they are being treated with an oral PDE-5 inhibitor.23
PHYSICAL EXAMINATION
The clinician who performs the physical examination should take into account the psychogenic, neurogenic, and vasculogenic causes of ED. The genitourinary examination alone is not sufficient; abdominal, vascular, and neurologic exams must be included. The patient should be assessed for body habitus, secondary sex characteristics (including ruling out gynecomastia), and lower extremity pulses.22
The genitourinary exam should include testicular, rectal, and penile examination to rule out physical abnormalities. Small testicles (< 5 mL) or testicular atrophy on palpation should lead the examiner to consider testosterone testing24,25 (see “Diagnostic Testing,” below). A digital rectal examination may reveal an enlarged prostate (this finding, in the presence of lower urinary tract symptoms, has been associated with ED26). Palpation of the penis for plaques and questioning about pain with erection or deviation of the erect penis can lead to a diagnosis of Peyronie’s disease27; if this is the case, the patient can be referred to urology for treatment.
The vascular system should be assessed by listening for abdominal or femoral bruits and the lower extremities checked for appropriate hair growth, skin color, and distal pulses. The examiner should note any scars indicating a history of bypass surgery, which may have been overlooked during the surgical history.
DIAGNOSTIC TESTING
A fasting glucose level and a lipid profile should be routinely obtained because of the links between ED and diabetes and CVD.28,29 A chemistry panel and complete blood count, if one has not been performed recently, can be used to assess the patient’s general health, with a thyroid-stimulating hormone (TSH) level tested in men who report fatigue or weakness.
Men who are older than 50 should be considered for prostate-specific antigen (PSA) testing. Testosterone levels (free and total) are generally reserved for patients with small or atrophic testicles25 or for those who report decreased libido with fatigue or other symptoms of hypogonadism, including depression and decreased muscle strength, muscle mass, or vitality.22,24,25,30 If testosterone levels are ordered, the patient should be counseled to have samples drawn in the early morning to avoid the influence of daily hormonal fluctuations. In patients found to have low testosterone levels (ie, < 300 ng/dL,13 occurring in 12.5% to 35% of men with ED24), prolactin testing may be considered next; in patients with ED, hypoprolactinemia is associated with dyslipidemia, metabolic syndrome, and other risk factors for cardiovascular events.29,31,32
Imaging Studies
A number of imaging studies, once frequently used in evaluation for ED, are considered outdated and are no longer performed. However, Doppler blood flow analysis or ultrasonographic penile blood flow studies can be useful for identifying and evaluating the specific causes of vasculogenic ED, including arterial insufficiency and veno-occlusive disease.33,34 Other conditions associated with ED, such as Peyronie’s disease and priapism, can also be identified through these modalities.33
TREATMENT
The PDE-5 Inhibitors
While historically not the first treatment available for ED, medical therapy is certainly the most popular option for men with ED. The oral PDE-5 inhibitors first became available in the 1990s. All three such agents currently available in the US—sildenafil, tadalafil, and vardenafil—have been demonstrated effective in improving and maintaining erections,35-38 but their pharmacokinetics differ,39 and few head-to-head studies have been conducted that demonstrate greater efficacy of one agent over another.39,40 It has been suggested that patients try all three medications to determine preference and satisfaction.39
Qaseem et al24 report that PDE-5 inhibitors demonstrated clinical benefit regardless of baseline severity of dysfunction or ED cause, including diabetes and depression. These medications require sexual stimulation to be effective and typically are effective about one hour after dosing.23 Tadalafil is remarkable for the length of its half-life, which makes it appropriate at 2.5- or 5.0-mg doses for once-daily dosing41; it is also noted for a relatively low incidence of associated flushing,42 but back pain is more common among tadalafil users than among men using sildenafil or vardenafil.11,39,43
In addition to back pain and myalgia, the most common adverse effects associated with PDE-5 inhibitor use are dyspepsia, flushing, headache, and nasal congestion.42 Because absorption of sildenafil is reduced by food intake, and vardenafil44 to a lesser extent, these agents are best avoided in close proximity to meals. Absorption of tadalafil is not affected by food.45 Higher doses of sildenafil and vardenafil were associated with greater benefit in treating ED.24,46
Note: All three PDE-5 inhibitors are contraindicated in men taking long-acting nitrates or nitroglycerin.24 Their effectiveness may be potentiated by use of erythromycin, ketoconazole, and HIV protease inhibitors.39 Information about dosing options and adverse effects can be found in Table 411.
Testosterone
Hypogonadism, though found in only 5% of men with ED,47 may be an indication for testosterone replacement therapy, and testosterone use has been found to improve libido in men with sexual dysfunction.48 However, the authors of the American College of Physicians clinical practice guidelines24 found insufficient evidence that testosterone replacement improved erections or quality of sexual intercourse. There was also insufficient evidence that testosterone plus sildenafil was more effective than sildenafil alone.24,49,50
Additional Pharmacologic Considerations
A careful review of the medication history for the patient with ED may lead the astute clinician to consider whether a change in current prescriptions might improve the man’s sexual function. Among the commonly used agents listed in Table 3, those with the greatest apparent impact on erections are thiazide diuretics and β-blockers, SSRIs, and tricyclic antidepressants.1,4
For a man who is interested in preserving potency, the clinician should select medications with the least effect on erectile function—for instance, an ACE inhibitor1 rather than a thiazide or β-blocker for the patient with hypertension. In the patient affected by depression, a trial of bupropion, substituted for or added to his current antidepressant, may be helpful.51 Medical therapies for hyperglycemia, hyperlipidemia, and hypertension should be considered if warranted, as should cardiovascular screening with exercise stress testing. (See box, “ED, CAD, and PDE-5 Inhibitors”52)
Alternative and Nonpharmacologic Options
A number of herbal products have been touted to improve sexual function. The FDA53 has issued press releases warning consumers about these and other alternatives to prescription medications. According to the FDA, many “sexual enhancement” products have been found to contain active ingredients resembling those found in one or more PDE-5 inhibitors. These products are in violation of federal law, and consumers are advised to avoid supplements that claim to produce effects similar to those of prescription drugs.53
By contrast, one potentially beneficial supplement currently under study is L-citrulline. As the body converts oral L-citrulline to L-arginine, vasodilation and endothelial function improve, often leading to resolution of mild ED. In a small, single-blind placebo-controlled study, patients who took L-citrulline (1.5 g/d in divided doses) reported improvement in hardness scale grading and increased satisfaction regarding sexual function. No adverse effects were reported, making L-citrulline a possible option for patients who hesitate to use a PDE-5 inhibitor.54
For patients with lack of response or contraindications to accepted medical therapy, other options include alprostadil intraurethral suppositories, penile prosthetic implants, vacuum erection devices, vascular surgery, yohimbine and other herbal therapies, and trazodone.1,14,55-59 These methods may require detailed counseling. Primary care providers who are unfamiliar with these modalities or reluctant to introduce them may wish to refer patients to urology.
PATIENT EDUCATION
Aggressive reduction in cardiovascular risks with smoking cessation, weight loss, and physical activity should be encouraged. In a study of obese men with ED (but without diabetes, hypertension, or hyperlipidemia), Esposito et al60 found that reducing caloric intake and increasing physical activity was associated with improved sexual function in about one-third of the subjects. Bicycle riders can decrease risks of perineal compression with newer seat designs.17
Smoking cessation alone has been shown to improve erectile function at one-year follow-up in at least 25% of men who stopped smoking, compared with none of the men who continued to smoke.61 Patients can help preserve endothelial function with efforts to maintain normal blood pressure and glycemic control.
Researchers are currently looking at occupational exposures as a cause of ED. Exposure to plastics containing bisphenol-A, for example, has been linked to decreased libido.62
CONCLUSION
In addition to addressing erectile dysfunction as a sexual problem, the health care provider should recognize its association with CVD, diabetes, depression, and other serious illnesses. However, it is also important to open a dialogue about sexual function to encourage the patient to discuss the problem of ED. Timely diagnosis and treatment of these conditions may be of even greater benefit to the patient than the effective therapies available for ED itself.
REFERENCES
1. McVary KT. Clinical practice: erectile dysfunction. N Engl J Med. 2007;357(24):2472-2481.
2. NIH Consensus Conference. Impotence: NIH Consensus Development Panel on Impotence. JAMA. 1993;270(1):83-90.
3. Hafez ES, Hafez SD. Erectile dysfunction: anatomical parameters, etiology, diagnosis, and therapy. Arch Androl. 2005;51(1):15-31.
4. Francis ME, Kusek JW, Nyberg LM, Eggers PW. The contribution of common medical conditions and drug exposures to erectile dysfunction in adult males. J Urol. 2007;178(2):591-596.
5. Saigal CS, Wessells H, Pace J, et al. Predictors and prevalence of erectile dysfunction in a racially diverse population. Arch Intern Med. 2006;166 (2):207-212.
6. Rosen RC, Fisher WA, Eardley I, et al. The multinational Men’s Attitudes to Life Events and Sexuality (MALES) study. I. Prevalence of erectile dysfunction and related health concerns in the general population. Curr Med Res Opin. 2004;20 (5):607-617.
7. Lindau ST, Schumm LP, Laumann EO, et al. A study of sexuality and health among older adults in the United States. N Engl J Med. 2007;357(8): 762-774.
8. Batty GD, Li Q, Czernichow S, et al. Erectile dysfunction and later cardiovascular disease in men with type 2 diabetes: prospective cohort study based on the ADVANCE (Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified-Release Controlled Evaluation) trial. J Am Coll Cardiol. 2010;56(23): 1908-1913.
9. Hodges LD, Kirby M, Solanki J, et al. The temporal relationship between erectile dysfunction and cardiovascular disease. Int J Clin Pract. 2007; 61(12):2019-2025.
10. Miner MM, Kuritzky L. Erectile dysfunction: a sentinel marker for cardiovascular disease in primary care. Cleve Clin J Med. 2007;74 suppl 3: S30-S37.
11. McCullough AR. An update on the PDE-5 inhibitors (PDE-5i). J Androl. 2003;24(6 suppl): S52-S58.
12. Rosen RC, Cappelleri JC, Smith MD, et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):
319-326.
13. Heidelbaugh JJ. Management of erectile dysfunction. Am Fam Physician. 2010;81(3):305-312.
14. Montague DK, Jarow JP, Broderick GA, et al; Erectile Dysfunction Guideline Update Panel. AUA guideline on the management of erectile dysfunction: an update (2006). American Urological Association Education and Research, Inc. www.auanet.org/content/guidelines-and-quality- care/clinical-guidelines.cfm?sub=ed. Accessed August 8, 2011.
15. Pohjantahti-Maaroos H, Palomäki A. Comparison of metabolic syndrome subjects with and without erectile dysfunction: levels of circulating oxidised LDL and arterial elasticity. Int J Clin Pract. 2011;65(3):274-280.
16. Lue TF. Male sexual dysfunction. In: Tanagho EA, McAninch JW, eds. Smith’s General Urology. 16th ed. San Francisco, CA: McGraw-Hill; 2004: 592-596.
17. Sommer F, Goldstein I, Korda JB. Bicycle riding and erectile dysfunction: a review. J Sex Med. 2010;7(7):2346-2358.
18. Feldman HA, Johannes CB, Derby CA, et al. Erectile dysfunction and coronary risk factors: prospective results from the Massachusetts male aging study. Prev Med. 2000;30(4):328-338.
19. Böhm M, Baumhäkel M, Probstfield JL, et al. Sexual function, satisfaction, and association of erectile dysfunction with cardiovascular disease and risk factors in cardiovascular high-risk patients: substudy of the ONgoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trial/Telmisartan Randomized AssessmeNT Study in ACE-INtolerant Subjects with Cardiovascular Disease (ONTARGET/TRANSCEND). Am Heart J. 2007;154(1):94-101.
20. Athanasiadis L, Papaharitou S, Salpiggidis G, et al. Educating physicians to treat erectile dysfunction patients: development and evaluation of a course on communication and management strategies. J Sex Med. 2006;3(1):47-55.
21. Kennedy SH, Rizvi S. Sexual dysfunction, depression, and the impact of antidepressants.
J Clin Psychopharmacol. 2009;29(2):157-164.
22. Diaz VA Jr, Close JD. Male sexual dysfunction. Prim Care. 2010;37(3):473-489, vii-viii.
23. Carson CC, Lue TF. Phosphodiesterase type 5 inhibitors for erectile dysfunction. BJU Int. 2005; 96(3):257-280.
24. Qaseem A, Snow V, Denberg TD, et al. Hormonal testing and pharmacologic treatment of erectile dysfunction: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2009;151(9):630-649.
25. Dandona P, Rosenberg MT. A practical guide to male hypogonadism in the primary care setting. Int J Clin Pract. 2010;64(6):682-696.
26. Paick SH, Meehan A, Lee M, et al. The relationship among lower urinary tract symptoms, prostate specific antigen and erectile dysfunction in men with benign prostatic hyperplasia: results from the Proscar Long-Term Efficacy and Safety Study. J Urol. 2005;173(3):903-907.
27. Smith JF, Walsh TJ, Lue TF. Peyronie’s disease: a critical appraisal of current diagnosis and treatment. Int J Impot Res. 2008;20(5):445-459.
28. Gazzaruso C, Coppola A, Giustina A. Erectile dysfunction and coronary artery disease in patients with diabetes. Curr Diabetes Rev. 2011; 7(2):143-147.
29. Vlachopoulos C, Ioakeimidis N, Terentes-Printzios D, Stefanidis C. The triad: erectile dysfunction—endothelial dysfunction—cardiovascular disease. Curr Pharm Des. 2008;14(35): 3700-3704.
30. Makhlouf AA, Mohamed MA, Seftel AD, Niedergerger C. Hypogonadism is associated with overt depression symptoms in men with erectile dysfunction. Int J Impot Res. 2008;20(2): 157-161.
31. Corona G, Rastrelli G, Boddi V, et al. Prolactin levels independently predict major cardiovascular events in patients with erectile dysfunction. Int J Androl. 2011;34(3):217-224.
32. Vlachopoulos C, Rokkas K, Ioakeimidis N, Stefanadis C. Inflammation, metabolic syndrome, erectile dysfunction, and coronary artery disease: common links. Eur Urol. 2007;52(6):1590-1600.
33. LeRoy TJ, Broderick GA. Doppler blood flow analysis of erectile function: who, when, and how. Urol Clin North Am. 2011;38(2):147-154.
34. Aversa A, Sarteschi LM. J Sex Med. The role of penile color-duplex ultrasound for the evaluation of erectile dysfunction. J Sex Med. 2007;4(5): 1437-1447.
35. Fink HA, MacDonald R, Rutks IR, et al. Sildenafil for male erectile dysfunction: a systematic review and meta-analysis. Arch Intern Med. 2002; 16(12):1349-1360.
36. Perimenis P, Roumeguere T, Heidler H, et al. Evaluation of patient expectations and treatment satisfaction after 1-year tadalafil therapy for erectile dysfunction: the DETECT study. J Sex Med. 2009;6(1):257-267.
37. Goldstein I, Kim E, Steers WD, et al. Efficacy and safety of tadalafil in men with erectile dysfunction with a high prevalence of comorbid conditions: results from MOMENTUS: multiple observations in men with erectile dysfunction in National Tadalafil Study in the US. J Sex Med. 2007;4(1):166-175.
38. Van Ahlen H, Zumbé J, Stauch K, Hanisch JU. The Real-Life Safety and Efficacy of vardenafil (REALISE) study: results in men from Europe and overseas with erectile dysfunction and cardiovascular or metabolic conditions. J Sex Med. 2010; 7(9):3161-3169.
39. Raheem AA, Kell P. Patient preference and satisfaction in erectile dysfunction therapy: a comparison of the three phosphodiesterase-5 inhibitors sildenafil, vardenafil and tadalafil. Patient Prefer Adherence. 2009;3:99-104.
40. Jannini EA, Isidori AM, Gravina GL, et al. The ENDOTRIAL study: a spontaneous, open-label, randomized, multicenter, crossover study on the efficacy of sildenafil, tadalafil, and vardenafil in the treatment of erectile dysfunction. J Sex Med. 2009;6(9):2547-2560.
41. Washington SL 3rd, Shindel AW. A once-daily dose of tadalafil for erectile dysfunction: compliance and efficacy. Drug Des Devel Ther. 2010 Sep 7;4:159-171.
42. Brock G, Glina S, Moncada I, et al. Likelihood of tadalafil-associated adverse events in integrated multiclinical trial database: classification tree analysis in men with erectile dysfunction. Urology. 2009;73(4):756-761.
43. Montorsi F, Avera A, Mocada I, et al. A randomized, double-blind, placebo-controlled, parallel study to assess the efficacy and safety of once-a-day tadalafil in men with erectile dysfunction who are naïve to PDE5 inhibitors. J Sex Med. 2011 Jun 27 [Epub ahead of print].
44. Rajagopalan P, Mazzu A, Xia C, et al. Effect of high-fat breakfast and moderate-fat evening meal on the pharmacokinetics of vardenafil, an oral phosphodiesterase-5 inhibitor for the treatment of erectile dysfunction. J Clin Pharmacol. 2003;43 (3):260-267.
45. Eardley I, Donatucci C, Corbin J, et al. Pharmacotherapy for erectile dysfunction. J Sex Med. 2010;7(1 pt 2):524-540.
46. Loran OB, Ströberg P, Lee SW, et al. Sildenafil citrate 100 mg starting dose in men with erectile dysfunction in an international, double-blind, placebo-controlled study: effect on the sexual experience and reducing feelings of anxiety about the next intercourse attempt. J Sex Med. 2009; 6(10):2826-2835.
47. Mihkail N. Does testosterone have a role in erectile function? Am J Med. 2006;119(5):373-382.
48. Boloña ER, Uraga MV, Haddad RM, et al. Testosterone use in men with sexual dysfunction: a systematic review and meta-analysis of randomized placebo-controlled trials. Mayo Clin Proc. 2007;82(1):20-28.
49. Shabsigh R, Kaufman JM, Steidle C, Padma-Nathan H. Randomized study of testosterone gel as adjunctive therapy to sildenafil in hypogonadal men with erectile dysfunction who do not respond to sildenafil alone. J Urol. 2004;172(2): 658-663.
50. Aversa A, Isidori AM, Spera G, et al. Androgens improve cavernous vasodilation and response to sildenafil in patients with erectile dysfunction. Clin Endocrinol (Oxf). 2003;58(5):632-638.
51. Safarinejad MR. The effects of the adjunctive bupropion on male sexual dysfunction induced by a selective serotonin reuptake inhibitor: a double-blind placebo-controlled and randomized study. BJU Int. 2010;106(6):840-847.
52. Gazzaruso C, Solerte SB, Pujia A, et al. Erectile dysfunction as a predictor of cardiovascular events and death in diabetic patients with angiographically proven asymptomatic coronary artery disease: a potential protective role for statins and 5-phosphodiesterase inhibitors. J Am Coll Cardiol. 2008;51(21):2040-2044.
53. FDA. Tainted sexual enhancement products. www.fda.gov/Drugs/ResourcesForYou/Consumers/BuyingUsing MedicineSafely/MedicationHealthFraud/ucm234539.htm. Accessed August 8, 2011.
54. Cormio L, De Siati M, Lorusso F, et al. Oral L-citrulline supplementation improves erection hardness in men with mild erectile dysfunction. Urology. 2011;77(1):119-122.
55. Padma-Nathan H, Hellstrom WJ, Kaiser FE, et al. Treatment of men with erectile dysfunction with transurethral alprostadil: Medicated Urethral System for Erection (MUSE) Study Group. N Engl J Med. 1997;33(1)6:1-17.
56. Wolter CE, Hellstrom JG. The hydrophilic-coated penile prosthesis: 1-year experience. J Sex Med. 2004:1(2):221-224.
57. Yuan J, Hoang AN, Romero CA, et al. Vacuum therapy in erectile dysfunction: science and clinical evidence. Int J Impot Res. 2010;22(4):211-219.
58. Lebret T, Hervé JM, Gorny P, et al. Efficacy and safety of a novel combination of L-arginine glutamate and yohimbine hydrochloride: a new oral therapy for erectile dysfunction. Eur Urol. 2002; 41(6):608-613.
59. Fink HA, MacDonald R, Rutks IR, Wilt TJ. Trazodone for erectile dysfunction: a systematic review and meta-analysis. BJU Int. 2003;92(4): 441-446.
60. Esposito K, Giugliano F, Di Palo C, et al. Effect of lifestyle changes on erectile dysfunction in obese men: a randomized controlled trial. JAMA. 2004;291(24):2978-2984.
61. Pourmand G, Alidaee M, Rasuli S, et al. Do cigarette smokers with erectile dysfunction benefit from stopping? A prospective study. BJU Int. 2004;94(9):1310-1313.
62. Li D, Zhou Z, Qing D, et al. Occupational exposure to bisphenol-A (BPA) and the risk of self-reported male sexual dysfunction. Hum Reprod. 2010;25(2):519-527.