User login
Benign prostatic hyperplasia: Treat or wait?
- Talk to every male patient over the age of 50 about urinary function (C).
- Utilize questionnaires, such as the International Prostate Symptom Score to evaluate the patient's perception of symptom severity and quality of life (A).
- Rule out potential causes of lower urinary tract symptoms with a thorough medical history, focused physical exam (including digital rectal examination and neurological assessments), and appropriate laboratory evaluations (C).
- When choosing treatment for benign prostatic hyperplasia, remember that quality of life is generally more important than symptom severity (A).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
"My wife is mad at me—and she's worried, too," says Dan, a 65-year-old patient of yours. "She's been telling me to come see you, but I've been putting it off.
"I've been getting up 4 and 5 times a night to urinate, and we can't drive an hour without me having to stop at least once to use a restroom."
With a deep sigh, Dan says: "My wife is worried that I have cancer or something."
"And I'm worried, too," he admits.
Benign prostatic hyperplasia (BPH), and its clinical expression as lower urinary tract symptoms—urinary frequency, urgency, nocturia, decreased force of stream, and incomplete bladder emptying—comprise a major health concern for many older men. Approximately 50% of men over age 60 have at least microscopic BPH, while 90% over age 90 have evidence of the abnormality.1
Many men fail to seek help for lower urinary tract symptoms associated with BPH,2-4 even though these often moderate to severe symptoms are associated with decreased quality of life, anxiety, and depression.5 Your patient may be uncomfortable broaching the subject, as Dan was, for fear that he may have cancer. He may dismiss the symptoms as a natural consequence of aging,6 or he may believe that there are no effective treatments or that treatment will cause unwanted side effects.
Bring up the subject with all men over 50
To dispel these misconceptions and ensure that there are no current or ensuing serious complications,4 you should routinely talk about urinary function with every male patient over age 50. Because the incidence of BPH increases not only with age but also with other comorbid conditions such as diabetes7 and erectile dysfunction (ED),8 you should discuss the symptoms and potential complications of BPH with patients who present with these comorbidities. You can reassure them that BPH is not cancer, nor is it a precursor to prostate cancer; rather it is a fairly common, treatable disorder.
What's right for your patient? Watchful waiting? a-Blocker therapy? Surgery?

Questionnaire can help, addresses quality of life
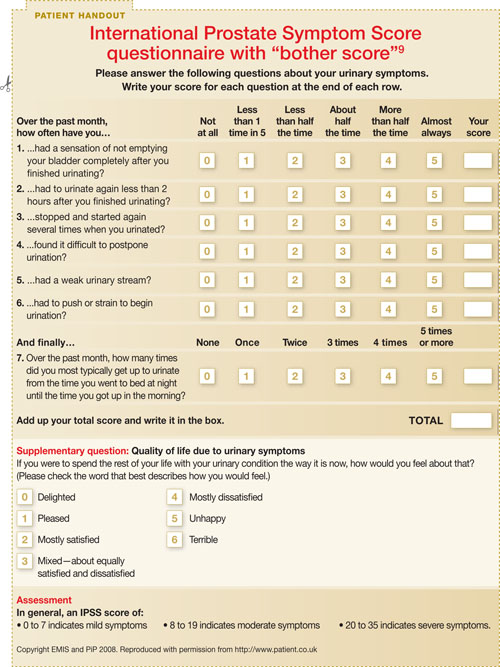
Questionnaires such as the International Prostate Symptom Score (IPSS) (PATIENT HANDOUT)9 and the similar American Urological Association symptom index (AUA-SI) (available on page 44 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf) can help you evaluate your patient's symptom severity.2,6
The IPSS, with 3 categories of symptom severity (mild 0 to 7, moderate 8 to 19, severe 20 to 35) and a global quality-of-life question also referred to as the "Bother Score," is a validated tool for monitoring disease distress and clinical change.10,11 The quality-of-life question is a good indicator for assessing whether watchful waiting might be preferred to active treatment.9,12
Further categorizing the symptoms is not helpful. Lower urinary tract symptoms have traditionally been divided into irritative symptoms such as nocturia, urgency, and frequency, attributed to bladder and prostatic smooth muscle contractions, and obstructive symptoms such as hesitancy, decreased force of stream, and incomplete emptying, attributed to increased glandular mass.1 This distinction, however, is not helpful inasmuch as irritative symptoms can result from increased tissue mass alone and obstructive symptoms from muscle hypertonicity alone; additionally, most BPH patients have a combination of both.13,14
Consider comorbidities and overactive bladder
Common comorbidities for a patient with BPH include obesity, diabetes mellitus, and low high-density lipoprotein levels. Both irritative and obstructive symptoms are likely, without prior lower urinary tract disorders or ongoing neurological disease.13-15 Multiple epidemiological studies have established clear, clinically relevant associations between BPH-related lower urinary tract symptoms and ED and ejaculatory dysfunction.8
It is also important to note that lower urinary tract symptoms may often arise due to overactive bladder; in fact, symptoms of overactive bladder and BPH overlap to a large degree.16 The diagnostic challenge is only increased by the fact that while overactive bladder is an additional cause of lower urinary tract symptoms, it may also coexist with BPH-related bladder outlet obstruction.17 The similarity in clinical presentation of the 2 conditions may make them hard to distinguish.
Rule out infection, urinary tract stones
There is general agreement about the need to exclude other potential etiologies of lower urinary tract symptoms in older men.4,15 Thus, you need to consider such causes as urinary tract stones, infections, or cancer; comorbid conditions that may affect bladder function or lead to polyuria; drug side effects; or sleep disturbances associated with chronic insomnia, depression, ethanol abuse, or sleep apnea.13,14
Digital rectal exam (DRE). The physical exam should include both a DRE and a search for neurological deficits to look for evidence that lower urinary tract symptoms are not BPH-related. The DRE should assess for stool impaction and prostate symmetry, nodularity, and consistency. Prostate volume estimates by DRE are not reliable and generally underestimate actual values while correlating poorly with BPH symptoms.14,18
Urinalysis. If you suspect BPH, you'll need to order a urinalysis to screen for infection, cancer, or stones and additional lab studies based on the patient's history, including measurements of serum creatinine, calcium, glucose, and prostate-specific antigen (PSA), among others.4,15
PSA values. These values should be checked if the patient's life expectancy is greater than a decade and a diagnosis of prostate cancer would influence treatment decisions. Adjustments of accepted norms should account for increasing age (40 to 50 years, 0-2.5 ng/mL; 51 to 60 years, 2.5-3.5 ng/mL; 61 to 70 years, 3.5-4.5 ng/mL; 71 to 80 years, 4.5-6.5 ng/mL), and urologic referral should be made as indicated.18
PSA determination is a more accurate reflection of prostate volume than a DRE and helps establish a pretreatment reference point before 5-a reductase inhibitor therapy.19 These drugs lower PSA concentrations approximately 50% and may complicate subsequent cancer screening.15
The US Preventive Services Task Force (USPSTF) clinical guidelines for prostate cancer screening notes that among patients with enlarged prostates, the specificity of PSA testing is lower, and thus PSA is a less accurate means of detecting cancer in BPH patients.20 Indeed, the USPSTF guidelines are ambivalent on the utility of PSA, in part because of the heterogeneity of prostate tumors, although they do confirm the greater accuracy of PSA testing over DRE.20
The guidelines state that screening is most effective at determining patients with a particularly good or poor long-term prognosis, which constitutes a fairly small minority of patients, but is less effective in the larger middle group.20 Regarding the particular means of testing PSA, the USPSTF guidelines note that free or complex testing is primarily useful to distinguish whether a patient should undergo a biopsy among those with a PSA level of 4.0 to 9.9 ng/mL.20 A more recent perspective from Cleveland Clinic clinicians indicates that the "PSA cutoff era" is now past and that decisions for further prostate cancer screening should be made with a patient's DRE and family history data in mind.21
Diagnostic studies. Noninvasive urine flow rates, postvoid residual measures, pressure-flow studies, cystoscopy, and renal or transrectal ultrasound are optional unless dictated by specific circumstances, including recurrent hematuria, pelvic pain, or urinary retention, in which case urologic consultation is indicated.4,15
Weigh patient preference against symptom severity
The treatment goals for a patient with BPH-related lower urinary tract symptoms must focus on improving and maintaining quality of life, achieving and sustaining symptom control, and avoiding disease progression.22 In choosing a specific treatment, weigh the patient's preferences against symptom severity and specific physiologic variables; even individuals with moderate IPSS ratings may improve (40%) or show no change (45%) with watchful waiting.23 (The AUA outlines treatment options for patients with moderate to severe symptoms in its BPH practice guidelines. They can be accessed on page 16 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Quality-of-life issues—how much lower urinary tract symptoms interfere with work, social life, sleep, sexual function, and travel—are generally more important than the symptoms per se.14 The AUA has published a diagnosis and treatment algorithm for BPH that is very helpful for practitioners.4 It is available on page 7 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Watchful waiting—even with high IPSS ratings
Watchful waiting is an option for patients experiencing minimal bother—even with high IPSS ratings—because the risk for progression is relatively small.4,14,15 If you choose this route, encourage the patient to minimize alcohol and caffeine use and the intake of fluids in the evening, and minimize the use of a-agonist, anticholinergic, antihistaminic, and calcium-channel blocker medications.
Where nocturia is a particular problem, diuretics timed to minimize night-time urine production, daytime naps, and use of antidiuretic hormones (although contraindicated in patients with congestive heart failure) may be appropriate.24,25 Notably, in the context of combined bladder outlet obstruction and detrusor overactivity validated by urodynamic studies, there are recent studies identifying a role for anticholinergics.26,27
Medical therapy before surgery
Medical therapy has supplanted surgery as the primary therapeutic tool for BPH-related lower urinary tract symptoms.4 a-Adrenergic antagonists decrease prostatic and urethral smooth muscle tone, induce tissue apoptosis through tumor growth factor-beta signaling, and increase detrusor muscle vascular supply, while 5-a reductase inhibitors block conversion of testosterone to dihydrotestosterone and reduce prostate volume ( TABLE ).4,14,15,28-40
a-Adrenergic blockers. Nonselective a-adrenergic blockers include terazosin, doxazosin, and alfuzosin. Their greater selectivity for nonprostatic peripheral vasculature a-1B receptors than for prostatic a-1A receptors account for their potential to cause orthostatic hypotension. A fourth agent, tamsulosin, is mostly selective for the prostatic a-1A receptor and does not have a clinically significant effect on blood pressure.30
At therapeutic doses, these drugs have comparable efficacy in lowering IPSS scores, increasing urine flow rates, and improving symptoms.4 Potential side effects include asthenia, headache, dizziness, and peripheral edema. Early postural hypotension and later rebound hypertension on withdrawal are primarily seen with terazosin and doxazosin, which require titration and tapering over 2 to 3 weeks when being introduced or eliminated. The uroselectivity of alfuzosin, as well as new dosing formulations, have helped reduce hypotensive side effects.28,29 Like tamsulosin, it can be started and stopped directly.
TABLE
Medical therapies for BPH at a glance4,14,15,28-40
| TYPE OF THERAPY | ACTIVITY | EFFICACY IN CLINICAL TRIALS | SIDE EFFECTS | INDICATIONS | NUMBER NEEDED TO TREAT* |
|---|---|---|---|---|---|
| a-Adrenergic blockers Nonselective Terazosin Doxazosin Alfuzosin Selective Tamsulosin |
|
|
|
| Terazosin 4.0 (to achieve >10% improvement in Boyarsky score, an older measure comparable to the IPSS)31 Doxazosin 13.7 (for the prevention of clinical progression)32 Alfuzosin 5.8 (to achieve =3 points improvement in IPSS)33 Tamsulosin 4.5 (to achieve =25% increase in AUA score)34 |
| 5- a Reductase inhibitors Dutasteride Finasteride |
|
| Dutasteride mild-to-moderate symptoms : 10 (to achieve 2-point improvement in AUA-SS) severe symptoms: 6.3 (to achieve 2-point improvement in AUA-SS)37,38 Finasteride 15.0 (for the prevention of clinical progression)32 | ||
| Combination therapy with a-Adrenergic blockers and 5-a reductase inhibitors |
|
|
| Combination of doxazosin + finasteride 8.4 (for the prevention of clinical progression)32 | |
| Phytotherapy Saw palmetto |
|
|
|
| N/A |
| *Number needed to treat (NNT) values should not be regarded as points of efficacy comparison since they are not consistently based on head-to-head trials, are derived from different patient populations, and may refer to different efficacy end points as well as different lengths of follow-up. | |||||
| AUA-SS, American Urological Association symptom score; BPH, benign prostatic hyperplasia; EAU, European Association of Urology; IPSS, International Prostate Symptom Score; LUTS, lower urinary tract symptoms; N/A, not available; PSA, prostate-specific antigen; QOL, quality of life. | |||||
Although infrequently reported in clinical trials, rhinitis and ejaculatory dysfunction are known side effects of tamsulosin and alfuzosin.30,41 a1-Blockers have recently been reported as possibly having an association with intraoperative floppy iris syndrome (IFIS), a surgical condition that has been observed during phacoemulsification cataract surgery.42 The etiology of this syndrome is unknown. Patients undergoing cataract surgery who are taking a1-blockers should inform their surgeons, who should be prepared for possible modifications to the surgical technique. The benefit of stopping a1-blocker therapy prior to cataract surgery has not been established.43-45
5- a Reductase inhibitors. Finasteride and dutasteride are comparable in efficacy and have been shown to decrease prostate volume (20%-30%), lower IPSS ratings 3 to 4 points, increase urine flow rates, and decrease urinary retention and the need for surgery (50%) when compared with placebo.15 Their clinical effect appears gradually over 3 to 6 months, and they are most beneficial when prostate volume exceeds 40 mL.35
Decreased libido (6%), ED (8%), and ejaculatory disorders (4%) are the main side effects of these drugs, as is their lowering of PSA levels by as much as half.15 This latter effect may prompt checking PSA velocities and free:total PSA ratios as a part of prostate cancer screening. Additionally, finasteride may reduce the prevalence of prostate cancer almost 25% compared with placebo, but more high-grade tumors may be associated with its use.36 The reason for this difference and its clinical importance require further study.36,46,47
Combination therapy. Combination therapy with a-adrenergic blockers and 5-a reductase inhibitors has increased due to results from the long-term (4.5 years) Medical Therapy of Prostatic Symptoms (MTOPS) study.32 It compared the efficacy of placebo, doxazosin, finasteride, and combination therapy on clinical progression measures of BPH. These were defined as an increase of 4 points on the IPSS, acute urinary retention, urinary incontinence, renal insufficiency, or recurrent urinary tract infections. All drug treatments significantly improved symptom scores, but the combination was clearly superior.32 Additionally, combination therapy and finasteride significantly reduced urinary retention and the need for surgery, whereas doxazosin did not.
The number needed to treat (NNT) for the prevention of a single instance of clinical progression over a 4-year period was 8.4 for combination therapy, compared with 13.7 for doxazosin monotherapy and 15.0 for finasteride monotherapy ( TABLE ).32
A secondary analysis, conducted to establish the NNT for disease progression in patients with larger baseline prostates or higher serum PSA, found that among patients with a PSA level >4.0 ng/mL, the NNT was 4.7 (vs 7.2 for finasteride), and for patients with a prostate volume >40 mL, the NNT was 4.9 (vs 7.2 for finasteride).32 These results suggest that patients with larger glands and higher PSA values, who are at greatest risk for progression, would benefit from combination approaches, although absolute threshold values are not yet clear.4
A combination of an a-adrenergic blocker and an anticholinergic medication may also be used in the treatment of comorbid lower urinary tract symptoms and overactive bladder. A 12-week placebo-controlled trial of a combination of tamsulosin and the anticholinergic tolterodine found significant benefits in terms of IPSS scores, urgency episodes, frequency of micturitions, quality-of-life scores, and patient perception of treatment benefit.48
Phytotherapy. Saw palmetto is derived from the ripe berries of the American dwarf palm (Serenoa repens or Sabal serrulata); retail sales in the United States totaled over $20 million in 2004.49 The mechanism of action is uncertain, but may involve antiandrogen activity. Short-term improvement of nocturia and peak urinary flow comparable with that of finasteride has been suggested by meta-analyses involving almost 3000 patients in trials ranging from 1 month to 1 year.39 However, neither American nor European guidelines recommend its use.4,15,40
A 6-month, double-blind, placebo-controlled trial of urtica dioica (stinging nettle) in 620 BPH patients found a significant improvement in IPSS scores, peak flow rates, and a small but significant reduction in prostate size among patients taking urtica dioica compared with baseline.50
Bothersome symptoms? Consider surgery
Transurethral resection of the prostate (TURP) was the primary surgical approach during most of the 20th century and remains the benchmark. TURP involves removing a portion of the prostate through the urethra.4 When compared with watchful waiting, TURP achieved better outcomes with men most bothered by symptoms at the outset. Watchful waiting was also considered safe, but 24% of this group underwent surgery during the 3 years. There were no increases in urinary incontinence or ED among surgically treated patients.51
TURP is indicated for patients with refractory urinary retention due to severe bladder outlet obstruction, recurrent urinary tract infections, progressive renal insufficiency, hematuria unresponsive to 5-a reductase inhibitors, bladder stones, and BPH-related hydronephrosis. Lower urinary tract symptom improvement is expected in 80% to 90% of cases, with a retained efficacy of 75% for at least 7 years and a risk of repeating surgery of only 1% annually.4,14,15 IPSS scores may decrease 15 to 20 points, but quality of life is enhanced only with severe lower urinary tract symptoms, and postoperative ejaculatory dysfunction (65%-70%) is expected, along with 1% to 2% perioperative mortality.15
It's important to note that TURP is a procedure that requires a hospital stay and is associated with a variety of potential side effects, including sexual dysfunction, bladder neck contracture, urinary tract infection, hematuria, and irritative voiding symptoms, while patients may also require blood transfusions.4,52
Other surgical therapies include open prostatectomies for patients with glands =80 mL and transurethral incision of the prostate (TUIP) for glands <30 mL.1,4,15 TUIP is a simpler outpatient operation than TURP. It offers equivalent symptomatic relief and less associated ejaculatory dysfunction or bleeding, but has a higher rate of reoperation.1,4,15 High-risk surgical candidates with severe urinary retention may also receive prostatic stents, but significant complications of pain, infection, and encrustation are common.4
Holmium laser enucleation of the prostate (HOLEP) is another alternative to TURP that has demonstrated equivalent efficacy in terms of AUA-SI scores, peak flow rates, and quality-of-life scores in studies of up to 3 years in length. Longer-term studies are required to determine its efficacy beyond that time frame.53-56
Minimally invasive route for high-risk patients
Transurethral needle ablation (TUNA) and transurethral microwave thermotherapy (TUMT) offer AUA-approved alternative treatment choices based on the severity of symptoms and the presence of complications.4 TUNA uses radiofrequency waves administered through 2 18-gauge needles to heat prostatic tissue. An outpatient procedure, TUNA is effective over the long term, demonstrating a low failure rate (25% after 5 years); however, temporary side effects such as irritative urinary symptoms and urinary retention can occur.4,57
With >100,000 procedures performed, TUMT is the most frequent minimally invasive treatment utilized worldwide. Heat destroys targeted prostatic tissue, while a cooling system protects the prostatic urethra. Its efficacy has been demonstrated by randomized trials, and its failure rate documented at 10% to 16% annually.4 Morbidity is related mainly to required indwelling catheterization for 4 to 6 weeks following intervention. However, it is an outpatient, low-risk procedure well-suited to high-risk patients or those who oppose surgery.
Correspondence
Darryl Chutka, MD, Division of Preventive and Occupational Medicine and Internal Medicine, Mayo Clinic College of Medicine, Rochester, MN 55905; [email protected].
1. Granville LJ. Prostate disease. In: Cobbs EL, Duthie EH, Murphy JB, eds. Geriatrics review syllabus: a core curriculum in geriatric medicine. 5th ed. Malden, Mass: Blackwell Publishing; 2002:384-385.
2. Collins MFM, Friedman RH, Ash A, Hall R, Moskowitz M. Underdetection of clinical benign prostatic hyperplasia in a general medical practice. J Gen Intern Med. 1996;11:513-518.
3. Hegarty NJ, Fitzpatrick JM. High intensity focused ultrasound in benign prostatic hyperplasia. Eur J Ultrasound. 1999;9:55-60.
4. AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagnosis and treatment recommendations. J Urol. 2003;170:530-547.
5. Welch G, Weinger K, Barry MJ. Quality-of-life impact of lower urinary tract symptom severity: results from the health professionals follow-up study. Urology. 2002;59:245-250.
6. Cunningham-Burley S, Allbutt, Garraway WM, Lee AJ, Russell EBAW. Perceptions of urinary symptoms and health-care-seeking behavior amongst men aged 40-79 years. Br J Gen Pract. 1996;46:349-352.
7. Wei JT, Calhoun E, Jacobsen SJ. Urologic diseases in America project: benign prostatic hyperplasia. J Urol. 2005;173:1256-1261.
8. Rosen RC, Giuliano F, Carson CC. Sexual dysfunction and lower urinary tract symptoms associated with benign prostatic hyperplasia. Eur Urol. 2005;47:824-837.
9. Assessing prostate symptoms. Patient UK. EMIS and Patient Information Publications 1997-2007. Available at: http://www.patient.co.uk/showdoc/23069171/. Accessed January 3, 2007.
10. O'Leary MP. Validity of the "bother score" in the evaluation and treatment of symptomatic benign prostatic hyperplasia. Rev Urol. 2005;7:1-10.
11. Barry MJ, Fowler FJ, Jr, O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, Cockett AT. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. 1992;148:1549-1557.
12. Barry MJ. Benign prostatic hyperplasia. In: Dale DC, Federman DD, eds. ACP Medicine. New York: WebMD; 2005.
13. Barry M, Roehrborn C. Management of benign prostate hyperplasia. Annu Rev Med. 1997;48:177-189.
14. Dubeau CE. Benign prostate disorders. In: Hazzard WR, Blass JP, Halter JB, Ouslander JG, Tinetti ME, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York: McGraw-Hill; 2003:1303-1310.
15. Madersbacher S, Alivizatos G, Nordling J, Sanz CR, Emberton M, de la Rosette JJ. EAU 2004 Guidelines on assessment, therapy and follow-up of men with lower urinary symptoms suggestive of benign prostatic obstruction (BPH Guidelines). Eur Urol. 2004;46:547-554.
16. Chapple CR, Roehrborn CG. A shifted paradigm for the further understanding, evaluation, and treatment of lower urinary tract symptoms in men: focus on the bladder. Eur Urol. 2006;49:651-659.
17. Knutson T, Edlund C, Fall M, Dahlstrand C. BPH with coexisting overactive bladder dysfunction—an everyday urological dilemma. Neurourol Urodyn. 2001;20:237-247.
18. Hellerstedt BA, Pienta KJ. In: Hazzard WR, Blass JP, Ouslander JG, Tinetti ME, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York: McGraw-Hill; 2003:1303-10.
19. Roehrborn CG, McConnell JD, Bonilla J, Rosenblatt S, et al. Serum prostate-specific antigen is a strong predictor of future prostate growth in men with benign prostatic hyperplasia: PROSCAR long-term efficacy and safety study. J Urol. 2000;163:13-20.
20. Harris R, Lohr KN. Screening for prostate cancer: an update of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137:917-929.
21. Jones JS, Klein E. Four no more: the 'PSA cutoff era' is over. Cleve Clin J Med. 2008;75:30-32.
22. O'Leary MP. Lower urinary tract symptoms/benign prostatic hyperplasia: Maintaining symptom control and reducing complications. Urology. 2003;62(Suppl 3A):15-23.
23. Oesterling JE. Benign prostatic hyperplasia: medical and minimally invasive treatment options. N Engl J Med. 1995;332:99-109.
24. Weiss JP, Blaivas JG. Nocturia. J Urol. 2000;163:5-12.
25. Reynard JM, Cannon A, Yang Q, Abrams P. A novel therapy for nocturnal polyuria: a double-blind randomized trial of furosemide against placebo. Br J Urol. 1998;81:215-218.
26. Abrams P, Kaplan S, De Konig Gans HJ, Millard R. Safety and tolerability of tolterodine for the treatment of overactive bladder in men with bladder outlet obstruction. J Urol. 2006;175:999-1004.
27. Athanasopoulos A, Gyftopoulos K, Giannitsas K, Fisfis J, Perimenis P, Barbalias G. Combination treatment with an alpha-blocker plus an anticholinergic for bladder outlet obstruction: a prospective, randomized controlled study. J Urol. 2003;169:2253-2256
28. van Kerrebroeck P, Jardin A, Laval KU, van Cangh P. Efficacy and safety of a new prolonged release formulation of alfuzosin 10 mg once daily versus alfuzosin 2.5 mg thrice daily and placebo in patients with symptomatic benign prostatic hyperplasia. Eur Urol. 2000;7:306-313.
29. Mottet N, Bressolle F, Delmas V, Robert M, Costa P. Prostatic tissual distribution of alfuzosin in patients with benign prostatic hyperplasia following repeated oral administration. Eur Urol. 2003;44:101-105.
30. Beduschi MC, Beduschi R, Oesterling JE. Alpha-blockade therapy for benign prostatic hyperplasia: from a nonselective to a more selective alpha1A-adrenergic antagonist. Urology. 1998;51:861-872.
31. Lepor H, Auerbach S, Puras-Baez A, et al. A randomized, placebo-controlled multicenter study of the efficacy and safety of terazosin in the treatment of benign prostatic hyperplasia. J Urol. 1992;148:1467-1474.
32. McConnell JD, Roehrborn CG, Bautista OM, et at. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387-2398.
33. Roehrborn CG. Efficacy and safety of once-daily alfuzosin in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a randomized, placebo-controlled trial. Urology. 2001;58:953-959.
34. Lepor H. Long-term evaluation of tamsulosin in benign prostatic hyperplasia: placebo-controlled, double-blind extension of phase III trial. Tamsulosin Investigator Group. Urology. 1998;51:901-906.
35. Clifford GM, Farmer RDT. Medical therapy for benign prostatic hyperplasia: a review of the literature. Eur Urol. 2000;38:2-19.
36. Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349:215-224.
37. Roehrborn CG. The clinical benefits of dutasteride treatment for LUTS and BPH. Rev Urol. 2004;6(Suppl 9):S22-SS30.
38. Roehrborn CG, Lukkarinen O, Mark S, Siami P, Ramsdell J, Zinner N. Long-term sustained improvement in symptoms of benign prostatic hyperplasia with the dual 5alpha-reductase inhibitor dutasteride: results of 4-year studies. BJU Int. 2005;96:572-577.
39. Edzard E. The risk-benefit profile of commonly used herbal therapies: ginkgo, St John's wort, ginseng, Echinacea, saw palmetto, and kava. Ann Intern Med. 2002;136:42-53.
40. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566.
41. Food and Drug Administration. ALFOTAM trial. Center for Drug Administration and Research. Available at: www.pbm.va.gov/criteria/Alpha-Blocker%20CFU%207-2005.pdf. Accessed November 16, 2006.
42. Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin. J Cataract Refract Surg. 2005;31:664-673.
43. Uroxatral [package insert]. Bridgewater, NJ: Sanofi-Aventis U.S.; 2007.
44. Cardura XL [package insert]. New York, NY: Pfizer Roerig; 2006.
45. Flomax [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2008.
46. Finasteride [package insert]. Whitehouse Station, NJ: Merck & Co. Inc.; 2007.
47. Dutasteride [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2005.
48. Kaplan SA, Roehrborn CG, Rovner ES, Carlsson M, Bavendam T, Guan Z. Tolterodine and tamsulosin for treatment of men with lower urinary tract symptoms and overactive bladder: a randomized controlled trial. JAMA. 2006;296:2319-2328.Erratum in: JAMA 2007; 297:1195.
49. Healing Herbs and Natural Remedies. Available at: http://www.herbsandnaturalremedies.com/topsellers.htm. Accessed January 3, 2007.
50. Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled, crossover study. J Herb Pharmacother. 2005;5:1-11.
51. Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. N Engl J Med. 1995;332:75-79.
52. Hammadeh MY, Madaan S, Hines J, Philp T. 5-year outcome of a prospective randomized trial to compare transurethral electrovaporization of the prostate and standard transurethral resection. Urology. 2003;61:1166-1171.
53. Ahyai SA, Lehrich K, Kuntz RM. Holmium laser enucleation versus transurethral resection of the prostate: 3-year follow-up results of a randomized clinical trial. Eur Urol. 2007;52:1456-1464.
54. Kuntz RM. Laser treatment of benign prostatic hyperplasia. World J Urol. 2007;25:241-247.
55. Gupta N, Sivaramakrishna, Kumar R, Dogra PN, Seth A. Comparison of standard transurethral resection, transurethral vapour resection and holmium laser enucleation of the prostate for managing benign prostatic hyperplasia of >40 g. BJU Int. 2006;97:85-89.
56. Tan AH, Gilling PJ, Kennett KM, Frampton C, Westenberg AM, Fraundorfer MR. A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). J Urol. 2003;170(4 Pt 1):1270-1274.
57. Zlotta AR, Giannakopoulos X, Maehlum O, Ostrem T, Schulman CC. Long-term evaluation of transurethral needle ablation of the prostate (TUNA) for treatment of symptomatic benign prostatic hyperplasia: clinical outcome up to five years from three centers. Eur Urol. 2003;44:89-93.
- Talk to every male patient over the age of 50 about urinary function (C).
- Utilize questionnaires, such as the International Prostate Symptom Score to evaluate the patient's perception of symptom severity and quality of life (A).
- Rule out potential causes of lower urinary tract symptoms with a thorough medical history, focused physical exam (including digital rectal examination and neurological assessments), and appropriate laboratory evaluations (C).
- When choosing treatment for benign prostatic hyperplasia, remember that quality of life is generally more important than symptom severity (A).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
"My wife is mad at me—and she's worried, too," says Dan, a 65-year-old patient of yours. "She's been telling me to come see you, but I've been putting it off.
"I've been getting up 4 and 5 times a night to urinate, and we can't drive an hour without me having to stop at least once to use a restroom."
With a deep sigh, Dan says: "My wife is worried that I have cancer or something."
"And I'm worried, too," he admits.
Benign prostatic hyperplasia (BPH), and its clinical expression as lower urinary tract symptoms—urinary frequency, urgency, nocturia, decreased force of stream, and incomplete bladder emptying—comprise a major health concern for many older men. Approximately 50% of men over age 60 have at least microscopic BPH, while 90% over age 90 have evidence of the abnormality.1
Many men fail to seek help for lower urinary tract symptoms associated with BPH,2-4 even though these often moderate to severe symptoms are associated with decreased quality of life, anxiety, and depression.5 Your patient may be uncomfortable broaching the subject, as Dan was, for fear that he may have cancer. He may dismiss the symptoms as a natural consequence of aging,6 or he may believe that there are no effective treatments or that treatment will cause unwanted side effects.
Bring up the subject with all men over 50
To dispel these misconceptions and ensure that there are no current or ensuing serious complications,4 you should routinely talk about urinary function with every male patient over age 50. Because the incidence of BPH increases not only with age but also with other comorbid conditions such as diabetes7 and erectile dysfunction (ED),8 you should discuss the symptoms and potential complications of BPH with patients who present with these comorbidities. You can reassure them that BPH is not cancer, nor is it a precursor to prostate cancer; rather it is a fairly common, treatable disorder.
What's right for your patient? Watchful waiting? a-Blocker therapy? Surgery?
Questionnaire can help, addresses quality of life
Questionnaires such as the International Prostate Symptom Score (IPSS) (PATIENT HANDOUT)9 and the similar American Urological Association symptom index (AUA-SI) (available on page 44 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf) can help you evaluate your patient's symptom severity.2,6
The IPSS, with 3 categories of symptom severity (mild 0 to 7, moderate 8 to 19, severe 20 to 35) and a global quality-of-life question also referred to as the "Bother Score," is a validated tool for monitoring disease distress and clinical change.10,11 The quality-of-life question is a good indicator for assessing whether watchful waiting might be preferred to active treatment.9,12
Further categorizing the symptoms is not helpful. Lower urinary tract symptoms have traditionally been divided into irritative symptoms such as nocturia, urgency, and frequency, attributed to bladder and prostatic smooth muscle contractions, and obstructive symptoms such as hesitancy, decreased force of stream, and incomplete emptying, attributed to increased glandular mass.1 This distinction, however, is not helpful inasmuch as irritative symptoms can result from increased tissue mass alone and obstructive symptoms from muscle hypertonicity alone; additionally, most BPH patients have a combination of both.13,14
Consider comorbidities and overactive bladder
Common comorbidities for a patient with BPH include obesity, diabetes mellitus, and low high-density lipoprotein levels. Both irritative and obstructive symptoms are likely, without prior lower urinary tract disorders or ongoing neurological disease.13-15 Multiple epidemiological studies have established clear, clinically relevant associations between BPH-related lower urinary tract symptoms and ED and ejaculatory dysfunction.8
It is also important to note that lower urinary tract symptoms may often arise due to overactive bladder; in fact, symptoms of overactive bladder and BPH overlap to a large degree.16 The diagnostic challenge is only increased by the fact that while overactive bladder is an additional cause of lower urinary tract symptoms, it may also coexist with BPH-related bladder outlet obstruction.17 The similarity in clinical presentation of the 2 conditions may make them hard to distinguish.
Rule out infection, urinary tract stones
There is general agreement about the need to exclude other potential etiologies of lower urinary tract symptoms in older men.4,15 Thus, you need to consider such causes as urinary tract stones, infections, or cancer; comorbid conditions that may affect bladder function or lead to polyuria; drug side effects; or sleep disturbances associated with chronic insomnia, depression, ethanol abuse, or sleep apnea.13,14
Digital rectal exam (DRE). The physical exam should include both a DRE and a search for neurological deficits to look for evidence that lower urinary tract symptoms are not BPH-related. The DRE should assess for stool impaction and prostate symmetry, nodularity, and consistency. Prostate volume estimates by DRE are not reliable and generally underestimate actual values while correlating poorly with BPH symptoms.14,18
Urinalysis. If you suspect BPH, you'll need to order a urinalysis to screen for infection, cancer, or stones and additional lab studies based on the patient's history, including measurements of serum creatinine, calcium, glucose, and prostate-specific antigen (PSA), among others.4,15
PSA values. These values should be checked if the patient's life expectancy is greater than a decade and a diagnosis of prostate cancer would influence treatment decisions. Adjustments of accepted norms should account for increasing age (40 to 50 years, 0-2.5 ng/mL; 51 to 60 years, 2.5-3.5 ng/mL; 61 to 70 years, 3.5-4.5 ng/mL; 71 to 80 years, 4.5-6.5 ng/mL), and urologic referral should be made as indicated.18
PSA determination is a more accurate reflection of prostate volume than a DRE and helps establish a pretreatment reference point before 5-a reductase inhibitor therapy.19 These drugs lower PSA concentrations approximately 50% and may complicate subsequent cancer screening.15
The US Preventive Services Task Force (USPSTF) clinical guidelines for prostate cancer screening notes that among patients with enlarged prostates, the specificity of PSA testing is lower, and thus PSA is a less accurate means of detecting cancer in BPH patients.20 Indeed, the USPSTF guidelines are ambivalent on the utility of PSA, in part because of the heterogeneity of prostate tumors, although they do confirm the greater accuracy of PSA testing over DRE.20
The guidelines state that screening is most effective at determining patients with a particularly good or poor long-term prognosis, which constitutes a fairly small minority of patients, but is less effective in the larger middle group.20 Regarding the particular means of testing PSA, the USPSTF guidelines note that free or complex testing is primarily useful to distinguish whether a patient should undergo a biopsy among those with a PSA level of 4.0 to 9.9 ng/mL.20 A more recent perspective from Cleveland Clinic clinicians indicates that the "PSA cutoff era" is now past and that decisions for further prostate cancer screening should be made with a patient's DRE and family history data in mind.21
Diagnostic studies. Noninvasive urine flow rates, postvoid residual measures, pressure-flow studies, cystoscopy, and renal or transrectal ultrasound are optional unless dictated by specific circumstances, including recurrent hematuria, pelvic pain, or urinary retention, in which case urologic consultation is indicated.4,15
Weigh patient preference against symptom severity
The treatment goals for a patient with BPH-related lower urinary tract symptoms must focus on improving and maintaining quality of life, achieving and sustaining symptom control, and avoiding disease progression.22 In choosing a specific treatment, weigh the patient's preferences against symptom severity and specific physiologic variables; even individuals with moderate IPSS ratings may improve (40%) or show no change (45%) with watchful waiting.23 (The AUA outlines treatment options for patients with moderate to severe symptoms in its BPH practice guidelines. They can be accessed on page 16 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Quality-of-life issues—how much lower urinary tract symptoms interfere with work, social life, sleep, sexual function, and travel—are generally more important than the symptoms per se.14 The AUA has published a diagnosis and treatment algorithm for BPH that is very helpful for practitioners.4 It is available on page 7 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Watchful waiting—even with high IPSS ratings
Watchful waiting is an option for patients experiencing minimal bother—even with high IPSS ratings—because the risk for progression is relatively small.4,14,15 If you choose this route, encourage the patient to minimize alcohol and caffeine use and the intake of fluids in the evening, and minimize the use of a-agonist, anticholinergic, antihistaminic, and calcium-channel blocker medications.
Where nocturia is a particular problem, diuretics timed to minimize night-time urine production, daytime naps, and use of antidiuretic hormones (although contraindicated in patients with congestive heart failure) may be appropriate.24,25 Notably, in the context of combined bladder outlet obstruction and detrusor overactivity validated by urodynamic studies, there are recent studies identifying a role for anticholinergics.26,27
Medical therapy before surgery
Medical therapy has supplanted surgery as the primary therapeutic tool for BPH-related lower urinary tract symptoms.4 a-Adrenergic antagonists decrease prostatic and urethral smooth muscle tone, induce tissue apoptosis through tumor growth factor-beta signaling, and increase detrusor muscle vascular supply, while 5-a reductase inhibitors block conversion of testosterone to dihydrotestosterone and reduce prostate volume ( TABLE ).4,14,15,28-40
a-Adrenergic blockers. Nonselective a-adrenergic blockers include terazosin, doxazosin, and alfuzosin. Their greater selectivity for nonprostatic peripheral vasculature a-1B receptors than for prostatic a-1A receptors account for their potential to cause orthostatic hypotension. A fourth agent, tamsulosin, is mostly selective for the prostatic a-1A receptor and does not have a clinically significant effect on blood pressure.30
At therapeutic doses, these drugs have comparable efficacy in lowering IPSS scores, increasing urine flow rates, and improving symptoms.4 Potential side effects include asthenia, headache, dizziness, and peripheral edema. Early postural hypotension and later rebound hypertension on withdrawal are primarily seen with terazosin and doxazosin, which require titration and tapering over 2 to 3 weeks when being introduced or eliminated. The uroselectivity of alfuzosin, as well as new dosing formulations, have helped reduce hypotensive side effects.28,29 Like tamsulosin, it can be started and stopped directly.
TABLE
Medical therapies for BPH at a glance4,14,15,28-40
| TYPE OF THERAPY | ACTIVITY | EFFICACY IN CLINICAL TRIALS | SIDE EFFECTS | INDICATIONS | NUMBER NEEDED TO TREAT* |
|---|---|---|---|---|---|
| a-Adrenergic blockers Nonselective Terazosin Doxazosin Alfuzosin Selective Tamsulosin |
|
|
|
| Terazosin 4.0 (to achieve >10% improvement in Boyarsky score, an older measure comparable to the IPSS)31 Doxazosin 13.7 (for the prevention of clinical progression)32 Alfuzosin 5.8 (to achieve =3 points improvement in IPSS)33 Tamsulosin 4.5 (to achieve =25% increase in AUA score)34 |
| 5- a Reductase inhibitors Dutasteride Finasteride |
|
| Dutasteride mild-to-moderate symptoms : 10 (to achieve 2-point improvement in AUA-SS) severe symptoms: 6.3 (to achieve 2-point improvement in AUA-SS)37,38 Finasteride 15.0 (for the prevention of clinical progression)32 | ||
| Combination therapy with a-Adrenergic blockers and 5-a reductase inhibitors |
|
|
| Combination of doxazosin + finasteride 8.4 (for the prevention of clinical progression)32 | |
| Phytotherapy Saw palmetto |
|
|
|
| N/A |
| *Number needed to treat (NNT) values should not be regarded as points of efficacy comparison since they are not consistently based on head-to-head trials, are derived from different patient populations, and may refer to different efficacy end points as well as different lengths of follow-up. | |||||
| AUA-SS, American Urological Association symptom score; BPH, benign prostatic hyperplasia; EAU, European Association of Urology; IPSS, International Prostate Symptom Score; LUTS, lower urinary tract symptoms; N/A, not available; PSA, prostate-specific antigen; QOL, quality of life. | |||||
Although infrequently reported in clinical trials, rhinitis and ejaculatory dysfunction are known side effects of tamsulosin and alfuzosin.30,41 a1-Blockers have recently been reported as possibly having an association with intraoperative floppy iris syndrome (IFIS), a surgical condition that has been observed during phacoemulsification cataract surgery.42 The etiology of this syndrome is unknown. Patients undergoing cataract surgery who are taking a1-blockers should inform their surgeons, who should be prepared for possible modifications to the surgical technique. The benefit of stopping a1-blocker therapy prior to cataract surgery has not been established.43-45
5- a Reductase inhibitors. Finasteride and dutasteride are comparable in efficacy and have been shown to decrease prostate volume (20%-30%), lower IPSS ratings 3 to 4 points, increase urine flow rates, and decrease urinary retention and the need for surgery (50%) when compared with placebo.15 Their clinical effect appears gradually over 3 to 6 months, and they are most beneficial when prostate volume exceeds 40 mL.35
Decreased libido (6%), ED (8%), and ejaculatory disorders (4%) are the main side effects of these drugs, as is their lowering of PSA levels by as much as half.15 This latter effect may prompt checking PSA velocities and free:total PSA ratios as a part of prostate cancer screening. Additionally, finasteride may reduce the prevalence of prostate cancer almost 25% compared with placebo, but more high-grade tumors may be associated with its use.36 The reason for this difference and its clinical importance require further study.36,46,47
Combination therapy. Combination therapy with a-adrenergic blockers and 5-a reductase inhibitors has increased due to results from the long-term (4.5 years) Medical Therapy of Prostatic Symptoms (MTOPS) study.32 It compared the efficacy of placebo, doxazosin, finasteride, and combination therapy on clinical progression measures of BPH. These were defined as an increase of 4 points on the IPSS, acute urinary retention, urinary incontinence, renal insufficiency, or recurrent urinary tract infections. All drug treatments significantly improved symptom scores, but the combination was clearly superior.32 Additionally, combination therapy and finasteride significantly reduced urinary retention and the need for surgery, whereas doxazosin did not.
The number needed to treat (NNT) for the prevention of a single instance of clinical progression over a 4-year period was 8.4 for combination therapy, compared with 13.7 for doxazosin monotherapy and 15.0 for finasteride monotherapy ( TABLE ).32
A secondary analysis, conducted to establish the NNT for disease progression in patients with larger baseline prostates or higher serum PSA, found that among patients with a PSA level >4.0 ng/mL, the NNT was 4.7 (vs 7.2 for finasteride), and for patients with a prostate volume >40 mL, the NNT was 4.9 (vs 7.2 for finasteride).32 These results suggest that patients with larger glands and higher PSA values, who are at greatest risk for progression, would benefit from combination approaches, although absolute threshold values are not yet clear.4
A combination of an a-adrenergic blocker and an anticholinergic medication may also be used in the treatment of comorbid lower urinary tract symptoms and overactive bladder. A 12-week placebo-controlled trial of a combination of tamsulosin and the anticholinergic tolterodine found significant benefits in terms of IPSS scores, urgency episodes, frequency of micturitions, quality-of-life scores, and patient perception of treatment benefit.48
Phytotherapy. Saw palmetto is derived from the ripe berries of the American dwarf palm (Serenoa repens or Sabal serrulata); retail sales in the United States totaled over $20 million in 2004.49 The mechanism of action is uncertain, but may involve antiandrogen activity. Short-term improvement of nocturia and peak urinary flow comparable with that of finasteride has been suggested by meta-analyses involving almost 3000 patients in trials ranging from 1 month to 1 year.39 However, neither American nor European guidelines recommend its use.4,15,40
A 6-month, double-blind, placebo-controlled trial of urtica dioica (stinging nettle) in 620 BPH patients found a significant improvement in IPSS scores, peak flow rates, and a small but significant reduction in prostate size among patients taking urtica dioica compared with baseline.50
Bothersome symptoms? Consider surgery
Transurethral resection of the prostate (TURP) was the primary surgical approach during most of the 20th century and remains the benchmark. TURP involves removing a portion of the prostate through the urethra.4 When compared with watchful waiting, TURP achieved better outcomes with men most bothered by symptoms at the outset. Watchful waiting was also considered safe, but 24% of this group underwent surgery during the 3 years. There were no increases in urinary incontinence or ED among surgically treated patients.51
TURP is indicated for patients with refractory urinary retention due to severe bladder outlet obstruction, recurrent urinary tract infections, progressive renal insufficiency, hematuria unresponsive to 5-a reductase inhibitors, bladder stones, and BPH-related hydronephrosis. Lower urinary tract symptom improvement is expected in 80% to 90% of cases, with a retained efficacy of 75% for at least 7 years and a risk of repeating surgery of only 1% annually.4,14,15 IPSS scores may decrease 15 to 20 points, but quality of life is enhanced only with severe lower urinary tract symptoms, and postoperative ejaculatory dysfunction (65%-70%) is expected, along with 1% to 2% perioperative mortality.15
It's important to note that TURP is a procedure that requires a hospital stay and is associated with a variety of potential side effects, including sexual dysfunction, bladder neck contracture, urinary tract infection, hematuria, and irritative voiding symptoms, while patients may also require blood transfusions.4,52
Other surgical therapies include open prostatectomies for patients with glands =80 mL and transurethral incision of the prostate (TUIP) for glands <30 mL.1,4,15 TUIP is a simpler outpatient operation than TURP. It offers equivalent symptomatic relief and less associated ejaculatory dysfunction or bleeding, but has a higher rate of reoperation.1,4,15 High-risk surgical candidates with severe urinary retention may also receive prostatic stents, but significant complications of pain, infection, and encrustation are common.4
Holmium laser enucleation of the prostate (HOLEP) is another alternative to TURP that has demonstrated equivalent efficacy in terms of AUA-SI scores, peak flow rates, and quality-of-life scores in studies of up to 3 years in length. Longer-term studies are required to determine its efficacy beyond that time frame.53-56
Minimally invasive route for high-risk patients
Transurethral needle ablation (TUNA) and transurethral microwave thermotherapy (TUMT) offer AUA-approved alternative treatment choices based on the severity of symptoms and the presence of complications.4 TUNA uses radiofrequency waves administered through 2 18-gauge needles to heat prostatic tissue. An outpatient procedure, TUNA is effective over the long term, demonstrating a low failure rate (25% after 5 years); however, temporary side effects such as irritative urinary symptoms and urinary retention can occur.4,57
With >100,000 procedures performed, TUMT is the most frequent minimally invasive treatment utilized worldwide. Heat destroys targeted prostatic tissue, while a cooling system protects the prostatic urethra. Its efficacy has been demonstrated by randomized trials, and its failure rate documented at 10% to 16% annually.4 Morbidity is related mainly to required indwelling catheterization for 4 to 6 weeks following intervention. However, it is an outpatient, low-risk procedure well-suited to high-risk patients or those who oppose surgery.
Correspondence
Darryl Chutka, MD, Division of Preventive and Occupational Medicine and Internal Medicine, Mayo Clinic College of Medicine, Rochester, MN 55905; [email protected].
- Talk to every male patient over the age of 50 about urinary function (C).
- Utilize questionnaires, such as the International Prostate Symptom Score to evaluate the patient's perception of symptom severity and quality of life (A).
- Rule out potential causes of lower urinary tract symptoms with a thorough medical history, focused physical exam (including digital rectal examination and neurological assessments), and appropriate laboratory evaluations (C).
- When choosing treatment for benign prostatic hyperplasia, remember that quality of life is generally more important than symptom severity (A).
Strength of recommendation (SOR)
- Good quality patient-oriented evidence
- Inconsistent or limited-quality patient-oriented evidence
- Consensus, usual practice, opinion, disease-oriented evidence, case series
"My wife is mad at me—and she's worried, too," says Dan, a 65-year-old patient of yours. "She's been telling me to come see you, but I've been putting it off.
"I've been getting up 4 and 5 times a night to urinate, and we can't drive an hour without me having to stop at least once to use a restroom."
With a deep sigh, Dan says: "My wife is worried that I have cancer or something."
"And I'm worried, too," he admits.
Benign prostatic hyperplasia (BPH), and its clinical expression as lower urinary tract symptoms—urinary frequency, urgency, nocturia, decreased force of stream, and incomplete bladder emptying—comprise a major health concern for many older men. Approximately 50% of men over age 60 have at least microscopic BPH, while 90% over age 90 have evidence of the abnormality.1
Many men fail to seek help for lower urinary tract symptoms associated with BPH,2-4 even though these often moderate to severe symptoms are associated with decreased quality of life, anxiety, and depression.5 Your patient may be uncomfortable broaching the subject, as Dan was, for fear that he may have cancer. He may dismiss the symptoms as a natural consequence of aging,6 or he may believe that there are no effective treatments or that treatment will cause unwanted side effects.
Bring up the subject with all men over 50
To dispel these misconceptions and ensure that there are no current or ensuing serious complications,4 you should routinely talk about urinary function with every male patient over age 50. Because the incidence of BPH increases not only with age but also with other comorbid conditions such as diabetes7 and erectile dysfunction (ED),8 you should discuss the symptoms and potential complications of BPH with patients who present with these comorbidities. You can reassure them that BPH is not cancer, nor is it a precursor to prostate cancer; rather it is a fairly common, treatable disorder.
What's right for your patient? Watchful waiting? a-Blocker therapy? Surgery?
Questionnaire can help, addresses quality of life
Questionnaires such as the International Prostate Symptom Score (IPSS) (PATIENT HANDOUT)9 and the similar American Urological Association symptom index (AUA-SI) (available on page 44 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf) can help you evaluate your patient's symptom severity.2,6
The IPSS, with 3 categories of symptom severity (mild 0 to 7, moderate 8 to 19, severe 20 to 35) and a global quality-of-life question also referred to as the "Bother Score," is a validated tool for monitoring disease distress and clinical change.10,11 The quality-of-life question is a good indicator for assessing whether watchful waiting might be preferred to active treatment.9,12
Further categorizing the symptoms is not helpful. Lower urinary tract symptoms have traditionally been divided into irritative symptoms such as nocturia, urgency, and frequency, attributed to bladder and prostatic smooth muscle contractions, and obstructive symptoms such as hesitancy, decreased force of stream, and incomplete emptying, attributed to increased glandular mass.1 This distinction, however, is not helpful inasmuch as irritative symptoms can result from increased tissue mass alone and obstructive symptoms from muscle hypertonicity alone; additionally, most BPH patients have a combination of both.13,14
Consider comorbidities and overactive bladder
Common comorbidities for a patient with BPH include obesity, diabetes mellitus, and low high-density lipoprotein levels. Both irritative and obstructive symptoms are likely, without prior lower urinary tract disorders or ongoing neurological disease.13-15 Multiple epidemiological studies have established clear, clinically relevant associations between BPH-related lower urinary tract symptoms and ED and ejaculatory dysfunction.8
It is also important to note that lower urinary tract symptoms may often arise due to overactive bladder; in fact, symptoms of overactive bladder and BPH overlap to a large degree.16 The diagnostic challenge is only increased by the fact that while overactive bladder is an additional cause of lower urinary tract symptoms, it may also coexist with BPH-related bladder outlet obstruction.17 The similarity in clinical presentation of the 2 conditions may make them hard to distinguish.
Rule out infection, urinary tract stones
There is general agreement about the need to exclude other potential etiologies of lower urinary tract symptoms in older men.4,15 Thus, you need to consider such causes as urinary tract stones, infections, or cancer; comorbid conditions that may affect bladder function or lead to polyuria; drug side effects; or sleep disturbances associated with chronic insomnia, depression, ethanol abuse, or sleep apnea.13,14
Digital rectal exam (DRE). The physical exam should include both a DRE and a search for neurological deficits to look for evidence that lower urinary tract symptoms are not BPH-related. The DRE should assess for stool impaction and prostate symmetry, nodularity, and consistency. Prostate volume estimates by DRE are not reliable and generally underestimate actual values while correlating poorly with BPH symptoms.14,18
Urinalysis. If you suspect BPH, you'll need to order a urinalysis to screen for infection, cancer, or stones and additional lab studies based on the patient's history, including measurements of serum creatinine, calcium, glucose, and prostate-specific antigen (PSA), among others.4,15
PSA values. These values should be checked if the patient's life expectancy is greater than a decade and a diagnosis of prostate cancer would influence treatment decisions. Adjustments of accepted norms should account for increasing age (40 to 50 years, 0-2.5 ng/mL; 51 to 60 years, 2.5-3.5 ng/mL; 61 to 70 years, 3.5-4.5 ng/mL; 71 to 80 years, 4.5-6.5 ng/mL), and urologic referral should be made as indicated.18
PSA determination is a more accurate reflection of prostate volume than a DRE and helps establish a pretreatment reference point before 5-a reductase inhibitor therapy.19 These drugs lower PSA concentrations approximately 50% and may complicate subsequent cancer screening.15
The US Preventive Services Task Force (USPSTF) clinical guidelines for prostate cancer screening notes that among patients with enlarged prostates, the specificity of PSA testing is lower, and thus PSA is a less accurate means of detecting cancer in BPH patients.20 Indeed, the USPSTF guidelines are ambivalent on the utility of PSA, in part because of the heterogeneity of prostate tumors, although they do confirm the greater accuracy of PSA testing over DRE.20
The guidelines state that screening is most effective at determining patients with a particularly good or poor long-term prognosis, which constitutes a fairly small minority of patients, but is less effective in the larger middle group.20 Regarding the particular means of testing PSA, the USPSTF guidelines note that free or complex testing is primarily useful to distinguish whether a patient should undergo a biopsy among those with a PSA level of 4.0 to 9.9 ng/mL.20 A more recent perspective from Cleveland Clinic clinicians indicates that the "PSA cutoff era" is now past and that decisions for further prostate cancer screening should be made with a patient's DRE and family history data in mind.21
Diagnostic studies. Noninvasive urine flow rates, postvoid residual measures, pressure-flow studies, cystoscopy, and renal or transrectal ultrasound are optional unless dictated by specific circumstances, including recurrent hematuria, pelvic pain, or urinary retention, in which case urologic consultation is indicated.4,15
Weigh patient preference against symptom severity
The treatment goals for a patient with BPH-related lower urinary tract symptoms must focus on improving and maintaining quality of life, achieving and sustaining symptom control, and avoiding disease progression.22 In choosing a specific treatment, weigh the patient's preferences against symptom severity and specific physiologic variables; even individuals with moderate IPSS ratings may improve (40%) or show no change (45%) with watchful waiting.23 (The AUA outlines treatment options for patients with moderate to severe symptoms in its BPH practice guidelines. They can be accessed on page 16 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Quality-of-life issues—how much lower urinary tract symptoms interfere with work, social life, sleep, sexual function, and travel—are generally more important than the symptoms per se.14 The AUA has published a diagnosis and treatment algorithm for BPH that is very helpful for practitioners.4 It is available on page 7 of http://www.auanet.org/guidelines/main_reports/bph_management/chapt_1_appendix.pdf.
Watchful waiting—even with high IPSS ratings
Watchful waiting is an option for patients experiencing minimal bother—even with high IPSS ratings—because the risk for progression is relatively small.4,14,15 If you choose this route, encourage the patient to minimize alcohol and caffeine use and the intake of fluids in the evening, and minimize the use of a-agonist, anticholinergic, antihistaminic, and calcium-channel blocker medications.
Where nocturia is a particular problem, diuretics timed to minimize night-time urine production, daytime naps, and use of antidiuretic hormones (although contraindicated in patients with congestive heart failure) may be appropriate.24,25 Notably, in the context of combined bladder outlet obstruction and detrusor overactivity validated by urodynamic studies, there are recent studies identifying a role for anticholinergics.26,27
Medical therapy before surgery
Medical therapy has supplanted surgery as the primary therapeutic tool for BPH-related lower urinary tract symptoms.4 a-Adrenergic antagonists decrease prostatic and urethral smooth muscle tone, induce tissue apoptosis through tumor growth factor-beta signaling, and increase detrusor muscle vascular supply, while 5-a reductase inhibitors block conversion of testosterone to dihydrotestosterone and reduce prostate volume ( TABLE ).4,14,15,28-40
a-Adrenergic blockers. Nonselective a-adrenergic blockers include terazosin, doxazosin, and alfuzosin. Their greater selectivity for nonprostatic peripheral vasculature a-1B receptors than for prostatic a-1A receptors account for their potential to cause orthostatic hypotension. A fourth agent, tamsulosin, is mostly selective for the prostatic a-1A receptor and does not have a clinically significant effect on blood pressure.30
At therapeutic doses, these drugs have comparable efficacy in lowering IPSS scores, increasing urine flow rates, and improving symptoms.4 Potential side effects include asthenia, headache, dizziness, and peripheral edema. Early postural hypotension and later rebound hypertension on withdrawal are primarily seen with terazosin and doxazosin, which require titration and tapering over 2 to 3 weeks when being introduced or eliminated. The uroselectivity of alfuzosin, as well as new dosing formulations, have helped reduce hypotensive side effects.28,29 Like tamsulosin, it can be started and stopped directly.
TABLE
Medical therapies for BPH at a glance4,14,15,28-40
| TYPE OF THERAPY | ACTIVITY | EFFICACY IN CLINICAL TRIALS | SIDE EFFECTS | INDICATIONS | NUMBER NEEDED TO TREAT* |
|---|---|---|---|---|---|
| a-Adrenergic blockers Nonselective Terazosin Doxazosin Alfuzosin Selective Tamsulosin |
|
|
|
| Terazosin 4.0 (to achieve >10% improvement in Boyarsky score, an older measure comparable to the IPSS)31 Doxazosin 13.7 (for the prevention of clinical progression)32 Alfuzosin 5.8 (to achieve =3 points improvement in IPSS)33 Tamsulosin 4.5 (to achieve =25% increase in AUA score)34 |
| 5- a Reductase inhibitors Dutasteride Finasteride |
|
| Dutasteride mild-to-moderate symptoms : 10 (to achieve 2-point improvement in AUA-SS) severe symptoms: 6.3 (to achieve 2-point improvement in AUA-SS)37,38 Finasteride 15.0 (for the prevention of clinical progression)32 | ||
| Combination therapy with a-Adrenergic blockers and 5-a reductase inhibitors |
|
|
| Combination of doxazosin + finasteride 8.4 (for the prevention of clinical progression)32 | |
| Phytotherapy Saw palmetto |
|
|
|
| N/A |
| *Number needed to treat (NNT) values should not be regarded as points of efficacy comparison since they are not consistently based on head-to-head trials, are derived from different patient populations, and may refer to different efficacy end points as well as different lengths of follow-up. | |||||
| AUA-SS, American Urological Association symptom score; BPH, benign prostatic hyperplasia; EAU, European Association of Urology; IPSS, International Prostate Symptom Score; LUTS, lower urinary tract symptoms; N/A, not available; PSA, prostate-specific antigen; QOL, quality of life. | |||||
Although infrequently reported in clinical trials, rhinitis and ejaculatory dysfunction are known side effects of tamsulosin and alfuzosin.30,41 a1-Blockers have recently been reported as possibly having an association with intraoperative floppy iris syndrome (IFIS), a surgical condition that has been observed during phacoemulsification cataract surgery.42 The etiology of this syndrome is unknown. Patients undergoing cataract surgery who are taking a1-blockers should inform their surgeons, who should be prepared for possible modifications to the surgical technique. The benefit of stopping a1-blocker therapy prior to cataract surgery has not been established.43-45
5- a Reductase inhibitors. Finasteride and dutasteride are comparable in efficacy and have been shown to decrease prostate volume (20%-30%), lower IPSS ratings 3 to 4 points, increase urine flow rates, and decrease urinary retention and the need for surgery (50%) when compared with placebo.15 Their clinical effect appears gradually over 3 to 6 months, and they are most beneficial when prostate volume exceeds 40 mL.35
Decreased libido (6%), ED (8%), and ejaculatory disorders (4%) are the main side effects of these drugs, as is their lowering of PSA levels by as much as half.15 This latter effect may prompt checking PSA velocities and free:total PSA ratios as a part of prostate cancer screening. Additionally, finasteride may reduce the prevalence of prostate cancer almost 25% compared with placebo, but more high-grade tumors may be associated with its use.36 The reason for this difference and its clinical importance require further study.36,46,47
Combination therapy. Combination therapy with a-adrenergic blockers and 5-a reductase inhibitors has increased due to results from the long-term (4.5 years) Medical Therapy of Prostatic Symptoms (MTOPS) study.32 It compared the efficacy of placebo, doxazosin, finasteride, and combination therapy on clinical progression measures of BPH. These were defined as an increase of 4 points on the IPSS, acute urinary retention, urinary incontinence, renal insufficiency, or recurrent urinary tract infections. All drug treatments significantly improved symptom scores, but the combination was clearly superior.32 Additionally, combination therapy and finasteride significantly reduced urinary retention and the need for surgery, whereas doxazosin did not.
The number needed to treat (NNT) for the prevention of a single instance of clinical progression over a 4-year period was 8.4 for combination therapy, compared with 13.7 for doxazosin monotherapy and 15.0 for finasteride monotherapy ( TABLE ).32
A secondary analysis, conducted to establish the NNT for disease progression in patients with larger baseline prostates or higher serum PSA, found that among patients with a PSA level >4.0 ng/mL, the NNT was 4.7 (vs 7.2 for finasteride), and for patients with a prostate volume >40 mL, the NNT was 4.9 (vs 7.2 for finasteride).32 These results suggest that patients with larger glands and higher PSA values, who are at greatest risk for progression, would benefit from combination approaches, although absolute threshold values are not yet clear.4
A combination of an a-adrenergic blocker and an anticholinergic medication may also be used in the treatment of comorbid lower urinary tract symptoms and overactive bladder. A 12-week placebo-controlled trial of a combination of tamsulosin and the anticholinergic tolterodine found significant benefits in terms of IPSS scores, urgency episodes, frequency of micturitions, quality-of-life scores, and patient perception of treatment benefit.48
Phytotherapy. Saw palmetto is derived from the ripe berries of the American dwarf palm (Serenoa repens or Sabal serrulata); retail sales in the United States totaled over $20 million in 2004.49 The mechanism of action is uncertain, but may involve antiandrogen activity. Short-term improvement of nocturia and peak urinary flow comparable with that of finasteride has been suggested by meta-analyses involving almost 3000 patients in trials ranging from 1 month to 1 year.39 However, neither American nor European guidelines recommend its use.4,15,40
A 6-month, double-blind, placebo-controlled trial of urtica dioica (stinging nettle) in 620 BPH patients found a significant improvement in IPSS scores, peak flow rates, and a small but significant reduction in prostate size among patients taking urtica dioica compared with baseline.50
Bothersome symptoms? Consider surgery
Transurethral resection of the prostate (TURP) was the primary surgical approach during most of the 20th century and remains the benchmark. TURP involves removing a portion of the prostate through the urethra.4 When compared with watchful waiting, TURP achieved better outcomes with men most bothered by symptoms at the outset. Watchful waiting was also considered safe, but 24% of this group underwent surgery during the 3 years. There were no increases in urinary incontinence or ED among surgically treated patients.51
TURP is indicated for patients with refractory urinary retention due to severe bladder outlet obstruction, recurrent urinary tract infections, progressive renal insufficiency, hematuria unresponsive to 5-a reductase inhibitors, bladder stones, and BPH-related hydronephrosis. Lower urinary tract symptom improvement is expected in 80% to 90% of cases, with a retained efficacy of 75% for at least 7 years and a risk of repeating surgery of only 1% annually.4,14,15 IPSS scores may decrease 15 to 20 points, but quality of life is enhanced only with severe lower urinary tract symptoms, and postoperative ejaculatory dysfunction (65%-70%) is expected, along with 1% to 2% perioperative mortality.15
It's important to note that TURP is a procedure that requires a hospital stay and is associated with a variety of potential side effects, including sexual dysfunction, bladder neck contracture, urinary tract infection, hematuria, and irritative voiding symptoms, while patients may also require blood transfusions.4,52
Other surgical therapies include open prostatectomies for patients with glands =80 mL and transurethral incision of the prostate (TUIP) for glands <30 mL.1,4,15 TUIP is a simpler outpatient operation than TURP. It offers equivalent symptomatic relief and less associated ejaculatory dysfunction or bleeding, but has a higher rate of reoperation.1,4,15 High-risk surgical candidates with severe urinary retention may also receive prostatic stents, but significant complications of pain, infection, and encrustation are common.4
Holmium laser enucleation of the prostate (HOLEP) is another alternative to TURP that has demonstrated equivalent efficacy in terms of AUA-SI scores, peak flow rates, and quality-of-life scores in studies of up to 3 years in length. Longer-term studies are required to determine its efficacy beyond that time frame.53-56
Minimally invasive route for high-risk patients
Transurethral needle ablation (TUNA) and transurethral microwave thermotherapy (TUMT) offer AUA-approved alternative treatment choices based on the severity of symptoms and the presence of complications.4 TUNA uses radiofrequency waves administered through 2 18-gauge needles to heat prostatic tissue. An outpatient procedure, TUNA is effective over the long term, demonstrating a low failure rate (25% after 5 years); however, temporary side effects such as irritative urinary symptoms and urinary retention can occur.4,57
With >100,000 procedures performed, TUMT is the most frequent minimally invasive treatment utilized worldwide. Heat destroys targeted prostatic tissue, while a cooling system protects the prostatic urethra. Its efficacy has been demonstrated by randomized trials, and its failure rate documented at 10% to 16% annually.4 Morbidity is related mainly to required indwelling catheterization for 4 to 6 weeks following intervention. However, it is an outpatient, low-risk procedure well-suited to high-risk patients or those who oppose surgery.
Correspondence
Darryl Chutka, MD, Division of Preventive and Occupational Medicine and Internal Medicine, Mayo Clinic College of Medicine, Rochester, MN 55905; [email protected].
1. Granville LJ. Prostate disease. In: Cobbs EL, Duthie EH, Murphy JB, eds. Geriatrics review syllabus: a core curriculum in geriatric medicine. 5th ed. Malden, Mass: Blackwell Publishing; 2002:384-385.
2. Collins MFM, Friedman RH, Ash A, Hall R, Moskowitz M. Underdetection of clinical benign prostatic hyperplasia in a general medical practice. J Gen Intern Med. 1996;11:513-518.
3. Hegarty NJ, Fitzpatrick JM. High intensity focused ultrasound in benign prostatic hyperplasia. Eur J Ultrasound. 1999;9:55-60.
4. AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagnosis and treatment recommendations. J Urol. 2003;170:530-547.
5. Welch G, Weinger K, Barry MJ. Quality-of-life impact of lower urinary tract symptom severity: results from the health professionals follow-up study. Urology. 2002;59:245-250.
6. Cunningham-Burley S, Allbutt, Garraway WM, Lee AJ, Russell EBAW. Perceptions of urinary symptoms and health-care-seeking behavior amongst men aged 40-79 years. Br J Gen Pract. 1996;46:349-352.
7. Wei JT, Calhoun E, Jacobsen SJ. Urologic diseases in America project: benign prostatic hyperplasia. J Urol. 2005;173:1256-1261.
8. Rosen RC, Giuliano F, Carson CC. Sexual dysfunction and lower urinary tract symptoms associated with benign prostatic hyperplasia. Eur Urol. 2005;47:824-837.
9. Assessing prostate symptoms. Patient UK. EMIS and Patient Information Publications 1997-2007. Available at: http://www.patient.co.uk/showdoc/23069171/. Accessed January 3, 2007.
10. O'Leary MP. Validity of the "bother score" in the evaluation and treatment of symptomatic benign prostatic hyperplasia. Rev Urol. 2005;7:1-10.
11. Barry MJ, Fowler FJ, Jr, O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, Cockett AT. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. 1992;148:1549-1557.
12. Barry MJ. Benign prostatic hyperplasia. In: Dale DC, Federman DD, eds. ACP Medicine. New York: WebMD; 2005.
13. Barry M, Roehrborn C. Management of benign prostate hyperplasia. Annu Rev Med. 1997;48:177-189.
14. Dubeau CE. Benign prostate disorders. In: Hazzard WR, Blass JP, Halter JB, Ouslander JG, Tinetti ME, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York: McGraw-Hill; 2003:1303-1310.
15. Madersbacher S, Alivizatos G, Nordling J, Sanz CR, Emberton M, de la Rosette JJ. EAU 2004 Guidelines on assessment, therapy and follow-up of men with lower urinary symptoms suggestive of benign prostatic obstruction (BPH Guidelines). Eur Urol. 2004;46:547-554.
16. Chapple CR, Roehrborn CG. A shifted paradigm for the further understanding, evaluation, and treatment of lower urinary tract symptoms in men: focus on the bladder. Eur Urol. 2006;49:651-659.
17. Knutson T, Edlund C, Fall M, Dahlstrand C. BPH with coexisting overactive bladder dysfunction—an everyday urological dilemma. Neurourol Urodyn. 2001;20:237-247.
18. Hellerstedt BA, Pienta KJ. In: Hazzard WR, Blass JP, Ouslander JG, Tinetti ME, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York: McGraw-Hill; 2003:1303-10.
19. Roehrborn CG, McConnell JD, Bonilla J, Rosenblatt S, et al. Serum prostate-specific antigen is a strong predictor of future prostate growth in men with benign prostatic hyperplasia: PROSCAR long-term efficacy and safety study. J Urol. 2000;163:13-20.
20. Harris R, Lohr KN. Screening for prostate cancer: an update of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137:917-929.
21. Jones JS, Klein E. Four no more: the 'PSA cutoff era' is over. Cleve Clin J Med. 2008;75:30-32.
22. O'Leary MP. Lower urinary tract symptoms/benign prostatic hyperplasia: Maintaining symptom control and reducing complications. Urology. 2003;62(Suppl 3A):15-23.
23. Oesterling JE. Benign prostatic hyperplasia: medical and minimally invasive treatment options. N Engl J Med. 1995;332:99-109.
24. Weiss JP, Blaivas JG. Nocturia. J Urol. 2000;163:5-12.
25. Reynard JM, Cannon A, Yang Q, Abrams P. A novel therapy for nocturnal polyuria: a double-blind randomized trial of furosemide against placebo. Br J Urol. 1998;81:215-218.
26. Abrams P, Kaplan S, De Konig Gans HJ, Millard R. Safety and tolerability of tolterodine for the treatment of overactive bladder in men with bladder outlet obstruction. J Urol. 2006;175:999-1004.
27. Athanasopoulos A, Gyftopoulos K, Giannitsas K, Fisfis J, Perimenis P, Barbalias G. Combination treatment with an alpha-blocker plus an anticholinergic for bladder outlet obstruction: a prospective, randomized controlled study. J Urol. 2003;169:2253-2256
28. van Kerrebroeck P, Jardin A, Laval KU, van Cangh P. Efficacy and safety of a new prolonged release formulation of alfuzosin 10 mg once daily versus alfuzosin 2.5 mg thrice daily and placebo in patients with symptomatic benign prostatic hyperplasia. Eur Urol. 2000;7:306-313.
29. Mottet N, Bressolle F, Delmas V, Robert M, Costa P. Prostatic tissual distribution of alfuzosin in patients with benign prostatic hyperplasia following repeated oral administration. Eur Urol. 2003;44:101-105.
30. Beduschi MC, Beduschi R, Oesterling JE. Alpha-blockade therapy for benign prostatic hyperplasia: from a nonselective to a more selective alpha1A-adrenergic antagonist. Urology. 1998;51:861-872.
31. Lepor H, Auerbach S, Puras-Baez A, et al. A randomized, placebo-controlled multicenter study of the efficacy and safety of terazosin in the treatment of benign prostatic hyperplasia. J Urol. 1992;148:1467-1474.
32. McConnell JD, Roehrborn CG, Bautista OM, et at. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387-2398.
33. Roehrborn CG. Efficacy and safety of once-daily alfuzosin in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a randomized, placebo-controlled trial. Urology. 2001;58:953-959.
34. Lepor H. Long-term evaluation of tamsulosin in benign prostatic hyperplasia: placebo-controlled, double-blind extension of phase III trial. Tamsulosin Investigator Group. Urology. 1998;51:901-906.
35. Clifford GM, Farmer RDT. Medical therapy for benign prostatic hyperplasia: a review of the literature. Eur Urol. 2000;38:2-19.
36. Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349:215-224.
37. Roehrborn CG. The clinical benefits of dutasteride treatment for LUTS and BPH. Rev Urol. 2004;6(Suppl 9):S22-SS30.
38. Roehrborn CG, Lukkarinen O, Mark S, Siami P, Ramsdell J, Zinner N. Long-term sustained improvement in symptoms of benign prostatic hyperplasia with the dual 5alpha-reductase inhibitor dutasteride: results of 4-year studies. BJU Int. 2005;96:572-577.
39. Edzard E. The risk-benefit profile of commonly used herbal therapies: ginkgo, St John's wort, ginseng, Echinacea, saw palmetto, and kava. Ann Intern Med. 2002;136:42-53.
40. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566.
41. Food and Drug Administration. ALFOTAM trial. Center for Drug Administration and Research. Available at: www.pbm.va.gov/criteria/Alpha-Blocker%20CFU%207-2005.pdf. Accessed November 16, 2006.
42. Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin. J Cataract Refract Surg. 2005;31:664-673.
43. Uroxatral [package insert]. Bridgewater, NJ: Sanofi-Aventis U.S.; 2007.
44. Cardura XL [package insert]. New York, NY: Pfizer Roerig; 2006.
45. Flomax [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2008.
46. Finasteride [package insert]. Whitehouse Station, NJ: Merck & Co. Inc.; 2007.
47. Dutasteride [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2005.
48. Kaplan SA, Roehrborn CG, Rovner ES, Carlsson M, Bavendam T, Guan Z. Tolterodine and tamsulosin for treatment of men with lower urinary tract symptoms and overactive bladder: a randomized controlled trial. JAMA. 2006;296:2319-2328.Erratum in: JAMA 2007; 297:1195.
49. Healing Herbs and Natural Remedies. Available at: http://www.herbsandnaturalremedies.com/topsellers.htm. Accessed January 3, 2007.
50. Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled, crossover study. J Herb Pharmacother. 2005;5:1-11.
51. Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. N Engl J Med. 1995;332:75-79.
52. Hammadeh MY, Madaan S, Hines J, Philp T. 5-year outcome of a prospective randomized trial to compare transurethral electrovaporization of the prostate and standard transurethral resection. Urology. 2003;61:1166-1171.
53. Ahyai SA, Lehrich K, Kuntz RM. Holmium laser enucleation versus transurethral resection of the prostate: 3-year follow-up results of a randomized clinical trial. Eur Urol. 2007;52:1456-1464.
54. Kuntz RM. Laser treatment of benign prostatic hyperplasia. World J Urol. 2007;25:241-247.
55. Gupta N, Sivaramakrishna, Kumar R, Dogra PN, Seth A. Comparison of standard transurethral resection, transurethral vapour resection and holmium laser enucleation of the prostate for managing benign prostatic hyperplasia of >40 g. BJU Int. 2006;97:85-89.
56. Tan AH, Gilling PJ, Kennett KM, Frampton C, Westenberg AM, Fraundorfer MR. A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). J Urol. 2003;170(4 Pt 1):1270-1274.
57. Zlotta AR, Giannakopoulos X, Maehlum O, Ostrem T, Schulman CC. Long-term evaluation of transurethral needle ablation of the prostate (TUNA) for treatment of symptomatic benign prostatic hyperplasia: clinical outcome up to five years from three centers. Eur Urol. 2003;44:89-93.
1. Granville LJ. Prostate disease. In: Cobbs EL, Duthie EH, Murphy JB, eds. Geriatrics review syllabus: a core curriculum in geriatric medicine. 5th ed. Malden, Mass: Blackwell Publishing; 2002:384-385.
2. Collins MFM, Friedman RH, Ash A, Hall R, Moskowitz M. Underdetection of clinical benign prostatic hyperplasia in a general medical practice. J Gen Intern Med. 1996;11:513-518.
3. Hegarty NJ, Fitzpatrick JM. High intensity focused ultrasound in benign prostatic hyperplasia. Eur J Ultrasound. 1999;9:55-60.
4. AUA Practice Guidelines Committee. AUA guideline on management of benign prostatic hyperplasia (2003). Chapter 1: Diagnosis and treatment recommendations. J Urol. 2003;170:530-547.
5. Welch G, Weinger K, Barry MJ. Quality-of-life impact of lower urinary tract symptom severity: results from the health professionals follow-up study. Urology. 2002;59:245-250.
6. Cunningham-Burley S, Allbutt, Garraway WM, Lee AJ, Russell EBAW. Perceptions of urinary symptoms and health-care-seeking behavior amongst men aged 40-79 years. Br J Gen Pract. 1996;46:349-352.
7. Wei JT, Calhoun E, Jacobsen SJ. Urologic diseases in America project: benign prostatic hyperplasia. J Urol. 2005;173:1256-1261.
8. Rosen RC, Giuliano F, Carson CC. Sexual dysfunction and lower urinary tract symptoms associated with benign prostatic hyperplasia. Eur Urol. 2005;47:824-837.
9. Assessing prostate symptoms. Patient UK. EMIS and Patient Information Publications 1997-2007. Available at: http://www.patient.co.uk/showdoc/23069171/. Accessed January 3, 2007.
10. O'Leary MP. Validity of the "bother score" in the evaluation and treatment of symptomatic benign prostatic hyperplasia. Rev Urol. 2005;7:1-10.
11. Barry MJ, Fowler FJ, Jr, O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, Cockett AT. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. 1992;148:1549-1557.
12. Barry MJ. Benign prostatic hyperplasia. In: Dale DC, Federman DD, eds. ACP Medicine. New York: WebMD; 2005.
13. Barry M, Roehrborn C. Management of benign prostate hyperplasia. Annu Rev Med. 1997;48:177-189.
14. Dubeau CE. Benign prostate disorders. In: Hazzard WR, Blass JP, Halter JB, Ouslander JG, Tinetti ME, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York: McGraw-Hill; 2003:1303-1310.
15. Madersbacher S, Alivizatos G, Nordling J, Sanz CR, Emberton M, de la Rosette JJ. EAU 2004 Guidelines on assessment, therapy and follow-up of men with lower urinary symptoms suggestive of benign prostatic obstruction (BPH Guidelines). Eur Urol. 2004;46:547-554.
16. Chapple CR, Roehrborn CG. A shifted paradigm for the further understanding, evaluation, and treatment of lower urinary tract symptoms in men: focus on the bladder. Eur Urol. 2006;49:651-659.
17. Knutson T, Edlund C, Fall M, Dahlstrand C. BPH with coexisting overactive bladder dysfunction—an everyday urological dilemma. Neurourol Urodyn. 2001;20:237-247.
18. Hellerstedt BA, Pienta KJ. In: Hazzard WR, Blass JP, Ouslander JG, Tinetti ME, eds. Principles of Geriatric Medicine and Gerontology. 5th ed. New York: McGraw-Hill; 2003:1303-10.
19. Roehrborn CG, McConnell JD, Bonilla J, Rosenblatt S, et al. Serum prostate-specific antigen is a strong predictor of future prostate growth in men with benign prostatic hyperplasia: PROSCAR long-term efficacy and safety study. J Urol. 2000;163:13-20.
20. Harris R, Lohr KN. Screening for prostate cancer: an update of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137:917-929.
21. Jones JS, Klein E. Four no more: the 'PSA cutoff era' is over. Cleve Clin J Med. 2008;75:30-32.
22. O'Leary MP. Lower urinary tract symptoms/benign prostatic hyperplasia: Maintaining symptom control and reducing complications. Urology. 2003;62(Suppl 3A):15-23.
23. Oesterling JE. Benign prostatic hyperplasia: medical and minimally invasive treatment options. N Engl J Med. 1995;332:99-109.
24. Weiss JP, Blaivas JG. Nocturia. J Urol. 2000;163:5-12.
25. Reynard JM, Cannon A, Yang Q, Abrams P. A novel therapy for nocturnal polyuria: a double-blind randomized trial of furosemide against placebo. Br J Urol. 1998;81:215-218.
26. Abrams P, Kaplan S, De Konig Gans HJ, Millard R. Safety and tolerability of tolterodine for the treatment of overactive bladder in men with bladder outlet obstruction. J Urol. 2006;175:999-1004.
27. Athanasopoulos A, Gyftopoulos K, Giannitsas K, Fisfis J, Perimenis P, Barbalias G. Combination treatment with an alpha-blocker plus an anticholinergic for bladder outlet obstruction: a prospective, randomized controlled study. J Urol. 2003;169:2253-2256
28. van Kerrebroeck P, Jardin A, Laval KU, van Cangh P. Efficacy and safety of a new prolonged release formulation of alfuzosin 10 mg once daily versus alfuzosin 2.5 mg thrice daily and placebo in patients with symptomatic benign prostatic hyperplasia. Eur Urol. 2000;7:306-313.
29. Mottet N, Bressolle F, Delmas V, Robert M, Costa P. Prostatic tissual distribution of alfuzosin in patients with benign prostatic hyperplasia following repeated oral administration. Eur Urol. 2003;44:101-105.
30. Beduschi MC, Beduschi R, Oesterling JE. Alpha-blockade therapy for benign prostatic hyperplasia: from a nonselective to a more selective alpha1A-adrenergic antagonist. Urology. 1998;51:861-872.
31. Lepor H, Auerbach S, Puras-Baez A, et al. A randomized, placebo-controlled multicenter study of the efficacy and safety of terazosin in the treatment of benign prostatic hyperplasia. J Urol. 1992;148:1467-1474.
32. McConnell JD, Roehrborn CG, Bautista OM, et at. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. N Engl J Med. 2003;349:2387-2398.
33. Roehrborn CG. Efficacy and safety of once-daily alfuzosin in the treatment of lower urinary tract symptoms and clinical benign prostatic hyperplasia: a randomized, placebo-controlled trial. Urology. 2001;58:953-959.
34. Lepor H. Long-term evaluation of tamsulosin in benign prostatic hyperplasia: placebo-controlled, double-blind extension of phase III trial. Tamsulosin Investigator Group. Urology. 1998;51:901-906.
35. Clifford GM, Farmer RDT. Medical therapy for benign prostatic hyperplasia: a review of the literature. Eur Urol. 2000;38:2-19.
36. Thompson IM, Goodman PJ, Tangen CM, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349:215-224.
37. Roehrborn CG. The clinical benefits of dutasteride treatment for LUTS and BPH. Rev Urol. 2004;6(Suppl 9):S22-SS30.
38. Roehrborn CG, Lukkarinen O, Mark S, Siami P, Ramsdell J, Zinner N. Long-term sustained improvement in symptoms of benign prostatic hyperplasia with the dual 5alpha-reductase inhibitor dutasteride: results of 4-year studies. BJU Int. 2005;96:572-577.
39. Edzard E. The risk-benefit profile of commonly used herbal therapies: ginkgo, St John's wort, ginseng, Echinacea, saw palmetto, and kava. Ann Intern Med. 2002;136:42-53.
40. Bent S, Kane C, Shinohara K, et al. Saw palmetto for benign prostatic hyperplasia. N Engl J Med. 2006;354:557-566.
41. Food and Drug Administration. ALFOTAM trial. Center for Drug Administration and Research. Available at: www.pbm.va.gov/criteria/Alpha-Blocker%20CFU%207-2005.pdf. Accessed November 16, 2006.
42. Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin. J Cataract Refract Surg. 2005;31:664-673.
43. Uroxatral [package insert]. Bridgewater, NJ: Sanofi-Aventis U.S.; 2007.
44. Cardura XL [package insert]. New York, NY: Pfizer Roerig; 2006.
45. Flomax [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2008.
46. Finasteride [package insert]. Whitehouse Station, NJ: Merck & Co. Inc.; 2007.
47. Dutasteride [package insert]. Research Triangle Park, NC: GlaxoSmithKline; 2005.
48. Kaplan SA, Roehrborn CG, Rovner ES, Carlsson M, Bavendam T, Guan Z. Tolterodine and tamsulosin for treatment of men with lower urinary tract symptoms and overactive bladder: a randomized controlled trial. JAMA. 2006;296:2319-2328.Erratum in: JAMA 2007; 297:1195.
49. Healing Herbs and Natural Remedies. Available at: http://www.herbsandnaturalremedies.com/topsellers.htm. Accessed January 3, 2007.
50. Safarinejad MR. Urtica dioica for treatment of benign prostatic hyperplasia: a prospective, randomized, double-blind, placebo-controlled, crossover study. J Herb Pharmacother. 2005;5:1-11.
51. Wasson JH, Reda DJ, Bruskewitz RC, Elinson J, Keller AM, Henderson WG. A comparison of transurethral surgery with watchful waiting for moderate symptoms of benign prostatic hyperplasia. N Engl J Med. 1995;332:75-79.
52. Hammadeh MY, Madaan S, Hines J, Philp T. 5-year outcome of a prospective randomized trial to compare transurethral electrovaporization of the prostate and standard transurethral resection. Urology. 2003;61:1166-1171.
53. Ahyai SA, Lehrich K, Kuntz RM. Holmium laser enucleation versus transurethral resection of the prostate: 3-year follow-up results of a randomized clinical trial. Eur Urol. 2007;52:1456-1464.
54. Kuntz RM. Laser treatment of benign prostatic hyperplasia. World J Urol. 2007;25:241-247.
55. Gupta N, Sivaramakrishna, Kumar R, Dogra PN, Seth A. Comparison of standard transurethral resection, transurethral vapour resection and holmium laser enucleation of the prostate for managing benign prostatic hyperplasia of >40 g. BJU Int. 2006;97:85-89.
56. Tan AH, Gilling PJ, Kennett KM, Frampton C, Westenberg AM, Fraundorfer MR. A randomized trial comparing holmium laser enucleation of the prostate with transurethral resection of the prostate for the treatment of bladder outlet obstruction secondary to benign prostatic hyperplasia in large glands (40 to 200 grams). J Urol. 2003;170(4 Pt 1):1270-1274.
57. Zlotta AR, Giannakopoulos X, Maehlum O, Ostrem T, Schulman CC. Long-term evaluation of transurethral needle ablation of the prostate (TUNA) for treatment of symptomatic benign prostatic hyperplasia: clinical outcome up to five years from three centers. Eur Urol. 2003;44:89-93.