User login
Depression and cardiovascular disease: Selected findings, controversies, and clinical implications from 2009
Many advances in the understanding of the relationship between depression and cardiovascular disease (CVD) were reported in 2009. As the study of this relationship encompasses cardiology, psychiatry, behavioral medicine, and many other fields, it is difficult to keep abreast of new developments. Relevant papers are found in a variety of journals. Therefore, we systematically searched the empirical research on depression and CVD published in English in 2009. Our search yielded nearly 500 articles. We review here a few of the most provocative and potentially influential findings. We begin with an overview of the methodology of our systematic review and then summarize the key findings and controversies we identified from the 2009 literature before exploring each key finding in detail.
METHODOLOGY OF OUR SYSTEMATIC SEARCH AND RATIONALE FOR FINDINGS REVIEWED
Previous evidence demonstrated that the presence of depressive symptoms or a diagnosis of a depressive disorder predicts poor prognosis and reduced survival rates after any coronary artery disease diagnosis, including myocardial infarction (MI) and unstable angina, as well as after coronary artery bypass graft surgery (CABG).1
We aimed to see how this evidence base was expanded in 2009 by using a systematic search strategy to retrieve the most relevant articles about depression and coronary heart disease (CHD) from the MEDLINE and Psyc-INFO (Ovid interface) databases. The most relevant subject headings and free text terms were identified and combined with “or.” The two sets were then combined with “and.” Terms included “depression,” “depressive disorder,” “depress$,” “coronary artery disease” (CAD) “coronary disease,” “acute coronary syndrome” (ACS), “cardiovascular disease” (CVD), “coronary heart disease,” and “heart diseas$.” The final set was limited to the English-language literature and identified 494 unique articles published during 2009.
Closer inspection of titles and abstracts revealed well more than 100 articles directly relevant to the science and management of patients with CVD and depression or pronounced depressive symptoms. In light of this quantity, a thorough review of all new findings, editorials, and reviews is not feasible. Thus, we review here a few exciting articles in several distinct topical areas that could influence views of the relationship between depression and CVD as well as how we screen for and treat depression in patients with CVD. As with any review that is not strictly evidence-based, our choice of articles is subjective and incomplete, but we hope it will stimulate discussion and further exploration.
SUMMARY OF KEY FINDINGS AND CONTROVERSIES
The following numbered topics emerged as common themes or controversies from our survey of the 2009 literature. The remainder of this article will review findings in each of these areas in detail and discuss important clinical implications as appropriate.
1. Antidepressant use and adverse cardiac events. In surprising findings, antidepressant use was associated with increased risk of incident stroke, CVD, and sudden cardiac death in multiple large observational cohort studies. It is not known if the association is caused by unmeasured confounders or depressive symptom severity, although controlling for symptom severity did not reduce this elevated risk in some studies. Another interesting possibility is that the treatment-resistant depressed patient is at particularly high risk of CVD and death.
2. Effects of depression intervention in CVD patients. Four exciting randomized controlled trials on depression intervention in patients with CVD reported important efficacy results and suggested future directions for larger, definitive trials of depression treatment for these patients.
3. Depression screening and treatment in CVD patients. In the absence of large randomized controlled trials, the debate continues on whether depression screening or any type of depression treatment is beneficial, harmless, or harmful to patients with CVD. Continuation of this debate does not serve the health and well-being of patients or the public. Less controversial—and thus less discussed—is the important insight that psychiatric patients with depression should be routinely screened for cardiac disease and risk factors, as they are clearly at risk of CVD. We await clinical trials in this area to ensure that screening leads to improved CVD outcomes.
OBSERVATIONAL EVIDENCE ON ANTIDEPRESSANT USE AND CVD OUTCOMES
In an analysis of the Nurses’ Health Study, Whang et al examined the relationship of depressive symptoms and antidepressant use with sudden cardiac death and adverse cardiac events in 63,469 women without CVD.2 Depressive symptoms were assessed using the Mental Health Index, a five-item subscale of the Short Form-36 Health Survey. Among women who reported antidepressant use, most (61%) were taking a selective serotonin reuptake inhibitor (SSRI; sertraline, fluoxetine, paroxetine, or citalopram), while 39% reported use of other antidepressants. Women taking antidepressants were more likely to suffer sudden cardiac death, with a fully adjusted hazard ratio (HR) of 3.34 (95% confidence interval [CI], 2.03–5.50).
Krantz et al examined psychotropic medication use and risk of adverse cardiovascular events in 519 women from the Women’s Ischemia Syndrome Evaluation.3 Enrolled women underwent coronary angiography, were separated into four groups according to their psychotropic medication use (none, anxiolytics only, antidepressants only, or both anxiolytics and antidepressants), and were observed for a median of 5.9 years. Results revealed that women who received both medications had a higher risk for adverse cardiovascular events and higher all-cause mortality compared with those using neither medication, even after controlling for anxious and depressive symptoms. In addition, whereas the use of antidepressant medication was associated with a doubling of risk for subsequent CVD events (HR = 2.16; 95% CI, 1.21–3.93) and all-cause mortality (HR = 2.15; 95% CI, 1.16–3.98), use of anxiolytic medication alone was not. While this study did not examine cause of death, cardiac death is likely to have constituted a large proportion of total mortality in this cohort selected for likelihood of CAD.
Although CVD and death have long been outcomes of interest for those studying the effects of depression, additional end points have recently been investigated as well. In a prospective cohort study of 136,293 community-dwelling postmenopausal women in the Women’s Health Initiative, Smoller et al found that new antidepressant use was significantly associated with increased incidence of stroke and all-cause mortality but not with incidence of CHD.4 The rate of stroke per 1,000 person-years was 2.99 for subjects with no antidepressant use versus 4.16 for patients with new SSRI use; the rate of all-cause death was 7.79 versus 12.77, respectively. The rate of all-cause death for subjects with new tricyclic antidepressant use was 14.14 per 1,000 person-years. To address potential confounding by indication, the researchers obtained a propensity score from a logistic regression model to predict any new antidepressant use from demographic, lifestyle, risk factor, and comorbidity variables measured at baseline. New SSRI use was associated with a doubling of the risk of incident hemorrhagic stroke as well as fatal stroke. There were no significant interactions between use of SSRIs and use of statins or aspirin in terms of risk of hemorrhagic stroke.
In an interesting observational study of 7,709 patients with confirmed CAD but without a diagnosis of heart failure or depression (and without current antidepressant use), May et al found that a subsequent diagnosis of depression was associated with a significant 50% increase in the risk of heart failure.5 There was no difference, however, between depressed patients who were using antidepressants and those who were not.
Increased risk of bleeding with SSRI use, particularly in patients with CAD, has also been a concern. Kim et al evaluated 1,380 adults who received any anti depressant before CABG for in-hospital mortality or any bleeding events.6 After controlling for the percentage of patients taking SSRIs (78%), there were no significant differences between those taking SSRIs and those taking non-SSRIs in the rate of any bleeding events (6.5% vs 7.2%; odds ratio [OR] = 0.93; 95% CI, 0.50–1.76) or in-hospital mortality (3.1% vs 2.3%; OR = 0.88; 95% CI, 0.47–1.65). There was no increased risk of bleeding associated with SSRI use when the analysis was restricted to patients who received antiplatelet and anticoagulant therapy. Thus, compared with patients who received non-SSRI antidepressants, patients who received SSRIs preoperatively had no increased risk of bleeding or in-hospital mortality after CABG; however, this study did not evaluate the effect of no antidepressant use.
Another study hypothesized that the use of any drug with the potential to prolong cardiac repolarization would be associated with an increased risk of sudden death.7 Use of individual drugs was analyzed among 1,010 cases of sudden unexplained death and 3,030 living primary care controls, all from the community. SSRI use was associated with a doubling of risk of sudden death (OR = 2.21; 95% CI, 1.61–3.05), and tricyclic antidepressant use was associated with a nonsignificant trend toward increased risk (OR = 1.44; 95% CI, 0.96–2.13). Further analysis that stratified patients according to prior CVD showed that most of the association of SSRIs with sudden death was in those with existing CVD and not in those without CVD. Other drugs found to raise sudden death risk included the typical and atypical antipsychotics.
Summary and clinical implications
The Nurses’ Health Study analysis by Whang et al suggested that antidepressant use triples the risk of sudden cardiac death in healthy women, and the authors suggested that the association between fatal ventricular arrhythmias and antidepressant use be examined further. 2 The analysis of the Women’s Health Initiative by Smoller et al found that use of SSRIs and tricyclic antidepressants doubled the risk of fatal stroke in healthy women.4 The analysis of the Women’s Ischemia Syndrome Evaluation by Krantz et al revealed a doubling of the risk of CVD and death in women taking antidepressants who had been referred for coronary angiography.3 At the same time, May et al found no increase in the risk of heart failure conversion with antidepressant use in patients with CAD,5 and Kim et al found no increase in the risk of bleeding with use of SSRIs compared with non-SSRI antidepressants in patients with CAD undergoing CABG.6 Finally, in a population- and community-based case-control study, SSRI use was associated with an increased risk of sudden death, particularly in patients with CVD.7 So what are we to make of these findings?8
In all observational studies (including those reviewed above), unmeasured confounders pose a threat to the validity of any causal conclusions. A study recently tested some of the proposed confounders that might have existed in the above studies. Waldman et al examined racial differences in depressive symptoms and antidepressant treatment among a cohort of 864 consecutive patients with CHD undergoing diagnostic coronary angiography (727 white and 137 African American).9 While levels of depression were similar between the white and African American patients, the African Americans were less likely than their white counter-parts to receive antidepressant medications. Patients with only some high school, men, and patients with more severe depressive symptoms were significantly more likely to receive a prescription for antidepressants. Clearly, low education, male sex, and elevated depressive symptoms are related to poor prognosis for CHD, and the simple interpretation that antidepressant use is causing poorer outcomes is problematic.8
Two additional interpretations of the observational findings should be considered. First, confounding by indication (depressive symptom severity) might exist in these studies.10 In other words, patients who are prescribed antidepressant medication may be those with the most severe depressive illness, and it could be this severity, rather than the antidepressant use, that is causally implicated in the CVD incidence.11 However, all of the studies reviewed above either directly controlled for depressive symptom severity (at least as obtained at baseline) or used propensity scores or stratified subjects based on depression severity. The results showed an increased risk among those who were taking antidepressants. However, none of the studies examined depressive symptom severity during or at the end of the study or depression diagnosis and severity before antidepressant use; these data are needed for a clearer understanding of whether the results were confounded by indication.
Second, these findings are also consistent with a treatment-resistant depression phenotype.12 Krantz et al caution that it is not clear from their observational study3 whether medication use itself or depression refractory to treatment is implicated in the increased risk of CVD events and mortality. Depression that is refractory to treatment may be the type of depression that places patients at risk for sudden death, stroke, or CHD recurrence, so it may not be the antidepressant use per se that is associated with this risk. This phenomenon was documented in a secondary analysis13 of the largest-to-date randomized controlled trial of patients with MI undergoing treatment for depression (ENRICHD).14 It showed that those whose depressive symptoms did not respond to treatment had a higher risk of late mortality (ie, death ≥ 6 months after acute MI). This finding was replicated in 2009 in an important follow-up15 of the SADHART trial16; among patients with MI and major depression, treatment-resistant depression (ie, depression that failed to improve substantially during treatment with either sertraline or placebo) was strongly and independently associated with long-term mortality (HR = 2.39; 95% CI, 1.39–2.44; P < .001).15
What is needed next? Testing the alternative hypothesis— ie, that an unmeasured confounder may exist—is difficult, requiring new observational studies and measurement of the putative third common causes or previously unmeasured confounder. Other putative confounders would then be hypothesized and would need to be included in additional observational studies. To properly test the putative confounding by depressive symptom severity, future observational studies should examine initial depressive symptom severity prior to antidepressant use and then collect data on depressive symptom severity and antidepressant use as time-varying covariates to CVD outcomes. To test whether treatment-resistant depression is the phenotype driving the spurious observational association between antidepressant use and increased risk of CVD, the phenotype and its underlying causal mechanisms need to be better understood. Of course, rigorous and adequately powered randomized controlled trials of antidepressant use in patients with CVD would be a more straightforward way to test the observational association between antidepressant use and increased risk of CVD. We turn now to the recently published randomized controlled trials in this field.
NEW EVIDENCE FROM RANDOMIZED TRIALS IN PATIENTS WITH CVD AND DEPRESSION
Concerns have been voiced for some time about the ability to effectively treat depression and whether an effective depression treatment will affect the risk of CVD recurrence and mortality.8 Adding to these concerns is our limited knowledge of the causal pathways and behavioral and biologic mechanisms implicated in this risk association.1 For these reasons, results from new randomized controlled trials, such as the four summarized below, are important.
Rollman et al compared the effectiveness of telephone-delivered collaborative care (treatment group) and usual physician care (control group) for improving mental health quality of life and reducing depressive symptoms in 302 patients with depression after CABG.17 Patients were observed for 8 months following randomization. Mental health quality of life and depressive symptoms were both significantly improved in the treatment group relative to the control group. Significantly more patients in the treatment group had a 50% or greater reduction in depressive symptoms (50.0% vs 29.6% in control group, P < .001; number needed to treat = 4.9 [95% CI, 3.2–10.4]). Men particularly benefited from the treatment. This trial suggests that collaborative care can be delivered effectively (and potentially cost-efficiently) over the phone.
Freedland et al also evaluated depression treatment in 123 patients with major or minor depression who underwent CABG.18 Their primary objective was to determine the efficacy of two behavioral treatments (cognitive behavioral therapy [CBT] or supportive stress management) compared with usual care. Significantly more patients in both the CBT group (71%) and the stress management group (57%) had a low score (indicating less severe depressive symptoms) on the clinician-based Hamilton Rating Scale for Depression compared with the usual care group (33%). These results were maintained 6 months after the end of the trial. Secondary measures of depressive symptoms, anxiety, and quality of life were also significantly improved in the depression treatment groups compared with the usual care group. This trial is important for the following reasons:
- The use of a second control group, the stress management group, represents a strict, high-quality design that controls for professional attention, generic or placebo therapy effect, and time or effort on the part of the patient.
- The second control group also provides treatment options for the patient, as both CBT and stress management were beneficial.
- Outcome assessors were blinded to treatment assignment, an important design feature in behavioral trials.
In a rigorously conducted randomized, double-blind, placebo-controlled trial, Carney et al tested whether 2 g/day of omega-3 acid ethyl esters (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) improved depressive symptoms in 122 patients with major depression and CHD.19 Patients in both the omega-3 and placebo groups received sertraline (50 mg/day) during the 10-week trial. A deficiency of omega-3 fatty acids has been implicated in both depression and CHD and is a possible causal link between the two diseases. Also, there is some evidence that the efficacy of antidepressants is increased by the addition of omega-3 supplementation. Unfortunately, there were no differences in self-reported or clinician-assessed depressive symptoms or in predefined depression remission at the study’s end. The trial included a 2-week adherence run-in period, ensuring that medication adherence in the trial was excellent (97%), and concluded that omega-3 supplementation, at least at these dosage levels, does not improve depression outcomes.
In the Coronary Psychosocial Evaluation Studies (COPES) randomized controlled trial, Davidson et al compared 6 months of an enhanced care intervention with usual depression care among 157 patients with ACS and persistently elevated depressive symptoms.20 Under the enhanced care intervention, patients received either problem-solving therapy or antidepressant medication, depending on their preference, and then had the option of later augmentation with the other treatment, intensification of the initial treatment, or switching of treatments, if indicated by depressive symptom severity (stepped care). The purpose of the trial was to determine the acceptability and efficacy of depression treatment among patients with ACS, who often neither agree with the diagnosis of depression nor had been seeking treatment for depression. Significantly more patients were satisfied with their depression care in the intervention arm, and depressive symptoms and major adverse cardiac events (nonfatal MI, hospitalization for unstable angina, or all-cause mortality) were significantly reduced in the intervention arm compared with the usual care arm. The absolute numbers were very small; at the end of the trial, 3 patients in the intervention group and 10 patients in the usual care group had major adverse cardiac events (4% and 13%, respectively; log-rank test, χ21 = 3.93; P = .047). The results suggested that involving patients in the type of depression care they receive (medication and/or psychotherapy) and stepping treatments aggressively may be methods to improve the treatment of depression in patients with CHD. In addition, persistently depressed patients may be an interesting patient group to select for future trials, as usual care has resulted in large reductions in depressive symptoms in some previous trials but not in this study of patients with persistent depression.
Summary and clinical implications
Each of these four efficacy trials adds critical information to the evidence base. Depressed patients who have undergone CABG can be effectively treated in primary care settings with integrative care,17 and CBT is also extremely effective for these patients.18 Additional studies of omega-3 supplementation should not be pursued at this time, but using a run-in period to better identify patients who are prepared to engage in treatment is a prudent idea and should be used in future trials in this area.19 Patients with CHD and persistent depressive symptoms are a promising group to target for depression therapy, and asking patients to choose their type of depression treatment may improve response to therapy for both depression and CHD.20
DEPRESSION SCREENING, REFERRAL, AND TREATMENT IN PATIENTS WITH CVD
We finish with the least evidence-based and most controversial issue in the area of depression and CVD. This controversy started in 2008 when the American Heart Association recommended in an advisory (endorsed by the American Psychiatric Association) that “screening tests for depressive symptoms should be applied to identify patients who may require further assessment and treatment” if appropriate referral for further depression assessment and treatment is available.21 Partly in response to this advisory, Thombs et al conducted a systematic review of the evidence on whether screening or treatment improves outcomes of depression or CVD in patients with CVD.22 They found no trial that tested whether depression screening was beneficial in patients with CVD, and the randomized controlled trials of depression treatment provided evidence of only mild improvement of depressive symptoms and no improvement in CVD outcome. Therefore, they questioned whether routine depression screening was appropriate.22
In at least eight editorials, letters, and reviews published on this subject in 2009, investigators continued to debate this issue.23–30 Below we provide a simplified list of reasons presented for and against screening and subsequent treatment raised in these articles.
Arguments for depression screening and treatment
The proponents of screening contend that depression is highly prevalent in patients with CVD and is clearly a risk marker for increased adverse events, reduced quality of life, and poorer adherence to treatment.24 They argue that since there are plausible biologic and behavioral mechanisms for this association, and since SSRI use improves depressive symptoms in other patient populations and is safe in patients with CVD, health care providers should not hesitate to screen and refer patients for appropriate depression treatment. At the same time, they have cautioned that SSRIs interact with anti coagulants and that bleeding should be monitored closely in patients with CVD who are taking SSRIs.24
Whooley28 noted that although there are controversial findings in this area, depression screening provided in conjunction with collaborative care depression management is cost-effective and has a documented positive impact on depression, if not on CVD outcomes.17,31 She observed that there are some costs to screening, such as false-positive findings (resulting in stigma for patients incorrectly diagnosed) and diversion of resources from other health care needs. However, Whooley suggested that primary care providers, rather than cardiologists, should conduct depression screening and that patients should undergo screening only when an established collaborative care treatment protocol exists.28
Carney et al argued that depression, like age, clearly marks CVD risk, and that health care providers should aggressively treat readily modifiable CVD risk factors.23 They added that because of the strong association between depression and medication nonadherence,32 providers should carefully monitor patient adherence to life-saving therapies.
Taking another tack, Shemesh and colleagues advocated the importance of documenting the prevalence of suicidal ideation and intent if recommendations to screen for depression in CVD patient populations were implemented.25 Using a sample of more than 1,000 patients with CVD, they determined the prevalence of suicidal ideation (12.0%) and the number of patients who required hospitalization for risk of suicide (0.5%) when routine depression screening occurred in a large cardiology clinic. They concluded that identification and stabilization of imminently suicidal patients would be a benefit of universal screening and that there is a high societal cost to neglecting suicidal ideation, intent, and risk in patients with CVD. However, more patients would need immediate thorough psychiatric evaluations for safety, which would affect resource allocation and cost in cardiology clinics.
Arguments against depression screening and treatment
The main argument against screening for and treating depression in patients with CVD is that there are neither randomized controlled trials nor systematic evidence-based reviews showing that screening for depression and/or referring for additional treatment sufficiently improves outcomes for depression or CVD, and that existing evidence does not support the recommendation to screen all patients with CVD.22,30 Furthermore, antidepressant use is associated with only mild improvement in depressive symptoms, even in other patient populations,33 and publication bias (“the file-drawer problem”) has prevented the publication of antidepressant trials with null results, thereby skewing the evidence base.34 In addition, considerable health care resources would be needed to mount such a large screening effort, and these resources would come at the expense of other efforts. Finally, the adverse effects of medications and the inevitability of some false-positive screening results must be weighed against any benefit that might occur with universal screening.35
In addition to the arguments above, Ziegelstein et al,29 in commenting on the American Heart Association advisory,21 wryly observed that there is far greater observational evidence that depressed patients seen in mental health settings are at risk for incident and recurrent CVD and that there should be universal screening and referral for CVD in patients with depression. They contended as well that the evidence is insufficient to recommend that patients with CVD undergo universal depression screening and referral.
Summary and clinical implications
Although we were hesitant to raise this tense and often emotional issue, we are in favor of routine, algorithm-based depression screening by all cardiologists, with the critical proviso that a nationwide and/or Centers for Medicare and Medicaid Services–coordinated randomized controlled trial be conducted to evaluate this practice. All patients with pronounced depressive symptoms should be referred to the trial, and two depression treatments should be evaluated, such as usual referral versus telephone-based collaborative care17 or enhanced depression care.20 Such a trial would allow us to ensure that data are collected on the cost,36 the benefit, and even the possible harms associated with routine depression screening for patients with CVD, and we could ascertain if there is an acceptable, beneficial treatment for depression that can be delivered and definitively tested.
- Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med 2008; 121( 11 suppl 2):S20–S27.
- Whang W, Kubzansky LD, Kawachi I, et al Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses’ Health Study. J Am Coll Cardiol 2009; 53:950–958.
- Krantz DS, Whittaker KS, Francis JL, et al Psychotropic medication use and risk of adverse cardiovascular events in women with suspected coronary artery disease: outcomes from the Women’s Ischemia Syndrome Evaluation (WISE) study. Heart 2009; 95:1901–1906.
- Smoller JW, Allison M, Cochrane BB, et al Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative study. Arch Intern Med 2009; 169:2128–2139.
- May HT, Horne BD, Carlquist JF, Sheng X, Joy E, Catinella AP. Depression after coronary artery disease is associated with heart failure. J Am Coll Cardiol 2009; 53:1440–1447.
- Kim DH, Daskalakis C, Whellan DJ, et al Safety of selective serotonin reuptake inhibitor in adults undergoing coronary artery bypass grafting. Am J Cardiol 2009; 103:1391–1395.
- Jolly K, Gammage MD, Cheng KK, Bradburn P, Banting MV, Langman MJ. Sudden death in patients receiving drugs tending to prolong the QT interval. Br J Clin Pharmacol 2009; 68:743–751.
- Jolly K, Langman MJ. Psychotropic medication: curing illness or creating problems? Heart 2009; 95:1893–1894.
- Waldman SV, Blumenthal JA, Babyak MA, et al Ethnic differences in the treatment of depression in patients with ischemic heart disease. Am Heart J 2009; 157:77–83.
- Salas M, Hofman A, Stricker BH. Confounding by indication: an example of variation in the use of epidemiologic terminology. Am J Epidemiol 1999; 149:981–983.
- Carney RM, Freedland KE. Treatment-resistant depression and sudden cardiac death [letter]. J Am Coll Cardiol 2009; 54:958–959.
- Carney RM, Freedland KE. Treatment-resistant depression and mortality after acute coronary syndrome. Am J Psychiatry 2009; 166:410–417.
- Carney RM, Blumenthal JA, Freedland KE, et al Depression and late mortality after myocardial infarction in the Enhancing Recovery in Coronary Heart Disease (ENRICHD) study. Psychosom Med 2004; 66:466–474.
- Berkman LF, Blumenthal J, Burg M, et al Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 2003; 289:3106–3116.
- Glassman AH, Bigger JT, Gaffney M. Psychiatric characteristics associated with long-term mortality among 361 patients having an acute coronary syndrome and major depression: seven-year follow-up of SADHART participants. Arch Gen Psychiatry 2009; 66:1022–1029.
- Glassman AH, O’Connor CM, Califf RM, et al Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002; 288:701–709.
- Rollman BL, Belnap BH, LeMenager MS, et al Telephone-delivered collaborative care for treating post-CABG depression: a randomized controlled trial. JAMA 2009; 302:2095–2103.
- Freedland KE, Skala JA, Carney RM, et al Treatment of depression after coronary artery bypass surgery: a randomized controlled trial. Arch Gen Psychiatry 2009; 66:387–396.
- Carney RM, Freedland KE, Rubin EH, Rich MW, Steinmeyer BC, Harris WS. Omega-3 augmentation of sertraline in treatment of depression in patients with coronary heart disease: a randomized controlled trial. JAMA 2009; 302:1651–1657.
- Davidson KW, Rieckmann N, Clemow L, et al Enhanced depression care for patients with acute coronary syndrome and persistent depressive symptoms: Coronary Psychosocial Evaluation Studies randomized controlled trial. Arch Intern Med 2010; 170:600–608.
- Lichtman JH, Bigger JT, Blumenthal JA, et al Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation 2008; 118:1768–1775.
- Thombs BD, de Jonge P, Coyne JC, et al Depression screening and patient outcomes in cardiovascular care: a systematic review. JAMA 2008; 300:2161–2171.
- Carney RM, Freedland KE, Jaffe AS. Depression screening in patients with heart disease [letter]. JAMA 2009; 301:1337–1338.
- Pozuelo L, Zhang J, Franco K, Tesar G, Penn M, Jiang W. Depression and heart disease: what do we know, and where are we headed? Cleve Clin J Med 2009; 76:59–70.
- Shemesh E, Annunziato RA, Rubinstein D, et al Screening for depression and suicidality in patients with cardiovascular illnesses. Am J Cardiol 2009; 104:1194–1197.
- Thombs BD, Adeponle AB, Kirmayer LJ, Rousseau C, Ziegelstein RC. More antidepressants for African Americans with coronary heart disease? Maybe—maybe not [letter]. Am Heart J 2009; 157:e33; author reply,e35–e37.
- Whang W, Davidson KW. Is it time to treat depression in patients with cardiovascular disease? Circulation 2009; 120:99–100.
- Whooley MA. To screen or not to screen? Depression in patients with cardiovascular disease. J Am Coll Cardiol 2009; 54:891–893.
- Ziegelstein RC, Thombs BD, Coyne JC, de Jonge P. Routine screening for depression in patients with coronary heart disease: never mind. J Am Coll Cardiol 2009; 54:886–890.
- Thombs BD, Jewett LR, Knafo R, Coyne JC, Ziegelstein RC. Learning from history: a commentary on the American Heart Association Science Advisory on depression screening. Am Heart J 2009; 158:503–505.
- Unutzer J, Katon W, Callahan CM, et al Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA 2002; 288:2836–2845.
- Rieckmann N, Gerin W, Kronish IM, et al Course of depressive symptoms and medication adherence after acute coronary syndromes: an electronic medication monitoring study. J Am Coll Cardiol 2006; 48:2218–2222.
- Kirsch I, Deacon BJ, Huedo-Medina TB, et al Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS Med 2008; 5:e45.
- Turner EH, Matthews AM, Linardatos E, Tell RA, Rosenthal R. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med 2008; 358:252–260.
- Thombs BD, de Jonge P, Ziegelstein RC. Depression screening in patients with heart disease [reply to letter]. JAMA 2009; 301:1338.
- Frasure-Smith N, Lespérance F. Depression and cardiac risk: present status and future directions. Heart 2010; 96:173–176.
Many advances in the understanding of the relationship between depression and cardiovascular disease (CVD) were reported in 2009. As the study of this relationship encompasses cardiology, psychiatry, behavioral medicine, and many other fields, it is difficult to keep abreast of new developments. Relevant papers are found in a variety of journals. Therefore, we systematically searched the empirical research on depression and CVD published in English in 2009. Our search yielded nearly 500 articles. We review here a few of the most provocative and potentially influential findings. We begin with an overview of the methodology of our systematic review and then summarize the key findings and controversies we identified from the 2009 literature before exploring each key finding in detail.
METHODOLOGY OF OUR SYSTEMATIC SEARCH AND RATIONALE FOR FINDINGS REVIEWED
Previous evidence demonstrated that the presence of depressive symptoms or a diagnosis of a depressive disorder predicts poor prognosis and reduced survival rates after any coronary artery disease diagnosis, including myocardial infarction (MI) and unstable angina, as well as after coronary artery bypass graft surgery (CABG).1
We aimed to see how this evidence base was expanded in 2009 by using a systematic search strategy to retrieve the most relevant articles about depression and coronary heart disease (CHD) from the MEDLINE and Psyc-INFO (Ovid interface) databases. The most relevant subject headings and free text terms were identified and combined with “or.” The two sets were then combined with “and.” Terms included “depression,” “depressive disorder,” “depress$,” “coronary artery disease” (CAD) “coronary disease,” “acute coronary syndrome” (ACS), “cardiovascular disease” (CVD), “coronary heart disease,” and “heart diseas$.” The final set was limited to the English-language literature and identified 494 unique articles published during 2009.
Closer inspection of titles and abstracts revealed well more than 100 articles directly relevant to the science and management of patients with CVD and depression or pronounced depressive symptoms. In light of this quantity, a thorough review of all new findings, editorials, and reviews is not feasible. Thus, we review here a few exciting articles in several distinct topical areas that could influence views of the relationship between depression and CVD as well as how we screen for and treat depression in patients with CVD. As with any review that is not strictly evidence-based, our choice of articles is subjective and incomplete, but we hope it will stimulate discussion and further exploration.
SUMMARY OF KEY FINDINGS AND CONTROVERSIES
The following numbered topics emerged as common themes or controversies from our survey of the 2009 literature. The remainder of this article will review findings in each of these areas in detail and discuss important clinical implications as appropriate.
1. Antidepressant use and adverse cardiac events. In surprising findings, antidepressant use was associated with increased risk of incident stroke, CVD, and sudden cardiac death in multiple large observational cohort studies. It is not known if the association is caused by unmeasured confounders or depressive symptom severity, although controlling for symptom severity did not reduce this elevated risk in some studies. Another interesting possibility is that the treatment-resistant depressed patient is at particularly high risk of CVD and death.
2. Effects of depression intervention in CVD patients. Four exciting randomized controlled trials on depression intervention in patients with CVD reported important efficacy results and suggested future directions for larger, definitive trials of depression treatment for these patients.
3. Depression screening and treatment in CVD patients. In the absence of large randomized controlled trials, the debate continues on whether depression screening or any type of depression treatment is beneficial, harmless, or harmful to patients with CVD. Continuation of this debate does not serve the health and well-being of patients or the public. Less controversial—and thus less discussed—is the important insight that psychiatric patients with depression should be routinely screened for cardiac disease and risk factors, as they are clearly at risk of CVD. We await clinical trials in this area to ensure that screening leads to improved CVD outcomes.
OBSERVATIONAL EVIDENCE ON ANTIDEPRESSANT USE AND CVD OUTCOMES
In an analysis of the Nurses’ Health Study, Whang et al examined the relationship of depressive symptoms and antidepressant use with sudden cardiac death and adverse cardiac events in 63,469 women without CVD.2 Depressive symptoms were assessed using the Mental Health Index, a five-item subscale of the Short Form-36 Health Survey. Among women who reported antidepressant use, most (61%) were taking a selective serotonin reuptake inhibitor (SSRI; sertraline, fluoxetine, paroxetine, or citalopram), while 39% reported use of other antidepressants. Women taking antidepressants were more likely to suffer sudden cardiac death, with a fully adjusted hazard ratio (HR) of 3.34 (95% confidence interval [CI], 2.03–5.50).
Krantz et al examined psychotropic medication use and risk of adverse cardiovascular events in 519 women from the Women’s Ischemia Syndrome Evaluation.3 Enrolled women underwent coronary angiography, were separated into four groups according to their psychotropic medication use (none, anxiolytics only, antidepressants only, or both anxiolytics and antidepressants), and were observed for a median of 5.9 years. Results revealed that women who received both medications had a higher risk for adverse cardiovascular events and higher all-cause mortality compared with those using neither medication, even after controlling for anxious and depressive symptoms. In addition, whereas the use of antidepressant medication was associated with a doubling of risk for subsequent CVD events (HR = 2.16; 95% CI, 1.21–3.93) and all-cause mortality (HR = 2.15; 95% CI, 1.16–3.98), use of anxiolytic medication alone was not. While this study did not examine cause of death, cardiac death is likely to have constituted a large proportion of total mortality in this cohort selected for likelihood of CAD.
Although CVD and death have long been outcomes of interest for those studying the effects of depression, additional end points have recently been investigated as well. In a prospective cohort study of 136,293 community-dwelling postmenopausal women in the Women’s Health Initiative, Smoller et al found that new antidepressant use was significantly associated with increased incidence of stroke and all-cause mortality but not with incidence of CHD.4 The rate of stroke per 1,000 person-years was 2.99 for subjects with no antidepressant use versus 4.16 for patients with new SSRI use; the rate of all-cause death was 7.79 versus 12.77, respectively. The rate of all-cause death for subjects with new tricyclic antidepressant use was 14.14 per 1,000 person-years. To address potential confounding by indication, the researchers obtained a propensity score from a logistic regression model to predict any new antidepressant use from demographic, lifestyle, risk factor, and comorbidity variables measured at baseline. New SSRI use was associated with a doubling of the risk of incident hemorrhagic stroke as well as fatal stroke. There were no significant interactions between use of SSRIs and use of statins or aspirin in terms of risk of hemorrhagic stroke.
In an interesting observational study of 7,709 patients with confirmed CAD but without a diagnosis of heart failure or depression (and without current antidepressant use), May et al found that a subsequent diagnosis of depression was associated with a significant 50% increase in the risk of heart failure.5 There was no difference, however, between depressed patients who were using antidepressants and those who were not.
Increased risk of bleeding with SSRI use, particularly in patients with CAD, has also been a concern. Kim et al evaluated 1,380 adults who received any anti depressant before CABG for in-hospital mortality or any bleeding events.6 After controlling for the percentage of patients taking SSRIs (78%), there were no significant differences between those taking SSRIs and those taking non-SSRIs in the rate of any bleeding events (6.5% vs 7.2%; odds ratio [OR] = 0.93; 95% CI, 0.50–1.76) or in-hospital mortality (3.1% vs 2.3%; OR = 0.88; 95% CI, 0.47–1.65). There was no increased risk of bleeding associated with SSRI use when the analysis was restricted to patients who received antiplatelet and anticoagulant therapy. Thus, compared with patients who received non-SSRI antidepressants, patients who received SSRIs preoperatively had no increased risk of bleeding or in-hospital mortality after CABG; however, this study did not evaluate the effect of no antidepressant use.
Another study hypothesized that the use of any drug with the potential to prolong cardiac repolarization would be associated with an increased risk of sudden death.7 Use of individual drugs was analyzed among 1,010 cases of sudden unexplained death and 3,030 living primary care controls, all from the community. SSRI use was associated with a doubling of risk of sudden death (OR = 2.21; 95% CI, 1.61–3.05), and tricyclic antidepressant use was associated with a nonsignificant trend toward increased risk (OR = 1.44; 95% CI, 0.96–2.13). Further analysis that stratified patients according to prior CVD showed that most of the association of SSRIs with sudden death was in those with existing CVD and not in those without CVD. Other drugs found to raise sudden death risk included the typical and atypical antipsychotics.
Summary and clinical implications
The Nurses’ Health Study analysis by Whang et al suggested that antidepressant use triples the risk of sudden cardiac death in healthy women, and the authors suggested that the association between fatal ventricular arrhythmias and antidepressant use be examined further. 2 The analysis of the Women’s Health Initiative by Smoller et al found that use of SSRIs and tricyclic antidepressants doubled the risk of fatal stroke in healthy women.4 The analysis of the Women’s Ischemia Syndrome Evaluation by Krantz et al revealed a doubling of the risk of CVD and death in women taking antidepressants who had been referred for coronary angiography.3 At the same time, May et al found no increase in the risk of heart failure conversion with antidepressant use in patients with CAD,5 and Kim et al found no increase in the risk of bleeding with use of SSRIs compared with non-SSRI antidepressants in patients with CAD undergoing CABG.6 Finally, in a population- and community-based case-control study, SSRI use was associated with an increased risk of sudden death, particularly in patients with CVD.7 So what are we to make of these findings?8
In all observational studies (including those reviewed above), unmeasured confounders pose a threat to the validity of any causal conclusions. A study recently tested some of the proposed confounders that might have existed in the above studies. Waldman et al examined racial differences in depressive symptoms and antidepressant treatment among a cohort of 864 consecutive patients with CHD undergoing diagnostic coronary angiography (727 white and 137 African American).9 While levels of depression were similar between the white and African American patients, the African Americans were less likely than their white counter-parts to receive antidepressant medications. Patients with only some high school, men, and patients with more severe depressive symptoms were significantly more likely to receive a prescription for antidepressants. Clearly, low education, male sex, and elevated depressive symptoms are related to poor prognosis for CHD, and the simple interpretation that antidepressant use is causing poorer outcomes is problematic.8
Two additional interpretations of the observational findings should be considered. First, confounding by indication (depressive symptom severity) might exist in these studies.10 In other words, patients who are prescribed antidepressant medication may be those with the most severe depressive illness, and it could be this severity, rather than the antidepressant use, that is causally implicated in the CVD incidence.11 However, all of the studies reviewed above either directly controlled for depressive symptom severity (at least as obtained at baseline) or used propensity scores or stratified subjects based on depression severity. The results showed an increased risk among those who were taking antidepressants. However, none of the studies examined depressive symptom severity during or at the end of the study or depression diagnosis and severity before antidepressant use; these data are needed for a clearer understanding of whether the results were confounded by indication.
Second, these findings are also consistent with a treatment-resistant depression phenotype.12 Krantz et al caution that it is not clear from their observational study3 whether medication use itself or depression refractory to treatment is implicated in the increased risk of CVD events and mortality. Depression that is refractory to treatment may be the type of depression that places patients at risk for sudden death, stroke, or CHD recurrence, so it may not be the antidepressant use per se that is associated with this risk. This phenomenon was documented in a secondary analysis13 of the largest-to-date randomized controlled trial of patients with MI undergoing treatment for depression (ENRICHD).14 It showed that those whose depressive symptoms did not respond to treatment had a higher risk of late mortality (ie, death ≥ 6 months after acute MI). This finding was replicated in 2009 in an important follow-up15 of the SADHART trial16; among patients with MI and major depression, treatment-resistant depression (ie, depression that failed to improve substantially during treatment with either sertraline or placebo) was strongly and independently associated with long-term mortality (HR = 2.39; 95% CI, 1.39–2.44; P < .001).15
What is needed next? Testing the alternative hypothesis— ie, that an unmeasured confounder may exist—is difficult, requiring new observational studies and measurement of the putative third common causes or previously unmeasured confounder. Other putative confounders would then be hypothesized and would need to be included in additional observational studies. To properly test the putative confounding by depressive symptom severity, future observational studies should examine initial depressive symptom severity prior to antidepressant use and then collect data on depressive symptom severity and antidepressant use as time-varying covariates to CVD outcomes. To test whether treatment-resistant depression is the phenotype driving the spurious observational association between antidepressant use and increased risk of CVD, the phenotype and its underlying causal mechanisms need to be better understood. Of course, rigorous and adequately powered randomized controlled trials of antidepressant use in patients with CVD would be a more straightforward way to test the observational association between antidepressant use and increased risk of CVD. We turn now to the recently published randomized controlled trials in this field.
NEW EVIDENCE FROM RANDOMIZED TRIALS IN PATIENTS WITH CVD AND DEPRESSION
Concerns have been voiced for some time about the ability to effectively treat depression and whether an effective depression treatment will affect the risk of CVD recurrence and mortality.8 Adding to these concerns is our limited knowledge of the causal pathways and behavioral and biologic mechanisms implicated in this risk association.1 For these reasons, results from new randomized controlled trials, such as the four summarized below, are important.
Rollman et al compared the effectiveness of telephone-delivered collaborative care (treatment group) and usual physician care (control group) for improving mental health quality of life and reducing depressive symptoms in 302 patients with depression after CABG.17 Patients were observed for 8 months following randomization. Mental health quality of life and depressive symptoms were both significantly improved in the treatment group relative to the control group. Significantly more patients in the treatment group had a 50% or greater reduction in depressive symptoms (50.0% vs 29.6% in control group, P < .001; number needed to treat = 4.9 [95% CI, 3.2–10.4]). Men particularly benefited from the treatment. This trial suggests that collaborative care can be delivered effectively (and potentially cost-efficiently) over the phone.
Freedland et al also evaluated depression treatment in 123 patients with major or minor depression who underwent CABG.18 Their primary objective was to determine the efficacy of two behavioral treatments (cognitive behavioral therapy [CBT] or supportive stress management) compared with usual care. Significantly more patients in both the CBT group (71%) and the stress management group (57%) had a low score (indicating less severe depressive symptoms) on the clinician-based Hamilton Rating Scale for Depression compared with the usual care group (33%). These results were maintained 6 months after the end of the trial. Secondary measures of depressive symptoms, anxiety, and quality of life were also significantly improved in the depression treatment groups compared with the usual care group. This trial is important for the following reasons:
- The use of a second control group, the stress management group, represents a strict, high-quality design that controls for professional attention, generic or placebo therapy effect, and time or effort on the part of the patient.
- The second control group also provides treatment options for the patient, as both CBT and stress management were beneficial.
- Outcome assessors were blinded to treatment assignment, an important design feature in behavioral trials.
In a rigorously conducted randomized, double-blind, placebo-controlled trial, Carney et al tested whether 2 g/day of omega-3 acid ethyl esters (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) improved depressive symptoms in 122 patients with major depression and CHD.19 Patients in both the omega-3 and placebo groups received sertraline (50 mg/day) during the 10-week trial. A deficiency of omega-3 fatty acids has been implicated in both depression and CHD and is a possible causal link between the two diseases. Also, there is some evidence that the efficacy of antidepressants is increased by the addition of omega-3 supplementation. Unfortunately, there were no differences in self-reported or clinician-assessed depressive symptoms or in predefined depression remission at the study’s end. The trial included a 2-week adherence run-in period, ensuring that medication adherence in the trial was excellent (97%), and concluded that omega-3 supplementation, at least at these dosage levels, does not improve depression outcomes.
In the Coronary Psychosocial Evaluation Studies (COPES) randomized controlled trial, Davidson et al compared 6 months of an enhanced care intervention with usual depression care among 157 patients with ACS and persistently elevated depressive symptoms.20 Under the enhanced care intervention, patients received either problem-solving therapy or antidepressant medication, depending on their preference, and then had the option of later augmentation with the other treatment, intensification of the initial treatment, or switching of treatments, if indicated by depressive symptom severity (stepped care). The purpose of the trial was to determine the acceptability and efficacy of depression treatment among patients with ACS, who often neither agree with the diagnosis of depression nor had been seeking treatment for depression. Significantly more patients were satisfied with their depression care in the intervention arm, and depressive symptoms and major adverse cardiac events (nonfatal MI, hospitalization for unstable angina, or all-cause mortality) were significantly reduced in the intervention arm compared with the usual care arm. The absolute numbers were very small; at the end of the trial, 3 patients in the intervention group and 10 patients in the usual care group had major adverse cardiac events (4% and 13%, respectively; log-rank test, χ21 = 3.93; P = .047). The results suggested that involving patients in the type of depression care they receive (medication and/or psychotherapy) and stepping treatments aggressively may be methods to improve the treatment of depression in patients with CHD. In addition, persistently depressed patients may be an interesting patient group to select for future trials, as usual care has resulted in large reductions in depressive symptoms in some previous trials but not in this study of patients with persistent depression.
Summary and clinical implications
Each of these four efficacy trials adds critical information to the evidence base. Depressed patients who have undergone CABG can be effectively treated in primary care settings with integrative care,17 and CBT is also extremely effective for these patients.18 Additional studies of omega-3 supplementation should not be pursued at this time, but using a run-in period to better identify patients who are prepared to engage in treatment is a prudent idea and should be used in future trials in this area.19 Patients with CHD and persistent depressive symptoms are a promising group to target for depression therapy, and asking patients to choose their type of depression treatment may improve response to therapy for both depression and CHD.20
DEPRESSION SCREENING, REFERRAL, AND TREATMENT IN PATIENTS WITH CVD
We finish with the least evidence-based and most controversial issue in the area of depression and CVD. This controversy started in 2008 when the American Heart Association recommended in an advisory (endorsed by the American Psychiatric Association) that “screening tests for depressive symptoms should be applied to identify patients who may require further assessment and treatment” if appropriate referral for further depression assessment and treatment is available.21 Partly in response to this advisory, Thombs et al conducted a systematic review of the evidence on whether screening or treatment improves outcomes of depression or CVD in patients with CVD.22 They found no trial that tested whether depression screening was beneficial in patients with CVD, and the randomized controlled trials of depression treatment provided evidence of only mild improvement of depressive symptoms and no improvement in CVD outcome. Therefore, they questioned whether routine depression screening was appropriate.22
In at least eight editorials, letters, and reviews published on this subject in 2009, investigators continued to debate this issue.23–30 Below we provide a simplified list of reasons presented for and against screening and subsequent treatment raised in these articles.
Arguments for depression screening and treatment
The proponents of screening contend that depression is highly prevalent in patients with CVD and is clearly a risk marker for increased adverse events, reduced quality of life, and poorer adherence to treatment.24 They argue that since there are plausible biologic and behavioral mechanisms for this association, and since SSRI use improves depressive symptoms in other patient populations and is safe in patients with CVD, health care providers should not hesitate to screen and refer patients for appropriate depression treatment. At the same time, they have cautioned that SSRIs interact with anti coagulants and that bleeding should be monitored closely in patients with CVD who are taking SSRIs.24
Whooley28 noted that although there are controversial findings in this area, depression screening provided in conjunction with collaborative care depression management is cost-effective and has a documented positive impact on depression, if not on CVD outcomes.17,31 She observed that there are some costs to screening, such as false-positive findings (resulting in stigma for patients incorrectly diagnosed) and diversion of resources from other health care needs. However, Whooley suggested that primary care providers, rather than cardiologists, should conduct depression screening and that patients should undergo screening only when an established collaborative care treatment protocol exists.28
Carney et al argued that depression, like age, clearly marks CVD risk, and that health care providers should aggressively treat readily modifiable CVD risk factors.23 They added that because of the strong association between depression and medication nonadherence,32 providers should carefully monitor patient adherence to life-saving therapies.
Taking another tack, Shemesh and colleagues advocated the importance of documenting the prevalence of suicidal ideation and intent if recommendations to screen for depression in CVD patient populations were implemented.25 Using a sample of more than 1,000 patients with CVD, they determined the prevalence of suicidal ideation (12.0%) and the number of patients who required hospitalization for risk of suicide (0.5%) when routine depression screening occurred in a large cardiology clinic. They concluded that identification and stabilization of imminently suicidal patients would be a benefit of universal screening and that there is a high societal cost to neglecting suicidal ideation, intent, and risk in patients with CVD. However, more patients would need immediate thorough psychiatric evaluations for safety, which would affect resource allocation and cost in cardiology clinics.
Arguments against depression screening and treatment
The main argument against screening for and treating depression in patients with CVD is that there are neither randomized controlled trials nor systematic evidence-based reviews showing that screening for depression and/or referring for additional treatment sufficiently improves outcomes for depression or CVD, and that existing evidence does not support the recommendation to screen all patients with CVD.22,30 Furthermore, antidepressant use is associated with only mild improvement in depressive symptoms, even in other patient populations,33 and publication bias (“the file-drawer problem”) has prevented the publication of antidepressant trials with null results, thereby skewing the evidence base.34 In addition, considerable health care resources would be needed to mount such a large screening effort, and these resources would come at the expense of other efforts. Finally, the adverse effects of medications and the inevitability of some false-positive screening results must be weighed against any benefit that might occur with universal screening.35
In addition to the arguments above, Ziegelstein et al,29 in commenting on the American Heart Association advisory,21 wryly observed that there is far greater observational evidence that depressed patients seen in mental health settings are at risk for incident and recurrent CVD and that there should be universal screening and referral for CVD in patients with depression. They contended as well that the evidence is insufficient to recommend that patients with CVD undergo universal depression screening and referral.
Summary and clinical implications
Although we were hesitant to raise this tense and often emotional issue, we are in favor of routine, algorithm-based depression screening by all cardiologists, with the critical proviso that a nationwide and/or Centers for Medicare and Medicaid Services–coordinated randomized controlled trial be conducted to evaluate this practice. All patients with pronounced depressive symptoms should be referred to the trial, and two depression treatments should be evaluated, such as usual referral versus telephone-based collaborative care17 or enhanced depression care.20 Such a trial would allow us to ensure that data are collected on the cost,36 the benefit, and even the possible harms associated with routine depression screening for patients with CVD, and we could ascertain if there is an acceptable, beneficial treatment for depression that can be delivered and definitively tested.
Many advances in the understanding of the relationship between depression and cardiovascular disease (CVD) were reported in 2009. As the study of this relationship encompasses cardiology, psychiatry, behavioral medicine, and many other fields, it is difficult to keep abreast of new developments. Relevant papers are found in a variety of journals. Therefore, we systematically searched the empirical research on depression and CVD published in English in 2009. Our search yielded nearly 500 articles. We review here a few of the most provocative and potentially influential findings. We begin with an overview of the methodology of our systematic review and then summarize the key findings and controversies we identified from the 2009 literature before exploring each key finding in detail.
METHODOLOGY OF OUR SYSTEMATIC SEARCH AND RATIONALE FOR FINDINGS REVIEWED
Previous evidence demonstrated that the presence of depressive symptoms or a diagnosis of a depressive disorder predicts poor prognosis and reduced survival rates after any coronary artery disease diagnosis, including myocardial infarction (MI) and unstable angina, as well as after coronary artery bypass graft surgery (CABG).1
We aimed to see how this evidence base was expanded in 2009 by using a systematic search strategy to retrieve the most relevant articles about depression and coronary heart disease (CHD) from the MEDLINE and Psyc-INFO (Ovid interface) databases. The most relevant subject headings and free text terms were identified and combined with “or.” The two sets were then combined with “and.” Terms included “depression,” “depressive disorder,” “depress$,” “coronary artery disease” (CAD) “coronary disease,” “acute coronary syndrome” (ACS), “cardiovascular disease” (CVD), “coronary heart disease,” and “heart diseas$.” The final set was limited to the English-language literature and identified 494 unique articles published during 2009.
Closer inspection of titles and abstracts revealed well more than 100 articles directly relevant to the science and management of patients with CVD and depression or pronounced depressive symptoms. In light of this quantity, a thorough review of all new findings, editorials, and reviews is not feasible. Thus, we review here a few exciting articles in several distinct topical areas that could influence views of the relationship between depression and CVD as well as how we screen for and treat depression in patients with CVD. As with any review that is not strictly evidence-based, our choice of articles is subjective and incomplete, but we hope it will stimulate discussion and further exploration.
SUMMARY OF KEY FINDINGS AND CONTROVERSIES
The following numbered topics emerged as common themes or controversies from our survey of the 2009 literature. The remainder of this article will review findings in each of these areas in detail and discuss important clinical implications as appropriate.
1. Antidepressant use and adverse cardiac events. In surprising findings, antidepressant use was associated with increased risk of incident stroke, CVD, and sudden cardiac death in multiple large observational cohort studies. It is not known if the association is caused by unmeasured confounders or depressive symptom severity, although controlling for symptom severity did not reduce this elevated risk in some studies. Another interesting possibility is that the treatment-resistant depressed patient is at particularly high risk of CVD and death.
2. Effects of depression intervention in CVD patients. Four exciting randomized controlled trials on depression intervention in patients with CVD reported important efficacy results and suggested future directions for larger, definitive trials of depression treatment for these patients.
3. Depression screening and treatment in CVD patients. In the absence of large randomized controlled trials, the debate continues on whether depression screening or any type of depression treatment is beneficial, harmless, or harmful to patients with CVD. Continuation of this debate does not serve the health and well-being of patients or the public. Less controversial—and thus less discussed—is the important insight that psychiatric patients with depression should be routinely screened for cardiac disease and risk factors, as they are clearly at risk of CVD. We await clinical trials in this area to ensure that screening leads to improved CVD outcomes.
OBSERVATIONAL EVIDENCE ON ANTIDEPRESSANT USE AND CVD OUTCOMES
In an analysis of the Nurses’ Health Study, Whang et al examined the relationship of depressive symptoms and antidepressant use with sudden cardiac death and adverse cardiac events in 63,469 women without CVD.2 Depressive symptoms were assessed using the Mental Health Index, a five-item subscale of the Short Form-36 Health Survey. Among women who reported antidepressant use, most (61%) were taking a selective serotonin reuptake inhibitor (SSRI; sertraline, fluoxetine, paroxetine, or citalopram), while 39% reported use of other antidepressants. Women taking antidepressants were more likely to suffer sudden cardiac death, with a fully adjusted hazard ratio (HR) of 3.34 (95% confidence interval [CI], 2.03–5.50).
Krantz et al examined psychotropic medication use and risk of adverse cardiovascular events in 519 women from the Women’s Ischemia Syndrome Evaluation.3 Enrolled women underwent coronary angiography, were separated into four groups according to their psychotropic medication use (none, anxiolytics only, antidepressants only, or both anxiolytics and antidepressants), and were observed for a median of 5.9 years. Results revealed that women who received both medications had a higher risk for adverse cardiovascular events and higher all-cause mortality compared with those using neither medication, even after controlling for anxious and depressive symptoms. In addition, whereas the use of antidepressant medication was associated with a doubling of risk for subsequent CVD events (HR = 2.16; 95% CI, 1.21–3.93) and all-cause mortality (HR = 2.15; 95% CI, 1.16–3.98), use of anxiolytic medication alone was not. While this study did not examine cause of death, cardiac death is likely to have constituted a large proportion of total mortality in this cohort selected for likelihood of CAD.
Although CVD and death have long been outcomes of interest for those studying the effects of depression, additional end points have recently been investigated as well. In a prospective cohort study of 136,293 community-dwelling postmenopausal women in the Women’s Health Initiative, Smoller et al found that new antidepressant use was significantly associated with increased incidence of stroke and all-cause mortality but not with incidence of CHD.4 The rate of stroke per 1,000 person-years was 2.99 for subjects with no antidepressant use versus 4.16 for patients with new SSRI use; the rate of all-cause death was 7.79 versus 12.77, respectively. The rate of all-cause death for subjects with new tricyclic antidepressant use was 14.14 per 1,000 person-years. To address potential confounding by indication, the researchers obtained a propensity score from a logistic regression model to predict any new antidepressant use from demographic, lifestyle, risk factor, and comorbidity variables measured at baseline. New SSRI use was associated with a doubling of the risk of incident hemorrhagic stroke as well as fatal stroke. There were no significant interactions between use of SSRIs and use of statins or aspirin in terms of risk of hemorrhagic stroke.
In an interesting observational study of 7,709 patients with confirmed CAD but without a diagnosis of heart failure or depression (and without current antidepressant use), May et al found that a subsequent diagnosis of depression was associated with a significant 50% increase in the risk of heart failure.5 There was no difference, however, between depressed patients who were using antidepressants and those who were not.
Increased risk of bleeding with SSRI use, particularly in patients with CAD, has also been a concern. Kim et al evaluated 1,380 adults who received any anti depressant before CABG for in-hospital mortality or any bleeding events.6 After controlling for the percentage of patients taking SSRIs (78%), there were no significant differences between those taking SSRIs and those taking non-SSRIs in the rate of any bleeding events (6.5% vs 7.2%; odds ratio [OR] = 0.93; 95% CI, 0.50–1.76) or in-hospital mortality (3.1% vs 2.3%; OR = 0.88; 95% CI, 0.47–1.65). There was no increased risk of bleeding associated with SSRI use when the analysis was restricted to patients who received antiplatelet and anticoagulant therapy. Thus, compared with patients who received non-SSRI antidepressants, patients who received SSRIs preoperatively had no increased risk of bleeding or in-hospital mortality after CABG; however, this study did not evaluate the effect of no antidepressant use.
Another study hypothesized that the use of any drug with the potential to prolong cardiac repolarization would be associated with an increased risk of sudden death.7 Use of individual drugs was analyzed among 1,010 cases of sudden unexplained death and 3,030 living primary care controls, all from the community. SSRI use was associated with a doubling of risk of sudden death (OR = 2.21; 95% CI, 1.61–3.05), and tricyclic antidepressant use was associated with a nonsignificant trend toward increased risk (OR = 1.44; 95% CI, 0.96–2.13). Further analysis that stratified patients according to prior CVD showed that most of the association of SSRIs with sudden death was in those with existing CVD and not in those without CVD. Other drugs found to raise sudden death risk included the typical and atypical antipsychotics.
Summary and clinical implications
The Nurses’ Health Study analysis by Whang et al suggested that antidepressant use triples the risk of sudden cardiac death in healthy women, and the authors suggested that the association between fatal ventricular arrhythmias and antidepressant use be examined further. 2 The analysis of the Women’s Health Initiative by Smoller et al found that use of SSRIs and tricyclic antidepressants doubled the risk of fatal stroke in healthy women.4 The analysis of the Women’s Ischemia Syndrome Evaluation by Krantz et al revealed a doubling of the risk of CVD and death in women taking antidepressants who had been referred for coronary angiography.3 At the same time, May et al found no increase in the risk of heart failure conversion with antidepressant use in patients with CAD,5 and Kim et al found no increase in the risk of bleeding with use of SSRIs compared with non-SSRI antidepressants in patients with CAD undergoing CABG.6 Finally, in a population- and community-based case-control study, SSRI use was associated with an increased risk of sudden death, particularly in patients with CVD.7 So what are we to make of these findings?8
In all observational studies (including those reviewed above), unmeasured confounders pose a threat to the validity of any causal conclusions. A study recently tested some of the proposed confounders that might have existed in the above studies. Waldman et al examined racial differences in depressive symptoms and antidepressant treatment among a cohort of 864 consecutive patients with CHD undergoing diagnostic coronary angiography (727 white and 137 African American).9 While levels of depression were similar between the white and African American patients, the African Americans were less likely than their white counter-parts to receive antidepressant medications. Patients with only some high school, men, and patients with more severe depressive symptoms were significantly more likely to receive a prescription for antidepressants. Clearly, low education, male sex, and elevated depressive symptoms are related to poor prognosis for CHD, and the simple interpretation that antidepressant use is causing poorer outcomes is problematic.8
Two additional interpretations of the observational findings should be considered. First, confounding by indication (depressive symptom severity) might exist in these studies.10 In other words, patients who are prescribed antidepressant medication may be those with the most severe depressive illness, and it could be this severity, rather than the antidepressant use, that is causally implicated in the CVD incidence.11 However, all of the studies reviewed above either directly controlled for depressive symptom severity (at least as obtained at baseline) or used propensity scores or stratified subjects based on depression severity. The results showed an increased risk among those who were taking antidepressants. However, none of the studies examined depressive symptom severity during or at the end of the study or depression diagnosis and severity before antidepressant use; these data are needed for a clearer understanding of whether the results were confounded by indication.
Second, these findings are also consistent with a treatment-resistant depression phenotype.12 Krantz et al caution that it is not clear from their observational study3 whether medication use itself or depression refractory to treatment is implicated in the increased risk of CVD events and mortality. Depression that is refractory to treatment may be the type of depression that places patients at risk for sudden death, stroke, or CHD recurrence, so it may not be the antidepressant use per se that is associated with this risk. This phenomenon was documented in a secondary analysis13 of the largest-to-date randomized controlled trial of patients with MI undergoing treatment for depression (ENRICHD).14 It showed that those whose depressive symptoms did not respond to treatment had a higher risk of late mortality (ie, death ≥ 6 months after acute MI). This finding was replicated in 2009 in an important follow-up15 of the SADHART trial16; among patients with MI and major depression, treatment-resistant depression (ie, depression that failed to improve substantially during treatment with either sertraline or placebo) was strongly and independently associated with long-term mortality (HR = 2.39; 95% CI, 1.39–2.44; P < .001).15
What is needed next? Testing the alternative hypothesis— ie, that an unmeasured confounder may exist—is difficult, requiring new observational studies and measurement of the putative third common causes or previously unmeasured confounder. Other putative confounders would then be hypothesized and would need to be included in additional observational studies. To properly test the putative confounding by depressive symptom severity, future observational studies should examine initial depressive symptom severity prior to antidepressant use and then collect data on depressive symptom severity and antidepressant use as time-varying covariates to CVD outcomes. To test whether treatment-resistant depression is the phenotype driving the spurious observational association between antidepressant use and increased risk of CVD, the phenotype and its underlying causal mechanisms need to be better understood. Of course, rigorous and adequately powered randomized controlled trials of antidepressant use in patients with CVD would be a more straightforward way to test the observational association between antidepressant use and increased risk of CVD. We turn now to the recently published randomized controlled trials in this field.
NEW EVIDENCE FROM RANDOMIZED TRIALS IN PATIENTS WITH CVD AND DEPRESSION
Concerns have been voiced for some time about the ability to effectively treat depression and whether an effective depression treatment will affect the risk of CVD recurrence and mortality.8 Adding to these concerns is our limited knowledge of the causal pathways and behavioral and biologic mechanisms implicated in this risk association.1 For these reasons, results from new randomized controlled trials, such as the four summarized below, are important.
Rollman et al compared the effectiveness of telephone-delivered collaborative care (treatment group) and usual physician care (control group) for improving mental health quality of life and reducing depressive symptoms in 302 patients with depression after CABG.17 Patients were observed for 8 months following randomization. Mental health quality of life and depressive symptoms were both significantly improved in the treatment group relative to the control group. Significantly more patients in the treatment group had a 50% or greater reduction in depressive symptoms (50.0% vs 29.6% in control group, P < .001; number needed to treat = 4.9 [95% CI, 3.2–10.4]). Men particularly benefited from the treatment. This trial suggests that collaborative care can be delivered effectively (and potentially cost-efficiently) over the phone.
Freedland et al also evaluated depression treatment in 123 patients with major or minor depression who underwent CABG.18 Their primary objective was to determine the efficacy of two behavioral treatments (cognitive behavioral therapy [CBT] or supportive stress management) compared with usual care. Significantly more patients in both the CBT group (71%) and the stress management group (57%) had a low score (indicating less severe depressive symptoms) on the clinician-based Hamilton Rating Scale for Depression compared with the usual care group (33%). These results were maintained 6 months after the end of the trial. Secondary measures of depressive symptoms, anxiety, and quality of life were also significantly improved in the depression treatment groups compared with the usual care group. This trial is important for the following reasons:
- The use of a second control group, the stress management group, represents a strict, high-quality design that controls for professional attention, generic or placebo therapy effect, and time or effort on the part of the patient.
- The second control group also provides treatment options for the patient, as both CBT and stress management were beneficial.
- Outcome assessors were blinded to treatment assignment, an important design feature in behavioral trials.
In a rigorously conducted randomized, double-blind, placebo-controlled trial, Carney et al tested whether 2 g/day of omega-3 acid ethyl esters (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) improved depressive symptoms in 122 patients with major depression and CHD.19 Patients in both the omega-3 and placebo groups received sertraline (50 mg/day) during the 10-week trial. A deficiency of omega-3 fatty acids has been implicated in both depression and CHD and is a possible causal link between the two diseases. Also, there is some evidence that the efficacy of antidepressants is increased by the addition of omega-3 supplementation. Unfortunately, there were no differences in self-reported or clinician-assessed depressive symptoms or in predefined depression remission at the study’s end. The trial included a 2-week adherence run-in period, ensuring that medication adherence in the trial was excellent (97%), and concluded that omega-3 supplementation, at least at these dosage levels, does not improve depression outcomes.
In the Coronary Psychosocial Evaluation Studies (COPES) randomized controlled trial, Davidson et al compared 6 months of an enhanced care intervention with usual depression care among 157 patients with ACS and persistently elevated depressive symptoms.20 Under the enhanced care intervention, patients received either problem-solving therapy or antidepressant medication, depending on their preference, and then had the option of later augmentation with the other treatment, intensification of the initial treatment, or switching of treatments, if indicated by depressive symptom severity (stepped care). The purpose of the trial was to determine the acceptability and efficacy of depression treatment among patients with ACS, who often neither agree with the diagnosis of depression nor had been seeking treatment for depression. Significantly more patients were satisfied with their depression care in the intervention arm, and depressive symptoms and major adverse cardiac events (nonfatal MI, hospitalization for unstable angina, or all-cause mortality) were significantly reduced in the intervention arm compared with the usual care arm. The absolute numbers were very small; at the end of the trial, 3 patients in the intervention group and 10 patients in the usual care group had major adverse cardiac events (4% and 13%, respectively; log-rank test, χ21 = 3.93; P = .047). The results suggested that involving patients in the type of depression care they receive (medication and/or psychotherapy) and stepping treatments aggressively may be methods to improve the treatment of depression in patients with CHD. In addition, persistently depressed patients may be an interesting patient group to select for future trials, as usual care has resulted in large reductions in depressive symptoms in some previous trials but not in this study of patients with persistent depression.
Summary and clinical implications
Each of these four efficacy trials adds critical information to the evidence base. Depressed patients who have undergone CABG can be effectively treated in primary care settings with integrative care,17 and CBT is also extremely effective for these patients.18 Additional studies of omega-3 supplementation should not be pursued at this time, but using a run-in period to better identify patients who are prepared to engage in treatment is a prudent idea and should be used in future trials in this area.19 Patients with CHD and persistent depressive symptoms are a promising group to target for depression therapy, and asking patients to choose their type of depression treatment may improve response to therapy for both depression and CHD.20
DEPRESSION SCREENING, REFERRAL, AND TREATMENT IN PATIENTS WITH CVD
We finish with the least evidence-based and most controversial issue in the area of depression and CVD. This controversy started in 2008 when the American Heart Association recommended in an advisory (endorsed by the American Psychiatric Association) that “screening tests for depressive symptoms should be applied to identify patients who may require further assessment and treatment” if appropriate referral for further depression assessment and treatment is available.21 Partly in response to this advisory, Thombs et al conducted a systematic review of the evidence on whether screening or treatment improves outcomes of depression or CVD in patients with CVD.22 They found no trial that tested whether depression screening was beneficial in patients with CVD, and the randomized controlled trials of depression treatment provided evidence of only mild improvement of depressive symptoms and no improvement in CVD outcome. Therefore, they questioned whether routine depression screening was appropriate.22
In at least eight editorials, letters, and reviews published on this subject in 2009, investigators continued to debate this issue.23–30 Below we provide a simplified list of reasons presented for and against screening and subsequent treatment raised in these articles.
Arguments for depression screening and treatment
The proponents of screening contend that depression is highly prevalent in patients with CVD and is clearly a risk marker for increased adverse events, reduced quality of life, and poorer adherence to treatment.24 They argue that since there are plausible biologic and behavioral mechanisms for this association, and since SSRI use improves depressive symptoms in other patient populations and is safe in patients with CVD, health care providers should not hesitate to screen and refer patients for appropriate depression treatment. At the same time, they have cautioned that SSRIs interact with anti coagulants and that bleeding should be monitored closely in patients with CVD who are taking SSRIs.24
Whooley28 noted that although there are controversial findings in this area, depression screening provided in conjunction with collaborative care depression management is cost-effective and has a documented positive impact on depression, if not on CVD outcomes.17,31 She observed that there are some costs to screening, such as false-positive findings (resulting in stigma for patients incorrectly diagnosed) and diversion of resources from other health care needs. However, Whooley suggested that primary care providers, rather than cardiologists, should conduct depression screening and that patients should undergo screening only when an established collaborative care treatment protocol exists.28
Carney et al argued that depression, like age, clearly marks CVD risk, and that health care providers should aggressively treat readily modifiable CVD risk factors.23 They added that because of the strong association between depression and medication nonadherence,32 providers should carefully monitor patient adherence to life-saving therapies.
Taking another tack, Shemesh and colleagues advocated the importance of documenting the prevalence of suicidal ideation and intent if recommendations to screen for depression in CVD patient populations were implemented.25 Using a sample of more than 1,000 patients with CVD, they determined the prevalence of suicidal ideation (12.0%) and the number of patients who required hospitalization for risk of suicide (0.5%) when routine depression screening occurred in a large cardiology clinic. They concluded that identification and stabilization of imminently suicidal patients would be a benefit of universal screening and that there is a high societal cost to neglecting suicidal ideation, intent, and risk in patients with CVD. However, more patients would need immediate thorough psychiatric evaluations for safety, which would affect resource allocation and cost in cardiology clinics.
Arguments against depression screening and treatment
The main argument against screening for and treating depression in patients with CVD is that there are neither randomized controlled trials nor systematic evidence-based reviews showing that screening for depression and/or referring for additional treatment sufficiently improves outcomes for depression or CVD, and that existing evidence does not support the recommendation to screen all patients with CVD.22,30 Furthermore, antidepressant use is associated with only mild improvement in depressive symptoms, even in other patient populations,33 and publication bias (“the file-drawer problem”) has prevented the publication of antidepressant trials with null results, thereby skewing the evidence base.34 In addition, considerable health care resources would be needed to mount such a large screening effort, and these resources would come at the expense of other efforts. Finally, the adverse effects of medications and the inevitability of some false-positive screening results must be weighed against any benefit that might occur with universal screening.35
In addition to the arguments above, Ziegelstein et al,29 in commenting on the American Heart Association advisory,21 wryly observed that there is far greater observational evidence that depressed patients seen in mental health settings are at risk for incident and recurrent CVD and that there should be universal screening and referral for CVD in patients with depression. They contended as well that the evidence is insufficient to recommend that patients with CVD undergo universal depression screening and referral.
Summary and clinical implications
Although we were hesitant to raise this tense and often emotional issue, we are in favor of routine, algorithm-based depression screening by all cardiologists, with the critical proviso that a nationwide and/or Centers for Medicare and Medicaid Services–coordinated randomized controlled trial be conducted to evaluate this practice. All patients with pronounced depressive symptoms should be referred to the trial, and two depression treatments should be evaluated, such as usual referral versus telephone-based collaborative care17 or enhanced depression care.20 Such a trial would allow us to ensure that data are collected on the cost,36 the benefit, and even the possible harms associated with routine depression screening for patients with CVD, and we could ascertain if there is an acceptable, beneficial treatment for depression that can be delivered and definitively tested.
- Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med 2008; 121( 11 suppl 2):S20–S27.
- Whang W, Kubzansky LD, Kawachi I, et al Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses’ Health Study. J Am Coll Cardiol 2009; 53:950–958.
- Krantz DS, Whittaker KS, Francis JL, et al Psychotropic medication use and risk of adverse cardiovascular events in women with suspected coronary artery disease: outcomes from the Women’s Ischemia Syndrome Evaluation (WISE) study. Heart 2009; 95:1901–1906.
- Smoller JW, Allison M, Cochrane BB, et al Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative study. Arch Intern Med 2009; 169:2128–2139.
- May HT, Horne BD, Carlquist JF, Sheng X, Joy E, Catinella AP. Depression after coronary artery disease is associated with heart failure. J Am Coll Cardiol 2009; 53:1440–1447.
- Kim DH, Daskalakis C, Whellan DJ, et al Safety of selective serotonin reuptake inhibitor in adults undergoing coronary artery bypass grafting. Am J Cardiol 2009; 103:1391–1395.
- Jolly K, Gammage MD, Cheng KK, Bradburn P, Banting MV, Langman MJ. Sudden death in patients receiving drugs tending to prolong the QT interval. Br J Clin Pharmacol 2009; 68:743–751.
- Jolly K, Langman MJ. Psychotropic medication: curing illness or creating problems? Heart 2009; 95:1893–1894.
- Waldman SV, Blumenthal JA, Babyak MA, et al Ethnic differences in the treatment of depression in patients with ischemic heart disease. Am Heart J 2009; 157:77–83.
- Salas M, Hofman A, Stricker BH. Confounding by indication: an example of variation in the use of epidemiologic terminology. Am J Epidemiol 1999; 149:981–983.
- Carney RM, Freedland KE. Treatment-resistant depression and sudden cardiac death [letter]. J Am Coll Cardiol 2009; 54:958–959.
- Carney RM, Freedland KE. Treatment-resistant depression and mortality after acute coronary syndrome. Am J Psychiatry 2009; 166:410–417.
- Carney RM, Blumenthal JA, Freedland KE, et al Depression and late mortality after myocardial infarction in the Enhancing Recovery in Coronary Heart Disease (ENRICHD) study. Psychosom Med 2004; 66:466–474.
- Berkman LF, Blumenthal J, Burg M, et al Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 2003; 289:3106–3116.
- Glassman AH, Bigger JT, Gaffney M. Psychiatric characteristics associated with long-term mortality among 361 patients having an acute coronary syndrome and major depression: seven-year follow-up of SADHART participants. Arch Gen Psychiatry 2009; 66:1022–1029.
- Glassman AH, O’Connor CM, Califf RM, et al Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002; 288:701–709.
- Rollman BL, Belnap BH, LeMenager MS, et al Telephone-delivered collaborative care for treating post-CABG depression: a randomized controlled trial. JAMA 2009; 302:2095–2103.
- Freedland KE, Skala JA, Carney RM, et al Treatment of depression after coronary artery bypass surgery: a randomized controlled trial. Arch Gen Psychiatry 2009; 66:387–396.
- Carney RM, Freedland KE, Rubin EH, Rich MW, Steinmeyer BC, Harris WS. Omega-3 augmentation of sertraline in treatment of depression in patients with coronary heart disease: a randomized controlled trial. JAMA 2009; 302:1651–1657.
- Davidson KW, Rieckmann N, Clemow L, et al Enhanced depression care for patients with acute coronary syndrome and persistent depressive symptoms: Coronary Psychosocial Evaluation Studies randomized controlled trial. Arch Intern Med 2010; 170:600–608.
- Lichtman JH, Bigger JT, Blumenthal JA, et al Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation 2008; 118:1768–1775.
- Thombs BD, de Jonge P, Coyne JC, et al Depression screening and patient outcomes in cardiovascular care: a systematic review. JAMA 2008; 300:2161–2171.
- Carney RM, Freedland KE, Jaffe AS. Depression screening in patients with heart disease [letter]. JAMA 2009; 301:1337–1338.
- Pozuelo L, Zhang J, Franco K, Tesar G, Penn M, Jiang W. Depression and heart disease: what do we know, and where are we headed? Cleve Clin J Med 2009; 76:59–70.
- Shemesh E, Annunziato RA, Rubinstein D, et al Screening for depression and suicidality in patients with cardiovascular illnesses. Am J Cardiol 2009; 104:1194–1197.
- Thombs BD, Adeponle AB, Kirmayer LJ, Rousseau C, Ziegelstein RC. More antidepressants for African Americans with coronary heart disease? Maybe—maybe not [letter]. Am Heart J 2009; 157:e33; author reply,e35–e37.
- Whang W, Davidson KW. Is it time to treat depression in patients with cardiovascular disease? Circulation 2009; 120:99–100.
- Whooley MA. To screen or not to screen? Depression in patients with cardiovascular disease. J Am Coll Cardiol 2009; 54:891–893.
- Ziegelstein RC, Thombs BD, Coyne JC, de Jonge P. Routine screening for depression in patients with coronary heart disease: never mind. J Am Coll Cardiol 2009; 54:886–890.
- Thombs BD, Jewett LR, Knafo R, Coyne JC, Ziegelstein RC. Learning from history: a commentary on the American Heart Association Science Advisory on depression screening. Am Heart J 2009; 158:503–505.
- Unutzer J, Katon W, Callahan CM, et al Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA 2002; 288:2836–2845.
- Rieckmann N, Gerin W, Kronish IM, et al Course of depressive symptoms and medication adherence after acute coronary syndromes: an electronic medication monitoring study. J Am Coll Cardiol 2006; 48:2218–2222.
- Kirsch I, Deacon BJ, Huedo-Medina TB, et al Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS Med 2008; 5:e45.
- Turner EH, Matthews AM, Linardatos E, Tell RA, Rosenthal R. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med 2008; 358:252–260.
- Thombs BD, de Jonge P, Ziegelstein RC. Depression screening in patients with heart disease [reply to letter]. JAMA 2009; 301:1338.
- Frasure-Smith N, Lespérance F. Depression and cardiac risk: present status and future directions. Heart 2010; 96:173–176.
- Carney RM, Freedland KE. Depression in patients with coronary heart disease. Am J Med 2008; 121( 11 suppl 2):S20–S27.
- Whang W, Kubzansky LD, Kawachi I, et al Depression and risk of sudden cardiac death and coronary heart disease in women: results from the Nurses’ Health Study. J Am Coll Cardiol 2009; 53:950–958.
- Krantz DS, Whittaker KS, Francis JL, et al Psychotropic medication use and risk of adverse cardiovascular events in women with suspected coronary artery disease: outcomes from the Women’s Ischemia Syndrome Evaluation (WISE) study. Heart 2009; 95:1901–1906.
- Smoller JW, Allison M, Cochrane BB, et al Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative study. Arch Intern Med 2009; 169:2128–2139.
- May HT, Horne BD, Carlquist JF, Sheng X, Joy E, Catinella AP. Depression after coronary artery disease is associated with heart failure. J Am Coll Cardiol 2009; 53:1440–1447.
- Kim DH, Daskalakis C, Whellan DJ, et al Safety of selective serotonin reuptake inhibitor in adults undergoing coronary artery bypass grafting. Am J Cardiol 2009; 103:1391–1395.
- Jolly K, Gammage MD, Cheng KK, Bradburn P, Banting MV, Langman MJ. Sudden death in patients receiving drugs tending to prolong the QT interval. Br J Clin Pharmacol 2009; 68:743–751.
- Jolly K, Langman MJ. Psychotropic medication: curing illness or creating problems? Heart 2009; 95:1893–1894.
- Waldman SV, Blumenthal JA, Babyak MA, et al Ethnic differences in the treatment of depression in patients with ischemic heart disease. Am Heart J 2009; 157:77–83.
- Salas M, Hofman A, Stricker BH. Confounding by indication: an example of variation in the use of epidemiologic terminology. Am J Epidemiol 1999; 149:981–983.
- Carney RM, Freedland KE. Treatment-resistant depression and sudden cardiac death [letter]. J Am Coll Cardiol 2009; 54:958–959.
- Carney RM, Freedland KE. Treatment-resistant depression and mortality after acute coronary syndrome. Am J Psychiatry 2009; 166:410–417.
- Carney RM, Blumenthal JA, Freedland KE, et al Depression and late mortality after myocardial infarction in the Enhancing Recovery in Coronary Heart Disease (ENRICHD) study. Psychosom Med 2004; 66:466–474.
- Berkman LF, Blumenthal J, Burg M, et al Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 2003; 289:3106–3116.
- Glassman AH, Bigger JT, Gaffney M. Psychiatric characteristics associated with long-term mortality among 361 patients having an acute coronary syndrome and major depression: seven-year follow-up of SADHART participants. Arch Gen Psychiatry 2009; 66:1022–1029.
- Glassman AH, O’Connor CM, Califf RM, et al Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002; 288:701–709.
- Rollman BL, Belnap BH, LeMenager MS, et al Telephone-delivered collaborative care for treating post-CABG depression: a randomized controlled trial. JAMA 2009; 302:2095–2103.
- Freedland KE, Skala JA, Carney RM, et al Treatment of depression after coronary artery bypass surgery: a randomized controlled trial. Arch Gen Psychiatry 2009; 66:387–396.
- Carney RM, Freedland KE, Rubin EH, Rich MW, Steinmeyer BC, Harris WS. Omega-3 augmentation of sertraline in treatment of depression in patients with coronary heart disease: a randomized controlled trial. JAMA 2009; 302:1651–1657.
- Davidson KW, Rieckmann N, Clemow L, et al Enhanced depression care for patients with acute coronary syndrome and persistent depressive symptoms: Coronary Psychosocial Evaluation Studies randomized controlled trial. Arch Intern Med 2010; 170:600–608.
- Lichtman JH, Bigger JT, Blumenthal JA, et al Depression and coronary heart disease: recommendations for screening, referral, and treatment: a science advisory from the American Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Psychiatric Association. Circulation 2008; 118:1768–1775.
- Thombs BD, de Jonge P, Coyne JC, et al Depression screening and patient outcomes in cardiovascular care: a systematic review. JAMA 2008; 300:2161–2171.
- Carney RM, Freedland KE, Jaffe AS. Depression screening in patients with heart disease [letter]. JAMA 2009; 301:1337–1338.
- Pozuelo L, Zhang J, Franco K, Tesar G, Penn M, Jiang W. Depression and heart disease: what do we know, and where are we headed? Cleve Clin J Med 2009; 76:59–70.
- Shemesh E, Annunziato RA, Rubinstein D, et al Screening for depression and suicidality in patients with cardiovascular illnesses. Am J Cardiol 2009; 104:1194–1197.
- Thombs BD, Adeponle AB, Kirmayer LJ, Rousseau C, Ziegelstein RC. More antidepressants for African Americans with coronary heart disease? Maybe—maybe not [letter]. Am Heart J 2009; 157:e33; author reply,e35–e37.
- Whang W, Davidson KW. Is it time to treat depression in patients with cardiovascular disease? Circulation 2009; 120:99–100.
- Whooley MA. To screen or not to screen? Depression in patients with cardiovascular disease. J Am Coll Cardiol 2009; 54:891–893.
- Ziegelstein RC, Thombs BD, Coyne JC, de Jonge P. Routine screening for depression in patients with coronary heart disease: never mind. J Am Coll Cardiol 2009; 54:886–890.
- Thombs BD, Jewett LR, Knafo R, Coyne JC, Ziegelstein RC. Learning from history: a commentary on the American Heart Association Science Advisory on depression screening. Am Heart J 2009; 158:503–505.
- Unutzer J, Katon W, Callahan CM, et al Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA 2002; 288:2836–2845.
- Rieckmann N, Gerin W, Kronish IM, et al Course of depressive symptoms and medication adherence after acute coronary syndromes: an electronic medication monitoring study. J Am Coll Cardiol 2006; 48:2218–2222.
- Kirsch I, Deacon BJ, Huedo-Medina TB, et al Initial severity and antidepressant benefits: a meta-analysis of data submitted to the Food and Drug Administration. PLoS Med 2008; 5:e45.
- Turner EH, Matthews AM, Linardatos E, Tell RA, Rosenthal R. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med 2008; 358:252–260.
- Thombs BD, de Jonge P, Ziegelstein RC. Depression screening in patients with heart disease [reply to letter]. JAMA 2009; 301:1338.
- Frasure-Smith N, Lespérance F. Depression and cardiac risk: present status and future directions. Heart 2010; 96:173–176.
Emotional predictors and behavioral triggers of acute coronary syndrome
Numerous systematic reviews indicate that psychosocial factors are predictive of an initial acute coronary syndrome (ACS),1–8 defined as myocardial infarction (MI), unstable angina, or sudden cardiac death. Psychosocial factors under active investigation for their role in ACS onset include chronic negative emotional states (eg, depression, hostility, anxiety) as well as situational and behavioral triggers (eg, acute anger, unusual intense physical activity). This review will present evidence for each grouping of risk markers and then discuss the studies required to better identify and treat patients who have these psychosocial vulnerabilities.
NEGATIVE EMOTIONAL STATES
Increasing epidemiologic and pathophysiologic evidence suggests that depression, anxiety, and hostility/anger may each be an independent risk factor for initial occurrence of a cardiovascular event.4,8 The vast majority of evidence has been accumulated for depression, and many meta-analyses and systematic reviews now indicate that depression—as either a clinical diagnosis or an elevation in self-reported symptoms—is a strong, consistent, independent predictor of ACS incidence.9–11
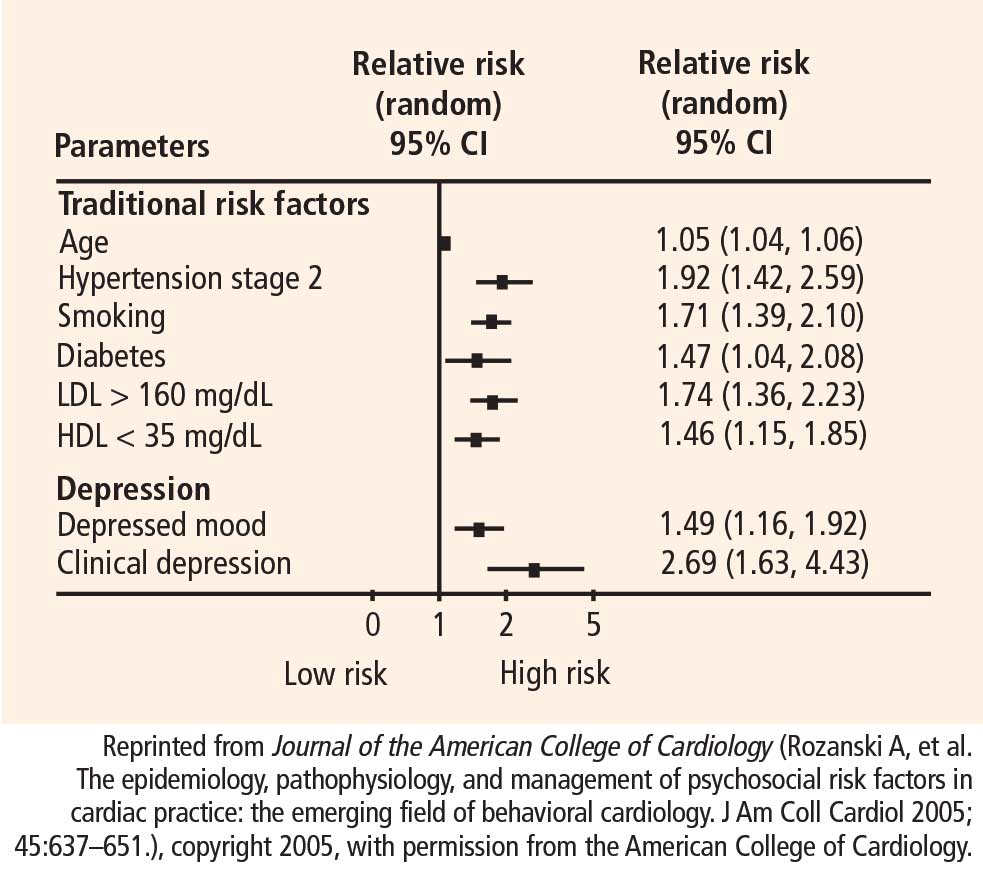
Major depression
Major depressive disorder is most appropriately diagnosed through direct patient interview, preferably by trained professionals who look for evidence of severely depressed mood lasting at least 2 consecutive weeks, other concomitant symptoms (such as change in eating or sleeping habits), and evidence of associated functional impairment. Because this interview approach is not convenient for large epidemiologic studies, evaluation of major depression by interview in longitudinal epidemiologic studies has been sparse,12,13 and only a limited number of other studies have also evaluated the role of a history of depressive disorders14 or a history of depression treatment.14–18
Depressive symptoms
The impact of self-reported depressive symptoms on cardiac outcomes has been studied more widely.in community settings, among the elderly, and in various cardiac settings.using scales such as the Beck Depression Inventory and the Center for Epidemiological Studies Depression Scale. Notably, these scales assess only the presence of recent depressive symptoms. Nevertheless, despite this important limitation, one-time assessment of healthy participants using these scales has generally revealed a significant relationship between depressive symptoms and future adverse cardiac events.9,18 As further evidence of a gradient relationship, the frequency of cardiac events increases as the level of depressive symptoms increases.13,19
Depression is a complex phenotype, and some have argued that subtypes, or intermediary phenotypes, of depression may be particularly predictive of ACS incidence and recurrence.20 Interestingly, the first article ever published documenting a link between depression and coronary artery disease focused exclusively on melancholic depression, or endogenous depression.21
Anxiety
Anxiety is defined as a future-oriented negative emotion resulting from perceived threat and accompanied by perceived lack of control and lack of predictability.22 Like depression, anxiety occurs along a continuum, but it is characterized as pathological when it becomes chronic, has intensity out of proportion to any real threat, and leaves the affected person with seriously impaired ability to function.
There are many recognized anxiety disorders, including generalized anxiety disorder, panic attacks, obsessive-compulsive disorder, posttraumatic stress syndrome, and various forms of phobia. As a group, these anxiety disorders constitute one of the most common forms of psychiatric illness. Moreover, anxiety disorders and major depression are highly comorbid.23 Although some interesting epidemiologic studies have indicated that anxiety may predict new ACS events,24–26 there are a few that have yielded mixed results.27,28
Hostility and anger
Angry and hostile feelings are overlapping emotions and, when experienced frequently, indicate broader, more enduring temperaments or personality styles. Hostility is a cynical, suspicious, and resentful attitude toward others; negative social exchanges, such as sarcasm or impatience, typify individuals with hostility. In contrast, individuals with anger difficulties can have warm, appropriate interpersonal skills and may display verbal aggression or other outbursts only when provoked. Unlike depressive and anxiety disorders, professionally diagnosed, syndromal anger and hostility are not yet recognized by psychiatric nosology.
Relatively few longitudinal studies have been conducted using measures of hostility in healthy cohorts. These studies have reported both the presence29,30 and the absence31 of positive associations. In a recent systematic review, 7 of 11 studies showed hostility to be a significant risk factor for CHD.8 A case-control study involving participants in the Multiple Risk Factor Intervention Trial (MRFIT) employed a structured interview (as opposed to a questionnaire) designed to elicit information regarding signs of hostility, including irritation, arrogance, uncooperativeness, and angry feelings.30 It revealed that men with high hostility levels were more likely to die of cardiovascular disease than men with low hostility levels (adjusted odds ratio = 1.61; 95% CI, 1.09 to 2.39) in this initially healthy but high-risk cohort.30 The investigators chose the structured interview to overcome participants’ potential to underreport or underrecognize hostile tendencies when completing a questionnaire.30
Over time, specific measurements of chronic anger,32–37 including both unhealthy anger expression34 and suppression,37 have accumulated, permitting examination of their relationship to adverse cardiac outcomes in longitudinal follow-up of disease-free cohorts. A number of these studies have shown a positive association.32,33,35–37 Moreover, a recent report from the Framingham study demonstrated an association between anger/hostility and the development of atrial fibrillation and total-cause mortality over a 10year period,38 and another study has observed a relationship between anger expression and development of stroke.39 Combined, these observations suggest that anger is worthy of further study as a factor in the development of CHD. As with hostility, however, various subscales have been used to study anger, which makes standardization across studies difficult.
Data specific to imminent ACS risk are few
The majority of the negative emotional states have not been tested for their ability to predict an ACS in the near future. Further, negative emotional and cognitive states that may be implicated in the development of CHD or other cardiovascular disease may be quantitatively or even qualitatively different from those psychosocial factors that identify a patient at imminent risk for an ACS.
SITUATIONAL AND BEHAVIORAL TRIGGERS
Evidence for imminent risk or trigger status can be obtained from retrospective reports, from witness accounts (if available), or prospectively from electronic diaries coupled with ambulatory electrocardiogram recordings or an implantable cardioverter-defibrillator (ICD). Triggers of an ACS include external stimuli (eg, cocaine use, air pollution, ambient temperature), patient activities (eg, eating a meal high in saturated fat, unusual physical exertion), and emotional reactions such as extreme anger or anxiety.1,2,7,40,41 Myocardial stunning has also been reported immediately after acute emotional stress but has generally been reversible in these cases.42,43 In an observational study, Burg et al found that ICD shocks preceded by an anger episode (as recorded by diary) were more frequent in patients with high trait levels of anger (according to the Speilberger Trait Personality Inventory) and that shocks preceded by an anxiety episode were more frequent in patients with high trait levels of anxiety.44 A systematic review by Strike and Steptoe showed that physical exertion (particularly in poorly conditioned individuals), emotional stress, anger, and extreme excitement are all probable triggers for an ACS.7 A recent meta-analysis suggests that emotional stress immediately precedes MI in approximately 7% of MI cases and is a more frequent ACS trigger for women than for men.1
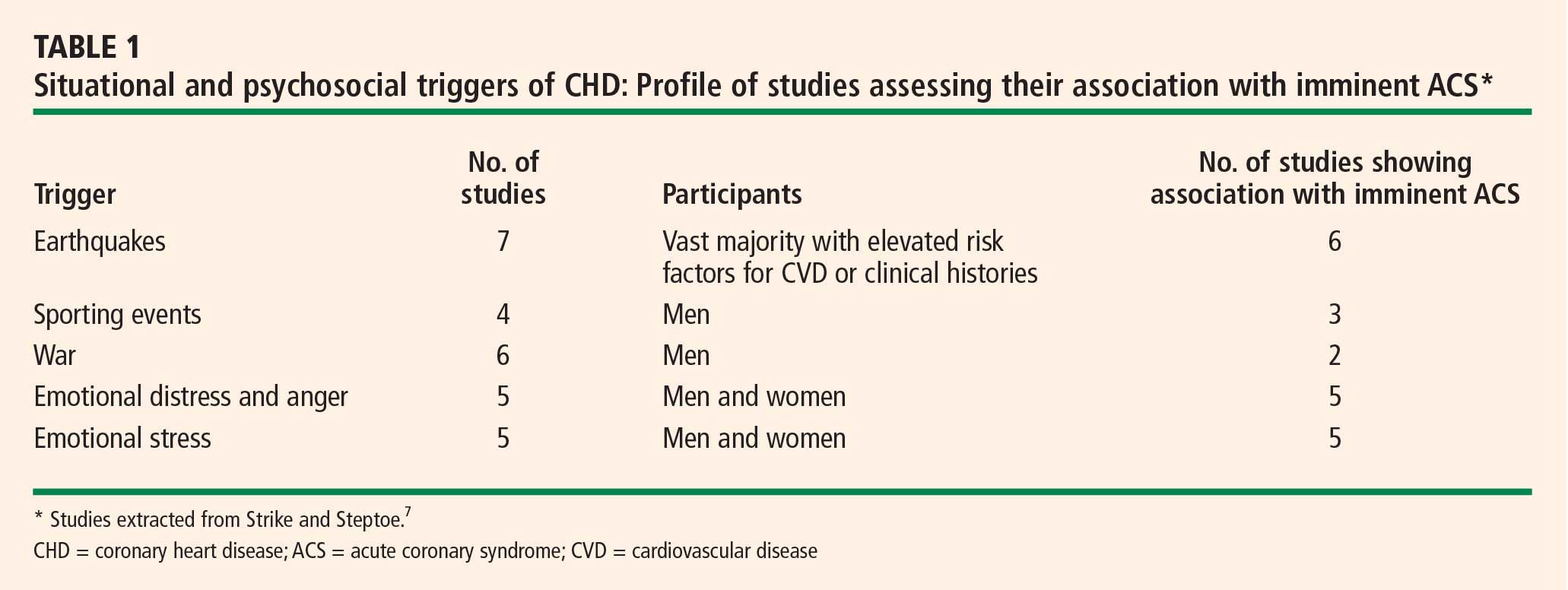
THE PSYCHOSOCIALLY VULNERABLE PATIENT
This selective overview suggests that patients’ emotional states are frequently implicated in the onset of an ACS but that the use of behavioral or emotional information to identify those at high risk for imminent ACS onset is not yet practical. Triggers are, by definition, state-like, but their impact may be amplified by trait-like characteristics, such as high dispositional anger, anxiety, hostility, or chronic environmental stress.
The previously mentioned analysis of the MRFIT study by Matthews et al30 suggests that patients identified as “high risk” by conventional risk factors, and who additionally possess high trait hostility, should be monitored closely, as they are at risk for cardiovascular death. Additionally, the Burg study of patients with ICDs suggests that arrhythmia may be induced by acute anxiety or anger in those prone to have such emotions chronically.44
Such studies have two research implications. First, controlled laboratory studies that induce acute negative emotion in those with chronic negative emotional states may help reveal the pathophysiologic processes implicated in immediate ACS onset. Interventions for these psychosocially vulnerable patients await such studies. Second, we must begin to consider that in addition to the psychosocially vulnerable patient, we may have psychosocially vulnerable situations, about which we know little at this time.
Acknowledgments
The author thanks Lucia Dettenborn, PhD, for her assistance with the presentation on which this manuscript, in part, is based.
This work was supported by grants HC-25197, HL-76857, HL-80665, and HL84034 from the National Heart, Lung, and Blood Institute. The project described was supported by grant number UL1 RR024156 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and the NIH Roadmap for Medical Research, and its contents are solely the responsibility of the author and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at http://www.ncrr.nih.gov. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
- Culić V, Eterović D, Mirić D. Meta-analysis of possible external triggers of acute myocardial infarction. Int J Cardiol 2005; 99:1–8.
- Kloner RA. Natural and unnatural triggers of myocardial infarction. Prog Cardiovasc Dis 2006; 48:285–300.
- Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146538 participants in 54 observational studies. Eur Heart J 2006; 27:2763–2774.
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol 2005; 45:637–651.
- Rosengren A, Hawken S, Ounpuu S, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364:953–962.
- Servoss SJ, Januzzi JL, Muller JE. Triggers of acute coronary syndromes. Prog Cardiovasc Dis 2002; 44:369–380.
- Strike PC, Steptoe A. Behavioral and emotional triggers of acute coronary syndromes: a systematic review and critique. Psychosom Med 2005; 67:179–186.
- Suls J, Bunde J. Anger, anxiety, and depression as risk factors for cardiovascular disease: the problems and implications of overlapping affective dispositions. Psychol Bull 2005; 131:260–300.
- Rugulies R. Depression as a predictor for coronary heart disease: a review and meta-analysis. Am J Prev Med 2002; 23:51–61.
- Wulsin LR, Singal BM. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003; 65:201–210.
- Van der Kooy K, van Hout H, Marwijk H, Marten H, Stehouwer C, Beekman A. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry 2007; 22:613–626.
- Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med 1998; 158:1422–1426.
- Penninx BW, Beekman AT, Honig A, et al. Depression and cardiac mortality: results from a community-based longitudinal study. Arch Gen Psychiatry 2001; 58:221–227.
- Pratt LA, Ford DE, Crum RM, Armenian HK, Gallo JJ, Eaton WW. Depression, psychotropic medication, and risk of myocardial infarction. Prospective data from the Baltimore ECA follow-up. Circulation 1996; 94:3123–3129.
- Cohen HW, Madhavan S, Alderman MH. History of treatment for depression: risk factor for myocardial infarction in hypertensive patients. Psychosom Med 2001; 63:203–209.
- Rutledge T, Reis SE, Olson MB, et al. Depression symptom severity and reported treatment history in the prediction of cardiac risk in women with suspected myocardial ischemia: the NHLBI-sponsored WISE study. Arch Gen Psychiatry 2006; 63:874–880.
- Sauer WH, Berlin JA, Kimmel SE. Effect of antidepressants and their relative affinity for the serotonin transporter on the risk of myocardial infarction. Circulation 2003; 108:32–36.
- Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women: the Women’s Health Initiative (WHI). Arch Intern Med 2004; 164:289–298.
- Rowan PJ, Haas D, Campbell JA, Maclean DR, Davidson KW. Depressive symptoms have an independent, gradient risk for coronary heart disease incidence in a random, population-based sample. Ann Epidemiol 2005; 15:316–320.
- Davidson KW, Rieckmann N, Rapp MA. Definitions and distinctions among depressive syndromes and symptoms: implications for a better understanding of the depression-cardiovascular disease association. Psychosom Med 2005; 67(Suppl 1):S6–S9.
- Malzberg B. Mortality among patients with involution melancholia. Am J Psychiatry 1937; 93:1231–1238.
- Barlow DH. Anxiety and its Disorders: The Nature and Treatment of Anxiety and Panic. New York, NY: Guilford Press; 1988.
- Hirschfeld RM. The comorbidity of major depression and anxiety disorders: recognition and management in primary care. Prim Care Companion J Clin Psychiatry 2001; 3:244–254.
- Kawachi I, Colditz GA, Ascherio A, et al. Prospective study of phobic anxiety and risk of coronary heart disease in men. Circulation 1994; 89:1992–1997.
- Kubzansky LD, Kawachi I, Weiss ST, Sparrow D. Anxiety and coronary heart disease: a synthesis of epidemiological, psychological, and experimental evidence. Ann Behav Med 1998; 20:47–58.
- Kubzansky LD, Kawachi I, Spiro A III, et al. Is worrying bad for your heart? A prospective study of worry and coronary heart disease in the Normative Aging Study. Circulation 1997; 95:818–824.
- Todaro JF, Shen BJ, Niaura R, Spiro A III, Ward KD. Effect of negative emotions on frequency of coronary heart disease (The Normative Aging Study). Am J Cardiol 2003; 92:901–906.
- McCarron P, Gunnell D, Harrison GL, Okasha M, Davey Smith G. Temperament in young adulthood and later mortality: prospective observational study. J Epidemiol Community Health 2003; 57:888–892.
- Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the Normative Aging Study. Psychosom Med 2000; 62:7–16.
- Matthews KA, Gump BB, Harris KF, Haney TL, Barefoot JC. Hostile behaviors predict cardiovascular mortality among men enrolled in the Multiple Risk Factor Intervention Trial. Circulation 2004; 109:66–70.
- Sykes DH, Arveiler D, Salters CP, et al. Psychosocial risk factors for heart disease in France and Northern Ireland: the Prospective Epidemiological Study of Myocardial Infarction (PRIME). Int J Epidemiol 2002; 31:1227–1234.
- Haynes SG, Feinleib M, Kannel WB. The relationship of psychosocial factors to coronary heart disease in the Framingham Study. III. Eight-year incidence of coronary heart disease. Am J Epidemiol 1980; 111:37–58.
- Chang PP, Ford DE, Meoni LA, Wang NY, Klag MJ. Anger in young men and subsequent premature cardiovascular disease: the Precursors Study. Arch Intern Med 2002; 162:901–906.
- Eng PM, Fitzmaurice G, Kubzansky LD, Rimm EB, Kawachi I. Anger expression and risk of stroke and coronary heart disease among male health professionals. Psychosom Med 2003; 65:100–110.
- Williams JE, Paton CC, Siegler IC, Eigenbrodt ML, Nieto FJ, Tyroler HA. Anger proneness predicts coronary heart disease risk: prospective analysis from the Atherosclerosis Risk in Communities (ARIC) study. Circulation 2000; 101:2034–2039.
- Kawachi I, Sparrow D, Spiro A III, Vokonas P, Weiss ST. A prospective study of anger and coronary heart disease. The Normative Aging Study. Circulation 1996; 94:2090–2095.
- Gallacher JE, Yarnell JW, Sweetnam PM, Elwood PC, Stansfeld SA. Anger and incident heart disease in the Caerphilly study. Psychosom Med 1999; 61:446–453.
- Eaker ED, Sullivan LM, Kelly-Hayes M, D’Agostino RB Sr, Benjamin EJ. Anger and hostility predict the development of atrial fibrillation in men in the Framingham Offspring Study. Circulation 2004; 109:1267–1271.
- Everson SA, Kaplan GA, Goldberg DE, Lakka TA, Sivenius J, Salonen JT. Anger expression and incident stroke: prospective evidence from the Kuopio ischemic heart disease study. Stroke 1999; 30:523–528.
- Mittleman MA, Maclure M, Nachnani M, Sherwood JB, Muller JE. Educational attainment, anger, and the risk of triggering myocardial infarction onset. The Determinants of Myocardial Infarction Onset Study Investigators. Arch Intern Med 1997; 157:769–775.
- Mittleman MA, Maclure M, Sherwood JB, et al. Triggering of acute myocardial infarction onset by episodes of anger. Determinants of Myocardial Infarction Onset Study Investigators. Circulation 1995; 92:1720–1725.
- Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med 2005; 352:539–548.
- Wittstein IS. The broken heart syndrome. Cleve Clin J Med 2007; 74(Suppl 1):S17–S22.
- Burg MM, Lampert R, Joska T, Batsford W, Jain D. Psychological traits and emotion-triggering of ICD shock-terminated arrhythmias. Psychosom Med 2004; 66:898–902.
- Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97:1837–1847.
Numerous systematic reviews indicate that psychosocial factors are predictive of an initial acute coronary syndrome (ACS),1–8 defined as myocardial infarction (MI), unstable angina, or sudden cardiac death. Psychosocial factors under active investigation for their role in ACS onset include chronic negative emotional states (eg, depression, hostility, anxiety) as well as situational and behavioral triggers (eg, acute anger, unusual intense physical activity). This review will present evidence for each grouping of risk markers and then discuss the studies required to better identify and treat patients who have these psychosocial vulnerabilities.
NEGATIVE EMOTIONAL STATES
Increasing epidemiologic and pathophysiologic evidence suggests that depression, anxiety, and hostility/anger may each be an independent risk factor for initial occurrence of a cardiovascular event.4,8 The vast majority of evidence has been accumulated for depression, and many meta-analyses and systematic reviews now indicate that depression—as either a clinical diagnosis or an elevation in self-reported symptoms—is a strong, consistent, independent predictor of ACS incidence.9–11
Major depression
Major depressive disorder is most appropriately diagnosed through direct patient interview, preferably by trained professionals who look for evidence of severely depressed mood lasting at least 2 consecutive weeks, other concomitant symptoms (such as change in eating or sleeping habits), and evidence of associated functional impairment. Because this interview approach is not convenient for large epidemiologic studies, evaluation of major depression by interview in longitudinal epidemiologic studies has been sparse,12,13 and only a limited number of other studies have also evaluated the role of a history of depressive disorders14 or a history of depression treatment.14–18
Depressive symptoms
The impact of self-reported depressive symptoms on cardiac outcomes has been studied more widely.in community settings, among the elderly, and in various cardiac settings.using scales such as the Beck Depression Inventory and the Center for Epidemiological Studies Depression Scale. Notably, these scales assess only the presence of recent depressive symptoms. Nevertheless, despite this important limitation, one-time assessment of healthy participants using these scales has generally revealed a significant relationship between depressive symptoms and future adverse cardiac events.9,18 As further evidence of a gradient relationship, the frequency of cardiac events increases as the level of depressive symptoms increases.13,19
Depression is a complex phenotype, and some have argued that subtypes, or intermediary phenotypes, of depression may be particularly predictive of ACS incidence and recurrence.20 Interestingly, the first article ever published documenting a link between depression and coronary artery disease focused exclusively on melancholic depression, or endogenous depression.21
Anxiety
Anxiety is defined as a future-oriented negative emotion resulting from perceived threat and accompanied by perceived lack of control and lack of predictability.22 Like depression, anxiety occurs along a continuum, but it is characterized as pathological when it becomes chronic, has intensity out of proportion to any real threat, and leaves the affected person with seriously impaired ability to function.
There are many recognized anxiety disorders, including generalized anxiety disorder, panic attacks, obsessive-compulsive disorder, posttraumatic stress syndrome, and various forms of phobia. As a group, these anxiety disorders constitute one of the most common forms of psychiatric illness. Moreover, anxiety disorders and major depression are highly comorbid.23 Although some interesting epidemiologic studies have indicated that anxiety may predict new ACS events,24–26 there are a few that have yielded mixed results.27,28
Hostility and anger
Angry and hostile feelings are overlapping emotions and, when experienced frequently, indicate broader, more enduring temperaments or personality styles. Hostility is a cynical, suspicious, and resentful attitude toward others; negative social exchanges, such as sarcasm or impatience, typify individuals with hostility. In contrast, individuals with anger difficulties can have warm, appropriate interpersonal skills and may display verbal aggression or other outbursts only when provoked. Unlike depressive and anxiety disorders, professionally diagnosed, syndromal anger and hostility are not yet recognized by psychiatric nosology.
Relatively few longitudinal studies have been conducted using measures of hostility in healthy cohorts. These studies have reported both the presence29,30 and the absence31 of positive associations. In a recent systematic review, 7 of 11 studies showed hostility to be a significant risk factor for CHD.8 A case-control study involving participants in the Multiple Risk Factor Intervention Trial (MRFIT) employed a structured interview (as opposed to a questionnaire) designed to elicit information regarding signs of hostility, including irritation, arrogance, uncooperativeness, and angry feelings.30 It revealed that men with high hostility levels were more likely to die of cardiovascular disease than men with low hostility levels (adjusted odds ratio = 1.61; 95% CI, 1.09 to 2.39) in this initially healthy but high-risk cohort.30 The investigators chose the structured interview to overcome participants’ potential to underreport or underrecognize hostile tendencies when completing a questionnaire.30
Over time, specific measurements of chronic anger,32–37 including both unhealthy anger expression34 and suppression,37 have accumulated, permitting examination of their relationship to adverse cardiac outcomes in longitudinal follow-up of disease-free cohorts. A number of these studies have shown a positive association.32,33,35–37 Moreover, a recent report from the Framingham study demonstrated an association between anger/hostility and the development of atrial fibrillation and total-cause mortality over a 10year period,38 and another study has observed a relationship between anger expression and development of stroke.39 Combined, these observations suggest that anger is worthy of further study as a factor in the development of CHD. As with hostility, however, various subscales have been used to study anger, which makes standardization across studies difficult.
Data specific to imminent ACS risk are few
The majority of the negative emotional states have not been tested for their ability to predict an ACS in the near future. Further, negative emotional and cognitive states that may be implicated in the development of CHD or other cardiovascular disease may be quantitatively or even qualitatively different from those psychosocial factors that identify a patient at imminent risk for an ACS.
SITUATIONAL AND BEHAVIORAL TRIGGERS
Evidence for imminent risk or trigger status can be obtained from retrospective reports, from witness accounts (if available), or prospectively from electronic diaries coupled with ambulatory electrocardiogram recordings or an implantable cardioverter-defibrillator (ICD). Triggers of an ACS include external stimuli (eg, cocaine use, air pollution, ambient temperature), patient activities (eg, eating a meal high in saturated fat, unusual physical exertion), and emotional reactions such as extreme anger or anxiety.1,2,7,40,41 Myocardial stunning has also been reported immediately after acute emotional stress but has generally been reversible in these cases.42,43 In an observational study, Burg et al found that ICD shocks preceded by an anger episode (as recorded by diary) were more frequent in patients with high trait levels of anger (according to the Speilberger Trait Personality Inventory) and that shocks preceded by an anxiety episode were more frequent in patients with high trait levels of anxiety.44 A systematic review by Strike and Steptoe showed that physical exertion (particularly in poorly conditioned individuals), emotional stress, anger, and extreme excitement are all probable triggers for an ACS.7 A recent meta-analysis suggests that emotional stress immediately precedes MI in approximately 7% of MI cases and is a more frequent ACS trigger for women than for men.1
THE PSYCHOSOCIALLY VULNERABLE PATIENT
This selective overview suggests that patients’ emotional states are frequently implicated in the onset of an ACS but that the use of behavioral or emotional information to identify those at high risk for imminent ACS onset is not yet practical. Triggers are, by definition, state-like, but their impact may be amplified by trait-like characteristics, such as high dispositional anger, anxiety, hostility, or chronic environmental stress.
The previously mentioned analysis of the MRFIT study by Matthews et al30 suggests that patients identified as “high risk” by conventional risk factors, and who additionally possess high trait hostility, should be monitored closely, as they are at risk for cardiovascular death. Additionally, the Burg study of patients with ICDs suggests that arrhythmia may be induced by acute anxiety or anger in those prone to have such emotions chronically.44
Such studies have two research implications. First, controlled laboratory studies that induce acute negative emotion in those with chronic negative emotional states may help reveal the pathophysiologic processes implicated in immediate ACS onset. Interventions for these psychosocially vulnerable patients await such studies. Second, we must begin to consider that in addition to the psychosocially vulnerable patient, we may have psychosocially vulnerable situations, about which we know little at this time.
Acknowledgments
The author thanks Lucia Dettenborn, PhD, for her assistance with the presentation on which this manuscript, in part, is based.
This work was supported by grants HC-25197, HL-76857, HL-80665, and HL84034 from the National Heart, Lung, and Blood Institute. The project described was supported by grant number UL1 RR024156 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and the NIH Roadmap for Medical Research, and its contents are solely the responsibility of the author and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at http://www.ncrr.nih.gov. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
Numerous systematic reviews indicate that psychosocial factors are predictive of an initial acute coronary syndrome (ACS),1–8 defined as myocardial infarction (MI), unstable angina, or sudden cardiac death. Psychosocial factors under active investigation for their role in ACS onset include chronic negative emotional states (eg, depression, hostility, anxiety) as well as situational and behavioral triggers (eg, acute anger, unusual intense physical activity). This review will present evidence for each grouping of risk markers and then discuss the studies required to better identify and treat patients who have these psychosocial vulnerabilities.
NEGATIVE EMOTIONAL STATES
Increasing epidemiologic and pathophysiologic evidence suggests that depression, anxiety, and hostility/anger may each be an independent risk factor for initial occurrence of a cardiovascular event.4,8 The vast majority of evidence has been accumulated for depression, and many meta-analyses and systematic reviews now indicate that depression—as either a clinical diagnosis or an elevation in self-reported symptoms—is a strong, consistent, independent predictor of ACS incidence.9–11
Major depression
Major depressive disorder is most appropriately diagnosed through direct patient interview, preferably by trained professionals who look for evidence of severely depressed mood lasting at least 2 consecutive weeks, other concomitant symptoms (such as change in eating or sleeping habits), and evidence of associated functional impairment. Because this interview approach is not convenient for large epidemiologic studies, evaluation of major depression by interview in longitudinal epidemiologic studies has been sparse,12,13 and only a limited number of other studies have also evaluated the role of a history of depressive disorders14 or a history of depression treatment.14–18
Depressive symptoms
The impact of self-reported depressive symptoms on cardiac outcomes has been studied more widely.in community settings, among the elderly, and in various cardiac settings.using scales such as the Beck Depression Inventory and the Center for Epidemiological Studies Depression Scale. Notably, these scales assess only the presence of recent depressive symptoms. Nevertheless, despite this important limitation, one-time assessment of healthy participants using these scales has generally revealed a significant relationship between depressive symptoms and future adverse cardiac events.9,18 As further evidence of a gradient relationship, the frequency of cardiac events increases as the level of depressive symptoms increases.13,19
Depression is a complex phenotype, and some have argued that subtypes, or intermediary phenotypes, of depression may be particularly predictive of ACS incidence and recurrence.20 Interestingly, the first article ever published documenting a link between depression and coronary artery disease focused exclusively on melancholic depression, or endogenous depression.21
Anxiety
Anxiety is defined as a future-oriented negative emotion resulting from perceived threat and accompanied by perceived lack of control and lack of predictability.22 Like depression, anxiety occurs along a continuum, but it is characterized as pathological when it becomes chronic, has intensity out of proportion to any real threat, and leaves the affected person with seriously impaired ability to function.
There are many recognized anxiety disorders, including generalized anxiety disorder, panic attacks, obsessive-compulsive disorder, posttraumatic stress syndrome, and various forms of phobia. As a group, these anxiety disorders constitute one of the most common forms of psychiatric illness. Moreover, anxiety disorders and major depression are highly comorbid.23 Although some interesting epidemiologic studies have indicated that anxiety may predict new ACS events,24–26 there are a few that have yielded mixed results.27,28
Hostility and anger
Angry and hostile feelings are overlapping emotions and, when experienced frequently, indicate broader, more enduring temperaments or personality styles. Hostility is a cynical, suspicious, and resentful attitude toward others; negative social exchanges, such as sarcasm or impatience, typify individuals with hostility. In contrast, individuals with anger difficulties can have warm, appropriate interpersonal skills and may display verbal aggression or other outbursts only when provoked. Unlike depressive and anxiety disorders, professionally diagnosed, syndromal anger and hostility are not yet recognized by psychiatric nosology.
Relatively few longitudinal studies have been conducted using measures of hostility in healthy cohorts. These studies have reported both the presence29,30 and the absence31 of positive associations. In a recent systematic review, 7 of 11 studies showed hostility to be a significant risk factor for CHD.8 A case-control study involving participants in the Multiple Risk Factor Intervention Trial (MRFIT) employed a structured interview (as opposed to a questionnaire) designed to elicit information regarding signs of hostility, including irritation, arrogance, uncooperativeness, and angry feelings.30 It revealed that men with high hostility levels were more likely to die of cardiovascular disease than men with low hostility levels (adjusted odds ratio = 1.61; 95% CI, 1.09 to 2.39) in this initially healthy but high-risk cohort.30 The investigators chose the structured interview to overcome participants’ potential to underreport or underrecognize hostile tendencies when completing a questionnaire.30
Over time, specific measurements of chronic anger,32–37 including both unhealthy anger expression34 and suppression,37 have accumulated, permitting examination of their relationship to adverse cardiac outcomes in longitudinal follow-up of disease-free cohorts. A number of these studies have shown a positive association.32,33,35–37 Moreover, a recent report from the Framingham study demonstrated an association between anger/hostility and the development of atrial fibrillation and total-cause mortality over a 10year period,38 and another study has observed a relationship between anger expression and development of stroke.39 Combined, these observations suggest that anger is worthy of further study as a factor in the development of CHD. As with hostility, however, various subscales have been used to study anger, which makes standardization across studies difficult.
Data specific to imminent ACS risk are few
The majority of the negative emotional states have not been tested for their ability to predict an ACS in the near future. Further, negative emotional and cognitive states that may be implicated in the development of CHD or other cardiovascular disease may be quantitatively or even qualitatively different from those psychosocial factors that identify a patient at imminent risk for an ACS.
SITUATIONAL AND BEHAVIORAL TRIGGERS
Evidence for imminent risk or trigger status can be obtained from retrospective reports, from witness accounts (if available), or prospectively from electronic diaries coupled with ambulatory electrocardiogram recordings or an implantable cardioverter-defibrillator (ICD). Triggers of an ACS include external stimuli (eg, cocaine use, air pollution, ambient temperature), patient activities (eg, eating a meal high in saturated fat, unusual physical exertion), and emotional reactions such as extreme anger or anxiety.1,2,7,40,41 Myocardial stunning has also been reported immediately after acute emotional stress but has generally been reversible in these cases.42,43 In an observational study, Burg et al found that ICD shocks preceded by an anger episode (as recorded by diary) were more frequent in patients with high trait levels of anger (according to the Speilberger Trait Personality Inventory) and that shocks preceded by an anxiety episode were more frequent in patients with high trait levels of anxiety.44 A systematic review by Strike and Steptoe showed that physical exertion (particularly in poorly conditioned individuals), emotional stress, anger, and extreme excitement are all probable triggers for an ACS.7 A recent meta-analysis suggests that emotional stress immediately precedes MI in approximately 7% of MI cases and is a more frequent ACS trigger for women than for men.1
THE PSYCHOSOCIALLY VULNERABLE PATIENT
This selective overview suggests that patients’ emotional states are frequently implicated in the onset of an ACS but that the use of behavioral or emotional information to identify those at high risk for imminent ACS onset is not yet practical. Triggers are, by definition, state-like, but their impact may be amplified by trait-like characteristics, such as high dispositional anger, anxiety, hostility, or chronic environmental stress.
The previously mentioned analysis of the MRFIT study by Matthews et al30 suggests that patients identified as “high risk” by conventional risk factors, and who additionally possess high trait hostility, should be monitored closely, as they are at risk for cardiovascular death. Additionally, the Burg study of patients with ICDs suggests that arrhythmia may be induced by acute anxiety or anger in those prone to have such emotions chronically.44
Such studies have two research implications. First, controlled laboratory studies that induce acute negative emotion in those with chronic negative emotional states may help reveal the pathophysiologic processes implicated in immediate ACS onset. Interventions for these psychosocially vulnerable patients await such studies. Second, we must begin to consider that in addition to the psychosocially vulnerable patient, we may have psychosocially vulnerable situations, about which we know little at this time.
Acknowledgments
The author thanks Lucia Dettenborn, PhD, for her assistance with the presentation on which this manuscript, in part, is based.
This work was supported by grants HC-25197, HL-76857, HL-80665, and HL84034 from the National Heart, Lung, and Blood Institute. The project described was supported by grant number UL1 RR024156 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and the NIH Roadmap for Medical Research, and its contents are solely the responsibility of the author and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at http://www.ncrr.nih.gov. Information on Re-engineering the Clinical Research Enterprise can be obtained from http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.
- Culić V, Eterović D, Mirić D. Meta-analysis of possible external triggers of acute myocardial infarction. Int J Cardiol 2005; 99:1–8.
- Kloner RA. Natural and unnatural triggers of myocardial infarction. Prog Cardiovasc Dis 2006; 48:285–300.
- Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146538 participants in 54 observational studies. Eur Heart J 2006; 27:2763–2774.
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol 2005; 45:637–651.
- Rosengren A, Hawken S, Ounpuu S, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364:953–962.
- Servoss SJ, Januzzi JL, Muller JE. Triggers of acute coronary syndromes. Prog Cardiovasc Dis 2002; 44:369–380.
- Strike PC, Steptoe A. Behavioral and emotional triggers of acute coronary syndromes: a systematic review and critique. Psychosom Med 2005; 67:179–186.
- Suls J, Bunde J. Anger, anxiety, and depression as risk factors for cardiovascular disease: the problems and implications of overlapping affective dispositions. Psychol Bull 2005; 131:260–300.
- Rugulies R. Depression as a predictor for coronary heart disease: a review and meta-analysis. Am J Prev Med 2002; 23:51–61.
- Wulsin LR, Singal BM. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003; 65:201–210.
- Van der Kooy K, van Hout H, Marwijk H, Marten H, Stehouwer C, Beekman A. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry 2007; 22:613–626.
- Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med 1998; 158:1422–1426.
- Penninx BW, Beekman AT, Honig A, et al. Depression and cardiac mortality: results from a community-based longitudinal study. Arch Gen Psychiatry 2001; 58:221–227.
- Pratt LA, Ford DE, Crum RM, Armenian HK, Gallo JJ, Eaton WW. Depression, psychotropic medication, and risk of myocardial infarction. Prospective data from the Baltimore ECA follow-up. Circulation 1996; 94:3123–3129.
- Cohen HW, Madhavan S, Alderman MH. History of treatment for depression: risk factor for myocardial infarction in hypertensive patients. Psychosom Med 2001; 63:203–209.
- Rutledge T, Reis SE, Olson MB, et al. Depression symptom severity and reported treatment history in the prediction of cardiac risk in women with suspected myocardial ischemia: the NHLBI-sponsored WISE study. Arch Gen Psychiatry 2006; 63:874–880.
- Sauer WH, Berlin JA, Kimmel SE. Effect of antidepressants and their relative affinity for the serotonin transporter on the risk of myocardial infarction. Circulation 2003; 108:32–36.
- Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women: the Women’s Health Initiative (WHI). Arch Intern Med 2004; 164:289–298.
- Rowan PJ, Haas D, Campbell JA, Maclean DR, Davidson KW. Depressive symptoms have an independent, gradient risk for coronary heart disease incidence in a random, population-based sample. Ann Epidemiol 2005; 15:316–320.
- Davidson KW, Rieckmann N, Rapp MA. Definitions and distinctions among depressive syndromes and symptoms: implications for a better understanding of the depression-cardiovascular disease association. Psychosom Med 2005; 67(Suppl 1):S6–S9.
- Malzberg B. Mortality among patients with involution melancholia. Am J Psychiatry 1937; 93:1231–1238.
- Barlow DH. Anxiety and its Disorders: The Nature and Treatment of Anxiety and Panic. New York, NY: Guilford Press; 1988.
- Hirschfeld RM. The comorbidity of major depression and anxiety disorders: recognition and management in primary care. Prim Care Companion J Clin Psychiatry 2001; 3:244–254.
- Kawachi I, Colditz GA, Ascherio A, et al. Prospective study of phobic anxiety and risk of coronary heart disease in men. Circulation 1994; 89:1992–1997.
- Kubzansky LD, Kawachi I, Weiss ST, Sparrow D. Anxiety and coronary heart disease: a synthesis of epidemiological, psychological, and experimental evidence. Ann Behav Med 1998; 20:47–58.
- Kubzansky LD, Kawachi I, Spiro A III, et al. Is worrying bad for your heart? A prospective study of worry and coronary heart disease in the Normative Aging Study. Circulation 1997; 95:818–824.
- Todaro JF, Shen BJ, Niaura R, Spiro A III, Ward KD. Effect of negative emotions on frequency of coronary heart disease (The Normative Aging Study). Am J Cardiol 2003; 92:901–906.
- McCarron P, Gunnell D, Harrison GL, Okasha M, Davey Smith G. Temperament in young adulthood and later mortality: prospective observational study. J Epidemiol Community Health 2003; 57:888–892.
- Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the Normative Aging Study. Psychosom Med 2000; 62:7–16.
- Matthews KA, Gump BB, Harris KF, Haney TL, Barefoot JC. Hostile behaviors predict cardiovascular mortality among men enrolled in the Multiple Risk Factor Intervention Trial. Circulation 2004; 109:66–70.
- Sykes DH, Arveiler D, Salters CP, et al. Psychosocial risk factors for heart disease in France and Northern Ireland: the Prospective Epidemiological Study of Myocardial Infarction (PRIME). Int J Epidemiol 2002; 31:1227–1234.
- Haynes SG, Feinleib M, Kannel WB. The relationship of psychosocial factors to coronary heart disease in the Framingham Study. III. Eight-year incidence of coronary heart disease. Am J Epidemiol 1980; 111:37–58.
- Chang PP, Ford DE, Meoni LA, Wang NY, Klag MJ. Anger in young men and subsequent premature cardiovascular disease: the Precursors Study. Arch Intern Med 2002; 162:901–906.
- Eng PM, Fitzmaurice G, Kubzansky LD, Rimm EB, Kawachi I. Anger expression and risk of stroke and coronary heart disease among male health professionals. Psychosom Med 2003; 65:100–110.
- Williams JE, Paton CC, Siegler IC, Eigenbrodt ML, Nieto FJ, Tyroler HA. Anger proneness predicts coronary heart disease risk: prospective analysis from the Atherosclerosis Risk in Communities (ARIC) study. Circulation 2000; 101:2034–2039.
- Kawachi I, Sparrow D, Spiro A III, Vokonas P, Weiss ST. A prospective study of anger and coronary heart disease. The Normative Aging Study. Circulation 1996; 94:2090–2095.
- Gallacher JE, Yarnell JW, Sweetnam PM, Elwood PC, Stansfeld SA. Anger and incident heart disease in the Caerphilly study. Psychosom Med 1999; 61:446–453.
- Eaker ED, Sullivan LM, Kelly-Hayes M, D’Agostino RB Sr, Benjamin EJ. Anger and hostility predict the development of atrial fibrillation in men in the Framingham Offspring Study. Circulation 2004; 109:1267–1271.
- Everson SA, Kaplan GA, Goldberg DE, Lakka TA, Sivenius J, Salonen JT. Anger expression and incident stroke: prospective evidence from the Kuopio ischemic heart disease study. Stroke 1999; 30:523–528.
- Mittleman MA, Maclure M, Nachnani M, Sherwood JB, Muller JE. Educational attainment, anger, and the risk of triggering myocardial infarction onset. The Determinants of Myocardial Infarction Onset Study Investigators. Arch Intern Med 1997; 157:769–775.
- Mittleman MA, Maclure M, Sherwood JB, et al. Triggering of acute myocardial infarction onset by episodes of anger. Determinants of Myocardial Infarction Onset Study Investigators. Circulation 1995; 92:1720–1725.
- Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med 2005; 352:539–548.
- Wittstein IS. The broken heart syndrome. Cleve Clin J Med 2007; 74(Suppl 1):S17–S22.
- Burg MM, Lampert R, Joska T, Batsford W, Jain D. Psychological traits and emotion-triggering of ICD shock-terminated arrhythmias. Psychosom Med 2004; 66:898–902.
- Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97:1837–1847.
- Culić V, Eterović D, Mirić D. Meta-analysis of possible external triggers of acute myocardial infarction. Int J Cardiol 2005; 99:1–8.
- Kloner RA. Natural and unnatural triggers of myocardial infarction. Prog Cardiovasc Dis 2006; 48:285–300.
- Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146538 participants in 54 observational studies. Eur Heart J 2006; 27:2763–2774.
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol 2005; 45:637–651.
- Rosengren A, Hawken S, Ounpuu S, et al. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study. Lancet 2004; 364:953–962.
- Servoss SJ, Januzzi JL, Muller JE. Triggers of acute coronary syndromes. Prog Cardiovasc Dis 2002; 44:369–380.
- Strike PC, Steptoe A. Behavioral and emotional triggers of acute coronary syndromes: a systematic review and critique. Psychosom Med 2005; 67:179–186.
- Suls J, Bunde J. Anger, anxiety, and depression as risk factors for cardiovascular disease: the problems and implications of overlapping affective dispositions. Psychol Bull 2005; 131:260–300.
- Rugulies R. Depression as a predictor for coronary heart disease: a review and meta-analysis. Am J Prev Med 2002; 23:51–61.
- Wulsin LR, Singal BM. Do depressive symptoms increase the risk for the onset of coronary disease? A systematic quantitative review. Psychosom Med 2003; 65:201–210.
- Van der Kooy K, van Hout H, Marwijk H, Marten H, Stehouwer C, Beekman A. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry 2007; 22:613–626.
- Ford DE, Mead LA, Chang PP, Cooper-Patrick L, Wang NY, Klag MJ. Depression is a risk factor for coronary artery disease in men: the Precursors Study. Arch Intern Med 1998; 158:1422–1426.
- Penninx BW, Beekman AT, Honig A, et al. Depression and cardiac mortality: results from a community-based longitudinal study. Arch Gen Psychiatry 2001; 58:221–227.
- Pratt LA, Ford DE, Crum RM, Armenian HK, Gallo JJ, Eaton WW. Depression, psychotropic medication, and risk of myocardial infarction. Prospective data from the Baltimore ECA follow-up. Circulation 1996; 94:3123–3129.
- Cohen HW, Madhavan S, Alderman MH. History of treatment for depression: risk factor for myocardial infarction in hypertensive patients. Psychosom Med 2001; 63:203–209.
- Rutledge T, Reis SE, Olson MB, et al. Depression symptom severity and reported treatment history in the prediction of cardiac risk in women with suspected myocardial ischemia: the NHLBI-sponsored WISE study. Arch Gen Psychiatry 2006; 63:874–880.
- Sauer WH, Berlin JA, Kimmel SE. Effect of antidepressants and their relative affinity for the serotonin transporter on the risk of myocardial infarction. Circulation 2003; 108:32–36.
- Wassertheil-Smoller S, Shumaker S, Ockene J, et al. Depression and cardiovascular sequelae in postmenopausal women: the Women’s Health Initiative (WHI). Arch Intern Med 2004; 164:289–298.
- Rowan PJ, Haas D, Campbell JA, Maclean DR, Davidson KW. Depressive symptoms have an independent, gradient risk for coronary heart disease incidence in a random, population-based sample. Ann Epidemiol 2005; 15:316–320.
- Davidson KW, Rieckmann N, Rapp MA. Definitions and distinctions among depressive syndromes and symptoms: implications for a better understanding of the depression-cardiovascular disease association. Psychosom Med 2005; 67(Suppl 1):S6–S9.
- Malzberg B. Mortality among patients with involution melancholia. Am J Psychiatry 1937; 93:1231–1238.
- Barlow DH. Anxiety and its Disorders: The Nature and Treatment of Anxiety and Panic. New York, NY: Guilford Press; 1988.
- Hirschfeld RM. The comorbidity of major depression and anxiety disorders: recognition and management in primary care. Prim Care Companion J Clin Psychiatry 2001; 3:244–254.
- Kawachi I, Colditz GA, Ascherio A, et al. Prospective study of phobic anxiety and risk of coronary heart disease in men. Circulation 1994; 89:1992–1997.
- Kubzansky LD, Kawachi I, Weiss ST, Sparrow D. Anxiety and coronary heart disease: a synthesis of epidemiological, psychological, and experimental evidence. Ann Behav Med 1998; 20:47–58.
- Kubzansky LD, Kawachi I, Spiro A III, et al. Is worrying bad for your heart? A prospective study of worry and coronary heart disease in the Normative Aging Study. Circulation 1997; 95:818–824.
- Todaro JF, Shen BJ, Niaura R, Spiro A III, Ward KD. Effect of negative emotions on frequency of coronary heart disease (The Normative Aging Study). Am J Cardiol 2003; 92:901–906.
- McCarron P, Gunnell D, Harrison GL, Okasha M, Davey Smith G. Temperament in young adulthood and later mortality: prospective observational study. J Epidemiol Community Health 2003; 57:888–892.
- Niaura R, Banks SM, Ward KD, et al. Hostility and the metabolic syndrome in older males: the Normative Aging Study. Psychosom Med 2000; 62:7–16.
- Matthews KA, Gump BB, Harris KF, Haney TL, Barefoot JC. Hostile behaviors predict cardiovascular mortality among men enrolled in the Multiple Risk Factor Intervention Trial. Circulation 2004; 109:66–70.
- Sykes DH, Arveiler D, Salters CP, et al. Psychosocial risk factors for heart disease in France and Northern Ireland: the Prospective Epidemiological Study of Myocardial Infarction (PRIME). Int J Epidemiol 2002; 31:1227–1234.
- Haynes SG, Feinleib M, Kannel WB. The relationship of psychosocial factors to coronary heart disease in the Framingham Study. III. Eight-year incidence of coronary heart disease. Am J Epidemiol 1980; 111:37–58.
- Chang PP, Ford DE, Meoni LA, Wang NY, Klag MJ. Anger in young men and subsequent premature cardiovascular disease: the Precursors Study. Arch Intern Med 2002; 162:901–906.
- Eng PM, Fitzmaurice G, Kubzansky LD, Rimm EB, Kawachi I. Anger expression and risk of stroke and coronary heart disease among male health professionals. Psychosom Med 2003; 65:100–110.
- Williams JE, Paton CC, Siegler IC, Eigenbrodt ML, Nieto FJ, Tyroler HA. Anger proneness predicts coronary heart disease risk: prospective analysis from the Atherosclerosis Risk in Communities (ARIC) study. Circulation 2000; 101:2034–2039.
- Kawachi I, Sparrow D, Spiro A III, Vokonas P, Weiss ST. A prospective study of anger and coronary heart disease. The Normative Aging Study. Circulation 1996; 94:2090–2095.
- Gallacher JE, Yarnell JW, Sweetnam PM, Elwood PC, Stansfeld SA. Anger and incident heart disease in the Caerphilly study. Psychosom Med 1999; 61:446–453.
- Eaker ED, Sullivan LM, Kelly-Hayes M, D’Agostino RB Sr, Benjamin EJ. Anger and hostility predict the development of atrial fibrillation in men in the Framingham Offspring Study. Circulation 2004; 109:1267–1271.
- Everson SA, Kaplan GA, Goldberg DE, Lakka TA, Sivenius J, Salonen JT. Anger expression and incident stroke: prospective evidence from the Kuopio ischemic heart disease study. Stroke 1999; 30:523–528.
- Mittleman MA, Maclure M, Nachnani M, Sherwood JB, Muller JE. Educational attainment, anger, and the risk of triggering myocardial infarction onset. The Determinants of Myocardial Infarction Onset Study Investigators. Arch Intern Med 1997; 157:769–775.
- Mittleman MA, Maclure M, Sherwood JB, et al. Triggering of acute myocardial infarction onset by episodes of anger. Determinants of Myocardial Infarction Onset Study Investigators. Circulation 1995; 92:1720–1725.
- Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med 2005; 352:539–548.
- Wittstein IS. The broken heart syndrome. Cleve Clin J Med 2007; 74(Suppl 1):S17–S22.
- Burg MM, Lampert R, Joska T, Batsford W, Jain D. Psychological traits and emotion-triggering of ICD shock-terminated arrhythmias. Psychosom Med 2004; 66:898–902.
- Wilson PW, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heart disease using risk factor categories. Circulation 1998; 97:1837–1847.