User login
How to help patients with olfactory reference syndrome
Ms. A, a 21-year-old teacher, recalled always having been “sensitive,” but when she started her first job at age 19 she began to believe that she emitted an offensive odor. She experienced thoughts that she passed offensive flatus, her breath had a fecal odor, and people noticed and were offended.
Gradually Ms. A became more convinced of these distressing beliefs and began to think that she permeated fecal odor through her skin. She also became sure that colleagues were talking about her and that they complained about her “disgusting” smell.
Patients with olfactory reference syndrome (ORS) falsely believe they emit an offensive body odor. Prominent referential thinking—believing that other people perceive the odor—also is common. To introduce you to ORS, we discuss its clinical diagnosis and treatment based on our review of several hundred cases, including the largest reported series of patients with ORS.1-4
Olfactory reference syndrome (ORS) has been described around the world for more than a century. In 1891, Potts described a delusional 50-year-old man who “had been troubled for the past three months with smelling a very bad odor, which he likened to that of a ‘back-house,’ and which came from his own person. [He believed] this smell was so very strong that other men objected to working with him….”
Despite its long history, the syndrome’s prevalence is not well-established. ORS probably is underdiagnosed and more common than generally recognized:
- In a tertiary psychiatry unit in London, 0.5% of 2,000 patients who were not systematically screened for ORS spontaneously reported ORS symptoms.
- In a self-report survey of 2,481 students in Japan, 2.1% had been concerned with emitting a strange bodily odor during the past year.
- In a study in a dental clinic in Japan, the majority of patients with a primary complaint of halitosis actually had “imaginary halitosis” (another term for ORS).
Clinical features of ors
Ms. A quit her job and felt confident enough to work again only when she performed a 2-hour daily cleansing routine, doused herself in per-fume, and placed an incontinence pad in her underwear. Despite these precautions, she still thought her colleagues avoided her.
She always averted her mouth when speaking, held her hand in front of her mouth, and sat far from others and close to the door in meetings. She tried to keep meeting room doors open and believed that colleagues held their hands to their noses to “protect” themselves from her odor.
ORS symptoms are most often reported as beginning when patients are in their mid 20s, although some reports suggest onset during puberty or adolescence.4 In clinical series, the ratio of men to women is approximately 2:1.
Preoccupation. Individuals with ORS are preoccupied with the belief that they emit an unpleasant or offensive body odor (Box 1),1,2,5-9 most commonly:
Although most reports suggest that patients focus on one odor, some describe being concerned about several smells simultaneously or different odors over time.10,11
Referential thinking. As the syndrome’s name implies, many ORS patients have delusions of reference, falsely believing that other people perceive the odor.3 They misinterpret the behavior of others, assuming it is a reaction to how the patient smells (Box 2).2,3
They may misperceive comments (such as, “It’s stuffy in here”), receiving perfume or soap as a gift, or behaviors such as people sniffing, touching or rubbing their nose, clearing their throat, opening a window to get fresh air, putting a newspaper in front of their face, or looking or moving toward or away from the patient.1,3,5,7
Because they are ashamed, embarrassed, and concerned about offending others with their odor,13 many patients engage in repetitive and “safety” behaviors intended to check, eliminate, or camouflage the supposed odor (Box 3).1,3,7,12,14
DSM-IV-TR classifies olfactory reference syndrome (ORS) as a delusional disorder, somatic type (the modern equivalent of monosymptomatic hypochondriacal psychosis). ORS also is mentioned in the text on social anxiety disorder. ORS may not be diagnosed if:
- criterion A for schizophrenia has ever been met
- or if symptoms are due to the direct physiologic effects of a substance or a general medical condition, such as a brain tumor or temporal lobe epilepsy.
Many patients report being able to smell the imagined odor, suggesting that they experience an olfactory hallucination. Pryse-Phillips described the olfactory hallucinations of her 36 ORS case patients as “a real and immediate perception… often perceived in the absence of other odors.”
ORS generally is regarded as delusional, with possible secondary illusional misinterpretations and referential thinking. ORS beliefs usually appear to be of delusional intensity, although some patients may have some—although limited—insight (that is, overvalued ideation).
Functional impairment. Individuals with ORS often avoid other people or believe that others avoid them.12 They are typically embarrassed and worried that others will be offended by the smell. They may:
- avoid activities such as dating
- break off engagements
- refuse to travel
- move to another town
- become housebound.3,7,10,12
The distress and impaired functioning may lead to psychiatric hospitalization, depression, suicidal ideation, suicide attempts, and completed suicide.7,10,12,15 Pryse-Phillips studied 36 patients with ORS and reported:
- nearly one-half (43%) experienced “suicidal ideas or action”
- 2 (5.6%) committed suicide.3
Some authors have questioned whether ORS can transform into schizophrenia, but others have found little evidence for this.3,6
Psychiatric comorbidity. Depression is mentioned most often in the literature.12,13 In Pryse-Phillips’ 36 ORS patients (who did not have a “primary” depressive disorder), depression symptoms tended to be severe.3 The depression generally is considered secondary to ORS, although Pryse-Phillips evaluated 50 additional patients with ORS symptoms whom she considered to have a “primary” depressive disorder.3 Other psychiatric comorbidities include bipolar disorder, personality disorder, schizophrenia, hypochondriasis, alcohol and/or drug abuse, obsessive-compulsive disorder (OCD), and body dysmorphic disorder.3,7,15 In a study of 200 individuals with body dysmorphic disorder, 8 had comorbid ORS.16
Diagnosing ORS
Clinical clues to ORS (Table 1) probably are not present in all patients and some are not specific to ORS. They appear to be common features of the illness, however, and may alert you to its presence. Our clinical impression is that many patients with ORS are secretive about their symptoms because they are ashamed of them. Thus, you need to be alert to clues and specifically inquire about ORS symptoms to detect its presence.
Criteria. DSM-IV-TR and ICD-10 lack specific diagnostic criteria for ORS, instead applying criteria for delusional disorder. One problem with this approach is that delusional disorder criteria specify that any co-occurring mood symptoms must be brief relative to the duration of the delusional periods. This requirement may not be valid when applied to ORS.
In our experience, some patients have protracted depressive symptoms that appear secondary to “primary” ORS symptoms, and another diagnosis—such as psychotic depression—does not appear to account for their symptoms.
We propose working diagnostic criteria for ORS (Table 2), which are similar to those proposed by Lochner and Stein17 and require empiric validation. Suggested questions for the patient interview (Table 3) can help you identify and diagnose ORS.
Differential diagnosis. Keep in mind that a false belief that one emits a bad smell may be a symptom of schizophrenia, and this would trump an ORS diagnosis if other schizophrenia symptoms are present. Some patients with severe depression may believe they smell bad as part of a nihilistic delusional belief system (such as in Cotard’s syndrome—nihilistic delusions in severe depression).
Whether to conceptualize a false belief about body odor as a symptom of depression or as ORS with comorbid or secondary depression may be unclear from case to case.
Table 1
Clinical clues to the presence of olfactory reference syndrome
| Referential thinking. Interpreting actions of others—such as opening a window, moving away, putting a hand to their nose, or making comments related to odors—as evidence that the person smells offensive |
| Excessive attempts to ‘disguise’ the smell, such as washing routines, clothes changing, clothes laundering, or using abundant perfume, deodorant, mouthwash, mints, or other forms of camouflage |
| Other excessive and repetitive behaviors, such as checking for or asking other people for reassurance about the odor |
| Social anxiety or avoidance of social activities, relationships, work, school, or other daily activities |
| Requests for treatment for the perceived odor from dentists, gastroenterologists, proctologists, or other nonpsychiatric physicians despite a negative medical workup |
Working diagnostic criteria for olfactory reference syndrome
| A. | Persistent false belief that one emits a malodorous smell; this belief may encompass a range of insight and does not have to be delusional |
| B. | The belief is time-consuming and preoccupies the individual for at least 1 hour per day |
| C. | The belief causes clinically significant distress or results in significant impairment in social, occupational, or other important areas of functioning |
| D. | The belief is not better accounted for by another mental disorder or a general medical condition |
Table 3
Diagnosing ORS: Suggested questions for patient interview
|
Treatment-seeking behavior
Ms. A consulted several proctologists and a dentist but was not convinced by their reassurance and continued to believe she “stank.” Her relationship with her boyfriend suffered because she continually asked for reassurance about how she smelled and avoided sexual intercourse because of her odor concerns.
Eventually she confronted her boss about her belief that her coworkers were complaining about her smell. Despite reassurance that she didn’t smell bad, she left her job.
Excessive showering or washing are among the repetitive, ritualistic or “safety” behaviors many patients with ORS engage in to check, eliminate, or camouflage supposed odor. Frequent clothes changing or laundering also is common.
Camouflaging attempts may include excessive use of deodorant, soap, cologne, powder, mints, mouthwash, or toothpaste; wearing layers of clothing; or smoking.
Many patients frequently check for the odor or its source (such as trying to smell their own breath or checking the anal area for seepage). Some patients use the toilet excessively or eat a special diet to try to minimize the smell. Others repeatedly seek reassurance about how they smell.
Avoidance behaviors are common and include sitting far from other people, moving as little as possible to avoid spreading the supposed odor, or averting the head or covering the mouth.
Convincing patients such as Ms. A of the falsity of their beliefs can be difficult,1 and some succeed in having medical procedures or surgery, such as excision of tonsils or axillary glands.3,7,12 To our knowledge, controlled prospective studies of nonpsychiatric treatments have not been done, but it appears that such treatments usually are ineffective.1,3,6,9
Psychiatric interventions. Convincing patients with ORS to obtain mental health treatment can be difficult.2,6 Patients with delusional halitosis “would rather go in search of a ‘better dentist’ than go to a psychiatrist.”1
To get patients to accept psychiatric treatment, we suggest an approach similar to that recommended for body dysmorphic disorder. It may be helpful, for example, to focus on the distress and disability caused by the odor preoccupation, rather than on whether the patient actually smells bad.
Medication and psychotherapy
Limited evidence. The ORS treatment literature is very limited, consisting largely of case reports and small case series. To our knowledge, no controlled treatment trials have been done, no treatments have been compared head to head, and most studies did not use standardized measurements of psychopathology.
Published data therefore must be interpreted cautiously. Some medication reports used relatively low doses and short treatment durations (although what constitutes an adequate therapeutic trial for ORS is not known). Psychotherapy reports often did not specify details of the intervention or the number and duration of sessions. It is not known whether adding a cognitive component to behavioral therapy enhances efficacy, and the combination of psychotherapy and medication has not been studied systematically. More methodologically rigorous treatment studies are needed.
Because of space limitations, we cite representative case reports in the following section of this treatment review, rather than all of the cases found in our literature search.
Antidepressants. Although most ORS patients are delusional, serotonin reuptake inhibitor (SRI) monotherapy has been reported to be efficacious in 10 of 15 cases (67%). Most of these patients received clomipramine.18 In reports of non-SRI antidepressants, 6 of 15 cases (43%) responded. Some patients’ symptoms responded to an antidepressant after failing to respond to antipsychotic treatment.19
Antipsychotics. Pimozide is the most studied medication for ORS, with 15 of 31 cases (48%) responding.2,20 In a series of 12 patients, pimozide responders received 2 to 4 mg/d, except for one patient who needed 6 mg/d.21 Patients usually responded within 1 to 4 weeks (an average time to response was not reported). In 2 of these cases, ORS symptoms recurred after pimozide was discontinued and then remitted again after it was restarted.21 In another report,2 7 of 14 patients (50%) responded to pimozide.
Clinicians using other first-generation antipsychotics (trifluoperazine, thioridazine, and chlorpromazine) reported a positive response in only 2 of 19 cases (11%).12,22
Combination therapy. Ten of 17 cases (59%) of ORS responded to combined treatment with an antidepressant and an antipsychotic.2,12
Other somatic treatments. Several reports found benzodiazepine monotherapy lacked efficacy, as was the case for electroconvulsive therapy.12,15 One report noted an unsuccessful outcome with leucotomy and a partial response with bilateral partial division of the thalamo-frontal tract.15
Psychosocial treatment. All reports of psychosocial therapies are single cases or small series, and none used a control intervention.2,7,14
Behavioral treatment has been efficacious, although patients require months to years to habituate. Several reports totalling 14 patients describe behavioral treatment over weeks to months.7,23 These treatments involved exposure to avoided social situations and response prevention, which consisted of refraining from repetitive or camouflaging behaviors such as showering, visits to the toilet, or deodorant use. Gomez-Perez and colleagues23 noted that exposure therapy was less effective for ORS than for social phobia or OCD.
One report described a patient with flatulence concerns who responded to a paradoxical intention consisting of instructions to emit gas as soon as it was experienced; at 1-year follow-up, her symptoms had not recurred.24
Psychodynamic interventions show no benefit for ORS symptoms.
Treatment summary
Ms. A became increasingly despondent and depressed. She eventually sought the help of her family doctor, who referred her to a psychiatrist. With a combination of a serotonergic antidepressant (escitalopram, 40 mg/d), a low-dose atypical antipsychotic (quetiapine, 50 mg at night), and cognitive-behavioral therapy, she started to re-engage in daily activities. During 6 months of treatment, the intensity of her belief about having body odor abated.
Limited data support the use of SRI monotherapy or an SRI plus an antipsychotic. Using SRI monotherapy for delusional patients may sound counterintuitive, but this approach appears efficacious for patients with delusional body dysmorphic disorder, which has similarities to ORS.17,25,26
Clinically, we have found the use of atypical antipsychotics as an adjunct to SRIs to be helpful, although this strategy has not been subjected to clinical trials. Pimozide alone or in combination with an antidepressant also appears promising, as does exposure and response prevention. Do not combine pimozide with clomipramine because of the risk of cardiac toxicity.
Related resources
- Phillips KA, Gunderson C, Gruber U, Castle DJ. Delusions of body malodour: the olfactory reference syndrome. In: Brewer W, Castle D, Pantelis C. Olfaction and the brain. Cambridge, UK: Cambridge University Press; 2006:334-53.
- Pryse-Phillips W. An olfactory reference syndrome. Acta Psychiatr Scand 1971;47:484-509.
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Escitalopram • Lexapro
- Pimozide • Orap
- Quetiapine • Seroquel
- Thioridazine • Mellaril
- Trifluoperazine • Stelazine
Dr. Phillips receives research support from the National Institute of Mental Health, the Food and Drug Administration, UCB Pharma, and Forest Pharmaceuticals.
Dr. Castle receives research support from Janssen-Cilag; is a consultant to Eli Lilly and Company., Bristol-Myers Squibb, and Lundbeck; and is a speaker for Eli Lilly and Co., sanofi-aventis, Bristol-Myers Squibb, Janssen-Cilag, Lundbeck, and Organon.
Acknowledgment
The authors would like to thank Craig Gunderson, MD, and Uschi Gruber, MB, for their assistance with a literature search on olfactory reference syndrome.
1. Iwu CO, Akpata O. Delusional halitosis. Review of the literature and analysis of 32 cases. Br Dent J 1989;167:294-6.
2. Osman AA. Monosymptomatic hypochondriacal psychosis in developing countries. Br J Psychiatry 1991;159:428-31.
3. Pryse-Phillips W. An olfactory reference syndrome. Acta Psychiatr Scand 1971;47:484-509.
4. Yamada M, Shigemoto T, Kashiwamura K, et al. Fear of emitting bad odors. Bull Yamaguchi Med Sch 1977;24:141-61.
5. Potts CS. Two cases of hallucination of smell. University of Pennsylvania Medical Magazine 1891;226.-
6. Forte FS. Olfactory hallucinations as a proctologic manifestation of early schizophrenia. Am J Surg 1952;84:620-2.
7. Marks I, Mishan J. Dysmorphophobic avoidance with disturbed bodily perception: a pilot study of exposure therapy. Br J Psychiatry 1988;152:674-8.
8. Kasahara Y, Kenji S. Ereuthophobia and allied conditions: a contribution toward the psychopathological and cross-cultural study of a borderline state. In: Arieti S, ed. The world biennial of psychiatry in psychotherapy. New York, NY: Basic Books, 1971.
9. Iwakura M, Yasuno Y, Shimura M, Sakamoto S. Clinical characteristics of halitosis: differences in two patient groups with primary and secondary complaints of halitosis. J Dent Res 1994;73:1568-74.
10. Johanson E. Mild paranoia. Acta Psychiatr Scand 1964;40:13-4.
11. Sutton RL. Bromidrosiphobia. JAMA 1919;72:1267-8.
12. Malasi TH, El-Hilu SR, Mirza IA, Fakhr El-Islam M. Olfactory delusional syndrome with various aetiologies. Br J Psychiatry 1990;156:256-60.
13. Alvarez WC. Practical leads to puzzling diagnoses. Philadelphia, PA: JB Lippincott; 1958.
14. Brotman AW, Jenike MA. Monosymptomatic hypochondriasis treated with tricyclic antidepressants. Am J Psychiatry 1984;141:1608-9.
15. Videbech T. Chronic olfactory paranoid syndromes. Acta Psychiatr Scand 1966;42:183-213.
16. Phillips KA, Menard W, Fay C, Weisberg R. Demographic characteristics, phenomenology, comorbidity, and family history in 200 individuals with body dysmorphic disorder. Psychosom 2005;46:317-32.
17. Lochner C, Stein DJ. Olfactory reference syndrome: diagnostic criteria and differential diagnosis. J Postgrad Med 2003;49:328-31.
18. Dominguez RA, Puig A. Olfactory reference syndrome responds to clomipramine but not fluoxetine: a case report. J Clin Psychiatry 1997;58:497-8.
19. Ross CA, Siddiqui AR, Matas M. DSM-III. Problems in diagnosis of paranoia and obsessive-compulsive disorder. Can J Psychiatry 1987;32:146-8.
20. Ulzen TPM. Pimozide-responsive monosymptomatic hypochondriacal psychosis in an adolescent. Can J Psychiatry 1993;38:153-4.
21. Riding J, Munro A. Pimozide in the treatment of monosymptomatic hypochondriacal psychosis. Acta Psychiatr Scand 1975;52:23-30.
22. Kong SG, Tan KH. Monosymptomatic hypochondriacal psychosis: a report of 3 cases. Singapore Med J 1984;25:432-5.
23. Gomen-Perez JD, Marks IM, Gutierrez-Fisac JL. Dysmorphophobia: clinical features and outcome with behavior therapy. Eur Psychiatry 1994;9:229-35.
24. Milan MA, Kolko DJ. Paradoxical intention in the treatment of obsessional flatulence ruminations. J Behav Ther Exp Psychiatry 1982;13:167-72.
25. Phillips KA. The broken mirror: understanding and treating body dysmorphic disorder. New York, NY: Oxford University Press; 1996 (revised and expanded edition, 2005; Japanese edition, 1999).
26. Marks IM. Fears, phobias, and rituals. Oxford, UK: Oxford University Press; 1987.
Ms. A, a 21-year-old teacher, recalled always having been “sensitive,” but when she started her first job at age 19 she began to believe that she emitted an offensive odor. She experienced thoughts that she passed offensive flatus, her breath had a fecal odor, and people noticed and were offended.
Gradually Ms. A became more convinced of these distressing beliefs and began to think that she permeated fecal odor through her skin. She also became sure that colleagues were talking about her and that they complained about her “disgusting” smell.
Patients with olfactory reference syndrome (ORS) falsely believe they emit an offensive body odor. Prominent referential thinking—believing that other people perceive the odor—also is common. To introduce you to ORS, we discuss its clinical diagnosis and treatment based on our review of several hundred cases, including the largest reported series of patients with ORS.1-4
Olfactory reference syndrome (ORS) has been described around the world for more than a century. In 1891, Potts described a delusional 50-year-old man who “had been troubled for the past three months with smelling a very bad odor, which he likened to that of a ‘back-house,’ and which came from his own person. [He believed] this smell was so very strong that other men objected to working with him….”
Despite its long history, the syndrome’s prevalence is not well-established. ORS probably is underdiagnosed and more common than generally recognized:
- In a tertiary psychiatry unit in London, 0.5% of 2,000 patients who were not systematically screened for ORS spontaneously reported ORS symptoms.
- In a self-report survey of 2,481 students in Japan, 2.1% had been concerned with emitting a strange bodily odor during the past year.
- In a study in a dental clinic in Japan, the majority of patients with a primary complaint of halitosis actually had “imaginary halitosis” (another term for ORS).
Clinical features of ors
Ms. A quit her job and felt confident enough to work again only when she performed a 2-hour daily cleansing routine, doused herself in per-fume, and placed an incontinence pad in her underwear. Despite these precautions, she still thought her colleagues avoided her.
She always averted her mouth when speaking, held her hand in front of her mouth, and sat far from others and close to the door in meetings. She tried to keep meeting room doors open and believed that colleagues held their hands to their noses to “protect” themselves from her odor.
ORS symptoms are most often reported as beginning when patients are in their mid 20s, although some reports suggest onset during puberty or adolescence.4 In clinical series, the ratio of men to women is approximately 2:1.
Preoccupation. Individuals with ORS are preoccupied with the belief that they emit an unpleasant or offensive body odor (Box 1),1,2,5-9 most commonly:
Although most reports suggest that patients focus on one odor, some describe being concerned about several smells simultaneously or different odors over time.10,11
Referential thinking. As the syndrome’s name implies, many ORS patients have delusions of reference, falsely believing that other people perceive the odor.3 They misinterpret the behavior of others, assuming it is a reaction to how the patient smells (Box 2).2,3
They may misperceive comments (such as, “It’s stuffy in here”), receiving perfume or soap as a gift, or behaviors such as people sniffing, touching or rubbing their nose, clearing their throat, opening a window to get fresh air, putting a newspaper in front of their face, or looking or moving toward or away from the patient.1,3,5,7
Because they are ashamed, embarrassed, and concerned about offending others with their odor,13 many patients engage in repetitive and “safety” behaviors intended to check, eliminate, or camouflage the supposed odor (Box 3).1,3,7,12,14
DSM-IV-TR classifies olfactory reference syndrome (ORS) as a delusional disorder, somatic type (the modern equivalent of monosymptomatic hypochondriacal psychosis). ORS also is mentioned in the text on social anxiety disorder. ORS may not be diagnosed if:
- criterion A for schizophrenia has ever been met
- or if symptoms are due to the direct physiologic effects of a substance or a general medical condition, such as a brain tumor or temporal lobe epilepsy.
Many patients report being able to smell the imagined odor, suggesting that they experience an olfactory hallucination. Pryse-Phillips described the olfactory hallucinations of her 36 ORS case patients as “a real and immediate perception… often perceived in the absence of other odors.”
ORS generally is regarded as delusional, with possible secondary illusional misinterpretations and referential thinking. ORS beliefs usually appear to be of delusional intensity, although some patients may have some—although limited—insight (that is, overvalued ideation).
Functional impairment. Individuals with ORS often avoid other people or believe that others avoid them.12 They are typically embarrassed and worried that others will be offended by the smell. They may:
- avoid activities such as dating
- break off engagements
- refuse to travel
- move to another town
- become housebound.3,7,10,12
The distress and impaired functioning may lead to psychiatric hospitalization, depression, suicidal ideation, suicide attempts, and completed suicide.7,10,12,15 Pryse-Phillips studied 36 patients with ORS and reported:
- nearly one-half (43%) experienced “suicidal ideas or action”
- 2 (5.6%) committed suicide.3
Some authors have questioned whether ORS can transform into schizophrenia, but others have found little evidence for this.3,6
Psychiatric comorbidity. Depression is mentioned most often in the literature.12,13 In Pryse-Phillips’ 36 ORS patients (who did not have a “primary” depressive disorder), depression symptoms tended to be severe.3 The depression generally is considered secondary to ORS, although Pryse-Phillips evaluated 50 additional patients with ORS symptoms whom she considered to have a “primary” depressive disorder.3 Other psychiatric comorbidities include bipolar disorder, personality disorder, schizophrenia, hypochondriasis, alcohol and/or drug abuse, obsessive-compulsive disorder (OCD), and body dysmorphic disorder.3,7,15 In a study of 200 individuals with body dysmorphic disorder, 8 had comorbid ORS.16
Diagnosing ORS
Clinical clues to ORS (Table 1) probably are not present in all patients and some are not specific to ORS. They appear to be common features of the illness, however, and may alert you to its presence. Our clinical impression is that many patients with ORS are secretive about their symptoms because they are ashamed of them. Thus, you need to be alert to clues and specifically inquire about ORS symptoms to detect its presence.
Criteria. DSM-IV-TR and ICD-10 lack specific diagnostic criteria for ORS, instead applying criteria for delusional disorder. One problem with this approach is that delusional disorder criteria specify that any co-occurring mood symptoms must be brief relative to the duration of the delusional periods. This requirement may not be valid when applied to ORS.
In our experience, some patients have protracted depressive symptoms that appear secondary to “primary” ORS symptoms, and another diagnosis—such as psychotic depression—does not appear to account for their symptoms.
We propose working diagnostic criteria for ORS (Table 2), which are similar to those proposed by Lochner and Stein17 and require empiric validation. Suggested questions for the patient interview (Table 3) can help you identify and diagnose ORS.
Differential diagnosis. Keep in mind that a false belief that one emits a bad smell may be a symptom of schizophrenia, and this would trump an ORS diagnosis if other schizophrenia symptoms are present. Some patients with severe depression may believe they smell bad as part of a nihilistic delusional belief system (such as in Cotard’s syndrome—nihilistic delusions in severe depression).
Whether to conceptualize a false belief about body odor as a symptom of depression or as ORS with comorbid or secondary depression may be unclear from case to case.
Table 1
Clinical clues to the presence of olfactory reference syndrome
| Referential thinking. Interpreting actions of others—such as opening a window, moving away, putting a hand to their nose, or making comments related to odors—as evidence that the person smells offensive |
| Excessive attempts to ‘disguise’ the smell, such as washing routines, clothes changing, clothes laundering, or using abundant perfume, deodorant, mouthwash, mints, or other forms of camouflage |
| Other excessive and repetitive behaviors, such as checking for or asking other people for reassurance about the odor |
| Social anxiety or avoidance of social activities, relationships, work, school, or other daily activities |
| Requests for treatment for the perceived odor from dentists, gastroenterologists, proctologists, or other nonpsychiatric physicians despite a negative medical workup |
Working diagnostic criteria for olfactory reference syndrome
| A. | Persistent false belief that one emits a malodorous smell; this belief may encompass a range of insight and does not have to be delusional |
| B. | The belief is time-consuming and preoccupies the individual for at least 1 hour per day |
| C. | The belief causes clinically significant distress or results in significant impairment in social, occupational, or other important areas of functioning |
| D. | The belief is not better accounted for by another mental disorder or a general medical condition |
Table 3
Diagnosing ORS: Suggested questions for patient interview
|
Treatment-seeking behavior
Ms. A consulted several proctologists and a dentist but was not convinced by their reassurance and continued to believe she “stank.” Her relationship with her boyfriend suffered because she continually asked for reassurance about how she smelled and avoided sexual intercourse because of her odor concerns.
Eventually she confronted her boss about her belief that her coworkers were complaining about her smell. Despite reassurance that she didn’t smell bad, she left her job.
Excessive showering or washing are among the repetitive, ritualistic or “safety” behaviors many patients with ORS engage in to check, eliminate, or camouflage supposed odor. Frequent clothes changing or laundering also is common.
Camouflaging attempts may include excessive use of deodorant, soap, cologne, powder, mints, mouthwash, or toothpaste; wearing layers of clothing; or smoking.
Many patients frequently check for the odor or its source (such as trying to smell their own breath or checking the anal area for seepage). Some patients use the toilet excessively or eat a special diet to try to minimize the smell. Others repeatedly seek reassurance about how they smell.
Avoidance behaviors are common and include sitting far from other people, moving as little as possible to avoid spreading the supposed odor, or averting the head or covering the mouth.
Convincing patients such as Ms. A of the falsity of their beliefs can be difficult,1 and some succeed in having medical procedures or surgery, such as excision of tonsils or axillary glands.3,7,12 To our knowledge, controlled prospective studies of nonpsychiatric treatments have not been done, but it appears that such treatments usually are ineffective.1,3,6,9
Psychiatric interventions. Convincing patients with ORS to obtain mental health treatment can be difficult.2,6 Patients with delusional halitosis “would rather go in search of a ‘better dentist’ than go to a psychiatrist.”1
To get patients to accept psychiatric treatment, we suggest an approach similar to that recommended for body dysmorphic disorder. It may be helpful, for example, to focus on the distress and disability caused by the odor preoccupation, rather than on whether the patient actually smells bad.
Medication and psychotherapy
Limited evidence. The ORS treatment literature is very limited, consisting largely of case reports and small case series. To our knowledge, no controlled treatment trials have been done, no treatments have been compared head to head, and most studies did not use standardized measurements of psychopathology.
Published data therefore must be interpreted cautiously. Some medication reports used relatively low doses and short treatment durations (although what constitutes an adequate therapeutic trial for ORS is not known). Psychotherapy reports often did not specify details of the intervention or the number and duration of sessions. It is not known whether adding a cognitive component to behavioral therapy enhances efficacy, and the combination of psychotherapy and medication has not been studied systematically. More methodologically rigorous treatment studies are needed.
Because of space limitations, we cite representative case reports in the following section of this treatment review, rather than all of the cases found in our literature search.
Antidepressants. Although most ORS patients are delusional, serotonin reuptake inhibitor (SRI) monotherapy has been reported to be efficacious in 10 of 15 cases (67%). Most of these patients received clomipramine.18 In reports of non-SRI antidepressants, 6 of 15 cases (43%) responded. Some patients’ symptoms responded to an antidepressant after failing to respond to antipsychotic treatment.19
Antipsychotics. Pimozide is the most studied medication for ORS, with 15 of 31 cases (48%) responding.2,20 In a series of 12 patients, pimozide responders received 2 to 4 mg/d, except for one patient who needed 6 mg/d.21 Patients usually responded within 1 to 4 weeks (an average time to response was not reported). In 2 of these cases, ORS symptoms recurred after pimozide was discontinued and then remitted again after it was restarted.21 In another report,2 7 of 14 patients (50%) responded to pimozide.
Clinicians using other first-generation antipsychotics (trifluoperazine, thioridazine, and chlorpromazine) reported a positive response in only 2 of 19 cases (11%).12,22
Combination therapy. Ten of 17 cases (59%) of ORS responded to combined treatment with an antidepressant and an antipsychotic.2,12
Other somatic treatments. Several reports found benzodiazepine monotherapy lacked efficacy, as was the case for electroconvulsive therapy.12,15 One report noted an unsuccessful outcome with leucotomy and a partial response with bilateral partial division of the thalamo-frontal tract.15
Psychosocial treatment. All reports of psychosocial therapies are single cases or small series, and none used a control intervention.2,7,14
Behavioral treatment has been efficacious, although patients require months to years to habituate. Several reports totalling 14 patients describe behavioral treatment over weeks to months.7,23 These treatments involved exposure to avoided social situations and response prevention, which consisted of refraining from repetitive or camouflaging behaviors such as showering, visits to the toilet, or deodorant use. Gomez-Perez and colleagues23 noted that exposure therapy was less effective for ORS than for social phobia or OCD.
One report described a patient with flatulence concerns who responded to a paradoxical intention consisting of instructions to emit gas as soon as it was experienced; at 1-year follow-up, her symptoms had not recurred.24
Psychodynamic interventions show no benefit for ORS symptoms.
Treatment summary
Ms. A became increasingly despondent and depressed. She eventually sought the help of her family doctor, who referred her to a psychiatrist. With a combination of a serotonergic antidepressant (escitalopram, 40 mg/d), a low-dose atypical antipsychotic (quetiapine, 50 mg at night), and cognitive-behavioral therapy, she started to re-engage in daily activities. During 6 months of treatment, the intensity of her belief about having body odor abated.
Limited data support the use of SRI monotherapy or an SRI plus an antipsychotic. Using SRI monotherapy for delusional patients may sound counterintuitive, but this approach appears efficacious for patients with delusional body dysmorphic disorder, which has similarities to ORS.17,25,26
Clinically, we have found the use of atypical antipsychotics as an adjunct to SRIs to be helpful, although this strategy has not been subjected to clinical trials. Pimozide alone or in combination with an antidepressant also appears promising, as does exposure and response prevention. Do not combine pimozide with clomipramine because of the risk of cardiac toxicity.
Related resources
- Phillips KA, Gunderson C, Gruber U, Castle DJ. Delusions of body malodour: the olfactory reference syndrome. In: Brewer W, Castle D, Pantelis C. Olfaction and the brain. Cambridge, UK: Cambridge University Press; 2006:334-53.
- Pryse-Phillips W. An olfactory reference syndrome. Acta Psychiatr Scand 1971;47:484-509.
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Escitalopram • Lexapro
- Pimozide • Orap
- Quetiapine • Seroquel
- Thioridazine • Mellaril
- Trifluoperazine • Stelazine
Dr. Phillips receives research support from the National Institute of Mental Health, the Food and Drug Administration, UCB Pharma, and Forest Pharmaceuticals.
Dr. Castle receives research support from Janssen-Cilag; is a consultant to Eli Lilly and Company., Bristol-Myers Squibb, and Lundbeck; and is a speaker for Eli Lilly and Co., sanofi-aventis, Bristol-Myers Squibb, Janssen-Cilag, Lundbeck, and Organon.
Acknowledgment
The authors would like to thank Craig Gunderson, MD, and Uschi Gruber, MB, for their assistance with a literature search on olfactory reference syndrome.
Ms. A, a 21-year-old teacher, recalled always having been “sensitive,” but when she started her first job at age 19 she began to believe that she emitted an offensive odor. She experienced thoughts that she passed offensive flatus, her breath had a fecal odor, and people noticed and were offended.
Gradually Ms. A became more convinced of these distressing beliefs and began to think that she permeated fecal odor through her skin. She also became sure that colleagues were talking about her and that they complained about her “disgusting” smell.
Patients with olfactory reference syndrome (ORS) falsely believe they emit an offensive body odor. Prominent referential thinking—believing that other people perceive the odor—also is common. To introduce you to ORS, we discuss its clinical diagnosis and treatment based on our review of several hundred cases, including the largest reported series of patients with ORS.1-4
Olfactory reference syndrome (ORS) has been described around the world for more than a century. In 1891, Potts described a delusional 50-year-old man who “had been troubled for the past three months with smelling a very bad odor, which he likened to that of a ‘back-house,’ and which came from his own person. [He believed] this smell was so very strong that other men objected to working with him….”
Despite its long history, the syndrome’s prevalence is not well-established. ORS probably is underdiagnosed and more common than generally recognized:
- In a tertiary psychiatry unit in London, 0.5% of 2,000 patients who were not systematically screened for ORS spontaneously reported ORS symptoms.
- In a self-report survey of 2,481 students in Japan, 2.1% had been concerned with emitting a strange bodily odor during the past year.
- In a study in a dental clinic in Japan, the majority of patients with a primary complaint of halitosis actually had “imaginary halitosis” (another term for ORS).
Clinical features of ors
Ms. A quit her job and felt confident enough to work again only when she performed a 2-hour daily cleansing routine, doused herself in per-fume, and placed an incontinence pad in her underwear. Despite these precautions, she still thought her colleagues avoided her.
She always averted her mouth when speaking, held her hand in front of her mouth, and sat far from others and close to the door in meetings. She tried to keep meeting room doors open and believed that colleagues held their hands to their noses to “protect” themselves from her odor.
ORS symptoms are most often reported as beginning when patients are in their mid 20s, although some reports suggest onset during puberty or adolescence.4 In clinical series, the ratio of men to women is approximately 2:1.
Preoccupation. Individuals with ORS are preoccupied with the belief that they emit an unpleasant or offensive body odor (Box 1),1,2,5-9 most commonly:
Although most reports suggest that patients focus on one odor, some describe being concerned about several smells simultaneously or different odors over time.10,11
Referential thinking. As the syndrome’s name implies, many ORS patients have delusions of reference, falsely believing that other people perceive the odor.3 They misinterpret the behavior of others, assuming it is a reaction to how the patient smells (Box 2).2,3
They may misperceive comments (such as, “It’s stuffy in here”), receiving perfume or soap as a gift, or behaviors such as people sniffing, touching or rubbing their nose, clearing their throat, opening a window to get fresh air, putting a newspaper in front of their face, or looking or moving toward or away from the patient.1,3,5,7
Because they are ashamed, embarrassed, and concerned about offending others with their odor,13 many patients engage in repetitive and “safety” behaviors intended to check, eliminate, or camouflage the supposed odor (Box 3).1,3,7,12,14
DSM-IV-TR classifies olfactory reference syndrome (ORS) as a delusional disorder, somatic type (the modern equivalent of monosymptomatic hypochondriacal psychosis). ORS also is mentioned in the text on social anxiety disorder. ORS may not be diagnosed if:
- criterion A for schizophrenia has ever been met
- or if symptoms are due to the direct physiologic effects of a substance or a general medical condition, such as a brain tumor or temporal lobe epilepsy.
Many patients report being able to smell the imagined odor, suggesting that they experience an olfactory hallucination. Pryse-Phillips described the olfactory hallucinations of her 36 ORS case patients as “a real and immediate perception… often perceived in the absence of other odors.”
ORS generally is regarded as delusional, with possible secondary illusional misinterpretations and referential thinking. ORS beliefs usually appear to be of delusional intensity, although some patients may have some—although limited—insight (that is, overvalued ideation).
Functional impairment. Individuals with ORS often avoid other people or believe that others avoid them.12 They are typically embarrassed and worried that others will be offended by the smell. They may:
- avoid activities such as dating
- break off engagements
- refuse to travel
- move to another town
- become housebound.3,7,10,12
The distress and impaired functioning may lead to psychiatric hospitalization, depression, suicidal ideation, suicide attempts, and completed suicide.7,10,12,15 Pryse-Phillips studied 36 patients with ORS and reported:
- nearly one-half (43%) experienced “suicidal ideas or action”
- 2 (5.6%) committed suicide.3
Some authors have questioned whether ORS can transform into schizophrenia, but others have found little evidence for this.3,6
Psychiatric comorbidity. Depression is mentioned most often in the literature.12,13 In Pryse-Phillips’ 36 ORS patients (who did not have a “primary” depressive disorder), depression symptoms tended to be severe.3 The depression generally is considered secondary to ORS, although Pryse-Phillips evaluated 50 additional patients with ORS symptoms whom she considered to have a “primary” depressive disorder.3 Other psychiatric comorbidities include bipolar disorder, personality disorder, schizophrenia, hypochondriasis, alcohol and/or drug abuse, obsessive-compulsive disorder (OCD), and body dysmorphic disorder.3,7,15 In a study of 200 individuals with body dysmorphic disorder, 8 had comorbid ORS.16
Diagnosing ORS
Clinical clues to ORS (Table 1) probably are not present in all patients and some are not specific to ORS. They appear to be common features of the illness, however, and may alert you to its presence. Our clinical impression is that many patients with ORS are secretive about their symptoms because they are ashamed of them. Thus, you need to be alert to clues and specifically inquire about ORS symptoms to detect its presence.
Criteria. DSM-IV-TR and ICD-10 lack specific diagnostic criteria for ORS, instead applying criteria for delusional disorder. One problem with this approach is that delusional disorder criteria specify that any co-occurring mood symptoms must be brief relative to the duration of the delusional periods. This requirement may not be valid when applied to ORS.
In our experience, some patients have protracted depressive symptoms that appear secondary to “primary” ORS symptoms, and another diagnosis—such as psychotic depression—does not appear to account for their symptoms.
We propose working diagnostic criteria for ORS (Table 2), which are similar to those proposed by Lochner and Stein17 and require empiric validation. Suggested questions for the patient interview (Table 3) can help you identify and diagnose ORS.
Differential diagnosis. Keep in mind that a false belief that one emits a bad smell may be a symptom of schizophrenia, and this would trump an ORS diagnosis if other schizophrenia symptoms are present. Some patients with severe depression may believe they smell bad as part of a nihilistic delusional belief system (such as in Cotard’s syndrome—nihilistic delusions in severe depression).
Whether to conceptualize a false belief about body odor as a symptom of depression or as ORS with comorbid or secondary depression may be unclear from case to case.
Table 1
Clinical clues to the presence of olfactory reference syndrome
| Referential thinking. Interpreting actions of others—such as opening a window, moving away, putting a hand to their nose, or making comments related to odors—as evidence that the person smells offensive |
| Excessive attempts to ‘disguise’ the smell, such as washing routines, clothes changing, clothes laundering, or using abundant perfume, deodorant, mouthwash, mints, or other forms of camouflage |
| Other excessive and repetitive behaviors, such as checking for or asking other people for reassurance about the odor |
| Social anxiety or avoidance of social activities, relationships, work, school, or other daily activities |
| Requests for treatment for the perceived odor from dentists, gastroenterologists, proctologists, or other nonpsychiatric physicians despite a negative medical workup |
Working diagnostic criteria for olfactory reference syndrome
| A. | Persistent false belief that one emits a malodorous smell; this belief may encompass a range of insight and does not have to be delusional |
| B. | The belief is time-consuming and preoccupies the individual for at least 1 hour per day |
| C. | The belief causes clinically significant distress or results in significant impairment in social, occupational, or other important areas of functioning |
| D. | The belief is not better accounted for by another mental disorder or a general medical condition |
Table 3
Diagnosing ORS: Suggested questions for patient interview
|
Treatment-seeking behavior
Ms. A consulted several proctologists and a dentist but was not convinced by their reassurance and continued to believe she “stank.” Her relationship with her boyfriend suffered because she continually asked for reassurance about how she smelled and avoided sexual intercourse because of her odor concerns.
Eventually she confronted her boss about her belief that her coworkers were complaining about her smell. Despite reassurance that she didn’t smell bad, she left her job.
Excessive showering or washing are among the repetitive, ritualistic or “safety” behaviors many patients with ORS engage in to check, eliminate, or camouflage supposed odor. Frequent clothes changing or laundering also is common.
Camouflaging attempts may include excessive use of deodorant, soap, cologne, powder, mints, mouthwash, or toothpaste; wearing layers of clothing; or smoking.
Many patients frequently check for the odor or its source (such as trying to smell their own breath or checking the anal area for seepage). Some patients use the toilet excessively or eat a special diet to try to minimize the smell. Others repeatedly seek reassurance about how they smell.
Avoidance behaviors are common and include sitting far from other people, moving as little as possible to avoid spreading the supposed odor, or averting the head or covering the mouth.
Convincing patients such as Ms. A of the falsity of their beliefs can be difficult,1 and some succeed in having medical procedures or surgery, such as excision of tonsils or axillary glands.3,7,12 To our knowledge, controlled prospective studies of nonpsychiatric treatments have not been done, but it appears that such treatments usually are ineffective.1,3,6,9
Psychiatric interventions. Convincing patients with ORS to obtain mental health treatment can be difficult.2,6 Patients with delusional halitosis “would rather go in search of a ‘better dentist’ than go to a psychiatrist.”1
To get patients to accept psychiatric treatment, we suggest an approach similar to that recommended for body dysmorphic disorder. It may be helpful, for example, to focus on the distress and disability caused by the odor preoccupation, rather than on whether the patient actually smells bad.
Medication and psychotherapy
Limited evidence. The ORS treatment literature is very limited, consisting largely of case reports and small case series. To our knowledge, no controlled treatment trials have been done, no treatments have been compared head to head, and most studies did not use standardized measurements of psychopathology.
Published data therefore must be interpreted cautiously. Some medication reports used relatively low doses and short treatment durations (although what constitutes an adequate therapeutic trial for ORS is not known). Psychotherapy reports often did not specify details of the intervention or the number and duration of sessions. It is not known whether adding a cognitive component to behavioral therapy enhances efficacy, and the combination of psychotherapy and medication has not been studied systematically. More methodologically rigorous treatment studies are needed.
Because of space limitations, we cite representative case reports in the following section of this treatment review, rather than all of the cases found in our literature search.
Antidepressants. Although most ORS patients are delusional, serotonin reuptake inhibitor (SRI) monotherapy has been reported to be efficacious in 10 of 15 cases (67%). Most of these patients received clomipramine.18 In reports of non-SRI antidepressants, 6 of 15 cases (43%) responded. Some patients’ symptoms responded to an antidepressant after failing to respond to antipsychotic treatment.19
Antipsychotics. Pimozide is the most studied medication for ORS, with 15 of 31 cases (48%) responding.2,20 In a series of 12 patients, pimozide responders received 2 to 4 mg/d, except for one patient who needed 6 mg/d.21 Patients usually responded within 1 to 4 weeks (an average time to response was not reported). In 2 of these cases, ORS symptoms recurred after pimozide was discontinued and then remitted again after it was restarted.21 In another report,2 7 of 14 patients (50%) responded to pimozide.
Clinicians using other first-generation antipsychotics (trifluoperazine, thioridazine, and chlorpromazine) reported a positive response in only 2 of 19 cases (11%).12,22
Combination therapy. Ten of 17 cases (59%) of ORS responded to combined treatment with an antidepressant and an antipsychotic.2,12
Other somatic treatments. Several reports found benzodiazepine monotherapy lacked efficacy, as was the case for electroconvulsive therapy.12,15 One report noted an unsuccessful outcome with leucotomy and a partial response with bilateral partial division of the thalamo-frontal tract.15
Psychosocial treatment. All reports of psychosocial therapies are single cases or small series, and none used a control intervention.2,7,14
Behavioral treatment has been efficacious, although patients require months to years to habituate. Several reports totalling 14 patients describe behavioral treatment over weeks to months.7,23 These treatments involved exposure to avoided social situations and response prevention, which consisted of refraining from repetitive or camouflaging behaviors such as showering, visits to the toilet, or deodorant use. Gomez-Perez and colleagues23 noted that exposure therapy was less effective for ORS than for social phobia or OCD.
One report described a patient with flatulence concerns who responded to a paradoxical intention consisting of instructions to emit gas as soon as it was experienced; at 1-year follow-up, her symptoms had not recurred.24
Psychodynamic interventions show no benefit for ORS symptoms.
Treatment summary
Ms. A became increasingly despondent and depressed. She eventually sought the help of her family doctor, who referred her to a psychiatrist. With a combination of a serotonergic antidepressant (escitalopram, 40 mg/d), a low-dose atypical antipsychotic (quetiapine, 50 mg at night), and cognitive-behavioral therapy, she started to re-engage in daily activities. During 6 months of treatment, the intensity of her belief about having body odor abated.
Limited data support the use of SRI monotherapy or an SRI plus an antipsychotic. Using SRI monotherapy for delusional patients may sound counterintuitive, but this approach appears efficacious for patients with delusional body dysmorphic disorder, which has similarities to ORS.17,25,26
Clinically, we have found the use of atypical antipsychotics as an adjunct to SRIs to be helpful, although this strategy has not been subjected to clinical trials. Pimozide alone or in combination with an antidepressant also appears promising, as does exposure and response prevention. Do not combine pimozide with clomipramine because of the risk of cardiac toxicity.
Related resources
- Phillips KA, Gunderson C, Gruber U, Castle DJ. Delusions of body malodour: the olfactory reference syndrome. In: Brewer W, Castle D, Pantelis C. Olfaction and the brain. Cambridge, UK: Cambridge University Press; 2006:334-53.
- Pryse-Phillips W. An olfactory reference syndrome. Acta Psychiatr Scand 1971;47:484-509.
- Chlorpromazine • Thorazine
- Clomipramine • Anafranil
- Escitalopram • Lexapro
- Pimozide • Orap
- Quetiapine • Seroquel
- Thioridazine • Mellaril
- Trifluoperazine • Stelazine
Dr. Phillips receives research support from the National Institute of Mental Health, the Food and Drug Administration, UCB Pharma, and Forest Pharmaceuticals.
Dr. Castle receives research support from Janssen-Cilag; is a consultant to Eli Lilly and Company., Bristol-Myers Squibb, and Lundbeck; and is a speaker for Eli Lilly and Co., sanofi-aventis, Bristol-Myers Squibb, Janssen-Cilag, Lundbeck, and Organon.
Acknowledgment
The authors would like to thank Craig Gunderson, MD, and Uschi Gruber, MB, for their assistance with a literature search on olfactory reference syndrome.
1. Iwu CO, Akpata O. Delusional halitosis. Review of the literature and analysis of 32 cases. Br Dent J 1989;167:294-6.
2. Osman AA. Monosymptomatic hypochondriacal psychosis in developing countries. Br J Psychiatry 1991;159:428-31.
3. Pryse-Phillips W. An olfactory reference syndrome. Acta Psychiatr Scand 1971;47:484-509.
4. Yamada M, Shigemoto T, Kashiwamura K, et al. Fear of emitting bad odors. Bull Yamaguchi Med Sch 1977;24:141-61.
5. Potts CS. Two cases of hallucination of smell. University of Pennsylvania Medical Magazine 1891;226.-
6. Forte FS. Olfactory hallucinations as a proctologic manifestation of early schizophrenia. Am J Surg 1952;84:620-2.
7. Marks I, Mishan J. Dysmorphophobic avoidance with disturbed bodily perception: a pilot study of exposure therapy. Br J Psychiatry 1988;152:674-8.
8. Kasahara Y, Kenji S. Ereuthophobia and allied conditions: a contribution toward the psychopathological and cross-cultural study of a borderline state. In: Arieti S, ed. The world biennial of psychiatry in psychotherapy. New York, NY: Basic Books, 1971.
9. Iwakura M, Yasuno Y, Shimura M, Sakamoto S. Clinical characteristics of halitosis: differences in two patient groups with primary and secondary complaints of halitosis. J Dent Res 1994;73:1568-74.
10. Johanson E. Mild paranoia. Acta Psychiatr Scand 1964;40:13-4.
11. Sutton RL. Bromidrosiphobia. JAMA 1919;72:1267-8.
12. Malasi TH, El-Hilu SR, Mirza IA, Fakhr El-Islam M. Olfactory delusional syndrome with various aetiologies. Br J Psychiatry 1990;156:256-60.
13. Alvarez WC. Practical leads to puzzling diagnoses. Philadelphia, PA: JB Lippincott; 1958.
14. Brotman AW, Jenike MA. Monosymptomatic hypochondriasis treated with tricyclic antidepressants. Am J Psychiatry 1984;141:1608-9.
15. Videbech T. Chronic olfactory paranoid syndromes. Acta Psychiatr Scand 1966;42:183-213.
16. Phillips KA, Menard W, Fay C, Weisberg R. Demographic characteristics, phenomenology, comorbidity, and family history in 200 individuals with body dysmorphic disorder. Psychosom 2005;46:317-32.
17. Lochner C, Stein DJ. Olfactory reference syndrome: diagnostic criteria and differential diagnosis. J Postgrad Med 2003;49:328-31.
18. Dominguez RA, Puig A. Olfactory reference syndrome responds to clomipramine but not fluoxetine: a case report. J Clin Psychiatry 1997;58:497-8.
19. Ross CA, Siddiqui AR, Matas M. DSM-III. Problems in diagnosis of paranoia and obsessive-compulsive disorder. Can J Psychiatry 1987;32:146-8.
20. Ulzen TPM. Pimozide-responsive monosymptomatic hypochondriacal psychosis in an adolescent. Can J Psychiatry 1993;38:153-4.
21. Riding J, Munro A. Pimozide in the treatment of monosymptomatic hypochondriacal psychosis. Acta Psychiatr Scand 1975;52:23-30.
22. Kong SG, Tan KH. Monosymptomatic hypochondriacal psychosis: a report of 3 cases. Singapore Med J 1984;25:432-5.
23. Gomen-Perez JD, Marks IM, Gutierrez-Fisac JL. Dysmorphophobia: clinical features and outcome with behavior therapy. Eur Psychiatry 1994;9:229-35.
24. Milan MA, Kolko DJ. Paradoxical intention in the treatment of obsessional flatulence ruminations. J Behav Ther Exp Psychiatry 1982;13:167-72.
25. Phillips KA. The broken mirror: understanding and treating body dysmorphic disorder. New York, NY: Oxford University Press; 1996 (revised and expanded edition, 2005; Japanese edition, 1999).
26. Marks IM. Fears, phobias, and rituals. Oxford, UK: Oxford University Press; 1987.
1. Iwu CO, Akpata O. Delusional halitosis. Review of the literature and analysis of 32 cases. Br Dent J 1989;167:294-6.
2. Osman AA. Monosymptomatic hypochondriacal psychosis in developing countries. Br J Psychiatry 1991;159:428-31.
3. Pryse-Phillips W. An olfactory reference syndrome. Acta Psychiatr Scand 1971;47:484-509.
4. Yamada M, Shigemoto T, Kashiwamura K, et al. Fear of emitting bad odors. Bull Yamaguchi Med Sch 1977;24:141-61.
5. Potts CS. Two cases of hallucination of smell. University of Pennsylvania Medical Magazine 1891;226.-
6. Forte FS. Olfactory hallucinations as a proctologic manifestation of early schizophrenia. Am J Surg 1952;84:620-2.
7. Marks I, Mishan J. Dysmorphophobic avoidance with disturbed bodily perception: a pilot study of exposure therapy. Br J Psychiatry 1988;152:674-8.
8. Kasahara Y, Kenji S. Ereuthophobia and allied conditions: a contribution toward the psychopathological and cross-cultural study of a borderline state. In: Arieti S, ed. The world biennial of psychiatry in psychotherapy. New York, NY: Basic Books, 1971.
9. Iwakura M, Yasuno Y, Shimura M, Sakamoto S. Clinical characteristics of halitosis: differences in two patient groups with primary and secondary complaints of halitosis. J Dent Res 1994;73:1568-74.
10. Johanson E. Mild paranoia. Acta Psychiatr Scand 1964;40:13-4.
11. Sutton RL. Bromidrosiphobia. JAMA 1919;72:1267-8.
12. Malasi TH, El-Hilu SR, Mirza IA, Fakhr El-Islam M. Olfactory delusional syndrome with various aetiologies. Br J Psychiatry 1990;156:256-60.
13. Alvarez WC. Practical leads to puzzling diagnoses. Philadelphia, PA: JB Lippincott; 1958.
14. Brotman AW, Jenike MA. Monosymptomatic hypochondriasis treated with tricyclic antidepressants. Am J Psychiatry 1984;141:1608-9.
15. Videbech T. Chronic olfactory paranoid syndromes. Acta Psychiatr Scand 1966;42:183-213.
16. Phillips KA, Menard W, Fay C, Weisberg R. Demographic characteristics, phenomenology, comorbidity, and family history in 200 individuals with body dysmorphic disorder. Psychosom 2005;46:317-32.
17. Lochner C, Stein DJ. Olfactory reference syndrome: diagnostic criteria and differential diagnosis. J Postgrad Med 2003;49:328-31.
18. Dominguez RA, Puig A. Olfactory reference syndrome responds to clomipramine but not fluoxetine: a case report. J Clin Psychiatry 1997;58:497-8.
19. Ross CA, Siddiqui AR, Matas M. DSM-III. Problems in diagnosis of paranoia and obsessive-compulsive disorder. Can J Psychiatry 1987;32:146-8.
20. Ulzen TPM. Pimozide-responsive monosymptomatic hypochondriacal psychosis in an adolescent. Can J Psychiatry 1993;38:153-4.
21. Riding J, Munro A. Pimozide in the treatment of monosymptomatic hypochondriacal psychosis. Acta Psychiatr Scand 1975;52:23-30.
22. Kong SG, Tan KH. Monosymptomatic hypochondriacal psychosis: a report of 3 cases. Singapore Med J 1984;25:432-5.
23. Gomen-Perez JD, Marks IM, Gutierrez-Fisac JL. Dysmorphophobia: clinical features and outcome with behavior therapy. Eur Psychiatry 1994;9:229-35.
24. Milan MA, Kolko DJ. Paradoxical intention in the treatment of obsessional flatulence ruminations. J Behav Ther Exp Psychiatry 1982;13:167-72.
25. Phillips KA. The broken mirror: understanding and treating body dysmorphic disorder. New York, NY: Oxford University Press; 1996 (revised and expanded edition, 2005; Japanese edition, 1999).
26. Marks IM. Fears, phobias, and rituals. Oxford, UK: Oxford University Press; 1987.
Captive of the mirror: ‘I pick at my face all day, every day’
Lying in the hospital bed, her face covered in bandages, Ms. S talked of suicide while awaiting reconstructive surgery on her nose: “If the only way to stop is by killing myself, I will.” When asked what she wanted to stop, she replied, “The picking. I pick at my face all day, every day.”
Ms. S, age 22, had picked a hole through the bridge of her nose, and her face was scarred and covered with scabs. Every morning for 5 years, she had gotten up, dressed, and then—after washing her face—felt intense, uncontrollable urges to pick at her face. Hours would go by and she was still picking, even as her face started to bleed: “I try to resist, but I can’t.”
Ms. S started picking her face when she was 17. She missed so much of high school because of time spent picking that she did not graduate. She now lives alone on medical disability. Conscious of her facial scarring, she rarely goes out in public. “People stare at me as if I’m a zoo animal; it’s so painful,” she says.
After her plastic surgery, she told the staff psychiatrist she had never sought help because she thought no one would understand her behavior. “It doesn’t make sense to me, and I’ve lived with it for years.”
Patients such as Ms. S often suffer in isolation for years, unaware that skin picking is a psychiatric disorder that can be treated successfully. Some are referred to psychiatrists through hospital emergency rooms or by dermatologists; others commit suicide, as Ms. S threatened to do.
In our practice, we recognize skin picking in patients with comorbid mood and anxiety disorders, body dysmorphic disorder (BDD), substance use disorders, impulse control disorders such as trichotillomania or kleptomania, and personality disorders.
Based on recent evidence and our experience, we discuss three steps to help you diagnose pathologic skin picking. We then examine treatment options that have shown benefit for skinpicking patients, including habit reversal psychotherapy and medications.
WHAT IS SKIN PICKING?
Pathologic skin picking is repetitive, ritualistic, or impulsive picking of normal skin, leading to tissue damage, personal distress, and impaired functioning.1 The behavior has been described for more than 100 years but remains poorly understood, under-diagnosed, and under-treated.2,3
Most people pick at their hands or face to a limited extent,4 and picking does not by itself suggest a psychiatric disorder. Pathology exists in the focus, duration, and extent of the behavior, as well as reasons for picking, associated emotions, and resulting problems. Persons with pathologic skin picking report irresistible, intrusive, and/or senseless thoughts of picking or impulses to pick, accompanied by marked distress.1 Pathologic skin picking is recurrent and usually results in noticeable skin damage, although many patients try to camouflage the lesions or scarring with makeup.
Pathologic skin picking’s prevalence is unknown. One early study estimated that 2% of dermatology patients suffer from skin picking.1 Two clinical studies found that 3.8% of college students4 and 28% of patients with BDD meet diagnostic criteria.5,6
TWEEZERS, RAZOR BLADES, KNIVES…
Persons who engage in pathologic skin picking typically spend substantial time picking. Most often they pick the face, but any body part—lips, arms, hands, or legs—may be the focus. They may pick at blemishes, pimples, scars, or healthy skin. Some use their hands and fingernails to pick, and others use pins, tweezers, razor blades, or knives. Picking may worsen in the evening.2,7
Although picking episodes may last only a few minutes, many patients have multiple episodes each day. Some pick for as long as 12 hours every day,2,5 which often leads to scarring and disfigurement. In one study, 90% of patients had at least minor tissue damage, 61% suffered infections, and 45% had “deep craters” because of picking.2
Reasons for picking. Many patients pick to relieve discomfort or tension.1 Others pick to improve their appearance, as in BDD, or to remove perceived dirt or contaminants, as in obsessive-compulsive disorder (OCD).1,5 Still others say they pick as a habit, with minimal awareness.1 Itching or uneven skin may also cause the behavior.1,3 We have found that a patient may pick for several of these reasons. Most report:
- tension before picking
- satisfaction during picking
- guilt, shame, and dysphoria after picking.1
Social impairment. Shame after picking episodes often leads patients to cover lesions with clothing or makeup and to avoid social contact.7 Substantial social and occupational impairment have been reported3,5,7 because of the hours spent picking and from avoiding people because of disfigurement.
Physical injury. Skin picking may cause serious injuries. Some of our patients have required emergency medical intervention and sutures after picking through a major blood vessel (such as the facial artery). One woman—who picked at a pimple on her neck with tweezers—lacerated her carotid artery, causing a near-fatal hemorrhage that required emergency surgery.8
Suicide risk. In a series of 123 patients with BDD, 33 (27%) excessively picked their skin and 10 of those who picked their skin (33%) had attempted suicide.5 In a case series of 31 patients with skin picking, 10% had attempted suicide.2 We know of several young women whose chief complaint was skin picking and who committed suicide.5
Gender. The gender ratio of patients with skin picking remains unclear. In two case series that totaled 65 patients, 87% to 92% of those with pathologic skin picking were female.2,7 In the series of patients with BDD, 58% of the 33 who compulsively picked their skin were female.5 On the other hand, most of 28 patients seen in a dermatology clinic for neurotic excoriations were male.9
Onset and chronicity. Pathologic skin picking may develop at any age, but it usually manifests in late adolescence or early adulthood, often after onset of a dermatologic illness such as acne2 or in response to itching.3 Although long-term studies have not been done, the disorder appears to often be chronic, with waxing and waning of picking intensity and frequency.1,2
Table 1
Skin picking: 3 steps to diagnosis and treatment
| Step 1: Assess reasons for skin picking Dermatologic or medical disorder?
Psychiatric disorder?
Impulse control disorder, not otherwise specified? |
| Step 2: Assess picking severity Treat comorbid mood or anxiety disorders Treat skin picking if:
|
| Step 3: Provide recommended treatment For adults Habit reversal therapy plus medication is usually necessary For children and adolescents Habit reversal therapy alone for mild to moderate symptoms Habit reversal therapy plus medication for severe symptoms |
Comorbid psychopathology. In clinical settings, common comorbid psychopathologies include mood disorders (in 48% to 68% of patients with skin picking), anxiety disorders (41% to 64%), and alcohol use disorders (39%).2
In one patient sample, 71% of skin pickers met criteria for at least one personality disorder (48% had obsessive-compulsive personality disorder, and 26% met criteria for borderline personality disorder).2
Table 2
Medications with evidence of benefit for skin picking*
| Medication | Dosage | Type of evidence |
|---|---|---|
| SSRIs | ||
| Citalopram | 40 mg/d | Case report (effective only with inositol augmentation)16 |
| Fluoxetine | 20 to 80 mg/d | Case reports5,14-15 and two double-blind studies23-24 |
| Fluvoxamine | 100 to 300 mg/d | Case report,8 open-label study,21 and double-blind trial22 |
| Sertraline | 50 to 200 mg/d | Open-label study9 |
| Other agents | ||
| Clomipramine | 50 mg/d | Case report3 |
| Doxepin | 30 mg/d | Case report1 |
| Naltrexone | 50 mg/d | Case report20 |
| Olanzapine | 2.5 to 7.5 mg/d | Case report17 |
| Pimozide | 4 mg/d | Case report18 |
| * Off-label uses; little scientific evidence supports using medications other than SSRIs for treating skin picking. Inform patients of the evidence for using any medication, risk of side effects including change in cardiac conduction (pimozide, clomipramine), seizure risk (pimozide, clomipramine), and tardive dyskinesia (pimozide), and potential interactions with other medications (all of the above). | ||
PRIMARY VS. SECONDARY DISORDER
Is skin picking an independent disorder or a symptom of other psychiatric disorders? Although skin picking is not included in DSM-IV and has no formal diagnostic criteria, some forms of this behavior may belong among the impulse control disorders.
Patients often report an urge to pick their skin in response to increasing tension,1,3 and picking results in transient relief or pleasure.1,2 This description mirrors that of other impulse control disorders, such as trichotillomania and kleptomania. In fact, one study found that trichotillomania and kleptomania were common comorbidities among patients with skin picking (23% and 16%, respectively).2 In 34 patients with psychogenic excoriation, only 7 (21%) appeared to have skin picking as a primary complaint, unaccounted for by another psychiatric disorder.7
Skin picking may also be a symptom of other psychiatric disorders. To determine whether another disorder is present, we ask patients why they pick their skin. Patients may be reluctant to reveal either the picking or the underlying disorder because of embarrassment and shame. The diagnosis can often be clarified by asking about the following conditions:
Body dysmorphic disorder. Nearly 30% of patients with BDD pick their skin to a pathologic extent.5,6 The purpose of picking in BDD is to remove or minimize a nonexistent or slight imperfection in appearance (such as scars, pimples, bumps).5,6
Obsessive-compulsive disorder. Patients with OCD may pick their skin in response to contamination obsessions.1 Picking is often repetitive and ritualistic, and—as with compulsions—the behavior may reduce tension.10
Genetic disorders. Skin picking may be a symptom of Prader-Willi syndrome, a genetic disorder characterized by muscular hypotonia, short stature, characteristic facial features, intellectual disabilities, hypogonadism, hyperphagia, and an increased obesity risk. In one study, 97% of patients with Prader-Willi syndrome engaged in skin picking.11
Delusional disorder. Delusions of parasitosis may result in skin picking, as patients attempt to remove imagined parasites or other vermin from on or under their skin.12
Dermatitis artefacta. Patients may consciously create skin lesions to assume the sick role. Onethird of patients presenting to dermatologists with a disease that is primarily psychiatric may be suffering from dermatitis artefacta.13
TREATMENT RECOMMENDATIONS
Successful clinical care of pathologic skin picking requires perseverance and patience from both patient and clinician.
Treatment begins with a thorough dermatologic examination for medical causes of skin picking (such as atopic dermatitis or scabies) and to treat excoriations (such as with antibiotics for infection). After the dermatologist has ruled out a medical cause, carefully assess the patient’s picking behavior and related psychiatric problems (Table 1).
- If picking is secondary to a psychiatric disorder, begin by providing appropriate treatment for that disorder.
- If picking results from BDD or OCD, we recommend habit reversal therapy combined with medication.
- If picking appears to be an independent impulse control disorder, simultaneous habit reversal therapy and medication is usually necessary to reduce symptoms.
SSRIs are a reasonable first medication because of evidence for their efficacy in reducing skin picking. Higher dosages—comparable to those used in treating OCD—are usually required to improve skin-picking behavior. You may need to try another SSRI if the first trial results in partial or no response.
In our experience, augmenting an SSRI with naltrexone, 50 mg/d, helps reduce intrusive urges to pick and is worth considering if SSRI therapy results in only partial response.
Children or adolescents. Depending upon symptom severity, a trial of habit reversal therapy may be appropriate before you recommend using medication.
EVIDENCE FOR DRUG THERAPY
Although few treatment studies have been done, skin picking does appear to respond to medication (Table 2).
Because no medications are approved to treat skin-picking behavior, inform patients of any “off-label” uses and the scientific or clinical evidence for considering medication treatment.
Case reports and case series. Selective serotonin reuptake inhibitors (SSRIs) appear most effective in patients with picking behavior, including:
- fluvoxamine, 300 mg/d, in one case report8
- fluoxetine, 20 to 80 mg/d, in several case reports.5,14-15
In a series of 33 patients with BDD and compulsive skin picking, one-half (49%) of a variety of SSRI treatment trials improved BDD symptoms and skin picking behavior. The percentage of patients who improved was not examined. Dermatologic treatment alone was effective for only 15% of patients.5
Medications other than SSRIs have also been studied. One patient improved within 3 weeks of taking the tricyclic antidepressant clomipramine, 50 mg/d.3 Another patient picked her skin less often 4 weeks after inositol, 18 grams/d, was added to citalopram, 40 mg/d. Inositol, a nonprescription isomer of glucose, is a precursor in the phosphatidylinositol second-messenger cycle, which may play a role at certain serotonin receptors.16 The patient was given 6 grams dissolved in water three times daily.
Case reports have also suggested that olanzapine, pimozide, doxepin, and naltrexone may be beneficial in reducing skin excoriations. These reports often involved patients with psychiatric and medical comorbidities.17-20
Table 3
Habit reversal: 5 components in patient learning
| Awareness about picking behavior |
| Relaxation to reduce anxiety |
| Competing responses to learn behaviors incompatible with picking (such as fist clenching) |
| Rewarding oneself for successfully resisting picking |
| Generalizing the behavioral control |
Open-label studies. In an open-label study of 28 patients with neurotic excoriation treated in a dermatology clinic, 68% improved within 1 month with sertraline, mean dosage 95 mg/d.9 Similarly, open-label fluvoxamine, mean dosage 112.5 mg/d, was effective in reducing skin excoriation in 7 of 14 patients treated for 12 weeks in a psychiatric setting.21
Double-blind studies. In a double-blind study using fluvoxamine with supportive psychotherapy in patients with psychocutaneous disorders, all five patients with acne excoriee improved after 4 weeks of medication treatment (none was randomized to placebo).22
In a 10-week, double-blind study, 10 patients were assigned to fluoxetine, mean dosage 53.0 ± 16.4 mg/d, and 11 to placebo. A patient self-report visual analog scale showed that fluoxetine was significantly more effective than placebo in reducing picking behavior. Two other measures did not show significant improvement, however, perhaps because of the small sample size.23
In a third study, 8 of 15 patients responded to open-label fluoxetine, 20 to 60 mg/d after 6 weeks. The responders were then randomized to 6 additional weeks of fluoxetine or placebo. All four patients assigned to continue active medication maintained their improvement. Symptoms returned to baseline by week 12 in the four assigned to placebo.24
EVIDENCE FOR HABIT REVERSAL THERAPY
No controlled trials have examined psychosocial treatments for skin picking, but several psychotherapeutic interventions appear promising. Habit reversal has shown promise in three case reports totaling seven patients and appears to reduce picking behavior within a few weeks.25-27
In a case series, three patients were successfully treated with habit reversal (Table 3) and cognitive-behavioral techniques, consisting of:
- awareness training (using a skin-picking diary)
- competing response techniques (such as making a fist or squeezing a ball)
- emotion regulation skills
- psychoeducation
- cognitive restructuring (such as using Socratic questioning to produce rational alternatives) in situations that elicit the urge to pick.28
In another case series, 22 dermatology patients with skin picking received psychotherapy with insight-oriented and behavioral components. Therapy included attention to developmental issues and active conflicts, cognitive restructuring, and tools to manage aggression and social relations. Although treatment duration varied— the mean was weekly for 14 months—skin lesions healed in 17 patients (77%).29
Related resources
- Obsessive-Compulsive Foundation http://www.ocfoundation.org
- Koran LM. Obsessive-compulsive and related disorders in adults: A comprehensive clinical guide. Cambridge, UK: Cambridge University Press, 1999.
- Phillips KA. The broken mirror: Recognizing and treating body dysmorphic disorder. New York: Oxford University Press, 1996.
Drug brand names
- Citalopram • Celexa
- Clomipramine • Anafranil
- Doxepin • Sinequan
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Pimozide • Orap
- Sertraline • Zoloft
Disclosure
Dr. Grant reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Phillips receives research support from Eli Lilly and Co., Forest Pharmaceuticals, and Gate Pharmaceuticals; she is a speaker for or consultant to Eli Lilly and Co., Forest Pharmaceuticals, and UCB Pharma.
1. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 2001;15:351-9.
2. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry 1999;60:454-9.
3. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry 1986;27:381-6.
4. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skinpicking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics 2000;41:210-15.
5. Phillips KA, Taub SL. Skin picking as a symptom of body dysmorphic disorder. Psychopharmacol Bull 1995;31:279-88.
6. Phillips KA, Diaz S. Gender differences in body dysmorphic disorder. J Nerv Ment Dis 1997;185:570-7
7. Arnold LM, McElroy SL, Mutasim DF, et al. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry 1998;59:509-14.
8. O’Sullivan RL, Phillips KA, Keuthen NJ, Wilhelm S. Near fatal skin picking from delusional body dysmorphic disorder responsive to fluvoxamine. Psychosomatics 1999;40:79-81.
9. Kalivas J, Kalivas L, Gilman D, Hayden CT. Sertraline in the treatment of neurotic excoriations and related disorders [letter]. Arch Dermatol 1996;132:589-90.
10. Stein DJ, Hollander E. Dermatology and conditions related to obsessive-compulsive disorder. J Am Acad Dermatol 1992;26:237-42.
11. Dykens E, Shah B. Psychiatric disorders in Prader-Willi syndrome: epidemiology and management. CNS Drugs 2003;17:167-78.
12. Bishop ER. Monosymptomatic hypochondriacal syndromes in dermatology. J Am Acad Dermatol 1983;9:152-8.
13. Koblenzer CS. Dermatitis artefacta: clinical features and approaches to treatment. Am J Clin Dermatol 2000;1:47-55.
14. Stein DJ, Hutt CS, Spitz JL, Hollander E. Compulsive picking and obsessive-compulsive disorder. Psychosomatics 1993;34:177-80.
15. Stout RJ. Fluoxetine for the treatment of compulsive facial picking [letter]. Am J Psychiatry 1990;147:370.-
16. Seedat S, Stein DJ, Harvey BH. Inositol in the treatment of trichotillomania and compulsive skin picking [letter]. J Clin Psychiatry 2001;62:60-1.
17. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: three case reports. Cutis 2000;66:143-6.
18. Duke EE. Clinical experience with pimozide: emphasis on its use in postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
19. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol 1987;26:541-3.
20. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone [letter]. J Clin Psychopharmacol 1989;9:448-9.
21. Arnold LM, Mutasim DF, Dwight MM, et al. An open clinical trial of fluvoxamine treatment of psychogenic excoriation. J Clin Psychopharmacol 1999;19:15-18.
22. Hendrickx B, Van Moffaert M, Spiers R, Von Frenckell R. The treatment of psychocutaneous disorders: a new approach. Curr Ther Res Clin Exp 1991;49:111-19.
23. Simeon D, Stein DJ, Gross S, et al. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry 1997;58:341-7.
24. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 2001;42:314-19.
25. Kent A, Drummond LM. Acne excoriee—a case report of treatment using habit-reversal. Clin Exp Dermatol 1989;14:163-4.
26. Rosenbaum MS, Ayllon T. The behavioral treatment of neurodermatitis through habit-reversal. Behav Res Ther 1981;19:313-18.
27. Twohig MP, Woods DW. Habit reversal as a treatment for chronic skin picking in typically developing adult male siblings. J App Behav Analysis 2001;34:217-20.
28. Deckersbach T, Wilhelm S, Keuthen NJ, et al. Cognitive-behavior therapy for self-injurious skin picking. Behav Modif 2002;26:361-77.
29. Fruensgaard K. Psychotherapy and neurotic excoriations. Int J Dermatol 1991;30:262-5.
Lying in the hospital bed, her face covered in bandages, Ms. S talked of suicide while awaiting reconstructive surgery on her nose: “If the only way to stop is by killing myself, I will.” When asked what she wanted to stop, she replied, “The picking. I pick at my face all day, every day.”
Ms. S, age 22, had picked a hole through the bridge of her nose, and her face was scarred and covered with scabs. Every morning for 5 years, she had gotten up, dressed, and then—after washing her face—felt intense, uncontrollable urges to pick at her face. Hours would go by and she was still picking, even as her face started to bleed: “I try to resist, but I can’t.”
Ms. S started picking her face when she was 17. She missed so much of high school because of time spent picking that she did not graduate. She now lives alone on medical disability. Conscious of her facial scarring, she rarely goes out in public. “People stare at me as if I’m a zoo animal; it’s so painful,” she says.
After her plastic surgery, she told the staff psychiatrist she had never sought help because she thought no one would understand her behavior. “It doesn’t make sense to me, and I’ve lived with it for years.”
Patients such as Ms. S often suffer in isolation for years, unaware that skin picking is a psychiatric disorder that can be treated successfully. Some are referred to psychiatrists through hospital emergency rooms or by dermatologists; others commit suicide, as Ms. S threatened to do.
In our practice, we recognize skin picking in patients with comorbid mood and anxiety disorders, body dysmorphic disorder (BDD), substance use disorders, impulse control disorders such as trichotillomania or kleptomania, and personality disorders.
Based on recent evidence and our experience, we discuss three steps to help you diagnose pathologic skin picking. We then examine treatment options that have shown benefit for skinpicking patients, including habit reversal psychotherapy and medications.
WHAT IS SKIN PICKING?
Pathologic skin picking is repetitive, ritualistic, or impulsive picking of normal skin, leading to tissue damage, personal distress, and impaired functioning.1 The behavior has been described for more than 100 years but remains poorly understood, under-diagnosed, and under-treated.2,3
Most people pick at their hands or face to a limited extent,4 and picking does not by itself suggest a psychiatric disorder. Pathology exists in the focus, duration, and extent of the behavior, as well as reasons for picking, associated emotions, and resulting problems. Persons with pathologic skin picking report irresistible, intrusive, and/or senseless thoughts of picking or impulses to pick, accompanied by marked distress.1 Pathologic skin picking is recurrent and usually results in noticeable skin damage, although many patients try to camouflage the lesions or scarring with makeup.
Pathologic skin picking’s prevalence is unknown. One early study estimated that 2% of dermatology patients suffer from skin picking.1 Two clinical studies found that 3.8% of college students4 and 28% of patients with BDD meet diagnostic criteria.5,6
TWEEZERS, RAZOR BLADES, KNIVES…
Persons who engage in pathologic skin picking typically spend substantial time picking. Most often they pick the face, but any body part—lips, arms, hands, or legs—may be the focus. They may pick at blemishes, pimples, scars, or healthy skin. Some use their hands and fingernails to pick, and others use pins, tweezers, razor blades, or knives. Picking may worsen in the evening.2,7
Although picking episodes may last only a few minutes, many patients have multiple episodes each day. Some pick for as long as 12 hours every day,2,5 which often leads to scarring and disfigurement. In one study, 90% of patients had at least minor tissue damage, 61% suffered infections, and 45% had “deep craters” because of picking.2
Reasons for picking. Many patients pick to relieve discomfort or tension.1 Others pick to improve their appearance, as in BDD, or to remove perceived dirt or contaminants, as in obsessive-compulsive disorder (OCD).1,5 Still others say they pick as a habit, with minimal awareness.1 Itching or uneven skin may also cause the behavior.1,3 We have found that a patient may pick for several of these reasons. Most report:
- tension before picking
- satisfaction during picking
- guilt, shame, and dysphoria after picking.1
Social impairment. Shame after picking episodes often leads patients to cover lesions with clothing or makeup and to avoid social contact.7 Substantial social and occupational impairment have been reported3,5,7 because of the hours spent picking and from avoiding people because of disfigurement.
Physical injury. Skin picking may cause serious injuries. Some of our patients have required emergency medical intervention and sutures after picking through a major blood vessel (such as the facial artery). One woman—who picked at a pimple on her neck with tweezers—lacerated her carotid artery, causing a near-fatal hemorrhage that required emergency surgery.8
Suicide risk. In a series of 123 patients with BDD, 33 (27%) excessively picked their skin and 10 of those who picked their skin (33%) had attempted suicide.5 In a case series of 31 patients with skin picking, 10% had attempted suicide.2 We know of several young women whose chief complaint was skin picking and who committed suicide.5
Gender. The gender ratio of patients with skin picking remains unclear. In two case series that totaled 65 patients, 87% to 92% of those with pathologic skin picking were female.2,7 In the series of patients with BDD, 58% of the 33 who compulsively picked their skin were female.5 On the other hand, most of 28 patients seen in a dermatology clinic for neurotic excoriations were male.9
Onset and chronicity. Pathologic skin picking may develop at any age, but it usually manifests in late adolescence or early adulthood, often after onset of a dermatologic illness such as acne2 or in response to itching.3 Although long-term studies have not been done, the disorder appears to often be chronic, with waxing and waning of picking intensity and frequency.1,2
Table 1
Skin picking: 3 steps to diagnosis and treatment
| Step 1: Assess reasons for skin picking Dermatologic or medical disorder?
Psychiatric disorder?
Impulse control disorder, not otherwise specified? |
| Step 2: Assess picking severity Treat comorbid mood or anxiety disorders Treat skin picking if:
|
| Step 3: Provide recommended treatment For adults Habit reversal therapy plus medication is usually necessary For children and adolescents Habit reversal therapy alone for mild to moderate symptoms Habit reversal therapy plus medication for severe symptoms |
Comorbid psychopathology. In clinical settings, common comorbid psychopathologies include mood disorders (in 48% to 68% of patients with skin picking), anxiety disorders (41% to 64%), and alcohol use disorders (39%).2
In one patient sample, 71% of skin pickers met criteria for at least one personality disorder (48% had obsessive-compulsive personality disorder, and 26% met criteria for borderline personality disorder).2
Table 2
Medications with evidence of benefit for skin picking*
| Medication | Dosage | Type of evidence |
|---|---|---|
| SSRIs | ||
| Citalopram | 40 mg/d | Case report (effective only with inositol augmentation)16 |
| Fluoxetine | 20 to 80 mg/d | Case reports5,14-15 and two double-blind studies23-24 |
| Fluvoxamine | 100 to 300 mg/d | Case report,8 open-label study,21 and double-blind trial22 |
| Sertraline | 50 to 200 mg/d | Open-label study9 |
| Other agents | ||
| Clomipramine | 50 mg/d | Case report3 |
| Doxepin | 30 mg/d | Case report1 |
| Naltrexone | 50 mg/d | Case report20 |
| Olanzapine | 2.5 to 7.5 mg/d | Case report17 |
| Pimozide | 4 mg/d | Case report18 |
| * Off-label uses; little scientific evidence supports using medications other than SSRIs for treating skin picking. Inform patients of the evidence for using any medication, risk of side effects including change in cardiac conduction (pimozide, clomipramine), seizure risk (pimozide, clomipramine), and tardive dyskinesia (pimozide), and potential interactions with other medications (all of the above). | ||
PRIMARY VS. SECONDARY DISORDER
Is skin picking an independent disorder or a symptom of other psychiatric disorders? Although skin picking is not included in DSM-IV and has no formal diagnostic criteria, some forms of this behavior may belong among the impulse control disorders.
Patients often report an urge to pick their skin in response to increasing tension,1,3 and picking results in transient relief or pleasure.1,2 This description mirrors that of other impulse control disorders, such as trichotillomania and kleptomania. In fact, one study found that trichotillomania and kleptomania were common comorbidities among patients with skin picking (23% and 16%, respectively).2 In 34 patients with psychogenic excoriation, only 7 (21%) appeared to have skin picking as a primary complaint, unaccounted for by another psychiatric disorder.7
Skin picking may also be a symptom of other psychiatric disorders. To determine whether another disorder is present, we ask patients why they pick their skin. Patients may be reluctant to reveal either the picking or the underlying disorder because of embarrassment and shame. The diagnosis can often be clarified by asking about the following conditions:
Body dysmorphic disorder. Nearly 30% of patients with BDD pick their skin to a pathologic extent.5,6 The purpose of picking in BDD is to remove or minimize a nonexistent or slight imperfection in appearance (such as scars, pimples, bumps).5,6
Obsessive-compulsive disorder. Patients with OCD may pick their skin in response to contamination obsessions.1 Picking is often repetitive and ritualistic, and—as with compulsions—the behavior may reduce tension.10
Genetic disorders. Skin picking may be a symptom of Prader-Willi syndrome, a genetic disorder characterized by muscular hypotonia, short stature, characteristic facial features, intellectual disabilities, hypogonadism, hyperphagia, and an increased obesity risk. In one study, 97% of patients with Prader-Willi syndrome engaged in skin picking.11
Delusional disorder. Delusions of parasitosis may result in skin picking, as patients attempt to remove imagined parasites or other vermin from on or under their skin.12
Dermatitis artefacta. Patients may consciously create skin lesions to assume the sick role. Onethird of patients presenting to dermatologists with a disease that is primarily psychiatric may be suffering from dermatitis artefacta.13
TREATMENT RECOMMENDATIONS
Successful clinical care of pathologic skin picking requires perseverance and patience from both patient and clinician.
Treatment begins with a thorough dermatologic examination for medical causes of skin picking (such as atopic dermatitis or scabies) and to treat excoriations (such as with antibiotics for infection). After the dermatologist has ruled out a medical cause, carefully assess the patient’s picking behavior and related psychiatric problems (Table 1).
- If picking is secondary to a psychiatric disorder, begin by providing appropriate treatment for that disorder.
- If picking results from BDD or OCD, we recommend habit reversal therapy combined with medication.
- If picking appears to be an independent impulse control disorder, simultaneous habit reversal therapy and medication is usually necessary to reduce symptoms.
SSRIs are a reasonable first medication because of evidence for their efficacy in reducing skin picking. Higher dosages—comparable to those used in treating OCD—are usually required to improve skin-picking behavior. You may need to try another SSRI if the first trial results in partial or no response.
In our experience, augmenting an SSRI with naltrexone, 50 mg/d, helps reduce intrusive urges to pick and is worth considering if SSRI therapy results in only partial response.
Children or adolescents. Depending upon symptom severity, a trial of habit reversal therapy may be appropriate before you recommend using medication.
EVIDENCE FOR DRUG THERAPY
Although few treatment studies have been done, skin picking does appear to respond to medication (Table 2).
Because no medications are approved to treat skin-picking behavior, inform patients of any “off-label” uses and the scientific or clinical evidence for considering medication treatment.
Case reports and case series. Selective serotonin reuptake inhibitors (SSRIs) appear most effective in patients with picking behavior, including:
- fluvoxamine, 300 mg/d, in one case report8
- fluoxetine, 20 to 80 mg/d, in several case reports.5,14-15
In a series of 33 patients with BDD and compulsive skin picking, one-half (49%) of a variety of SSRI treatment trials improved BDD symptoms and skin picking behavior. The percentage of patients who improved was not examined. Dermatologic treatment alone was effective for only 15% of patients.5
Medications other than SSRIs have also been studied. One patient improved within 3 weeks of taking the tricyclic antidepressant clomipramine, 50 mg/d.3 Another patient picked her skin less often 4 weeks after inositol, 18 grams/d, was added to citalopram, 40 mg/d. Inositol, a nonprescription isomer of glucose, is a precursor in the phosphatidylinositol second-messenger cycle, which may play a role at certain serotonin receptors.16 The patient was given 6 grams dissolved in water three times daily.
Case reports have also suggested that olanzapine, pimozide, doxepin, and naltrexone may be beneficial in reducing skin excoriations. These reports often involved patients with psychiatric and medical comorbidities.17-20
Table 3
Habit reversal: 5 components in patient learning
| Awareness about picking behavior |
| Relaxation to reduce anxiety |
| Competing responses to learn behaviors incompatible with picking (such as fist clenching) |
| Rewarding oneself for successfully resisting picking |
| Generalizing the behavioral control |
Open-label studies. In an open-label study of 28 patients with neurotic excoriation treated in a dermatology clinic, 68% improved within 1 month with sertraline, mean dosage 95 mg/d.9 Similarly, open-label fluvoxamine, mean dosage 112.5 mg/d, was effective in reducing skin excoriation in 7 of 14 patients treated for 12 weeks in a psychiatric setting.21
Double-blind studies. In a double-blind study using fluvoxamine with supportive psychotherapy in patients with psychocutaneous disorders, all five patients with acne excoriee improved after 4 weeks of medication treatment (none was randomized to placebo).22
In a 10-week, double-blind study, 10 patients were assigned to fluoxetine, mean dosage 53.0 ± 16.4 mg/d, and 11 to placebo. A patient self-report visual analog scale showed that fluoxetine was significantly more effective than placebo in reducing picking behavior. Two other measures did not show significant improvement, however, perhaps because of the small sample size.23
In a third study, 8 of 15 patients responded to open-label fluoxetine, 20 to 60 mg/d after 6 weeks. The responders were then randomized to 6 additional weeks of fluoxetine or placebo. All four patients assigned to continue active medication maintained their improvement. Symptoms returned to baseline by week 12 in the four assigned to placebo.24
EVIDENCE FOR HABIT REVERSAL THERAPY
No controlled trials have examined psychosocial treatments for skin picking, but several psychotherapeutic interventions appear promising. Habit reversal has shown promise in three case reports totaling seven patients and appears to reduce picking behavior within a few weeks.25-27
In a case series, three patients were successfully treated with habit reversal (Table 3) and cognitive-behavioral techniques, consisting of:
- awareness training (using a skin-picking diary)
- competing response techniques (such as making a fist or squeezing a ball)
- emotion regulation skills
- psychoeducation
- cognitive restructuring (such as using Socratic questioning to produce rational alternatives) in situations that elicit the urge to pick.28
In another case series, 22 dermatology patients with skin picking received psychotherapy with insight-oriented and behavioral components. Therapy included attention to developmental issues and active conflicts, cognitive restructuring, and tools to manage aggression and social relations. Although treatment duration varied— the mean was weekly for 14 months—skin lesions healed in 17 patients (77%).29
Related resources
- Obsessive-Compulsive Foundation http://www.ocfoundation.org
- Koran LM. Obsessive-compulsive and related disorders in adults: A comprehensive clinical guide. Cambridge, UK: Cambridge University Press, 1999.
- Phillips KA. The broken mirror: Recognizing and treating body dysmorphic disorder. New York: Oxford University Press, 1996.
Drug brand names
- Citalopram • Celexa
- Clomipramine • Anafranil
- Doxepin • Sinequan
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Pimozide • Orap
- Sertraline • Zoloft
Disclosure
Dr. Grant reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Phillips receives research support from Eli Lilly and Co., Forest Pharmaceuticals, and Gate Pharmaceuticals; she is a speaker for or consultant to Eli Lilly and Co., Forest Pharmaceuticals, and UCB Pharma.
Lying in the hospital bed, her face covered in bandages, Ms. S talked of suicide while awaiting reconstructive surgery on her nose: “If the only way to stop is by killing myself, I will.” When asked what she wanted to stop, she replied, “The picking. I pick at my face all day, every day.”
Ms. S, age 22, had picked a hole through the bridge of her nose, and her face was scarred and covered with scabs. Every morning for 5 years, she had gotten up, dressed, and then—after washing her face—felt intense, uncontrollable urges to pick at her face. Hours would go by and she was still picking, even as her face started to bleed: “I try to resist, but I can’t.”
Ms. S started picking her face when she was 17. She missed so much of high school because of time spent picking that she did not graduate. She now lives alone on medical disability. Conscious of her facial scarring, she rarely goes out in public. “People stare at me as if I’m a zoo animal; it’s so painful,” she says.
After her plastic surgery, she told the staff psychiatrist she had never sought help because she thought no one would understand her behavior. “It doesn’t make sense to me, and I’ve lived with it for years.”
Patients such as Ms. S often suffer in isolation for years, unaware that skin picking is a psychiatric disorder that can be treated successfully. Some are referred to psychiatrists through hospital emergency rooms or by dermatologists; others commit suicide, as Ms. S threatened to do.
In our practice, we recognize skin picking in patients with comorbid mood and anxiety disorders, body dysmorphic disorder (BDD), substance use disorders, impulse control disorders such as trichotillomania or kleptomania, and personality disorders.
Based on recent evidence and our experience, we discuss three steps to help you diagnose pathologic skin picking. We then examine treatment options that have shown benefit for skinpicking patients, including habit reversal psychotherapy and medications.
WHAT IS SKIN PICKING?
Pathologic skin picking is repetitive, ritualistic, or impulsive picking of normal skin, leading to tissue damage, personal distress, and impaired functioning.1 The behavior has been described for more than 100 years but remains poorly understood, under-diagnosed, and under-treated.2,3
Most people pick at their hands or face to a limited extent,4 and picking does not by itself suggest a psychiatric disorder. Pathology exists in the focus, duration, and extent of the behavior, as well as reasons for picking, associated emotions, and resulting problems. Persons with pathologic skin picking report irresistible, intrusive, and/or senseless thoughts of picking or impulses to pick, accompanied by marked distress.1 Pathologic skin picking is recurrent and usually results in noticeable skin damage, although many patients try to camouflage the lesions or scarring with makeup.
Pathologic skin picking’s prevalence is unknown. One early study estimated that 2% of dermatology patients suffer from skin picking.1 Two clinical studies found that 3.8% of college students4 and 28% of patients with BDD meet diagnostic criteria.5,6
TWEEZERS, RAZOR BLADES, KNIVES…
Persons who engage in pathologic skin picking typically spend substantial time picking. Most often they pick the face, but any body part—lips, arms, hands, or legs—may be the focus. They may pick at blemishes, pimples, scars, or healthy skin. Some use their hands and fingernails to pick, and others use pins, tweezers, razor blades, or knives. Picking may worsen in the evening.2,7
Although picking episodes may last only a few minutes, many patients have multiple episodes each day. Some pick for as long as 12 hours every day,2,5 which often leads to scarring and disfigurement. In one study, 90% of patients had at least minor tissue damage, 61% suffered infections, and 45% had “deep craters” because of picking.2
Reasons for picking. Many patients pick to relieve discomfort or tension.1 Others pick to improve their appearance, as in BDD, or to remove perceived dirt or contaminants, as in obsessive-compulsive disorder (OCD).1,5 Still others say they pick as a habit, with minimal awareness.1 Itching or uneven skin may also cause the behavior.1,3 We have found that a patient may pick for several of these reasons. Most report:
- tension before picking
- satisfaction during picking
- guilt, shame, and dysphoria after picking.1
Social impairment. Shame after picking episodes often leads patients to cover lesions with clothing or makeup and to avoid social contact.7 Substantial social and occupational impairment have been reported3,5,7 because of the hours spent picking and from avoiding people because of disfigurement.
Physical injury. Skin picking may cause serious injuries. Some of our patients have required emergency medical intervention and sutures after picking through a major blood vessel (such as the facial artery). One woman—who picked at a pimple on her neck with tweezers—lacerated her carotid artery, causing a near-fatal hemorrhage that required emergency surgery.8
Suicide risk. In a series of 123 patients with BDD, 33 (27%) excessively picked their skin and 10 of those who picked their skin (33%) had attempted suicide.5 In a case series of 31 patients with skin picking, 10% had attempted suicide.2 We know of several young women whose chief complaint was skin picking and who committed suicide.5
Gender. The gender ratio of patients with skin picking remains unclear. In two case series that totaled 65 patients, 87% to 92% of those with pathologic skin picking were female.2,7 In the series of patients with BDD, 58% of the 33 who compulsively picked their skin were female.5 On the other hand, most of 28 patients seen in a dermatology clinic for neurotic excoriations were male.9
Onset and chronicity. Pathologic skin picking may develop at any age, but it usually manifests in late adolescence or early adulthood, often after onset of a dermatologic illness such as acne2 or in response to itching.3 Although long-term studies have not been done, the disorder appears to often be chronic, with waxing and waning of picking intensity and frequency.1,2
Table 1
Skin picking: 3 steps to diagnosis and treatment
| Step 1: Assess reasons for skin picking Dermatologic or medical disorder?
Psychiatric disorder?
Impulse control disorder, not otherwise specified? |
| Step 2: Assess picking severity Treat comorbid mood or anxiety disorders Treat skin picking if:
|
| Step 3: Provide recommended treatment For adults Habit reversal therapy plus medication is usually necessary For children and adolescents Habit reversal therapy alone for mild to moderate symptoms Habit reversal therapy plus medication for severe symptoms |
Comorbid psychopathology. In clinical settings, common comorbid psychopathologies include mood disorders (in 48% to 68% of patients with skin picking), anxiety disorders (41% to 64%), and alcohol use disorders (39%).2
In one patient sample, 71% of skin pickers met criteria for at least one personality disorder (48% had obsessive-compulsive personality disorder, and 26% met criteria for borderline personality disorder).2
Table 2
Medications with evidence of benefit for skin picking*
| Medication | Dosage | Type of evidence |
|---|---|---|
| SSRIs | ||
| Citalopram | 40 mg/d | Case report (effective only with inositol augmentation)16 |
| Fluoxetine | 20 to 80 mg/d | Case reports5,14-15 and two double-blind studies23-24 |
| Fluvoxamine | 100 to 300 mg/d | Case report,8 open-label study,21 and double-blind trial22 |
| Sertraline | 50 to 200 mg/d | Open-label study9 |
| Other agents | ||
| Clomipramine | 50 mg/d | Case report3 |
| Doxepin | 30 mg/d | Case report1 |
| Naltrexone | 50 mg/d | Case report20 |
| Olanzapine | 2.5 to 7.5 mg/d | Case report17 |
| Pimozide | 4 mg/d | Case report18 |
| * Off-label uses; little scientific evidence supports using medications other than SSRIs for treating skin picking. Inform patients of the evidence for using any medication, risk of side effects including change in cardiac conduction (pimozide, clomipramine), seizure risk (pimozide, clomipramine), and tardive dyskinesia (pimozide), and potential interactions with other medications (all of the above). | ||
PRIMARY VS. SECONDARY DISORDER
Is skin picking an independent disorder or a symptom of other psychiatric disorders? Although skin picking is not included in DSM-IV and has no formal diagnostic criteria, some forms of this behavior may belong among the impulse control disorders.
Patients often report an urge to pick their skin in response to increasing tension,1,3 and picking results in transient relief or pleasure.1,2 This description mirrors that of other impulse control disorders, such as trichotillomania and kleptomania. In fact, one study found that trichotillomania and kleptomania were common comorbidities among patients with skin picking (23% and 16%, respectively).2 In 34 patients with psychogenic excoriation, only 7 (21%) appeared to have skin picking as a primary complaint, unaccounted for by another psychiatric disorder.7
Skin picking may also be a symptom of other psychiatric disorders. To determine whether another disorder is present, we ask patients why they pick their skin. Patients may be reluctant to reveal either the picking or the underlying disorder because of embarrassment and shame. The diagnosis can often be clarified by asking about the following conditions:
Body dysmorphic disorder. Nearly 30% of patients with BDD pick their skin to a pathologic extent.5,6 The purpose of picking in BDD is to remove or minimize a nonexistent or slight imperfection in appearance (such as scars, pimples, bumps).5,6
Obsessive-compulsive disorder. Patients with OCD may pick their skin in response to contamination obsessions.1 Picking is often repetitive and ritualistic, and—as with compulsions—the behavior may reduce tension.10
Genetic disorders. Skin picking may be a symptom of Prader-Willi syndrome, a genetic disorder characterized by muscular hypotonia, short stature, characteristic facial features, intellectual disabilities, hypogonadism, hyperphagia, and an increased obesity risk. In one study, 97% of patients with Prader-Willi syndrome engaged in skin picking.11
Delusional disorder. Delusions of parasitosis may result in skin picking, as patients attempt to remove imagined parasites or other vermin from on or under their skin.12
Dermatitis artefacta. Patients may consciously create skin lesions to assume the sick role. Onethird of patients presenting to dermatologists with a disease that is primarily psychiatric may be suffering from dermatitis artefacta.13
TREATMENT RECOMMENDATIONS
Successful clinical care of pathologic skin picking requires perseverance and patience from both patient and clinician.
Treatment begins with a thorough dermatologic examination for medical causes of skin picking (such as atopic dermatitis or scabies) and to treat excoriations (such as with antibiotics for infection). After the dermatologist has ruled out a medical cause, carefully assess the patient’s picking behavior and related psychiatric problems (Table 1).
- If picking is secondary to a psychiatric disorder, begin by providing appropriate treatment for that disorder.
- If picking results from BDD or OCD, we recommend habit reversal therapy combined with medication.
- If picking appears to be an independent impulse control disorder, simultaneous habit reversal therapy and medication is usually necessary to reduce symptoms.
SSRIs are a reasonable first medication because of evidence for their efficacy in reducing skin picking. Higher dosages—comparable to those used in treating OCD—are usually required to improve skin-picking behavior. You may need to try another SSRI if the first trial results in partial or no response.
In our experience, augmenting an SSRI with naltrexone, 50 mg/d, helps reduce intrusive urges to pick and is worth considering if SSRI therapy results in only partial response.
Children or adolescents. Depending upon symptom severity, a trial of habit reversal therapy may be appropriate before you recommend using medication.
EVIDENCE FOR DRUG THERAPY
Although few treatment studies have been done, skin picking does appear to respond to medication (Table 2).
Because no medications are approved to treat skin-picking behavior, inform patients of any “off-label” uses and the scientific or clinical evidence for considering medication treatment.
Case reports and case series. Selective serotonin reuptake inhibitors (SSRIs) appear most effective in patients with picking behavior, including:
- fluvoxamine, 300 mg/d, in one case report8
- fluoxetine, 20 to 80 mg/d, in several case reports.5,14-15
In a series of 33 patients with BDD and compulsive skin picking, one-half (49%) of a variety of SSRI treatment trials improved BDD symptoms and skin picking behavior. The percentage of patients who improved was not examined. Dermatologic treatment alone was effective for only 15% of patients.5
Medications other than SSRIs have also been studied. One patient improved within 3 weeks of taking the tricyclic antidepressant clomipramine, 50 mg/d.3 Another patient picked her skin less often 4 weeks after inositol, 18 grams/d, was added to citalopram, 40 mg/d. Inositol, a nonprescription isomer of glucose, is a precursor in the phosphatidylinositol second-messenger cycle, which may play a role at certain serotonin receptors.16 The patient was given 6 grams dissolved in water three times daily.
Case reports have also suggested that olanzapine, pimozide, doxepin, and naltrexone may be beneficial in reducing skin excoriations. These reports often involved patients with psychiatric and medical comorbidities.17-20
Table 3
Habit reversal: 5 components in patient learning
| Awareness about picking behavior |
| Relaxation to reduce anxiety |
| Competing responses to learn behaviors incompatible with picking (such as fist clenching) |
| Rewarding oneself for successfully resisting picking |
| Generalizing the behavioral control |
Open-label studies. In an open-label study of 28 patients with neurotic excoriation treated in a dermatology clinic, 68% improved within 1 month with sertraline, mean dosage 95 mg/d.9 Similarly, open-label fluvoxamine, mean dosage 112.5 mg/d, was effective in reducing skin excoriation in 7 of 14 patients treated for 12 weeks in a psychiatric setting.21
Double-blind studies. In a double-blind study using fluvoxamine with supportive psychotherapy in patients with psychocutaneous disorders, all five patients with acne excoriee improved after 4 weeks of medication treatment (none was randomized to placebo).22
In a 10-week, double-blind study, 10 patients were assigned to fluoxetine, mean dosage 53.0 ± 16.4 mg/d, and 11 to placebo. A patient self-report visual analog scale showed that fluoxetine was significantly more effective than placebo in reducing picking behavior. Two other measures did not show significant improvement, however, perhaps because of the small sample size.23
In a third study, 8 of 15 patients responded to open-label fluoxetine, 20 to 60 mg/d after 6 weeks. The responders were then randomized to 6 additional weeks of fluoxetine or placebo. All four patients assigned to continue active medication maintained their improvement. Symptoms returned to baseline by week 12 in the four assigned to placebo.24
EVIDENCE FOR HABIT REVERSAL THERAPY
No controlled trials have examined psychosocial treatments for skin picking, but several psychotherapeutic interventions appear promising. Habit reversal has shown promise in three case reports totaling seven patients and appears to reduce picking behavior within a few weeks.25-27
In a case series, three patients were successfully treated with habit reversal (Table 3) and cognitive-behavioral techniques, consisting of:
- awareness training (using a skin-picking diary)
- competing response techniques (such as making a fist or squeezing a ball)
- emotion regulation skills
- psychoeducation
- cognitive restructuring (such as using Socratic questioning to produce rational alternatives) in situations that elicit the urge to pick.28
In another case series, 22 dermatology patients with skin picking received psychotherapy with insight-oriented and behavioral components. Therapy included attention to developmental issues and active conflicts, cognitive restructuring, and tools to manage aggression and social relations. Although treatment duration varied— the mean was weekly for 14 months—skin lesions healed in 17 patients (77%).29
Related resources
- Obsessive-Compulsive Foundation http://www.ocfoundation.org
- Koran LM. Obsessive-compulsive and related disorders in adults: A comprehensive clinical guide. Cambridge, UK: Cambridge University Press, 1999.
- Phillips KA. The broken mirror: Recognizing and treating body dysmorphic disorder. New York: Oxford University Press, 1996.
Drug brand names
- Citalopram • Celexa
- Clomipramine • Anafranil
- Doxepin • Sinequan
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Naltrexone • ReVia
- Olanzapine • Zyprexa
- Pimozide • Orap
- Sertraline • Zoloft
Disclosure
Dr. Grant reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Dr. Phillips receives research support from Eli Lilly and Co., Forest Pharmaceuticals, and Gate Pharmaceuticals; she is a speaker for or consultant to Eli Lilly and Co., Forest Pharmaceuticals, and UCB Pharma.
1. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 2001;15:351-9.
2. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry 1999;60:454-9.
3. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry 1986;27:381-6.
4. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skinpicking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics 2000;41:210-15.
5. Phillips KA, Taub SL. Skin picking as a symptom of body dysmorphic disorder. Psychopharmacol Bull 1995;31:279-88.
6. Phillips KA, Diaz S. Gender differences in body dysmorphic disorder. J Nerv Ment Dis 1997;185:570-7
7. Arnold LM, McElroy SL, Mutasim DF, et al. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry 1998;59:509-14.
8. O’Sullivan RL, Phillips KA, Keuthen NJ, Wilhelm S. Near fatal skin picking from delusional body dysmorphic disorder responsive to fluvoxamine. Psychosomatics 1999;40:79-81.
9. Kalivas J, Kalivas L, Gilman D, Hayden CT. Sertraline in the treatment of neurotic excoriations and related disorders [letter]. Arch Dermatol 1996;132:589-90.
10. Stein DJ, Hollander E. Dermatology and conditions related to obsessive-compulsive disorder. J Am Acad Dermatol 1992;26:237-42.
11. Dykens E, Shah B. Psychiatric disorders in Prader-Willi syndrome: epidemiology and management. CNS Drugs 2003;17:167-78.
12. Bishop ER. Monosymptomatic hypochondriacal syndromes in dermatology. J Am Acad Dermatol 1983;9:152-8.
13. Koblenzer CS. Dermatitis artefacta: clinical features and approaches to treatment. Am J Clin Dermatol 2000;1:47-55.
14. Stein DJ, Hutt CS, Spitz JL, Hollander E. Compulsive picking and obsessive-compulsive disorder. Psychosomatics 1993;34:177-80.
15. Stout RJ. Fluoxetine for the treatment of compulsive facial picking [letter]. Am J Psychiatry 1990;147:370.-
16. Seedat S, Stein DJ, Harvey BH. Inositol in the treatment of trichotillomania and compulsive skin picking [letter]. J Clin Psychiatry 2001;62:60-1.
17. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: three case reports. Cutis 2000;66:143-6.
18. Duke EE. Clinical experience with pimozide: emphasis on its use in postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
19. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol 1987;26:541-3.
20. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone [letter]. J Clin Psychopharmacol 1989;9:448-9.
21. Arnold LM, Mutasim DF, Dwight MM, et al. An open clinical trial of fluvoxamine treatment of psychogenic excoriation. J Clin Psychopharmacol 1999;19:15-18.
22. Hendrickx B, Van Moffaert M, Spiers R, Von Frenckell R. The treatment of psychocutaneous disorders: a new approach. Curr Ther Res Clin Exp 1991;49:111-19.
23. Simeon D, Stein DJ, Gross S, et al. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry 1997;58:341-7.
24. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 2001;42:314-19.
25. Kent A, Drummond LM. Acne excoriee—a case report of treatment using habit-reversal. Clin Exp Dermatol 1989;14:163-4.
26. Rosenbaum MS, Ayllon T. The behavioral treatment of neurodermatitis through habit-reversal. Behav Res Ther 1981;19:313-18.
27. Twohig MP, Woods DW. Habit reversal as a treatment for chronic skin picking in typically developing adult male siblings. J App Behav Analysis 2001;34:217-20.
28. Deckersbach T, Wilhelm S, Keuthen NJ, et al. Cognitive-behavior therapy for self-injurious skin picking. Behav Modif 2002;26:361-77.
29. Fruensgaard K. Psychotherapy and neurotic excoriations. Int J Dermatol 1991;30:262-5.
1. Arnold LM, Auchenbach MB, McElroy SL. Psychogenic excoriation: clinical features, proposed diagnostic criteria, epidemiology and approaches to treatment. CNS Drugs 2001;15:351-9.
2. Wilhelm S, Keuthen NJ, Deckersbach T, et al. Self-injurious skin picking: clinical characteristics and comorbidity. J Clin Psychiatry 1999;60:454-9.
3. Gupta MA, Gupta AK, Haberman HF. Neurotic excoriations: a review and some new perspectives. Compr Psychiatry 1986;27:381-6.
4. Keuthen NJ, Deckersbach T, Wilhelm S, et al. Repetitive skinpicking in a student population and comparison with a sample of self-injurious skin-pickers. Psychosomatics 2000;41:210-15.
5. Phillips KA, Taub SL. Skin picking as a symptom of body dysmorphic disorder. Psychopharmacol Bull 1995;31:279-88.
6. Phillips KA, Diaz S. Gender differences in body dysmorphic disorder. J Nerv Ment Dis 1997;185:570-7
7. Arnold LM, McElroy SL, Mutasim DF, et al. Characteristics of 34 adults with psychogenic excoriation. J Clin Psychiatry 1998;59:509-14.
8. O’Sullivan RL, Phillips KA, Keuthen NJ, Wilhelm S. Near fatal skin picking from delusional body dysmorphic disorder responsive to fluvoxamine. Psychosomatics 1999;40:79-81.
9. Kalivas J, Kalivas L, Gilman D, Hayden CT. Sertraline in the treatment of neurotic excoriations and related disorders [letter]. Arch Dermatol 1996;132:589-90.
10. Stein DJ, Hollander E. Dermatology and conditions related to obsessive-compulsive disorder. J Am Acad Dermatol 1992;26:237-42.
11. Dykens E, Shah B. Psychiatric disorders in Prader-Willi syndrome: epidemiology and management. CNS Drugs 2003;17:167-78.
12. Bishop ER. Monosymptomatic hypochondriacal syndromes in dermatology. J Am Acad Dermatol 1983;9:152-8.
13. Koblenzer CS. Dermatitis artefacta: clinical features and approaches to treatment. Am J Clin Dermatol 2000;1:47-55.
14. Stein DJ, Hutt CS, Spitz JL, Hollander E. Compulsive picking and obsessive-compulsive disorder. Psychosomatics 1993;34:177-80.
15. Stout RJ. Fluoxetine for the treatment of compulsive facial picking [letter]. Am J Psychiatry 1990;147:370.-
16. Seedat S, Stein DJ, Harvey BH. Inositol in the treatment of trichotillomania and compulsive skin picking [letter]. J Clin Psychiatry 2001;62:60-1.
17. Gupta MA, Gupta AK. Olanzapine is effective in the management of some self-induced dermatoses: three case reports. Cutis 2000;66:143-6.
18. Duke EE. Clinical experience with pimozide: emphasis on its use in postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
19. Harris BA, Sherertz EF, Flowers FP. Improvement of chronic neurotic excoriations with oral doxepin therapy. Int J Dermatol 1987;26:541-3.
20. Lienemann J, Walker FD. Reversal of self-abusive behavior with naltrexone [letter]. J Clin Psychopharmacol 1989;9:448-9.
21. Arnold LM, Mutasim DF, Dwight MM, et al. An open clinical trial of fluvoxamine treatment of psychogenic excoriation. J Clin Psychopharmacol 1999;19:15-18.
22. Hendrickx B, Van Moffaert M, Spiers R, Von Frenckell R. The treatment of psychocutaneous disorders: a new approach. Curr Ther Res Clin Exp 1991;49:111-19.
23. Simeon D, Stein DJ, Gross S, et al. A double-blind trial of fluoxetine in pathologic skin picking. J Clin Psychiatry 1997;58:341-7.
24. Bloch MR, Elliott M, Thompson H, Koran LM. Fluoxetine in pathologic skin-picking: open-label and double-blind results. Psychosomatics 2001;42:314-19.
25. Kent A, Drummond LM. Acne excoriee—a case report of treatment using habit-reversal. Clin Exp Dermatol 1989;14:163-4.
26. Rosenbaum MS, Ayllon T. The behavioral treatment of neurodermatitis through habit-reversal. Behav Res Ther 1981;19:313-18.
27. Twohig MP, Woods DW. Habit reversal as a treatment for chronic skin picking in typically developing adult male siblings. J App Behav Analysis 2001;34:217-20.
28. Deckersbach T, Wilhelm S, Keuthen NJ, et al. Cognitive-behavior therapy for self-injurious skin picking. Behav Modif 2002;26:361-77.
29. Fruensgaard K. Psychotherapy and neurotic excoriations. Int J Dermatol 1991;30:262-5.
‘I’m as ugly as the elephant man’: How to recognize and treat body dysmorphic disorder
A 52-year-old man becomes intoxicated with alcohol so he can lie in his backyard and get a tan. Convinced that his skin is too pale and that he looks “like a ghost,” he is so self-conscious about how he looks that he can’t go outside without drinking excessively.
An attractive 23-year-old woman dropped out of the 10th grade because of her “hideous” appearance and has hidden in her bedroom in her parents’ house ever since. She leaves her room no more than once a month, only after covering her face with a veil, not letting even her family see her face.
A middle-aged man cuts his nose open with a razor blade, trying to remove his nasal cartilage and replace it with chicken cartilage, in the desired shape.
These patients have body dysmorphic disorder (BDD), a somatoform disorder that the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) defines as a preoccupation with an imagined defect in appearance; if a slight physical anomaly is present, the person's concern is markedly excessive. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning that are not attributed to another mental disorder.
Most of us are dissatisfied with some aspect of how we look. In fact, more than half of all women and nearly half of all men in the United States are dissatisfied with their overall appearance.1 As the preceding cases illustrate, however, BDD does not consist simply of normal appearance concerns.
BDD is a relatively common disorder2 (Box 1) that occurs in children as well as adults. It usually begins during the early teenage years.2 BDD has been described around the world for more than a century.3 It causes notable distress and impaired functioning, and can lead to suicide.4 This disorder typically goes undiagnosed in clinical settings, however, in part because many patients are too embarrassed and ashamed to discuss their symptoms with their physicians unless specifically asked.2,5 BDD often masquerades as other psychiatric disorders, and misdiagnosis appears common6 (Table 1). Diagnosing BDD is usually straightforward, however, and can be achieved using the questions in Box 2.4 Clues to the presence of BDD are presented in Box 3; patients who present with any of them should be carefully evaluated for BDD.
- 1 in 8 psychiatric inpatients (13%)
- 1 in 7 to nearly half of outpatients with atypical major depression (14%-42%)
- 1 in 8 to 9 outpatients with social phobia (11%-13%)
- 1 in 3 to 12 outpatients with obsessive-compulsive disorder (8%-37%)
- 1 in 8 patients seeking dermatologic treatment (12%)
- 1 in 7 to 15 patients seeking cosmetic surgery (6%-15%)
- Nearly 1 in 100 to more than 1 in 50 people in the general population (0.7%-2.3%)
Perceptions of patients with BDD
Individuals with BDD obsess that there is something wrong with their appearance when in fact they look fine; the perceived flaw is actually minimal or nonexistent.7 Prior to treatment, insight is usually poor or absent, however, so that most patients are convinced or fairly certain that they look abnormal.2,8 They may describe the perceived flaw as unattractive or deformed, or they may even say that they look like a freak, a monster, or the “elephant man” (Box 4). Individuals with this disorder think about the perceived appearance flaws, on average, for 3 to 8 hours a day, and they usually find the thoughts difficult to resist or control.9 Diagnostic errors that cause BDD to be missed
Table 1
Diagnostic errors that cause BDD to be missed
| Misdiagnosis | Diagnostic error | How to avoid the error |
|---|---|---|
| Depression | The depressive symptoms that often coexist with BDD are diagnosed and BDD is missed; or BDD symptoms are considered a symptom of depression. In the author’s clinical experience, this is the most common diagnostic error. | Look for BDD in all depressed patients; appearance concerns may not be simply a symptom of depression. |
| Social phobia | Social anxiety is a common consequence of BDD, which may be misdiagnosed as social phobia or avoidant personality disorder. | Explore the cause of social anxiety or avoidance and determine whether it is secondary to BDD. |
| Agoraphobia | Many BDD patients are housebound at some point, which may be misdiagnosed as agoraphobia. | Explore the cause of avoidance and determine whether it is due to BDD. |
| OCD | BDD’s prominent obsessions and compulsive behaviors may be misdiagnosed as OCD. | If the obsessions and behaviors focus on physical appearance, BDD is the more accurate diagnosis. |
| Panic disorder | Panic attacks that occur when looking in the mirror or experiencing referential thinking can be misdiagnosed as panic disorder. | Determine whether panic attacks have BDD-related triggers; if so, BDD should be diagnosed. |
| Trichotillomania | Some BDD patients remove their body, head, or facial hair in an effort to improve their appearance, which may be misdiagnosed as trichotillomania. | Determine whether hair removal reflects thoughts that the hair does not look right and is intended to improve appearance; if so, the patient may have BDD. |
| Schizophrenia. | Because BDD beliefs are often delusional, and many patients have referential thinking, occasionally patients are misdiagnosed with Schizophrenia | If psychotic symptoms are largely limited to a nonbizarre delusional belief about one’s physical appearance and/or related delusions of reference, BDD is the more accurate diagnosis. |
Although repetitive behaviors are not part of BDD’s diagnostic criteria, virtually all patients perform such behaviors, usually in an attempt to improve, hide, examine, or be reassured about the perceived flaw.7,9 (See Box 3 for a partial listing.) These behaviors are usually time-consuming, occurring for many hours a day, and, like the preoccupations, are typically difficult to resist or control. With the exception of camouflaging, however, they often do not diminish appearance concerns. In fact, some of them (e.g., mirror checking) may actually increase anxiety about the perceived flaw.
Comorbidity is common in patients seen in clinical settings.2,8 Major depression is the most frequent comorbid disorder, which often appears secondary to BDD.10 Other common comorbidities include substance-use disorders, obsessive-compulsive disorder (OCD), social phobia, and personality disorders (most often, avoidant personality disorder).
Individuals with BDD are distressed over their appearance, many to the point of contemplating, attempting, or completing suicide.4,5 Nearly one quarter of patients seen in a clinical setting have attempted suicide.9 Although some patients appear to function reasonably well, they usually function below their capacity—for example, by avoiding social situations or meetings at work where others will see them. Others are completely incapacitated by their BDD symptoms, unable to work or socialize, and may be housebound for years.2,8,9 In a study that used the SF-36 to measure health-related quality of life, outpatients with BDD scored notably worse in all mental health domains than did the general U.S. population and patients with depression, type II diabetes, or a recent myocardial infarction.2
- Are you worried about your appearance in any way? If yes: What is your concern? OR Are you unhappy with how you look? If yes: What is your concern?
- Does this concern preoccupy you? That is, do you think about it a lot and wish you could worry about it less? OR If you add up all the time you spend each day thinking about your appearance, how much time would you estimate you spend?
- What effect has this preoccupation with your appearance had on your life? Has it:
BDD is diagnosed in patients who 1) are concerned about a minimal or nonexistent appearance flaw, 2) are preoccupied with the “flaw” (e.g., think about it for at least an hour a day), and 3) experience clinically significant distress or impairment in functioning as a result of their concern.

- Mirror checking or avoidance, or checking other reflective surfaces, such as windows, car bumpers, or the backs of spoons
- Reassurance seeking, that is, asking other people how they look or insisting that they look bad
- Skin picking, which may be manifested by skin lesions or scarring
- Excessive grooming, for example hair styling, applying makeup, shaving, tweezing hair, or cutting hair or wigs
- Camouflaging with a hat, toupee, makeup, sunglasses, clothes, or body position
- Excessive tanning, to darken “pale” skin
- Ideas or delusions of reference, thinking others take special notice of the “flaw” in a negative way (e.g., mock it or stare at it)
- Treatment-resistant anxiety, especially social anxiety, or depression
- Social avoidance or being housebound
- Unnecessary surgery, dermatologic treatment, or other nonpsychiatric treatment (e.g., electrolysis)
Guidelines for treating BDD
- Establish trust. It is important to convey that you take the patient’s appearance concerns seriously. Many patients with BDD fear being considered silly or vain and do not divulge their symptoms. It is usually best to avoid reassuring patients that they look fine, since they usually do not believe the reassurance and can interpret it as trivializing their concerns.
- Provide psychoeducation. Explain to patients that they have a relatively common and treatable body image disorder. To decrease the patient’s reluctance to accept the diagnosis and treatment, it can be helpful to emphasize the excessive preoccupation, distress, and other problems their symptoms are causing. Discussions about whether the defect is “real” are usually fruitless, unless the patient already has good insight, which is rare. Several educational books and Web sites for patients are available. See Related Resources.
- Target BDD symptoms in treatment. Ignoring BDD symptoms and focusing treatment on other symptoms only may be unsuccessful because effective treatment for BDD differs in some important ways from that of most other psychiatric disorders, such as depression.10 It appears, for example, that non-selective serotonin reuptake inhibitor (SSRI) antidepressants are generally ineffective for BDD, unless used at higher SSRI doses than are often needed for depression. BDD symptoms also do not necessarily improve in concert with symptoms of other disorders, such as depression or OCD.10
- Avoid nonpsychiatric medical treatment. Although no one can predict how an individual patient will respond to nonpsychiatric treatment, (e.g., surgery or dermatologic treatment), explain that as best we know, such treatment usually appears to be ineffective for BDD and even can make the symptoms worse.11
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’

Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
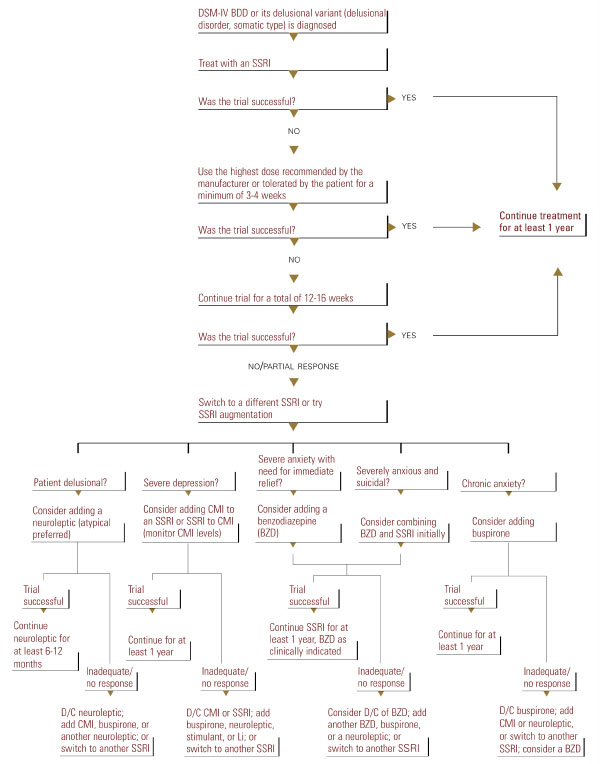
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).
- Treat for 12 to 16 weeks with an SSRI before concluding that the medication is ineffective. The average time to response is between 6 to 9 weeks.12,14,16 Clinical experience suggests that with continued treatment, relapse is rare and many patients further improve.
- Try sequential SSRIs if the first or second one does not work. A substantial percentage of patients who fail an initial SSRI trial will respond to a subsequent SSRI.17
- Continue an effective SSRI for at least 1 year before discontinuing it, as relapse appears likely with discontinuation.17 Severely ill patients may require treatment for life.
- Several SSRI augmentation and combination strategies might be helpful (Figure 1).16,17 If clomipramine is used in combination with an SSRI, the clomipramine level should be monitored.
What is the role of psychotherapy?
Although research on psychotherapy for BDD is limited, findings from clinical series and studies using waiting-list controls indicate that cognitive-behavioral therapy (CBT) is often effective.18-20 In contrast, supportive psychotherapy and insight-oriented and psychodynamic psychotherapy alone appear to be ineffective.9 CBT usually consists of a cognitive element (e.g., changing distorted views of the appearance “flaw”), exposure to feared and avoided situations (often social), and response prevention, avoiding repetitive behaviors such as excessive grooming.
- Consider using CBT as a first-line approach for milder BDD without significant comorbidity requiring pharmacotherapy.
- Use more intensive CBT treatment including frequent sessions and use of homework rather than less intensive treatment, although the optimal number and frequency of sessions is unknown.
- Consider maintenance and booster sessions for patients with more severe BDD following treatment to prevent relapse.
- Consider combining CBT and an SSRI. Although it is not known whether a combination of these treatments is more effective than either one alone, they are compatible and their combination may benefit certain patients. For patients with severe BDD, especially very depressed or suicidal patients, it is probably best to use CBT in combination with medication only, as sicker patients may not be able to tolerate or participate in CBT without first experiencing some improvement with medication.
- Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
- Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
- Phillips KA, Van Noppen B, Shapiro L. Learning to Live with Body Dysmorphic Disorder. Milford, Conn: Obsessive-Compulsive Foundation, 1997.
- Body Dysmorphic Disorder (BDD)and Body Image Program Homepage at Butler Hospital (Providence, RI). http://www.bodyimageprogram.com
Drug brand names
- Bupropion • Wellbutrin, Zyban
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Ativan, Diastat, Halcion
- Fluoxetine • Prozac, Sarafem
- Fluvoxamine • Luvox
- Mirtazapine • Remeron, Remeron Solitab
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The author reports that she receives grant support and occasional speaking honoraria from Eli Lilly and Co.; receives grant support from Forest Pharmaceuticals and Gate Pharmaceuticals; is on the speakers' bureau of Solvay Pharmaceuticals; and serves as a consultant for Wyeth-Ayerst Pharmaceuticals.
1. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
2. Phillips KA. Body dysmorphic disorder. In: Phillips KA, ed. Somatoform and Factitious Disorders. Washington DC: American Psychiatric Publishing, 2001.
3. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry. 1991;148:1138-1149.
4. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
5. Grant JE, et al. Prevalence and clinical features of body dysmorphic disorder in adolescent and adult psychiatric inpatients. J Clin Psychiatry. 2001;62:517-522.
6. Phillips KA. Body dysmorphic disorder: diagnostic controversies and treatment challenges. Bull Menninger Clin. 2000;64:18-35.
7. Hollander E, Cohen LJ, Simeon D. Body dysmorphic disorder. Psychiatric Annals. 1993;23:359-364.
8. Phillips KA, Castle DJ. Body dysmorphic disorder. In: Castle DJ, Phillips KA, eds. Disorders of Body Image. Hampshire, England: Wrightson Biomedical, in press.
9. Phillips KA, McElroy SL, Keck PE, Jr, Pope HG, Jr, Hudson JI. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry. 1993;150:302-308.
10. Phillips KA: Body dysmorphic disorder and depression: theoretical considerations and treatment strategies. Psychiatry Quart. 1999;70:313-331.
11. Phillips KA, Grant JD, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics, in press.
12. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry. 1998;59:165-171.
13. Hollander E, Allen A, Kwon J, Aronowitz B, Schmeidler J, Wong C, Simeon D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry. 1999;56:1033-1039.
14. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry, in press.
15. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: review of the evidence and a recommended treatment approach. CNS Spectrums, in press.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatric Clin North Am. 2000;7:59-82.
17. Phillips KA, Albertini RS, Siniscalchi J, Khan A, Robinson M. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry. 2001;721-727.
18. Neziroglu FA, Yaryura-Tobias JA. Exposure, response prevention, and cognitive therapy in the treatment of body dysmorphic disorder. Behav Ther. 1993;24:431-438.
19. Veale D, Gournay K, Dryden W, Boocock A, Shah F, Willson R, Walburn J. Body dysmorphic disorder: a cognitive behavioural model and pilot randomized controlled trial. Behav Res Therapeut. 1996;34:717-729.
20. Wilhelm S, Otto MW, Lohr B, Deckersback T. Cognitive behavior group therapy for body dysmorphic disorder: a case series. Behav Res Ther. 1999;37:71-75.
A 52-year-old man becomes intoxicated with alcohol so he can lie in his backyard and get a tan. Convinced that his skin is too pale and that he looks “like a ghost,” he is so self-conscious about how he looks that he can’t go outside without drinking excessively.
An attractive 23-year-old woman dropped out of the 10th grade because of her “hideous” appearance and has hidden in her bedroom in her parents’ house ever since. She leaves her room no more than once a month, only after covering her face with a veil, not letting even her family see her face.
A middle-aged man cuts his nose open with a razor blade, trying to remove his nasal cartilage and replace it with chicken cartilage, in the desired shape.
These patients have body dysmorphic disorder (BDD), a somatoform disorder that the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) defines as a preoccupation with an imagined defect in appearance; if a slight physical anomaly is present, the person's concern is markedly excessive. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning that are not attributed to another mental disorder.
Most of us are dissatisfied with some aspect of how we look. In fact, more than half of all women and nearly half of all men in the United States are dissatisfied with their overall appearance.1 As the preceding cases illustrate, however, BDD does not consist simply of normal appearance concerns.
BDD is a relatively common disorder2 (Box 1) that occurs in children as well as adults. It usually begins during the early teenage years.2 BDD has been described around the world for more than a century.3 It causes notable distress and impaired functioning, and can lead to suicide.4 This disorder typically goes undiagnosed in clinical settings, however, in part because many patients are too embarrassed and ashamed to discuss their symptoms with their physicians unless specifically asked.2,5 BDD often masquerades as other psychiatric disorders, and misdiagnosis appears common6 (Table 1). Diagnosing BDD is usually straightforward, however, and can be achieved using the questions in Box 2.4 Clues to the presence of BDD are presented in Box 3; patients who present with any of them should be carefully evaluated for BDD.
- 1 in 8 psychiatric inpatients (13%)
- 1 in 7 to nearly half of outpatients with atypical major depression (14%-42%)
- 1 in 8 to 9 outpatients with social phobia (11%-13%)
- 1 in 3 to 12 outpatients with obsessive-compulsive disorder (8%-37%)
- 1 in 8 patients seeking dermatologic treatment (12%)
- 1 in 7 to 15 patients seeking cosmetic surgery (6%-15%)
- Nearly 1 in 100 to more than 1 in 50 people in the general population (0.7%-2.3%)
Perceptions of patients with BDD
Individuals with BDD obsess that there is something wrong with their appearance when in fact they look fine; the perceived flaw is actually minimal or nonexistent.7 Prior to treatment, insight is usually poor or absent, however, so that most patients are convinced or fairly certain that they look abnormal.2,8 They may describe the perceived flaw as unattractive or deformed, or they may even say that they look like a freak, a monster, or the “elephant man” (Box 4). Individuals with this disorder think about the perceived appearance flaws, on average, for 3 to 8 hours a day, and they usually find the thoughts difficult to resist or control.9 Diagnostic errors that cause BDD to be missed
Table 1
Diagnostic errors that cause BDD to be missed
| Misdiagnosis | Diagnostic error | How to avoid the error |
|---|---|---|
| Depression | The depressive symptoms that often coexist with BDD are diagnosed and BDD is missed; or BDD symptoms are considered a symptom of depression. In the author’s clinical experience, this is the most common diagnostic error. | Look for BDD in all depressed patients; appearance concerns may not be simply a symptom of depression. |
| Social phobia | Social anxiety is a common consequence of BDD, which may be misdiagnosed as social phobia or avoidant personality disorder. | Explore the cause of social anxiety or avoidance and determine whether it is secondary to BDD. |
| Agoraphobia | Many BDD patients are housebound at some point, which may be misdiagnosed as agoraphobia. | Explore the cause of avoidance and determine whether it is due to BDD. |
| OCD | BDD’s prominent obsessions and compulsive behaviors may be misdiagnosed as OCD. | If the obsessions and behaviors focus on physical appearance, BDD is the more accurate diagnosis. |
| Panic disorder | Panic attacks that occur when looking in the mirror or experiencing referential thinking can be misdiagnosed as panic disorder. | Determine whether panic attacks have BDD-related triggers; if so, BDD should be diagnosed. |
| Trichotillomania | Some BDD patients remove their body, head, or facial hair in an effort to improve their appearance, which may be misdiagnosed as trichotillomania. | Determine whether hair removal reflects thoughts that the hair does not look right and is intended to improve appearance; if so, the patient may have BDD. |
| Schizophrenia. | Because BDD beliefs are often delusional, and many patients have referential thinking, occasionally patients are misdiagnosed with Schizophrenia | If psychotic symptoms are largely limited to a nonbizarre delusional belief about one’s physical appearance and/or related delusions of reference, BDD is the more accurate diagnosis. |
Although repetitive behaviors are not part of BDD’s diagnostic criteria, virtually all patients perform such behaviors, usually in an attempt to improve, hide, examine, or be reassured about the perceived flaw.7,9 (See Box 3 for a partial listing.) These behaviors are usually time-consuming, occurring for many hours a day, and, like the preoccupations, are typically difficult to resist or control. With the exception of camouflaging, however, they often do not diminish appearance concerns. In fact, some of them (e.g., mirror checking) may actually increase anxiety about the perceived flaw.
Comorbidity is common in patients seen in clinical settings.2,8 Major depression is the most frequent comorbid disorder, which often appears secondary to BDD.10 Other common comorbidities include substance-use disorders, obsessive-compulsive disorder (OCD), social phobia, and personality disorders (most often, avoidant personality disorder).
Individuals with BDD are distressed over their appearance, many to the point of contemplating, attempting, or completing suicide.4,5 Nearly one quarter of patients seen in a clinical setting have attempted suicide.9 Although some patients appear to function reasonably well, they usually function below their capacity—for example, by avoiding social situations or meetings at work where others will see them. Others are completely incapacitated by their BDD symptoms, unable to work or socialize, and may be housebound for years.2,8,9 In a study that used the SF-36 to measure health-related quality of life, outpatients with BDD scored notably worse in all mental health domains than did the general U.S. population and patients with depression, type II diabetes, or a recent myocardial infarction.2
- Are you worried about your appearance in any way? If yes: What is your concern? OR Are you unhappy with how you look? If yes: What is your concern?
- Does this concern preoccupy you? That is, do you think about it a lot and wish you could worry about it less? OR If you add up all the time you spend each day thinking about your appearance, how much time would you estimate you spend?
- What effect has this preoccupation with your appearance had on your life? Has it:
BDD is diagnosed in patients who 1) are concerned about a minimal or nonexistent appearance flaw, 2) are preoccupied with the “flaw” (e.g., think about it for at least an hour a day), and 3) experience clinically significant distress or impairment in functioning as a result of their concern.
- Mirror checking or avoidance, or checking other reflective surfaces, such as windows, car bumpers, or the backs of spoons
- Reassurance seeking, that is, asking other people how they look or insisting that they look bad
- Skin picking, which may be manifested by skin lesions or scarring
- Excessive grooming, for example hair styling, applying makeup, shaving, tweezing hair, or cutting hair or wigs
- Camouflaging with a hat, toupee, makeup, sunglasses, clothes, or body position
- Excessive tanning, to darken “pale” skin
- Ideas or delusions of reference, thinking others take special notice of the “flaw” in a negative way (e.g., mock it or stare at it)
- Treatment-resistant anxiety, especially social anxiety, or depression
- Social avoidance or being housebound
- Unnecessary surgery, dermatologic treatment, or other nonpsychiatric treatment (e.g., electrolysis)
Guidelines for treating BDD
- Establish trust. It is important to convey that you take the patient’s appearance concerns seriously. Many patients with BDD fear being considered silly or vain and do not divulge their symptoms. It is usually best to avoid reassuring patients that they look fine, since they usually do not believe the reassurance and can interpret it as trivializing their concerns.
- Provide psychoeducation. Explain to patients that they have a relatively common and treatable body image disorder. To decrease the patient’s reluctance to accept the diagnosis and treatment, it can be helpful to emphasize the excessive preoccupation, distress, and other problems their symptoms are causing. Discussions about whether the defect is “real” are usually fruitless, unless the patient already has good insight, which is rare. Several educational books and Web sites for patients are available. See Related Resources.
- Target BDD symptoms in treatment. Ignoring BDD symptoms and focusing treatment on other symptoms only may be unsuccessful because effective treatment for BDD differs in some important ways from that of most other psychiatric disorders, such as depression.10 It appears, for example, that non-selective serotonin reuptake inhibitor (SSRI) antidepressants are generally ineffective for BDD, unless used at higher SSRI doses than are often needed for depression. BDD symptoms also do not necessarily improve in concert with symptoms of other disorders, such as depression or OCD.10
- Avoid nonpsychiatric medical treatment. Although no one can predict how an individual patient will respond to nonpsychiatric treatment, (e.g., surgery or dermatologic treatment), explain that as best we know, such treatment usually appears to be ineffective for BDD and even can make the symptoms worse.11
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’
Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).
- Treat for 12 to 16 weeks with an SSRI before concluding that the medication is ineffective. The average time to response is between 6 to 9 weeks.12,14,16 Clinical experience suggests that with continued treatment, relapse is rare and many patients further improve.
- Try sequential SSRIs if the first or second one does not work. A substantial percentage of patients who fail an initial SSRI trial will respond to a subsequent SSRI.17
- Continue an effective SSRI for at least 1 year before discontinuing it, as relapse appears likely with discontinuation.17 Severely ill patients may require treatment for life.
- Several SSRI augmentation and combination strategies might be helpful (Figure 1).16,17 If clomipramine is used in combination with an SSRI, the clomipramine level should be monitored.
What is the role of psychotherapy?
Although research on psychotherapy for BDD is limited, findings from clinical series and studies using waiting-list controls indicate that cognitive-behavioral therapy (CBT) is often effective.18-20 In contrast, supportive psychotherapy and insight-oriented and psychodynamic psychotherapy alone appear to be ineffective.9 CBT usually consists of a cognitive element (e.g., changing distorted views of the appearance “flaw”), exposure to feared and avoided situations (often social), and response prevention, avoiding repetitive behaviors such as excessive grooming.
- Consider using CBT as a first-line approach for milder BDD without significant comorbidity requiring pharmacotherapy.
- Use more intensive CBT treatment including frequent sessions and use of homework rather than less intensive treatment, although the optimal number and frequency of sessions is unknown.
- Consider maintenance and booster sessions for patients with more severe BDD following treatment to prevent relapse.
- Consider combining CBT and an SSRI. Although it is not known whether a combination of these treatments is more effective than either one alone, they are compatible and their combination may benefit certain patients. For patients with severe BDD, especially very depressed or suicidal patients, it is probably best to use CBT in combination with medication only, as sicker patients may not be able to tolerate or participate in CBT without first experiencing some improvement with medication.
- Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
- Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
- Phillips KA, Van Noppen B, Shapiro L. Learning to Live with Body Dysmorphic Disorder. Milford, Conn: Obsessive-Compulsive Foundation, 1997.
- Body Dysmorphic Disorder (BDD)and Body Image Program Homepage at Butler Hospital (Providence, RI). http://www.bodyimageprogram.com
Drug brand names
- Bupropion • Wellbutrin, Zyban
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Ativan, Diastat, Halcion
- Fluoxetine • Prozac, Sarafem
- Fluvoxamine • Luvox
- Mirtazapine • Remeron, Remeron Solitab
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The author reports that she receives grant support and occasional speaking honoraria from Eli Lilly and Co.; receives grant support from Forest Pharmaceuticals and Gate Pharmaceuticals; is on the speakers' bureau of Solvay Pharmaceuticals; and serves as a consultant for Wyeth-Ayerst Pharmaceuticals.
A 52-year-old man becomes intoxicated with alcohol so he can lie in his backyard and get a tan. Convinced that his skin is too pale and that he looks “like a ghost,” he is so self-conscious about how he looks that he can’t go outside without drinking excessively.
An attractive 23-year-old woman dropped out of the 10th grade because of her “hideous” appearance and has hidden in her bedroom in her parents’ house ever since. She leaves her room no more than once a month, only after covering her face with a veil, not letting even her family see her face.
A middle-aged man cuts his nose open with a razor blade, trying to remove his nasal cartilage and replace it with chicken cartilage, in the desired shape.
These patients have body dysmorphic disorder (BDD), a somatoform disorder that the Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM-IV) defines as a preoccupation with an imagined defect in appearance; if a slight physical anomaly is present, the person's concern is markedly excessive. The preoccupation causes clinically significant distress or impairment in social, occupational, or other important areas of functioning that are not attributed to another mental disorder.
Most of us are dissatisfied with some aspect of how we look. In fact, more than half of all women and nearly half of all men in the United States are dissatisfied with their overall appearance.1 As the preceding cases illustrate, however, BDD does not consist simply of normal appearance concerns.
BDD is a relatively common disorder2 (Box 1) that occurs in children as well as adults. It usually begins during the early teenage years.2 BDD has been described around the world for more than a century.3 It causes notable distress and impaired functioning, and can lead to suicide.4 This disorder typically goes undiagnosed in clinical settings, however, in part because many patients are too embarrassed and ashamed to discuss their symptoms with their physicians unless specifically asked.2,5 BDD often masquerades as other psychiatric disorders, and misdiagnosis appears common6 (Table 1). Diagnosing BDD is usually straightforward, however, and can be achieved using the questions in Box 2.4 Clues to the presence of BDD are presented in Box 3; patients who present with any of them should be carefully evaluated for BDD.
- 1 in 8 psychiatric inpatients (13%)
- 1 in 7 to nearly half of outpatients with atypical major depression (14%-42%)
- 1 in 8 to 9 outpatients with social phobia (11%-13%)
- 1 in 3 to 12 outpatients with obsessive-compulsive disorder (8%-37%)
- 1 in 8 patients seeking dermatologic treatment (12%)
- 1 in 7 to 15 patients seeking cosmetic surgery (6%-15%)
- Nearly 1 in 100 to more than 1 in 50 people in the general population (0.7%-2.3%)
Perceptions of patients with BDD
Individuals with BDD obsess that there is something wrong with their appearance when in fact they look fine; the perceived flaw is actually minimal or nonexistent.7 Prior to treatment, insight is usually poor or absent, however, so that most patients are convinced or fairly certain that they look abnormal.2,8 They may describe the perceived flaw as unattractive or deformed, or they may even say that they look like a freak, a monster, or the “elephant man” (Box 4). Individuals with this disorder think about the perceived appearance flaws, on average, for 3 to 8 hours a day, and they usually find the thoughts difficult to resist or control.9 Diagnostic errors that cause BDD to be missed
Table 1
Diagnostic errors that cause BDD to be missed
| Misdiagnosis | Diagnostic error | How to avoid the error |
|---|---|---|
| Depression | The depressive symptoms that often coexist with BDD are diagnosed and BDD is missed; or BDD symptoms are considered a symptom of depression. In the author’s clinical experience, this is the most common diagnostic error. | Look for BDD in all depressed patients; appearance concerns may not be simply a symptom of depression. |
| Social phobia | Social anxiety is a common consequence of BDD, which may be misdiagnosed as social phobia or avoidant personality disorder. | Explore the cause of social anxiety or avoidance and determine whether it is secondary to BDD. |
| Agoraphobia | Many BDD patients are housebound at some point, which may be misdiagnosed as agoraphobia. | Explore the cause of avoidance and determine whether it is due to BDD. |
| OCD | BDD’s prominent obsessions and compulsive behaviors may be misdiagnosed as OCD. | If the obsessions and behaviors focus on physical appearance, BDD is the more accurate diagnosis. |
| Panic disorder | Panic attacks that occur when looking in the mirror or experiencing referential thinking can be misdiagnosed as panic disorder. | Determine whether panic attacks have BDD-related triggers; if so, BDD should be diagnosed. |
| Trichotillomania | Some BDD patients remove their body, head, or facial hair in an effort to improve their appearance, which may be misdiagnosed as trichotillomania. | Determine whether hair removal reflects thoughts that the hair does not look right and is intended to improve appearance; if so, the patient may have BDD. |
| Schizophrenia. | Because BDD beliefs are often delusional, and many patients have referential thinking, occasionally patients are misdiagnosed with Schizophrenia | If psychotic symptoms are largely limited to a nonbizarre delusional belief about one’s physical appearance and/or related delusions of reference, BDD is the more accurate diagnosis. |
Although repetitive behaviors are not part of BDD’s diagnostic criteria, virtually all patients perform such behaviors, usually in an attempt to improve, hide, examine, or be reassured about the perceived flaw.7,9 (See Box 3 for a partial listing.) These behaviors are usually time-consuming, occurring for many hours a day, and, like the preoccupations, are typically difficult to resist or control. With the exception of camouflaging, however, they often do not diminish appearance concerns. In fact, some of them (e.g., mirror checking) may actually increase anxiety about the perceived flaw.
Comorbidity is common in patients seen in clinical settings.2,8 Major depression is the most frequent comorbid disorder, which often appears secondary to BDD.10 Other common comorbidities include substance-use disorders, obsessive-compulsive disorder (OCD), social phobia, and personality disorders (most often, avoidant personality disorder).
Individuals with BDD are distressed over their appearance, many to the point of contemplating, attempting, or completing suicide.4,5 Nearly one quarter of patients seen in a clinical setting have attempted suicide.9 Although some patients appear to function reasonably well, they usually function below their capacity—for example, by avoiding social situations or meetings at work where others will see them. Others are completely incapacitated by their BDD symptoms, unable to work or socialize, and may be housebound for years.2,8,9 In a study that used the SF-36 to measure health-related quality of life, outpatients with BDD scored notably worse in all mental health domains than did the general U.S. population and patients with depression, type II diabetes, or a recent myocardial infarction.2
- Are you worried about your appearance in any way? If yes: What is your concern? OR Are you unhappy with how you look? If yes: What is your concern?
- Does this concern preoccupy you? That is, do you think about it a lot and wish you could worry about it less? OR If you add up all the time you spend each day thinking about your appearance, how much time would you estimate you spend?
- What effect has this preoccupation with your appearance had on your life? Has it:
BDD is diagnosed in patients who 1) are concerned about a minimal or nonexistent appearance flaw, 2) are preoccupied with the “flaw” (e.g., think about it for at least an hour a day), and 3) experience clinically significant distress or impairment in functioning as a result of their concern.
- Mirror checking or avoidance, or checking other reflective surfaces, such as windows, car bumpers, or the backs of spoons
- Reassurance seeking, that is, asking other people how they look or insisting that they look bad
- Skin picking, which may be manifested by skin lesions or scarring
- Excessive grooming, for example hair styling, applying makeup, shaving, tweezing hair, or cutting hair or wigs
- Camouflaging with a hat, toupee, makeup, sunglasses, clothes, or body position
- Excessive tanning, to darken “pale” skin
- Ideas or delusions of reference, thinking others take special notice of the “flaw” in a negative way (e.g., mock it or stare at it)
- Treatment-resistant anxiety, especially social anxiety, or depression
- Social avoidance or being housebound
- Unnecessary surgery, dermatologic treatment, or other nonpsychiatric treatment (e.g., electrolysis)
Guidelines for treating BDD
- Establish trust. It is important to convey that you take the patient’s appearance concerns seriously. Many patients with BDD fear being considered silly or vain and do not divulge their symptoms. It is usually best to avoid reassuring patients that they look fine, since they usually do not believe the reassurance and can interpret it as trivializing their concerns.
- Provide psychoeducation. Explain to patients that they have a relatively common and treatable body image disorder. To decrease the patient’s reluctance to accept the diagnosis and treatment, it can be helpful to emphasize the excessive preoccupation, distress, and other problems their symptoms are causing. Discussions about whether the defect is “real” are usually fruitless, unless the patient already has good insight, which is rare. Several educational books and Web sites for patients are available. See Related Resources.
- Target BDD symptoms in treatment. Ignoring BDD symptoms and focusing treatment on other symptoms only may be unsuccessful because effective treatment for BDD differs in some important ways from that of most other psychiatric disorders, such as depression.10 It appears, for example, that non-selective serotonin reuptake inhibitor (SSRI) antidepressants are generally ineffective for BDD, unless used at higher SSRI doses than are often needed for depression. BDD symptoms also do not necessarily improve in concert with symptoms of other disorders, such as depression or OCD.10
- Avoid nonpsychiatric medical treatment. Although no one can predict how an individual patient will respond to nonpsychiatric treatment, (e.g., surgery or dermatologic treatment), explain that as best we know, such treatment usually appears to be ineffective for BDD and even can make the symptoms worse.11
Which psychopharmaceuticals should you consider?
Although BDD’s response to pharmacotherapy has received far less investigation than that of many other psychiatric disorders, research on this treatment approach has dramatically increased in recent years. The following strategies are suggested on the basis of evidence from controlled studies, open-label trials, and the author’s clinical experience (Figure 1):2,6,8,12-17
‘I’m as ugly as the elephant man’
Chris is a shy, anxious-appearing, 31-year-old man who was hospitalized after attempting suicide. He wears a baseball cap pulled down over his forehead and partially covering his eyes. It is difficult for him to reveal the reason for his suicide attempt: “It’s really hard to talk about this. I don’t know if I can. It’s too embarrassing.” Then he adds, “Well I guess I should tell you—after all, I’m in the hospital because of it. It’s my nose—these huge pock marks on my nose. They’re grotesque! I look like a monster. I’m as ugly as the elephant man!
“These marks on my nose are all I can think about. I’ve thought about them for hours a day every day for the past 15 years. I even have nightmares about them. And I think that everyone can see them and that they laugh at me because of them. That’s why I wear this hat all the time. And that’s why I couldn’t talk to you in a bright room. You’d notice the marks and see how ugly I am.” Chris actually appeared entirely normal, but no one could convince him of this.
“This has affected me in a lot of ways,” Chris adds. “This may be hard for you to believe, but this problem has ruined my life. All I can think about is my face, and I spend hours a day looking at the marks in the mirror. I just can’t resist. I thought I looked so ugly that I started missing more and more work, and I stopped going out with my friends and my girlfriend. I got so anxious when people looked at me that I started staying in the house most of the time. Sometimes when I did go out, I went through red lights so I wouldn’t have to sit at the light, where people might be staring at me. The hat helped a little, but it didn’t cover all the marks. I tried covering them with makeup for a while, but I thought people could see the makeup so that didn’t really help. The only time I really felt comfortable is when I wore my nephew’s Batman mask on Halloween—then no one could see the marks.
I finally missed so much work that I was fired. My girlfriend stuck it out with me for a long time, but finally she couldn’t take it any more. One thing that was really hard for her was that I started asking her about 50 times a day whether I looked OK and whether she could see the marks—I think that was the final straw. If I had a choice, I’d rather have cancer. It must be less painful. This is like an arrow through my heart.”
Chris had a notable, although only partial, response to fluoxetine 100 mg/d and buspirone 60 mg/d (higher doses of fluoxetine and buspirone were tried but were not more effective). Adding clonazepam was helpful for severe anxiety. Clomipramine, venlafaxine, lithium, mirtazapine, and various antipsychotics were sequentially added to this regimen, with minimal success, although a second trial of olanzapine, at a higher dose (15 mg/d) than he had been willing to try previously, further decreased Chris’ BDD and depressive symptoms. The addition of bupropion was somewhat helpful for depression but not for BDD.
Figure 1 Proposed pharmacotherapy for treating BDD
- Use an SSRI as a first-line approach. Other medications, including other antidepressants, appear less effective than SSRIs or clomipramine.2,8,9,13,15 An SSRI or clomipramine is also recommended for patients with delusional BDD (those who are completely convinced that they look abnormal and cannot be convinced otherwise), as Proposed pharmacotherapy for treating BDD these patients appear to respond to SSRIs as well as nondelusional patients do.12-17
- Use the maximum recommended or tolerated SSRI dose if lower doses are ineffective. Although no studies have compared different SSRI dosages, BDD appears to often require higher doses than those that are typically used for depression.
In a chart-review study of 90 patients with BDD treated in the author’s clinical practice, the mean SSRI doses used were fluoxetine 66.7 ±23.5 mg/d, fluvoxamine 308.3 ±49.2 mg/d, paroxetine 55.0 ± 12.9 mg/d, sertraline 202.1 ± 45.8 mg/d, and clomipramine 203.3 ±52.5 mg/d.17 Some patients respond only to doses higher than the maximum recommended dose (for example, 80-100 mg/d of citalopram or paroxetine).
- Treat for 12 to 16 weeks with an SSRI before concluding that the medication is ineffective. The average time to response is between 6 to 9 weeks.12,14,16 Clinical experience suggests that with continued treatment, relapse is rare and many patients further improve.
- Try sequential SSRIs if the first or second one does not work. A substantial percentage of patients who fail an initial SSRI trial will respond to a subsequent SSRI.17
- Continue an effective SSRI for at least 1 year before discontinuing it, as relapse appears likely with discontinuation.17 Severely ill patients may require treatment for life.
- Several SSRI augmentation and combination strategies might be helpful (Figure 1).16,17 If clomipramine is used in combination with an SSRI, the clomipramine level should be monitored.
What is the role of psychotherapy?
Although research on psychotherapy for BDD is limited, findings from clinical series and studies using waiting-list controls indicate that cognitive-behavioral therapy (CBT) is often effective.18-20 In contrast, supportive psychotherapy and insight-oriented and psychodynamic psychotherapy alone appear to be ineffective.9 CBT usually consists of a cognitive element (e.g., changing distorted views of the appearance “flaw”), exposure to feared and avoided situations (often social), and response prevention, avoiding repetitive behaviors such as excessive grooming.
- Consider using CBT as a first-line approach for milder BDD without significant comorbidity requiring pharmacotherapy.
- Use more intensive CBT treatment including frequent sessions and use of homework rather than less intensive treatment, although the optimal number and frequency of sessions is unknown.
- Consider maintenance and booster sessions for patients with more severe BDD following treatment to prevent relapse.
- Consider combining CBT and an SSRI. Although it is not known whether a combination of these treatments is more effective than either one alone, they are compatible and their combination may benefit certain patients. For patients with severe BDD, especially very depressed or suicidal patients, it is probably best to use CBT in combination with medication only, as sicker patients may not be able to tolerate or participate in CBT without first experiencing some improvement with medication.
- Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
- Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
- Phillips KA, Van Noppen B, Shapiro L. Learning to Live with Body Dysmorphic Disorder. Milford, Conn: Obsessive-Compulsive Foundation, 1997.
- Body Dysmorphic Disorder (BDD)and Body Image Program Homepage at Butler Hospital (Providence, RI). http://www.bodyimageprogram.com
Drug brand names
- Bupropion • Wellbutrin, Zyban
- Buspirone • Buspar
- Citalopram • Celexa
- Clomipramine • Anafranil
- Clonazepam • Ativan, Diastat, Halcion
- Fluoxetine • Prozac, Sarafem
- Fluvoxamine • Luvox
- Mirtazapine • Remeron, Remeron Solitab
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The author reports that she receives grant support and occasional speaking honoraria from Eli Lilly and Co.; receives grant support from Forest Pharmaceuticals and Gate Pharmaceuticals; is on the speakers' bureau of Solvay Pharmaceuticals; and serves as a consultant for Wyeth-Ayerst Pharmaceuticals.
1. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
2. Phillips KA. Body dysmorphic disorder. In: Phillips KA, ed. Somatoform and Factitious Disorders. Washington DC: American Psychiatric Publishing, 2001.
3. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry. 1991;148:1138-1149.
4. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
5. Grant JE, et al. Prevalence and clinical features of body dysmorphic disorder in adolescent and adult psychiatric inpatients. J Clin Psychiatry. 2001;62:517-522.
6. Phillips KA. Body dysmorphic disorder: diagnostic controversies and treatment challenges. Bull Menninger Clin. 2000;64:18-35.
7. Hollander E, Cohen LJ, Simeon D. Body dysmorphic disorder. Psychiatric Annals. 1993;23:359-364.
8. Phillips KA, Castle DJ. Body dysmorphic disorder. In: Castle DJ, Phillips KA, eds. Disorders of Body Image. Hampshire, England: Wrightson Biomedical, in press.
9. Phillips KA, McElroy SL, Keck PE, Jr, Pope HG, Jr, Hudson JI. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry. 1993;150:302-308.
10. Phillips KA: Body dysmorphic disorder and depression: theoretical considerations and treatment strategies. Psychiatry Quart. 1999;70:313-331.
11. Phillips KA, Grant JD, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics, in press.
12. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry. 1998;59:165-171.
13. Hollander E, Allen A, Kwon J, Aronowitz B, Schmeidler J, Wong C, Simeon D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry. 1999;56:1033-1039.
14. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry, in press.
15. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: review of the evidence and a recommended treatment approach. CNS Spectrums, in press.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatric Clin North Am. 2000;7:59-82.
17. Phillips KA, Albertini RS, Siniscalchi J, Khan A, Robinson M. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry. 2001;721-727.
18. Neziroglu FA, Yaryura-Tobias JA. Exposure, response prevention, and cognitive therapy in the treatment of body dysmorphic disorder. Behav Ther. 1993;24:431-438.
19. Veale D, Gournay K, Dryden W, Boocock A, Shah F, Willson R, Walburn J. Body dysmorphic disorder: a cognitive behavioural model and pilot randomized controlled trial. Behav Res Therapeut. 1996;34:717-729.
20. Wilhelm S, Otto MW, Lohr B, Deckersback T. Cognitive behavior group therapy for body dysmorphic disorder: a case series. Behav Res Ther. 1999;37:71-75.
1. Pope HG, Phillips KA, Olivardia R. The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, NY: The Free Press, 2000.
2. Phillips KA. Body dysmorphic disorder. In: Phillips KA, ed. Somatoform and Factitious Disorders. Washington DC: American Psychiatric Publishing, 2001.
3. Phillips KA. Body dysmorphic disorder: the distress of imagined ugliness. Am J Psychiatry. 1991;148:1138-1149.
4. Phillips KA. The Broken Mirror: Understanding and Treating Body Dysmorphic Disorder. New York, NY: Oxford University Press, 1996.
5. Grant JE, et al. Prevalence and clinical features of body dysmorphic disorder in adolescent and adult psychiatric inpatients. J Clin Psychiatry. 2001;62:517-522.
6. Phillips KA. Body dysmorphic disorder: diagnostic controversies and treatment challenges. Bull Menninger Clin. 2000;64:18-35.
7. Hollander E, Cohen LJ, Simeon D. Body dysmorphic disorder. Psychiatric Annals. 1993;23:359-364.
8. Phillips KA, Castle DJ. Body dysmorphic disorder. In: Castle DJ, Phillips KA, eds. Disorders of Body Image. Hampshire, England: Wrightson Biomedical, in press.
9. Phillips KA, McElroy SL, Keck PE, Jr, Pope HG, Jr, Hudson JI. Body dysmorphic disorder: 30 cases of imagined ugliness. Am J Psychiatry. 1993;150:302-308.
10. Phillips KA: Body dysmorphic disorder and depression: theoretical considerations and treatment strategies. Psychiatry Quart. 1999;70:313-331.
11. Phillips KA, Grant JD, Siniscalchi J, Albertini RS. Surgical and nonpsychiatric medical treatment of patients with body dysmorphic disorder. Psychosomatics, in press.
12. Phillips KA, Dwight MM, McElroy SL. Efficacy and safety of fluvoxamine in body dysmorphic disorder. J Clin Psychiatry. 1998;59:165-171.
13. Hollander E, Allen A, Kwon J, Aronowitz B, Schmeidler J, Wong C, Simeon D. Clomipramine vs desipramine crossover trial in body dysmorphic disorder: selective efficacy of a serotonin reuptake inhibitor in imagined ugliness. Arch Gen Psychiatry. 1999;56:1033-1039.
14. Phillips KA, Albertini RS, Rasmussen SA. A randomized placebo-controlled trial of fluoxetine in body dysmorphic disorder. Arch Gen Psychiatry, in press.
15. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: review of the evidence and a recommended treatment approach. CNS Spectrums, in press.
16. Phillips KA. Pharmacologic treatment of body dysmorphic disorder: a review of empirical data and a proposed treatment algorithm. Psychiatric Clin North Am. 2000;7:59-82.
17. Phillips KA, Albertini RS, Siniscalchi J, Khan A, Robinson M. Effectiveness of pharmacotherapy for body dysmorphic disorder: a chart-review study. J Clin Psychiatry. 2001;721-727.
18. Neziroglu FA, Yaryura-Tobias JA. Exposure, response prevention, and cognitive therapy in the treatment of body dysmorphic disorder. Behav Ther. 1993;24:431-438.
19. Veale D, Gournay K, Dryden W, Boocock A, Shah F, Willson R, Walburn J. Body dysmorphic disorder: a cognitive behavioural model and pilot randomized controlled trial. Behav Res Therapeut. 1996;34:717-729.
20. Wilhelm S, Otto MW, Lohr B, Deckersback T. Cognitive behavior group therapy for body dysmorphic disorder: a case series. Behav Res Ther. 1999;37:71-75.