User login
Larry Beresford is an Oakland, Calif.-based freelance medical journalist with a breadth of experience writing about the policy, financial, clinical, management and human aspects of hospice, palliative care, end-of-life care, death, and dying. He is a longtime contributor to The Hospitalist, for which he covers re-admissions, pain management, palliative care, physician stress and burnout, quality improvement, waste prevention, practice management, innovation, and technology. He also contributes to Medscape. Learn more about his work at www.larryberesford.com; follow him on Twitter @larryberesford.
A Resting Place
When his hospital’s board of trustees was considering a palliative-care program seven years ago, hospitalist Stephen Bekanich, MD, wasn’t sure what to expect. What he did know was that his hospitalist group could provide the University of Utah Health System in Salt Lake City answers to staffing and financial issues surrounding the addition of a palliative-care service.

“They looked around and decided the hospitalist group would be the best place to house [the service], based on our experience with a range of medical management issues and the fact that we’re around 24 hours, seven days a week,” says Dr. Bekanich, who in 2006 became the first medical director of the palliative-care service at University of Utah Hospital.
The hospital board eventually selected palliative care as one of its annual projects, Dr. Bekanich says, not just because it was the right thing to do, but also because palliative care increasingly is used as a quality marker for hospitals. Dr. Bekanich says he took the assignment because it provides a nice buffer and change of pace from the stress of full-time HM service. Several colleagues joined him in rotating through palliative care coverage, although he continued to carry a pager most days and nights to support the physicians, advanced practice nurses, social worker, and chaplain with challenging cases.
After six months of operation, Dr. Bekanich went before his hospital board to discuss the program. He presented hospital data that showed the service had helped save the hospital $600,000, along with “thank-you letters” from grateful families and mentions in obituaries.
—Steven Pantilat, MD, SFHM, director, Univ, of California at San Francisco palliative care service, SHM past president
“A couple of months later, I realized that we needed another nurse practitioner to staff the growing caseload,” he explains. “I went to the chief medical officer and he said to me, ‘I don’t need to see the numbers. I know you’re doing a great job. Just tell me what you need.’ ”
Widely extolled for relieving the physical suffering and emotional distress of seriously ill patients, palliative care has seen rapid advancement in recent years, not only as a humanitarian impulse, but also as a legitimate and recognized medical subspecialty and career choice. Palliative care has its own board certification, fellowships, and training opportunities. For working hospitalists, this subspecialty can complement a career path and enhance job satisfaction. For HM groups, it represents diversification and an additional, albeit modest, income stream, as well as opportunities to improve the quality of hospital care.
“Palliative medicine is recognized by the American Board of Medical Specialties [ABMS] and nine of its medical specialty boards, which is very significant,” says Steven Pantilat, MD, SFHM, a hospitalist at the University of California at San Francisco (UCSF) Medical Center, medical director of UCSF’s palliative-care service. “Along with that come fellowships.”
The Basics
Palliative care’s focus is managing patients’ symptoms, maximizing quality of life, and clarifying treatment goals—regardless of diagnosis or other treatments they might be receiving. It is not hospice care, which is defined by Medicare as treatment for patients with a terminal prognosis of six months or less (see “Hospice and Palliative: End-of-Life Care Siblings,” p. 21). Palliative care and hospice care utilize many of the same techniques, and are combined in the ABMS program for certifying subspecialist physicians.
The interdisciplinary consultation service, where a palliative care consultant rounds with a team that might include physicians, nurses, social workers, pharmacists, and chaplains, is the most common palliative-care model in the hospital setting, but other approaches include dedicated units and community-based programs.
The latest data from the American Hospital Association (AHA) and the Center to Advance Palliative Care (CAPC) count 1,486 operational palliative-care programs in U.S. acute-care hospitals, more than twice as many as a decade before.1 Currently, the demand for physicians certified in hospice and palliative medicine outstrips the supply, which poses challenges to those trying to hire as well as bona fide opportunities for qualified physicians hoping to pursue their dream jobs in the field, says Dr. Pantilat, a past president of SHM.
“A few years ago, it was cutting-edge for hospitals to just have a palliative care program,” Dr. Pantilat says, “but now the focus is on quality and the qualifications of the palliative care physicians and other professionals. Expectations for what palliative care will deliver will only go up.”
UCSF’s palliative care service “lives” within its HM division. Five of the six palliative care attending physicians are hospitalists. They divide weeklong assignments on the service into seven-day commitments at the hospital; each shift includes an on-call pager for night coverage.
A palliative-care shift can be just as emotionally demanding as an HM shift, although usually with fewer patients. One big difference: More time is needed for each palliative care consult, Dr. Pantilat says. A typical consult consists of an intense conversation with the patient and family to explore the patient’s prognosis, family values, and goals for treatment and pain relief.
Additionally, palliative care physicians routinely discuss the psychosocial and spiritual distress that the patient and family normally encounter.
Know When to Call for Help
Hospitalist involvement in palliative care varies by service, individual experience, and institution guidelines. Generally, though, it starts with an understanding of what the service provides and determining when is the right time to call a palliative-care consultant for help (see “Your Page Is Welcomed,” p. 22).
Hospitalists can obtain basic training and incorporate palliative-care principles and practices into the care of all hospitalized patients (see “Training Opportunities,” p. 22). If your hospital has a palliative-care service, hospitalists could join an advisory committee or provide backup coverage. If no such service exists, hospitalists could advocate with other physicians and hospital administrators to start one, Dr. Pantilat says.
Some hospitalists go deeper, developing subspecialty expertise and board certification in palliative medicine.
For HM groups, integration with a palliative-care service could mean taking on medical management of the service. If your group chooses to go this route, experts suggest you research how busy the service could be and gauge the interest of physicians in your group. Also check on the willingness of hospitalists in the group who are not interested in working on the palliative care service; they could help free up time for those who want to do it.
What Every Hospitalist Should Know
The basic clinical skills needed to perform palliative medicine include:
- Titrating opioid analgesics;
- Using adjuvant pain medications;
- Managing nonpain-related symptoms, including nausea, vomiting, constipation, dyspnea, seizures, and anorexia;
- Managing delirium, anxiety, and depression;
- Communicating sensitive information;
- Working with cultural issues and differences; and
- Bereavement support for families.
“Every hospitalist should know how to elicit a patient’s goals of care and incorporate them into routine treatment, be fluid and comfortable discussing advance-care planning, and possess basic skills in pain management,” says Jeanie Youngwerth, MD, hospitalist and director of the palliative-care service at the University of Colorado Denver. “Unfortunately, we’re not there yet as a field, given current residency training in internal medicine. Our center has a hospitalist residency training track, and those residents all get dedicated, palliative care experience.”
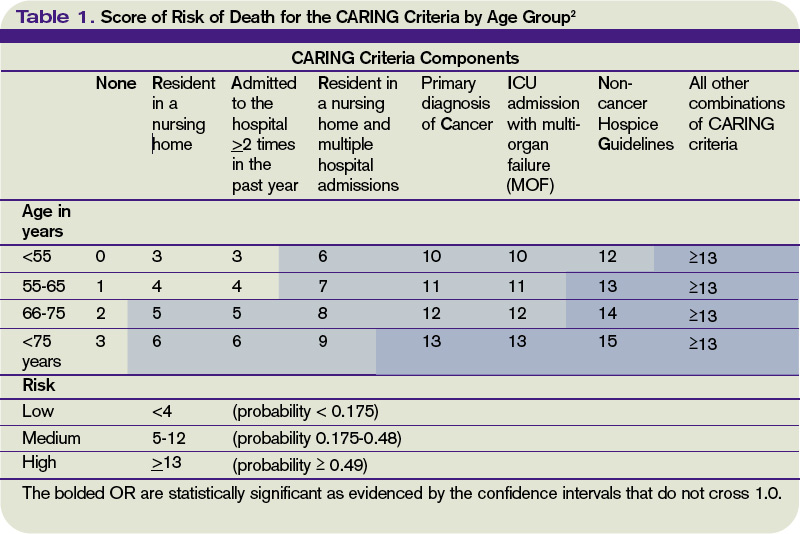
Knowing when to refer a patient to a palliative-care specialist is another important skill, Dr. Youngwerth explains. The CARING criteria, developed by Dr. Youngwerth’s colleagues at UC Denver, are a simple set of prognostic markers that identify patients with limited life expectancy at the time of hospital admission. The CARING criteria are a set of prognostic criteria that incorporate cancer diagnosis, repeated hospital admissions, ICU stays with multi-organ failure, residence in a nursing home, and meeting non-cancer hospice guidelines developed by the National Hospice Organization, which collectively correlate with the need for a palliative-care consultation (see Table 1, above).2
A simpler way to initially assess a patient’s need for palliative care is to ask yourself: Would you be surprised if you found out this patient had died within a year? “If physicians don’t think the patient is going to be alive in a year, then they should incorporate palliative care into the care plan,” Dr. Youngwerth says. “The next question is: Should I do it myself, or refer for a palliative-care consultation?”
Dr. Bekanich, who starting this month will head a new palliative care program at the University of Miami that features a 10-bed inpatient unit, encourages hospitalists to avoid focusing only on terminally ill patients when considering a palliative consult. Any seriously ill patient with unmet needs could benefit from a referral, he says.
“Lots of hospitalists are good at controlling nausea and vomiting, but if the symptoms are refractory or have uncommon presentations, I would like to get on board as the palliative care consultant,” Dr. Bekanich says. “I have also tried to emphasize to my group the importance of timely family meetings.
“If they don’t have the time or the skills, or if they expect a difficult meeting, for example, due to religious or cultural differences, send these patients our way. And when there are ethical issues that need to be addressed, or a particular need for educating patients and families about the disease process and what to expect, I like consultations like that.”
Bad Business or New Revenue Stream?
The traditional business model for palliative-care services has focused on the potential contributions to the hospital’s bottom line through reduced length of stay and cost avoidance for a group of patients who can be among the hospital’s most challenging and expensive. Palliative care saves time and money by working with patients and their families to clarify their values and treatment preferences, which routinely differ from standard treatment modes.
A recent multisite study of palliative care by Morrison et al found that the use of palliative care services saved from $1,700 to $4,900 per admission in direct costs, compared with similar patients who did not receive palliative care.3 The savings were realized primarily through reduced laboratory, pharmacy, and ICU costs.
Cost avoidance, combined with palliative care’s contributions to quality and patient satisfaction, is essential to the field’s growth. Even though physician consultation visits are billable, a palliative-care service rarely covers its staffing costs solely with billing revenue. A service requires nonbillable support from administration and midlevel providers, including nurses and social workers.
“Integrating palliative care into the work of hospitalists is a great idea,” says Jean Kutner, MD, head of the division of general internal medicine at the University of Colorado Denver. However, there are important issues related to scheduling, availability, and commitment that need to be explored before a group launches a new service. “I’d want to have discussions about how the palliative-care business model fits with our hospital medicine model and an agreement with the hospital on goals and metrics,” she says.
Hospitalists Fill a Need
Whether a full-fledged palliative-care service fits your group’s dynamic or not, hospitalists as a whole should be competent in basic palliative care. Community and rural hospitals need HM to bridge this gap and deliver quality care to seriously ill patients.

“I started at a community hospital, Eden Medical Center in Castro Valley, California. I had a personal interest in palliative care and realized there’s a tremendous need for it in community hospitals,” says Heather A. Harris, MD, a hospitalist at San Francisco General Hospital who previously worked with Dr. Pantilat’s palliative care service at UCSF. “We deal with end-of-life issues on a regular basis—whether recognized or not—based on our caseloads and requests for consultations.
“I got a little perspective about palliative care while a resident at UCSF. But as I’ve gotten further into this, I have come to realize that there is an actual skill set that needs to be learned to do it properly.”
Dr. Harris says there is a big difference between physicians helping patients with end-of-life issues the best they can and being part of a “dedicated, interdisciplinary team.”
“Palliative care is a wonderful opportunity for hospitalists,” she says. “It’s already part of your practice. Why not do it in a more organized fashion?” TH
Larry Beresford is a freelance medical writer based in Oakland, Calif.
References
- Palliative care programs continue rapid growth in U.S. hospitals. Center to Advance Palliative Care website. Available at: www.capc.org/news-and-events/releases/04-05-10. Accessed July 15, 2010.
- Fischer SM, Gozansky WS, Sauaia A, Min SJ, Kutner JS, Kramer A. A practical tool to identify patients who may benefit from a palliative approach: the CARING criteria. J Pain Symptom Manage. 2006;31(4):285-292.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
When his hospital’s board of trustees was considering a palliative-care program seven years ago, hospitalist Stephen Bekanich, MD, wasn’t sure what to expect. What he did know was that his hospitalist group could provide the University of Utah Health System in Salt Lake City answers to staffing and financial issues surrounding the addition of a palliative-care service.
“They looked around and decided the hospitalist group would be the best place to house [the service], based on our experience with a range of medical management issues and the fact that we’re around 24 hours, seven days a week,” says Dr. Bekanich, who in 2006 became the first medical director of the palliative-care service at University of Utah Hospital.
The hospital board eventually selected palliative care as one of its annual projects, Dr. Bekanich says, not just because it was the right thing to do, but also because palliative care increasingly is used as a quality marker for hospitals. Dr. Bekanich says he took the assignment because it provides a nice buffer and change of pace from the stress of full-time HM service. Several colleagues joined him in rotating through palliative care coverage, although he continued to carry a pager most days and nights to support the physicians, advanced practice nurses, social worker, and chaplain with challenging cases.
After six months of operation, Dr. Bekanich went before his hospital board to discuss the program. He presented hospital data that showed the service had helped save the hospital $600,000, along with “thank-you letters” from grateful families and mentions in obituaries.
—Steven Pantilat, MD, SFHM, director, Univ, of California at San Francisco palliative care service, SHM past president
“A couple of months later, I realized that we needed another nurse practitioner to staff the growing caseload,” he explains. “I went to the chief medical officer and he said to me, ‘I don’t need to see the numbers. I know you’re doing a great job. Just tell me what you need.’ ”
Widely extolled for relieving the physical suffering and emotional distress of seriously ill patients, palliative care has seen rapid advancement in recent years, not only as a humanitarian impulse, but also as a legitimate and recognized medical subspecialty and career choice. Palliative care has its own board certification, fellowships, and training opportunities. For working hospitalists, this subspecialty can complement a career path and enhance job satisfaction. For HM groups, it represents diversification and an additional, albeit modest, income stream, as well as opportunities to improve the quality of hospital care.
“Palliative medicine is recognized by the American Board of Medical Specialties [ABMS] and nine of its medical specialty boards, which is very significant,” says Steven Pantilat, MD, SFHM, a hospitalist at the University of California at San Francisco (UCSF) Medical Center, medical director of UCSF’s palliative-care service. “Along with that come fellowships.”
The Basics
Palliative care’s focus is managing patients’ symptoms, maximizing quality of life, and clarifying treatment goals—regardless of diagnosis or other treatments they might be receiving. It is not hospice care, which is defined by Medicare as treatment for patients with a terminal prognosis of six months or less (see “Hospice and Palliative: End-of-Life Care Siblings,” p. 21). Palliative care and hospice care utilize many of the same techniques, and are combined in the ABMS program for certifying subspecialist physicians.
The interdisciplinary consultation service, where a palliative care consultant rounds with a team that might include physicians, nurses, social workers, pharmacists, and chaplains, is the most common palliative-care model in the hospital setting, but other approaches include dedicated units and community-based programs.
The latest data from the American Hospital Association (AHA) and the Center to Advance Palliative Care (CAPC) count 1,486 operational palliative-care programs in U.S. acute-care hospitals, more than twice as many as a decade before.1 Currently, the demand for physicians certified in hospice and palliative medicine outstrips the supply, which poses challenges to those trying to hire as well as bona fide opportunities for qualified physicians hoping to pursue their dream jobs in the field, says Dr. Pantilat, a past president of SHM.
“A few years ago, it was cutting-edge for hospitals to just have a palliative care program,” Dr. Pantilat says, “but now the focus is on quality and the qualifications of the palliative care physicians and other professionals. Expectations for what palliative care will deliver will only go up.”
UCSF’s palliative care service “lives” within its HM division. Five of the six palliative care attending physicians are hospitalists. They divide weeklong assignments on the service into seven-day commitments at the hospital; each shift includes an on-call pager for night coverage.
A palliative-care shift can be just as emotionally demanding as an HM shift, although usually with fewer patients. One big difference: More time is needed for each palliative care consult, Dr. Pantilat says. A typical consult consists of an intense conversation with the patient and family to explore the patient’s prognosis, family values, and goals for treatment and pain relief.
Additionally, palliative care physicians routinely discuss the psychosocial and spiritual distress that the patient and family normally encounter.
Know When to Call for Help
Hospitalist involvement in palliative care varies by service, individual experience, and institution guidelines. Generally, though, it starts with an understanding of what the service provides and determining when is the right time to call a palliative-care consultant for help (see “Your Page Is Welcomed,” p. 22).
Hospitalists can obtain basic training and incorporate palliative-care principles and practices into the care of all hospitalized patients (see “Training Opportunities,” p. 22). If your hospital has a palliative-care service, hospitalists could join an advisory committee or provide backup coverage. If no such service exists, hospitalists could advocate with other physicians and hospital administrators to start one, Dr. Pantilat says.
Some hospitalists go deeper, developing subspecialty expertise and board certification in palliative medicine.
For HM groups, integration with a palliative-care service could mean taking on medical management of the service. If your group chooses to go this route, experts suggest you research how busy the service could be and gauge the interest of physicians in your group. Also check on the willingness of hospitalists in the group who are not interested in working on the palliative care service; they could help free up time for those who want to do it.
What Every Hospitalist Should Know
The basic clinical skills needed to perform palliative medicine include:
- Titrating opioid analgesics;
- Using adjuvant pain medications;
- Managing nonpain-related symptoms, including nausea, vomiting, constipation, dyspnea, seizures, and anorexia;
- Managing delirium, anxiety, and depression;
- Communicating sensitive information;
- Working with cultural issues and differences; and
- Bereavement support for families.
“Every hospitalist should know how to elicit a patient’s goals of care and incorporate them into routine treatment, be fluid and comfortable discussing advance-care planning, and possess basic skills in pain management,” says Jeanie Youngwerth, MD, hospitalist and director of the palliative-care service at the University of Colorado Denver. “Unfortunately, we’re not there yet as a field, given current residency training in internal medicine. Our center has a hospitalist residency training track, and those residents all get dedicated, palliative care experience.”
Knowing when to refer a patient to a palliative-care specialist is another important skill, Dr. Youngwerth explains. The CARING criteria, developed by Dr. Youngwerth’s colleagues at UC Denver, are a simple set of prognostic markers that identify patients with limited life expectancy at the time of hospital admission. The CARING criteria are a set of prognostic criteria that incorporate cancer diagnosis, repeated hospital admissions, ICU stays with multi-organ failure, residence in a nursing home, and meeting non-cancer hospice guidelines developed by the National Hospice Organization, which collectively correlate with the need for a palliative-care consultation (see Table 1, above).2
A simpler way to initially assess a patient’s need for palliative care is to ask yourself: Would you be surprised if you found out this patient had died within a year? “If physicians don’t think the patient is going to be alive in a year, then they should incorporate palliative care into the care plan,” Dr. Youngwerth says. “The next question is: Should I do it myself, or refer for a palliative-care consultation?”
Dr. Bekanich, who starting this month will head a new palliative care program at the University of Miami that features a 10-bed inpatient unit, encourages hospitalists to avoid focusing only on terminally ill patients when considering a palliative consult. Any seriously ill patient with unmet needs could benefit from a referral, he says.
“Lots of hospitalists are good at controlling nausea and vomiting, but if the symptoms are refractory or have uncommon presentations, I would like to get on board as the palliative care consultant,” Dr. Bekanich says. “I have also tried to emphasize to my group the importance of timely family meetings.
“If they don’t have the time or the skills, or if they expect a difficult meeting, for example, due to religious or cultural differences, send these patients our way. And when there are ethical issues that need to be addressed, or a particular need for educating patients and families about the disease process and what to expect, I like consultations like that.”
Bad Business or New Revenue Stream?
The traditional business model for palliative-care services has focused on the potential contributions to the hospital’s bottom line through reduced length of stay and cost avoidance for a group of patients who can be among the hospital’s most challenging and expensive. Palliative care saves time and money by working with patients and their families to clarify their values and treatment preferences, which routinely differ from standard treatment modes.
A recent multisite study of palliative care by Morrison et al found that the use of palliative care services saved from $1,700 to $4,900 per admission in direct costs, compared with similar patients who did not receive palliative care.3 The savings were realized primarily through reduced laboratory, pharmacy, and ICU costs.
Cost avoidance, combined with palliative care’s contributions to quality and patient satisfaction, is essential to the field’s growth. Even though physician consultation visits are billable, a palliative-care service rarely covers its staffing costs solely with billing revenue. A service requires nonbillable support from administration and midlevel providers, including nurses and social workers.
“Integrating palliative care into the work of hospitalists is a great idea,” says Jean Kutner, MD, head of the division of general internal medicine at the University of Colorado Denver. However, there are important issues related to scheduling, availability, and commitment that need to be explored before a group launches a new service. “I’d want to have discussions about how the palliative-care business model fits with our hospital medicine model and an agreement with the hospital on goals and metrics,” she says.
Hospitalists Fill a Need
Whether a full-fledged palliative-care service fits your group’s dynamic or not, hospitalists as a whole should be competent in basic palliative care. Community and rural hospitals need HM to bridge this gap and deliver quality care to seriously ill patients.
“I started at a community hospital, Eden Medical Center in Castro Valley, California. I had a personal interest in palliative care and realized there’s a tremendous need for it in community hospitals,” says Heather A. Harris, MD, a hospitalist at San Francisco General Hospital who previously worked with Dr. Pantilat’s palliative care service at UCSF. “We deal with end-of-life issues on a regular basis—whether recognized or not—based on our caseloads and requests for consultations.
“I got a little perspective about palliative care while a resident at UCSF. But as I’ve gotten further into this, I have come to realize that there is an actual skill set that needs to be learned to do it properly.”
Dr. Harris says there is a big difference between physicians helping patients with end-of-life issues the best they can and being part of a “dedicated, interdisciplinary team.”
“Palliative care is a wonderful opportunity for hospitalists,” she says. “It’s already part of your practice. Why not do it in a more organized fashion?” TH
Larry Beresford is a freelance medical writer based in Oakland, Calif.
References
- Palliative care programs continue rapid growth in U.S. hospitals. Center to Advance Palliative Care website. Available at: www.capc.org/news-and-events/releases/04-05-10. Accessed July 15, 2010.
- Fischer SM, Gozansky WS, Sauaia A, Min SJ, Kutner JS, Kramer A. A practical tool to identify patients who may benefit from a palliative approach: the CARING criteria. J Pain Symptom Manage. 2006;31(4):285-292.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
When his hospital’s board of trustees was considering a palliative-care program seven years ago, hospitalist Stephen Bekanich, MD, wasn’t sure what to expect. What he did know was that his hospitalist group could provide the University of Utah Health System in Salt Lake City answers to staffing and financial issues surrounding the addition of a palliative-care service.
“They looked around and decided the hospitalist group would be the best place to house [the service], based on our experience with a range of medical management issues and the fact that we’re around 24 hours, seven days a week,” says Dr. Bekanich, who in 2006 became the first medical director of the palliative-care service at University of Utah Hospital.
The hospital board eventually selected palliative care as one of its annual projects, Dr. Bekanich says, not just because it was the right thing to do, but also because palliative care increasingly is used as a quality marker for hospitals. Dr. Bekanich says he took the assignment because it provides a nice buffer and change of pace from the stress of full-time HM service. Several colleagues joined him in rotating through palliative care coverage, although he continued to carry a pager most days and nights to support the physicians, advanced practice nurses, social worker, and chaplain with challenging cases.
After six months of operation, Dr. Bekanich went before his hospital board to discuss the program. He presented hospital data that showed the service had helped save the hospital $600,000, along with “thank-you letters” from grateful families and mentions in obituaries.
—Steven Pantilat, MD, SFHM, director, Univ, of California at San Francisco palliative care service, SHM past president
“A couple of months later, I realized that we needed another nurse practitioner to staff the growing caseload,” he explains. “I went to the chief medical officer and he said to me, ‘I don’t need to see the numbers. I know you’re doing a great job. Just tell me what you need.’ ”
Widely extolled for relieving the physical suffering and emotional distress of seriously ill patients, palliative care has seen rapid advancement in recent years, not only as a humanitarian impulse, but also as a legitimate and recognized medical subspecialty and career choice. Palliative care has its own board certification, fellowships, and training opportunities. For working hospitalists, this subspecialty can complement a career path and enhance job satisfaction. For HM groups, it represents diversification and an additional, albeit modest, income stream, as well as opportunities to improve the quality of hospital care.
“Palliative medicine is recognized by the American Board of Medical Specialties [ABMS] and nine of its medical specialty boards, which is very significant,” says Steven Pantilat, MD, SFHM, a hospitalist at the University of California at San Francisco (UCSF) Medical Center, medical director of UCSF’s palliative-care service. “Along with that come fellowships.”
The Basics
Palliative care’s focus is managing patients’ symptoms, maximizing quality of life, and clarifying treatment goals—regardless of diagnosis or other treatments they might be receiving. It is not hospice care, which is defined by Medicare as treatment for patients with a terminal prognosis of six months or less (see “Hospice and Palliative: End-of-Life Care Siblings,” p. 21). Palliative care and hospice care utilize many of the same techniques, and are combined in the ABMS program for certifying subspecialist physicians.
The interdisciplinary consultation service, where a palliative care consultant rounds with a team that might include physicians, nurses, social workers, pharmacists, and chaplains, is the most common palliative-care model in the hospital setting, but other approaches include dedicated units and community-based programs.
The latest data from the American Hospital Association (AHA) and the Center to Advance Palliative Care (CAPC) count 1,486 operational palliative-care programs in U.S. acute-care hospitals, more than twice as many as a decade before.1 Currently, the demand for physicians certified in hospice and palliative medicine outstrips the supply, which poses challenges to those trying to hire as well as bona fide opportunities for qualified physicians hoping to pursue their dream jobs in the field, says Dr. Pantilat, a past president of SHM.
“A few years ago, it was cutting-edge for hospitals to just have a palliative care program,” Dr. Pantilat says, “but now the focus is on quality and the qualifications of the palliative care physicians and other professionals. Expectations for what palliative care will deliver will only go up.”
UCSF’s palliative care service “lives” within its HM division. Five of the six palliative care attending physicians are hospitalists. They divide weeklong assignments on the service into seven-day commitments at the hospital; each shift includes an on-call pager for night coverage.
A palliative-care shift can be just as emotionally demanding as an HM shift, although usually with fewer patients. One big difference: More time is needed for each palliative care consult, Dr. Pantilat says. A typical consult consists of an intense conversation with the patient and family to explore the patient’s prognosis, family values, and goals for treatment and pain relief.
Additionally, palliative care physicians routinely discuss the psychosocial and spiritual distress that the patient and family normally encounter.
Know When to Call for Help
Hospitalist involvement in palliative care varies by service, individual experience, and institution guidelines. Generally, though, it starts with an understanding of what the service provides and determining when is the right time to call a palliative-care consultant for help (see “Your Page Is Welcomed,” p. 22).
Hospitalists can obtain basic training and incorporate palliative-care principles and practices into the care of all hospitalized patients (see “Training Opportunities,” p. 22). If your hospital has a palliative-care service, hospitalists could join an advisory committee or provide backup coverage. If no such service exists, hospitalists could advocate with other physicians and hospital administrators to start one, Dr. Pantilat says.
Some hospitalists go deeper, developing subspecialty expertise and board certification in palliative medicine.
For HM groups, integration with a palliative-care service could mean taking on medical management of the service. If your group chooses to go this route, experts suggest you research how busy the service could be and gauge the interest of physicians in your group. Also check on the willingness of hospitalists in the group who are not interested in working on the palliative care service; they could help free up time for those who want to do it.
What Every Hospitalist Should Know
The basic clinical skills needed to perform palliative medicine include:
- Titrating opioid analgesics;
- Using adjuvant pain medications;
- Managing nonpain-related symptoms, including nausea, vomiting, constipation, dyspnea, seizures, and anorexia;
- Managing delirium, anxiety, and depression;
- Communicating sensitive information;
- Working with cultural issues and differences; and
- Bereavement support for families.
“Every hospitalist should know how to elicit a patient’s goals of care and incorporate them into routine treatment, be fluid and comfortable discussing advance-care planning, and possess basic skills in pain management,” says Jeanie Youngwerth, MD, hospitalist and director of the palliative-care service at the University of Colorado Denver. “Unfortunately, we’re not there yet as a field, given current residency training in internal medicine. Our center has a hospitalist residency training track, and those residents all get dedicated, palliative care experience.”
Knowing when to refer a patient to a palliative-care specialist is another important skill, Dr. Youngwerth explains. The CARING criteria, developed by Dr. Youngwerth’s colleagues at UC Denver, are a simple set of prognostic markers that identify patients with limited life expectancy at the time of hospital admission. The CARING criteria are a set of prognostic criteria that incorporate cancer diagnosis, repeated hospital admissions, ICU stays with multi-organ failure, residence in a nursing home, and meeting non-cancer hospice guidelines developed by the National Hospice Organization, which collectively correlate with the need for a palliative-care consultation (see Table 1, above).2
A simpler way to initially assess a patient’s need for palliative care is to ask yourself: Would you be surprised if you found out this patient had died within a year? “If physicians don’t think the patient is going to be alive in a year, then they should incorporate palliative care into the care plan,” Dr. Youngwerth says. “The next question is: Should I do it myself, or refer for a palliative-care consultation?”
Dr. Bekanich, who starting this month will head a new palliative care program at the University of Miami that features a 10-bed inpatient unit, encourages hospitalists to avoid focusing only on terminally ill patients when considering a palliative consult. Any seriously ill patient with unmet needs could benefit from a referral, he says.
“Lots of hospitalists are good at controlling nausea and vomiting, but if the symptoms are refractory or have uncommon presentations, I would like to get on board as the palliative care consultant,” Dr. Bekanich says. “I have also tried to emphasize to my group the importance of timely family meetings.
“If they don’t have the time or the skills, or if they expect a difficult meeting, for example, due to religious or cultural differences, send these patients our way. And when there are ethical issues that need to be addressed, or a particular need for educating patients and families about the disease process and what to expect, I like consultations like that.”
Bad Business or New Revenue Stream?
The traditional business model for palliative-care services has focused on the potential contributions to the hospital’s bottom line through reduced length of stay and cost avoidance for a group of patients who can be among the hospital’s most challenging and expensive. Palliative care saves time and money by working with patients and their families to clarify their values and treatment preferences, which routinely differ from standard treatment modes.
A recent multisite study of palliative care by Morrison et al found that the use of palliative care services saved from $1,700 to $4,900 per admission in direct costs, compared with similar patients who did not receive palliative care.3 The savings were realized primarily through reduced laboratory, pharmacy, and ICU costs.
Cost avoidance, combined with palliative care’s contributions to quality and patient satisfaction, is essential to the field’s growth. Even though physician consultation visits are billable, a palliative-care service rarely covers its staffing costs solely with billing revenue. A service requires nonbillable support from administration and midlevel providers, including nurses and social workers.
“Integrating palliative care into the work of hospitalists is a great idea,” says Jean Kutner, MD, head of the division of general internal medicine at the University of Colorado Denver. However, there are important issues related to scheduling, availability, and commitment that need to be explored before a group launches a new service. “I’d want to have discussions about how the palliative-care business model fits with our hospital medicine model and an agreement with the hospital on goals and metrics,” she says.
Hospitalists Fill a Need
Whether a full-fledged palliative-care service fits your group’s dynamic or not, hospitalists as a whole should be competent in basic palliative care. Community and rural hospitals need HM to bridge this gap and deliver quality care to seriously ill patients.
“I started at a community hospital, Eden Medical Center in Castro Valley, California. I had a personal interest in palliative care and realized there’s a tremendous need for it in community hospitals,” says Heather A. Harris, MD, a hospitalist at San Francisco General Hospital who previously worked with Dr. Pantilat’s palliative care service at UCSF. “We deal with end-of-life issues on a regular basis—whether recognized or not—based on our caseloads and requests for consultations.
“I got a little perspective about palliative care while a resident at UCSF. But as I’ve gotten further into this, I have come to realize that there is an actual skill set that needs to be learned to do it properly.”
Dr. Harris says there is a big difference between physicians helping patients with end-of-life issues the best they can and being part of a “dedicated, interdisciplinary team.”
“Palliative care is a wonderful opportunity for hospitalists,” she says. “It’s already part of your practice. Why not do it in a more organized fashion?” TH
Larry Beresford is a freelance medical writer based in Oakland, Calif.
References
- Palliative care programs continue rapid growth in U.S. hospitals. Center to Advance Palliative Care website. Available at: www.capc.org/news-and-events/releases/04-05-10. Accessed July 15, 2010.
- Fischer SM, Gozansky WS, Sauaia A, Min SJ, Kutner JS, Kramer A. A practical tool to identify patients who may benefit from a palliative approach: the CARING criteria. J Pain Symptom Manage. 2006;31(4):285-292.
- Morrison RS, Penrod JD, Cassel JB, et al. Cost savings associated with US hospital palliative care consultation programs. Arch Intern Med. 2008;168(16):1783-1790.
ONLINE EXCLUSIVE: Audio interviews with Project BOOST Michigan principals
Warm Welcome
Advocates for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) presented a standing-room-only policy briefing June 8 on Capitol Hill to explain an innovative quality-improvement (QI) initiative and new collaboration with Blue Cross Blue Shield of Michigan (BCBSM) to increase patient safety and reduce preventable hospital readmissions.
“The room was packed,” says David Share, MD, BCBSM’s executive medical director for healthcare quality. About 60 people were in attendance, mostly House and Senate legislative aides, along with a few representatives of third-party health organizations. Dr. Share, one of the presenters, says many of the staffers were well aware of the challenges of hospital-based practice. “I would say the crowd was remarkably attentive during our presentation,” he says.
SHM developed BOOST in 2008 to help hospitals and hospitalists systematically improve discharge processes through evidence-based interventions, management tools and resources, and expert mentoring. In January, BOOST was implemented in 15 Michigan hospitals with financial support from BCBSM. A 20-hospital partnership with the California HealthCare Foundation was announced in April, and more than 60 hospitals in 24 states now participate.
“These legislative staffers, who are responsible for crafting health-reform legislation, were given an in-depth understanding of how the provider community can take ownership of the challenges of transforming systems of care,” Dr. Share says. “I hope what they learned was that when payors … establish incentives for providers to transform healthcare systems, providers can do that very creatively and effectively in ways that affect patient care, patient well-being, and patient outcomes—both in terms of quality and cost.”
Hospitalist Scott Flanders, MD, SFHM, professor of medicine and director of the inpatient program at the University of Michigan in Ann Arbor, also spoke at the briefing. “I think our Michigan collaborative is a nice example of a local, provider-based, payor-supported quality initiative that will tackle an important problem and lead to a lot of collaboration and learning,” says Dr. Flanders, SHM’s immediate past president.
Also speaking at the briefing were Project BOOST principal investigator Mark Williams, MD, FHM, chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and representatives of the national Blue Cross/Blue Shield Association and the American Hospital Association, who discussed other initiatives that have successfully targeted the hospital readmission problem. “Not all readmissions are preventable. Some are necessary and important,” Dr. Flanders says, adding that the challenge is to distinguish between the necessary and the avoidable.
While there are no current legislative proposals involving Project BOOST, the initiative is aligned with a number of provisions aimed at reducing readmissions and improving care transitions, which are contained in the Patient Protection and Affordable Care Act passed in March. “Given the costs of readmissions, directly supporting demonstration projects like this would be a wise investment in improving healthcare quality,” says Dr. Flanders, adding that he heard suggestions at the briefing that the Centers for Medicare & Medicaid Services’ (CMS) Center for Innovation should consider supporting initiatives like BOOST.
Dr. Share, who calls payor support for the BOOST collaboration an example of its incentive programs with physician groups, says hospitalists are essential to partnerships with other providers, including PCPs, and the systems improvements necessary in the hospital setting.
“We’re actually bridging the gap between the hospital and the medical office,” he says. TH
Advocates for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) presented a standing-room-only policy briefing June 8 on Capitol Hill to explain an innovative quality-improvement (QI) initiative and new collaboration with Blue Cross Blue Shield of Michigan (BCBSM) to increase patient safety and reduce preventable hospital readmissions.
“The room was packed,” says David Share, MD, BCBSM’s executive medical director for healthcare quality. About 60 people were in attendance, mostly House and Senate legislative aides, along with a few representatives of third-party health organizations. Dr. Share, one of the presenters, says many of the staffers were well aware of the challenges of hospital-based practice. “I would say the crowd was remarkably attentive during our presentation,” he says.
SHM developed BOOST in 2008 to help hospitals and hospitalists systematically improve discharge processes through evidence-based interventions, management tools and resources, and expert mentoring. In January, BOOST was implemented in 15 Michigan hospitals with financial support from BCBSM. A 20-hospital partnership with the California HealthCare Foundation was announced in April, and more than 60 hospitals in 24 states now participate.
“These legislative staffers, who are responsible for crafting health-reform legislation, were given an in-depth understanding of how the provider community can take ownership of the challenges of transforming systems of care,” Dr. Share says. “I hope what they learned was that when payors … establish incentives for providers to transform healthcare systems, providers can do that very creatively and effectively in ways that affect patient care, patient well-being, and patient outcomes—both in terms of quality and cost.”
Hospitalist Scott Flanders, MD, SFHM, professor of medicine and director of the inpatient program at the University of Michigan in Ann Arbor, also spoke at the briefing. “I think our Michigan collaborative is a nice example of a local, provider-based, payor-supported quality initiative that will tackle an important problem and lead to a lot of collaboration and learning,” says Dr. Flanders, SHM’s immediate past president.
Also speaking at the briefing were Project BOOST principal investigator Mark Williams, MD, FHM, chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and representatives of the national Blue Cross/Blue Shield Association and the American Hospital Association, who discussed other initiatives that have successfully targeted the hospital readmission problem. “Not all readmissions are preventable. Some are necessary and important,” Dr. Flanders says, adding that the challenge is to distinguish between the necessary and the avoidable.
While there are no current legislative proposals involving Project BOOST, the initiative is aligned with a number of provisions aimed at reducing readmissions and improving care transitions, which are contained in the Patient Protection and Affordable Care Act passed in March. “Given the costs of readmissions, directly supporting demonstration projects like this would be a wise investment in improving healthcare quality,” says Dr. Flanders, adding that he heard suggestions at the briefing that the Centers for Medicare & Medicaid Services’ (CMS) Center for Innovation should consider supporting initiatives like BOOST.
Dr. Share, who calls payor support for the BOOST collaboration an example of its incentive programs with physician groups, says hospitalists are essential to partnerships with other providers, including PCPs, and the systems improvements necessary in the hospital setting.
“We’re actually bridging the gap between the hospital and the medical office,” he says. TH
Advocates for SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions) presented a standing-room-only policy briefing June 8 on Capitol Hill to explain an innovative quality-improvement (QI) initiative and new collaboration with Blue Cross Blue Shield of Michigan (BCBSM) to increase patient safety and reduce preventable hospital readmissions.
“The room was packed,” says David Share, MD, BCBSM’s executive medical director for healthcare quality. About 60 people were in attendance, mostly House and Senate legislative aides, along with a few representatives of third-party health organizations. Dr. Share, one of the presenters, says many of the staffers were well aware of the challenges of hospital-based practice. “I would say the crowd was remarkably attentive during our presentation,” he says.
SHM developed BOOST in 2008 to help hospitals and hospitalists systematically improve discharge processes through evidence-based interventions, management tools and resources, and expert mentoring. In January, BOOST was implemented in 15 Michigan hospitals with financial support from BCBSM. A 20-hospital partnership with the California HealthCare Foundation was announced in April, and more than 60 hospitals in 24 states now participate.
“These legislative staffers, who are responsible for crafting health-reform legislation, were given an in-depth understanding of how the provider community can take ownership of the challenges of transforming systems of care,” Dr. Share says. “I hope what they learned was that when payors … establish incentives for providers to transform healthcare systems, providers can do that very creatively and effectively in ways that affect patient care, patient well-being, and patient outcomes—both in terms of quality and cost.”
Hospitalist Scott Flanders, MD, SFHM, professor of medicine and director of the inpatient program at the University of Michigan in Ann Arbor, also spoke at the briefing. “I think our Michigan collaborative is a nice example of a local, provider-based, payor-supported quality initiative that will tackle an important problem and lead to a lot of collaboration and learning,” says Dr. Flanders, SHM’s immediate past president.
Also speaking at the briefing were Project BOOST principal investigator Mark Williams, MD, FHM, chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and representatives of the national Blue Cross/Blue Shield Association and the American Hospital Association, who discussed other initiatives that have successfully targeted the hospital readmission problem. “Not all readmissions are preventable. Some are necessary and important,” Dr. Flanders says, adding that the challenge is to distinguish between the necessary and the avoidable.
While there are no current legislative proposals involving Project BOOST, the initiative is aligned with a number of provisions aimed at reducing readmissions and improving care transitions, which are contained in the Patient Protection and Affordable Care Act passed in March. “Given the costs of readmissions, directly supporting demonstration projects like this would be a wise investment in improving healthcare quality,” says Dr. Flanders, adding that he heard suggestions at the briefing that the Centers for Medicare & Medicaid Services’ (CMS) Center for Innovation should consider supporting initiatives like BOOST.
Dr. Share, who calls payor support for the BOOST collaboration an example of its incentive programs with physician groups, says hospitalists are essential to partnerships with other providers, including PCPs, and the systems improvements necessary in the hospital setting.
“We’re actually bridging the gap between the hospital and the medical office,” he says. TH
ONLINE EXCLUSIVE: Palliative Care Documentation Key to Core Measures
A growing number of publicly reported hospital quality initiatives include severity-adjusted hospital mortality rates. Although individual hospitalists are unlikely to be rated based on their patients’ mortality, this is an important component of how hospitals are evaluated—and thus a natural target for the hospital’s quality-improvement (QI) efforts and for hospitalists’ participation in them.
The challenge is that some hospital-connected deaths are unavoidable, predictable, and even appropriate when care plans focused on maximizing comfort and quality of life replace medical efforts to stave off death. Referring seriously ill patients to the hospital’s palliative-care service or to a community hospice can influence a hospital’s mortality rate, but not always in the same ways.
Where hospice care and palliative care fit in hospital mortality rates, how they are defined and counted, and how predictable deaths are either included or excluded from hospitals’ risk-adjusted mortality tallies vary between the reporting programs, according to J. Brian Cassel, PhD, senior analyst at Virginia Commonwealth University (VCU), a presenter at the National Hospice and Palliative Care Organization’s Management and Leadership Conference in April 2010 in Washington, D.C.
“Hospitals are naturally concerned about mortality rates because they want to be seen as quality health providers,” Dr. Cassel says. “How hospital mortality rates are determined can be quite complex,” with varied data sources and various methods of adjusting for severity and balancing mortality with other quality metrics. Dr. Cassel says he began digging into mortality data when concerns were raised that VCU’s acute-palliative-care unit might be causing the medical center’s overall mortality rates to spike. His research found that the unit’s operation was probably neutral relative to VCU’s overall mortality rates.
Typically, the risk-adjusted mortality rate is for selected diagnoses but counts deaths from all causes, either during the index hospitalization or within 30 days of that admission, Dr. Cassel says. Three examples of QI programs that use mortality data: CMS’ Hospital Compare, which publicly reports data on patient satisfaction and hospital processes and outcomes, including mortality; U.S. News & World Report’s “Best Hospitals” list, for which one-third of total scores are derived from its mortality index; and HealthGrades, a Golden, Colo.-based company that ranks hospitals and other health providers within a region, one condition or procedure at a time.
An ICD-9 billing code, V66.7 for “palliative care encounter,” can flag the involvement of palliative-care consultants on a hospital case, although this code often goes unused and should be among the top nine listed diagnoses in order to turn up in most quality calculations. Palliative-care consultants can help promote the use and higher positioning of this code in hospital billing, along with more complete documentation of comorbidities and symptoms. It also is possible that involving hospice and palliative-care teams with seriously ill patients earlier in their disease progression could help manage their care in community settings, avoiding hospitalizations when death is likely in the next few months.
Some hospitals might choose to refer patients thought to be close to death to contracted hospice programs—and some hospice and palliative-care advocates are using the rates as conversation starters with hospital administrators. Dr. Cassel’s advice for those advocates: Know which quality-measurement systems the hospital’s leadership follows, where adjusted mortality rates fit in those systems, and how hospice and palliative care affect them.
Regardless of mortality metrics, Dr. Cassell says, a clinician’s primary responsibility is to provide the best possible care to patients and families, reflecting their values, hopes, and treatment goals.
A growing number of publicly reported hospital quality initiatives include severity-adjusted hospital mortality rates. Although individual hospitalists are unlikely to be rated based on their patients’ mortality, this is an important component of how hospitals are evaluated—and thus a natural target for the hospital’s quality-improvement (QI) efforts and for hospitalists’ participation in them.
The challenge is that some hospital-connected deaths are unavoidable, predictable, and even appropriate when care plans focused on maximizing comfort and quality of life replace medical efforts to stave off death. Referring seriously ill patients to the hospital’s palliative-care service or to a community hospice can influence a hospital’s mortality rate, but not always in the same ways.
Where hospice care and palliative care fit in hospital mortality rates, how they are defined and counted, and how predictable deaths are either included or excluded from hospitals’ risk-adjusted mortality tallies vary between the reporting programs, according to J. Brian Cassel, PhD, senior analyst at Virginia Commonwealth University (VCU), a presenter at the National Hospice and Palliative Care Organization’s Management and Leadership Conference in April 2010 in Washington, D.C.
“Hospitals are naturally concerned about mortality rates because they want to be seen as quality health providers,” Dr. Cassel says. “How hospital mortality rates are determined can be quite complex,” with varied data sources and various methods of adjusting for severity and balancing mortality with other quality metrics. Dr. Cassel says he began digging into mortality data when concerns were raised that VCU’s acute-palliative-care unit might be causing the medical center’s overall mortality rates to spike. His research found that the unit’s operation was probably neutral relative to VCU’s overall mortality rates.
Typically, the risk-adjusted mortality rate is for selected diagnoses but counts deaths from all causes, either during the index hospitalization or within 30 days of that admission, Dr. Cassel says. Three examples of QI programs that use mortality data: CMS’ Hospital Compare, which publicly reports data on patient satisfaction and hospital processes and outcomes, including mortality; U.S. News & World Report’s “Best Hospitals” list, for which one-third of total scores are derived from its mortality index; and HealthGrades, a Golden, Colo.-based company that ranks hospitals and other health providers within a region, one condition or procedure at a time.
An ICD-9 billing code, V66.7 for “palliative care encounter,” can flag the involvement of palliative-care consultants on a hospital case, although this code often goes unused and should be among the top nine listed diagnoses in order to turn up in most quality calculations. Palliative-care consultants can help promote the use and higher positioning of this code in hospital billing, along with more complete documentation of comorbidities and symptoms. It also is possible that involving hospice and palliative-care teams with seriously ill patients earlier in their disease progression could help manage their care in community settings, avoiding hospitalizations when death is likely in the next few months.
Some hospitals might choose to refer patients thought to be close to death to contracted hospice programs—and some hospice and palliative-care advocates are using the rates as conversation starters with hospital administrators. Dr. Cassel’s advice for those advocates: Know which quality-measurement systems the hospital’s leadership follows, where adjusted mortality rates fit in those systems, and how hospice and palliative care affect them.
Regardless of mortality metrics, Dr. Cassell says, a clinician’s primary responsibility is to provide the best possible care to patients and families, reflecting their values, hopes, and treatment goals.
A growing number of publicly reported hospital quality initiatives include severity-adjusted hospital mortality rates. Although individual hospitalists are unlikely to be rated based on their patients’ mortality, this is an important component of how hospitals are evaluated—and thus a natural target for the hospital’s quality-improvement (QI) efforts and for hospitalists’ participation in them.
The challenge is that some hospital-connected deaths are unavoidable, predictable, and even appropriate when care plans focused on maximizing comfort and quality of life replace medical efforts to stave off death. Referring seriously ill patients to the hospital’s palliative-care service or to a community hospice can influence a hospital’s mortality rate, but not always in the same ways.
Where hospice care and palliative care fit in hospital mortality rates, how they are defined and counted, and how predictable deaths are either included or excluded from hospitals’ risk-adjusted mortality tallies vary between the reporting programs, according to J. Brian Cassel, PhD, senior analyst at Virginia Commonwealth University (VCU), a presenter at the National Hospice and Palliative Care Organization’s Management and Leadership Conference in April 2010 in Washington, D.C.
“Hospitals are naturally concerned about mortality rates because they want to be seen as quality health providers,” Dr. Cassel says. “How hospital mortality rates are determined can be quite complex,” with varied data sources and various methods of adjusting for severity and balancing mortality with other quality metrics. Dr. Cassel says he began digging into mortality data when concerns were raised that VCU’s acute-palliative-care unit might be causing the medical center’s overall mortality rates to spike. His research found that the unit’s operation was probably neutral relative to VCU’s overall mortality rates.
Typically, the risk-adjusted mortality rate is for selected diagnoses but counts deaths from all causes, either during the index hospitalization or within 30 days of that admission, Dr. Cassel says. Three examples of QI programs that use mortality data: CMS’ Hospital Compare, which publicly reports data on patient satisfaction and hospital processes and outcomes, including mortality; U.S. News & World Report’s “Best Hospitals” list, for which one-third of total scores are derived from its mortality index; and HealthGrades, a Golden, Colo.-based company that ranks hospitals and other health providers within a region, one condition or procedure at a time.
An ICD-9 billing code, V66.7 for “palliative care encounter,” can flag the involvement of palliative-care consultants on a hospital case, although this code often goes unused and should be among the top nine listed diagnoses in order to turn up in most quality calculations. Palliative-care consultants can help promote the use and higher positioning of this code in hospital billing, along with more complete documentation of comorbidities and symptoms. It also is possible that involving hospice and palliative-care teams with seriously ill patients earlier in their disease progression could help manage their care in community settings, avoiding hospitalizations when death is likely in the next few months.
Some hospitals might choose to refer patients thought to be close to death to contracted hospice programs—and some hospice and palliative-care advocates are using the rates as conversation starters with hospital administrators. Dr. Cassel’s advice for those advocates: Know which quality-measurement systems the hospital’s leadership follows, where adjusted mortality rates fit in those systems, and how hospice and palliative care affect them.
Regardless of mortality metrics, Dr. Cassell says, a clinician’s primary responsibility is to provide the best possible care to patients and families, reflecting their values, hopes, and treatment goals.
ONLINE EXCLUSIVE: Audio interview with a pediatric hospitalist who is starting a palliative care team
Handoffs Smoother in Rural Communities
Before Matthew Schreiber, MD, became chief medical officer of Piedmont Hospital in Atlanta, he was director of hospitalist services for the four-hospital Piedmont health system, and before that, a hospitalist for the system’s smallest hospital, 35-bed Piedmont Mountainside in Jasper, Ga., population 2,000, so he knows just how different transitions of care are between hospitals large and small.
In many rural communities, the hospitalist concept has only recently been introduced, and patients are accustomed to PCPs being responsible for all of their medical care. But it can be easier to achieve high-quality handoffs in rural areas because the number of physicians involved is much smaller, Dr. Schreiber says.
“At Piedmont Mountainside, only eight physicians made most of our referrals. It was possible to memorize their office numbers and their call-coverage arrangements,” he explains. Some doctors are accessible 24 hours, seven days a week, while others take their patients’ charts home overnight in case they get called. This encourages an individualized approach to communicating with them. “It makes the care feel more personal, with a different level of accountability,” Dr. Schreiber says. “You feel a connection to the patient and the doctor—and that your job isn’t done when the patient goes home.”
Rural hospitals and doctors also tend to have closer relationships with community services like home health agencies. “We can give the medication list to the home health nurse and say, ‘This is what we think the patient is taking. We want you to go in and find out what they’re actually taking and reconcile the two,’ ” Dr. Schreiber says.
However, small and rural hospitals—particularly stand-alone and critical access facilities—are less likely to have computerized tools for automating and facilitating care transitions, Dr. Schreiber says. In some cases, the rural hospitalist carries a pager and takes calls 24/7.
Dr. Schreiber says it’s important to hand patients a piece of paper that summarizes their condition, key events in the hospitalization, and new medications, all in patient-friendly language, to take home and post on the refrigerator. “In our experience, patients hold onto this document and bring it to the doctor’s office or even to the emergency room,” he says, adding that if the formal discharge summary doesn’t reach the PCP in time, this summary could be a godsend.
Visit our website for more information about local and national efforts to improve care transitions.
Check out the SHM website for information on Project BOOST (Better Outcomes for Older Adults through Safer Transitions), a national QI initiative to improve handoffs and transitions.
Before Matthew Schreiber, MD, became chief medical officer of Piedmont Hospital in Atlanta, he was director of hospitalist services for the four-hospital Piedmont health system, and before that, a hospitalist for the system’s smallest hospital, 35-bed Piedmont Mountainside in Jasper, Ga., population 2,000, so he knows just how different transitions of care are between hospitals large and small.
In many rural communities, the hospitalist concept has only recently been introduced, and patients are accustomed to PCPs being responsible for all of their medical care. But it can be easier to achieve high-quality handoffs in rural areas because the number of physicians involved is much smaller, Dr. Schreiber says.
“At Piedmont Mountainside, only eight physicians made most of our referrals. It was possible to memorize their office numbers and their call-coverage arrangements,” he explains. Some doctors are accessible 24 hours, seven days a week, while others take their patients’ charts home overnight in case they get called. This encourages an individualized approach to communicating with them. “It makes the care feel more personal, with a different level of accountability,” Dr. Schreiber says. “You feel a connection to the patient and the doctor—and that your job isn’t done when the patient goes home.”
Rural hospitals and doctors also tend to have closer relationships with community services like home health agencies. “We can give the medication list to the home health nurse and say, ‘This is what we think the patient is taking. We want you to go in and find out what they’re actually taking and reconcile the two,’ ” Dr. Schreiber says.
However, small and rural hospitals—particularly stand-alone and critical access facilities—are less likely to have computerized tools for automating and facilitating care transitions, Dr. Schreiber says. In some cases, the rural hospitalist carries a pager and takes calls 24/7.
Dr. Schreiber says it’s important to hand patients a piece of paper that summarizes their condition, key events in the hospitalization, and new medications, all in patient-friendly language, to take home and post on the refrigerator. “In our experience, patients hold onto this document and bring it to the doctor’s office or even to the emergency room,” he says, adding that if the formal discharge summary doesn’t reach the PCP in time, this summary could be a godsend.
Visit our website for more information about local and national efforts to improve care transitions.
Check out the SHM website for information on Project BOOST (Better Outcomes for Older Adults through Safer Transitions), a national QI initiative to improve handoffs and transitions.
Before Matthew Schreiber, MD, became chief medical officer of Piedmont Hospital in Atlanta, he was director of hospitalist services for the four-hospital Piedmont health system, and before that, a hospitalist for the system’s smallest hospital, 35-bed Piedmont Mountainside in Jasper, Ga., population 2,000, so he knows just how different transitions of care are between hospitals large and small.
In many rural communities, the hospitalist concept has only recently been introduced, and patients are accustomed to PCPs being responsible for all of their medical care. But it can be easier to achieve high-quality handoffs in rural areas because the number of physicians involved is much smaller, Dr. Schreiber says.
“At Piedmont Mountainside, only eight physicians made most of our referrals. It was possible to memorize their office numbers and their call-coverage arrangements,” he explains. Some doctors are accessible 24 hours, seven days a week, while others take their patients’ charts home overnight in case they get called. This encourages an individualized approach to communicating with them. “It makes the care feel more personal, with a different level of accountability,” Dr. Schreiber says. “You feel a connection to the patient and the doctor—and that your job isn’t done when the patient goes home.”
Rural hospitals and doctors also tend to have closer relationships with community services like home health agencies. “We can give the medication list to the home health nurse and say, ‘This is what we think the patient is taking. We want you to go in and find out what they’re actually taking and reconcile the two,’ ” Dr. Schreiber says.
However, small and rural hospitals—particularly stand-alone and critical access facilities—are less likely to have computerized tools for automating and facilitating care transitions, Dr. Schreiber says. In some cases, the rural hospitalist carries a pager and takes calls 24/7.
Dr. Schreiber says it’s important to hand patients a piece of paper that summarizes their condition, key events in the hospitalization, and new medications, all in patient-friendly language, to take home and post on the refrigerator. “In our experience, patients hold onto this document and bring it to the doctor’s office or even to the emergency room,” he says, adding that if the formal discharge summary doesn’t reach the PCP in time, this summary could be a godsend.
Visit our website for more information about local and national efforts to improve care transitions.
Check out the SHM website for information on Project BOOST (Better Outcomes for Older Adults through Safer Transitions), a national QI initiative to improve handoffs and transitions.
Change You Should Believe In
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2

—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.

“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.

—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”

Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions

Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?

SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups

One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2
—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.
“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.
—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”
Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions
Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?
SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups
One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
Christina Payne, MD, is a third-year resident at Emory University Hospital in Atlanta who will begin her first hospitalist job, with Emory in September. In spite of her dearth of practical experience, she already has experience researching one of the most vexing problems confronting HM: how to improve transitions of care.
Dr. Payne has been studying the benefits of a structured electronic tool that generates a standardized sign-out list of a hospital team’s full census at the time of shift change, compared with the usual, highly variable sign-out practices of medical residents. At a poster presentation at Internal Medicine 2010 in April in Toronto, Dr. Payne and colleagues reported that residents using the tool were twice as confident at performing handoffs, had lower rates of perceived near-miss events, and were happier.1
“Hospitalists everywhere are starting to realize the importance of trying to reduce opportunities for human error that occur during care transitions,” Dr. Payne says. “The biggest thing I learned from this research is the importance of standardizing the handoff process [with information communicated consistently].
“It is essential to keep communication lines open,” Dr. Payne adds. “No tool can replace the importance of communication between doctors and the need to sit down and talk. The ideal signout happens in a quiet room where the two of you can talk about active patients and achieve rapport. But, realistically, how often does that happen?”
Standardization is one of a handful of strategies hospitalists, researchers, and policymakers are using to tackle transitions—both in-hospital handoffs and post-discharge transitions—with outpatient care. Some hospitalists are using practice simulations and training strategies; others have implemented medication reconciliation checks at every discharge, checklists and other communication strategies, team-based quality-improvement (QI) initiatives, and new technologies to enhance and streamline communication. Some interventions follow the patient from the hospital to the community physician with a phone call, follow-up clinic, or other contact; others aim to empower the patient to be a better self-advocate. But for hospitalists, the challenge is to communicate the right amount of transfer information to the right receiver at the right time.
No matter the technique, the goal is the same: Improve the handoff and discharge process in a way that promotes efficiency and patient safety. And hospitalists are at the forefront of the changing landscape of care transitions.
Under the Microscope
Care transitions of all kinds are under the magnifying glass of national healthcare reform, with growing recognition of the need to make care safer and reduce the preventable, costly hospital readmissions caused by incomplete handoffs. Care transitions for hospitalists include internal handoffs, both at daily shift changes and at service changes when an outgoing provider is leaving after a period of consecutive daily shifts. These typically involve a sign-out process and face-to-face encounter, with some kind of written backup. One teaching institution reported that such handoffs take place 4,000 times per day in the hospital, or 1.6 million times per year.2
—Arpana Vidyarthi, MD, University of California at San Francisco
Geographical transitions can be from one floor or department to another, or out the hospital door to another facility or home. Transitions typically involve a discharge process and a written discharge summary. Care transitions also include hospital admissions, which put the hospitalist in the role of handoff receiver rather than initiator, plus a variety of other transitions involving nurses, physician extenders, and other practitioners.
Each transition is a major decision point in the course of a patient’s hospitalization; each transition also presents a time of heightened vulnerability (e.g., potential communication breakdowns, medication errors, patient anxiety or confusion, etc.). In fact, according to a Transitions of Care Consensus Policy Statement published in 2009 by SHM and five other medical societies, handoffs are ubiquitous in HM, with significant patient safety and quality deficiencies in handoffs existing in the current system.3
Poor communication at the time of handoff has been implicated in near-misses and adverse events in a variety of healthcare contexts, including 70% of hospital sentinel events studied by The Joint Commission, which named standardized handoffs (with an opportunity for interactive communication) as a National Patient Safety Goal in 2006.4 The federal government is studying care transitions, supporting demonstration projects for Medicare enrollees, and including readmission rates in national hospital report card data.
“Transitions of care and handoffs are a huge focus right now because of the increased fragmentation of care in the United States. Hospitalists are in charge of a greater percentage of hospitalized patients, which means more coordination of care is needed,” says Vineet Arora, MD, MA, FHM, assistant professor of medicine and associate director of the internal-medicine residency at the University of Chicago, and chair of the SHM task force on handoffs.
Inadequate communication and poor care transitions can undermine hospitalists’ best care-planning efforts, erode patients’ and families’ confidence and satisfaction with hospital care, and leave primary-care physicians (PCPs) feeling unsatisfied with the relationship. As many as 1 in 5 Medicare beneficiary hospitalizations result in a readmission within 30 days, and while not all of these are preventable, far too many are.5 Another prospective cohort study found that 1 in 5 patients discharged from the hospital to the home experienced an adverse event within three weeks of discharge.6 Complex comorbidities, advanced age, unknown PCP, and limited healthcare literacy present hospitalists with extremely difficult transitions.
Patient safety and cost control are the linchpins to national efforts to improve transitions of care. Dr. Arora recently coauthored an original research paper, which will be published in the Journal of Hospital Medicine in September, showing older hospitalized patients are twice as likely to report problems after discharge if their PCPs were not aware they were hospitalized.
“With escalating healthcare costs, people are looking at ways to save money and reduce redundant care,” Dr. Arora explains, pointing out, as an example, repeated tests resulting from inadequate communication between healthcare providers.
The System Must Change
“All of the effort we put into saving someone’s life—the years of experience, training, medical school, and residency—all of it comes to bear on that hospitalized patient. And it can all be unraveled at the time of discharge if it’s not handled properly,” says Arpana Vidyarthi, MD, a hospitalist and director of quality at the University of California at San Francisco.
Dr. Vidyarthi views in-hospital and discharge transitions as integrally related. “The analysis is similar, even if different techniques may be needed,” she says, adding that, fundamentally, it involves having a system that allows people—or forces them—to do the “right thing.”
That’s why achieving effective care transitions will require more than just a standardized tool or process, Dr. Vidyarthi says. “This is about understanding the ways people communicate and finding ways to train them to communicate better,” she says. “The problem we have is not a lack of information, but how to communicate what, to whom, and when.”
What’s really needed, Dr. Vidyarthi says, is a hospital’s commitment to more effective transitions and its hospitalists’ leadership in driving a comprehensive, multidisciplinary, team- and evidence-based QI process. The new process should be a QI-based solution to a hospital’s care-transitions issues. “Before you can standardize your process, you need to understand it,” she says. “This is a complex problem, and it needs a multifaceted solution. But this lies squarely within the hospitalist arena. We’re part of everything that happens in the hospital.
—Anuj Dalal, MD, Brigham and Women’s Hospital, Boston
Hospital administrators are looking to HM to solve transition and readmission problems now, says Tina Budnitz, MPH, BOOST Project Director (Better Outcomes for Older Adults through Safe Transitions). She expects the scrutiny from the C-suite, legislators, and watchdog groups to increase as the spotlight continues to shine on the healthcare system.
“Any hospitalist can act as a leader in their institution,” Budnitz says. “Be a change agent, pull a group together, and start asking questions: Do we have safe care-transitions practices and processes in place? Just by asking the right question, you can be a catalyst for the system.”
Budnitz also emphasizes the importance of teamwork in the hospital setting. “How can I help my teammates? What am I communicating to the nurses on rounds?” she says. “Can you initiate dialogue with your outpatient medical groups: ‘These faxes we’re sending you—is that information getting to you in ways and times that are helpful? And, by the way, when your patient is admitted, this information would really help me.’ ”
Innovative Strategies
One of the most important initiatives responding to concerns about care transitions is Project BOOST (www.hos pitalmedicine.org/BOOST), a comprehensive toolkit for improving a hospital’s transitions of care. The project aims to build a national consensus for best practices in transitions; collaborate with representatives from the Agency for Healthcare Research and Quality (AHRQ), the Centers for Medicare and Medicaid Services (CMS), and the Joint Commission; and develop a national resource library, Budnitz says.
“Project BOOST not only puts forth best practices for admitting patients, planning for discharge, and then doing the discharge, it also helps show facilities how to change their systems, with resources and tools for analyzing and re-engineering the system,” she says. “Sites get one-to-one assistance from a mentor.”
Six hospitals signed on to the pilot program in 2008; 24 more joined last year. In January, SHM announced a collaborative with the University of Michigan and Blue Cross Blue Shield of Michigan for 15 Michigan hospitals to receive training and mentorship starting in May. And last month, SHM and the California HealthCare Foundation announced a Project BOOST initiative for 20 of the health system’s hospitals (see “California Dreamin’”, p. 6). Other free resources offered on the BOOST Web portal include clinical, data collection, and project management tools. SHM also has a DVD that explains how to use the “teachback” method to improve communication with patients.
Jennifer Myers, MD, FHM, assistant professor of clinical medicine and patient-safety officer at the Hospital of the University of Pennsylvania in Philadelphia, is a Project BOOST participant who spearheaded a process change to improve the quality of her facility’s discharge summary, along with accompanying resident education.7 The discharge summary recently was integrated with the hospital’s electronic health record (EHR) system.
“We’ve gone from dictating the discharge summary to an electronic version completed by the hospitalist, with prompts for key components of the summary, which allows us to create summaries more efficiently—ideally on the day of discharge, but usually within 48 hours,” Dr. Myers says. “We previously researched whether teaching made a difference in the quality of discharges; we found that it did. So we look forward to standardizing our teaching approach around this important topic for all residents.”
Another care-transitions innovation receiving a lot of attention from the government and the private sector is Project RED (Re-Engineered Discharge), led by Brian Jack, MD, vice chair of the department of family medicine at Boston Medical Center. The Project RED research group develops and tests strategies to improve the hospital discharge process to promote patient safety and reduce rehospitalization rates.
“We used re-engineering tools borrowed from other fields, brought together experts from all over the hospital, divided up the whole discharge process, and identified key principles,” Dr. Jack explains. The resulting discharge strategy is reflected in an 11-item checklist of discrete, mutually reinforcing components, which have been shown to reduce rehospitalization rates by 32% while raising patient satisfaction.8 It includes comprehensive discharge and after-hospital plans, a nurse discharge advocate, and a medication reconciliation phone call to the patient. A virtual “patient advocate,” a computerized avatar named Louise, is now being tested. If successful, it will allow patients to interact with a touch-screen teacher of the after-care plan who has time to work at the patient’s pace.
Technology and Transitions
Informatics can be a key player in facilitating care transitions, says Anuj Dalal, MD, a hospitalist and instructor in medicine at Brigham and Women’s Hospital in Boston. He is using one of his hospital’s technological strengths—a well-established, firewall-protected e-mail system—to help improve the discharge process.
“We decided to try to improve awareness of test results pending at the time of discharge,” Dr. Dalal explains. “We created an intervention that automatically triggers an e-mail with the finalized test results to the responsible providers. The intervention creates a loop of communication between the inpatient attending and the PCP. What we hope to show in our research over the next year or two is whether the intervention actually increases awareness of test results by providers.”
One thing to remember is that “all kinds of things can go wrong with care transitions,” no matter the size of the institution, the experience of the staff, or technological limitations, says Vineet Chopra, MD, FACP, a hospitalist at the University of Michigan Health System in Ann Arbor. “The problems of transitions vary from place to place, day to day, time of day, shift changes; and let’s not forget physician extenders and the other members of the healthcare team,” he says. “The more complicated the team, the more complicated the information needing to be handed off becomes.”
Who Else Is Looking at Transitions of Care?
SHM convened the Handoffs Task Force in 2006. The team systematically reviewed the literature and published recommendations in the September 2009 Journal of Hospital Medicine.9 The recommendations are aimed at both community and academic hospitals, as well as hospitalists and other healthcare providers. A new collaborative designed to supplement Project BOOST for hospitalist group handoffs and help put the guidelines into practice is in the works, says Dr. Arora, the task force’s chair.
SHM and five medical groups, including the American College of Physicians, issued a Transitions of Care Consensus Statement, published in the July 2009 issue of the Journal of Hospital Medicine.5 Guiding principles relate to education, measurement, accountability, timely interchange of information, inclusion of patient and family, respect for the medical home, and the need for national standards.
The Joint Commission’s Center for Transforming Health Care, established in 2009 to solve healthcare’s most critical safety and quality problems, has made handoff communications its second major target, and is now working with 10 healthcare systems. Standardized handoff processes and communications were the subject of the Joint Commission’s 2006 National Patient Safety Goal, while the Comprehensive Accreditation Manual for Hospitals also specifies that before a hospital discharges or transfers a patient, it should inform and educate the patient about his or her follow-up care and services.
“We now have a safety goal under review dealing with medication reconciliation, and there are relevant standards related to culturally sensitive communication and low-literacy-level communication,” says Deborah Zadzam, PhD, RN, FAAN, director of international quality and performance measures for Joint Commission Resources. “The essential message the Joint Commission has for hospitalists is to communicate clearly, effectively and thoroughly; don’t assume you are understood or that you understand.”—LB
Before he joined the group at the university, Dr. Chopra worked at a community hospital, St. Joseph’s Mercy Hospital in Hot Springs, Ark. “It’s hard to come up with a one-size-fits-all solution when there are so many variables,” he says. At the community hospital, “we mandated that the hospitalist call the PCP at the time of discharge. At the academic medical center, we share an EHR with the PCPs and can reach them electronically. We are required to have the discharge summary in the computer before the patient leaves the hospital, and we mandate that hospitalists are reachable by e-mail or phone when they are off.
“I’m not a believer in throwing more technology at problems and just adding more layers of information tools,” Dr. Chopra adds. “Hospitalists who used to carry stethoscopes now also have a clipboard, phone, pager, PDA, and nine different signouts in their pockets. What we want to do is make their life easier. Here, we are looking at technology as a means to do that.”
Dr. Chopra and hospitalist colleague Prasanth Gosineni, MD, have been working with an Ann Arbor tech company called Synaptin to develop a lightweight, mobile client application designed to work on smartphones. Still in pilot testing, it would allow for task-oriented and priority-based messaging in real time and the systematic transfer of important information for the next hospitalist shift.
“You need to be able to share information in a systematic way, but that’s only half of the answer. The other half is the ability to ask specific questions,” Dr. Chopra says. “Technology doesn’t take away from the face-to-face encounter that needs to happen. Nothing will replace face time, but part of the solution is to provide data efficiently and in a way that is easily accessible.”
Dr. Chopra admits that EHR presents both positives and negatives to improved transitions and patient care, “depending on how well it works and what smart features it offers,” he says, “but also recognizing that EHR and other technologies have also taken us farther away from face-to-face exchanges. Some would say that’s part of the problem.”
Handoffs, discharges, and other transitions are ubiquitous in HM—and fraught with the potential for costly and harmful errors. The ideal of an interactive, face-to-face handoff simply is not available for many care transitions. However, hospitalists are challenged to find solutions that will work in their hospitals, with their teams, and their types of patients. Patients and policymakers expect nothing less. TH
Larry Beresford is a freelance writer based in Oakland, Calif.
References
- Payne C, Stein J, Dressler D. Implementation of a structured electronic tool to improve patient handoffs and resident satisfaction. Poster abstract: Internal Medicine 2010, April 21-24, 2010, Toronto.
- Vidyarthi AR. Triple Handoff. AHRQ WebM&M website. Available at: webmm.ahrq.gov/case.aspx? caseID=134. Published May 2006. Accessed May 29, 2010.
- Snow V, Beck D, Budnitz T, et al. Transitions of Care Consensus Policy Statement: American College of Physicians, Society of General Internal Medicine, Society of Hospital Medicine, American Geriatrics Society, American College of Emergency Physicians, and Society for Academic Emergency Medicine. J Hosp Med. 2009;4(6):364-370.
- 2006 National Patient Safety Goals. The Joint Commission website. Available at: www.jointcommission.org/PatientSafety/NationalPatientSafetyGoals/06_npsgs.htm. Accessed June 8, 2010.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009; 2:360:1418-1428.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161-167.
- Myers JS, Jaipaul CK, Kogan JR, Krekun S, Bellini LM, Shea JA. Are discharge summaries teachable? The effects of a discharge summary curriculum on the quality of discharge summaries in an internal medicine residency program. Acad Med. 2006; 81(10):S5-S8.
- Jack BW, Chetty VK, Anthony D, et al. A reengineered hospital discharge program to decrease rehospitalization: a randomized trial. Ann Intern Med. 2009;150(3):178-187.
- Arora VM, Manjarrez E, Dressler DD, Basaviah P, Halasyamani L, Kripalani S. Hospitalist handoffs: a systematic review and task force recommendations. J Hosp Med. 2009;4(7): 433-440.
- Halasyamani L, Kripalani S, Coleman E, et al. Transition of care for hospitalized elderly patients—development of a discharge checklist for hospitalists. J Hosp Med. 2006;1(6):354-360.
- Schnipper JL, Kirwin JL, Cotugno MC, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Int Med. 2006;166(5):565-571.
- Dudas V, Bookwalter T, Kerr KM, Pantilat SZ. The impact of follow-up telephone calls to patients after hospitalization. Am J Med. 2001;111(9B): 26S-30S.
Care Transition Tips for Hospitalists and Groups
One recognized key to effective internal handoffs is the face-to-face verbal update, with opportunities to ask questions, priority given to sicker patients, and a written backup filling in the blanks with information that might become important as the patient’s condition changes. But if that is not practical for your HM group, what tools and processes will come closest to the ideal?
A key to effective discharge from the hospital is connection with the PCP, although face-to-face encounters with PCPs are highly unlikely. Hospitalists say there are levels of connection with PCPs, from the urgent (“I need to talk to someone right now”) to the routine (“It’s OK if they get this information tomorrow”). Many often wonder if there should be two levels of discharge communication with PCPs: an immediate message relaying crucial information and a formal discharge summary coming later.
For HM groups, the following is a list of suggestions from transitions-of-care researchers:
- Keep accurate and up-to-date contact information, including preferred communication medium, on referring physicians; survey them on their satisfaction with the discharge communications they receive from hospitalists.
- Partner with hospital administrators and with patient-safety and quality officers to address handoff issues.
- Partner with IT staff to help bridge the divide between clinicians and information technology.
- Track such outcomes as rehospitalization rates.
- Offer formal training on handoffs, discharges, and effective communication to physicians and other providers.
- Standardize the signout process, with computerized tools when appropriate, and create automated systems for following up on tests and lab results that come back after discharge.
- Structure shifts and their overlaps to help facilitate signouts.
- Consider implementing a discharge checklist.10
- Develop a strategy for medication reconciliation, with someone assigned to the process, be that a hospitalist, pharmacist or nurse.11
- Advocate for a post-discharge call-back policy by assigned staff at defined intervals, either for every patient discharged or for those targeted as higher-risk.12
- Consider creating a post-discharge clinic and/or a phone number that discharged patients can call to clarify post-discharge questions and concerns.
For individual hospitalists:
- Understand the transition process, where it fails, and why.
- Be open to changing the way you do things. Be accountable for transitions, and a role model for others.
- Focus on the present—today’s baseline, current to-do items, and what to expect next in the patient’s care.
- Track patients and their future discharge needs from the day of admission. What’s the likely date for going home? What does the patient need to learn in the meantime? Help nurses focus on achieving those needs and, if possible, schedule the initial outpatient clinic appointment before the patient leaves the hospital.
- Take time to talk your patients, listen to their concerns and confirm their understanding of what lies ahead.
For hospitalists on the receiving end of transition messages:
- Actively listen—stay focused, limit interruptions, take notes.
- Ask questions to ensure your understanding and read back what you understand to be the communication.
- Have a system for keeping track of to-do items requiring follow-up.—LB
ONLINE EXCLUSIVE: Audio interviews with transitions of care experts
ONLINE EXCLUSIVE: Simulator Training Program Aims to Improve Hospital Handoffs
Few medical students receive formal training in how to perform patient handoffs effectively and efficiently, says Vineet Arora, MD, FHM, who chairs an SHM task force on improving handoffs. Most pick it up on the job, but Dr. Arora and her colleagues at the University of Chicago—where she is associate director of the internal-medicine residency program—and at the University of Michigan have been exploring ways to improve the process through education.1 Handoffs and care transitions are a major focus for hospital quality-improvement (QI) efforts nationally.
Dr. Arora’s group created an “observed simulation handoff experience” for medical students and residents, “offering an air of authenticity to the experience without the high-risk environment of learning on live patients,” she explains. Students who have completed an interactive training session perform the simulation at a computer station. They are provided with two types of information: static data about the mock patient—including such information as diagnosis, primary-care physician, and code status from a history and physical report—and video clips offering “a virtual, real-time barrage of constant updates” about the patient’s changing clinical status.
“They are given some time to extract and synthesize the important data for a handoff, and then they go in and perform the handoff in person to a ‘standardized receiver,’ ” Dr. Arora explains. The receiver is a resident or other clinician familiar both with the case and how the handoff should go, and who then provides a standardized evaluation, grade, and feedback.
“The goal is to teach students the triggers that need to be incorporated into an effective handoff,” Dr. Arora says. Her group also reviewed concepts of good handoffs from the medical literature and worked with a psychology expert in human communication.
“How do you teach people to give good handoffs? We don’t know all of the answers, but we think you have to start somewhere,” she says. “Technology can be a great facilitator to make handoffs go better. It’s not a perfect substitute for face-to-face, interactive handoffs, but it can dramatically inform care transitions.”
Larry Beresford is a freelance writer based in Oakland, Calif.
1. Farnan JM, Paro JA, Rodriguez RM, et al. Hand-off education and evaluation: piloting the observed simulated hand-off experience (OSHE). J Gen Intern Med. 2010;25(2):129-134.
Few medical students receive formal training in how to perform patient handoffs effectively and efficiently, says Vineet Arora, MD, FHM, who chairs an SHM task force on improving handoffs. Most pick it up on the job, but Dr. Arora and her colleagues at the University of Chicago—where she is associate director of the internal-medicine residency program—and at the University of Michigan have been exploring ways to improve the process through education.1 Handoffs and care transitions are a major focus for hospital quality-improvement (QI) efforts nationally.
Dr. Arora’s group created an “observed simulation handoff experience” for medical students and residents, “offering an air of authenticity to the experience without the high-risk environment of learning on live patients,” she explains. Students who have completed an interactive training session perform the simulation at a computer station. They are provided with two types of information: static data about the mock patient—including such information as diagnosis, primary-care physician, and code status from a history and physical report—and video clips offering “a virtual, real-time barrage of constant updates” about the patient’s changing clinical status.
“They are given some time to extract and synthesize the important data for a handoff, and then they go in and perform the handoff in person to a ‘standardized receiver,’ ” Dr. Arora explains. The receiver is a resident or other clinician familiar both with the case and how the handoff should go, and who then provides a standardized evaluation, grade, and feedback.
“The goal is to teach students the triggers that need to be incorporated into an effective handoff,” Dr. Arora says. Her group also reviewed concepts of good handoffs from the medical literature and worked with a psychology expert in human communication.
“How do you teach people to give good handoffs? We don’t know all of the answers, but we think you have to start somewhere,” she says. “Technology can be a great facilitator to make handoffs go better. It’s not a perfect substitute for face-to-face, interactive handoffs, but it can dramatically inform care transitions.”
Larry Beresford is a freelance writer based in Oakland, Calif.
1. Farnan JM, Paro JA, Rodriguez RM, et al. Hand-off education and evaluation: piloting the observed simulated hand-off experience (OSHE). J Gen Intern Med. 2010;25(2):129-134.
Few medical students receive formal training in how to perform patient handoffs effectively and efficiently, says Vineet Arora, MD, FHM, who chairs an SHM task force on improving handoffs. Most pick it up on the job, but Dr. Arora and her colleagues at the University of Chicago—where she is associate director of the internal-medicine residency program—and at the University of Michigan have been exploring ways to improve the process through education.1 Handoffs and care transitions are a major focus for hospital quality-improvement (QI) efforts nationally.
Dr. Arora’s group created an “observed simulation handoff experience” for medical students and residents, “offering an air of authenticity to the experience without the high-risk environment of learning on live patients,” she explains. Students who have completed an interactive training session perform the simulation at a computer station. They are provided with two types of information: static data about the mock patient—including such information as diagnosis, primary-care physician, and code status from a history and physical report—and video clips offering “a virtual, real-time barrage of constant updates” about the patient’s changing clinical status.
“They are given some time to extract and synthesize the important data for a handoff, and then they go in and perform the handoff in person to a ‘standardized receiver,’ ” Dr. Arora explains. The receiver is a resident or other clinician familiar both with the case and how the handoff should go, and who then provides a standardized evaluation, grade, and feedback.
“The goal is to teach students the triggers that need to be incorporated into an effective handoff,” Dr. Arora says. Her group also reviewed concepts of good handoffs from the medical literature and worked with a psychology expert in human communication.
“How do you teach people to give good handoffs? We don’t know all of the answers, but we think you have to start somewhere,” she says. “Technology can be a great facilitator to make handoffs go better. It’s not a perfect substitute for face-to-face, interactive handoffs, but it can dramatically inform care transitions.”
Larry Beresford is a freelance writer based in Oakland, Calif.
1. Farnan JM, Paro JA, Rodriguez RM, et al. Hand-off education and evaluation: piloting the observed simulated hand-off experience (OSHE). J Gen Intern Med. 2010;25(2):129-134.
Talking the Talk
On May 26, members of SHM’s Public Policy Committee visited Capitol Hill to meet with members of Congress and their legislative staffs. Now in their fifth year, the annual “Hill Day” meetings have evolved from explaining “What is a hospitalist?” to substantive discussions about HM’s impact on improving the quality and efficiency of healthcare and reducing preventable rehospitalizations.
“We don’t go in with an agenda to ask for things” or to guard professional turf, says Eric Siegal, MD, SFHM, committee chair and a critical care fellow at the University of Wisconsin School of Medicine in Madison. “People on the Hill who talk to us recognize that we are the experts [on improving the quality of hospital care]. They say to us: ‘You are different than the other medical associations; you really represent the solution.’ ”
The committee highlighted Project BOOST (Better Outcomes for Older Adults through Safe Transitions), SHM’s national quality initiative aimed at helping to improve care transitions and reduce rehospitalizations—–a major focus in the healthcare reform legislation.
Committee members also discussed SHM's support for a permanent repeal of the Sustainable Growth Rate (SGR). Physician reimbursement to Medicare patients technically was cut by 21% on June 1. The House passed another stopgap measure, but the Senate adjourned before a vote and is expected to raise the topic again early next week.
Committee member Patrick Torcson, MD, SFHM, a hospitalist at St. Tammany Parish Hospital in Covington, La., spent 30 minutes with Sen. David Vitter (R-La.), among his other Congressional encounters. “I had to be respectful and mindful of our senators’ and representatives’ different positions on healthcare reform,” Dr. Torcson explains, adding Vitter voted against the Patient Protection and Affordable Care Act, which was passed in March. “But he couldn’t have been more engaging with me. We talked about all aspects of hospital medicine.”
Find out the latest information on SGR reform and contact your legislators in support of permanent repeal through SHM's Legislative Action Center.
On May 26, members of SHM’s Public Policy Committee visited Capitol Hill to meet with members of Congress and their legislative staffs. Now in their fifth year, the annual “Hill Day” meetings have evolved from explaining “What is a hospitalist?” to substantive discussions about HM’s impact on improving the quality and efficiency of healthcare and reducing preventable rehospitalizations.
“We don’t go in with an agenda to ask for things” or to guard professional turf, says Eric Siegal, MD, SFHM, committee chair and a critical care fellow at the University of Wisconsin School of Medicine in Madison. “People on the Hill who talk to us recognize that we are the experts [on improving the quality of hospital care]. They say to us: ‘You are different than the other medical associations; you really represent the solution.’ ”
The committee highlighted Project BOOST (Better Outcomes for Older Adults through Safe Transitions), SHM’s national quality initiative aimed at helping to improve care transitions and reduce rehospitalizations—–a major focus in the healthcare reform legislation.
Committee members also discussed SHM's support for a permanent repeal of the Sustainable Growth Rate (SGR). Physician reimbursement to Medicare patients technically was cut by 21% on June 1. The House passed another stopgap measure, but the Senate adjourned before a vote and is expected to raise the topic again early next week.
Committee member Patrick Torcson, MD, SFHM, a hospitalist at St. Tammany Parish Hospital in Covington, La., spent 30 minutes with Sen. David Vitter (R-La.), among his other Congressional encounters. “I had to be respectful and mindful of our senators’ and representatives’ different positions on healthcare reform,” Dr. Torcson explains, adding Vitter voted against the Patient Protection and Affordable Care Act, which was passed in March. “But he couldn’t have been more engaging with me. We talked about all aspects of hospital medicine.”
Find out the latest information on SGR reform and contact your legislators in support of permanent repeal through SHM's Legislative Action Center.
On May 26, members of SHM’s Public Policy Committee visited Capitol Hill to meet with members of Congress and their legislative staffs. Now in their fifth year, the annual “Hill Day” meetings have evolved from explaining “What is a hospitalist?” to substantive discussions about HM’s impact on improving the quality and efficiency of healthcare and reducing preventable rehospitalizations.
“We don’t go in with an agenda to ask for things” or to guard professional turf, says Eric Siegal, MD, SFHM, committee chair and a critical care fellow at the University of Wisconsin School of Medicine in Madison. “People on the Hill who talk to us recognize that we are the experts [on improving the quality of hospital care]. They say to us: ‘You are different than the other medical associations; you really represent the solution.’ ”
The committee highlighted Project BOOST (Better Outcomes for Older Adults through Safe Transitions), SHM’s national quality initiative aimed at helping to improve care transitions and reduce rehospitalizations—–a major focus in the healthcare reform legislation.
Committee members also discussed SHM's support for a permanent repeal of the Sustainable Growth Rate (SGR). Physician reimbursement to Medicare patients technically was cut by 21% on June 1. The House passed another stopgap measure, but the Senate adjourned before a vote and is expected to raise the topic again early next week.
Committee member Patrick Torcson, MD, SFHM, a hospitalist at St. Tammany Parish Hospital in Covington, La., spent 30 minutes with Sen. David Vitter (R-La.), among his other Congressional encounters. “I had to be respectful and mindful of our senators’ and representatives’ different positions on healthcare reform,” Dr. Torcson explains, adding Vitter voted against the Patient Protection and Affordable Care Act, which was passed in March. “But he couldn’t have been more engaging with me. We talked about all aspects of hospital medicine.”
Find out the latest information on SGR reform and contact your legislators in support of permanent repeal through SHM's Legislative Action Center.