User login
My go-to Web resources for quick ICD-10 coding questions
An OBG Management reader recently requested assistance finding an app or Web site that would be helpful for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) coding, particularly for practicing ObGyns. It is not surprising that I have received this question, as we already are seeing a ton of smartphone apps that promise to search through the code descriptions quickly. None of these apps are ObGyn-specific but, given the vast amount, deciding which one is the best option to purchase and download can be a challenge.
Purchase considerations
Before you buy, decide what features you are looking for and make sure the app you have chosen can deliver what you need. Pay special attention to any reviews to learn the app’s pros and the cons. For instance, some apps offer code conversion from ICD-9 to ICD-10. Keep in mind, however, that not all conversions are accurate, and your search may just lead you to another unspecified code. Some apps will offer a decision tree, which is ideal. What you would like to avoid is an app that generates a list of 200 codes from a single search term.
A useful resource that I have found is this Buyers Guide to Mobile ICD-10 Apps from mHealthNews.1 This guide compares and contrasts the available apps (as of March 2014) for Android and Apple products. Some, you will note, are free; others are not. Try out a few before choosing. While several companies have developed products geared for ICD-10, many are not geared for mobile use and may have a substantial purchase price. Many of them also seem to be geared toward coders, not toward physician users.
My picks
ICD-10 Search was developed by e-MDs.2 It appears that this search program is part of a more extensive product that e-MDs sells, but for the time being, is free. This app deserves a look, especially because the decision tree format quickly gets you to the most specific code.
ICD-10 Code Lookup is the official offering from the Centers for Medicare & Medicaid Services (CMS).3 After you type in the term you are looking for, you get the search results in code order. The more specific your search terms, the closer you will get to the needed code. One caveat: the search mode is not set up to accept all clinical terms. For instance, I typed in "menorrhagia" and got 0 results; I typed in “menstruation, frequent” and I received 2 codes.
I hope this information is helpful, and I wish you an easy transition from ICD-9 to ICD-10.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
1. Schwartz E. Buyers guide to mobile ICD-10 apps. mHealthNews. http://www.mhealthnews.com/news/buyers-guide-mobile-icd-10-apps-smartphone-Apple-Android?page=0. Published March 24, 2014. Accessed September 16, 2015.
2. ICD-10 Search. e-MDs, Inc. http://app.icd10survivalkit.com/#tabDiagnosis. Accessed September 16, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 Code Lookup. https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx?KeyWord=follicular%20cyst&bc=AAAAAAAAAAACAA%3d%3d&. Accessed September 16, 2015.
An OBG Management reader recently requested assistance finding an app or Web site that would be helpful for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) coding, particularly for practicing ObGyns. It is not surprising that I have received this question, as we already are seeing a ton of smartphone apps that promise to search through the code descriptions quickly. None of these apps are ObGyn-specific but, given the vast amount, deciding which one is the best option to purchase and download can be a challenge.
Purchase considerations
Before you buy, decide what features you are looking for and make sure the app you have chosen can deliver what you need. Pay special attention to any reviews to learn the app’s pros and the cons. For instance, some apps offer code conversion from ICD-9 to ICD-10. Keep in mind, however, that not all conversions are accurate, and your search may just lead you to another unspecified code. Some apps will offer a decision tree, which is ideal. What you would like to avoid is an app that generates a list of 200 codes from a single search term.
A useful resource that I have found is this Buyers Guide to Mobile ICD-10 Apps from mHealthNews.1 This guide compares and contrasts the available apps (as of March 2014) for Android and Apple products. Some, you will note, are free; others are not. Try out a few before choosing. While several companies have developed products geared for ICD-10, many are not geared for mobile use and may have a substantial purchase price. Many of them also seem to be geared toward coders, not toward physician users.
My picks
ICD-10 Search was developed by e-MDs.2 It appears that this search program is part of a more extensive product that e-MDs sells, but for the time being, is free. This app deserves a look, especially because the decision tree format quickly gets you to the most specific code.
ICD-10 Code Lookup is the official offering from the Centers for Medicare & Medicaid Services (CMS).3 After you type in the term you are looking for, you get the search results in code order. The more specific your search terms, the closer you will get to the needed code. One caveat: the search mode is not set up to accept all clinical terms. For instance, I typed in "menorrhagia" and got 0 results; I typed in “menstruation, frequent” and I received 2 codes.
I hope this information is helpful, and I wish you an easy transition from ICD-9 to ICD-10.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
An OBG Management reader recently requested assistance finding an app or Web site that would be helpful for International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10) coding, particularly for practicing ObGyns. It is not surprising that I have received this question, as we already are seeing a ton of smartphone apps that promise to search through the code descriptions quickly. None of these apps are ObGyn-specific but, given the vast amount, deciding which one is the best option to purchase and download can be a challenge.
Purchase considerations
Before you buy, decide what features you are looking for and make sure the app you have chosen can deliver what you need. Pay special attention to any reviews to learn the app’s pros and the cons. For instance, some apps offer code conversion from ICD-9 to ICD-10. Keep in mind, however, that not all conversions are accurate, and your search may just lead you to another unspecified code. Some apps will offer a decision tree, which is ideal. What you would like to avoid is an app that generates a list of 200 codes from a single search term.
A useful resource that I have found is this Buyers Guide to Mobile ICD-10 Apps from mHealthNews.1 This guide compares and contrasts the available apps (as of March 2014) for Android and Apple products. Some, you will note, are free; others are not. Try out a few before choosing. While several companies have developed products geared for ICD-10, many are not geared for mobile use and may have a substantial purchase price. Many of them also seem to be geared toward coders, not toward physician users.
My picks
ICD-10 Search was developed by e-MDs.2 It appears that this search program is part of a more extensive product that e-MDs sells, but for the time being, is free. This app deserves a look, especially because the decision tree format quickly gets you to the most specific code.
ICD-10 Code Lookup is the official offering from the Centers for Medicare & Medicaid Services (CMS).3 After you type in the term you are looking for, you get the search results in code order. The more specific your search terms, the closer you will get to the needed code. One caveat: the search mode is not set up to accept all clinical terms. For instance, I typed in "menorrhagia" and got 0 results; I typed in “menstruation, frequent” and I received 2 codes.
I hope this information is helpful, and I wish you an easy transition from ICD-9 to ICD-10.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
1. Schwartz E. Buyers guide to mobile ICD-10 apps. mHealthNews. http://www.mhealthnews.com/news/buyers-guide-mobile-icd-10-apps-smartphone-Apple-Android?page=0. Published March 24, 2014. Accessed September 16, 2015.
2. ICD-10 Search. e-MDs, Inc. http://app.icd10survivalkit.com/#tabDiagnosis. Accessed September 16, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 Code Lookup. https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx?KeyWord=follicular%20cyst&bc=AAAAAAAAAAACAA%3d%3d&. Accessed September 16, 2015.
1. Schwartz E. Buyers guide to mobile ICD-10 apps. mHealthNews. http://www.mhealthnews.com/news/buyers-guide-mobile-icd-10-apps-smartphone-Apple-Android?page=0. Published March 24, 2014. Accessed September 16, 2015.
2. ICD-10 Search. e-MDs, Inc. http://app.icd10survivalkit.com/#tabDiagnosis. Accessed September 16, 2015.
3. Centers for Medicare & Medicaid Services. ICD-10 Code Lookup. https://www.cms.gov/medicare-coverage-database/staticpages/icd-10-code-lookup.aspx?KeyWord=follicular%20cyst&bc=AAAAAAAAAAACAA%3d%3d&. Accessed September 16, 2015.
ICD-10-CM documentation and coding for obstetric procedures

The countdown is on for the big coding switch. Last month I wrote about changes in International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes that will occur in relation to gynecologic services, but now it’s time to tackle obstetric services. For obstetricians, the changes will be all about definitions. And documentation of obstetric conditions will be more complicated due to several factors, including the need to report trimester information and gestational age, use of a placeholder code, more complex guidelines for certain conditions, chorionicity for multiple gestations, and use of a 7th digit to identify the fetus with a problem.
No one is expecting clinicians to instantly be fluent in code-speak, but in order for the most specific diagnoses to be reported, the clinical documentation must be spot on. Think of it this way: ICD-10-CM is not requiring you to document more, it’s requiring you to document more precisely.
How to get started
Figuring out where you are now goes a long way toward knowing where you need to be when the calendar changes to October 1—and the best way to do it is to perform a gap analysis. This analysis can be carried out by the clinician or a qualified practice staff person.
To begin, run a report of the distinct obstetric codes you have billed in 2015 by frequency. Then sort them in numeric order so that each individual code category is captured for all of the 5th digits (and the code then will be counted as a single code). Finally, review 5 medical records for each of the top 10 reported diagnosis categories and determine whether you could have reported a more specific ICD-10-CM code.
The information you gain will go a long way toward identifying potential weaknesses in the documentation, or, if you are currently using an electronic health record (EHR) to look up a code, it will point up any weak points in searching for the right code, based on your specific documentation at the encounter. Remember, practice makes perfect…eventually.
Well-trained staff can help
Not only must you, the clinician, learn about the part your clinical documentation will play in providing the most specific information that will lead to a very specific code, but your coding and billing staff will need training as well. They are the ones who should be checking your claims for accuracy from October 1 forward, as they will know the basic rules about which codes can be billed together, code order, place codes, and so on. In other words, while you as a clinician should be responsible for picking the more specific code in ICD-10-CM, your staff is your backup when you don’t.
Feedback from your staff on how the claims are being processed and, perhaps, the overuse of unspecified codes will keep you moving toward the goal of complete and precise clinical documentation and the reporting of diagnoses at the highest level possible given the documentation.
Highlights of ICD-10-CM obstetric coding
Given the complexity of obstetric coding, this article deals only with the most important changes. It will be up to each clinician to learn the rules that surround the diagnostic codes that you report most frequently. Here again, a trained staff can help by preparing specific coding tools for the most frequently used diagnoses, including notes about what must be in the record to report the most specific code.
Trimester, gestational age, and timing definitions
The majority of obstetric complication codes (these are the codes that start with the letter “O”) and the “Z” codes for supervision of a normal pregnancy require trimester information to be valid. In the outpatient setting, the trimester will be based on the gestational age at the date of the encounter. For inpatient admissions, the trimester will be based on the age at the time of admission; if the patient is hospitalized over more than one trimester, it is the admission trimester that continues to be recorded, not the discharge trimester.
Although there are codes that indicate an unspecified trimester, they should be reported rarely if this information is, in fact, available. Trimesters are defined as:
- first: less than 14 weeks, 0 days
- second: 14 weeks, 0 days to less than 28 weeks, 0 days
- third: 28 weeks, 0 days until delivery.
Examples of trimester codes include:
- O25.11Malnutrition in pregnancy, first trimester
- O14.02 Mild to moderate preeclampsia, second trimester
- O24.013 Preexisting diabetes mellitus, type 1, in pregnancy, third trimester.
However, definitions in ICD-10-CM go beyond this, and these definitions will have to be taken into account to provide sufficient documentation to report the condition. In ICD-9-CM, a missed abortion and early hemorrhage in pregnancy occurred prior to 22 completed weeks, but in ICD-10-CM that definition changes to prior to 20 completed weeks.
Additional definitions that may impact coding:
- preterm labor or delivery: 20 completed weeks to less than 37 completed weeks
- full-term labor or delivery: 37 completed weeks to 40 completed weeks
- postterm pregnancy: more than 40 completed weeks to 42 completed weeks
- prolonged pregnancy: more than 42 completed weeks.
You also will be required to include a code for gestational age any time you report an obstetric complication. This and the trimester information will change as the pregnancy advances, so always be sure that the code selected matches the gestational age on the flow sheet at the time of the encounter. The gestational age code is Z3A.__, with the final 2 digits representing the weeks of gestation (for instance, from 27 weeks, 0 days to 27 weeks, 6 days, the final 2 digits will be “27”).
ICD-10-CM also has different conventions when it comes to timing as it relates to conditions that are present during the episode in which the patient delivers. When this is the case, an “in childbirth” code must be selected instead of assigning the diagnosis by trimester, if one is available. There also are codes that are specific to “in the puer-perium,” and these generally will be reported after the patient has been discharged after delivery but also would be reported if there is no “in childbirth” code available at the time of delivery. The code categories to which this concept will apply are:
- preexisting hypertension
- diabetes mellitus
- malnutrition
- liver and biliary tract disorders
- subluxation of symphysis (pubis)
- obstetric embolism
- maternal infectious and parasitic diseases classifiable elsewhere
- other maternal diseases classifiable elsewhere
- maternal malignant neoplasms, traumatic injuries, and abuse classifiable elsewhere.
Taking time to read a code description from a search program or drop-down menu also will be important because some codes refer to “of the puerperium” versus “complicating the puerperium” or “in the puerperium.” The first reference means that the condition develops after delivery, while the second and third terms mean that it developed prior to delivery. For example, code O90.81, Anemia of the puerperium, refers to anemia that develops following delivery, while code O99.03 Anemia complicating the puerperium, denotes preexisting anemia that is still present in the postpartum period.
Multiple gestation coding and the 7th digit
The first thing you will notice here is that several code categories require a 7th numeric character of 0 or 1 through 9. This rule will apply to the following categories:
- complications specific to multiple gestation
- maternal care for malpresentation of fetus
- maternal care for disproportion
- maternal care for known or suspected fetal abnormality and damage
- maternal care for other fetal problems
- polyhydramnios
- other disorders of amniotic fluid and membranes
- preterm labor with preterm delivery
- term delivery with preterm labor
- obstructed labor due to malposition and malpresentation of fetus
- labor and delivery with umbilical cord complications.
A 7th character of 0 will be reported if this is a singleton pregnancy, and the numbers 1 through 5 and 9 refer to which fetus of the multiple gestation has the problem. The number 9 would indicate any fetus that was not labeled as 1 to 5.
The trick in documentation will be identifying the fetus with the problem consistently while still recognizing that, in some cases, such as fetal position, twins may switch places. On the other hand, if one fetus is small for dates, chances are good that this fetus will remain so during pregnancy when twins are present.
A code will be denied as invalid without this 7th digit, so it will be good practice for the clinician to document this information at each visit.
Additional information in regard to multiple gestations will be the chorionicity of the pregnancy, if known, but there will also be an “unable to determine” and an “unspecified” code available if that better fits the documentation for the visit. Note, however, that there is no code for a trichorionic/ triamniotic pregnancy; therefore, only the unspecified code would be reported in that case. In addition, if there is a continuing pregnancy after fetal loss, the cause must be identified within the code (that is, fetal reduction, fetal demise [and retained], or spontaneous abortion).
Documentation requirements for certain conditions
If you plan on reporting any complication of pregnancy at the time of the encounter, information about that condition needs to be part of the antepartum flow sheet comments. If, at the time of the encounter, a condition the patient has is not addressed and the entire visit involves only routine care, you would report the code for routine supervision of preg- nancy rather than the complication code. If the complication is again addressed at a later visit, the complication code would be reported again for that visit. The routine supervision code and the complication code cannot be reported on the record for the same encounter under ICD-10-CM rules.
Hypertension. Documentation needs to state whether the hypertension is preexisting or gestational. If it is preexisting, it needs to be identified as essential or secondary. If the patient also has hypertensive heart disease or chronic kidney disease, this information should be included, as different codes must be selected.
Diabetes. The documentation needs to state whether it is preexisting or gestational. If preexisting, you must document whether it is type 1 or type 2. If it is type 2, you must report an additional code for long-term insulin use, if applicable. The assumption for a woman with type 1 diabetes is that she is always insulin-dependent, so long-term use is not reported separately. Note, however, that neither metformin nor glyburide is considered insulin and there is no mechanism for reporting control with these medications.
If diabetes is gestational, you must indicate whether the patient’s blood glucose level is controlled by diet or insulin. If both, report only the insulin. There is no code for the use of other medications for the control of gestational diabetes, so you would have to report an unspecified code in that case.
Also note that ICD-10-CM differentiates between an abnormal 1-hour glucose tolerance test (GTT) and gestational diabetes. Unless a 3-specimen or 4-specimen GTT has been performed and results are abnormal, a diagnosis of gestational diabetes should not be reported.
An additional code outside of the obstetric complication chapter is required to denote any manifestations of diabetes. If there are none, then a diabetes uncomplicated manifestation code must be reported.
Preterm labor and delivery. Your documentation must clearly indicate whether the patient has preterm labor with preterm delivery or whether the delivery is term in addition to the trimester. For instance, if you document that Mary presents with preterm labor at 27 weeks, 2 days and delivers a girl at 28 weeks, 6 days, your code will describe Preterm labor second trimester with preterm delivery third trimester. However, if Susan presents with preterm labor at 30 weeks, 2 days and is managed until 37 weeks, 1 day, when she delivers a baby boy, your code would describe Term delivery with preterm labor, third trimester.
New coding options
Among the new coding options under ICD-10-CM:
- Abnormal findings on antenatal screening. These would be reported when the antenatal test is abnormal but you have not yet determined a definitive diagnosis.
- Alcohol, drug, and tobacco use during pregnancy. If you report any of these codes, you must also report a manifestation code for the patient’s condition. If the use is uncomplicated, you would report that code instead.
- Abuse of the pregnant patient. You can report sexual, physical, or psychological abuse, but you also must report a code for any applicable injury to the patient and identify the abuser, if known.
- Pruritic urticarial papules and plaques of pregnancy
- Retained intrauterine contraceptive device in pregnancy
- Maternal care due to uterine scar from other previous surgery. This would mean a surgery other than a previous cesarean delivery.
- Maternal care for (suspected) damage to the fetus by other medical procedures
- Maternal care for hydrops fetalis
- Maternal care for viable fetus in abdominal pregnancy
- Malignant neoplasm complicating pregnancy
- Failed attempt at vaginal birth after previous cesarean delivery
- Supervision of high-risk pregnancy due to social problems (for instance, a homeless patient)
- Rh incompatibility status (when you lack confirmation of serum antibodies and are giving prophylactic Rho[D] immune globulin).
CMS takes steps to ease transition to ICD-10-CM
To help health care providers get “up to speed” on the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), which takes effect October 1, 2015, the Centers for Medicare and Medicaid Services (CMS) has launched a new series for specialists. A guide tailored to ObGyns is available at http://roadto10.org/example-practice-obgyn. The guide includes:
Parting words
ICD-10-CM may seem like the end of the world, but its difficulty is exaggerated. If you fail to prepare, you will fail, and money coming in the door may be affected. If you prepare with training and practice, you will have a short learning curve. I wish you all the best. If you have specific questions about your practice, don’t hesitate to let us know so they can be addressed early.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The countdown is on for the big coding switch. Last month I wrote about changes in International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes that will occur in relation to gynecologic services, but now it’s time to tackle obstetric services. For obstetricians, the changes will be all about definitions. And documentation of obstetric conditions will be more complicated due to several factors, including the need to report trimester information and gestational age, use of a placeholder code, more complex guidelines for certain conditions, chorionicity for multiple gestations, and use of a 7th digit to identify the fetus with a problem.
No one is expecting clinicians to instantly be fluent in code-speak, but in order for the most specific diagnoses to be reported, the clinical documentation must be spot on. Think of it this way: ICD-10-CM is not requiring you to document more, it’s requiring you to document more precisely.
How to get started
Figuring out where you are now goes a long way toward knowing where you need to be when the calendar changes to October 1—and the best way to do it is to perform a gap analysis. This analysis can be carried out by the clinician or a qualified practice staff person.
To begin, run a report of the distinct obstetric codes you have billed in 2015 by frequency. Then sort them in numeric order so that each individual code category is captured for all of the 5th digits (and the code then will be counted as a single code). Finally, review 5 medical records for each of the top 10 reported diagnosis categories and determine whether you could have reported a more specific ICD-10-CM code.
The information you gain will go a long way toward identifying potential weaknesses in the documentation, or, if you are currently using an electronic health record (EHR) to look up a code, it will point up any weak points in searching for the right code, based on your specific documentation at the encounter. Remember, practice makes perfect…eventually.
Well-trained staff can help
Not only must you, the clinician, learn about the part your clinical documentation will play in providing the most specific information that will lead to a very specific code, but your coding and billing staff will need training as well. They are the ones who should be checking your claims for accuracy from October 1 forward, as they will know the basic rules about which codes can be billed together, code order, place codes, and so on. In other words, while you as a clinician should be responsible for picking the more specific code in ICD-10-CM, your staff is your backup when you don’t.
Feedback from your staff on how the claims are being processed and, perhaps, the overuse of unspecified codes will keep you moving toward the goal of complete and precise clinical documentation and the reporting of diagnoses at the highest level possible given the documentation.
Highlights of ICD-10-CM obstetric coding
Given the complexity of obstetric coding, this article deals only with the most important changes. It will be up to each clinician to learn the rules that surround the diagnostic codes that you report most frequently. Here again, a trained staff can help by preparing specific coding tools for the most frequently used diagnoses, including notes about what must be in the record to report the most specific code.
Trimester, gestational age, and timing definitions
The majority of obstetric complication codes (these are the codes that start with the letter “O”) and the “Z” codes for supervision of a normal pregnancy require trimester information to be valid. In the outpatient setting, the trimester will be based on the gestational age at the date of the encounter. For inpatient admissions, the trimester will be based on the age at the time of admission; if the patient is hospitalized over more than one trimester, it is the admission trimester that continues to be recorded, not the discharge trimester.
Although there are codes that indicate an unspecified trimester, they should be reported rarely if this information is, in fact, available. Trimesters are defined as:
- first: less than 14 weeks, 0 days
- second: 14 weeks, 0 days to less than 28 weeks, 0 days
- third: 28 weeks, 0 days until delivery.
Examples of trimester codes include:
- O25.11Malnutrition in pregnancy, first trimester
- O14.02 Mild to moderate preeclampsia, second trimester
- O24.013 Preexisting diabetes mellitus, type 1, in pregnancy, third trimester.
However, definitions in ICD-10-CM go beyond this, and these definitions will have to be taken into account to provide sufficient documentation to report the condition. In ICD-9-CM, a missed abortion and early hemorrhage in pregnancy occurred prior to 22 completed weeks, but in ICD-10-CM that definition changes to prior to 20 completed weeks.
Additional definitions that may impact coding:
- preterm labor or delivery: 20 completed weeks to less than 37 completed weeks
- full-term labor or delivery: 37 completed weeks to 40 completed weeks
- postterm pregnancy: more than 40 completed weeks to 42 completed weeks
- prolonged pregnancy: more than 42 completed weeks.
You also will be required to include a code for gestational age any time you report an obstetric complication. This and the trimester information will change as the pregnancy advances, so always be sure that the code selected matches the gestational age on the flow sheet at the time of the encounter. The gestational age code is Z3A.__, with the final 2 digits representing the weeks of gestation (for instance, from 27 weeks, 0 days to 27 weeks, 6 days, the final 2 digits will be “27”).
ICD-10-CM also has different conventions when it comes to timing as it relates to conditions that are present during the episode in which the patient delivers. When this is the case, an “in childbirth” code must be selected instead of assigning the diagnosis by trimester, if one is available. There also are codes that are specific to “in the puer-perium,” and these generally will be reported after the patient has been discharged after delivery but also would be reported if there is no “in childbirth” code available at the time of delivery. The code categories to which this concept will apply are:
- preexisting hypertension
- diabetes mellitus
- malnutrition
- liver and biliary tract disorders
- subluxation of symphysis (pubis)
- obstetric embolism
- maternal infectious and parasitic diseases classifiable elsewhere
- other maternal diseases classifiable elsewhere
- maternal malignant neoplasms, traumatic injuries, and abuse classifiable elsewhere.
Taking time to read a code description from a search program or drop-down menu also will be important because some codes refer to “of the puerperium” versus “complicating the puerperium” or “in the puerperium.” The first reference means that the condition develops after delivery, while the second and third terms mean that it developed prior to delivery. For example, code O90.81, Anemia of the puerperium, refers to anemia that develops following delivery, while code O99.03 Anemia complicating the puerperium, denotes preexisting anemia that is still present in the postpartum period.
Multiple gestation coding and the 7th digit
The first thing you will notice here is that several code categories require a 7th numeric character of 0 or 1 through 9. This rule will apply to the following categories:
- complications specific to multiple gestation
- maternal care for malpresentation of fetus
- maternal care for disproportion
- maternal care for known or suspected fetal abnormality and damage
- maternal care for other fetal problems
- polyhydramnios
- other disorders of amniotic fluid and membranes
- preterm labor with preterm delivery
- term delivery with preterm labor
- obstructed labor due to malposition and malpresentation of fetus
- labor and delivery with umbilical cord complications.
A 7th character of 0 will be reported if this is a singleton pregnancy, and the numbers 1 through 5 and 9 refer to which fetus of the multiple gestation has the problem. The number 9 would indicate any fetus that was not labeled as 1 to 5.
The trick in documentation will be identifying the fetus with the problem consistently while still recognizing that, in some cases, such as fetal position, twins may switch places. On the other hand, if one fetus is small for dates, chances are good that this fetus will remain so during pregnancy when twins are present.
A code will be denied as invalid without this 7th digit, so it will be good practice for the clinician to document this information at each visit.
Additional information in regard to multiple gestations will be the chorionicity of the pregnancy, if known, but there will also be an “unable to determine” and an “unspecified” code available if that better fits the documentation for the visit. Note, however, that there is no code for a trichorionic/ triamniotic pregnancy; therefore, only the unspecified code would be reported in that case. In addition, if there is a continuing pregnancy after fetal loss, the cause must be identified within the code (that is, fetal reduction, fetal demise [and retained], or spontaneous abortion).
Documentation requirements for certain conditions
If you plan on reporting any complication of pregnancy at the time of the encounter, information about that condition needs to be part of the antepartum flow sheet comments. If, at the time of the encounter, a condition the patient has is not addressed and the entire visit involves only routine care, you would report the code for routine supervision of preg- nancy rather than the complication code. If the complication is again addressed at a later visit, the complication code would be reported again for that visit. The routine supervision code and the complication code cannot be reported on the record for the same encounter under ICD-10-CM rules.
Hypertension. Documentation needs to state whether the hypertension is preexisting or gestational. If it is preexisting, it needs to be identified as essential or secondary. If the patient also has hypertensive heart disease or chronic kidney disease, this information should be included, as different codes must be selected.
Diabetes. The documentation needs to state whether it is preexisting or gestational. If preexisting, you must document whether it is type 1 or type 2. If it is type 2, you must report an additional code for long-term insulin use, if applicable. The assumption for a woman with type 1 diabetes is that she is always insulin-dependent, so long-term use is not reported separately. Note, however, that neither metformin nor glyburide is considered insulin and there is no mechanism for reporting control with these medications.
If diabetes is gestational, you must indicate whether the patient’s blood glucose level is controlled by diet or insulin. If both, report only the insulin. There is no code for the use of other medications for the control of gestational diabetes, so you would have to report an unspecified code in that case.
Also note that ICD-10-CM differentiates between an abnormal 1-hour glucose tolerance test (GTT) and gestational diabetes. Unless a 3-specimen or 4-specimen GTT has been performed and results are abnormal, a diagnosis of gestational diabetes should not be reported.
An additional code outside of the obstetric complication chapter is required to denote any manifestations of diabetes. If there are none, then a diabetes uncomplicated manifestation code must be reported.
Preterm labor and delivery. Your documentation must clearly indicate whether the patient has preterm labor with preterm delivery or whether the delivery is term in addition to the trimester. For instance, if you document that Mary presents with preterm labor at 27 weeks, 2 days and delivers a girl at 28 weeks, 6 days, your code will describe Preterm labor second trimester with preterm delivery third trimester. However, if Susan presents with preterm labor at 30 weeks, 2 days and is managed until 37 weeks, 1 day, when she delivers a baby boy, your code would describe Term delivery with preterm labor, third trimester.
New coding options
Among the new coding options under ICD-10-CM:
- Abnormal findings on antenatal screening. These would be reported when the antenatal test is abnormal but you have not yet determined a definitive diagnosis.
- Alcohol, drug, and tobacco use during pregnancy. If you report any of these codes, you must also report a manifestation code for the patient’s condition. If the use is uncomplicated, you would report that code instead.
- Abuse of the pregnant patient. You can report sexual, physical, or psychological abuse, but you also must report a code for any applicable injury to the patient and identify the abuser, if known.
- Pruritic urticarial papules and plaques of pregnancy
- Retained intrauterine contraceptive device in pregnancy
- Maternal care due to uterine scar from other previous surgery. This would mean a surgery other than a previous cesarean delivery.
- Maternal care for (suspected) damage to the fetus by other medical procedures
- Maternal care for hydrops fetalis
- Maternal care for viable fetus in abdominal pregnancy
- Malignant neoplasm complicating pregnancy
- Failed attempt at vaginal birth after previous cesarean delivery
- Supervision of high-risk pregnancy due to social problems (for instance, a homeless patient)
- Rh incompatibility status (when you lack confirmation of serum antibodies and are giving prophylactic Rho[D] immune globulin).
CMS takes steps to ease transition to ICD-10-CM
To help health care providers get “up to speed” on the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), which takes effect October 1, 2015, the Centers for Medicare and Medicaid Services (CMS) has launched a new series for specialists. A guide tailored to ObGyns is available at http://roadto10.org/example-practice-obgyn. The guide includes:
Parting words
ICD-10-CM may seem like the end of the world, but its difficulty is exaggerated. If you fail to prepare, you will fail, and money coming in the door may be affected. If you prepare with training and practice, you will have a short learning curve. I wish you all the best. If you have specific questions about your practice, don’t hesitate to let us know so they can be addressed early.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The countdown is on for the big coding switch. Last month I wrote about changes in International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes that will occur in relation to gynecologic services, but now it’s time to tackle obstetric services. For obstetricians, the changes will be all about definitions. And documentation of obstetric conditions will be more complicated due to several factors, including the need to report trimester information and gestational age, use of a placeholder code, more complex guidelines for certain conditions, chorionicity for multiple gestations, and use of a 7th digit to identify the fetus with a problem.
No one is expecting clinicians to instantly be fluent in code-speak, but in order for the most specific diagnoses to be reported, the clinical documentation must be spot on. Think of it this way: ICD-10-CM is not requiring you to document more, it’s requiring you to document more precisely.
How to get started
Figuring out where you are now goes a long way toward knowing where you need to be when the calendar changes to October 1—and the best way to do it is to perform a gap analysis. This analysis can be carried out by the clinician or a qualified practice staff person.
To begin, run a report of the distinct obstetric codes you have billed in 2015 by frequency. Then sort them in numeric order so that each individual code category is captured for all of the 5th digits (and the code then will be counted as a single code). Finally, review 5 medical records for each of the top 10 reported diagnosis categories and determine whether you could have reported a more specific ICD-10-CM code.
The information you gain will go a long way toward identifying potential weaknesses in the documentation, or, if you are currently using an electronic health record (EHR) to look up a code, it will point up any weak points in searching for the right code, based on your specific documentation at the encounter. Remember, practice makes perfect…eventually.
Well-trained staff can help
Not only must you, the clinician, learn about the part your clinical documentation will play in providing the most specific information that will lead to a very specific code, but your coding and billing staff will need training as well. They are the ones who should be checking your claims for accuracy from October 1 forward, as they will know the basic rules about which codes can be billed together, code order, place codes, and so on. In other words, while you as a clinician should be responsible for picking the more specific code in ICD-10-CM, your staff is your backup when you don’t.
Feedback from your staff on how the claims are being processed and, perhaps, the overuse of unspecified codes will keep you moving toward the goal of complete and precise clinical documentation and the reporting of diagnoses at the highest level possible given the documentation.
Highlights of ICD-10-CM obstetric coding
Given the complexity of obstetric coding, this article deals only with the most important changes. It will be up to each clinician to learn the rules that surround the diagnostic codes that you report most frequently. Here again, a trained staff can help by preparing specific coding tools for the most frequently used diagnoses, including notes about what must be in the record to report the most specific code.
Trimester, gestational age, and timing definitions
The majority of obstetric complication codes (these are the codes that start with the letter “O”) and the “Z” codes for supervision of a normal pregnancy require trimester information to be valid. In the outpatient setting, the trimester will be based on the gestational age at the date of the encounter. For inpatient admissions, the trimester will be based on the age at the time of admission; if the patient is hospitalized over more than one trimester, it is the admission trimester that continues to be recorded, not the discharge trimester.
Although there are codes that indicate an unspecified trimester, they should be reported rarely if this information is, in fact, available. Trimesters are defined as:
- first: less than 14 weeks, 0 days
- second: 14 weeks, 0 days to less than 28 weeks, 0 days
- third: 28 weeks, 0 days until delivery.
Examples of trimester codes include:
- O25.11Malnutrition in pregnancy, first trimester
- O14.02 Mild to moderate preeclampsia, second trimester
- O24.013 Preexisting diabetes mellitus, type 1, in pregnancy, third trimester.
However, definitions in ICD-10-CM go beyond this, and these definitions will have to be taken into account to provide sufficient documentation to report the condition. In ICD-9-CM, a missed abortion and early hemorrhage in pregnancy occurred prior to 22 completed weeks, but in ICD-10-CM that definition changes to prior to 20 completed weeks.
Additional definitions that may impact coding:
- preterm labor or delivery: 20 completed weeks to less than 37 completed weeks
- full-term labor or delivery: 37 completed weeks to 40 completed weeks
- postterm pregnancy: more than 40 completed weeks to 42 completed weeks
- prolonged pregnancy: more than 42 completed weeks.
You also will be required to include a code for gestational age any time you report an obstetric complication. This and the trimester information will change as the pregnancy advances, so always be sure that the code selected matches the gestational age on the flow sheet at the time of the encounter. The gestational age code is Z3A.__, with the final 2 digits representing the weeks of gestation (for instance, from 27 weeks, 0 days to 27 weeks, 6 days, the final 2 digits will be “27”).
ICD-10-CM also has different conventions when it comes to timing as it relates to conditions that are present during the episode in which the patient delivers. When this is the case, an “in childbirth” code must be selected instead of assigning the diagnosis by trimester, if one is available. There also are codes that are specific to “in the puer-perium,” and these generally will be reported after the patient has been discharged after delivery but also would be reported if there is no “in childbirth” code available at the time of delivery. The code categories to which this concept will apply are:
- preexisting hypertension
- diabetes mellitus
- malnutrition
- liver and biliary tract disorders
- subluxation of symphysis (pubis)
- obstetric embolism
- maternal infectious and parasitic diseases classifiable elsewhere
- other maternal diseases classifiable elsewhere
- maternal malignant neoplasms, traumatic injuries, and abuse classifiable elsewhere.
Taking time to read a code description from a search program or drop-down menu also will be important because some codes refer to “of the puerperium” versus “complicating the puerperium” or “in the puerperium.” The first reference means that the condition develops after delivery, while the second and third terms mean that it developed prior to delivery. For example, code O90.81, Anemia of the puerperium, refers to anemia that develops following delivery, while code O99.03 Anemia complicating the puerperium, denotes preexisting anemia that is still present in the postpartum period.
Multiple gestation coding and the 7th digit
The first thing you will notice here is that several code categories require a 7th numeric character of 0 or 1 through 9. This rule will apply to the following categories:
- complications specific to multiple gestation
- maternal care for malpresentation of fetus
- maternal care for disproportion
- maternal care for known or suspected fetal abnormality and damage
- maternal care for other fetal problems
- polyhydramnios
- other disorders of amniotic fluid and membranes
- preterm labor with preterm delivery
- term delivery with preterm labor
- obstructed labor due to malposition and malpresentation of fetus
- labor and delivery with umbilical cord complications.
A 7th character of 0 will be reported if this is a singleton pregnancy, and the numbers 1 through 5 and 9 refer to which fetus of the multiple gestation has the problem. The number 9 would indicate any fetus that was not labeled as 1 to 5.
The trick in documentation will be identifying the fetus with the problem consistently while still recognizing that, in some cases, such as fetal position, twins may switch places. On the other hand, if one fetus is small for dates, chances are good that this fetus will remain so during pregnancy when twins are present.
A code will be denied as invalid without this 7th digit, so it will be good practice for the clinician to document this information at each visit.
Additional information in regard to multiple gestations will be the chorionicity of the pregnancy, if known, but there will also be an “unable to determine” and an “unspecified” code available if that better fits the documentation for the visit. Note, however, that there is no code for a trichorionic/ triamniotic pregnancy; therefore, only the unspecified code would be reported in that case. In addition, if there is a continuing pregnancy after fetal loss, the cause must be identified within the code (that is, fetal reduction, fetal demise [and retained], or spontaneous abortion).
Documentation requirements for certain conditions
If you plan on reporting any complication of pregnancy at the time of the encounter, information about that condition needs to be part of the antepartum flow sheet comments. If, at the time of the encounter, a condition the patient has is not addressed and the entire visit involves only routine care, you would report the code for routine supervision of preg- nancy rather than the complication code. If the complication is again addressed at a later visit, the complication code would be reported again for that visit. The routine supervision code and the complication code cannot be reported on the record for the same encounter under ICD-10-CM rules.
Hypertension. Documentation needs to state whether the hypertension is preexisting or gestational. If it is preexisting, it needs to be identified as essential or secondary. If the patient also has hypertensive heart disease or chronic kidney disease, this information should be included, as different codes must be selected.
Diabetes. The documentation needs to state whether it is preexisting or gestational. If preexisting, you must document whether it is type 1 or type 2. If it is type 2, you must report an additional code for long-term insulin use, if applicable. The assumption for a woman with type 1 diabetes is that she is always insulin-dependent, so long-term use is not reported separately. Note, however, that neither metformin nor glyburide is considered insulin and there is no mechanism for reporting control with these medications.
If diabetes is gestational, you must indicate whether the patient’s blood glucose level is controlled by diet or insulin. If both, report only the insulin. There is no code for the use of other medications for the control of gestational diabetes, so you would have to report an unspecified code in that case.
Also note that ICD-10-CM differentiates between an abnormal 1-hour glucose tolerance test (GTT) and gestational diabetes. Unless a 3-specimen or 4-specimen GTT has been performed and results are abnormal, a diagnosis of gestational diabetes should not be reported.
An additional code outside of the obstetric complication chapter is required to denote any manifestations of diabetes. If there are none, then a diabetes uncomplicated manifestation code must be reported.
Preterm labor and delivery. Your documentation must clearly indicate whether the patient has preterm labor with preterm delivery or whether the delivery is term in addition to the trimester. For instance, if you document that Mary presents with preterm labor at 27 weeks, 2 days and delivers a girl at 28 weeks, 6 days, your code will describe Preterm labor second trimester with preterm delivery third trimester. However, if Susan presents with preterm labor at 30 weeks, 2 days and is managed until 37 weeks, 1 day, when she delivers a baby boy, your code would describe Term delivery with preterm labor, third trimester.
New coding options
Among the new coding options under ICD-10-CM:
- Abnormal findings on antenatal screening. These would be reported when the antenatal test is abnormal but you have not yet determined a definitive diagnosis.
- Alcohol, drug, and tobacco use during pregnancy. If you report any of these codes, you must also report a manifestation code for the patient’s condition. If the use is uncomplicated, you would report that code instead.
- Abuse of the pregnant patient. You can report sexual, physical, or psychological abuse, but you also must report a code for any applicable injury to the patient and identify the abuser, if known.
- Pruritic urticarial papules and plaques of pregnancy
- Retained intrauterine contraceptive device in pregnancy
- Maternal care due to uterine scar from other previous surgery. This would mean a surgery other than a previous cesarean delivery.
- Maternal care for (suspected) damage to the fetus by other medical procedures
- Maternal care for hydrops fetalis
- Maternal care for viable fetus in abdominal pregnancy
- Malignant neoplasm complicating pregnancy
- Failed attempt at vaginal birth after previous cesarean delivery
- Supervision of high-risk pregnancy due to social problems (for instance, a homeless patient)
- Rh incompatibility status (when you lack confirmation of serum antibodies and are giving prophylactic Rho[D] immune globulin).
CMS takes steps to ease transition to ICD-10-CM
To help health care providers get “up to speed” on the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM), which takes effect October 1, 2015, the Centers for Medicare and Medicaid Services (CMS) has launched a new series for specialists. A guide tailored to ObGyns is available at http://roadto10.org/example-practice-obgyn. The guide includes:
Parting words
ICD-10-CM may seem like the end of the world, but its difficulty is exaggerated. If you fail to prepare, you will fail, and money coming in the door may be affected. If you prepare with training and practice, you will have a short learning curve. I wish you all the best. If you have specific questions about your practice, don’t hesitate to let us know so they can be addressed early.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In this Article
- How to do a gap analysis
- Highlights of OB coding
- Condition-specific coding notations

ICD-10-CM documentation and coding for GYN procedures

In 2 months, the new coding set will become the only accepted format for diagnostic coding on medical claims. By now, most clinicians and their staffs should have begun the training process, including the examination of current documentation patterns, to ensure that the more specific International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes can be reported.
In 2014, I informed you about the more general changes that are to come in the format and ideas for preparation.1 But now it is time to get down to the nitty-gritty (or granularity, if you prefer) of this coding format to ensure correct coding every time for your gynecology services. A separate article will appear in the September 2015 issue of OBG Management to describe diagnostic coding for obstetric care.
No wheel reinvention necessary
Many of the guidelines for ICD-9-CM will transfer over to ICD-10-CM, so it will not be necessary to reinvent the wheel—but there are important changes that will affect both your documentation and payers’ requirements for the highest level of specificity. There also will be some instructions in the tabular section of ICD-10-CM that will let you know whether a combination of codes can or cannot be reported together (called “excludes” notes). In the beginning, this process may require additional communication between practice staff and clinicians.
However, if your practice has prepared a teaching document that outlines currently used codes and compares them with ICD-10-CM code choices and provides comments in regard to issues such as code combinations, conversion to the new system should be almost seamless.
Remember, the documentation of the clinician drives the selection of the code. The less information provided, the less specificity—and the result may be increased denials due to medical necessity for procedures and treatments.
Most reported codes will begin with “N”
Although the format of the codes will change under ICD-10-CM, diagnostic reporting will remain the same for most of the gynecologic conditions reported, and clinicians should be aware that the codes they will be reporting mainly will come from those that begin with “N.” One advantage: None of these codes require a 7th character or utilize the “x” placeholder code. In fact, the majority of codes from this chapter will have a one-to-one counterpart in the ICD-9-CM codes. A few exceptions are outlined below.
In addition to the core of “N” codes, a handful of codes will come from other chapters to capture reasons for a gynecologic encounter or surgery. For instance, “Z” codes will be reported for encounters for reasons other than illness and include codes for contraceptive and procreative management, general counseling, history of diseases, preventive gynecologic examinations, and screening scenarios, to name just a few. “R” codes will be used most often for general signs and symptoms, such as abdominal pain or nausea and vomiting.
Your documentation will need to change in some important areas
When you see a patient for an injury to the urinary or pelvic organs that is not a complication of a procedure, or for a complication of a genitourinary prosthetic device, implant, or graft, you will need to document whether this is an initial or subsequent encounter or a sequela. This information is added as a 7th alpha character (a = initial, d = subsequent, s = sequela).
ICD-10-CM defines an initial encounter as the time period in which the patient is actively being treated. A subsequent encounter would be reported after the patient’s active treatment, while she is receiving routine care during the healing or recovery phase. For instance, you would report the encounter as subsequent when the patient is seen after her surgery for an injury to the ovary due to an automobile accident, but you would report an initial encounter for all visits through the surgical date of service when a patient presents with symptoms of mesh erosion requiring surgery. Sequela refers to a condition that developed as a result of another condition. For instance, if the patient’s intrauterine device (IUD) becomes embedded in the ostium due to an undetected uterine fibroid, that is a sequela.
The requirement to indicate laterality also will affect documentation, but this concept is limited to a few codes that might be reported by ObGyns. A designation of the right versus left organ will be required for reported cases of primary, secondary, borderline, or benign tumors of the breast, ovary, fallopian tube, broad ligament, and round ligament, as well as cancer in situ of the breast. However, the terms “bilateral” and “unilateral” are applied only to codes that describe hernias, acquired absence of the ovaries, and injuries to the ovaries and fallopian tubes that are not due to a surgical complication.
Unspecified codes still play a role
Unspecified ICD-10-CM codes still come into play when the clinician does not have enough information to assign a more specific code—that is, when, by the end of an encounter, no further information is available to assign a more specific diagnosis. For example, if a patient has signs of a fibroid upon examination, only the unspecified code can be reported until the clinician can discover whether it is intramural, submucosal, or subserosal. However, it would be equally incorrect to assign an unspecified code to an encounter once the nature of the fibroid has been determined.
Take note of these differences in coding
Here is a list of important new gynecologic coding requirements, which are presented in alphabetical order.
Amenorrhea, oligomenorrhea (N91.0–N91.5) and dysmenorrhea (N94.4–N94.5) will require documentation to indicate whether the condition is primary or secondary. Although an unspecified code is available, once treatment is begun the cause should be known and documented.
Artificial insemination problems will have a section:
- N98.0 Infection associated with artificial insemination
- N98.1 Hyperstimulation of ovaries
- N98.2 Complications of attempted introduction of fertilized ovum following in vitro fertilization
- N98.3 Complications of attempted introduction of embryo in embryo transfer
- N98.8 Other complications associated with artificial fertilization
- N98.9 Complication associated with artificial fertilization, unspecified.
Breast cancer codes will require documentation of which breast and what part of the breast is affected.
Contraceptive management highlights:
- Injectable contraceptives will have new codes for the initial prescription (Z30.013) and subsequent surveillance (Z30.42)
- IUD encounter for the prescription will have a new code (Z30.014), which is reported when the IUD is not being inserted on the same day
- Subdermal contraceptive implant surveillance will no longer have a specific code but will be included in the “other” contraceptive code Z30.49.
Conversion of a laparoscopic procedure to an open procedure will not have a code.
Cystocele, unspecified, will have code N81.10.
Dysplasia of vagina will be expanded into 3 codes based on mild, moderate, or unspecified: N89.0–N89.3.
Female genitourinary cancer codes:
- Documentation of right or left organs and which part of the uterus is affected will be required
- Cancer in situ of cervix will be expanded by site on the cervix: D06.0–D06.7
- Cancer in situ of the endometrium will have a specific code: D07.0.
Genuine stress urinary incontinence will only be referred to as stress incontinence (male or female). The code is now located in the urinary section of Chapter N: N39.3.
Genitourinary complications due to procedures and surgery will be organized in 1 section: N99
- Some conditions have more than 1 code based on cause:
- N99.2 Stricture of vagina due to surgical complication
- N89.5 Stricture of vagina not due to surgical complication
- N99.4 Pelvic adhesions due to surgical complication
- N73.6 Pelvic adhesions not due to surgical complication - Other codes will differentiate between intraoperative or postprocedure complications and whether the surgery is on the genitourinary system or a different surgery:
- N99.61 Intraoperative hemorrhage and hematoma of a genitourinary system organ or structure complicating a genitourinary system procedure
- N99.62 Intraoperative hemorrhage and hematoma of a genitourinary system organ or structure complicating other procedure
- N99.820 Postprocedural hemorrhage and hematoma of a genitourinary system organ or structure following a genitourinary system procedure
- N99.821 Postprocedural hemorrhage and hematoma of a genitourinary system organ or structure following other procedure.
Gynecologic examinations will have to include information on whether or not there were genitourinary abnormal findings on the exam. If so, an additional secondary code will be required to identify the abnormality: Z01.411 and finding code. (Without abnormal findings: Z01.419.) For instance, a diagnosis of bacterial vaginosis is made during the examination. The abnormal findings are not those from other areas such as the breast or thyroid.
Hematuria documentation must differentiate between gross: R31.0, benign essential:R31.1, or other forms: R31.2.
High-risk sexual behavior problems must be documented by heterosexual, bisexual, or homosexual behavior: Z72.51–Z72.53.
Hormonal contraceptives, long-term use, will have a specific code: Z79.3.
Hyperplasia without atypia (simple, complex, or benign) will be rolled into a single code: N85.01.
Immunizations, prophylactic, will not have specific codes as to type. An encounter for any type of immunization is Z23.
Pelvic pain will have its own symptom code: R10.2.
Personal history for cancer has been expanded:
- Personal history of cancer in situ:
- Z86.000 of breast
- Z86.001 of cervix uteri
- Z86.008 of other site - Personal history of benign neoplasm:
- Z86.012 of other benign neoplasm
- Z86.03 of uncertain behavior (borderline malignancies).
Procedures not carried out will be expanded in ICD-10 to include 2 new codes:
- Z53.01 Procedure contraindicated due to patient smoking
- Z53.21 Procedure not carried out because patient left before seeing physician.
Procreative management changes:
- Artificial insemination will not have a specific code
- New code for male factor infertility: Z31.81
- New code for Rh incompatibility: Z31.82. This code would be used when the patient presents for prophylactic rho(D) immune globulin in addition to the Z23 code for immunization. This code also would be reported for the patient being tested for isoimmunization with no test result at the time of the visit.
Uterine prolapse without vaginal wall prolapse (618.1) will not have a code replacement.
Vaginal conditions such as vaginal lacerations (old), leukorrhea not specified as infective, and vaginal hematoma will be represented by an “other” code: N89.8.
Vulvar cyst will have its own code: N90.7.
Vulvovaginitis has been expanded into category codes for acute, subacute/chronic conditions of both the vagina and the vulva, which changes the documentation requirements in order to code correctly: N76.0–N76.3.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. Witt M. Moving forward with ICD-10: capitalize on this extra time. OBG Manag. 2014;26(7):17, 18, 20.
In 2 months, the new coding set will become the only accepted format for diagnostic coding on medical claims. By now, most clinicians and their staffs should have begun the training process, including the examination of current documentation patterns, to ensure that the more specific International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes can be reported.
In 2014, I informed you about the more general changes that are to come in the format and ideas for preparation.1 But now it is time to get down to the nitty-gritty (or granularity, if you prefer) of this coding format to ensure correct coding every time for your gynecology services. A separate article will appear in the September 2015 issue of OBG Management to describe diagnostic coding for obstetric care.
No wheel reinvention necessary
Many of the guidelines for ICD-9-CM will transfer over to ICD-10-CM, so it will not be necessary to reinvent the wheel—but there are important changes that will affect both your documentation and payers’ requirements for the highest level of specificity. There also will be some instructions in the tabular section of ICD-10-CM that will let you know whether a combination of codes can or cannot be reported together (called “excludes” notes). In the beginning, this process may require additional communication between practice staff and clinicians.
However, if your practice has prepared a teaching document that outlines currently used codes and compares them with ICD-10-CM code choices and provides comments in regard to issues such as code combinations, conversion to the new system should be almost seamless.
Remember, the documentation of the clinician drives the selection of the code. The less information provided, the less specificity—and the result may be increased denials due to medical necessity for procedures and treatments.
Most reported codes will begin with “N”
Although the format of the codes will change under ICD-10-CM, diagnostic reporting will remain the same for most of the gynecologic conditions reported, and clinicians should be aware that the codes they will be reporting mainly will come from those that begin with “N.” One advantage: None of these codes require a 7th character or utilize the “x” placeholder code. In fact, the majority of codes from this chapter will have a one-to-one counterpart in the ICD-9-CM codes. A few exceptions are outlined below.
In addition to the core of “N” codes, a handful of codes will come from other chapters to capture reasons for a gynecologic encounter or surgery. For instance, “Z” codes will be reported for encounters for reasons other than illness and include codes for contraceptive and procreative management, general counseling, history of diseases, preventive gynecologic examinations, and screening scenarios, to name just a few. “R” codes will be used most often for general signs and symptoms, such as abdominal pain or nausea and vomiting.
Your documentation will need to change in some important areas
When you see a patient for an injury to the urinary or pelvic organs that is not a complication of a procedure, or for a complication of a genitourinary prosthetic device, implant, or graft, you will need to document whether this is an initial or subsequent encounter or a sequela. This information is added as a 7th alpha character (a = initial, d = subsequent, s = sequela).
ICD-10-CM defines an initial encounter as the time period in which the patient is actively being treated. A subsequent encounter would be reported after the patient’s active treatment, while she is receiving routine care during the healing or recovery phase. For instance, you would report the encounter as subsequent when the patient is seen after her surgery for an injury to the ovary due to an automobile accident, but you would report an initial encounter for all visits through the surgical date of service when a patient presents with symptoms of mesh erosion requiring surgery. Sequela refers to a condition that developed as a result of another condition. For instance, if the patient’s intrauterine device (IUD) becomes embedded in the ostium due to an undetected uterine fibroid, that is a sequela.
The requirement to indicate laterality also will affect documentation, but this concept is limited to a few codes that might be reported by ObGyns. A designation of the right versus left organ will be required for reported cases of primary, secondary, borderline, or benign tumors of the breast, ovary, fallopian tube, broad ligament, and round ligament, as well as cancer in situ of the breast. However, the terms “bilateral” and “unilateral” are applied only to codes that describe hernias, acquired absence of the ovaries, and injuries to the ovaries and fallopian tubes that are not due to a surgical complication.
Unspecified codes still play a role
Unspecified ICD-10-CM codes still come into play when the clinician does not have enough information to assign a more specific code—that is, when, by the end of an encounter, no further information is available to assign a more specific diagnosis. For example, if a patient has signs of a fibroid upon examination, only the unspecified code can be reported until the clinician can discover whether it is intramural, submucosal, or subserosal. However, it would be equally incorrect to assign an unspecified code to an encounter once the nature of the fibroid has been determined.
Take note of these differences in coding
Here is a list of important new gynecologic coding requirements, which are presented in alphabetical order.
Amenorrhea, oligomenorrhea (N91.0–N91.5) and dysmenorrhea (N94.4–N94.5) will require documentation to indicate whether the condition is primary or secondary. Although an unspecified code is available, once treatment is begun the cause should be known and documented.
Artificial insemination problems will have a section:
- N98.0 Infection associated with artificial insemination
- N98.1 Hyperstimulation of ovaries
- N98.2 Complications of attempted introduction of fertilized ovum following in vitro fertilization
- N98.3 Complications of attempted introduction of embryo in embryo transfer
- N98.8 Other complications associated with artificial fertilization
- N98.9 Complication associated with artificial fertilization, unspecified.
Breast cancer codes will require documentation of which breast and what part of the breast is affected.
Contraceptive management highlights:
- Injectable contraceptives will have new codes for the initial prescription (Z30.013) and subsequent surveillance (Z30.42)
- IUD encounter for the prescription will have a new code (Z30.014), which is reported when the IUD is not being inserted on the same day
- Subdermal contraceptive implant surveillance will no longer have a specific code but will be included in the “other” contraceptive code Z30.49.
Conversion of a laparoscopic procedure to an open procedure will not have a code.
Cystocele, unspecified, will have code N81.10.
Dysplasia of vagina will be expanded into 3 codes based on mild, moderate, or unspecified: N89.0–N89.3.
Female genitourinary cancer codes:
- Documentation of right or left organs and which part of the uterus is affected will be required
- Cancer in situ of cervix will be expanded by site on the cervix: D06.0–D06.7
- Cancer in situ of the endometrium will have a specific code: D07.0.
Genuine stress urinary incontinence will only be referred to as stress incontinence (male or female). The code is now located in the urinary section of Chapter N: N39.3.
Genitourinary complications due to procedures and surgery will be organized in 1 section: N99
- Some conditions have more than 1 code based on cause:
- N99.2 Stricture of vagina due to surgical complication
- N89.5 Stricture of vagina not due to surgical complication
- N99.4 Pelvic adhesions due to surgical complication
- N73.6 Pelvic adhesions not due to surgical complication - Other codes will differentiate between intraoperative or postprocedure complications and whether the surgery is on the genitourinary system or a different surgery:
- N99.61 Intraoperative hemorrhage and hematoma of a genitourinary system organ or structure complicating a genitourinary system procedure
- N99.62 Intraoperative hemorrhage and hematoma of a genitourinary system organ or structure complicating other procedure
- N99.820 Postprocedural hemorrhage and hematoma of a genitourinary system organ or structure following a genitourinary system procedure
- N99.821 Postprocedural hemorrhage and hematoma of a genitourinary system organ or structure following other procedure.
Gynecologic examinations will have to include information on whether or not there were genitourinary abnormal findings on the exam. If so, an additional secondary code will be required to identify the abnormality: Z01.411 and finding code. (Without abnormal findings: Z01.419.) For instance, a diagnosis of bacterial vaginosis is made during the examination. The abnormal findings are not those from other areas such as the breast or thyroid.
Hematuria documentation must differentiate between gross: R31.0, benign essential:R31.1, or other forms: R31.2.
High-risk sexual behavior problems must be documented by heterosexual, bisexual, or homosexual behavior: Z72.51–Z72.53.
Hormonal contraceptives, long-term use, will have a specific code: Z79.3.
Hyperplasia without atypia (simple, complex, or benign) will be rolled into a single code: N85.01.
Immunizations, prophylactic, will not have specific codes as to type. An encounter for any type of immunization is Z23.
Pelvic pain will have its own symptom code: R10.2.
Personal history for cancer has been expanded:
- Personal history of cancer in situ:
- Z86.000 of breast
- Z86.001 of cervix uteri
- Z86.008 of other site - Personal history of benign neoplasm:
- Z86.012 of other benign neoplasm
- Z86.03 of uncertain behavior (borderline malignancies).
Procedures not carried out will be expanded in ICD-10 to include 2 new codes:
- Z53.01 Procedure contraindicated due to patient smoking
- Z53.21 Procedure not carried out because patient left before seeing physician.
Procreative management changes:
- Artificial insemination will not have a specific code
- New code for male factor infertility: Z31.81
- New code for Rh incompatibility: Z31.82. This code would be used when the patient presents for prophylactic rho(D) immune globulin in addition to the Z23 code for immunization. This code also would be reported for the patient being tested for isoimmunization with no test result at the time of the visit.
Uterine prolapse without vaginal wall prolapse (618.1) will not have a code replacement.
Vaginal conditions such as vaginal lacerations (old), leukorrhea not specified as infective, and vaginal hematoma will be represented by an “other” code: N89.8.
Vulvar cyst will have its own code: N90.7.
Vulvovaginitis has been expanded into category codes for acute, subacute/chronic conditions of both the vagina and the vulva, which changes the documentation requirements in order to code correctly: N76.0–N76.3.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
In 2 months, the new coding set will become the only accepted format for diagnostic coding on medical claims. By now, most clinicians and their staffs should have begun the training process, including the examination of current documentation patterns, to ensure that the more specific International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes can be reported.
In 2014, I informed you about the more general changes that are to come in the format and ideas for preparation.1 But now it is time to get down to the nitty-gritty (or granularity, if you prefer) of this coding format to ensure correct coding every time for your gynecology services. A separate article will appear in the September 2015 issue of OBG Management to describe diagnostic coding for obstetric care.
No wheel reinvention necessary
Many of the guidelines for ICD-9-CM will transfer over to ICD-10-CM, so it will not be necessary to reinvent the wheel—but there are important changes that will affect both your documentation and payers’ requirements for the highest level of specificity. There also will be some instructions in the tabular section of ICD-10-CM that will let you know whether a combination of codes can or cannot be reported together (called “excludes” notes). In the beginning, this process may require additional communication between practice staff and clinicians.
However, if your practice has prepared a teaching document that outlines currently used codes and compares them with ICD-10-CM code choices and provides comments in regard to issues such as code combinations, conversion to the new system should be almost seamless.
Remember, the documentation of the clinician drives the selection of the code. The less information provided, the less specificity—and the result may be increased denials due to medical necessity for procedures and treatments.
Most reported codes will begin with “N”
Although the format of the codes will change under ICD-10-CM, diagnostic reporting will remain the same for most of the gynecologic conditions reported, and clinicians should be aware that the codes they will be reporting mainly will come from those that begin with “N.” One advantage: None of these codes require a 7th character or utilize the “x” placeholder code. In fact, the majority of codes from this chapter will have a one-to-one counterpart in the ICD-9-CM codes. A few exceptions are outlined below.
In addition to the core of “N” codes, a handful of codes will come from other chapters to capture reasons for a gynecologic encounter or surgery. For instance, “Z” codes will be reported for encounters for reasons other than illness and include codes for contraceptive and procreative management, general counseling, history of diseases, preventive gynecologic examinations, and screening scenarios, to name just a few. “R” codes will be used most often for general signs and symptoms, such as abdominal pain or nausea and vomiting.
Your documentation will need to change in some important areas
When you see a patient for an injury to the urinary or pelvic organs that is not a complication of a procedure, or for a complication of a genitourinary prosthetic device, implant, or graft, you will need to document whether this is an initial or subsequent encounter or a sequela. This information is added as a 7th alpha character (a = initial, d = subsequent, s = sequela).
ICD-10-CM defines an initial encounter as the time period in which the patient is actively being treated. A subsequent encounter would be reported after the patient’s active treatment, while she is receiving routine care during the healing or recovery phase. For instance, you would report the encounter as subsequent when the patient is seen after her surgery for an injury to the ovary due to an automobile accident, but you would report an initial encounter for all visits through the surgical date of service when a patient presents with symptoms of mesh erosion requiring surgery. Sequela refers to a condition that developed as a result of another condition. For instance, if the patient’s intrauterine device (IUD) becomes embedded in the ostium due to an undetected uterine fibroid, that is a sequela.
The requirement to indicate laterality also will affect documentation, but this concept is limited to a few codes that might be reported by ObGyns. A designation of the right versus left organ will be required for reported cases of primary, secondary, borderline, or benign tumors of the breast, ovary, fallopian tube, broad ligament, and round ligament, as well as cancer in situ of the breast. However, the terms “bilateral” and “unilateral” are applied only to codes that describe hernias, acquired absence of the ovaries, and injuries to the ovaries and fallopian tubes that are not due to a surgical complication.
Unspecified codes still play a role
Unspecified ICD-10-CM codes still come into play when the clinician does not have enough information to assign a more specific code—that is, when, by the end of an encounter, no further information is available to assign a more specific diagnosis. For example, if a patient has signs of a fibroid upon examination, only the unspecified code can be reported until the clinician can discover whether it is intramural, submucosal, or subserosal. However, it would be equally incorrect to assign an unspecified code to an encounter once the nature of the fibroid has been determined.
Take note of these differences in coding
Here is a list of important new gynecologic coding requirements, which are presented in alphabetical order.
Amenorrhea, oligomenorrhea (N91.0–N91.5) and dysmenorrhea (N94.4–N94.5) will require documentation to indicate whether the condition is primary or secondary. Although an unspecified code is available, once treatment is begun the cause should be known and documented.
Artificial insemination problems will have a section:
- N98.0 Infection associated with artificial insemination
- N98.1 Hyperstimulation of ovaries
- N98.2 Complications of attempted introduction of fertilized ovum following in vitro fertilization
- N98.3 Complications of attempted introduction of embryo in embryo transfer
- N98.8 Other complications associated with artificial fertilization
- N98.9 Complication associated with artificial fertilization, unspecified.
Breast cancer codes will require documentation of which breast and what part of the breast is affected.
Contraceptive management highlights:
- Injectable contraceptives will have new codes for the initial prescription (Z30.013) and subsequent surveillance (Z30.42)
- IUD encounter for the prescription will have a new code (Z30.014), which is reported when the IUD is not being inserted on the same day
- Subdermal contraceptive implant surveillance will no longer have a specific code but will be included in the “other” contraceptive code Z30.49.
Conversion of a laparoscopic procedure to an open procedure will not have a code.
Cystocele, unspecified, will have code N81.10.
Dysplasia of vagina will be expanded into 3 codes based on mild, moderate, or unspecified: N89.0–N89.3.
Female genitourinary cancer codes:
- Documentation of right or left organs and which part of the uterus is affected will be required
- Cancer in situ of cervix will be expanded by site on the cervix: D06.0–D06.7
- Cancer in situ of the endometrium will have a specific code: D07.0.
Genuine stress urinary incontinence will only be referred to as stress incontinence (male or female). The code is now located in the urinary section of Chapter N: N39.3.
Genitourinary complications due to procedures and surgery will be organized in 1 section: N99
- Some conditions have more than 1 code based on cause:
- N99.2 Stricture of vagina due to surgical complication
- N89.5 Stricture of vagina not due to surgical complication
- N99.4 Pelvic adhesions due to surgical complication
- N73.6 Pelvic adhesions not due to surgical complication - Other codes will differentiate between intraoperative or postprocedure complications and whether the surgery is on the genitourinary system or a different surgery:
- N99.61 Intraoperative hemorrhage and hematoma of a genitourinary system organ or structure complicating a genitourinary system procedure
- N99.62 Intraoperative hemorrhage and hematoma of a genitourinary system organ or structure complicating other procedure
- N99.820 Postprocedural hemorrhage and hematoma of a genitourinary system organ or structure following a genitourinary system procedure
- N99.821 Postprocedural hemorrhage and hematoma of a genitourinary system organ or structure following other procedure.
Gynecologic examinations will have to include information on whether or not there were genitourinary abnormal findings on the exam. If so, an additional secondary code will be required to identify the abnormality: Z01.411 and finding code. (Without abnormal findings: Z01.419.) For instance, a diagnosis of bacterial vaginosis is made during the examination. The abnormal findings are not those from other areas such as the breast or thyroid.
Hematuria documentation must differentiate between gross: R31.0, benign essential:R31.1, or other forms: R31.2.
High-risk sexual behavior problems must be documented by heterosexual, bisexual, or homosexual behavior: Z72.51–Z72.53.
Hormonal contraceptives, long-term use, will have a specific code: Z79.3.
Hyperplasia without atypia (simple, complex, or benign) will be rolled into a single code: N85.01.
Immunizations, prophylactic, will not have specific codes as to type. An encounter for any type of immunization is Z23.
Pelvic pain will have its own symptom code: R10.2.
Personal history for cancer has been expanded:
- Personal history of cancer in situ:
- Z86.000 of breast
- Z86.001 of cervix uteri
- Z86.008 of other site - Personal history of benign neoplasm:
- Z86.012 of other benign neoplasm
- Z86.03 of uncertain behavior (borderline malignancies).
Procedures not carried out will be expanded in ICD-10 to include 2 new codes:
- Z53.01 Procedure contraindicated due to patient smoking
- Z53.21 Procedure not carried out because patient left before seeing physician.
Procreative management changes:
- Artificial insemination will not have a specific code
- New code for male factor infertility: Z31.81
- New code for Rh incompatibility: Z31.82. This code would be used when the patient presents for prophylactic rho(D) immune globulin in addition to the Z23 code for immunization. This code also would be reported for the patient being tested for isoimmunization with no test result at the time of the visit.
Uterine prolapse without vaginal wall prolapse (618.1) will not have a code replacement.
Vaginal conditions such as vaginal lacerations (old), leukorrhea not specified as infective, and vaginal hematoma will be represented by an “other” code: N89.8.
Vulvar cyst will have its own code: N90.7.
Vulvovaginitis has been expanded into category codes for acute, subacute/chronic conditions of both the vagina and the vulva, which changes the documentation requirements in order to code correctly: N76.0–N76.3.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Reference
1. Witt M. Moving forward with ICD-10: capitalize on this extra time. OBG Manag. 2014;26(7):17, 18, 20.
Reference
1. Witt M. Moving forward with ICD-10: capitalize on this extra time. OBG Manag. 2014;26(7):17, 18, 20.
ObGyn Medicare and CPT coding changes that could affect your income in 2015

At least one, if not many, of the coding changes highlighted below is likely to modify the incomes of ObGyns in the upcoming year. Here, I outline the 2015 changes that are most likely to affect your practice to some degree.
Medicare changes kick off a melancholy 2015
Surgical global periods: A move to eliminate them is underway
I begin this article not with a new or revised code, but with an active proposal, which, if implemented, could adversely affect your surgical income in a few short years.
Starting in 2017, the Centers for Medicare and Medicaid Services (CMS) has indicated that it will change all surgical codes to 0-day global periods. They plan on starting by converting 10-day global codes to 0-day codes in 2017, and then move on to the conversion of 90-day global codes in 2018. This is being proposed because of an Office of Inspector General (OIG) finding that many surgeons are not providing the evaluation and management (E/M) services included in the surgical code; therefore, Medicare is reimbursing for surgical procedures at a higher rate than warranted. In addition, the number of assigned visits may no longer reflect current care protocols, which again may mean that Medicare is not paying appropriately.
The immediate effect of this proposal—which has been adopted in the final rule published in the November 13, 2014, Federal Register—would be a reduction in payment for the converted codes due to a decrease in the assigned relative value units (RVUs). In addition, surgeons would need to document and provide the level of service for all preoperative and postoperative care, which may lead some payers to begin scrutinizing both levels of service billed and frequency of visits before and after surgical procedures.
CMS is still looking for any additional comments from physicians on this conversion process and such comments can be submitted electronically through a link at www.regulations.gov. Reference the final rule as CMS-1612-FC in your reply.
Medicare reimbursements poised to decrease in April
The calendar year 2015 conversion factor will remain at $35.80 from January 1 through March 31, 2015, as mandated by section 101 of the Protecting Access to Medicare Act of 2014. This represents the amount that will be multiplied by the geographically adjusted RVU for a code to determine the final Medicare allowable per procedure or service billed. Effective April 1, 2015, the conversion factor based on the sustainable growth rate (SGR) formula will be only $28.22—representing a 21.2% decrease—unless Congress acts to override this mandate.
Code bundling leads to lost Medicare compensation
Hysterectomy bundling. Effective October 1, 2014, CMS began permanently bundling anterior/posterior colporrhaphy and colpopexy procedures into all vaginal and laparoscopic-assisted hysterectomy codes. By permanently, CMS means that no modifier can be used to report Current Procedural Terminology (CPT) code 57260 (anterior and posterior [A&P] repair) or codes 57280, 57282, 57283 (abdominal, and vaginal approach colpopexy procedures) separately when performed with a vaginal or laparoscopic-assisted hysterectomy.
The American Congress of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS) wrote to CMS in May with regard to these edits and objected to them strongly. These organizations will continue to work with CMS to get them removed. Until then, physicians who perform anterior/posterior colporrhaphy and colpopexy procedures with a vaginal or laparoscopic-assisted hysterectomy will need to clearly make a case in the operative report for the need to perform the additional procedures in order to add a modifier -22 (Increased procedural services) to the hysterectomy code for consideration of additional payment. If an A&P repair is performed, it would not be appropriate to bill only an anterior repair (CPT code 57240) or a posterior repair (CPT code 57250) to obtain some separate reimbursement as this would represent inaccurate coding.
Hysteroscopy bundling. Another edit that will affect ObGyns is the bundling of CPT code 58558 (Hysteroscopy, surgical; with sampling [biopsy] of endometrium and/or poly-pectomy, with or without D&C) into codes for hysteroscopic removal of a fibroid (58561) and the removal of an impacted foreign body (58562).
Previously, these codes could have been billed together, but now only the addition of a modifier -22 to the primary procedure (myomectomy or foreign body removal) presents any chance for additional reimbursement. In order to report the modifier, Medicare has indicated that the documentation must clearly support the additional work in accomplishing the primary procedure, including a statement of how much time it added to the normal procedure.
Awareness of new or revised CPT codes could benefit your earnings
The 2015 CPT code set includes several changes, including laboratory and vaccination codes, which may be of interest to your practice. Because of Health Insurance Portability and Accountability Act (HIPAA) requirements, insurers were required to accept new codes on January 1, 2015.
Added: Fetal chromosomal aneuploidy code for genomic sequencing
On January 1, 2014, CPT added a new code to report cell-free DNA to screen for fetal aneuploidy. This new code is 81507 (Fetal aneuploidy [trisomy 21, 18, and 13] DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy), and it was added to report the Harmony™ Prenatal Test.
For 2015, another new code, 81420 (Fetal chromosomal aneuploidy [eg, trisomy 21, monosomy X] genomic sequence analysis panel, circulating cell-free fetal DNA in maternal blood, must include analysis of chromosomes 13, 18, and 21), was added. This code represents a more comprehensive analysis and would therefore not be reported or ordered with code 81507. This new code requires a genomic sequence analysis panel.
HPV revisions extend beyond new codes
The codes for HPV testing have been redefined. These codes have been deleted: 87620-87622 (Infectious agent detection by nucleic acid [DNA or RNA]; papillomavirus, human, direct probe technique/amplified probe technique/quantification). In their place are three new codes to choose from:
- 87623, Human papillomavirus (HPV), low-risk types (eg, 6, 11, 42, 43, 44)
- 87624, Human papillomavirus (HPV), high-risk types (eg, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68)
- 87625, Human papillomavirus (HPV), types 16 and 18 only, includes type 45, if performed.
This coding change may be significant for payment as some payers will cover testing for high-risk HPV types only, so be sure your practice management team is aware of the latest rules for ordering HPV testing for your patients. Otherwise, patients could be faced with unexpected out-of-pocket expenses.
Egg freezing recognized as mainstream
- Infertility laboratories will be pleased to learn that CPT has changed the status of the code for cryopreservation of oocytes from a Category III to a Category I code. This means that this technology has now proven itself as a mainstream procedure, warranting a Category I CPT code. The new code is 89337 (Cryopreservation, mature oocyte[s]), which replaces the deleted code 0059T (Cryopreservation; oocyte[s]).
Vaccination codes for 2015
Almost every year new codes are added, and 2015 is no different. This year, you will see codes for:
- 90651, Human papillomavirus vaccine types 6, 11, 16, 18, 31, 33, 45, 52, 58, nonavalent (HPV), 3 dose schedule, for intramuscular use
- 90630, Influenza virus vaccine, quadrivalent (IIV4), split virus, preservative free, for intradermal use.
There is also a revision to the flu virus vaccine code 90654 to indicate that it represents a trivalent preservative-free vaccine. See the TABLE below for a complete list of all the vaccines by trade name and CPT/Medicare Healthcare Common Procedure Coding System (HCPCS) codes for the 2014−2015 flu season.
Keep in mind that reporting administration of the flu vaccine is different for Medicare than for private payers. Administration code G0008 and diagnosis code V04.81 (Need for prophylactic vaccination and inoculation against influenza) would be reported in conjunction with the appropriate vaccine code for Medicare, while CPT instructs you to report 90471 instead for the administration. When we switch to ICD-10 diagnostic coding on October 1, 2015, the code V04.81 becomes Z23 (Encounter for immunization).
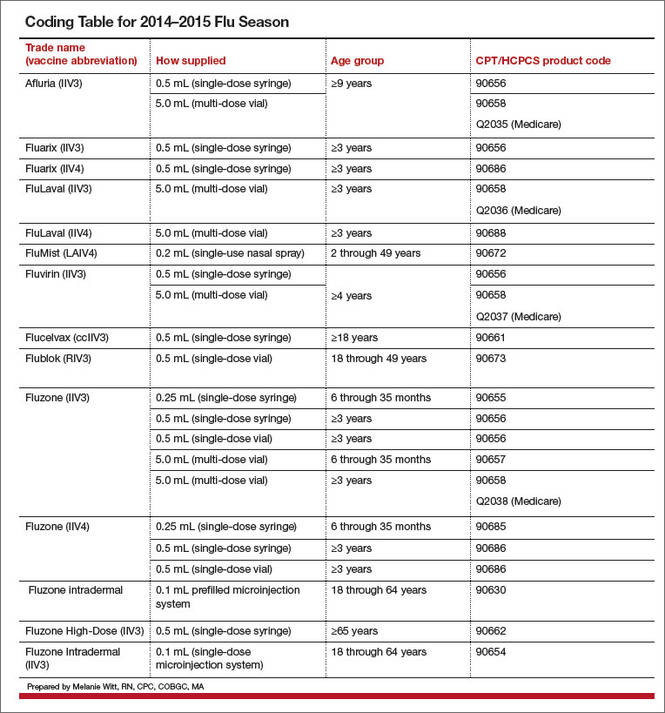
Three new codes for anoscopy
The first two codes were formerly Category III codes representing new technology, but now have proven to be more mainstream.
- 46601, Anoscopy; diagnostic, with high-resolution magnification (HRA) (eg, colposcope, operating microscope) and chemical agent enhancement, including collection of specimen(s) by brushing or washing, when performed
- 46607, Anoscopy; diagnostic, with high-resolution magnification (HRA) (eg, colposcope, operating microscope) and chemical agent enhancement, with biopsy, single or multiple
- 0377T, Anoscopy with directed submucosal injection of bulking agent for fecal incontinence.
Replacement codes for vertebral fracture assessments
If your practice is performing or ordering vertebral assessments for patients, there are two new codes to report. The old code, 77082 (Dual-energy X-ray absorptiometry [DXA], bone density study, 1 or more sites; vertebral fracture assessment) for vertebral fracture assessment has been deleted and replaced with:
- 77085, Dual-energy X-ray absorptiometry (DXA), bone density study, 1 or more sites; axial skeleton (eg, hips, pelvis, spine), including vertebral fracture assessment
- 77086, Vertebral fracture assessment via dual-energy X-ray absorptiometry (DXA).
Coding for breast ultrasound and tomosynthesis get more descriptive—at least for private insurance
The CPT Editorial Panel created three codes to describe digital breast tomosynthesis services and two new codes for a breast ultrasound.
- 77061, Digital breast tomosynthesis; unilateral
- 77062, Digital breast tomosynthesis; bilateral
- 77063, Screening digital breast tomosynthesis, bilateral (List separately in addition to the code for the primary procedure.)
- 76641, Ultrasound, breast, unilateral, real time with image documentation, including axilla when performed; complete
- 76642, Ultrasound, breast, unilateral, … ; limited.
Medicare, on the other hand, has decided to create a G code for tomosynthesis, which is the only code that will be accepted for payment if the patient meets her high-risk criteria for performance of this test.
Under Medicare rules you would report/order the following codes for mammographic services:
- Film (use CPT codes)
- 77056, Mammography; bilateral
- 77057, Screening mammography, bilateral (2-view film study of each breast)
- 2D digital (use G0202, G0204, and G0206)
- G0204, Diagnostic mammography, producing direct digital image, bilateral, all views
- G0206, Diagnostic mammography, producing direct digital image, unilateral, all views
- 3D screening (use G0202 for 2D digital plus the new CPT code 77063 for 3D)
procedure.)
- 3D diagnostic (use G0204 or G0206 for the 2D digital plus the new G code G0279 for 3D)
Modifier 59 becomes more specific
Another Medicare coding change that may affect ObGyns is the addition of new Medicare modifiers that are intended to eventually replace the modifier -59. This new list of modifiers will need to be appended to bundled procedures to more clearly explain why the secondary procedures should be paid separately. At the most recent American Medical Association (AMA) CPT symposium in Chicago, Illinois, CMS medical directors indicated that the new modifiers should be used only when the clinician is given instructions to do so by the carrier. Until then, the modifier -59 should continue to be used by most clinicians.
Here are the new modifiers, with an example of their use with currently bundled procedures that allow a modifier -59 to be used under certain circumstances:
- -XE: Separate encounter (A service that is distinct because it occurred during a separate encounter.) For instance, a patient presents to the office in the morning to have an abscess on her labia near her urethra incised and drained (56405). She returns in the afternoon to have a temporary catheter inserted because she states she cannot urinate and you decide to put in a temporary Foley catheter (51702) until the swelling has gone down. Add the modifier XE to 51702 to indicate it was performed at a different patient encounter.
- -XP: Separate practitioner (A service that is distinct because it was performed by a different practitioner.) Normally, Medicare will reimburse an unaffiliated clinician for performing a procedure that is bundled, since the bundling edits apply to the billing surgeon. But when two physicians from the same practice each are performing a different procedure at the same operative session that would otherwise be bundled, this new modifier will make that clear.
For example, Dr. Bates is performing a laparoscopic paravaginal defect repair (57423) and calls Dr. Clark, a urogynecologist in his practice, to remove severe adhesions from the ureters. The claim should go in under the same tax ID number, with the code 50715 listed first (as it has greater RVUs) and code 57423 reported with the -XP modifier.
- -XS: Separate structure (A service that is distinct because it was performed on a separate organ/structure.) Dr. Scott is performing the removal of endometrial implants around the left fallopian tube and in the cul-de-sac and notices that the right fallopian tube appears closed. He performs chromotubation on the right fallopian tube and notes that the right tube is blocked. Billing in this case would be 58662, 58350-XS.
- -XU: Unusual non-overlapping service (The use of a service that is distinct because it does not overlap usual components of the main service.) Mary has Medicare coverage and presents at 20 weeks 4 days gestation with bleeding and labor pains. Her examination shows bulging membranes that rupture when you attempt to remove the cerclage suture. You note a large rent in the cervix, but cannot get to the cerclage sutures as the patient is in active labor and beginning to bear down. The fetus and placenta are delivered a short time later through the rent in the cervix. You repair the rent in the cervix following delivery.
In this case, code 59400-52 (reduced services since the patient delivered at 20 weeks and there were reduced antepartum services), and 57720-XU because the repair of the cervix is not part of the usual services for a vaginal delivery.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
At least one, if not many, of the coding changes highlighted below is likely to modify the incomes of ObGyns in the upcoming year. Here, I outline the 2015 changes that are most likely to affect your practice to some degree.
Medicare changes kick off a melancholy 2015
Surgical global periods: A move to eliminate them is underway
I begin this article not with a new or revised code, but with an active proposal, which, if implemented, could adversely affect your surgical income in a few short years.
Starting in 2017, the Centers for Medicare and Medicaid Services (CMS) has indicated that it will change all surgical codes to 0-day global periods. They plan on starting by converting 10-day global codes to 0-day codes in 2017, and then move on to the conversion of 90-day global codes in 2018. This is being proposed because of an Office of Inspector General (OIG) finding that many surgeons are not providing the evaluation and management (E/M) services included in the surgical code; therefore, Medicare is reimbursing for surgical procedures at a higher rate than warranted. In addition, the number of assigned visits may no longer reflect current care protocols, which again may mean that Medicare is not paying appropriately.
The immediate effect of this proposal—which has been adopted in the final rule published in the November 13, 2014, Federal Register—would be a reduction in payment for the converted codes due to a decrease in the assigned relative value units (RVUs). In addition, surgeons would need to document and provide the level of service for all preoperative and postoperative care, which may lead some payers to begin scrutinizing both levels of service billed and frequency of visits before and after surgical procedures.
CMS is still looking for any additional comments from physicians on this conversion process and such comments can be submitted electronically through a link at www.regulations.gov. Reference the final rule as CMS-1612-FC in your reply.
Medicare reimbursements poised to decrease in April
The calendar year 2015 conversion factor will remain at $35.80 from January 1 through March 31, 2015, as mandated by section 101 of the Protecting Access to Medicare Act of 2014. This represents the amount that will be multiplied by the geographically adjusted RVU for a code to determine the final Medicare allowable per procedure or service billed. Effective April 1, 2015, the conversion factor based on the sustainable growth rate (SGR) formula will be only $28.22—representing a 21.2% decrease—unless Congress acts to override this mandate.
Code bundling leads to lost Medicare compensation
Hysterectomy bundling. Effective October 1, 2014, CMS began permanently bundling anterior/posterior colporrhaphy and colpopexy procedures into all vaginal and laparoscopic-assisted hysterectomy codes. By permanently, CMS means that no modifier can be used to report Current Procedural Terminology (CPT) code 57260 (anterior and posterior [A&P] repair) or codes 57280, 57282, 57283 (abdominal, and vaginal approach colpopexy procedures) separately when performed with a vaginal or laparoscopic-assisted hysterectomy.
The American Congress of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS) wrote to CMS in May with regard to these edits and objected to them strongly. These organizations will continue to work with CMS to get them removed. Until then, physicians who perform anterior/posterior colporrhaphy and colpopexy procedures with a vaginal or laparoscopic-assisted hysterectomy will need to clearly make a case in the operative report for the need to perform the additional procedures in order to add a modifier -22 (Increased procedural services) to the hysterectomy code for consideration of additional payment. If an A&P repair is performed, it would not be appropriate to bill only an anterior repair (CPT code 57240) or a posterior repair (CPT code 57250) to obtain some separate reimbursement as this would represent inaccurate coding.
Hysteroscopy bundling. Another edit that will affect ObGyns is the bundling of CPT code 58558 (Hysteroscopy, surgical; with sampling [biopsy] of endometrium and/or poly-pectomy, with or without D&C) into codes for hysteroscopic removal of a fibroid (58561) and the removal of an impacted foreign body (58562).
Previously, these codes could have been billed together, but now only the addition of a modifier -22 to the primary procedure (myomectomy or foreign body removal) presents any chance for additional reimbursement. In order to report the modifier, Medicare has indicated that the documentation must clearly support the additional work in accomplishing the primary procedure, including a statement of how much time it added to the normal procedure.
Awareness of new or revised CPT codes could benefit your earnings
The 2015 CPT code set includes several changes, including laboratory and vaccination codes, which may be of interest to your practice. Because of Health Insurance Portability and Accountability Act (HIPAA) requirements, insurers were required to accept new codes on January 1, 2015.
Added: Fetal chromosomal aneuploidy code for genomic sequencing
On January 1, 2014, CPT added a new code to report cell-free DNA to screen for fetal aneuploidy. This new code is 81507 (Fetal aneuploidy [trisomy 21, 18, and 13] DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy), and it was added to report the Harmony™ Prenatal Test.
For 2015, another new code, 81420 (Fetal chromosomal aneuploidy [eg, trisomy 21, monosomy X] genomic sequence analysis panel, circulating cell-free fetal DNA in maternal blood, must include analysis of chromosomes 13, 18, and 21), was added. This code represents a more comprehensive analysis and would therefore not be reported or ordered with code 81507. This new code requires a genomic sequence analysis panel.
HPV revisions extend beyond new codes
The codes for HPV testing have been redefined. These codes have been deleted: 87620-87622 (Infectious agent detection by nucleic acid [DNA or RNA]; papillomavirus, human, direct probe technique/amplified probe technique/quantification). In their place are three new codes to choose from:
- 87623, Human papillomavirus (HPV), low-risk types (eg, 6, 11, 42, 43, 44)
- 87624, Human papillomavirus (HPV), high-risk types (eg, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68)
- 87625, Human papillomavirus (HPV), types 16 and 18 only, includes type 45, if performed.
This coding change may be significant for payment as some payers will cover testing for high-risk HPV types only, so be sure your practice management team is aware of the latest rules for ordering HPV testing for your patients. Otherwise, patients could be faced with unexpected out-of-pocket expenses.
Egg freezing recognized as mainstream
- Infertility laboratories will be pleased to learn that CPT has changed the status of the code for cryopreservation of oocytes from a Category III to a Category I code. This means that this technology has now proven itself as a mainstream procedure, warranting a Category I CPT code. The new code is 89337 (Cryopreservation, mature oocyte[s]), which replaces the deleted code 0059T (Cryopreservation; oocyte[s]).
Vaccination codes for 2015
Almost every year new codes are added, and 2015 is no different. This year, you will see codes for:
- 90651, Human papillomavirus vaccine types 6, 11, 16, 18, 31, 33, 45, 52, 58, nonavalent (HPV), 3 dose schedule, for intramuscular use
- 90630, Influenza virus vaccine, quadrivalent (IIV4), split virus, preservative free, for intradermal use.
There is also a revision to the flu virus vaccine code 90654 to indicate that it represents a trivalent preservative-free vaccine. See the TABLE below for a complete list of all the vaccines by trade name and CPT/Medicare Healthcare Common Procedure Coding System (HCPCS) codes for the 2014−2015 flu season.
Keep in mind that reporting administration of the flu vaccine is different for Medicare than for private payers. Administration code G0008 and diagnosis code V04.81 (Need for prophylactic vaccination and inoculation against influenza) would be reported in conjunction with the appropriate vaccine code for Medicare, while CPT instructs you to report 90471 instead for the administration. When we switch to ICD-10 diagnostic coding on October 1, 2015, the code V04.81 becomes Z23 (Encounter for immunization).
Three new codes for anoscopy
The first two codes were formerly Category III codes representing new technology, but now have proven to be more mainstream.
- 46601, Anoscopy; diagnostic, with high-resolution magnification (HRA) (eg, colposcope, operating microscope) and chemical agent enhancement, including collection of specimen(s) by brushing or washing, when performed
- 46607, Anoscopy; diagnostic, with high-resolution magnification (HRA) (eg, colposcope, operating microscope) and chemical agent enhancement, with biopsy, single or multiple
- 0377T, Anoscopy with directed submucosal injection of bulking agent for fecal incontinence.
Replacement codes for vertebral fracture assessments
If your practice is performing or ordering vertebral assessments for patients, there are two new codes to report. The old code, 77082 (Dual-energy X-ray absorptiometry [DXA], bone density study, 1 or more sites; vertebral fracture assessment) for vertebral fracture assessment has been deleted and replaced with:
- 77085, Dual-energy X-ray absorptiometry (DXA), bone density study, 1 or more sites; axial skeleton (eg, hips, pelvis, spine), including vertebral fracture assessment
- 77086, Vertebral fracture assessment via dual-energy X-ray absorptiometry (DXA).
Coding for breast ultrasound and tomosynthesis get more descriptive—at least for private insurance
The CPT Editorial Panel created three codes to describe digital breast tomosynthesis services and two new codes for a breast ultrasound.
- 77061, Digital breast tomosynthesis; unilateral
- 77062, Digital breast tomosynthesis; bilateral
- 77063, Screening digital breast tomosynthesis, bilateral (List separately in addition to the code for the primary procedure.)
- 76641, Ultrasound, breast, unilateral, real time with image documentation, including axilla when performed; complete
- 76642, Ultrasound, breast, unilateral, … ; limited.
Medicare, on the other hand, has decided to create a G code for tomosynthesis, which is the only code that will be accepted for payment if the patient meets her high-risk criteria for performance of this test.
Under Medicare rules you would report/order the following codes for mammographic services:
- Film (use CPT codes)
- 77056, Mammography; bilateral
- 77057, Screening mammography, bilateral (2-view film study of each breast)
- 2D digital (use G0202, G0204, and G0206)
- G0204, Diagnostic mammography, producing direct digital image, bilateral, all views
- G0206, Diagnostic mammography, producing direct digital image, unilateral, all views
- 3D screening (use G0202 for 2D digital plus the new CPT code 77063 for 3D)
procedure.)
- 3D diagnostic (use G0204 or G0206 for the 2D digital plus the new G code G0279 for 3D)
Modifier 59 becomes more specific
Another Medicare coding change that may affect ObGyns is the addition of new Medicare modifiers that are intended to eventually replace the modifier -59. This new list of modifiers will need to be appended to bundled procedures to more clearly explain why the secondary procedures should be paid separately. At the most recent American Medical Association (AMA) CPT symposium in Chicago, Illinois, CMS medical directors indicated that the new modifiers should be used only when the clinician is given instructions to do so by the carrier. Until then, the modifier -59 should continue to be used by most clinicians.
Here are the new modifiers, with an example of their use with currently bundled procedures that allow a modifier -59 to be used under certain circumstances:
- -XE: Separate encounter (A service that is distinct because it occurred during a separate encounter.) For instance, a patient presents to the office in the morning to have an abscess on her labia near her urethra incised and drained (56405). She returns in the afternoon to have a temporary catheter inserted because she states she cannot urinate and you decide to put in a temporary Foley catheter (51702) until the swelling has gone down. Add the modifier XE to 51702 to indicate it was performed at a different patient encounter.
- -XP: Separate practitioner (A service that is distinct because it was performed by a different practitioner.) Normally, Medicare will reimburse an unaffiliated clinician for performing a procedure that is bundled, since the bundling edits apply to the billing surgeon. But when two physicians from the same practice each are performing a different procedure at the same operative session that would otherwise be bundled, this new modifier will make that clear.
For example, Dr. Bates is performing a laparoscopic paravaginal defect repair (57423) and calls Dr. Clark, a urogynecologist in his practice, to remove severe adhesions from the ureters. The claim should go in under the same tax ID number, with the code 50715 listed first (as it has greater RVUs) and code 57423 reported with the -XP modifier.
- -XS: Separate structure (A service that is distinct because it was performed on a separate organ/structure.) Dr. Scott is performing the removal of endometrial implants around the left fallopian tube and in the cul-de-sac and notices that the right fallopian tube appears closed. He performs chromotubation on the right fallopian tube and notes that the right tube is blocked. Billing in this case would be 58662, 58350-XS.
- -XU: Unusual non-overlapping service (The use of a service that is distinct because it does not overlap usual components of the main service.) Mary has Medicare coverage and presents at 20 weeks 4 days gestation with bleeding and labor pains. Her examination shows bulging membranes that rupture when you attempt to remove the cerclage suture. You note a large rent in the cervix, but cannot get to the cerclage sutures as the patient is in active labor and beginning to bear down. The fetus and placenta are delivered a short time later through the rent in the cervix. You repair the rent in the cervix following delivery.
In this case, code 59400-52 (reduced services since the patient delivered at 20 weeks and there were reduced antepartum services), and 57720-XU because the repair of the cervix is not part of the usual services for a vaginal delivery.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
At least one, if not many, of the coding changes highlighted below is likely to modify the incomes of ObGyns in the upcoming year. Here, I outline the 2015 changes that are most likely to affect your practice to some degree.
Medicare changes kick off a melancholy 2015
Surgical global periods: A move to eliminate them is underway
I begin this article not with a new or revised code, but with an active proposal, which, if implemented, could adversely affect your surgical income in a few short years.
Starting in 2017, the Centers for Medicare and Medicaid Services (CMS) has indicated that it will change all surgical codes to 0-day global periods. They plan on starting by converting 10-day global codes to 0-day codes in 2017, and then move on to the conversion of 90-day global codes in 2018. This is being proposed because of an Office of Inspector General (OIG) finding that many surgeons are not providing the evaluation and management (E/M) services included in the surgical code; therefore, Medicare is reimbursing for surgical procedures at a higher rate than warranted. In addition, the number of assigned visits may no longer reflect current care protocols, which again may mean that Medicare is not paying appropriately.
The immediate effect of this proposal—which has been adopted in the final rule published in the November 13, 2014, Federal Register—would be a reduction in payment for the converted codes due to a decrease in the assigned relative value units (RVUs). In addition, surgeons would need to document and provide the level of service for all preoperative and postoperative care, which may lead some payers to begin scrutinizing both levels of service billed and frequency of visits before and after surgical procedures.
CMS is still looking for any additional comments from physicians on this conversion process and such comments can be submitted electronically through a link at www.regulations.gov. Reference the final rule as CMS-1612-FC in your reply.
Medicare reimbursements poised to decrease in April
The calendar year 2015 conversion factor will remain at $35.80 from January 1 through March 31, 2015, as mandated by section 101 of the Protecting Access to Medicare Act of 2014. This represents the amount that will be multiplied by the geographically adjusted RVU for a code to determine the final Medicare allowable per procedure or service billed. Effective April 1, 2015, the conversion factor based on the sustainable growth rate (SGR) formula will be only $28.22—representing a 21.2% decrease—unless Congress acts to override this mandate.
Code bundling leads to lost Medicare compensation
Hysterectomy bundling. Effective October 1, 2014, CMS began permanently bundling anterior/posterior colporrhaphy and colpopexy procedures into all vaginal and laparoscopic-assisted hysterectomy codes. By permanently, CMS means that no modifier can be used to report Current Procedural Terminology (CPT) code 57260 (anterior and posterior [A&P] repair) or codes 57280, 57282, 57283 (abdominal, and vaginal approach colpopexy procedures) separately when performed with a vaginal or laparoscopic-assisted hysterectomy.
The American Congress of Obstetricians and Gynecologists (ACOG) and the American Urogynecologic Society (AUGS) wrote to CMS in May with regard to these edits and objected to them strongly. These organizations will continue to work with CMS to get them removed. Until then, physicians who perform anterior/posterior colporrhaphy and colpopexy procedures with a vaginal or laparoscopic-assisted hysterectomy will need to clearly make a case in the operative report for the need to perform the additional procedures in order to add a modifier -22 (Increased procedural services) to the hysterectomy code for consideration of additional payment. If an A&P repair is performed, it would not be appropriate to bill only an anterior repair (CPT code 57240) or a posterior repair (CPT code 57250) to obtain some separate reimbursement as this would represent inaccurate coding.
Hysteroscopy bundling. Another edit that will affect ObGyns is the bundling of CPT code 58558 (Hysteroscopy, surgical; with sampling [biopsy] of endometrium and/or poly-pectomy, with or without D&C) into codes for hysteroscopic removal of a fibroid (58561) and the removal of an impacted foreign body (58562).
Previously, these codes could have been billed together, but now only the addition of a modifier -22 to the primary procedure (myomectomy or foreign body removal) presents any chance for additional reimbursement. In order to report the modifier, Medicare has indicated that the documentation must clearly support the additional work in accomplishing the primary procedure, including a statement of how much time it added to the normal procedure.
Awareness of new or revised CPT codes could benefit your earnings
The 2015 CPT code set includes several changes, including laboratory and vaccination codes, which may be of interest to your practice. Because of Health Insurance Portability and Accountability Act (HIPAA) requirements, insurers were required to accept new codes on January 1, 2015.
Added: Fetal chromosomal aneuploidy code for genomic sequencing
On January 1, 2014, CPT added a new code to report cell-free DNA to screen for fetal aneuploidy. This new code is 81507 (Fetal aneuploidy [trisomy 21, 18, and 13] DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy), and it was added to report the Harmony™ Prenatal Test.
For 2015, another new code, 81420 (Fetal chromosomal aneuploidy [eg, trisomy 21, monosomy X] genomic sequence analysis panel, circulating cell-free fetal DNA in maternal blood, must include analysis of chromosomes 13, 18, and 21), was added. This code represents a more comprehensive analysis and would therefore not be reported or ordered with code 81507. This new code requires a genomic sequence analysis panel.
HPV revisions extend beyond new codes
The codes for HPV testing have been redefined. These codes have been deleted: 87620-87622 (Infectious agent detection by nucleic acid [DNA or RNA]; papillomavirus, human, direct probe technique/amplified probe technique/quantification). In their place are three new codes to choose from:
- 87623, Human papillomavirus (HPV), low-risk types (eg, 6, 11, 42, 43, 44)
- 87624, Human papillomavirus (HPV), high-risk types (eg, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68)
- 87625, Human papillomavirus (HPV), types 16 and 18 only, includes type 45, if performed.
This coding change may be significant for payment as some payers will cover testing for high-risk HPV types only, so be sure your practice management team is aware of the latest rules for ordering HPV testing for your patients. Otherwise, patients could be faced with unexpected out-of-pocket expenses.
Egg freezing recognized as mainstream
- Infertility laboratories will be pleased to learn that CPT has changed the status of the code for cryopreservation of oocytes from a Category III to a Category I code. This means that this technology has now proven itself as a mainstream procedure, warranting a Category I CPT code. The new code is 89337 (Cryopreservation, mature oocyte[s]), which replaces the deleted code 0059T (Cryopreservation; oocyte[s]).
Vaccination codes for 2015
Almost every year new codes are added, and 2015 is no different. This year, you will see codes for:
- 90651, Human papillomavirus vaccine types 6, 11, 16, 18, 31, 33, 45, 52, 58, nonavalent (HPV), 3 dose schedule, for intramuscular use
- 90630, Influenza virus vaccine, quadrivalent (IIV4), split virus, preservative free, for intradermal use.
There is also a revision to the flu virus vaccine code 90654 to indicate that it represents a trivalent preservative-free vaccine. See the TABLE below for a complete list of all the vaccines by trade name and CPT/Medicare Healthcare Common Procedure Coding System (HCPCS) codes for the 2014−2015 flu season.
Keep in mind that reporting administration of the flu vaccine is different for Medicare than for private payers. Administration code G0008 and diagnosis code V04.81 (Need for prophylactic vaccination and inoculation against influenza) would be reported in conjunction with the appropriate vaccine code for Medicare, while CPT instructs you to report 90471 instead for the administration. When we switch to ICD-10 diagnostic coding on October 1, 2015, the code V04.81 becomes Z23 (Encounter for immunization).
Three new codes for anoscopy
The first two codes were formerly Category III codes representing new technology, but now have proven to be more mainstream.
- 46601, Anoscopy; diagnostic, with high-resolution magnification (HRA) (eg, colposcope, operating microscope) and chemical agent enhancement, including collection of specimen(s) by brushing or washing, when performed
- 46607, Anoscopy; diagnostic, with high-resolution magnification (HRA) (eg, colposcope, operating microscope) and chemical agent enhancement, with biopsy, single or multiple
- 0377T, Anoscopy with directed submucosal injection of bulking agent for fecal incontinence.
Replacement codes for vertebral fracture assessments
If your practice is performing or ordering vertebral assessments for patients, there are two new codes to report. The old code, 77082 (Dual-energy X-ray absorptiometry [DXA], bone density study, 1 or more sites; vertebral fracture assessment) for vertebral fracture assessment has been deleted and replaced with:
- 77085, Dual-energy X-ray absorptiometry (DXA), bone density study, 1 or more sites; axial skeleton (eg, hips, pelvis, spine), including vertebral fracture assessment
- 77086, Vertebral fracture assessment via dual-energy X-ray absorptiometry (DXA).
Coding for breast ultrasound and tomosynthesis get more descriptive—at least for private insurance
The CPT Editorial Panel created three codes to describe digital breast tomosynthesis services and two new codes for a breast ultrasound.
- 77061, Digital breast tomosynthesis; unilateral
- 77062, Digital breast tomosynthesis; bilateral
- 77063, Screening digital breast tomosynthesis, bilateral (List separately in addition to the code for the primary procedure.)
- 76641, Ultrasound, breast, unilateral, real time with image documentation, including axilla when performed; complete
- 76642, Ultrasound, breast, unilateral, … ; limited.
Medicare, on the other hand, has decided to create a G code for tomosynthesis, which is the only code that will be accepted for payment if the patient meets her high-risk criteria for performance of this test.
Under Medicare rules you would report/order the following codes for mammographic services:
- Film (use CPT codes)
- 77056, Mammography; bilateral
- 77057, Screening mammography, bilateral (2-view film study of each breast)
- 2D digital (use G0202, G0204, and G0206)
- G0204, Diagnostic mammography, producing direct digital image, bilateral, all views
- G0206, Diagnostic mammography, producing direct digital image, unilateral, all views
- 3D screening (use G0202 for 2D digital plus the new CPT code 77063 for 3D)
procedure.)
- 3D diagnostic (use G0204 or G0206 for the 2D digital plus the new G code G0279 for 3D)
Modifier 59 becomes more specific
Another Medicare coding change that may affect ObGyns is the addition of new Medicare modifiers that are intended to eventually replace the modifier -59. This new list of modifiers will need to be appended to bundled procedures to more clearly explain why the secondary procedures should be paid separately. At the most recent American Medical Association (AMA) CPT symposium in Chicago, Illinois, CMS medical directors indicated that the new modifiers should be used only when the clinician is given instructions to do so by the carrier. Until then, the modifier -59 should continue to be used by most clinicians.
Here are the new modifiers, with an example of their use with currently bundled procedures that allow a modifier -59 to be used under certain circumstances:
- -XE: Separate encounter (A service that is distinct because it occurred during a separate encounter.) For instance, a patient presents to the office in the morning to have an abscess on her labia near her urethra incised and drained (56405). She returns in the afternoon to have a temporary catheter inserted because she states she cannot urinate and you decide to put in a temporary Foley catheter (51702) until the swelling has gone down. Add the modifier XE to 51702 to indicate it was performed at a different patient encounter.
- -XP: Separate practitioner (A service that is distinct because it was performed by a different practitioner.) Normally, Medicare will reimburse an unaffiliated clinician for performing a procedure that is bundled, since the bundling edits apply to the billing surgeon. But when two physicians from the same practice each are performing a different procedure at the same operative session that would otherwise be bundled, this new modifier will make that clear.
For example, Dr. Bates is performing a laparoscopic paravaginal defect repair (57423) and calls Dr. Clark, a urogynecologist in his practice, to remove severe adhesions from the ureters. The claim should go in under the same tax ID number, with the code 50715 listed first (as it has greater RVUs) and code 57423 reported with the -XP modifier.
- -XS: Separate structure (A service that is distinct because it was performed on a separate organ/structure.) Dr. Scott is performing the removal of endometrial implants around the left fallopian tube and in the cul-de-sac and notices that the right fallopian tube appears closed. He performs chromotubation on the right fallopian tube and notes that the right tube is blocked. Billing in this case would be 58662, 58350-XS.
- -XU: Unusual non-overlapping service (The use of a service that is distinct because it does not overlap usual components of the main service.) Mary has Medicare coverage and presents at 20 weeks 4 days gestation with bleeding and labor pains. Her examination shows bulging membranes that rupture when you attempt to remove the cerclage suture. You note a large rent in the cervix, but cannot get to the cerclage sutures as the patient is in active labor and beginning to bear down. The fetus and placenta are delivered a short time later through the rent in the cervix. You repair the rent in the cervix following delivery.
In this case, code 59400-52 (reduced services since the patient delivered at 20 weeks and there were reduced antepartum services), and 57720-XU because the repair of the cervix is not part of the usual services for a vaginal delivery.
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Moving forward with ICD-10: Capitalize on this extra time

Yes, we have been here before. Another day, another delay in implementing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). But, do not expect another postponement. If you are already conducting training sessions to move to the new system come next October, continue to do so. If you have not yet started, now is the time to start. ICD-10-CM is coming to your practice, and it will change everything.
“Why the switch?” you ask?
This change in our diagnostic coding system is required to allow coding for increased specificity in the reporting of diseases and recently recognized conditions as well as to maintain our status with respect to the rest of the world (which has been using ICD-10 for years). It also will be essential to use this coding system with the electronic medical record (EMR), so that meaningful use can be demonstrated more easily. Keep in mind that failure to show meaningful use will lead to penalties in the future. This new system offers improvements over ICD-9-CM in coding primary care encounters, external causes of injury, mental disorders, neoplasms, obstetric complications, and preventive health. It also allows physicians to demonstrate severity of illness in a way that is not possible with ICD-9-CM.
There will be 65,000 more codes than currently exist in ICD-9-CM. No physician will be able to keep all of these code numbers handy, but by making changes to clinician documentation and applying diagnostic coding guidelines correctly within the framework of the new system, the transition will not be onerous. And consider that, while the number of new codes is great, the number of codes used in the typical ObGyn practice will be a fraction of that number.
Related article: As ICD-10 conversion nears, keep these factors in mind to ensure proper reimbursements in 2014. Barbara S. Levy, MD (Audiocast, January 2014)
For ICD-10, documentation is paramount
The most important issue when considering overall coding and practice changes will be recognizing that clinician documentation will be the key to coding the highest level of specificity—and this high level of specificity may be required by most payers when deciding to reimburse for treatments rendered. Complete documentation sets the stage for the severity of illness and should in fact result in fewer denials for medical necessity.
For the new process to work efficiently, however, without a lot of delays due to coders and billers having to get more information from clinician offices before sending out claims, your understanding of and “buy-in” to the more clinically specific documentation will be essential.
To explain, under ICD-9-CM coding, simply documenting amenorrhea was acceptable. But when we switch to ICD-10-CM, documentation will need to specify whether the amenorrhea was primary or secondary. This more specific diagnostic coding will make a difference in the health statistics we collect. These data are used for research and to make decisions about allocation of resources—all essential components to excellent quality patient care.
The codes themselves will look different, which may be why some are resisting the change. Instead of the up to five digits required in ICD-9-CM, ICD-10-CM will require up to seven characters. All of the ICD-10-CM codes begin with a letter, may require a placeholder code of “x” as part of the code number, and the seventh character can be either a number or a letter. For instance, with some ICD-10-CM diagnoses reported by ObGyns, a seventh character might require documentation of the encounter as being initial, subsequent, or a sequel; in other cases, that seventh character will be used to identify which fetus has the problem identified by the diagnostic code.
Related article: The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century. Q&A with Barbara S. Levy, MD (Practice Management; February 2013)
Your understanding, although not a necessity, is best for all involved
In truth, most clinicians are not familiar with code formats and code numbers within our current ICD-9-CM code set. The expectation that you will suddenly become fluent in ICD-10-CM “code speak” is not realistic. But an understanding of the new codes in relation to documentation expectations will go a long way to making this transition as smooth as possible. For instance, when a patient currently presents reporting vaginal pain that is found to be due to erosion of a previously placed mesh, the code 628.31 (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue) is reported. But in ICD-10-CM, the documentation would need to include whether this was an initial encounter and the code would become T83.711A (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue, initial encounter).
Smart search. The good news is that most EMR products will have a “smart search” program available for clinicians to pick the correct code based on the search criteria. The bad news is that you will have to be a bit more exact in the search terms you use to make the process easy. For instance, the patient has pelvic pain but you search only on the term “pain.” That term by itself will result in about 100 codes to select from, and the order of the codes may mean that the correct code for pelvic pain is 25 codes down the list. However, if you instead search on the term “pelvic pain,” the one and only code for this condition will be listed and you can simply select it and move on.
Develop cheat sheets. Health-care professionals who are not using an EMR or some sort of computerized code search program will have a harder time, but the use of multiple paper “cheat sheets” for general gynecology, family planning, surgical cases, urology, infertility, obstetrics, etc., will ease that burden. Practice management staff can develop these forms, built on the codes that are currently being reported by the clinician. Place all of the options to replace the older code on the sheet so the correct selection can be made.
For instance, if the provider previously had reported vaginitis with one code, when we move to ICD-10-CM the code would expand to four code selections based on documentation of acute vaginitis, subacute and chronic vaginitis, acute vulvitis, or subacute and chronic vulvitis. If you only had documented vaginitis in the medical record, this gives you the opportunity to refine the documentation to something more specific that supports selection of the correct code and supports the medical need for management options.
Related article: Dos, don’ts, and dollars: Making the switch to an HER. Neil H. Baum, MD; Paul Kepper, MS. (Practice Management; November 2013)
Take advantage of the extra time
Now that we have a delay in the rollout, take this time to critically examine your documentation styles, and practice selecting ICD-10-CM codes before it counts toward payment or nonpayment of a claim. When the time comes, your practice will be fluent in the new system and there will be no delays in getting claims out the door or payment due to incorrect diagnostic coding. In other words, practice makes perfect.
In fact, some ObGyn practices that were ready for the new system have decided to switch to ICD-10-CM coding as of October 1, 2014. They will code each encounter by reporting both the ICD-9-CM code and the ICD-10-CM code on the revised CMS claim form or electronic billing format that permits dual diagnostic coding. This type of experience will ensure that all physicians and other health-care professionals in the practice have ample opportunity to improve their documentation and make any adjustments before the 2015 deadline.
Related article: The 2014 CPT and Medicare code changes affecting ObGyn practice. Melanie Witt, RN, CPC, COBGC, MA (Reimbursement Adviser; January 2014)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Yes, we have been here before. Another day, another delay in implementing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). But, do not expect another postponement. If you are already conducting training sessions to move to the new system come next October, continue to do so. If you have not yet started, now is the time to start. ICD-10-CM is coming to your practice, and it will change everything.
“Why the switch?” you ask?
This change in our diagnostic coding system is required to allow coding for increased specificity in the reporting of diseases and recently recognized conditions as well as to maintain our status with respect to the rest of the world (which has been using ICD-10 for years). It also will be essential to use this coding system with the electronic medical record (EMR), so that meaningful use can be demonstrated more easily. Keep in mind that failure to show meaningful use will lead to penalties in the future. This new system offers improvements over ICD-9-CM in coding primary care encounters, external causes of injury, mental disorders, neoplasms, obstetric complications, and preventive health. It also allows physicians to demonstrate severity of illness in a way that is not possible with ICD-9-CM.
There will be 65,000 more codes than currently exist in ICD-9-CM. No physician will be able to keep all of these code numbers handy, but by making changes to clinician documentation and applying diagnostic coding guidelines correctly within the framework of the new system, the transition will not be onerous. And consider that, while the number of new codes is great, the number of codes used in the typical ObGyn practice will be a fraction of that number.
Related article: As ICD-10 conversion nears, keep these factors in mind to ensure proper reimbursements in 2014. Barbara S. Levy, MD (Audiocast, January 2014)
For ICD-10, documentation is paramount
The most important issue when considering overall coding and practice changes will be recognizing that clinician documentation will be the key to coding the highest level of specificity—and this high level of specificity may be required by most payers when deciding to reimburse for treatments rendered. Complete documentation sets the stage for the severity of illness and should in fact result in fewer denials for medical necessity.
For the new process to work efficiently, however, without a lot of delays due to coders and billers having to get more information from clinician offices before sending out claims, your understanding of and “buy-in” to the more clinically specific documentation will be essential.
To explain, under ICD-9-CM coding, simply documenting amenorrhea was acceptable. But when we switch to ICD-10-CM, documentation will need to specify whether the amenorrhea was primary or secondary. This more specific diagnostic coding will make a difference in the health statistics we collect. These data are used for research and to make decisions about allocation of resources—all essential components to excellent quality patient care.
The codes themselves will look different, which may be why some are resisting the change. Instead of the up to five digits required in ICD-9-CM, ICD-10-CM will require up to seven characters. All of the ICD-10-CM codes begin with a letter, may require a placeholder code of “x” as part of the code number, and the seventh character can be either a number or a letter. For instance, with some ICD-10-CM diagnoses reported by ObGyns, a seventh character might require documentation of the encounter as being initial, subsequent, or a sequel; in other cases, that seventh character will be used to identify which fetus has the problem identified by the diagnostic code.
Related article: The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century. Q&A with Barbara S. Levy, MD (Practice Management; February 2013)
Your understanding, although not a necessity, is best for all involved
In truth, most clinicians are not familiar with code formats and code numbers within our current ICD-9-CM code set. The expectation that you will suddenly become fluent in ICD-10-CM “code speak” is not realistic. But an understanding of the new codes in relation to documentation expectations will go a long way to making this transition as smooth as possible. For instance, when a patient currently presents reporting vaginal pain that is found to be due to erosion of a previously placed mesh, the code 628.31 (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue) is reported. But in ICD-10-CM, the documentation would need to include whether this was an initial encounter and the code would become T83.711A (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue, initial encounter).
Smart search. The good news is that most EMR products will have a “smart search” program available for clinicians to pick the correct code based on the search criteria. The bad news is that you will have to be a bit more exact in the search terms you use to make the process easy. For instance, the patient has pelvic pain but you search only on the term “pain.” That term by itself will result in about 100 codes to select from, and the order of the codes may mean that the correct code for pelvic pain is 25 codes down the list. However, if you instead search on the term “pelvic pain,” the one and only code for this condition will be listed and you can simply select it and move on.
Develop cheat sheets. Health-care professionals who are not using an EMR or some sort of computerized code search program will have a harder time, but the use of multiple paper “cheat sheets” for general gynecology, family planning, surgical cases, urology, infertility, obstetrics, etc., will ease that burden. Practice management staff can develop these forms, built on the codes that are currently being reported by the clinician. Place all of the options to replace the older code on the sheet so the correct selection can be made.
For instance, if the provider previously had reported vaginitis with one code, when we move to ICD-10-CM the code would expand to four code selections based on documentation of acute vaginitis, subacute and chronic vaginitis, acute vulvitis, or subacute and chronic vulvitis. If you only had documented vaginitis in the medical record, this gives you the opportunity to refine the documentation to something more specific that supports selection of the correct code and supports the medical need for management options.
Related article: Dos, don’ts, and dollars: Making the switch to an HER. Neil H. Baum, MD; Paul Kepper, MS. (Practice Management; November 2013)
Take advantage of the extra time
Now that we have a delay in the rollout, take this time to critically examine your documentation styles, and practice selecting ICD-10-CM codes before it counts toward payment or nonpayment of a claim. When the time comes, your practice will be fluent in the new system and there will be no delays in getting claims out the door or payment due to incorrect diagnostic coding. In other words, practice makes perfect.
In fact, some ObGyn practices that were ready for the new system have decided to switch to ICD-10-CM coding as of October 1, 2014. They will code each encounter by reporting both the ICD-9-CM code and the ICD-10-CM code on the revised CMS claim form or electronic billing format that permits dual diagnostic coding. This type of experience will ensure that all physicians and other health-care professionals in the practice have ample opportunity to improve their documentation and make any adjustments before the 2015 deadline.
Related article: The 2014 CPT and Medicare code changes affecting ObGyn practice. Melanie Witt, RN, CPC, COBGC, MA (Reimbursement Adviser; January 2014)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
Yes, we have been here before. Another day, another delay in implementing International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). But, do not expect another postponement. If you are already conducting training sessions to move to the new system come next October, continue to do so. If you have not yet started, now is the time to start. ICD-10-CM is coming to your practice, and it will change everything.
“Why the switch?” you ask?
This change in our diagnostic coding system is required to allow coding for increased specificity in the reporting of diseases and recently recognized conditions as well as to maintain our status with respect to the rest of the world (which has been using ICD-10 for years). It also will be essential to use this coding system with the electronic medical record (EMR), so that meaningful use can be demonstrated more easily. Keep in mind that failure to show meaningful use will lead to penalties in the future. This new system offers improvements over ICD-9-CM in coding primary care encounters, external causes of injury, mental disorders, neoplasms, obstetric complications, and preventive health. It also allows physicians to demonstrate severity of illness in a way that is not possible with ICD-9-CM.
There will be 65,000 more codes than currently exist in ICD-9-CM. No physician will be able to keep all of these code numbers handy, but by making changes to clinician documentation and applying diagnostic coding guidelines correctly within the framework of the new system, the transition will not be onerous. And consider that, while the number of new codes is great, the number of codes used in the typical ObGyn practice will be a fraction of that number.
Related article: As ICD-10 conversion nears, keep these factors in mind to ensure proper reimbursements in 2014. Barbara S. Levy, MD (Audiocast, January 2014)
For ICD-10, documentation is paramount
The most important issue when considering overall coding and practice changes will be recognizing that clinician documentation will be the key to coding the highest level of specificity—and this high level of specificity may be required by most payers when deciding to reimburse for treatments rendered. Complete documentation sets the stage for the severity of illness and should in fact result in fewer denials for medical necessity.
For the new process to work efficiently, however, without a lot of delays due to coders and billers having to get more information from clinician offices before sending out claims, your understanding of and “buy-in” to the more clinically specific documentation will be essential.
To explain, under ICD-9-CM coding, simply documenting amenorrhea was acceptable. But when we switch to ICD-10-CM, documentation will need to specify whether the amenorrhea was primary or secondary. This more specific diagnostic coding will make a difference in the health statistics we collect. These data are used for research and to make decisions about allocation of resources—all essential components to excellent quality patient care.
The codes themselves will look different, which may be why some are resisting the change. Instead of the up to five digits required in ICD-9-CM, ICD-10-CM will require up to seven characters. All of the ICD-10-CM codes begin with a letter, may require a placeholder code of “x” as part of the code number, and the seventh character can be either a number or a letter. For instance, with some ICD-10-CM diagnoses reported by ObGyns, a seventh character might require documentation of the encounter as being initial, subsequent, or a sequel; in other cases, that seventh character will be used to identify which fetus has the problem identified by the diagnostic code.
Related article: The economics of surgical gynecology: How we can not only survive, but thrive, in the 21st Century. Q&A with Barbara S. Levy, MD (Practice Management; February 2013)
Your understanding, although not a necessity, is best for all involved
In truth, most clinicians are not familiar with code formats and code numbers within our current ICD-9-CM code set. The expectation that you will suddenly become fluent in ICD-10-CM “code speak” is not realistic. But an understanding of the new codes in relation to documentation expectations will go a long way to making this transition as smooth as possible. For instance, when a patient currently presents reporting vaginal pain that is found to be due to erosion of a previously placed mesh, the code 628.31 (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue) is reported. But in ICD-10-CM, the documentation would need to include whether this was an initial encounter and the code would become T83.711A (Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue, initial encounter).
Smart search. The good news is that most EMR products will have a “smart search” program available for clinicians to pick the correct code based on the search criteria. The bad news is that you will have to be a bit more exact in the search terms you use to make the process easy. For instance, the patient has pelvic pain but you search only on the term “pain.” That term by itself will result in about 100 codes to select from, and the order of the codes may mean that the correct code for pelvic pain is 25 codes down the list. However, if you instead search on the term “pelvic pain,” the one and only code for this condition will be listed and you can simply select it and move on.
Develop cheat sheets. Health-care professionals who are not using an EMR or some sort of computerized code search program will have a harder time, but the use of multiple paper “cheat sheets” for general gynecology, family planning, surgical cases, urology, infertility, obstetrics, etc., will ease that burden. Practice management staff can develop these forms, built on the codes that are currently being reported by the clinician. Place all of the options to replace the older code on the sheet so the correct selection can be made.
For instance, if the provider previously had reported vaginitis with one code, when we move to ICD-10-CM the code would expand to four code selections based on documentation of acute vaginitis, subacute and chronic vaginitis, acute vulvitis, or subacute and chronic vulvitis. If you only had documented vaginitis in the medical record, this gives you the opportunity to refine the documentation to something more specific that supports selection of the correct code and supports the medical need for management options.
Related article: Dos, don’ts, and dollars: Making the switch to an HER. Neil H. Baum, MD; Paul Kepper, MS. (Practice Management; November 2013)
Take advantage of the extra time
Now that we have a delay in the rollout, take this time to critically examine your documentation styles, and practice selecting ICD-10-CM codes before it counts toward payment or nonpayment of a claim. When the time comes, your practice will be fluent in the new system and there will be no delays in getting claims out the door or payment due to incorrect diagnostic coding. In other words, practice makes perfect.
In fact, some ObGyn practices that were ready for the new system have decided to switch to ICD-10-CM coding as of October 1, 2014. They will code each encounter by reporting both the ICD-9-CM code and the ICD-10-CM code on the revised CMS claim form or electronic billing format that permits dual diagnostic coding. This type of experience will ensure that all physicians and other health-care professionals in the practice have ample opportunity to improve their documentation and make any adjustments before the 2015 deadline.
Related article: The 2014 CPT and Medicare code changes affecting ObGyn practice. Melanie Witt, RN, CPC, COBGC, MA (Reimbursement Adviser; January 2014)
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]

The 2014 CPT and Medicare code changes affecting ObGyn practice
The code set of the 2014 Current Procedural Terminology (CPT), which took effect on January 1, includes several changes that affect all women’s health-care providers, including:
a clarification of who should bill discharge-day management
the addition of interprofessional telephone and Internet consultations
new codes for image-guided fluid drainage
new codes for fibroid embolization and laparoscopic ablation of fibroids.
There are also some new laboratory codes: one that captures the work of the noninvasive prenatal DNA test Harmony, and one to test for Trichomonas vaginalis. Finally, the code for anogenital examinations was revised to reflect current practice.
Medicare also has made some changes you should note, related to the levonorgestrel-releasing intrauterine system Skyla and billing for “incident to” services, and the type of provider who can order a fecal occult blood test. In addition, Medicare changes to some of the practice expense relative value units (RVUs) and geographic payment adjustor values will have an impact on some frequently used ObGyn services.
The changes to the CPT code set took effect January 1. Because of Health Insurance Portability and Accountability Act (HIPAA) requirements, insurers were required to accept new codes on that date.
CPT CODE CHANGES
Discharge-day management coding clarified
Codes 99238 and 99239 should be reported by the admitting provider for all services rendered on the date of discharge as long as the admission and discharge were not on the same date of service. Concurrent hospital services performed by the nonadmitting clinician on the date of discharge should be billed instead as a subsequent inpatient hospital encounter (codes 99231–99233).
Interprofessional phone and Web consultations now reimbursed
Most clinicians at one time or another end up giving advice to another health-care provider about the care of a patient he or she never sees and, up until 2014, there was no way to ask for reimbursement for this additional work. Starting on January 1, however, there were four new codes to allow a consultant clinician to report this work. These services, of a consulting physician who has specific specialty expertise, typically will be provided in complex or urgent situations where a timely face-to-face service with the patient may not be feasible.
The new codes are billed based on total documented cumulative time spent (to account for more than one telephone/Internet contact to complete the consultation request). The codes are for interprofessional telephone/Internet assessment and management service provided by a consultative physician including a verbal and written report to the patient’s treating/requesting physician or other qualified health-care professional, with varying time intervals for medical consultative discussion and review:
99446 5–10 minutes
99447 11–20 minutes
99448 21–30 minutes
99449 31 minutes or more
Like all new codes, these have some very specific requirements:
The billing physician cannot have had a face-to-face encounter with the patient within the past 14 days. If the consultation leads to scheduling a face-to-face appointment or surgery within 14 days, these codes cannot be reported.
If the consultation is to accept transfer of care or arrange for an immediate face-to-face encounter with the consulting physician, these codes should not be billed.
The documentation must include a review of all pertinent medical records, studies, medications, etc., that may be required to render an opinion on how to proceed with care of the patient, and reviewing of any data is not reported separately.
The patient either can be new to the consultant or can be established (with a new or an exacerbated problem).
The majority of the service (more than 50%) must be devoted to the medical consultative verbal/Internet real-time discussion, and not be reported more than once within a 7-day interval.
The request for advice by the qualified health-care professional must be documented in the patient’s medical record, including the reason for the request.
There must be a verbal opinion report and written report from the consultant to the treating physician.
The treating physician who asks for the telephone/Internet advice can report a prolonged services, non–face-to-face code if the time exceeds the typical time of a problem E/M service by 30 minutes to get credit for the discussion with the consultant.
CASE
As an example, Dr. Moody, Mary’s primary care physician, has ordered a computed tomography scan for her due to reports of sharp epigastric pain. A large mass in the area of the right ovary is detected. Dr. Moody phones Dr. Gerard, the patient’s ObGyn of record, for an opinion about additional testing for this mass. Mary was last seen by Dr. Gerard at her well-woman visit 8 months ago; there were no complaints reported or problems detected.
Dr. Gerard recommends that additional views of the mass be obtained and that a CA 125 test be performed due to Mary’s family history of ovarian cancer. He also recommends that Mary be sent for a consultation with a gynecologic oncologist as soon as possible. The total time spent on this consultation is 15 minutes, and Dr. Gerard reports Mary’s consultative session to her insurance company with CPT code 99447.
Image-guided drainage of a fluid collection
CPT code 10030 has been added to report image-guided drainage of a fluid collection using a catheter for areas just under the skin. This code would be used if the patient had an abscess, hematoma, seroma, lymphocele, or cyst that was drained percutaneously. For instance, this code could be reported for a hematoma located in the abdominal wall or just under the skin. The code bundles image guidance, but it can be reported more than once if there is more than one collection drained with a separate catheter.
CPT also has added additional codes for image-guided fluid collection drainage by catheter (eg, abscess, hematoma, seroma, lymphocele, cyst) of visceral, peritoneal, or retroperitoneal collections. The codes for these procedures are:
49405...; visceral (eg, kidney, liver, spleen, lung/mediastinum), percutaneous
49406...; peritoneal or retroperitoneal, percutaneous
49407...; peritoneal or retroperitoneal, transvaginal or transrectal
With the addition of these new codes, the old code 58823 has been eliminated.
Uterine fibroid treatment
There are two changes with regard to the treatment of uterine fibroids. First, CPT code 37210 (Uterine fibroid embolization [UFE, embolization of the uterine arteries to treat uterine fibroids, leiomyomata], percutaneous approach inclusive of vascular access, vessel selection, embolization, and all radiologic supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the procedure) has been eliminated and replaced by a more general code that will apply to any tumor or organ. This new code is 37243 (Vascular embolization or occlusion, inclusive of all radiological supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the intervention; for tumors, organ ischemia, or infarction).
Second, there is now a Category III code for the laparoscopic ablation of uterine fibroids: 0336T (Laparoscopy, surgical, ablation of uterine fibroid[s], including intraoperative ultrasound guidance and monitoring, radiofrequency). Clinical research has shown that radiofrequency ablation (RFA) is effective in treating fibroids, resolving associated symptoms in more than 80% of treated patients. Because RFA is not yet a standard of care, this Category III code must be reported in order for data on its use to be collected. Under CPT rules, you may not use an unlisted code in place of the Category III code for this procedure. If you are performing RFA, it may be considered experimental by some payers, but you can still make a case for payment with the submission of adequate documentation with the claim in the form of peer-reviewed articles and the patient’s circumstances that preclude more standard surgeries.
Anogenital examination coding
Code 99170 was revised to reflect current practice. The procedure is not always performed with a colposcope, but usually requires digital imaging for legal recoding and documentation. The revised code reads “anogenital examination, magnified, in childhood for suspected trauma, including image recording when performed.” Moderate sedation, if performed, may be billed separately using code 99143-99150.
LABORATORY CODE CHANGES
Cell-free DNA testing code added
As of January 1, there is a new code to report cell-free prenatal DNA testing to screen for fetal aneuploidy. This new code is 81507 (Fetal aneuploidy [trisomy 21, 18, and 13] DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy).
Related Article: Update on Obstetrics Jaimey Pauli, MD, and John T. Repke, MD (January 2014)
In addition, the code 84112, which used to be defined as “placental alpha microglobulin-1 (PAMG-1), cervicovaginal secretion, qualitative,” has been revised. The revision was done to make it clear that it can be ordered for other proteins that are tested in amniotic fluid. Code 84112 is now defined as follows: Evaluation of cervicovaginal fluid for specific amniotic fluid protein(s) (eg, placental alpha microglobulin-1 [PAMG-1], placental protein 12 [PP12], alpha-fetoprotein), qualitative, each specimen.
This test is normally ordered to determine whether the fetal membranes have ruptured, but this is not a Clinical Laboratory Improvement Amendments (CLIA) waived or Provider Performed Microscopy Procedures (PPMP) test. Therefore, only the laboratory with the applicable CLIA certificate can bill for it.
There are now two code options for T vaginalis testing
To the existing code 87660 (direct probe technique) is added the new code 87661, T vaginalis, amplified probe technique.
Three new codes for the flu vaccine:
90673, Flublok (effective January 2013)
90686, Fluzone, preservative-free (effective December 2012)
90688, FluLaval (effective August 2013)
In addition, Medicare has deleted code G2033, which was used to report Flublok. It will now accept the CPT code 90673 for this influenza product.
Keep in mind that reporting the administration of the influenza vaccine is different for Medicare than private payers. Administration code G0008 and diagnosis code V04.81 would be reported in conjunction with the appropriate vaccine code for Medicare, while CPT instructs you to report 90471 instead for the administration.
MEDICARE CODING CHANGES
Skyla. The new code is J7301, levonorgestrel-releasing intrauterine contraceptive, 13.5 mg. This replaces the temporary code Q0090, which was added by Medicare on July 1, 2013.
Related Article: 5 IUD myths dispelled Anne A. Moore, DNP, APN (September 2013)
More providers can order fecal occult blood tests. To expand access to screening fecal occult blood testing, Medicare has revised the rules on who can order these tests. Effective January 1, 2014, not only a physician but also the billing physician’s assistant (PA), certified nurse specialist (CNS), or nurse practitioner (NP) can order the test. But as before January 1, the physician, PA, CNS, or NP is responsible for using the results of the screening test in the overall management of the patient’s medical care.
“Incident to” providers must be state-licensed. Medicare recently became aware that it was being billed in several situations for ‘‘incident to’’ services that were provided by auxiliary personnel (rather than the physician or practitioner billing for the services) who did not meet the state standards for those services. For this reason, Medicare has revised the “incident to” rules to make it clear that the person who is assigned to provide the aspect of the service must be licensed within their state to provide the services performed.
SGR fate, and your reimbursement, unknown at this time
At the time this article was finalized, there was no information about the fate of the Medicare payment mechanism for 2014. If the sustained growth formula used to calculate the Medicare conversion factor for physician reimbursement is not fixed by Congress, the projected 2014 conversion factor will be $27.2006, a decrease from the current conversion factor of $34.023.
But even without concrete, final information on this complicating factor, changes to the geographic adjustment units (which in turn determine the payment allowance for physicians based on their practice location), as well as changes to the practice expense RVUs for such office procedures as urodynamic testing, may spell decreased payments in 2014 from Medicare or payers who use Medicare as the basis for reimbursement.
Some states will fare better than others. The geographic payment cost index for all but a handful of states will be adjusted downward. The good news is that if you practice in Alabama, Alaska, Colorado, Connecticut, Delaware, Louisiana, Minnesota, New Hampshire, New Mexico, New York, Virginia, certain areas of California (San Francisco, Los Angeles, Marin County), and the Washington DC area, your geographic factors will increase. This increase may offset any decrease in the RVUs.
ObGyn reimbursements hardest hit by decreased RVUs. The RVUs for 2014 for the technical component of all the urodynamic testing codes will be reduced by 6% to 40%, with the biggest hit coming to codes 51726-51727 (complex cystometrogram with urethral and voiding pressure studies). In-office procedures such as endometrial ablation, endometrial cryoablation, and hysteroscopic sterilization will see around an 8% decrease to the practice expense RVUs. This same reduction will be noticed in the technical-component reimbursement for gynecologic and obstetric ultrasounds, with the notable exception that the RVUs were increased for umbilical artery Doppler.
The final result for increased or decreased payments via the relative value system will therefore depend on your practice location, and whether you are billing the technical component only for many of these procedures (and, of course, the final outcome of the SGR). WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
The code set of the 2014 Current Procedural Terminology (CPT), which took effect on January 1, includes several changes that affect all women’s health-care providers, including:
a clarification of who should bill discharge-day management
the addition of interprofessional telephone and Internet consultations
new codes for image-guided fluid drainage
new codes for fibroid embolization and laparoscopic ablation of fibroids.
There are also some new laboratory codes: one that captures the work of the noninvasive prenatal DNA test Harmony, and one to test for Trichomonas vaginalis. Finally, the code for anogenital examinations was revised to reflect current practice.
Medicare also has made some changes you should note, related to the levonorgestrel-releasing intrauterine system Skyla and billing for “incident to” services, and the type of provider who can order a fecal occult blood test. In addition, Medicare changes to some of the practice expense relative value units (RVUs) and geographic payment adjustor values will have an impact on some frequently used ObGyn services.
The changes to the CPT code set took effect January 1. Because of Health Insurance Portability and Accountability Act (HIPAA) requirements, insurers were required to accept new codes on that date.
CPT CODE CHANGES
Discharge-day management coding clarified
Codes 99238 and 99239 should be reported by the admitting provider for all services rendered on the date of discharge as long as the admission and discharge were not on the same date of service. Concurrent hospital services performed by the nonadmitting clinician on the date of discharge should be billed instead as a subsequent inpatient hospital encounter (codes 99231–99233).
Interprofessional phone and Web consultations now reimbursed
Most clinicians at one time or another end up giving advice to another health-care provider about the care of a patient he or she never sees and, up until 2014, there was no way to ask for reimbursement for this additional work. Starting on January 1, however, there were four new codes to allow a consultant clinician to report this work. These services, of a consulting physician who has specific specialty expertise, typically will be provided in complex or urgent situations where a timely face-to-face service with the patient may not be feasible.
The new codes are billed based on total documented cumulative time spent (to account for more than one telephone/Internet contact to complete the consultation request). The codes are for interprofessional telephone/Internet assessment and management service provided by a consultative physician including a verbal and written report to the patient’s treating/requesting physician or other qualified health-care professional, with varying time intervals for medical consultative discussion and review:
99446 5–10 minutes
99447 11–20 minutes
99448 21–30 minutes
99449 31 minutes or more
Like all new codes, these have some very specific requirements:
The billing physician cannot have had a face-to-face encounter with the patient within the past 14 days. If the consultation leads to scheduling a face-to-face appointment or surgery within 14 days, these codes cannot be reported.
If the consultation is to accept transfer of care or arrange for an immediate face-to-face encounter with the consulting physician, these codes should not be billed.
The documentation must include a review of all pertinent medical records, studies, medications, etc., that may be required to render an opinion on how to proceed with care of the patient, and reviewing of any data is not reported separately.
The patient either can be new to the consultant or can be established (with a new or an exacerbated problem).
The majority of the service (more than 50%) must be devoted to the medical consultative verbal/Internet real-time discussion, and not be reported more than once within a 7-day interval.
The request for advice by the qualified health-care professional must be documented in the patient’s medical record, including the reason for the request.
There must be a verbal opinion report and written report from the consultant to the treating physician.
The treating physician who asks for the telephone/Internet advice can report a prolonged services, non–face-to-face code if the time exceeds the typical time of a problem E/M service by 30 minutes to get credit for the discussion with the consultant.
CASE
As an example, Dr. Moody, Mary’s primary care physician, has ordered a computed tomography scan for her due to reports of sharp epigastric pain. A large mass in the area of the right ovary is detected. Dr. Moody phones Dr. Gerard, the patient’s ObGyn of record, for an opinion about additional testing for this mass. Mary was last seen by Dr. Gerard at her well-woman visit 8 months ago; there were no complaints reported or problems detected.
Dr. Gerard recommends that additional views of the mass be obtained and that a CA 125 test be performed due to Mary’s family history of ovarian cancer. He also recommends that Mary be sent for a consultation with a gynecologic oncologist as soon as possible. The total time spent on this consultation is 15 minutes, and Dr. Gerard reports Mary’s consultative session to her insurance company with CPT code 99447.
Image-guided drainage of a fluid collection
CPT code 10030 has been added to report image-guided drainage of a fluid collection using a catheter for areas just under the skin. This code would be used if the patient had an abscess, hematoma, seroma, lymphocele, or cyst that was drained percutaneously. For instance, this code could be reported for a hematoma located in the abdominal wall or just under the skin. The code bundles image guidance, but it can be reported more than once if there is more than one collection drained with a separate catheter.
CPT also has added additional codes for image-guided fluid collection drainage by catheter (eg, abscess, hematoma, seroma, lymphocele, cyst) of visceral, peritoneal, or retroperitoneal collections. The codes for these procedures are:
49405...; visceral (eg, kidney, liver, spleen, lung/mediastinum), percutaneous
49406...; peritoneal or retroperitoneal, percutaneous
49407...; peritoneal or retroperitoneal, transvaginal or transrectal
With the addition of these new codes, the old code 58823 has been eliminated.
Uterine fibroid treatment
There are two changes with regard to the treatment of uterine fibroids. First, CPT code 37210 (Uterine fibroid embolization [UFE, embolization of the uterine arteries to treat uterine fibroids, leiomyomata], percutaneous approach inclusive of vascular access, vessel selection, embolization, and all radiologic supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the procedure) has been eliminated and replaced by a more general code that will apply to any tumor or organ. This new code is 37243 (Vascular embolization or occlusion, inclusive of all radiological supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the intervention; for tumors, organ ischemia, or infarction).
Second, there is now a Category III code for the laparoscopic ablation of uterine fibroids: 0336T (Laparoscopy, surgical, ablation of uterine fibroid[s], including intraoperative ultrasound guidance and monitoring, radiofrequency). Clinical research has shown that radiofrequency ablation (RFA) is effective in treating fibroids, resolving associated symptoms in more than 80% of treated patients. Because RFA is not yet a standard of care, this Category III code must be reported in order for data on its use to be collected. Under CPT rules, you may not use an unlisted code in place of the Category III code for this procedure. If you are performing RFA, it may be considered experimental by some payers, but you can still make a case for payment with the submission of adequate documentation with the claim in the form of peer-reviewed articles and the patient’s circumstances that preclude more standard surgeries.
Anogenital examination coding
Code 99170 was revised to reflect current practice. The procedure is not always performed with a colposcope, but usually requires digital imaging for legal recoding and documentation. The revised code reads “anogenital examination, magnified, in childhood for suspected trauma, including image recording when performed.” Moderate sedation, if performed, may be billed separately using code 99143-99150.
LABORATORY CODE CHANGES
Cell-free DNA testing code added
As of January 1, there is a new code to report cell-free prenatal DNA testing to screen for fetal aneuploidy. This new code is 81507 (Fetal aneuploidy [trisomy 21, 18, and 13] DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy).
Related Article: Update on Obstetrics Jaimey Pauli, MD, and John T. Repke, MD (January 2014)
In addition, the code 84112, which used to be defined as “placental alpha microglobulin-1 (PAMG-1), cervicovaginal secretion, qualitative,” has been revised. The revision was done to make it clear that it can be ordered for other proteins that are tested in amniotic fluid. Code 84112 is now defined as follows: Evaluation of cervicovaginal fluid for specific amniotic fluid protein(s) (eg, placental alpha microglobulin-1 [PAMG-1], placental protein 12 [PP12], alpha-fetoprotein), qualitative, each specimen.
This test is normally ordered to determine whether the fetal membranes have ruptured, but this is not a Clinical Laboratory Improvement Amendments (CLIA) waived or Provider Performed Microscopy Procedures (PPMP) test. Therefore, only the laboratory with the applicable CLIA certificate can bill for it.
There are now two code options for T vaginalis testing
To the existing code 87660 (direct probe technique) is added the new code 87661, T vaginalis, amplified probe technique.
Three new codes for the flu vaccine:
90673, Flublok (effective January 2013)
90686, Fluzone, preservative-free (effective December 2012)
90688, FluLaval (effective August 2013)
In addition, Medicare has deleted code G2033, which was used to report Flublok. It will now accept the CPT code 90673 for this influenza product.
Keep in mind that reporting the administration of the influenza vaccine is different for Medicare than private payers. Administration code G0008 and diagnosis code V04.81 would be reported in conjunction with the appropriate vaccine code for Medicare, while CPT instructs you to report 90471 instead for the administration.
MEDICARE CODING CHANGES
Skyla. The new code is J7301, levonorgestrel-releasing intrauterine contraceptive, 13.5 mg. This replaces the temporary code Q0090, which was added by Medicare on July 1, 2013.
Related Article: 5 IUD myths dispelled Anne A. Moore, DNP, APN (September 2013)
More providers can order fecal occult blood tests. To expand access to screening fecal occult blood testing, Medicare has revised the rules on who can order these tests. Effective January 1, 2014, not only a physician but also the billing physician’s assistant (PA), certified nurse specialist (CNS), or nurse practitioner (NP) can order the test. But as before January 1, the physician, PA, CNS, or NP is responsible for using the results of the screening test in the overall management of the patient’s medical care.
“Incident to” providers must be state-licensed. Medicare recently became aware that it was being billed in several situations for ‘‘incident to’’ services that were provided by auxiliary personnel (rather than the physician or practitioner billing for the services) who did not meet the state standards for those services. For this reason, Medicare has revised the “incident to” rules to make it clear that the person who is assigned to provide the aspect of the service must be licensed within their state to provide the services performed.
SGR fate, and your reimbursement, unknown at this time
At the time this article was finalized, there was no information about the fate of the Medicare payment mechanism for 2014. If the sustained growth formula used to calculate the Medicare conversion factor for physician reimbursement is not fixed by Congress, the projected 2014 conversion factor will be $27.2006, a decrease from the current conversion factor of $34.023.
But even without concrete, final information on this complicating factor, changes to the geographic adjustment units (which in turn determine the payment allowance for physicians based on their practice location), as well as changes to the practice expense RVUs for such office procedures as urodynamic testing, may spell decreased payments in 2014 from Medicare or payers who use Medicare as the basis for reimbursement.
Some states will fare better than others. The geographic payment cost index for all but a handful of states will be adjusted downward. The good news is that if you practice in Alabama, Alaska, Colorado, Connecticut, Delaware, Louisiana, Minnesota, New Hampshire, New Mexico, New York, Virginia, certain areas of California (San Francisco, Los Angeles, Marin County), and the Washington DC area, your geographic factors will increase. This increase may offset any decrease in the RVUs.
ObGyn reimbursements hardest hit by decreased RVUs. The RVUs for 2014 for the technical component of all the urodynamic testing codes will be reduced by 6% to 40%, with the biggest hit coming to codes 51726-51727 (complex cystometrogram with urethral and voiding pressure studies). In-office procedures such as endometrial ablation, endometrial cryoablation, and hysteroscopic sterilization will see around an 8% decrease to the practice expense RVUs. This same reduction will be noticed in the technical-component reimbursement for gynecologic and obstetric ultrasounds, with the notable exception that the RVUs were increased for umbilical artery Doppler.
The final result for increased or decreased payments via the relative value system will therefore depend on your practice location, and whether you are billing the technical component only for many of these procedures (and, of course, the final outcome of the SGR). WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
The code set of the 2014 Current Procedural Terminology (CPT), which took effect on January 1, includes several changes that affect all women’s health-care providers, including:
a clarification of who should bill discharge-day management
the addition of interprofessional telephone and Internet consultations
new codes for image-guided fluid drainage
new codes for fibroid embolization and laparoscopic ablation of fibroids.
There are also some new laboratory codes: one that captures the work of the noninvasive prenatal DNA test Harmony, and one to test for Trichomonas vaginalis. Finally, the code for anogenital examinations was revised to reflect current practice.
Medicare also has made some changes you should note, related to the levonorgestrel-releasing intrauterine system Skyla and billing for “incident to” services, and the type of provider who can order a fecal occult blood test. In addition, Medicare changes to some of the practice expense relative value units (RVUs) and geographic payment adjustor values will have an impact on some frequently used ObGyn services.
The changes to the CPT code set took effect January 1. Because of Health Insurance Portability and Accountability Act (HIPAA) requirements, insurers were required to accept new codes on that date.
CPT CODE CHANGES
Discharge-day management coding clarified
Codes 99238 and 99239 should be reported by the admitting provider for all services rendered on the date of discharge as long as the admission and discharge were not on the same date of service. Concurrent hospital services performed by the nonadmitting clinician on the date of discharge should be billed instead as a subsequent inpatient hospital encounter (codes 99231–99233).
Interprofessional phone and Web consultations now reimbursed
Most clinicians at one time or another end up giving advice to another health-care provider about the care of a patient he or she never sees and, up until 2014, there was no way to ask for reimbursement for this additional work. Starting on January 1, however, there were four new codes to allow a consultant clinician to report this work. These services, of a consulting physician who has specific specialty expertise, typically will be provided in complex or urgent situations where a timely face-to-face service with the patient may not be feasible.
The new codes are billed based on total documented cumulative time spent (to account for more than one telephone/Internet contact to complete the consultation request). The codes are for interprofessional telephone/Internet assessment and management service provided by a consultative physician including a verbal and written report to the patient’s treating/requesting physician or other qualified health-care professional, with varying time intervals for medical consultative discussion and review:
99446 5–10 minutes
99447 11–20 minutes
99448 21–30 minutes
99449 31 minutes or more
Like all new codes, these have some very specific requirements:
The billing physician cannot have had a face-to-face encounter with the patient within the past 14 days. If the consultation leads to scheduling a face-to-face appointment or surgery within 14 days, these codes cannot be reported.
If the consultation is to accept transfer of care or arrange for an immediate face-to-face encounter with the consulting physician, these codes should not be billed.
The documentation must include a review of all pertinent medical records, studies, medications, etc., that may be required to render an opinion on how to proceed with care of the patient, and reviewing of any data is not reported separately.
The patient either can be new to the consultant or can be established (with a new or an exacerbated problem).
The majority of the service (more than 50%) must be devoted to the medical consultative verbal/Internet real-time discussion, and not be reported more than once within a 7-day interval.
The request for advice by the qualified health-care professional must be documented in the patient’s medical record, including the reason for the request.
There must be a verbal opinion report and written report from the consultant to the treating physician.
The treating physician who asks for the telephone/Internet advice can report a prolonged services, non–face-to-face code if the time exceeds the typical time of a problem E/M service by 30 minutes to get credit for the discussion with the consultant.
CASE
As an example, Dr. Moody, Mary’s primary care physician, has ordered a computed tomography scan for her due to reports of sharp epigastric pain. A large mass in the area of the right ovary is detected. Dr. Moody phones Dr. Gerard, the patient’s ObGyn of record, for an opinion about additional testing for this mass. Mary was last seen by Dr. Gerard at her well-woman visit 8 months ago; there were no complaints reported or problems detected.
Dr. Gerard recommends that additional views of the mass be obtained and that a CA 125 test be performed due to Mary’s family history of ovarian cancer. He also recommends that Mary be sent for a consultation with a gynecologic oncologist as soon as possible. The total time spent on this consultation is 15 minutes, and Dr. Gerard reports Mary’s consultative session to her insurance company with CPT code 99447.
Image-guided drainage of a fluid collection
CPT code 10030 has been added to report image-guided drainage of a fluid collection using a catheter for areas just under the skin. This code would be used if the patient had an abscess, hematoma, seroma, lymphocele, or cyst that was drained percutaneously. For instance, this code could be reported for a hematoma located in the abdominal wall or just under the skin. The code bundles image guidance, but it can be reported more than once if there is more than one collection drained with a separate catheter.
CPT also has added additional codes for image-guided fluid collection drainage by catheter (eg, abscess, hematoma, seroma, lymphocele, cyst) of visceral, peritoneal, or retroperitoneal collections. The codes for these procedures are:
49405...; visceral (eg, kidney, liver, spleen, lung/mediastinum), percutaneous
49406...; peritoneal or retroperitoneal, percutaneous
49407...; peritoneal or retroperitoneal, transvaginal or transrectal
With the addition of these new codes, the old code 58823 has been eliminated.
Uterine fibroid treatment
There are two changes with regard to the treatment of uterine fibroids. First, CPT code 37210 (Uterine fibroid embolization [UFE, embolization of the uterine arteries to treat uterine fibroids, leiomyomata], percutaneous approach inclusive of vascular access, vessel selection, embolization, and all radiologic supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the procedure) has been eliminated and replaced by a more general code that will apply to any tumor or organ. This new code is 37243 (Vascular embolization or occlusion, inclusive of all radiological supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the intervention; for tumors, organ ischemia, or infarction).
Second, there is now a Category III code for the laparoscopic ablation of uterine fibroids: 0336T (Laparoscopy, surgical, ablation of uterine fibroid[s], including intraoperative ultrasound guidance and monitoring, radiofrequency). Clinical research has shown that radiofrequency ablation (RFA) is effective in treating fibroids, resolving associated symptoms in more than 80% of treated patients. Because RFA is not yet a standard of care, this Category III code must be reported in order for data on its use to be collected. Under CPT rules, you may not use an unlisted code in place of the Category III code for this procedure. If you are performing RFA, it may be considered experimental by some payers, but you can still make a case for payment with the submission of adequate documentation with the claim in the form of peer-reviewed articles and the patient’s circumstances that preclude more standard surgeries.
Anogenital examination coding
Code 99170 was revised to reflect current practice. The procedure is not always performed with a colposcope, but usually requires digital imaging for legal recoding and documentation. The revised code reads “anogenital examination, magnified, in childhood for suspected trauma, including image recording when performed.” Moderate sedation, if performed, may be billed separately using code 99143-99150.
LABORATORY CODE CHANGES
Cell-free DNA testing code added
As of January 1, there is a new code to report cell-free prenatal DNA testing to screen for fetal aneuploidy. This new code is 81507 (Fetal aneuploidy [trisomy 21, 18, and 13] DNA sequence analysis of selected regions using maternal plasma, algorithm reported as a risk score for each trisomy).
Related Article: Update on Obstetrics Jaimey Pauli, MD, and John T. Repke, MD (January 2014)
In addition, the code 84112, which used to be defined as “placental alpha microglobulin-1 (PAMG-1), cervicovaginal secretion, qualitative,” has been revised. The revision was done to make it clear that it can be ordered for other proteins that are tested in amniotic fluid. Code 84112 is now defined as follows: Evaluation of cervicovaginal fluid for specific amniotic fluid protein(s) (eg, placental alpha microglobulin-1 [PAMG-1], placental protein 12 [PP12], alpha-fetoprotein), qualitative, each specimen.
This test is normally ordered to determine whether the fetal membranes have ruptured, but this is not a Clinical Laboratory Improvement Amendments (CLIA) waived or Provider Performed Microscopy Procedures (PPMP) test. Therefore, only the laboratory with the applicable CLIA certificate can bill for it.
There are now two code options for T vaginalis testing
To the existing code 87660 (direct probe technique) is added the new code 87661, T vaginalis, amplified probe technique.
Three new codes for the flu vaccine:
90673, Flublok (effective January 2013)
90686, Fluzone, preservative-free (effective December 2012)
90688, FluLaval (effective August 2013)
In addition, Medicare has deleted code G2033, which was used to report Flublok. It will now accept the CPT code 90673 for this influenza product.
Keep in mind that reporting the administration of the influenza vaccine is different for Medicare than private payers. Administration code G0008 and diagnosis code V04.81 would be reported in conjunction with the appropriate vaccine code for Medicare, while CPT instructs you to report 90471 instead for the administration.
MEDICARE CODING CHANGES
Skyla. The new code is J7301, levonorgestrel-releasing intrauterine contraceptive, 13.5 mg. This replaces the temporary code Q0090, which was added by Medicare on July 1, 2013.
Related Article: 5 IUD myths dispelled Anne A. Moore, DNP, APN (September 2013)
More providers can order fecal occult blood tests. To expand access to screening fecal occult blood testing, Medicare has revised the rules on who can order these tests. Effective January 1, 2014, not only a physician but also the billing physician’s assistant (PA), certified nurse specialist (CNS), or nurse practitioner (NP) can order the test. But as before January 1, the physician, PA, CNS, or NP is responsible for using the results of the screening test in the overall management of the patient’s medical care.
“Incident to” providers must be state-licensed. Medicare recently became aware that it was being billed in several situations for ‘‘incident to’’ services that were provided by auxiliary personnel (rather than the physician or practitioner billing for the services) who did not meet the state standards for those services. For this reason, Medicare has revised the “incident to” rules to make it clear that the person who is assigned to provide the aspect of the service must be licensed within their state to provide the services performed.
SGR fate, and your reimbursement, unknown at this time
At the time this article was finalized, there was no information about the fate of the Medicare payment mechanism for 2014. If the sustained growth formula used to calculate the Medicare conversion factor for physician reimbursement is not fixed by Congress, the projected 2014 conversion factor will be $27.2006, a decrease from the current conversion factor of $34.023.
But even without concrete, final information on this complicating factor, changes to the geographic adjustment units (which in turn determine the payment allowance for physicians based on their practice location), as well as changes to the practice expense RVUs for such office procedures as urodynamic testing, may spell decreased payments in 2014 from Medicare or payers who use Medicare as the basis for reimbursement.
Some states will fare better than others. The geographic payment cost index for all but a handful of states will be adjusted downward. The good news is that if you practice in Alabama, Alaska, Colorado, Connecticut, Delaware, Louisiana, Minnesota, New Hampshire, New Mexico, New York, Virginia, certain areas of California (San Francisco, Los Angeles, Marin County), and the Washington DC area, your geographic factors will increase. This increase may offset any decrease in the RVUs.
ObGyn reimbursements hardest hit by decreased RVUs. The RVUs for 2014 for the technical component of all the urodynamic testing codes will be reduced by 6% to 40%, with the biggest hit coming to codes 51726-51727 (complex cystometrogram with urethral and voiding pressure studies). In-office procedures such as endometrial ablation, endometrial cryoablation, and hysteroscopic sterilization will see around an 8% decrease to the practice expense RVUs. This same reduction will be noticed in the technical-component reimbursement for gynecologic and obstetric ultrasounds, with the notable exception that the RVUs were increased for umbilical artery Doppler.
The final result for increased or decreased payments via the relative value system will therefore depend on your practice location, and whether you are billing the technical component only for many of these procedures (and, of course, the final outcome of the SGR). WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: [email protected]
WATCH for Melanie Witt’s update on ICD-10 conversion ahead of its official release date later this year.

The new year brings refinements to CPT and Medicare codes
Ms. Witt reports no financial relationships relevant to this article.
Among changes to Current Procedural Terminology (CPT) that took effect on January 1 are several of interest to our specialty:
- the addition of “typical” times to the evaluation and management (E/M) codes for same-day admission and discharge
- a new code for bladder injection
- bundling of imaging guidance associated with percutaneous implantation of a neurostimulator electrode array, if performed, using code 64561, Percutaneous implantation of neurostimulator electrode array; sacral nerve (transforaminal placement).
In addition, CPT made it clear that all E/M codes can be reported by qualified nonphysician health-care providers, as well as physicians. As for Medicare, coding for administration of depot medroxyprogesterone acetate (Depo-Provera) has been modified, as has the billing process for interpretation of ultrasonography performed outside of the office.
Because of requirements in the Health Insurance Portability and Accountability Act (HIPAA), insurers were required to accept the new codes and revisions on January 1.
Providers can now characterize their level of service by how long it took to provide
As I mentioned, typical times have been added to the set of observation and inpatient care codes that involve admission and discharge on the same date of service. Until now, these codes did not have a pre-assigned typical time, and the provider had to select the level of service based solely on three key components: history, examination, and medical decision-making. The addition of times allows the provider to select the level of service based on counseling or coordination of care, if that activity dominated the visit.
The typical times are:
- 99234, 40 minutes
- 99235, 50 minutes
- 99236, 55 minutes.
Chemodenervation of the bladder gets its own code
A new code, 52287, cystourethroscopy, with injection(s) for chemodenervation of the bladder, has been added to CPT. This procedure is performed to treat idiopathic overactive bladder that can’t be managed any other way. It typically involves the injection of botulinum. Before January 1, this procedure was reported using codes 52000 and 64614, but this approach represented an inexact match.
Payers will be looking closely at diagnostic coding for this procedure. The most frequently accepted diagnostic codes are:
- 596.51, hypertonicity of bladder
- 596.54, neurogenic bladder NOS
- 596.55, detrusor sphincter dyssynergia
- 596.59, other functional disorder of bladder
- 788.41, urinary frequency.
Because costs will vary, depending on the chemotoxin used, the agent may be reported separately using the descriptive “J” code or another Medicare-designated alphanumeric code, such as J0585, injection of botulinum toxin type A, 1 unit.
Qualified providers now include nonphysicians as well as physicians
CPT has clarified that all E/M codes can be reported not only by physicians but by qualified nonphysicians as well.
CPT also changed wording in each of the codes so that the use of counseling time applies to all providers when counseling dominates the visit. In other words, if a payer allows someone other than a physician to provide and bill for a service, the CPT E/M codes can be used by all providers who qualify and have documented the service. These changes have no effect on the codes themselves.
Please note, however, that registered nurses and licensed practical nurses are not normally recognized as billing providers and will still be restricted to code 99211, Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician. Usually, with this code, presenting problems are minimal. Typically, 5 minutes are spent performing or supervising these services. This code is often referred to as the “nurse-only” code.
As a result of this clarification, references to physicians have been removed from CPT code 59300, Episiotomy or vaginal repair, by other than attending. This change signifies that this code may be reported by any qualified provider who did not perform the delivery or was not covering for a physician group who billed for the delivery.
Three new codes for the flu vaccine
Two of the new codes are CPT codes, and the other is for Medicare:
- 90653, Influenza vaccine, inactivated, subunit, adjuvanted, for intramuscular use
- 90672, Influenza virus vaccine, live, for intranasal use
- Q2034, Agriflu.
Keep in mind that the administration of the flu vaccine is reported differently for Medicare, compared with private payers. Administration code G0008 and diagnosis code V04.81 would be reported in conjunction with the appropriate vaccine code for Medicare. CPT requires that code 90471 be reported for administration.
CPT also revised all flu vaccine codes (90655–90660) to include the term “trivalent” to signify that all flu vaccines are made up of three strains of the virus.
Medicare refines billing for MPA administration
When billing for MPA or MPA in combination with estradiol, be aware that Medicare has eliminated the J codes for these drugs, replacing them with a single new code.
The deleted codes are:
- J1051, medroxyprogesterone acetate, 50 mg
- J1055, medroxyprogesterone acetate, 150 mg, for contraceptive use
- J1056, medroxyprogesterone acetate/ estradiol cypionate, 5 mg/25 mg.
The new code is J1050, medroxyprogesterone acetate, 1 mg. To use it, you must indicate the dosage as a quantity. For example, if you injected 150 mg, you would use code J1050 x 150 on the claim. The diagnosis code will indicate the reason for the injection—that is, medical treatment or contraception. In the event that the combination drug is being administered, separate billing of J1000, Injection, depo-estradiol cypionate, up to 5 mg, would need to be reported in addition to J1050.
Medicare has also issued a national policy on Place of Service (POS) billing because the office of the inspector general has found that physicians and other suppliers frequently report an incorrect POS, and Medicare pays more for some sites. Medicare rules for the billing of POS for the professional component of an imaging service are changing, effective April 1, 2013. This rule was postponed from its original date of October 1, 2012. Under this rule, when the professional and technical components of a service are performed in different locations, the appropriate POS to report for the interpretive aspect is the location where the technical component was performed. This change would apply to an ObGyn practice that contracts out for the technical component of an ultrasound but performs the interpretation in the office. In that case, the POS should not be listed as “office” or POS 11, but should match the POS of the imaging contractor.
We want to hear from you! Tell us what you think.
Ms. Witt reports no financial relationships relevant to this article.
Among changes to Current Procedural Terminology (CPT) that took effect on January 1 are several of interest to our specialty:
- the addition of “typical” times to the evaluation and management (E/M) codes for same-day admission and discharge
- a new code for bladder injection
- bundling of imaging guidance associated with percutaneous implantation of a neurostimulator electrode array, if performed, using code 64561, Percutaneous implantation of neurostimulator electrode array; sacral nerve (transforaminal placement).
In addition, CPT made it clear that all E/M codes can be reported by qualified nonphysician health-care providers, as well as physicians. As for Medicare, coding for administration of depot medroxyprogesterone acetate (Depo-Provera) has been modified, as has the billing process for interpretation of ultrasonography performed outside of the office.
Because of requirements in the Health Insurance Portability and Accountability Act (HIPAA), insurers were required to accept the new codes and revisions on January 1.
Providers can now characterize their level of service by how long it took to provide
As I mentioned, typical times have been added to the set of observation and inpatient care codes that involve admission and discharge on the same date of service. Until now, these codes did not have a pre-assigned typical time, and the provider had to select the level of service based solely on three key components: history, examination, and medical decision-making. The addition of times allows the provider to select the level of service based on counseling or coordination of care, if that activity dominated the visit.
The typical times are:
- 99234, 40 minutes
- 99235, 50 minutes
- 99236, 55 minutes.
Chemodenervation of the bladder gets its own code
A new code, 52287, cystourethroscopy, with injection(s) for chemodenervation of the bladder, has been added to CPT. This procedure is performed to treat idiopathic overactive bladder that can’t be managed any other way. It typically involves the injection of botulinum. Before January 1, this procedure was reported using codes 52000 and 64614, but this approach represented an inexact match.
Payers will be looking closely at diagnostic coding for this procedure. The most frequently accepted diagnostic codes are:
- 596.51, hypertonicity of bladder
- 596.54, neurogenic bladder NOS
- 596.55, detrusor sphincter dyssynergia
- 596.59, other functional disorder of bladder
- 788.41, urinary frequency.
Because costs will vary, depending on the chemotoxin used, the agent may be reported separately using the descriptive “J” code or another Medicare-designated alphanumeric code, such as J0585, injection of botulinum toxin type A, 1 unit.
Qualified providers now include nonphysicians as well as physicians
CPT has clarified that all E/M codes can be reported not only by physicians but by qualified nonphysicians as well.
CPT also changed wording in each of the codes so that the use of counseling time applies to all providers when counseling dominates the visit. In other words, if a payer allows someone other than a physician to provide and bill for a service, the CPT E/M codes can be used by all providers who qualify and have documented the service. These changes have no effect on the codes themselves.
Please note, however, that registered nurses and licensed practical nurses are not normally recognized as billing providers and will still be restricted to code 99211, Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician. Usually, with this code, presenting problems are minimal. Typically, 5 minutes are spent performing or supervising these services. This code is often referred to as the “nurse-only” code.
As a result of this clarification, references to physicians have been removed from CPT code 59300, Episiotomy or vaginal repair, by other than attending. This change signifies that this code may be reported by any qualified provider who did not perform the delivery or was not covering for a physician group who billed for the delivery.
Three new codes for the flu vaccine
Two of the new codes are CPT codes, and the other is for Medicare:
- 90653, Influenza vaccine, inactivated, subunit, adjuvanted, for intramuscular use
- 90672, Influenza virus vaccine, live, for intranasal use
- Q2034, Agriflu.
Keep in mind that the administration of the flu vaccine is reported differently for Medicare, compared with private payers. Administration code G0008 and diagnosis code V04.81 would be reported in conjunction with the appropriate vaccine code for Medicare. CPT requires that code 90471 be reported for administration.
CPT also revised all flu vaccine codes (90655–90660) to include the term “trivalent” to signify that all flu vaccines are made up of three strains of the virus.
Medicare refines billing for MPA administration
When billing for MPA or MPA in combination with estradiol, be aware that Medicare has eliminated the J codes for these drugs, replacing them with a single new code.
The deleted codes are:
- J1051, medroxyprogesterone acetate, 50 mg
- J1055, medroxyprogesterone acetate, 150 mg, for contraceptive use
- J1056, medroxyprogesterone acetate/ estradiol cypionate, 5 mg/25 mg.
The new code is J1050, medroxyprogesterone acetate, 1 mg. To use it, you must indicate the dosage as a quantity. For example, if you injected 150 mg, you would use code J1050 x 150 on the claim. The diagnosis code will indicate the reason for the injection—that is, medical treatment or contraception. In the event that the combination drug is being administered, separate billing of J1000, Injection, depo-estradiol cypionate, up to 5 mg, would need to be reported in addition to J1050.
Medicare has also issued a national policy on Place of Service (POS) billing because the office of the inspector general has found that physicians and other suppliers frequently report an incorrect POS, and Medicare pays more for some sites. Medicare rules for the billing of POS for the professional component of an imaging service are changing, effective April 1, 2013. This rule was postponed from its original date of October 1, 2012. Under this rule, when the professional and technical components of a service are performed in different locations, the appropriate POS to report for the interpretive aspect is the location where the technical component was performed. This change would apply to an ObGyn practice that contracts out for the technical component of an ultrasound but performs the interpretation in the office. In that case, the POS should not be listed as “office” or POS 11, but should match the POS of the imaging contractor.
We want to hear from you! Tell us what you think.
Ms. Witt reports no financial relationships relevant to this article.
Among changes to Current Procedural Terminology (CPT) that took effect on January 1 are several of interest to our specialty:
- the addition of “typical” times to the evaluation and management (E/M) codes for same-day admission and discharge
- a new code for bladder injection
- bundling of imaging guidance associated with percutaneous implantation of a neurostimulator electrode array, if performed, using code 64561, Percutaneous implantation of neurostimulator electrode array; sacral nerve (transforaminal placement).
In addition, CPT made it clear that all E/M codes can be reported by qualified nonphysician health-care providers, as well as physicians. As for Medicare, coding for administration of depot medroxyprogesterone acetate (Depo-Provera) has been modified, as has the billing process for interpretation of ultrasonography performed outside of the office.
Because of requirements in the Health Insurance Portability and Accountability Act (HIPAA), insurers were required to accept the new codes and revisions on January 1.
Providers can now characterize their level of service by how long it took to provide
As I mentioned, typical times have been added to the set of observation and inpatient care codes that involve admission and discharge on the same date of service. Until now, these codes did not have a pre-assigned typical time, and the provider had to select the level of service based solely on three key components: history, examination, and medical decision-making. The addition of times allows the provider to select the level of service based on counseling or coordination of care, if that activity dominated the visit.
The typical times are:
- 99234, 40 minutes
- 99235, 50 minutes
- 99236, 55 minutes.
Chemodenervation of the bladder gets its own code
A new code, 52287, cystourethroscopy, with injection(s) for chemodenervation of the bladder, has been added to CPT. This procedure is performed to treat idiopathic overactive bladder that can’t be managed any other way. It typically involves the injection of botulinum. Before January 1, this procedure was reported using codes 52000 and 64614, but this approach represented an inexact match.
Payers will be looking closely at diagnostic coding for this procedure. The most frequently accepted diagnostic codes are:
- 596.51, hypertonicity of bladder
- 596.54, neurogenic bladder NOS
- 596.55, detrusor sphincter dyssynergia
- 596.59, other functional disorder of bladder
- 788.41, urinary frequency.
Because costs will vary, depending on the chemotoxin used, the agent may be reported separately using the descriptive “J” code or another Medicare-designated alphanumeric code, such as J0585, injection of botulinum toxin type A, 1 unit.
Qualified providers now include nonphysicians as well as physicians
CPT has clarified that all E/M codes can be reported not only by physicians but by qualified nonphysicians as well.
CPT also changed wording in each of the codes so that the use of counseling time applies to all providers when counseling dominates the visit. In other words, if a payer allows someone other than a physician to provide and bill for a service, the CPT E/M codes can be used by all providers who qualify and have documented the service. These changes have no effect on the codes themselves.
Please note, however, that registered nurses and licensed practical nurses are not normally recognized as billing providers and will still be restricted to code 99211, Office or other outpatient visit for the evaluation and management of an established patient, that may not require the presence of a physician. Usually, with this code, presenting problems are minimal. Typically, 5 minutes are spent performing or supervising these services. This code is often referred to as the “nurse-only” code.
As a result of this clarification, references to physicians have been removed from CPT code 59300, Episiotomy or vaginal repair, by other than attending. This change signifies that this code may be reported by any qualified provider who did not perform the delivery or was not covering for a physician group who billed for the delivery.
Three new codes for the flu vaccine
Two of the new codes are CPT codes, and the other is for Medicare:
- 90653, Influenza vaccine, inactivated, subunit, adjuvanted, for intramuscular use
- 90672, Influenza virus vaccine, live, for intranasal use
- Q2034, Agriflu.
Keep in mind that the administration of the flu vaccine is reported differently for Medicare, compared with private payers. Administration code G0008 and diagnosis code V04.81 would be reported in conjunction with the appropriate vaccine code for Medicare. CPT requires that code 90471 be reported for administration.
CPT also revised all flu vaccine codes (90655–90660) to include the term “trivalent” to signify that all flu vaccines are made up of three strains of the virus.
Medicare refines billing for MPA administration
When billing for MPA or MPA in combination with estradiol, be aware that Medicare has eliminated the J codes for these drugs, replacing them with a single new code.
The deleted codes are:
- J1051, medroxyprogesterone acetate, 50 mg
- J1055, medroxyprogesterone acetate, 150 mg, for contraceptive use
- J1056, medroxyprogesterone acetate/ estradiol cypionate, 5 mg/25 mg.
The new code is J1050, medroxyprogesterone acetate, 1 mg. To use it, you must indicate the dosage as a quantity. For example, if you injected 150 mg, you would use code J1050 x 150 on the claim. The diagnosis code will indicate the reason for the injection—that is, medical treatment or contraception. In the event that the combination drug is being administered, separate billing of J1000, Injection, depo-estradiol cypionate, up to 5 mg, would need to be reported in addition to J1050.
Medicare has also issued a national policy on Place of Service (POS) billing because the office of the inspector general has found that physicians and other suppliers frequently report an incorrect POS, and Medicare pays more for some sites. Medicare rules for the billing of POS for the professional component of an imaging service are changing, effective April 1, 2013. This rule was postponed from its original date of October 1, 2012. Under this rule, when the professional and technical components of a service are performed in different locations, the appropriate POS to report for the interpretive aspect is the location where the technical component was performed. This change would apply to an ObGyn practice that contracts out for the technical component of an ultrasound but performs the interpretation in the office. In that case, the POS should not be listed as “office” or POS 11, but should match the POS of the imaging contractor.
We want to hear from you! Tell us what you think.
Preventive coding can be a snap
Your age-based guide to comprehensive well-woman care
Robert L. Barbieri, MD (October 2012)
Download Medicare Guide
Guide to Billing the Medicare Annual Exam
Melanie Witt, RN, CPC, COBGC, MA (October 2012)
Coding and billing for the care provided at a well-woman visit can be uncomplicated if you know the right codes for the right program. Here, I present information for straightforward preventive care. (I am assuming the patient has not also presented with a significant problem at the same visit.)
First, a patient who is not Medicare-eligible should have the annual well-woman exam billed using the CPT preventive medicine codes. There are some private insurers, however, that will only accept HCPCS codes for an annual gyn exam. These special codes are:
S0610 Annual gynecological examination, new patient
S0612 Annual gynecological examination, established patient
S0613 Annual gynecological examination; clinical breast examination without pelvic evaluation
Notably, Aetna Cigna, and United Healthcare require these codes for a gyn exam, but many BC/BS programs, for whom these codes were originally created, are now reverting to the CPT preventive medicine codes for all preventive care.
The CPT preventive codes are grouped by age and require an age- and gender-appropriate history, examination, and counseling/anticipatory guidance. The Medicare E/M documentation guidelines do not apply to preventive services, and a head-to-toe examination is also not required. CPT recognizes ACOG as an authoritative body to make recommendations for the expected preventive service for women, and if such a service is provided and documented, the preventive codes are to be reported.
The chart below summarizes the CPT preventive codes by patient status and age in comparison to ACOG age groupings.
| New Patient Preventive Medicine Code | |||
|---|---|---|---|
| New patient codes include an initial comprehensive preventive medicine evaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99384 (12–17 years) 99385 (18–39 years) | ACOG: 19–39 years 99385 (18–39 years) | ACOG: 40–64 years 99386 (40–64 years) | ACOG: 65 years and older 99387 (65 years and older) |
| Established Patient Preventive Medicine Codes | |||
| Established patient codes include periodic comprehensive preventive medicine reevaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99394 (12–17 years) 99395 (18–39 years) | ACOG: 19–39 years 99395 (18–39 years) | ACOG: 40–64 years 99396 (40–64 years) | ACOG: 65 years and older 99397 (65 years and older) |
The main code
The appropriate diagnostic link for the CPT preventive gyn annual well-woman exam is V72.31, whether or not a Pap specimen is collected. The collection of the Pap specimen is included in the preventive service, as is counseling regarding birth control, or general questions about preventing problems, including hormone replacement therapy.
If a pelvic examination is not performed, say because the patient is young and not sexually active, but an examination of other areas is carried out, the same preventive codes are reported, but the diagnosis code changes to V70.0, general health exam.
What about Medicare?
Coding. Medicare requirements are somewhat different. First, Medicare covers only a small portion of the preventive service; that is, they cover a physical examination of the genital organs and breasts and the collection and conveyance of a Pap specimen to the lab in the covered year only. Think of the complete preventive service as described in CPT as a pie—Medicare pays for 2 slices of that pie in a covered year. The two codes for these services are:
G0101 (Cervical or vaginal cancer screening; pelvic and clinical breast examination)
Q0091 (Screening Papanicolaou smear; obtaining, preparing, and conveyance of cervical or vaginal smear to laboratory)
If the patient is at low risk for developing cervical or vaginal cancer, the screening pelvic exam and Pap collection are paid every 2 years. If the woman is at high risk, Medicare will cover this portion of the encounter every year. The high-risk criteria must be re-documented every year and must include one of the following:
- Early onset of sexual activity (under age 16)
- Multiple sexual partners (five or more in a lifetime)
- History of a sexually transmitted disease (including HIV infection)
- Fewer than three negative Pap smears within the previous 7 years
- Diethylstilbestrol (DES)-exposed daughters of women who took DES during pregnancy.
If the Medicare-eligible patient is still of childbearing age, she is also considered high-risk if she has had an examination that indicated the presence of cervical or vaginal cancer or other genital abnormalities during any of the preceding 3 years. Note that these criteria do not include a history of breast cancer or a past history of cancer more than 3 years ago.
Billing. Because Medicare is paying only for a portion of the preventive service, you will need to subtract the Medicare allowable for codes G0101 and Q0091 from your normal fee for the preventive service.
- Example: If your usual fee for 99397 is $200, and the Medicare allowable for both the G and Q service is $82, you will charge the patient for the noncovered parts of the service at the rate of $118, and you will bill Medicare for their share of $82. You will collect from all sources the $200 for the preventive service. Remember, however, to get the patient to sign an ABN with regard to the Medicare part of the service. This will ensure that, if denied by Medicare, the patient will be held fully responsible for the denied amount.
The Medicare modifier is –GA (add it to codes G0101 and Q0091). Diagnostic coding is V72.31 (because a pelvic exam is performed). This code may also be linked to the collection code. For a high-risk patient, use code V15.89 (rather than V72.31). This code must be linked to the G and Q codes.
“Guide to Billing the Medicare Annual Exam” is a detailed Medicare checklist offered by the author that includes all billing scenarios for a Medicare patient. Click here to download a PDF.
Ms. Witt can be contacted directly at [email protected] should you have additional questions regarding coding and billing for preventive services.
We want to hear from you! Tell us what you think.
Your age-based guide to comprehensive well-woman care
Robert L. Barbieri, MD (October 2012)
Download Medicare Guide
Guide to Billing the Medicare Annual Exam
Melanie Witt, RN, CPC, COBGC, MA (October 2012)
Coding and billing for the care provided at a well-woman visit can be uncomplicated if you know the right codes for the right program. Here, I present information for straightforward preventive care. (I am assuming the patient has not also presented with a significant problem at the same visit.)
First, a patient who is not Medicare-eligible should have the annual well-woman exam billed using the CPT preventive medicine codes. There are some private insurers, however, that will only accept HCPCS codes for an annual gyn exam. These special codes are:
S0610 Annual gynecological examination, new patient
S0612 Annual gynecological examination, established patient
S0613 Annual gynecological examination; clinical breast examination without pelvic evaluation
Notably, Aetna Cigna, and United Healthcare require these codes for a gyn exam, but many BC/BS programs, for whom these codes were originally created, are now reverting to the CPT preventive medicine codes for all preventive care.
The CPT preventive codes are grouped by age and require an age- and gender-appropriate history, examination, and counseling/anticipatory guidance. The Medicare E/M documentation guidelines do not apply to preventive services, and a head-to-toe examination is also not required. CPT recognizes ACOG as an authoritative body to make recommendations for the expected preventive service for women, and if such a service is provided and documented, the preventive codes are to be reported.
The chart below summarizes the CPT preventive codes by patient status and age in comparison to ACOG age groupings.
| New Patient Preventive Medicine Code | |||
|---|---|---|---|
| New patient codes include an initial comprehensive preventive medicine evaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99384 (12–17 years) 99385 (18–39 years) | ACOG: 19–39 years 99385 (18–39 years) | ACOG: 40–64 years 99386 (40–64 years) | ACOG: 65 years and older 99387 (65 years and older) |
| Established Patient Preventive Medicine Codes | |||
| Established patient codes include periodic comprehensive preventive medicine reevaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99394 (12–17 years) 99395 (18–39 years) | ACOG: 19–39 years 99395 (18–39 years) | ACOG: 40–64 years 99396 (40–64 years) | ACOG: 65 years and older 99397 (65 years and older) |
The main code
The appropriate diagnostic link for the CPT preventive gyn annual well-woman exam is V72.31, whether or not a Pap specimen is collected. The collection of the Pap specimen is included in the preventive service, as is counseling regarding birth control, or general questions about preventing problems, including hormone replacement therapy.
If a pelvic examination is not performed, say because the patient is young and not sexually active, but an examination of other areas is carried out, the same preventive codes are reported, but the diagnosis code changes to V70.0, general health exam.
What about Medicare?
Coding. Medicare requirements are somewhat different. First, Medicare covers only a small portion of the preventive service; that is, they cover a physical examination of the genital organs and breasts and the collection and conveyance of a Pap specimen to the lab in the covered year only. Think of the complete preventive service as described in CPT as a pie—Medicare pays for 2 slices of that pie in a covered year. The two codes for these services are:
G0101 (Cervical or vaginal cancer screening; pelvic and clinical breast examination)
Q0091 (Screening Papanicolaou smear; obtaining, preparing, and conveyance of cervical or vaginal smear to laboratory)
If the patient is at low risk for developing cervical or vaginal cancer, the screening pelvic exam and Pap collection are paid every 2 years. If the woman is at high risk, Medicare will cover this portion of the encounter every year. The high-risk criteria must be re-documented every year and must include one of the following:
- Early onset of sexual activity (under age 16)
- Multiple sexual partners (five or more in a lifetime)
- History of a sexually transmitted disease (including HIV infection)
- Fewer than three negative Pap smears within the previous 7 years
- Diethylstilbestrol (DES)-exposed daughters of women who took DES during pregnancy.
If the Medicare-eligible patient is still of childbearing age, she is also considered high-risk if she has had an examination that indicated the presence of cervical or vaginal cancer or other genital abnormalities during any of the preceding 3 years. Note that these criteria do not include a history of breast cancer or a past history of cancer more than 3 years ago.
Billing. Because Medicare is paying only for a portion of the preventive service, you will need to subtract the Medicare allowable for codes G0101 and Q0091 from your normal fee for the preventive service.
- Example: If your usual fee for 99397 is $200, and the Medicare allowable for both the G and Q service is $82, you will charge the patient for the noncovered parts of the service at the rate of $118, and you will bill Medicare for their share of $82. You will collect from all sources the $200 for the preventive service. Remember, however, to get the patient to sign an ABN with regard to the Medicare part of the service. This will ensure that, if denied by Medicare, the patient will be held fully responsible for the denied amount.
The Medicare modifier is –GA (add it to codes G0101 and Q0091). Diagnostic coding is V72.31 (because a pelvic exam is performed). This code may also be linked to the collection code. For a high-risk patient, use code V15.89 (rather than V72.31). This code must be linked to the G and Q codes.
“Guide to Billing the Medicare Annual Exam” is a detailed Medicare checklist offered by the author that includes all billing scenarios for a Medicare patient. Click here to download a PDF.
Ms. Witt can be contacted directly at [email protected] should you have additional questions regarding coding and billing for preventive services.
We want to hear from you! Tell us what you think.
Your age-based guide to comprehensive well-woman care
Robert L. Barbieri, MD (October 2012)
Download Medicare Guide
Guide to Billing the Medicare Annual Exam
Melanie Witt, RN, CPC, COBGC, MA (October 2012)
Coding and billing for the care provided at a well-woman visit can be uncomplicated if you know the right codes for the right program. Here, I present information for straightforward preventive care. (I am assuming the patient has not also presented with a significant problem at the same visit.)
First, a patient who is not Medicare-eligible should have the annual well-woman exam billed using the CPT preventive medicine codes. There are some private insurers, however, that will only accept HCPCS codes for an annual gyn exam. These special codes are:
S0610 Annual gynecological examination, new patient
S0612 Annual gynecological examination, established patient
S0613 Annual gynecological examination; clinical breast examination without pelvic evaluation
Notably, Aetna Cigna, and United Healthcare require these codes for a gyn exam, but many BC/BS programs, for whom these codes were originally created, are now reverting to the CPT preventive medicine codes for all preventive care.
The CPT preventive codes are grouped by age and require an age- and gender-appropriate history, examination, and counseling/anticipatory guidance. The Medicare E/M documentation guidelines do not apply to preventive services, and a head-to-toe examination is also not required. CPT recognizes ACOG as an authoritative body to make recommendations for the expected preventive service for women, and if such a service is provided and documented, the preventive codes are to be reported.
The chart below summarizes the CPT preventive codes by patient status and age in comparison to ACOG age groupings.
| New Patient Preventive Medicine Code | |||
|---|---|---|---|
| New patient codes include an initial comprehensive preventive medicine evaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99384 (12–17 years) 99385 (18–39 years) | ACOG: 19–39 years 99385 (18–39 years) | ACOG: 40–64 years 99386 (40–64 years) | ACOG: 65 years and older 99387 (65 years and older) |
| Established Patient Preventive Medicine Codes | |||
| Established patient codes include periodic comprehensive preventive medicine reevaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99394 (12–17 years) 99395 (18–39 years) | ACOG: 19–39 years 99395 (18–39 years) | ACOG: 40–64 years 99396 (40–64 years) | ACOG: 65 years and older 99397 (65 years and older) |
The main code
The appropriate diagnostic link for the CPT preventive gyn annual well-woman exam is V72.31, whether or not a Pap specimen is collected. The collection of the Pap specimen is included in the preventive service, as is counseling regarding birth control, or general questions about preventing problems, including hormone replacement therapy.
If a pelvic examination is not performed, say because the patient is young and not sexually active, but an examination of other areas is carried out, the same preventive codes are reported, but the diagnosis code changes to V70.0, general health exam.
What about Medicare?
Coding. Medicare requirements are somewhat different. First, Medicare covers only a small portion of the preventive service; that is, they cover a physical examination of the genital organs and breasts and the collection and conveyance of a Pap specimen to the lab in the covered year only. Think of the complete preventive service as described in CPT as a pie—Medicare pays for 2 slices of that pie in a covered year. The two codes for these services are:
G0101 (Cervical or vaginal cancer screening; pelvic and clinical breast examination)
Q0091 (Screening Papanicolaou smear; obtaining, preparing, and conveyance of cervical or vaginal smear to laboratory)
If the patient is at low risk for developing cervical or vaginal cancer, the screening pelvic exam and Pap collection are paid every 2 years. If the woman is at high risk, Medicare will cover this portion of the encounter every year. The high-risk criteria must be re-documented every year and must include one of the following:
- Early onset of sexual activity (under age 16)
- Multiple sexual partners (five or more in a lifetime)
- History of a sexually transmitted disease (including HIV infection)
- Fewer than three negative Pap smears within the previous 7 years
- Diethylstilbestrol (DES)-exposed daughters of women who took DES during pregnancy.
If the Medicare-eligible patient is still of childbearing age, she is also considered high-risk if she has had an examination that indicated the presence of cervical or vaginal cancer or other genital abnormalities during any of the preceding 3 years. Note that these criteria do not include a history of breast cancer or a past history of cancer more than 3 years ago.
Billing. Because Medicare is paying only for a portion of the preventive service, you will need to subtract the Medicare allowable for codes G0101 and Q0091 from your normal fee for the preventive service.
- Example: If your usual fee for 99397 is $200, and the Medicare allowable for both the G and Q service is $82, you will charge the patient for the noncovered parts of the service at the rate of $118, and you will bill Medicare for their share of $82. You will collect from all sources the $200 for the preventive service. Remember, however, to get the patient to sign an ABN with regard to the Medicare part of the service. This will ensure that, if denied by Medicare, the patient will be held fully responsible for the denied amount.
The Medicare modifier is –GA (add it to codes G0101 and Q0091). Diagnostic coding is V72.31 (because a pelvic exam is performed). This code may also be linked to the collection code. For a high-risk patient, use code V15.89 (rather than V72.31). This code must be linked to the G and Q codes.
“Guide to Billing the Medicare Annual Exam” is a detailed Medicare checklist offered by the author that includes all billing scenarios for a Medicare patient. Click here to download a PDF.
Ms. Witt can be contacted directly at [email protected] should you have additional questions regarding coding and billing for preventive services.
We want to hear from you! Tell us what you think.
Change has come again to ICD-9 diagnostic codes
Did you know? When October 1 rolled around a short time ago, so did new codes for you to learn in the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
If you consider that unpleasant news for your billing efforts, I also have what I consider good news: The 2012 fiscal year is the final year for changes to ICD-9-CM codes: On October 1, 2013, the nation switches to 10th Revision (that is, ICD-10-CM) codes. The National Center for Health Statistics has indicated that the only changes to ICD-9 codes permitted from now on are ones describing new diseases that require immediate reporting during this transition/freeze period.
This last set of changes isn’t as massive as what we saw in previous years. Nevertheless, the changes certainly enhance the ability of ObGyn practices to report the reasons for patient encounters.
The major gyn change this year involves reporting vaginal mesh complications. There are several new obstetric codes, too, to enhance reporting of cesarean delivery and management of high-risk OB conditions.
The new codes were added to the national code set on October 1. As in prior years, there is no grace period.
Changes to obstetric codes
ANTIPHOSPHOLIPID ANTIBODY
Antiphospholipid syndrome and lupus anticoagulant are associated with complications of pregnancy that include fetal loss, fetal growth restriction, preeclampsia, thrombosis, and autoimmune thrombocytopenia. Until now, the obstetrician reporting 649.3x (Coagulation defects complicating pregnancy, childbirth, or the puerperium), had only two secondary code options to further describe the patient’s condition: 795.79, used to report a finding of antiphospholipid antibody in a blood specimen, and 289.81, antiphospholipid antibody with hypercoagulable state.
A new code, 286.53 (Antiphospholipid antibody with hemorrhagic disorder), provides a third option when reporting 649.3x.
CHEMICAL PREGNANCY AND BLIGHTED OVUM
Fertility clinics and physicians who specialize in the use of assisted reproductive technology requested a code to identify patients who have what is referred to (imprecisely) as a “false-positive pregnancy,” “chemical pregnancy,” or “biochemical pregnancy.” These terms do not, however, accurately describe a pregnancy achieved using hormone stimulation or other such “chemical” methods.
In some cases, of course, a woman’s pregnancy test comes back positive, indicating a serum human chorionic gonadotropin (hCG) level, but, when she is followed with ultrasonography, no fetus is present—in effect, she has had an early miscarriage. But there has been no ICD-9 code to use at this stage that discriminates between confirmed ectopic pregnancy and confirmed miscarriage—only a code for a laboratory finding.
To improve the specificity of coding, therefore, and to track such pregnancies, existing code 631 (Other abnormal product of conception) has been expanded and divided in two:
| 631.0 | Inappropriate rise (decline) of quantitative hCG in early pregnancy |
| 631.8 | Other abnormal products of conception |
Documentation by the physician that signals that 631.0 should be reported might include a reference to biochemical pregnancy, chemical pregnancy, or an inappropriate level of quantitative hCG for gestational age in early pregnancy. For 631.8 to be reported, documentation might mention such findings as a “blighted ovum” or “fleshy mole.”
Note: Because of this code expansion, the three-digit code 631 will no longer be a valid code for billing purposes.
ELECTIVE CESAREAN DELIVERY BEFORE 39 WEEKS’ GESTATION
ACOG requested new codes for elective cesarean delivery before 39 weeks’ gestation—a scenario that is one of the new markers of quality of care. Whereas ICD-9 has two diagnosis codes that mention cesarean delivery (654.2x, [Previous cesarean delivery not otherwise specified] and 669.71 [Cesarean delivery, without mention of indication]), neither code captures a case in which a woman presents in labor at 37 to 38 weeks’ gestation and the physician determines that it is best to deliver at that time rather than try to take measures that will forestall delivery until the 39th week.
Although ICD-9 already also has a code for early onset of delivery (644.21), it applies only to pregnancies before 37 completed weeks.
The new codes are:
| 649.81 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with or without mention of antepartum condition |
| 649.82 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with mention of postpartum complication |
Note: The new code has two options for a fifth digit:
- Reporting a fifth digit 1 indicates that the patient may, or may not, have had a complication in the antepartum period that is related to early onset of labor.
- Reporting a fifth digit 2 indicates that the patient developed a complication after delivery (but before discharge) that is related to the delivery.
For any hospitalization that results in a delivery, you must select a fifth digit 1 or 2; the choice depends on the overriding complication. You may not list code 649.8 twice—i.e., once with a fifth digit 1 and once with a fifth digit 2.
If the patient had a condition that was documented to be why cesarean delivery was medically indicated, list that as a secondary diagnosis—for example, cephalopelvic disproportion (653.4x) or prior cesarean delivery (654.2x).
SUPERVISION OF HIGH-RISK PREGNANCY
Code subcategory V23.4 (Pregnancy with other poor obstetric history) had only two coding options before October 1, 2011: V23.41 (Pregnancy with history of pre-term labor) and V23.49 (Pregnancy with other poor obstetric history).
Ectopic pregnancy. ACOG considers that it is important to track patients who had a prior ectopic pregnancy because such a history gives rise to an increased risk of ectopic pregnancy during the current pregnancy. Therefore, a new code for this status was requested by ACOG, and provided.
Note: Use the new history code only until the patient is confirmed not to have an ectopic pregnancy, if that is the outcome. Once you’ve confirmed that she has only a normal, intrauterine pregnancy, the risk posed by her history no longer has an impact on the current pregnancy. (ICD-9 rules direct you to report conditions that require active intervention or a change in routine care of the pregnancy—not conditions that merely exist without the need for intervention or additional monitoring.)
The new code is:
| V23.42 | Pregnancy with history of ectopic pregnancy |
Fetal viability. There was also no specific code before October 1 to report the need for a sonogram to check fetal viability, especially when a previously confirmed pregnancy comes into question because of the apparent absence of a fetal heartbeat on examination of the mother. In such a case, an additional sonogram might be required beyond the initial scan to confirm fetal demise or a continuing viable pregnancy. Until now, either of these findings could have been reported only with codes that do not accurately describe the situation, such as 659.7 (Abnormality in fetal heart rate or rhythm); V28.89 (Other specified antenatal screening); and V23.89 (Other high-risk pregnancy).
The new code is:
| V23.87 | Pregnancy with inconclusive fetal viability |
Changes to gyn codes
An effective surgical treatment for vaginal vault prolapse is sacrocolpopexy that uses a graft to suspend the upper vagina to the anterior longitudinal ligament of the sacrum. But, regrettably, synthetic graft material has also been associated with erosion of the mesh and subsequent pelvic infection (by erosion into surrounding organs or tissue). Exposure of the mesh in the vagina can also occur (see “Take this simplified approach to correcting exposure of vaginal mesh” in the July 2011 issue, available at obgmanagement.com).
Before October 1, erosion or exposure of mesh (without infection) would have been reported with code 996.39 (Mechanical complication of a genitourinary device, implant and graft) or 996.76 (Other complications due to genitourinary device, implant, and graft). With creation of a new subcategory code, 629.3 (Complication of implanted vaginal mesh and other prosthetic materials), however, these specific complications can be reported and tracked. The new codes also give you a specific linking diagnosis for revision of the mesh.
The two new codes are:
| 629.31 | Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue (e.g., into pelvic floor muscles) |
| 629.32 | Exposure of implanted vaginal mesh and other prosthetic materials into vagina (e.g., through the vaginal wall) |
Note: If the patient’s graft material has caused fibrosis, hemorrhage, occlusion, or pain, continue to report 996.76. And, of course, any infection or inflammatory reaction caused by mesh is reported with existing code 996.65.
Because erosion and exposure can occur at the same time, it is proper to report both new codes, if that is the case.
HISTORY OF GESTATIONAL DIABETES
Code V12.2 (Personal history of endocrine, metabolic, and immunity disorders) has been expanded and divided into two five-digit codes:
| V12.21 | Gestational diabetes |
| V12.29 | Other endocrine, metabolic, and immunity disorders |
With this change, four-digit code V12.2 became an invalid diagnosis code; your claim will be denied if you report it as the reason for an encounter.
Note: Code V12.21 may not be reported as a primary diagnosis for an obstetrical patient. Instead, a personal history that may be having an impact on the current pregnancy should be reported with a V23.xx code (Supervision of high risk pregnancy), until (and if) the patient develops a condition.
For example: If a patient had gestational diabetes during a prior pregnancy, she risks developing it again in the current pregnancy. In that case, report V23.49 (Pregnancy with other poor obstetric history) as the primary code and assign V12.21 as the secondary code.
LONG-TERM USE OF BISPHOSPHONATES
In a woman being treated to prevent loss of bone mass, the side-effect profile of the medication and the need to measure its effectiveness require regular follow-up visits. Effective October 1, code V58.68 (Long-term [current] use of bisphosphonates) should be reported for these follow-up visits. The code can be also used to support ordering follow-up bone densitometry.
Medications that might be applicable here are alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel), and zoledronic acid (Reclast).
Download a free copy of the complete addenda of ICD-9-CM code changes that have been made for fiscal year 2012 at: www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
We want to hear from you! Tell us what you think.
Did you know? When October 1 rolled around a short time ago, so did new codes for you to learn in the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
If you consider that unpleasant news for your billing efforts, I also have what I consider good news: The 2012 fiscal year is the final year for changes to ICD-9-CM codes: On October 1, 2013, the nation switches to 10th Revision (that is, ICD-10-CM) codes. The National Center for Health Statistics has indicated that the only changes to ICD-9 codes permitted from now on are ones describing new diseases that require immediate reporting during this transition/freeze period.
This last set of changes isn’t as massive as what we saw in previous years. Nevertheless, the changes certainly enhance the ability of ObGyn practices to report the reasons for patient encounters.
The major gyn change this year involves reporting vaginal mesh complications. There are several new obstetric codes, too, to enhance reporting of cesarean delivery and management of high-risk OB conditions.
The new codes were added to the national code set on October 1. As in prior years, there is no grace period.
Changes to obstetric codes
ANTIPHOSPHOLIPID ANTIBODY
Antiphospholipid syndrome and lupus anticoagulant are associated with complications of pregnancy that include fetal loss, fetal growth restriction, preeclampsia, thrombosis, and autoimmune thrombocytopenia. Until now, the obstetrician reporting 649.3x (Coagulation defects complicating pregnancy, childbirth, or the puerperium), had only two secondary code options to further describe the patient’s condition: 795.79, used to report a finding of antiphospholipid antibody in a blood specimen, and 289.81, antiphospholipid antibody with hypercoagulable state.
A new code, 286.53 (Antiphospholipid antibody with hemorrhagic disorder), provides a third option when reporting 649.3x.
CHEMICAL PREGNANCY AND BLIGHTED OVUM
Fertility clinics and physicians who specialize in the use of assisted reproductive technology requested a code to identify patients who have what is referred to (imprecisely) as a “false-positive pregnancy,” “chemical pregnancy,” or “biochemical pregnancy.” These terms do not, however, accurately describe a pregnancy achieved using hormone stimulation or other such “chemical” methods.
In some cases, of course, a woman’s pregnancy test comes back positive, indicating a serum human chorionic gonadotropin (hCG) level, but, when she is followed with ultrasonography, no fetus is present—in effect, she has had an early miscarriage. But there has been no ICD-9 code to use at this stage that discriminates between confirmed ectopic pregnancy and confirmed miscarriage—only a code for a laboratory finding.
To improve the specificity of coding, therefore, and to track such pregnancies, existing code 631 (Other abnormal product of conception) has been expanded and divided in two:
| 631.0 | Inappropriate rise (decline) of quantitative hCG in early pregnancy |
| 631.8 | Other abnormal products of conception |
Documentation by the physician that signals that 631.0 should be reported might include a reference to biochemical pregnancy, chemical pregnancy, or an inappropriate level of quantitative hCG for gestational age in early pregnancy. For 631.8 to be reported, documentation might mention such findings as a “blighted ovum” or “fleshy mole.”
Note: Because of this code expansion, the three-digit code 631 will no longer be a valid code for billing purposes.
ELECTIVE CESAREAN DELIVERY BEFORE 39 WEEKS’ GESTATION
ACOG requested new codes for elective cesarean delivery before 39 weeks’ gestation—a scenario that is one of the new markers of quality of care. Whereas ICD-9 has two diagnosis codes that mention cesarean delivery (654.2x, [Previous cesarean delivery not otherwise specified] and 669.71 [Cesarean delivery, without mention of indication]), neither code captures a case in which a woman presents in labor at 37 to 38 weeks’ gestation and the physician determines that it is best to deliver at that time rather than try to take measures that will forestall delivery until the 39th week.
Although ICD-9 already also has a code for early onset of delivery (644.21), it applies only to pregnancies before 37 completed weeks.
The new codes are:
| 649.81 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with or without mention of antepartum condition |
| 649.82 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with mention of postpartum complication |
Note: The new code has two options for a fifth digit:
- Reporting a fifth digit 1 indicates that the patient may, or may not, have had a complication in the antepartum period that is related to early onset of labor.
- Reporting a fifth digit 2 indicates that the patient developed a complication after delivery (but before discharge) that is related to the delivery.
For any hospitalization that results in a delivery, you must select a fifth digit 1 or 2; the choice depends on the overriding complication. You may not list code 649.8 twice—i.e., once with a fifth digit 1 and once with a fifth digit 2.
If the patient had a condition that was documented to be why cesarean delivery was medically indicated, list that as a secondary diagnosis—for example, cephalopelvic disproportion (653.4x) or prior cesarean delivery (654.2x).
SUPERVISION OF HIGH-RISK PREGNANCY
Code subcategory V23.4 (Pregnancy with other poor obstetric history) had only two coding options before October 1, 2011: V23.41 (Pregnancy with history of pre-term labor) and V23.49 (Pregnancy with other poor obstetric history).
Ectopic pregnancy. ACOG considers that it is important to track patients who had a prior ectopic pregnancy because such a history gives rise to an increased risk of ectopic pregnancy during the current pregnancy. Therefore, a new code for this status was requested by ACOG, and provided.
Note: Use the new history code only until the patient is confirmed not to have an ectopic pregnancy, if that is the outcome. Once you’ve confirmed that she has only a normal, intrauterine pregnancy, the risk posed by her history no longer has an impact on the current pregnancy. (ICD-9 rules direct you to report conditions that require active intervention or a change in routine care of the pregnancy—not conditions that merely exist without the need for intervention or additional monitoring.)
The new code is:
| V23.42 | Pregnancy with history of ectopic pregnancy |
Fetal viability. There was also no specific code before October 1 to report the need for a sonogram to check fetal viability, especially when a previously confirmed pregnancy comes into question because of the apparent absence of a fetal heartbeat on examination of the mother. In such a case, an additional sonogram might be required beyond the initial scan to confirm fetal demise or a continuing viable pregnancy. Until now, either of these findings could have been reported only with codes that do not accurately describe the situation, such as 659.7 (Abnormality in fetal heart rate or rhythm); V28.89 (Other specified antenatal screening); and V23.89 (Other high-risk pregnancy).
The new code is:
| V23.87 | Pregnancy with inconclusive fetal viability |
Changes to gyn codes
An effective surgical treatment for vaginal vault prolapse is sacrocolpopexy that uses a graft to suspend the upper vagina to the anterior longitudinal ligament of the sacrum. But, regrettably, synthetic graft material has also been associated with erosion of the mesh and subsequent pelvic infection (by erosion into surrounding organs or tissue). Exposure of the mesh in the vagina can also occur (see “Take this simplified approach to correcting exposure of vaginal mesh” in the July 2011 issue, available at obgmanagement.com).
Before October 1, erosion or exposure of mesh (without infection) would have been reported with code 996.39 (Mechanical complication of a genitourinary device, implant and graft) or 996.76 (Other complications due to genitourinary device, implant, and graft). With creation of a new subcategory code, 629.3 (Complication of implanted vaginal mesh and other prosthetic materials), however, these specific complications can be reported and tracked. The new codes also give you a specific linking diagnosis for revision of the mesh.
The two new codes are:
| 629.31 | Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue (e.g., into pelvic floor muscles) |
| 629.32 | Exposure of implanted vaginal mesh and other prosthetic materials into vagina (e.g., through the vaginal wall) |
Note: If the patient’s graft material has caused fibrosis, hemorrhage, occlusion, or pain, continue to report 996.76. And, of course, any infection or inflammatory reaction caused by mesh is reported with existing code 996.65.
Because erosion and exposure can occur at the same time, it is proper to report both new codes, if that is the case.
HISTORY OF GESTATIONAL DIABETES
Code V12.2 (Personal history of endocrine, metabolic, and immunity disorders) has been expanded and divided into two five-digit codes:
| V12.21 | Gestational diabetes |
| V12.29 | Other endocrine, metabolic, and immunity disorders |
With this change, four-digit code V12.2 became an invalid diagnosis code; your claim will be denied if you report it as the reason for an encounter.
Note: Code V12.21 may not be reported as a primary diagnosis for an obstetrical patient. Instead, a personal history that may be having an impact on the current pregnancy should be reported with a V23.xx code (Supervision of high risk pregnancy), until (and if) the patient develops a condition.
For example: If a patient had gestational diabetes during a prior pregnancy, she risks developing it again in the current pregnancy. In that case, report V23.49 (Pregnancy with other poor obstetric history) as the primary code and assign V12.21 as the secondary code.
LONG-TERM USE OF BISPHOSPHONATES
In a woman being treated to prevent loss of bone mass, the side-effect profile of the medication and the need to measure its effectiveness require regular follow-up visits. Effective October 1, code V58.68 (Long-term [current] use of bisphosphonates) should be reported for these follow-up visits. The code can be also used to support ordering follow-up bone densitometry.
Medications that might be applicable here are alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel), and zoledronic acid (Reclast).
Download a free copy of the complete addenda of ICD-9-CM code changes that have been made for fiscal year 2012 at: www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
We want to hear from you! Tell us what you think.
Did you know? When October 1 rolled around a short time ago, so did new codes for you to learn in the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM).
If you consider that unpleasant news for your billing efforts, I also have what I consider good news: The 2012 fiscal year is the final year for changes to ICD-9-CM codes: On October 1, 2013, the nation switches to 10th Revision (that is, ICD-10-CM) codes. The National Center for Health Statistics has indicated that the only changes to ICD-9 codes permitted from now on are ones describing new diseases that require immediate reporting during this transition/freeze period.
This last set of changes isn’t as massive as what we saw in previous years. Nevertheless, the changes certainly enhance the ability of ObGyn practices to report the reasons for patient encounters.
The major gyn change this year involves reporting vaginal mesh complications. There are several new obstetric codes, too, to enhance reporting of cesarean delivery and management of high-risk OB conditions.
The new codes were added to the national code set on October 1. As in prior years, there is no grace period.
Changes to obstetric codes
ANTIPHOSPHOLIPID ANTIBODY
Antiphospholipid syndrome and lupus anticoagulant are associated with complications of pregnancy that include fetal loss, fetal growth restriction, preeclampsia, thrombosis, and autoimmune thrombocytopenia. Until now, the obstetrician reporting 649.3x (Coagulation defects complicating pregnancy, childbirth, or the puerperium), had only two secondary code options to further describe the patient’s condition: 795.79, used to report a finding of antiphospholipid antibody in a blood specimen, and 289.81, antiphospholipid antibody with hypercoagulable state.
A new code, 286.53 (Antiphospholipid antibody with hemorrhagic disorder), provides a third option when reporting 649.3x.
CHEMICAL PREGNANCY AND BLIGHTED OVUM
Fertility clinics and physicians who specialize in the use of assisted reproductive technology requested a code to identify patients who have what is referred to (imprecisely) as a “false-positive pregnancy,” “chemical pregnancy,” or “biochemical pregnancy.” These terms do not, however, accurately describe a pregnancy achieved using hormone stimulation or other such “chemical” methods.
In some cases, of course, a woman’s pregnancy test comes back positive, indicating a serum human chorionic gonadotropin (hCG) level, but, when she is followed with ultrasonography, no fetus is present—in effect, she has had an early miscarriage. But there has been no ICD-9 code to use at this stage that discriminates between confirmed ectopic pregnancy and confirmed miscarriage—only a code for a laboratory finding.
To improve the specificity of coding, therefore, and to track such pregnancies, existing code 631 (Other abnormal product of conception) has been expanded and divided in two:
| 631.0 | Inappropriate rise (decline) of quantitative hCG in early pregnancy |
| 631.8 | Other abnormal products of conception |
Documentation by the physician that signals that 631.0 should be reported might include a reference to biochemical pregnancy, chemical pregnancy, or an inappropriate level of quantitative hCG for gestational age in early pregnancy. For 631.8 to be reported, documentation might mention such findings as a “blighted ovum” or “fleshy mole.”
Note: Because of this code expansion, the three-digit code 631 will no longer be a valid code for billing purposes.
ELECTIVE CESAREAN DELIVERY BEFORE 39 WEEKS’ GESTATION
ACOG requested new codes for elective cesarean delivery before 39 weeks’ gestation—a scenario that is one of the new markers of quality of care. Whereas ICD-9 has two diagnosis codes that mention cesarean delivery (654.2x, [Previous cesarean delivery not otherwise specified] and 669.71 [Cesarean delivery, without mention of indication]), neither code captures a case in which a woman presents in labor at 37 to 38 weeks’ gestation and the physician determines that it is best to deliver at that time rather than try to take measures that will forestall delivery until the 39th week.
Although ICD-9 already also has a code for early onset of delivery (644.21), it applies only to pregnancies before 37 completed weeks.
The new codes are:
| 649.81 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with or without mention of antepartum condition |
| 649.82 | Onset (spontaneous) of labor after 37 completed weeks of gestation but before 39 completed weeks’ gestation, with delivery by (planned) cesarean section, delivered, with mention of postpartum complication |
Note: The new code has two options for a fifth digit:
- Reporting a fifth digit 1 indicates that the patient may, or may not, have had a complication in the antepartum period that is related to early onset of labor.
- Reporting a fifth digit 2 indicates that the patient developed a complication after delivery (but before discharge) that is related to the delivery.
For any hospitalization that results in a delivery, you must select a fifth digit 1 or 2; the choice depends on the overriding complication. You may not list code 649.8 twice—i.e., once with a fifth digit 1 and once with a fifth digit 2.
If the patient had a condition that was documented to be why cesarean delivery was medically indicated, list that as a secondary diagnosis—for example, cephalopelvic disproportion (653.4x) or prior cesarean delivery (654.2x).
SUPERVISION OF HIGH-RISK PREGNANCY
Code subcategory V23.4 (Pregnancy with other poor obstetric history) had only two coding options before October 1, 2011: V23.41 (Pregnancy with history of pre-term labor) and V23.49 (Pregnancy with other poor obstetric history).
Ectopic pregnancy. ACOG considers that it is important to track patients who had a prior ectopic pregnancy because such a history gives rise to an increased risk of ectopic pregnancy during the current pregnancy. Therefore, a new code for this status was requested by ACOG, and provided.
Note: Use the new history code only until the patient is confirmed not to have an ectopic pregnancy, if that is the outcome. Once you’ve confirmed that she has only a normal, intrauterine pregnancy, the risk posed by her history no longer has an impact on the current pregnancy. (ICD-9 rules direct you to report conditions that require active intervention or a change in routine care of the pregnancy—not conditions that merely exist without the need for intervention or additional monitoring.)
The new code is:
| V23.42 | Pregnancy with history of ectopic pregnancy |
Fetal viability. There was also no specific code before October 1 to report the need for a sonogram to check fetal viability, especially when a previously confirmed pregnancy comes into question because of the apparent absence of a fetal heartbeat on examination of the mother. In such a case, an additional sonogram might be required beyond the initial scan to confirm fetal demise or a continuing viable pregnancy. Until now, either of these findings could have been reported only with codes that do not accurately describe the situation, such as 659.7 (Abnormality in fetal heart rate or rhythm); V28.89 (Other specified antenatal screening); and V23.89 (Other high-risk pregnancy).
The new code is:
| V23.87 | Pregnancy with inconclusive fetal viability |
Changes to gyn codes
An effective surgical treatment for vaginal vault prolapse is sacrocolpopexy that uses a graft to suspend the upper vagina to the anterior longitudinal ligament of the sacrum. But, regrettably, synthetic graft material has also been associated with erosion of the mesh and subsequent pelvic infection (by erosion into surrounding organs or tissue). Exposure of the mesh in the vagina can also occur (see “Take this simplified approach to correcting exposure of vaginal mesh” in the July 2011 issue, available at obgmanagement.com).
Before October 1, erosion or exposure of mesh (without infection) would have been reported with code 996.39 (Mechanical complication of a genitourinary device, implant and graft) or 996.76 (Other complications due to genitourinary device, implant, and graft). With creation of a new subcategory code, 629.3 (Complication of implanted vaginal mesh and other prosthetic materials), however, these specific complications can be reported and tracked. The new codes also give you a specific linking diagnosis for revision of the mesh.
The two new codes are:
| 629.31 | Erosion of implanted vaginal mesh and other prosthetic materials to surrounding organ or tissue (e.g., into pelvic floor muscles) |
| 629.32 | Exposure of implanted vaginal mesh and other prosthetic materials into vagina (e.g., through the vaginal wall) |
Note: If the patient’s graft material has caused fibrosis, hemorrhage, occlusion, or pain, continue to report 996.76. And, of course, any infection or inflammatory reaction caused by mesh is reported with existing code 996.65.
Because erosion and exposure can occur at the same time, it is proper to report both new codes, if that is the case.
HISTORY OF GESTATIONAL DIABETES
Code V12.2 (Personal history of endocrine, metabolic, and immunity disorders) has been expanded and divided into two five-digit codes:
| V12.21 | Gestational diabetes |
| V12.29 | Other endocrine, metabolic, and immunity disorders |
With this change, four-digit code V12.2 became an invalid diagnosis code; your claim will be denied if you report it as the reason for an encounter.
Note: Code V12.21 may not be reported as a primary diagnosis for an obstetrical patient. Instead, a personal history that may be having an impact on the current pregnancy should be reported with a V23.xx code (Supervision of high risk pregnancy), until (and if) the patient develops a condition.
For example: If a patient had gestational diabetes during a prior pregnancy, she risks developing it again in the current pregnancy. In that case, report V23.49 (Pregnancy with other poor obstetric history) as the primary code and assign V12.21 as the secondary code.
LONG-TERM USE OF BISPHOSPHONATES
In a woman being treated to prevent loss of bone mass, the side-effect profile of the medication and the need to measure its effectiveness require regular follow-up visits. Effective October 1, code V58.68 (Long-term [current] use of bisphosphonates) should be reported for these follow-up visits. The code can be also used to support ordering follow-up bone densitometry.
Medications that might be applicable here are alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel), and zoledronic acid (Reclast).
Download a free copy of the complete addenda of ICD-9-CM code changes that have been made for fiscal year 2012 at: www.cdc.gov/nchs/icd/icd9cm_addenda_guidelines.htm
We want to hear from you! Tell us what you think.
Changes to the CPT code set and Medicare billing
The Current Procedural Terminology (CPT) code set for 2011 includes several changes of interest to ObGyns. These include 1) guideline clarifications regarding wound debridement and obstetric care codes; 2) new codes for subsequent observation care; micro-remodeling of the bladder neck; insertion of a vaginal after-loading device; and 3) a lab code for detecting amniotic fluid in cervicovaginal secretions (using the AmniSure kit).
There is also a new code for vaccine counseling that will have an impact on you if your practice offers the human papillomavirus (HPV) vaccine to patients younger than 19 years.
There are changes to Medicare this year that you should take note of if you care for these patients, particularly in the area of preventive visit billing.
CPT and Medicare changes both took effect on January 1. The Health Insurance Portability and Accountability Act (HIPAA) requires that insurers accepted the new codes on that date.
Changes to the CPT code set
OBSERVATION CARE
One of the biggest headaches for medical practices has been standardized coding and billing for observation care that lasts more than 1 day. In the past, payers accepted a problem E/M for Day 2 of observation care, or instructed practices to code an unlisted E/M service. Now, you may report all care rendered in the observation setting with the addition of three new codes for subsequent care:
99244 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: problem focused interval history, problem focused examination; medical decision making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
99225 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: an expanded problem focused interval history; an expanded problem focused examination; medical decision making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
99226 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: a detailed interval history; a detailed examination; medical decision making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Note that each of these codes 1) “suggests” the status of the patient for each level of billing, and 2) includes a typical time. This means that, unlike the observation care admission codes or the observation admission/same-day discharge codes, time that is spent with the patient, or on the unit, may be used to select the code—if you document 1) the requirement that more than 50% of the typical time was spent on counseling or coordination of care, or both, and 2) a detailed description of this activity.
Codes for wound debridement were given a facelift with the addition of a new guideline that addresses both surgical and medical debridement. The surgical debridement codes, (11042–11047) are now reported on the basis of the depth of tissue removed and the surface area of the wound. This means that codes 11040 and 11041 were deleted to make room for new and revised codes.
This change will mean that, when you report these codes, you will need to document more information to bill. It’s also understood that coding separately for debridement of dermis or epidermis at the same time you code for debriding underlying structures would be inappropriate.
CPT has also indicated that active wound management codes 97597 and 97598 can now be reported by physicians or nonphysician providers as long as the provider has direct (one-on-one) contact. These codes should be reported for skin-surface debridement only.
The new and revised codes (some of which have been published in CPT in nonsequential order) are:
11042 Debridement, subcutaneous tissue (includes epidermis and dermis, if performed); first 20 sq cm or less
+11045 (new add-on code reported with 11042 only) each additional 20 sq cm or part thereof
11043 Debridement, muscle and/or facia (includes epidermis, dermis, and subcutaneous tissue, if performed); first 20 sq cm or less
+11046 (new add-on code reported with 11043 only) each additional 20 sq cm or part thereof
11044 Debridement, bone (includes epidermis, dermis, subcutaneous tissue, muscle and/or fascia, if performed); first 20 sq cm or less
+11047 (new add-on code reported with 11044 only) each additional 20 sq cm or part thereof
97597 Debridement (e.g., high pressure waterjet with/without suction, sharp selective debridement with scissors, scalpel and forceps), open wound, (e.g., fibrin, devitalized epidermis and/or dermis, exudate, debris, biofilm), including topical application(s), wound assessment, use of a whirlpool, when performed and instruction(s) for ongoing care, per session, total wound(s) surface area; first 20 sq cm or less
+95798 (add-on code reported with 97597 only) Each additional 20 sq cm, or part thereof.
TRANSURETHRAL RADIOFREQUENCY
Category III code 0193T, which described transurethral radiofrequency micro-remodeling for stress urinary incontinence, has been deleted and converted to a Category I CPT code, 53860 (Transurethral radiofrequency micro-remodeling of the female bladder neck and proximal urethra for stress urinary incontinence). The procedure includes a periurethral block and flushing the bladder with a lidocaine slurry, and can be performed in the office.
In all, the procedure requires nine treatment cycles during the session, but the code is billed only once. Catheterization and measurement of a voiding sample after the procedure are included in the code.
AFTERLOADING DEVICES FOR CLINICAL BRACHYTHERAPY
CPT revised—slightly—existing code 57155, and added code 57156 (Insertion of a vaginal radiation afterloading apparatus for clinical brachytherapy).
- Code 57155 was revised to clarify that only a single tandem is inserted into the uterus. There had been confusion earlier in this regard.
- The new code describes a procedure that may also include dilation of the vaginal canal to remove postradiation adhesions. That procedure also involves 1) placement of bladder and rectal catheters and 2) radiographic imaging to confirm placement, which are not coded separately.
CLARIFICATION OF OBSTETRIC GUIDELINES
Been having problems with payers and their interpretation of the delivery only, postpartum only, and delivery with postpartum care codes? CPT has, at last, clarified what you can, and cannot, bill in those circumstances. (Keep in mind, however, that you may not unbundle these procedures if more extensive care is provided: Most payers want you to bill the global OB care code that includes antepartum, intrapartum, and postpartum care.)
In some cases (such as Medicaid), the payer stipulates that only the physician who actually performed the delivery may bill for it, even if the delivering physician is covering for, or is a member of, the same group practice as the primary attending of record. The “delivery-only” codes should be reported when 1) an unaffiliated physician has delivered the baby but will not be providing any outpatient postpartum care or 2) the payer has specified this method of billing for the covering or affiliated provider.
CPT has clarified that delivery-only codes (59409, 59514, or 59612, 59620) include admission to the hospital, the admission history and physical exam, uncomplicated labor and delivery (including delivery of the placenta, or use of forceps or vacuum extraction). These codes do not include inpatient rounding or discharge day care after delivery (and, of course, include no outpatient postpartum care). When, as the delivering physician, you also provide inpatient postdelivery care, therefore, you may additionally bill subsequent hospital care codes and discharge day management codes (99231-99233, 99238-99239).
If the unaffiliated physician performs the delivery and also intends on providing outpatient postpartum care, the CPT codes for delivery with postpartum are to be reported (59410, 59515, 59614, 59622). In addition to the delivery, these codes include all inpatient and outpatient postpartum care. And finally, for those physicians who are only providing outpatient postpartum care, the code 59430, Postpartum care only, should be reported.
PLACENTAL ALPHA MICROGLOBULIN-1
A new code, 84112 (Placental alpha microglobulin-1 [PAMG-11], cervicovaginal secretion, qualitative), has been added to allow the clinical laboratory to bill for this immunoassay that detects amniotic fluid in the secretions. Physician work involves collection of the specimen but, under CPT rules, collection is included as part of any E/M service.
Note: An existing code for this test that is used by Blue Cross/Blue Shield payers (S3628) remains valid in 2011.
HPV VACCINE COUNSELING
Before January 1, 2011, if you counseled a patient about the HPV vaccine, you could report preventive counseling codes, such as 99401–99404, in addition to the vaccine administration code, 90471 (Immunization administration, 1 vaccine). Now, however, you have a new code for counseling and vaccine administration for a patient who is younger than 19 years—the age group most likely to be counseled about this vaccine. When you see, and counsel, such a patient before administering the vaccine, on the same date of service, code 90460 (Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qualified health care profession; first vaccine/toxoid component), and 90649 for the quadrivalent or 90650 for the bivalent HPV vaccine.
If your patient is 19 years or older and requires counseling, continue to bill 99401– 99404 for counseling, with 90471 for immunization and 90649 or 90650 for the vaccine. Keep in mind: Whether you report 90460 or the 9940X codes, you are required to document the content of the counseling. Codes 9940X also require documentation of the duration of counseling.
INFLUENZA VACCINE
New codes have been established for the flu vaccine, but you won’t be using them: They are intended to address future pandemic strains of influenza. This year’s vaccine contains the H1N1 strain, but is coded as the normal seasonal flu vaccine, based on the type given:
90656 (preservative-free)
90658 (split virus)
90660 (intranasal)
90662 (enhanced vaccine for patients older than 65 years).
Changes to Medicare billing
Some of the coding and billing changes this year that have an impact on ObGyn practice come from the Centers of Medicare and Medicaid Services (CMS) and the Affordable Care Act.
TIMELY FILING
The Affordable Care Act calls for a reduction in the maximum time period for submission of Medicare fee-for-service claims. Before January 1, a provider had 15 to 27 months to submit first-time claims to Medicare. Now, these claims must be filed within a calendar year of the date of service. Exceptions can be made for retroactive entitlement or in situations in which there is a secondary payer.
PAYMENTS TO CERTIFIED NURSE MIDWIVES
Next, more good news—if you employ a certified nurse midwife (CNM) in your practice. Before January 1, Medicare reimbursed direct billing from a CNM at only 65% of the Medicare Physician Fee Schedule. Now, a CNM is paid the same as a physician when she (he) bills under her own number.
In the past, some practices billed for the services of a CNM under “incident to” rules, to capture the physician payment—but this also meant that the CNM could not see a new patient. Under the change I’m describing, all CNMs can bill Medicare directly; see new patients; and be paid the same as the physician is paid. In addition, CNMs are no longer required to be supervised by a physician when they perform diagnostic tests that fall under the scope of their practice.
ANNUAL WELLNESS VISIT
The Affordable Care Act extended preventive coverage to Medicare beneficiaries in the form of an annual wellness visit. The two new codes here have been valued based on a level 4-problem new and established E/M service:
G0438 Annual wellness visit, including personalized prevention plan services, first visit
G0439 Annual wellness visit, including personalized prevention plan services, subsequent visit
Payment for the initial visit is made only beginning the second year the patient is eligible for Medicare Part B—during the first year of coverage, only the Initial Preventive Physical Examination (IPPE) (the “Welcome to Medicare”) exam will be covered.
CMS has stated that only one physician will be paid for the initial visit; when the patient returns to the same or a new physician in the third year, only a subsequent visit will be paid. It is, therefore, important that this information be conveyed to any new physician who sees the patient.
The annual codes can be billed in addition to any other preventive service, such as G0101 or Q0091; no modifier is needed for this combination. Medicare has waived both the copayment and the deductible for the annual wellness visit, as well as all Medicare-covered preventive services that have been recommended with a grade of “A” (“strongly recommends”) or “B” (“recommends”) by the US Preventive Services Task Force.
The annual wellness visit requires seven elements at a minimum (i.e., you may document and perform more elements than this, but not fewer):
- Establish or update the patient’s medical and family history
- List her current medical providers and suppliers and all prescribed medications
- Record measurements of height, weight, body mass index (initial visit only), blood pressure, and other routine measurements
- Detect any cognitive impairment
- Establish or update a screening schedule for the next 5 to 10 years, including screenings appropriate for the general population, and any additional screenings that may be appropriate because of her particular risk factors
- Review the patient’s 1) potential (i.e., risk factors) for depression, based on use of an appropriate screening instrument, and 2) functional ability and level of safety based on direct observation or screening questions
- Furnish 1) personalized health advice and 2) refer her appropriately to health education or preventive services.
CMS has also indicated that, although they will pay for a problem E/M service and the annual wellness visit on the same date of service with a modifier -25 added to the E/M service, they expect this type of billing to be rare—because of the nature of the wellness visit, which is time-intensive. They also expect that, given these requirements, the patient will not be billed additionally for a noncovered preventive service.
We want to hear from you! Tell us what you think.
The Current Procedural Terminology (CPT) code set for 2011 includes several changes of interest to ObGyns. These include 1) guideline clarifications regarding wound debridement and obstetric care codes; 2) new codes for subsequent observation care; micro-remodeling of the bladder neck; insertion of a vaginal after-loading device; and 3) a lab code for detecting amniotic fluid in cervicovaginal secretions (using the AmniSure kit).
There is also a new code for vaccine counseling that will have an impact on you if your practice offers the human papillomavirus (HPV) vaccine to patients younger than 19 years.
There are changes to Medicare this year that you should take note of if you care for these patients, particularly in the area of preventive visit billing.
CPT and Medicare changes both took effect on January 1. The Health Insurance Portability and Accountability Act (HIPAA) requires that insurers accepted the new codes on that date.
Changes to the CPT code set
OBSERVATION CARE
One of the biggest headaches for medical practices has been standardized coding and billing for observation care that lasts more than 1 day. In the past, payers accepted a problem E/M for Day 2 of observation care, or instructed practices to code an unlisted E/M service. Now, you may report all care rendered in the observation setting with the addition of three new codes for subsequent care:
99244 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: problem focused interval history, problem focused examination; medical decision making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
99225 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: an expanded problem focused interval history; an expanded problem focused examination; medical decision making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
99226 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: a detailed interval history; a detailed examination; medical decision making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Note that each of these codes 1) “suggests” the status of the patient for each level of billing, and 2) includes a typical time. This means that, unlike the observation care admission codes or the observation admission/same-day discharge codes, time that is spent with the patient, or on the unit, may be used to select the code—if you document 1) the requirement that more than 50% of the typical time was spent on counseling or coordination of care, or both, and 2) a detailed description of this activity.
Codes for wound debridement were given a facelift with the addition of a new guideline that addresses both surgical and medical debridement. The surgical debridement codes, (11042–11047) are now reported on the basis of the depth of tissue removed and the surface area of the wound. This means that codes 11040 and 11041 were deleted to make room for new and revised codes.
This change will mean that, when you report these codes, you will need to document more information to bill. It’s also understood that coding separately for debridement of dermis or epidermis at the same time you code for debriding underlying structures would be inappropriate.
CPT has also indicated that active wound management codes 97597 and 97598 can now be reported by physicians or nonphysician providers as long as the provider has direct (one-on-one) contact. These codes should be reported for skin-surface debridement only.
The new and revised codes (some of which have been published in CPT in nonsequential order) are:
11042 Debridement, subcutaneous tissue (includes epidermis and dermis, if performed); first 20 sq cm or less
+11045 (new add-on code reported with 11042 only) each additional 20 sq cm or part thereof
11043 Debridement, muscle and/or facia (includes epidermis, dermis, and subcutaneous tissue, if performed); first 20 sq cm or less
+11046 (new add-on code reported with 11043 only) each additional 20 sq cm or part thereof
11044 Debridement, bone (includes epidermis, dermis, subcutaneous tissue, muscle and/or fascia, if performed); first 20 sq cm or less
+11047 (new add-on code reported with 11044 only) each additional 20 sq cm or part thereof
97597 Debridement (e.g., high pressure waterjet with/without suction, sharp selective debridement with scissors, scalpel and forceps), open wound, (e.g., fibrin, devitalized epidermis and/or dermis, exudate, debris, biofilm), including topical application(s), wound assessment, use of a whirlpool, when performed and instruction(s) for ongoing care, per session, total wound(s) surface area; first 20 sq cm or less
+95798 (add-on code reported with 97597 only) Each additional 20 sq cm, or part thereof.
TRANSURETHRAL RADIOFREQUENCY
Category III code 0193T, which described transurethral radiofrequency micro-remodeling for stress urinary incontinence, has been deleted and converted to a Category I CPT code, 53860 (Transurethral radiofrequency micro-remodeling of the female bladder neck and proximal urethra for stress urinary incontinence). The procedure includes a periurethral block and flushing the bladder with a lidocaine slurry, and can be performed in the office.
In all, the procedure requires nine treatment cycles during the session, but the code is billed only once. Catheterization and measurement of a voiding sample after the procedure are included in the code.
AFTERLOADING DEVICES FOR CLINICAL BRACHYTHERAPY
CPT revised—slightly—existing code 57155, and added code 57156 (Insertion of a vaginal radiation afterloading apparatus for clinical brachytherapy).
- Code 57155 was revised to clarify that only a single tandem is inserted into the uterus. There had been confusion earlier in this regard.
- The new code describes a procedure that may also include dilation of the vaginal canal to remove postradiation adhesions. That procedure also involves 1) placement of bladder and rectal catheters and 2) radiographic imaging to confirm placement, which are not coded separately.
CLARIFICATION OF OBSTETRIC GUIDELINES
Been having problems with payers and their interpretation of the delivery only, postpartum only, and delivery with postpartum care codes? CPT has, at last, clarified what you can, and cannot, bill in those circumstances. (Keep in mind, however, that you may not unbundle these procedures if more extensive care is provided: Most payers want you to bill the global OB care code that includes antepartum, intrapartum, and postpartum care.)
In some cases (such as Medicaid), the payer stipulates that only the physician who actually performed the delivery may bill for it, even if the delivering physician is covering for, or is a member of, the same group practice as the primary attending of record. The “delivery-only” codes should be reported when 1) an unaffiliated physician has delivered the baby but will not be providing any outpatient postpartum care or 2) the payer has specified this method of billing for the covering or affiliated provider.
CPT has clarified that delivery-only codes (59409, 59514, or 59612, 59620) include admission to the hospital, the admission history and physical exam, uncomplicated labor and delivery (including delivery of the placenta, or use of forceps or vacuum extraction). These codes do not include inpatient rounding or discharge day care after delivery (and, of course, include no outpatient postpartum care). When, as the delivering physician, you also provide inpatient postdelivery care, therefore, you may additionally bill subsequent hospital care codes and discharge day management codes (99231-99233, 99238-99239).
If the unaffiliated physician performs the delivery and also intends on providing outpatient postpartum care, the CPT codes for delivery with postpartum are to be reported (59410, 59515, 59614, 59622). In addition to the delivery, these codes include all inpatient and outpatient postpartum care. And finally, for those physicians who are only providing outpatient postpartum care, the code 59430, Postpartum care only, should be reported.
PLACENTAL ALPHA MICROGLOBULIN-1
A new code, 84112 (Placental alpha microglobulin-1 [PAMG-11], cervicovaginal secretion, qualitative), has been added to allow the clinical laboratory to bill for this immunoassay that detects amniotic fluid in the secretions. Physician work involves collection of the specimen but, under CPT rules, collection is included as part of any E/M service.
Note: An existing code for this test that is used by Blue Cross/Blue Shield payers (S3628) remains valid in 2011.
HPV VACCINE COUNSELING
Before January 1, 2011, if you counseled a patient about the HPV vaccine, you could report preventive counseling codes, such as 99401–99404, in addition to the vaccine administration code, 90471 (Immunization administration, 1 vaccine). Now, however, you have a new code for counseling and vaccine administration for a patient who is younger than 19 years—the age group most likely to be counseled about this vaccine. When you see, and counsel, such a patient before administering the vaccine, on the same date of service, code 90460 (Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qualified health care profession; first vaccine/toxoid component), and 90649 for the quadrivalent or 90650 for the bivalent HPV vaccine.
If your patient is 19 years or older and requires counseling, continue to bill 99401– 99404 for counseling, with 90471 for immunization and 90649 or 90650 for the vaccine. Keep in mind: Whether you report 90460 or the 9940X codes, you are required to document the content of the counseling. Codes 9940X also require documentation of the duration of counseling.
INFLUENZA VACCINE
New codes have been established for the flu vaccine, but you won’t be using them: They are intended to address future pandemic strains of influenza. This year’s vaccine contains the H1N1 strain, but is coded as the normal seasonal flu vaccine, based on the type given:
90656 (preservative-free)
90658 (split virus)
90660 (intranasal)
90662 (enhanced vaccine for patients older than 65 years).
Changes to Medicare billing
Some of the coding and billing changes this year that have an impact on ObGyn practice come from the Centers of Medicare and Medicaid Services (CMS) and the Affordable Care Act.
TIMELY FILING
The Affordable Care Act calls for a reduction in the maximum time period for submission of Medicare fee-for-service claims. Before January 1, a provider had 15 to 27 months to submit first-time claims to Medicare. Now, these claims must be filed within a calendar year of the date of service. Exceptions can be made for retroactive entitlement or in situations in which there is a secondary payer.
PAYMENTS TO CERTIFIED NURSE MIDWIVES
Next, more good news—if you employ a certified nurse midwife (CNM) in your practice. Before January 1, Medicare reimbursed direct billing from a CNM at only 65% of the Medicare Physician Fee Schedule. Now, a CNM is paid the same as a physician when she (he) bills under her own number.
In the past, some practices billed for the services of a CNM under “incident to” rules, to capture the physician payment—but this also meant that the CNM could not see a new patient. Under the change I’m describing, all CNMs can bill Medicare directly; see new patients; and be paid the same as the physician is paid. In addition, CNMs are no longer required to be supervised by a physician when they perform diagnostic tests that fall under the scope of their practice.
ANNUAL WELLNESS VISIT
The Affordable Care Act extended preventive coverage to Medicare beneficiaries in the form of an annual wellness visit. The two new codes here have been valued based on a level 4-problem new and established E/M service:
G0438 Annual wellness visit, including personalized prevention plan services, first visit
G0439 Annual wellness visit, including personalized prevention plan services, subsequent visit
Payment for the initial visit is made only beginning the second year the patient is eligible for Medicare Part B—during the first year of coverage, only the Initial Preventive Physical Examination (IPPE) (the “Welcome to Medicare”) exam will be covered.
CMS has stated that only one physician will be paid for the initial visit; when the patient returns to the same or a new physician in the third year, only a subsequent visit will be paid. It is, therefore, important that this information be conveyed to any new physician who sees the patient.
The annual codes can be billed in addition to any other preventive service, such as G0101 or Q0091; no modifier is needed for this combination. Medicare has waived both the copayment and the deductible for the annual wellness visit, as well as all Medicare-covered preventive services that have been recommended with a grade of “A” (“strongly recommends”) or “B” (“recommends”) by the US Preventive Services Task Force.
The annual wellness visit requires seven elements at a minimum (i.e., you may document and perform more elements than this, but not fewer):
- Establish or update the patient’s medical and family history
- List her current medical providers and suppliers and all prescribed medications
- Record measurements of height, weight, body mass index (initial visit only), blood pressure, and other routine measurements
- Detect any cognitive impairment
- Establish or update a screening schedule for the next 5 to 10 years, including screenings appropriate for the general population, and any additional screenings that may be appropriate because of her particular risk factors
- Review the patient’s 1) potential (i.e., risk factors) for depression, based on use of an appropriate screening instrument, and 2) functional ability and level of safety based on direct observation or screening questions
- Furnish 1) personalized health advice and 2) refer her appropriately to health education or preventive services.
CMS has also indicated that, although they will pay for a problem E/M service and the annual wellness visit on the same date of service with a modifier -25 added to the E/M service, they expect this type of billing to be rare—because of the nature of the wellness visit, which is time-intensive. They also expect that, given these requirements, the patient will not be billed additionally for a noncovered preventive service.
We want to hear from you! Tell us what you think.
The Current Procedural Terminology (CPT) code set for 2011 includes several changes of interest to ObGyns. These include 1) guideline clarifications regarding wound debridement and obstetric care codes; 2) new codes for subsequent observation care; micro-remodeling of the bladder neck; insertion of a vaginal after-loading device; and 3) a lab code for detecting amniotic fluid in cervicovaginal secretions (using the AmniSure kit).
There is also a new code for vaccine counseling that will have an impact on you if your practice offers the human papillomavirus (HPV) vaccine to patients younger than 19 years.
There are changes to Medicare this year that you should take note of if you care for these patients, particularly in the area of preventive visit billing.
CPT and Medicare changes both took effect on January 1. The Health Insurance Portability and Accountability Act (HIPAA) requires that insurers accepted the new codes on that date.
Changes to the CPT code set
OBSERVATION CARE
One of the biggest headaches for medical practices has been standardized coding and billing for observation care that lasts more than 1 day. In the past, payers accepted a problem E/M for Day 2 of observation care, or instructed practices to code an unlisted E/M service. Now, you may report all care rendered in the observation setting with the addition of three new codes for subsequent care:
99244 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: problem focused interval history, problem focused examination; medical decision making that is straightforward or of low complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is stable, recovering, or improving. Physicians typically spend 15 minutes at the bedside and on the patient’s hospital floor or unit.
99225 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: an expanded problem focused interval history; an expanded problem focused examination; medical decision making of moderate complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is responding inadequately to therapy or has developed a minor complication. Physicians typically spend 25 minutes at the bedside and on the patient’s hospital floor or unit.
99226 Subsequent observation care, per day, for the evaluation and management of a patient, which requires at least 2 of these 3 key components: a detailed interval history; a detailed examination; medical decision making of high complexity. Counseling and/or coordination of care with other providers or agencies are provided consistent with the nature of the problem(s) and the patient’s and/or family’s needs. Usually, the patient is unstable or has developed a significant complication or a significant new problem. Physicians typically spend 35 minutes at the bedside and on the patient’s hospital floor or unit.
Note that each of these codes 1) “suggests” the status of the patient for each level of billing, and 2) includes a typical time. This means that, unlike the observation care admission codes or the observation admission/same-day discharge codes, time that is spent with the patient, or on the unit, may be used to select the code—if you document 1) the requirement that more than 50% of the typical time was spent on counseling or coordination of care, or both, and 2) a detailed description of this activity.
Codes for wound debridement were given a facelift with the addition of a new guideline that addresses both surgical and medical debridement. The surgical debridement codes, (11042–11047) are now reported on the basis of the depth of tissue removed and the surface area of the wound. This means that codes 11040 and 11041 were deleted to make room for new and revised codes.
This change will mean that, when you report these codes, you will need to document more information to bill. It’s also understood that coding separately for debridement of dermis or epidermis at the same time you code for debriding underlying structures would be inappropriate.
CPT has also indicated that active wound management codes 97597 and 97598 can now be reported by physicians or nonphysician providers as long as the provider has direct (one-on-one) contact. These codes should be reported for skin-surface debridement only.
The new and revised codes (some of which have been published in CPT in nonsequential order) are:
11042 Debridement, subcutaneous tissue (includes epidermis and dermis, if performed); first 20 sq cm or less
+11045 (new add-on code reported with 11042 only) each additional 20 sq cm or part thereof
11043 Debridement, muscle and/or facia (includes epidermis, dermis, and subcutaneous tissue, if performed); first 20 sq cm or less
+11046 (new add-on code reported with 11043 only) each additional 20 sq cm or part thereof
11044 Debridement, bone (includes epidermis, dermis, subcutaneous tissue, muscle and/or fascia, if performed); first 20 sq cm or less
+11047 (new add-on code reported with 11044 only) each additional 20 sq cm or part thereof
97597 Debridement (e.g., high pressure waterjet with/without suction, sharp selective debridement with scissors, scalpel and forceps), open wound, (e.g., fibrin, devitalized epidermis and/or dermis, exudate, debris, biofilm), including topical application(s), wound assessment, use of a whirlpool, when performed and instruction(s) for ongoing care, per session, total wound(s) surface area; first 20 sq cm or less
+95798 (add-on code reported with 97597 only) Each additional 20 sq cm, or part thereof.
TRANSURETHRAL RADIOFREQUENCY
Category III code 0193T, which described transurethral radiofrequency micro-remodeling for stress urinary incontinence, has been deleted and converted to a Category I CPT code, 53860 (Transurethral radiofrequency micro-remodeling of the female bladder neck and proximal urethra for stress urinary incontinence). The procedure includes a periurethral block and flushing the bladder with a lidocaine slurry, and can be performed in the office.
In all, the procedure requires nine treatment cycles during the session, but the code is billed only once. Catheterization and measurement of a voiding sample after the procedure are included in the code.
AFTERLOADING DEVICES FOR CLINICAL BRACHYTHERAPY
CPT revised—slightly—existing code 57155, and added code 57156 (Insertion of a vaginal radiation afterloading apparatus for clinical brachytherapy).
- Code 57155 was revised to clarify that only a single tandem is inserted into the uterus. There had been confusion earlier in this regard.
- The new code describes a procedure that may also include dilation of the vaginal canal to remove postradiation adhesions. That procedure also involves 1) placement of bladder and rectal catheters and 2) radiographic imaging to confirm placement, which are not coded separately.
CLARIFICATION OF OBSTETRIC GUIDELINES
Been having problems with payers and their interpretation of the delivery only, postpartum only, and delivery with postpartum care codes? CPT has, at last, clarified what you can, and cannot, bill in those circumstances. (Keep in mind, however, that you may not unbundle these procedures if more extensive care is provided: Most payers want you to bill the global OB care code that includes antepartum, intrapartum, and postpartum care.)
In some cases (such as Medicaid), the payer stipulates that only the physician who actually performed the delivery may bill for it, even if the delivering physician is covering for, or is a member of, the same group practice as the primary attending of record. The “delivery-only” codes should be reported when 1) an unaffiliated physician has delivered the baby but will not be providing any outpatient postpartum care or 2) the payer has specified this method of billing for the covering or affiliated provider.
CPT has clarified that delivery-only codes (59409, 59514, or 59612, 59620) include admission to the hospital, the admission history and physical exam, uncomplicated labor and delivery (including delivery of the placenta, or use of forceps or vacuum extraction). These codes do not include inpatient rounding or discharge day care after delivery (and, of course, include no outpatient postpartum care). When, as the delivering physician, you also provide inpatient postdelivery care, therefore, you may additionally bill subsequent hospital care codes and discharge day management codes (99231-99233, 99238-99239).
If the unaffiliated physician performs the delivery and also intends on providing outpatient postpartum care, the CPT codes for delivery with postpartum are to be reported (59410, 59515, 59614, 59622). In addition to the delivery, these codes include all inpatient and outpatient postpartum care. And finally, for those physicians who are only providing outpatient postpartum care, the code 59430, Postpartum care only, should be reported.
PLACENTAL ALPHA MICROGLOBULIN-1
A new code, 84112 (Placental alpha microglobulin-1 [PAMG-11], cervicovaginal secretion, qualitative), has been added to allow the clinical laboratory to bill for this immunoassay that detects amniotic fluid in the secretions. Physician work involves collection of the specimen but, under CPT rules, collection is included as part of any E/M service.
Note: An existing code for this test that is used by Blue Cross/Blue Shield payers (S3628) remains valid in 2011.
HPV VACCINE COUNSELING
Before January 1, 2011, if you counseled a patient about the HPV vaccine, you could report preventive counseling codes, such as 99401–99404, in addition to the vaccine administration code, 90471 (Immunization administration, 1 vaccine). Now, however, you have a new code for counseling and vaccine administration for a patient who is younger than 19 years—the age group most likely to be counseled about this vaccine. When you see, and counsel, such a patient before administering the vaccine, on the same date of service, code 90460 (Immunization administration through 18 years of age via any route of administration, with counseling by physician or other qualified health care profession; first vaccine/toxoid component), and 90649 for the quadrivalent or 90650 for the bivalent HPV vaccine.
If your patient is 19 years or older and requires counseling, continue to bill 99401– 99404 for counseling, with 90471 for immunization and 90649 or 90650 for the vaccine. Keep in mind: Whether you report 90460 or the 9940X codes, you are required to document the content of the counseling. Codes 9940X also require documentation of the duration of counseling.
INFLUENZA VACCINE
New codes have been established for the flu vaccine, but you won’t be using them: They are intended to address future pandemic strains of influenza. This year’s vaccine contains the H1N1 strain, but is coded as the normal seasonal flu vaccine, based on the type given:
90656 (preservative-free)
90658 (split virus)
90660 (intranasal)
90662 (enhanced vaccine for patients older than 65 years).
Changes to Medicare billing
Some of the coding and billing changes this year that have an impact on ObGyn practice come from the Centers of Medicare and Medicaid Services (CMS) and the Affordable Care Act.
TIMELY FILING
The Affordable Care Act calls for a reduction in the maximum time period for submission of Medicare fee-for-service claims. Before January 1, a provider had 15 to 27 months to submit first-time claims to Medicare. Now, these claims must be filed within a calendar year of the date of service. Exceptions can be made for retroactive entitlement or in situations in which there is a secondary payer.
PAYMENTS TO CERTIFIED NURSE MIDWIVES
Next, more good news—if you employ a certified nurse midwife (CNM) in your practice. Before January 1, Medicare reimbursed direct billing from a CNM at only 65% of the Medicare Physician Fee Schedule. Now, a CNM is paid the same as a physician when she (he) bills under her own number.
In the past, some practices billed for the services of a CNM under “incident to” rules, to capture the physician payment—but this also meant that the CNM could not see a new patient. Under the change I’m describing, all CNMs can bill Medicare directly; see new patients; and be paid the same as the physician is paid. In addition, CNMs are no longer required to be supervised by a physician when they perform diagnostic tests that fall under the scope of their practice.
ANNUAL WELLNESS VISIT
The Affordable Care Act extended preventive coverage to Medicare beneficiaries in the form of an annual wellness visit. The two new codes here have been valued based on a level 4-problem new and established E/M service:
G0438 Annual wellness visit, including personalized prevention plan services, first visit
G0439 Annual wellness visit, including personalized prevention plan services, subsequent visit
Payment for the initial visit is made only beginning the second year the patient is eligible for Medicare Part B—during the first year of coverage, only the Initial Preventive Physical Examination (IPPE) (the “Welcome to Medicare”) exam will be covered.
CMS has stated that only one physician will be paid for the initial visit; when the patient returns to the same or a new physician in the third year, only a subsequent visit will be paid. It is, therefore, important that this information be conveyed to any new physician who sees the patient.
The annual codes can be billed in addition to any other preventive service, such as G0101 or Q0091; no modifier is needed for this combination. Medicare has waived both the copayment and the deductible for the annual wellness visit, as well as all Medicare-covered preventive services that have been recommended with a grade of “A” (“strongly recommends”) or “B” (“recommends”) by the US Preventive Services Task Force.
The annual wellness visit requires seven elements at a minimum (i.e., you may document and perform more elements than this, but not fewer):
- Establish or update the patient’s medical and family history
- List her current medical providers and suppliers and all prescribed medications
- Record measurements of height, weight, body mass index (initial visit only), blood pressure, and other routine measurements
- Detect any cognitive impairment
- Establish or update a screening schedule for the next 5 to 10 years, including screenings appropriate for the general population, and any additional screenings that may be appropriate because of her particular risk factors
- Review the patient’s 1) potential (i.e., risk factors) for depression, based on use of an appropriate screening instrument, and 2) functional ability and level of safety based on direct observation or screening questions
- Furnish 1) personalized health advice and 2) refer her appropriately to health education or preventive services.
CMS has also indicated that, although they will pay for a problem E/M service and the annual wellness visit on the same date of service with a modifier -25 added to the E/M service, they expect this type of billing to be rare—because of the nature of the wellness visit, which is time-intensive. They also expect that, given these requirements, the patient will not be billed additionally for a noncovered preventive service.
We want to hear from you! Tell us what you think.
IN THIS ARTICLE