User login
VA Academic Detailing Service: Implementation and Lessons Learned
National and international studies have shown that academic detailing (AD) interventions improve the quality of evidence-based health care and provide a positive return on investment.1-5 Many health care systems are investing in AD to improve patient care. Existing systems typically tasked with containing drug costs address neither underprescribing and overselection of high-risk agents, which could result in adverse outcomes, nor nondrug alternatives to treatment.
Academic detailing uses marketing strategies (similar to those of the pharmaceutical industry) to deliver evidence-based information to health care providers (HCPs) but without sales goals. The information is disseminated primarily through one-on-one and small-group educational outreach sessions. The goal of AD is to influence clinician decision making and care delivery behavior and promote evidence-based treatment and monitoring. The academic detailer focuses on delivering targeted messages, embedded within provider handouts, and uses audit and feedback tools to help the clinician identify patients for whom treatment plan change may be warranted. Clinicians also are given patient education tools to use in their discussions with veterans. These tools are used to help veterans take charge of their health. Academic detailing has an advantage over didactic lectures because it provides customized content and barrier resolution strategies to meet clinicians’ individual needs and local constraints.
Although the ability of AD to effectively improve the quality of medical care has been thoroughly studied, much less is known about the cost-effectiveness of AD. Historically, capturing the short- and long-term benefits and costs of AD interventions has been difficult. Eliminating AD’s confounding variables also has proven difficult.
Effectiveness of AD
Principal areas that impact the effectiveness of AD programs include geographic concentration of the medical issue across the prescriber population, differences in costs/outcomes between current practice and optimal practice, number of detailing sessions required to effect change, and the short- and long-term impact on outcomes. These considerations should influence the design of AD programs to gain maximum program efficiency and effectiveness.
Concentration of the Medical Issue
The more geographically concentrated the priority prescribers are, the greater the potential impact of AD. Geographic concentration can reduce travel and administrative costs. Prescribers also may have a high concentration of the targeted patient population; therefore, an intervention specifically targeting high-volume or geographically concentrated populations can be more efficient and effective.
Differences Between Current and Optimal Practice
Academic detailing is most effective when a large gap between desired practice and actual practice has been identified. An AD intervention may be highly cost-effective without immediately reducing overall health care costs. For example, if the gap in practice is due to undertreatment of a disease, then an AD intervention may increase short-term treatment costs but eventually achieve better long-term outcomes in the target population. However, establishing cause-and-effect relationships when dealing with long-term outcomes and confounding variables can be difficult.
Interventions in which the evidence is compelling and current practices are not well established may require only 1 AD visit to induce change. In addition, accelerated integration of the evidence into practice can be seen when operational changes, such as formulary restrictions or policies, are mandated. Multiple sessions often are required to effect change when the change is complicated to initiate, when a formidable learning curve exists, or where current practice is heavily ingrained. Subsequently, intensive discussions and an investment in designing practice delivery of the recommendation are needed to consistently achieve the care delivery goal.
Short- vs Long-Term Impact on Outcomes
For some interventions, specific and readily measurable changes occur almost immediately. For example, switching a high-cost medication to a low-cost alternative provides an immediate cost benefit. In other interventions, such as reduction of future complications, the benefits might be long-term. In such cases, a longer period and a more complex analysis are necessary to measure the impact.
Academic Detailing Service
In 2010, a VA AD Service pilot program began as an intervention to improve evidence-based treatment of mental illness. The pilot was funded through the VA T21 Healthcare Transformational Initiatives, which are designed to support new programs that enhance veteran-centric health care. The VISN 21 and 22 pilot locations included 11 medical centers and 73 clinics in Nevada, California, the Pacific Islands, and the Philippines.
An oversight steering committee was formed. It included leaders from Patient Care Services, Mental Health Services (MHS), and Pharmacy Benefits Management Services (PBM). Clinical pharmacy specialists (CPSs) were chosen to function as academic detailers because they are considered medication experts by prescribers and health care teams. The pilot employed 6.0 full-time employment equivalents (FTEEs) CPSs who were residency trained, held doctorate degrees in pharmacy, and had VA practice experience. The VA AD Service used several strategies to promote evidence-based treatment of common mental health disorders.
Program Materials
The key components of the VA AD Service were educational outreach programming, informatics tool development and dissemination, and barrier resolution. The first step in each campaign was the development of educational program materials designed to facilitate discussion and promote evidence-based practice. The academic detailers along with key VA thought leaders developed provider handouts, provider pocket cards, and patient education materials to support each educational topic. The program materials required the translation of evidence-based research into clinical practice and strategic educational and operational development by individuals who understand complex pharmacotherapy.
Provider handouts, embedded with key messages, served as a summary guide to the information presented and included action statements that highlighted recommendations that would influence behaviors. The handout content reflected recommendations based on the VA/DoD Practice Guidelines, the VA National Formulary, and relevant new and emerging literature on the mental health topic being addressed. When possible, existing VA/DoD and MHS educational resources were used to supplement the handouts.
The pocket cards provided actionable information about treatment recommendations. For example, the provider handout for posttraumatic stress disorder (PTSD) recommended to “consider prazosin for use in veterans with combat associated nightmares” and reviewed the literature to support that recommendation. These pocket cards also provided information on prazosin dosing, titration, common drug interactions, and adverse effects. In addition, patient education resources such as handouts and brochures were designed to engage veterans in their mental health care. These educational materials were vital to ensuring the VA workforce and the veterans being served were well educated on evidence-based treatment and acting on the evolving information produced by the latest research.
Academic detailers used these tools during educational outreach sessions to inform and assess the provider’s knowledge of evidence-based treatment and to review areas where the provider desired further education of the evidence. These educational sessions focused on leadership in mental health, pharmacy service, the medical center overall, and priority clinicians identified as having the greatest opportunity for change. Academic detailers also met with the priority provider clinical support teams (nurses, pharmacists, social workers, psychologists, dieticians, etc) to ensure that the message passed along to veterans was consistent among all team members. Clinicians with the greatest opportunity for change, or priority HCPs, varied based on the particular educational topic. For example, if the educational topic were focused on PTSD, prescribers with large panels of patients with PTSD would be prioritized. Investment in the educational outreach specifically identified clinicians who had the greatest opportunity to transform practice with the clinical recommendations, which in turn, identified the greatest opportunity for the academic detailer to influence behavior changes and improve health care for veterans.
Dashboard
Clinicians were identified by the AD Service using the AD dashboard. This informatics tool included actionable patient information, which was developed for each educational topic. The dashboards were available for use by both academic detailers and clinical team members to support evidence-based treatment and to seek patients who might benefit from an evaluation of care. These audit and feedback tools leveraged regional and national data to produce a clinical performance dashboard that generated visually intuitive reports at the VISN, station, provider, and individual patient levels. Data collection for the dashboards included robust and complex data sets that were updated daily. These tools allowed clinicians to see a snapshot of their patient panel and assess patient-level information in order to change individual care.
Barrier resolution and implementation support is another important aspect of the VA AD program. Education without system solutions is cause for provider and patient frustration. Academic detailers worked with their local site to identify available resources, and they often resolved problems within the system to promote evidence-based treatment. Examples included assisting with the clozapine registration process, creating quick orders to assist with dosing for commonly used medications, and creating treatment letters within the computer system that HCPs could quickly send to the patient. Each academic detailer also worked with local facilities to assess where policies and protocols could support the AD campaign initiatives. Resources at each VA required tailored solutions and collaboration with leadership, and clinicians at each site were key to a successful AD program.
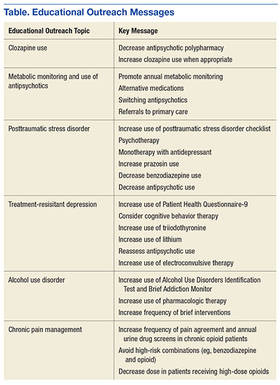
Educational outreach topics covered thus far by the VA AD program include clozapine utilization, metabolic monitoring and use of antipsychotics, PTSD, treatment-resistant depression, alcohol use disorder, and chronic pain management. Each topic focused on specific key messages or key points that are emphasized during the detailing visit with the provider (Table).
Lessons Learned
This pilot program identified several changes that should be considered for future implementation. First, leadership must endorse and support educational sessions with clinicians. Introduction of educational programming begins with creating a collaborative relationship with health care system leadership. Each medical center in the pilot program had an infrastructure of Mental Health, Primary Care, and Pharmacy Service leaders who supported the AD program. In addition, AD Service participation on committees, such as Mental Health Executive Committee, Mental Health Task Force, VISN PBM, and Medication Safety, allows the AD program’s members to network with clinicians and align its key messages with the goals of the facility and leadership. Aligning with existing programs enhances and promotes resources for clinicians and supports leadership and performance goals.
To collaborate, HCPs needs to understand how the AD program benefits them. Before clinicians are approached regarding participation, the AD program should be developed into a branded collaborative program that offers numerous benefits to them, their practice, and their patients. The program must provide a clear and credible answer to the question, “Why should I spend my time meeting with you?”
Second, reaching HCPs for face-to-face encounters over large geographic areas requires an organized network of academic detailers with adequate administrative support. Partnerships with staff already present in the clinic are essential for consistent reinforcement and delivery of the key messages. These partnerships allow station-level staff to continually identify opportunities to act on the key messages. By using local champions, the AD Service can effectively cover a large territory. Providing education to remote facilities can be done by telephone or video teleconferencing.
Third, many HCPs recognize the value this program can add to their practice and have requested follow-up sessions with the academic detailers. To better understand the needs, baseline knowledge, readiness, and receptivity of target audiences, the AD Service should deploy an informal needs assessment to HCPs. The feedback can be used to prepare the appropriate strategies and messaging during AD sessions.
Fourth, the VA chose to use CPSs with experience working as provider extenders for medication management as the primary academic detailers for this pilot. It should be noted that AD services in other national and international systems are successfully performed by other types of HCPs with this same level of qualifications and expertise. Regardless of profession, the academic detailer must have the qualifications and expertise necessary to empower clinical personnel. Without this expertise, provider buy-in is difficult to obtain. As a result, behavior change will be less likely. Pharmacists currently serve as the drug information experts for patients and health care teams. They are valued across professions for their knowledge of medication management, and they have the capacity to recommend nonpharmacologic evidence-based treatments. In addition, using drug information experts as academic detailers allows them to serve as a resource for more complex patient cases.
Finally, providing real-time audit and feedback tools with educational resources gives clinicians tangible actions to improve the care they deliver and proactively target interventions anticipated in the upcoming appointments. It is helpful for HCPs to see the culture of their prescribing compared with prescribers across the network because this can identify areas for improvement and highlight strong practices. Use of audit and feedback tools with a team approach allows for delegation of duties where team members may contribute and collaborate to reach patient goals and improve patient care. Using information technology to deliver this product to health care teams is an important component of the AD program. For successful implementation, resources are needed from both clinicians and the Office of Information and Technology to develop and maintain these powerful tools.
Conclusion
The VA AD Service uses a multifaceted approach to promote the use of evidence-based treatment in veterans with mental illness. Academic detailers, along with key thought leaders, identified opportunities to improve care with solutions for applying evidenced-based medicine. Several items are considered necessary for successful AD program implementation, based on the pilot program. These included endorsement and support by leadership; needs assessment prior to key message development to fully understand the needs, baseline knowledge, readiness, and receptivity of target audiences; highly qualified academic detailers with the training, expertise, and communication skills necessary to empower clinical personnel; and real-time audit and feedback tools with education to give clinicians tangible actions to improve care.
The VA AD Service, including provision of educational services, clinical consultation, health systems barrier resolution, and audit and feedback tools, presents a new opportunity for pharmacists to improve the quality of care of veterans. The impact of the VA AD program on evidence-based care prescribing is being analyzed and will be reported in the future.
1. O’Brien MA, Rogers S, Jamtvedt G, et al. Educational outreach visits: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007;4:CD000409.
2. Meehan TP, Van Hoof TJ, Giannotti TE, et al. A descriptive study of educational outreach to promote use of quality improvement tools in primary care private practice. Am J Med Qual. 2009;24(2):90-98.
3. Simon SR, Rodriguez HP, Majumdar SR, et al. Economic analysis of a randomized trial of academic detailing interventions to improve use of antihypertensive medications. J Clin Hypertens (Greenwich). 2007;9(1):15-20.
4. Solomon DH, Van Houten L, Glynn RJ, et al. Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med. 2001;161(15):1897-1902
5. Patel B, Afghan S. Effects of an educational outreach campaign (IMPACT) on depression management delivered to general practitioners in one primary care trust. Ment Health Fam Med. 2009;6(3):155-162.
National and international studies have shown that academic detailing (AD) interventions improve the quality of evidence-based health care and provide a positive return on investment.1-5 Many health care systems are investing in AD to improve patient care. Existing systems typically tasked with containing drug costs address neither underprescribing and overselection of high-risk agents, which could result in adverse outcomes, nor nondrug alternatives to treatment.
Academic detailing uses marketing strategies (similar to those of the pharmaceutical industry) to deliver evidence-based information to health care providers (HCPs) but without sales goals. The information is disseminated primarily through one-on-one and small-group educational outreach sessions. The goal of AD is to influence clinician decision making and care delivery behavior and promote evidence-based treatment and monitoring. The academic detailer focuses on delivering targeted messages, embedded within provider handouts, and uses audit and feedback tools to help the clinician identify patients for whom treatment plan change may be warranted. Clinicians also are given patient education tools to use in their discussions with veterans. These tools are used to help veterans take charge of their health. Academic detailing has an advantage over didactic lectures because it provides customized content and barrier resolution strategies to meet clinicians’ individual needs and local constraints.
Although the ability of AD to effectively improve the quality of medical care has been thoroughly studied, much less is known about the cost-effectiveness of AD. Historically, capturing the short- and long-term benefits and costs of AD interventions has been difficult. Eliminating AD’s confounding variables also has proven difficult.
Effectiveness of AD
Principal areas that impact the effectiveness of AD programs include geographic concentration of the medical issue across the prescriber population, differences in costs/outcomes between current practice and optimal practice, number of detailing sessions required to effect change, and the short- and long-term impact on outcomes. These considerations should influence the design of AD programs to gain maximum program efficiency and effectiveness.
Concentration of the Medical Issue
The more geographically concentrated the priority prescribers are, the greater the potential impact of AD. Geographic concentration can reduce travel and administrative costs. Prescribers also may have a high concentration of the targeted patient population; therefore, an intervention specifically targeting high-volume or geographically concentrated populations can be more efficient and effective.
Differences Between Current and Optimal Practice
Academic detailing is most effective when a large gap between desired practice and actual practice has been identified. An AD intervention may be highly cost-effective without immediately reducing overall health care costs. For example, if the gap in practice is due to undertreatment of a disease, then an AD intervention may increase short-term treatment costs but eventually achieve better long-term outcomes in the target population. However, establishing cause-and-effect relationships when dealing with long-term outcomes and confounding variables can be difficult.
Interventions in which the evidence is compelling and current practices are not well established may require only 1 AD visit to induce change. In addition, accelerated integration of the evidence into practice can be seen when operational changes, such as formulary restrictions or policies, are mandated. Multiple sessions often are required to effect change when the change is complicated to initiate, when a formidable learning curve exists, or where current practice is heavily ingrained. Subsequently, intensive discussions and an investment in designing practice delivery of the recommendation are needed to consistently achieve the care delivery goal.
Short- vs Long-Term Impact on Outcomes
For some interventions, specific and readily measurable changes occur almost immediately. For example, switching a high-cost medication to a low-cost alternative provides an immediate cost benefit. In other interventions, such as reduction of future complications, the benefits might be long-term. In such cases, a longer period and a more complex analysis are necessary to measure the impact.
Academic Detailing Service
In 2010, a VA AD Service pilot program began as an intervention to improve evidence-based treatment of mental illness. The pilot was funded through the VA T21 Healthcare Transformational Initiatives, which are designed to support new programs that enhance veteran-centric health care. The VISN 21 and 22 pilot locations included 11 medical centers and 73 clinics in Nevada, California, the Pacific Islands, and the Philippines.
An oversight steering committee was formed. It included leaders from Patient Care Services, Mental Health Services (MHS), and Pharmacy Benefits Management Services (PBM). Clinical pharmacy specialists (CPSs) were chosen to function as academic detailers because they are considered medication experts by prescribers and health care teams. The pilot employed 6.0 full-time employment equivalents (FTEEs) CPSs who were residency trained, held doctorate degrees in pharmacy, and had VA practice experience. The VA AD Service used several strategies to promote evidence-based treatment of common mental health disorders.
Program Materials
The key components of the VA AD Service were educational outreach programming, informatics tool development and dissemination, and barrier resolution. The first step in each campaign was the development of educational program materials designed to facilitate discussion and promote evidence-based practice. The academic detailers along with key VA thought leaders developed provider handouts, provider pocket cards, and patient education materials to support each educational topic. The program materials required the translation of evidence-based research into clinical practice and strategic educational and operational development by individuals who understand complex pharmacotherapy.
Provider handouts, embedded with key messages, served as a summary guide to the information presented and included action statements that highlighted recommendations that would influence behaviors. The handout content reflected recommendations based on the VA/DoD Practice Guidelines, the VA National Formulary, and relevant new and emerging literature on the mental health topic being addressed. When possible, existing VA/DoD and MHS educational resources were used to supplement the handouts.
The pocket cards provided actionable information about treatment recommendations. For example, the provider handout for posttraumatic stress disorder (PTSD) recommended to “consider prazosin for use in veterans with combat associated nightmares” and reviewed the literature to support that recommendation. These pocket cards also provided information on prazosin dosing, titration, common drug interactions, and adverse effects. In addition, patient education resources such as handouts and brochures were designed to engage veterans in their mental health care. These educational materials were vital to ensuring the VA workforce and the veterans being served were well educated on evidence-based treatment and acting on the evolving information produced by the latest research.
Academic detailers used these tools during educational outreach sessions to inform and assess the provider’s knowledge of evidence-based treatment and to review areas where the provider desired further education of the evidence. These educational sessions focused on leadership in mental health, pharmacy service, the medical center overall, and priority clinicians identified as having the greatest opportunity for change. Academic detailers also met with the priority provider clinical support teams (nurses, pharmacists, social workers, psychologists, dieticians, etc) to ensure that the message passed along to veterans was consistent among all team members. Clinicians with the greatest opportunity for change, or priority HCPs, varied based on the particular educational topic. For example, if the educational topic were focused on PTSD, prescribers with large panels of patients with PTSD would be prioritized. Investment in the educational outreach specifically identified clinicians who had the greatest opportunity to transform practice with the clinical recommendations, which in turn, identified the greatest opportunity for the academic detailer to influence behavior changes and improve health care for veterans.
Dashboard
Clinicians were identified by the AD Service using the AD dashboard. This informatics tool included actionable patient information, which was developed for each educational topic. The dashboards were available for use by both academic detailers and clinical team members to support evidence-based treatment and to seek patients who might benefit from an evaluation of care. These audit and feedback tools leveraged regional and national data to produce a clinical performance dashboard that generated visually intuitive reports at the VISN, station, provider, and individual patient levels. Data collection for the dashboards included robust and complex data sets that were updated daily. These tools allowed clinicians to see a snapshot of their patient panel and assess patient-level information in order to change individual care.
Barrier resolution and implementation support is another important aspect of the VA AD program. Education without system solutions is cause for provider and patient frustration. Academic detailers worked with their local site to identify available resources, and they often resolved problems within the system to promote evidence-based treatment. Examples included assisting with the clozapine registration process, creating quick orders to assist with dosing for commonly used medications, and creating treatment letters within the computer system that HCPs could quickly send to the patient. Each academic detailer also worked with local facilities to assess where policies and protocols could support the AD campaign initiatives. Resources at each VA required tailored solutions and collaboration with leadership, and clinicians at each site were key to a successful AD program.
Educational outreach topics covered thus far by the VA AD program include clozapine utilization, metabolic monitoring and use of antipsychotics, PTSD, treatment-resistant depression, alcohol use disorder, and chronic pain management. Each topic focused on specific key messages or key points that are emphasized during the detailing visit with the provider (Table).
Lessons Learned
This pilot program identified several changes that should be considered for future implementation. First, leadership must endorse and support educational sessions with clinicians. Introduction of educational programming begins with creating a collaborative relationship with health care system leadership. Each medical center in the pilot program had an infrastructure of Mental Health, Primary Care, and Pharmacy Service leaders who supported the AD program. In addition, AD Service participation on committees, such as Mental Health Executive Committee, Mental Health Task Force, VISN PBM, and Medication Safety, allows the AD program’s members to network with clinicians and align its key messages with the goals of the facility and leadership. Aligning with existing programs enhances and promotes resources for clinicians and supports leadership and performance goals.
To collaborate, HCPs needs to understand how the AD program benefits them. Before clinicians are approached regarding participation, the AD program should be developed into a branded collaborative program that offers numerous benefits to them, their practice, and their patients. The program must provide a clear and credible answer to the question, “Why should I spend my time meeting with you?”
Second, reaching HCPs for face-to-face encounters over large geographic areas requires an organized network of academic detailers with adequate administrative support. Partnerships with staff already present in the clinic are essential for consistent reinforcement and delivery of the key messages. These partnerships allow station-level staff to continually identify opportunities to act on the key messages. By using local champions, the AD Service can effectively cover a large territory. Providing education to remote facilities can be done by telephone or video teleconferencing.
Third, many HCPs recognize the value this program can add to their practice and have requested follow-up sessions with the academic detailers. To better understand the needs, baseline knowledge, readiness, and receptivity of target audiences, the AD Service should deploy an informal needs assessment to HCPs. The feedback can be used to prepare the appropriate strategies and messaging during AD sessions.
Fourth, the VA chose to use CPSs with experience working as provider extenders for medication management as the primary academic detailers for this pilot. It should be noted that AD services in other national and international systems are successfully performed by other types of HCPs with this same level of qualifications and expertise. Regardless of profession, the academic detailer must have the qualifications and expertise necessary to empower clinical personnel. Without this expertise, provider buy-in is difficult to obtain. As a result, behavior change will be less likely. Pharmacists currently serve as the drug information experts for patients and health care teams. They are valued across professions for their knowledge of medication management, and they have the capacity to recommend nonpharmacologic evidence-based treatments. In addition, using drug information experts as academic detailers allows them to serve as a resource for more complex patient cases.
Finally, providing real-time audit and feedback tools with educational resources gives clinicians tangible actions to improve the care they deliver and proactively target interventions anticipated in the upcoming appointments. It is helpful for HCPs to see the culture of their prescribing compared with prescribers across the network because this can identify areas for improvement and highlight strong practices. Use of audit and feedback tools with a team approach allows for delegation of duties where team members may contribute and collaborate to reach patient goals and improve patient care. Using information technology to deliver this product to health care teams is an important component of the AD program. For successful implementation, resources are needed from both clinicians and the Office of Information and Technology to develop and maintain these powerful tools.
Conclusion
The VA AD Service uses a multifaceted approach to promote the use of evidence-based treatment in veterans with mental illness. Academic detailers, along with key thought leaders, identified opportunities to improve care with solutions for applying evidenced-based medicine. Several items are considered necessary for successful AD program implementation, based on the pilot program. These included endorsement and support by leadership; needs assessment prior to key message development to fully understand the needs, baseline knowledge, readiness, and receptivity of target audiences; highly qualified academic detailers with the training, expertise, and communication skills necessary to empower clinical personnel; and real-time audit and feedback tools with education to give clinicians tangible actions to improve care.
The VA AD Service, including provision of educational services, clinical consultation, health systems barrier resolution, and audit and feedback tools, presents a new opportunity for pharmacists to improve the quality of care of veterans. The impact of the VA AD program on evidence-based care prescribing is being analyzed and will be reported in the future.
National and international studies have shown that academic detailing (AD) interventions improve the quality of evidence-based health care and provide a positive return on investment.1-5 Many health care systems are investing in AD to improve patient care. Existing systems typically tasked with containing drug costs address neither underprescribing and overselection of high-risk agents, which could result in adverse outcomes, nor nondrug alternatives to treatment.
Academic detailing uses marketing strategies (similar to those of the pharmaceutical industry) to deliver evidence-based information to health care providers (HCPs) but without sales goals. The information is disseminated primarily through one-on-one and small-group educational outreach sessions. The goal of AD is to influence clinician decision making and care delivery behavior and promote evidence-based treatment and monitoring. The academic detailer focuses on delivering targeted messages, embedded within provider handouts, and uses audit and feedback tools to help the clinician identify patients for whom treatment plan change may be warranted. Clinicians also are given patient education tools to use in their discussions with veterans. These tools are used to help veterans take charge of their health. Academic detailing has an advantage over didactic lectures because it provides customized content and barrier resolution strategies to meet clinicians’ individual needs and local constraints.
Although the ability of AD to effectively improve the quality of medical care has been thoroughly studied, much less is known about the cost-effectiveness of AD. Historically, capturing the short- and long-term benefits and costs of AD interventions has been difficult. Eliminating AD’s confounding variables also has proven difficult.
Effectiveness of AD
Principal areas that impact the effectiveness of AD programs include geographic concentration of the medical issue across the prescriber population, differences in costs/outcomes between current practice and optimal practice, number of detailing sessions required to effect change, and the short- and long-term impact on outcomes. These considerations should influence the design of AD programs to gain maximum program efficiency and effectiveness.
Concentration of the Medical Issue
The more geographically concentrated the priority prescribers are, the greater the potential impact of AD. Geographic concentration can reduce travel and administrative costs. Prescribers also may have a high concentration of the targeted patient population; therefore, an intervention specifically targeting high-volume or geographically concentrated populations can be more efficient and effective.
Differences Between Current and Optimal Practice
Academic detailing is most effective when a large gap between desired practice and actual practice has been identified. An AD intervention may be highly cost-effective without immediately reducing overall health care costs. For example, if the gap in practice is due to undertreatment of a disease, then an AD intervention may increase short-term treatment costs but eventually achieve better long-term outcomes in the target population. However, establishing cause-and-effect relationships when dealing with long-term outcomes and confounding variables can be difficult.
Interventions in which the evidence is compelling and current practices are not well established may require only 1 AD visit to induce change. In addition, accelerated integration of the evidence into practice can be seen when operational changes, such as formulary restrictions or policies, are mandated. Multiple sessions often are required to effect change when the change is complicated to initiate, when a formidable learning curve exists, or where current practice is heavily ingrained. Subsequently, intensive discussions and an investment in designing practice delivery of the recommendation are needed to consistently achieve the care delivery goal.
Short- vs Long-Term Impact on Outcomes
For some interventions, specific and readily measurable changes occur almost immediately. For example, switching a high-cost medication to a low-cost alternative provides an immediate cost benefit. In other interventions, such as reduction of future complications, the benefits might be long-term. In such cases, a longer period and a more complex analysis are necessary to measure the impact.
Academic Detailing Service
In 2010, a VA AD Service pilot program began as an intervention to improve evidence-based treatment of mental illness. The pilot was funded through the VA T21 Healthcare Transformational Initiatives, which are designed to support new programs that enhance veteran-centric health care. The VISN 21 and 22 pilot locations included 11 medical centers and 73 clinics in Nevada, California, the Pacific Islands, and the Philippines.
An oversight steering committee was formed. It included leaders from Patient Care Services, Mental Health Services (MHS), and Pharmacy Benefits Management Services (PBM). Clinical pharmacy specialists (CPSs) were chosen to function as academic detailers because they are considered medication experts by prescribers and health care teams. The pilot employed 6.0 full-time employment equivalents (FTEEs) CPSs who were residency trained, held doctorate degrees in pharmacy, and had VA practice experience. The VA AD Service used several strategies to promote evidence-based treatment of common mental health disorders.
Program Materials
The key components of the VA AD Service were educational outreach programming, informatics tool development and dissemination, and barrier resolution. The first step in each campaign was the development of educational program materials designed to facilitate discussion and promote evidence-based practice. The academic detailers along with key VA thought leaders developed provider handouts, provider pocket cards, and patient education materials to support each educational topic. The program materials required the translation of evidence-based research into clinical practice and strategic educational and operational development by individuals who understand complex pharmacotherapy.
Provider handouts, embedded with key messages, served as a summary guide to the information presented and included action statements that highlighted recommendations that would influence behaviors. The handout content reflected recommendations based on the VA/DoD Practice Guidelines, the VA National Formulary, and relevant new and emerging literature on the mental health topic being addressed. When possible, existing VA/DoD and MHS educational resources were used to supplement the handouts.
The pocket cards provided actionable information about treatment recommendations. For example, the provider handout for posttraumatic stress disorder (PTSD) recommended to “consider prazosin for use in veterans with combat associated nightmares” and reviewed the literature to support that recommendation. These pocket cards also provided information on prazosin dosing, titration, common drug interactions, and adverse effects. In addition, patient education resources such as handouts and brochures were designed to engage veterans in their mental health care. These educational materials were vital to ensuring the VA workforce and the veterans being served were well educated on evidence-based treatment and acting on the evolving information produced by the latest research.
Academic detailers used these tools during educational outreach sessions to inform and assess the provider’s knowledge of evidence-based treatment and to review areas where the provider desired further education of the evidence. These educational sessions focused on leadership in mental health, pharmacy service, the medical center overall, and priority clinicians identified as having the greatest opportunity for change. Academic detailers also met with the priority provider clinical support teams (nurses, pharmacists, social workers, psychologists, dieticians, etc) to ensure that the message passed along to veterans was consistent among all team members. Clinicians with the greatest opportunity for change, or priority HCPs, varied based on the particular educational topic. For example, if the educational topic were focused on PTSD, prescribers with large panels of patients with PTSD would be prioritized. Investment in the educational outreach specifically identified clinicians who had the greatest opportunity to transform practice with the clinical recommendations, which in turn, identified the greatest opportunity for the academic detailer to influence behavior changes and improve health care for veterans.
Dashboard
Clinicians were identified by the AD Service using the AD dashboard. This informatics tool included actionable patient information, which was developed for each educational topic. The dashboards were available for use by both academic detailers and clinical team members to support evidence-based treatment and to seek patients who might benefit from an evaluation of care. These audit and feedback tools leveraged regional and national data to produce a clinical performance dashboard that generated visually intuitive reports at the VISN, station, provider, and individual patient levels. Data collection for the dashboards included robust and complex data sets that were updated daily. These tools allowed clinicians to see a snapshot of their patient panel and assess patient-level information in order to change individual care.
Barrier resolution and implementation support is another important aspect of the VA AD program. Education without system solutions is cause for provider and patient frustration. Academic detailers worked with their local site to identify available resources, and they often resolved problems within the system to promote evidence-based treatment. Examples included assisting with the clozapine registration process, creating quick orders to assist with dosing for commonly used medications, and creating treatment letters within the computer system that HCPs could quickly send to the patient. Each academic detailer also worked with local facilities to assess where policies and protocols could support the AD campaign initiatives. Resources at each VA required tailored solutions and collaboration with leadership, and clinicians at each site were key to a successful AD program.
Educational outreach topics covered thus far by the VA AD program include clozapine utilization, metabolic monitoring and use of antipsychotics, PTSD, treatment-resistant depression, alcohol use disorder, and chronic pain management. Each topic focused on specific key messages or key points that are emphasized during the detailing visit with the provider (Table).
Lessons Learned
This pilot program identified several changes that should be considered for future implementation. First, leadership must endorse and support educational sessions with clinicians. Introduction of educational programming begins with creating a collaborative relationship with health care system leadership. Each medical center in the pilot program had an infrastructure of Mental Health, Primary Care, and Pharmacy Service leaders who supported the AD program. In addition, AD Service participation on committees, such as Mental Health Executive Committee, Mental Health Task Force, VISN PBM, and Medication Safety, allows the AD program’s members to network with clinicians and align its key messages with the goals of the facility and leadership. Aligning with existing programs enhances and promotes resources for clinicians and supports leadership and performance goals.
To collaborate, HCPs needs to understand how the AD program benefits them. Before clinicians are approached regarding participation, the AD program should be developed into a branded collaborative program that offers numerous benefits to them, their practice, and their patients. The program must provide a clear and credible answer to the question, “Why should I spend my time meeting with you?”
Second, reaching HCPs for face-to-face encounters over large geographic areas requires an organized network of academic detailers with adequate administrative support. Partnerships with staff already present in the clinic are essential for consistent reinforcement and delivery of the key messages. These partnerships allow station-level staff to continually identify opportunities to act on the key messages. By using local champions, the AD Service can effectively cover a large territory. Providing education to remote facilities can be done by telephone or video teleconferencing.
Third, many HCPs recognize the value this program can add to their practice and have requested follow-up sessions with the academic detailers. To better understand the needs, baseline knowledge, readiness, and receptivity of target audiences, the AD Service should deploy an informal needs assessment to HCPs. The feedback can be used to prepare the appropriate strategies and messaging during AD sessions.
Fourth, the VA chose to use CPSs with experience working as provider extenders for medication management as the primary academic detailers for this pilot. It should be noted that AD services in other national and international systems are successfully performed by other types of HCPs with this same level of qualifications and expertise. Regardless of profession, the academic detailer must have the qualifications and expertise necessary to empower clinical personnel. Without this expertise, provider buy-in is difficult to obtain. As a result, behavior change will be less likely. Pharmacists currently serve as the drug information experts for patients and health care teams. They are valued across professions for their knowledge of medication management, and they have the capacity to recommend nonpharmacologic evidence-based treatments. In addition, using drug information experts as academic detailers allows them to serve as a resource for more complex patient cases.
Finally, providing real-time audit and feedback tools with educational resources gives clinicians tangible actions to improve the care they deliver and proactively target interventions anticipated in the upcoming appointments. It is helpful for HCPs to see the culture of their prescribing compared with prescribers across the network because this can identify areas for improvement and highlight strong practices. Use of audit and feedback tools with a team approach allows for delegation of duties where team members may contribute and collaborate to reach patient goals and improve patient care. Using information technology to deliver this product to health care teams is an important component of the AD program. For successful implementation, resources are needed from both clinicians and the Office of Information and Technology to develop and maintain these powerful tools.
Conclusion
The VA AD Service uses a multifaceted approach to promote the use of evidence-based treatment in veterans with mental illness. Academic detailers, along with key thought leaders, identified opportunities to improve care with solutions for applying evidenced-based medicine. Several items are considered necessary for successful AD program implementation, based on the pilot program. These included endorsement and support by leadership; needs assessment prior to key message development to fully understand the needs, baseline knowledge, readiness, and receptivity of target audiences; highly qualified academic detailers with the training, expertise, and communication skills necessary to empower clinical personnel; and real-time audit and feedback tools with education to give clinicians tangible actions to improve care.
The VA AD Service, including provision of educational services, clinical consultation, health systems barrier resolution, and audit and feedback tools, presents a new opportunity for pharmacists to improve the quality of care of veterans. The impact of the VA AD program on evidence-based care prescribing is being analyzed and will be reported in the future.
1. O’Brien MA, Rogers S, Jamtvedt G, et al. Educational outreach visits: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007;4:CD000409.
2. Meehan TP, Van Hoof TJ, Giannotti TE, et al. A descriptive study of educational outreach to promote use of quality improvement tools in primary care private practice. Am J Med Qual. 2009;24(2):90-98.
3. Simon SR, Rodriguez HP, Majumdar SR, et al. Economic analysis of a randomized trial of academic detailing interventions to improve use of antihypertensive medications. J Clin Hypertens (Greenwich). 2007;9(1):15-20.
4. Solomon DH, Van Houten L, Glynn RJ, et al. Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med. 2001;161(15):1897-1902
5. Patel B, Afghan S. Effects of an educational outreach campaign (IMPACT) on depression management delivered to general practitioners in one primary care trust. Ment Health Fam Med. 2009;6(3):155-162.
1. O’Brien MA, Rogers S, Jamtvedt G, et al. Educational outreach visits: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007;4:CD000409.
2. Meehan TP, Van Hoof TJ, Giannotti TE, et al. A descriptive study of educational outreach to promote use of quality improvement tools in primary care private practice. Am J Med Qual. 2009;24(2):90-98.
3. Simon SR, Rodriguez HP, Majumdar SR, et al. Economic analysis of a randomized trial of academic detailing interventions to improve use of antihypertensive medications. J Clin Hypertens (Greenwich). 2007;9(1):15-20.
4. Solomon DH, Van Houten L, Glynn RJ, et al. Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med. 2001;161(15):1897-1902
5. Patel B, Afghan S. Effects of an educational outreach campaign (IMPACT) on depression management delivered to general practitioners in one primary care trust. Ment Health Fam Med. 2009;6(3):155-162.