User login
New Medicare Rule Will Reimburse Physicians for Advance Care Planning
Hospitalists care for patients with the most serious, chronic, and complex illnesses. As a result, they are often faced with the daunting task of counseling their patients to help them clearly define their end-of-life wishes. The mere subject of death is met with apprehension and avoidance, but its inevitability warrants an early discussion.
End-of-life care, also known as Advance Care Planning (ACP), enables patients to formulate advanced directives: a living will, the designation of a healthcare proxy, Medical Orders for Life-Sustaining Treatment (MOLST), and the preparation for hospice care, among others. Patients should start thinking about their healthcare options and share such important decisions with their physicians and family before the need for hospitalization.
On October 30, 2015, the Centers for Medicare and Medicaid Services (CMS) released the final payment rules for Medicare reimbursement of physicians who consult with their patients on advance care planning. This separate payment system under the 2016 Physician Fee Schedule will impact the almost 55 million Medicare beneficiaries and their healthcare providers.
Effective January 1, 2016, Medicare will pay $86 for 30 minutes of ACP in a physician’s office and will pay $80 for the same service in a hospital (CPT billing code 99497). In both settings, Medicare will pay up to $75 for 30 additional minutes of consultation (add-on CPT billing code 99498). Such counseling can take place during a senior’s annual wellness visit or during a routine office visit and at various stages of health, always “at the discretion of the beneficiary.”
Six years ago, proposed legislation on Medicare reimbursement for ACP under the Accountable Care Act (ACA) sparked political debate over fears that the implementation of so-called “death panels” could influence decisions to avoid medical care. The goal was to reduce healthcare costs, but these controversial provisions were dropped with the passage of the ACA. This time, there was less resistance.
Proponents of this new legislation, such as the American Medical Association and the American Academy of Palliative and Hospice Medicine, say that this rule will encourage physicians to make time for these lengthy discussions and facilitate patient choices while improving quality of care for seniors. Opponents, including the Association of American Physicians and Surgeons, contend that such payments will “create financial incentives to persuade patients to consent to the denial of care.”
Patrick Conway, MD, CMS' chief medical officer, told the New York Times, "We received overwhelmingly positive comments about the importance of these conversations between physicians and patients. We know that many patients and families want to have these discussions."
Future endeavors should focus on efforts to improve the quality of delivering end-of-life care that honors and upholds a patient’s wishes. Strengthening the clinical training of physicians in palliative care, developing quality metrics and standards, and educating the public should remain a top priority.
Will tying a financial incentive to these services have an impact on the cost and quality of care delivered? Hospitalists can begin billing for valuable services they are already providing on a daily basis, and can better coordinate inpatient medical care when more seniors have clear advanced directives. TH
Dr. Zeitoun is a member of Team Hospitalist.
Hospitalists care for patients with the most serious, chronic, and complex illnesses. As a result, they are often faced with the daunting task of counseling their patients to help them clearly define their end-of-life wishes. The mere subject of death is met with apprehension and avoidance, but its inevitability warrants an early discussion.
End-of-life care, also known as Advance Care Planning (ACP), enables patients to formulate advanced directives: a living will, the designation of a healthcare proxy, Medical Orders for Life-Sustaining Treatment (MOLST), and the preparation for hospice care, among others. Patients should start thinking about their healthcare options and share such important decisions with their physicians and family before the need for hospitalization.
On October 30, 2015, the Centers for Medicare and Medicaid Services (CMS) released the final payment rules for Medicare reimbursement of physicians who consult with their patients on advance care planning. This separate payment system under the 2016 Physician Fee Schedule will impact the almost 55 million Medicare beneficiaries and their healthcare providers.
Effective January 1, 2016, Medicare will pay $86 for 30 minutes of ACP in a physician’s office and will pay $80 for the same service in a hospital (CPT billing code 99497). In both settings, Medicare will pay up to $75 for 30 additional minutes of consultation (add-on CPT billing code 99498). Such counseling can take place during a senior’s annual wellness visit or during a routine office visit and at various stages of health, always “at the discretion of the beneficiary.”
Six years ago, proposed legislation on Medicare reimbursement for ACP under the Accountable Care Act (ACA) sparked political debate over fears that the implementation of so-called “death panels” could influence decisions to avoid medical care. The goal was to reduce healthcare costs, but these controversial provisions were dropped with the passage of the ACA. This time, there was less resistance.
Proponents of this new legislation, such as the American Medical Association and the American Academy of Palliative and Hospice Medicine, say that this rule will encourage physicians to make time for these lengthy discussions and facilitate patient choices while improving quality of care for seniors. Opponents, including the Association of American Physicians and Surgeons, contend that such payments will “create financial incentives to persuade patients to consent to the denial of care.”
Patrick Conway, MD, CMS' chief medical officer, told the New York Times, "We received overwhelmingly positive comments about the importance of these conversations between physicians and patients. We know that many patients and families want to have these discussions."
Future endeavors should focus on efforts to improve the quality of delivering end-of-life care that honors and upholds a patient’s wishes. Strengthening the clinical training of physicians in palliative care, developing quality metrics and standards, and educating the public should remain a top priority.
Will tying a financial incentive to these services have an impact on the cost and quality of care delivered? Hospitalists can begin billing for valuable services they are already providing on a daily basis, and can better coordinate inpatient medical care when more seniors have clear advanced directives. TH
Dr. Zeitoun is a member of Team Hospitalist.
Hospitalists care for patients with the most serious, chronic, and complex illnesses. As a result, they are often faced with the daunting task of counseling their patients to help them clearly define their end-of-life wishes. The mere subject of death is met with apprehension and avoidance, but its inevitability warrants an early discussion.
End-of-life care, also known as Advance Care Planning (ACP), enables patients to formulate advanced directives: a living will, the designation of a healthcare proxy, Medical Orders for Life-Sustaining Treatment (MOLST), and the preparation for hospice care, among others. Patients should start thinking about their healthcare options and share such important decisions with their physicians and family before the need for hospitalization.
On October 30, 2015, the Centers for Medicare and Medicaid Services (CMS) released the final payment rules for Medicare reimbursement of physicians who consult with their patients on advance care planning. This separate payment system under the 2016 Physician Fee Schedule will impact the almost 55 million Medicare beneficiaries and their healthcare providers.
Effective January 1, 2016, Medicare will pay $86 for 30 minutes of ACP in a physician’s office and will pay $80 for the same service in a hospital (CPT billing code 99497). In both settings, Medicare will pay up to $75 for 30 additional minutes of consultation (add-on CPT billing code 99498). Such counseling can take place during a senior’s annual wellness visit or during a routine office visit and at various stages of health, always “at the discretion of the beneficiary.”
Six years ago, proposed legislation on Medicare reimbursement for ACP under the Accountable Care Act (ACA) sparked political debate over fears that the implementation of so-called “death panels” could influence decisions to avoid medical care. The goal was to reduce healthcare costs, but these controversial provisions were dropped with the passage of the ACA. This time, there was less resistance.
Proponents of this new legislation, such as the American Medical Association and the American Academy of Palliative and Hospice Medicine, say that this rule will encourage physicians to make time for these lengthy discussions and facilitate patient choices while improving quality of care for seniors. Opponents, including the Association of American Physicians and Surgeons, contend that such payments will “create financial incentives to persuade patients to consent to the denial of care.”
Patrick Conway, MD, CMS' chief medical officer, told the New York Times, "We received overwhelmingly positive comments about the importance of these conversations between physicians and patients. We know that many patients and families want to have these discussions."
Future endeavors should focus on efforts to improve the quality of delivering end-of-life care that honors and upholds a patient’s wishes. Strengthening the clinical training of physicians in palliative care, developing quality metrics and standards, and educating the public should remain a top priority.
Will tying a financial incentive to these services have an impact on the cost and quality of care delivered? Hospitalists can begin billing for valuable services they are already providing on a daily basis, and can better coordinate inpatient medical care when more seniors have clear advanced directives. TH
Dr. Zeitoun is a member of Team Hospitalist.
What the SGR Repeal Means for Hospitalists
The long awaited permanent repeal of the poorly designed Sustainable Growth Rate (SGR) came just in time to avert the 21.2% Medicare physician payment cut that would have taken effect on April 1st, 2015. The SGR formula was first enacted in the Balanced Budget Act of 1997 with the intent to control Medicare spending on physician services. The federal budget sequester in the Budget Control Act of 2011 led to heightened speculation of doom and gloom about the U.S. debt and, ultimately, the necessity of a massive reduction in Medicare payments. Over the past decade, lawmakers have managed to pass 17 various delays and adjustments to keep spending in line with the target SGR. In its place, Congress finally passed H.R. 2, the Medicare Access and CHIP Reauthorization Act (MACRA), which was signed into law by President Obama on April 16, 2015.
What physicians should expect:
(1) The bill includes a 0.5% physician pay increase per year for the next five years beginning July 1, 2015.
(2) It incentivizes physicians to use alternate payment models that focus on care coordination and preventive care.
(3) It consolidates the three existing Medicare quality reporting programs known as the Physician Quality Reporting System (PQRS), Meaningful Use of Electronic Health Records, and the Physician Value-Based Payment Modifier, as well as their associated penalties into a single value-based performance program called the Merit-based Incentive Payment System (MIPS) which starts in 2019.
Is this good for hospitalists? While hospitalists are now protected from the 21% pay cut, we are still faced with increasing burden of legislative mandates on quality metrics. This has created unique challenges for acute inpatient care. The current individual incentive programs will remain in effect until MIPS in 2019, mandating the reporting of PQRS and VBPMs in order to avoid penalties. As such, we will need to continue to focus our efforts on meeting these challenges by aligning our performance measures with that of our institutions. This includes helping to develop alternative payment mechanisms (APMs), such as accountable care organizations (ACOs), patient-centered medical homes, bundled-payment arrangements, and other models. Of note, physicians involved in APMs will not be subject to MIPS assessment and will receive an annual 5% increase from 2019-2024.
The legislation creates other concerns such as the planned enforcement of Medicare's “2-midnight” rule, the requirement of EHR to be interoperable by the end of 2018, and the uncertainty of fairness of CMS in assessing quality and incentive payments. And the question remains, will Congress shift its attention to lowering payments for hospitals and non-physician providers to offset the once expected Medicare cuts? Hospitalists are distinctively qualified to potentially make headway given our already very active involvement in hospital process improvements. It will be in our best interest to stay vocal at the hospital, local, and national level.
The long awaited permanent repeal of the poorly designed Sustainable Growth Rate (SGR) came just in time to avert the 21.2% Medicare physician payment cut that would have taken effect on April 1st, 2015. The SGR formula was first enacted in the Balanced Budget Act of 1997 with the intent to control Medicare spending on physician services. The federal budget sequester in the Budget Control Act of 2011 led to heightened speculation of doom and gloom about the U.S. debt and, ultimately, the necessity of a massive reduction in Medicare payments. Over the past decade, lawmakers have managed to pass 17 various delays and adjustments to keep spending in line with the target SGR. In its place, Congress finally passed H.R. 2, the Medicare Access and CHIP Reauthorization Act (MACRA), which was signed into law by President Obama on April 16, 2015.
What physicians should expect:
(1) The bill includes a 0.5% physician pay increase per year for the next five years beginning July 1, 2015.
(2) It incentivizes physicians to use alternate payment models that focus on care coordination and preventive care.
(3) It consolidates the three existing Medicare quality reporting programs known as the Physician Quality Reporting System (PQRS), Meaningful Use of Electronic Health Records, and the Physician Value-Based Payment Modifier, as well as their associated penalties into a single value-based performance program called the Merit-based Incentive Payment System (MIPS) which starts in 2019.
Is this good for hospitalists? While hospitalists are now protected from the 21% pay cut, we are still faced with increasing burden of legislative mandates on quality metrics. This has created unique challenges for acute inpatient care. The current individual incentive programs will remain in effect until MIPS in 2019, mandating the reporting of PQRS and VBPMs in order to avoid penalties. As such, we will need to continue to focus our efforts on meeting these challenges by aligning our performance measures with that of our institutions. This includes helping to develop alternative payment mechanisms (APMs), such as accountable care organizations (ACOs), patient-centered medical homes, bundled-payment arrangements, and other models. Of note, physicians involved in APMs will not be subject to MIPS assessment and will receive an annual 5% increase from 2019-2024.
The legislation creates other concerns such as the planned enforcement of Medicare's “2-midnight” rule, the requirement of EHR to be interoperable by the end of 2018, and the uncertainty of fairness of CMS in assessing quality and incentive payments. And the question remains, will Congress shift its attention to lowering payments for hospitals and non-physician providers to offset the once expected Medicare cuts? Hospitalists are distinctively qualified to potentially make headway given our already very active involvement in hospital process improvements. It will be in our best interest to stay vocal at the hospital, local, and national level.
The long awaited permanent repeal of the poorly designed Sustainable Growth Rate (SGR) came just in time to avert the 21.2% Medicare physician payment cut that would have taken effect on April 1st, 2015. The SGR formula was first enacted in the Balanced Budget Act of 1997 with the intent to control Medicare spending on physician services. The federal budget sequester in the Budget Control Act of 2011 led to heightened speculation of doom and gloom about the U.S. debt and, ultimately, the necessity of a massive reduction in Medicare payments. Over the past decade, lawmakers have managed to pass 17 various delays and adjustments to keep spending in line with the target SGR. In its place, Congress finally passed H.R. 2, the Medicare Access and CHIP Reauthorization Act (MACRA), which was signed into law by President Obama on April 16, 2015.
What physicians should expect:
(1) The bill includes a 0.5% physician pay increase per year for the next five years beginning July 1, 2015.
(2) It incentivizes physicians to use alternate payment models that focus on care coordination and preventive care.
(3) It consolidates the three existing Medicare quality reporting programs known as the Physician Quality Reporting System (PQRS), Meaningful Use of Electronic Health Records, and the Physician Value-Based Payment Modifier, as well as their associated penalties into a single value-based performance program called the Merit-based Incentive Payment System (MIPS) which starts in 2019.
Is this good for hospitalists? While hospitalists are now protected from the 21% pay cut, we are still faced with increasing burden of legislative mandates on quality metrics. This has created unique challenges for acute inpatient care. The current individual incentive programs will remain in effect until MIPS in 2019, mandating the reporting of PQRS and VBPMs in order to avoid penalties. As such, we will need to continue to focus our efforts on meeting these challenges by aligning our performance measures with that of our institutions. This includes helping to develop alternative payment mechanisms (APMs), such as accountable care organizations (ACOs), patient-centered medical homes, bundled-payment arrangements, and other models. Of note, physicians involved in APMs will not be subject to MIPS assessment and will receive an annual 5% increase from 2019-2024.
The legislation creates other concerns such as the planned enforcement of Medicare's “2-midnight” rule, the requirement of EHR to be interoperable by the end of 2018, and the uncertainty of fairness of CMS in assessing quality and incentive payments. And the question remains, will Congress shift its attention to lowering payments for hospitals and non-physician providers to offset the once expected Medicare cuts? Hospitalists are distinctively qualified to potentially make headway given our already very active involvement in hospital process improvements. It will be in our best interest to stay vocal at the hospital, local, and national level.
Bedside Procedures and Ultrasound: Evidence and Cost of Doing Business
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.

They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
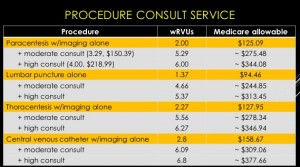
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
- Create a business plan;
- Find institutional financial and political support;
- Start small and selective;
- Plan for standardization and training of colleagues;
- Create a credentialing/privileging process;
- Bill for services and consider billing for full consults; and
- Gather baseline and follow-up data.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
- Create a business plan;
- Find institutional financial and political support;
- Start small and selective;
- Plan for standardization and training of colleagues;
- Create a credentialing/privileging process;
- Bill for services and consider billing for full consults; and
- Gather baseline and follow-up data.
HM15 presenters: Joshua D. Lenchus, DO, FACP, SFHM, and Nilam Soni, MD, FHM
Summary: Drs. Lenchus and Soni focused on the forces that are driving the value and success of established procedure teams in hospital medicine groups (HMGs). These stem from a need to rapidly address the growing shortage of skilled internists who can perform diagnostic and therapeutic procedures, thus leading to a subset of hospitalists who are willing to provide these services, particularly with the assistance of bedside ultrasonography.
They stressed the importance of providing a platform that is preemptive, proprietary, and scalable. With a defined set of value-creating metrics such as faster turn-around times, a reduction in complication rates, and ultimately a reduction in cost, LOS, and utilization, data must be collected to adequately measure the impact of these services on the institution.
They also discussed the key components necessary to create a procedure service, starting with the logistics of adequate training and demonstration of competence, proper staffing, supplies and equipment, ultrasound image archiving, and the use of documentation templates. The process is followed by the development of pre-procedure and post-procedure guidelines, as well as standardized procedural techniques.
The session also reviewed billing practices and professional fees. An analysis was made comparing Medicare reimbursement and work RVUs for each procedure service with and without a full procedure consultation. A complete consultation significantly increases the allowable fee and associated wRVU. The caveat is that billing for consults is limited to services rendered for patients that are not cared for by the same hospitalist group.
Furthermore, sub-specialists historically perform these procedures. The argument can be made that hospitalists will reduce an unnecessary burden on interventional radiologists, thereby enabling them to focus on more acomplex invasive and highly technical procedures.
The key to success is the ability to find a strategic partner in the C-suite who will directly or indirectly provide the financial and political support. Other sources of funding include private foundations, medical schools, the Department of Veteran Affairs, and such patient safety organizations as AHRQ, IOM, and IHI. HMG leaders also should consider scalability across other hospitalist groups.
“If you build it, they will come."
HM takeaways
- Create a business plan;
- Find institutional financial and political support;
- Start small and selective;
- Plan for standardization and training of colleagues;
- Create a credentialing/privileging process;
- Bill for services and consider billing for full consults; and
- Gather baseline and follow-up data.