User login
Preventive Dental Services in Primary Care
Millions of Americans currently lack access to dental care and oral health preventive services because of financial and/or geographic obstacles.1,2 Although community water fluoridation has benefited many Americans during the past 50 years, difficulties in obtaining dental care is a persistent public health challenge.2 Primary care providers (PCPs) can help improve health population-wide by educating patients in good dental hygiene and offering preventive oral health services to patients who would otherwise go without them.
The chief components of preventive dental care include daily brushing with fluoride toothpaste, flossing, routine dental check-ups and professional dental cleanings provided by a licensed dentist and staff, and use of dental sealants and topical fluoride. During the primary care appointment, a routine intraoral exam, including inspection of both hard and soft oral tissues for leukoplakia, gross decay, stained dental structures, and other pathologic changes, is essential. Primary care patients who use any form of tobacco should undergo inspection of the intraoral surfaces of the lips and assessment for adenopathy of the surrounding lymph nodes.
Counseling, including recommending routine preventive dental services (and, for some patients, allaying their fears of seeing a dentist2,3), and positive reinforcement of good oral hygiene practices should be addressed during every primary care encounter. Identifying patients without access to professional dental care is important, as the PCP may be their only source of oral health education, including referrals to local dental clinics.
Application of topical fluoride is an important means of improving dental health, and a cost-effective procedure for both patients and providers4 (see “Fluoride Use,”2,3,5-16). By following published guidelines for use of topical fluoride varnish, PCPs can reduce decay and mineralize enamel, thereby protecting the patient against enamel erosion.6,11,17 This service can and should be offered in primary care offices to patients who lack access to routine dental care and are likely to benefit from this effective weapon against tooth decay.
BEA, AGE 3
Bea lives with her mother and four older brothers and sisters. She is enrolled in Medicaid, but her mother has been unable to locate dental services for any of her children. With every call to a dental office within a 30-minute commute from their home, Bea’s mother has been told, “We don’t accept Medicaid.”
Under her state’s Medicaid plan, Bea has been seen for her primary health care needs since she was a newborn. She was bottle-fed from birth; her mother reports she has stopped taking the bottle to bed within the past few months. While conducting her three-year well-child exam, you note gross decay (see Figure 1).
Dental Services for Children
Nationwide, Medicaid is required to provide coverage for dental services for enrolled children, as well as those who qualify for the CHIP (Children’s Health Insurance Program).20 However, there is no mandate for privately owned dental practices to accept Medicaid payments.
Lack of dental care is the greatest unmet health care need in American children.21 In children without health insurance, access to dental care is most challenging, and those enrolled in Medicaid are the second least likely to receive services. As a result of these and other factors, one-third of US children ages 3 to 5 have dental caries in their primary teeth, and one in every four US children is estimated to have untreated decay2,21-23 (see Figure 2). African-American and Hispanic children experience greater disparities in dental care than do those of other ethnicities.21
Dental decay is the most common chronic illness of childhood (five times as common as asthma), with higher incidence in low-income and minority preschool children.1,24,25 Tooth decay affects growth patterns and nutrition, with associated pain and infection interfering with school attendance.
The small number of dentists who treat children and are willing to accept Medicaid reimbursement is a significant concern. In most dental programs, dedicated pedodontic training is optional. The mismatch of number of qualified dentists to the growing population of such patients is projected to worsen in the coming years.23
Potential solutions to correct this mismatch of dental services accessible to the underserved have included26-31:
- Addition of paraprofessional dental therapists (persons who have received two years’ training in a specific academic program) to the health care team, in public health clinics, schools, and other settings
- Interprofessional dental education (ie, cross-training physicians, NPs, PAs, and RNs in preventive dental services)
- An increasingly diverse array of competent providers who are trained, authorized, and compensated to provide evidence-based care
- Removing licensure restrictions for non–US-trained dentists
- Financial incentives for dentists to practice in dental Health Professional Shortage Areas
- Improved education of parents regarding the benefits of routine dental services.
The Institute of Medicine (IOM)26 has challenged state legislatures to mandate a one-year dental residency to be completed among underserved populations before dental licensure is granted. This challenge reflects the IOM’s acknowledgement that dental services, essential to patients’ well-being, are grossly lacking in the US.
Dental Care Education for Parents
Healthy baby teeth help children eat well and speak clearly. Decayed and abscessed teeth cause the same degree of pain and suffering in young children as they do in adults. Thus, regardless of ethnicity or socioeconomic status, all parents should be routinely encouraged to oversee daily dental hygiene practices for their children; it is important for PCPs to explain to parents their expectations in this regard.
Dental care for children should begin as soon as the first tooth erupts. New teeth should be cleaned daily with a soft cloth and inspected by parents for any discolorations. From age 2 years until children are able to clean all dental surfaces adequately (age 7 or 8), parents should brush their children’s teeth at least once daily with a toothbrush, after applying a thin film of fluoride toothpaste. Children should undergo their first professional dental check-up at about age 1 year.19,26
Parents must be made aware of other factors that can impair their children’s dental health. For example, the foods most likely to promote dental decay contain highly fermentable carbohydrates, are highly processed and sticky, and cause oral pH levels to fall below 5.5 (at which point demineralization may occur).32 Examples include presweetened cereals, dried fruits, cookies, and potato chips. Cheese, peanuts, meat, and eggs are less cariogenic.
Other important teaching points are “don’ts”: putting a baby to bed with a bottle that contains anything but a sugar-free liquid; using spill-proof spouted cups filled with juice or other sugary drinks all day; serving a large proportion of cariogenic foods.
BREANNE, AGE 22
Breanne attends a community college, where she is studying business. She reports to the college health clinic, complaining of an intermittent sharp pain in one of her lower molars over the past four days, occurring when she eats or drinks anything cold.
Before she turned 21, Breanne received routine dental services under her parents’ insurance. Now a full-time student no longer covered by her parents’ plan, she has no income with which to purchase dental coverage. Years ago, Breanne received dental sealants on all of her molars in a school-based program, and she routinely brushes daily (see Figure 3). She says she “usually remembers to floss.”
Dental Concerns in Young Adults
Up to one-third of Americans, including college-age students, lack access to oral health services.33 Use of annual dental services, including school-based care, significantly reduces young adults’ risk for tooth loss.34 From early adulthood on, poor dental health is associated with cardiovascular and respiratory disease, cerebral ischemia, diabetes, difficulty with chewing and oral pain, and poor self-image.24
PCPs should emphasize the importance of preventive services as they examine the oral structure during routine health care encounters. Adding the question, “When did you last have a dental exam?” can launch an effective discussion about the importance of good dental health.
Tooth surfaces with pits and fissures are the most vulnerable to decay. Dental sealants can protect these vulnerable areas, reducing decay by 60% to 82%.2,32,35 Sealants are the most effective preventive measure for reducing cavity formation; they are not harmful to fillings and can actually reduce the progression of decay when applied over small existing carious lesions.35 Currently, however, only 30% and 38% of children and adolescents, respectively, have undergone application of sealants.36 Thus, it is vital for PCPs to recommend dental sealants to all their patients.35,37,38
Young adults should also be questioned about their exercise patterns. While daily exercise is of benefit to good health, young adults who engage in too-frequent, overly vigorous exercise have been found vulnerable to dental erosion.39 This irreversible condition can result from the rapid breathing, sweat-induced dehydration, and decreased salivary flow associated with strenuous exercise. Reduced salivary flow disrupts the protection against erosive acids afforded by bathing of teeth with saliva, leading to a fivefold greater risk for developing erosions. Patients should be encouraged to hydrate before exercise to reduce these risks.39
Dental Health Notes for Young Women
For female patients of childbearing age like Breanne, dental health is important not only for the patient, but for her future children as well. Poor maternal dental health has been associated with preterm births and low birth weights.40-43 Women who have health insurance, who are in good general health, and who regularly visit a primary care medical provider are also the most likely to see a dental care provider during pregnancy.40
Pregnancy is associated with a risk for poor dental care in any population.42,44 During pregnancy, Medicaid-enrolled women are 30% less likely to see a dentist than women with private health insurance, and women with no health insurance are 70% less likely to see a dentist.44 Among pregnant women who experience a dental problem, less than half will schedule a dental appointment. Postponing dental care till after delivery incurs additional risk, as the new mother will be busy with her child and may have lost her health care coverage in the interim.
Dental concerns commonly encountered during pregnancy are listed in Table 3.41,42 There is also evidence that maternal transmission of mutans streptococci can lead to early childhood caries,42,45 further highlighting the importance of dental care during pregnancy (eg, use of chlorhexidine rinses in pregnant women with dental caries42). The association between periodontal disease and preterm delivery and lower birth weights40-43 makes it critical to reduce maternal periodontal inflammation through timely dental referrals.
SAUL, AGE 42
Saul, a lifelong resident of Mississippi, has worked in construction since age 18. He has never had health or dental insurance and thus he rarely seeks preventive services. As he recalls, he has had “two fillings in my jaw teeth since I was a kid,” but otherwise has had no dental care. He brushes daily to avoid having to see a dentist. He is presenting today as a new patient only because he has a rash.
Benefits of Fluoride Use During Middle Age
Dental care needs peak between ages 55 and 64, with the majority of care prompted by dental decay46 (see Figure 4). A discussion about dental health should be raised when the PCP completes the review of systems or while discussing other preventive services. The option of fluoride varnish should not be overlooked in a patient of any age, particularly one with a recognizable deficiency of preventive dental services. Explaining the benefits of topical fluoride varnish (see “Fluoride Use”) and offering an opportunity to receive it in the office may persuade a patient like Saul to take advantage of this proven anticarious procedure.

Patients who undergo this safe procedure should be reminded to continue brushing daily with fluoridated toothpaste and drinking fluoridated water (if it is available).50
GILL, AGE 77
Gill grew up in Grant County, New Mexico, in an area not far from Silver City; there, fluoride supplementation in the local water did not begin until Gill was about 40. His family never stressed oral hygiene, and his remaining teeth show gross plaque and decay.
He sees you routinely for his chronic illnesses, and today he has presented for his annual physical. Gill has Medicare without supplemental insurance.
Dental Care in the Medicare Years
Medicare does not cover preventive dental services unless hospitalization is required; in that case, it is covered under Medicare Part A.51 Publicly supported dental services are primarily offered for children, leaving Medicare recipients responsible for the costs of dental care. As a last resort, some patients will seek dental care at a hospital emergency department (ED). Most often prompted to visit the ED for relief of pain triggered by dental fractures or abscesses, patients usually leave with pain medications and antibiotics only; their general dental health needs remain unmet.52
The most common dental concerns among elderly patients include edentulism (toothlessness, which is reported in one in four Medicare beneficiaries1), xerostomia (dry mouth), periodontal disease, ill-fitting or worn prosthetics, and progressive decay affecting fractured teeth1 (see Figure 5). As many elderly patients endure a combination of these uncomfortable, possibly painful, conditions, it is important for the PCP to inquire about them during the physical exam and the review of symptoms. At each step, a window of opportunity opens to make appropriate recommendations.

Significant Comorbidities
It is important for PCPs to recognize the association between certain diseases and poor oral health. With the progression of age, the risk increases for type 2 diabetes. Among older diabetic patients with periodontitis (and the systemic inflammation associated with it), the difficulty of maintaining glycemic control increases as well.53 Conversely, diabetic patients who are immunocompromised are at elevated risk for periodontitis. In more than 20 years of formal data collection, periodontists have identified and confirmed an anecdotal relationship between diabetes and severe periodontal disease.26
Elderly patients with poor dental health are also at increased risk for chronic kidney disease. Periodontal disease alone increases the risk for nephropathy 1.5-fold to twofold.54Finally, patients’ risk for oral cancer increases with age. Known risk factors for oral cancers include smoking, use of chewing tobacco, alcohol consumption, chronic friction, and exposure to ultraviolet radiation.55 Survival rates for oral cancers are poor, reemphasizing the need for a thorough oral exam during primary care visits.
Other Challenges for Older Patients
Members of ethnic minority groups and lower-income populations, men, patients with cognitive impairment, and persons who never completed high school are the most likely to avoid, discontinue, or lack access to dental services.56 Loss of dental coverage on retirement is associated with a significant decline in elderly patients’ use of dental services. Though now living on a fraction of their preretirement income, millions of retirees are required to pay out-of-pocket for dental services.57
Topical fluoride varnish alone cannot alleviate this multimillion dollar concern, but using it to reinforce retirees’ remaining enamel and prevent caries can help reduce their dental care expenditures. However, until federal and state policymakers act to cover preventive services,2,58 PCPs have little to offer elderly patients beyond oral hygiene education and in-office application of topical fluoride.
Strategies to Reinforce Dental Health
In practices where electronic medical records are in use, a recommendation for dental services should be printed as a patient reminder. Printed recommendations and referrals from PCPs do improve patient compliance.59 In addition to the printed office summary, older patients can be handed a summary of oral health suggestions from the National Institute on Aging, NIH59 (www.nia.nih.gov/health/publication/taking-care-your-teeth-and-mouth).
CONCLUSION
For most Americans with dental health insurance, access to services, and a willingness to practice good oral hygiene, dental care quality is above average. However, health care disparities and a lack of dental coverage prevent millions of Americans from routinely seeking dental services—making it essential for PCPs to promote oral hygiene and offer professional dental referrals with patients of all ages. Topical fluoride varnish, which can reduce the risk for decay as well as progression of existing decay, is an important preventive service that is within the scope of primary care practice.
1. Kaiser Commission. Medicaid and the uninsured: oral health in the US: key facts (2012). www.kff.org/uninsured/upload/8324.pdf. Accessed February 11, 2013.
2. Healthy People 2020. Oral health. www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=32. Accessed February 11, 2013.
3. CDC. Community water fluoridation: other fluoride products (2011). www.cdc.gov/fluoridation/other.htm. Accessed February 11, 2013.
4. American Academy of Pediatrics. Advocacy: Medicaid, fluoride varnish (2011). www.paaap.org/adv_medicaid_pg2.php. Accessed February 11, 2013.
5. National Institute of Dental and Craniofacial Research, NIH. The story of fluoridation (2011). www.nidcr.nih.gov/oralhealth/topics/fluoride/thestoryoffluoridation.htm. Accessed February 11, 2013.
6. Yu H, Attin T, Wiegand A, Buchalla W. Effects of various fluoride solutions on enamel erosion in vitro. Caries Res. 2010;44(4):390-401.
7. Bertness J, Holt K, eds; National Maternal & Child Oral Health Resource Center. Fluoride varnish: a resource guide (2010). www.mchoralhealth.org/PDFs/ResGuideFlVarnish.pdf. Accessed February 11, 2013.
8. Lee YE, Baek HJ, Choi YH, et al. Comparison of remineralization effect of three topical fluoride regimens on enamel initial carious lesions. J Dent. 2010;38(2):166-171.
9. New Zealand Guidelines Group. Guidelines for the use of fluorides (2009). Wellington, New Zealand: New Zealand Ministry of Health. www.guideline.gov/content.aspx?id=25685&search=fluoride+varnish. Accessed February 11, 2013.
10. O’Keefe E. Fluoride varnish may be effective in preschoolers. Evid Based Dent. 2011;12(2):41-42.
11. American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Am Dent Assoc. 2006;137(8):1151-1159.
12. MassHealth. Health and Human Services. Fluoride varnish training for health-care professionals (2012). www.mass.gov/eohhs/gov/newsroom/masshealth/providers/fluoride-varnish-training-for-health-care.html. Accessed February 11, 2013.
13. Collins FM; Academy of Dental Therapeutics and Stomatology. The development and utilization of fluoride varnish (2011). www.ineedce.com/courses/2093/PDF/1106cei_varnish_web4.pdf. Accessed February 11, 2013.
14. New York State Department of Health. Improving the oral health of young children: fluoride varnish training materials and oral health information for child health care providers (2010). www.health.ny.gov/prevention/dental/child_oral_health_fluoride_varnish_for_hcp.htm. Accessed February 11, 2013.
15. Missouri Department of Health and Senior Services. Fluoride varnish application training for Missouri Oral Health Preventive Services Program. http://mohealthysmiles.typepad.com/Fluoride_Varnish_App_Training.pdf. Accessed February 15, 2013.
16. American Academy of Pediatrics. Oral health coding fact sheet for primary care physicians (2010). www2.aap.org/oralhealth/docs/OHCoding.pdf. Accessed February 11, 2013.
17. Chersoni S, Bertacci A, Pashley D, et al. In vivo effects of fluoride on enamel permeability. Clin Oral Investig. 2011;15(4):443-449.
18. National Interprofessional Initiative on Oral Health. Smiles for life curriculum (2011). www.niioh.org/smiles-life-curriculum. Accessed February 11, 2013.
19. Douglass AB, Gonsalves W, Maier R, et al. Smiles for Life: a national oral health curriculum for family medicine. Fam Med. 2007;39(2):88-90.
20. Medicaid.gov. Children’s Health Insurance Program (CHIP). www.medicaid .gov/Medicaid-CHIP-Program-Information/By-Topics/Childrens-Health-Insurance-Program-CHIP/Childrens-Health-Insurance-Program-CHIP.html. Accessed February 11, 2013.
21. Pourat N, Finocchio L. Racial and ethnic disparities in dental care for publicly insured children. Health Aff (Millwood). 2010;29(7):1356-1363.
22. Edelstein BL, Chinn CH. Update on disparities in oral health and access to dental care for America’s children. Acad Pediatr. 2009;9(6):415-419.
23. Seale NS, McWhorter AG, Moulradian WE. Dental education’s role in improving children’s oral health and access to care. Acad Pediatr. 2009;9(6):440-445.
24. National Institute of Dental and Craniofacial Research, NIH. Oral Health in America: A Report of the Surgeon General (Executive Summary; 2011). www.nidcr.nih.gov/datastatistics/surgeongeneral/report/executivesummary.htm. Accessed February 5, 2013.
25. Grembowski D, Spiekerman C, Milgrom P. Social gradients in dental health among low-income mothers and their young children. J Health Care Poor Underserved. 2012;23(2):570-588.
26. Institute of Medicine of the National Academies. Improving access to oral health care for vulnerable and underserved populations (2011). www.iom.edu/~/media/Files/Report Files/2011/Improving-Access-to-Oral-Health-Care-for-Vulnerable-and-Underserved-Populations/oralhealthaccess2011reportbrief.pdf. Accessed February 11, 2013.
27. Bertolami CN. Access to dental care: is there a problem? Am J Public Health. 2011;101(10):1817.
28. Bazargan N, Chi DL, Milgrom P. Exploring the potential for foreign-trained dentists to address workforce shortages and improve access to dental care for vulnerable populations in the United States: a case study from Washington State. BMC Health Serv Res. 2010;10:336-343.
29. Nash DA. Adding dental therapists to the health care team to improve access to oral health care for children. Acad Pediatr. 2009;9(6):446-451.
30. Liao CC, Ganz ML, Jiang H, Chelmow T. The impact of the public insurance expansions on children’s use of preventive dental care. Matern Child Health J. 2010;14(1):58-66.
31. Duley SI, Fitzpatrick PG, Zornosa X, Barnes WG. A center for oral health promotion: establishing an inter-professional paradigm for dental hygiene, health care management and nursing education. J Dent Hyg. 2012;86(2):63-70.
32. Ritter AV, Eidson RS, Donovan TE. Dental caries: etiology, clinical characteristics, risk assessment, and management. In: Heymann HO, Swift EJ Jr, Ritter AV, eds. Sturdevant’s Art and Science of Operative Dentistry. 6th ed. St. Louis: Elsevier-Mosby; 2012:41-89.
33. Shaefer HL, Miller M. Improving access to oral health care services among underserved populations in the US: is there a role for mid-level dental providers? J Health Care Poor Underserved. 2011;22(3):740-744.
34. Li KY, Wong MC, Lam KF, Schwarz E. Age, period, and cohort analysis of regular dental care behavior and edentulism: a marginal approach. BMC Oral Health. 2011;11:9.
35. Beauchamp J, Caufield PW, Crall JJ, et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008;139(3):257-268.
36. National Institute of Dental and Craniofacial Research, NIH. Dental sealants in children (age 8 to 11)(2011). www.nidcr.nih.gov/DataStatistics/FindDataByTopic/DentalSealants/Children. Accessed February 11, 2013.
37. Gore DR. The use of dental sealants in adults: a long-neglected preventive measure. Int J Dent Hyg. 2010;8(3):198-203.
38. Devlin D, Henshaw M. Improving access to preventive dental services through a school-based dental sealant program. J Dent Hyg. 2011;85(3):211-219.
39. Mulic A, Tveit AB, Songe D, et al. Dental erosive wear and salivary flow rate in physically active young adults. BMC Oral Health. 2012;12:8.
40. Kaylor MB, Polivka BJ, Chaudry R, et al. Dental services utilization by women of child-bearing age by socioeconomic status. J Community Health. 2010;35(2):190-197.
41. Michalowicz BS, Hodges JS, DiAngelis AJ, et al; OPT Study. Treatment of periodontal disease and the risk of preterm birth. N Engl J Med. 2006;355(18):1885-1894.
42. Silk H, Douglass AB, Douglass JM, Silk L. Oral health during pregnancy. Am Fam Physician. 2008;77(8):1139-1144.
43. Clothier B, Stringer M, Jeffcoat MK. Periodontal disease and pregnancy outcomes: exposure, risk and intervention. Best Pract Res Clin Obstet Gynaecol. 2007;21(3):451-466.
44. Ressler-Maerlender J, Krishna R, Robison V. Oral health during pregnancy: current research. J Womens Health (Larchmt). 2005;14(10):880-882.
45. Berkowitz RJ. Acquisition and transmission of mutans streptococci. J Calif Dent Assoc. 2003;31(2):135-138.
46. Vollmer WM, Papas AS, Bader JD, et al; PACS Collaborative Research Group. Design of the Prevention of Adult Caries Study (PACS): a randomized clinical trial assessing the effect of chlorhexidine dental coating for the protection of adult caries. BMC Oral Health. 2010;10:23.
47. Dhull KS, Nandlal B. Effect of low-concentration daily fluoride application on fluoride release of giomer and compomer: an in vitro study. J Indian Soc Pedod Prev Dent. 2011;29(1):39-45.
48. Naumova EA, Kuehnl P, Hertenstein P, et al. Fluoride bioavailability in saliva and plaque. BMC Oral Health. 2012;12:3.
49. Duckworth RM, Maguire A, Omid N, et al. Effect of rinsing with mouthwash after brushing with fluoridated toothpaste on salivary fluoride concentration. Caries Res. 2009;43(5):391-396.
50. Opydo-Szymaczek J, Opydo J. Salivary fluoride concentrations and fluoride ingestion following application of preparations containing high concentration of fluoride. Biol Trace Elem Res. 2010;137(2):159-167.
51. Medicare.gov. Your Medicare coverage: dental services. www.medicare.gov/coverage/dental-services.html. Accessed February 11, 2013.
52. Quiñonez C, Ieraci L, Guttmann A. Potentially preventable hospital use for dental conditions: implications for expanding dental coverage for low income populations. J Health Care Poor Underserved. 2011;22(3):1048-1058.
53. Deshpande K, Jain A, Sharma RK, et al. Diabetes and periodontitis. J Indian Soc Periodontol. 2010;14(4):207-212.
54. Grubbs V, Plantinga LC, Tuot DS, Powe NR. Chronic kidney disease and use of dental services in a United States public healthcare system: a retrospective cohort study. BMC Nephrol. 2012;13:16.
55. Nair DR, Pruthy R, Pawar U, Chaturvedi P. Oral cancer: premalignant conditions and screening—an update. J Cancer Res Ther. 2012;8 suppl 1:S57-S66.
56. Wu B, Plassman BL, Lian J, Wei L. Cognitive function and dental care utilization among community-dwelling older adults. Am J Public Health. 2007;97(12):2216-2221.
57. Manski RJ, Moeller JF, St Clair PA, et al. The influence of changes in dental care coverage on dental care utilization among retirees and near-retirees in the United States, 2004-2006. Am J Public Health. 2011;101(10):1882-1891.
58. Moeller JF, Chen H, Manski RJ. Investing in preventive dental care for the Medicare population: a preliminary analysis. Am J Public Health. 2010;100(11):2262-2269.
59. National Institute on Aging, NIH. AgePage: Taking care of your teeth and mouth (2011). www.nia.nih.gov/health/publication/taking-care-your-teeth-and-mouth. Accessed February 6, 2013.
Millions of Americans currently lack access to dental care and oral health preventive services because of financial and/or geographic obstacles.1,2 Although community water fluoridation has benefited many Americans during the past 50 years, difficulties in obtaining dental care is a persistent public health challenge.2 Primary care providers (PCPs) can help improve health population-wide by educating patients in good dental hygiene and offering preventive oral health services to patients who would otherwise go without them.
The chief components of preventive dental care include daily brushing with fluoride toothpaste, flossing, routine dental check-ups and professional dental cleanings provided by a licensed dentist and staff, and use of dental sealants and topical fluoride. During the primary care appointment, a routine intraoral exam, including inspection of both hard and soft oral tissues for leukoplakia, gross decay, stained dental structures, and other pathologic changes, is essential. Primary care patients who use any form of tobacco should undergo inspection of the intraoral surfaces of the lips and assessment for adenopathy of the surrounding lymph nodes.
Counseling, including recommending routine preventive dental services (and, for some patients, allaying their fears of seeing a dentist2,3), and positive reinforcement of good oral hygiene practices should be addressed during every primary care encounter. Identifying patients without access to professional dental care is important, as the PCP may be their only source of oral health education, including referrals to local dental clinics.
Application of topical fluoride is an important means of improving dental health, and a cost-effective procedure for both patients and providers4 (see “Fluoride Use,”2,3,5-16). By following published guidelines for use of topical fluoride varnish, PCPs can reduce decay and mineralize enamel, thereby protecting the patient against enamel erosion.6,11,17 This service can and should be offered in primary care offices to patients who lack access to routine dental care and are likely to benefit from this effective weapon against tooth decay.
BEA, AGE 3
Bea lives with her mother and four older brothers and sisters. She is enrolled in Medicaid, but her mother has been unable to locate dental services for any of her children. With every call to a dental office within a 30-minute commute from their home, Bea’s mother has been told, “We don’t accept Medicaid.”
Under her state’s Medicaid plan, Bea has been seen for her primary health care needs since she was a newborn. She was bottle-fed from birth; her mother reports she has stopped taking the bottle to bed within the past few months. While conducting her three-year well-child exam, you note gross decay (see Figure 1).
Dental Services for Children
Nationwide, Medicaid is required to provide coverage for dental services for enrolled children, as well as those who qualify for the CHIP (Children’s Health Insurance Program).20 However, there is no mandate for privately owned dental practices to accept Medicaid payments.
Lack of dental care is the greatest unmet health care need in American children.21 In children without health insurance, access to dental care is most challenging, and those enrolled in Medicaid are the second least likely to receive services. As a result of these and other factors, one-third of US children ages 3 to 5 have dental caries in their primary teeth, and one in every four US children is estimated to have untreated decay2,21-23 (see Figure 2). African-American and Hispanic children experience greater disparities in dental care than do those of other ethnicities.21
Dental decay is the most common chronic illness of childhood (five times as common as asthma), with higher incidence in low-income and minority preschool children.1,24,25 Tooth decay affects growth patterns and nutrition, with associated pain and infection interfering with school attendance.
The small number of dentists who treat children and are willing to accept Medicaid reimbursement is a significant concern. In most dental programs, dedicated pedodontic training is optional. The mismatch of number of qualified dentists to the growing population of such patients is projected to worsen in the coming years.23
Potential solutions to correct this mismatch of dental services accessible to the underserved have included26-31:
- Addition of paraprofessional dental therapists (persons who have received two years’ training in a specific academic program) to the health care team, in public health clinics, schools, and other settings
- Interprofessional dental education (ie, cross-training physicians, NPs, PAs, and RNs in preventive dental services)
- An increasingly diverse array of competent providers who are trained, authorized, and compensated to provide evidence-based care
- Removing licensure restrictions for non–US-trained dentists
- Financial incentives for dentists to practice in dental Health Professional Shortage Areas
- Improved education of parents regarding the benefits of routine dental services.
The Institute of Medicine (IOM)26 has challenged state legislatures to mandate a one-year dental residency to be completed among underserved populations before dental licensure is granted. This challenge reflects the IOM’s acknowledgement that dental services, essential to patients’ well-being, are grossly lacking in the US.
Dental Care Education for Parents
Healthy baby teeth help children eat well and speak clearly. Decayed and abscessed teeth cause the same degree of pain and suffering in young children as they do in adults. Thus, regardless of ethnicity or socioeconomic status, all parents should be routinely encouraged to oversee daily dental hygiene practices for their children; it is important for PCPs to explain to parents their expectations in this regard.
Dental care for children should begin as soon as the first tooth erupts. New teeth should be cleaned daily with a soft cloth and inspected by parents for any discolorations. From age 2 years until children are able to clean all dental surfaces adequately (age 7 or 8), parents should brush their children’s teeth at least once daily with a toothbrush, after applying a thin film of fluoride toothpaste. Children should undergo their first professional dental check-up at about age 1 year.19,26
Parents must be made aware of other factors that can impair their children’s dental health. For example, the foods most likely to promote dental decay contain highly fermentable carbohydrates, are highly processed and sticky, and cause oral pH levels to fall below 5.5 (at which point demineralization may occur).32 Examples include presweetened cereals, dried fruits, cookies, and potato chips. Cheese, peanuts, meat, and eggs are less cariogenic.
Other important teaching points are “don’ts”: putting a baby to bed with a bottle that contains anything but a sugar-free liquid; using spill-proof spouted cups filled with juice or other sugary drinks all day; serving a large proportion of cariogenic foods.
BREANNE, AGE 22
Breanne attends a community college, where she is studying business. She reports to the college health clinic, complaining of an intermittent sharp pain in one of her lower molars over the past four days, occurring when she eats or drinks anything cold.
Before she turned 21, Breanne received routine dental services under her parents’ insurance. Now a full-time student no longer covered by her parents’ plan, she has no income with which to purchase dental coverage. Years ago, Breanne received dental sealants on all of her molars in a school-based program, and she routinely brushes daily (see Figure 3). She says she “usually remembers to floss.”
Dental Concerns in Young Adults
Up to one-third of Americans, including college-age students, lack access to oral health services.33 Use of annual dental services, including school-based care, significantly reduces young adults’ risk for tooth loss.34 From early adulthood on, poor dental health is associated with cardiovascular and respiratory disease, cerebral ischemia, diabetes, difficulty with chewing and oral pain, and poor self-image.24
PCPs should emphasize the importance of preventive services as they examine the oral structure during routine health care encounters. Adding the question, “When did you last have a dental exam?” can launch an effective discussion about the importance of good dental health.
Tooth surfaces with pits and fissures are the most vulnerable to decay. Dental sealants can protect these vulnerable areas, reducing decay by 60% to 82%.2,32,35 Sealants are the most effective preventive measure for reducing cavity formation; they are not harmful to fillings and can actually reduce the progression of decay when applied over small existing carious lesions.35 Currently, however, only 30% and 38% of children and adolescents, respectively, have undergone application of sealants.36 Thus, it is vital for PCPs to recommend dental sealants to all their patients.35,37,38
Young adults should also be questioned about their exercise patterns. While daily exercise is of benefit to good health, young adults who engage in too-frequent, overly vigorous exercise have been found vulnerable to dental erosion.39 This irreversible condition can result from the rapid breathing, sweat-induced dehydration, and decreased salivary flow associated with strenuous exercise. Reduced salivary flow disrupts the protection against erosive acids afforded by bathing of teeth with saliva, leading to a fivefold greater risk for developing erosions. Patients should be encouraged to hydrate before exercise to reduce these risks.39
Dental Health Notes for Young Women
For female patients of childbearing age like Breanne, dental health is important not only for the patient, but for her future children as well. Poor maternal dental health has been associated with preterm births and low birth weights.40-43 Women who have health insurance, who are in good general health, and who regularly visit a primary care medical provider are also the most likely to see a dental care provider during pregnancy.40
Pregnancy is associated with a risk for poor dental care in any population.42,44 During pregnancy, Medicaid-enrolled women are 30% less likely to see a dentist than women with private health insurance, and women with no health insurance are 70% less likely to see a dentist.44 Among pregnant women who experience a dental problem, less than half will schedule a dental appointment. Postponing dental care till after delivery incurs additional risk, as the new mother will be busy with her child and may have lost her health care coverage in the interim.
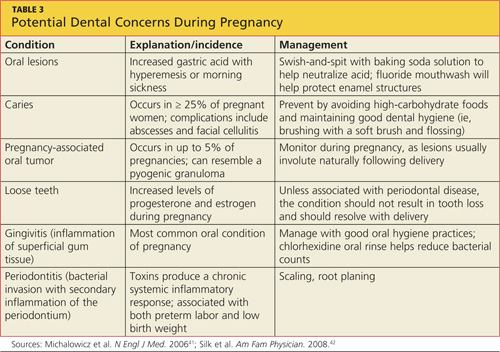
Dental concerns commonly encountered during pregnancy are listed in Table 3.41,42 There is also evidence that maternal transmission of mutans streptococci can lead to early childhood caries,42,45 further highlighting the importance of dental care during pregnancy (eg, use of chlorhexidine rinses in pregnant women with dental caries42). The association between periodontal disease and preterm delivery and lower birth weights40-43 makes it critical to reduce maternal periodontal inflammation through timely dental referrals.
SAUL, AGE 42
Saul, a lifelong resident of Mississippi, has worked in construction since age 18. He has never had health or dental insurance and thus he rarely seeks preventive services. As he recalls, he has had “two fillings in my jaw teeth since I was a kid,” but otherwise has had no dental care. He brushes daily to avoid having to see a dentist. He is presenting today as a new patient only because he has a rash.
Benefits of Fluoride Use During Middle Age
Dental care needs peak between ages 55 and 64, with the majority of care prompted by dental decay46 (see Figure 4). A discussion about dental health should be raised when the PCP completes the review of systems or while discussing other preventive services. The option of fluoride varnish should not be overlooked in a patient of any age, particularly one with a recognizable deficiency of preventive dental services. Explaining the benefits of topical fluoride varnish (see “Fluoride Use”) and offering an opportunity to receive it in the office may persuade a patient like Saul to take advantage of this proven anticarious procedure.
Patients who undergo this safe procedure should be reminded to continue brushing daily with fluoridated toothpaste and drinking fluoridated water (if it is available).50
GILL, AGE 77
Gill grew up in Grant County, New Mexico, in an area not far from Silver City; there, fluoride supplementation in the local water did not begin until Gill was about 40. His family never stressed oral hygiene, and his remaining teeth show gross plaque and decay.
He sees you routinely for his chronic illnesses, and today he has presented for his annual physical. Gill has Medicare without supplemental insurance.
Dental Care in the Medicare Years
Medicare does not cover preventive dental services unless hospitalization is required; in that case, it is covered under Medicare Part A.51 Publicly supported dental services are primarily offered for children, leaving Medicare recipients responsible for the costs of dental care. As a last resort, some patients will seek dental care at a hospital emergency department (ED). Most often prompted to visit the ED for relief of pain triggered by dental fractures or abscesses, patients usually leave with pain medications and antibiotics only; their general dental health needs remain unmet.52
The most common dental concerns among elderly patients include edentulism (toothlessness, which is reported in one in four Medicare beneficiaries1), xerostomia (dry mouth), periodontal disease, ill-fitting or worn prosthetics, and progressive decay affecting fractured teeth1 (see Figure 5). As many elderly patients endure a combination of these uncomfortable, possibly painful, conditions, it is important for the PCP to inquire about them during the physical exam and the review of symptoms. At each step, a window of opportunity opens to make appropriate recommendations.
Significant Comorbidities
It is important for PCPs to recognize the association between certain diseases and poor oral health. With the progression of age, the risk increases for type 2 diabetes. Among older diabetic patients with periodontitis (and the systemic inflammation associated with it), the difficulty of maintaining glycemic control increases as well.53 Conversely, diabetic patients who are immunocompromised are at elevated risk for periodontitis. In more than 20 years of formal data collection, periodontists have identified and confirmed an anecdotal relationship between diabetes and severe periodontal disease.26
Elderly patients with poor dental health are also at increased risk for chronic kidney disease. Periodontal disease alone increases the risk for nephropathy 1.5-fold to twofold.54Finally, patients’ risk for oral cancer increases with age. Known risk factors for oral cancers include smoking, use of chewing tobacco, alcohol consumption, chronic friction, and exposure to ultraviolet radiation.55 Survival rates for oral cancers are poor, reemphasizing the need for a thorough oral exam during primary care visits.
Other Challenges for Older Patients
Members of ethnic minority groups and lower-income populations, men, patients with cognitive impairment, and persons who never completed high school are the most likely to avoid, discontinue, or lack access to dental services.56 Loss of dental coverage on retirement is associated with a significant decline in elderly patients’ use of dental services. Though now living on a fraction of their preretirement income, millions of retirees are required to pay out-of-pocket for dental services.57
Topical fluoride varnish alone cannot alleviate this multimillion dollar concern, but using it to reinforce retirees’ remaining enamel and prevent caries can help reduce their dental care expenditures. However, until federal and state policymakers act to cover preventive services,2,58 PCPs have little to offer elderly patients beyond oral hygiene education and in-office application of topical fluoride.
Strategies to Reinforce Dental Health
In practices where electronic medical records are in use, a recommendation for dental services should be printed as a patient reminder. Printed recommendations and referrals from PCPs do improve patient compliance.59 In addition to the printed office summary, older patients can be handed a summary of oral health suggestions from the National Institute on Aging, NIH59 (www.nia.nih.gov/health/publication/taking-care-your-teeth-and-mouth).
CONCLUSION
For most Americans with dental health insurance, access to services, and a willingness to practice good oral hygiene, dental care quality is above average. However, health care disparities and a lack of dental coverage prevent millions of Americans from routinely seeking dental services—making it essential for PCPs to promote oral hygiene and offer professional dental referrals with patients of all ages. Topical fluoride varnish, which can reduce the risk for decay as well as progression of existing decay, is an important preventive service that is within the scope of primary care practice.
Millions of Americans currently lack access to dental care and oral health preventive services because of financial and/or geographic obstacles.1,2 Although community water fluoridation has benefited many Americans during the past 50 years, difficulties in obtaining dental care is a persistent public health challenge.2 Primary care providers (PCPs) can help improve health population-wide by educating patients in good dental hygiene and offering preventive oral health services to patients who would otherwise go without them.
The chief components of preventive dental care include daily brushing with fluoride toothpaste, flossing, routine dental check-ups and professional dental cleanings provided by a licensed dentist and staff, and use of dental sealants and topical fluoride. During the primary care appointment, a routine intraoral exam, including inspection of both hard and soft oral tissues for leukoplakia, gross decay, stained dental structures, and other pathologic changes, is essential. Primary care patients who use any form of tobacco should undergo inspection of the intraoral surfaces of the lips and assessment for adenopathy of the surrounding lymph nodes.
Counseling, including recommending routine preventive dental services (and, for some patients, allaying their fears of seeing a dentist2,3), and positive reinforcement of good oral hygiene practices should be addressed during every primary care encounter. Identifying patients without access to professional dental care is important, as the PCP may be their only source of oral health education, including referrals to local dental clinics.
Application of topical fluoride is an important means of improving dental health, and a cost-effective procedure for both patients and providers4 (see “Fluoride Use,”2,3,5-16). By following published guidelines for use of topical fluoride varnish, PCPs can reduce decay and mineralize enamel, thereby protecting the patient against enamel erosion.6,11,17 This service can and should be offered in primary care offices to patients who lack access to routine dental care and are likely to benefit from this effective weapon against tooth decay.
BEA, AGE 3
Bea lives with her mother and four older brothers and sisters. She is enrolled in Medicaid, but her mother has been unable to locate dental services for any of her children. With every call to a dental office within a 30-minute commute from their home, Bea’s mother has been told, “We don’t accept Medicaid.”
Under her state’s Medicaid plan, Bea has been seen for her primary health care needs since she was a newborn. She was bottle-fed from birth; her mother reports she has stopped taking the bottle to bed within the past few months. While conducting her three-year well-child exam, you note gross decay (see Figure 1).
Dental Services for Children
Nationwide, Medicaid is required to provide coverage for dental services for enrolled children, as well as those who qualify for the CHIP (Children’s Health Insurance Program).20 However, there is no mandate for privately owned dental practices to accept Medicaid payments.
Lack of dental care is the greatest unmet health care need in American children.21 In children without health insurance, access to dental care is most challenging, and those enrolled in Medicaid are the second least likely to receive services. As a result of these and other factors, one-third of US children ages 3 to 5 have dental caries in their primary teeth, and one in every four US children is estimated to have untreated decay2,21-23 (see Figure 2). African-American and Hispanic children experience greater disparities in dental care than do those of other ethnicities.21
Dental decay is the most common chronic illness of childhood (five times as common as asthma), with higher incidence in low-income and minority preschool children.1,24,25 Tooth decay affects growth patterns and nutrition, with associated pain and infection interfering with school attendance.
The small number of dentists who treat children and are willing to accept Medicaid reimbursement is a significant concern. In most dental programs, dedicated pedodontic training is optional. The mismatch of number of qualified dentists to the growing population of such patients is projected to worsen in the coming years.23
Potential solutions to correct this mismatch of dental services accessible to the underserved have included26-31:
- Addition of paraprofessional dental therapists (persons who have received two years’ training in a specific academic program) to the health care team, in public health clinics, schools, and other settings
- Interprofessional dental education (ie, cross-training physicians, NPs, PAs, and RNs in preventive dental services)
- An increasingly diverse array of competent providers who are trained, authorized, and compensated to provide evidence-based care
- Removing licensure restrictions for non–US-trained dentists
- Financial incentives for dentists to practice in dental Health Professional Shortage Areas
- Improved education of parents regarding the benefits of routine dental services.
The Institute of Medicine (IOM)26 has challenged state legislatures to mandate a one-year dental residency to be completed among underserved populations before dental licensure is granted. This challenge reflects the IOM’s acknowledgement that dental services, essential to patients’ well-being, are grossly lacking in the US.
Dental Care Education for Parents
Healthy baby teeth help children eat well and speak clearly. Decayed and abscessed teeth cause the same degree of pain and suffering in young children as they do in adults. Thus, regardless of ethnicity or socioeconomic status, all parents should be routinely encouraged to oversee daily dental hygiene practices for their children; it is important for PCPs to explain to parents their expectations in this regard.
Dental care for children should begin as soon as the first tooth erupts. New teeth should be cleaned daily with a soft cloth and inspected by parents for any discolorations. From age 2 years until children are able to clean all dental surfaces adequately (age 7 or 8), parents should brush their children’s teeth at least once daily with a toothbrush, after applying a thin film of fluoride toothpaste. Children should undergo their first professional dental check-up at about age 1 year.19,26
Parents must be made aware of other factors that can impair their children’s dental health. For example, the foods most likely to promote dental decay contain highly fermentable carbohydrates, are highly processed and sticky, and cause oral pH levels to fall below 5.5 (at which point demineralization may occur).32 Examples include presweetened cereals, dried fruits, cookies, and potato chips. Cheese, peanuts, meat, and eggs are less cariogenic.
Other important teaching points are “don’ts”: putting a baby to bed with a bottle that contains anything but a sugar-free liquid; using spill-proof spouted cups filled with juice or other sugary drinks all day; serving a large proportion of cariogenic foods.
BREANNE, AGE 22
Breanne attends a community college, where she is studying business. She reports to the college health clinic, complaining of an intermittent sharp pain in one of her lower molars over the past four days, occurring when she eats or drinks anything cold.
Before she turned 21, Breanne received routine dental services under her parents’ insurance. Now a full-time student no longer covered by her parents’ plan, she has no income with which to purchase dental coverage. Years ago, Breanne received dental sealants on all of her molars in a school-based program, and she routinely brushes daily (see Figure 3). She says she “usually remembers to floss.”
Dental Concerns in Young Adults
Up to one-third of Americans, including college-age students, lack access to oral health services.33 Use of annual dental services, including school-based care, significantly reduces young adults’ risk for tooth loss.34 From early adulthood on, poor dental health is associated with cardiovascular and respiratory disease, cerebral ischemia, diabetes, difficulty with chewing and oral pain, and poor self-image.24
PCPs should emphasize the importance of preventive services as they examine the oral structure during routine health care encounters. Adding the question, “When did you last have a dental exam?” can launch an effective discussion about the importance of good dental health.
Tooth surfaces with pits and fissures are the most vulnerable to decay. Dental sealants can protect these vulnerable areas, reducing decay by 60% to 82%.2,32,35 Sealants are the most effective preventive measure for reducing cavity formation; they are not harmful to fillings and can actually reduce the progression of decay when applied over small existing carious lesions.35 Currently, however, only 30% and 38% of children and adolescents, respectively, have undergone application of sealants.36 Thus, it is vital for PCPs to recommend dental sealants to all their patients.35,37,38
Young adults should also be questioned about their exercise patterns. While daily exercise is of benefit to good health, young adults who engage in too-frequent, overly vigorous exercise have been found vulnerable to dental erosion.39 This irreversible condition can result from the rapid breathing, sweat-induced dehydration, and decreased salivary flow associated with strenuous exercise. Reduced salivary flow disrupts the protection against erosive acids afforded by bathing of teeth with saliva, leading to a fivefold greater risk for developing erosions. Patients should be encouraged to hydrate before exercise to reduce these risks.39
Dental Health Notes for Young Women
For female patients of childbearing age like Breanne, dental health is important not only for the patient, but for her future children as well. Poor maternal dental health has been associated with preterm births and low birth weights.40-43 Women who have health insurance, who are in good general health, and who regularly visit a primary care medical provider are also the most likely to see a dental care provider during pregnancy.40
Pregnancy is associated with a risk for poor dental care in any population.42,44 During pregnancy, Medicaid-enrolled women are 30% less likely to see a dentist than women with private health insurance, and women with no health insurance are 70% less likely to see a dentist.44 Among pregnant women who experience a dental problem, less than half will schedule a dental appointment. Postponing dental care till after delivery incurs additional risk, as the new mother will be busy with her child and may have lost her health care coverage in the interim.
Dental concerns commonly encountered during pregnancy are listed in Table 3.41,42 There is also evidence that maternal transmission of mutans streptococci can lead to early childhood caries,42,45 further highlighting the importance of dental care during pregnancy (eg, use of chlorhexidine rinses in pregnant women with dental caries42). The association between periodontal disease and preterm delivery and lower birth weights40-43 makes it critical to reduce maternal periodontal inflammation through timely dental referrals.
SAUL, AGE 42
Saul, a lifelong resident of Mississippi, has worked in construction since age 18. He has never had health or dental insurance and thus he rarely seeks preventive services. As he recalls, he has had “two fillings in my jaw teeth since I was a kid,” but otherwise has had no dental care. He brushes daily to avoid having to see a dentist. He is presenting today as a new patient only because he has a rash.
Benefits of Fluoride Use During Middle Age
Dental care needs peak between ages 55 and 64, with the majority of care prompted by dental decay46 (see Figure 4). A discussion about dental health should be raised when the PCP completes the review of systems or while discussing other preventive services. The option of fluoride varnish should not be overlooked in a patient of any age, particularly one with a recognizable deficiency of preventive dental services. Explaining the benefits of topical fluoride varnish (see “Fluoride Use”) and offering an opportunity to receive it in the office may persuade a patient like Saul to take advantage of this proven anticarious procedure.
Patients who undergo this safe procedure should be reminded to continue brushing daily with fluoridated toothpaste and drinking fluoridated water (if it is available).50
GILL, AGE 77
Gill grew up in Grant County, New Mexico, in an area not far from Silver City; there, fluoride supplementation in the local water did not begin until Gill was about 40. His family never stressed oral hygiene, and his remaining teeth show gross plaque and decay.
He sees you routinely for his chronic illnesses, and today he has presented for his annual physical. Gill has Medicare without supplemental insurance.
Dental Care in the Medicare Years
Medicare does not cover preventive dental services unless hospitalization is required; in that case, it is covered under Medicare Part A.51 Publicly supported dental services are primarily offered for children, leaving Medicare recipients responsible for the costs of dental care. As a last resort, some patients will seek dental care at a hospital emergency department (ED). Most often prompted to visit the ED for relief of pain triggered by dental fractures or abscesses, patients usually leave with pain medications and antibiotics only; their general dental health needs remain unmet.52
The most common dental concerns among elderly patients include edentulism (toothlessness, which is reported in one in four Medicare beneficiaries1), xerostomia (dry mouth), periodontal disease, ill-fitting or worn prosthetics, and progressive decay affecting fractured teeth1 (see Figure 5). As many elderly patients endure a combination of these uncomfortable, possibly painful, conditions, it is important for the PCP to inquire about them during the physical exam and the review of symptoms. At each step, a window of opportunity opens to make appropriate recommendations.
Significant Comorbidities
It is important for PCPs to recognize the association between certain diseases and poor oral health. With the progression of age, the risk increases for type 2 diabetes. Among older diabetic patients with periodontitis (and the systemic inflammation associated with it), the difficulty of maintaining glycemic control increases as well.53 Conversely, diabetic patients who are immunocompromised are at elevated risk for periodontitis. In more than 20 years of formal data collection, periodontists have identified and confirmed an anecdotal relationship between diabetes and severe periodontal disease.26
Elderly patients with poor dental health are also at increased risk for chronic kidney disease. Periodontal disease alone increases the risk for nephropathy 1.5-fold to twofold.54Finally, patients’ risk for oral cancer increases with age. Known risk factors for oral cancers include smoking, use of chewing tobacco, alcohol consumption, chronic friction, and exposure to ultraviolet radiation.55 Survival rates for oral cancers are poor, reemphasizing the need for a thorough oral exam during primary care visits.
Other Challenges for Older Patients
Members of ethnic minority groups and lower-income populations, men, patients with cognitive impairment, and persons who never completed high school are the most likely to avoid, discontinue, or lack access to dental services.56 Loss of dental coverage on retirement is associated with a significant decline in elderly patients’ use of dental services. Though now living on a fraction of their preretirement income, millions of retirees are required to pay out-of-pocket for dental services.57
Topical fluoride varnish alone cannot alleviate this multimillion dollar concern, but using it to reinforce retirees’ remaining enamel and prevent caries can help reduce their dental care expenditures. However, until federal and state policymakers act to cover preventive services,2,58 PCPs have little to offer elderly patients beyond oral hygiene education and in-office application of topical fluoride.
Strategies to Reinforce Dental Health
In practices where electronic medical records are in use, a recommendation for dental services should be printed as a patient reminder. Printed recommendations and referrals from PCPs do improve patient compliance.59 In addition to the printed office summary, older patients can be handed a summary of oral health suggestions from the National Institute on Aging, NIH59 (www.nia.nih.gov/health/publication/taking-care-your-teeth-and-mouth).
CONCLUSION
For most Americans with dental health insurance, access to services, and a willingness to practice good oral hygiene, dental care quality is above average. However, health care disparities and a lack of dental coverage prevent millions of Americans from routinely seeking dental services—making it essential for PCPs to promote oral hygiene and offer professional dental referrals with patients of all ages. Topical fluoride varnish, which can reduce the risk for decay as well as progression of existing decay, is an important preventive service that is within the scope of primary care practice.
1. Kaiser Commission. Medicaid and the uninsured: oral health in the US: key facts (2012). www.kff.org/uninsured/upload/8324.pdf. Accessed February 11, 2013.
2. Healthy People 2020. Oral health. www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=32. Accessed February 11, 2013.
3. CDC. Community water fluoridation: other fluoride products (2011). www.cdc.gov/fluoridation/other.htm. Accessed February 11, 2013.
4. American Academy of Pediatrics. Advocacy: Medicaid, fluoride varnish (2011). www.paaap.org/adv_medicaid_pg2.php. Accessed February 11, 2013.
5. National Institute of Dental and Craniofacial Research, NIH. The story of fluoridation (2011). www.nidcr.nih.gov/oralhealth/topics/fluoride/thestoryoffluoridation.htm. Accessed February 11, 2013.
6. Yu H, Attin T, Wiegand A, Buchalla W. Effects of various fluoride solutions on enamel erosion in vitro. Caries Res. 2010;44(4):390-401.
7. Bertness J, Holt K, eds; National Maternal & Child Oral Health Resource Center. Fluoride varnish: a resource guide (2010). www.mchoralhealth.org/PDFs/ResGuideFlVarnish.pdf. Accessed February 11, 2013.
8. Lee YE, Baek HJ, Choi YH, et al. Comparison of remineralization effect of three topical fluoride regimens on enamel initial carious lesions. J Dent. 2010;38(2):166-171.
9. New Zealand Guidelines Group. Guidelines for the use of fluorides (2009). Wellington, New Zealand: New Zealand Ministry of Health. www.guideline.gov/content.aspx?id=25685&search=fluoride+varnish. Accessed February 11, 2013.
10. O’Keefe E. Fluoride varnish may be effective in preschoolers. Evid Based Dent. 2011;12(2):41-42.
11. American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Am Dent Assoc. 2006;137(8):1151-1159.
12. MassHealth. Health and Human Services. Fluoride varnish training for health-care professionals (2012). www.mass.gov/eohhs/gov/newsroom/masshealth/providers/fluoride-varnish-training-for-health-care.html. Accessed February 11, 2013.
13. Collins FM; Academy of Dental Therapeutics and Stomatology. The development and utilization of fluoride varnish (2011). www.ineedce.com/courses/2093/PDF/1106cei_varnish_web4.pdf. Accessed February 11, 2013.
14. New York State Department of Health. Improving the oral health of young children: fluoride varnish training materials and oral health information for child health care providers (2010). www.health.ny.gov/prevention/dental/child_oral_health_fluoride_varnish_for_hcp.htm. Accessed February 11, 2013.
15. Missouri Department of Health and Senior Services. Fluoride varnish application training for Missouri Oral Health Preventive Services Program. http://mohealthysmiles.typepad.com/Fluoride_Varnish_App_Training.pdf. Accessed February 15, 2013.
16. American Academy of Pediatrics. Oral health coding fact sheet for primary care physicians (2010). www2.aap.org/oralhealth/docs/OHCoding.pdf. Accessed February 11, 2013.
17. Chersoni S, Bertacci A, Pashley D, et al. In vivo effects of fluoride on enamel permeability. Clin Oral Investig. 2011;15(4):443-449.
18. National Interprofessional Initiative on Oral Health. Smiles for life curriculum (2011). www.niioh.org/smiles-life-curriculum. Accessed February 11, 2013.
19. Douglass AB, Gonsalves W, Maier R, et al. Smiles for Life: a national oral health curriculum for family medicine. Fam Med. 2007;39(2):88-90.
20. Medicaid.gov. Children’s Health Insurance Program (CHIP). www.medicaid .gov/Medicaid-CHIP-Program-Information/By-Topics/Childrens-Health-Insurance-Program-CHIP/Childrens-Health-Insurance-Program-CHIP.html. Accessed February 11, 2013.
21. Pourat N, Finocchio L. Racial and ethnic disparities in dental care for publicly insured children. Health Aff (Millwood). 2010;29(7):1356-1363.
22. Edelstein BL, Chinn CH. Update on disparities in oral health and access to dental care for America’s children. Acad Pediatr. 2009;9(6):415-419.
23. Seale NS, McWhorter AG, Moulradian WE. Dental education’s role in improving children’s oral health and access to care. Acad Pediatr. 2009;9(6):440-445.
24. National Institute of Dental and Craniofacial Research, NIH. Oral Health in America: A Report of the Surgeon General (Executive Summary; 2011). www.nidcr.nih.gov/datastatistics/surgeongeneral/report/executivesummary.htm. Accessed February 5, 2013.
25. Grembowski D, Spiekerman C, Milgrom P. Social gradients in dental health among low-income mothers and their young children. J Health Care Poor Underserved. 2012;23(2):570-588.
26. Institute of Medicine of the National Academies. Improving access to oral health care for vulnerable and underserved populations (2011). www.iom.edu/~/media/Files/Report Files/2011/Improving-Access-to-Oral-Health-Care-for-Vulnerable-and-Underserved-Populations/oralhealthaccess2011reportbrief.pdf. Accessed February 11, 2013.
27. Bertolami CN. Access to dental care: is there a problem? Am J Public Health. 2011;101(10):1817.
28. Bazargan N, Chi DL, Milgrom P. Exploring the potential for foreign-trained dentists to address workforce shortages and improve access to dental care for vulnerable populations in the United States: a case study from Washington State. BMC Health Serv Res. 2010;10:336-343.
29. Nash DA. Adding dental therapists to the health care team to improve access to oral health care for children. Acad Pediatr. 2009;9(6):446-451.
30. Liao CC, Ganz ML, Jiang H, Chelmow T. The impact of the public insurance expansions on children’s use of preventive dental care. Matern Child Health J. 2010;14(1):58-66.
31. Duley SI, Fitzpatrick PG, Zornosa X, Barnes WG. A center for oral health promotion: establishing an inter-professional paradigm for dental hygiene, health care management and nursing education. J Dent Hyg. 2012;86(2):63-70.
32. Ritter AV, Eidson RS, Donovan TE. Dental caries: etiology, clinical characteristics, risk assessment, and management. In: Heymann HO, Swift EJ Jr, Ritter AV, eds. Sturdevant’s Art and Science of Operative Dentistry. 6th ed. St. Louis: Elsevier-Mosby; 2012:41-89.
33. Shaefer HL, Miller M. Improving access to oral health care services among underserved populations in the US: is there a role for mid-level dental providers? J Health Care Poor Underserved. 2011;22(3):740-744.
34. Li KY, Wong MC, Lam KF, Schwarz E. Age, period, and cohort analysis of regular dental care behavior and edentulism: a marginal approach. BMC Oral Health. 2011;11:9.
35. Beauchamp J, Caufield PW, Crall JJ, et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008;139(3):257-268.
36. National Institute of Dental and Craniofacial Research, NIH. Dental sealants in children (age 8 to 11)(2011). www.nidcr.nih.gov/DataStatistics/FindDataByTopic/DentalSealants/Children. Accessed February 11, 2013.
37. Gore DR. The use of dental sealants in adults: a long-neglected preventive measure. Int J Dent Hyg. 2010;8(3):198-203.
38. Devlin D, Henshaw M. Improving access to preventive dental services through a school-based dental sealant program. J Dent Hyg. 2011;85(3):211-219.
39. Mulic A, Tveit AB, Songe D, et al. Dental erosive wear and salivary flow rate in physically active young adults. BMC Oral Health. 2012;12:8.
40. Kaylor MB, Polivka BJ, Chaudry R, et al. Dental services utilization by women of child-bearing age by socioeconomic status. J Community Health. 2010;35(2):190-197.
41. Michalowicz BS, Hodges JS, DiAngelis AJ, et al; OPT Study. Treatment of periodontal disease and the risk of preterm birth. N Engl J Med. 2006;355(18):1885-1894.
42. Silk H, Douglass AB, Douglass JM, Silk L. Oral health during pregnancy. Am Fam Physician. 2008;77(8):1139-1144.
43. Clothier B, Stringer M, Jeffcoat MK. Periodontal disease and pregnancy outcomes: exposure, risk and intervention. Best Pract Res Clin Obstet Gynaecol. 2007;21(3):451-466.
44. Ressler-Maerlender J, Krishna R, Robison V. Oral health during pregnancy: current research. J Womens Health (Larchmt). 2005;14(10):880-882.
45. Berkowitz RJ. Acquisition and transmission of mutans streptococci. J Calif Dent Assoc. 2003;31(2):135-138.
46. Vollmer WM, Papas AS, Bader JD, et al; PACS Collaborative Research Group. Design of the Prevention of Adult Caries Study (PACS): a randomized clinical trial assessing the effect of chlorhexidine dental coating for the protection of adult caries. BMC Oral Health. 2010;10:23.
47. Dhull KS, Nandlal B. Effect of low-concentration daily fluoride application on fluoride release of giomer and compomer: an in vitro study. J Indian Soc Pedod Prev Dent. 2011;29(1):39-45.
48. Naumova EA, Kuehnl P, Hertenstein P, et al. Fluoride bioavailability in saliva and plaque. BMC Oral Health. 2012;12:3.
49. Duckworth RM, Maguire A, Omid N, et al. Effect of rinsing with mouthwash after brushing with fluoridated toothpaste on salivary fluoride concentration. Caries Res. 2009;43(5):391-396.
50. Opydo-Szymaczek J, Opydo J. Salivary fluoride concentrations and fluoride ingestion following application of preparations containing high concentration of fluoride. Biol Trace Elem Res. 2010;137(2):159-167.
51. Medicare.gov. Your Medicare coverage: dental services. www.medicare.gov/coverage/dental-services.html. Accessed February 11, 2013.
52. Quiñonez C, Ieraci L, Guttmann A. Potentially preventable hospital use for dental conditions: implications for expanding dental coverage for low income populations. J Health Care Poor Underserved. 2011;22(3):1048-1058.
53. Deshpande K, Jain A, Sharma RK, et al. Diabetes and periodontitis. J Indian Soc Periodontol. 2010;14(4):207-212.
54. Grubbs V, Plantinga LC, Tuot DS, Powe NR. Chronic kidney disease and use of dental services in a United States public healthcare system: a retrospective cohort study. BMC Nephrol. 2012;13:16.
55. Nair DR, Pruthy R, Pawar U, Chaturvedi P. Oral cancer: premalignant conditions and screening—an update. J Cancer Res Ther. 2012;8 suppl 1:S57-S66.
56. Wu B, Plassman BL, Lian J, Wei L. Cognitive function and dental care utilization among community-dwelling older adults. Am J Public Health. 2007;97(12):2216-2221.
57. Manski RJ, Moeller JF, St Clair PA, et al. The influence of changes in dental care coverage on dental care utilization among retirees and near-retirees in the United States, 2004-2006. Am J Public Health. 2011;101(10):1882-1891.
58. Moeller JF, Chen H, Manski RJ. Investing in preventive dental care for the Medicare population: a preliminary analysis. Am J Public Health. 2010;100(11):2262-2269.
59. National Institute on Aging, NIH. AgePage: Taking care of your teeth and mouth (2011). www.nia.nih.gov/health/publication/taking-care-your-teeth-and-mouth. Accessed February 6, 2013.
1. Kaiser Commission. Medicaid and the uninsured: oral health in the US: key facts (2012). www.kff.org/uninsured/upload/8324.pdf. Accessed February 11, 2013.
2. Healthy People 2020. Oral health. www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=32. Accessed February 11, 2013.
3. CDC. Community water fluoridation: other fluoride products (2011). www.cdc.gov/fluoridation/other.htm. Accessed February 11, 2013.
4. American Academy of Pediatrics. Advocacy: Medicaid, fluoride varnish (2011). www.paaap.org/adv_medicaid_pg2.php. Accessed February 11, 2013.
5. National Institute of Dental and Craniofacial Research, NIH. The story of fluoridation (2011). www.nidcr.nih.gov/oralhealth/topics/fluoride/thestoryoffluoridation.htm. Accessed February 11, 2013.
6. Yu H, Attin T, Wiegand A, Buchalla W. Effects of various fluoride solutions on enamel erosion in vitro. Caries Res. 2010;44(4):390-401.
7. Bertness J, Holt K, eds; National Maternal & Child Oral Health Resource Center. Fluoride varnish: a resource guide (2010). www.mchoralhealth.org/PDFs/ResGuideFlVarnish.pdf. Accessed February 11, 2013.
8. Lee YE, Baek HJ, Choi YH, et al. Comparison of remineralization effect of three topical fluoride regimens on enamel initial carious lesions. J Dent. 2010;38(2):166-171.
9. New Zealand Guidelines Group. Guidelines for the use of fluorides (2009). Wellington, New Zealand: New Zealand Ministry of Health. www.guideline.gov/content.aspx?id=25685&search=fluoride+varnish. Accessed February 11, 2013.
10. O’Keefe E. Fluoride varnish may be effective in preschoolers. Evid Based Dent. 2011;12(2):41-42.
11. American Dental Association Council on Scientific Affairs. Professionally applied topical fluoride: evidence-based clinical recommendations. J Am Dent Assoc. 2006;137(8):1151-1159.
12. MassHealth. Health and Human Services. Fluoride varnish training for health-care professionals (2012). www.mass.gov/eohhs/gov/newsroom/masshealth/providers/fluoride-varnish-training-for-health-care.html. Accessed February 11, 2013.
13. Collins FM; Academy of Dental Therapeutics and Stomatology. The development and utilization of fluoride varnish (2011). www.ineedce.com/courses/2093/PDF/1106cei_varnish_web4.pdf. Accessed February 11, 2013.
14. New York State Department of Health. Improving the oral health of young children: fluoride varnish training materials and oral health information for child health care providers (2010). www.health.ny.gov/prevention/dental/child_oral_health_fluoride_varnish_for_hcp.htm. Accessed February 11, 2013.
15. Missouri Department of Health and Senior Services. Fluoride varnish application training for Missouri Oral Health Preventive Services Program. http://mohealthysmiles.typepad.com/Fluoride_Varnish_App_Training.pdf. Accessed February 15, 2013.
16. American Academy of Pediatrics. Oral health coding fact sheet for primary care physicians (2010). www2.aap.org/oralhealth/docs/OHCoding.pdf. Accessed February 11, 2013.
17. Chersoni S, Bertacci A, Pashley D, et al. In vivo effects of fluoride on enamel permeability. Clin Oral Investig. 2011;15(4):443-449.
18. National Interprofessional Initiative on Oral Health. Smiles for life curriculum (2011). www.niioh.org/smiles-life-curriculum. Accessed February 11, 2013.
19. Douglass AB, Gonsalves W, Maier R, et al. Smiles for Life: a national oral health curriculum for family medicine. Fam Med. 2007;39(2):88-90.
20. Medicaid.gov. Children’s Health Insurance Program (CHIP). www.medicaid .gov/Medicaid-CHIP-Program-Information/By-Topics/Childrens-Health-Insurance-Program-CHIP/Childrens-Health-Insurance-Program-CHIP.html. Accessed February 11, 2013.
21. Pourat N, Finocchio L. Racial and ethnic disparities in dental care for publicly insured children. Health Aff (Millwood). 2010;29(7):1356-1363.
22. Edelstein BL, Chinn CH. Update on disparities in oral health and access to dental care for America’s children. Acad Pediatr. 2009;9(6):415-419.
23. Seale NS, McWhorter AG, Moulradian WE. Dental education’s role in improving children’s oral health and access to care. Acad Pediatr. 2009;9(6):440-445.
24. National Institute of Dental and Craniofacial Research, NIH. Oral Health in America: A Report of the Surgeon General (Executive Summary; 2011). www.nidcr.nih.gov/datastatistics/surgeongeneral/report/executivesummary.htm. Accessed February 5, 2013.
25. Grembowski D, Spiekerman C, Milgrom P. Social gradients in dental health among low-income mothers and their young children. J Health Care Poor Underserved. 2012;23(2):570-588.
26. Institute of Medicine of the National Academies. Improving access to oral health care for vulnerable and underserved populations (2011). www.iom.edu/~/media/Files/Report Files/2011/Improving-Access-to-Oral-Health-Care-for-Vulnerable-and-Underserved-Populations/oralhealthaccess2011reportbrief.pdf. Accessed February 11, 2013.
27. Bertolami CN. Access to dental care: is there a problem? Am J Public Health. 2011;101(10):1817.
28. Bazargan N, Chi DL, Milgrom P. Exploring the potential for foreign-trained dentists to address workforce shortages and improve access to dental care for vulnerable populations in the United States: a case study from Washington State. BMC Health Serv Res. 2010;10:336-343.
29. Nash DA. Adding dental therapists to the health care team to improve access to oral health care for children. Acad Pediatr. 2009;9(6):446-451.
30. Liao CC, Ganz ML, Jiang H, Chelmow T. The impact of the public insurance expansions on children’s use of preventive dental care. Matern Child Health J. 2010;14(1):58-66.
31. Duley SI, Fitzpatrick PG, Zornosa X, Barnes WG. A center for oral health promotion: establishing an inter-professional paradigm for dental hygiene, health care management and nursing education. J Dent Hyg. 2012;86(2):63-70.
32. Ritter AV, Eidson RS, Donovan TE. Dental caries: etiology, clinical characteristics, risk assessment, and management. In: Heymann HO, Swift EJ Jr, Ritter AV, eds. Sturdevant’s Art and Science of Operative Dentistry. 6th ed. St. Louis: Elsevier-Mosby; 2012:41-89.
33. Shaefer HL, Miller M. Improving access to oral health care services among underserved populations in the US: is there a role for mid-level dental providers? J Health Care Poor Underserved. 2011;22(3):740-744.
34. Li KY, Wong MC, Lam KF, Schwarz E. Age, period, and cohort analysis of regular dental care behavior and edentulism: a marginal approach. BMC Oral Health. 2011;11:9.
35. Beauchamp J, Caufield PW, Crall JJ, et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2008;139(3):257-268.
36. National Institute of Dental and Craniofacial Research, NIH. Dental sealants in children (age 8 to 11)(2011). www.nidcr.nih.gov/DataStatistics/FindDataByTopic/DentalSealants/Children. Accessed February 11, 2013.
37. Gore DR. The use of dental sealants in adults: a long-neglected preventive measure. Int J Dent Hyg. 2010;8(3):198-203.
38. Devlin D, Henshaw M. Improving access to preventive dental services through a school-based dental sealant program. J Dent Hyg. 2011;85(3):211-219.
39. Mulic A, Tveit AB, Songe D, et al. Dental erosive wear and salivary flow rate in physically active young adults. BMC Oral Health. 2012;12:8.
40. Kaylor MB, Polivka BJ, Chaudry R, et al. Dental services utilization by women of child-bearing age by socioeconomic status. J Community Health. 2010;35(2):190-197.
41. Michalowicz BS, Hodges JS, DiAngelis AJ, et al; OPT Study. Treatment of periodontal disease and the risk of preterm birth. N Engl J Med. 2006;355(18):1885-1894.
42. Silk H, Douglass AB, Douglass JM, Silk L. Oral health during pregnancy. Am Fam Physician. 2008;77(8):1139-1144.
43. Clothier B, Stringer M, Jeffcoat MK. Periodontal disease and pregnancy outcomes: exposure, risk and intervention. Best Pract Res Clin Obstet Gynaecol. 2007;21(3):451-466.
44. Ressler-Maerlender J, Krishna R, Robison V. Oral health during pregnancy: current research. J Womens Health (Larchmt). 2005;14(10):880-882.
45. Berkowitz RJ. Acquisition and transmission of mutans streptococci. J Calif Dent Assoc. 2003;31(2):135-138.
46. Vollmer WM, Papas AS, Bader JD, et al; PACS Collaborative Research Group. Design of the Prevention of Adult Caries Study (PACS): a randomized clinical trial assessing the effect of chlorhexidine dental coating for the protection of adult caries. BMC Oral Health. 2010;10:23.
47. Dhull KS, Nandlal B. Effect of low-concentration daily fluoride application on fluoride release of giomer and compomer: an in vitro study. J Indian Soc Pedod Prev Dent. 2011;29(1):39-45.
48. Naumova EA, Kuehnl P, Hertenstein P, et al. Fluoride bioavailability in saliva and plaque. BMC Oral Health. 2012;12:3.
49. Duckworth RM, Maguire A, Omid N, et al. Effect of rinsing with mouthwash after brushing with fluoridated toothpaste on salivary fluoride concentration. Caries Res. 2009;43(5):391-396.
50. Opydo-Szymaczek J, Opydo J. Salivary fluoride concentrations and fluoride ingestion following application of preparations containing high concentration of fluoride. Biol Trace Elem Res. 2010;137(2):159-167.
51. Medicare.gov. Your Medicare coverage: dental services. www.medicare.gov/coverage/dental-services.html. Accessed February 11, 2013.
52. Quiñonez C, Ieraci L, Guttmann A. Potentially preventable hospital use for dental conditions: implications for expanding dental coverage for low income populations. J Health Care Poor Underserved. 2011;22(3):1048-1058.
53. Deshpande K, Jain A, Sharma RK, et al. Diabetes and periodontitis. J Indian Soc Periodontol. 2010;14(4):207-212.
54. Grubbs V, Plantinga LC, Tuot DS, Powe NR. Chronic kidney disease and use of dental services in a United States public healthcare system: a retrospective cohort study. BMC Nephrol. 2012;13:16.
55. Nair DR, Pruthy R, Pawar U, Chaturvedi P. Oral cancer: premalignant conditions and screening—an update. J Cancer Res Ther. 2012;8 suppl 1:S57-S66.
56. Wu B, Plassman BL, Lian J, Wei L. Cognitive function and dental care utilization among community-dwelling older adults. Am J Public Health. 2007;97(12):2216-2221.
57. Manski RJ, Moeller JF, St Clair PA, et al. The influence of changes in dental care coverage on dental care utilization among retirees and near-retirees in the United States, 2004-2006. Am J Public Health. 2011;101(10):1882-1891.
58. Moeller JF, Chen H, Manski RJ. Investing in preventive dental care for the Medicare population: a preliminary analysis. Am J Public Health. 2010;100(11):2262-2269.
59. National Institute on Aging, NIH. AgePage: Taking care of your teeth and mouth (2011). www.nia.nih.gov/health/publication/taking-care-your-teeth-and-mouth. Accessed February 6, 2013.