User login
Drowning episodes: Prevention and resuscitation tips
› Recommend swimming lessons for all children ages 4 and older. C
› Consider antibiotics after a drowning event only if the water is known to be contaminated or the victim has aspirated a large volume of water. C
› Monitor asymptomatic patients for at least 4 hours after a drowning event. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A young mother in your practice wants her toddler to begin swimming lessons because her family loves water activities. How would you advise her? In fielding an urgent call about a drowning incident, what priorities would you urge regarding resuscitation at the scene? For a stabilized patient following a drowning episode, when might antibiotics be indicated? This article covers these issues as well as follow-up matters such as assisted ventilation and tiered hypothermia intervention.
Drowning likely occurs more often than is reported
Worldwide, drowning accounts for more than 388,000 deaths annually and is the third leading cause of unintentional injury death. Low- and middle-income countries represent 96% of the yearly total.1 As reported in the United States, nearly 6000 individuals are hospitalized and nearly 4000 die from drowning events annually.2 But these figures likely underestimate the true rate, as many drowning fatalities are officially attributed to floods, boating accidents, or other associated events. Nonfatal drownings often go unreported.
Children under the age of 5 years have the highest drowning mortality worldwide, and drowning is the leading cause of unintentional injury death for this age group in many countries, including the United States.1,2 Men are nearly 4 times as likely to die from drowning than women.2 Predictably, in the United States most drowning happens on the weekend and during summer months. More than half of drownings in children younger than 4 years occur in swimming pools; with increasing age, drowning is more likely to occur in natural bodies of water.2 With adults in higher income countries, alcohol is a significant contributor to drowning events during recreational activities.3-5
Much effort has been made in recent years to standardize the nomenclature and treatment of drowning episodes. The International World Congress on Drowning met in the Netherlands in 2002, and established the definition of drowning as “the process of experiencing respiratory impairment from submersion/immersion in liquid.”6 Submersion refers to the complete submergence of the victim under the water, while immersion implies that the victim’s airway remains above the water.
The Congress recommended that terms such as “wet-drowning,” “dry-drowning,” and “near-drowning” be discontinued in favor of the outcome classifications “death,” “no morbidity,” and “morbidity.” The “morbidity” subgroup was further characterized as “moderately disabled,” “severely disabled,” “vegetative state/coma,” and “brain death.” This meeting established guidelines on the treatment of drowning victims in addition to outlining points for future research.6
Physiologic chain of events in drowning
An unexpected immersion in water, particularly cold water, causes a reflexive inspiratory gasp, and some degree of aspiration occurs in most, if not all, cases of drowning. Aspiration further impairs victims’ ability to hold their breath or breathe normally.5,7,8 It decreases lung compliance due to surfactant washout or intrapulmonary shunting and thereby leads to hypoxia. Aspiration-induced severe laryngospasm can also lead to hypoxia. Pulmonary edema and acute respiratory distress syndrome (ARDS) can follow.
The cardiovascular effects of drowning mirror those seen in hypoxia. Initially, apnea leads to decreased oxygen saturation and precipitates tachycardia and hypertension. Bradycardia and hypotension follow and blood is shunted to vital organs, such as the brain, heart, and lungs.9 This phenomenon is accelerated in cold water and leads to “swimming failure,” the impaired ability of the victim to swim because of decreased perfusion of the extremities.5,7,8,10
“Autonomic conflict” has been proposed as an additional mechanism for morbidity and mortality from drowning episodes. Breath holding and immersion in cold water each can induce cardiac arrhythmias. When combined, these events may increase the risk of an arrhythmogenic state secondary to opposing chronotropic effects: the diving reflex (bradycardia via parasympathetic activation), and the cold shock response (tachycardia via sympathetic activation). This is thought to be an underreported cause of death in drowning, as arrhythmias are undetectable during autopsy.8,11
Drowning prevention
The American Academy of Pediatrics (AAP) recommends swimming lessons for most children ages 4 years and older.12 Previously, swimming lessons were not recommended for children ages 1 to 4 because evidence of benefit was lacking, and there was some concern that it might reduce children’s caution around water and reduce parents’ perceived level of need for supervision. Although data are still conflicting, some reports have since shown benefit in early swimming lessons for
toddlers.13,14
As of 2010, the AAP acknowledges that training may be beneficial for children in this age group, but cautions that not all children will be ready for swimming by this age.12 Infant water safety programs for children under the age of 1 are not recommended because evidence of benefit is lacking.12
Evidence is growing to support teaching basic water survival skills in low- to middle-income countries where water sources are abundant, particularly in Southeast Asia. Specifically, the SwimSafe survival swimming program has yielded impressive results in Bangladesh.15 This program targets children starting at age 5, and involves 20 lessons teaching basic water survival and rescue skills.
Results have shown a 93% reduction in drowning rates for children enrolled in the program, compared with those not enrolled.15 Subsequent analyses have proposed that swimming lessons for children in these parts of the world would be as cost effective as current attempts to prevent diarrheal and respiratory diseases in the same areas.16
Additional preventive measures that are effective in the United States include 4-sided pool fencing, use of personal flotation devices, and bystander cardiopulmonary
resuscitation (CPR).2,5,17
On-scene evaluation and treatment
Drowning victims can appear mottled and have minimal or no peripheral pulses despite a heartbeat. Rescuers may assume the victim is dead when, in fact, there is cardiac function. Because initial assessment in this situation is difficult, CPR should begin, if possible, the moment the victim is out of the water. Successful on-scene resuscitation is the surest predictor of survival.9,18 In fact, delay of CPR until the arrival of emergency personnel lessens the likelihood of survival.19
CPR applied to drowning. For cardiogenic cardiac arrest, chest compressions alone may be better than compressions with rescue breathing. For victims of drowning, though, coordinated compressions and rescue breathing are recommended.20 The
2010 revision of the American Heart Association Guidelines for CPR and Emergency Cardiovascular Care emphasize “compression first” for CPR in cases of cardiogenic cardiac arrest, but continue to support the traditional Airway-Breathing-Chest Compressions sequence for drowning victims in its Special Situations section.21
Ventricular fibrillation (VF) is rare after submersion injury. An external defibrillator should be used when available, but it is unlikely to play a significant role in initial resuscitation.9
Don’t attempt to remove water from the victim’s mouth before resuscitation. The volume of fluid in the oral cavity is usually insignificant, and trying to remove it by abdominal thrusts or Heimlich maneuver will delay CPR and may injure the patient.21
Cervical spine injury is uncommon in drowning episodes, making cervical spine immobilization unnecessary unless the mechanism of injury is known or if there are clinical signs suggesting such injury. Needless cervical spine immobilization can interfere with adequate ventilation.22,23 However, concern for head or cervical spine injury is warranted when recovering an unconscious victim from shallow water, where such injuries are more likely to result from falling or diving into the water.24
Administer oxygen supplementation when available to all spontaneously breathing individuals. Individuals who respond well to initial resuscitation and who don’t require intubation tend to have a very good prognosis overall.25
Total time of submersion and the temperature of the water have bearing on the likelihood of survival. Only in rare cases have victims survived submersion lasting longer than 30 minutes. Ten minutes generally is considered the “point of no return.”9,26 This is consistent with data suggesting 10 minutes of hypoxic insult causes irreversible neurologic damage, with each additional minute rapidly leading to coma.20 However, to complicate matters, unlike cardiac arrest victims, drowning victims can lose cerebral blood flow slowly after respiratory impairment, which makes duration of submersion a potentially unreliable predictor of neurologic outcome.20,26
Does hypothermia have a protective effect? Hypothermia can occur in water 85°F (30°C) or cooler.10 It has been hypothesized that resuscitation can be achieved after longer periods of submersion in cold water. However, the considerable debate on this topic has been based on little more than case reports.
For hypothermia to have a protective effect on neurologic function, cooling must take place rapidly and, ideally, before any hypoxic insult. The water would have to be exceptionally cold, likely less than 50°F (10°C).27 The greater surface-to-volume ratio in children enables more rapid cooling and quicker onset of hypothermia, which may explain why they seem to have better neurologic outcomes than adults after prolonged submersion.28
Hypothermia can also be protective if the victim is breathing when cooling begins, such as while floating or swimming in cold water before drowning.29 This was the likely scenario in a reported case of a Norwegian kayaker who called for help after capsizing in 38°F (3.3°C) seawater. Despite having been in cardiac arrest for over 3 hours, the individual experienced a spontaneous return of circulation and was discharged after 32 days with no neurologic deficits.29
Correcting hypothermia after rescue. Conscious patients with no cardiovascular or respiratory compromise should have wet clothing removed at the scene in exchange for blankets, towels, or warm dry clothing. Advise rescuers to attempt no further rewarming at the scene. With unconscious patients, take only simple measures to prevent further heat loss, and focus on transport and resuscitative efforts.24
Hospital management
Attempts have been made to create a prognostic or predictive scoring system for drowning victims presenting to the emergency department. Factors thought to have bearing on mortality include duration of submersion, victim’s age, Glasgow Coma Scale (GCS) score, pupillary reactivity, and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score.23,30,31 Other measurements, such as core temperature, blood pH, and response to painful stimuli, correlate poorly with mortality.31 Hyperkalemia is repeatedly mentioned as a predictor of a poor neurologic outcome, as it is thought to indicate hypoxia before the onset of cooling.8,26,32 The best predictor of a good outcome is consciousness at the time of arrival at the emergency department.4
Continued ventilation assistance is critical. As with prehospital resuscitation efforts, ventilation is critical to in-hospital management. For patients who are breathing spontaneously, continuous positive airway pressure or bi-level positive airway pressure can reduce hypoxia in pulmonary edema. Standard indications of the need for intubation include decreased level of consciousness or concern for ability to protect the airway, hypoxia despite a high fraction of inspired oxygen (FiO2), or persistent hypercapnia even with adequate noninvasive ventilatory support.33
Victims may swallow large amounts of liquid during drowning; for intubated patients, advise orogastric tube placement to prevent aspiration of gastric contents. The reliability of pulse oximetry has been called into question in this setting and may be less accurate for victims who are hypothermic or who have been submerged in cold water.23,34
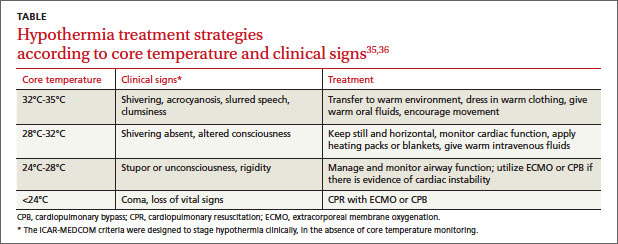
Tiered intervention for hypothermia. In the hospital setting, passive rewarming is indicated for individuals with a body core temperature of 89.6°F to 95°F (32°C-35°C). Remove wet clothing; cover the victim with warm, dry towels or blankets; and give warm oral fluids and urge movement.
Individuals with core temperatures between 82.4°F to 89.6°F (28°C-32°C) require active external rewarming by applying heat directly to the skin via hot packs, warm blankets, and insulation. These patients should remain in a horizontal position with little movement, if possible, to avoid cold peripheral blood rapidly shifting to the core and precipitating an arrhythmia. Warmed intravenous fluids are appropriate as well.
With a core temperature less than 82.4°F (28°C), aggressive rewarming with extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass (CPB) may be warranted as this individual will likely have unstable or absent vital signs (TABLE).35,36 Some authorities advise that drowning victims with severe hypothermia and cardiac arrest should be resuscitated at facilities with CPB capability.27,28,37
Inducing hypothermia therapeutically is still unproven. Although not tested specifically on drowning victims, therapeutic hypothermia would seem to have theoretical benefit for their resuscitation. In cardiogenic cardiac arrest, good evidence exists for improved neurologic outcomes with therapeutic hypothermia,38 and this benefit might extend to drowning victims given their similar neurologic injury. No specific pharmacologic therapies have shown benefit in preventing loss of cerebral function.9
Monitor for clinical worsening. The concept of “secondary drowning,” a term now abandoned, referred to the phenomenon of clinical worsening hours after the initial drowning episode and resuscitation. This occurrence is now thought to be due to laryngospasm or to the progressive development of pulmonary edema from the aspiration of small amounts of water. Evidence supports monitoring asymptomatic patients; however, the period of suggested monitoring varies between 4 and 24 hours after the incident.8,22,24
Imaging, if delayed, may be useful. Imaging immediately after a drowning episode is an unreliable predictor of outcome and should be sought only if trauma or symptoms dictate. Cranial computed tomography (CT) has yielded normal findings in drowning victims with a GCS score as low as 4.
If CT is performed, any abnormality detected within 2 to 3 days of injury is a strong predictor of a poor neurologic outcome.39 Magnetic resonance imaging can be beneficial when performed more than 24 hours after resuscitation, preferably within a 4- to 7-day window.20 Lung ultrasound has been used as a bedside tool to monitor progression of pulmonary edema, and could serve the same purpose in drowning recovery.40
Anticipate respiratory complications. Since only a small amount of water is usually aspirated during a drowning event, the salinity of the aspirate is unlikely to cause significant disruption in hemodynamic or electrolyte balance.17,20 However, even a small amount of aspirated water, particularly fresh water, can disrupt gas exchange by washing out surfactant. This can rapidly precipitate ARDS. Not surprisingly, the use of exogenous surfactant has been studied in limited case reports and has had positive results.41-43 However, large trials have not yet been conducted, mostly because of the significant cost associated with surfactant therapy.
Antibiotics are rarely indicated prophylactically. Pneumonia after a drowning event is potentially fatal. It is more common in patients who have been intubated, and is therefore thought to be a hospital-acquired infection rather than a direct result of the drowning event.
Frequently, pneumonia after drowning is caused by pathogens native to the upper airway, when a victim is unable to protect his or her upper airway.44 In these cases, start broad spectrum antibiotics, with particular concern for organisms of the upper oropharynx. Also take into consideration species native to the body of water in which the victim was immersed.44
Routine prophylaxis with antibiotics, although common, is not recommended. Exceptions may be victims of drowning in known contaminated water or victims with high volumes of water aspiration.25 Some experts recommend blood cultures for victims who have aspirated, regardless of the presence or absence of infection.24 However, this recommendation seems to be based on opinion.
CORRESPONDENCE
Sean C. Engel, MD, 6600 Excelsior Boulevard Suite 100, St. Louis Park, MN 55426; [email protected]
1. World Health Organization. Drowning. World Health Organization Web site. Available at: http://www.who.int/mediacentre/factsheets/fs347/en/. Accessed December 28, 2014.
2. Centers for Disease Control and Prevention (CDC). Drowning—United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61:344-447.
3. Driscoll TR, Harrison JE, Steenkamp M. Alcohol and drowning in Australia. Inj Control Saf Promot. 2004;11:175-181.
4. Szpilman D. Near-drowning and drowning classification: a proposal to stratify mortality based on the analysis of 1,831 cases. Chest. 1997;112:660-665.
5. Hudson D, Ekman R, Svanström L. Survival of immersions during recreational boating events in Alaska, 1999-2004. Accid Anal Prev. 2007;39:437-443.
6. International Life Saving Federation. Drowning Report. International Life Saving Federation Web site. Available at: http://www.ilsf.org/sites/ilsf.org/files/filefield/drowningcongress.doc. Accessed December 28, 2014.
7. Brooks CJ, Howard KA, Neifer SK. How much did cold shock and swimming failure contribute to drowning deaths in the fishing industry in British Columbia 1976-2002? Occup Med (Lond). 2005;55:459-462.
8. Golden FS, Tipton MJ, Scott RC. Immersion, near-drowning and drowning. Br J Anaesth. 1997;79:214-225.
9. Bierens JJ, Knape JT, Gelissen HP. Drowning. Curr Opin Crit Care. 2002;8:578-586.
10. Ducharme MB, Lounsbury DS. Self-rescue swimming in cold water: the latest advice. Appl Physiol Nutr Metab. 2007;32:799-807.
11. Shattock MJ, Tipton MJ. ‘Autonomic conflict’: a different way to die during cold water immersion? J Physiol. 2012;590(pt 14):3219-3230.
12. Weiss J; American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention. Prevention of drowning. Pediatrics. 2010;126:e253-e262.
13.Yang L, Nong QQ, Li CL, et al. Risk factors for childhood drowning in rural regions of a developing country: a case-control study. Inj Prev. 2007;13:178-182.
14. Brenner RA, Taneja GS, Haynie DL, et al. The association between swimming lessons and drowning in childhood: a case-control study. Arch Pediatr Adolesc Med. 2009;163:203-210.
15. Rahman A, Rahman F, Hossain J, et al. Survival swimming - effectiveness of SwimSafe in preventing drowning in mid and late childhood. Abstract presented at: World Conference on Drowning Prevention; May 10-13, 2011; Danang, Vietnam.
16. Linnan M, Rahman A, Scarr J, et al. Child drowning: Evidence for a newly recognized cause of child mortality in low and middle income countries in Asia. Florence, Italy: UNICEF Office of Research. UNICEF Web site. Available at: www.unicef-irc.org/publications/pdf/drowning.pdf. Accessed December 28, 2014.
17. Salomez F, Vincent JL. Drowning: a review of epidemiology, pathophysiology, treatment and prevention. Resuscitation. 2004;63:261-268.
18. Venema AM, Groothoff JW, Bierens JJ. The role of bystanders during rescue and resuscitation of drowning victims. Resuscitation. 2010;81:434-439.
19. Pepe PE, Wigginton JG, Mann DM, et al. Prospective, decade-long, population-based study of pediatric drowning related incidents. Acad Emerg Med. 2002;9:516-517.
20. Topjian AA, Berg RA, Bierens JJ, et al. Brain resuscitation in the drowning victim. Neurocrit Care. 2012;17:441-467.
21. Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 suppl 3):S829-S861.
22. Ibsen LM, Koch T. Submersion and asphyxial injury. Crit Care Med. 2002;30(11 suppl):S402-S408.
23. Schilling UM, Bortolin M. Drowning. Minerva Anethesiol. 2012;78:69-77.
24. Harries M. Near drowning. BMJ. 2003;327:1336-1338.
25. Gregorakos L, Markou N, Psalida V, et al. Near-drowning: clinical course of lung injury in adults. Lung. 2009;187:93-97.
26. Eich C, Bräuer A, Timmermann A, et al. Outcome of 12 drowned children with attempted resuscitation on cardiopulmonary bypass: an analysis of variables based on the “Utstein Style for Drowning”. Resuscitation. 2007;75:42-52.
27. Wollenek G, Honarwar N, Golej J, et al. Cold water submersion and cardiac arrest in treatment of severe hypothermia with cardiopulmonary bypass. Resuscitation. 2002;52:255-263.
28. Letsou GV, Kopf GS, Elefteriades JA, et al. Is cardiopulmonary bypass effective for treatment of hypothermic arrest due to drowning or exposure? Arch Surg. 1992;127:525-528.
29. Lund FK, Torgersen JG, Flaatten HK. Heart rate monitored hypothermia and drowning in a 48-year-old man. survival without sequelae: a case report. Cases J. 2009;2:6204.
30. Ballesteros MA, Gutiérrez-Cuadra M, Muñoz P, et al. Prognostic factors and outcome after drowning in an adult population. Acta Anaesthesiol Scand. 2009;53:935-940.
31. Nichter MA, Everett PB. Childhood near-drowning: is cardiopulmonary resuscitation always indicated? Crit Care Med. 1989;17:993-995.
32. Schaller MD, Fischer AP, Perret CH. Hyperkalemia. A prognostic factor during acute severe hypothermia. JAMA. 1990;264:1842-1845.
33. O’Connor MF, Ovassapian A. Airway management. In: Hall JB, Schmidt GA, Wood LD, eds. Principles of Critical Care. 3rd ed. New York, NY: McGraw-Hill; 2005.
34. Montenij LJ, de Vries W, Schwarte L, et al. Feasibility of pulse oximetry in the initial prehospital management of victims of drowning: a preliminary study. Resuscitation. 2011;82:1235-1238.
35. Brown DJ, Brugger H, Boyd J, et al. Accidental hypothermia. N Engl J Med. 2012;367:1930-1938.
36. Durrer B, Brugger H, Syme D; International Commission for Mountain Emergency Medicine. The medical on-site treatment of hypothermia: ICAR-MEDCOM recommendation. High Alt Med Biol. 2003;4:99-103.
37. Coskun KO, Popov AF, Schmitto JD, et al. Extracorporeal circulation for rewarming in drowning and near-drowning pediatric patients. Artif Organs. 2010;34:1026-1030.
38. Arrich J, Holzer M, Havel C, et al. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation. Cochrane Database Syst Rev. 2012;9:CD004128.
39. Rafaat KT, Spear RM, Kuelbs C, et al. Cranial computed tomographic findings in a large group of children with drowning: diagnostic, prognostic, and forensic implications. Pediatr Crit Care Med. 2008;9:567-572.
40. Laursen CB, Davidsen JR, Madsen PH. Utility of lung ultrasound in near-drowning victims. BMJ Case Rep. 2012;2012.
41. Ugras M, Guraksin O, Sen TA, et al. Surfactant replacement therapy in a pediatric near-drowning case in manure. Pediatr Emerg Care. 2012;28:913-914.
42. Kapur N, Slater A, McEniery J, et al. Therapeutic bronchoscopy in a child with sand aspiration and respiratory failure from near drowning—case report and literature review. Pediatr Pulmonol. 2009;44:1043-1047.
43. Staudinger T, Bankier A, Strohmaier W, et al. Exogenous surfactant therapy in a patient with adult respiratory distress syndrome after near drowning. Resuscitation. 1997;35:179-182.
44. Tadié JM, Heming N, Serve E, et al. Drowning associated pneumonia: a descriptive cohort. Resuscitation. 2012;83:399-401.
› Recommend swimming lessons for all children ages 4 and older. C
› Consider antibiotics after a drowning event only if the water is known to be contaminated or the victim has aspirated a large volume of water. C
› Monitor asymptomatic patients for at least 4 hours after a drowning event. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A young mother in your practice wants her toddler to begin swimming lessons because her family loves water activities. How would you advise her? In fielding an urgent call about a drowning incident, what priorities would you urge regarding resuscitation at the scene? For a stabilized patient following a drowning episode, when might antibiotics be indicated? This article covers these issues as well as follow-up matters such as assisted ventilation and tiered hypothermia intervention.
Drowning likely occurs more often than is reported
Worldwide, drowning accounts for more than 388,000 deaths annually and is the third leading cause of unintentional injury death. Low- and middle-income countries represent 96% of the yearly total.1 As reported in the United States, nearly 6000 individuals are hospitalized and nearly 4000 die from drowning events annually.2 But these figures likely underestimate the true rate, as many drowning fatalities are officially attributed to floods, boating accidents, or other associated events. Nonfatal drownings often go unreported.
Children under the age of 5 years have the highest drowning mortality worldwide, and drowning is the leading cause of unintentional injury death for this age group in many countries, including the United States.1,2 Men are nearly 4 times as likely to die from drowning than women.2 Predictably, in the United States most drowning happens on the weekend and during summer months. More than half of drownings in children younger than 4 years occur in swimming pools; with increasing age, drowning is more likely to occur in natural bodies of water.2 With adults in higher income countries, alcohol is a significant contributor to drowning events during recreational activities.3-5
Much effort has been made in recent years to standardize the nomenclature and treatment of drowning episodes. The International World Congress on Drowning met in the Netherlands in 2002, and established the definition of drowning as “the process of experiencing respiratory impairment from submersion/immersion in liquid.”6 Submersion refers to the complete submergence of the victim under the water, while immersion implies that the victim’s airway remains above the water.
The Congress recommended that terms such as “wet-drowning,” “dry-drowning,” and “near-drowning” be discontinued in favor of the outcome classifications “death,” “no morbidity,” and “morbidity.” The “morbidity” subgroup was further characterized as “moderately disabled,” “severely disabled,” “vegetative state/coma,” and “brain death.” This meeting established guidelines on the treatment of drowning victims in addition to outlining points for future research.6
Physiologic chain of events in drowning
An unexpected immersion in water, particularly cold water, causes a reflexive inspiratory gasp, and some degree of aspiration occurs in most, if not all, cases of drowning. Aspiration further impairs victims’ ability to hold their breath or breathe normally.5,7,8 It decreases lung compliance due to surfactant washout or intrapulmonary shunting and thereby leads to hypoxia. Aspiration-induced severe laryngospasm can also lead to hypoxia. Pulmonary edema and acute respiratory distress syndrome (ARDS) can follow.
The cardiovascular effects of drowning mirror those seen in hypoxia. Initially, apnea leads to decreased oxygen saturation and precipitates tachycardia and hypertension. Bradycardia and hypotension follow and blood is shunted to vital organs, such as the brain, heart, and lungs.9 This phenomenon is accelerated in cold water and leads to “swimming failure,” the impaired ability of the victim to swim because of decreased perfusion of the extremities.5,7,8,10
“Autonomic conflict” has been proposed as an additional mechanism for morbidity and mortality from drowning episodes. Breath holding and immersion in cold water each can induce cardiac arrhythmias. When combined, these events may increase the risk of an arrhythmogenic state secondary to opposing chronotropic effects: the diving reflex (bradycardia via parasympathetic activation), and the cold shock response (tachycardia via sympathetic activation). This is thought to be an underreported cause of death in drowning, as arrhythmias are undetectable during autopsy.8,11
Drowning prevention
The American Academy of Pediatrics (AAP) recommends swimming lessons for most children ages 4 years and older.12 Previously, swimming lessons were not recommended for children ages 1 to 4 because evidence of benefit was lacking, and there was some concern that it might reduce children’s caution around water and reduce parents’ perceived level of need for supervision. Although data are still conflicting, some reports have since shown benefit in early swimming lessons for
toddlers.13,14
As of 2010, the AAP acknowledges that training may be beneficial for children in this age group, but cautions that not all children will be ready for swimming by this age.12 Infant water safety programs for children under the age of 1 are not recommended because evidence of benefit is lacking.12
Evidence is growing to support teaching basic water survival skills in low- to middle-income countries where water sources are abundant, particularly in Southeast Asia. Specifically, the SwimSafe survival swimming program has yielded impressive results in Bangladesh.15 This program targets children starting at age 5, and involves 20 lessons teaching basic water survival and rescue skills.
Results have shown a 93% reduction in drowning rates for children enrolled in the program, compared with those not enrolled.15 Subsequent analyses have proposed that swimming lessons for children in these parts of the world would be as cost effective as current attempts to prevent diarrheal and respiratory diseases in the same areas.16
Additional preventive measures that are effective in the United States include 4-sided pool fencing, use of personal flotation devices, and bystander cardiopulmonary
resuscitation (CPR).2,5,17
On-scene evaluation and treatment
Drowning victims can appear mottled and have minimal or no peripheral pulses despite a heartbeat. Rescuers may assume the victim is dead when, in fact, there is cardiac function. Because initial assessment in this situation is difficult, CPR should begin, if possible, the moment the victim is out of the water. Successful on-scene resuscitation is the surest predictor of survival.9,18 In fact, delay of CPR until the arrival of emergency personnel lessens the likelihood of survival.19
CPR applied to drowning. For cardiogenic cardiac arrest, chest compressions alone may be better than compressions with rescue breathing. For victims of drowning, though, coordinated compressions and rescue breathing are recommended.20 The
2010 revision of the American Heart Association Guidelines for CPR and Emergency Cardiovascular Care emphasize “compression first” for CPR in cases of cardiogenic cardiac arrest, but continue to support the traditional Airway-Breathing-Chest Compressions sequence for drowning victims in its Special Situations section.21
Ventricular fibrillation (VF) is rare after submersion injury. An external defibrillator should be used when available, but it is unlikely to play a significant role in initial resuscitation.9
Don’t attempt to remove water from the victim’s mouth before resuscitation. The volume of fluid in the oral cavity is usually insignificant, and trying to remove it by abdominal thrusts or Heimlich maneuver will delay CPR and may injure the patient.21
Cervical spine injury is uncommon in drowning episodes, making cervical spine immobilization unnecessary unless the mechanism of injury is known or if there are clinical signs suggesting such injury. Needless cervical spine immobilization can interfere with adequate ventilation.22,23 However, concern for head or cervical spine injury is warranted when recovering an unconscious victim from shallow water, where such injuries are more likely to result from falling or diving into the water.24
Administer oxygen supplementation when available to all spontaneously breathing individuals. Individuals who respond well to initial resuscitation and who don’t require intubation tend to have a very good prognosis overall.25
Total time of submersion and the temperature of the water have bearing on the likelihood of survival. Only in rare cases have victims survived submersion lasting longer than 30 minutes. Ten minutes generally is considered the “point of no return.”9,26 This is consistent with data suggesting 10 minutes of hypoxic insult causes irreversible neurologic damage, with each additional minute rapidly leading to coma.20 However, to complicate matters, unlike cardiac arrest victims, drowning victims can lose cerebral blood flow slowly after respiratory impairment, which makes duration of submersion a potentially unreliable predictor of neurologic outcome.20,26
Does hypothermia have a protective effect? Hypothermia can occur in water 85°F (30°C) or cooler.10 It has been hypothesized that resuscitation can be achieved after longer periods of submersion in cold water. However, the considerable debate on this topic has been based on little more than case reports.
For hypothermia to have a protective effect on neurologic function, cooling must take place rapidly and, ideally, before any hypoxic insult. The water would have to be exceptionally cold, likely less than 50°F (10°C).27 The greater surface-to-volume ratio in children enables more rapid cooling and quicker onset of hypothermia, which may explain why they seem to have better neurologic outcomes than adults after prolonged submersion.28
Hypothermia can also be protective if the victim is breathing when cooling begins, such as while floating or swimming in cold water before drowning.29 This was the likely scenario in a reported case of a Norwegian kayaker who called for help after capsizing in 38°F (3.3°C) seawater. Despite having been in cardiac arrest for over 3 hours, the individual experienced a spontaneous return of circulation and was discharged after 32 days with no neurologic deficits.29
Correcting hypothermia after rescue. Conscious patients with no cardiovascular or respiratory compromise should have wet clothing removed at the scene in exchange for blankets, towels, or warm dry clothing. Advise rescuers to attempt no further rewarming at the scene. With unconscious patients, take only simple measures to prevent further heat loss, and focus on transport and resuscitative efforts.24
Hospital management
Attempts have been made to create a prognostic or predictive scoring system for drowning victims presenting to the emergency department. Factors thought to have bearing on mortality include duration of submersion, victim’s age, Glasgow Coma Scale (GCS) score, pupillary reactivity, and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score.23,30,31 Other measurements, such as core temperature, blood pH, and response to painful stimuli, correlate poorly with mortality.31 Hyperkalemia is repeatedly mentioned as a predictor of a poor neurologic outcome, as it is thought to indicate hypoxia before the onset of cooling.8,26,32 The best predictor of a good outcome is consciousness at the time of arrival at the emergency department.4
Continued ventilation assistance is critical. As with prehospital resuscitation efforts, ventilation is critical to in-hospital management. For patients who are breathing spontaneously, continuous positive airway pressure or bi-level positive airway pressure can reduce hypoxia in pulmonary edema. Standard indications of the need for intubation include decreased level of consciousness or concern for ability to protect the airway, hypoxia despite a high fraction of inspired oxygen (FiO2), or persistent hypercapnia even with adequate noninvasive ventilatory support.33
Victims may swallow large amounts of liquid during drowning; for intubated patients, advise orogastric tube placement to prevent aspiration of gastric contents. The reliability of pulse oximetry has been called into question in this setting and may be less accurate for victims who are hypothermic or who have been submerged in cold water.23,34
Tiered intervention for hypothermia. In the hospital setting, passive rewarming is indicated for individuals with a body core temperature of 89.6°F to 95°F (32°C-35°C). Remove wet clothing; cover the victim with warm, dry towels or blankets; and give warm oral fluids and urge movement.
Individuals with core temperatures between 82.4°F to 89.6°F (28°C-32°C) require active external rewarming by applying heat directly to the skin via hot packs, warm blankets, and insulation. These patients should remain in a horizontal position with little movement, if possible, to avoid cold peripheral blood rapidly shifting to the core and precipitating an arrhythmia. Warmed intravenous fluids are appropriate as well.
With a core temperature less than 82.4°F (28°C), aggressive rewarming with extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass (CPB) may be warranted as this individual will likely have unstable or absent vital signs (TABLE).35,36 Some authorities advise that drowning victims with severe hypothermia and cardiac arrest should be resuscitated at facilities with CPB capability.27,28,37
Inducing hypothermia therapeutically is still unproven. Although not tested specifically on drowning victims, therapeutic hypothermia would seem to have theoretical benefit for their resuscitation. In cardiogenic cardiac arrest, good evidence exists for improved neurologic outcomes with therapeutic hypothermia,38 and this benefit might extend to drowning victims given their similar neurologic injury. No specific pharmacologic therapies have shown benefit in preventing loss of cerebral function.9
Monitor for clinical worsening. The concept of “secondary drowning,” a term now abandoned, referred to the phenomenon of clinical worsening hours after the initial drowning episode and resuscitation. This occurrence is now thought to be due to laryngospasm or to the progressive development of pulmonary edema from the aspiration of small amounts of water. Evidence supports monitoring asymptomatic patients; however, the period of suggested monitoring varies between 4 and 24 hours after the incident.8,22,24
Imaging, if delayed, may be useful. Imaging immediately after a drowning episode is an unreliable predictor of outcome and should be sought only if trauma or symptoms dictate. Cranial computed tomography (CT) has yielded normal findings in drowning victims with a GCS score as low as 4.
If CT is performed, any abnormality detected within 2 to 3 days of injury is a strong predictor of a poor neurologic outcome.39 Magnetic resonance imaging can be beneficial when performed more than 24 hours after resuscitation, preferably within a 4- to 7-day window.20 Lung ultrasound has been used as a bedside tool to monitor progression of pulmonary edema, and could serve the same purpose in drowning recovery.40
Anticipate respiratory complications. Since only a small amount of water is usually aspirated during a drowning event, the salinity of the aspirate is unlikely to cause significant disruption in hemodynamic or electrolyte balance.17,20 However, even a small amount of aspirated water, particularly fresh water, can disrupt gas exchange by washing out surfactant. This can rapidly precipitate ARDS. Not surprisingly, the use of exogenous surfactant has been studied in limited case reports and has had positive results.41-43 However, large trials have not yet been conducted, mostly because of the significant cost associated with surfactant therapy.
Antibiotics are rarely indicated prophylactically. Pneumonia after a drowning event is potentially fatal. It is more common in patients who have been intubated, and is therefore thought to be a hospital-acquired infection rather than a direct result of the drowning event.
Frequently, pneumonia after drowning is caused by pathogens native to the upper airway, when a victim is unable to protect his or her upper airway.44 In these cases, start broad spectrum antibiotics, with particular concern for organisms of the upper oropharynx. Also take into consideration species native to the body of water in which the victim was immersed.44
Routine prophylaxis with antibiotics, although common, is not recommended. Exceptions may be victims of drowning in known contaminated water or victims with high volumes of water aspiration.25 Some experts recommend blood cultures for victims who have aspirated, regardless of the presence or absence of infection.24 However, this recommendation seems to be based on opinion.
CORRESPONDENCE
Sean C. Engel, MD, 6600 Excelsior Boulevard Suite 100, St. Louis Park, MN 55426; [email protected]
› Recommend swimming lessons for all children ages 4 and older. C
› Consider antibiotics after a drowning event only if the water is known to be contaminated or the victim has aspirated a large volume of water. C
› Monitor asymptomatic patients for at least 4 hours after a drowning event. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
A young mother in your practice wants her toddler to begin swimming lessons because her family loves water activities. How would you advise her? In fielding an urgent call about a drowning incident, what priorities would you urge regarding resuscitation at the scene? For a stabilized patient following a drowning episode, when might antibiotics be indicated? This article covers these issues as well as follow-up matters such as assisted ventilation and tiered hypothermia intervention.
Drowning likely occurs more often than is reported
Worldwide, drowning accounts for more than 388,000 deaths annually and is the third leading cause of unintentional injury death. Low- and middle-income countries represent 96% of the yearly total.1 As reported in the United States, nearly 6000 individuals are hospitalized and nearly 4000 die from drowning events annually.2 But these figures likely underestimate the true rate, as many drowning fatalities are officially attributed to floods, boating accidents, or other associated events. Nonfatal drownings often go unreported.
Children under the age of 5 years have the highest drowning mortality worldwide, and drowning is the leading cause of unintentional injury death for this age group in many countries, including the United States.1,2 Men are nearly 4 times as likely to die from drowning than women.2 Predictably, in the United States most drowning happens on the weekend and during summer months. More than half of drownings in children younger than 4 years occur in swimming pools; with increasing age, drowning is more likely to occur in natural bodies of water.2 With adults in higher income countries, alcohol is a significant contributor to drowning events during recreational activities.3-5
Much effort has been made in recent years to standardize the nomenclature and treatment of drowning episodes. The International World Congress on Drowning met in the Netherlands in 2002, and established the definition of drowning as “the process of experiencing respiratory impairment from submersion/immersion in liquid.”6 Submersion refers to the complete submergence of the victim under the water, while immersion implies that the victim’s airway remains above the water.
The Congress recommended that terms such as “wet-drowning,” “dry-drowning,” and “near-drowning” be discontinued in favor of the outcome classifications “death,” “no morbidity,” and “morbidity.” The “morbidity” subgroup was further characterized as “moderately disabled,” “severely disabled,” “vegetative state/coma,” and “brain death.” This meeting established guidelines on the treatment of drowning victims in addition to outlining points for future research.6
Physiologic chain of events in drowning
An unexpected immersion in water, particularly cold water, causes a reflexive inspiratory gasp, and some degree of aspiration occurs in most, if not all, cases of drowning. Aspiration further impairs victims’ ability to hold their breath or breathe normally.5,7,8 It decreases lung compliance due to surfactant washout or intrapulmonary shunting and thereby leads to hypoxia. Aspiration-induced severe laryngospasm can also lead to hypoxia. Pulmonary edema and acute respiratory distress syndrome (ARDS) can follow.
The cardiovascular effects of drowning mirror those seen in hypoxia. Initially, apnea leads to decreased oxygen saturation and precipitates tachycardia and hypertension. Bradycardia and hypotension follow and blood is shunted to vital organs, such as the brain, heart, and lungs.9 This phenomenon is accelerated in cold water and leads to “swimming failure,” the impaired ability of the victim to swim because of decreased perfusion of the extremities.5,7,8,10
“Autonomic conflict” has been proposed as an additional mechanism for morbidity and mortality from drowning episodes. Breath holding and immersion in cold water each can induce cardiac arrhythmias. When combined, these events may increase the risk of an arrhythmogenic state secondary to opposing chronotropic effects: the diving reflex (bradycardia via parasympathetic activation), and the cold shock response (tachycardia via sympathetic activation). This is thought to be an underreported cause of death in drowning, as arrhythmias are undetectable during autopsy.8,11
Drowning prevention
The American Academy of Pediatrics (AAP) recommends swimming lessons for most children ages 4 years and older.12 Previously, swimming lessons were not recommended for children ages 1 to 4 because evidence of benefit was lacking, and there was some concern that it might reduce children’s caution around water and reduce parents’ perceived level of need for supervision. Although data are still conflicting, some reports have since shown benefit in early swimming lessons for
toddlers.13,14
As of 2010, the AAP acknowledges that training may be beneficial for children in this age group, but cautions that not all children will be ready for swimming by this age.12 Infant water safety programs for children under the age of 1 are not recommended because evidence of benefit is lacking.12
Evidence is growing to support teaching basic water survival skills in low- to middle-income countries where water sources are abundant, particularly in Southeast Asia. Specifically, the SwimSafe survival swimming program has yielded impressive results in Bangladesh.15 This program targets children starting at age 5, and involves 20 lessons teaching basic water survival and rescue skills.
Results have shown a 93% reduction in drowning rates for children enrolled in the program, compared with those not enrolled.15 Subsequent analyses have proposed that swimming lessons for children in these parts of the world would be as cost effective as current attempts to prevent diarrheal and respiratory diseases in the same areas.16
Additional preventive measures that are effective in the United States include 4-sided pool fencing, use of personal flotation devices, and bystander cardiopulmonary
resuscitation (CPR).2,5,17
On-scene evaluation and treatment
Drowning victims can appear mottled and have minimal or no peripheral pulses despite a heartbeat. Rescuers may assume the victim is dead when, in fact, there is cardiac function. Because initial assessment in this situation is difficult, CPR should begin, if possible, the moment the victim is out of the water. Successful on-scene resuscitation is the surest predictor of survival.9,18 In fact, delay of CPR until the arrival of emergency personnel lessens the likelihood of survival.19
CPR applied to drowning. For cardiogenic cardiac arrest, chest compressions alone may be better than compressions with rescue breathing. For victims of drowning, though, coordinated compressions and rescue breathing are recommended.20 The
2010 revision of the American Heart Association Guidelines for CPR and Emergency Cardiovascular Care emphasize “compression first” for CPR in cases of cardiogenic cardiac arrest, but continue to support the traditional Airway-Breathing-Chest Compressions sequence for drowning victims in its Special Situations section.21
Ventricular fibrillation (VF) is rare after submersion injury. An external defibrillator should be used when available, but it is unlikely to play a significant role in initial resuscitation.9
Don’t attempt to remove water from the victim’s mouth before resuscitation. The volume of fluid in the oral cavity is usually insignificant, and trying to remove it by abdominal thrusts or Heimlich maneuver will delay CPR and may injure the patient.21
Cervical spine injury is uncommon in drowning episodes, making cervical spine immobilization unnecessary unless the mechanism of injury is known or if there are clinical signs suggesting such injury. Needless cervical spine immobilization can interfere with adequate ventilation.22,23 However, concern for head or cervical spine injury is warranted when recovering an unconscious victim from shallow water, where such injuries are more likely to result from falling or diving into the water.24
Administer oxygen supplementation when available to all spontaneously breathing individuals. Individuals who respond well to initial resuscitation and who don’t require intubation tend to have a very good prognosis overall.25
Total time of submersion and the temperature of the water have bearing on the likelihood of survival. Only in rare cases have victims survived submersion lasting longer than 30 minutes. Ten minutes generally is considered the “point of no return.”9,26 This is consistent with data suggesting 10 minutes of hypoxic insult causes irreversible neurologic damage, with each additional minute rapidly leading to coma.20 However, to complicate matters, unlike cardiac arrest victims, drowning victims can lose cerebral blood flow slowly after respiratory impairment, which makes duration of submersion a potentially unreliable predictor of neurologic outcome.20,26
Does hypothermia have a protective effect? Hypothermia can occur in water 85°F (30°C) or cooler.10 It has been hypothesized that resuscitation can be achieved after longer periods of submersion in cold water. However, the considerable debate on this topic has been based on little more than case reports.
For hypothermia to have a protective effect on neurologic function, cooling must take place rapidly and, ideally, before any hypoxic insult. The water would have to be exceptionally cold, likely less than 50°F (10°C).27 The greater surface-to-volume ratio in children enables more rapid cooling and quicker onset of hypothermia, which may explain why they seem to have better neurologic outcomes than adults after prolonged submersion.28
Hypothermia can also be protective if the victim is breathing when cooling begins, such as while floating or swimming in cold water before drowning.29 This was the likely scenario in a reported case of a Norwegian kayaker who called for help after capsizing in 38°F (3.3°C) seawater. Despite having been in cardiac arrest for over 3 hours, the individual experienced a spontaneous return of circulation and was discharged after 32 days with no neurologic deficits.29
Correcting hypothermia after rescue. Conscious patients with no cardiovascular or respiratory compromise should have wet clothing removed at the scene in exchange for blankets, towels, or warm dry clothing. Advise rescuers to attempt no further rewarming at the scene. With unconscious patients, take only simple measures to prevent further heat loss, and focus on transport and resuscitative efforts.24
Hospital management
Attempts have been made to create a prognostic or predictive scoring system for drowning victims presenting to the emergency department. Factors thought to have bearing on mortality include duration of submersion, victim’s age, Glasgow Coma Scale (GCS) score, pupillary reactivity, and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score.23,30,31 Other measurements, such as core temperature, blood pH, and response to painful stimuli, correlate poorly with mortality.31 Hyperkalemia is repeatedly mentioned as a predictor of a poor neurologic outcome, as it is thought to indicate hypoxia before the onset of cooling.8,26,32 The best predictor of a good outcome is consciousness at the time of arrival at the emergency department.4
Continued ventilation assistance is critical. As with prehospital resuscitation efforts, ventilation is critical to in-hospital management. For patients who are breathing spontaneously, continuous positive airway pressure or bi-level positive airway pressure can reduce hypoxia in pulmonary edema. Standard indications of the need for intubation include decreased level of consciousness or concern for ability to protect the airway, hypoxia despite a high fraction of inspired oxygen (FiO2), or persistent hypercapnia even with adequate noninvasive ventilatory support.33
Victims may swallow large amounts of liquid during drowning; for intubated patients, advise orogastric tube placement to prevent aspiration of gastric contents. The reliability of pulse oximetry has been called into question in this setting and may be less accurate for victims who are hypothermic or who have been submerged in cold water.23,34
Tiered intervention for hypothermia. In the hospital setting, passive rewarming is indicated for individuals with a body core temperature of 89.6°F to 95°F (32°C-35°C). Remove wet clothing; cover the victim with warm, dry towels or blankets; and give warm oral fluids and urge movement.
Individuals with core temperatures between 82.4°F to 89.6°F (28°C-32°C) require active external rewarming by applying heat directly to the skin via hot packs, warm blankets, and insulation. These patients should remain in a horizontal position with little movement, if possible, to avoid cold peripheral blood rapidly shifting to the core and precipitating an arrhythmia. Warmed intravenous fluids are appropriate as well.
With a core temperature less than 82.4°F (28°C), aggressive rewarming with extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass (CPB) may be warranted as this individual will likely have unstable or absent vital signs (TABLE).35,36 Some authorities advise that drowning victims with severe hypothermia and cardiac arrest should be resuscitated at facilities with CPB capability.27,28,37
Inducing hypothermia therapeutically is still unproven. Although not tested specifically on drowning victims, therapeutic hypothermia would seem to have theoretical benefit for their resuscitation. In cardiogenic cardiac arrest, good evidence exists for improved neurologic outcomes with therapeutic hypothermia,38 and this benefit might extend to drowning victims given their similar neurologic injury. No specific pharmacologic therapies have shown benefit in preventing loss of cerebral function.9
Monitor for clinical worsening. The concept of “secondary drowning,” a term now abandoned, referred to the phenomenon of clinical worsening hours after the initial drowning episode and resuscitation. This occurrence is now thought to be due to laryngospasm or to the progressive development of pulmonary edema from the aspiration of small amounts of water. Evidence supports monitoring asymptomatic patients; however, the period of suggested monitoring varies between 4 and 24 hours after the incident.8,22,24
Imaging, if delayed, may be useful. Imaging immediately after a drowning episode is an unreliable predictor of outcome and should be sought only if trauma or symptoms dictate. Cranial computed tomography (CT) has yielded normal findings in drowning victims with a GCS score as low as 4.
If CT is performed, any abnormality detected within 2 to 3 days of injury is a strong predictor of a poor neurologic outcome.39 Magnetic resonance imaging can be beneficial when performed more than 24 hours after resuscitation, preferably within a 4- to 7-day window.20 Lung ultrasound has been used as a bedside tool to monitor progression of pulmonary edema, and could serve the same purpose in drowning recovery.40
Anticipate respiratory complications. Since only a small amount of water is usually aspirated during a drowning event, the salinity of the aspirate is unlikely to cause significant disruption in hemodynamic or electrolyte balance.17,20 However, even a small amount of aspirated water, particularly fresh water, can disrupt gas exchange by washing out surfactant. This can rapidly precipitate ARDS. Not surprisingly, the use of exogenous surfactant has been studied in limited case reports and has had positive results.41-43 However, large trials have not yet been conducted, mostly because of the significant cost associated with surfactant therapy.
Antibiotics are rarely indicated prophylactically. Pneumonia after a drowning event is potentially fatal. It is more common in patients who have been intubated, and is therefore thought to be a hospital-acquired infection rather than a direct result of the drowning event.
Frequently, pneumonia after drowning is caused by pathogens native to the upper airway, when a victim is unable to protect his or her upper airway.44 In these cases, start broad spectrum antibiotics, with particular concern for organisms of the upper oropharynx. Also take into consideration species native to the body of water in which the victim was immersed.44
Routine prophylaxis with antibiotics, although common, is not recommended. Exceptions may be victims of drowning in known contaminated water or victims with high volumes of water aspiration.25 Some experts recommend blood cultures for victims who have aspirated, regardless of the presence or absence of infection.24 However, this recommendation seems to be based on opinion.
CORRESPONDENCE
Sean C. Engel, MD, 6600 Excelsior Boulevard Suite 100, St. Louis Park, MN 55426; [email protected]
1. World Health Organization. Drowning. World Health Organization Web site. Available at: http://www.who.int/mediacentre/factsheets/fs347/en/. Accessed December 28, 2014.
2. Centers for Disease Control and Prevention (CDC). Drowning—United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61:344-447.
3. Driscoll TR, Harrison JE, Steenkamp M. Alcohol and drowning in Australia. Inj Control Saf Promot. 2004;11:175-181.
4. Szpilman D. Near-drowning and drowning classification: a proposal to stratify mortality based on the analysis of 1,831 cases. Chest. 1997;112:660-665.
5. Hudson D, Ekman R, Svanström L. Survival of immersions during recreational boating events in Alaska, 1999-2004. Accid Anal Prev. 2007;39:437-443.
6. International Life Saving Federation. Drowning Report. International Life Saving Federation Web site. Available at: http://www.ilsf.org/sites/ilsf.org/files/filefield/drowningcongress.doc. Accessed December 28, 2014.
7. Brooks CJ, Howard KA, Neifer SK. How much did cold shock and swimming failure contribute to drowning deaths in the fishing industry in British Columbia 1976-2002? Occup Med (Lond). 2005;55:459-462.
8. Golden FS, Tipton MJ, Scott RC. Immersion, near-drowning and drowning. Br J Anaesth. 1997;79:214-225.
9. Bierens JJ, Knape JT, Gelissen HP. Drowning. Curr Opin Crit Care. 2002;8:578-586.
10. Ducharme MB, Lounsbury DS. Self-rescue swimming in cold water: the latest advice. Appl Physiol Nutr Metab. 2007;32:799-807.
11. Shattock MJ, Tipton MJ. ‘Autonomic conflict’: a different way to die during cold water immersion? J Physiol. 2012;590(pt 14):3219-3230.
12. Weiss J; American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention. Prevention of drowning. Pediatrics. 2010;126:e253-e262.
13.Yang L, Nong QQ, Li CL, et al. Risk factors for childhood drowning in rural regions of a developing country: a case-control study. Inj Prev. 2007;13:178-182.
14. Brenner RA, Taneja GS, Haynie DL, et al. The association between swimming lessons and drowning in childhood: a case-control study. Arch Pediatr Adolesc Med. 2009;163:203-210.
15. Rahman A, Rahman F, Hossain J, et al. Survival swimming - effectiveness of SwimSafe in preventing drowning in mid and late childhood. Abstract presented at: World Conference on Drowning Prevention; May 10-13, 2011; Danang, Vietnam.
16. Linnan M, Rahman A, Scarr J, et al. Child drowning: Evidence for a newly recognized cause of child mortality in low and middle income countries in Asia. Florence, Italy: UNICEF Office of Research. UNICEF Web site. Available at: www.unicef-irc.org/publications/pdf/drowning.pdf. Accessed December 28, 2014.
17. Salomez F, Vincent JL. Drowning: a review of epidemiology, pathophysiology, treatment and prevention. Resuscitation. 2004;63:261-268.
18. Venema AM, Groothoff JW, Bierens JJ. The role of bystanders during rescue and resuscitation of drowning victims. Resuscitation. 2010;81:434-439.
19. Pepe PE, Wigginton JG, Mann DM, et al. Prospective, decade-long, population-based study of pediatric drowning related incidents. Acad Emerg Med. 2002;9:516-517.
20. Topjian AA, Berg RA, Bierens JJ, et al. Brain resuscitation in the drowning victim. Neurocrit Care. 2012;17:441-467.
21. Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 suppl 3):S829-S861.
22. Ibsen LM, Koch T. Submersion and asphyxial injury. Crit Care Med. 2002;30(11 suppl):S402-S408.
23. Schilling UM, Bortolin M. Drowning. Minerva Anethesiol. 2012;78:69-77.
24. Harries M. Near drowning. BMJ. 2003;327:1336-1338.
25. Gregorakos L, Markou N, Psalida V, et al. Near-drowning: clinical course of lung injury in adults. Lung. 2009;187:93-97.
26. Eich C, Bräuer A, Timmermann A, et al. Outcome of 12 drowned children with attempted resuscitation on cardiopulmonary bypass: an analysis of variables based on the “Utstein Style for Drowning”. Resuscitation. 2007;75:42-52.
27. Wollenek G, Honarwar N, Golej J, et al. Cold water submersion and cardiac arrest in treatment of severe hypothermia with cardiopulmonary bypass. Resuscitation. 2002;52:255-263.
28. Letsou GV, Kopf GS, Elefteriades JA, et al. Is cardiopulmonary bypass effective for treatment of hypothermic arrest due to drowning or exposure? Arch Surg. 1992;127:525-528.
29. Lund FK, Torgersen JG, Flaatten HK. Heart rate monitored hypothermia and drowning in a 48-year-old man. survival without sequelae: a case report. Cases J. 2009;2:6204.
30. Ballesteros MA, Gutiérrez-Cuadra M, Muñoz P, et al. Prognostic factors and outcome after drowning in an adult population. Acta Anaesthesiol Scand. 2009;53:935-940.
31. Nichter MA, Everett PB. Childhood near-drowning: is cardiopulmonary resuscitation always indicated? Crit Care Med. 1989;17:993-995.
32. Schaller MD, Fischer AP, Perret CH. Hyperkalemia. A prognostic factor during acute severe hypothermia. JAMA. 1990;264:1842-1845.
33. O’Connor MF, Ovassapian A. Airway management. In: Hall JB, Schmidt GA, Wood LD, eds. Principles of Critical Care. 3rd ed. New York, NY: McGraw-Hill; 2005.
34. Montenij LJ, de Vries W, Schwarte L, et al. Feasibility of pulse oximetry in the initial prehospital management of victims of drowning: a preliminary study. Resuscitation. 2011;82:1235-1238.
35. Brown DJ, Brugger H, Boyd J, et al. Accidental hypothermia. N Engl J Med. 2012;367:1930-1938.
36. Durrer B, Brugger H, Syme D; International Commission for Mountain Emergency Medicine. The medical on-site treatment of hypothermia: ICAR-MEDCOM recommendation. High Alt Med Biol. 2003;4:99-103.
37. Coskun KO, Popov AF, Schmitto JD, et al. Extracorporeal circulation for rewarming in drowning and near-drowning pediatric patients. Artif Organs. 2010;34:1026-1030.
38. Arrich J, Holzer M, Havel C, et al. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation. Cochrane Database Syst Rev. 2012;9:CD004128.
39. Rafaat KT, Spear RM, Kuelbs C, et al. Cranial computed tomographic findings in a large group of children with drowning: diagnostic, prognostic, and forensic implications. Pediatr Crit Care Med. 2008;9:567-572.
40. Laursen CB, Davidsen JR, Madsen PH. Utility of lung ultrasound in near-drowning victims. BMJ Case Rep. 2012;2012.
41. Ugras M, Guraksin O, Sen TA, et al. Surfactant replacement therapy in a pediatric near-drowning case in manure. Pediatr Emerg Care. 2012;28:913-914.
42. Kapur N, Slater A, McEniery J, et al. Therapeutic bronchoscopy in a child with sand aspiration and respiratory failure from near drowning—case report and literature review. Pediatr Pulmonol. 2009;44:1043-1047.
43. Staudinger T, Bankier A, Strohmaier W, et al. Exogenous surfactant therapy in a patient with adult respiratory distress syndrome after near drowning. Resuscitation. 1997;35:179-182.
44. Tadié JM, Heming N, Serve E, et al. Drowning associated pneumonia: a descriptive cohort. Resuscitation. 2012;83:399-401.
1. World Health Organization. Drowning. World Health Organization Web site. Available at: http://www.who.int/mediacentre/factsheets/fs347/en/. Accessed December 28, 2014.
2. Centers for Disease Control and Prevention (CDC). Drowning—United States, 2005-2009. MMWR Morb Mortal Wkly Rep. 2012;61:344-447.
3. Driscoll TR, Harrison JE, Steenkamp M. Alcohol and drowning in Australia. Inj Control Saf Promot. 2004;11:175-181.
4. Szpilman D. Near-drowning and drowning classification: a proposal to stratify mortality based on the analysis of 1,831 cases. Chest. 1997;112:660-665.
5. Hudson D, Ekman R, Svanström L. Survival of immersions during recreational boating events in Alaska, 1999-2004. Accid Anal Prev. 2007;39:437-443.
6. International Life Saving Federation. Drowning Report. International Life Saving Federation Web site. Available at: http://www.ilsf.org/sites/ilsf.org/files/filefield/drowningcongress.doc. Accessed December 28, 2014.
7. Brooks CJ, Howard KA, Neifer SK. How much did cold shock and swimming failure contribute to drowning deaths in the fishing industry in British Columbia 1976-2002? Occup Med (Lond). 2005;55:459-462.
8. Golden FS, Tipton MJ, Scott RC. Immersion, near-drowning and drowning. Br J Anaesth. 1997;79:214-225.
9. Bierens JJ, Knape JT, Gelissen HP. Drowning. Curr Opin Crit Care. 2002;8:578-586.
10. Ducharme MB, Lounsbury DS. Self-rescue swimming in cold water: the latest advice. Appl Physiol Nutr Metab. 2007;32:799-807.
11. Shattock MJ, Tipton MJ. ‘Autonomic conflict’: a different way to die during cold water immersion? J Physiol. 2012;590(pt 14):3219-3230.
12. Weiss J; American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention. Prevention of drowning. Pediatrics. 2010;126:e253-e262.
13.Yang L, Nong QQ, Li CL, et al. Risk factors for childhood drowning in rural regions of a developing country: a case-control study. Inj Prev. 2007;13:178-182.
14. Brenner RA, Taneja GS, Haynie DL, et al. The association between swimming lessons and drowning in childhood: a case-control study. Arch Pediatr Adolesc Med. 2009;163:203-210.
15. Rahman A, Rahman F, Hossain J, et al. Survival swimming - effectiveness of SwimSafe in preventing drowning in mid and late childhood. Abstract presented at: World Conference on Drowning Prevention; May 10-13, 2011; Danang, Vietnam.
16. Linnan M, Rahman A, Scarr J, et al. Child drowning: Evidence for a newly recognized cause of child mortality in low and middle income countries in Asia. Florence, Italy: UNICEF Office of Research. UNICEF Web site. Available at: www.unicef-irc.org/publications/pdf/drowning.pdf. Accessed December 28, 2014.
17. Salomez F, Vincent JL. Drowning: a review of epidemiology, pathophysiology, treatment and prevention. Resuscitation. 2004;63:261-268.
18. Venema AM, Groothoff JW, Bierens JJ. The role of bystanders during rescue and resuscitation of drowning victims. Resuscitation. 2010;81:434-439.
19. Pepe PE, Wigginton JG, Mann DM, et al. Prospective, decade-long, population-based study of pediatric drowning related incidents. Acad Emerg Med. 2002;9:516-517.
20. Topjian AA, Berg RA, Bierens JJ, et al. Brain resuscitation in the drowning victim. Neurocrit Care. 2012;17:441-467.
21. Vanden Hoek TL, Morrison LJ, Shuster M, et al. Part 12: cardiac arrest in special situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122(18 suppl 3):S829-S861.
22. Ibsen LM, Koch T. Submersion and asphyxial injury. Crit Care Med. 2002;30(11 suppl):S402-S408.
23. Schilling UM, Bortolin M. Drowning. Minerva Anethesiol. 2012;78:69-77.
24. Harries M. Near drowning. BMJ. 2003;327:1336-1338.
25. Gregorakos L, Markou N, Psalida V, et al. Near-drowning: clinical course of lung injury in adults. Lung. 2009;187:93-97.
26. Eich C, Bräuer A, Timmermann A, et al. Outcome of 12 drowned children with attempted resuscitation on cardiopulmonary bypass: an analysis of variables based on the “Utstein Style for Drowning”. Resuscitation. 2007;75:42-52.
27. Wollenek G, Honarwar N, Golej J, et al. Cold water submersion and cardiac arrest in treatment of severe hypothermia with cardiopulmonary bypass. Resuscitation. 2002;52:255-263.
28. Letsou GV, Kopf GS, Elefteriades JA, et al. Is cardiopulmonary bypass effective for treatment of hypothermic arrest due to drowning or exposure? Arch Surg. 1992;127:525-528.
29. Lund FK, Torgersen JG, Flaatten HK. Heart rate monitored hypothermia and drowning in a 48-year-old man. survival without sequelae: a case report. Cases J. 2009;2:6204.
30. Ballesteros MA, Gutiérrez-Cuadra M, Muñoz P, et al. Prognostic factors and outcome after drowning in an adult population. Acta Anaesthesiol Scand. 2009;53:935-940.
31. Nichter MA, Everett PB. Childhood near-drowning: is cardiopulmonary resuscitation always indicated? Crit Care Med. 1989;17:993-995.
32. Schaller MD, Fischer AP, Perret CH. Hyperkalemia. A prognostic factor during acute severe hypothermia. JAMA. 1990;264:1842-1845.
33. O’Connor MF, Ovassapian A. Airway management. In: Hall JB, Schmidt GA, Wood LD, eds. Principles of Critical Care. 3rd ed. New York, NY: McGraw-Hill; 2005.
34. Montenij LJ, de Vries W, Schwarte L, et al. Feasibility of pulse oximetry in the initial prehospital management of victims of drowning: a preliminary study. Resuscitation. 2011;82:1235-1238.
35. Brown DJ, Brugger H, Boyd J, et al. Accidental hypothermia. N Engl J Med. 2012;367:1930-1938.
36. Durrer B, Brugger H, Syme D; International Commission for Mountain Emergency Medicine. The medical on-site treatment of hypothermia: ICAR-MEDCOM recommendation. High Alt Med Biol. 2003;4:99-103.
37. Coskun KO, Popov AF, Schmitto JD, et al. Extracorporeal circulation for rewarming in drowning and near-drowning pediatric patients. Artif Organs. 2010;34:1026-1030.
38. Arrich J, Holzer M, Havel C, et al. Hypothermia for neuroprotection in adults after cardiopulmonary resuscitation. Cochrane Database Syst Rev. 2012;9:CD004128.
39. Rafaat KT, Spear RM, Kuelbs C, et al. Cranial computed tomographic findings in a large group of children with drowning: diagnostic, prognostic, and forensic implications. Pediatr Crit Care Med. 2008;9:567-572.
40. Laursen CB, Davidsen JR, Madsen PH. Utility of lung ultrasound in near-drowning victims. BMJ Case Rep. 2012;2012.
41. Ugras M, Guraksin O, Sen TA, et al. Surfactant replacement therapy in a pediatric near-drowning case in manure. Pediatr Emerg Care. 2012;28:913-914.
42. Kapur N, Slater A, McEniery J, et al. Therapeutic bronchoscopy in a child with sand aspiration and respiratory failure from near drowning—case report and literature review. Pediatr Pulmonol. 2009;44:1043-1047.
43. Staudinger T, Bankier A, Strohmaier W, et al. Exogenous surfactant therapy in a patient with adult respiratory distress syndrome after near drowning. Resuscitation. 1997;35:179-182.
44. Tadié JM, Heming N, Serve E, et al. Drowning associated pneumonia: a descriptive cohort. Resuscitation. 2012;83:399-401.
