User login
The Treatment of Adults with Essential Hypertension
- Only 53% of hypertensive patients are being treated, and only 24% have their hypertension under control.
- The first step in planning the treatment of a patient with essential hypertension is to categorize the patient’s risk status.
- The target blood pressure of patients who have diabetes or renal failure should be less than 130/85.
- Diuretics are safe, well tolerated, effective, relatively inexpensive, and convenient for initial drug treatment of hypertension in patients who do not have concomitant illness.
- Alpha-adrenergic blockers should be used with caution in the treatment of hypertension.
- Ambulatory blood pressure measurements predict cardiovascular events more closely than clinic blood pressure measurements.
Hypertension is arbitrarily defined as diastolic blood pressure (DBP) of 90 mm Hg or higher, systolic blood pressure (SBP) of 140 mm Hg or higher, or both, on 3 separate occasions. Essential hypertension is hypertension without an identifiable cause. Essential hypertension, also known as primary or idiopathic hypertension, accounts for at least 95% of all cases of hypertension.
According to the third National Health and Nutrition Examination Survey (NHANES III), approximately 60% of the 50 million Americans with hypertension are at increased risk for cardiovascular disease resulting from uncontrolled hypertension. This is because only 53% of hypertensive patients are being treated and only 24% have their hypertension under control.1 Physicians must play an active role in identifying and treating hypertension.
In an earlier Applied Evidence article2 an approach to the diagnosis of hypertension was presented. This article reviews the treatment of essential hypertension in adults and the prognosis of untreated hypertension. Risk stratification, alternative therapies, lifestyle modification, drug therapy, and prognosis will each be reviewed sequentially.
Risk stratification
The decision to treat hypertension and the choice of treatment is affected by the patient’s risk of morbidity and mortality if the blood pressure remains untreated or under-treated. According to the recommendations of the sixth report of the Joint National Committee on the Prevention, Diagnosis, Evaluation, and Treatment of High Blood Pressure (JNC-VI), the first step in planning treatment of a patient with essential hypertension is to categorize the patient’s risk status.3 The patient is placed in 1 of 9 treatment categories according to his or her blood pressure category, cardiovascular risk factors, and evidence of end-organ damage found during the initial evaluation (Table 1). Once the treatment category is identified, initial treatment should begin (Figure 1). Subsequent treatment depends on the patient’s response to initial treatment (Figure 2).
Patients should be monitored regularly to be sure they do not develop signs and symptoms that would place them in a different category and mandate more aggressive treatment. After a patient’s blood pressure has been controlled for 1 year, it may be possible to decrease the dose or the number of antihypertensive drugs—especially among patients who make significant lifestyle changes.4
The effectiveness of therapy varies depending on the patient’s cardiovascular risk. The New Zealand Guidelines Group has developed a helpful risk calculator based on the Framingham Heart Study for estimating a patient’s cardiovascular risk. This calculator incorporates sex, age, systolic blood pressure, smoking status, total cholesterol, high-density lipoprotein cholesterol, presence or absence of diabetes, and presence or absence of electrocardiogram evidence of left ventricular hypertrophy. This helpful risk calculator may be downloaded from the Web site of the New Zealand Guidelines Group at http://www.nzgg.org.nz/library/gl_complete/bloodpressure/appendix.cfm#app3. Alternatively, the University of Sheffield Medical School has developed tables to estimate an individual’s risk of heart disease based on cardiovascular risk factors including age, sex, cholesterol level, and presence or absence of smoking, hypertension, and diabetes—Sheffield tables.5 Software for handheld computers (Palm and PocketPC) that helps you estimate risk is available at www.jfponline.com.
Regardless of the method used, the benefit of treatment increases steadily as the patient’s current cardiovascular risk increases. With a 5-year cardiovascular risk of less than 2.5%, more than 120 patients have to be treated for 5 years to prevent 1 cardiovascular event; this number decreases to 25 patients with a risk of between 5% and 10%, and only 13 with a risk of between 20% and 24%.6 It is tempting to assume that the benefit of hypertension treatment is related to reduction in blood pressure whether achieved by drug therapy, lifestyle modification, or alternative therapy. However, this has not been established and it is important to consider the evidence supporting the benefit of each of these therapeutic options (Table 2).
TABLE 1
HYPERTENSION RISK STRATIFICATION AND TREATMENT CATEGORIES
| Blood Pressure Category | Risk Group A* | Risk Group B* | Risk Group C* |
|---|---|---|---|
| High-normal (130 – 139/85 – 89) | Lifestyle modification† | Lifestyle modification | Lifestyle modification and drug therapy |
| Stage 1 (140 – 159/0 – 99) | Lifestyle modification (12-month trial) | Lifestyle modification (6-month trial) | Lifestyle modification and drug therapy |
| Stage 2 or 3 (≥ 160 / ≤100) | Lifestyle modification and drug therapy | Lifestyle modification and drug therapy | Lifestyle modification and drug therapy |
| *Risk groups: A = no risk factors, end-organ damage, or clinical cardiovascular disease; B = 1 risk factor other than diabetes, no end-organ damage, and no clinical cardiovascular disease; C = Diabetes, end-organ damage, or clinic cardiovascular disease. | |||
| † Lifestyle modification should be included in the treatment plan of all patients receiving drug therapy. | |||
FIGURE 1
ALGORITHM FOR INITIAL MANAGEMENT OF HYPERTENSION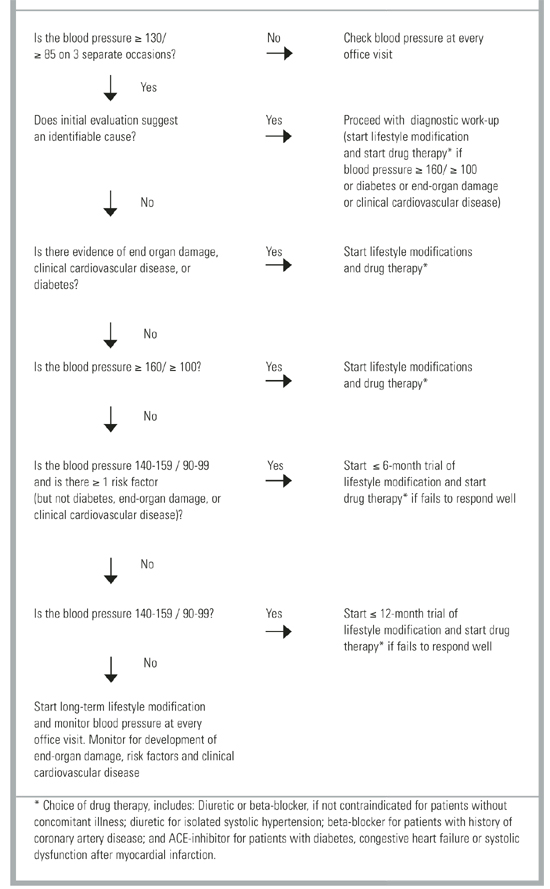
FIGURE 2
ALGORITHM FOR SUBSEQUENT MANAGEMENT OF HYPERTENSION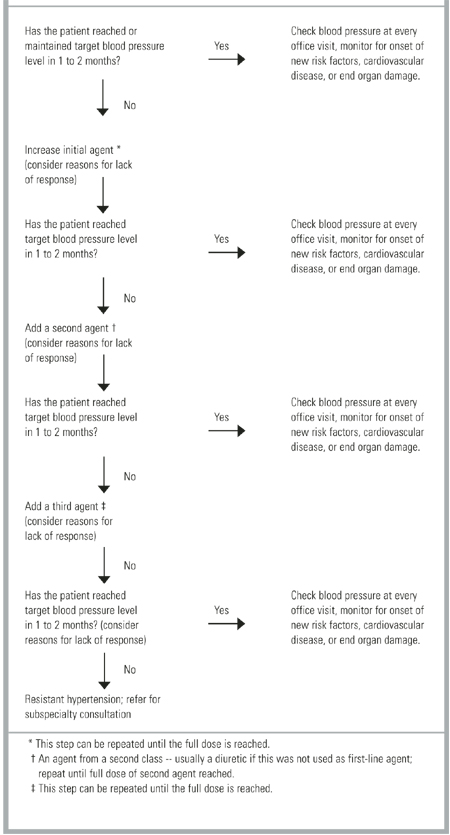
TABLE 2
NUMBER NEEDED TO TREAT (NNT) FOR SPECIFIC ANTIHYPERTENSIVE TREATMENTS
| Medication | Level of Evidence | NNT (95% CI)* | Comment |
|---|---|---|---|
| Low-Dose Thiazide | 1a | 18 (14-23) | Adults with systolic blood pressure |
| ≥ 160 or diastolic blood pressure | |||
| ≥90 regardless of age or comorbidities. | |||
| High-Dose Thiazide | 1a | 67 (48-111) | |
| Beta-Blocker | 1a | 142 (71-1000) | Drug vs no treatment comparison.14 |
| Calcium-Channel Blockers | 1b | 45 (30-102) | Isolated systolic hypertension in older patients, drug vs no treatment comparison.22 |
| ACE inhibitors | 1b | NS | Captopril versus diuretic or ß-blocker. |
| Alpha-agonists | 1b | NS | Doxazosin versus chlorthalidone, increased congestive heart in doxazosin group.7 |
| ARBs | NA | NA | Patient-oriented outcomes not available. |
| Sodium Restriction | 1a | NA | May reduce blood pressure but lacks evidence of reduced morbidity or mortality.27-35 |
| Weight Loss | 1a | NA | |
| Exercise | 1a | NA | |
| Low-Fat Diet | 1b | NA | |
| Limited Alcohol | 5 | NA | |
| Potassium Supplement | 1a | NA | |
| Fish Oil Supplement | 1a | NA | |
| Acupuncture | NA | NA | No evidence of blood pressure reduction or reduced morbidity or mortality.36-43 |
| Biofeedback | NA | NA | |
| Herbal Medicine | NA | NA | |
| Transcendental Meditation | NA | NA | |
| Yoga | NA | NA | |
| *For total cardiovascular events over 5 years. | |||
| NS denotes no significant difference from comparison drug; NA, not applicable; ACE, angiotensin-converting enzyme; ARBs, angiotensin-receptor blockers. | |||
Treatment
Drug Therapy
Patients who require drug treatment for hypertension should begin with a low dose of the initial medication, and that dose should be slowly titrated upward every 1 to 2 months (Figure 2). The JNC-VI recommends a diuretic or a ß-blocker with once daily dosing and 24-hour efficacy as the initial treatment for most hypertensive patients. However, the choice of initial medication will be affected by concomitant illnesses: (1) ß-blockers are recommended for the initial treatment of patients with hypertension and a history of coronary artery disease; (2) diuretics are suggested for the initial treatment of isolated systolic hypertension; (3) and angiotensin-converting enzyme (ACE) inhibitors are recommended for hypertensive patients who have systolic dysfunction after myocardial infarction, diabetic nephropathy, or congestive heart failure. Angiotensin II receptor blockers may be used in patients who cannot tolerate ACE inhibitors because of cough or rash. Alpha-adrenergic blockers should be used with caution in light of evidence that they may increase the risk of cardiovascular events (especially congestive heart failure).7
Among patients who do not have concomitant illness, the choice of drug therapy is controversial. A case-control study and a meta-analysis suggested that short-acting calcium channel blockers (CCBs) increase cardiovascular mortality.8,9 Unfortunately, these studies were not designed to establish a causal relationship. A recent nonsystematic review suggested that short-acting CCBs should be avoided and that conventional therapies were more effective than long-acting CCBs.10 An earlier non-systematic review suggested that short- and intermediate-acting CCBs were associated with increased cardiovascular mortality and morbidity. However, a well-designed cohort study of patients with coronary artery disease failed to reveal an increase in adverse effects among patients taking short-acting CCBs.11 Furthermore, randomized controlled trials suggest that diuretics, ß-blockers, and long-acting CCBs are equally effective in preventing cardiovascular mortality and morbidity.12,13 Physicians who treat hypertension must choose the best initial treatment for patients who do not have concomitant illness. Fortunately, safety, tolerability, efficacy, price, and simplicity can guide the physician to an ideal drug for most hypertensive patients.
Low-dose thiazide diuretics (the equivalent of 25 to 50 mg of hydrochlorothiazide) appear better tolerated than ß-blockers or CCBs.14 Treatment with ß-blockers, CCBs, and ACE inhibitors is also more expensive (75% to 85% more) than diuretic therapy.15 The cost savings offered by diuretics complement the fact that diuretics are safe, effective, and may be dosed once daily. In short, in addition to being the drug of choice for isolated systolic hypertension, low-dose thiazide diuretics are the ideal initial drug treatment of patients without concomitant illness. It should be noted that higher doses of thiazide diuretics offer proportionately less blood pressure reduction and greater risk of hypokalemia.16
Antihypertensive treatment reduces morbidity and mortality for all stages of hypertension, but people with the greatest baseline cardiovascular risk (eg, older patients and patients with higher levels of blood pressure) have the most to gain from treatment.17,18 There is no conclusive evidence to suggest that lowering blood pressure to below 140/80 reduces morbidity or mortality in most patients. However, patients who have diabetes or renal failure benefit from more aggressive management of blood pressure.19,20 Therefore, the JNC-VI recommends a target blood pressure of less than 130/85 for these patients.
The JNC-VI recommendation to start with a low-dose diuretic is supported by the evidence across a spectrum of patient-oriented outcomes. The effectiveness of diuretics and ß-blockers as first-line agents has been confirmed by long-term clinical trials.14,21 However, low-dose thiazides appear effective against a broader range of outcomes than high-dose thiazides and ß-blockers (Table 3). There is also evidence to suggest that CCBs and ACE inhibitors may be effective first-line agents, but fewer patients have been studied who take CCBs and ACE inhibitors than those who take diuretics and ß-blockers.22,23
Most patients with hypertension will respond to 1 (approximately 50%) or 2 (approximately 30%) antihypertensive medications.19,24,25 As noted earlier, failure to respond to treatment suggests an identifiable cause of hypertension. Among patients who do not have a secondary cause of hypertension, inadequate drug treatment (often failure to start a diuretic) and noncompliance are among the most common causes of resistant hypertension.26
When patients who are receiving drug therapy fail to reach the target blood pressure goal or fail to maintain the blood pressure goal, they should have the initial drug dose increased until the goal is reached (Figure 2). Those who fail initial drug therapy at full doses should have a second drug added and increased until the blood pressure goal is reached. Those who fail initial and second drug therapy at full doses should have a third drug added and increased until the pressure goal is reached. Patients who fail to reach the goal on maximal doses of 3 drugs have, by definition, resistant hypertension and will require evaluation by a physician with expertise in managing resistant hypertension. A cause should be sought each time a patient fails to respond to a drug or fails to maintain blood pressure control on a drug that had previously controlled the pressure (Table 3).
TABLE 3
PARTIAL LISTING OF CAUSES OF FAILURE TO REACH OR MAINTAIN TARGET BLOOD PRESSURE
| Volume overload: failure to start a diuretic |
| Nonadherence to therapy: dementia, side effects, complex regimen |
| Drug-induced: prescription, over-the-counter, herbal, or illicit drugs |
| Diet/stimulant induced: caffeine, licorice, salt, alcohol, nicotine |
| Associated conditions: obesity, sleep apnea, anxiety, chronic pain |
| Identifiable causes: chronic renal disease, renovascular disease, hyperaldosteronism, Cushing’s syndrome, pheochromocytoma |
| Pseudoresistance: wrong cuff size, white-coat hypertension |
Lifestyle modifications
Several lifestyle modifications are recommended in all treatment categories. Aerobic exercise (45 to 60 minutes at least 3 days per week), low-salt, low-fat, and high fruit and vegetable diet, limited alcohol consumption (less than 3 drinks per day), and modest weight loss (3% to 9% of total body weight) have been demonstrated to yield modest blood pressure reductions, but there is insufficient evidence to suggest that these measures alone reduce morbidity or mortality in hypertensive patients.27-33 A systematic review of randomized controlled trials found an average 4.4/2.5 mm Hg reduction in blood pressure with no evidence of harm (among patients who were not at risk for hyperkalemia) when diet was supplemented with about 2000 mg of potassium daily.34 A comparable reduction in blood pressure was seen with a daily supplement of more than 3 grams of fish oil.35 Research concerning the value of calcium and magnesium supplementation is conflicting and insufficient for supplementation to be considered standard therapy at this time.
Alternative therapy
The number and the quality of studies evaluating acupuncture, biofeedback, herbal medicine, transcendental meditation, and yoga are, for the most part, limited. They have focused on reduction in blood pressure, not patient-oriented outcomes, such as a reduction in morbidity and mortality. Acupuncture does not appear to have a significant effect on blood pressure levels.36,37 Biofeedback and other behavioral techniques have not been demonstrated to reduce blood pressure.38,39 The effect of garlic on blood pressure is unclear with mixed study results.40,41 Transcendental meditation and yoga may reduce blood pressure, but studies of these modalities are small and the experimental designs have a limited capacity to detect an independent treatment effect or a placebo effect.42,43
Therefore, physicians who include any of these modalities in their hypertension treatment plan should carefully monitor each patient for adequacy of blood pressure control, development of risk factors, and evidence of end-organ damage. At this time, alternative therapies should be considered experimental adjuncts to lifestyle modification and medical therapy that have not been shown to improve patient-oriented outcomes.
Follow-up of patients with hypertension
Follow-up visits should be designed to identify new risk factors, evidence of end-organ damage, and adequacy of blood pressure control. Follow-up visits may include an interval history, limited physical examination, radiologic evaluation, and laboratory testing. The frequency and nature of follow-up hypertension evaluations will vary according to the presence or absence of preexisting risk factors, evidence of end-organ damage, the nature of the treatment the patient is receiving, and the stability of blood pressure control. Unfortunately, there is little evidence to support specific recommendations for the frequency and nature of follow-up hypertension evaluations.
In the absence of evidence, several general principles may be suggested. Patients should be seen within 2 months of initiation of treatment. Follow-up history should focus on the cardiovascular and neurologic review of systems. The examination should include a focused cardiovascular work-up (eg, retinopathy, carotid bruits). Consideration should be given to periodic laboratory testing for diabetes, renal insufficiency, and hyperlipidemia. Periodic (but less frequent) chest x-rays and electrocardiograms may be helpful to detect cardiomegaly, but there is no evidence to support such testing in the absence of symptoms.
Follow-up visits should be more frequent among patients who have marginal blood pressure control, preexisting risk factors, or end-organ damage. Evaluations may be less frequent among those with good control and no preexisting risk factors or endorgan damage. Office visits and testing should be more frequent whenever changes are made in treatment. The frequency and nature of follow-up testing will also depend on the nature of treatment. Patients taking diuretics should have their potassium levels checked periodically. Renal function and potassium should be monitored in patients who are taking ACE inhibitors, especially during the first few weeks of therapy.
Patients willing to regularly monitor their blood pressure at home may require less frequent follow-up than those who leave it to the physician to check. Patients who monitor their blood pressure at home should have their sphygmomanometers validated initially and periodically.44 It is important to remember that home blood pressure measurements are consistently lower and more closely correlated with cardiovascular outcomes than are clinic blood pressure measurements.45-47
Prognosis
It is difficult to estimate the precise impact blood pressure control has on morbidity and mortality, but it is clear that high blood pressure, if unrecognized or untreated, substantially increases the morbidity and mortality associated with coronary disease, heart failure, renal failure, and stroke.17 In an early study of untreated hypertension there was a close relationship between blood pressure level and cardiovascular morbidity over 14 years of observation. This study revealed that hypertensive patients (those with a blood pressure of 160/95) had cardiovascular morbidity rates (coronary artery disease, claudication, stroke, and congestive heart failure) 2 to 3 times higher than normotensive patients.48 The impact of inadequately controlled blood pressure on morbidity and mortality among patients with diabetes is especially problematic.49 Over 9 years, when compared with diabetic patients with less tight control (< 180/105 mm Hg), those with tight blood pressure control (< 150/85 mm Hg) had a 24% reduction in sudden death, hyperglycemic or hypoglycemic death, fatal or nonfatal myocardial infarction, angina, heart failure, fatal or nonfatal stroke, renal failure, amputation, vitreous hemorrhage, and retinal hemorrhage.
Finally, renal function deteriorates more rapidly when blood pressure control is inadequate in patients with chronic renal disease of diverse causes.20 Over 2 years, when compared with patients with renal failure who had less tight control (mean arterial pressure 107 mm Hg), renal failure patients with tight control (mean arterial blood pressure 92 mm Hg) had significantly less proteinuria and lower rates of decline in renal function. Whether this translates into a significant improvement in the risk of end-stage renal disease is unknown.
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the third national health and nutrition examination survey, 1988-1991. Hypertension 1995;25:305-13.
2. Dosh S. The diagnosis of essential and secondary hypertension in adults. J Fam Pract 2001;50:707-12.
3. Joint National Committee on the Prevention Detection. Evaluation and Treatment of High Blood Pressure. the sixth report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
4. Whelton P, Appelgate W, Ettinger W, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of non-pharmacologic interventions in the elderly (TONE). JAMA 1996;279:839-46.
5. Wallis E, Ramsay L, Haq I, Ghahramani P, Jackson P. Coronary and cardiovascular risk estimation for the primary prevention: validation of a new Sheffield table in the 1995 Scottish health survey. Br Med J 2000;320:671-76.
6. Baker S, Priest P, Jackson R. Using thresholds based on risk of cardiovascular disease to target treatment for hypertension: modelling events averted and number treated. Br Med J 2000;320:680-85.
7. ALLHAT Collaborative Research Group. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone. J Am Med Assoc 2000;283:1967-75.
8. Psaty B, Heckbert S, Koepsell T, et al. The risk of myocardial infarction associated with anti-hypertensive drug therapies. JAMA 1995;274:620-25.
9. Furberg C, Psaty B, Meyer J. Nifedipine: dose related increase in mortality in patients with coronary heart disease. Circulation 1995;92:1326-31.
10. Kizer J, Kimmel S. Epidemiologic review of the calcium channel blocker drugs. Arch Intern Med 2001;161:1145-58.
11. Braun S, Boyo V, Behar S, et al. Calcium antagonists did not increase mortality in patients with coronary artery disease. J Am Coll Cardiol 1996;28:7-11.
12. Hansson L, Hedner T, Lund-Johansen P, et al. Randomized trial of effects of calcium antagonists compared with diuretics and B-blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000;356:359-65.
13. Hansson L, Lindholm L, Ekbohm T, Dahlof B. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity. The Swedish trial in old patients with hypertension-2 study. Lancet 1999;354:1751-56.
14. Wright J, Lee C, Chambers G. Systematic review of antihypertensive therapies: does evidence assist in choosing a first-line drug? Can Med Assoc J 1999;161:25-32.
15. Ramsey S, Niel N, Sullivan S, Perfetto E. An economic evaluation of the JNC hypertension guidelines using data from a randomized controlled trial. J Am Board Fam Pract 1999;12:105-14.
16. Wright J. Choosing a first-line drug in the management of elevated blood pressure: What is the evidence?: 1 Thiazide diuretics. Can Med Assoc J 2000;163:57-60.
17. Gueyffier F, Froment A, Gouton M. New meta-analysis of treatment trials of hypertension: improving the estimate of therapeutic benefit. J Hum Hypertens 1996;10:1-8.
18. Mulrow C, Cornell J, Herrera C, Kadri A, Farnett L, Aguilar C. Hypertension in the elderly: implications and generalizability of randomized trials. JAMA 1994;272:1932-38.
19. Hansson L, Zanchetti A, Carruthers S, Dahlof B. Effects of intensive blood pressure lowering and low dose aspirin in patients with hypertension: principal results of the hypertension optimal treatment (HOT) randomised trial. Lancet 1998;351:1755-62.
20. Peterson J, Adler S, Burkart J, Greene J. Blood pressure control, proteinuria, and the progression of renal disease. Ann Intern Med 1995;123:754-62.
21. Psaty B, Smith N, Siscovick D, Koepsell T, Weiss N. Health outcomes associated with antihypertensive therapies used as first-line agents: A systematic review and meta-analysis. J Am Med Assoc 1197;277:739-45.
22. Staessen J, Fagard R, Celis H, Arabidze C, Birkenhager W. Randomised double-blind comparison of placebo and active treatment in older patients with isolated systolic hypertension. Lancet 1997;350:757-64.
23. Investigators THOPES. Effect of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. New Eng J Med 2000;342:145-53.
24. Masterson B, Reda D, Preston R, et al. Response to a second single antihypertensive agent used as monotherapy for hypertension after failure of the initial drug. Arch Intern Med 1995;155:1757-62.
25. Tuomilehto J, Rastenyte D, Birkenhager W, et al. Systolic hypertension in Europe trial investigators. Effects of calcium-channel blockers in older patients with diabetes and systolic hypertension. New Eng J Med 1999;340:677-84.
26. Yakovlevitch M, Black HR. Resistant hypertension in a tertiary care clinic. Arch Intern Med 1991;151:1786-92.
27. Halbert J, Silagy C, Finucane P, Withers R. The effectiveness of exercise training in lowering blood pressure: a metaanalysis of randomized controlled trials of 4 weeks or longer. J Human Hypertension 1997;10:641-49.
28. Ebrahim S, Davey G. Lowering blood pressure: a systematic review of sustained effects of non-pharmacologic interventions. J Public Health Med 1998;4:441-48.
29. Appel L, Moore T, Obarzanek E, Vollmer W. A clinical trail of the effects of dietary patterns on blood pressure. New Eng J Med 1997;336:1117-24.
30. Appel L, Espeland M, Easter L, Wilson A, Folmar S, Lacy C. Effects of reduced sodium intake on hypertension control in older individuals. Results from the trial of nonpharmacologic interventions in the elderly (TONE). Arch Intern Med 2001;161:685-93.
31. Beilin L, Puddey I, Burke V. Alcohol and hypertension: kill or cure? J Human Hypertension 1996;10(Suppl 2):1-5.
32. Corrigan S, Raczynski J, Swencionis C, Jennings S. Weight reduction in the prevention and treatment of hypertension: a review of representative clinical trials. Am J Health Promo 1991;5:208-14.
33. Mulrow C, Chiquette E, Angel L, Cornell J. Dieting to reduce body weight for controlling hypertension in adults. The Cochrane Library 2001.
34. Whelton P, He J, Cutler J, Brancati F, Appel L. Effects of oral potassium on blood pressure: meta-analysis of randomized controlled trials. JAMA 1997;277:1624-32.
35. Morris M, Sacks F, Rosner B. Regulation on blood pressure: does fish oil lower blood pressure?: analysis of controlled trials. Circulation 1993;88:523-33.
36. Sugioka K, Woods M, Mueller R. An unsuccessful attempt to treat hypertension with acupuncture. Am J Chinese Med 1977;5:39-44.
37. Kraft K, Coulon S. Effect of a standardized acupuncture treatment on complaints, blood pressure, and serum lipids of hypertensive, postmenopausal women. A randomized controlled clinical study. Forschende Komplementarmedizin 1999;6:74-79.
38. Eisenberg D, Delblanco T, Berkey C, et al. Cognitive and behavioral techniques and hypertension: a meta-analysis. Ann Intern Med 1993;118:964-72.
39. Hunyor S, Henderson R, Saroj K, Carter N, et al. Placebo-controlled biofeedback blood pressure effect in hypertensive humans. Hypertension 1997;29:1225-31.
40. Auer W. Hypertension and hyperlipidemia: garlic helps in mild cases. Br J Clin Pract 1990;69(Suppl):3-6.
41. Ackerman R, Mulrow C, Ramirez G, Gardner C, Mobidoni L, Lawrence V. Garlic shows promise for improving some cardiovascular risk factors. Arch Intern Med 2001;161:813-24.
42. Patel C. Twelve-month follow-up of yoga and bio-feedback in the management of hypertension. Lancet 1975;1:62-64.
43. Sundar S, Agrawal S, Singh V, Bhattacharya S, et al. Role of yoga in management of essential hypertension. Acta Cardiologica 1984;39:203-08.
44. White W, Berson A, Robbins C, Jamieson M, Prisant L. National standard for measurement of resting and ambulatory blood pressure with automated sphygmomanometers. Hypertension 1993;21:504-09.
45. Staessen J, Byttebier G, Butinx F, Celis H, O’Brien E. Antihypertensive treatment based on conventional or ambulatory blood pressure measurement. J Am Med Assoc 1997;278:1065-72.
46. Ohkubo T, Imai Y, Tsuji I, Nagai K, Ito S. Reference values for 24-hour ambulatory blood pressure monitoring based on a prognostic criterion: the Ohasma study. Hypertension 1998;32:255-59.
47. Staessen J, Thijs L, Fagard R, O’Brien E, Eoin T. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. JAMA 1999;282:539-46.
48. Kannel W, Wolf P, Verter J, McNamara P. Epidemiologic assessment of the role of blood pressure in stroke: the Framingham study. JAMA 1970;214:301-10.
49. Turner R, Holman R, Stratton I, Cull C. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. Br Med J 1998;317:703-12.
- Only 53% of hypertensive patients are being treated, and only 24% have their hypertension under control.
- The first step in planning the treatment of a patient with essential hypertension is to categorize the patient’s risk status.
- The target blood pressure of patients who have diabetes or renal failure should be less than 130/85.
- Diuretics are safe, well tolerated, effective, relatively inexpensive, and convenient for initial drug treatment of hypertension in patients who do not have concomitant illness.
- Alpha-adrenergic blockers should be used with caution in the treatment of hypertension.
- Ambulatory blood pressure measurements predict cardiovascular events more closely than clinic blood pressure measurements.
Hypertension is arbitrarily defined as diastolic blood pressure (DBP) of 90 mm Hg or higher, systolic blood pressure (SBP) of 140 mm Hg or higher, or both, on 3 separate occasions. Essential hypertension is hypertension without an identifiable cause. Essential hypertension, also known as primary or idiopathic hypertension, accounts for at least 95% of all cases of hypertension.
According to the third National Health and Nutrition Examination Survey (NHANES III), approximately 60% of the 50 million Americans with hypertension are at increased risk for cardiovascular disease resulting from uncontrolled hypertension. This is because only 53% of hypertensive patients are being treated and only 24% have their hypertension under control.1 Physicians must play an active role in identifying and treating hypertension.
In an earlier Applied Evidence article2 an approach to the diagnosis of hypertension was presented. This article reviews the treatment of essential hypertension in adults and the prognosis of untreated hypertension. Risk stratification, alternative therapies, lifestyle modification, drug therapy, and prognosis will each be reviewed sequentially.
Risk stratification
The decision to treat hypertension and the choice of treatment is affected by the patient’s risk of morbidity and mortality if the blood pressure remains untreated or under-treated. According to the recommendations of the sixth report of the Joint National Committee on the Prevention, Diagnosis, Evaluation, and Treatment of High Blood Pressure (JNC-VI), the first step in planning treatment of a patient with essential hypertension is to categorize the patient’s risk status.3 The patient is placed in 1 of 9 treatment categories according to his or her blood pressure category, cardiovascular risk factors, and evidence of end-organ damage found during the initial evaluation (Table 1). Once the treatment category is identified, initial treatment should begin (Figure 1). Subsequent treatment depends on the patient’s response to initial treatment (Figure 2).
Patients should be monitored regularly to be sure they do not develop signs and symptoms that would place them in a different category and mandate more aggressive treatment. After a patient’s blood pressure has been controlled for 1 year, it may be possible to decrease the dose or the number of antihypertensive drugs—especially among patients who make significant lifestyle changes.4
The effectiveness of therapy varies depending on the patient’s cardiovascular risk. The New Zealand Guidelines Group has developed a helpful risk calculator based on the Framingham Heart Study for estimating a patient’s cardiovascular risk. This calculator incorporates sex, age, systolic blood pressure, smoking status, total cholesterol, high-density lipoprotein cholesterol, presence or absence of diabetes, and presence or absence of electrocardiogram evidence of left ventricular hypertrophy. This helpful risk calculator may be downloaded from the Web site of the New Zealand Guidelines Group at http://www.nzgg.org.nz/library/gl_complete/bloodpressure/appendix.cfm#app3. Alternatively, the University of Sheffield Medical School has developed tables to estimate an individual’s risk of heart disease based on cardiovascular risk factors including age, sex, cholesterol level, and presence or absence of smoking, hypertension, and diabetes—Sheffield tables.5 Software for handheld computers (Palm and PocketPC) that helps you estimate risk is available at www.jfponline.com.
Regardless of the method used, the benefit of treatment increases steadily as the patient’s current cardiovascular risk increases. With a 5-year cardiovascular risk of less than 2.5%, more than 120 patients have to be treated for 5 years to prevent 1 cardiovascular event; this number decreases to 25 patients with a risk of between 5% and 10%, and only 13 with a risk of between 20% and 24%.6 It is tempting to assume that the benefit of hypertension treatment is related to reduction in blood pressure whether achieved by drug therapy, lifestyle modification, or alternative therapy. However, this has not been established and it is important to consider the evidence supporting the benefit of each of these therapeutic options (Table 2).
TABLE 1
HYPERTENSION RISK STRATIFICATION AND TREATMENT CATEGORIES
| Blood Pressure Category | Risk Group A* | Risk Group B* | Risk Group C* |
|---|---|---|---|
| High-normal (130 – 139/85 – 89) | Lifestyle modification† | Lifestyle modification | Lifestyle modification and drug therapy |
| Stage 1 (140 – 159/0 – 99) | Lifestyle modification (12-month trial) | Lifestyle modification (6-month trial) | Lifestyle modification and drug therapy |
| Stage 2 or 3 (≥ 160 / ≤100) | Lifestyle modification and drug therapy | Lifestyle modification and drug therapy | Lifestyle modification and drug therapy |
| *Risk groups: A = no risk factors, end-organ damage, or clinical cardiovascular disease; B = 1 risk factor other than diabetes, no end-organ damage, and no clinical cardiovascular disease; C = Diabetes, end-organ damage, or clinic cardiovascular disease. | |||
| † Lifestyle modification should be included in the treatment plan of all patients receiving drug therapy. | |||
FIGURE 1
ALGORITHM FOR INITIAL MANAGEMENT OF HYPERTENSION
FIGURE 2
ALGORITHM FOR SUBSEQUENT MANAGEMENT OF HYPERTENSION
TABLE 2
NUMBER NEEDED TO TREAT (NNT) FOR SPECIFIC ANTIHYPERTENSIVE TREATMENTS
| Medication | Level of Evidence | NNT (95% CI)* | Comment |
|---|---|---|---|
| Low-Dose Thiazide | 1a | 18 (14-23) | Adults with systolic blood pressure |
| ≥ 160 or diastolic blood pressure | |||
| ≥90 regardless of age or comorbidities. | |||
| High-Dose Thiazide | 1a | 67 (48-111) | |
| Beta-Blocker | 1a | 142 (71-1000) | Drug vs no treatment comparison.14 |
| Calcium-Channel Blockers | 1b | 45 (30-102) | Isolated systolic hypertension in older patients, drug vs no treatment comparison.22 |
| ACE inhibitors | 1b | NS | Captopril versus diuretic or ß-blocker. |
| Alpha-agonists | 1b | NS | Doxazosin versus chlorthalidone, increased congestive heart in doxazosin group.7 |
| ARBs | NA | NA | Patient-oriented outcomes not available. |
| Sodium Restriction | 1a | NA | May reduce blood pressure but lacks evidence of reduced morbidity or mortality.27-35 |
| Weight Loss | 1a | NA | |
| Exercise | 1a | NA | |
| Low-Fat Diet | 1b | NA | |
| Limited Alcohol | 5 | NA | |
| Potassium Supplement | 1a | NA | |
| Fish Oil Supplement | 1a | NA | |
| Acupuncture | NA | NA | No evidence of blood pressure reduction or reduced morbidity or mortality.36-43 |
| Biofeedback | NA | NA | |
| Herbal Medicine | NA | NA | |
| Transcendental Meditation | NA | NA | |
| Yoga | NA | NA | |
| *For total cardiovascular events over 5 years. | |||
| NS denotes no significant difference from comparison drug; NA, not applicable; ACE, angiotensin-converting enzyme; ARBs, angiotensin-receptor blockers. | |||
Treatment
Drug Therapy
Patients who require drug treatment for hypertension should begin with a low dose of the initial medication, and that dose should be slowly titrated upward every 1 to 2 months (Figure 2). The JNC-VI recommends a diuretic or a ß-blocker with once daily dosing and 24-hour efficacy as the initial treatment for most hypertensive patients. However, the choice of initial medication will be affected by concomitant illnesses: (1) ß-blockers are recommended for the initial treatment of patients with hypertension and a history of coronary artery disease; (2) diuretics are suggested for the initial treatment of isolated systolic hypertension; (3) and angiotensin-converting enzyme (ACE) inhibitors are recommended for hypertensive patients who have systolic dysfunction after myocardial infarction, diabetic nephropathy, or congestive heart failure. Angiotensin II receptor blockers may be used in patients who cannot tolerate ACE inhibitors because of cough or rash. Alpha-adrenergic blockers should be used with caution in light of evidence that they may increase the risk of cardiovascular events (especially congestive heart failure).7
Among patients who do not have concomitant illness, the choice of drug therapy is controversial. A case-control study and a meta-analysis suggested that short-acting calcium channel blockers (CCBs) increase cardiovascular mortality.8,9 Unfortunately, these studies were not designed to establish a causal relationship. A recent nonsystematic review suggested that short-acting CCBs should be avoided and that conventional therapies were more effective than long-acting CCBs.10 An earlier non-systematic review suggested that short- and intermediate-acting CCBs were associated with increased cardiovascular mortality and morbidity. However, a well-designed cohort study of patients with coronary artery disease failed to reveal an increase in adverse effects among patients taking short-acting CCBs.11 Furthermore, randomized controlled trials suggest that diuretics, ß-blockers, and long-acting CCBs are equally effective in preventing cardiovascular mortality and morbidity.12,13 Physicians who treat hypertension must choose the best initial treatment for patients who do not have concomitant illness. Fortunately, safety, tolerability, efficacy, price, and simplicity can guide the physician to an ideal drug for most hypertensive patients.
Low-dose thiazide diuretics (the equivalent of 25 to 50 mg of hydrochlorothiazide) appear better tolerated than ß-blockers or CCBs.14 Treatment with ß-blockers, CCBs, and ACE inhibitors is also more expensive (75% to 85% more) than diuretic therapy.15 The cost savings offered by diuretics complement the fact that diuretics are safe, effective, and may be dosed once daily. In short, in addition to being the drug of choice for isolated systolic hypertension, low-dose thiazide diuretics are the ideal initial drug treatment of patients without concomitant illness. It should be noted that higher doses of thiazide diuretics offer proportionately less blood pressure reduction and greater risk of hypokalemia.16
Antihypertensive treatment reduces morbidity and mortality for all stages of hypertension, but people with the greatest baseline cardiovascular risk (eg, older patients and patients with higher levels of blood pressure) have the most to gain from treatment.17,18 There is no conclusive evidence to suggest that lowering blood pressure to below 140/80 reduces morbidity or mortality in most patients. However, patients who have diabetes or renal failure benefit from more aggressive management of blood pressure.19,20 Therefore, the JNC-VI recommends a target blood pressure of less than 130/85 for these patients.
The JNC-VI recommendation to start with a low-dose diuretic is supported by the evidence across a spectrum of patient-oriented outcomes. The effectiveness of diuretics and ß-blockers as first-line agents has been confirmed by long-term clinical trials.14,21 However, low-dose thiazides appear effective against a broader range of outcomes than high-dose thiazides and ß-blockers (Table 3). There is also evidence to suggest that CCBs and ACE inhibitors may be effective first-line agents, but fewer patients have been studied who take CCBs and ACE inhibitors than those who take diuretics and ß-blockers.22,23
Most patients with hypertension will respond to 1 (approximately 50%) or 2 (approximately 30%) antihypertensive medications.19,24,25 As noted earlier, failure to respond to treatment suggests an identifiable cause of hypertension. Among patients who do not have a secondary cause of hypertension, inadequate drug treatment (often failure to start a diuretic) and noncompliance are among the most common causes of resistant hypertension.26
When patients who are receiving drug therapy fail to reach the target blood pressure goal or fail to maintain the blood pressure goal, they should have the initial drug dose increased until the goal is reached (Figure 2). Those who fail initial drug therapy at full doses should have a second drug added and increased until the blood pressure goal is reached. Those who fail initial and second drug therapy at full doses should have a third drug added and increased until the pressure goal is reached. Patients who fail to reach the goal on maximal doses of 3 drugs have, by definition, resistant hypertension and will require evaluation by a physician with expertise in managing resistant hypertension. A cause should be sought each time a patient fails to respond to a drug or fails to maintain blood pressure control on a drug that had previously controlled the pressure (Table 3).
TABLE 3
PARTIAL LISTING OF CAUSES OF FAILURE TO REACH OR MAINTAIN TARGET BLOOD PRESSURE
| Volume overload: failure to start a diuretic |
| Nonadherence to therapy: dementia, side effects, complex regimen |
| Drug-induced: prescription, over-the-counter, herbal, or illicit drugs |
| Diet/stimulant induced: caffeine, licorice, salt, alcohol, nicotine |
| Associated conditions: obesity, sleep apnea, anxiety, chronic pain |
| Identifiable causes: chronic renal disease, renovascular disease, hyperaldosteronism, Cushing’s syndrome, pheochromocytoma |
| Pseudoresistance: wrong cuff size, white-coat hypertension |
Lifestyle modifications
Several lifestyle modifications are recommended in all treatment categories. Aerobic exercise (45 to 60 minutes at least 3 days per week), low-salt, low-fat, and high fruit and vegetable diet, limited alcohol consumption (less than 3 drinks per day), and modest weight loss (3% to 9% of total body weight) have been demonstrated to yield modest blood pressure reductions, but there is insufficient evidence to suggest that these measures alone reduce morbidity or mortality in hypertensive patients.27-33 A systematic review of randomized controlled trials found an average 4.4/2.5 mm Hg reduction in blood pressure with no evidence of harm (among patients who were not at risk for hyperkalemia) when diet was supplemented with about 2000 mg of potassium daily.34 A comparable reduction in blood pressure was seen with a daily supplement of more than 3 grams of fish oil.35 Research concerning the value of calcium and magnesium supplementation is conflicting and insufficient for supplementation to be considered standard therapy at this time.
Alternative therapy
The number and the quality of studies evaluating acupuncture, biofeedback, herbal medicine, transcendental meditation, and yoga are, for the most part, limited. They have focused on reduction in blood pressure, not patient-oriented outcomes, such as a reduction in morbidity and mortality. Acupuncture does not appear to have a significant effect on blood pressure levels.36,37 Biofeedback and other behavioral techniques have not been demonstrated to reduce blood pressure.38,39 The effect of garlic on blood pressure is unclear with mixed study results.40,41 Transcendental meditation and yoga may reduce blood pressure, but studies of these modalities are small and the experimental designs have a limited capacity to detect an independent treatment effect or a placebo effect.42,43
Therefore, physicians who include any of these modalities in their hypertension treatment plan should carefully monitor each patient for adequacy of blood pressure control, development of risk factors, and evidence of end-organ damage. At this time, alternative therapies should be considered experimental adjuncts to lifestyle modification and medical therapy that have not been shown to improve patient-oriented outcomes.
Follow-up of patients with hypertension
Follow-up visits should be designed to identify new risk factors, evidence of end-organ damage, and adequacy of blood pressure control. Follow-up visits may include an interval history, limited physical examination, radiologic evaluation, and laboratory testing. The frequency and nature of follow-up hypertension evaluations will vary according to the presence or absence of preexisting risk factors, evidence of end-organ damage, the nature of the treatment the patient is receiving, and the stability of blood pressure control. Unfortunately, there is little evidence to support specific recommendations for the frequency and nature of follow-up hypertension evaluations.
In the absence of evidence, several general principles may be suggested. Patients should be seen within 2 months of initiation of treatment. Follow-up history should focus on the cardiovascular and neurologic review of systems. The examination should include a focused cardiovascular work-up (eg, retinopathy, carotid bruits). Consideration should be given to periodic laboratory testing for diabetes, renal insufficiency, and hyperlipidemia. Periodic (but less frequent) chest x-rays and electrocardiograms may be helpful to detect cardiomegaly, but there is no evidence to support such testing in the absence of symptoms.
Follow-up visits should be more frequent among patients who have marginal blood pressure control, preexisting risk factors, or end-organ damage. Evaluations may be less frequent among those with good control and no preexisting risk factors or endorgan damage. Office visits and testing should be more frequent whenever changes are made in treatment. The frequency and nature of follow-up testing will also depend on the nature of treatment. Patients taking diuretics should have their potassium levels checked periodically. Renal function and potassium should be monitored in patients who are taking ACE inhibitors, especially during the first few weeks of therapy.
Patients willing to regularly monitor their blood pressure at home may require less frequent follow-up than those who leave it to the physician to check. Patients who monitor their blood pressure at home should have their sphygmomanometers validated initially and periodically.44 It is important to remember that home blood pressure measurements are consistently lower and more closely correlated with cardiovascular outcomes than are clinic blood pressure measurements.45-47
Prognosis
It is difficult to estimate the precise impact blood pressure control has on morbidity and mortality, but it is clear that high blood pressure, if unrecognized or untreated, substantially increases the morbidity and mortality associated with coronary disease, heart failure, renal failure, and stroke.17 In an early study of untreated hypertension there was a close relationship between blood pressure level and cardiovascular morbidity over 14 years of observation. This study revealed that hypertensive patients (those with a blood pressure of 160/95) had cardiovascular morbidity rates (coronary artery disease, claudication, stroke, and congestive heart failure) 2 to 3 times higher than normotensive patients.48 The impact of inadequately controlled blood pressure on morbidity and mortality among patients with diabetes is especially problematic.49 Over 9 years, when compared with diabetic patients with less tight control (< 180/105 mm Hg), those with tight blood pressure control (< 150/85 mm Hg) had a 24% reduction in sudden death, hyperglycemic or hypoglycemic death, fatal or nonfatal myocardial infarction, angina, heart failure, fatal or nonfatal stroke, renal failure, amputation, vitreous hemorrhage, and retinal hemorrhage.
Finally, renal function deteriorates more rapidly when blood pressure control is inadequate in patients with chronic renal disease of diverse causes.20 Over 2 years, when compared with patients with renal failure who had less tight control (mean arterial pressure 107 mm Hg), renal failure patients with tight control (mean arterial blood pressure 92 mm Hg) had significantly less proteinuria and lower rates of decline in renal function. Whether this translates into a significant improvement in the risk of end-stage renal disease is unknown.
- Only 53% of hypertensive patients are being treated, and only 24% have their hypertension under control.
- The first step in planning the treatment of a patient with essential hypertension is to categorize the patient’s risk status.
- The target blood pressure of patients who have diabetes or renal failure should be less than 130/85.
- Diuretics are safe, well tolerated, effective, relatively inexpensive, and convenient for initial drug treatment of hypertension in patients who do not have concomitant illness.
- Alpha-adrenergic blockers should be used with caution in the treatment of hypertension.
- Ambulatory blood pressure measurements predict cardiovascular events more closely than clinic blood pressure measurements.
Hypertension is arbitrarily defined as diastolic blood pressure (DBP) of 90 mm Hg or higher, systolic blood pressure (SBP) of 140 mm Hg or higher, or both, on 3 separate occasions. Essential hypertension is hypertension without an identifiable cause. Essential hypertension, also known as primary or idiopathic hypertension, accounts for at least 95% of all cases of hypertension.
According to the third National Health and Nutrition Examination Survey (NHANES III), approximately 60% of the 50 million Americans with hypertension are at increased risk for cardiovascular disease resulting from uncontrolled hypertension. This is because only 53% of hypertensive patients are being treated and only 24% have their hypertension under control.1 Physicians must play an active role in identifying and treating hypertension.
In an earlier Applied Evidence article2 an approach to the diagnosis of hypertension was presented. This article reviews the treatment of essential hypertension in adults and the prognosis of untreated hypertension. Risk stratification, alternative therapies, lifestyle modification, drug therapy, and prognosis will each be reviewed sequentially.
Risk stratification
The decision to treat hypertension and the choice of treatment is affected by the patient’s risk of morbidity and mortality if the blood pressure remains untreated or under-treated. According to the recommendations of the sixth report of the Joint National Committee on the Prevention, Diagnosis, Evaluation, and Treatment of High Blood Pressure (JNC-VI), the first step in planning treatment of a patient with essential hypertension is to categorize the patient’s risk status.3 The patient is placed in 1 of 9 treatment categories according to his or her blood pressure category, cardiovascular risk factors, and evidence of end-organ damage found during the initial evaluation (Table 1). Once the treatment category is identified, initial treatment should begin (Figure 1). Subsequent treatment depends on the patient’s response to initial treatment (Figure 2).
Patients should be monitored regularly to be sure they do not develop signs and symptoms that would place them in a different category and mandate more aggressive treatment. After a patient’s blood pressure has been controlled for 1 year, it may be possible to decrease the dose or the number of antihypertensive drugs—especially among patients who make significant lifestyle changes.4
The effectiveness of therapy varies depending on the patient’s cardiovascular risk. The New Zealand Guidelines Group has developed a helpful risk calculator based on the Framingham Heart Study for estimating a patient’s cardiovascular risk. This calculator incorporates sex, age, systolic blood pressure, smoking status, total cholesterol, high-density lipoprotein cholesterol, presence or absence of diabetes, and presence or absence of electrocardiogram evidence of left ventricular hypertrophy. This helpful risk calculator may be downloaded from the Web site of the New Zealand Guidelines Group at http://www.nzgg.org.nz/library/gl_complete/bloodpressure/appendix.cfm#app3. Alternatively, the University of Sheffield Medical School has developed tables to estimate an individual’s risk of heart disease based on cardiovascular risk factors including age, sex, cholesterol level, and presence or absence of smoking, hypertension, and diabetes—Sheffield tables.5 Software for handheld computers (Palm and PocketPC) that helps you estimate risk is available at www.jfponline.com.
Regardless of the method used, the benefit of treatment increases steadily as the patient’s current cardiovascular risk increases. With a 5-year cardiovascular risk of less than 2.5%, more than 120 patients have to be treated for 5 years to prevent 1 cardiovascular event; this number decreases to 25 patients with a risk of between 5% and 10%, and only 13 with a risk of between 20% and 24%.6 It is tempting to assume that the benefit of hypertension treatment is related to reduction in blood pressure whether achieved by drug therapy, lifestyle modification, or alternative therapy. However, this has not been established and it is important to consider the evidence supporting the benefit of each of these therapeutic options (Table 2).
TABLE 1
HYPERTENSION RISK STRATIFICATION AND TREATMENT CATEGORIES
| Blood Pressure Category | Risk Group A* | Risk Group B* | Risk Group C* |
|---|---|---|---|
| High-normal (130 – 139/85 – 89) | Lifestyle modification† | Lifestyle modification | Lifestyle modification and drug therapy |
| Stage 1 (140 – 159/0 – 99) | Lifestyle modification (12-month trial) | Lifestyle modification (6-month trial) | Lifestyle modification and drug therapy |
| Stage 2 or 3 (≥ 160 / ≤100) | Lifestyle modification and drug therapy | Lifestyle modification and drug therapy | Lifestyle modification and drug therapy |
| *Risk groups: A = no risk factors, end-organ damage, or clinical cardiovascular disease; B = 1 risk factor other than diabetes, no end-organ damage, and no clinical cardiovascular disease; C = Diabetes, end-organ damage, or clinic cardiovascular disease. | |||
| † Lifestyle modification should be included in the treatment plan of all patients receiving drug therapy. | |||
FIGURE 1
ALGORITHM FOR INITIAL MANAGEMENT OF HYPERTENSION
FIGURE 2
ALGORITHM FOR SUBSEQUENT MANAGEMENT OF HYPERTENSION
TABLE 2
NUMBER NEEDED TO TREAT (NNT) FOR SPECIFIC ANTIHYPERTENSIVE TREATMENTS
| Medication | Level of Evidence | NNT (95% CI)* | Comment |
|---|---|---|---|
| Low-Dose Thiazide | 1a | 18 (14-23) | Adults with systolic blood pressure |
| ≥ 160 or diastolic blood pressure | |||
| ≥90 regardless of age or comorbidities. | |||
| High-Dose Thiazide | 1a | 67 (48-111) | |
| Beta-Blocker | 1a | 142 (71-1000) | Drug vs no treatment comparison.14 |
| Calcium-Channel Blockers | 1b | 45 (30-102) | Isolated systolic hypertension in older patients, drug vs no treatment comparison.22 |
| ACE inhibitors | 1b | NS | Captopril versus diuretic or ß-blocker. |
| Alpha-agonists | 1b | NS | Doxazosin versus chlorthalidone, increased congestive heart in doxazosin group.7 |
| ARBs | NA | NA | Patient-oriented outcomes not available. |
| Sodium Restriction | 1a | NA | May reduce blood pressure but lacks evidence of reduced morbidity or mortality.27-35 |
| Weight Loss | 1a | NA | |
| Exercise | 1a | NA | |
| Low-Fat Diet | 1b | NA | |
| Limited Alcohol | 5 | NA | |
| Potassium Supplement | 1a | NA | |
| Fish Oil Supplement | 1a | NA | |
| Acupuncture | NA | NA | No evidence of blood pressure reduction or reduced morbidity or mortality.36-43 |
| Biofeedback | NA | NA | |
| Herbal Medicine | NA | NA | |
| Transcendental Meditation | NA | NA | |
| Yoga | NA | NA | |
| *For total cardiovascular events over 5 years. | |||
| NS denotes no significant difference from comparison drug; NA, not applicable; ACE, angiotensin-converting enzyme; ARBs, angiotensin-receptor blockers. | |||
Treatment
Drug Therapy
Patients who require drug treatment for hypertension should begin with a low dose of the initial medication, and that dose should be slowly titrated upward every 1 to 2 months (Figure 2). The JNC-VI recommends a diuretic or a ß-blocker with once daily dosing and 24-hour efficacy as the initial treatment for most hypertensive patients. However, the choice of initial medication will be affected by concomitant illnesses: (1) ß-blockers are recommended for the initial treatment of patients with hypertension and a history of coronary artery disease; (2) diuretics are suggested for the initial treatment of isolated systolic hypertension; (3) and angiotensin-converting enzyme (ACE) inhibitors are recommended for hypertensive patients who have systolic dysfunction after myocardial infarction, diabetic nephropathy, or congestive heart failure. Angiotensin II receptor blockers may be used in patients who cannot tolerate ACE inhibitors because of cough or rash. Alpha-adrenergic blockers should be used with caution in light of evidence that they may increase the risk of cardiovascular events (especially congestive heart failure).7
Among patients who do not have concomitant illness, the choice of drug therapy is controversial. A case-control study and a meta-analysis suggested that short-acting calcium channel blockers (CCBs) increase cardiovascular mortality.8,9 Unfortunately, these studies were not designed to establish a causal relationship. A recent nonsystematic review suggested that short-acting CCBs should be avoided and that conventional therapies were more effective than long-acting CCBs.10 An earlier non-systematic review suggested that short- and intermediate-acting CCBs were associated with increased cardiovascular mortality and morbidity. However, a well-designed cohort study of patients with coronary artery disease failed to reveal an increase in adverse effects among patients taking short-acting CCBs.11 Furthermore, randomized controlled trials suggest that diuretics, ß-blockers, and long-acting CCBs are equally effective in preventing cardiovascular mortality and morbidity.12,13 Physicians who treat hypertension must choose the best initial treatment for patients who do not have concomitant illness. Fortunately, safety, tolerability, efficacy, price, and simplicity can guide the physician to an ideal drug for most hypertensive patients.
Low-dose thiazide diuretics (the equivalent of 25 to 50 mg of hydrochlorothiazide) appear better tolerated than ß-blockers or CCBs.14 Treatment with ß-blockers, CCBs, and ACE inhibitors is also more expensive (75% to 85% more) than diuretic therapy.15 The cost savings offered by diuretics complement the fact that diuretics are safe, effective, and may be dosed once daily. In short, in addition to being the drug of choice for isolated systolic hypertension, low-dose thiazide diuretics are the ideal initial drug treatment of patients without concomitant illness. It should be noted that higher doses of thiazide diuretics offer proportionately less blood pressure reduction and greater risk of hypokalemia.16
Antihypertensive treatment reduces morbidity and mortality for all stages of hypertension, but people with the greatest baseline cardiovascular risk (eg, older patients and patients with higher levels of blood pressure) have the most to gain from treatment.17,18 There is no conclusive evidence to suggest that lowering blood pressure to below 140/80 reduces morbidity or mortality in most patients. However, patients who have diabetes or renal failure benefit from more aggressive management of blood pressure.19,20 Therefore, the JNC-VI recommends a target blood pressure of less than 130/85 for these patients.
The JNC-VI recommendation to start with a low-dose diuretic is supported by the evidence across a spectrum of patient-oriented outcomes. The effectiveness of diuretics and ß-blockers as first-line agents has been confirmed by long-term clinical trials.14,21 However, low-dose thiazides appear effective against a broader range of outcomes than high-dose thiazides and ß-blockers (Table 3). There is also evidence to suggest that CCBs and ACE inhibitors may be effective first-line agents, but fewer patients have been studied who take CCBs and ACE inhibitors than those who take diuretics and ß-blockers.22,23
Most patients with hypertension will respond to 1 (approximately 50%) or 2 (approximately 30%) antihypertensive medications.19,24,25 As noted earlier, failure to respond to treatment suggests an identifiable cause of hypertension. Among patients who do not have a secondary cause of hypertension, inadequate drug treatment (often failure to start a diuretic) and noncompliance are among the most common causes of resistant hypertension.26
When patients who are receiving drug therapy fail to reach the target blood pressure goal or fail to maintain the blood pressure goal, they should have the initial drug dose increased until the goal is reached (Figure 2). Those who fail initial drug therapy at full doses should have a second drug added and increased until the blood pressure goal is reached. Those who fail initial and second drug therapy at full doses should have a third drug added and increased until the pressure goal is reached. Patients who fail to reach the goal on maximal doses of 3 drugs have, by definition, resistant hypertension and will require evaluation by a physician with expertise in managing resistant hypertension. A cause should be sought each time a patient fails to respond to a drug or fails to maintain blood pressure control on a drug that had previously controlled the pressure (Table 3).
TABLE 3
PARTIAL LISTING OF CAUSES OF FAILURE TO REACH OR MAINTAIN TARGET BLOOD PRESSURE
| Volume overload: failure to start a diuretic |
| Nonadherence to therapy: dementia, side effects, complex regimen |
| Drug-induced: prescription, over-the-counter, herbal, or illicit drugs |
| Diet/stimulant induced: caffeine, licorice, salt, alcohol, nicotine |
| Associated conditions: obesity, sleep apnea, anxiety, chronic pain |
| Identifiable causes: chronic renal disease, renovascular disease, hyperaldosteronism, Cushing’s syndrome, pheochromocytoma |
| Pseudoresistance: wrong cuff size, white-coat hypertension |
Lifestyle modifications
Several lifestyle modifications are recommended in all treatment categories. Aerobic exercise (45 to 60 minutes at least 3 days per week), low-salt, low-fat, and high fruit and vegetable diet, limited alcohol consumption (less than 3 drinks per day), and modest weight loss (3% to 9% of total body weight) have been demonstrated to yield modest blood pressure reductions, but there is insufficient evidence to suggest that these measures alone reduce morbidity or mortality in hypertensive patients.27-33 A systematic review of randomized controlled trials found an average 4.4/2.5 mm Hg reduction in blood pressure with no evidence of harm (among patients who were not at risk for hyperkalemia) when diet was supplemented with about 2000 mg of potassium daily.34 A comparable reduction in blood pressure was seen with a daily supplement of more than 3 grams of fish oil.35 Research concerning the value of calcium and magnesium supplementation is conflicting and insufficient for supplementation to be considered standard therapy at this time.
Alternative therapy
The number and the quality of studies evaluating acupuncture, biofeedback, herbal medicine, transcendental meditation, and yoga are, for the most part, limited. They have focused on reduction in blood pressure, not patient-oriented outcomes, such as a reduction in morbidity and mortality. Acupuncture does not appear to have a significant effect on blood pressure levels.36,37 Biofeedback and other behavioral techniques have not been demonstrated to reduce blood pressure.38,39 The effect of garlic on blood pressure is unclear with mixed study results.40,41 Transcendental meditation and yoga may reduce blood pressure, but studies of these modalities are small and the experimental designs have a limited capacity to detect an independent treatment effect or a placebo effect.42,43
Therefore, physicians who include any of these modalities in their hypertension treatment plan should carefully monitor each patient for adequacy of blood pressure control, development of risk factors, and evidence of end-organ damage. At this time, alternative therapies should be considered experimental adjuncts to lifestyle modification and medical therapy that have not been shown to improve patient-oriented outcomes.
Follow-up of patients with hypertension
Follow-up visits should be designed to identify new risk factors, evidence of end-organ damage, and adequacy of blood pressure control. Follow-up visits may include an interval history, limited physical examination, radiologic evaluation, and laboratory testing. The frequency and nature of follow-up hypertension evaluations will vary according to the presence or absence of preexisting risk factors, evidence of end-organ damage, the nature of the treatment the patient is receiving, and the stability of blood pressure control. Unfortunately, there is little evidence to support specific recommendations for the frequency and nature of follow-up hypertension evaluations.
In the absence of evidence, several general principles may be suggested. Patients should be seen within 2 months of initiation of treatment. Follow-up history should focus on the cardiovascular and neurologic review of systems. The examination should include a focused cardiovascular work-up (eg, retinopathy, carotid bruits). Consideration should be given to periodic laboratory testing for diabetes, renal insufficiency, and hyperlipidemia. Periodic (but less frequent) chest x-rays and electrocardiograms may be helpful to detect cardiomegaly, but there is no evidence to support such testing in the absence of symptoms.
Follow-up visits should be more frequent among patients who have marginal blood pressure control, preexisting risk factors, or end-organ damage. Evaluations may be less frequent among those with good control and no preexisting risk factors or endorgan damage. Office visits and testing should be more frequent whenever changes are made in treatment. The frequency and nature of follow-up testing will also depend on the nature of treatment. Patients taking diuretics should have their potassium levels checked periodically. Renal function and potassium should be monitored in patients who are taking ACE inhibitors, especially during the first few weeks of therapy.
Patients willing to regularly monitor their blood pressure at home may require less frequent follow-up than those who leave it to the physician to check. Patients who monitor their blood pressure at home should have their sphygmomanometers validated initially and periodically.44 It is important to remember that home blood pressure measurements are consistently lower and more closely correlated with cardiovascular outcomes than are clinic blood pressure measurements.45-47
Prognosis
It is difficult to estimate the precise impact blood pressure control has on morbidity and mortality, but it is clear that high blood pressure, if unrecognized or untreated, substantially increases the morbidity and mortality associated with coronary disease, heart failure, renal failure, and stroke.17 In an early study of untreated hypertension there was a close relationship between blood pressure level and cardiovascular morbidity over 14 years of observation. This study revealed that hypertensive patients (those with a blood pressure of 160/95) had cardiovascular morbidity rates (coronary artery disease, claudication, stroke, and congestive heart failure) 2 to 3 times higher than normotensive patients.48 The impact of inadequately controlled blood pressure on morbidity and mortality among patients with diabetes is especially problematic.49 Over 9 years, when compared with diabetic patients with less tight control (< 180/105 mm Hg), those with tight blood pressure control (< 150/85 mm Hg) had a 24% reduction in sudden death, hyperglycemic or hypoglycemic death, fatal or nonfatal myocardial infarction, angina, heart failure, fatal or nonfatal stroke, renal failure, amputation, vitreous hemorrhage, and retinal hemorrhage.
Finally, renal function deteriorates more rapidly when blood pressure control is inadequate in patients with chronic renal disease of diverse causes.20 Over 2 years, when compared with patients with renal failure who had less tight control (mean arterial pressure 107 mm Hg), renal failure patients with tight control (mean arterial blood pressure 92 mm Hg) had significantly less proteinuria and lower rates of decline in renal function. Whether this translates into a significant improvement in the risk of end-stage renal disease is unknown.
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the third national health and nutrition examination survey, 1988-1991. Hypertension 1995;25:305-13.
2. Dosh S. The diagnosis of essential and secondary hypertension in adults. J Fam Pract 2001;50:707-12.
3. Joint National Committee on the Prevention Detection. Evaluation and Treatment of High Blood Pressure. the sixth report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
4. Whelton P, Appelgate W, Ettinger W, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of non-pharmacologic interventions in the elderly (TONE). JAMA 1996;279:839-46.
5. Wallis E, Ramsay L, Haq I, Ghahramani P, Jackson P. Coronary and cardiovascular risk estimation for the primary prevention: validation of a new Sheffield table in the 1995 Scottish health survey. Br Med J 2000;320:671-76.
6. Baker S, Priest P, Jackson R. Using thresholds based on risk of cardiovascular disease to target treatment for hypertension: modelling events averted and number treated. Br Med J 2000;320:680-85.
7. ALLHAT Collaborative Research Group. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone. J Am Med Assoc 2000;283:1967-75.
8. Psaty B, Heckbert S, Koepsell T, et al. The risk of myocardial infarction associated with anti-hypertensive drug therapies. JAMA 1995;274:620-25.
9. Furberg C, Psaty B, Meyer J. Nifedipine: dose related increase in mortality in patients with coronary heart disease. Circulation 1995;92:1326-31.
10. Kizer J, Kimmel S. Epidemiologic review of the calcium channel blocker drugs. Arch Intern Med 2001;161:1145-58.
11. Braun S, Boyo V, Behar S, et al. Calcium antagonists did not increase mortality in patients with coronary artery disease. J Am Coll Cardiol 1996;28:7-11.
12. Hansson L, Hedner T, Lund-Johansen P, et al. Randomized trial of effects of calcium antagonists compared with diuretics and B-blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000;356:359-65.
13. Hansson L, Lindholm L, Ekbohm T, Dahlof B. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity. The Swedish trial in old patients with hypertension-2 study. Lancet 1999;354:1751-56.
14. Wright J, Lee C, Chambers G. Systematic review of antihypertensive therapies: does evidence assist in choosing a first-line drug? Can Med Assoc J 1999;161:25-32.
15. Ramsey S, Niel N, Sullivan S, Perfetto E. An economic evaluation of the JNC hypertension guidelines using data from a randomized controlled trial. J Am Board Fam Pract 1999;12:105-14.
16. Wright J. Choosing a first-line drug in the management of elevated blood pressure: What is the evidence?: 1 Thiazide diuretics. Can Med Assoc J 2000;163:57-60.
17. Gueyffier F, Froment A, Gouton M. New meta-analysis of treatment trials of hypertension: improving the estimate of therapeutic benefit. J Hum Hypertens 1996;10:1-8.
18. Mulrow C, Cornell J, Herrera C, Kadri A, Farnett L, Aguilar C. Hypertension in the elderly: implications and generalizability of randomized trials. JAMA 1994;272:1932-38.
19. Hansson L, Zanchetti A, Carruthers S, Dahlof B. Effects of intensive blood pressure lowering and low dose aspirin in patients with hypertension: principal results of the hypertension optimal treatment (HOT) randomised trial. Lancet 1998;351:1755-62.
20. Peterson J, Adler S, Burkart J, Greene J. Blood pressure control, proteinuria, and the progression of renal disease. Ann Intern Med 1995;123:754-62.
21. Psaty B, Smith N, Siscovick D, Koepsell T, Weiss N. Health outcomes associated with antihypertensive therapies used as first-line agents: A systematic review and meta-analysis. J Am Med Assoc 1197;277:739-45.
22. Staessen J, Fagard R, Celis H, Arabidze C, Birkenhager W. Randomised double-blind comparison of placebo and active treatment in older patients with isolated systolic hypertension. Lancet 1997;350:757-64.
23. Investigators THOPES. Effect of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. New Eng J Med 2000;342:145-53.
24. Masterson B, Reda D, Preston R, et al. Response to a second single antihypertensive agent used as monotherapy for hypertension after failure of the initial drug. Arch Intern Med 1995;155:1757-62.
25. Tuomilehto J, Rastenyte D, Birkenhager W, et al. Systolic hypertension in Europe trial investigators. Effects of calcium-channel blockers in older patients with diabetes and systolic hypertension. New Eng J Med 1999;340:677-84.
26. Yakovlevitch M, Black HR. Resistant hypertension in a tertiary care clinic. Arch Intern Med 1991;151:1786-92.
27. Halbert J, Silagy C, Finucane P, Withers R. The effectiveness of exercise training in lowering blood pressure: a metaanalysis of randomized controlled trials of 4 weeks or longer. J Human Hypertension 1997;10:641-49.
28. Ebrahim S, Davey G. Lowering blood pressure: a systematic review of sustained effects of non-pharmacologic interventions. J Public Health Med 1998;4:441-48.
29. Appel L, Moore T, Obarzanek E, Vollmer W. A clinical trail of the effects of dietary patterns on blood pressure. New Eng J Med 1997;336:1117-24.
30. Appel L, Espeland M, Easter L, Wilson A, Folmar S, Lacy C. Effects of reduced sodium intake on hypertension control in older individuals. Results from the trial of nonpharmacologic interventions in the elderly (TONE). Arch Intern Med 2001;161:685-93.
31. Beilin L, Puddey I, Burke V. Alcohol and hypertension: kill or cure? J Human Hypertension 1996;10(Suppl 2):1-5.
32. Corrigan S, Raczynski J, Swencionis C, Jennings S. Weight reduction in the prevention and treatment of hypertension: a review of representative clinical trials. Am J Health Promo 1991;5:208-14.
33. Mulrow C, Chiquette E, Angel L, Cornell J. Dieting to reduce body weight for controlling hypertension in adults. The Cochrane Library 2001.
34. Whelton P, He J, Cutler J, Brancati F, Appel L. Effects of oral potassium on blood pressure: meta-analysis of randomized controlled trials. JAMA 1997;277:1624-32.
35. Morris M, Sacks F, Rosner B. Regulation on blood pressure: does fish oil lower blood pressure?: analysis of controlled trials. Circulation 1993;88:523-33.
36. Sugioka K, Woods M, Mueller R. An unsuccessful attempt to treat hypertension with acupuncture. Am J Chinese Med 1977;5:39-44.
37. Kraft K, Coulon S. Effect of a standardized acupuncture treatment on complaints, blood pressure, and serum lipids of hypertensive, postmenopausal women. A randomized controlled clinical study. Forschende Komplementarmedizin 1999;6:74-79.
38. Eisenberg D, Delblanco T, Berkey C, et al. Cognitive and behavioral techniques and hypertension: a meta-analysis. Ann Intern Med 1993;118:964-72.
39. Hunyor S, Henderson R, Saroj K, Carter N, et al. Placebo-controlled biofeedback blood pressure effect in hypertensive humans. Hypertension 1997;29:1225-31.
40. Auer W. Hypertension and hyperlipidemia: garlic helps in mild cases. Br J Clin Pract 1990;69(Suppl):3-6.
41. Ackerman R, Mulrow C, Ramirez G, Gardner C, Mobidoni L, Lawrence V. Garlic shows promise for improving some cardiovascular risk factors. Arch Intern Med 2001;161:813-24.
42. Patel C. Twelve-month follow-up of yoga and bio-feedback in the management of hypertension. Lancet 1975;1:62-64.
43. Sundar S, Agrawal S, Singh V, Bhattacharya S, et al. Role of yoga in management of essential hypertension. Acta Cardiologica 1984;39:203-08.
44. White W, Berson A, Robbins C, Jamieson M, Prisant L. National standard for measurement of resting and ambulatory blood pressure with automated sphygmomanometers. Hypertension 1993;21:504-09.
45. Staessen J, Byttebier G, Butinx F, Celis H, O’Brien E. Antihypertensive treatment based on conventional or ambulatory blood pressure measurement. J Am Med Assoc 1997;278:1065-72.
46. Ohkubo T, Imai Y, Tsuji I, Nagai K, Ito S. Reference values for 24-hour ambulatory blood pressure monitoring based on a prognostic criterion: the Ohasma study. Hypertension 1998;32:255-59.
47. Staessen J, Thijs L, Fagard R, O’Brien E, Eoin T. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. JAMA 1999;282:539-46.
48. Kannel W, Wolf P, Verter J, McNamara P. Epidemiologic assessment of the role of blood pressure in stroke: the Framingham study. JAMA 1970;214:301-10.
49. Turner R, Holman R, Stratton I, Cull C. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. Br Med J 1998;317:703-12.
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the third national health and nutrition examination survey, 1988-1991. Hypertension 1995;25:305-13.
2. Dosh S. The diagnosis of essential and secondary hypertension in adults. J Fam Pract 2001;50:707-12.
3. Joint National Committee on the Prevention Detection. Evaluation and Treatment of High Blood Pressure. the sixth report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
4. Whelton P, Appelgate W, Ettinger W, et al. Sodium reduction and weight loss in the treatment of hypertension in older persons: a randomized controlled trial of non-pharmacologic interventions in the elderly (TONE). JAMA 1996;279:839-46.
5. Wallis E, Ramsay L, Haq I, Ghahramani P, Jackson P. Coronary and cardiovascular risk estimation for the primary prevention: validation of a new Sheffield table in the 1995 Scottish health survey. Br Med J 2000;320:671-76.
6. Baker S, Priest P, Jackson R. Using thresholds based on risk of cardiovascular disease to target treatment for hypertension: modelling events averted and number treated. Br Med J 2000;320:680-85.
7. ALLHAT Collaborative Research Group. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone. J Am Med Assoc 2000;283:1967-75.
8. Psaty B, Heckbert S, Koepsell T, et al. The risk of myocardial infarction associated with anti-hypertensive drug therapies. JAMA 1995;274:620-25.
9. Furberg C, Psaty B, Meyer J. Nifedipine: dose related increase in mortality in patients with coronary heart disease. Circulation 1995;92:1326-31.
10. Kizer J, Kimmel S. Epidemiologic review of the calcium channel blocker drugs. Arch Intern Med 2001;161:1145-58.
11. Braun S, Boyo V, Behar S, et al. Calcium antagonists did not increase mortality in patients with coronary artery disease. J Am Coll Cardiol 1996;28:7-11.
12. Hansson L, Hedner T, Lund-Johansen P, et al. Randomized trial of effects of calcium antagonists compared with diuretics and B-blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000;356:359-65.
13. Hansson L, Lindholm L, Ekbohm T, Dahlof B. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity. The Swedish trial in old patients with hypertension-2 study. Lancet 1999;354:1751-56.
14. Wright J, Lee C, Chambers G. Systematic review of antihypertensive therapies: does evidence assist in choosing a first-line drug? Can Med Assoc J 1999;161:25-32.
15. Ramsey S, Niel N, Sullivan S, Perfetto E. An economic evaluation of the JNC hypertension guidelines using data from a randomized controlled trial. J Am Board Fam Pract 1999;12:105-14.
16. Wright J. Choosing a first-line drug in the management of elevated blood pressure: What is the evidence?: 1 Thiazide diuretics. Can Med Assoc J 2000;163:57-60.
17. Gueyffier F, Froment A, Gouton M. New meta-analysis of treatment trials of hypertension: improving the estimate of therapeutic benefit. J Hum Hypertens 1996;10:1-8.
18. Mulrow C, Cornell J, Herrera C, Kadri A, Farnett L, Aguilar C. Hypertension in the elderly: implications and generalizability of randomized trials. JAMA 1994;272:1932-38.
19. Hansson L, Zanchetti A, Carruthers S, Dahlof B. Effects of intensive blood pressure lowering and low dose aspirin in patients with hypertension: principal results of the hypertension optimal treatment (HOT) randomised trial. Lancet 1998;351:1755-62.
20. Peterson J, Adler S, Burkart J, Greene J. Blood pressure control, proteinuria, and the progression of renal disease. Ann Intern Med 1995;123:754-62.
21. Psaty B, Smith N, Siscovick D, Koepsell T, Weiss N. Health outcomes associated with antihypertensive therapies used as first-line agents: A systematic review and meta-analysis. J Am Med Assoc 1197;277:739-45.
22. Staessen J, Fagard R, Celis H, Arabidze C, Birkenhager W. Randomised double-blind comparison of placebo and active treatment in older patients with isolated systolic hypertension. Lancet 1997;350:757-64.
23. Investigators THOPES. Effect of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. New Eng J Med 2000;342:145-53.
24. Masterson B, Reda D, Preston R, et al. Response to a second single antihypertensive agent used as monotherapy for hypertension after failure of the initial drug. Arch Intern Med 1995;155:1757-62.
25. Tuomilehto J, Rastenyte D, Birkenhager W, et al. Systolic hypertension in Europe trial investigators. Effects of calcium-channel blockers in older patients with diabetes and systolic hypertension. New Eng J Med 1999;340:677-84.
26. Yakovlevitch M, Black HR. Resistant hypertension in a tertiary care clinic. Arch Intern Med 1991;151:1786-92.
27. Halbert J, Silagy C, Finucane P, Withers R. The effectiveness of exercise training in lowering blood pressure: a metaanalysis of randomized controlled trials of 4 weeks or longer. J Human Hypertension 1997;10:641-49.
28. Ebrahim S, Davey G. Lowering blood pressure: a systematic review of sustained effects of non-pharmacologic interventions. J Public Health Med 1998;4:441-48.
29. Appel L, Moore T, Obarzanek E, Vollmer W. A clinical trail of the effects of dietary patterns on blood pressure. New Eng J Med 1997;336:1117-24.
30. Appel L, Espeland M, Easter L, Wilson A, Folmar S, Lacy C. Effects of reduced sodium intake on hypertension control in older individuals. Results from the trial of nonpharmacologic interventions in the elderly (TONE). Arch Intern Med 2001;161:685-93.
31. Beilin L, Puddey I, Burke V. Alcohol and hypertension: kill or cure? J Human Hypertension 1996;10(Suppl 2):1-5.
32. Corrigan S, Raczynski J, Swencionis C, Jennings S. Weight reduction in the prevention and treatment of hypertension: a review of representative clinical trials. Am J Health Promo 1991;5:208-14.
33. Mulrow C, Chiquette E, Angel L, Cornell J. Dieting to reduce body weight for controlling hypertension in adults. The Cochrane Library 2001.
34. Whelton P, He J, Cutler J, Brancati F, Appel L. Effects of oral potassium on blood pressure: meta-analysis of randomized controlled trials. JAMA 1997;277:1624-32.
35. Morris M, Sacks F, Rosner B. Regulation on blood pressure: does fish oil lower blood pressure?: analysis of controlled trials. Circulation 1993;88:523-33.
36. Sugioka K, Woods M, Mueller R. An unsuccessful attempt to treat hypertension with acupuncture. Am J Chinese Med 1977;5:39-44.
37. Kraft K, Coulon S. Effect of a standardized acupuncture treatment on complaints, blood pressure, and serum lipids of hypertensive, postmenopausal women. A randomized controlled clinical study. Forschende Komplementarmedizin 1999;6:74-79.
38. Eisenberg D, Delblanco T, Berkey C, et al. Cognitive and behavioral techniques and hypertension: a meta-analysis. Ann Intern Med 1993;118:964-72.
39. Hunyor S, Henderson R, Saroj K, Carter N, et al. Placebo-controlled biofeedback blood pressure effect in hypertensive humans. Hypertension 1997;29:1225-31.
40. Auer W. Hypertension and hyperlipidemia: garlic helps in mild cases. Br J Clin Pract 1990;69(Suppl):3-6.
41. Ackerman R, Mulrow C, Ramirez G, Gardner C, Mobidoni L, Lawrence V. Garlic shows promise for improving some cardiovascular risk factors. Arch Intern Med 2001;161:813-24.
42. Patel C. Twelve-month follow-up of yoga and bio-feedback in the management of hypertension. Lancet 1975;1:62-64.
43. Sundar S, Agrawal S, Singh V, Bhattacharya S, et al. Role of yoga in management of essential hypertension. Acta Cardiologica 1984;39:203-08.
44. White W, Berson A, Robbins C, Jamieson M, Prisant L. National standard for measurement of resting and ambulatory blood pressure with automated sphygmomanometers. Hypertension 1993;21:504-09.
45. Staessen J, Byttebier G, Butinx F, Celis H, O’Brien E. Antihypertensive treatment based on conventional or ambulatory blood pressure measurement. J Am Med Assoc 1997;278:1065-72.
46. Ohkubo T, Imai Y, Tsuji I, Nagai K, Ito S. Reference values for 24-hour ambulatory blood pressure monitoring based on a prognostic criterion: the Ohasma study. Hypertension 1998;32:255-59.
47. Staessen J, Thijs L, Fagard R, O’Brien E, Eoin T. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. JAMA 1999;282:539-46.
48. Kannel W, Wolf P, Verter J, McNamara P. Epidemiologic assessment of the role of blood pressure in stroke: the Framingham study. JAMA 1970;214:301-10.
49. Turner R, Holman R, Stratton I, Cull C. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. Br Med J 1998;317:703-12.
The Diagnosis of Essential and Secondary Hypertension in Adults
Hypertension is arbitrarily defined as a diastolic blood pressure (DBP) of 90 mm Hg or higher, a systolic blood pressure (SBP) equal to or higher than 140 mm Hg, or both, on 3 separate occasions. It affects 24% of the population of the United States and is common among black (28%), white (24%), and Hispanic (14%) Americans. The prevalence of hypertension increases with age and is more than 70% among people 65 years and older. Among principal diagnoses given by family physicians for outpatient visits, only acute respiratory tract infection (7%) is more common than hypertension (6%). The annual direct medical cost of caring for hypertension exceeds $10 billion.
This article will discuss the pathophysiology and diagnosis of hypertension from an evidence-based perspective. An upcoming Applied Evidence article will cover treatment of hypertension and prognosis.
Pathophysiology
Idiopathic, or essential, hypertension accounts for more than 95% of cases and appears to be caused by a complex interaction between genetic predisposition and environmental factors. The predisposition to essential hypertension is polygenic in origin and may find full expression when combined with environmental factors, such as obesity, low physical activity levels, high stress levels, high alcohol consumption, high dietary sodium, and low dietary potassium, calcium, and magnesium. The complex interaction of genetics and environment may affect sodium, catecholamines, the renin-angiotensin system, insulin, and cell membrane function, causing elevation of the blood pressure.
The more common identifiable causes of hypertension include chronic renal disease (2%-5%), renovascular disease—including renal artery atherosclerosis and fibromuscular dysplasia—(0.2%-0.7%), Cushing syndrome (0.1%-0.6%), pheochromocytoma (0.04%-0.1%), and primary hyperaldosteronism (0.01%-0.3%). Although obesity, excessive alcohol consumption, oral contraceptive therapy, and sleep apnea may cause hypertension, they are not typically included as identifiable causes of hypertension. The prevalence of the latter conditions as identifiable causes of hypertension remains to be defined.
Diagnosis
The presence of hypertension must be confirmed by blood pressure measurements obtained with proper technique. The blood pressure of all patients 18 years and older should be measured at each health care visit because of the high prevalence of hypertension. Patients should be encouraged to abstain from nicotine and caffeine for at least 30 minutes before the measurement of the blood pressure. Measurement should be made with a mercury sphygmomanometer or a recently calibrated aneroid device. The bladder of the blood pressure cuff should encircle 80% of the arm. The pressure should be taken after at least 5 minutes of rest with the patient sitting, back supported, and arm bared and supported at heart level. The first sound heard (phase 1) is the SBP, and the last sound heard (phase 5) is the DBP. Two readings separated by 2 minutes should be averaged. Hypertension is present when an accurately measured blood pressure is high on 3 separate occasions.
A major consensus report, the Sixth Report of the Joint National Committee on Prevention Detection, Evaluation, and Treatment of High Blood Pressure,11 designates 6 categories of blood pressure:
- Optimal—SBP less than 120 mm; DBP less than 80 mm
- Normal—SBP less than 130 mm; DBP less than 85 mm
- High normal—SBP is 130 to 139 mm; DBP is 85 to 89 mm
- Stage 1 hypertension—SBP is 140 to 159 mm; DBP is 90 to 99 mm
- Stage 2 hypertension—SBP is 160 to 179 mm; DBP is 100 to 109 mm
- Stage 3 hypertension—SBP is 180 mm or higher; DBP is 110 mm or higher
It is important to note that the recommended diagnostic evaluation is based on a consensus and should not be considered evidence-based. A complete history, physical examination, and limited diagnostic testing (urinalysis, complete blood count, potassium, sodium, fasting glucose, creatinine, total cholesterol, high-density cholesterol, and electrocardiogram) are recommended once the presence of hypertension has been confirmed. This evaluation has 3 purposes:
- Identify other cardiovascular risk factors. Most patients with hypertension have multiple cardiovascular risk factors at the time of initial evaluation. Risk factors include smoking, hyperlipidemia, diabetes, age older than 60 years, sex (men or postmenopausal women), and family history of cardiovascular disease in a female relative before age 65 years or a male relative before 55 years.
- Identify end-organ damage. Evidence of end-organ damage includes left ventricular hypertrophy, angina, previous myocardial infarction, previous angioplasty or coronary revascularization, heart failure, stroke or transient ischemic attack, nephropathy, peripheral arterial disease, and retinopathy.
- Identify secondary causes of hypertension. Estimating the pretest probability of a secondary (identifiable) cause of hypertension is problematic, because referral bias is a major problem in hypertension prevalence studies; patients are typically included in these studies only after being referred to a study center by their primary care physician for resistant or difficult to control hypertension. On the basis of the best available estimates, it would be reasonable to assume that patients presenting to primary care physicians have a 5% probability of an identifiable cause of hypertension.
The diagnostic evaluation serves to identify other cardiovascular risk factors and end-organ damage in patients with high-normal blood pressure or hypertension. This information is used to identify 3 risk groups: Group A includes patients with no other cardiovascular risk factor, cardiovascular disease, or evidence of end-organ damage; group B includes patients who do not have cardiovascular disease or end-organ damage but have 1 or more of the major risk factors other than diabetes mellitus; and group C includes patients who have cardiovascular disease, other end-organ damage, or diabetes mellitus. The risk associated with hypertension and the intensity of recommended treatment increases progressively as a person moves from risk group A through risk group C.
The diagnostic evaluation may also reveal patients who are more likely to have an identifiable cause of hypertension. The probability of an identifiable cause of hypertension is increased by the onset of hypertension outside the normal age for essential hypertension (30-55 years), sudden onset or worsening of hypertension, stage 3 hypertension, and blood pressure that responds poorly to treatment. Elevated creatinine levels suggest hypertension caused by renal parenchymal disease. Abdominal or flank bruits, hypokalemia, or a significant rise in the serum creatinine level after an angiotensin-converting enzyme inhibitor is started suggests renovascular hypertension. Osteoporosis, truncal obesity, moon face, purple striae, muscle weakness, easy bruising, hirsutism, hyperglycemia, hypokalemia, and hyperlipidemia suggest Cushing syndrome. Labile hypertension, orthostatic hypotension, headache, palpitations, pallor, and diaphoresis suggests pheochromocytoma. Isolated hypokalemia may be caused by hyperaldosteronism.
Unfortunately, the accuracy of the history, physical examination, and preliminary diagnostic testing for patients presenting with hypertension has not been adequately studied. Therefore, estimating the pretest probability of a secondary cause of hypertension in a patient with specific clinical characteristics must be considered crude at best. The best available evidence is shown in Table 1.
Diagnostic Strategy
Patients whose initial history, physical, and laboratory evaluation suggest the possibility of a secondary cause of hypertension should undergo additional testing. The search for the secondary cause of hypertension should focus on chronic renal disease, renovascular hypertension, pheochromocytoma, Cushing syndrome, and primary aldosteronism, depending on the clinical scenario Table 2.
Chronic renal disease will be evident from the blood urea nitrogen, creatinine, and the urinalysis results. The diagnostic approach to other causes of hypertension is more complicated.
Although renal artery stenosis is suggested by the presence of an abdominal or flank bruit, it is an insensitive test (sensitivity=65%; specificity=90%). It is useful when positive (positive likelihood ratio=6.5) but does not rule out renal artery stenosis when negative (negative likelihood ratio=0.4). A clinical decision rule has been developed and validated that integrates several findings from the history and physical examination. Software to implement this decision rule in clinical practice, using Palm or PocketPC hand-held computers, is available at no charge from the JFP Web site at PC download.
Duplex sonography is very accurate (sensitivity=98%; specificity=98%) when the study is adequate but is often nondiagnostic in obese patients. For these patients, magnetic resonance angiography (MRA) is better (sensitivity=93%; specificity=95%). Captopril renal scanning (CRS) is less sensitive and less specific than either sonography or MRA. Renal artery stenosis is confirmed by the highly accurate but more invasive reference standard test of conventional angiography.
Pheochromocytoma is rare even in the presence of suggestive symptoms (headache, palpitations, and excessive and inappropriate perspiration), but failure to identify this disease can have disastrous consequences. Therefore, patients who have suggestive signs and symptoms should be screened for pheochromocytoma. However, the standard for screening pheochromocytoma remains controversial. A 24-hour urinary metanephrine (cutoff point of >3.70 nmol/day ) is highly sensitive and specific when done well, but urine collection is inconvenient and may be incomplete. Plasma metanephrines (metanephrine >0.66 nmol/L or normetanephrine >0.30 nmol/L) are easy to obtain, 100% sensitive, and may represent a good screening test for pheochromocytoma. Because they have limited specificity (85%), a positive plasma metanephrine should be confirmed by the 24-hour urinary metanephrine-to-creatinine ratio (cutoff point of >0.354; specificity=98%) before proceeding to anatomical localization of the tumor.
Two imaging studies are commonly used to localize pheochromocytomas. Metaiodobenzylguanidine (MIBG) scintigraphy is more specific but less sensitive than computed tomography (CT). Relying on CT to guide surgery is less likely to miss tumors than MIBG scintigraphy (CT sensitivity = 100% vs MIBG=88%) but is more likely to result in unnecessary surgery because of the lower specificity (CT specificity = 50%; MIBG=89%).
The 24-hour urinary free cortisol (cutoff point >90 mg/day; sensitivity=100%; specificity=98%) is a useful screening test for Cushing syndrome. It is very sensitive, but false-positives may be seen in patients with depression and polycystic ovarian syndrome. The single-dose (1 mg) overnight dexamethasone suppression test is equally sensitive but is a little less specific than the 24-hour urinary cortisol. However, this test is relatively simple for patients. The patient takes 1 mg of dexamethasone at midnight, and the plasma cortisol level is drawn in the morning (cutoff point >100 nmol). The combined dexamethasone and corticotropin-releasing hormone (CRH) suppression test, which has both a sensitivity and a specificity of almost 100%, can be used to confirm the diagnosis of Cushing syndrome. However, it is a little more complicated for the patient. The patient takes 0.5 mg of dexamethasone at noon on the first day and repeats this dose every 6 hours for a total of 8 doses (ending at 6 am on the third day). Two hours after the last dose the patient is given an intravenous bolus of CRH (1 μg/kg), and 15 minutes later a plasma cortisol is drawn. A cortisol level greater than 38 nmol is the cutoff point for this test.
The coexistence of hypertension and spontaneous or diuretic-induced hypokalemia is strongly suggestive of primary aldosteronism. However, it is important to remember that many (if not most) patients with primary aldosteronism do not have hypokalemia. In the past, screening for primary aldosteronism was accomplished by measuring urinary aldosterone levels after oral or intravenous salt loading. The sensitivity of these tests is 90% to 95%, and they carry a risk of precipitous elevation of blood pressure due to volume expansion or hypokalemia. Measuring the plasma renin and aldosterone levels can be used to test for hyperaldosteronism. Various cut points and ratios have been suggested, but the plasma aldosterone-to-renin ratio (cutoff point >25) is currently the most useful screening test for hyperaldosteronism. For this test the patient is asked to rise at 6 am and remain ambulatory for 2 hours, at which time the plasma aldosterone and renin levels are drawn. Beta-blockers and dihydropyridine calcium channel blockers must be stopped for 2 weeks, and spironolactone and loop diuretics must be stopped for 6 weeks before the test. Primary aldosteronism can be confirmed by the fludrocortisone suppression test.
Acknowledgments
Special thanks to Kathleen Dosh, MS; Greg Tan, MD; and Mark Povich, DO, for help during the initial editing of this paper.
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension 1995;25:305-13.
2. Barker W, Mullooly J, Linton K. Trends in hypertension prevalence, treatment, and control: in a well-defined older population. Hypertension 1998;31:552-59.
3. Schappert S, Nelson C. National Ambulatory Medical Care Survey: 1995-96 summary. Vital Health Stat 1999;142:1-122.
4. Stason W. Opportunities to improve cost-effectiveness of treatment of hypertension. Hypertension 1991;18:1161-66.
5. Lander E, Schork N. Genetic dissection of complex traits. Science 1994;265:2037-48.
6. Stevens V, Obarzanek E, Cook N, Lee I-M. Long-term weight loss and changes in blood pressure: results of the trials of hypertension prevention, phase II. Ann Intern Med 2001;134:1-11.
7. Moore R, Levine D, Southard J, Entwisle G, Shapiro S. Alcohol consumption and blood pressure in the 1982 Maryland Hypertension Survey. Am J Hypertens 1990;3:1-7.
8. Chasan-Taber L, Willett W, Manson J, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996;94:483-89.
9. Nieto F, Young T, Lind B, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study: Sleep Heart Health Study. JAMA 2000;283:1829-36.
10. Reeves R. Does this patient have hypertension? How to measure blood pressure. JAMA 1995;273:1211-18.
11. Joint National Committee on Prevention. Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
12. Fuster V, Pearson T. 27th Bethesda conference: matching the intensity of risk factor management with the hazard for coronary disease events. September 14-15, 1995. J Am Coll Cardiol 1996;27:957-1047.
13. Rudnick K, Sackett D, Hirst S, Holmes C. Hypertension in a family practice. Can Med Assoc J 1977;117:492-97.
14. Sinclair A, Isles C, Brown I, Cameron H, Murray G, Robertson J. Secondary hypertension in a blood pressure clinic. Arch Intern Med 1987;147:1289-93.
15. Anderson G, Blakeman N, Streeten D. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens 1994;12:609-15.
16. Tucker R, Labarthe D. Frequency of surgical treatment for hypertension in adults at the Mayo Clinic from 1973 through 1975. Mayo Clin Proc 1977;52:549-55.
17. Gifford R. Evaluation of the hypertensive patient. Chest 1973;64:336-40.
18. Krjnen P, Jaarsveld B, Steyerberg E, Schalekamp M. A clinical prediction rule for renal artery stenosis. Ann Intern Med 1998;129:705-11.
19. Berglund AS, Hulthen UL, Manhem P, Thorsson O, Wollmer P, Tornquist C. Metaiodobenzylguanidine (MIBG) scintigraphy and computed tomography (CT) in clinical practice: primary and secondary evaluation for localization of phaeochromocytomas. J Intern Med 2001;249:247-51.
20. Yanovski J, Cutler G, Chrousos G, Nieman L. Corticotropin-releasing hormone stimulation following low-dose dexamethasone administration: a new test to distinguish Cushing’s syndrome from pseudo-Cushing’s states. JAMA 1993;269:2232-38.
21. Blumenfeld J, Sealey J, Schussel Y, Vaughan E. Diagnosis and treatment of primary aldosteronism. Ann Intern Med 1994;121:877-85.
22. Fardella C, Lorena M, Gomez-Sanchez C, Cortes J. Primary hyperaldosteronism in essential hypertensives: prevalence, biochemical profile, and molecular biology. J Clin Endocrinol Metabol 2000;85:1863-67.
23. Streeten D, Tomycz N, Anderson G. Reliability of screening methods for the diagnosis of primary aldosteronism. Am J Med 1979;67:403-13.
24. Bravo E, Tarazi R, Dustan H, Fouad F. The changing clinical spectrum of primary aldosteronism. Am J Med 1983;74:641-51.
25. Gordon R. Primary aldosteronism. J Endocrinol Invest 1995;18:495-511.
26. Anderson G, Blakeman N, Streeten D. Prediction of renovascular hypertension. Am J Hypertens 1988;1:301-04.
27. Manger W, Gifford R. Clinical and experimental pheochromocytoma. Cambridge, Mass: Blackwell Science; 1996.
28. Nugent C, Warner H, Dunn J, Tyler F. Probability theory in the diagnosis of Cushing’s syndrome. J Clin Endocrinol Metabol 1964;24:621-27.
29. Fishman L, Kuchel O, Liddle G, Michelakis A. Incidence of primary hyperaldosteronism in uncomplicated ‘essential’ hypertension. JAMA 1968;205:85-90.
30. Fenton S, Lyttle J, Pantridge J. Diagnosis and results of surgery in renovascular hypertension. Lancet 1966;2:117-21.
31. de Haan M, Kouwenhoven M, Thelissen G, Koster D. Renovascular disease in patients with hypertension: detection with systolic and diastolic gating in three-dimensional, phase-contrast MR angiography. Radiology 1996;198:449-56.
32. Olin J, Piedmonte M, Young J, DeAnna S. The utility of duplex ultrasound screening of renal arteries for diagnosing significant renal artery stenosis. Ann Intern Med 1995;122:833-38.
33. Setaro J, Chen C, Hoffer P, Black H. Captopril renography in the diagnosis of renal artery stenosis and the prediction of improvement with revascularization: the Yale Vascular Center experience. Am J Hypertens 1991;4:698S-705S.
34. Jacques W, Lenders M, Keiser H, Goldstein D. Plasma metanephrines in the diagnosis of pheochromocytoma. Ann Intern Med 1995;123:101-09.
35. Heron E, Chatellier G, Billaud E, Foos E. The urinary metanephrine-to-creatinine ratio for the diagnosis of pheochromocytoma. Ann Intern Med 1996;125:300-03.
36. Mengden T, Habmann P, Mullen J, Vetter W. Urinary free cortisol versus 17-hydroxysteroids: a comparative study of their diagnostic value in Cushing’s syndrome. Clin Invest 1992;70:545-48.
37. Montwill J, Igoe D, McKenna T. The overnight dexamethasone test is the procedure of choice in screening for Cushing’s syndrome. Steroids 1994;59:296-98.
38. Weinberger M, Fineberg N. The diagnosis of primary aldosteronism and separation of two major subtypes. Arch Intern Med 1993;153:2125-29.
Hypertension is arbitrarily defined as a diastolic blood pressure (DBP) of 90 mm Hg or higher, a systolic blood pressure (SBP) equal to or higher than 140 mm Hg, or both, on 3 separate occasions. It affects 24% of the population of the United States and is common among black (28%), white (24%), and Hispanic (14%) Americans. The prevalence of hypertension increases with age and is more than 70% among people 65 years and older. Among principal diagnoses given by family physicians for outpatient visits, only acute respiratory tract infection (7%) is more common than hypertension (6%). The annual direct medical cost of caring for hypertension exceeds $10 billion.
This article will discuss the pathophysiology and diagnosis of hypertension from an evidence-based perspective. An upcoming Applied Evidence article will cover treatment of hypertension and prognosis.
Pathophysiology
Idiopathic, or essential, hypertension accounts for more than 95% of cases and appears to be caused by a complex interaction between genetic predisposition and environmental factors. The predisposition to essential hypertension is polygenic in origin and may find full expression when combined with environmental factors, such as obesity, low physical activity levels, high stress levels, high alcohol consumption, high dietary sodium, and low dietary potassium, calcium, and magnesium. The complex interaction of genetics and environment may affect sodium, catecholamines, the renin-angiotensin system, insulin, and cell membrane function, causing elevation of the blood pressure.
The more common identifiable causes of hypertension include chronic renal disease (2%-5%), renovascular disease—including renal artery atherosclerosis and fibromuscular dysplasia—(0.2%-0.7%), Cushing syndrome (0.1%-0.6%), pheochromocytoma (0.04%-0.1%), and primary hyperaldosteronism (0.01%-0.3%). Although obesity, excessive alcohol consumption, oral contraceptive therapy, and sleep apnea may cause hypertension, they are not typically included as identifiable causes of hypertension. The prevalence of the latter conditions as identifiable causes of hypertension remains to be defined.
Diagnosis
The presence of hypertension must be confirmed by blood pressure measurements obtained with proper technique. The blood pressure of all patients 18 years and older should be measured at each health care visit because of the high prevalence of hypertension. Patients should be encouraged to abstain from nicotine and caffeine for at least 30 minutes before the measurement of the blood pressure. Measurement should be made with a mercury sphygmomanometer or a recently calibrated aneroid device. The bladder of the blood pressure cuff should encircle 80% of the arm. The pressure should be taken after at least 5 minutes of rest with the patient sitting, back supported, and arm bared and supported at heart level. The first sound heard (phase 1) is the SBP, and the last sound heard (phase 5) is the DBP. Two readings separated by 2 minutes should be averaged. Hypertension is present when an accurately measured blood pressure is high on 3 separate occasions.
A major consensus report, the Sixth Report of the Joint National Committee on Prevention Detection, Evaluation, and Treatment of High Blood Pressure,11 designates 6 categories of blood pressure:
- Optimal—SBP less than 120 mm; DBP less than 80 mm
- Normal—SBP less than 130 mm; DBP less than 85 mm
- High normal—SBP is 130 to 139 mm; DBP is 85 to 89 mm
- Stage 1 hypertension—SBP is 140 to 159 mm; DBP is 90 to 99 mm
- Stage 2 hypertension—SBP is 160 to 179 mm; DBP is 100 to 109 mm
- Stage 3 hypertension—SBP is 180 mm or higher; DBP is 110 mm or higher
It is important to note that the recommended diagnostic evaluation is based on a consensus and should not be considered evidence-based. A complete history, physical examination, and limited diagnostic testing (urinalysis, complete blood count, potassium, sodium, fasting glucose, creatinine, total cholesterol, high-density cholesterol, and electrocardiogram) are recommended once the presence of hypertension has been confirmed. This evaluation has 3 purposes:
- Identify other cardiovascular risk factors. Most patients with hypertension have multiple cardiovascular risk factors at the time of initial evaluation. Risk factors include smoking, hyperlipidemia, diabetes, age older than 60 years, sex (men or postmenopausal women), and family history of cardiovascular disease in a female relative before age 65 years or a male relative before 55 years.
- Identify end-organ damage. Evidence of end-organ damage includes left ventricular hypertrophy, angina, previous myocardial infarction, previous angioplasty or coronary revascularization, heart failure, stroke or transient ischemic attack, nephropathy, peripheral arterial disease, and retinopathy.
- Identify secondary causes of hypertension. Estimating the pretest probability of a secondary (identifiable) cause of hypertension is problematic, because referral bias is a major problem in hypertension prevalence studies; patients are typically included in these studies only after being referred to a study center by their primary care physician for resistant or difficult to control hypertension. On the basis of the best available estimates, it would be reasonable to assume that patients presenting to primary care physicians have a 5% probability of an identifiable cause of hypertension.
The diagnostic evaluation serves to identify other cardiovascular risk factors and end-organ damage in patients with high-normal blood pressure or hypertension. This information is used to identify 3 risk groups: Group A includes patients with no other cardiovascular risk factor, cardiovascular disease, or evidence of end-organ damage; group B includes patients who do not have cardiovascular disease or end-organ damage but have 1 or more of the major risk factors other than diabetes mellitus; and group C includes patients who have cardiovascular disease, other end-organ damage, or diabetes mellitus. The risk associated with hypertension and the intensity of recommended treatment increases progressively as a person moves from risk group A through risk group C.
The diagnostic evaluation may also reveal patients who are more likely to have an identifiable cause of hypertension. The probability of an identifiable cause of hypertension is increased by the onset of hypertension outside the normal age for essential hypertension (30-55 years), sudden onset or worsening of hypertension, stage 3 hypertension, and blood pressure that responds poorly to treatment. Elevated creatinine levels suggest hypertension caused by renal parenchymal disease. Abdominal or flank bruits, hypokalemia, or a significant rise in the serum creatinine level after an angiotensin-converting enzyme inhibitor is started suggests renovascular hypertension. Osteoporosis, truncal obesity, moon face, purple striae, muscle weakness, easy bruising, hirsutism, hyperglycemia, hypokalemia, and hyperlipidemia suggest Cushing syndrome. Labile hypertension, orthostatic hypotension, headache, palpitations, pallor, and diaphoresis suggests pheochromocytoma. Isolated hypokalemia may be caused by hyperaldosteronism.
Unfortunately, the accuracy of the history, physical examination, and preliminary diagnostic testing for patients presenting with hypertension has not been adequately studied. Therefore, estimating the pretest probability of a secondary cause of hypertension in a patient with specific clinical characteristics must be considered crude at best. The best available evidence is shown in Table 1.
Diagnostic Strategy
Patients whose initial history, physical, and laboratory evaluation suggest the possibility of a secondary cause of hypertension should undergo additional testing. The search for the secondary cause of hypertension should focus on chronic renal disease, renovascular hypertension, pheochromocytoma, Cushing syndrome, and primary aldosteronism, depending on the clinical scenario Table 2.
Chronic renal disease will be evident from the blood urea nitrogen, creatinine, and the urinalysis results. The diagnostic approach to other causes of hypertension is more complicated.
Although renal artery stenosis is suggested by the presence of an abdominal or flank bruit, it is an insensitive test (sensitivity=65%; specificity=90%). It is useful when positive (positive likelihood ratio=6.5) but does not rule out renal artery stenosis when negative (negative likelihood ratio=0.4). A clinical decision rule has been developed and validated that integrates several findings from the history and physical examination. Software to implement this decision rule in clinical practice, using Palm or PocketPC hand-held computers, is available at no charge from the JFP Web site at PC download.
Duplex sonography is very accurate (sensitivity=98%; specificity=98%) when the study is adequate but is often nondiagnostic in obese patients. For these patients, magnetic resonance angiography (MRA) is better (sensitivity=93%; specificity=95%). Captopril renal scanning (CRS) is less sensitive and less specific than either sonography or MRA. Renal artery stenosis is confirmed by the highly accurate but more invasive reference standard test of conventional angiography.
Pheochromocytoma is rare even in the presence of suggestive symptoms (headache, palpitations, and excessive and inappropriate perspiration), but failure to identify this disease can have disastrous consequences. Therefore, patients who have suggestive signs and symptoms should be screened for pheochromocytoma. However, the standard for screening pheochromocytoma remains controversial. A 24-hour urinary metanephrine (cutoff point of >3.70 nmol/day ) is highly sensitive and specific when done well, but urine collection is inconvenient and may be incomplete. Plasma metanephrines (metanephrine >0.66 nmol/L or normetanephrine >0.30 nmol/L) are easy to obtain, 100% sensitive, and may represent a good screening test for pheochromocytoma. Because they have limited specificity (85%), a positive plasma metanephrine should be confirmed by the 24-hour urinary metanephrine-to-creatinine ratio (cutoff point of >0.354; specificity=98%) before proceeding to anatomical localization of the tumor.
Two imaging studies are commonly used to localize pheochromocytomas. Metaiodobenzylguanidine (MIBG) scintigraphy is more specific but less sensitive than computed tomography (CT). Relying on CT to guide surgery is less likely to miss tumors than MIBG scintigraphy (CT sensitivity = 100% vs MIBG=88%) but is more likely to result in unnecessary surgery because of the lower specificity (CT specificity = 50%; MIBG=89%).
The 24-hour urinary free cortisol (cutoff point >90 mg/day; sensitivity=100%; specificity=98%) is a useful screening test for Cushing syndrome. It is very sensitive, but false-positives may be seen in patients with depression and polycystic ovarian syndrome. The single-dose (1 mg) overnight dexamethasone suppression test is equally sensitive but is a little less specific than the 24-hour urinary cortisol. However, this test is relatively simple for patients. The patient takes 1 mg of dexamethasone at midnight, and the plasma cortisol level is drawn in the morning (cutoff point >100 nmol). The combined dexamethasone and corticotropin-releasing hormone (CRH) suppression test, which has both a sensitivity and a specificity of almost 100%, can be used to confirm the diagnosis of Cushing syndrome. However, it is a little more complicated for the patient. The patient takes 0.5 mg of dexamethasone at noon on the first day and repeats this dose every 6 hours for a total of 8 doses (ending at 6 am on the third day). Two hours after the last dose the patient is given an intravenous bolus of CRH (1 μg/kg), and 15 minutes later a plasma cortisol is drawn. A cortisol level greater than 38 nmol is the cutoff point for this test.
The coexistence of hypertension and spontaneous or diuretic-induced hypokalemia is strongly suggestive of primary aldosteronism. However, it is important to remember that many (if not most) patients with primary aldosteronism do not have hypokalemia. In the past, screening for primary aldosteronism was accomplished by measuring urinary aldosterone levels after oral or intravenous salt loading. The sensitivity of these tests is 90% to 95%, and they carry a risk of precipitous elevation of blood pressure due to volume expansion or hypokalemia. Measuring the plasma renin and aldosterone levels can be used to test for hyperaldosteronism. Various cut points and ratios have been suggested, but the plasma aldosterone-to-renin ratio (cutoff point >25) is currently the most useful screening test for hyperaldosteronism. For this test the patient is asked to rise at 6 am and remain ambulatory for 2 hours, at which time the plasma aldosterone and renin levels are drawn. Beta-blockers and dihydropyridine calcium channel blockers must be stopped for 2 weeks, and spironolactone and loop diuretics must be stopped for 6 weeks before the test. Primary aldosteronism can be confirmed by the fludrocortisone suppression test.
Acknowledgments
Special thanks to Kathleen Dosh, MS; Greg Tan, MD; and Mark Povich, DO, for help during the initial editing of this paper.
Hypertension is arbitrarily defined as a diastolic blood pressure (DBP) of 90 mm Hg or higher, a systolic blood pressure (SBP) equal to or higher than 140 mm Hg, or both, on 3 separate occasions. It affects 24% of the population of the United States and is common among black (28%), white (24%), and Hispanic (14%) Americans. The prevalence of hypertension increases with age and is more than 70% among people 65 years and older. Among principal diagnoses given by family physicians for outpatient visits, only acute respiratory tract infection (7%) is more common than hypertension (6%). The annual direct medical cost of caring for hypertension exceeds $10 billion.
This article will discuss the pathophysiology and diagnosis of hypertension from an evidence-based perspective. An upcoming Applied Evidence article will cover treatment of hypertension and prognosis.
Pathophysiology
Idiopathic, or essential, hypertension accounts for more than 95% of cases and appears to be caused by a complex interaction between genetic predisposition and environmental factors. The predisposition to essential hypertension is polygenic in origin and may find full expression when combined with environmental factors, such as obesity, low physical activity levels, high stress levels, high alcohol consumption, high dietary sodium, and low dietary potassium, calcium, and magnesium. The complex interaction of genetics and environment may affect sodium, catecholamines, the renin-angiotensin system, insulin, and cell membrane function, causing elevation of the blood pressure.
The more common identifiable causes of hypertension include chronic renal disease (2%-5%), renovascular disease—including renal artery atherosclerosis and fibromuscular dysplasia—(0.2%-0.7%), Cushing syndrome (0.1%-0.6%), pheochromocytoma (0.04%-0.1%), and primary hyperaldosteronism (0.01%-0.3%). Although obesity, excessive alcohol consumption, oral contraceptive therapy, and sleep apnea may cause hypertension, they are not typically included as identifiable causes of hypertension. The prevalence of the latter conditions as identifiable causes of hypertension remains to be defined.
Diagnosis
The presence of hypertension must be confirmed by blood pressure measurements obtained with proper technique. The blood pressure of all patients 18 years and older should be measured at each health care visit because of the high prevalence of hypertension. Patients should be encouraged to abstain from nicotine and caffeine for at least 30 minutes before the measurement of the blood pressure. Measurement should be made with a mercury sphygmomanometer or a recently calibrated aneroid device. The bladder of the blood pressure cuff should encircle 80% of the arm. The pressure should be taken after at least 5 minutes of rest with the patient sitting, back supported, and arm bared and supported at heart level. The first sound heard (phase 1) is the SBP, and the last sound heard (phase 5) is the DBP. Two readings separated by 2 minutes should be averaged. Hypertension is present when an accurately measured blood pressure is high on 3 separate occasions.
A major consensus report, the Sixth Report of the Joint National Committee on Prevention Detection, Evaluation, and Treatment of High Blood Pressure,11 designates 6 categories of blood pressure:
- Optimal—SBP less than 120 mm; DBP less than 80 mm
- Normal—SBP less than 130 mm; DBP less than 85 mm
- High normal—SBP is 130 to 139 mm; DBP is 85 to 89 mm
- Stage 1 hypertension—SBP is 140 to 159 mm; DBP is 90 to 99 mm
- Stage 2 hypertension—SBP is 160 to 179 mm; DBP is 100 to 109 mm
- Stage 3 hypertension—SBP is 180 mm or higher; DBP is 110 mm or higher
It is important to note that the recommended diagnostic evaluation is based on a consensus and should not be considered evidence-based. A complete history, physical examination, and limited diagnostic testing (urinalysis, complete blood count, potassium, sodium, fasting glucose, creatinine, total cholesterol, high-density cholesterol, and electrocardiogram) are recommended once the presence of hypertension has been confirmed. This evaluation has 3 purposes:
- Identify other cardiovascular risk factors. Most patients with hypertension have multiple cardiovascular risk factors at the time of initial evaluation. Risk factors include smoking, hyperlipidemia, diabetes, age older than 60 years, sex (men or postmenopausal women), and family history of cardiovascular disease in a female relative before age 65 years or a male relative before 55 years.
- Identify end-organ damage. Evidence of end-organ damage includes left ventricular hypertrophy, angina, previous myocardial infarction, previous angioplasty or coronary revascularization, heart failure, stroke or transient ischemic attack, nephropathy, peripheral arterial disease, and retinopathy.
- Identify secondary causes of hypertension. Estimating the pretest probability of a secondary (identifiable) cause of hypertension is problematic, because referral bias is a major problem in hypertension prevalence studies; patients are typically included in these studies only after being referred to a study center by their primary care physician for resistant or difficult to control hypertension. On the basis of the best available estimates, it would be reasonable to assume that patients presenting to primary care physicians have a 5% probability of an identifiable cause of hypertension.
The diagnostic evaluation serves to identify other cardiovascular risk factors and end-organ damage in patients with high-normal blood pressure or hypertension. This information is used to identify 3 risk groups: Group A includes patients with no other cardiovascular risk factor, cardiovascular disease, or evidence of end-organ damage; group B includes patients who do not have cardiovascular disease or end-organ damage but have 1 or more of the major risk factors other than diabetes mellitus; and group C includes patients who have cardiovascular disease, other end-organ damage, or diabetes mellitus. The risk associated with hypertension and the intensity of recommended treatment increases progressively as a person moves from risk group A through risk group C.
The diagnostic evaluation may also reveal patients who are more likely to have an identifiable cause of hypertension. The probability of an identifiable cause of hypertension is increased by the onset of hypertension outside the normal age for essential hypertension (30-55 years), sudden onset or worsening of hypertension, stage 3 hypertension, and blood pressure that responds poorly to treatment. Elevated creatinine levels suggest hypertension caused by renal parenchymal disease. Abdominal or flank bruits, hypokalemia, or a significant rise in the serum creatinine level after an angiotensin-converting enzyme inhibitor is started suggests renovascular hypertension. Osteoporosis, truncal obesity, moon face, purple striae, muscle weakness, easy bruising, hirsutism, hyperglycemia, hypokalemia, and hyperlipidemia suggest Cushing syndrome. Labile hypertension, orthostatic hypotension, headache, palpitations, pallor, and diaphoresis suggests pheochromocytoma. Isolated hypokalemia may be caused by hyperaldosteronism.
Unfortunately, the accuracy of the history, physical examination, and preliminary diagnostic testing for patients presenting with hypertension has not been adequately studied. Therefore, estimating the pretest probability of a secondary cause of hypertension in a patient with specific clinical characteristics must be considered crude at best. The best available evidence is shown in Table 1.
Diagnostic Strategy
Patients whose initial history, physical, and laboratory evaluation suggest the possibility of a secondary cause of hypertension should undergo additional testing. The search for the secondary cause of hypertension should focus on chronic renal disease, renovascular hypertension, pheochromocytoma, Cushing syndrome, and primary aldosteronism, depending on the clinical scenario Table 2.
Chronic renal disease will be evident from the blood urea nitrogen, creatinine, and the urinalysis results. The diagnostic approach to other causes of hypertension is more complicated.
Although renal artery stenosis is suggested by the presence of an abdominal or flank bruit, it is an insensitive test (sensitivity=65%; specificity=90%). It is useful when positive (positive likelihood ratio=6.5) but does not rule out renal artery stenosis when negative (negative likelihood ratio=0.4). A clinical decision rule has been developed and validated that integrates several findings from the history and physical examination. Software to implement this decision rule in clinical practice, using Palm or PocketPC hand-held computers, is available at no charge from the JFP Web site at PC download.
Duplex sonography is very accurate (sensitivity=98%; specificity=98%) when the study is adequate but is often nondiagnostic in obese patients. For these patients, magnetic resonance angiography (MRA) is better (sensitivity=93%; specificity=95%). Captopril renal scanning (CRS) is less sensitive and less specific than either sonography or MRA. Renal artery stenosis is confirmed by the highly accurate but more invasive reference standard test of conventional angiography.
Pheochromocytoma is rare even in the presence of suggestive symptoms (headache, palpitations, and excessive and inappropriate perspiration), but failure to identify this disease can have disastrous consequences. Therefore, patients who have suggestive signs and symptoms should be screened for pheochromocytoma. However, the standard for screening pheochromocytoma remains controversial. A 24-hour urinary metanephrine (cutoff point of >3.70 nmol/day ) is highly sensitive and specific when done well, but urine collection is inconvenient and may be incomplete. Plasma metanephrines (metanephrine >0.66 nmol/L or normetanephrine >0.30 nmol/L) are easy to obtain, 100% sensitive, and may represent a good screening test for pheochromocytoma. Because they have limited specificity (85%), a positive plasma metanephrine should be confirmed by the 24-hour urinary metanephrine-to-creatinine ratio (cutoff point of >0.354; specificity=98%) before proceeding to anatomical localization of the tumor.
Two imaging studies are commonly used to localize pheochromocytomas. Metaiodobenzylguanidine (MIBG) scintigraphy is more specific but less sensitive than computed tomography (CT). Relying on CT to guide surgery is less likely to miss tumors than MIBG scintigraphy (CT sensitivity = 100% vs MIBG=88%) but is more likely to result in unnecessary surgery because of the lower specificity (CT specificity = 50%; MIBG=89%).
The 24-hour urinary free cortisol (cutoff point >90 mg/day; sensitivity=100%; specificity=98%) is a useful screening test for Cushing syndrome. It is very sensitive, but false-positives may be seen in patients with depression and polycystic ovarian syndrome. The single-dose (1 mg) overnight dexamethasone suppression test is equally sensitive but is a little less specific than the 24-hour urinary cortisol. However, this test is relatively simple for patients. The patient takes 1 mg of dexamethasone at midnight, and the plasma cortisol level is drawn in the morning (cutoff point >100 nmol). The combined dexamethasone and corticotropin-releasing hormone (CRH) suppression test, which has both a sensitivity and a specificity of almost 100%, can be used to confirm the diagnosis of Cushing syndrome. However, it is a little more complicated for the patient. The patient takes 0.5 mg of dexamethasone at noon on the first day and repeats this dose every 6 hours for a total of 8 doses (ending at 6 am on the third day). Two hours after the last dose the patient is given an intravenous bolus of CRH (1 μg/kg), and 15 minutes later a plasma cortisol is drawn. A cortisol level greater than 38 nmol is the cutoff point for this test.
The coexistence of hypertension and spontaneous or diuretic-induced hypokalemia is strongly suggestive of primary aldosteronism. However, it is important to remember that many (if not most) patients with primary aldosteronism do not have hypokalemia. In the past, screening for primary aldosteronism was accomplished by measuring urinary aldosterone levels after oral or intravenous salt loading. The sensitivity of these tests is 90% to 95%, and they carry a risk of precipitous elevation of blood pressure due to volume expansion or hypokalemia. Measuring the plasma renin and aldosterone levels can be used to test for hyperaldosteronism. Various cut points and ratios have been suggested, but the plasma aldosterone-to-renin ratio (cutoff point >25) is currently the most useful screening test for hyperaldosteronism. For this test the patient is asked to rise at 6 am and remain ambulatory for 2 hours, at which time the plasma aldosterone and renin levels are drawn. Beta-blockers and dihydropyridine calcium channel blockers must be stopped for 2 weeks, and spironolactone and loop diuretics must be stopped for 6 weeks before the test. Primary aldosteronism can be confirmed by the fludrocortisone suppression test.
Acknowledgments
Special thanks to Kathleen Dosh, MS; Greg Tan, MD; and Mark Povich, DO, for help during the initial editing of this paper.
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension 1995;25:305-13.
2. Barker W, Mullooly J, Linton K. Trends in hypertension prevalence, treatment, and control: in a well-defined older population. Hypertension 1998;31:552-59.
3. Schappert S, Nelson C. National Ambulatory Medical Care Survey: 1995-96 summary. Vital Health Stat 1999;142:1-122.
4. Stason W. Opportunities to improve cost-effectiveness of treatment of hypertension. Hypertension 1991;18:1161-66.
5. Lander E, Schork N. Genetic dissection of complex traits. Science 1994;265:2037-48.
6. Stevens V, Obarzanek E, Cook N, Lee I-M. Long-term weight loss and changes in blood pressure: results of the trials of hypertension prevention, phase II. Ann Intern Med 2001;134:1-11.
7. Moore R, Levine D, Southard J, Entwisle G, Shapiro S. Alcohol consumption and blood pressure in the 1982 Maryland Hypertension Survey. Am J Hypertens 1990;3:1-7.
8. Chasan-Taber L, Willett W, Manson J, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996;94:483-89.
9. Nieto F, Young T, Lind B, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study: Sleep Heart Health Study. JAMA 2000;283:1829-36.
10. Reeves R. Does this patient have hypertension? How to measure blood pressure. JAMA 1995;273:1211-18.
11. Joint National Committee on Prevention. Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
12. Fuster V, Pearson T. 27th Bethesda conference: matching the intensity of risk factor management with the hazard for coronary disease events. September 14-15, 1995. J Am Coll Cardiol 1996;27:957-1047.
13. Rudnick K, Sackett D, Hirst S, Holmes C. Hypertension in a family practice. Can Med Assoc J 1977;117:492-97.
14. Sinclair A, Isles C, Brown I, Cameron H, Murray G, Robertson J. Secondary hypertension in a blood pressure clinic. Arch Intern Med 1987;147:1289-93.
15. Anderson G, Blakeman N, Streeten D. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens 1994;12:609-15.
16. Tucker R, Labarthe D. Frequency of surgical treatment for hypertension in adults at the Mayo Clinic from 1973 through 1975. Mayo Clin Proc 1977;52:549-55.
17. Gifford R. Evaluation of the hypertensive patient. Chest 1973;64:336-40.
18. Krjnen P, Jaarsveld B, Steyerberg E, Schalekamp M. A clinical prediction rule for renal artery stenosis. Ann Intern Med 1998;129:705-11.
19. Berglund AS, Hulthen UL, Manhem P, Thorsson O, Wollmer P, Tornquist C. Metaiodobenzylguanidine (MIBG) scintigraphy and computed tomography (CT) in clinical practice: primary and secondary evaluation for localization of phaeochromocytomas. J Intern Med 2001;249:247-51.
20. Yanovski J, Cutler G, Chrousos G, Nieman L. Corticotropin-releasing hormone stimulation following low-dose dexamethasone administration: a new test to distinguish Cushing’s syndrome from pseudo-Cushing’s states. JAMA 1993;269:2232-38.
21. Blumenfeld J, Sealey J, Schussel Y, Vaughan E. Diagnosis and treatment of primary aldosteronism. Ann Intern Med 1994;121:877-85.
22. Fardella C, Lorena M, Gomez-Sanchez C, Cortes J. Primary hyperaldosteronism in essential hypertensives: prevalence, biochemical profile, and molecular biology. J Clin Endocrinol Metabol 2000;85:1863-67.
23. Streeten D, Tomycz N, Anderson G. Reliability of screening methods for the diagnosis of primary aldosteronism. Am J Med 1979;67:403-13.
24. Bravo E, Tarazi R, Dustan H, Fouad F. The changing clinical spectrum of primary aldosteronism. Am J Med 1983;74:641-51.
25. Gordon R. Primary aldosteronism. J Endocrinol Invest 1995;18:495-511.
26. Anderson G, Blakeman N, Streeten D. Prediction of renovascular hypertension. Am J Hypertens 1988;1:301-04.
27. Manger W, Gifford R. Clinical and experimental pheochromocytoma. Cambridge, Mass: Blackwell Science; 1996.
28. Nugent C, Warner H, Dunn J, Tyler F. Probability theory in the diagnosis of Cushing’s syndrome. J Clin Endocrinol Metabol 1964;24:621-27.
29. Fishman L, Kuchel O, Liddle G, Michelakis A. Incidence of primary hyperaldosteronism in uncomplicated ‘essential’ hypertension. JAMA 1968;205:85-90.
30. Fenton S, Lyttle J, Pantridge J. Diagnosis and results of surgery in renovascular hypertension. Lancet 1966;2:117-21.
31. de Haan M, Kouwenhoven M, Thelissen G, Koster D. Renovascular disease in patients with hypertension: detection with systolic and diastolic gating in three-dimensional, phase-contrast MR angiography. Radiology 1996;198:449-56.
32. Olin J, Piedmonte M, Young J, DeAnna S. The utility of duplex ultrasound screening of renal arteries for diagnosing significant renal artery stenosis. Ann Intern Med 1995;122:833-38.
33. Setaro J, Chen C, Hoffer P, Black H. Captopril renography in the diagnosis of renal artery stenosis and the prediction of improvement with revascularization: the Yale Vascular Center experience. Am J Hypertens 1991;4:698S-705S.
34. Jacques W, Lenders M, Keiser H, Goldstein D. Plasma metanephrines in the diagnosis of pheochromocytoma. Ann Intern Med 1995;123:101-09.
35. Heron E, Chatellier G, Billaud E, Foos E. The urinary metanephrine-to-creatinine ratio for the diagnosis of pheochromocytoma. Ann Intern Med 1996;125:300-03.
36. Mengden T, Habmann P, Mullen J, Vetter W. Urinary free cortisol versus 17-hydroxysteroids: a comparative study of their diagnostic value in Cushing’s syndrome. Clin Invest 1992;70:545-48.
37. Montwill J, Igoe D, McKenna T. The overnight dexamethasone test is the procedure of choice in screening for Cushing’s syndrome. Steroids 1994;59:296-98.
38. Weinberger M, Fineberg N. The diagnosis of primary aldosteronism and separation of two major subtypes. Arch Intern Med 1993;153:2125-29.
1. Burt V, Whelton P, Rocella E, Brown C, Cutler J. Prevalence of hypertension in the US population: results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension 1995;25:305-13.
2. Barker W, Mullooly J, Linton K. Trends in hypertension prevalence, treatment, and control: in a well-defined older population. Hypertension 1998;31:552-59.
3. Schappert S, Nelson C. National Ambulatory Medical Care Survey: 1995-96 summary. Vital Health Stat 1999;142:1-122.
4. Stason W. Opportunities to improve cost-effectiveness of treatment of hypertension. Hypertension 1991;18:1161-66.
5. Lander E, Schork N. Genetic dissection of complex traits. Science 1994;265:2037-48.
6. Stevens V, Obarzanek E, Cook N, Lee I-M. Long-term weight loss and changes in blood pressure: results of the trials of hypertension prevention, phase II. Ann Intern Med 2001;134:1-11.
7. Moore R, Levine D, Southard J, Entwisle G, Shapiro S. Alcohol consumption and blood pressure in the 1982 Maryland Hypertension Survey. Am J Hypertens 1990;3:1-7.
8. Chasan-Taber L, Willett W, Manson J, et al. Prospective study of oral contraceptives and hypertension among women in the United States. Circulation 1996;94:483-89.
9. Nieto F, Young T, Lind B, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a large community-based study: Sleep Heart Health Study. JAMA 2000;283:1829-36.
10. Reeves R. Does this patient have hypertension? How to measure blood pressure. JAMA 1995;273:1211-18.
11. Joint National Committee on Prevention. Evaluation and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI). Arch Intern Med 1997;157:2413-46.
12. Fuster V, Pearson T. 27th Bethesda conference: matching the intensity of risk factor management with the hazard for coronary disease events. September 14-15, 1995. J Am Coll Cardiol 1996;27:957-1047.
13. Rudnick K, Sackett D, Hirst S, Holmes C. Hypertension in a family practice. Can Med Assoc J 1977;117:492-97.
14. Sinclair A, Isles C, Brown I, Cameron H, Murray G, Robertson J. Secondary hypertension in a blood pressure clinic. Arch Intern Med 1987;147:1289-93.
15. Anderson G, Blakeman N, Streeten D. The effect of age on prevalence of secondary forms of hypertension in 4429 consecutively referred patients. J Hypertens 1994;12:609-15.
16. Tucker R, Labarthe D. Frequency of surgical treatment for hypertension in adults at the Mayo Clinic from 1973 through 1975. Mayo Clin Proc 1977;52:549-55.
17. Gifford R. Evaluation of the hypertensive patient. Chest 1973;64:336-40.
18. Krjnen P, Jaarsveld B, Steyerberg E, Schalekamp M. A clinical prediction rule for renal artery stenosis. Ann Intern Med 1998;129:705-11.
19. Berglund AS, Hulthen UL, Manhem P, Thorsson O, Wollmer P, Tornquist C. Metaiodobenzylguanidine (MIBG) scintigraphy and computed tomography (CT) in clinical practice: primary and secondary evaluation for localization of phaeochromocytomas. J Intern Med 2001;249:247-51.
20. Yanovski J, Cutler G, Chrousos G, Nieman L. Corticotropin-releasing hormone stimulation following low-dose dexamethasone administration: a new test to distinguish Cushing’s syndrome from pseudo-Cushing’s states. JAMA 1993;269:2232-38.
21. Blumenfeld J, Sealey J, Schussel Y, Vaughan E. Diagnosis and treatment of primary aldosteronism. Ann Intern Med 1994;121:877-85.
22. Fardella C, Lorena M, Gomez-Sanchez C, Cortes J. Primary hyperaldosteronism in essential hypertensives: prevalence, biochemical profile, and molecular biology. J Clin Endocrinol Metabol 2000;85:1863-67.
23. Streeten D, Tomycz N, Anderson G. Reliability of screening methods for the diagnosis of primary aldosteronism. Am J Med 1979;67:403-13.
24. Bravo E, Tarazi R, Dustan H, Fouad F. The changing clinical spectrum of primary aldosteronism. Am J Med 1983;74:641-51.
25. Gordon R. Primary aldosteronism. J Endocrinol Invest 1995;18:495-511.
26. Anderson G, Blakeman N, Streeten D. Prediction of renovascular hypertension. Am J Hypertens 1988;1:301-04.
27. Manger W, Gifford R. Clinical and experimental pheochromocytoma. Cambridge, Mass: Blackwell Science; 1996.
28. Nugent C, Warner H, Dunn J, Tyler F. Probability theory in the diagnosis of Cushing’s syndrome. J Clin Endocrinol Metabol 1964;24:621-27.
29. Fishman L, Kuchel O, Liddle G, Michelakis A. Incidence of primary hyperaldosteronism in uncomplicated ‘essential’ hypertension. JAMA 1968;205:85-90.
30. Fenton S, Lyttle J, Pantridge J. Diagnosis and results of surgery in renovascular hypertension. Lancet 1966;2:117-21.
31. de Haan M, Kouwenhoven M, Thelissen G, Koster D. Renovascular disease in patients with hypertension: detection with systolic and diastolic gating in three-dimensional, phase-contrast MR angiography. Radiology 1996;198:449-56.
32. Olin J, Piedmonte M, Young J, DeAnna S. The utility of duplex ultrasound screening of renal arteries for diagnosing significant renal artery stenosis. Ann Intern Med 1995;122:833-38.
33. Setaro J, Chen C, Hoffer P, Black H. Captopril renography in the diagnosis of renal artery stenosis and the prediction of improvement with revascularization: the Yale Vascular Center experience. Am J Hypertens 1991;4:698S-705S.
34. Jacques W, Lenders M, Keiser H, Goldstein D. Plasma metanephrines in the diagnosis of pheochromocytoma. Ann Intern Med 1995;123:101-09.
35. Heron E, Chatellier G, Billaud E, Foos E. The urinary metanephrine-to-creatinine ratio for the diagnosis of pheochromocytoma. Ann Intern Med 1996;125:300-03.
36. Mengden T, Habmann P, Mullen J, Vetter W. Urinary free cortisol versus 17-hydroxysteroids: a comparative study of their diagnostic value in Cushing’s syndrome. Clin Invest 1992;70:545-48.
37. Montwill J, Igoe D, McKenna T. The overnight dexamethasone test is the procedure of choice in screening for Cushing’s syndrome. Steroids 1994;59:296-98.
38. Weinberger M, Fineberg N. The diagnosis of primary aldosteronism and separation of two major subtypes. Arch Intern Med 1993;153:2125-29.