User login
Acute Stroke Patient with Atrial Fibrillation
INITIAL EVALUATION
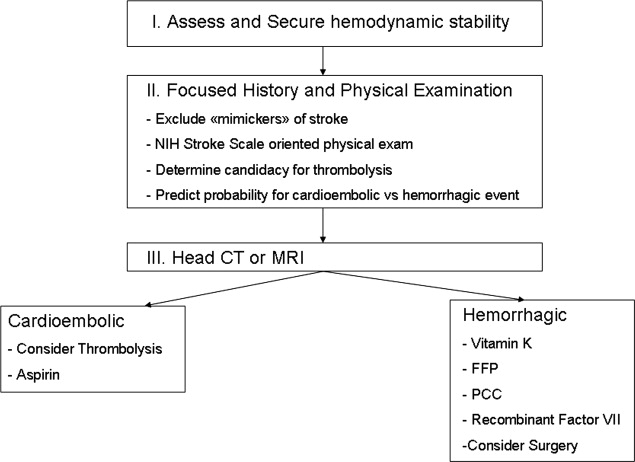
The approach to patients with acute stroke symptoms should always start with the stabilization of the airway, breathing, and circulation. A fast clinical investigation for possible mimickers of an acute stroke (head trauma, migraines, epilepsy, infection, hypoglycemia, other metabolic derangements, and intoxications) is the next step. The history and physical examination should be guided by the National Institutes of Health stroke scale, which has been widely accepted by the American Stroke Association (ASA), the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.2, 9 Strict control of electrolytes, glucose, and fever, management of blood pressure depending on thetype of stroke, and prophylaxis for deep vein thrombosis/pulmonary embolism, aspiration, dehydration, hypoxemia, malnutrition, and pressure sores should be initiated.9, 10 All patients with suspected acute stroke must be promptly assessed for thrombolytic therapy on the basis of the time since onset of symptoms and the National Institutes of Health stroke scale. Noncontrast computed tomography of the brain is the first step for differentiating between ischemic and hemorrhagic events.3, 9 There is an increased interest in the use of magnetic resonance imaging to detect acute intracranial hemorrhage (ICH) and its ability to detect stroke earlier than computed tomography.911 Multimodal computed tomography and magnetic resonance imaging provide additional information that will improve the diagnosis of ischemic stroke, and they have been added as a class I recommendation to the most recent stroke guidelines.9, 12 Computed tomographic angiography and perfusion computed tomography may precisely describe details regarding the site of occlusion, infarct core, salvageable brain tissue, and collateral flow that can improve patient selection for intravenous or intra‐arterial thrombolysis and exclude stroke mimics.9, 13
ISCHEMIC STROKE
Thrombolysis
In the setting of acute ischemic stroke, the patient should be promptly evaluated for thrombolytic therapy according to the American College of Chest Physicians guidelines.14 Intravenous r‐TPA (recombinant tissue plasminogen activator) is given only to 1% to 2% of stroke patients in the United States. This low percentage is mainly due to delayed presentation to an emergency department beyond the 3‐hour treatment window.15 Clear benefit has been proven for eligible patients if thrombolytic therapy is administered within 3 hours from the initiation of symptoms, although no subgroup analysis has been done in patients with atrial fibrillation.9 The efficacy of intravenous thrombolysis within the 3‐hour time window is similar between different stroke subtypes; therefore, its administration should not be delayed in order to investigate its etiology.16 Intravenous thrombolysis remains the standard of care, but recent studies have demonstrated that intra‐arterial administration, despite its risks, may be more effective in selected patients.9, 1719 Patients most likely to benefit from intra‐arterial thrombolysis are those with middle cerebral artery occlusion of less than 6 hours (Prolyse in Acute Cerebral Thromboembolism Trials I and II) and patients with severe basilar artery stroke.17, 19 A recent study in Germany has demonstrated that intra‐arterial thrombolysis may be superior to intravenous thrombolysis in the 3‐ to 6‐hour treatment window.19 The updated 2007 guidelines from the American Heart Association (AHA)/ASA have included intra‐arterial thrombolysis for specific patients who are not eligible for intravenous thrombolysis when this can be performed at experienced stroke centers.9 Thrombolysis reduces overall disability and improves the quality of life in appropriately selected patients. The risk of hemorrhage is approximately 5.2%.20 After intravenous thrombolysis, approximately one‐third of patients ultimately develop re‐occlusion of the artery, especially patients with only partial recanalization. This may lead to neurologic deterioration and higher in‐hospital mortality.21 According to more recent studies, ultrasound‐enhanced thrombolysis may augment tissue plasminogen activator induced arterial recanalization by continuous transcranial Doppler.22 Symptomatic hemorrhagic transformation of the infarction remains the primary concern with the administration of intravenous rtTPA.23, 24 Despite the apparent risks of ICH, atrial fibrillation patients not on warfarin should always be promptly referred for thrombolysis whenever they are eligible.
Heparin
For many years, clinicians have believed in the role of heparin in patients with atrial fibrillation, especially after intracranial hemorrhage is excluded by negative initial noncontrast head computed tomography.25 The most obvious pathophysiologic mechanism in patients with atrial fibrillation is cardioembolism. Therefore, it was believed that heparin could contribute to the resolution of the responsible clot. Two large international trials (the Heparin in Acute Embolic Stroke Trial and the International Stroke Trial), confirmed by multiple smaller ones, have investigated the use of heparin (unfractionated or low‐molecular‐weight heparin) at therapeutic doses in the setting of an acute ischemic event.2628 Surprisingly, none of them showed a statistically significant benefit, but instead they showed a clear increase in hemorrhagic events. Therefore, routine use of unfractionated heparin or low‐molecular‐weight heparin at therapeutic doses should be avoided in the acute setting of a stroke.28, 29
Aspirin
Among the antiplatelet agents, aspirin is the only well‐studied agent for the treatment of acute ischemic stroke. It has been proven that during the first 24 hours after stroke, there is substantial platelet activation that can be inhibited by aspirin.30, 31 Two major trials, the Chinese Acute Stroke Trial and the International Stroke Trial, have demonstrated the benefit of early aspirin use in patients with stroke and atrial fibrillation.30 Both proved a decrease in recurrent stroke without a significant increase in hemorrhaging. The recommended dose of aspirin is 325 mg/day.9 Currently, clopidogrel alone or in combination with aspirin and the intravenous administration of antiplatelet agents that inhibit the glycoprotein IIb/IIIa receptor are class III recommendations. They should not be used outside the setting of clinical trials.9
Warfarin
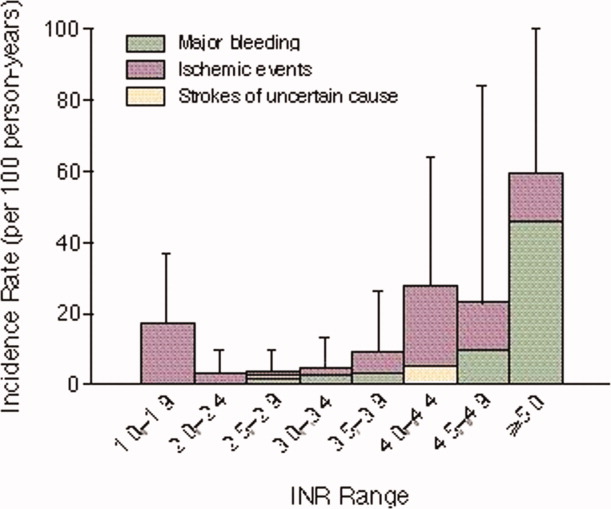
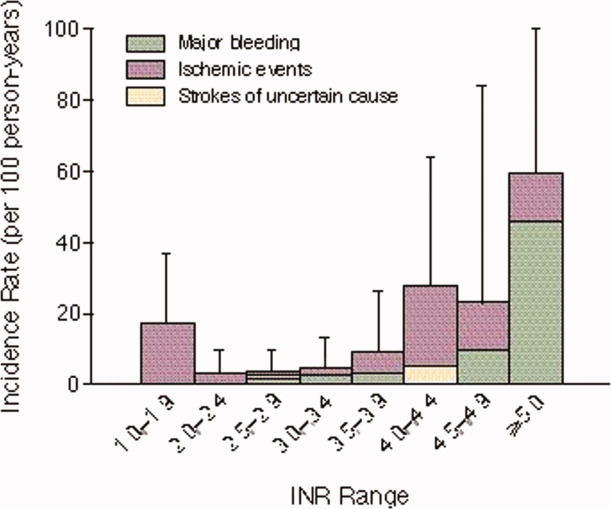
It is well known that atrial fibrillation increases the risk of ischemic stroke by a factor of 5.32 Studies have shown that maintaining the INR above 2.0 decreases not only the frequency but also the severity and mortality of ischemic events.4, 8, 32 The National Anticoagulation Benchmark Outcomes Report has shown that in the highest risk atrial fibrillation patients, only 55% receive warfarin and 21% do not receive aspirin or warfarin.33 This discrepancy results from the fact that warfarin is the second most common drug, after insulin, responsible for adverse drug events in emergency room visits. In atrial fibrillation patients on warfarin who present to the emergency with an acute stroke, there are no clear guidelines regarding the continued use of warfarin at therapeutic doses (target INR = 2.03.0). Warfarin is usually not initiated in the acute setting until the patient is medically stable. The exact time at which warfarin can be started or resumed after an acute ischemic stroke remains to be determined.34 Usually, it is preferable to start it within 1 week after the event, given the risk of early recurrent acute stroke during the next 2 to 4 weeks after the initial stroke.35
HEMORRHAGIC STROKE/ICH
Introduction
The risk of spontaneous ICH is 0.15%/year in patients over 70 years old and increases to 0.3% to 0.8% when patients are on therapeutic doses of warfarin with INR between 2 and 3.36, 37 Given the multiple interactions of warfarin with other medications, this is a significant concern because ICH is associated with substantial neurological deterioration.38 Although most warfarin‐induced ICH occurs in patients with therapeutic INR, it becomes the most prevalent mechanism when the INR exceeds 5.0, and it should be highly suspected.1, 4 Therefore, prompt determination of INR is critical in the initial evaluation of acute stroke in patients with atrial fibrillation. Age is the most important predisposing factor for ICH in patients with atrial fibrillation. There is almost a 50% increase in warfarin‐induced bleeding for every decade of age above 40.39 Cerebral amyloid angiopathy plays an important role in warfarin‐associated lobar ICH in the elderly, and it may contribute to the patient candidacy for warfarin treatment in the near future.40 On the other hand, a hemorrhagic stroke can be an iatrogenic complication of initiation of warfarin, heparin, or early thrombolysis because symptomatic hemorrhagic transformation of the infarction is the main and most lethal side effect of intravenous rtTPA in the treatment of acute ischemic stroke.24 ICH is associated with a 30% to 50% mortality rate, and it represents the most lethal and least treatable form of stroke.32 It has been suggested that macroalbuminuria is an independent predictor of hemorrhagic transformation and particularly of severe hemorrhage in patients with acute ischemic stroke, but specific guidelines for screening or special management of those patients do not currently exist.33 ICH is a medical emergency with high mortality and should be recognized and treated promptly. Recently, the AHA and ASA have published updated guidelines for the management of spontaneous ICH in adults.12
Vitamin K
All experts agree that anticoagulation should be urgently reversed in the setting of ICH. Although high doses of intravenous vitamin K (1020 mg) are usually enough to reverse the anticoagulant effect of warfarin, it may take up to 12 to 24 hours to act, and it depends on intact liver function. Given the high mortality of this condition, vitamin K as monotherapy is considered inadequate, and a more aggressive approach is recommended.41
Fresh Frozen Plasma (FFP)
In the United States, for many years FFP has been considered the standard of care for the acute reversal of warfarin‐associated anticoagulation.42 In general, 10 to 15 cc/kg FFP is used.43 Timing rather than dosage seems to be more important for a better clinical outcome.44 The use of FFP is complicated by the delayed time for thawing and compatibility check, volume overload, and sometimes inadequate and unpredictable correction. The median time for door‐to‐INR normalization is 30 hours, which is a significant delay for such a potentially fatal condition. Another possible complication of FFP is the report of increasing hematomas.45
Prothrombin Complex Concentrates (PCCs)
PCCs contain vitamin K dependent coagulation factors II, VII, IX, and X, the factors deficient in warfarin therapy.44, 46 Therefore, a PCC dose of 25 to 59 U/kg has been used in life‐threatening bleeding, resulting in a decrease in the median INR from 3.8 to 1.3 immediately after administration.42 PCCs should always be given with vitamin K. Thrombotic events have been described with the infusion of PCCs, but no clear guidelines have been published.42 A recent study from the Mayo Clinic showed that many experts suggest its use in the urgent condition of warfarin‐associated ICH.41 PCCs are widely used in the European community and have previously been cited as the agent of choice for urgent warfarin reversal.42, 47, 48 A recent study comparing PCCs with FFP and vitamin K has demonstrated that PCCs may be superior to FFP and vitamin K by reducing the risk of hematoma growth.49
Recombinant Factor VIIa
Recombinant factor VIIa is a preparation of activated coagulation factor VII (factor VIIa) that is produced by recombinant DNA technology.50 It was initially used for the treatment of inhibitors in patients with hemophilia. It has also been used in the past to correct anticoagulation in patients with acute ICH,36 but most studies have been done in patients with hemophilia or factor VII deficiency.50 Major limitations include cost, prothrombotic potential, and lack of correction of other coagulation factors dependent on vitamin K. Studies have shown that factor VII may be a safe, rapid, and effective way of reversing anticoagulation and may offer an improved quality of life to patients with ICH.51, 52 Factor Seven for Acute Hemorrhagic Stroke Treatment, a large phase III trial, is in progress, but preliminary results are controversial regarding the reduction in the size of hemorrhage, mortality, and improvement of functional outcome.32 In a recent article from the Mayo Clinic,41 several experts on clinical stroke, neurologic intensive care, and hematology suggest its use, alone or with FFP, for the urgent reversal of INR in the clinical setting of warfarin‐associated ICH. Currently, according to the 2007 AHA/ASA updated guidelines, recombinant factor VIIa can be administered within the first 3 to 4 hours after onset of ICH to slow progression of bleeding, although its efficacy and safety remain to be confirmed (class IIb recommendation).12
Surgical Evacuation
Despite the clear guidelines for the indications of surgery in spontaneous intracranial bleeding,12 the role of surgical evacuation in patients with supratherapeutic INR is not well defined. Many neurosurgeons are reluctant to operate in the setting of impaired hemostasis. The International Surgical Trial in Intracerebral Hemorrhage showed no clear benefit of early neurosurgical intervention compared to conservative treatment.53 Different surgical trials have shown different outcomes.54 The selection of patients who would benefit from surgery depends on the location and size of the hemorrhage, coagulation status, and Glasgow Coma Scale.55 Patients with rapidly expanding hematomas in a surgically accessible intracranial territory are more likely to benefit from a neurosurgical intervention. Newer surgical techniques with a computed‐tomography‐guided stereotactic approach or endoscopy‐guided evacuation in emerging ICH may offer better outcomes.56
RECENT ADVANCES
Mechanical Embolectomy
Mechanical embolectomy is a growing field of neurology with a promising interventional approach to the treatment of embolic strokes.57, 58 Patients with atrial fibrillation will probably be one of the patient groups who will receive maximum benefit when the efficacy and safety of the procedure are established. Endovascular reperfusion via mechanical embolectomy is offered to patients who are ineligible for thrombolytics, and it extends the time window up to 8 hours.58 For the first time, in 2007 the AHA/ASA guidelines have included the Mechanical Embolus Removal in Cerebral Ischemia device as a reasonable intervention for extraction of intra‐arterial thrombi in carefully selected patients.9
Left Atrial Appendage (LAA) Occlusion
The LAA is the source of 91% of embolic thrombi in patients with atrial fibrillation.59 Therefore, surgical or percutaneous removal or occlusion of the LAA would be an important treatment option, especially in high‐risk patients intolerant of warfarin or with recurrent strokes, despite anticoagulation. Several surgical techniques and percutaneous LAA occlusion devices have been studied with different success rates and safety characteristics.6063 Currently, there are no official guidelines for the use of those interventions.
Genetic Testing for Warfarin Sensitivity
Warfarin is the second most common drug, after insulin, to require emergency room visits for adverse drug events. In September 2007, the Food and Drug Administration approved the Nanosphere Verigene Warfarin Metabolism Nucleic Acid Test, which detects variants of 2 genes (CYP2C9 and VKORC1) implicated in the unexpected response to warfarin.6466 Guidelines for the applied use of these tests are currently under development.66
CONCLUSION
On average, there is a new stroke every 45 seconds, and every 3 to 4 minutes, someone dies from a stroke in the United States. Atrial fibrillation accounts for one‐fourth of all strokes in the elderly population. Acute stroke in anticoagulated patients with atrial fibrillation is a common, challenging scenario in emergency departments because many questions remain unanswered (Table 1). A special and prompt approach from the clinician is needed to achieve effective management and avoid potentially fatal complications (Figure 2). Many hospitals in the United States have formed stroke teams to ensure prompt clinical and radiographic assessment of stroke patients. Only early recognition of cardioembolic or hemorrhagic strokes in atrial fibrillation patients can lead to aggressive management of this potentially fatal and disabling condition.
| 1. When can warfarin be safely started after an acute cardioembolic stroke? |
| 2. Could heparin in lower doses be beneficial without the risk of bleeding? |
| 3. Should we repeat thrombolysis in cases of re‐occlusion? |
| 4. What is the role of other antithrombotic and antiplatelet agents in these patients? |
- ,.The Atlas of Heart Disease and Stroke.Geneva, Switzerland:World Health Organization;2004.
- National Institute of Neurological Disorders and Stroke. NIH Stroke Scale. Available at: http://www.ninds.nih.gov/doctors/NIH_stroke_scale_booklet.pdf. Accessed January2008.
- Royal College of Physicians.National Clinical Guidelines for Stroke.2nd ed.Prepared by the Intercollegiate Stroke Working Party.London:RCP,2004.
- The European Atrial Fibrillation Trial Study Group.Optimal oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and recent cerebral ischemia.N Engl J Med.1995;333:5–10.
- ,,, et al.Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation.Ann Intern Med.2004;141(10):745–752.
- ,.Antithrombotic treatment in atrial fibrillation.Heart.2007;93(1):39–44.
- ,,, et al.Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin.Circulation.2004;110(16):2287–2292.
- ,,.Atrial fibrillation.Med J Aust.2007;186(4):197–202.
- ,,, et al.Guidelines for the early management of adults with ischemic stroke. A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups.Stroke.2007;38(5):1655–1711.
- ,,, et al.MRI of acute post‐ischemic cerebral hemorrhage in stroke patients: diagnosis with T2*‐weighted gradient‐echo sequences.Neuroradiology.2001;43(10):809–815.
- ,,, et al.Emergency imaging of cerebrovascular accidents.J Neuroradiol.2004;31(4):327–333.
- ,,, et al.Guidelines for the management of spontaneous intracerebral hemorrhage in adults. 2007 update. A guideline from the American Heart Association, American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group.Stroke.2007;38(6):2001–2023.
- ,,,,,.Systematic comparison of perfusion‐CT and CT‐angiography in acute stroke patients.Ann Neurol.2007;61(6):533–543.
- ,,,,.Antithrombotic and thrombolytic therapy for ischemic stroke: the seventh ACCP conference on antithrombotic and thrombolytic therapy.Chest.2004;126(3 suppl):S483–S512.
- .Acute ischemic stroke treatment in 2007.Circulation.2007;116(13):1504–1514.
- ,,,,.Efficacy of IV tissue plasminogen activator in acute stroke: does stroke subtype really matter?Neurology.2003;61(1):71–75.
- ,,,,,.Efficacy of intraarterial thrombolysis of basilar artery stroke.J Stroke Cerebrovasc Dis.1999;8(1):22–27.
- ,,, et al.Treatment of acute ischemic brain infarction with the assistance of local intraarterial thrombolysis with recombinant tissue‐type plasminogen activator.Acta Radiol.2007;48(7):774–780.
- ,,,,.Intra‐arterial thrombolysis using rt‐PA in patients with acute stroke due to vessel occlusion of anterior and/or posterior cerebral circulation.Neuroradiology.2008;50(1):75–83.
- .Tissue plasminogen activator for acute ischemic stroke in clinical practice: a meta‐analysis of safety data.Stroke.2003;34:2847–2850.
- ,.Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator.Neurology.2002;59:862–867.
- ,,, et al.Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke.Stroke.2007;38(3):948–954.
- ,,,.Thrombolysis for acute ischemic stroke.Cochrane Database Syst Rev.2003;(3):CD000213.
- ,,, et al.Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt‐PA stroke trials.Lancet.2004;363:768–774.
- ,,,,,.Trends in medical care of hospitalized stroke patients between 1980 and 1990: the Minnesota stroke survey.J Stroke Cerebrovasc Dis.1998;7(1):76–84.
- ,,,.Low molecular‐weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double‐blind randomized study. HAEST Study Group. Heparin in Acute Embolic Stroke Trial.Lancet.2000;355(9211):1205–1210.
- International Stroke Trial Collaborative Group.The International Stroke Trial (IST): a randomized trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischemic stroke.Lancet.1997;349(9065):1569–1581.
- .Emergent use of anticoagulation for treatment of patients with ischemic stroke.Stroke.2002;33:856–861.
- ,,,.Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke: a meta‐analysis of randomized controlled trials.Stroke.2007;38(2):423–430.
- .The results of CAPRIE, IST and CAST. International Stroke Trial. Chinese Acute Stroke Trial.Thromb Res1998;92(1 suppl 1):S13–S16.
- ,,,,.Platelet activation and lipid peroxidation in patients with acute ischemic stroke.Stroke.1997;28:1557–1563.
- ,,, et al.Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation elaine.N Engl J Med.2003;349:1019–1026.
- ,,,.Hospitalized patients with atrial fibrillation and a high risk of stroke are not being provided with adequate anticoagulation.J Am Coll Cardiol.2005;46(9):1729–1736.
- ,.Preventing stroke in patients with atrial fibrillation.JAMA.1999;281(19):1830–1835.
- ,.Atrial fibrillation, stroke, and acute antithrombotic therapy: analysis of randomized clinical trials.Stroke.2002;33(11):2722–2727.
- ,,, et al.Recombinant factor VIIa for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage.Mayo Clin Proc.2004;79(12):1495–1500.
- ,,,.Managing the therapeutic dilemma: patients with spontaneous intracerebral hemorrhage and urgent need for anticoagulation.J Neurol.2000;247(3):209–214.
- ,,, et al.Early hemorrhage growth in patients with intracerebral hemorrhage.Stroke.1997;28:1–5.
- ,,.Bleeding complications in oral anticoagulant therapy: an analysis of risk factors.Arch Intern Med.1993;153:1557–1562.
- ,,,.Warfarin‐associated hemorrhage and cerebral amyloid angiopathy: a genetic and pathologic study.Neurology.2000;55(7):947–951.
- ,,, et al.Treatment of warfarin‐associated intracerebral hemorrhage: literature review and expert opinion.Mayo Clinic Proc.2007;82(1):82–92.
- ,,,,.Urgent reversal of warfarin with prothrombin complex concentrate.J Thromb Haemost.2006;4(5):967–970.
- ,.The headache over warfarin in British neurosurgical intensive care units: a national survey of current practice.Intensive Care Med.2007;33(11):1946–1953.
- ,,, et al.Timing of fresh frozen plasma administration and rapid correction of coagulopathy in warfarin‐related intracerebral hemorrhage.Stroke.2006;37(1):151–155.
- ,,,.Progression of warfarin‐associated intracerebral hemorrhage after INR normalization with FFP.Neurology.2006;67(7):1272–1274.
- ,,, et al.Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study.Blood Coagul Fibrinolysis.2007;18(6):565–570.
- ,,, et al.Guidelines for the use of fresh‐frozen plasma, cryoprecipitate and cryosupernatant.Br J Hematol.2004;126(1):11–28.
- ,,,,,.The pharmacology and management of vitamin K antagonists. The seventh ACCP conference on antithrombotic and thrombolytic therapy.Chest.2004;126:204s–33s.
- ,,, et al.Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy. Comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates.Stroke.2006;37:1465.
- ,.Recombinant factor VIIa.BioDrugs.1999;12(1):71–77.
- ,,, et al.Impact of recombinant activated factor VII on health‐related quality of life after intracerebral hemorrhage.Cerebrovasc Dis.2007;24(2–3):219–225.
- ,,, et al.Recombinant activated factor VII for acute intracerebral hemorrhage: US phase IIA trial.Neurocrit Care.2006;4(3):206–214.
- ,,, et al.Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial.Lancet.2005;365(9457):387–397.
- ,,,,,.Advances in the care of patients with intracerebral hemorrhage.Mayo Clin Proc.2007;82(8):987–990.
- ,,,.Surgery for intracerebral hemorrhage.Neurol Sci.2004;25:s10–s11.
- ,,,.Endoscopy‐guided removal of spontaneous intracerebral hemorrhage: comparison with computer tomography‐guided stereotactic evacuation.Childs Nerv Syst.2007;23(6):677–683.
- ,.Endovascular reperfusion therapy in acute ischaemic stroke.Acta Neurol Scand Suppl.2007;187:22–29.
- .Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I.AJNR Am J Neuroradiol.2006;27(6):1177–1182.
- ,.Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation.Ann Thorac Surg.1996;61(2):755–759.
- ,,, et al.Percutaneous devices for stroke prevention.Cardiovasc Revasc Med.2007;8(3):216–225.
- ,,.Sealing the left atrial appendage: ready for prime time?Am J Med Sci.2007;333(5):285–289.
- ,,, et al.Initial worldwide experience with the WATCHMAN left atrial appendage system for stroke prevention in atrial fibrillation.J Am Coll Cardiol.2007;49(13):1490–1495.
- ,.Left atrial appendage exclusion for stroke prevention in patients with nonrheumatic atrial fibrillation.Stroke.2007;38(2 suppl):624–630.
- FDA News. FDA clears genetic lab test for warfarin sensitivity. Available at: http://www.fda.gov/bbs/topics/news/2007/new01701.html. Accessed January2008.
- .Pharmacogenomics and warfarin therapy.Issues Emerg Health Technol.2007;(104):1–8.
- ,,.Advancing stroke therapeutics through genetic understanding.Curr Drug Targets.2007;8(7):850–859.
INITIAL EVALUATION
The approach to patients with acute stroke symptoms should always start with the stabilization of the airway, breathing, and circulation. A fast clinical investigation for possible mimickers of an acute stroke (head trauma, migraines, epilepsy, infection, hypoglycemia, other metabolic derangements, and intoxications) is the next step. The history and physical examination should be guided by the National Institutes of Health stroke scale, which has been widely accepted by the American Stroke Association (ASA), the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.2, 9 Strict control of electrolytes, glucose, and fever, management of blood pressure depending on thetype of stroke, and prophylaxis for deep vein thrombosis/pulmonary embolism, aspiration, dehydration, hypoxemia, malnutrition, and pressure sores should be initiated.9, 10 All patients with suspected acute stroke must be promptly assessed for thrombolytic therapy on the basis of the time since onset of symptoms and the National Institutes of Health stroke scale. Noncontrast computed tomography of the brain is the first step for differentiating between ischemic and hemorrhagic events.3, 9 There is an increased interest in the use of magnetic resonance imaging to detect acute intracranial hemorrhage (ICH) and its ability to detect stroke earlier than computed tomography.911 Multimodal computed tomography and magnetic resonance imaging provide additional information that will improve the diagnosis of ischemic stroke, and they have been added as a class I recommendation to the most recent stroke guidelines.9, 12 Computed tomographic angiography and perfusion computed tomography may precisely describe details regarding the site of occlusion, infarct core, salvageable brain tissue, and collateral flow that can improve patient selection for intravenous or intra‐arterial thrombolysis and exclude stroke mimics.9, 13
ISCHEMIC STROKE
Thrombolysis
In the setting of acute ischemic stroke, the patient should be promptly evaluated for thrombolytic therapy according to the American College of Chest Physicians guidelines.14 Intravenous r‐TPA (recombinant tissue plasminogen activator) is given only to 1% to 2% of stroke patients in the United States. This low percentage is mainly due to delayed presentation to an emergency department beyond the 3‐hour treatment window.15 Clear benefit has been proven for eligible patients if thrombolytic therapy is administered within 3 hours from the initiation of symptoms, although no subgroup analysis has been done in patients with atrial fibrillation.9 The efficacy of intravenous thrombolysis within the 3‐hour time window is similar between different stroke subtypes; therefore, its administration should not be delayed in order to investigate its etiology.16 Intravenous thrombolysis remains the standard of care, but recent studies have demonstrated that intra‐arterial administration, despite its risks, may be more effective in selected patients.9, 1719 Patients most likely to benefit from intra‐arterial thrombolysis are those with middle cerebral artery occlusion of less than 6 hours (Prolyse in Acute Cerebral Thromboembolism Trials I and II) and patients with severe basilar artery stroke.17, 19 A recent study in Germany has demonstrated that intra‐arterial thrombolysis may be superior to intravenous thrombolysis in the 3‐ to 6‐hour treatment window.19 The updated 2007 guidelines from the American Heart Association (AHA)/ASA have included intra‐arterial thrombolysis for specific patients who are not eligible for intravenous thrombolysis when this can be performed at experienced stroke centers.9 Thrombolysis reduces overall disability and improves the quality of life in appropriately selected patients. The risk of hemorrhage is approximately 5.2%.20 After intravenous thrombolysis, approximately one‐third of patients ultimately develop re‐occlusion of the artery, especially patients with only partial recanalization. This may lead to neurologic deterioration and higher in‐hospital mortality.21 According to more recent studies, ultrasound‐enhanced thrombolysis may augment tissue plasminogen activator induced arterial recanalization by continuous transcranial Doppler.22 Symptomatic hemorrhagic transformation of the infarction remains the primary concern with the administration of intravenous rtTPA.23, 24 Despite the apparent risks of ICH, atrial fibrillation patients not on warfarin should always be promptly referred for thrombolysis whenever they are eligible.
Heparin
For many years, clinicians have believed in the role of heparin in patients with atrial fibrillation, especially after intracranial hemorrhage is excluded by negative initial noncontrast head computed tomography.25 The most obvious pathophysiologic mechanism in patients with atrial fibrillation is cardioembolism. Therefore, it was believed that heparin could contribute to the resolution of the responsible clot. Two large international trials (the Heparin in Acute Embolic Stroke Trial and the International Stroke Trial), confirmed by multiple smaller ones, have investigated the use of heparin (unfractionated or low‐molecular‐weight heparin) at therapeutic doses in the setting of an acute ischemic event.2628 Surprisingly, none of them showed a statistically significant benefit, but instead they showed a clear increase in hemorrhagic events. Therefore, routine use of unfractionated heparin or low‐molecular‐weight heparin at therapeutic doses should be avoided in the acute setting of a stroke.28, 29
Aspirin
Among the antiplatelet agents, aspirin is the only well‐studied agent for the treatment of acute ischemic stroke. It has been proven that during the first 24 hours after stroke, there is substantial platelet activation that can be inhibited by aspirin.30, 31 Two major trials, the Chinese Acute Stroke Trial and the International Stroke Trial, have demonstrated the benefit of early aspirin use in patients with stroke and atrial fibrillation.30 Both proved a decrease in recurrent stroke without a significant increase in hemorrhaging. The recommended dose of aspirin is 325 mg/day.9 Currently, clopidogrel alone or in combination with aspirin and the intravenous administration of antiplatelet agents that inhibit the glycoprotein IIb/IIIa receptor are class III recommendations. They should not be used outside the setting of clinical trials.9
Warfarin
It is well known that atrial fibrillation increases the risk of ischemic stroke by a factor of 5.32 Studies have shown that maintaining the INR above 2.0 decreases not only the frequency but also the severity and mortality of ischemic events.4, 8, 32 The National Anticoagulation Benchmark Outcomes Report has shown that in the highest risk atrial fibrillation patients, only 55% receive warfarin and 21% do not receive aspirin or warfarin.33 This discrepancy results from the fact that warfarin is the second most common drug, after insulin, responsible for adverse drug events in emergency room visits. In atrial fibrillation patients on warfarin who present to the emergency with an acute stroke, there are no clear guidelines regarding the continued use of warfarin at therapeutic doses (target INR = 2.03.0). Warfarin is usually not initiated in the acute setting until the patient is medically stable. The exact time at which warfarin can be started or resumed after an acute ischemic stroke remains to be determined.34 Usually, it is preferable to start it within 1 week after the event, given the risk of early recurrent acute stroke during the next 2 to 4 weeks after the initial stroke.35
HEMORRHAGIC STROKE/ICH
Introduction
The risk of spontaneous ICH is 0.15%/year in patients over 70 years old and increases to 0.3% to 0.8% when patients are on therapeutic doses of warfarin with INR between 2 and 3.36, 37 Given the multiple interactions of warfarin with other medications, this is a significant concern because ICH is associated with substantial neurological deterioration.38 Although most warfarin‐induced ICH occurs in patients with therapeutic INR, it becomes the most prevalent mechanism when the INR exceeds 5.0, and it should be highly suspected.1, 4 Therefore, prompt determination of INR is critical in the initial evaluation of acute stroke in patients with atrial fibrillation. Age is the most important predisposing factor for ICH in patients with atrial fibrillation. There is almost a 50% increase in warfarin‐induced bleeding for every decade of age above 40.39 Cerebral amyloid angiopathy plays an important role in warfarin‐associated lobar ICH in the elderly, and it may contribute to the patient candidacy for warfarin treatment in the near future.40 On the other hand, a hemorrhagic stroke can be an iatrogenic complication of initiation of warfarin, heparin, or early thrombolysis because symptomatic hemorrhagic transformation of the infarction is the main and most lethal side effect of intravenous rtTPA in the treatment of acute ischemic stroke.24 ICH is associated with a 30% to 50% mortality rate, and it represents the most lethal and least treatable form of stroke.32 It has been suggested that macroalbuminuria is an independent predictor of hemorrhagic transformation and particularly of severe hemorrhage in patients with acute ischemic stroke, but specific guidelines for screening or special management of those patients do not currently exist.33 ICH is a medical emergency with high mortality and should be recognized and treated promptly. Recently, the AHA and ASA have published updated guidelines for the management of spontaneous ICH in adults.12
Vitamin K
All experts agree that anticoagulation should be urgently reversed in the setting of ICH. Although high doses of intravenous vitamin K (1020 mg) are usually enough to reverse the anticoagulant effect of warfarin, it may take up to 12 to 24 hours to act, and it depends on intact liver function. Given the high mortality of this condition, vitamin K as monotherapy is considered inadequate, and a more aggressive approach is recommended.41
Fresh Frozen Plasma (FFP)
In the United States, for many years FFP has been considered the standard of care for the acute reversal of warfarin‐associated anticoagulation.42 In general, 10 to 15 cc/kg FFP is used.43 Timing rather than dosage seems to be more important for a better clinical outcome.44 The use of FFP is complicated by the delayed time for thawing and compatibility check, volume overload, and sometimes inadequate and unpredictable correction. The median time for door‐to‐INR normalization is 30 hours, which is a significant delay for such a potentially fatal condition. Another possible complication of FFP is the report of increasing hematomas.45
Prothrombin Complex Concentrates (PCCs)
PCCs contain vitamin K dependent coagulation factors II, VII, IX, and X, the factors deficient in warfarin therapy.44, 46 Therefore, a PCC dose of 25 to 59 U/kg has been used in life‐threatening bleeding, resulting in a decrease in the median INR from 3.8 to 1.3 immediately after administration.42 PCCs should always be given with vitamin K. Thrombotic events have been described with the infusion of PCCs, but no clear guidelines have been published.42 A recent study from the Mayo Clinic showed that many experts suggest its use in the urgent condition of warfarin‐associated ICH.41 PCCs are widely used in the European community and have previously been cited as the agent of choice for urgent warfarin reversal.42, 47, 48 A recent study comparing PCCs with FFP and vitamin K has demonstrated that PCCs may be superior to FFP and vitamin K by reducing the risk of hematoma growth.49
Recombinant Factor VIIa
Recombinant factor VIIa is a preparation of activated coagulation factor VII (factor VIIa) that is produced by recombinant DNA technology.50 It was initially used for the treatment of inhibitors in patients with hemophilia. It has also been used in the past to correct anticoagulation in patients with acute ICH,36 but most studies have been done in patients with hemophilia or factor VII deficiency.50 Major limitations include cost, prothrombotic potential, and lack of correction of other coagulation factors dependent on vitamin K. Studies have shown that factor VII may be a safe, rapid, and effective way of reversing anticoagulation and may offer an improved quality of life to patients with ICH.51, 52 Factor Seven for Acute Hemorrhagic Stroke Treatment, a large phase III trial, is in progress, but preliminary results are controversial regarding the reduction in the size of hemorrhage, mortality, and improvement of functional outcome.32 In a recent article from the Mayo Clinic,41 several experts on clinical stroke, neurologic intensive care, and hematology suggest its use, alone or with FFP, for the urgent reversal of INR in the clinical setting of warfarin‐associated ICH. Currently, according to the 2007 AHA/ASA updated guidelines, recombinant factor VIIa can be administered within the first 3 to 4 hours after onset of ICH to slow progression of bleeding, although its efficacy and safety remain to be confirmed (class IIb recommendation).12
Surgical Evacuation
Despite the clear guidelines for the indications of surgery in spontaneous intracranial bleeding,12 the role of surgical evacuation in patients with supratherapeutic INR is not well defined. Many neurosurgeons are reluctant to operate in the setting of impaired hemostasis. The International Surgical Trial in Intracerebral Hemorrhage showed no clear benefit of early neurosurgical intervention compared to conservative treatment.53 Different surgical trials have shown different outcomes.54 The selection of patients who would benefit from surgery depends on the location and size of the hemorrhage, coagulation status, and Glasgow Coma Scale.55 Patients with rapidly expanding hematomas in a surgically accessible intracranial territory are more likely to benefit from a neurosurgical intervention. Newer surgical techniques with a computed‐tomography‐guided stereotactic approach or endoscopy‐guided evacuation in emerging ICH may offer better outcomes.56
RECENT ADVANCES
Mechanical Embolectomy
Mechanical embolectomy is a growing field of neurology with a promising interventional approach to the treatment of embolic strokes.57, 58 Patients with atrial fibrillation will probably be one of the patient groups who will receive maximum benefit when the efficacy and safety of the procedure are established. Endovascular reperfusion via mechanical embolectomy is offered to patients who are ineligible for thrombolytics, and it extends the time window up to 8 hours.58 For the first time, in 2007 the AHA/ASA guidelines have included the Mechanical Embolus Removal in Cerebral Ischemia device as a reasonable intervention for extraction of intra‐arterial thrombi in carefully selected patients.9
Left Atrial Appendage (LAA) Occlusion
The LAA is the source of 91% of embolic thrombi in patients with atrial fibrillation.59 Therefore, surgical or percutaneous removal or occlusion of the LAA would be an important treatment option, especially in high‐risk patients intolerant of warfarin or with recurrent strokes, despite anticoagulation. Several surgical techniques and percutaneous LAA occlusion devices have been studied with different success rates and safety characteristics.6063 Currently, there are no official guidelines for the use of those interventions.
Genetic Testing for Warfarin Sensitivity
Warfarin is the second most common drug, after insulin, to require emergency room visits for adverse drug events. In September 2007, the Food and Drug Administration approved the Nanosphere Verigene Warfarin Metabolism Nucleic Acid Test, which detects variants of 2 genes (CYP2C9 and VKORC1) implicated in the unexpected response to warfarin.6466 Guidelines for the applied use of these tests are currently under development.66
CONCLUSION
On average, there is a new stroke every 45 seconds, and every 3 to 4 minutes, someone dies from a stroke in the United States. Atrial fibrillation accounts for one‐fourth of all strokes in the elderly population. Acute stroke in anticoagulated patients with atrial fibrillation is a common, challenging scenario in emergency departments because many questions remain unanswered (Table 1). A special and prompt approach from the clinician is needed to achieve effective management and avoid potentially fatal complications (Figure 2). Many hospitals in the United States have formed stroke teams to ensure prompt clinical and radiographic assessment of stroke patients. Only early recognition of cardioembolic or hemorrhagic strokes in atrial fibrillation patients can lead to aggressive management of this potentially fatal and disabling condition.
| 1. When can warfarin be safely started after an acute cardioembolic stroke? |
| 2. Could heparin in lower doses be beneficial without the risk of bleeding? |
| 3. Should we repeat thrombolysis in cases of re‐occlusion? |
| 4. What is the role of other antithrombotic and antiplatelet agents in these patients? |
INITIAL EVALUATION
The approach to patients with acute stroke symptoms should always start with the stabilization of the airway, breathing, and circulation. A fast clinical investigation for possible mimickers of an acute stroke (head trauma, migraines, epilepsy, infection, hypoglycemia, other metabolic derangements, and intoxications) is the next step. The history and physical examination should be guided by the National Institutes of Health stroke scale, which has been widely accepted by the American Stroke Association (ASA), the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.2, 9 Strict control of electrolytes, glucose, and fever, management of blood pressure depending on thetype of stroke, and prophylaxis for deep vein thrombosis/pulmonary embolism, aspiration, dehydration, hypoxemia, malnutrition, and pressure sores should be initiated.9, 10 All patients with suspected acute stroke must be promptly assessed for thrombolytic therapy on the basis of the time since onset of symptoms and the National Institutes of Health stroke scale. Noncontrast computed tomography of the brain is the first step for differentiating between ischemic and hemorrhagic events.3, 9 There is an increased interest in the use of magnetic resonance imaging to detect acute intracranial hemorrhage (ICH) and its ability to detect stroke earlier than computed tomography.911 Multimodal computed tomography and magnetic resonance imaging provide additional information that will improve the diagnosis of ischemic stroke, and they have been added as a class I recommendation to the most recent stroke guidelines.9, 12 Computed tomographic angiography and perfusion computed tomography may precisely describe details regarding the site of occlusion, infarct core, salvageable brain tissue, and collateral flow that can improve patient selection for intravenous or intra‐arterial thrombolysis and exclude stroke mimics.9, 13
ISCHEMIC STROKE
Thrombolysis
In the setting of acute ischemic stroke, the patient should be promptly evaluated for thrombolytic therapy according to the American College of Chest Physicians guidelines.14 Intravenous r‐TPA (recombinant tissue plasminogen activator) is given only to 1% to 2% of stroke patients in the United States. This low percentage is mainly due to delayed presentation to an emergency department beyond the 3‐hour treatment window.15 Clear benefit has been proven for eligible patients if thrombolytic therapy is administered within 3 hours from the initiation of symptoms, although no subgroup analysis has been done in patients with atrial fibrillation.9 The efficacy of intravenous thrombolysis within the 3‐hour time window is similar between different stroke subtypes; therefore, its administration should not be delayed in order to investigate its etiology.16 Intravenous thrombolysis remains the standard of care, but recent studies have demonstrated that intra‐arterial administration, despite its risks, may be more effective in selected patients.9, 1719 Patients most likely to benefit from intra‐arterial thrombolysis are those with middle cerebral artery occlusion of less than 6 hours (Prolyse in Acute Cerebral Thromboembolism Trials I and II) and patients with severe basilar artery stroke.17, 19 A recent study in Germany has demonstrated that intra‐arterial thrombolysis may be superior to intravenous thrombolysis in the 3‐ to 6‐hour treatment window.19 The updated 2007 guidelines from the American Heart Association (AHA)/ASA have included intra‐arterial thrombolysis for specific patients who are not eligible for intravenous thrombolysis when this can be performed at experienced stroke centers.9 Thrombolysis reduces overall disability and improves the quality of life in appropriately selected patients. The risk of hemorrhage is approximately 5.2%.20 After intravenous thrombolysis, approximately one‐third of patients ultimately develop re‐occlusion of the artery, especially patients with only partial recanalization. This may lead to neurologic deterioration and higher in‐hospital mortality.21 According to more recent studies, ultrasound‐enhanced thrombolysis may augment tissue plasminogen activator induced arterial recanalization by continuous transcranial Doppler.22 Symptomatic hemorrhagic transformation of the infarction remains the primary concern with the administration of intravenous rtTPA.23, 24 Despite the apparent risks of ICH, atrial fibrillation patients not on warfarin should always be promptly referred for thrombolysis whenever they are eligible.
Heparin
For many years, clinicians have believed in the role of heparin in patients with atrial fibrillation, especially after intracranial hemorrhage is excluded by negative initial noncontrast head computed tomography.25 The most obvious pathophysiologic mechanism in patients with atrial fibrillation is cardioembolism. Therefore, it was believed that heparin could contribute to the resolution of the responsible clot. Two large international trials (the Heparin in Acute Embolic Stroke Trial and the International Stroke Trial), confirmed by multiple smaller ones, have investigated the use of heparin (unfractionated or low‐molecular‐weight heparin) at therapeutic doses in the setting of an acute ischemic event.2628 Surprisingly, none of them showed a statistically significant benefit, but instead they showed a clear increase in hemorrhagic events. Therefore, routine use of unfractionated heparin or low‐molecular‐weight heparin at therapeutic doses should be avoided in the acute setting of a stroke.28, 29
Aspirin
Among the antiplatelet agents, aspirin is the only well‐studied agent for the treatment of acute ischemic stroke. It has been proven that during the first 24 hours after stroke, there is substantial platelet activation that can be inhibited by aspirin.30, 31 Two major trials, the Chinese Acute Stroke Trial and the International Stroke Trial, have demonstrated the benefit of early aspirin use in patients with stroke and atrial fibrillation.30 Both proved a decrease in recurrent stroke without a significant increase in hemorrhaging. The recommended dose of aspirin is 325 mg/day.9 Currently, clopidogrel alone or in combination with aspirin and the intravenous administration of antiplatelet agents that inhibit the glycoprotein IIb/IIIa receptor are class III recommendations. They should not be used outside the setting of clinical trials.9
Warfarin
It is well known that atrial fibrillation increases the risk of ischemic stroke by a factor of 5.32 Studies have shown that maintaining the INR above 2.0 decreases not only the frequency but also the severity and mortality of ischemic events.4, 8, 32 The National Anticoagulation Benchmark Outcomes Report has shown that in the highest risk atrial fibrillation patients, only 55% receive warfarin and 21% do not receive aspirin or warfarin.33 This discrepancy results from the fact that warfarin is the second most common drug, after insulin, responsible for adverse drug events in emergency room visits. In atrial fibrillation patients on warfarin who present to the emergency with an acute stroke, there are no clear guidelines regarding the continued use of warfarin at therapeutic doses (target INR = 2.03.0). Warfarin is usually not initiated in the acute setting until the patient is medically stable. The exact time at which warfarin can be started or resumed after an acute ischemic stroke remains to be determined.34 Usually, it is preferable to start it within 1 week after the event, given the risk of early recurrent acute stroke during the next 2 to 4 weeks after the initial stroke.35
HEMORRHAGIC STROKE/ICH
Introduction
The risk of spontaneous ICH is 0.15%/year in patients over 70 years old and increases to 0.3% to 0.8% when patients are on therapeutic doses of warfarin with INR between 2 and 3.36, 37 Given the multiple interactions of warfarin with other medications, this is a significant concern because ICH is associated with substantial neurological deterioration.38 Although most warfarin‐induced ICH occurs in patients with therapeutic INR, it becomes the most prevalent mechanism when the INR exceeds 5.0, and it should be highly suspected.1, 4 Therefore, prompt determination of INR is critical in the initial evaluation of acute stroke in patients with atrial fibrillation. Age is the most important predisposing factor for ICH in patients with atrial fibrillation. There is almost a 50% increase in warfarin‐induced bleeding for every decade of age above 40.39 Cerebral amyloid angiopathy plays an important role in warfarin‐associated lobar ICH in the elderly, and it may contribute to the patient candidacy for warfarin treatment in the near future.40 On the other hand, a hemorrhagic stroke can be an iatrogenic complication of initiation of warfarin, heparin, or early thrombolysis because symptomatic hemorrhagic transformation of the infarction is the main and most lethal side effect of intravenous rtTPA in the treatment of acute ischemic stroke.24 ICH is associated with a 30% to 50% mortality rate, and it represents the most lethal and least treatable form of stroke.32 It has been suggested that macroalbuminuria is an independent predictor of hemorrhagic transformation and particularly of severe hemorrhage in patients with acute ischemic stroke, but specific guidelines for screening or special management of those patients do not currently exist.33 ICH is a medical emergency with high mortality and should be recognized and treated promptly. Recently, the AHA and ASA have published updated guidelines for the management of spontaneous ICH in adults.12
Vitamin K
All experts agree that anticoagulation should be urgently reversed in the setting of ICH. Although high doses of intravenous vitamin K (1020 mg) are usually enough to reverse the anticoagulant effect of warfarin, it may take up to 12 to 24 hours to act, and it depends on intact liver function. Given the high mortality of this condition, vitamin K as monotherapy is considered inadequate, and a more aggressive approach is recommended.41
Fresh Frozen Plasma (FFP)
In the United States, for many years FFP has been considered the standard of care for the acute reversal of warfarin‐associated anticoagulation.42 In general, 10 to 15 cc/kg FFP is used.43 Timing rather than dosage seems to be more important for a better clinical outcome.44 The use of FFP is complicated by the delayed time for thawing and compatibility check, volume overload, and sometimes inadequate and unpredictable correction. The median time for door‐to‐INR normalization is 30 hours, which is a significant delay for such a potentially fatal condition. Another possible complication of FFP is the report of increasing hematomas.45
Prothrombin Complex Concentrates (PCCs)
PCCs contain vitamin K dependent coagulation factors II, VII, IX, and X, the factors deficient in warfarin therapy.44, 46 Therefore, a PCC dose of 25 to 59 U/kg has been used in life‐threatening bleeding, resulting in a decrease in the median INR from 3.8 to 1.3 immediately after administration.42 PCCs should always be given with vitamin K. Thrombotic events have been described with the infusion of PCCs, but no clear guidelines have been published.42 A recent study from the Mayo Clinic showed that many experts suggest its use in the urgent condition of warfarin‐associated ICH.41 PCCs are widely used in the European community and have previously been cited as the agent of choice for urgent warfarin reversal.42, 47, 48 A recent study comparing PCCs with FFP and vitamin K has demonstrated that PCCs may be superior to FFP and vitamin K by reducing the risk of hematoma growth.49
Recombinant Factor VIIa
Recombinant factor VIIa is a preparation of activated coagulation factor VII (factor VIIa) that is produced by recombinant DNA technology.50 It was initially used for the treatment of inhibitors in patients with hemophilia. It has also been used in the past to correct anticoagulation in patients with acute ICH,36 but most studies have been done in patients with hemophilia or factor VII deficiency.50 Major limitations include cost, prothrombotic potential, and lack of correction of other coagulation factors dependent on vitamin K. Studies have shown that factor VII may be a safe, rapid, and effective way of reversing anticoagulation and may offer an improved quality of life to patients with ICH.51, 52 Factor Seven for Acute Hemorrhagic Stroke Treatment, a large phase III trial, is in progress, but preliminary results are controversial regarding the reduction in the size of hemorrhage, mortality, and improvement of functional outcome.32 In a recent article from the Mayo Clinic,41 several experts on clinical stroke, neurologic intensive care, and hematology suggest its use, alone or with FFP, for the urgent reversal of INR in the clinical setting of warfarin‐associated ICH. Currently, according to the 2007 AHA/ASA updated guidelines, recombinant factor VIIa can be administered within the first 3 to 4 hours after onset of ICH to slow progression of bleeding, although its efficacy and safety remain to be confirmed (class IIb recommendation).12
Surgical Evacuation
Despite the clear guidelines for the indications of surgery in spontaneous intracranial bleeding,12 the role of surgical evacuation in patients with supratherapeutic INR is not well defined. Many neurosurgeons are reluctant to operate in the setting of impaired hemostasis. The International Surgical Trial in Intracerebral Hemorrhage showed no clear benefit of early neurosurgical intervention compared to conservative treatment.53 Different surgical trials have shown different outcomes.54 The selection of patients who would benefit from surgery depends on the location and size of the hemorrhage, coagulation status, and Glasgow Coma Scale.55 Patients with rapidly expanding hematomas in a surgically accessible intracranial territory are more likely to benefit from a neurosurgical intervention. Newer surgical techniques with a computed‐tomography‐guided stereotactic approach or endoscopy‐guided evacuation in emerging ICH may offer better outcomes.56
RECENT ADVANCES
Mechanical Embolectomy
Mechanical embolectomy is a growing field of neurology with a promising interventional approach to the treatment of embolic strokes.57, 58 Patients with atrial fibrillation will probably be one of the patient groups who will receive maximum benefit when the efficacy and safety of the procedure are established. Endovascular reperfusion via mechanical embolectomy is offered to patients who are ineligible for thrombolytics, and it extends the time window up to 8 hours.58 For the first time, in 2007 the AHA/ASA guidelines have included the Mechanical Embolus Removal in Cerebral Ischemia device as a reasonable intervention for extraction of intra‐arterial thrombi in carefully selected patients.9
Left Atrial Appendage (LAA) Occlusion
The LAA is the source of 91% of embolic thrombi in patients with atrial fibrillation.59 Therefore, surgical or percutaneous removal or occlusion of the LAA would be an important treatment option, especially in high‐risk patients intolerant of warfarin or with recurrent strokes, despite anticoagulation. Several surgical techniques and percutaneous LAA occlusion devices have been studied with different success rates and safety characteristics.6063 Currently, there are no official guidelines for the use of those interventions.
Genetic Testing for Warfarin Sensitivity
Warfarin is the second most common drug, after insulin, to require emergency room visits for adverse drug events. In September 2007, the Food and Drug Administration approved the Nanosphere Verigene Warfarin Metabolism Nucleic Acid Test, which detects variants of 2 genes (CYP2C9 and VKORC1) implicated in the unexpected response to warfarin.6466 Guidelines for the applied use of these tests are currently under development.66
CONCLUSION
On average, there is a new stroke every 45 seconds, and every 3 to 4 minutes, someone dies from a stroke in the United States. Atrial fibrillation accounts for one‐fourth of all strokes in the elderly population. Acute stroke in anticoagulated patients with atrial fibrillation is a common, challenging scenario in emergency departments because many questions remain unanswered (Table 1). A special and prompt approach from the clinician is needed to achieve effective management and avoid potentially fatal complications (Figure 2). Many hospitals in the United States have formed stroke teams to ensure prompt clinical and radiographic assessment of stroke patients. Only early recognition of cardioembolic or hemorrhagic strokes in atrial fibrillation patients can lead to aggressive management of this potentially fatal and disabling condition.
| 1. When can warfarin be safely started after an acute cardioembolic stroke? |
| 2. Could heparin in lower doses be beneficial without the risk of bleeding? |
| 3. Should we repeat thrombolysis in cases of re‐occlusion? |
| 4. What is the role of other antithrombotic and antiplatelet agents in these patients? |
- ,.The Atlas of Heart Disease and Stroke.Geneva, Switzerland:World Health Organization;2004.
- National Institute of Neurological Disorders and Stroke. NIH Stroke Scale. Available at: http://www.ninds.nih.gov/doctors/NIH_stroke_scale_booklet.pdf. Accessed January2008.
- Royal College of Physicians.National Clinical Guidelines for Stroke.2nd ed.Prepared by the Intercollegiate Stroke Working Party.London:RCP,2004.
- The European Atrial Fibrillation Trial Study Group.Optimal oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and recent cerebral ischemia.N Engl J Med.1995;333:5–10.
- ,,, et al.Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation.Ann Intern Med.2004;141(10):745–752.
- ,.Antithrombotic treatment in atrial fibrillation.Heart.2007;93(1):39–44.
- ,,, et al.Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin.Circulation.2004;110(16):2287–2292.
- ,,.Atrial fibrillation.Med J Aust.2007;186(4):197–202.
- ,,, et al.Guidelines for the early management of adults with ischemic stroke. A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups.Stroke.2007;38(5):1655–1711.
- ,,, et al.MRI of acute post‐ischemic cerebral hemorrhage in stroke patients: diagnosis with T2*‐weighted gradient‐echo sequences.Neuroradiology.2001;43(10):809–815.
- ,,, et al.Emergency imaging of cerebrovascular accidents.J Neuroradiol.2004;31(4):327–333.
- ,,, et al.Guidelines for the management of spontaneous intracerebral hemorrhage in adults. 2007 update. A guideline from the American Heart Association, American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group.Stroke.2007;38(6):2001–2023.
- ,,,,,.Systematic comparison of perfusion‐CT and CT‐angiography in acute stroke patients.Ann Neurol.2007;61(6):533–543.
- ,,,,.Antithrombotic and thrombolytic therapy for ischemic stroke: the seventh ACCP conference on antithrombotic and thrombolytic therapy.Chest.2004;126(3 suppl):S483–S512.
- .Acute ischemic stroke treatment in 2007.Circulation.2007;116(13):1504–1514.
- ,,,,.Efficacy of IV tissue plasminogen activator in acute stroke: does stroke subtype really matter?Neurology.2003;61(1):71–75.
- ,,,,,.Efficacy of intraarterial thrombolysis of basilar artery stroke.J Stroke Cerebrovasc Dis.1999;8(1):22–27.
- ,,, et al.Treatment of acute ischemic brain infarction with the assistance of local intraarterial thrombolysis with recombinant tissue‐type plasminogen activator.Acta Radiol.2007;48(7):774–780.
- ,,,,.Intra‐arterial thrombolysis using rt‐PA in patients with acute stroke due to vessel occlusion of anterior and/or posterior cerebral circulation.Neuroradiology.2008;50(1):75–83.
- .Tissue plasminogen activator for acute ischemic stroke in clinical practice: a meta‐analysis of safety data.Stroke.2003;34:2847–2850.
- ,.Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator.Neurology.2002;59:862–867.
- ,,, et al.Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke.Stroke.2007;38(3):948–954.
- ,,,.Thrombolysis for acute ischemic stroke.Cochrane Database Syst Rev.2003;(3):CD000213.
- ,,, et al.Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt‐PA stroke trials.Lancet.2004;363:768–774.
- ,,,,,.Trends in medical care of hospitalized stroke patients between 1980 and 1990: the Minnesota stroke survey.J Stroke Cerebrovasc Dis.1998;7(1):76–84.
- ,,,.Low molecular‐weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double‐blind randomized study. HAEST Study Group. Heparin in Acute Embolic Stroke Trial.Lancet.2000;355(9211):1205–1210.
- International Stroke Trial Collaborative Group.The International Stroke Trial (IST): a randomized trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischemic stroke.Lancet.1997;349(9065):1569–1581.
- .Emergent use of anticoagulation for treatment of patients with ischemic stroke.Stroke.2002;33:856–861.
- ,,,.Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke: a meta‐analysis of randomized controlled trials.Stroke.2007;38(2):423–430.
- .The results of CAPRIE, IST and CAST. International Stroke Trial. Chinese Acute Stroke Trial.Thromb Res1998;92(1 suppl 1):S13–S16.
- ,,,,.Platelet activation and lipid peroxidation in patients with acute ischemic stroke.Stroke.1997;28:1557–1563.
- ,,, et al.Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation elaine.N Engl J Med.2003;349:1019–1026.
- ,,,.Hospitalized patients with atrial fibrillation and a high risk of stroke are not being provided with adequate anticoagulation.J Am Coll Cardiol.2005;46(9):1729–1736.
- ,.Preventing stroke in patients with atrial fibrillation.JAMA.1999;281(19):1830–1835.
- ,.Atrial fibrillation, stroke, and acute antithrombotic therapy: analysis of randomized clinical trials.Stroke.2002;33(11):2722–2727.
- ,,, et al.Recombinant factor VIIa for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage.Mayo Clin Proc.2004;79(12):1495–1500.
- ,,,.Managing the therapeutic dilemma: patients with spontaneous intracerebral hemorrhage and urgent need for anticoagulation.J Neurol.2000;247(3):209–214.
- ,,, et al.Early hemorrhage growth in patients with intracerebral hemorrhage.Stroke.1997;28:1–5.
- ,,.Bleeding complications in oral anticoagulant therapy: an analysis of risk factors.Arch Intern Med.1993;153:1557–1562.
- ,,,.Warfarin‐associated hemorrhage and cerebral amyloid angiopathy: a genetic and pathologic study.Neurology.2000;55(7):947–951.
- ,,, et al.Treatment of warfarin‐associated intracerebral hemorrhage: literature review and expert opinion.Mayo Clinic Proc.2007;82(1):82–92.
- ,,,,.Urgent reversal of warfarin with prothrombin complex concentrate.J Thromb Haemost.2006;4(5):967–970.
- ,.The headache over warfarin in British neurosurgical intensive care units: a national survey of current practice.Intensive Care Med.2007;33(11):1946–1953.
- ,,, et al.Timing of fresh frozen plasma administration and rapid correction of coagulopathy in warfarin‐related intracerebral hemorrhage.Stroke.2006;37(1):151–155.
- ,,,.Progression of warfarin‐associated intracerebral hemorrhage after INR normalization with FFP.Neurology.2006;67(7):1272–1274.
- ,,, et al.Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study.Blood Coagul Fibrinolysis.2007;18(6):565–570.
- ,,, et al.Guidelines for the use of fresh‐frozen plasma, cryoprecipitate and cryosupernatant.Br J Hematol.2004;126(1):11–28.
- ,,,,,.The pharmacology and management of vitamin K antagonists. The seventh ACCP conference on antithrombotic and thrombolytic therapy.Chest.2004;126:204s–33s.
- ,,, et al.Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy. Comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates.Stroke.2006;37:1465.
- ,.Recombinant factor VIIa.BioDrugs.1999;12(1):71–77.
- ,,, et al.Impact of recombinant activated factor VII on health‐related quality of life after intracerebral hemorrhage.Cerebrovasc Dis.2007;24(2–3):219–225.
- ,,, et al.Recombinant activated factor VII for acute intracerebral hemorrhage: US phase IIA trial.Neurocrit Care.2006;4(3):206–214.
- ,,, et al.Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial.Lancet.2005;365(9457):387–397.
- ,,,,,.Advances in the care of patients with intracerebral hemorrhage.Mayo Clin Proc.2007;82(8):987–990.
- ,,,.Surgery for intracerebral hemorrhage.Neurol Sci.2004;25:s10–s11.
- ,,,.Endoscopy‐guided removal of spontaneous intracerebral hemorrhage: comparison with computer tomography‐guided stereotactic evacuation.Childs Nerv Syst.2007;23(6):677–683.
- ,.Endovascular reperfusion therapy in acute ischaemic stroke.Acta Neurol Scand Suppl.2007;187:22–29.
- .Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I.AJNR Am J Neuroradiol.2006;27(6):1177–1182.
- ,.Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation.Ann Thorac Surg.1996;61(2):755–759.
- ,,, et al.Percutaneous devices for stroke prevention.Cardiovasc Revasc Med.2007;8(3):216–225.
- ,,.Sealing the left atrial appendage: ready for prime time?Am J Med Sci.2007;333(5):285–289.
- ,,, et al.Initial worldwide experience with the WATCHMAN left atrial appendage system for stroke prevention in atrial fibrillation.J Am Coll Cardiol.2007;49(13):1490–1495.
- ,.Left atrial appendage exclusion for stroke prevention in patients with nonrheumatic atrial fibrillation.Stroke.2007;38(2 suppl):624–630.
- FDA News. FDA clears genetic lab test for warfarin sensitivity. Available at: http://www.fda.gov/bbs/topics/news/2007/new01701.html. Accessed January2008.
- .Pharmacogenomics and warfarin therapy.Issues Emerg Health Technol.2007;(104):1–8.
- ,,.Advancing stroke therapeutics through genetic understanding.Curr Drug Targets.2007;8(7):850–859.
- ,.The Atlas of Heart Disease and Stroke.Geneva, Switzerland:World Health Organization;2004.
- National Institute of Neurological Disorders and Stroke. NIH Stroke Scale. Available at: http://www.ninds.nih.gov/doctors/NIH_stroke_scale_booklet.pdf. Accessed January2008.
- Royal College of Physicians.National Clinical Guidelines for Stroke.2nd ed.Prepared by the Intercollegiate Stroke Working Party.London:RCP,2004.
- The European Atrial Fibrillation Trial Study Group.Optimal oral anticoagulant therapy in patients with nonrheumatic atrial fibrillation and recent cerebral ischemia.N Engl J Med.1995;333:5–10.
- ,,, et al.Advanced age, anticoagulation intensity, and risk for intracranial hemorrhage among patients taking warfarin for atrial fibrillation.Ann Intern Med.2004;141(10):745–752.
- ,.Antithrombotic treatment in atrial fibrillation.Heart.2007;93(1):39–44.
- ,,, et al.Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin.Circulation.2004;110(16):2287–2292.
- ,,.Atrial fibrillation.Med J Aust.2007;186(4):197–202.
- ,,, et al.Guidelines for the early management of adults with ischemic stroke. A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups.Stroke.2007;38(5):1655–1711.
- ,,, et al.MRI of acute post‐ischemic cerebral hemorrhage in stroke patients: diagnosis with T2*‐weighted gradient‐echo sequences.Neuroradiology.2001;43(10):809–815.
- ,,, et al.Emergency imaging of cerebrovascular accidents.J Neuroradiol.2004;31(4):327–333.
- ,,, et al.Guidelines for the management of spontaneous intracerebral hemorrhage in adults. 2007 update. A guideline from the American Heart Association, American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group.Stroke.2007;38(6):2001–2023.
- ,,,,,.Systematic comparison of perfusion‐CT and CT‐angiography in acute stroke patients.Ann Neurol.2007;61(6):533–543.
- ,,,,.Antithrombotic and thrombolytic therapy for ischemic stroke: the seventh ACCP conference on antithrombotic and thrombolytic therapy.Chest.2004;126(3 suppl):S483–S512.
- .Acute ischemic stroke treatment in 2007.Circulation.2007;116(13):1504–1514.
- ,,,,.Efficacy of IV tissue plasminogen activator in acute stroke: does stroke subtype really matter?Neurology.2003;61(1):71–75.
- ,,,,,.Efficacy of intraarterial thrombolysis of basilar artery stroke.J Stroke Cerebrovasc Dis.1999;8(1):22–27.
- ,,, et al.Treatment of acute ischemic brain infarction with the assistance of local intraarterial thrombolysis with recombinant tissue‐type plasminogen activator.Acta Radiol.2007;48(7):774–780.
- ,,,,.Intra‐arterial thrombolysis using rt‐PA in patients with acute stroke due to vessel occlusion of anterior and/or posterior cerebral circulation.Neuroradiology.2008;50(1):75–83.
- .Tissue plasminogen activator for acute ischemic stroke in clinical practice: a meta‐analysis of safety data.Stroke.2003;34:2847–2850.
- ,.Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator.Neurology.2002;59:862–867.
- ,,, et al.Site of arterial occlusion identified by transcranial Doppler predicts the response to intravenous thrombolysis for stroke.Stroke.2007;38(3):948–954.
- ,,,.Thrombolysis for acute ischemic stroke.Cochrane Database Syst Rev.2003;(3):CD000213.
- ,,, et al.Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt‐PA stroke trials.Lancet.2004;363:768–774.
- ,,,,,.Trends in medical care of hospitalized stroke patients between 1980 and 1990: the Minnesota stroke survey.J Stroke Cerebrovasc Dis.1998;7(1):76–84.
- ,,,.Low molecular‐weight heparin versus aspirin in patients with acute ischaemic stroke and atrial fibrillation: a double‐blind randomized study. HAEST Study Group. Heparin in Acute Embolic Stroke Trial.Lancet.2000;355(9211):1205–1210.
- International Stroke Trial Collaborative Group.The International Stroke Trial (IST): a randomized trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischemic stroke.Lancet.1997;349(9065):1569–1581.
- .Emergent use of anticoagulation for treatment of patients with ischemic stroke.Stroke.2002;33:856–861.
- ,,,.Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke: a meta‐analysis of randomized controlled trials.Stroke.2007;38(2):423–430.
- .The results of CAPRIE, IST and CAST. International Stroke Trial. Chinese Acute Stroke Trial.Thromb Res1998;92(1 suppl 1):S13–S16.
- ,,,,.Platelet activation and lipid peroxidation in patients with acute ischemic stroke.Stroke.1997;28:1557–1563.
- ,,, et al.Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation elaine.N Engl J Med.2003;349:1019–1026.
- ,,,.Hospitalized patients with atrial fibrillation and a high risk of stroke are not being provided with adequate anticoagulation.J Am Coll Cardiol.2005;46(9):1729–1736.
- ,.Preventing stroke in patients with atrial fibrillation.JAMA.1999;281(19):1830–1835.
- ,.Atrial fibrillation, stroke, and acute antithrombotic therapy: analysis of randomized clinical trials.Stroke.2002;33(11):2722–2727.
- ,,, et al.Recombinant factor VIIa for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage.Mayo Clin Proc.2004;79(12):1495–1500.
- ,,,.Managing the therapeutic dilemma: patients with spontaneous intracerebral hemorrhage and urgent need for anticoagulation.J Neurol.2000;247(3):209–214.
- ,,, et al.Early hemorrhage growth in patients with intracerebral hemorrhage.Stroke.1997;28:1–5.
- ,,.Bleeding complications in oral anticoagulant therapy: an analysis of risk factors.Arch Intern Med.1993;153:1557–1562.
- ,,,.Warfarin‐associated hemorrhage and cerebral amyloid angiopathy: a genetic and pathologic study.Neurology.2000;55(7):947–951.
- ,,, et al.Treatment of warfarin‐associated intracerebral hemorrhage: literature review and expert opinion.Mayo Clinic Proc.2007;82(1):82–92.
- ,,,,.Urgent reversal of warfarin with prothrombin complex concentrate.J Thromb Haemost.2006;4(5):967–970.
- ,.The headache over warfarin in British neurosurgical intensive care units: a national survey of current practice.Intensive Care Med.2007;33(11):1946–1953.
- ,,, et al.Timing of fresh frozen plasma administration and rapid correction of coagulopathy in warfarin‐related intracerebral hemorrhage.Stroke.2006;37(1):151–155.
- ,,,.Progression of warfarin‐associated intracerebral hemorrhage after INR normalization with FFP.Neurology.2006;67(7):1272–1274.
- ,,, et al.Successful emergency reversal of phenprocoumon anticoagulation with prothrombin complex concentrate: a prospective clinical study.Blood Coagul Fibrinolysis.2007;18(6):565–570.
- ,,, et al.Guidelines for the use of fresh‐frozen plasma, cryoprecipitate and cryosupernatant.Br J Hematol.2004;126(1):11–28.
- ,,,,,.The pharmacology and management of vitamin K antagonists. The seventh ACCP conference on antithrombotic and thrombolytic therapy.Chest.2004;126:204s–33s.
- ,,, et al.Hematoma growth and outcome in treated neurocritical care patients with intracerebral hemorrhage related to oral anticoagulant therapy. Comparison of acute treatment strategies using vitamin K, fresh frozen plasma, and prothrombin complex concentrates.Stroke.2006;37:1465.
- ,.Recombinant factor VIIa.BioDrugs.1999;12(1):71–77.
- ,,, et al.Impact of recombinant activated factor VII on health‐related quality of life after intracerebral hemorrhage.Cerebrovasc Dis.2007;24(2–3):219–225.
- ,,, et al.Recombinant activated factor VII for acute intracerebral hemorrhage: US phase IIA trial.Neurocrit Care.2006;4(3):206–214.
- ,,, et al.Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial.Lancet.2005;365(9457):387–397.
- ,,,,,.Advances in the care of patients with intracerebral hemorrhage.Mayo Clin Proc.2007;82(8):987–990.
- ,,,.Surgery for intracerebral hemorrhage.Neurol Sci.2004;25:s10–s11.
- ,,,.Endoscopy‐guided removal of spontaneous intracerebral hemorrhage: comparison with computer tomography‐guided stereotactic evacuation.Childs Nerv Syst.2007;23(6):677–683.
- ,.Endovascular reperfusion therapy in acute ischaemic stroke.Acta Neurol Scand Suppl.2007;187:22–29.
- .Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I.AJNR Am J Neuroradiol.2006;27(6):1177–1182.
- ,.Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation.Ann Thorac Surg.1996;61(2):755–759.
- ,,, et al.Percutaneous devices for stroke prevention.Cardiovasc Revasc Med.2007;8(3):216–225.
- ,,.Sealing the left atrial appendage: ready for prime time?Am J Med Sci.2007;333(5):285–289.
- ,,, et al.Initial worldwide experience with the WATCHMAN left atrial appendage system for stroke prevention in atrial fibrillation.J Am Coll Cardiol.2007;49(13):1490–1495.
- ,.Left atrial appendage exclusion for stroke prevention in patients with nonrheumatic atrial fibrillation.Stroke.2007;38(2 suppl):624–630.
- FDA News. FDA clears genetic lab test for warfarin sensitivity. Available at: http://www.fda.gov/bbs/topics/news/2007/new01701.html. Accessed January2008.
- .Pharmacogenomics and warfarin therapy.Issues Emerg Health Technol.2007;(104):1–8.
- ,,.Advancing stroke therapeutics through genetic understanding.Curr Drug Targets.2007;8(7):850–859.