User login
Electrical Alternans and Pulsus Paradoxus
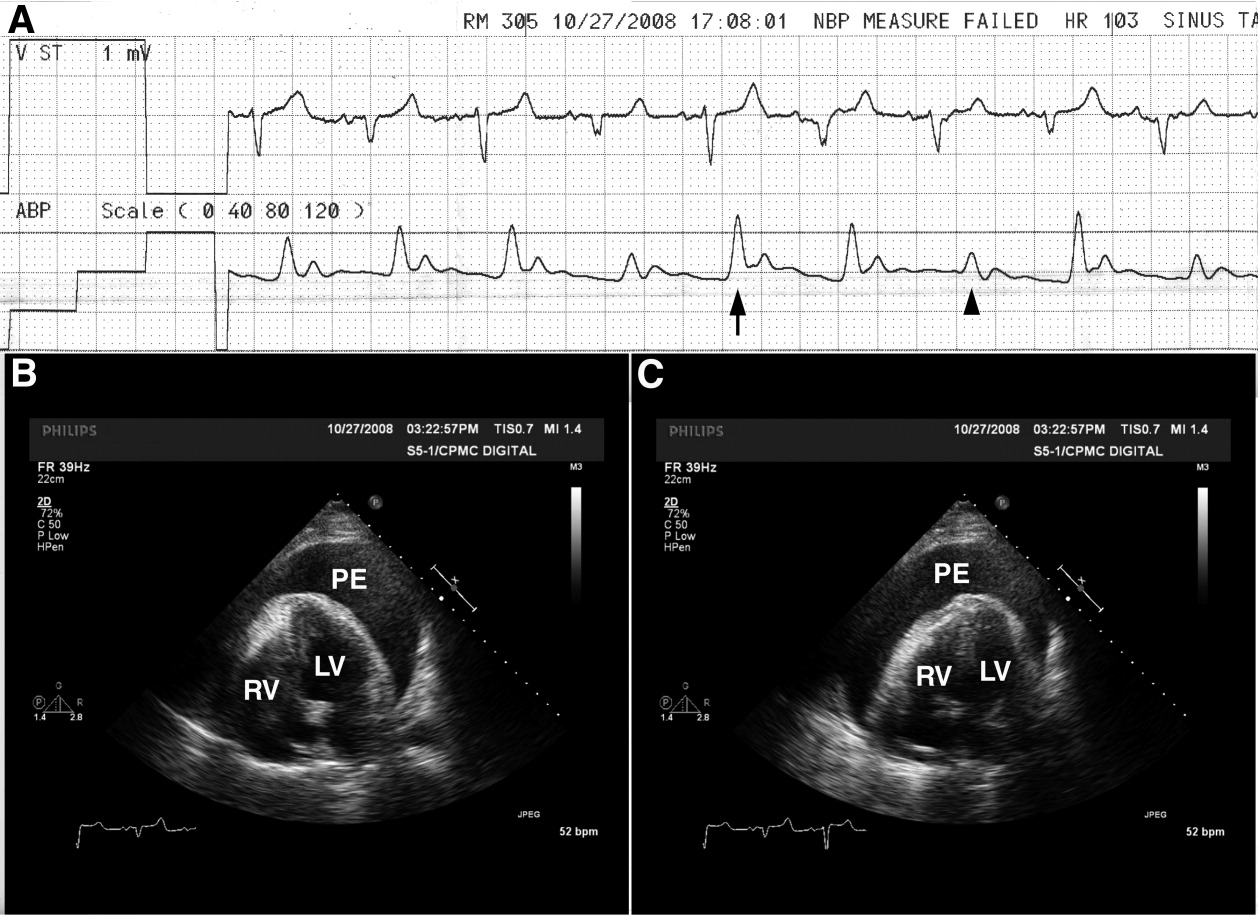
A 65‐year‐old man with chronic obstructive pulmonary disease and right lung nodule presented with dyspnea. Physical examination revealed a pulse of 130 beats per minute, respiratory rate of 28 times per minute, blood pressure of 100/60 mm Hg, estimated jugular venous pressure of greater than 15 cm above the right atrium at a 45‐degree semirecumbent position, and distant heart sounds. He subsequently developed hypotension and an arterial line was placed. A single‐channel electrocardiogram (Figure 1A; upper tracing) demonstrated electrical alternans. Simultaneous arterial line (Figure 1A; lower tracing) showed decreased systolic blood pressure from 136 mm Hg (Figure 1A; arrow) to 96 mm Hg (Figure 1A; arrowhead) with inspiration, consistent with exaggerated pulsus paradoxus. A transthoracic echocardiogram confirmed a large pericardial effusion with the heart oscillating from side (Figure 1B) to side (Figure 1C) within the pericardial sac. Pericardiocentesis was performed and 1100 mL of bloody pericardial fluid was removed with prompt resolution of hypotension, tachycardia, electrical alternans, and abnormal pulsus paradoxus. Pericardial effusion (PE), right ventricle (RV), and left ventricle (LV) are depicted in Figure 1B, C.
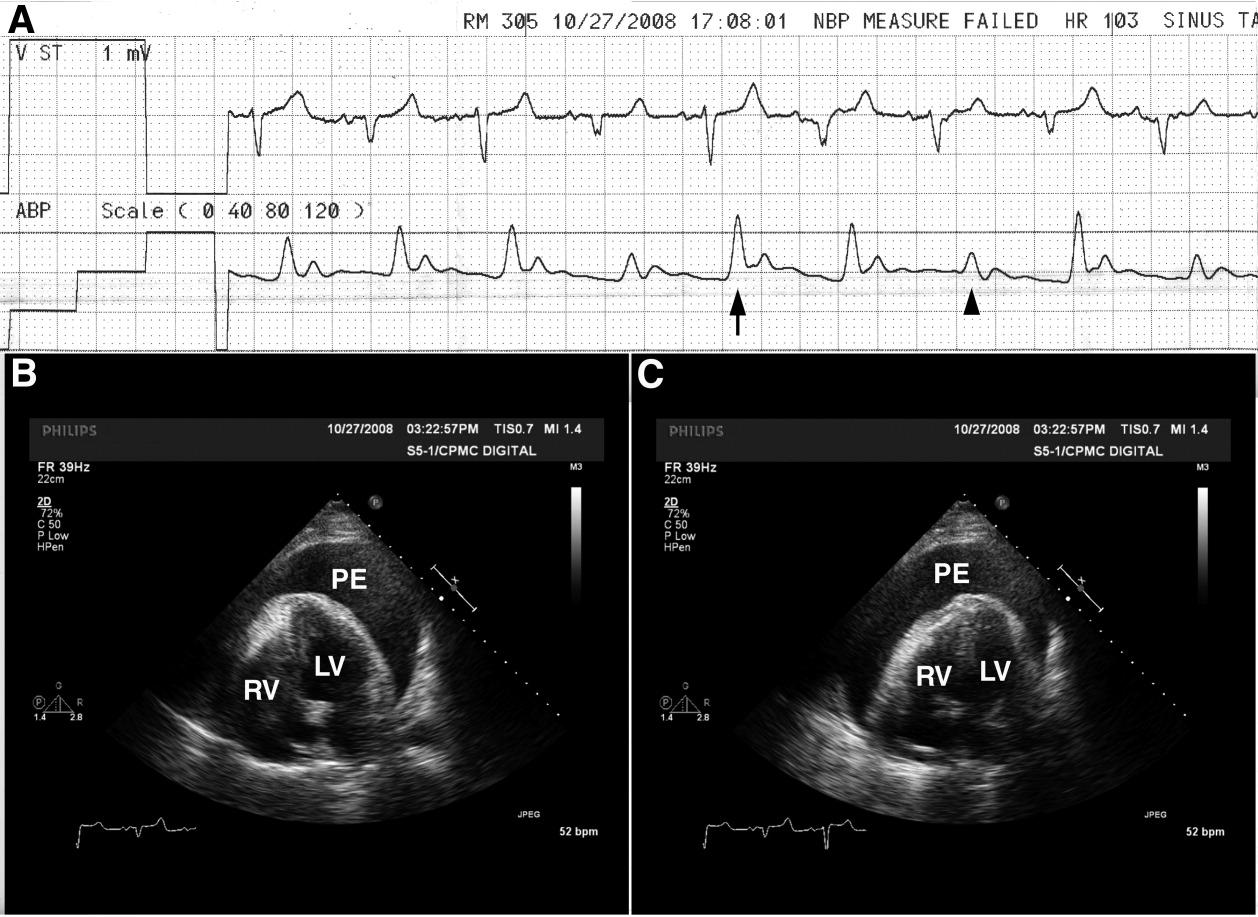
The etiology of this patient's pericardial effusion was felt to be due to metastatic pericardial disease from lung cancer. The mechanism of electrical alternans is felt to be due to motion as the heart oscillates back and forth within the pericardial sac.1 The exaggerated pulsus paradoxus reflects decreased LV filling during inspiration as RV filling increases and compresses the LV, referred to as ventricular interdependence.
- ,,.Quantitative echocardiographic assessment in pericardial disease.Echocardiography.1997;14:207–214.
A 65‐year‐old man with chronic obstructive pulmonary disease and right lung nodule presented with dyspnea. Physical examination revealed a pulse of 130 beats per minute, respiratory rate of 28 times per minute, blood pressure of 100/60 mm Hg, estimated jugular venous pressure of greater than 15 cm above the right atrium at a 45‐degree semirecumbent position, and distant heart sounds. He subsequently developed hypotension and an arterial line was placed. A single‐channel electrocardiogram (Figure 1A; upper tracing) demonstrated electrical alternans. Simultaneous arterial line (Figure 1A; lower tracing) showed decreased systolic blood pressure from 136 mm Hg (Figure 1A; arrow) to 96 mm Hg (Figure 1A; arrowhead) with inspiration, consistent with exaggerated pulsus paradoxus. A transthoracic echocardiogram confirmed a large pericardial effusion with the heart oscillating from side (Figure 1B) to side (Figure 1C) within the pericardial sac. Pericardiocentesis was performed and 1100 mL of bloody pericardial fluid was removed with prompt resolution of hypotension, tachycardia, electrical alternans, and abnormal pulsus paradoxus. Pericardial effusion (PE), right ventricle (RV), and left ventricle (LV) are depicted in Figure 1B, C.
The etiology of this patient's pericardial effusion was felt to be due to metastatic pericardial disease from lung cancer. The mechanism of electrical alternans is felt to be due to motion as the heart oscillates back and forth within the pericardial sac.1 The exaggerated pulsus paradoxus reflects decreased LV filling during inspiration as RV filling increases and compresses the LV, referred to as ventricular interdependence.
A 65‐year‐old man with chronic obstructive pulmonary disease and right lung nodule presented with dyspnea. Physical examination revealed a pulse of 130 beats per minute, respiratory rate of 28 times per minute, blood pressure of 100/60 mm Hg, estimated jugular venous pressure of greater than 15 cm above the right atrium at a 45‐degree semirecumbent position, and distant heart sounds. He subsequently developed hypotension and an arterial line was placed. A single‐channel electrocardiogram (Figure 1A; upper tracing) demonstrated electrical alternans. Simultaneous arterial line (Figure 1A; lower tracing) showed decreased systolic blood pressure from 136 mm Hg (Figure 1A; arrow) to 96 mm Hg (Figure 1A; arrowhead) with inspiration, consistent with exaggerated pulsus paradoxus. A transthoracic echocardiogram confirmed a large pericardial effusion with the heart oscillating from side (Figure 1B) to side (Figure 1C) within the pericardial sac. Pericardiocentesis was performed and 1100 mL of bloody pericardial fluid was removed with prompt resolution of hypotension, tachycardia, electrical alternans, and abnormal pulsus paradoxus. Pericardial effusion (PE), right ventricle (RV), and left ventricle (LV) are depicted in Figure 1B, C.
The etiology of this patient's pericardial effusion was felt to be due to metastatic pericardial disease from lung cancer. The mechanism of electrical alternans is felt to be due to motion as the heart oscillates back and forth within the pericardial sac.1 The exaggerated pulsus paradoxus reflects decreased LV filling during inspiration as RV filling increases and compresses the LV, referred to as ventricular interdependence.
- ,,.Quantitative echocardiographic assessment in pericardial disease.Echocardiography.1997;14:207–214.
- ,,.Quantitative echocardiographic assessment in pericardial disease.Echocardiography.1997;14:207–214.