User login
Clinical biofeedback therapy is one of the many new approaches in health care aimed at helping individuals take responsibility for their well-being, including responsibility for the cognitive, emotional, and behavioral changes needed to effect healthy physiologic change. This article provides a brief survey of biofeedback therapy by defining what biofeedback involves, reviewing the various modalities that it can serve to monitor, discussing major models of biofeedback therapy, and outlining criteria for evaluating the efficacy of biofeedback interventions.
BIOFEEDBACK: BOTH PROCESS AND INSTRUMENTATION
Biofeedback refers to both a process and the instrumentation used in that process.
The process is one of learning to use physiologic information that is monitored and “fed back” through biofeedback instruments. The term dates from 1969, when it was coined to describe laboratory procedures that had been developed in the 1940s in which research subjects learned to modify heart rate, blood flow, and other physiologic functions that were not normally thought of as being subject to conscious control. Feedback itself has been present through much of human history, particularly through the use of mirrored surfaces to practice the expression of emotion.1
Biofeedback instruments monitor one or more physiologic processes, measure what is monitored and transform that measurement into auditory and/or visual signals, and present what is monitored and measured in a simple, direct, and immediate way. Biofeedback equipment typically is noninvasive. The instruments provide continuous monitoring and transformation of physiologic data into understandable feedback for the patient being monitored. Current computerized instruments can provide simultaneous displays and recording of multiple channels of physiologic information. The goal is to enable the individual being monitored to change some physiologic process, guided by the information provided by the biofeedback equipment. How many training sessions are necessary varies with the individual and the disorder, ranging from a few to 50 or more. Our experience is that the great majority of patients obtain benefit in 8 to 12 sessions.
MULTIPLE MODALITIES FOR MONITORING
Multiple modalities can be monitored via biofeedback. Surface electromyography is perhaps the most commonly used instrumentation. Other commonly used measures in a psychophysiologic/biofeedback assessment are respiration rate and depth, skin surface temperature (particularly at the fingertips), cardiovascular reactivity (particularly heart rate and blood pressure), and electrodermal response.2
Feedback of real-time physiologic data is limited only by one’s creativity and technological capabilities. Most of the early noncomputerized equipment provided feedback through the onset and offset of sounds, the changing of tones and volume, the turning on and off of lights, and digital numeric displays indicating both the direction of change and absolute values (such as digital peripheral temperature). Current computerized equipment uses such feedback features as computer games, which the patient “wins” by reaching a goal (such as a systolic blood pressure level below 130 mm Hg), mandalas that can be filled in with colors of the patient’s choosing as he or she progresses in the desired direction, and complex computer-generated figures and graphs.
Electroencephalographic biofeedback (neurofeedback) has become a separate area of study and application, with particular use in the treatment of attention deficit disorder. A baseline electroencephalogram is used in neurofeedback assessment to identify abnormal patterns, and follow-up training is provided to teach the patient to change these patterns in a healthy direction.3
More recently, heart rate variability has come into use as a measure of adaptability or autonomic balance. Soviet scientists were the first to study heart rate variability biofeedback, working with cosmonauts in measuring autonomic function. They found that the low-frequency (0.1-Hz) bands produced the highest frequency-specific oscillations in heart rate variability, and training typically proceeds in increasing amplitude of the low-frequency band (also called the baroreceptor band). Because diminished heart rate variability is a predictor of increased risk for cardiac mortality, teaching patients to increase heart rate variability made sense. The training involves instruction in breathing at an identified resonant frequency that is related to optimal low-frequency band power.4
LEARNING AND MODELS OF BIOFEEDBACK
Accurate feedback facilitates the learning of any skill, whether it be sinking a golf putt, solving an algebra problem, or controlling physiologic behavior. A man playing darts blindfolded is unlikely to achieve as good a score as he would with the blindfold off, because feedback makes a difference.5
Four conditions are important for effective learning;5 the learner must:
- Have the capacity to respond
- Be motivated to learn
- Be positively reinforced for learning
- Be given accurate information about the results of the learning effort.
Direct feedback learning model
The direct feedback learning model assumes that adding feedback to the other important conditions of learning will result in a patient gaining control of the relevant physiology being targeted. This model has been used in treating many disorders, including Raynaud phenomenon and urinary and fecal incontinence.
Biofeedback training in this model may involve a coach/instructor/therapist only to the extent of explaining the equipment and its use. In other words, the coach “teaches the patient how to use the mirror.” More commonly.particularly for training in lowered arousal for patients in whom stress reactivity is a significant factor in the development and maintenance of excessive (sympathetic nervous system) arousal that leads to symptoms.a skilled therapist is present. The therapist not only teaches the patient how to use information from biofeedback instruments but also guides the patient in identifying and changing cognitive, emotional, and behavioral patterns that contribute to excessive reactivity. The relationship of physiologic reactivity to the subject matter under discussion also helps diagnostically in identifying stressful areas of life, particularly in psychophysiologic responders who are repressive and denying and who are not good at identifying the stressors in their lives. The equipment becomes a mirror that lets the patient see a problem that he or she had not identified as such.5
Therapeutic/stress-management/biofeedback model
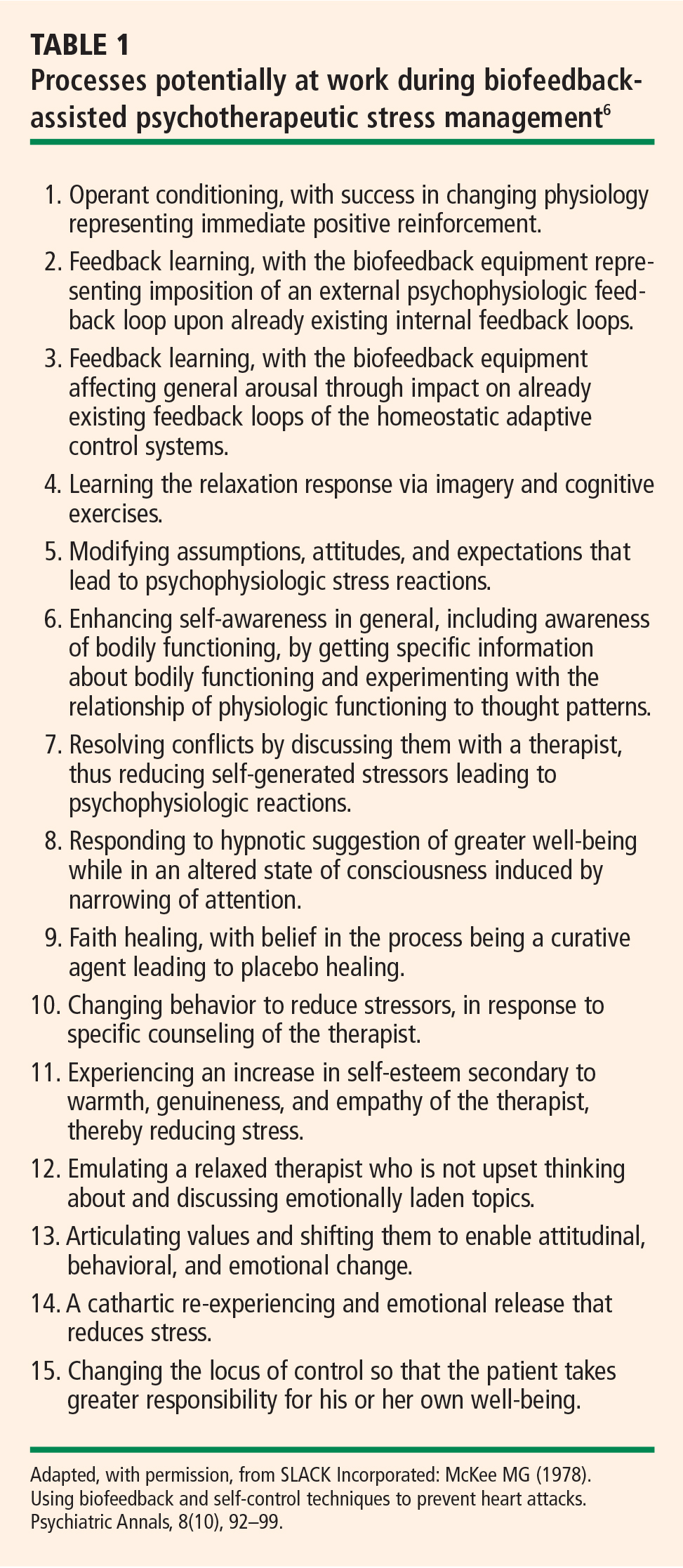
When treating patients with disordered physiology (including autonomic imbalance) in the therapeutic/stress-management/biofeedback model, it is essential to understand each patient as an individual. In this model, stress management and psychotherapeutic interventions address particular vulnerabilities that lead to excessive arousal. This approach starts with a psychophysiologic assessment in which resting levels of relevant physiologic dimensions are measured; this is followed by imposition of stressors to measure reactivity and then by a recovery period in which rate and extent of recovery are measured. An interview and psychological test help determine which cognitive, emotional and behavioral patterns contribute to vulnerability. Patients typically respond well to this approach. It is common for patients to use such descriptions as, “I break out in a cold sweat when I’m stressed,” or “I feel heartsick when I’m stressed,” which suggests that the notion of mind-body interaction resonates with patients.6
CRITERIA FOR EVALUATING EFFICACY OF BIOFEEDBACK INTERVENTIONS
Several years ago a task force of the Association for Applied Psychophysiology and Biofeedback and the Society for Neuronal Regulation published criteria for evaluating the clinical efficacy of biofeedback/psychophysiologic interventions.7 These criteria are detailed below.3,7
Level 1: Not empirically supported
This designation applies to interventions supported only by anecdotal reports and/or case studies in non–peer-reviewed venues (ie, not empirically supported).
Level 2: Possibly efficacious
This applies to interventions supported by at least one study of sufficient statistical power with well-identified outcome measures but which lacked randomized assignment to a control condition internal to the study.
Level 3: Probably efficacious
This applies to interventions supported by multiple observational studies, clinical studies, wait-list–controlled studies, and within-subject and intrasubject replication studies that demonstrate efficacy.
Level 4: Efficacious
a. In a comparison with a no-treatment control group, alternative treatment group, or sham (placebo) control using randomized assignment, the intervention is shown to be statistically significantly superior to the control condition, or the intervention is equivalent to a treatment of established efficacy in a study with sufficient power to detect moderate differences, and
b. The studies have been conducted with a population treated for a specific problem, for whom inclusion criteria are delineated in a reliable, operationally defined manner, and
c. The study used valid and clearly specified outcome measures related to the problem being treated, and
d. The data were subjected to appropriate data analysis, and
e. The diagnostic and treatment variables and procedures were clearly defined in a manner that permits replication of the study by independent researchers, and
f. The superiority or equivalence of the intervention has been shown in at least two independent research settings.
Level 5: Efficacious and specific
This designation applies when the intervention has been shown to be superior to credible sham therapy, pill therapy, or alternative bona fide treatment in at least two independent research settings.
Efficacy ratings for specific disorders
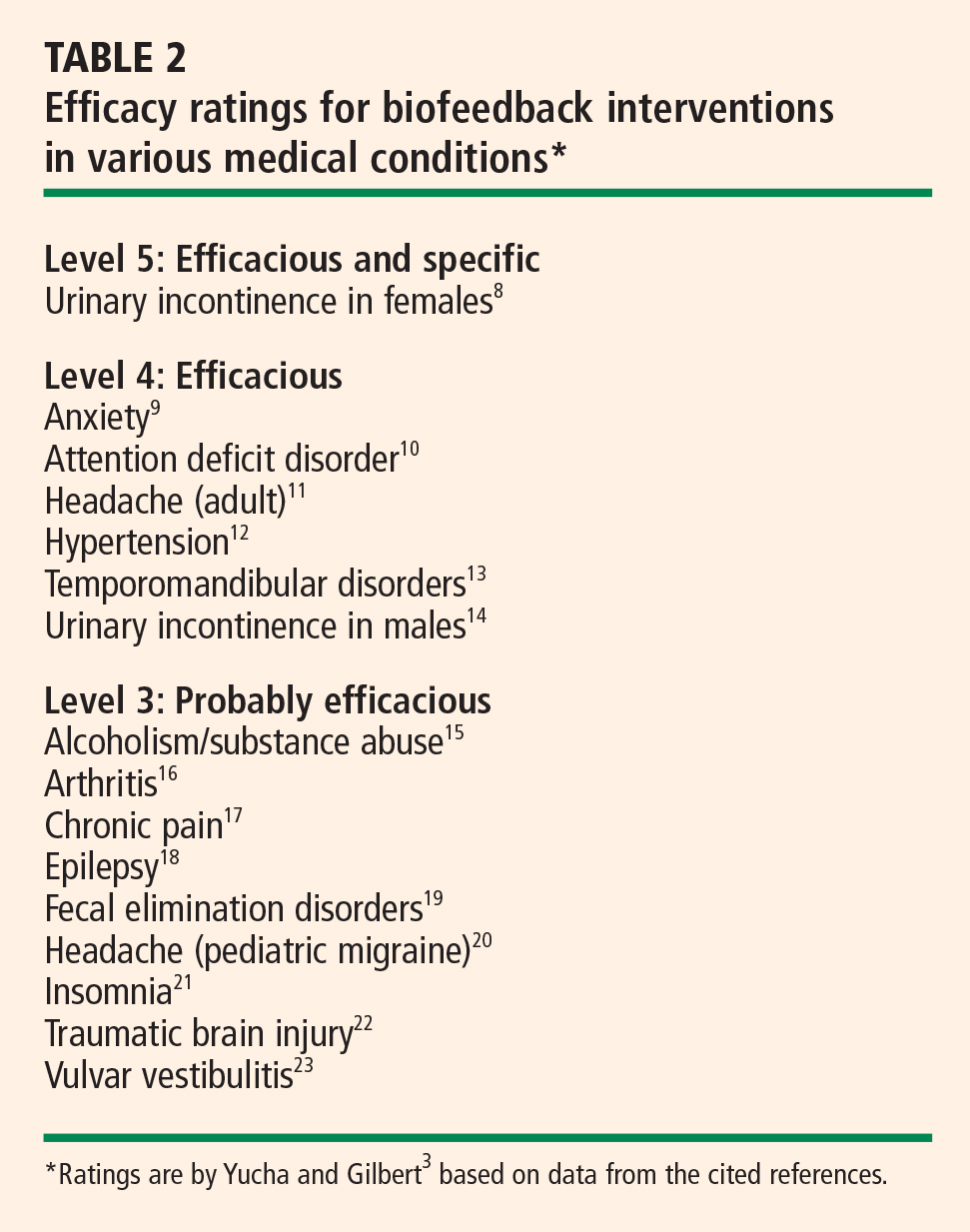
Despite high standards, biofeedback thrives
The above criteria represent high standards. Since biofeedback training is often more like physical therapy or learning a language, double-blind protocols usually are not feasible, nor is sham training. Moreover, the effectiveness of training is perhaps even more difficult to assess in daily practice, with the inevitable multiplicity of confounding variables. Nevertheless, biofeedback training for many disorders is standing the test of both time and outcomes research, and it is increasingly embraced by the public and recognized by health care insurers and professionals alike.
- Gaarder KR, Montgomery PS. Clinical biofeedback: a procedural manual. Baltimore, MD: Williams and Wilkins; 1977.
- Schwartz MS, Andrasik F. Biofeedback: a practitioner’s guide. 3rd ed. New York, NY: Guilford Press; 2003.
- Yucha C, Gilbert C. Evidence-based practice in biofeedback and neurofeedback. Wheat Ridge, CO: Association for Applied Psychophysiology and Biofeedback; 2004.
- Lehrer PM, Vaschillo E, Lu SE, et al. Heart rate variability biofeedback: effects of age on heart rate variability, baroreflex gain, and asthma. Chest 2006; 129:278–284.
- McKee MG. Contributions of psychophysiologic monitoring to diagnosis and treatment of chronic head pain: a case study. Headache Q 1991; II(4):327–330.
- McKee MG. Using biofeedback and self-control techniques to prevent heart attacks. Psychiatr Ann 1978; 8:10.
- Moss D, Gunkelman J. Task Force Report on methodology and empirically supported treatments: introduction. Appl Psychophysiol Biofeedback 2002; 27:271–272.
- Weatherall M. Biofeedback or pelvic floor muscle exercises for female genuine stress incontinence: a meta-analysis of trials identified in a systematic review. BJU Int 1999; 83:1015–1016.
- Wenck LS, Leu PW, D’Amato RC. Evaluating the efficacy of a biofeedback intervention to reduce children’s anxiety. J Clin Psychol 1996; 52:469–473.
- Kaiser DA, Othmer S. Effect of neurofeedback on variables of attention in a large multi-center trial. J Neurother 2000; 4:5–15.
- Silberstein SD, for the US Headache Consortium. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55:754–762.
- Yucha CB, Clark L, Smith M, Uris P, Lafleur B, Duval S. The effect of biofeedback in hypertension. Appl Nurs Res 2001; 14:29–35.
- Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain 1999; 13:29–37.
- Van Kampen M, De Weerdt W, Van Poppel H, De Ridder D, Feys H, Baert L. Effect of pelvic-floor re-education on duration and degree of incontinence after radical prostatectomy: a randomised controlled trial. Lancet 2000; 355:98–102.
- Saxby E, Peniston EG. Alpha-theta brainwave neurofeedback training: an effective treatment for male and female alcoholics with depressive symptoms. J Clin Psychol 1995; 51:685–693.
- Lavigne JV, Ross CK, Berry SL, Hayford JR, Pachman LM. Evaluation of a psychological treatment package for treating pain in juvenile rheumatoid arthritis. Arthritis Care Res 1992; 5:101–110.
- Humphreys PA, Gevirtz RN. Treatment of recurrent abdominal pain: components analysis of four treatment protocols. J Pediatr Gastroenterol Nutr 2000; 31:47–51.
- Kotchoubey B, Strehl U, Uhlmann C, et al. Modification of slow cortical potentials in patients with refractory epilepsy: a controlled outcome study. Epilepsia 2001; 42:406–416.
- Chiarioni G, Bassotti G, Stanganini S, Vantini I, Whitehead WE. Sensory retraining is key to biofeedback therapy for formed stool fecal incontinence. Am J Gastroenterol 2002; 97:109–117.
- Labbé EE. Treatment of childhood migraine with autogenic training and skin temperature biofeedback: a component analysis. Headache 1995; 35:10–13.
- Morin CM, Hauri PJ, Espie CA, Spielman AJ, Buysse DJ, Bootzin RR. Nonpharmacologic treatment of chronic insomnia. An American Academy of Sleep Medicine review. Sleep 1999; 22:1134–1156.
- Thornton K. Improvement/rehabilitation of memory functioning with neurotherapy/QEEG biofeedback. J Head Trauma Rehabil 2000; 15:1285–1296.
- Bergeron S, Binik YM, Khalifé S, et al. A randomized comparison of group cognitive–behavioral therapy, surface electromyographic biofeedback, and vestibulectomy in the treatment of dyspareunia resulting from vulvar vestibulitis. Pain 2001; 91:297–306.
Clinical biofeedback therapy is one of the many new approaches in health care aimed at helping individuals take responsibility for their well-being, including responsibility for the cognitive, emotional, and behavioral changes needed to effect healthy physiologic change. This article provides a brief survey of biofeedback therapy by defining what biofeedback involves, reviewing the various modalities that it can serve to monitor, discussing major models of biofeedback therapy, and outlining criteria for evaluating the efficacy of biofeedback interventions.
BIOFEEDBACK: BOTH PROCESS AND INSTRUMENTATION
Biofeedback refers to both a process and the instrumentation used in that process.
The process is one of learning to use physiologic information that is monitored and “fed back” through biofeedback instruments. The term dates from 1969, when it was coined to describe laboratory procedures that had been developed in the 1940s in which research subjects learned to modify heart rate, blood flow, and other physiologic functions that were not normally thought of as being subject to conscious control. Feedback itself has been present through much of human history, particularly through the use of mirrored surfaces to practice the expression of emotion.1
Biofeedback instruments monitor one or more physiologic processes, measure what is monitored and transform that measurement into auditory and/or visual signals, and present what is monitored and measured in a simple, direct, and immediate way. Biofeedback equipment typically is noninvasive. The instruments provide continuous monitoring and transformation of physiologic data into understandable feedback for the patient being monitored. Current computerized instruments can provide simultaneous displays and recording of multiple channels of physiologic information. The goal is to enable the individual being monitored to change some physiologic process, guided by the information provided by the biofeedback equipment. How many training sessions are necessary varies with the individual and the disorder, ranging from a few to 50 or more. Our experience is that the great majority of patients obtain benefit in 8 to 12 sessions.
MULTIPLE MODALITIES FOR MONITORING
Multiple modalities can be monitored via biofeedback. Surface electromyography is perhaps the most commonly used instrumentation. Other commonly used measures in a psychophysiologic/biofeedback assessment are respiration rate and depth, skin surface temperature (particularly at the fingertips), cardiovascular reactivity (particularly heart rate and blood pressure), and electrodermal response.2
Feedback of real-time physiologic data is limited only by one’s creativity and technological capabilities. Most of the early noncomputerized equipment provided feedback through the onset and offset of sounds, the changing of tones and volume, the turning on and off of lights, and digital numeric displays indicating both the direction of change and absolute values (such as digital peripheral temperature). Current computerized equipment uses such feedback features as computer games, which the patient “wins” by reaching a goal (such as a systolic blood pressure level below 130 mm Hg), mandalas that can be filled in with colors of the patient’s choosing as he or she progresses in the desired direction, and complex computer-generated figures and graphs.
Electroencephalographic biofeedback (neurofeedback) has become a separate area of study and application, with particular use in the treatment of attention deficit disorder. A baseline electroencephalogram is used in neurofeedback assessment to identify abnormal patterns, and follow-up training is provided to teach the patient to change these patterns in a healthy direction.3
More recently, heart rate variability has come into use as a measure of adaptability or autonomic balance. Soviet scientists were the first to study heart rate variability biofeedback, working with cosmonauts in measuring autonomic function. They found that the low-frequency (0.1-Hz) bands produced the highest frequency-specific oscillations in heart rate variability, and training typically proceeds in increasing amplitude of the low-frequency band (also called the baroreceptor band). Because diminished heart rate variability is a predictor of increased risk for cardiac mortality, teaching patients to increase heart rate variability made sense. The training involves instruction in breathing at an identified resonant frequency that is related to optimal low-frequency band power.4
LEARNING AND MODELS OF BIOFEEDBACK
Accurate feedback facilitates the learning of any skill, whether it be sinking a golf putt, solving an algebra problem, or controlling physiologic behavior. A man playing darts blindfolded is unlikely to achieve as good a score as he would with the blindfold off, because feedback makes a difference.5
Four conditions are important for effective learning;5 the learner must:
- Have the capacity to respond
- Be motivated to learn
- Be positively reinforced for learning
- Be given accurate information about the results of the learning effort.
Direct feedback learning model
The direct feedback learning model assumes that adding feedback to the other important conditions of learning will result in a patient gaining control of the relevant physiology being targeted. This model has been used in treating many disorders, including Raynaud phenomenon and urinary and fecal incontinence.
Biofeedback training in this model may involve a coach/instructor/therapist only to the extent of explaining the equipment and its use. In other words, the coach “teaches the patient how to use the mirror.” More commonly.particularly for training in lowered arousal for patients in whom stress reactivity is a significant factor in the development and maintenance of excessive (sympathetic nervous system) arousal that leads to symptoms.a skilled therapist is present. The therapist not only teaches the patient how to use information from biofeedback instruments but also guides the patient in identifying and changing cognitive, emotional, and behavioral patterns that contribute to excessive reactivity. The relationship of physiologic reactivity to the subject matter under discussion also helps diagnostically in identifying stressful areas of life, particularly in psychophysiologic responders who are repressive and denying and who are not good at identifying the stressors in their lives. The equipment becomes a mirror that lets the patient see a problem that he or she had not identified as such.5
Therapeutic/stress-management/biofeedback model
When treating patients with disordered physiology (including autonomic imbalance) in the therapeutic/stress-management/biofeedback model, it is essential to understand each patient as an individual. In this model, stress management and psychotherapeutic interventions address particular vulnerabilities that lead to excessive arousal. This approach starts with a psychophysiologic assessment in which resting levels of relevant physiologic dimensions are measured; this is followed by imposition of stressors to measure reactivity and then by a recovery period in which rate and extent of recovery are measured. An interview and psychological test help determine which cognitive, emotional and behavioral patterns contribute to vulnerability. Patients typically respond well to this approach. It is common for patients to use such descriptions as, “I break out in a cold sweat when I’m stressed,” or “I feel heartsick when I’m stressed,” which suggests that the notion of mind-body interaction resonates with patients.6
CRITERIA FOR EVALUATING EFFICACY OF BIOFEEDBACK INTERVENTIONS
Several years ago a task force of the Association for Applied Psychophysiology and Biofeedback and the Society for Neuronal Regulation published criteria for evaluating the clinical efficacy of biofeedback/psychophysiologic interventions.7 These criteria are detailed below.3,7
Level 1: Not empirically supported
This designation applies to interventions supported only by anecdotal reports and/or case studies in non–peer-reviewed venues (ie, not empirically supported).
Level 2: Possibly efficacious
This applies to interventions supported by at least one study of sufficient statistical power with well-identified outcome measures but which lacked randomized assignment to a control condition internal to the study.
Level 3: Probably efficacious
This applies to interventions supported by multiple observational studies, clinical studies, wait-list–controlled studies, and within-subject and intrasubject replication studies that demonstrate efficacy.
Level 4: Efficacious
a. In a comparison with a no-treatment control group, alternative treatment group, or sham (placebo) control using randomized assignment, the intervention is shown to be statistically significantly superior to the control condition, or the intervention is equivalent to a treatment of established efficacy in a study with sufficient power to detect moderate differences, and
b. The studies have been conducted with a population treated for a specific problem, for whom inclusion criteria are delineated in a reliable, operationally defined manner, and
c. The study used valid and clearly specified outcome measures related to the problem being treated, and
d. The data were subjected to appropriate data analysis, and
e. The diagnostic and treatment variables and procedures were clearly defined in a manner that permits replication of the study by independent researchers, and
f. The superiority or equivalence of the intervention has been shown in at least two independent research settings.
Level 5: Efficacious and specific
This designation applies when the intervention has been shown to be superior to credible sham therapy, pill therapy, or alternative bona fide treatment in at least two independent research settings.
Efficacy ratings for specific disorders
Despite high standards, biofeedback thrives
The above criteria represent high standards. Since biofeedback training is often more like physical therapy or learning a language, double-blind protocols usually are not feasible, nor is sham training. Moreover, the effectiveness of training is perhaps even more difficult to assess in daily practice, with the inevitable multiplicity of confounding variables. Nevertheless, biofeedback training for many disorders is standing the test of both time and outcomes research, and it is increasingly embraced by the public and recognized by health care insurers and professionals alike.
Clinical biofeedback therapy is one of the many new approaches in health care aimed at helping individuals take responsibility for their well-being, including responsibility for the cognitive, emotional, and behavioral changes needed to effect healthy physiologic change. This article provides a brief survey of biofeedback therapy by defining what biofeedback involves, reviewing the various modalities that it can serve to monitor, discussing major models of biofeedback therapy, and outlining criteria for evaluating the efficacy of biofeedback interventions.
BIOFEEDBACK: BOTH PROCESS AND INSTRUMENTATION
Biofeedback refers to both a process and the instrumentation used in that process.
The process is one of learning to use physiologic information that is monitored and “fed back” through biofeedback instruments. The term dates from 1969, when it was coined to describe laboratory procedures that had been developed in the 1940s in which research subjects learned to modify heart rate, blood flow, and other physiologic functions that were not normally thought of as being subject to conscious control. Feedback itself has been present through much of human history, particularly through the use of mirrored surfaces to practice the expression of emotion.1
Biofeedback instruments monitor one or more physiologic processes, measure what is monitored and transform that measurement into auditory and/or visual signals, and present what is monitored and measured in a simple, direct, and immediate way. Biofeedback equipment typically is noninvasive. The instruments provide continuous monitoring and transformation of physiologic data into understandable feedback for the patient being monitored. Current computerized instruments can provide simultaneous displays and recording of multiple channels of physiologic information. The goal is to enable the individual being monitored to change some physiologic process, guided by the information provided by the biofeedback equipment. How many training sessions are necessary varies with the individual and the disorder, ranging from a few to 50 or more. Our experience is that the great majority of patients obtain benefit in 8 to 12 sessions.
MULTIPLE MODALITIES FOR MONITORING
Multiple modalities can be monitored via biofeedback. Surface electromyography is perhaps the most commonly used instrumentation. Other commonly used measures in a psychophysiologic/biofeedback assessment are respiration rate and depth, skin surface temperature (particularly at the fingertips), cardiovascular reactivity (particularly heart rate and blood pressure), and electrodermal response.2
Feedback of real-time physiologic data is limited only by one’s creativity and technological capabilities. Most of the early noncomputerized equipment provided feedback through the onset and offset of sounds, the changing of tones and volume, the turning on and off of lights, and digital numeric displays indicating both the direction of change and absolute values (such as digital peripheral temperature). Current computerized equipment uses such feedback features as computer games, which the patient “wins” by reaching a goal (such as a systolic blood pressure level below 130 mm Hg), mandalas that can be filled in with colors of the patient’s choosing as he or she progresses in the desired direction, and complex computer-generated figures and graphs.
Electroencephalographic biofeedback (neurofeedback) has become a separate area of study and application, with particular use in the treatment of attention deficit disorder. A baseline electroencephalogram is used in neurofeedback assessment to identify abnormal patterns, and follow-up training is provided to teach the patient to change these patterns in a healthy direction.3
More recently, heart rate variability has come into use as a measure of adaptability or autonomic balance. Soviet scientists were the first to study heart rate variability biofeedback, working with cosmonauts in measuring autonomic function. They found that the low-frequency (0.1-Hz) bands produced the highest frequency-specific oscillations in heart rate variability, and training typically proceeds in increasing amplitude of the low-frequency band (also called the baroreceptor band). Because diminished heart rate variability is a predictor of increased risk for cardiac mortality, teaching patients to increase heart rate variability made sense. The training involves instruction in breathing at an identified resonant frequency that is related to optimal low-frequency band power.4
LEARNING AND MODELS OF BIOFEEDBACK
Accurate feedback facilitates the learning of any skill, whether it be sinking a golf putt, solving an algebra problem, or controlling physiologic behavior. A man playing darts blindfolded is unlikely to achieve as good a score as he would with the blindfold off, because feedback makes a difference.5
Four conditions are important for effective learning;5 the learner must:
- Have the capacity to respond
- Be motivated to learn
- Be positively reinforced for learning
- Be given accurate information about the results of the learning effort.
Direct feedback learning model
The direct feedback learning model assumes that adding feedback to the other important conditions of learning will result in a patient gaining control of the relevant physiology being targeted. This model has been used in treating many disorders, including Raynaud phenomenon and urinary and fecal incontinence.
Biofeedback training in this model may involve a coach/instructor/therapist only to the extent of explaining the equipment and its use. In other words, the coach “teaches the patient how to use the mirror.” More commonly.particularly for training in lowered arousal for patients in whom stress reactivity is a significant factor in the development and maintenance of excessive (sympathetic nervous system) arousal that leads to symptoms.a skilled therapist is present. The therapist not only teaches the patient how to use information from biofeedback instruments but also guides the patient in identifying and changing cognitive, emotional, and behavioral patterns that contribute to excessive reactivity. The relationship of physiologic reactivity to the subject matter under discussion also helps diagnostically in identifying stressful areas of life, particularly in psychophysiologic responders who are repressive and denying and who are not good at identifying the stressors in their lives. The equipment becomes a mirror that lets the patient see a problem that he or she had not identified as such.5
Therapeutic/stress-management/biofeedback model
When treating patients with disordered physiology (including autonomic imbalance) in the therapeutic/stress-management/biofeedback model, it is essential to understand each patient as an individual. In this model, stress management and psychotherapeutic interventions address particular vulnerabilities that lead to excessive arousal. This approach starts with a psychophysiologic assessment in which resting levels of relevant physiologic dimensions are measured; this is followed by imposition of stressors to measure reactivity and then by a recovery period in which rate and extent of recovery are measured. An interview and psychological test help determine which cognitive, emotional and behavioral patterns contribute to vulnerability. Patients typically respond well to this approach. It is common for patients to use such descriptions as, “I break out in a cold sweat when I’m stressed,” or “I feel heartsick when I’m stressed,” which suggests that the notion of mind-body interaction resonates with patients.6
CRITERIA FOR EVALUATING EFFICACY OF BIOFEEDBACK INTERVENTIONS
Several years ago a task force of the Association for Applied Psychophysiology and Biofeedback and the Society for Neuronal Regulation published criteria for evaluating the clinical efficacy of biofeedback/psychophysiologic interventions.7 These criteria are detailed below.3,7
Level 1: Not empirically supported
This designation applies to interventions supported only by anecdotal reports and/or case studies in non–peer-reviewed venues (ie, not empirically supported).
Level 2: Possibly efficacious
This applies to interventions supported by at least one study of sufficient statistical power with well-identified outcome measures but which lacked randomized assignment to a control condition internal to the study.
Level 3: Probably efficacious
This applies to interventions supported by multiple observational studies, clinical studies, wait-list–controlled studies, and within-subject and intrasubject replication studies that demonstrate efficacy.
Level 4: Efficacious
a. In a comparison with a no-treatment control group, alternative treatment group, or sham (placebo) control using randomized assignment, the intervention is shown to be statistically significantly superior to the control condition, or the intervention is equivalent to a treatment of established efficacy in a study with sufficient power to detect moderate differences, and
b. The studies have been conducted with a population treated for a specific problem, for whom inclusion criteria are delineated in a reliable, operationally defined manner, and
c. The study used valid and clearly specified outcome measures related to the problem being treated, and
d. The data were subjected to appropriate data analysis, and
e. The diagnostic and treatment variables and procedures were clearly defined in a manner that permits replication of the study by independent researchers, and
f. The superiority or equivalence of the intervention has been shown in at least two independent research settings.
Level 5: Efficacious and specific
This designation applies when the intervention has been shown to be superior to credible sham therapy, pill therapy, or alternative bona fide treatment in at least two independent research settings.
Efficacy ratings for specific disorders
Despite high standards, biofeedback thrives
The above criteria represent high standards. Since biofeedback training is often more like physical therapy or learning a language, double-blind protocols usually are not feasible, nor is sham training. Moreover, the effectiveness of training is perhaps even more difficult to assess in daily practice, with the inevitable multiplicity of confounding variables. Nevertheless, biofeedback training for many disorders is standing the test of both time and outcomes research, and it is increasingly embraced by the public and recognized by health care insurers and professionals alike.
- Gaarder KR, Montgomery PS. Clinical biofeedback: a procedural manual. Baltimore, MD: Williams and Wilkins; 1977.
- Schwartz MS, Andrasik F. Biofeedback: a practitioner’s guide. 3rd ed. New York, NY: Guilford Press; 2003.
- Yucha C, Gilbert C. Evidence-based practice in biofeedback and neurofeedback. Wheat Ridge, CO: Association for Applied Psychophysiology and Biofeedback; 2004.
- Lehrer PM, Vaschillo E, Lu SE, et al. Heart rate variability biofeedback: effects of age on heart rate variability, baroreflex gain, and asthma. Chest 2006; 129:278–284.
- McKee MG. Contributions of psychophysiologic monitoring to diagnosis and treatment of chronic head pain: a case study. Headache Q 1991; II(4):327–330.
- McKee MG. Using biofeedback and self-control techniques to prevent heart attacks. Psychiatr Ann 1978; 8:10.
- Moss D, Gunkelman J. Task Force Report on methodology and empirically supported treatments: introduction. Appl Psychophysiol Biofeedback 2002; 27:271–272.
- Weatherall M. Biofeedback or pelvic floor muscle exercises for female genuine stress incontinence: a meta-analysis of trials identified in a systematic review. BJU Int 1999; 83:1015–1016.
- Wenck LS, Leu PW, D’Amato RC. Evaluating the efficacy of a biofeedback intervention to reduce children’s anxiety. J Clin Psychol 1996; 52:469–473.
- Kaiser DA, Othmer S. Effect of neurofeedback on variables of attention in a large multi-center trial. J Neurother 2000; 4:5–15.
- Silberstein SD, for the US Headache Consortium. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55:754–762.
- Yucha CB, Clark L, Smith M, Uris P, Lafleur B, Duval S. The effect of biofeedback in hypertension. Appl Nurs Res 2001; 14:29–35.
- Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain 1999; 13:29–37.
- Van Kampen M, De Weerdt W, Van Poppel H, De Ridder D, Feys H, Baert L. Effect of pelvic-floor re-education on duration and degree of incontinence after radical prostatectomy: a randomised controlled trial. Lancet 2000; 355:98–102.
- Saxby E, Peniston EG. Alpha-theta brainwave neurofeedback training: an effective treatment for male and female alcoholics with depressive symptoms. J Clin Psychol 1995; 51:685–693.
- Lavigne JV, Ross CK, Berry SL, Hayford JR, Pachman LM. Evaluation of a psychological treatment package for treating pain in juvenile rheumatoid arthritis. Arthritis Care Res 1992; 5:101–110.
- Humphreys PA, Gevirtz RN. Treatment of recurrent abdominal pain: components analysis of four treatment protocols. J Pediatr Gastroenterol Nutr 2000; 31:47–51.
- Kotchoubey B, Strehl U, Uhlmann C, et al. Modification of slow cortical potentials in patients with refractory epilepsy: a controlled outcome study. Epilepsia 2001; 42:406–416.
- Chiarioni G, Bassotti G, Stanganini S, Vantini I, Whitehead WE. Sensory retraining is key to biofeedback therapy for formed stool fecal incontinence. Am J Gastroenterol 2002; 97:109–117.
- Labbé EE. Treatment of childhood migraine with autogenic training and skin temperature biofeedback: a component analysis. Headache 1995; 35:10–13.
- Morin CM, Hauri PJ, Espie CA, Spielman AJ, Buysse DJ, Bootzin RR. Nonpharmacologic treatment of chronic insomnia. An American Academy of Sleep Medicine review. Sleep 1999; 22:1134–1156.
- Thornton K. Improvement/rehabilitation of memory functioning with neurotherapy/QEEG biofeedback. J Head Trauma Rehabil 2000; 15:1285–1296.
- Bergeron S, Binik YM, Khalifé S, et al. A randomized comparison of group cognitive–behavioral therapy, surface electromyographic biofeedback, and vestibulectomy in the treatment of dyspareunia resulting from vulvar vestibulitis. Pain 2001; 91:297–306.
- Gaarder KR, Montgomery PS. Clinical biofeedback: a procedural manual. Baltimore, MD: Williams and Wilkins; 1977.
- Schwartz MS, Andrasik F. Biofeedback: a practitioner’s guide. 3rd ed. New York, NY: Guilford Press; 2003.
- Yucha C, Gilbert C. Evidence-based practice in biofeedback and neurofeedback. Wheat Ridge, CO: Association for Applied Psychophysiology and Biofeedback; 2004.
- Lehrer PM, Vaschillo E, Lu SE, et al. Heart rate variability biofeedback: effects of age on heart rate variability, baroreflex gain, and asthma. Chest 2006; 129:278–284.
- McKee MG. Contributions of psychophysiologic monitoring to diagnosis and treatment of chronic head pain: a case study. Headache Q 1991; II(4):327–330.
- McKee MG. Using biofeedback and self-control techniques to prevent heart attacks. Psychiatr Ann 1978; 8:10.
- Moss D, Gunkelman J. Task Force Report on methodology and empirically supported treatments: introduction. Appl Psychophysiol Biofeedback 2002; 27:271–272.
- Weatherall M. Biofeedback or pelvic floor muscle exercises for female genuine stress incontinence: a meta-analysis of trials identified in a systematic review. BJU Int 1999; 83:1015–1016.
- Wenck LS, Leu PW, D’Amato RC. Evaluating the efficacy of a biofeedback intervention to reduce children’s anxiety. J Clin Psychol 1996; 52:469–473.
- Kaiser DA, Othmer S. Effect of neurofeedback on variables of attention in a large multi-center trial. J Neurother 2000; 4:5–15.
- Silberstein SD, for the US Headache Consortium. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000; 55:754–762.
- Yucha CB, Clark L, Smith M, Uris P, Lafleur B, Duval S. The effect of biofeedback in hypertension. Appl Nurs Res 2001; 14:29–35.
- Crider AB, Glaros AG. A meta-analysis of EMG biofeedback treatment of temporomandibular disorders. J Orofac Pain 1999; 13:29–37.
- Van Kampen M, De Weerdt W, Van Poppel H, De Ridder D, Feys H, Baert L. Effect of pelvic-floor re-education on duration and degree of incontinence after radical prostatectomy: a randomised controlled trial. Lancet 2000; 355:98–102.
- Saxby E, Peniston EG. Alpha-theta brainwave neurofeedback training: an effective treatment for male and female alcoholics with depressive symptoms. J Clin Psychol 1995; 51:685–693.
- Lavigne JV, Ross CK, Berry SL, Hayford JR, Pachman LM. Evaluation of a psychological treatment package for treating pain in juvenile rheumatoid arthritis. Arthritis Care Res 1992; 5:101–110.
- Humphreys PA, Gevirtz RN. Treatment of recurrent abdominal pain: components analysis of four treatment protocols. J Pediatr Gastroenterol Nutr 2000; 31:47–51.
- Kotchoubey B, Strehl U, Uhlmann C, et al. Modification of slow cortical potentials in patients with refractory epilepsy: a controlled outcome study. Epilepsia 2001; 42:406–416.
- Chiarioni G, Bassotti G, Stanganini S, Vantini I, Whitehead WE. Sensory retraining is key to biofeedback therapy for formed stool fecal incontinence. Am J Gastroenterol 2002; 97:109–117.
- Labbé EE. Treatment of childhood migraine with autogenic training and skin temperature biofeedback: a component analysis. Headache 1995; 35:10–13.
- Morin CM, Hauri PJ, Espie CA, Spielman AJ, Buysse DJ, Bootzin RR. Nonpharmacologic treatment of chronic insomnia. An American Academy of Sleep Medicine review. Sleep 1999; 22:1134–1156.
- Thornton K. Improvement/rehabilitation of memory functioning with neurotherapy/QEEG biofeedback. J Head Trauma Rehabil 2000; 15:1285–1296.
- Bergeron S, Binik YM, Khalifé S, et al. A randomized comparison of group cognitive–behavioral therapy, surface electromyographic biofeedback, and vestibulectomy in the treatment of dyspareunia resulting from vulvar vestibulitis. Pain 2001; 91:297–306.