User login
ANSWER
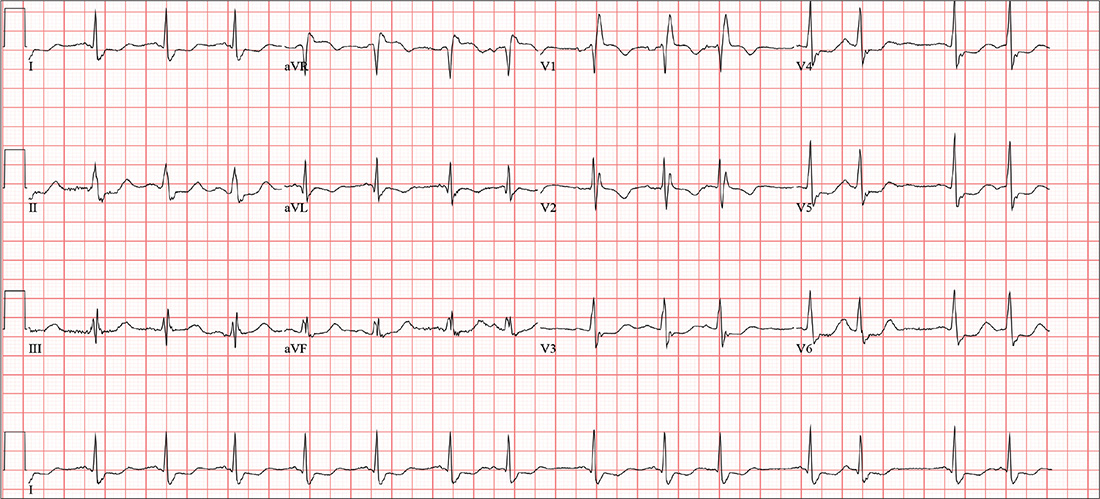
This ECG demonstrates sinus rhythm with premature atrial contractions (PACs), a normal axis, a right bundle branch block, a prolonged QTc interval, and T-wave abnormalities suggestive of lateral ischemia.
Sinus rhythm is indicated by a P wave for every QRS complex and a QRS complex for every P wave with a consistent PR interval.
PACs are seen on the seventh, 10th, and 12th beats on the rhythm strip. Notice that the R-R interval is shortened, the R wave of the PACs is identical to that of sinus rhythm, and there is a compensatory pause following the PAC before the sinus rhythm ensues. The R-wave axis of 26° is within the normal range (–30° to 90°).
A right bundle branch block is identified by a QRS duration > 120 ms (156 ms), an RSR’ “rabbit ear” pattern in the anterior precordial leads (particularly lead V1), and slurred S waves in leads I and aVL. Although opinions vary, a QTc interval > 460 ms in women (> 440 ms in men) is typically considered prolonged. This patient fits that criteria (529 ms). Finally, the ST depressions in leads V4 to V6 suggest lateral ischemia.
A comparison of this ECG to one obtained a year ago showed no difference, with the exception of new-onset PACs. The patient was cleared for surgical repair of her forearm fracture.
ANSWER
This ECG demonstrates sinus rhythm with premature atrial contractions (PACs), a normal axis, a right bundle branch block, a prolonged QTc interval, and T-wave abnormalities suggestive of lateral ischemia.
Sinus rhythm is indicated by a P wave for every QRS complex and a QRS complex for every P wave with a consistent PR interval.
PACs are seen on the seventh, 10th, and 12th beats on the rhythm strip. Notice that the R-R interval is shortened, the R wave of the PACs is identical to that of sinus rhythm, and there is a compensatory pause following the PAC before the sinus rhythm ensues. The R-wave axis of 26° is within the normal range (–30° to 90°).
A right bundle branch block is identified by a QRS duration > 120 ms (156 ms), an RSR’ “rabbit ear” pattern in the anterior precordial leads (particularly lead V1), and slurred S waves in leads I and aVL. Although opinions vary, a QTc interval > 460 ms in women (> 440 ms in men) is typically considered prolonged. This patient fits that criteria (529 ms). Finally, the ST depressions in leads V4 to V6 suggest lateral ischemia.
A comparison of this ECG to one obtained a year ago showed no difference, with the exception of new-onset PACs. The patient was cleared for surgical repair of her forearm fracture.
ANSWER
This ECG demonstrates sinus rhythm with premature atrial contractions (PACs), a normal axis, a right bundle branch block, a prolonged QTc interval, and T-wave abnormalities suggestive of lateral ischemia.
Sinus rhythm is indicated by a P wave for every QRS complex and a QRS complex for every P wave with a consistent PR interval.
PACs are seen on the seventh, 10th, and 12th beats on the rhythm strip. Notice that the R-R interval is shortened, the R wave of the PACs is identical to that of sinus rhythm, and there is a compensatory pause following the PAC before the sinus rhythm ensues. The R-wave axis of 26° is within the normal range (–30° to 90°).
A right bundle branch block is identified by a QRS duration > 120 ms (156 ms), an RSR’ “rabbit ear” pattern in the anterior precordial leads (particularly lead V1), and slurred S waves in leads I and aVL. Although opinions vary, a QTc interval > 460 ms in women (> 440 ms in men) is typically considered prolonged. This patient fits that criteria (529 ms). Finally, the ST depressions in leads V4 to V6 suggest lateral ischemia.
A comparison of this ECG to one obtained a year ago showed no difference, with the exception of new-onset PACs. The patient was cleared for surgical repair of her forearm fracture.
A 74-year-old woman becomes dizzy and slips in the shower. She instinctively extends her left arm and feels a snap as it hits the floor. H
Medical history is remarkable for hypertension, hypothyroidism, renal insufficiency, and benign positional vertigo. The patient denies cardiac history, including angina, dyspnea, or syncope. She describes her prefall dizziness as similar to her vertigo-related symptoms.
Family history is remarkable for hypertension, type 2 diabetes, stroke (mother), and myocardial infarction (brother). Her father’s medical history is unknown.
The patient is a retired high school librarian. She has never smoked or used recreational drugs, but she does enjoy a daily “nightcap” of brandy. Her current medications include furosemide, metoprolol, and levothyroxine. She has no known drug allergies.
She denies any recent infection, including cold or flu. A 12-point review of systems is unremarkable. Vital signs include a blood pressure of 142/88 mm Hg; pulse, 88 beats/min; respiratory rate, 14 breaths/min-1; and temperature, 98.4°F. Her height is 5’6” and her weight, 147 lb.
The patient is alert, cooperative, and oriented to person, place, and time. HEENT exam is remarkable for corrective lenses and bilateral hearing aids. There is no obvious sign of head trauma. The neck is supple, and there are no carotid bruits or jugular venous distention. The thyroid is small but palpable. The lungs are clear in all fields without rales, rhonchi, or wheezes.
Cardiac exam reveals a regular rate of 88 beats/min with occasional pauses. There is a soft II/VI murmur of mitral regurgitation heard at the left lower sternal border. There are no extra heart sounds or rubs. The abdomen is soft and nontender. There is no palpable organomegaly.
The extremities demonstrate full range of motion. Pulses are full and equal bilaterally, and there is no peripheral edema. The neurologic exam is intact.
An ECG shows a ventricular rate of 87 beats/min; PR interval, 156 ms; QRS duration, 138 ms; QT/QTc interval, 440/529 ms; P axis, 58°; R axis, 26°; and T axis, 105°. What is your interpretation?
