User login
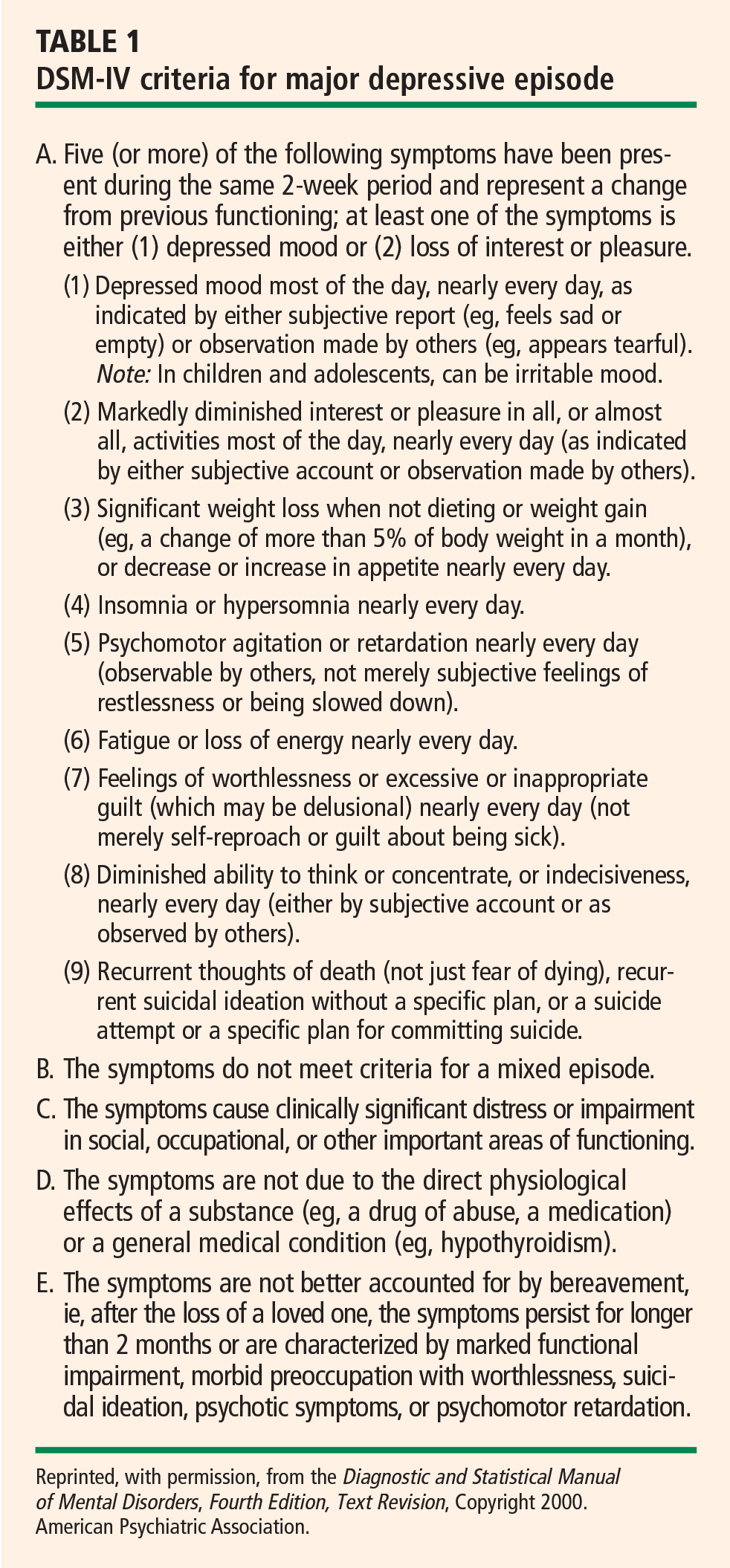
Minor depressive disorder (mDD) is not an official DSM-IV diagnosis but is used for research purposes; it is similar to MDD in duration but requires that only two to four symptoms be present.
EPIDEMIOLOGY OF DEPRESSION
Depression is a widespread and often chronic condition. Lifetime prevalence estimates for MDD are approximately 15% to 20%;2,3 1-year prevalence estimates are 5% to 10%;2,4 and point prevalence estimates range from 4% to 7%.3,5 Moreover, MDD is characterized by high rates of relapse: 22% to 50% of patients suffer recurrent episodes within 6 months after recovery.6
Women are twice as likely as men to be diagnosed with MDD, with lifetime prevalence rates of 10% to 25% in women versus 5% to 12% in men.1
Although rates of depression do not appear to increase with age, MDD often goes undertreated in older adults3 and in cardiac patients.7
DIAGNOSING AND ASSESSING DEPRESSION
The gold standard for diagnosing MDD is a clinical interview. Commonly used instruments include the Diagnostic Interview Schedule8 and the Composite International Diagnostic Interview.9 The Structured Clinical Interview for DSM-IV Axis I Disorders10 and the Schedule for Affective Disorders and Schizophrenia11 are frequently used semistructured interviews.
The most common clinical instruments for assessing the severity of depressive symptoms are the Hamilton Rating Scale for Depression (HAM-D),12 which is a clinician-rated scale, and various psychometric questionnaires, including the Beck Depression Inventory (BDI)13,14 and the Center for Epidemiological Studies Depression Scale (CES-D).15
THE DEPRESSION–HEART DISEASE LINK
Depression as a primary risk factor
Depression as a secondary risk factor
Depression is an even stronger risk factor for cardiac events in patients with established CHD. Point estimates range from 14% to as high as 47%, with higher rates in patients with unstable angina and in patients awaiting coronary artery bypass graft (CABG) surgery; an additional 20% of patients exhibit elevated depressive symptoms or minor depression (mDD).19–25
Prospective studies have shown that depression increases the risk for death or nonfatal cardiac events approximately 2.5-fold in patients with CHD. For instance, Frasure-Smith et al followed 896 patients with a recent acute MI and found that the presence of depressive symptoms as indicated by an elevated BDI score was a significant predictor of cardiac mortality after controlling for multivariate predictors of mortality (odds ratio [OR] = 3.29 for women and 3.05 for men).26
Two recent meta-analyses confirmed the association between depression and adverse clinical outcomes in patients with CHD.27,28 For example, van Melle et al reported that post-MI depression was associated with a 2- to 2.5-fold increase in the risk of adverse health outcomes.28 In this analysis, depression’s effect on cardiac mortality and all-cause mortality was especially pronounced in older studies (before 1992) (OR = 3.2) compared with more recent studies (after 1992) (OR = 2.01).28
Duke University researchers have conducted several prospective studies in various cardiac populations.29–31 Barefoot et al assessed 1,250 patients with documented CHD using the Zung Self-Rating Depression Scale at the time of diagnostic coronary angiography and followed them for up to 19.4 years.29 Results showed that patients with moderate to severe depression were at 69% greater risk for cardiac death and 78% greater risk for all-cause death than were their nondepressed counterparts.
We also recently reported results from a prospective study that followed 204 patients with heart failure over a median interval of 3 years.31 Clinically significant symptoms of depression (BDI score ≥ 10) were associated with a hazard ratio of 1.56 (95% CI, 1.07 to 2.29) for the combined end point of death or cardiovascular hospitalization. These observations included adjustment for plasma NT-proBNP level, ejection fraction, and other established risk factors, suggesting that heightened risk of adverse clinical outcomes associated with depressive symptoms is not simply a reflection of the severity of heart failure.
In summary, a number of observational studies have demonstrated that depression is associated with increased risk of morbidity and mortality both in healthy populations and in a variety of populations with established cardiac disease.
BIOBEHAVIORAL MECHANISMS LINKING DEPRESSION AND CHD
A number of biobehavioral mechanisms have been hypothesized to underlie the relationship between depression and CHD. Most evidence is derived from cross-sectional studies and suggests that depression is associated with traditional risk factors for CHD, such as hypertension, diabetes, and insulin resistance,32,33 as well as changes in platelet reactivity,34 dysregulation of the autonomic nervous system35 and hypothalamic-pituitary-adrenal axis,36 and alterations in the immune response/inflammation.37 Depression is also associated with behavioral factors that are in turn associated with CHD risk, such as reduced treatment adherence,38 smoking,39 and physical inactivity.40
STUDIES OF DEPRESSION TREATMENT IN CARDIAC PATIENTS
Successful treatments for depression in patients with CHD may have the potential to improve not only quality of life but also cardiovascular and physical health. Several treatments for depression exist for use in the general population, such as antidepressant medication or psychotherapy.41 However, only three studies have tested the efficacy of these treatments in patients with CHD: SADHART, ENRICHD, and CREATE.42–44
SADHART (Sertraline Antidepressant Heart Attack Randomized Trial) was a safety and efficacy evaluation of antidepressant medication in patients with MDD and a recent MI or unstable angina.42 It showed only modest differences in reductions in depressive symptoms between sertraline recipients and placebo recipients, and it lacked statistical power to examine the impact of treatment on hard clinical end points.
ENRICHD (Enhancing Recovery in Coronary Heart Disease Patients) assessed the effect of psychosocial treatment on survival among more than than 2,400 post-MI patients.43 Although this trial found that cognitive behavior therapy resulted in significant, albeit small, improvements in depressive symptoms compared with usual care, it failed to demonstrate that treating depression and low social support was associated with increased survival.
CREATE (Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy), a recent placebo-controlled trial, assessed the value of antidepressant medication and clinical management in patients with CHD.44 The study’s 284 patients, all of whom had CHD as well as MDD and a HAM-D score of 20 or greater, underwent two separate randomizations: (1) to 12 weeks of interpersonal therapy plus clinical management or 12 weeks of clinical management alone, and (2) to 12 weeks of citalopram therapy or matching placebo. There was no difference between interpersonal therapy and clinical management alone; however, citalopram was superior to placebo in reducing HAM-D scores and demonstrated better remission rates (35.9% with citalopram vs 22.5% with placebo). The same therapists who provided interpersonal therapy also performed the clinical management, so it could be argued that this was why additional interpersonal therapist time did not result in greater reductions in depressive symptoms than did clinical management alone. Furthermore, this study did not examine the effects of depression therapy on clinical outcomes.
EXERCISE AS A TREATMENT FOR DEPRESSION
There is growing evidence that exercise may be an effective treatment for depression.45 Most of the existing studies of exercise for depression have focused on aerobic exercise.
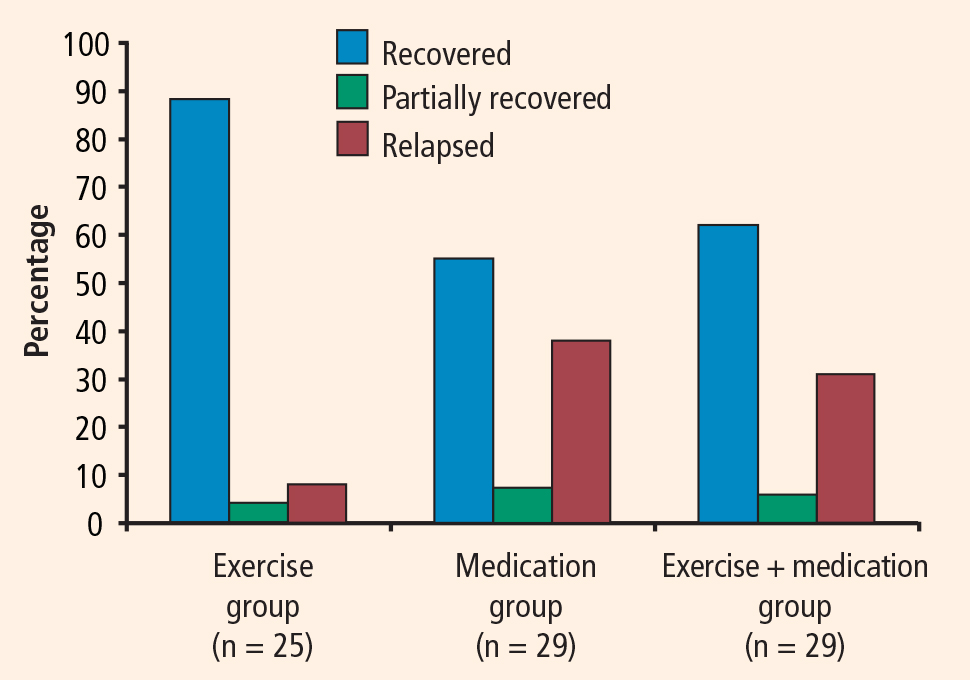
In the relatively large SMILE study (Standard Medical Intervention and Long-term Exercise),46 conducted at Duke University, 156 adult noncardiac patients with MDD were randomized to 4 months of treatment with supervised aerobic exercise, antidepressant medication (sertraline), or a combination of exercise and medication. Although antidepressant medication was associated with faster reductions in depression in the first 4 weeks of treatment among mildly depressed patients, exercise was as effective as antidepressant medication in treating depression by the end of the 16-week intervention for all participants.
Exercise generally is considered safe for most patients with stable CHD.48 Some studies of exercise treatments for patients with CHD have tracked depressive symptoms and thus have provided insight into the potential efficacy of exercise as a treatment for depression in this population. Although most of these studies have reported significant improvements in depression after completion of an exercise program, many have had important methodologic limitations, including absence of a control group. In one of the few controlled studies in this area, Stern et al49 randomized 106 men who had a recent acute MI and elevated depression, anxiety, or low fitness to 12 weeks of exercise training, group therapy, or usual care (control). At 1-year follow-up, subjects in both the exercise and counseling groups showed improvements in depression relative to controls.
EFFECT OF EXERCISE ON CARDIOVASCULAR RISK FACTORS AND OUTCOMES
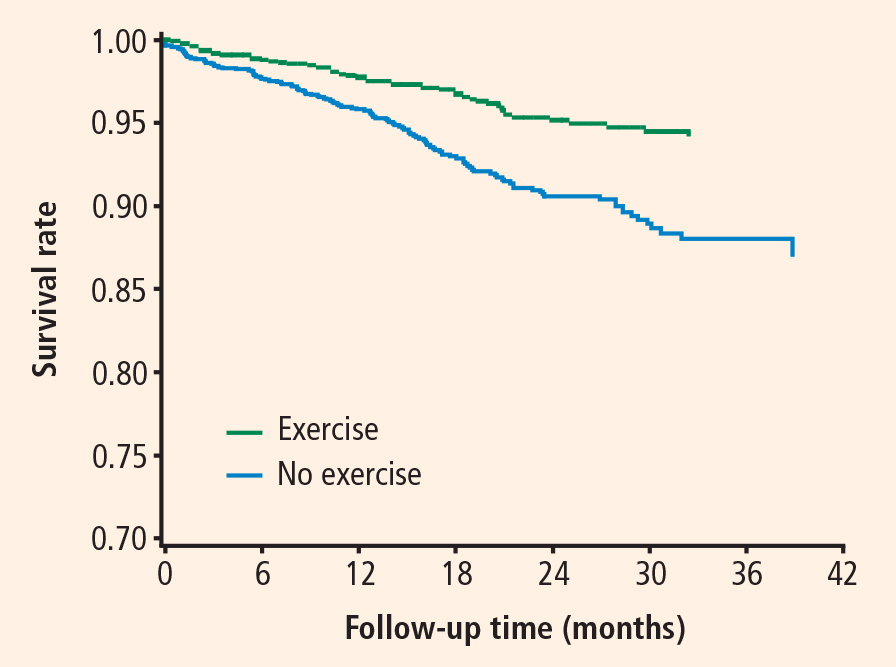
Exercise is a particularly promising intervention for depression in patients with CHD because it has well-documented cardiovascular benefits. In addition to the well-established role of exercise interventions in primary prevention, such interventions have been shown to improve outcomes for patients with CHD.50
Jolliffe et al conducted a meta-analysis comparing exercise-only interventions, comprehensive rehabilitation (including educational and behavioral components such as dietary changes and stress reduction in addition to exercise), and usual care.51 Exercise-only interventions were associated with reductions in both all-cause and cardiac mortality relative to usual care. Comprehensive rehabilitation, on the other hand, was not associated with statistically significant reductions in all-cause mortality relative to usual care, but it was associated with a decreased risk for cardiac mortality, to a slightly lesser extent than exercise-only interventions.
The evidence that exercise affects depression, CHD risk factors, and CHD outcomes suggests that exercise is a particularly promising intervention for depression in this population.
UPBEAT trial promises further insight
A new Duke University study known as UPBEAT (Understanding Prognostic Benefits of Exercise and Antidepressant Treatment) is randomizing 200 patients with elevated depressive symptoms to exercise, antidepressant therapy (sertraline), or placebo for 4 months.53 A variety of “biomarkers” of risk are being assessed, including measures of heart rate variability, vascular function, inflammation, and platelet aggregation. Results of this 5-year trial should be available by 2011.
CONCLUSIONS
Although depression has emerged as an important risk factor for CHD, there is no consensus on the optimal way to treat depression in patients with CHD. Interventions that are guided by an understanding of the mechanisms linking depression to CHD may prove to be most effective in improving both depression and physical health outcomes.
Exercise targets many of the mechanisms by which depression may be associated with increased risk, including autonomic nervous system activity, hypothalamic-pituitary-adrenal axis function, platelet activation, vascular function, and inflammation. Moreover, a growing body of evidence suggests that exercise is an effective treatment for depression that may be comparable in effect to antidepressant medication, at least in select subgroups (eg, patients who are receptive to exercise as a treatment for depression). The value of exercise training—not only for improving quality of life, but also for improving “biomarkers” of risk and other relevant health outcomes—is the focus of our current research efforts.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Text Revision. 4th ed. Washington, DC: American Psychiatric Association; 2000.
- Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8–19.
- Steffens DC, Skoog I, Norton MC, et al. Prevalence of depression and its treatment in an elderly population: the Cache County study. Arch Gen Psychiatry 2000; 57:601–617.
- Regier DA, Narrow WE, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Ayuso-Mateos JL, Vazquez-Barquero JL, Dowrick C, et al. Depressive disorders in Europe: prevalence figures from the ODIN study. Br J Psychiatry 2001; 179:308–316.
- Belsher G, Costello CG. Relapse after recovery from unipolar depression: a critical review. Psychol Bull 1988; 104:84–96.
- Carney RM, Rich MW, Tevelde A, Saini J, Clark K, Jaffe AS. Major depressive disorder in coronary artery disease. Am J Cardiol 1987; 60:1273–1275.
- Robins LN, Helzer JE, Crougham J, Ratliff K. National Institute of Mental Health diagnostic interview schedule. Arch Gen Psychiatry 1981; 38:381–389.
- World Health Organization. Composite International Diagnostic Interview. Geneva, Switzerland: World Health Organization; 1990.
- First M, Spitzer L, Gibbon M. Structured clinical interview for axis I DSM-IV disorders. Washington, DC: American Psychiatric Press; 1995.
- Endicott J, Spitzer RL. The schedule for affective disorders and schizophrenia. Arch Gen Psychiatry 1978; 35:837–844.
- Hamilton M. A rating scale for depression. J Neurol 1960; 23:56–61.
- Beck AT, Ward CH, Mendelsohn M. An inventory for measuring depression. Arch Gen Psychiatry 1961; 4:561–571.
- Beck AT, Steer RA, Brown GK. Beck Depression Inventory Manual. 2nd ed. San Antonio, TX: The Psychological Corporation; 1996.
- Hautzinger M. The CES-D scale: a depression-rating scale for research in the general population. Diagnostica 1988; 34:167–173.
- Lett H, Blumenthal J, Babyak M, Sherwood A, Strauman T, Robins C. Depression as a risk factor for coronary artery disease: evidence, mechanisms, and treatment. Psychosom Med 2004; 66:305–315.
- Rugulies R. Depression as a predictor for coronary heart disease. A review and meta-analysis. Am J Prev Med 2002; 23:51–61.
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol 2005; 45:637–651.
- Carney RM, Rich MW, Freedland KE, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988; 50:627–633.
- Schleifer SJ, Macari-Hinson MM, Coyle DA, et al. The nature and course of depression following myocardial infarction. Arch Intern Med 1989; 149:1785–1789.
- Frasure-Smith N, Lesperance F, Talajic M. Depression following myocardial infarction. Impact on 6-month survival. JAMA 1993; 270:1819–1825.
- Lesperance F, Frasure-Smith N, Juneau M, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000; 160:1354–1360.
- Connerney I, Shapiro PA, McLaughlin JS, Bagiella E, Sloan RP. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001; 358:1766–1771.
- Jiang W, Alexander J, Christopher E, et al. Relationship of depression to increased risk of mortality and rehospitalization in patients with congestive heart failure. Arch Intern Med 2001; 161:1849–1856.
- Burker EJ, Blumenthal JA, Feldman M, et al. Depression in male and female patients undergoing cardiac surgery. Br J Clin Psychol 1995; 34:119–128.
- Frasure-Smith N, Lesperance F, Juneau M, Talajic M, Bourassa MG. Gender, depression, and one-year prognosis after myocardial infarction. Psychosom Med 1999; 61:26–37.
- Barth J, Schumacher M, Hermann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med 2004; 66:802–813.
- van Melle JP, de Jong P, Spijkerman TA, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis. Psychosom Med 2004; 66:814–822.
- Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol 1996; 78:613–617.
- Blumenthal JA, Lett H, Babyak M, et al. Depression as a risk factor for mortality after coronary artery bypass surgery. Lancet 2003; 362:604–609.
- Sherwood A, Blumenthal JA, Trivedi R, et al. Relationship of depression to mortality and hospitalization in patients with heart failure. Arch Intern Med 2007; 167:367–373.
- Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2001; 24:1069–1078.
- Thakore JH, Richards PJ, Reznek RH, Martin A, Dinan TG. Increased intra-abdominal fat deposition in patients with major depressive illness as measured by computed tomography. Biol Psychiatry 1997; 41:1140–1142.
- Musselman DL, Tomer A, Manatunga AK, et al. Exaggerated platelet reactivity in major depression. Am J Psychiatry 1996; 153:1313–1317.
- Delgado PL, Moreno FA. Role of norepinephrine in depression. J Clin Psychiatry 2000; 61:5–12.
- Akil H, Haskett RF, Young EA, et al. Multiple HPA profiles in endogenous depression: effect of age and sex on cortisol and beta-endorphin. Biol Psychiatry 1993; 33:73–85.
- Kop WJ, Gottdiener JS, Tangen CM, et al. Inflammation and coagulation factors in persons > 65 years of age with symptoms of depression but without evidence of myocardial ischemia. Am J Cardiol 2002; 89:419–424.
- Carney RM, Freedland KE, Eisen SA, Rich MW, Jaffe AS. Major depression and medication adherence in elderly patients with coronary artery disease. Health Psychol 1995; 14:88–90.
- Lehto S, Koukkunen H, Hintikka J, Viinamaki H, Laakso M, Pyorala K. Depression after coronary heart disease events. Scand Cardiovasc J 2000; 34:580–583.
- Camacho TC, Roberts RE, Lazarus NB, Kaplan GA, Cohen RD. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol 1991; 134:220–231.
- Depression Guideline Panel. Depression in Primary Care: Volume 2. Treatment of Depression, Clinical Practice Guideline, No. 5. Rockville, MD: Agency for Health Care Policy and Research, Public Health Service, US Dept of Health and Human Services; 1993.
- Glassman AH, O’Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002; 288:701–709.
- Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 2003; 289:3106–3116.
- Lesperance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA 2007; 297:367–379.
- Brosse AL, Sheets ES, Lett HS, Blumenthal JA. Exercise and the treatment of clinical depression in adults: recent findings and future directions. Sports Med 2002; 32:741–760.
- Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med 1999; 159:2349–2356.
- Babyak M, Blumenthal JA, Herman S, et al. Exercise treatment for major depression: maintenance of therapeutic benefit at 10 months. Psychosom Med 2000; 62:633–638.
- Franklin BA, Bonzheim K, Gordon S, Timmis GC. Safety of medically supervised outpatient cardiac rehabilitation exercise therapy: a 16-year follow-up. Chest 1998; 114:902–906.
- Stern MJ, Gorman PA, Kaslow L. The group counseling v exercise therapy study. A controlled intervention with subjects following myocardial infarction. Arch Intern Med 1983; 143:1719–1725.
- Oldridge NB, Guyatt GH, Fischer ME, Rimm AA. Cardiac rehabilitation after myocardial infarction. Combined experience of randomized clinical trials. JAMA 1988; 260:945–950.
- Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2001; (1):CD001800.
- Blumenthal JA, Babyak MA, Carney RM, et al. Exercise, depression, and mortality after myocardial infarction in the ENRICHD trial. Med Sci Sports Exerc 2004; 36:746–755.
- Blumenthal JA, Sherwood A, Rogers SD, et al. Understanding prognostic benefits of exercise and antidepressant therapy for persons with depression and heart disease: the UPBEAT study—rationale, design, and methodological issues. Clin Trials 2007; 4:548–559.
Minor depressive disorder (mDD) is not an official DSM-IV diagnosis but is used for research purposes; it is similar to MDD in duration but requires that only two to four symptoms be present.
EPIDEMIOLOGY OF DEPRESSION
Depression is a widespread and often chronic condition. Lifetime prevalence estimates for MDD are approximately 15% to 20%;2,3 1-year prevalence estimates are 5% to 10%;2,4 and point prevalence estimates range from 4% to 7%.3,5 Moreover, MDD is characterized by high rates of relapse: 22% to 50% of patients suffer recurrent episodes within 6 months after recovery.6
Women are twice as likely as men to be diagnosed with MDD, with lifetime prevalence rates of 10% to 25% in women versus 5% to 12% in men.1
Although rates of depression do not appear to increase with age, MDD often goes undertreated in older adults3 and in cardiac patients.7
DIAGNOSING AND ASSESSING DEPRESSION
The gold standard for diagnosing MDD is a clinical interview. Commonly used instruments include the Diagnostic Interview Schedule8 and the Composite International Diagnostic Interview.9 The Structured Clinical Interview for DSM-IV Axis I Disorders10 and the Schedule for Affective Disorders and Schizophrenia11 are frequently used semistructured interviews.
The most common clinical instruments for assessing the severity of depressive symptoms are the Hamilton Rating Scale for Depression (HAM-D),12 which is a clinician-rated scale, and various psychometric questionnaires, including the Beck Depression Inventory (BDI)13,14 and the Center for Epidemiological Studies Depression Scale (CES-D).15
THE DEPRESSION–HEART DISEASE LINK
Depression as a primary risk factor
Depression as a secondary risk factor
Depression is an even stronger risk factor for cardiac events in patients with established CHD. Point estimates range from 14% to as high as 47%, with higher rates in patients with unstable angina and in patients awaiting coronary artery bypass graft (CABG) surgery; an additional 20% of patients exhibit elevated depressive symptoms or minor depression (mDD).19–25
Prospective studies have shown that depression increases the risk for death or nonfatal cardiac events approximately 2.5-fold in patients with CHD. For instance, Frasure-Smith et al followed 896 patients with a recent acute MI and found that the presence of depressive symptoms as indicated by an elevated BDI score was a significant predictor of cardiac mortality after controlling for multivariate predictors of mortality (odds ratio [OR] = 3.29 for women and 3.05 for men).26
Two recent meta-analyses confirmed the association between depression and adverse clinical outcomes in patients with CHD.27,28 For example, van Melle et al reported that post-MI depression was associated with a 2- to 2.5-fold increase in the risk of adverse health outcomes.28 In this analysis, depression’s effect on cardiac mortality and all-cause mortality was especially pronounced in older studies (before 1992) (OR = 3.2) compared with more recent studies (after 1992) (OR = 2.01).28
Duke University researchers have conducted several prospective studies in various cardiac populations.29–31 Barefoot et al assessed 1,250 patients with documented CHD using the Zung Self-Rating Depression Scale at the time of diagnostic coronary angiography and followed them for up to 19.4 years.29 Results showed that patients with moderate to severe depression were at 69% greater risk for cardiac death and 78% greater risk for all-cause death than were their nondepressed counterparts.
We also recently reported results from a prospective study that followed 204 patients with heart failure over a median interval of 3 years.31 Clinically significant symptoms of depression (BDI score ≥ 10) were associated with a hazard ratio of 1.56 (95% CI, 1.07 to 2.29) for the combined end point of death or cardiovascular hospitalization. These observations included adjustment for plasma NT-proBNP level, ejection fraction, and other established risk factors, suggesting that heightened risk of adverse clinical outcomes associated with depressive symptoms is not simply a reflection of the severity of heart failure.
In summary, a number of observational studies have demonstrated that depression is associated with increased risk of morbidity and mortality both in healthy populations and in a variety of populations with established cardiac disease.
BIOBEHAVIORAL MECHANISMS LINKING DEPRESSION AND CHD
A number of biobehavioral mechanisms have been hypothesized to underlie the relationship between depression and CHD. Most evidence is derived from cross-sectional studies and suggests that depression is associated with traditional risk factors for CHD, such as hypertension, diabetes, and insulin resistance,32,33 as well as changes in platelet reactivity,34 dysregulation of the autonomic nervous system35 and hypothalamic-pituitary-adrenal axis,36 and alterations in the immune response/inflammation.37 Depression is also associated with behavioral factors that are in turn associated with CHD risk, such as reduced treatment adherence,38 smoking,39 and physical inactivity.40
STUDIES OF DEPRESSION TREATMENT IN CARDIAC PATIENTS
Successful treatments for depression in patients with CHD may have the potential to improve not only quality of life but also cardiovascular and physical health. Several treatments for depression exist for use in the general population, such as antidepressant medication or psychotherapy.41 However, only three studies have tested the efficacy of these treatments in patients with CHD: SADHART, ENRICHD, and CREATE.42–44
SADHART (Sertraline Antidepressant Heart Attack Randomized Trial) was a safety and efficacy evaluation of antidepressant medication in patients with MDD and a recent MI or unstable angina.42 It showed only modest differences in reductions in depressive symptoms between sertraline recipients and placebo recipients, and it lacked statistical power to examine the impact of treatment on hard clinical end points.
ENRICHD (Enhancing Recovery in Coronary Heart Disease Patients) assessed the effect of psychosocial treatment on survival among more than than 2,400 post-MI patients.43 Although this trial found that cognitive behavior therapy resulted in significant, albeit small, improvements in depressive symptoms compared with usual care, it failed to demonstrate that treating depression and low social support was associated with increased survival.
CREATE (Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy), a recent placebo-controlled trial, assessed the value of antidepressant medication and clinical management in patients with CHD.44 The study’s 284 patients, all of whom had CHD as well as MDD and a HAM-D score of 20 or greater, underwent two separate randomizations: (1) to 12 weeks of interpersonal therapy plus clinical management or 12 weeks of clinical management alone, and (2) to 12 weeks of citalopram therapy or matching placebo. There was no difference between interpersonal therapy and clinical management alone; however, citalopram was superior to placebo in reducing HAM-D scores and demonstrated better remission rates (35.9% with citalopram vs 22.5% with placebo). The same therapists who provided interpersonal therapy also performed the clinical management, so it could be argued that this was why additional interpersonal therapist time did not result in greater reductions in depressive symptoms than did clinical management alone. Furthermore, this study did not examine the effects of depression therapy on clinical outcomes.
EXERCISE AS A TREATMENT FOR DEPRESSION
There is growing evidence that exercise may be an effective treatment for depression.45 Most of the existing studies of exercise for depression have focused on aerobic exercise.
In the relatively large SMILE study (Standard Medical Intervention and Long-term Exercise),46 conducted at Duke University, 156 adult noncardiac patients with MDD were randomized to 4 months of treatment with supervised aerobic exercise, antidepressant medication (sertraline), or a combination of exercise and medication. Although antidepressant medication was associated with faster reductions in depression in the first 4 weeks of treatment among mildly depressed patients, exercise was as effective as antidepressant medication in treating depression by the end of the 16-week intervention for all participants.
Exercise generally is considered safe for most patients with stable CHD.48 Some studies of exercise treatments for patients with CHD have tracked depressive symptoms and thus have provided insight into the potential efficacy of exercise as a treatment for depression in this population. Although most of these studies have reported significant improvements in depression after completion of an exercise program, many have had important methodologic limitations, including absence of a control group. In one of the few controlled studies in this area, Stern et al49 randomized 106 men who had a recent acute MI and elevated depression, anxiety, or low fitness to 12 weeks of exercise training, group therapy, or usual care (control). At 1-year follow-up, subjects in both the exercise and counseling groups showed improvements in depression relative to controls.
EFFECT OF EXERCISE ON CARDIOVASCULAR RISK FACTORS AND OUTCOMES
Exercise is a particularly promising intervention for depression in patients with CHD because it has well-documented cardiovascular benefits. In addition to the well-established role of exercise interventions in primary prevention, such interventions have been shown to improve outcomes for patients with CHD.50
Jolliffe et al conducted a meta-analysis comparing exercise-only interventions, comprehensive rehabilitation (including educational and behavioral components such as dietary changes and stress reduction in addition to exercise), and usual care.51 Exercise-only interventions were associated with reductions in both all-cause and cardiac mortality relative to usual care. Comprehensive rehabilitation, on the other hand, was not associated with statistically significant reductions in all-cause mortality relative to usual care, but it was associated with a decreased risk for cardiac mortality, to a slightly lesser extent than exercise-only interventions.
The evidence that exercise affects depression, CHD risk factors, and CHD outcomes suggests that exercise is a particularly promising intervention for depression in this population.
UPBEAT trial promises further insight
A new Duke University study known as UPBEAT (Understanding Prognostic Benefits of Exercise and Antidepressant Treatment) is randomizing 200 patients with elevated depressive symptoms to exercise, antidepressant therapy (sertraline), or placebo for 4 months.53 A variety of “biomarkers” of risk are being assessed, including measures of heart rate variability, vascular function, inflammation, and platelet aggregation. Results of this 5-year trial should be available by 2011.
CONCLUSIONS
Although depression has emerged as an important risk factor for CHD, there is no consensus on the optimal way to treat depression in patients with CHD. Interventions that are guided by an understanding of the mechanisms linking depression to CHD may prove to be most effective in improving both depression and physical health outcomes.
Exercise targets many of the mechanisms by which depression may be associated with increased risk, including autonomic nervous system activity, hypothalamic-pituitary-adrenal axis function, platelet activation, vascular function, and inflammation. Moreover, a growing body of evidence suggests that exercise is an effective treatment for depression that may be comparable in effect to antidepressant medication, at least in select subgroups (eg, patients who are receptive to exercise as a treatment for depression). The value of exercise training—not only for improving quality of life, but also for improving “biomarkers” of risk and other relevant health outcomes—is the focus of our current research efforts.
Minor depressive disorder (mDD) is not an official DSM-IV diagnosis but is used for research purposes; it is similar to MDD in duration but requires that only two to four symptoms be present.
EPIDEMIOLOGY OF DEPRESSION
Depression is a widespread and often chronic condition. Lifetime prevalence estimates for MDD are approximately 15% to 20%;2,3 1-year prevalence estimates are 5% to 10%;2,4 and point prevalence estimates range from 4% to 7%.3,5 Moreover, MDD is characterized by high rates of relapse: 22% to 50% of patients suffer recurrent episodes within 6 months after recovery.6
Women are twice as likely as men to be diagnosed with MDD, with lifetime prevalence rates of 10% to 25% in women versus 5% to 12% in men.1
Although rates of depression do not appear to increase with age, MDD often goes undertreated in older adults3 and in cardiac patients.7
DIAGNOSING AND ASSESSING DEPRESSION
The gold standard for diagnosing MDD is a clinical interview. Commonly used instruments include the Diagnostic Interview Schedule8 and the Composite International Diagnostic Interview.9 The Structured Clinical Interview for DSM-IV Axis I Disorders10 and the Schedule for Affective Disorders and Schizophrenia11 are frequently used semistructured interviews.
The most common clinical instruments for assessing the severity of depressive symptoms are the Hamilton Rating Scale for Depression (HAM-D),12 which is a clinician-rated scale, and various psychometric questionnaires, including the Beck Depression Inventory (BDI)13,14 and the Center for Epidemiological Studies Depression Scale (CES-D).15
THE DEPRESSION–HEART DISEASE LINK
Depression as a primary risk factor
Depression as a secondary risk factor
Depression is an even stronger risk factor for cardiac events in patients with established CHD. Point estimates range from 14% to as high as 47%, with higher rates in patients with unstable angina and in patients awaiting coronary artery bypass graft (CABG) surgery; an additional 20% of patients exhibit elevated depressive symptoms or minor depression (mDD).19–25
Prospective studies have shown that depression increases the risk for death or nonfatal cardiac events approximately 2.5-fold in patients with CHD. For instance, Frasure-Smith et al followed 896 patients with a recent acute MI and found that the presence of depressive symptoms as indicated by an elevated BDI score was a significant predictor of cardiac mortality after controlling for multivariate predictors of mortality (odds ratio [OR] = 3.29 for women and 3.05 for men).26
Two recent meta-analyses confirmed the association between depression and adverse clinical outcomes in patients with CHD.27,28 For example, van Melle et al reported that post-MI depression was associated with a 2- to 2.5-fold increase in the risk of adverse health outcomes.28 In this analysis, depression’s effect on cardiac mortality and all-cause mortality was especially pronounced in older studies (before 1992) (OR = 3.2) compared with more recent studies (after 1992) (OR = 2.01).28
Duke University researchers have conducted several prospective studies in various cardiac populations.29–31 Barefoot et al assessed 1,250 patients with documented CHD using the Zung Self-Rating Depression Scale at the time of diagnostic coronary angiography and followed them for up to 19.4 years.29 Results showed that patients with moderate to severe depression were at 69% greater risk for cardiac death and 78% greater risk for all-cause death than were their nondepressed counterparts.
We also recently reported results from a prospective study that followed 204 patients with heart failure over a median interval of 3 years.31 Clinically significant symptoms of depression (BDI score ≥ 10) were associated with a hazard ratio of 1.56 (95% CI, 1.07 to 2.29) for the combined end point of death or cardiovascular hospitalization. These observations included adjustment for plasma NT-proBNP level, ejection fraction, and other established risk factors, suggesting that heightened risk of adverse clinical outcomes associated with depressive symptoms is not simply a reflection of the severity of heart failure.
In summary, a number of observational studies have demonstrated that depression is associated with increased risk of morbidity and mortality both in healthy populations and in a variety of populations with established cardiac disease.
BIOBEHAVIORAL MECHANISMS LINKING DEPRESSION AND CHD
A number of biobehavioral mechanisms have been hypothesized to underlie the relationship between depression and CHD. Most evidence is derived from cross-sectional studies and suggests that depression is associated with traditional risk factors for CHD, such as hypertension, diabetes, and insulin resistance,32,33 as well as changes in platelet reactivity,34 dysregulation of the autonomic nervous system35 and hypothalamic-pituitary-adrenal axis,36 and alterations in the immune response/inflammation.37 Depression is also associated with behavioral factors that are in turn associated with CHD risk, such as reduced treatment adherence,38 smoking,39 and physical inactivity.40
STUDIES OF DEPRESSION TREATMENT IN CARDIAC PATIENTS
Successful treatments for depression in patients with CHD may have the potential to improve not only quality of life but also cardiovascular and physical health. Several treatments for depression exist for use in the general population, such as antidepressant medication or psychotherapy.41 However, only three studies have tested the efficacy of these treatments in patients with CHD: SADHART, ENRICHD, and CREATE.42–44
SADHART (Sertraline Antidepressant Heart Attack Randomized Trial) was a safety and efficacy evaluation of antidepressant medication in patients with MDD and a recent MI or unstable angina.42 It showed only modest differences in reductions in depressive symptoms between sertraline recipients and placebo recipients, and it lacked statistical power to examine the impact of treatment on hard clinical end points.
ENRICHD (Enhancing Recovery in Coronary Heart Disease Patients) assessed the effect of psychosocial treatment on survival among more than than 2,400 post-MI patients.43 Although this trial found that cognitive behavior therapy resulted in significant, albeit small, improvements in depressive symptoms compared with usual care, it failed to demonstrate that treating depression and low social support was associated with increased survival.
CREATE (Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy), a recent placebo-controlled trial, assessed the value of antidepressant medication and clinical management in patients with CHD.44 The study’s 284 patients, all of whom had CHD as well as MDD and a HAM-D score of 20 or greater, underwent two separate randomizations: (1) to 12 weeks of interpersonal therapy plus clinical management or 12 weeks of clinical management alone, and (2) to 12 weeks of citalopram therapy or matching placebo. There was no difference between interpersonal therapy and clinical management alone; however, citalopram was superior to placebo in reducing HAM-D scores and demonstrated better remission rates (35.9% with citalopram vs 22.5% with placebo). The same therapists who provided interpersonal therapy also performed the clinical management, so it could be argued that this was why additional interpersonal therapist time did not result in greater reductions in depressive symptoms than did clinical management alone. Furthermore, this study did not examine the effects of depression therapy on clinical outcomes.
EXERCISE AS A TREATMENT FOR DEPRESSION
There is growing evidence that exercise may be an effective treatment for depression.45 Most of the existing studies of exercise for depression have focused on aerobic exercise.
In the relatively large SMILE study (Standard Medical Intervention and Long-term Exercise),46 conducted at Duke University, 156 adult noncardiac patients with MDD were randomized to 4 months of treatment with supervised aerobic exercise, antidepressant medication (sertraline), or a combination of exercise and medication. Although antidepressant medication was associated with faster reductions in depression in the first 4 weeks of treatment among mildly depressed patients, exercise was as effective as antidepressant medication in treating depression by the end of the 16-week intervention for all participants.
Exercise generally is considered safe for most patients with stable CHD.48 Some studies of exercise treatments for patients with CHD have tracked depressive symptoms and thus have provided insight into the potential efficacy of exercise as a treatment for depression in this population. Although most of these studies have reported significant improvements in depression after completion of an exercise program, many have had important methodologic limitations, including absence of a control group. In one of the few controlled studies in this area, Stern et al49 randomized 106 men who had a recent acute MI and elevated depression, anxiety, or low fitness to 12 weeks of exercise training, group therapy, or usual care (control). At 1-year follow-up, subjects in both the exercise and counseling groups showed improvements in depression relative to controls.
EFFECT OF EXERCISE ON CARDIOVASCULAR RISK FACTORS AND OUTCOMES
Exercise is a particularly promising intervention for depression in patients with CHD because it has well-documented cardiovascular benefits. In addition to the well-established role of exercise interventions in primary prevention, such interventions have been shown to improve outcomes for patients with CHD.50
Jolliffe et al conducted a meta-analysis comparing exercise-only interventions, comprehensive rehabilitation (including educational and behavioral components such as dietary changes and stress reduction in addition to exercise), and usual care.51 Exercise-only interventions were associated with reductions in both all-cause and cardiac mortality relative to usual care. Comprehensive rehabilitation, on the other hand, was not associated with statistically significant reductions in all-cause mortality relative to usual care, but it was associated with a decreased risk for cardiac mortality, to a slightly lesser extent than exercise-only interventions.
The evidence that exercise affects depression, CHD risk factors, and CHD outcomes suggests that exercise is a particularly promising intervention for depression in this population.
UPBEAT trial promises further insight
A new Duke University study known as UPBEAT (Understanding Prognostic Benefits of Exercise and Antidepressant Treatment) is randomizing 200 patients with elevated depressive symptoms to exercise, antidepressant therapy (sertraline), or placebo for 4 months.53 A variety of “biomarkers” of risk are being assessed, including measures of heart rate variability, vascular function, inflammation, and platelet aggregation. Results of this 5-year trial should be available by 2011.
CONCLUSIONS
Although depression has emerged as an important risk factor for CHD, there is no consensus on the optimal way to treat depression in patients with CHD. Interventions that are guided by an understanding of the mechanisms linking depression to CHD may prove to be most effective in improving both depression and physical health outcomes.
Exercise targets many of the mechanisms by which depression may be associated with increased risk, including autonomic nervous system activity, hypothalamic-pituitary-adrenal axis function, platelet activation, vascular function, and inflammation. Moreover, a growing body of evidence suggests that exercise is an effective treatment for depression that may be comparable in effect to antidepressant medication, at least in select subgroups (eg, patients who are receptive to exercise as a treatment for depression). The value of exercise training—not only for improving quality of life, but also for improving “biomarkers” of risk and other relevant health outcomes—is the focus of our current research efforts.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Text Revision. 4th ed. Washington, DC: American Psychiatric Association; 2000.
- Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8–19.
- Steffens DC, Skoog I, Norton MC, et al. Prevalence of depression and its treatment in an elderly population: the Cache County study. Arch Gen Psychiatry 2000; 57:601–617.
- Regier DA, Narrow WE, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Ayuso-Mateos JL, Vazquez-Barquero JL, Dowrick C, et al. Depressive disorders in Europe: prevalence figures from the ODIN study. Br J Psychiatry 2001; 179:308–316.
- Belsher G, Costello CG. Relapse after recovery from unipolar depression: a critical review. Psychol Bull 1988; 104:84–96.
- Carney RM, Rich MW, Tevelde A, Saini J, Clark K, Jaffe AS. Major depressive disorder in coronary artery disease. Am J Cardiol 1987; 60:1273–1275.
- Robins LN, Helzer JE, Crougham J, Ratliff K. National Institute of Mental Health diagnostic interview schedule. Arch Gen Psychiatry 1981; 38:381–389.
- World Health Organization. Composite International Diagnostic Interview. Geneva, Switzerland: World Health Organization; 1990.
- First M, Spitzer L, Gibbon M. Structured clinical interview for axis I DSM-IV disorders. Washington, DC: American Psychiatric Press; 1995.
- Endicott J, Spitzer RL. The schedule for affective disorders and schizophrenia. Arch Gen Psychiatry 1978; 35:837–844.
- Hamilton M. A rating scale for depression. J Neurol 1960; 23:56–61.
- Beck AT, Ward CH, Mendelsohn M. An inventory for measuring depression. Arch Gen Psychiatry 1961; 4:561–571.
- Beck AT, Steer RA, Brown GK. Beck Depression Inventory Manual. 2nd ed. San Antonio, TX: The Psychological Corporation; 1996.
- Hautzinger M. The CES-D scale: a depression-rating scale for research in the general population. Diagnostica 1988; 34:167–173.
- Lett H, Blumenthal J, Babyak M, Sherwood A, Strauman T, Robins C. Depression as a risk factor for coronary artery disease: evidence, mechanisms, and treatment. Psychosom Med 2004; 66:305–315.
- Rugulies R. Depression as a predictor for coronary heart disease. A review and meta-analysis. Am J Prev Med 2002; 23:51–61.
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol 2005; 45:637–651.
- Carney RM, Rich MW, Freedland KE, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988; 50:627–633.
- Schleifer SJ, Macari-Hinson MM, Coyle DA, et al. The nature and course of depression following myocardial infarction. Arch Intern Med 1989; 149:1785–1789.
- Frasure-Smith N, Lesperance F, Talajic M. Depression following myocardial infarction. Impact on 6-month survival. JAMA 1993; 270:1819–1825.
- Lesperance F, Frasure-Smith N, Juneau M, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000; 160:1354–1360.
- Connerney I, Shapiro PA, McLaughlin JS, Bagiella E, Sloan RP. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001; 358:1766–1771.
- Jiang W, Alexander J, Christopher E, et al. Relationship of depression to increased risk of mortality and rehospitalization in patients with congestive heart failure. Arch Intern Med 2001; 161:1849–1856.
- Burker EJ, Blumenthal JA, Feldman M, et al. Depression in male and female patients undergoing cardiac surgery. Br J Clin Psychol 1995; 34:119–128.
- Frasure-Smith N, Lesperance F, Juneau M, Talajic M, Bourassa MG. Gender, depression, and one-year prognosis after myocardial infarction. Psychosom Med 1999; 61:26–37.
- Barth J, Schumacher M, Hermann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med 2004; 66:802–813.
- van Melle JP, de Jong P, Spijkerman TA, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis. Psychosom Med 2004; 66:814–822.
- Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol 1996; 78:613–617.
- Blumenthal JA, Lett H, Babyak M, et al. Depression as a risk factor for mortality after coronary artery bypass surgery. Lancet 2003; 362:604–609.
- Sherwood A, Blumenthal JA, Trivedi R, et al. Relationship of depression to mortality and hospitalization in patients with heart failure. Arch Intern Med 2007; 167:367–373.
- Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2001; 24:1069–1078.
- Thakore JH, Richards PJ, Reznek RH, Martin A, Dinan TG. Increased intra-abdominal fat deposition in patients with major depressive illness as measured by computed tomography. Biol Psychiatry 1997; 41:1140–1142.
- Musselman DL, Tomer A, Manatunga AK, et al. Exaggerated platelet reactivity in major depression. Am J Psychiatry 1996; 153:1313–1317.
- Delgado PL, Moreno FA. Role of norepinephrine in depression. J Clin Psychiatry 2000; 61:5–12.
- Akil H, Haskett RF, Young EA, et al. Multiple HPA profiles in endogenous depression: effect of age and sex on cortisol and beta-endorphin. Biol Psychiatry 1993; 33:73–85.
- Kop WJ, Gottdiener JS, Tangen CM, et al. Inflammation and coagulation factors in persons > 65 years of age with symptoms of depression but without evidence of myocardial ischemia. Am J Cardiol 2002; 89:419–424.
- Carney RM, Freedland KE, Eisen SA, Rich MW, Jaffe AS. Major depression and medication adherence in elderly patients with coronary artery disease. Health Psychol 1995; 14:88–90.
- Lehto S, Koukkunen H, Hintikka J, Viinamaki H, Laakso M, Pyorala K. Depression after coronary heart disease events. Scand Cardiovasc J 2000; 34:580–583.
- Camacho TC, Roberts RE, Lazarus NB, Kaplan GA, Cohen RD. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol 1991; 134:220–231.
- Depression Guideline Panel. Depression in Primary Care: Volume 2. Treatment of Depression, Clinical Practice Guideline, No. 5. Rockville, MD: Agency for Health Care Policy and Research, Public Health Service, US Dept of Health and Human Services; 1993.
- Glassman AH, O’Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002; 288:701–709.
- Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 2003; 289:3106–3116.
- Lesperance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA 2007; 297:367–379.
- Brosse AL, Sheets ES, Lett HS, Blumenthal JA. Exercise and the treatment of clinical depression in adults: recent findings and future directions. Sports Med 2002; 32:741–760.
- Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med 1999; 159:2349–2356.
- Babyak M, Blumenthal JA, Herman S, et al. Exercise treatment for major depression: maintenance of therapeutic benefit at 10 months. Psychosom Med 2000; 62:633–638.
- Franklin BA, Bonzheim K, Gordon S, Timmis GC. Safety of medically supervised outpatient cardiac rehabilitation exercise therapy: a 16-year follow-up. Chest 1998; 114:902–906.
- Stern MJ, Gorman PA, Kaslow L. The group counseling v exercise therapy study. A controlled intervention with subjects following myocardial infarction. Arch Intern Med 1983; 143:1719–1725.
- Oldridge NB, Guyatt GH, Fischer ME, Rimm AA. Cardiac rehabilitation after myocardial infarction. Combined experience of randomized clinical trials. JAMA 1988; 260:945–950.
- Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2001; (1):CD001800.
- Blumenthal JA, Babyak MA, Carney RM, et al. Exercise, depression, and mortality after myocardial infarction in the ENRICHD trial. Med Sci Sports Exerc 2004; 36:746–755.
- Blumenthal JA, Sherwood A, Rogers SD, et al. Understanding prognostic benefits of exercise and antidepressant therapy for persons with depression and heart disease: the UPBEAT study—rationale, design, and methodological issues. Clin Trials 2007; 4:548–559.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Text Revision. 4th ed. Washington, DC: American Psychiatric Association; 2000.
- Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry 1994; 51:8–19.
- Steffens DC, Skoog I, Norton MC, et al. Prevalence of depression and its treatment in an elderly population: the Cache County study. Arch Gen Psychiatry 2000; 57:601–617.
- Regier DA, Narrow WE, Rae DS, Manderscheid RW, Locke BZ, Goodwin FK. The de facto US mental and addictive disorders service system. Epidemiologic catchment area prospective 1-year prevalence rates of disorders and services. Arch Gen Psychiatry 1993; 50:85–94.
- Ayuso-Mateos JL, Vazquez-Barquero JL, Dowrick C, et al. Depressive disorders in Europe: prevalence figures from the ODIN study. Br J Psychiatry 2001; 179:308–316.
- Belsher G, Costello CG. Relapse after recovery from unipolar depression: a critical review. Psychol Bull 1988; 104:84–96.
- Carney RM, Rich MW, Tevelde A, Saini J, Clark K, Jaffe AS. Major depressive disorder in coronary artery disease. Am J Cardiol 1987; 60:1273–1275.
- Robins LN, Helzer JE, Crougham J, Ratliff K. National Institute of Mental Health diagnostic interview schedule. Arch Gen Psychiatry 1981; 38:381–389.
- World Health Organization. Composite International Diagnostic Interview. Geneva, Switzerland: World Health Organization; 1990.
- First M, Spitzer L, Gibbon M. Structured clinical interview for axis I DSM-IV disorders. Washington, DC: American Psychiatric Press; 1995.
- Endicott J, Spitzer RL. The schedule for affective disorders and schizophrenia. Arch Gen Psychiatry 1978; 35:837–844.
- Hamilton M. A rating scale for depression. J Neurol 1960; 23:56–61.
- Beck AT, Ward CH, Mendelsohn M. An inventory for measuring depression. Arch Gen Psychiatry 1961; 4:561–571.
- Beck AT, Steer RA, Brown GK. Beck Depression Inventory Manual. 2nd ed. San Antonio, TX: The Psychological Corporation; 1996.
- Hautzinger M. The CES-D scale: a depression-rating scale for research in the general population. Diagnostica 1988; 34:167–173.
- Lett H, Blumenthal J, Babyak M, Sherwood A, Strauman T, Robins C. Depression as a risk factor for coronary artery disease: evidence, mechanisms, and treatment. Psychosom Med 2004; 66:305–315.
- Rugulies R. Depression as a predictor for coronary heart disease. A review and meta-analysis. Am J Prev Med 2002; 23:51–61.
- Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: the emerging field of behavioral cardiology. J Am Coll Cardiol 2005; 45:637–651.
- Carney RM, Rich MW, Freedland KE, et al. Major depressive disorder predicts cardiac events in patients with coronary artery disease. Psychosom Med 1988; 50:627–633.
- Schleifer SJ, Macari-Hinson MM, Coyle DA, et al. The nature and course of depression following myocardial infarction. Arch Intern Med 1989; 149:1785–1789.
- Frasure-Smith N, Lesperance F, Talajic M. Depression following myocardial infarction. Impact on 6-month survival. JAMA 1993; 270:1819–1825.
- Lesperance F, Frasure-Smith N, Juneau M, Theroux P. Depression and 1-year prognosis in unstable angina. Arch Intern Med 2000; 160:1354–1360.
- Connerney I, Shapiro PA, McLaughlin JS, Bagiella E, Sloan RP. Relation between depression after coronary artery bypass surgery and 12-month outcome: a prospective study. Lancet 2001; 358:1766–1771.
- Jiang W, Alexander J, Christopher E, et al. Relationship of depression to increased risk of mortality and rehospitalization in patients with congestive heart failure. Arch Intern Med 2001; 161:1849–1856.
- Burker EJ, Blumenthal JA, Feldman M, et al. Depression in male and female patients undergoing cardiac surgery. Br J Clin Psychol 1995; 34:119–128.
- Frasure-Smith N, Lesperance F, Juneau M, Talajic M, Bourassa MG. Gender, depression, and one-year prognosis after myocardial infarction. Psychosom Med 1999; 61:26–37.
- Barth J, Schumacher M, Hermann-Lingen C. Depression as a risk factor for mortality in patients with coronary heart disease: a meta-analysis. Psychosom Med 2004; 66:802–813.
- van Melle JP, de Jong P, Spijkerman TA, et al. Prognostic association of depression following myocardial infarction with mortality and cardiovascular events: a meta-analysis. Psychosom Med 2004; 66:814–822.
- Barefoot JC, Helms MJ, Mark DB, et al. Depression and long-term mortality risk in patients with coronary artery disease. Am J Cardiol 1996; 78:613–617.
- Blumenthal JA, Lett H, Babyak M, et al. Depression as a risk factor for mortality after coronary artery bypass surgery. Lancet 2003; 362:604–609.
- Sherwood A, Blumenthal JA, Trivedi R, et al. Relationship of depression to mortality and hospitalization in patients with heart failure. Arch Intern Med 2007; 167:367–373.
- Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 2001; 24:1069–1078.
- Thakore JH, Richards PJ, Reznek RH, Martin A, Dinan TG. Increased intra-abdominal fat deposition in patients with major depressive illness as measured by computed tomography. Biol Psychiatry 1997; 41:1140–1142.
- Musselman DL, Tomer A, Manatunga AK, et al. Exaggerated platelet reactivity in major depression. Am J Psychiatry 1996; 153:1313–1317.
- Delgado PL, Moreno FA. Role of norepinephrine in depression. J Clin Psychiatry 2000; 61:5–12.
- Akil H, Haskett RF, Young EA, et al. Multiple HPA profiles in endogenous depression: effect of age and sex on cortisol and beta-endorphin. Biol Psychiatry 1993; 33:73–85.
- Kop WJ, Gottdiener JS, Tangen CM, et al. Inflammation and coagulation factors in persons > 65 years of age with symptoms of depression but without evidence of myocardial ischemia. Am J Cardiol 2002; 89:419–424.
- Carney RM, Freedland KE, Eisen SA, Rich MW, Jaffe AS. Major depression and medication adherence in elderly patients with coronary artery disease. Health Psychol 1995; 14:88–90.
- Lehto S, Koukkunen H, Hintikka J, Viinamaki H, Laakso M, Pyorala K. Depression after coronary heart disease events. Scand Cardiovasc J 2000; 34:580–583.
- Camacho TC, Roberts RE, Lazarus NB, Kaplan GA, Cohen RD. Physical activity and depression: evidence from the Alameda County Study. Am J Epidemiol 1991; 134:220–231.
- Depression Guideline Panel. Depression in Primary Care: Volume 2. Treatment of Depression, Clinical Practice Guideline, No. 5. Rockville, MD: Agency for Health Care Policy and Research, Public Health Service, US Dept of Health and Human Services; 1993.
- Glassman AH, O’Connor CM, Califf RM, et al. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA 2002; 288:701–709.
- Berkman LF, Blumenthal J, Burg M, et al. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) randomized trial. JAMA 2003; 289:3106–3116.
- Lesperance F, Frasure-Smith N, Koszycki D, et al. Effects of citalopram and interpersonal psychotherapy on depression in patients with coronary artery disease: the Canadian Cardiac Randomized Evaluation of Antidepressant and Psychotherapy Efficacy (CREATE) trial. JAMA 2007; 297:367–379.
- Brosse AL, Sheets ES, Lett HS, Blumenthal JA. Exercise and the treatment of clinical depression in adults: recent findings and future directions. Sports Med 2002; 32:741–760.
- Blumenthal JA, Babyak MA, Moore KA, et al. Effects of exercise training on older patients with major depression. Arch Intern Med 1999; 159:2349–2356.
- Babyak M, Blumenthal JA, Herman S, et al. Exercise treatment for major depression: maintenance of therapeutic benefit at 10 months. Psychosom Med 2000; 62:633–638.
- Franklin BA, Bonzheim K, Gordon S, Timmis GC. Safety of medically supervised outpatient cardiac rehabilitation exercise therapy: a 16-year follow-up. Chest 1998; 114:902–906.
- Stern MJ, Gorman PA, Kaslow L. The group counseling v exercise therapy study. A controlled intervention with subjects following myocardial infarction. Arch Intern Med 1983; 143:1719–1725.
- Oldridge NB, Guyatt GH, Fischer ME, Rimm AA. Cardiac rehabilitation after myocardial infarction. Combined experience of randomized clinical trials. JAMA 1988; 260:945–950.
- Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev 2001; (1):CD001800.
- Blumenthal JA, Babyak MA, Carney RM, et al. Exercise, depression, and mortality after myocardial infarction in the ENRICHD trial. Med Sci Sports Exerc 2004; 36:746–755.
- Blumenthal JA, Sherwood A, Rogers SD, et al. Understanding prognostic benefits of exercise and antidepressant therapy for persons with depression and heart disease: the UPBEAT study—rationale, design, and methodological issues. Clin Trials 2007; 4:548–559.