User login
- While continuing to improve recognition of migraine in your patient population, pay particular attention to the adherence rate among those for whom you have prescribed a triptan.
- Ask patients who discontinue triptan therapy why they made that decision. Besides adverse effects from the agent, reasons may include medication cost, influence of comorbidities, or triptan interaction with medications you may not have known about.
Despite more than 5 million consultations annually, relatively little is known about the treatment of migraine in primary care. Much of the literature is projected from population surveys or reports concerning patients referred for specialist care or those entering treatment studies.
Our study is the largest reported to gather data directly from patients treated for migraine in family practice. The participating practices represent a spectrum of communities and practice types. As minimal differences exist in practice patterns between family physicians who participate in research networks and all family physicians1, these findings may more accurately reflect the current status in family practice than other studies.
We believe that this study indicates family physicians offer triptans to most patients consulting specifically for migraine and that adherence issues contribute significantly to the perceived low rates of use of these medications in primary care. In recent years, considerable effort has gone into increasing the diagnosis of migraine and promoting the more extensive use of triptans in primary care patients (see article on page 1038 in this issue). Family physicians must certainly continue to improve the recognition of migraine; but attention to patient concerns about triptans and efforts to enhance adherence and appropriate use of these medications is obviously essential. We must continue efforts to better understand why some 30% or more of migraine patients in primary care practice discontinue a therapy that has been found to be highly effective and well accepted by patients in clinical studies.
Migraine-specific prescribing in primary care is better than commonly reported
Between 1990 and 1998, the number of physician office visits for migraine doubled to more than 5 million per year.2 Of the more than 28 million US adults with migraine, approximately 70% of women and 50% of men are now believed to have consulted a physician at least once,3 and two thirds of these patients have made 5 or more physician visits for migraine.4 More than 72% of migraine-related physician visits are to primary care physicians, the most to family physicians.1
Nevertheless, the headache literature routinely describes migraine as “undertreated” in primary care.5-7 In particular, primary care physicians are perceived to under-prescribe triptans,7-11 the most effective migraine-specific medications available, widely regarded as “the gold standard” for acute migraine therapy of all but mild attacks.12-16 Population surveys estimate that only some 13% to 20% of migraine sufferers have been prescribed triptans.4,5,9,17 A 1995 study of migraine patients enrolled in a health maintenance organization reported that 11.4% used subcutaneous sumatriptan; however, oral triptans were not included in the study.18 Ten years later, another study of health plan enrollees estimated that only 11% of those meeting strict criteria for migraine were prescribed triptans or ergots.7
These low percentages do not correlate with our experience of primary care practice nor with data indicating substantial sales of triptans in the US.19 As we have not identified any studies that directly address prescribing by primary care physicians for migraine, we conducted a survey of patients who consulted family physicians for migraine during 2002.
Some of the differences between our findings and those based on prescription data could be attributed to the use of samples (reported to be particularly common in migraine treatment during this period), or difficulties in patient recall of medications.
Diagnosis of migraine not always coded. A more significant source of difference between our findings and those of population-based surveys is in the diagnosis of migraine. Most surveys use patient-reported symptoms for diagnosis, and hence the population of migraine sufferers includes those who have not had a physician visit coded for migraine. Our interest is in the primary care consultation specifically for migraine.
If a physician concludes a patient has migraine, this diagnosis is highly likely to be correct,20 and our findings indicate that a migraine-specific medication is commonly offered. We strongly support ongoing efforts to improve the recognition of migraine by all physicians and emphasize that our results are based only on patients identified by migraine-coded primary care visits.
Why do patients discontinue triptans?
The finding that about one third of patients discontinued triptan use may be surprising in view of the widely reported efficacy16 and tolerability24 of these medications, but this is almost identical to the results of a study of 663 patients of a US headache clinic.25 Significant rates of triptan discontinuation have been reported by other studies.
A study based on British general practice pharmacy records reported 55% of patients not renewing a triptan prescription during 1 year of follow-up,26 and an older study of patients attending a Dutch neurology clinic found that 25% of sumatriptan users discontinued this drug over a 2-year period.27 One US primary care treatment study found that on enrollment, 62% of 143 migraine patients had previously used triptans or ergotamines but had discontinued therapy.28
As in our study, the principal stated reason for discontinuation in the Dutch study27 was lack of efficacy. Conversely, in the US primary care study only 13% of patients gave lack of efficacy as the principal reason for discontinuation but 20% cited cost and 55% cited nonprescribing by physicians.28
As shown in the TABLE, the most striking differences between patients who discontinued triptans and those who continued were in patient satisfaction with treatment and current use of narcotic medication for migraine, but the higher grades of MIDAS scores (FIGURE) were also significantly more common in the patients who discontinued.
This study was not designed to assess if these factors caused or resulted from triptan discontinuation, but the association of triptan “failure” with 3 other significant negative factors could indicate subgroups of patients with especially high morbidity from migraine or risk of poor response to migraine-specific treatment. Future studies are needed to better characterize patients who discontinue, especially to examine the roles of comorbidities, total medication use, and the role of subspecialty referral.
TABLE
Differences between patients who discontinued triptans and those who continued
| DISCONTINUERS | CONTINUERS | P VALUE | |
|---|---|---|---|
| Disability (MIDAS score) | |||
| Grade I or II | 34 | 98 | .034 |
| Grade III or IV | 86 | 145 | |
| Medication coverage* | |||
| All or some | 106 | 216 | .904 |
| None | 14 | 28 | |
| Patient satisfaction | |||
| Satisfied | 71 | 201 | <.001 |
| Dissatisfied | 49 | 44 | |
| Gender | |||
| Female | 103 | 216 | .39 |
| Male | 18 | 27 | |
| Current narcotic use | |||
| Use | 57 | 54 | <.001 |
| No use | 64 | 191 | |
| * Payment by health insurance for migraine medications | |||
| Sample size calculated for alpha=0.05 and power=1–beta=0.80. | |||
Limitations of this study
This study has several weaknesses, mainly the low response rate and potential biases in patient selection and participation. A headache survey mailed to 200 randomly selected patients in a single British general practice reported a response rate of 61%29and the American Migraine II Survey reported response rates of 59% to 69% of households.4 Considerations of patient confidentiality, cost, and burdening busy practices limited our ability to use many of the strategies recommended to increase response rate.30 The highest response rates were from those smaller practices where the office staff expressed most interest in the study.
Although ICD coding has shortcomings as a technique of identifying a study population, it is reported to be very accurate for specific conditions such as migraine and for patients with insurance.31,32 We did not include questions to verify that patients met International Headache Society (IHS) criteria for migraine33 because of concerns about the length of the survey and because a positive diagnosis of migraine by a family physician is reported to be likely accurate 98% of the time.20 Examining how the accuracy of diagnosis and the various subtypes of migraine impact treatment would be interesting additions to a future study.
For this study, we used 10 community practices—5 rural and 5 urban, and all associated with the Kansas Practice Research Network—to conduct an observational, cross-sectional study of adult patients who consulted family physicians because of migraine during 2002. The 5 rural practices served communities ranging from 835 to 6313 in population and were selected to represent the different geographic regions of the state. Similarly, the 5 urban practices represented different demographic areas within the city of Wichita (population 344,284).
Patients were identified by use of migraine-specific ICD-9 codes (all subgroups of ICD 9-346) for the consultation. The only exclusion was of patients aged less than 18 years. The 15-item written survey (FIGURE W1) gathered demographic data and incorporated the standardized Migraine Disability Assessment Score (MIDAS) questionnaire (FIGURE),21,22 as well as questions about migraine experience, medications, and satisfaction with treatment.
The MIDAS questionnaire is a simple 5-item written instrument (FIGURE) developed from more complex measures of headache and morbidity specifically to assess impact on daily activities. Its validity, reliability, and ease of use have been confirmed in population studies and busy clinical settings.21-23 The survey asked patients to name all medications (prescription, nonprescription, or other, including herbal remedies) usually used for migraine. In addition, a specific question addressed current or previous use of the triptans available at the time of the study—ie, naratriptan (Amerge), sumatriptan (Imitrex—injection, oral, or nasal spray), rizatriptan (Maxalt), zolmitriptan (Zomig), almotriptan (Axert), and frovatriptan (Frova). This question used both generic and trade names for the medication. Patients who reported previous but not current use of any triptan were asked to describe their reasons for discontinuation in their own words.
Patients received the survey by mail, along with a cover letter from their personal physicians inviting them to participate in the study and instructions to return the anonymous survey directly to the primary investigator. Patients were assured that neither their personal physicians nor the researchers could identify participants and that their ongoing medical care would not be altered in any way by their participation in the survey or by the information provided. The study was approved by the University of Kansas School of Medicine Institutional Review Board.
Data were entered into a Microsoft Access 2000 file and 2 data entry personnel performed data editing to verify each entry. Data were analyzed using Microsoft Excel. Analysis was completed using the statistical program SPSS for Windows V.11.0 (SPSS Inc, Chicago, Ill). The principal modes of data analysis included chi-square, Kruskal-Wallis, independent samples t-tests, and analysis of variance (ANOVA). A probability value of less than 0.05 was considered statistically significant.
Results
The 10 participating practices identified 992 patients aged 18 or older who consulted at least once during 2002 primarily for a migraine-related diagnosis. After 3 mailings, 447 surveys suitable for analysis were returned (a response rate of 45%). For individual practices, the number of patients surveyed ranged from 9 to 540, and the response rates were from27.5% to 72%. Responders did not differ from nonresponders in age or gender distribution.
The respondents were predominantly female (83%) with a mean age of 44 years (range, 18–82). Two thirds of the respondents had experienced migraine for more than 10 years, and most reported that migraine significantly impacted their lives. Sixty percent of patients scored 10 or more on the MIDAS scale, indicating moderate-severe migraine-related disability.
Most respondents (85.5%) had private insurance. Only 14% reported having no assistance with payment for migraine medications, and 58% reported that “all” or “most” of their migraine medications were paid by insurance plans. Seventy-three percent of respondents were “satisfied” or “very satisfied” with medical treatment for migraine and only 5% “very dissatisfied.”
Participants reported using a wide range of prescription and nonprescription medications. Overall, 366 (82%) patients reported experience with triptans. Of these patients, 206 (56%) had used more than 1 triptan. Current triptan use was reported by 245 (55%) of all respondents. Among the 121 patients who reported discontinuation of triptans, the most common reason provided was lack of efficacy (57%), followed by adverse effects (24%).
Statistically significant differences were found between patients who continued triptan therapy and those who discontinued in migraine disability (MIDAS scores), satisfaction with migraine treatment, and reported use of narcotic medication for migraine (TABLE). Patients who discontinued triptan therapy did not differ significantly from those who continued in age, gender, number of years with migraine, insurance type, use of prophylactic migraine medication or reported use of analgesics, combination medications, ergots, “other,” or “no” medications to treat migraine attacks.
Although surveys were returned directly to the researchers without identifying information and patients were assured that information would not be shared with participating physicians, the study design could have inhibited negative comments about medical care. Conversely, patients who were angry, upset, or disappointed about migraine care could have been motivated to complete the survey.34 Migraine patients who consult physicians are reported to have more severe migraine, more comorbidities, decreased quality of life, and to consult significantly more frequently for multiple medical conditions than other patients.35,36
FIGURE
The MIDAS questionnaire is valid, reliable, and easy to use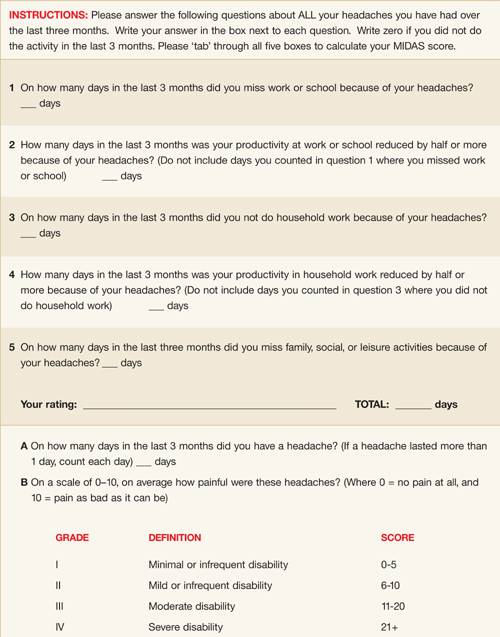
Acknowledgments
The authors acknowledge substantial assistance from Nolem Llong, Terry Ast, Nicole Rogers, and Mary Hursey in the conduct of the study and preparation of this manuscript and the assistance of the physicians of the Kansas Practice Research Network. The study was funded in part by the AAFP Practice Based Research Network Research Stimulation Grant.
CORRESPONDENCE
Anne Walling MB, ChB, FFPHM, University of Kansas School of Medicine–Wichita, Department of Family and Community Medicine, 1010 North Kansas, Wichita, KS 67214. E-mail: [email protected]
1. Nutting PA, Baier M, Werner JJ, Cutter G, Reed FM, Orzano AJ. Practice patterns of family physicians in practice-based research networks: a report from ASPN. J Am Board Fam Pract 1999;12:278-284.
2. Gibbs TS, Fleischer AB, Feldman SR, Sam MC, O’Donovan CA. Health care utilization in patients with migraine: demographics and patterns of care in the ambulatory setting. Headache 2003;43:330-335.
3. Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American migraine study II. Headache 2001;41:646-657.
4. Lipton RB, Scher AI, Kolodner K, Liberman J, Steiner TJ, Stewart WF. Migraine in the United States: Epidemiology and patterns of health care use. Neurology 2002;58:885-894.
5. Lipton RB, Diamond S, Reed M, Diamond M, Stewart WF. Migraine diagnosis and treatment: results from the American Migraine Study II. Headache 2001;41:638-645.
6. Maizels M. Model interventions to improve headache outcomes in health care systems. In Reducing the Burden of Headache, Olesen J, Steiner TJ, Lipton RB (eds). New York: Oxford University Press; 2003:290-301.
7. Bigal ME, Kolodner KB, Lafata JE, Leotta C, Lipton RB. Patterns of medical diagnosis and treatment of migraine and probable migraine in a health plan. Cephalalgia 2006;26:43-49.
8. Cady R, Dodrick DW. Diagnosis and treatment of migraine. Mayo Clin Proc 2002;77:255-261.
9. Lipton RB, Scher AI, Steiner TJ, et al. Patterns of health care utilization for migraine in England and in the United States Neurology 2003;60:441-448.
10. Loder EW, Lipton RB. Conclusion: how primary care physicians can help their patients with migraine. Am J Med 2005;118:45S-46S.
11. Loder EW, Sheftell F. The quality of headache treatment in the United States: review and analysis of recent data. Headache 2005;45:939-946.
12. Snow V, Weiss K, Wall EM, Mottur-Pilson C. Pharmacologic management of acute attacks of migraine and prevention of migraine headache. Ann Intern Med 2002;137:840-849.
13. Lipton RB, Cutrer FM, Goadsby PJ, et al. How treatment priorities influence triptan p in clinical practice: perspectives of migraine sufferers, neurologists, and primary care physicians. Curr Med Res Opin 2005;21:413-424.
14. Gallagher RM, Cutrer FM. Migraine: diagnosis, management, and new treatment options. Am J Man Care 2002;8:S58-S73.
15. Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000;55:754-763.
16. Ferrari MD, Roon KI, Lipton RB, Goadsby PJ. Oral triptans (setotonin 5-HT1B/1D agonists) in acute migraine treatment: a meta-analysis of 53 trials. Lancet 2001;358:1668-1675.
17. Lohman JJHM, van der Kuy-de Ree MM. Patterns of specific antimigraine drug use—a study based on the records of 18 community pharmacies. Cephalalgia 2004;25:214-218.
18. Von Korff M, Black LK, Saunders K, Galer BS. Headache medication-use among primary care headache patients in a health maintenance organization. Cephalalgia 1999;19:575-580.
19. Available at: www.pozen.com/product/migraine.asppjbpubs.com/script_reports/migraine.htm.
20. Tepper SJ, Dahlof CG, Dowson A, et al. Prevalence and diagnosis of migraine in patients consulting their physician with a complaint of a headache: data from the Landmark Study. Headache 2004;44:856-864.
21. Stewart WF, Lipton RB, Kolodner K, Liberman J, Sawyer J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia 1000;19:107-114.
22. Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment Score in (MIDAS) n comparison to a diary-based measure in a population sample of migraine sufferers. Pain 2000;88:41-52.
23. Andrasik F, Lipchik GL, McCroy DC, Wittrock DA. Outcome measurement in behavioral headache research: headache parameters and psychosocial outcomes. Headache 2005;45:429-437.
24. Welch KMS, Mathew NT, Rosamond W, et al. Tolerability of sumatriptan: clinical trials and post-marketing experience. Cephalalgia 2000;20:687-695.
25. Robbins L. Triptans versus analgesics. Headache 2002;42:903-907.
26. Savini N, Martin A, Browning D. Switching patients with migraine from sumatriptan to other triptans increases primary care costs. Int J Clin Prac 2004;58:758-763.
27. Visser WH, de Vriend RHM, Jaspers NMWH, Ferrari MD. Sumatriptan in clinical practice: a 2-year review of 453 migraine patients. Neurology 1996;47:46-51.
28. Powers C, Szeto S, Pangtay D, Bort T, Cervi M, Cady R. Evaluation of migraineurs’ p for naratriptan over conventional first-line agents. Arch Fam Med 2000;9:753-757.
29. Boardman HF. Headaches in primary care: a pilot study. Cephalalgia 2000;20:364.-
30. Edwards P, Roberts I, Clarke M, et al. Increasing response rates to postal questionnaires: systematic review. BMJ 2002;324:1183-1193.
31. Chao J, Gillanders WG, Flocke SA, et al. Billing for physician services: a comparison of actual billing with CPT codes assigned by direct observation. J Fam Pract 1998;47:28-32.
32. Stange KC, Zyzanski SJ, Smith TF, et al. How valid are medical records and patient questionnaires for physician profiling and health services research? A comparison of direct observation of patients visits. Med Care 1998;36:851-857.
33. Headache Classification Subcommittee of the International Headache Society The international classification of headache disorders 2nd ed. Cephalalgia 2004;24:S1-S150.
34. Scott A, Smith RD. Keeping the customer satisfied: issues in the interpretation and use of patient satisfaction surveys. Int J Qual Health Care 1994;6:353-359.
35. Linet MS, Celentano DC, Stewart WF. Headache characteristics associated with physician consultation: a population-based survey. Am J Prevent Med 1991;7:40-46.
36. Lafata JE, Moon C, Leotta C, Kolodner K, Poisson L, Lipton RB. The medical care utilization and costs associated with migraine headache. J Gen Intern Med 2004;19:1005-1012.
- While continuing to improve recognition of migraine in your patient population, pay particular attention to the adherence rate among those for whom you have prescribed a triptan.
- Ask patients who discontinue triptan therapy why they made that decision. Besides adverse effects from the agent, reasons may include medication cost, influence of comorbidities, or triptan interaction with medications you may not have known about.
Despite more than 5 million consultations annually, relatively little is known about the treatment of migraine in primary care. Much of the literature is projected from population surveys or reports concerning patients referred for specialist care or those entering treatment studies.
Our study is the largest reported to gather data directly from patients treated for migraine in family practice. The participating practices represent a spectrum of communities and practice types. As minimal differences exist in practice patterns between family physicians who participate in research networks and all family physicians1, these findings may more accurately reflect the current status in family practice than other studies.
We believe that this study indicates family physicians offer triptans to most patients consulting specifically for migraine and that adherence issues contribute significantly to the perceived low rates of use of these medications in primary care. In recent years, considerable effort has gone into increasing the diagnosis of migraine and promoting the more extensive use of triptans in primary care patients (see article on page 1038 in this issue). Family physicians must certainly continue to improve the recognition of migraine; but attention to patient concerns about triptans and efforts to enhance adherence and appropriate use of these medications is obviously essential. We must continue efforts to better understand why some 30% or more of migraine patients in primary care practice discontinue a therapy that has been found to be highly effective and well accepted by patients in clinical studies.
Migraine-specific prescribing in primary care is better than commonly reported
Between 1990 and 1998, the number of physician office visits for migraine doubled to more than 5 million per year.2 Of the more than 28 million US adults with migraine, approximately 70% of women and 50% of men are now believed to have consulted a physician at least once,3 and two thirds of these patients have made 5 or more physician visits for migraine.4 More than 72% of migraine-related physician visits are to primary care physicians, the most to family physicians.1
Nevertheless, the headache literature routinely describes migraine as “undertreated” in primary care.5-7 In particular, primary care physicians are perceived to under-prescribe triptans,7-11 the most effective migraine-specific medications available, widely regarded as “the gold standard” for acute migraine therapy of all but mild attacks.12-16 Population surveys estimate that only some 13% to 20% of migraine sufferers have been prescribed triptans.4,5,9,17 A 1995 study of migraine patients enrolled in a health maintenance organization reported that 11.4% used subcutaneous sumatriptan; however, oral triptans were not included in the study.18 Ten years later, another study of health plan enrollees estimated that only 11% of those meeting strict criteria for migraine were prescribed triptans or ergots.7
These low percentages do not correlate with our experience of primary care practice nor with data indicating substantial sales of triptans in the US.19 As we have not identified any studies that directly address prescribing by primary care physicians for migraine, we conducted a survey of patients who consulted family physicians for migraine during 2002.
Some of the differences between our findings and those based on prescription data could be attributed to the use of samples (reported to be particularly common in migraine treatment during this period), or difficulties in patient recall of medications.
Diagnosis of migraine not always coded. A more significant source of difference between our findings and those of population-based surveys is in the diagnosis of migraine. Most surveys use patient-reported symptoms for diagnosis, and hence the population of migraine sufferers includes those who have not had a physician visit coded for migraine. Our interest is in the primary care consultation specifically for migraine.
If a physician concludes a patient has migraine, this diagnosis is highly likely to be correct,20 and our findings indicate that a migraine-specific medication is commonly offered. We strongly support ongoing efforts to improve the recognition of migraine by all physicians and emphasize that our results are based only on patients identified by migraine-coded primary care visits.
Why do patients discontinue triptans?
The finding that about one third of patients discontinued triptan use may be surprising in view of the widely reported efficacy16 and tolerability24 of these medications, but this is almost identical to the results of a study of 663 patients of a US headache clinic.25 Significant rates of triptan discontinuation have been reported by other studies.
A study based on British general practice pharmacy records reported 55% of patients not renewing a triptan prescription during 1 year of follow-up,26 and an older study of patients attending a Dutch neurology clinic found that 25% of sumatriptan users discontinued this drug over a 2-year period.27 One US primary care treatment study found that on enrollment, 62% of 143 migraine patients had previously used triptans or ergotamines but had discontinued therapy.28
As in our study, the principal stated reason for discontinuation in the Dutch study27 was lack of efficacy. Conversely, in the US primary care study only 13% of patients gave lack of efficacy as the principal reason for discontinuation but 20% cited cost and 55% cited nonprescribing by physicians.28
As shown in the TABLE, the most striking differences between patients who discontinued triptans and those who continued were in patient satisfaction with treatment and current use of narcotic medication for migraine, but the higher grades of MIDAS scores (FIGURE) were also significantly more common in the patients who discontinued.
This study was not designed to assess if these factors caused or resulted from triptan discontinuation, but the association of triptan “failure” with 3 other significant negative factors could indicate subgroups of patients with especially high morbidity from migraine or risk of poor response to migraine-specific treatment. Future studies are needed to better characterize patients who discontinue, especially to examine the roles of comorbidities, total medication use, and the role of subspecialty referral.
TABLE
Differences between patients who discontinued triptans and those who continued
| DISCONTINUERS | CONTINUERS | P VALUE | |
|---|---|---|---|
| Disability (MIDAS score) | |||
| Grade I or II | 34 | 98 | .034 |
| Grade III or IV | 86 | 145 | |
| Medication coverage* | |||
| All or some | 106 | 216 | .904 |
| None | 14 | 28 | |
| Patient satisfaction | |||
| Satisfied | 71 | 201 | <.001 |
| Dissatisfied | 49 | 44 | |
| Gender | |||
| Female | 103 | 216 | .39 |
| Male | 18 | 27 | |
| Current narcotic use | |||
| Use | 57 | 54 | <.001 |
| No use | 64 | 191 | |
| * Payment by health insurance for migraine medications | |||
| Sample size calculated for alpha=0.05 and power=1–beta=0.80. | |||
Limitations of this study
This study has several weaknesses, mainly the low response rate and potential biases in patient selection and participation. A headache survey mailed to 200 randomly selected patients in a single British general practice reported a response rate of 61%29and the American Migraine II Survey reported response rates of 59% to 69% of households.4 Considerations of patient confidentiality, cost, and burdening busy practices limited our ability to use many of the strategies recommended to increase response rate.30 The highest response rates were from those smaller practices where the office staff expressed most interest in the study.
Although ICD coding has shortcomings as a technique of identifying a study population, it is reported to be very accurate for specific conditions such as migraine and for patients with insurance.31,32 We did not include questions to verify that patients met International Headache Society (IHS) criteria for migraine33 because of concerns about the length of the survey and because a positive diagnosis of migraine by a family physician is reported to be likely accurate 98% of the time.20 Examining how the accuracy of diagnosis and the various subtypes of migraine impact treatment would be interesting additions to a future study.
For this study, we used 10 community practices—5 rural and 5 urban, and all associated with the Kansas Practice Research Network—to conduct an observational, cross-sectional study of adult patients who consulted family physicians because of migraine during 2002. The 5 rural practices served communities ranging from 835 to 6313 in population and were selected to represent the different geographic regions of the state. Similarly, the 5 urban practices represented different demographic areas within the city of Wichita (population 344,284).
Patients were identified by use of migraine-specific ICD-9 codes (all subgroups of ICD 9-346) for the consultation. The only exclusion was of patients aged less than 18 years. The 15-item written survey (FIGURE W1) gathered demographic data and incorporated the standardized Migraine Disability Assessment Score (MIDAS) questionnaire (FIGURE),21,22 as well as questions about migraine experience, medications, and satisfaction with treatment.
The MIDAS questionnaire is a simple 5-item written instrument (FIGURE) developed from more complex measures of headache and morbidity specifically to assess impact on daily activities. Its validity, reliability, and ease of use have been confirmed in population studies and busy clinical settings.21-23 The survey asked patients to name all medications (prescription, nonprescription, or other, including herbal remedies) usually used for migraine. In addition, a specific question addressed current or previous use of the triptans available at the time of the study—ie, naratriptan (Amerge), sumatriptan (Imitrex—injection, oral, or nasal spray), rizatriptan (Maxalt), zolmitriptan (Zomig), almotriptan (Axert), and frovatriptan (Frova). This question used both generic and trade names for the medication. Patients who reported previous but not current use of any triptan were asked to describe their reasons for discontinuation in their own words.
Patients received the survey by mail, along with a cover letter from their personal physicians inviting them to participate in the study and instructions to return the anonymous survey directly to the primary investigator. Patients were assured that neither their personal physicians nor the researchers could identify participants and that their ongoing medical care would not be altered in any way by their participation in the survey or by the information provided. The study was approved by the University of Kansas School of Medicine Institutional Review Board.
Data were entered into a Microsoft Access 2000 file and 2 data entry personnel performed data editing to verify each entry. Data were analyzed using Microsoft Excel. Analysis was completed using the statistical program SPSS for Windows V.11.0 (SPSS Inc, Chicago, Ill). The principal modes of data analysis included chi-square, Kruskal-Wallis, independent samples t-tests, and analysis of variance (ANOVA). A probability value of less than 0.05 was considered statistically significant.
Results
The 10 participating practices identified 992 patients aged 18 or older who consulted at least once during 2002 primarily for a migraine-related diagnosis. After 3 mailings, 447 surveys suitable for analysis were returned (a response rate of 45%). For individual practices, the number of patients surveyed ranged from 9 to 540, and the response rates were from27.5% to 72%. Responders did not differ from nonresponders in age or gender distribution.
The respondents were predominantly female (83%) with a mean age of 44 years (range, 18–82). Two thirds of the respondents had experienced migraine for more than 10 years, and most reported that migraine significantly impacted their lives. Sixty percent of patients scored 10 or more on the MIDAS scale, indicating moderate-severe migraine-related disability.
Most respondents (85.5%) had private insurance. Only 14% reported having no assistance with payment for migraine medications, and 58% reported that “all” or “most” of their migraine medications were paid by insurance plans. Seventy-three percent of respondents were “satisfied” or “very satisfied” with medical treatment for migraine and only 5% “very dissatisfied.”
Participants reported using a wide range of prescription and nonprescription medications. Overall, 366 (82%) patients reported experience with triptans. Of these patients, 206 (56%) had used more than 1 triptan. Current triptan use was reported by 245 (55%) of all respondents. Among the 121 patients who reported discontinuation of triptans, the most common reason provided was lack of efficacy (57%), followed by adverse effects (24%).
Statistically significant differences were found between patients who continued triptan therapy and those who discontinued in migraine disability (MIDAS scores), satisfaction with migraine treatment, and reported use of narcotic medication for migraine (TABLE). Patients who discontinued triptan therapy did not differ significantly from those who continued in age, gender, number of years with migraine, insurance type, use of prophylactic migraine medication or reported use of analgesics, combination medications, ergots, “other,” or “no” medications to treat migraine attacks.
Although surveys were returned directly to the researchers without identifying information and patients were assured that information would not be shared with participating physicians, the study design could have inhibited negative comments about medical care. Conversely, patients who were angry, upset, or disappointed about migraine care could have been motivated to complete the survey.34 Migraine patients who consult physicians are reported to have more severe migraine, more comorbidities, decreased quality of life, and to consult significantly more frequently for multiple medical conditions than other patients.35,36
FIGURE
The MIDAS questionnaire is valid, reliable, and easy to use
Acknowledgments
The authors acknowledge substantial assistance from Nolem Llong, Terry Ast, Nicole Rogers, and Mary Hursey in the conduct of the study and preparation of this manuscript and the assistance of the physicians of the Kansas Practice Research Network. The study was funded in part by the AAFP Practice Based Research Network Research Stimulation Grant.
CORRESPONDENCE
Anne Walling MB, ChB, FFPHM, University of Kansas School of Medicine–Wichita, Department of Family and Community Medicine, 1010 North Kansas, Wichita, KS 67214. E-mail: [email protected]
- While continuing to improve recognition of migraine in your patient population, pay particular attention to the adherence rate among those for whom you have prescribed a triptan.
- Ask patients who discontinue triptan therapy why they made that decision. Besides adverse effects from the agent, reasons may include medication cost, influence of comorbidities, or triptan interaction with medications you may not have known about.
Despite more than 5 million consultations annually, relatively little is known about the treatment of migraine in primary care. Much of the literature is projected from population surveys or reports concerning patients referred for specialist care or those entering treatment studies.
Our study is the largest reported to gather data directly from patients treated for migraine in family practice. The participating practices represent a spectrum of communities and practice types. As minimal differences exist in practice patterns between family physicians who participate in research networks and all family physicians1, these findings may more accurately reflect the current status in family practice than other studies.
We believe that this study indicates family physicians offer triptans to most patients consulting specifically for migraine and that adherence issues contribute significantly to the perceived low rates of use of these medications in primary care. In recent years, considerable effort has gone into increasing the diagnosis of migraine and promoting the more extensive use of triptans in primary care patients (see article on page 1038 in this issue). Family physicians must certainly continue to improve the recognition of migraine; but attention to patient concerns about triptans and efforts to enhance adherence and appropriate use of these medications is obviously essential. We must continue efforts to better understand why some 30% or more of migraine patients in primary care practice discontinue a therapy that has been found to be highly effective and well accepted by patients in clinical studies.
Migraine-specific prescribing in primary care is better than commonly reported
Between 1990 and 1998, the number of physician office visits for migraine doubled to more than 5 million per year.2 Of the more than 28 million US adults with migraine, approximately 70% of women and 50% of men are now believed to have consulted a physician at least once,3 and two thirds of these patients have made 5 or more physician visits for migraine.4 More than 72% of migraine-related physician visits are to primary care physicians, the most to family physicians.1
Nevertheless, the headache literature routinely describes migraine as “undertreated” in primary care.5-7 In particular, primary care physicians are perceived to under-prescribe triptans,7-11 the most effective migraine-specific medications available, widely regarded as “the gold standard” for acute migraine therapy of all but mild attacks.12-16 Population surveys estimate that only some 13% to 20% of migraine sufferers have been prescribed triptans.4,5,9,17 A 1995 study of migraine patients enrolled in a health maintenance organization reported that 11.4% used subcutaneous sumatriptan; however, oral triptans were not included in the study.18 Ten years later, another study of health plan enrollees estimated that only 11% of those meeting strict criteria for migraine were prescribed triptans or ergots.7
These low percentages do not correlate with our experience of primary care practice nor with data indicating substantial sales of triptans in the US.19 As we have not identified any studies that directly address prescribing by primary care physicians for migraine, we conducted a survey of patients who consulted family physicians for migraine during 2002.
Some of the differences between our findings and those based on prescription data could be attributed to the use of samples (reported to be particularly common in migraine treatment during this period), or difficulties in patient recall of medications.
Diagnosis of migraine not always coded. A more significant source of difference between our findings and those of population-based surveys is in the diagnosis of migraine. Most surveys use patient-reported symptoms for diagnosis, and hence the population of migraine sufferers includes those who have not had a physician visit coded for migraine. Our interest is in the primary care consultation specifically for migraine.
If a physician concludes a patient has migraine, this diagnosis is highly likely to be correct,20 and our findings indicate that a migraine-specific medication is commonly offered. We strongly support ongoing efforts to improve the recognition of migraine by all physicians and emphasize that our results are based only on patients identified by migraine-coded primary care visits.
Why do patients discontinue triptans?
The finding that about one third of patients discontinued triptan use may be surprising in view of the widely reported efficacy16 and tolerability24 of these medications, but this is almost identical to the results of a study of 663 patients of a US headache clinic.25 Significant rates of triptan discontinuation have been reported by other studies.
A study based on British general practice pharmacy records reported 55% of patients not renewing a triptan prescription during 1 year of follow-up,26 and an older study of patients attending a Dutch neurology clinic found that 25% of sumatriptan users discontinued this drug over a 2-year period.27 One US primary care treatment study found that on enrollment, 62% of 143 migraine patients had previously used triptans or ergotamines but had discontinued therapy.28
As in our study, the principal stated reason for discontinuation in the Dutch study27 was lack of efficacy. Conversely, in the US primary care study only 13% of patients gave lack of efficacy as the principal reason for discontinuation but 20% cited cost and 55% cited nonprescribing by physicians.28
As shown in the TABLE, the most striking differences between patients who discontinued triptans and those who continued were in patient satisfaction with treatment and current use of narcotic medication for migraine, but the higher grades of MIDAS scores (FIGURE) were also significantly more common in the patients who discontinued.
This study was not designed to assess if these factors caused or resulted from triptan discontinuation, but the association of triptan “failure” with 3 other significant negative factors could indicate subgroups of patients with especially high morbidity from migraine or risk of poor response to migraine-specific treatment. Future studies are needed to better characterize patients who discontinue, especially to examine the roles of comorbidities, total medication use, and the role of subspecialty referral.
TABLE
Differences between patients who discontinued triptans and those who continued
| DISCONTINUERS | CONTINUERS | P VALUE | |
|---|---|---|---|
| Disability (MIDAS score) | |||
| Grade I or II | 34 | 98 | .034 |
| Grade III or IV | 86 | 145 | |
| Medication coverage* | |||
| All or some | 106 | 216 | .904 |
| None | 14 | 28 | |
| Patient satisfaction | |||
| Satisfied | 71 | 201 | <.001 |
| Dissatisfied | 49 | 44 | |
| Gender | |||
| Female | 103 | 216 | .39 |
| Male | 18 | 27 | |
| Current narcotic use | |||
| Use | 57 | 54 | <.001 |
| No use | 64 | 191 | |
| * Payment by health insurance for migraine medications | |||
| Sample size calculated for alpha=0.05 and power=1–beta=0.80. | |||
Limitations of this study
This study has several weaknesses, mainly the low response rate and potential biases in patient selection and participation. A headache survey mailed to 200 randomly selected patients in a single British general practice reported a response rate of 61%29and the American Migraine II Survey reported response rates of 59% to 69% of households.4 Considerations of patient confidentiality, cost, and burdening busy practices limited our ability to use many of the strategies recommended to increase response rate.30 The highest response rates were from those smaller practices where the office staff expressed most interest in the study.
Although ICD coding has shortcomings as a technique of identifying a study population, it is reported to be very accurate for specific conditions such as migraine and for patients with insurance.31,32 We did not include questions to verify that patients met International Headache Society (IHS) criteria for migraine33 because of concerns about the length of the survey and because a positive diagnosis of migraine by a family physician is reported to be likely accurate 98% of the time.20 Examining how the accuracy of diagnosis and the various subtypes of migraine impact treatment would be interesting additions to a future study.
For this study, we used 10 community practices—5 rural and 5 urban, and all associated with the Kansas Practice Research Network—to conduct an observational, cross-sectional study of adult patients who consulted family physicians because of migraine during 2002. The 5 rural practices served communities ranging from 835 to 6313 in population and were selected to represent the different geographic regions of the state. Similarly, the 5 urban practices represented different demographic areas within the city of Wichita (population 344,284).
Patients were identified by use of migraine-specific ICD-9 codes (all subgroups of ICD 9-346) for the consultation. The only exclusion was of patients aged less than 18 years. The 15-item written survey (FIGURE W1) gathered demographic data and incorporated the standardized Migraine Disability Assessment Score (MIDAS) questionnaire (FIGURE),21,22 as well as questions about migraine experience, medications, and satisfaction with treatment.
The MIDAS questionnaire is a simple 5-item written instrument (FIGURE) developed from more complex measures of headache and morbidity specifically to assess impact on daily activities. Its validity, reliability, and ease of use have been confirmed in population studies and busy clinical settings.21-23 The survey asked patients to name all medications (prescription, nonprescription, or other, including herbal remedies) usually used for migraine. In addition, a specific question addressed current or previous use of the triptans available at the time of the study—ie, naratriptan (Amerge), sumatriptan (Imitrex—injection, oral, or nasal spray), rizatriptan (Maxalt), zolmitriptan (Zomig), almotriptan (Axert), and frovatriptan (Frova). This question used both generic and trade names for the medication. Patients who reported previous but not current use of any triptan were asked to describe their reasons for discontinuation in their own words.
Patients received the survey by mail, along with a cover letter from their personal physicians inviting them to participate in the study and instructions to return the anonymous survey directly to the primary investigator. Patients were assured that neither their personal physicians nor the researchers could identify participants and that their ongoing medical care would not be altered in any way by their participation in the survey or by the information provided. The study was approved by the University of Kansas School of Medicine Institutional Review Board.
Data were entered into a Microsoft Access 2000 file and 2 data entry personnel performed data editing to verify each entry. Data were analyzed using Microsoft Excel. Analysis was completed using the statistical program SPSS for Windows V.11.0 (SPSS Inc, Chicago, Ill). The principal modes of data analysis included chi-square, Kruskal-Wallis, independent samples t-tests, and analysis of variance (ANOVA). A probability value of less than 0.05 was considered statistically significant.
Results
The 10 participating practices identified 992 patients aged 18 or older who consulted at least once during 2002 primarily for a migraine-related diagnosis. After 3 mailings, 447 surveys suitable for analysis were returned (a response rate of 45%). For individual practices, the number of patients surveyed ranged from 9 to 540, and the response rates were from27.5% to 72%. Responders did not differ from nonresponders in age or gender distribution.
The respondents were predominantly female (83%) with a mean age of 44 years (range, 18–82). Two thirds of the respondents had experienced migraine for more than 10 years, and most reported that migraine significantly impacted their lives. Sixty percent of patients scored 10 or more on the MIDAS scale, indicating moderate-severe migraine-related disability.
Most respondents (85.5%) had private insurance. Only 14% reported having no assistance with payment for migraine medications, and 58% reported that “all” or “most” of their migraine medications were paid by insurance plans. Seventy-three percent of respondents were “satisfied” or “very satisfied” with medical treatment for migraine and only 5% “very dissatisfied.”
Participants reported using a wide range of prescription and nonprescription medications. Overall, 366 (82%) patients reported experience with triptans. Of these patients, 206 (56%) had used more than 1 triptan. Current triptan use was reported by 245 (55%) of all respondents. Among the 121 patients who reported discontinuation of triptans, the most common reason provided was lack of efficacy (57%), followed by adverse effects (24%).
Statistically significant differences were found between patients who continued triptan therapy and those who discontinued in migraine disability (MIDAS scores), satisfaction with migraine treatment, and reported use of narcotic medication for migraine (TABLE). Patients who discontinued triptan therapy did not differ significantly from those who continued in age, gender, number of years with migraine, insurance type, use of prophylactic migraine medication or reported use of analgesics, combination medications, ergots, “other,” or “no” medications to treat migraine attacks.
Although surveys were returned directly to the researchers without identifying information and patients were assured that information would not be shared with participating physicians, the study design could have inhibited negative comments about medical care. Conversely, patients who were angry, upset, or disappointed about migraine care could have been motivated to complete the survey.34 Migraine patients who consult physicians are reported to have more severe migraine, more comorbidities, decreased quality of life, and to consult significantly more frequently for multiple medical conditions than other patients.35,36
FIGURE
The MIDAS questionnaire is valid, reliable, and easy to use
Acknowledgments
The authors acknowledge substantial assistance from Nolem Llong, Terry Ast, Nicole Rogers, and Mary Hursey in the conduct of the study and preparation of this manuscript and the assistance of the physicians of the Kansas Practice Research Network. The study was funded in part by the AAFP Practice Based Research Network Research Stimulation Grant.
CORRESPONDENCE
Anne Walling MB, ChB, FFPHM, University of Kansas School of Medicine–Wichita, Department of Family and Community Medicine, 1010 North Kansas, Wichita, KS 67214. E-mail: [email protected]
1. Nutting PA, Baier M, Werner JJ, Cutter G, Reed FM, Orzano AJ. Practice patterns of family physicians in practice-based research networks: a report from ASPN. J Am Board Fam Pract 1999;12:278-284.
2. Gibbs TS, Fleischer AB, Feldman SR, Sam MC, O’Donovan CA. Health care utilization in patients with migraine: demographics and patterns of care in the ambulatory setting. Headache 2003;43:330-335.
3. Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American migraine study II. Headache 2001;41:646-657.
4. Lipton RB, Scher AI, Kolodner K, Liberman J, Steiner TJ, Stewart WF. Migraine in the United States: Epidemiology and patterns of health care use. Neurology 2002;58:885-894.
5. Lipton RB, Diamond S, Reed M, Diamond M, Stewart WF. Migraine diagnosis and treatment: results from the American Migraine Study II. Headache 2001;41:638-645.
6. Maizels M. Model interventions to improve headache outcomes in health care systems. In Reducing the Burden of Headache, Olesen J, Steiner TJ, Lipton RB (eds). New York: Oxford University Press; 2003:290-301.
7. Bigal ME, Kolodner KB, Lafata JE, Leotta C, Lipton RB. Patterns of medical diagnosis and treatment of migraine and probable migraine in a health plan. Cephalalgia 2006;26:43-49.
8. Cady R, Dodrick DW. Diagnosis and treatment of migraine. Mayo Clin Proc 2002;77:255-261.
9. Lipton RB, Scher AI, Steiner TJ, et al. Patterns of health care utilization for migraine in England and in the United States Neurology 2003;60:441-448.
10. Loder EW, Lipton RB. Conclusion: how primary care physicians can help their patients with migraine. Am J Med 2005;118:45S-46S.
11. Loder EW, Sheftell F. The quality of headache treatment in the United States: review and analysis of recent data. Headache 2005;45:939-946.
12. Snow V, Weiss K, Wall EM, Mottur-Pilson C. Pharmacologic management of acute attacks of migraine and prevention of migraine headache. Ann Intern Med 2002;137:840-849.
13. Lipton RB, Cutrer FM, Goadsby PJ, et al. How treatment priorities influence triptan p in clinical practice: perspectives of migraine sufferers, neurologists, and primary care physicians. Curr Med Res Opin 2005;21:413-424.
14. Gallagher RM, Cutrer FM. Migraine: diagnosis, management, and new treatment options. Am J Man Care 2002;8:S58-S73.
15. Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000;55:754-763.
16. Ferrari MD, Roon KI, Lipton RB, Goadsby PJ. Oral triptans (setotonin 5-HT1B/1D agonists) in acute migraine treatment: a meta-analysis of 53 trials. Lancet 2001;358:1668-1675.
17. Lohman JJHM, van der Kuy-de Ree MM. Patterns of specific antimigraine drug use—a study based on the records of 18 community pharmacies. Cephalalgia 2004;25:214-218.
18. Von Korff M, Black LK, Saunders K, Galer BS. Headache medication-use among primary care headache patients in a health maintenance organization. Cephalalgia 1999;19:575-580.
19. Available at: www.pozen.com/product/migraine.asppjbpubs.com/script_reports/migraine.htm.
20. Tepper SJ, Dahlof CG, Dowson A, et al. Prevalence and diagnosis of migraine in patients consulting their physician with a complaint of a headache: data from the Landmark Study. Headache 2004;44:856-864.
21. Stewart WF, Lipton RB, Kolodner K, Liberman J, Sawyer J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia 1000;19:107-114.
22. Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment Score in (MIDAS) n comparison to a diary-based measure in a population sample of migraine sufferers. Pain 2000;88:41-52.
23. Andrasik F, Lipchik GL, McCroy DC, Wittrock DA. Outcome measurement in behavioral headache research: headache parameters and psychosocial outcomes. Headache 2005;45:429-437.
24. Welch KMS, Mathew NT, Rosamond W, et al. Tolerability of sumatriptan: clinical trials and post-marketing experience. Cephalalgia 2000;20:687-695.
25. Robbins L. Triptans versus analgesics. Headache 2002;42:903-907.
26. Savini N, Martin A, Browning D. Switching patients with migraine from sumatriptan to other triptans increases primary care costs. Int J Clin Prac 2004;58:758-763.
27. Visser WH, de Vriend RHM, Jaspers NMWH, Ferrari MD. Sumatriptan in clinical practice: a 2-year review of 453 migraine patients. Neurology 1996;47:46-51.
28. Powers C, Szeto S, Pangtay D, Bort T, Cervi M, Cady R. Evaluation of migraineurs’ p for naratriptan over conventional first-line agents. Arch Fam Med 2000;9:753-757.
29. Boardman HF. Headaches in primary care: a pilot study. Cephalalgia 2000;20:364.-
30. Edwards P, Roberts I, Clarke M, et al. Increasing response rates to postal questionnaires: systematic review. BMJ 2002;324:1183-1193.
31. Chao J, Gillanders WG, Flocke SA, et al. Billing for physician services: a comparison of actual billing with CPT codes assigned by direct observation. J Fam Pract 1998;47:28-32.
32. Stange KC, Zyzanski SJ, Smith TF, et al. How valid are medical records and patient questionnaires for physician profiling and health services research? A comparison of direct observation of patients visits. Med Care 1998;36:851-857.
33. Headache Classification Subcommittee of the International Headache Society The international classification of headache disorders 2nd ed. Cephalalgia 2004;24:S1-S150.
34. Scott A, Smith RD. Keeping the customer satisfied: issues in the interpretation and use of patient satisfaction surveys. Int J Qual Health Care 1994;6:353-359.
35. Linet MS, Celentano DC, Stewart WF. Headache characteristics associated with physician consultation: a population-based survey. Am J Prevent Med 1991;7:40-46.
36. Lafata JE, Moon C, Leotta C, Kolodner K, Poisson L, Lipton RB. The medical care utilization and costs associated with migraine headache. J Gen Intern Med 2004;19:1005-1012.
1. Nutting PA, Baier M, Werner JJ, Cutter G, Reed FM, Orzano AJ. Practice patterns of family physicians in practice-based research networks: a report from ASPN. J Am Board Fam Pract 1999;12:278-284.
2. Gibbs TS, Fleischer AB, Feldman SR, Sam MC, O’Donovan CA. Health care utilization in patients with migraine: demographics and patterns of care in the ambulatory setting. Headache 2003;43:330-335.
3. Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American migraine study II. Headache 2001;41:646-657.
4. Lipton RB, Scher AI, Kolodner K, Liberman J, Steiner TJ, Stewart WF. Migraine in the United States: Epidemiology and patterns of health care use. Neurology 2002;58:885-894.
5. Lipton RB, Diamond S, Reed M, Diamond M, Stewart WF. Migraine diagnosis and treatment: results from the American Migraine Study II. Headache 2001;41:638-645.
6. Maizels M. Model interventions to improve headache outcomes in health care systems. In Reducing the Burden of Headache, Olesen J, Steiner TJ, Lipton RB (eds). New York: Oxford University Press; 2003:290-301.
7. Bigal ME, Kolodner KB, Lafata JE, Leotta C, Lipton RB. Patterns of medical diagnosis and treatment of migraine and probable migraine in a health plan. Cephalalgia 2006;26:43-49.
8. Cady R, Dodrick DW. Diagnosis and treatment of migraine. Mayo Clin Proc 2002;77:255-261.
9. Lipton RB, Scher AI, Steiner TJ, et al. Patterns of health care utilization for migraine in England and in the United States Neurology 2003;60:441-448.
10. Loder EW, Lipton RB. Conclusion: how primary care physicians can help their patients with migraine. Am J Med 2005;118:45S-46S.
11. Loder EW, Sheftell F. The quality of headache treatment in the United States: review and analysis of recent data. Headache 2005;45:939-946.
12. Snow V, Weiss K, Wall EM, Mottur-Pilson C. Pharmacologic management of acute attacks of migraine and prevention of migraine headache. Ann Intern Med 2002;137:840-849.
13. Lipton RB, Cutrer FM, Goadsby PJ, et al. How treatment priorities influence triptan p in clinical practice: perspectives of migraine sufferers, neurologists, and primary care physicians. Curr Med Res Opin 2005;21:413-424.
14. Gallagher RM, Cutrer FM. Migraine: diagnosis, management, and new treatment options. Am J Man Care 2002;8:S58-S73.
15. Silberstein SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2000;55:754-763.
16. Ferrari MD, Roon KI, Lipton RB, Goadsby PJ. Oral triptans (setotonin 5-HT1B/1D agonists) in acute migraine treatment: a meta-analysis of 53 trials. Lancet 2001;358:1668-1675.
17. Lohman JJHM, van der Kuy-de Ree MM. Patterns of specific antimigraine drug use—a study based on the records of 18 community pharmacies. Cephalalgia 2004;25:214-218.
18. Von Korff M, Black LK, Saunders K, Galer BS. Headache medication-use among primary care headache patients in a health maintenance organization. Cephalalgia 1999;19:575-580.
19. Available at: www.pozen.com/product/migraine.asppjbpubs.com/script_reports/migraine.htm.
20. Tepper SJ, Dahlof CG, Dowson A, et al. Prevalence and diagnosis of migraine in patients consulting their physician with a complaint of a headache: data from the Landmark Study. Headache 2004;44:856-864.
21. Stewart WF, Lipton RB, Kolodner K, Liberman J, Sawyer J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia 1000;19:107-114.
22. Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN. Validity of the Migraine Disability Assessment Score in (MIDAS) n comparison to a diary-based measure in a population sample of migraine sufferers. Pain 2000;88:41-52.
23. Andrasik F, Lipchik GL, McCroy DC, Wittrock DA. Outcome measurement in behavioral headache research: headache parameters and psychosocial outcomes. Headache 2005;45:429-437.
24. Welch KMS, Mathew NT, Rosamond W, et al. Tolerability of sumatriptan: clinical trials and post-marketing experience. Cephalalgia 2000;20:687-695.
25. Robbins L. Triptans versus analgesics. Headache 2002;42:903-907.
26. Savini N, Martin A, Browning D. Switching patients with migraine from sumatriptan to other triptans increases primary care costs. Int J Clin Prac 2004;58:758-763.
27. Visser WH, de Vriend RHM, Jaspers NMWH, Ferrari MD. Sumatriptan in clinical practice: a 2-year review of 453 migraine patients. Neurology 1996;47:46-51.
28. Powers C, Szeto S, Pangtay D, Bort T, Cervi M, Cady R. Evaluation of migraineurs’ p for naratriptan over conventional first-line agents. Arch Fam Med 2000;9:753-757.
29. Boardman HF. Headaches in primary care: a pilot study. Cephalalgia 2000;20:364.-
30. Edwards P, Roberts I, Clarke M, et al. Increasing response rates to postal questionnaires: systematic review. BMJ 2002;324:1183-1193.
31. Chao J, Gillanders WG, Flocke SA, et al. Billing for physician services: a comparison of actual billing with CPT codes assigned by direct observation. J Fam Pract 1998;47:28-32.
32. Stange KC, Zyzanski SJ, Smith TF, et al. How valid are medical records and patient questionnaires for physician profiling and health services research? A comparison of direct observation of patients visits. Med Care 1998;36:851-857.
33. Headache Classification Subcommittee of the International Headache Society The international classification of headache disorders 2nd ed. Cephalalgia 2004;24:S1-S150.
34. Scott A, Smith RD. Keeping the customer satisfied: issues in the interpretation and use of patient satisfaction surveys. Int J Qual Health Care 1994;6:353-359.
35. Linet MS, Celentano DC, Stewart WF. Headache characteristics associated with physician consultation: a population-based survey. Am J Prevent Med 1991;7:40-46.
36. Lafata JE, Moon C, Leotta C, Kolodner K, Poisson L, Lipton RB. The medical care utilization and costs associated with migraine headache. J Gen Intern Med 2004;19:1005-1012.