User login
- Oral creatine supplementation combined with resistance training increases maximal weight young men can lift.
- It is unknown whether this increase in strength translates into improvement in sports performance.
- Evidence in the existing literature is insufficient to draw conclusions about the effect of creatine in women or older individuals.
- Because no long-term studies have been performed on the safety of creatine supplementation, its use should not be universally recommended.
Creatine has gained widespread popularity during the past decade as a possible performance-enhancing agent among professional and recreational athletes. It is the most widely used performance-enhancing supplement among youth aged 10 to 17 years,1 with 15% to 30% of high school athletes2,3 and 48% of male Division I college athletes4 reporting creatine use. Considered a nutritional supplement, it is not regulated by the United States Food and Drug Administration nor is it banned by the International Olympic Committee or National Collegiate Athletic Association. Because of the widespread use of creatine, primary care providers must be knowledgeable about its effectiveness and safety.
Oral creatine monohydrate increases skeletal muscle creatine concentration by 16% to 50%,5-7 but whether it is an effective ergogenic aid remains controversial. Multiple studies have investigated this question, but many have been small, often including fewer than 10 subjects, and results have been conflicting. Several reviews8-14 have addressed the effectiveness of creatine, but there has not been a systematic and comprehensive meta-analysis to resolve the uncertainties in the literature or to quantify the magnitude of the effect of creatine. To evaluate whether oral creatine supplementation improves strength and power in healthy adults, and further to quantify the effect, we performed a meta-analysis of randomized and matched controlled trials investigating creatine supplementation and strength.
Methods
Search strategy
To identify possible studies for inclusion, 1 author (M.F.M.) searched the MEDLINE electronic database (1966–2000) using the terms “creatine supplementation” or “creatine” combined with “strength” or “power.” Another MEDLINE search (1966–2000) was independently conducted by another author (R.L.D.) using the term “creatine not kinase” combined with a previously published search strategy to comprehensively identify randomized clinical trials.15 We searched the Cochrane Controlled Trials Register using the term “creatine not kinase.” We manually reviewed bibliographies of identified studies, abstracts from American College of Sports Medicine annual meetings (1999 and 2000), and a reference list distributed by an expert on the subject at the annual meeting of the American Medical Society for Sports Medicine (2000). Titles and available abstracts were screened and relevant articles retrieved. An expert in the field was contacted for sources of unpublished data.
Inclusion and exclusion criteria
Two reviewers independently assessed articles for inclusion. A third reviewer was consulted to resolve discrepancies. We used the following inclusion criteria: (1) the articles reported results of randomized or matched placebo-controlled trials investigating the effect of oral creatine supplementation on strength or power with or without concomitant resistance training; (2) the study subjects were healthy men or women older than 16 years with or without previous athletic training; and (3) the studies were published in any language. Given the general disagreement regarding the time required for muscle creatine concentration to return to presupplementation levels after discontinuing oral creatine,16-18 studies using a crossover design were excluded from the statistical analysis unless data from the first arm, before crossover, could be abstracted or obtained from the original investigator. Outcomes were measures of strength or power of any muscle group, including maximal weight lifted; peak power achieved in maximal (sprint) cycle ergometry; and peak knee flexion/extension torque in isokinetic dynamometer testing. Measurements of endurance, such as time to fatigue on cycle ergometer and number of repetitions achieved in submaximal weight lifting, were excluded. For studies reporting outcome per kilogram of body weight, we contacted investigators to obtain absolute outcome values and excluded studies if uncorrected data were not received. We also excluded articles that evaluated outcomes not investigated in at least 2 other studies. Finally, if we could not extract data in a usable form, we contacted investigators to obtain adequate data.
Quality assessment
Two independent reviewers appraised articles to determine methodological quality with respect to risk of bias under the following categories: method of randomization, allocation concealment, blinding, similarity of study groups, withdrawals and dropouts, and intention-to-treat analysis. Each study that met inclusion criteria was given a quality score, with a maximum possible score of 10, using a tool adapted from the Cochrane Handbook.19 The quality assessment data are presented but were not used to exclude or rank any study.
Data abstraction and statistical analysis
Two independent reviewers abstracted data, and a third reviewer resolved differences. For studies investigating multiple sprints, data from the first sprint only were included in statistical analysis because the first sprint is when peak power achievement is expected. A weighted mean difference (WMD) between creatine and placebo groups was calculated for each outcome using Review Manager 4.1 software (developed by The Cochrane Collaboration). A fixed effects model was used unless statistical heterogeneity was significant (P < .05), in which case a random effects model was used. Subanalyses were planned on several factors that were anticipated to be sources for variation, including (1) dose and duration of creatine administration, (2) concomitant resistance training, (3) different baseline level of physical training, (4) age, and (5) sex.
Results
Description of studies
After reviewing titles and available abstracts of more than 500 articles, we retrieved 66 potentially relevant studies, 16 of which met inclusion criteria for the analysis.17,20-34 Characteristics of these studies are summarized in the Table. Included studies represented 20 discrete samples and 414 subjects. Two studies20,21 evaluated creatine supplementation in men older than 60 years, whereas all the others studied younger subjects (range, 18–36 years). Only 1 study included women.17 Creatine dosages were similar across included studies (typically 20 g/d for the first 4–7 days of supplementation and 5 g/d thereafter). Studies that evaluated maximal weight lifting performance were more likely to include adjuvant resistance training programs in their protocols than those that evaluated cycle ergometry sprint or isokinetic dynamometer performance. None included cycle ergometry training.
TABLE
Characteristics of included studies
| Reference | No. subjects (sex) | Dose per day and duration | Training level | Weight training during study? | Outcome measurement | Quality score (out of 10) | Comparability of creatine & placebo groups at baseline* |
|---|---|---|---|---|---|---|---|
| Barnett 1996 | 17 (M) | 280 mg/kg ×4 d | Active | No | CP | 2.5 | + |
| Cooke 1995 | 12 (M) | 20 g ×5 d | Untrained | No | CP | 2.5 | + |
| Cooke 1997† | 80 (M) | 20 g ×5 d | Trained or active | No | CP | 2 | +++ |
| Dawson 1995‡ | 18 (M), 22(M) | 20 g ×5 d | Active | No | CP | 3 | +++ |
| Jones 1999 | 16 (M) | 20 g ×5 d then 5 g ×10 wk | Trained | Yes | CM | 3 | +++ |
| Stone 1999 | 20 (M) | 0.22 g/kg ×35 d | Trained | Yes | CM, BP, S | 4.5 | +++ |
| Kelly 1998 | 18 (M) | 20 g ×5 d then 5 g ×26 d | Trained | Yes | 3BP | 2 | – |
| Noonan 1998 | 39 (M) | 20 g ×5 d then 300 mg/kg ×8 wk | Trained | Yes | BP | 5.5 | +++ |
| Peeters 1999 | 35 (M) | 20 g ×3 d then 10 g ×6 wk | Trained | Yes | BP | 3 | +++ |
| Vandenberghe 1997 | 19 (F) | 20 g ×4 d then 5 g ×10 wk | Untrained | Yes | BP, S | 5 | +++ |
| Pearson 1999 | 16 (M) | 5 g ×10 wk | Trained | Yes | BP, S, PT | 3 | +++ |
| Volek 1999 | 19 (M) | 25 g ×7 d then 5 g ×12 wk | Trained | Yes | BP, S | 4.5 | +++ |
| Gilliam 2000 | 23 (M) | 20 g ×5 d | Active but untrained | No | PT | 2.5 | + |
| Rawson 1999§ | 20 (M) | 20 g ×10 d then 4 g ×20 d | Untrained | No | AF, PT | 4.5 | +++ |
| Rawson 2000§ | 17 (M) | 20 g ×5 d | Untrained | No | AF | 3.5 | +++ |
| Becque 2000 | 23 (M) | 20 g ×5 d then 2 g ×6 wk | Trained | Yes | AF | 5 | + |
| *Comparability between groups was assessed for age, anthropomorphic measurements, and strength outcomes. +++ = similar for all 3 characteristics; + = similar for strength outcome measurements; – = not comparable at baseline for strength outcome. | |||||||
| †Four protocols with 20 subjects each evaluating the same strength outcome measurement reported in Cooke 1997. | |||||||
| ‡Two separate experiments reported in Dawson 1995. | |||||||
| §Included subjects > 60 years old; in all others subjects were < 36 years old. | |||||||
| AF, 1 repetition maximum arm flexor strength; BP, 1 repetition maximum bench press strength; 3BP, 3 repetition maximum bench press strength; CM, cycle ergometer mean peak power; CP, cycle ergometer peak power; PT, isokinetic leg flexion/extension peak torque; S, 1 repetition maximum squat strength. | |||||||
Methodological quality of included studies
The methodological quality of studies was generally low (Table). The mean quality score was 3.5 ± 1.2 (mean ± SD) out of a possible 10 (range, 2–5.5). None of the studies identified the method of randomization used or specifically reported an intention-to-treat analysis. None specifically reported masking of outcome assessment. In general, these significant flaws in study design would tend to result in overestimation of the benefit of creatine supplementation.
Absolute strength
When 1- to 3-repetition maximum bench press strength measurements were statistically combined (they were homogeneous), the creatine supplementation group showed an absolute strength increase of 6.85 kg (95% confidence interval [CI], 5.24–8.47; n = 143) lifted per repetition greater than that seen with placebo alone (Figure 1). There was no additional advantage in strength performance after 9 to 12 weeks of supplementation (WMD = 6.6 kg; 95% CI, 3.5–9.5) compared with 4 to 8 weeks of supplementation (WMD = 6.6 kg; 95% CI, 4.8–8.4). Subanalysis for an interaction with resistance training, previous training level, age, or sex was not possible because all studies measuring bench press strength except one17 investigated creatine supple mentation in previously trained young men who continued resistance training during supplementation. The 1 study in previously sedentary young women17 did find a trend toward increased bench press strength, although independently this change was not statistically significant.
There was no significant difference in 1-repetition maximum arm flexor strength with creatine supplementation (WMD = 1.53 kg; 95% CI, –1.07 to 4.13; n = 60; Figure 2). However, 2 trials20,21 of the 3 evaluating this outcome studied subjects older than 60 years and did not employ adjuvant weight training programs. The study that incorporated resistance training and evaluated younger subjects22 found a modest (29.9% vs 16.5%) improvement in 1-repetition maximum arm flexor strength with creatine compared with placebo.
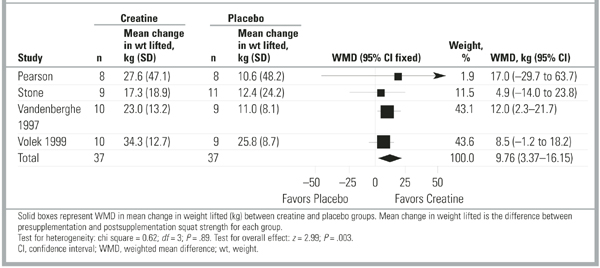
For 1-repetition maximum squat, creatine supplementation resulted in a strength increase of 9.76 kg (95% CI, 3.37–16.15; n = 74) greater than that of placebo (Figure 3). There was no advantage to longer-term supplementation (10.9 kg more than placebo [95% CI, 3.4–18.4] for 5–6 weeks compared with 10.4 kg [95% CI, 3.5–17.2] for 10–12 weeks). Again, in all but 1 study17 measuring squat performance, subjects were previously trained young men engaging in adjuvant resistance training programs, so subanalysis for other variables was not possible. For previously sedentary women, Vandenberghe et al17 found no difference at 5 weeks, but they did find a significant improvement in 1-repetition maximum squat performance with creatine supplementation at 10 weeks. Tests for heterogeneity were nonsignificant for all absolute strength variables.
To evaluate for publication bias, we examined funnel plots of each of the 3 absolute strength outcomes (bench press, arm flexor, and squat exercises). No evidence of publication bias was demonstrated. Figure W1 (available on the JFP Web site: http://www.jfponline.com) depicts a composite funnel plot of all 3 outcomes using a standardized mean difference to allow comparison between these 3 different outcomes.
FIGURE 1 Studies assessing 1- to 3-repetition maximum bench press strength
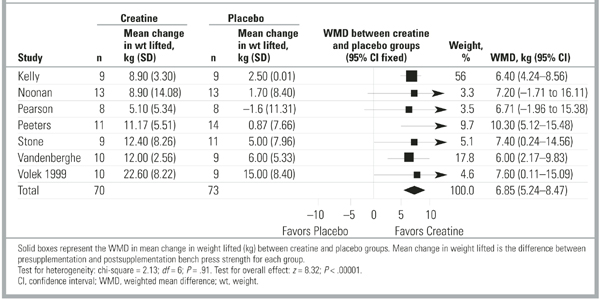
FIGURE 2 Studies assessing 1-repetition maximum arm flexor strength
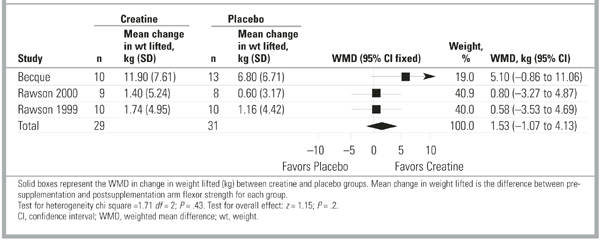
FIGURE 3 Studies assessing 1-repetition maximum squat strength
Cycle ergometer peak power
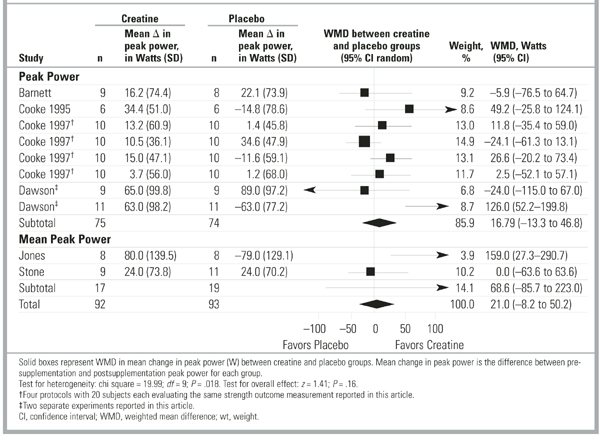
Creatine supplementation had no effect on peak power production during cycle ergometry sprint (Figure 4). Results among studies were widely variable (test for heterogeneity P= .035), so a random effects model was used to pool data. The summary weighted mean difference of 16.79 W (95% CI, –13.26 to 46.84; n = 149) was insignificant, both statistically (test for overall effect P= .3) and clinically, because this represents approximately a 1% change greater than baseline. Two studies23,24 looked at mean peak power across a series of 15-to 30-second sprints and found inconsistent results, with a summary weighted mean difference of 68.61 W (95% CI, –85.74 to 222.97; n = 36). Of note, for the 2 studies24,25 that demonstrated improved performance with creatine, the difference was accentuated by an unexplained but pronounced worsening of performance after supplementation in the placebo groups.
FIGURE 4 Studies assessing cycle ergometer sprint peak power
Dynamometer peak torque
Only 3 studies21,26,27 evaluated peak torque, and all used slightly different outcome assessments. One study26 reported average peak torque across 30 isokinetic leg flexion/extension contractions; 1 study21 reported the sum of peak torque across 5 sets of 30 isokinetic leg flexion/extension contractions; and 1 study27 gave peak torque data for isokinetic leg extension but did not describe precisely how peak torque was determined. There was no difference between creatine and placebo for isokinetic leg flexion/extension peak torque using a standardized mean difference to account for variations in measurement of this outcome. Tests for heterogeneity were nonsignificant for this outcome (P= .19).
Adverse effects
Four studies commented on short-term adverse effects of creatine supplementation. Three studies17,23,28 found no difference between creatine and placebo. One study21 reported gastrointestinal upset, rash, or headache in 3 subjects taking creatine and no adverse effects in subjects taking placebo. None of these studies was designed to evaluate long-term adverse effects of creatine supplementation, and there were no reports of longer-term follow up.
Discussion
This is the first study to report quantitatively the effect of creatine supplementation on strength performance from meta-analysis of the existing literature. We found that oral creatine supplementation improves maximal resistance exercise performance in previously trained young men. There is insufficient evidence that creatine improves other measures of strength, such as cycle ergometry sprint peak power or isokinetic dynamometer peak torque, or that creatine improves strength in women or older individuals. The effect of creatine on endurance, submaximal exercise, or actual “on-field” athletic performance was not addressed.
Creatine’s ergogenic properties may result from allowing increased work during training and decreasing recovery time. If so, creatine must be combined with adjuvant training to increase strength and power. Only studies investigating maximal weight-lifting performance incorporated resistance-training programs specific to the outcome being measured. Three studies included weight training but investigated non–weight-lifting outcomes,23,24,27 and only 1 study24 found a benefit from creatine supplementation. It is unclear whether the lack of effect for non–weight-lifting outcomes means that creatine is not beneficial unless combined with specific adjuvant training or that creatine simply is not ergogenic for outcomes other than maximal weight lifted.
This meta-analysis has some limitations. Our definition of strength included only “pure strength” or “power” measurements to allow statistical comparisons between similar outcomes. Because muscle strength is related to muscle endurance, researchers may define strength differently. It is not obvious at what point an exercise becomes a test of endurance and not just strength, but there is a physiologic basis for believing that creatine supplementation would more markedly improve performance in maximal or shorter duration exercises (ie, requiring strength and not endurance). The inclusion criteria for this project were determined before study review and selection and were applied consistently across all studies.
The quality and design of identified studies was another limitation. Most were small and did not fully delineate their randomization or blinding strategies. Multiple variations in study protocols made combining results of different studies somewhat problematic. Unfortunately, meta-regression or subanalysis for variables such as concurrent resistance training, previous training level, age, and sex were not possible because too few studies evaluated these variables independently of one another. Almost all of the studies finding a benefit of creatine supplementation were in young, previously trained men who engaged in resistance training concomitantly with supplementation, and the outcome measured was maximal weight lifted. Those studies not finding a difference were generally of less highly trained or older individuals, did not include resistance training, and more often investigated outcomes other than maximal weight lifted. This meta-analysis identifies that it is impossible to conclude from the existing literature which combination of variables is necessary to see a benefit of creatine supplementation.
More information is needed on the safety of creatine supplementation. Although a recent review35 reported no significant short-term adverse effects, no adequate long-term studies have been conducted. Two retrospective trials36,37 reported no adverse effects from longer-term (up to 5 years) creatine supplementation;however, neither study was randomized, blinded, or controlled, and neither had sufficient statistical power to detect uncommon adverse effects. Additionally, the designs of these studies precluded the possibility of detecting serious adverse effects such as death or disability. There have been case reports of renal dysfunction due to creatine38-40 and, as of 1998, the Food and Drug Administration had received 32 adverse event reports including seizures, myopathy, rhabdomyolosis, cardiac arrhythmia, and death.41
Given the popularity of nutritional supplements among all levels of athletes, clinicians cannot avoid questions about the effectiveness and safety of creatine supplementation. This meta-analysis demonstrated that oral creatine does improve performance during maximal resistance exercises in young men. However, we found no benefit for outcomes other than maximal weight lifted, suggesting that creatine may not improve actual performance in more complex movements requiring strength, speed, and coordination of multiple muscle groups. Studies investigating the effect of creatine in actual athletic performance are lacking.
Several important questions remain to be answered about creatine. What are the effects for women and older individuals? Is resistance training necessary to see strength performance improvement? Are these improvements in strength accompanied by improved athletic performance? How long do the effects of creatine remain after discontinuing supplementation? Most importantly, what is the long-term safety profile of creatine? Without further research to answer these questions, we cannot support the use of creatine supplementation for performance enhancement despite evidence for a positive impact on some components of strength.
Drug therapy for prevention and treatment of postmenopausal osteoporosis
| Drug (trade name) | Indication and dosage | Possible side effects (% of patients) | Cost per month* |
|---|---|---|---|
| Calcium and vitamin D (generic,Tums,Citracal, and others) | Prevention and treatment: 1200 –1500 mg/day calcium and 800 IU/day vitamin D | Nausea,dyspepsia (uncommon), constipation (10%) | $5 (both) |
| Estrogen †(Premarin,Ogen,Estrace, Estraderm,and others) | Prevention: 0.625 mg/day conjugated equine estrogen or the equivalent;0.3 mg/day may be effective | Nausea,breast tenderness, vaginal bleeding, mood alterations, headache, bloating | $14 –$28 |
| Alendronate (Fosamax) | Prevention:5 mg/day or 35 mg/week Treatment:10 mg/day or 70 mg/wk | Nausea, dyspepsia, esophageal irritation | $67 |
| Risedronate (Actonel) | Prevention and treatment: 5 mg/day or 35 mg/week | Abdominal pain, esophageal irritation | $67 |
| Raloxifene (Evista) | Treatment: 60 mg/day | Hot flashes (6%), leg cramps (3%) | $70 |
| Calcitonin nasal spray (Miacalcin) | Treatment:200 IU/day (1 spray in 1 nostril per day) | Rhinitis (5%), epistaxis, sinusitis | $66 |
| *Average wholesale cost to the pharmacy for 30 days of therapy; (Drug Topics Red Book. Montvale, NJ; Medical Economics Co., Inc, 2002.) | |||
| †Women with a uterus need to take a progestin such as medroxyprogesterone acetate (Provera $30/month, generic $9/month) or a combination estrogen/progestin product (Prempro $33/monh, FemHRT $26/month). | |||
On page 868 of the October issue a name was misspelled; the correct name is Brian S. Alper.
In the table appearing on page 877 of the October issue, the entry for Fosamax inadvertently combined prevention and treatment dosages. The corrected entry is shown below.
· Acknowledgments ·
This study was supported in part by a Faculty Development in Family Medicine Grant (No. 5D45 PE 55052-09) and a National Research Service Award Grant (No. 1T32 PE 10030-03) from the United States Department of Health and Human Services. The authors thank Craig Young, MD, who assisted in the conception of this project; Chris McLaughlin, who provided editorial assistance; and Veronica Ruleford, who assisted with the preparation of the manuscript.
1. USA Today. Survey: More than 1 million kids use sports supplements. USA Today. August 28, 2001. Available at: www.usatoday.com/news/nation/2001/08/28/youth-supplements.htm. Accessed October 8, 2002.
2. McGuine TA, Sullivan JC, Bernhardt DT. Creatine supplementation in high school football players. Clin J Sport Med 2001;11(4):247-53.
3. Ray TR, Eck JC, Covington LA, Murphy RB, Williams R, Knudtson J. Use of oral creatine as an ergogenic aid for increased sports performance: perceptions of adolescent athletes. South Med J 2001;94(6):608-12.
4. LaBotz M, Smith BW. Creatine supplement use in an NCAA Division I athletic program. Clin J Sport Med 1999;9(3):167-9.
5. Harris RC, Soderlund K, Hultman E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci 1992;83:367-74.
6. Vandenberghe K, Van Hecke P, Van Leemputte M, Vanstapel F, Hespel P. Phosphocreatine resynthesis is not affected by creatine loading. Med Sci Sports Exerc 1999;31(2):236-42.
7. Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. J Appl Physiol 1996;812:32-7.
8. Terjung RL, Clarkson P, Eichner ER, Greenhaff PL, Hespel PJ, Israel RG, et al. American College of Sports Medicine roundtable. The physiological and health effects of oral creatine supplementation. Med Sci Sports Exerc 2000;32(3):706-17.
9. Kreider RB. Dietary supplements and the promotion of muscle growth with resistance exercise. Sports Med 1999;27(2):97-110.
10. Mujika I, Padilla S. Creatine supplementation as an ergogenic aid for sports performance in highly trained athletes: a critical review. Int J Sports Med 1997;18(7):491-6.
11. Juhn MS, Tarnopolsky M. Oral creatine supplementation and athletic performance: a critical review. Clin J Sport Med 1998;8(4):286-97.
12. Volek JS, Kraemer WJ. Creatine supplementation: its effect on human muscular performance and body composition. J Strength Cond Res 1996;10(3):200-10.
13. Maughan RJ. Creatine supplementation and exercise performance. Int J Sport Nutr 1995;5:94-101.
14. Kraemer WJ, Volek JS. Creatine supplementation. Its role in human performance. Clin Sports Med 1999;18(3):651-66.
15. Dickersin K, Scherer R, Lefebvre C. Systematic reviews: identifying relevant studies for systematic reviews. Br Med J 1994;309(6964):1286-91.
16. Febbraio MA, Flanagan TR, Snow RJ, Zhao S, Carey MF. Effect of creatine supplementation on intramuscular TCr, metabolism and performance during intermittent, supramaximal exercise in humans. Acta Physiol Scand 1995;155(4):387-95.
17. Vandenberghe K, Goris M, Van Hecke P, Van Leemputte M, Vangerven L, Hespel P. Long-term creatine intake is beneficial to muscle performance during resistance training. J Appl Physiol 1997;83:2055-63.
18. Greenhaff PL. Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5(suppl):S100-10.
19. The Cochrane Collaboration. The Cochrane Handbook (Online). Available at: http://www.cochrane.dk/cochrane/handbook/hbook CONTENTS__6_ASSESSMENT_OF_STUDY_.htm. Accessed June 2001.
20. Rawson ES, Clarkson PM. Acute creatine supplementation in older men. Int J Sports Med 2000;21(1):71-5.
21. Rawson ES, Wehnert ML, Clarkson PM. Effects of 30 days of creatine ingestion in older men. Eur J Appl Physiol 1999;80(2):139-44.
22. Becque MD, Lochmann JD, Melrose DR. Effects of oral creatine supplementation on muscular strength and body composition. Med Sci Sports Exerc 2000;32(3):654-8.
23. Stone MH, Sanborn K, Smith LL, O’Bryant HS, Hoke T, Utter AC, et al. Effects of in-season (5 weeks) creatine and pyruvate supplementation on anaerobic performance and body composition in American football players. Int J Sport Nutr 1999;9(2):146-65.
24. Jones AM, Atter T, Georg KP. Oral creatine supplementation improves multiple sprint performance in elite ice-hockey players. J Sports Med Phys Fitness 1999;39(3):189-96.
25. Dawson B, Cutler M, Moody A, Lawrence S, Goodman C, Randall N. Effects of oral creatine loading on single and repeated maximal short sprints. Aust J Sci Med Sport 1995;27(3):56-61.
26. Gilliam JD, Hohzorn C, Martin D, Trimble MH. Effect of oral creatine supplementation on isokinetic torque production. Med Sci Sports Exerc 2000;32(5):993-6.
27. Pearson DR, Hamby DG, Russel W, Harris T. Long-term effects of creatine monohydrate on strength and power. J Strength Cond Res 1999;13(3):187-92.
28. Volek JS, Duncan ND, Mazzetti SA, Staron RS, Putukian M, Gomez AL, et al. Performance and muscle fiber adaptations to creatine supplementation and heavy resistance training. Med Sci Sports Exerc 1999;31(8):1147-56.
29. Barnett C, Hinds M, Jenkins DG. Effects of oral creatine supplementation on multiple sprint cycle performance. Aust J Sci Med Sport 1996;28(1):35-9.
30. Cooke WH, Grandjean PW, Barnes WS. Effect of oral creatine supplementation on power output and fatigue during bicycle ergometry. J Appl Physiol 1995;78:670-3.
31. Cooke WH, Barnes WS. The influence of recovery duration on high-intensity exercise performance after oral creatine supplementation. Can J Appl Physiol 1997;22(5):454-67.
32. Kelly VG, Jenkins DG. Effect of oral creatine supplementation on near-maximal strength and repeated sets of high-intensity bench press exercise. J Strength Cond Res 1998;12(2):109-15.
33. Noonan D, Berg K, Latin RW, Wagner JC, Reimers K. Effects of varying dosages of oral creatine relative to fat free body mass on strength and body composition. J Strength Cond Res 1998;12(2):104-8.
34. Peeters BM, Lantz CD, Mayhew JL. Effect of oral creatine monohydrate and creatine phosphate supplementation on maximal strength indices, body composition, and blood pressure. J Strength Cond Res 1999;13(1):3-9.
35. Juhn MS, Tarnopolsky M. Potential side effects of oral creatine supplementation: a critical review. Clin J Sport Med 1998;8(4):298-304.
36. Poortmans JR, Francaux M. Long-term oral creatine supplementation does not impair renal function in healthy athletes. Med Sci Sports Exerc 1999;31(8):1108-10.
37. Schilling BK, Stone MH, Utter A, Kearney JT, Johnson M, Coglianese R, et al. Creatine supplementation and health variables: a retrospective study. Med Sci Sports Exerc 2001;33(2):183-8.
38. Pritchard NR, Kalra PA. Renal dysfunction accompanying oral creatine supplementation [letter]. Lancet 1998;351:125-23.
39. Koshy KM, Griswold E, Schneeberger EE. Interstitial nephritis in a patient taking creatine [letter]. New Engl J Med 1999;340:814-5.
40. Kuehl KS, Goldberg L, Elliot D. Renal insufficiency after creatine supplementation in a college football athlete [abstract]. Med Sci Sports Exerc 1998;30(suppl 5):S235.-
41. United States Food and Drug Administration The Special Nutritionals Adverse Event Monitoring System. Available at: http://vm.cfsan.fda.gov/cgibin/aems.cgi?QUERY= creatine&STYPE =EXACT. Accessed March 3, 2001.
- Oral creatine supplementation combined with resistance training increases maximal weight young men can lift.
- It is unknown whether this increase in strength translates into improvement in sports performance.
- Evidence in the existing literature is insufficient to draw conclusions about the effect of creatine in women or older individuals.
- Because no long-term studies have been performed on the safety of creatine supplementation, its use should not be universally recommended.
Creatine has gained widespread popularity during the past decade as a possible performance-enhancing agent among professional and recreational athletes. It is the most widely used performance-enhancing supplement among youth aged 10 to 17 years,1 with 15% to 30% of high school athletes2,3 and 48% of male Division I college athletes4 reporting creatine use. Considered a nutritional supplement, it is not regulated by the United States Food and Drug Administration nor is it banned by the International Olympic Committee or National Collegiate Athletic Association. Because of the widespread use of creatine, primary care providers must be knowledgeable about its effectiveness and safety.
Oral creatine monohydrate increases skeletal muscle creatine concentration by 16% to 50%,5-7 but whether it is an effective ergogenic aid remains controversial. Multiple studies have investigated this question, but many have been small, often including fewer than 10 subjects, and results have been conflicting. Several reviews8-14 have addressed the effectiveness of creatine, but there has not been a systematic and comprehensive meta-analysis to resolve the uncertainties in the literature or to quantify the magnitude of the effect of creatine. To evaluate whether oral creatine supplementation improves strength and power in healthy adults, and further to quantify the effect, we performed a meta-analysis of randomized and matched controlled trials investigating creatine supplementation and strength.
Methods
Search strategy
To identify possible studies for inclusion, 1 author (M.F.M.) searched the MEDLINE electronic database (1966–2000) using the terms “creatine supplementation” or “creatine” combined with “strength” or “power.” Another MEDLINE search (1966–2000) was independently conducted by another author (R.L.D.) using the term “creatine not kinase” combined with a previously published search strategy to comprehensively identify randomized clinical trials.15 We searched the Cochrane Controlled Trials Register using the term “creatine not kinase.” We manually reviewed bibliographies of identified studies, abstracts from American College of Sports Medicine annual meetings (1999 and 2000), and a reference list distributed by an expert on the subject at the annual meeting of the American Medical Society for Sports Medicine (2000). Titles and available abstracts were screened and relevant articles retrieved. An expert in the field was contacted for sources of unpublished data.
Inclusion and exclusion criteria
Two reviewers independently assessed articles for inclusion. A third reviewer was consulted to resolve discrepancies. We used the following inclusion criteria: (1) the articles reported results of randomized or matched placebo-controlled trials investigating the effect of oral creatine supplementation on strength or power with or without concomitant resistance training; (2) the study subjects were healthy men or women older than 16 years with or without previous athletic training; and (3) the studies were published in any language. Given the general disagreement regarding the time required for muscle creatine concentration to return to presupplementation levels after discontinuing oral creatine,16-18 studies using a crossover design were excluded from the statistical analysis unless data from the first arm, before crossover, could be abstracted or obtained from the original investigator. Outcomes were measures of strength or power of any muscle group, including maximal weight lifted; peak power achieved in maximal (sprint) cycle ergometry; and peak knee flexion/extension torque in isokinetic dynamometer testing. Measurements of endurance, such as time to fatigue on cycle ergometer and number of repetitions achieved in submaximal weight lifting, were excluded. For studies reporting outcome per kilogram of body weight, we contacted investigators to obtain absolute outcome values and excluded studies if uncorrected data were not received. We also excluded articles that evaluated outcomes not investigated in at least 2 other studies. Finally, if we could not extract data in a usable form, we contacted investigators to obtain adequate data.
Quality assessment
Two independent reviewers appraised articles to determine methodological quality with respect to risk of bias under the following categories: method of randomization, allocation concealment, blinding, similarity of study groups, withdrawals and dropouts, and intention-to-treat analysis. Each study that met inclusion criteria was given a quality score, with a maximum possible score of 10, using a tool adapted from the Cochrane Handbook.19 The quality assessment data are presented but were not used to exclude or rank any study.
Data abstraction and statistical analysis
Two independent reviewers abstracted data, and a third reviewer resolved differences. For studies investigating multiple sprints, data from the first sprint only were included in statistical analysis because the first sprint is when peak power achievement is expected. A weighted mean difference (WMD) between creatine and placebo groups was calculated for each outcome using Review Manager 4.1 software (developed by The Cochrane Collaboration). A fixed effects model was used unless statistical heterogeneity was significant (P < .05), in which case a random effects model was used. Subanalyses were planned on several factors that were anticipated to be sources for variation, including (1) dose and duration of creatine administration, (2) concomitant resistance training, (3) different baseline level of physical training, (4) age, and (5) sex.
Results
Description of studies
After reviewing titles and available abstracts of more than 500 articles, we retrieved 66 potentially relevant studies, 16 of which met inclusion criteria for the analysis.17,20-34 Characteristics of these studies are summarized in the Table. Included studies represented 20 discrete samples and 414 subjects. Two studies20,21 evaluated creatine supplementation in men older than 60 years, whereas all the others studied younger subjects (range, 18–36 years). Only 1 study included women.17 Creatine dosages were similar across included studies (typically 20 g/d for the first 4–7 days of supplementation and 5 g/d thereafter). Studies that evaluated maximal weight lifting performance were more likely to include adjuvant resistance training programs in their protocols than those that evaluated cycle ergometry sprint or isokinetic dynamometer performance. None included cycle ergometry training.
TABLE
Characteristics of included studies
| Reference | No. subjects (sex) | Dose per day and duration | Training level | Weight training during study? | Outcome measurement | Quality score (out of 10) | Comparability of creatine & placebo groups at baseline* |
|---|---|---|---|---|---|---|---|
| Barnett 1996 | 17 (M) | 280 mg/kg ×4 d | Active | No | CP | 2.5 | + |
| Cooke 1995 | 12 (M) | 20 g ×5 d | Untrained | No | CP | 2.5 | + |
| Cooke 1997† | 80 (M) | 20 g ×5 d | Trained or active | No | CP | 2 | +++ |
| Dawson 1995‡ | 18 (M), 22(M) | 20 g ×5 d | Active | No | CP | 3 | +++ |
| Jones 1999 | 16 (M) | 20 g ×5 d then 5 g ×10 wk | Trained | Yes | CM | 3 | +++ |
| Stone 1999 | 20 (M) | 0.22 g/kg ×35 d | Trained | Yes | CM, BP, S | 4.5 | +++ |
| Kelly 1998 | 18 (M) | 20 g ×5 d then 5 g ×26 d | Trained | Yes | 3BP | 2 | – |
| Noonan 1998 | 39 (M) | 20 g ×5 d then 300 mg/kg ×8 wk | Trained | Yes | BP | 5.5 | +++ |
| Peeters 1999 | 35 (M) | 20 g ×3 d then 10 g ×6 wk | Trained | Yes | BP | 3 | +++ |
| Vandenberghe 1997 | 19 (F) | 20 g ×4 d then 5 g ×10 wk | Untrained | Yes | BP, S | 5 | +++ |
| Pearson 1999 | 16 (M) | 5 g ×10 wk | Trained | Yes | BP, S, PT | 3 | +++ |
| Volek 1999 | 19 (M) | 25 g ×7 d then 5 g ×12 wk | Trained | Yes | BP, S | 4.5 | +++ |
| Gilliam 2000 | 23 (M) | 20 g ×5 d | Active but untrained | No | PT | 2.5 | + |
| Rawson 1999§ | 20 (M) | 20 g ×10 d then 4 g ×20 d | Untrained | No | AF, PT | 4.5 | +++ |
| Rawson 2000§ | 17 (M) | 20 g ×5 d | Untrained | No | AF | 3.5 | +++ |
| Becque 2000 | 23 (M) | 20 g ×5 d then 2 g ×6 wk | Trained | Yes | AF | 5 | + |
| *Comparability between groups was assessed for age, anthropomorphic measurements, and strength outcomes. +++ = similar for all 3 characteristics; + = similar for strength outcome measurements; – = not comparable at baseline for strength outcome. | |||||||
| †Four protocols with 20 subjects each evaluating the same strength outcome measurement reported in Cooke 1997. | |||||||
| ‡Two separate experiments reported in Dawson 1995. | |||||||
| §Included subjects > 60 years old; in all others subjects were < 36 years old. | |||||||
| AF, 1 repetition maximum arm flexor strength; BP, 1 repetition maximum bench press strength; 3BP, 3 repetition maximum bench press strength; CM, cycle ergometer mean peak power; CP, cycle ergometer peak power; PT, isokinetic leg flexion/extension peak torque; S, 1 repetition maximum squat strength. | |||||||
Methodological quality of included studies
The methodological quality of studies was generally low (Table). The mean quality score was 3.5 ± 1.2 (mean ± SD) out of a possible 10 (range, 2–5.5). None of the studies identified the method of randomization used or specifically reported an intention-to-treat analysis. None specifically reported masking of outcome assessment. In general, these significant flaws in study design would tend to result in overestimation of the benefit of creatine supplementation.
Absolute strength
When 1- to 3-repetition maximum bench press strength measurements were statistically combined (they were homogeneous), the creatine supplementation group showed an absolute strength increase of 6.85 kg (95% confidence interval [CI], 5.24–8.47; n = 143) lifted per repetition greater than that seen with placebo alone (Figure 1). There was no additional advantage in strength performance after 9 to 12 weeks of supplementation (WMD = 6.6 kg; 95% CI, 3.5–9.5) compared with 4 to 8 weeks of supplementation (WMD = 6.6 kg; 95% CI, 4.8–8.4). Subanalysis for an interaction with resistance training, previous training level, age, or sex was not possible because all studies measuring bench press strength except one17 investigated creatine supple mentation in previously trained young men who continued resistance training during supplementation. The 1 study in previously sedentary young women17 did find a trend toward increased bench press strength, although independently this change was not statistically significant.
There was no significant difference in 1-repetition maximum arm flexor strength with creatine supplementation (WMD = 1.53 kg; 95% CI, –1.07 to 4.13; n = 60; Figure 2). However, 2 trials20,21 of the 3 evaluating this outcome studied subjects older than 60 years and did not employ adjuvant weight training programs. The study that incorporated resistance training and evaluated younger subjects22 found a modest (29.9% vs 16.5%) improvement in 1-repetition maximum arm flexor strength with creatine compared with placebo.
For 1-repetition maximum squat, creatine supplementation resulted in a strength increase of 9.76 kg (95% CI, 3.37–16.15; n = 74) greater than that of placebo (Figure 3). There was no advantage to longer-term supplementation (10.9 kg more than placebo [95% CI, 3.4–18.4] for 5–6 weeks compared with 10.4 kg [95% CI, 3.5–17.2] for 10–12 weeks). Again, in all but 1 study17 measuring squat performance, subjects were previously trained young men engaging in adjuvant resistance training programs, so subanalysis for other variables was not possible. For previously sedentary women, Vandenberghe et al17 found no difference at 5 weeks, but they did find a significant improvement in 1-repetition maximum squat performance with creatine supplementation at 10 weeks. Tests for heterogeneity were nonsignificant for all absolute strength variables.
To evaluate for publication bias, we examined funnel plots of each of the 3 absolute strength outcomes (bench press, arm flexor, and squat exercises). No evidence of publication bias was demonstrated. Figure W1 (available on the JFP Web site: http://www.jfponline.com) depicts a composite funnel plot of all 3 outcomes using a standardized mean difference to allow comparison between these 3 different outcomes.
FIGURE 1 Studies assessing 1- to 3-repetition maximum bench press strength
FIGURE 2 Studies assessing 1-repetition maximum arm flexor strength
FIGURE 3 Studies assessing 1-repetition maximum squat strength
Cycle ergometer peak power
Creatine supplementation had no effect on peak power production during cycle ergometry sprint (Figure 4). Results among studies were widely variable (test for heterogeneity P= .035), so a random effects model was used to pool data. The summary weighted mean difference of 16.79 W (95% CI, –13.26 to 46.84; n = 149) was insignificant, both statistically (test for overall effect P= .3) and clinically, because this represents approximately a 1% change greater than baseline. Two studies23,24 looked at mean peak power across a series of 15-to 30-second sprints and found inconsistent results, with a summary weighted mean difference of 68.61 W (95% CI, –85.74 to 222.97; n = 36). Of note, for the 2 studies24,25 that demonstrated improved performance with creatine, the difference was accentuated by an unexplained but pronounced worsening of performance after supplementation in the placebo groups.
FIGURE 4 Studies assessing cycle ergometer sprint peak power
Dynamometer peak torque
Only 3 studies21,26,27 evaluated peak torque, and all used slightly different outcome assessments. One study26 reported average peak torque across 30 isokinetic leg flexion/extension contractions; 1 study21 reported the sum of peak torque across 5 sets of 30 isokinetic leg flexion/extension contractions; and 1 study27 gave peak torque data for isokinetic leg extension but did not describe precisely how peak torque was determined. There was no difference between creatine and placebo for isokinetic leg flexion/extension peak torque using a standardized mean difference to account for variations in measurement of this outcome. Tests for heterogeneity were nonsignificant for this outcome (P= .19).
Adverse effects
Four studies commented on short-term adverse effects of creatine supplementation. Three studies17,23,28 found no difference between creatine and placebo. One study21 reported gastrointestinal upset, rash, or headache in 3 subjects taking creatine and no adverse effects in subjects taking placebo. None of these studies was designed to evaluate long-term adverse effects of creatine supplementation, and there were no reports of longer-term follow up.
Discussion
This is the first study to report quantitatively the effect of creatine supplementation on strength performance from meta-analysis of the existing literature. We found that oral creatine supplementation improves maximal resistance exercise performance in previously trained young men. There is insufficient evidence that creatine improves other measures of strength, such as cycle ergometry sprint peak power or isokinetic dynamometer peak torque, or that creatine improves strength in women or older individuals. The effect of creatine on endurance, submaximal exercise, or actual “on-field” athletic performance was not addressed.
Creatine’s ergogenic properties may result from allowing increased work during training and decreasing recovery time. If so, creatine must be combined with adjuvant training to increase strength and power. Only studies investigating maximal weight-lifting performance incorporated resistance-training programs specific to the outcome being measured. Three studies included weight training but investigated non–weight-lifting outcomes,23,24,27 and only 1 study24 found a benefit from creatine supplementation. It is unclear whether the lack of effect for non–weight-lifting outcomes means that creatine is not beneficial unless combined with specific adjuvant training or that creatine simply is not ergogenic for outcomes other than maximal weight lifted.
This meta-analysis has some limitations. Our definition of strength included only “pure strength” or “power” measurements to allow statistical comparisons between similar outcomes. Because muscle strength is related to muscle endurance, researchers may define strength differently. It is not obvious at what point an exercise becomes a test of endurance and not just strength, but there is a physiologic basis for believing that creatine supplementation would more markedly improve performance in maximal or shorter duration exercises (ie, requiring strength and not endurance). The inclusion criteria for this project were determined before study review and selection and were applied consistently across all studies.
The quality and design of identified studies was another limitation. Most were small and did not fully delineate their randomization or blinding strategies. Multiple variations in study protocols made combining results of different studies somewhat problematic. Unfortunately, meta-regression or subanalysis for variables such as concurrent resistance training, previous training level, age, and sex were not possible because too few studies evaluated these variables independently of one another. Almost all of the studies finding a benefit of creatine supplementation were in young, previously trained men who engaged in resistance training concomitantly with supplementation, and the outcome measured was maximal weight lifted. Those studies not finding a difference were generally of less highly trained or older individuals, did not include resistance training, and more often investigated outcomes other than maximal weight lifted. This meta-analysis identifies that it is impossible to conclude from the existing literature which combination of variables is necessary to see a benefit of creatine supplementation.
More information is needed on the safety of creatine supplementation. Although a recent review35 reported no significant short-term adverse effects, no adequate long-term studies have been conducted. Two retrospective trials36,37 reported no adverse effects from longer-term (up to 5 years) creatine supplementation;however, neither study was randomized, blinded, or controlled, and neither had sufficient statistical power to detect uncommon adverse effects. Additionally, the designs of these studies precluded the possibility of detecting serious adverse effects such as death or disability. There have been case reports of renal dysfunction due to creatine38-40 and, as of 1998, the Food and Drug Administration had received 32 adverse event reports including seizures, myopathy, rhabdomyolosis, cardiac arrhythmia, and death.41
Given the popularity of nutritional supplements among all levels of athletes, clinicians cannot avoid questions about the effectiveness and safety of creatine supplementation. This meta-analysis demonstrated that oral creatine does improve performance during maximal resistance exercises in young men. However, we found no benefit for outcomes other than maximal weight lifted, suggesting that creatine may not improve actual performance in more complex movements requiring strength, speed, and coordination of multiple muscle groups. Studies investigating the effect of creatine in actual athletic performance are lacking.
Several important questions remain to be answered about creatine. What are the effects for women and older individuals? Is resistance training necessary to see strength performance improvement? Are these improvements in strength accompanied by improved athletic performance? How long do the effects of creatine remain after discontinuing supplementation? Most importantly, what is the long-term safety profile of creatine? Without further research to answer these questions, we cannot support the use of creatine supplementation for performance enhancement despite evidence for a positive impact on some components of strength.
Drug therapy for prevention and treatment of postmenopausal osteoporosis
| Drug (trade name) | Indication and dosage | Possible side effects (% of patients) | Cost per month* |
|---|---|---|---|
| Calcium and vitamin D (generic,Tums,Citracal, and others) | Prevention and treatment: 1200 –1500 mg/day calcium and 800 IU/day vitamin D | Nausea,dyspepsia (uncommon), constipation (10%) | $5 (both) |
| Estrogen †(Premarin,Ogen,Estrace, Estraderm,and others) | Prevention: 0.625 mg/day conjugated equine estrogen or the equivalent;0.3 mg/day may be effective | Nausea,breast tenderness, vaginal bleeding, mood alterations, headache, bloating | $14 –$28 |
| Alendronate (Fosamax) | Prevention:5 mg/day or 35 mg/week Treatment:10 mg/day or 70 mg/wk | Nausea, dyspepsia, esophageal irritation | $67 |
| Risedronate (Actonel) | Prevention and treatment: 5 mg/day or 35 mg/week | Abdominal pain, esophageal irritation | $67 |
| Raloxifene (Evista) | Treatment: 60 mg/day | Hot flashes (6%), leg cramps (3%) | $70 |
| Calcitonin nasal spray (Miacalcin) | Treatment:200 IU/day (1 spray in 1 nostril per day) | Rhinitis (5%), epistaxis, sinusitis | $66 |
| *Average wholesale cost to the pharmacy for 30 days of therapy; (Drug Topics Red Book. Montvale, NJ; Medical Economics Co., Inc, 2002.) | |||
| †Women with a uterus need to take a progestin such as medroxyprogesterone acetate (Provera $30/month, generic $9/month) or a combination estrogen/progestin product (Prempro $33/monh, FemHRT $26/month). | |||
On page 868 of the October issue a name was misspelled; the correct name is Brian S. Alper.
In the table appearing on page 877 of the October issue, the entry for Fosamax inadvertently combined prevention and treatment dosages. The corrected entry is shown below.
· Acknowledgments ·
This study was supported in part by a Faculty Development in Family Medicine Grant (No. 5D45 PE 55052-09) and a National Research Service Award Grant (No. 1T32 PE 10030-03) from the United States Department of Health and Human Services. The authors thank Craig Young, MD, who assisted in the conception of this project; Chris McLaughlin, who provided editorial assistance; and Veronica Ruleford, who assisted with the preparation of the manuscript.
- Oral creatine supplementation combined with resistance training increases maximal weight young men can lift.
- It is unknown whether this increase in strength translates into improvement in sports performance.
- Evidence in the existing literature is insufficient to draw conclusions about the effect of creatine in women or older individuals.
- Because no long-term studies have been performed on the safety of creatine supplementation, its use should not be universally recommended.
Creatine has gained widespread popularity during the past decade as a possible performance-enhancing agent among professional and recreational athletes. It is the most widely used performance-enhancing supplement among youth aged 10 to 17 years,1 with 15% to 30% of high school athletes2,3 and 48% of male Division I college athletes4 reporting creatine use. Considered a nutritional supplement, it is not regulated by the United States Food and Drug Administration nor is it banned by the International Olympic Committee or National Collegiate Athletic Association. Because of the widespread use of creatine, primary care providers must be knowledgeable about its effectiveness and safety.
Oral creatine monohydrate increases skeletal muscle creatine concentration by 16% to 50%,5-7 but whether it is an effective ergogenic aid remains controversial. Multiple studies have investigated this question, but many have been small, often including fewer than 10 subjects, and results have been conflicting. Several reviews8-14 have addressed the effectiveness of creatine, but there has not been a systematic and comprehensive meta-analysis to resolve the uncertainties in the literature or to quantify the magnitude of the effect of creatine. To evaluate whether oral creatine supplementation improves strength and power in healthy adults, and further to quantify the effect, we performed a meta-analysis of randomized and matched controlled trials investigating creatine supplementation and strength.
Methods
Search strategy
To identify possible studies for inclusion, 1 author (M.F.M.) searched the MEDLINE electronic database (1966–2000) using the terms “creatine supplementation” or “creatine” combined with “strength” or “power.” Another MEDLINE search (1966–2000) was independently conducted by another author (R.L.D.) using the term “creatine not kinase” combined with a previously published search strategy to comprehensively identify randomized clinical trials.15 We searched the Cochrane Controlled Trials Register using the term “creatine not kinase.” We manually reviewed bibliographies of identified studies, abstracts from American College of Sports Medicine annual meetings (1999 and 2000), and a reference list distributed by an expert on the subject at the annual meeting of the American Medical Society for Sports Medicine (2000). Titles and available abstracts were screened and relevant articles retrieved. An expert in the field was contacted for sources of unpublished data.
Inclusion and exclusion criteria
Two reviewers independently assessed articles for inclusion. A third reviewer was consulted to resolve discrepancies. We used the following inclusion criteria: (1) the articles reported results of randomized or matched placebo-controlled trials investigating the effect of oral creatine supplementation on strength or power with or without concomitant resistance training; (2) the study subjects were healthy men or women older than 16 years with or without previous athletic training; and (3) the studies were published in any language. Given the general disagreement regarding the time required for muscle creatine concentration to return to presupplementation levels after discontinuing oral creatine,16-18 studies using a crossover design were excluded from the statistical analysis unless data from the first arm, before crossover, could be abstracted or obtained from the original investigator. Outcomes were measures of strength or power of any muscle group, including maximal weight lifted; peak power achieved in maximal (sprint) cycle ergometry; and peak knee flexion/extension torque in isokinetic dynamometer testing. Measurements of endurance, such as time to fatigue on cycle ergometer and number of repetitions achieved in submaximal weight lifting, were excluded. For studies reporting outcome per kilogram of body weight, we contacted investigators to obtain absolute outcome values and excluded studies if uncorrected data were not received. We also excluded articles that evaluated outcomes not investigated in at least 2 other studies. Finally, if we could not extract data in a usable form, we contacted investigators to obtain adequate data.
Quality assessment
Two independent reviewers appraised articles to determine methodological quality with respect to risk of bias under the following categories: method of randomization, allocation concealment, blinding, similarity of study groups, withdrawals and dropouts, and intention-to-treat analysis. Each study that met inclusion criteria was given a quality score, with a maximum possible score of 10, using a tool adapted from the Cochrane Handbook.19 The quality assessment data are presented but were not used to exclude or rank any study.
Data abstraction and statistical analysis
Two independent reviewers abstracted data, and a third reviewer resolved differences. For studies investigating multiple sprints, data from the first sprint only were included in statistical analysis because the first sprint is when peak power achievement is expected. A weighted mean difference (WMD) between creatine and placebo groups was calculated for each outcome using Review Manager 4.1 software (developed by The Cochrane Collaboration). A fixed effects model was used unless statistical heterogeneity was significant (P < .05), in which case a random effects model was used. Subanalyses were planned on several factors that were anticipated to be sources for variation, including (1) dose and duration of creatine administration, (2) concomitant resistance training, (3) different baseline level of physical training, (4) age, and (5) sex.
Results
Description of studies
After reviewing titles and available abstracts of more than 500 articles, we retrieved 66 potentially relevant studies, 16 of which met inclusion criteria for the analysis.17,20-34 Characteristics of these studies are summarized in the Table. Included studies represented 20 discrete samples and 414 subjects. Two studies20,21 evaluated creatine supplementation in men older than 60 years, whereas all the others studied younger subjects (range, 18–36 years). Only 1 study included women.17 Creatine dosages were similar across included studies (typically 20 g/d for the first 4–7 days of supplementation and 5 g/d thereafter). Studies that evaluated maximal weight lifting performance were more likely to include adjuvant resistance training programs in their protocols than those that evaluated cycle ergometry sprint or isokinetic dynamometer performance. None included cycle ergometry training.
TABLE
Characteristics of included studies
| Reference | No. subjects (sex) | Dose per day and duration | Training level | Weight training during study? | Outcome measurement | Quality score (out of 10) | Comparability of creatine & placebo groups at baseline* |
|---|---|---|---|---|---|---|---|
| Barnett 1996 | 17 (M) | 280 mg/kg ×4 d | Active | No | CP | 2.5 | + |
| Cooke 1995 | 12 (M) | 20 g ×5 d | Untrained | No | CP | 2.5 | + |
| Cooke 1997† | 80 (M) | 20 g ×5 d | Trained or active | No | CP | 2 | +++ |
| Dawson 1995‡ | 18 (M), 22(M) | 20 g ×5 d | Active | No | CP | 3 | +++ |
| Jones 1999 | 16 (M) | 20 g ×5 d then 5 g ×10 wk | Trained | Yes | CM | 3 | +++ |
| Stone 1999 | 20 (M) | 0.22 g/kg ×35 d | Trained | Yes | CM, BP, S | 4.5 | +++ |
| Kelly 1998 | 18 (M) | 20 g ×5 d then 5 g ×26 d | Trained | Yes | 3BP | 2 | – |
| Noonan 1998 | 39 (M) | 20 g ×5 d then 300 mg/kg ×8 wk | Trained | Yes | BP | 5.5 | +++ |
| Peeters 1999 | 35 (M) | 20 g ×3 d then 10 g ×6 wk | Trained | Yes | BP | 3 | +++ |
| Vandenberghe 1997 | 19 (F) | 20 g ×4 d then 5 g ×10 wk | Untrained | Yes | BP, S | 5 | +++ |
| Pearson 1999 | 16 (M) | 5 g ×10 wk | Trained | Yes | BP, S, PT | 3 | +++ |
| Volek 1999 | 19 (M) | 25 g ×7 d then 5 g ×12 wk | Trained | Yes | BP, S | 4.5 | +++ |
| Gilliam 2000 | 23 (M) | 20 g ×5 d | Active but untrained | No | PT | 2.5 | + |
| Rawson 1999§ | 20 (M) | 20 g ×10 d then 4 g ×20 d | Untrained | No | AF, PT | 4.5 | +++ |
| Rawson 2000§ | 17 (M) | 20 g ×5 d | Untrained | No | AF | 3.5 | +++ |
| Becque 2000 | 23 (M) | 20 g ×5 d then 2 g ×6 wk | Trained | Yes | AF | 5 | + |
| *Comparability between groups was assessed for age, anthropomorphic measurements, and strength outcomes. +++ = similar for all 3 characteristics; + = similar for strength outcome measurements; – = not comparable at baseline for strength outcome. | |||||||
| †Four protocols with 20 subjects each evaluating the same strength outcome measurement reported in Cooke 1997. | |||||||
| ‡Two separate experiments reported in Dawson 1995. | |||||||
| §Included subjects > 60 years old; in all others subjects were < 36 years old. | |||||||
| AF, 1 repetition maximum arm flexor strength; BP, 1 repetition maximum bench press strength; 3BP, 3 repetition maximum bench press strength; CM, cycle ergometer mean peak power; CP, cycle ergometer peak power; PT, isokinetic leg flexion/extension peak torque; S, 1 repetition maximum squat strength. | |||||||
Methodological quality of included studies
The methodological quality of studies was generally low (Table). The mean quality score was 3.5 ± 1.2 (mean ± SD) out of a possible 10 (range, 2–5.5). None of the studies identified the method of randomization used or specifically reported an intention-to-treat analysis. None specifically reported masking of outcome assessment. In general, these significant flaws in study design would tend to result in overestimation of the benefit of creatine supplementation.
Absolute strength
When 1- to 3-repetition maximum bench press strength measurements were statistically combined (they were homogeneous), the creatine supplementation group showed an absolute strength increase of 6.85 kg (95% confidence interval [CI], 5.24–8.47; n = 143) lifted per repetition greater than that seen with placebo alone (Figure 1). There was no additional advantage in strength performance after 9 to 12 weeks of supplementation (WMD = 6.6 kg; 95% CI, 3.5–9.5) compared with 4 to 8 weeks of supplementation (WMD = 6.6 kg; 95% CI, 4.8–8.4). Subanalysis for an interaction with resistance training, previous training level, age, or sex was not possible because all studies measuring bench press strength except one17 investigated creatine supple mentation in previously trained young men who continued resistance training during supplementation. The 1 study in previously sedentary young women17 did find a trend toward increased bench press strength, although independently this change was not statistically significant.
There was no significant difference in 1-repetition maximum arm flexor strength with creatine supplementation (WMD = 1.53 kg; 95% CI, –1.07 to 4.13; n = 60; Figure 2). However, 2 trials20,21 of the 3 evaluating this outcome studied subjects older than 60 years and did not employ adjuvant weight training programs. The study that incorporated resistance training and evaluated younger subjects22 found a modest (29.9% vs 16.5%) improvement in 1-repetition maximum arm flexor strength with creatine compared with placebo.
For 1-repetition maximum squat, creatine supplementation resulted in a strength increase of 9.76 kg (95% CI, 3.37–16.15; n = 74) greater than that of placebo (Figure 3). There was no advantage to longer-term supplementation (10.9 kg more than placebo [95% CI, 3.4–18.4] for 5–6 weeks compared with 10.4 kg [95% CI, 3.5–17.2] for 10–12 weeks). Again, in all but 1 study17 measuring squat performance, subjects were previously trained young men engaging in adjuvant resistance training programs, so subanalysis for other variables was not possible. For previously sedentary women, Vandenberghe et al17 found no difference at 5 weeks, but they did find a significant improvement in 1-repetition maximum squat performance with creatine supplementation at 10 weeks. Tests for heterogeneity were nonsignificant for all absolute strength variables.
To evaluate for publication bias, we examined funnel plots of each of the 3 absolute strength outcomes (bench press, arm flexor, and squat exercises). No evidence of publication bias was demonstrated. Figure W1 (available on the JFP Web site: http://www.jfponline.com) depicts a composite funnel plot of all 3 outcomes using a standardized mean difference to allow comparison between these 3 different outcomes.
FIGURE 1 Studies assessing 1- to 3-repetition maximum bench press strength
FIGURE 2 Studies assessing 1-repetition maximum arm flexor strength
FIGURE 3 Studies assessing 1-repetition maximum squat strength
Cycle ergometer peak power
Creatine supplementation had no effect on peak power production during cycle ergometry sprint (Figure 4). Results among studies were widely variable (test for heterogeneity P= .035), so a random effects model was used to pool data. The summary weighted mean difference of 16.79 W (95% CI, –13.26 to 46.84; n = 149) was insignificant, both statistically (test for overall effect P= .3) and clinically, because this represents approximately a 1% change greater than baseline. Two studies23,24 looked at mean peak power across a series of 15-to 30-second sprints and found inconsistent results, with a summary weighted mean difference of 68.61 W (95% CI, –85.74 to 222.97; n = 36). Of note, for the 2 studies24,25 that demonstrated improved performance with creatine, the difference was accentuated by an unexplained but pronounced worsening of performance after supplementation in the placebo groups.
FIGURE 4 Studies assessing cycle ergometer sprint peak power
Dynamometer peak torque
Only 3 studies21,26,27 evaluated peak torque, and all used slightly different outcome assessments. One study26 reported average peak torque across 30 isokinetic leg flexion/extension contractions; 1 study21 reported the sum of peak torque across 5 sets of 30 isokinetic leg flexion/extension contractions; and 1 study27 gave peak torque data for isokinetic leg extension but did not describe precisely how peak torque was determined. There was no difference between creatine and placebo for isokinetic leg flexion/extension peak torque using a standardized mean difference to account for variations in measurement of this outcome. Tests for heterogeneity were nonsignificant for this outcome (P= .19).
Adverse effects
Four studies commented on short-term adverse effects of creatine supplementation. Three studies17,23,28 found no difference between creatine and placebo. One study21 reported gastrointestinal upset, rash, or headache in 3 subjects taking creatine and no adverse effects in subjects taking placebo. None of these studies was designed to evaluate long-term adverse effects of creatine supplementation, and there were no reports of longer-term follow up.
Discussion
This is the first study to report quantitatively the effect of creatine supplementation on strength performance from meta-analysis of the existing literature. We found that oral creatine supplementation improves maximal resistance exercise performance in previously trained young men. There is insufficient evidence that creatine improves other measures of strength, such as cycle ergometry sprint peak power or isokinetic dynamometer peak torque, or that creatine improves strength in women or older individuals. The effect of creatine on endurance, submaximal exercise, or actual “on-field” athletic performance was not addressed.
Creatine’s ergogenic properties may result from allowing increased work during training and decreasing recovery time. If so, creatine must be combined with adjuvant training to increase strength and power. Only studies investigating maximal weight-lifting performance incorporated resistance-training programs specific to the outcome being measured. Three studies included weight training but investigated non–weight-lifting outcomes,23,24,27 and only 1 study24 found a benefit from creatine supplementation. It is unclear whether the lack of effect for non–weight-lifting outcomes means that creatine is not beneficial unless combined with specific adjuvant training or that creatine simply is not ergogenic for outcomes other than maximal weight lifted.
This meta-analysis has some limitations. Our definition of strength included only “pure strength” or “power” measurements to allow statistical comparisons between similar outcomes. Because muscle strength is related to muscle endurance, researchers may define strength differently. It is not obvious at what point an exercise becomes a test of endurance and not just strength, but there is a physiologic basis for believing that creatine supplementation would more markedly improve performance in maximal or shorter duration exercises (ie, requiring strength and not endurance). The inclusion criteria for this project were determined before study review and selection and were applied consistently across all studies.
The quality and design of identified studies was another limitation. Most were small and did not fully delineate their randomization or blinding strategies. Multiple variations in study protocols made combining results of different studies somewhat problematic. Unfortunately, meta-regression or subanalysis for variables such as concurrent resistance training, previous training level, age, and sex were not possible because too few studies evaluated these variables independently of one another. Almost all of the studies finding a benefit of creatine supplementation were in young, previously trained men who engaged in resistance training concomitantly with supplementation, and the outcome measured was maximal weight lifted. Those studies not finding a difference were generally of less highly trained or older individuals, did not include resistance training, and more often investigated outcomes other than maximal weight lifted. This meta-analysis identifies that it is impossible to conclude from the existing literature which combination of variables is necessary to see a benefit of creatine supplementation.
More information is needed on the safety of creatine supplementation. Although a recent review35 reported no significant short-term adverse effects, no adequate long-term studies have been conducted. Two retrospective trials36,37 reported no adverse effects from longer-term (up to 5 years) creatine supplementation;however, neither study was randomized, blinded, or controlled, and neither had sufficient statistical power to detect uncommon adverse effects. Additionally, the designs of these studies precluded the possibility of detecting serious adverse effects such as death or disability. There have been case reports of renal dysfunction due to creatine38-40 and, as of 1998, the Food and Drug Administration had received 32 adverse event reports including seizures, myopathy, rhabdomyolosis, cardiac arrhythmia, and death.41
Given the popularity of nutritional supplements among all levels of athletes, clinicians cannot avoid questions about the effectiveness and safety of creatine supplementation. This meta-analysis demonstrated that oral creatine does improve performance during maximal resistance exercises in young men. However, we found no benefit for outcomes other than maximal weight lifted, suggesting that creatine may not improve actual performance in more complex movements requiring strength, speed, and coordination of multiple muscle groups. Studies investigating the effect of creatine in actual athletic performance are lacking.
Several important questions remain to be answered about creatine. What are the effects for women and older individuals? Is resistance training necessary to see strength performance improvement? Are these improvements in strength accompanied by improved athletic performance? How long do the effects of creatine remain after discontinuing supplementation? Most importantly, what is the long-term safety profile of creatine? Without further research to answer these questions, we cannot support the use of creatine supplementation for performance enhancement despite evidence for a positive impact on some components of strength.
Drug therapy for prevention and treatment of postmenopausal osteoporosis
| Drug (trade name) | Indication and dosage | Possible side effects (% of patients) | Cost per month* |
|---|---|---|---|
| Calcium and vitamin D (generic,Tums,Citracal, and others) | Prevention and treatment: 1200 –1500 mg/day calcium and 800 IU/day vitamin D | Nausea,dyspepsia (uncommon), constipation (10%) | $5 (both) |
| Estrogen †(Premarin,Ogen,Estrace, Estraderm,and others) | Prevention: 0.625 mg/day conjugated equine estrogen or the equivalent;0.3 mg/day may be effective | Nausea,breast tenderness, vaginal bleeding, mood alterations, headache, bloating | $14 –$28 |
| Alendronate (Fosamax) | Prevention:5 mg/day or 35 mg/week Treatment:10 mg/day or 70 mg/wk | Nausea, dyspepsia, esophageal irritation | $67 |
| Risedronate (Actonel) | Prevention and treatment: 5 mg/day or 35 mg/week | Abdominal pain, esophageal irritation | $67 |
| Raloxifene (Evista) | Treatment: 60 mg/day | Hot flashes (6%), leg cramps (3%) | $70 |
| Calcitonin nasal spray (Miacalcin) | Treatment:200 IU/day (1 spray in 1 nostril per day) | Rhinitis (5%), epistaxis, sinusitis | $66 |
| *Average wholesale cost to the pharmacy for 30 days of therapy; (Drug Topics Red Book. Montvale, NJ; Medical Economics Co., Inc, 2002.) | |||
| †Women with a uterus need to take a progestin such as medroxyprogesterone acetate (Provera $30/month, generic $9/month) or a combination estrogen/progestin product (Prempro $33/monh, FemHRT $26/month). | |||
On page 868 of the October issue a name was misspelled; the correct name is Brian S. Alper.
In the table appearing on page 877 of the October issue, the entry for Fosamax inadvertently combined prevention and treatment dosages. The corrected entry is shown below.
· Acknowledgments ·
This study was supported in part by a Faculty Development in Family Medicine Grant (No. 5D45 PE 55052-09) and a National Research Service Award Grant (No. 1T32 PE 10030-03) from the United States Department of Health and Human Services. The authors thank Craig Young, MD, who assisted in the conception of this project; Chris McLaughlin, who provided editorial assistance; and Veronica Ruleford, who assisted with the preparation of the manuscript.
1. USA Today. Survey: More than 1 million kids use sports supplements. USA Today. August 28, 2001. Available at: www.usatoday.com/news/nation/2001/08/28/youth-supplements.htm. Accessed October 8, 2002.
2. McGuine TA, Sullivan JC, Bernhardt DT. Creatine supplementation in high school football players. Clin J Sport Med 2001;11(4):247-53.
3. Ray TR, Eck JC, Covington LA, Murphy RB, Williams R, Knudtson J. Use of oral creatine as an ergogenic aid for increased sports performance: perceptions of adolescent athletes. South Med J 2001;94(6):608-12.
4. LaBotz M, Smith BW. Creatine supplement use in an NCAA Division I athletic program. Clin J Sport Med 1999;9(3):167-9.
5. Harris RC, Soderlund K, Hultman E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci 1992;83:367-74.
6. Vandenberghe K, Van Hecke P, Van Leemputte M, Vanstapel F, Hespel P. Phosphocreatine resynthesis is not affected by creatine loading. Med Sci Sports Exerc 1999;31(2):236-42.
7. Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. J Appl Physiol 1996;812:32-7.
8. Terjung RL, Clarkson P, Eichner ER, Greenhaff PL, Hespel PJ, Israel RG, et al. American College of Sports Medicine roundtable. The physiological and health effects of oral creatine supplementation. Med Sci Sports Exerc 2000;32(3):706-17.
9. Kreider RB. Dietary supplements and the promotion of muscle growth with resistance exercise. Sports Med 1999;27(2):97-110.
10. Mujika I, Padilla S. Creatine supplementation as an ergogenic aid for sports performance in highly trained athletes: a critical review. Int J Sports Med 1997;18(7):491-6.
11. Juhn MS, Tarnopolsky M. Oral creatine supplementation and athletic performance: a critical review. Clin J Sport Med 1998;8(4):286-97.
12. Volek JS, Kraemer WJ. Creatine supplementation: its effect on human muscular performance and body composition. J Strength Cond Res 1996;10(3):200-10.
13. Maughan RJ. Creatine supplementation and exercise performance. Int J Sport Nutr 1995;5:94-101.
14. Kraemer WJ, Volek JS. Creatine supplementation. Its role in human performance. Clin Sports Med 1999;18(3):651-66.
15. Dickersin K, Scherer R, Lefebvre C. Systematic reviews: identifying relevant studies for systematic reviews. Br Med J 1994;309(6964):1286-91.
16. Febbraio MA, Flanagan TR, Snow RJ, Zhao S, Carey MF. Effect of creatine supplementation on intramuscular TCr, metabolism and performance during intermittent, supramaximal exercise in humans. Acta Physiol Scand 1995;155(4):387-95.
17. Vandenberghe K, Goris M, Van Hecke P, Van Leemputte M, Vangerven L, Hespel P. Long-term creatine intake is beneficial to muscle performance during resistance training. J Appl Physiol 1997;83:2055-63.
18. Greenhaff PL. Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5(suppl):S100-10.
19. The Cochrane Collaboration. The Cochrane Handbook (Online). Available at: http://www.cochrane.dk/cochrane/handbook/hbook CONTENTS__6_ASSESSMENT_OF_STUDY_.htm. Accessed June 2001.
20. Rawson ES, Clarkson PM. Acute creatine supplementation in older men. Int J Sports Med 2000;21(1):71-5.
21. Rawson ES, Wehnert ML, Clarkson PM. Effects of 30 days of creatine ingestion in older men. Eur J Appl Physiol 1999;80(2):139-44.
22. Becque MD, Lochmann JD, Melrose DR. Effects of oral creatine supplementation on muscular strength and body composition. Med Sci Sports Exerc 2000;32(3):654-8.
23. Stone MH, Sanborn K, Smith LL, O’Bryant HS, Hoke T, Utter AC, et al. Effects of in-season (5 weeks) creatine and pyruvate supplementation on anaerobic performance and body composition in American football players. Int J Sport Nutr 1999;9(2):146-65.
24. Jones AM, Atter T, Georg KP. Oral creatine supplementation improves multiple sprint performance in elite ice-hockey players. J Sports Med Phys Fitness 1999;39(3):189-96.
25. Dawson B, Cutler M, Moody A, Lawrence S, Goodman C, Randall N. Effects of oral creatine loading on single and repeated maximal short sprints. Aust J Sci Med Sport 1995;27(3):56-61.
26. Gilliam JD, Hohzorn C, Martin D, Trimble MH. Effect of oral creatine supplementation on isokinetic torque production. Med Sci Sports Exerc 2000;32(5):993-6.
27. Pearson DR, Hamby DG, Russel W, Harris T. Long-term effects of creatine monohydrate on strength and power. J Strength Cond Res 1999;13(3):187-92.
28. Volek JS, Duncan ND, Mazzetti SA, Staron RS, Putukian M, Gomez AL, et al. Performance and muscle fiber adaptations to creatine supplementation and heavy resistance training. Med Sci Sports Exerc 1999;31(8):1147-56.
29. Barnett C, Hinds M, Jenkins DG. Effects of oral creatine supplementation on multiple sprint cycle performance. Aust J Sci Med Sport 1996;28(1):35-9.
30. Cooke WH, Grandjean PW, Barnes WS. Effect of oral creatine supplementation on power output and fatigue during bicycle ergometry. J Appl Physiol 1995;78:670-3.
31. Cooke WH, Barnes WS. The influence of recovery duration on high-intensity exercise performance after oral creatine supplementation. Can J Appl Physiol 1997;22(5):454-67.
32. Kelly VG, Jenkins DG. Effect of oral creatine supplementation on near-maximal strength and repeated sets of high-intensity bench press exercise. J Strength Cond Res 1998;12(2):109-15.
33. Noonan D, Berg K, Latin RW, Wagner JC, Reimers K. Effects of varying dosages of oral creatine relative to fat free body mass on strength and body composition. J Strength Cond Res 1998;12(2):104-8.
34. Peeters BM, Lantz CD, Mayhew JL. Effect of oral creatine monohydrate and creatine phosphate supplementation on maximal strength indices, body composition, and blood pressure. J Strength Cond Res 1999;13(1):3-9.
35. Juhn MS, Tarnopolsky M. Potential side effects of oral creatine supplementation: a critical review. Clin J Sport Med 1998;8(4):298-304.
36. Poortmans JR, Francaux M. Long-term oral creatine supplementation does not impair renal function in healthy athletes. Med Sci Sports Exerc 1999;31(8):1108-10.
37. Schilling BK, Stone MH, Utter A, Kearney JT, Johnson M, Coglianese R, et al. Creatine supplementation and health variables: a retrospective study. Med Sci Sports Exerc 2001;33(2):183-8.
38. Pritchard NR, Kalra PA. Renal dysfunction accompanying oral creatine supplementation [letter]. Lancet 1998;351:125-23.
39. Koshy KM, Griswold E, Schneeberger EE. Interstitial nephritis in a patient taking creatine [letter]. New Engl J Med 1999;340:814-5.
40. Kuehl KS, Goldberg L, Elliot D. Renal insufficiency after creatine supplementation in a college football athlete [abstract]. Med Sci Sports Exerc 1998;30(suppl 5):S235.-
41. United States Food and Drug Administration The Special Nutritionals Adverse Event Monitoring System. Available at: http://vm.cfsan.fda.gov/cgibin/aems.cgi?QUERY= creatine&STYPE =EXACT. Accessed March 3, 2001.
1. USA Today. Survey: More than 1 million kids use sports supplements. USA Today. August 28, 2001. Available at: www.usatoday.com/news/nation/2001/08/28/youth-supplements.htm. Accessed October 8, 2002.
2. McGuine TA, Sullivan JC, Bernhardt DT. Creatine supplementation in high school football players. Clin J Sport Med 2001;11(4):247-53.
3. Ray TR, Eck JC, Covington LA, Murphy RB, Williams R, Knudtson J. Use of oral creatine as an ergogenic aid for increased sports performance: perceptions of adolescent athletes. South Med J 2001;94(6):608-12.
4. LaBotz M, Smith BW. Creatine supplement use in an NCAA Division I athletic program. Clin J Sport Med 1999;9(3):167-9.
5. Harris RC, Soderlund K, Hultman E. Elevation of creatine in resting and exercised muscle of normal subjects by creatine supplementation. Clin Sci 1992;83:367-74.
6. Vandenberghe K, Van Hecke P, Van Leemputte M, Vanstapel F, Hespel P. Phosphocreatine resynthesis is not affected by creatine loading. Med Sci Sports Exerc 1999;31(2):236-42.
7. Hultman E, Soderlund K, Timmons JA, Cederblad G, Greenhaff PL. Muscle creatine loading in men. J Appl Physiol 1996;812:32-7.
8. Terjung RL, Clarkson P, Eichner ER, Greenhaff PL, Hespel PJ, Israel RG, et al. American College of Sports Medicine roundtable. The physiological and health effects of oral creatine supplementation. Med Sci Sports Exerc 2000;32(3):706-17.
9. Kreider RB. Dietary supplements and the promotion of muscle growth with resistance exercise. Sports Med 1999;27(2):97-110.
10. Mujika I, Padilla S. Creatine supplementation as an ergogenic aid for sports performance in highly trained athletes: a critical review. Int J Sports Med 1997;18(7):491-6.
11. Juhn MS, Tarnopolsky M. Oral creatine supplementation and athletic performance: a critical review. Clin J Sport Med 1998;8(4):286-97.
12. Volek JS, Kraemer WJ. Creatine supplementation: its effect on human muscular performance and body composition. J Strength Cond Res 1996;10(3):200-10.
13. Maughan RJ. Creatine supplementation and exercise performance. Int J Sport Nutr 1995;5:94-101.
14. Kraemer WJ, Volek JS. Creatine supplementation. Its role in human performance. Clin Sports Med 1999;18(3):651-66.
15. Dickersin K, Scherer R, Lefebvre C. Systematic reviews: identifying relevant studies for systematic reviews. Br Med J 1994;309(6964):1286-91.
16. Febbraio MA, Flanagan TR, Snow RJ, Zhao S, Carey MF. Effect of creatine supplementation on intramuscular TCr, metabolism and performance during intermittent, supramaximal exercise in humans. Acta Physiol Scand 1995;155(4):387-95.
17. Vandenberghe K, Goris M, Van Hecke P, Van Leemputte M, Vangerven L, Hespel P. Long-term creatine intake is beneficial to muscle performance during resistance training. J Appl Physiol 1997;83:2055-63.
18. Greenhaff PL. Creatine and its application as an ergogenic aid. Int J Sport Nutr 1995;5(suppl):S100-10.
19. The Cochrane Collaboration. The Cochrane Handbook (Online). Available at: http://www.cochrane.dk/cochrane/handbook/hbook CONTENTS__6_ASSESSMENT_OF_STUDY_.htm. Accessed June 2001.
20. Rawson ES, Clarkson PM. Acute creatine supplementation in older men. Int J Sports Med 2000;21(1):71-5.
21. Rawson ES, Wehnert ML, Clarkson PM. Effects of 30 days of creatine ingestion in older men. Eur J Appl Physiol 1999;80(2):139-44.
22. Becque MD, Lochmann JD, Melrose DR. Effects of oral creatine supplementation on muscular strength and body composition. Med Sci Sports Exerc 2000;32(3):654-8.
23. Stone MH, Sanborn K, Smith LL, O’Bryant HS, Hoke T, Utter AC, et al. Effects of in-season (5 weeks) creatine and pyruvate supplementation on anaerobic performance and body composition in American football players. Int J Sport Nutr 1999;9(2):146-65.
24. Jones AM, Atter T, Georg KP. Oral creatine supplementation improves multiple sprint performance in elite ice-hockey players. J Sports Med Phys Fitness 1999;39(3):189-96.
25. Dawson B, Cutler M, Moody A, Lawrence S, Goodman C, Randall N. Effects of oral creatine loading on single and repeated maximal short sprints. Aust J Sci Med Sport 1995;27(3):56-61.
26. Gilliam JD, Hohzorn C, Martin D, Trimble MH. Effect of oral creatine supplementation on isokinetic torque production. Med Sci Sports Exerc 2000;32(5):993-6.
27. Pearson DR, Hamby DG, Russel W, Harris T. Long-term effects of creatine monohydrate on strength and power. J Strength Cond Res 1999;13(3):187-92.
28. Volek JS, Duncan ND, Mazzetti SA, Staron RS, Putukian M, Gomez AL, et al. Performance and muscle fiber adaptations to creatine supplementation and heavy resistance training. Med Sci Sports Exerc 1999;31(8):1147-56.
29. Barnett C, Hinds M, Jenkins DG. Effects of oral creatine supplementation on multiple sprint cycle performance. Aust J Sci Med Sport 1996;28(1):35-9.
30. Cooke WH, Grandjean PW, Barnes WS. Effect of oral creatine supplementation on power output and fatigue during bicycle ergometry. J Appl Physiol 1995;78:670-3.
31. Cooke WH, Barnes WS. The influence of recovery duration on high-intensity exercise performance after oral creatine supplementation. Can J Appl Physiol 1997;22(5):454-67.
32. Kelly VG, Jenkins DG. Effect of oral creatine supplementation on near-maximal strength and repeated sets of high-intensity bench press exercise. J Strength Cond Res 1998;12(2):109-15.
33. Noonan D, Berg K, Latin RW, Wagner JC, Reimers K. Effects of varying dosages of oral creatine relative to fat free body mass on strength and body composition. J Strength Cond Res 1998;12(2):104-8.
34. Peeters BM, Lantz CD, Mayhew JL. Effect of oral creatine monohydrate and creatine phosphate supplementation on maximal strength indices, body composition, and blood pressure. J Strength Cond Res 1999;13(1):3-9.
35. Juhn MS, Tarnopolsky M. Potential side effects of oral creatine supplementation: a critical review. Clin J Sport Med 1998;8(4):298-304.
36. Poortmans JR, Francaux M. Long-term oral creatine supplementation does not impair renal function in healthy athletes. Med Sci Sports Exerc 1999;31(8):1108-10.
37. Schilling BK, Stone MH, Utter A, Kearney JT, Johnson M, Coglianese R, et al. Creatine supplementation and health variables: a retrospective study. Med Sci Sports Exerc 2001;33(2):183-8.
38. Pritchard NR, Kalra PA. Renal dysfunction accompanying oral creatine supplementation [letter]. Lancet 1998;351:125-23.
39. Koshy KM, Griswold E, Schneeberger EE. Interstitial nephritis in a patient taking creatine [letter]. New Engl J Med 1999;340:814-5.
40. Kuehl KS, Goldberg L, Elliot D. Renal insufficiency after creatine supplementation in a college football athlete [abstract]. Med Sci Sports Exerc 1998;30(suppl 5):S235.-
41. United States Food and Drug Administration The Special Nutritionals Adverse Event Monitoring System. Available at: http://vm.cfsan.fda.gov/cgibin/aems.cgi?QUERY= creatine&STYPE =EXACT. Accessed March 3, 2001.