User login
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
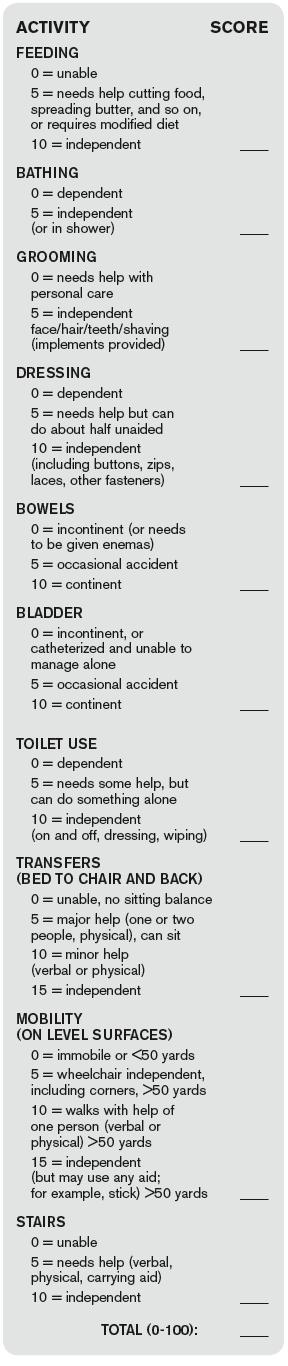
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.


References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.
References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.
“I didn’t get out of bed for 10 days”
—Anonymous patient admitted to a skilled nursing facility post-hospitalization for a COPD exacerbation
Readmission penalties, “Medicare spending per beneficiary” under value-based purchasing, and the move to accountable care are propelling hospitalists to do more to ensure our patients recover well in the least restrictive setting, without returning to the hospital. As we build systems to support patient recovery, we are focused on a medical model, paying attention to managing diseases and reconciling medications. At the same time, there is a growing awareness that functional status and mobility are critical pieces of patient care during and post-hospitalization.
Regardless of principal diagnosis and comorbidities, patients’ functional mobility ultimately determines their trajectory during recovery. To illustrate the importance of functional status and outcomes, one study showed that models predicting readmission based on functional measures outperformed those based on comorbidities.1
The negative effects of hospitalization on patient mobility, and in turn, on recovery, have been recognized for a long time. Immobility is associated with functional decline, which contributes to falls, increased length of stay, delirium, loss of ability to perform activities of daily living, and loss of ambulatory independence. A number of studies have reported successful early mobility programs in critical care and surgical patients.2 Fewer have been reported in general medical patients.3 Taken together, they suggest that a program for mobilizing patients, using a team approach, is an important part of recovery during and after hospitalization.
The purpose of this column is to report the components of one healthcare system’s mobility program for general medical-surgical patients.
Early Mobility: A Case Study
St Luke’s University Health Network (SLUHN) in northeastern Pennsylvania has implemented an early mobility program as part of its broader strategy to reduce readmissions and discharge as many patients home as possible. Although the SLUHN early mobility program depends on nursing, nursing assistants, and the judicious use of therapists, physician leadership during implementation and maintenance of the program has been essential. Moreover, because the program represents a culture shift, especially for nursing, leadership and change management are crucial ingredients for success. Below are the key steps in the SLUHN early mobility program.
Establish baseline functional status. Recording baseline function is an essential first step. For patients admitted through the ED, nurses collect ambulatory status, patient needs for assistance, ambulatory aids/special equipment, and history of falls. They populate an SBAR (situation, background, assessment, recommendation) form with this information and, as part of the handoff, ensure that it is transmitted to the inpatient nurse receiving the patient.
Obtain and document Barthel Index score. SLUHN uses the Barthel Index (see Figure 1) to establish a patient’s degree of independence and need for supervision. The index is scored on a 0-100 scale, with a higher score corresponding to a greater degree of independence. SLUHN created three categories: 0-59, stage 1; 60-84, stage 2; 85-100, stage 3.
Patient mobility plan. Based on the Barthel-derived stage, a patient is assigned a mobility plan.
The role of nursing. The patient’s registered nurse is responsible for implementing the “patient mobility plan.” The nurse initiates an “interdisciplinary plan of care,” in which the mobility stage is written on the SBAR handoff report tool. The report is discussed at change of shift and at multidisciplinary rounds. Nursing also communicates the mobility plan to the nursing assistants and assigns responsibilities for the mobility plan (activities of daily living, out of bed, ambulation, and so on), including verifying documentation of daily activities and assessing the patient’s response to the activity level of the assigned stage.
Further, nursing maintains and revises the mobility status on the SBAR, updates progress toward outcomes on the care plan, consults with the physician and team regarding the discharge plan, and discusses progress with the patient and family.
The role of the nursing/patient care assistant. The nursing assistant is responsible for implementing elements of the plan, such as activities of daily living, getting out of bed, and ambulation, under the guidance of the nurse. The nursing assistant reports patient responses to activity level and reflects mobility goals back to the patient verbally and through white board messaging.
Patient progress in mobility. When a patient sustains progress at one stage for 24 hours, the nurse aims to move the patient to the next stage by reevaluating the Barthel Index and going through the same steps as those followed during the initial scoring. The process moves the patient to higher activity levels, unless there are intervening problems affecting mobility.
In such cases, according to the Barthel Index, the patient may remain at the same—or be moved to a lower—activity level. In practice, patients are assessed each shift, and those with higher function (stage 3) are progressed to unsupervised ambulation.
The role of physical and occupational therapy. Although the role of physical and occupational therapists in the SLUHN mobility program is well codified, it is reserved for patients with complex rehabilitation needs due to the number of patients requiring rehabilitation.
In sum, this patient mobility program–for non-ICU hospitalized patients–relies on:
- Documentation of baseline function;
- Independent scoring using the Barthel Index;
- Creation of clear roles for nursing, nursing assistants, and therapists; and
- Reevaluation of patients at regular intervals based on the Barthel Index, so that they may progress to greater activity levels (or to lower levels in the case of a setback).
A key subsequent step, an evaluation of the program’s performance in terms of readmissions, transfer rates to a skilled nursing facility, and skilled facility length of stay, has shown positive results in all three domains.
References
- Shi SL, Girrard P, Goldstein R, et al. Functional status outperforms comorbidities in predicting acute care readmissions in medically complex patients. J Gen Intern Med. 2015;30(11):1688-1695.
- Dammeyer JA, Baldwin N, Packard D, et al. Mobilizing outcomes: implementation of a nurse-led multidisciplinary mobility program. Crit Care Nurs Q. 2013;36(1):109-119.
- Wood W, Tschannen D, Trotsky A, et al. A mobility program for an inpatient acute care medical unit. Am J Nurs. 2014;114(10):34-40.
- Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61-65.