User login
A new prognostic score is more accurate than the commonly used Model for End-Stage Liver Disease (MELD) in predicting post–transjugular intrahepatic portosystemic shunt (TIPS) survival, researchers say.
The Freiburg Index of Post-TIPS Survival (FIPS) could help patients and doctors weigh the benefits and risks of the procedure, said Chongtu Yang, MD, a postgraduate fellow at the Huazhong University of Science and Technology, Wuhan, China.
“For patients defined as high risk, the TIPS procedure may not be the optimal choice, and transplantation may be better,” Dr. Yang told this news organization. He cautioned that FIPS needs further validation before being applied in clinical practice.
The study by Dr. Yang and his colleagues was published online Feb. 9 in the American Journal of Roentgenology. To their knowledge, this is the first study to validate FIPS in a cohort of Asian patients.
Decompensated cirrhosis can cause variceal bleeding and refractory ascites and may be life threatening. TIPS can manage these complications but comes with its own risks.
To determine which patients can best benefit from the procedure, researchers have proposed a variety of prognostic scoring systems. Some were developed for other purposes, such as predicting survival following hospitalization, rather than specifically for TIPS. Additionally, few studies have compared these approaches to each other.
A four-way comparison
To fill that gap, Dr. Yang and his colleagues compared four predictive models: the MELD, the sodium MELD (MELD-Na), the Chronic Liver Failure–Consortium Acute Decompensation (CLIF-CAD), and FIPS.
The MELD score uses serum bilirubin, serum creatinine, and the international normalized ratio (INR) of prothrombin time. MELD-Na adds sodium to this algorithm. The CLIF-CAD score is calculated using age, serum creatinine, INR, white blood count, and sodium level. FIPS, which was recently devised to predict results with TIPS, uses age, bilirubin, albumin, and creatinine.
To see which yielded more accurate predictions, Dr. Yang and his colleagues followed 383 patients with cirrhosis (mean age, 55 years; 341 with variceal bleeding and 42 with refractory ascites) who underwent TIPS placement at Wuhan Union Hospital between January 2016 and August 2021.
The most common cause of cirrhosis was hepatitis B infection (58.2% of patients), followed by hepatitis C infection (11.7%) and alcohol use (13.6%).
The researchers followed the patients for a median of 23.4 months. They lost track of 31 patients over that time, and another 72 died. The survival rate after TIPS placement was 92.3% at 6 months, 87.8% at 12 months, and 81.2% at 24 months. Thirty-seven patients received a TIPS revision.
In their first measure of the models’ accuracy, the researchers used a concordance index, which compares actual results with predicted results. The number of concordant pairs are divided by the total number of possible evaluation pairs. A score of 1 represents 100% accuracy.
By this measure, the prediction of survival at 6 months was highest for FIPS followed by CLIF-CAD, MELD, and MELD-Na. However, the confidence intervals overlapped.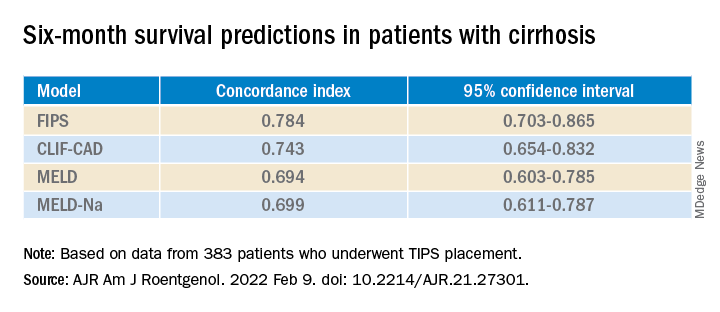
FIPS also scored highest in the concordance index at 12 and 24 months.
In a second measure of the models’ accuracy, the researchers used Brier scores, which calculate the mean squared error between predicted probabilities and actual values. Like the concordance index, Brier scores range from 0.0 to 1.0 but differ in that the lowest Brier score number represents the highest accuracy.
At 6 months, the CLIF-CAD score was the best, at 0.074. MELD and FIPS were equivalent at 0.075, with MELD-Na coming in at 0.077. However, FIPS attained slightly better scores than the other systems at 12 and 24 months.
Is FIPS worth implementing?
With scores this close, it may not be worth changing the predictive model clinicians use for choosing TIPS candidates, said Nancy Reau, MD, chief of hepatology at Rush University Medical Center, Chicago, who was not involved in the study.
MELD scores are already programmed into many electronic medical record systems in the United States, and clinicians are familiar with using that system to aid in further decisions, such as decisions regarding other kinds of surgery, she told this news organization.
“If you’re going to try to advocate for a new system, you really have to show that the performance of the predictive score is monumentally better than the tried and true,” she said.
Dr. Yang and Dr. Reau report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new prognostic score is more accurate than the commonly used Model for End-Stage Liver Disease (MELD) in predicting post–transjugular intrahepatic portosystemic shunt (TIPS) survival, researchers say.
The Freiburg Index of Post-TIPS Survival (FIPS) could help patients and doctors weigh the benefits and risks of the procedure, said Chongtu Yang, MD, a postgraduate fellow at the Huazhong University of Science and Technology, Wuhan, China.
“For patients defined as high risk, the TIPS procedure may not be the optimal choice, and transplantation may be better,” Dr. Yang told this news organization. He cautioned that FIPS needs further validation before being applied in clinical practice.
The study by Dr. Yang and his colleagues was published online Feb. 9 in the American Journal of Roentgenology. To their knowledge, this is the first study to validate FIPS in a cohort of Asian patients.
Decompensated cirrhosis can cause variceal bleeding and refractory ascites and may be life threatening. TIPS can manage these complications but comes with its own risks.
To determine which patients can best benefit from the procedure, researchers have proposed a variety of prognostic scoring systems. Some were developed for other purposes, such as predicting survival following hospitalization, rather than specifically for TIPS. Additionally, few studies have compared these approaches to each other.
A four-way comparison
To fill that gap, Dr. Yang and his colleagues compared four predictive models: the MELD, the sodium MELD (MELD-Na), the Chronic Liver Failure–Consortium Acute Decompensation (CLIF-CAD), and FIPS.
The MELD score uses serum bilirubin, serum creatinine, and the international normalized ratio (INR) of prothrombin time. MELD-Na adds sodium to this algorithm. The CLIF-CAD score is calculated using age, serum creatinine, INR, white blood count, and sodium level. FIPS, which was recently devised to predict results with TIPS, uses age, bilirubin, albumin, and creatinine.
To see which yielded more accurate predictions, Dr. Yang and his colleagues followed 383 patients with cirrhosis (mean age, 55 years; 341 with variceal bleeding and 42 with refractory ascites) who underwent TIPS placement at Wuhan Union Hospital between January 2016 and August 2021.
The most common cause of cirrhosis was hepatitis B infection (58.2% of patients), followed by hepatitis C infection (11.7%) and alcohol use (13.6%).
The researchers followed the patients for a median of 23.4 months. They lost track of 31 patients over that time, and another 72 died. The survival rate after TIPS placement was 92.3% at 6 months, 87.8% at 12 months, and 81.2% at 24 months. Thirty-seven patients received a TIPS revision.
In their first measure of the models’ accuracy, the researchers used a concordance index, which compares actual results with predicted results. The number of concordant pairs are divided by the total number of possible evaluation pairs. A score of 1 represents 100% accuracy.
By this measure, the prediction of survival at 6 months was highest for FIPS followed by CLIF-CAD, MELD, and MELD-Na. However, the confidence intervals overlapped.
FIPS also scored highest in the concordance index at 12 and 24 months.
In a second measure of the models’ accuracy, the researchers used Brier scores, which calculate the mean squared error between predicted probabilities and actual values. Like the concordance index, Brier scores range from 0.0 to 1.0 but differ in that the lowest Brier score number represents the highest accuracy.
At 6 months, the CLIF-CAD score was the best, at 0.074. MELD and FIPS were equivalent at 0.075, with MELD-Na coming in at 0.077. However, FIPS attained slightly better scores than the other systems at 12 and 24 months.
Is FIPS worth implementing?
With scores this close, it may not be worth changing the predictive model clinicians use for choosing TIPS candidates, said Nancy Reau, MD, chief of hepatology at Rush University Medical Center, Chicago, who was not involved in the study.
MELD scores are already programmed into many electronic medical record systems in the United States, and clinicians are familiar with using that system to aid in further decisions, such as decisions regarding other kinds of surgery, she told this news organization.
“If you’re going to try to advocate for a new system, you really have to show that the performance of the predictive score is monumentally better than the tried and true,” she said.
Dr. Yang and Dr. Reau report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new prognostic score is more accurate than the commonly used Model for End-Stage Liver Disease (MELD) in predicting post–transjugular intrahepatic portosystemic shunt (TIPS) survival, researchers say.
The Freiburg Index of Post-TIPS Survival (FIPS) could help patients and doctors weigh the benefits and risks of the procedure, said Chongtu Yang, MD, a postgraduate fellow at the Huazhong University of Science and Technology, Wuhan, China.
“For patients defined as high risk, the TIPS procedure may not be the optimal choice, and transplantation may be better,” Dr. Yang told this news organization. He cautioned that FIPS needs further validation before being applied in clinical practice.
The study by Dr. Yang and his colleagues was published online Feb. 9 in the American Journal of Roentgenology. To their knowledge, this is the first study to validate FIPS in a cohort of Asian patients.
Decompensated cirrhosis can cause variceal bleeding and refractory ascites and may be life threatening. TIPS can manage these complications but comes with its own risks.
To determine which patients can best benefit from the procedure, researchers have proposed a variety of prognostic scoring systems. Some were developed for other purposes, such as predicting survival following hospitalization, rather than specifically for TIPS. Additionally, few studies have compared these approaches to each other.
A four-way comparison
To fill that gap, Dr. Yang and his colleagues compared four predictive models: the MELD, the sodium MELD (MELD-Na), the Chronic Liver Failure–Consortium Acute Decompensation (CLIF-CAD), and FIPS.
The MELD score uses serum bilirubin, serum creatinine, and the international normalized ratio (INR) of prothrombin time. MELD-Na adds sodium to this algorithm. The CLIF-CAD score is calculated using age, serum creatinine, INR, white blood count, and sodium level. FIPS, which was recently devised to predict results with TIPS, uses age, bilirubin, albumin, and creatinine.
To see which yielded more accurate predictions, Dr. Yang and his colleagues followed 383 patients with cirrhosis (mean age, 55 years; 341 with variceal bleeding and 42 with refractory ascites) who underwent TIPS placement at Wuhan Union Hospital between January 2016 and August 2021.
The most common cause of cirrhosis was hepatitis B infection (58.2% of patients), followed by hepatitis C infection (11.7%) and alcohol use (13.6%).
The researchers followed the patients for a median of 23.4 months. They lost track of 31 patients over that time, and another 72 died. The survival rate after TIPS placement was 92.3% at 6 months, 87.8% at 12 months, and 81.2% at 24 months. Thirty-seven patients received a TIPS revision.
In their first measure of the models’ accuracy, the researchers used a concordance index, which compares actual results with predicted results. The number of concordant pairs are divided by the total number of possible evaluation pairs. A score of 1 represents 100% accuracy.
By this measure, the prediction of survival at 6 months was highest for FIPS followed by CLIF-CAD, MELD, and MELD-Na. However, the confidence intervals overlapped.
FIPS also scored highest in the concordance index at 12 and 24 months.
In a second measure of the models’ accuracy, the researchers used Brier scores, which calculate the mean squared error between predicted probabilities and actual values. Like the concordance index, Brier scores range from 0.0 to 1.0 but differ in that the lowest Brier score number represents the highest accuracy.
At 6 months, the CLIF-CAD score was the best, at 0.074. MELD and FIPS were equivalent at 0.075, with MELD-Na coming in at 0.077. However, FIPS attained slightly better scores than the other systems at 12 and 24 months.
Is FIPS worth implementing?
With scores this close, it may not be worth changing the predictive model clinicians use for choosing TIPS candidates, said Nancy Reau, MD, chief of hepatology at Rush University Medical Center, Chicago, who was not involved in the study.
MELD scores are already programmed into many electronic medical record systems in the United States, and clinicians are familiar with using that system to aid in further decisions, such as decisions regarding other kinds of surgery, she told this news organization.
“If you’re going to try to advocate for a new system, you really have to show that the performance of the predictive score is monumentally better than the tried and true,” she said.
Dr. Yang and Dr. Reau report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF ROENTGENOLOGY