User login
ABSTRACT
Purpose Gastroesophageal reflux disease (GERD) affects up to 25% of the western population, and the annual expenditure for managing GERD is estimated to be more than $14 billion. Most GERD patients do not consult a specialist, but rather rely on their primary care physician for symptom management. Research has shown that many patients—regardless of diagnosis—do not fully understand what their doctors tell them and remain uncertain as to what they are supposed to do to take care of themselves. To determine if patients are adequately educated in the management of GERD, we conducted a survey.
Method We administered a survey to patients with GERD in an outpatient setting and explored their knowledge of such management practices as modification of behavior and diet and use of medication.
Results Of 333 patients enrolled, 66% reported having an in-depth discussion with their primary care physician. Among patients taking a proton pump inhibitor, 85% of those who’d had an in-depth discussion were aware of the best time to take their medication, compared with only 18% of those who did not have an in-depth discussion. In addition, patients who’d had in-depth conversations were significantly more likely than those who didn’t to know some of the behavior modification measures that might improve their symptoms.
Conclusion Our study underscores the need for primary care providers to fully discuss GERD with their patients to improve overall management of the disease.
Gastroesophageal reflux disease (GERD) affects between 15% and 25% of populations in Western countries, and is estimated to account for health care costs totaling more than $14 billion.1 In North America, the prevalence of reflux symptoms is increasing, on average by 5% annually1—this despite significant improvements in the identification and treatment of the disorder. Could it be that improvement in physician-patient communication is also needed to ensure management success?
Most GERD patients are seen in the primary care (PC) setting. Although patient education is an important aspect of treating GERD, physicians often lack sufficient time to educate patients properly. Research has shown that many patients, regardless of diagnosis, do not fully understand what their doctors tell them and remain uncertain of what they are supposed to do to take care of themselves.2,3
In this article, we report the results of a simple survey administered in the PC setting to patients experiencing symptomatic GERD that necessitated the use of a medication. We hypothesized that patients were not adequately informed about their condition and that patient adherence was associated with the depth of dialogue with their physician.
METHODS
This study was approved by the Advocate Lutheran General Hospital Institutional Review Board. Fellows and faculty in the Advocate Lutheran General Hospital gastroenterology fellowship program developed the survey collaboratively and carried out the study at the Advocate Medical Group outpatient PC clinic and at local physicians’ offices. We opened participation to all patients >18 years of age with previously diagnosed GERD who visited affiliated outpatient clinics or offices during the data collection period between January 2009 and May 2010. There were no additional criteria or selection screens.
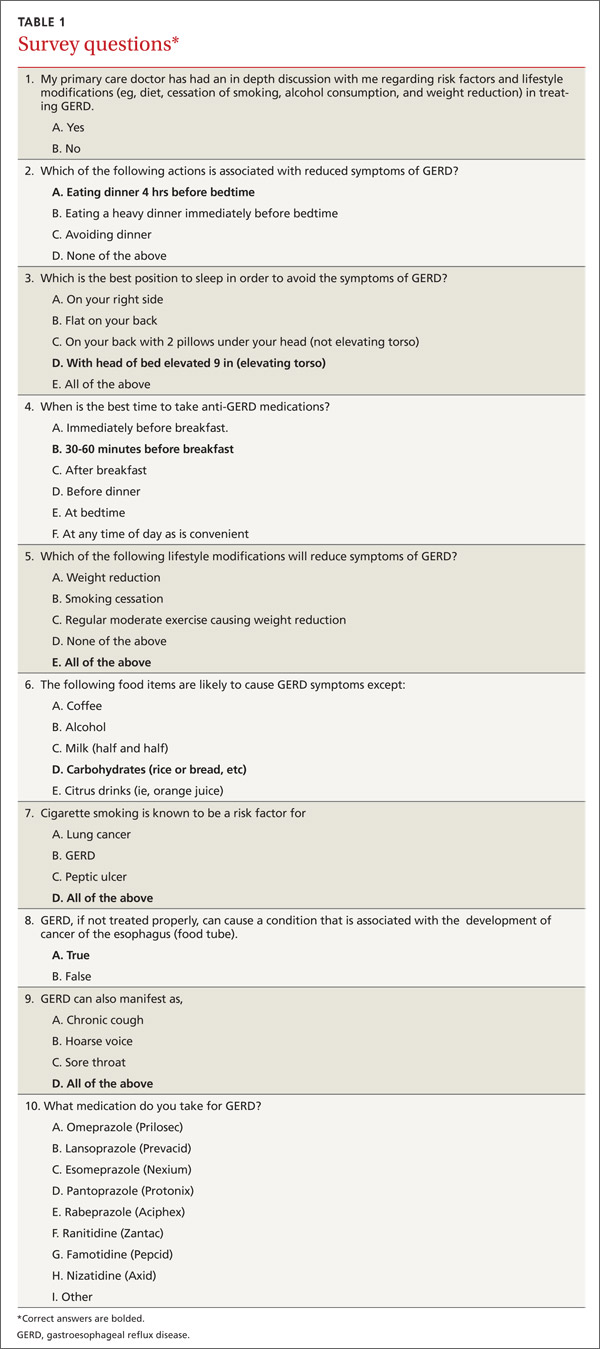
After obtaining a patient’s informed consent, an attending physician or resident handed the patient a multiple-choice survey (TABLE 1), but did not supervise the activity. A clerk collected the completed surveys and separated responses from personally identifiable information before entering results into a database.
Since one of the major goals of this study was to relate patient perception of the quality and clarity of education received from the physician to actual understanding of GERD, we intentionally avoided giving precise descriptions of the qualitative terms used in the survey, such as “in-depth,” “best,” and “likely.” We did, however, provide definitions and descriptions for nonqualitative words and terms, such as GERD and sleeping position. A clerk or administering physician fielded patients’ questions about the survey. We did not attempt to make comparisons between our survey and other available surveys.4,5
What we expected to find. Based on expert consultation with attending gastrointestinal faculty at our institution, we expected that approximately 30% of GERD patients would not have an in-depth discussion with their PC physician regarding lifestyle modifications and risk factors affecting GERD. We planned a study of independent cases (those not having an in-depth discussion) and controls (those having an in-depth discussion), with 2 controls per case. Our primary endpoint was the survey item that asked patients to specify the best time for taking their proton-pump inhibitor (PPI). We expected that 70% of the controls and 50% of independent cases would know the correct time to take their PPI medication. Our null hypothesis stated that the rates for case and control subjects would be equal with a probability (power) of 0.80. To reject the null hypothesis, we needed a minimum total sample of 207 patients taking a PPI (138 control subjects and 69 case subjects). The Type I error probability associated with this test of this null hypothesis is .05.6
We reported descriptive statistics for categorical and continuous data, and performed between-group statistical comparisons on survey items via the Chi-square test or Fisher’s Exact test when necessary. We performed age comparisons with the Independent t-test. We considered a 2-tailed value of .05 as statistically significant in all analyses, which we conducted with SPSS software (International Business Machines, Chicago, Ill).
RESULTS
All 333 patients invited to participate gave informed consent and completed the survey in its entirety. Patients were evenly distributed by gender. The median age of all patients was 44±13.1 years (range, 19-83). Approximately two-thirds of patients (66%) perceived that discussions with their PC physicians regarding lifestyle modifications and risk factors affecting GERD were “in-depth.”
We examined the gender and age of patients as functions of perceived discussion level. Men and women were equally likely to have in-depth discussions with their physicians (P>.05). On the other hand, younger patients were more likely than older ones to have in-depth discussions. The mean age of the patients who reported having an in-depth discussion was 42.6±13.1 years; of those who did not have an in-depth discussion, the mean age was 46.0±12.9 years (P<.05). However, for each individual survey question, the number of correct responses did not correlate with age, suggesting that age is not a true predictor of level of discussion.
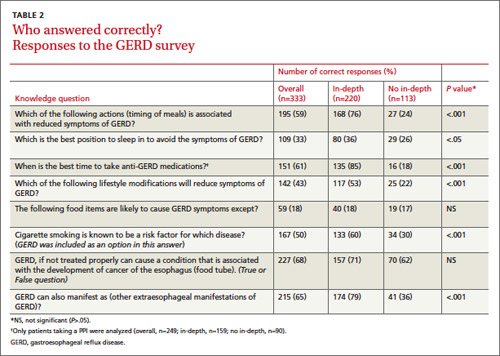
Approximately one-third of patients (32%) were not aware that untreated GERD can be associated with increased risk of cancer of the esophagus, although there was no significant difference between discussion level groups (P>.05) (TABLE 2). Similar numbers of patients reported being aware of best sleeping position (33%), with those in the in-depth discussion group exhibiting a better understanding of the best position (36% vs 26%, respectively; P<.05). Patients perceiving they had an in-depth discussion with their PC physicians were significantly more likely than those in the other group to know the appropriate time to eat dinner (76% vs 24%, respectively; P<.001). Overall and without respect to discussion level, few patients understood dietary guidelines (18%, P>.05).
Patients having an in-depth discussion with their primary care physician were also more likely to know the best time to take antireflux medications (85% vs 18%, respectively, P<.001); that GERD symptoms can be reduced through lifestyle modifications (53% vs 22%, respectively; P<.001); and that GERD can manifest as chronic cough, hoarse voice, or sore throat (79% vs 36%, respectively; P<.001).
DISCUSSION
We conducted a simple, easy-to-use survey to gain an appreciation of patients’ levels of understanding of GERD after discussion with their physicians. Specifically, the survey related a patient’s perceived level of discussion to his or her knowledge of facts pertinent to GERD, including personal lifestyle choices. Importantly, the patient’s perception of the quality of discussion was surveyed, as perception and reality are not always in agreement.
Although the American Gastroenterological Association advocates that physicians should have in-depth discussions with their patients with respect to the disease process and lifestyle modifications, this is not typical.4,7
In our study, 66% of patients perceived that they had an in-depth discussion with their PC physician regarding factors affecting GERD. Of patients taking a PPI, 85% of those having in-depth discussions were aware of the correct time to take their medication. Of those not having an in-depth discussion, only 18% gave the correct answer, which is no better than a random guess (20%) and suggests that, essentially, none of these patients knew when to take their medication.
Study limitations. We did not validate our survey against other surveys or within our patient population; additional efforts are therefore warranted in this regard. Future studies might also explore how duration and severity of symptoms prior to patient-physician discussions, socioeconomic status, and education level influence the relationship between perception of care and understanding of GERD. A follow-up survey would help to define whether these discussions translate into improved disease management.
In spite of the limitations of our survey, our data clearly demonstrate that knowledge of GERD correlates with the perceived level of discussion that patients have with their physician, and that a large percentage of patients do not fully understand their condition and methods to manage it. Patients who did have an in-depth discussion with their primary care provider were likely to be better educated with regard to GERD. Because of the prevalence of GERD,1,7,8 its association with increased health care costs and reduced quality of life,1,8 and predominant management at the primary care level, we recommend that PC physicians place more emphasis on the education of patients diagnosed with GERD.
CORRESPONDENCE
Naser M. Khan, MD, Advanced Gastroenterology Associates, Doctors Office Building 3, Suite 2300b, 1555 Barrington Road, Hoffman Estates, IL 60169; [email protected]
1. Richter JE. The many manifestations of gastroesophageal reflux disease: presentation, evaluation, and treatment. Gastroenterol Clin North Am. 2007;36:577-599, vii-ix.
2. Kessels RPC. Patients’ memory for medical information. J R Soc Med. 2003;96:219-222.
3. Makaryus AN, Friedman EA. Patients’ understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80:991-994.
4. American Gastroenterological Association. New Nationwide Survey Identifies Need for Increased Dialogue Between Gastroesophageal Reflux Disease or Frequent Heartburn Sufferers and Health Care Providers. Available at: http://www.gastro.org/news/articles/2011/03/23/new-nationwide-survey-identifiesneed-for-increased-dialogue-between-gastroesophageal-reflux-disease-or-frequent-heartburn-sufferers-and-health-careproviders. Accessed July 19, 2012.
5. ClinicalTrials.gov. National Survey on Gastroesophageal Reflux Disease (GERD) Patients (LINEA). Available at: http://clinicaltrials.gov/ct2/show/NCT00695838. Accessed July 19, 2012.
6. Dupont WD, Plummer WD. PS power and sample size program available for free on the internet. Control Clin Trials. 1997;18:274.
7. Kahrilas PJ, Shaheen NJ, Vaezi MF; American Gastroenterological Association Institute; Clinical Practice and Quality Management Committee. American Gastroenterological Association Institute technical review on the management of gastroesophageal reflux disease. Gastroenterology. 2008;135:1392-1413, 1413.e1-e5.
8. El-Serag HB. Time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007;5:17-26.
ABSTRACT
Purpose Gastroesophageal reflux disease (GERD) affects up to 25% of the western population, and the annual expenditure for managing GERD is estimated to be more than $14 billion. Most GERD patients do not consult a specialist, but rather rely on their primary care physician for symptom management. Research has shown that many patients—regardless of diagnosis—do not fully understand what their doctors tell them and remain uncertain as to what they are supposed to do to take care of themselves. To determine if patients are adequately educated in the management of GERD, we conducted a survey.
Method We administered a survey to patients with GERD in an outpatient setting and explored their knowledge of such management practices as modification of behavior and diet and use of medication.
Results Of 333 patients enrolled, 66% reported having an in-depth discussion with their primary care physician. Among patients taking a proton pump inhibitor, 85% of those who’d had an in-depth discussion were aware of the best time to take their medication, compared with only 18% of those who did not have an in-depth discussion. In addition, patients who’d had in-depth conversations were significantly more likely than those who didn’t to know some of the behavior modification measures that might improve their symptoms.
Conclusion Our study underscores the need for primary care providers to fully discuss GERD with their patients to improve overall management of the disease.
Gastroesophageal reflux disease (GERD) affects between 15% and 25% of populations in Western countries, and is estimated to account for health care costs totaling more than $14 billion.1 In North America, the prevalence of reflux symptoms is increasing, on average by 5% annually1—this despite significant improvements in the identification and treatment of the disorder. Could it be that improvement in physician-patient communication is also needed to ensure management success?
Most GERD patients are seen in the primary care (PC) setting. Although patient education is an important aspect of treating GERD, physicians often lack sufficient time to educate patients properly. Research has shown that many patients, regardless of diagnosis, do not fully understand what their doctors tell them and remain uncertain of what they are supposed to do to take care of themselves.2,3
In this article, we report the results of a simple survey administered in the PC setting to patients experiencing symptomatic GERD that necessitated the use of a medication. We hypothesized that patients were not adequately informed about their condition and that patient adherence was associated with the depth of dialogue with their physician.
METHODS
This study was approved by the Advocate Lutheran General Hospital Institutional Review Board. Fellows and faculty in the Advocate Lutheran General Hospital gastroenterology fellowship program developed the survey collaboratively and carried out the study at the Advocate Medical Group outpatient PC clinic and at local physicians’ offices. We opened participation to all patients >18 years of age with previously diagnosed GERD who visited affiliated outpatient clinics or offices during the data collection period between January 2009 and May 2010. There were no additional criteria or selection screens.
After obtaining a patient’s informed consent, an attending physician or resident handed the patient a multiple-choice survey (TABLE 1), but did not supervise the activity. A clerk collected the completed surveys and separated responses from personally identifiable information before entering results into a database.
Since one of the major goals of this study was to relate patient perception of the quality and clarity of education received from the physician to actual understanding of GERD, we intentionally avoided giving precise descriptions of the qualitative terms used in the survey, such as “in-depth,” “best,” and “likely.” We did, however, provide definitions and descriptions for nonqualitative words and terms, such as GERD and sleeping position. A clerk or administering physician fielded patients’ questions about the survey. We did not attempt to make comparisons between our survey and other available surveys.4,5
What we expected to find. Based on expert consultation with attending gastrointestinal faculty at our institution, we expected that approximately 30% of GERD patients would not have an in-depth discussion with their PC physician regarding lifestyle modifications and risk factors affecting GERD. We planned a study of independent cases (those not having an in-depth discussion) and controls (those having an in-depth discussion), with 2 controls per case. Our primary endpoint was the survey item that asked patients to specify the best time for taking their proton-pump inhibitor (PPI). We expected that 70% of the controls and 50% of independent cases would know the correct time to take their PPI medication. Our null hypothesis stated that the rates for case and control subjects would be equal with a probability (power) of 0.80. To reject the null hypothesis, we needed a minimum total sample of 207 patients taking a PPI (138 control subjects and 69 case subjects). The Type I error probability associated with this test of this null hypothesis is .05.6
We reported descriptive statistics for categorical and continuous data, and performed between-group statistical comparisons on survey items via the Chi-square test or Fisher’s Exact test when necessary. We performed age comparisons with the Independent t-test. We considered a 2-tailed value of .05 as statistically significant in all analyses, which we conducted with SPSS software (International Business Machines, Chicago, Ill).
RESULTS
All 333 patients invited to participate gave informed consent and completed the survey in its entirety. Patients were evenly distributed by gender. The median age of all patients was 44±13.1 years (range, 19-83). Approximately two-thirds of patients (66%) perceived that discussions with their PC physicians regarding lifestyle modifications and risk factors affecting GERD were “in-depth.”
We examined the gender and age of patients as functions of perceived discussion level. Men and women were equally likely to have in-depth discussions with their physicians (P>.05). On the other hand, younger patients were more likely than older ones to have in-depth discussions. The mean age of the patients who reported having an in-depth discussion was 42.6±13.1 years; of those who did not have an in-depth discussion, the mean age was 46.0±12.9 years (P<.05). However, for each individual survey question, the number of correct responses did not correlate with age, suggesting that age is not a true predictor of level of discussion.
Approximately one-third of patients (32%) were not aware that untreated GERD can be associated with increased risk of cancer of the esophagus, although there was no significant difference between discussion level groups (P>.05) (TABLE 2). Similar numbers of patients reported being aware of best sleeping position (33%), with those in the in-depth discussion group exhibiting a better understanding of the best position (36% vs 26%, respectively; P<.05). Patients perceiving they had an in-depth discussion with their PC physicians were significantly more likely than those in the other group to know the appropriate time to eat dinner (76% vs 24%, respectively; P<.001). Overall and without respect to discussion level, few patients understood dietary guidelines (18%, P>.05).
Patients having an in-depth discussion with their primary care physician were also more likely to know the best time to take antireflux medications (85% vs 18%, respectively, P<.001); that GERD symptoms can be reduced through lifestyle modifications (53% vs 22%, respectively; P<.001); and that GERD can manifest as chronic cough, hoarse voice, or sore throat (79% vs 36%, respectively; P<.001).
DISCUSSION
We conducted a simple, easy-to-use survey to gain an appreciation of patients’ levels of understanding of GERD after discussion with their physicians. Specifically, the survey related a patient’s perceived level of discussion to his or her knowledge of facts pertinent to GERD, including personal lifestyle choices. Importantly, the patient’s perception of the quality of discussion was surveyed, as perception and reality are not always in agreement.
Although the American Gastroenterological Association advocates that physicians should have in-depth discussions with their patients with respect to the disease process and lifestyle modifications, this is not typical.4,7
In our study, 66% of patients perceived that they had an in-depth discussion with their PC physician regarding factors affecting GERD. Of patients taking a PPI, 85% of those having in-depth discussions were aware of the correct time to take their medication. Of those not having an in-depth discussion, only 18% gave the correct answer, which is no better than a random guess (20%) and suggests that, essentially, none of these patients knew when to take their medication.
Study limitations. We did not validate our survey against other surveys or within our patient population; additional efforts are therefore warranted in this regard. Future studies might also explore how duration and severity of symptoms prior to patient-physician discussions, socioeconomic status, and education level influence the relationship between perception of care and understanding of GERD. A follow-up survey would help to define whether these discussions translate into improved disease management.
In spite of the limitations of our survey, our data clearly demonstrate that knowledge of GERD correlates with the perceived level of discussion that patients have with their physician, and that a large percentage of patients do not fully understand their condition and methods to manage it. Patients who did have an in-depth discussion with their primary care provider were likely to be better educated with regard to GERD. Because of the prevalence of GERD,1,7,8 its association with increased health care costs and reduced quality of life,1,8 and predominant management at the primary care level, we recommend that PC physicians place more emphasis on the education of patients diagnosed with GERD.
CORRESPONDENCE
Naser M. Khan, MD, Advanced Gastroenterology Associates, Doctors Office Building 3, Suite 2300b, 1555 Barrington Road, Hoffman Estates, IL 60169; [email protected]
ABSTRACT
Purpose Gastroesophageal reflux disease (GERD) affects up to 25% of the western population, and the annual expenditure for managing GERD is estimated to be more than $14 billion. Most GERD patients do not consult a specialist, but rather rely on their primary care physician for symptom management. Research has shown that many patients—regardless of diagnosis—do not fully understand what their doctors tell them and remain uncertain as to what they are supposed to do to take care of themselves. To determine if patients are adequately educated in the management of GERD, we conducted a survey.
Method We administered a survey to patients with GERD in an outpatient setting and explored their knowledge of such management practices as modification of behavior and diet and use of medication.
Results Of 333 patients enrolled, 66% reported having an in-depth discussion with their primary care physician. Among patients taking a proton pump inhibitor, 85% of those who’d had an in-depth discussion were aware of the best time to take their medication, compared with only 18% of those who did not have an in-depth discussion. In addition, patients who’d had in-depth conversations were significantly more likely than those who didn’t to know some of the behavior modification measures that might improve their symptoms.
Conclusion Our study underscores the need for primary care providers to fully discuss GERD with their patients to improve overall management of the disease.
Gastroesophageal reflux disease (GERD) affects between 15% and 25% of populations in Western countries, and is estimated to account for health care costs totaling more than $14 billion.1 In North America, the prevalence of reflux symptoms is increasing, on average by 5% annually1—this despite significant improvements in the identification and treatment of the disorder. Could it be that improvement in physician-patient communication is also needed to ensure management success?
Most GERD patients are seen in the primary care (PC) setting. Although patient education is an important aspect of treating GERD, physicians often lack sufficient time to educate patients properly. Research has shown that many patients, regardless of diagnosis, do not fully understand what their doctors tell them and remain uncertain of what they are supposed to do to take care of themselves.2,3
In this article, we report the results of a simple survey administered in the PC setting to patients experiencing symptomatic GERD that necessitated the use of a medication. We hypothesized that patients were not adequately informed about their condition and that patient adherence was associated with the depth of dialogue with their physician.
METHODS
This study was approved by the Advocate Lutheran General Hospital Institutional Review Board. Fellows and faculty in the Advocate Lutheran General Hospital gastroenterology fellowship program developed the survey collaboratively and carried out the study at the Advocate Medical Group outpatient PC clinic and at local physicians’ offices. We opened participation to all patients >18 years of age with previously diagnosed GERD who visited affiliated outpatient clinics or offices during the data collection period between January 2009 and May 2010. There were no additional criteria or selection screens.
After obtaining a patient’s informed consent, an attending physician or resident handed the patient a multiple-choice survey (TABLE 1), but did not supervise the activity. A clerk collected the completed surveys and separated responses from personally identifiable information before entering results into a database.
Since one of the major goals of this study was to relate patient perception of the quality and clarity of education received from the physician to actual understanding of GERD, we intentionally avoided giving precise descriptions of the qualitative terms used in the survey, such as “in-depth,” “best,” and “likely.” We did, however, provide definitions and descriptions for nonqualitative words and terms, such as GERD and sleeping position. A clerk or administering physician fielded patients’ questions about the survey. We did not attempt to make comparisons between our survey and other available surveys.4,5
What we expected to find. Based on expert consultation with attending gastrointestinal faculty at our institution, we expected that approximately 30% of GERD patients would not have an in-depth discussion with their PC physician regarding lifestyle modifications and risk factors affecting GERD. We planned a study of independent cases (those not having an in-depth discussion) and controls (those having an in-depth discussion), with 2 controls per case. Our primary endpoint was the survey item that asked patients to specify the best time for taking their proton-pump inhibitor (PPI). We expected that 70% of the controls and 50% of independent cases would know the correct time to take their PPI medication. Our null hypothesis stated that the rates for case and control subjects would be equal with a probability (power) of 0.80. To reject the null hypothesis, we needed a minimum total sample of 207 patients taking a PPI (138 control subjects and 69 case subjects). The Type I error probability associated with this test of this null hypothesis is .05.6
We reported descriptive statistics for categorical and continuous data, and performed between-group statistical comparisons on survey items via the Chi-square test or Fisher’s Exact test when necessary. We performed age comparisons with the Independent t-test. We considered a 2-tailed value of .05 as statistically significant in all analyses, which we conducted with SPSS software (International Business Machines, Chicago, Ill).
RESULTS
All 333 patients invited to participate gave informed consent and completed the survey in its entirety. Patients were evenly distributed by gender. The median age of all patients was 44±13.1 years (range, 19-83). Approximately two-thirds of patients (66%) perceived that discussions with their PC physicians regarding lifestyle modifications and risk factors affecting GERD were “in-depth.”
We examined the gender and age of patients as functions of perceived discussion level. Men and women were equally likely to have in-depth discussions with their physicians (P>.05). On the other hand, younger patients were more likely than older ones to have in-depth discussions. The mean age of the patients who reported having an in-depth discussion was 42.6±13.1 years; of those who did not have an in-depth discussion, the mean age was 46.0±12.9 years (P<.05). However, for each individual survey question, the number of correct responses did not correlate with age, suggesting that age is not a true predictor of level of discussion.
Approximately one-third of patients (32%) were not aware that untreated GERD can be associated with increased risk of cancer of the esophagus, although there was no significant difference between discussion level groups (P>.05) (TABLE 2). Similar numbers of patients reported being aware of best sleeping position (33%), with those in the in-depth discussion group exhibiting a better understanding of the best position (36% vs 26%, respectively; P<.05). Patients perceiving they had an in-depth discussion with their PC physicians were significantly more likely than those in the other group to know the appropriate time to eat dinner (76% vs 24%, respectively; P<.001). Overall and without respect to discussion level, few patients understood dietary guidelines (18%, P>.05).
Patients having an in-depth discussion with their primary care physician were also more likely to know the best time to take antireflux medications (85% vs 18%, respectively, P<.001); that GERD symptoms can be reduced through lifestyle modifications (53% vs 22%, respectively; P<.001); and that GERD can manifest as chronic cough, hoarse voice, or sore throat (79% vs 36%, respectively; P<.001).
DISCUSSION
We conducted a simple, easy-to-use survey to gain an appreciation of patients’ levels of understanding of GERD after discussion with their physicians. Specifically, the survey related a patient’s perceived level of discussion to his or her knowledge of facts pertinent to GERD, including personal lifestyle choices. Importantly, the patient’s perception of the quality of discussion was surveyed, as perception and reality are not always in agreement.
Although the American Gastroenterological Association advocates that physicians should have in-depth discussions with their patients with respect to the disease process and lifestyle modifications, this is not typical.4,7
In our study, 66% of patients perceived that they had an in-depth discussion with their PC physician regarding factors affecting GERD. Of patients taking a PPI, 85% of those having in-depth discussions were aware of the correct time to take their medication. Of those not having an in-depth discussion, only 18% gave the correct answer, which is no better than a random guess (20%) and suggests that, essentially, none of these patients knew when to take their medication.
Study limitations. We did not validate our survey against other surveys or within our patient population; additional efforts are therefore warranted in this regard. Future studies might also explore how duration and severity of symptoms prior to patient-physician discussions, socioeconomic status, and education level influence the relationship between perception of care and understanding of GERD. A follow-up survey would help to define whether these discussions translate into improved disease management.
In spite of the limitations of our survey, our data clearly demonstrate that knowledge of GERD correlates with the perceived level of discussion that patients have with their physician, and that a large percentage of patients do not fully understand their condition and methods to manage it. Patients who did have an in-depth discussion with their primary care provider were likely to be better educated with regard to GERD. Because of the prevalence of GERD,1,7,8 its association with increased health care costs and reduced quality of life,1,8 and predominant management at the primary care level, we recommend that PC physicians place more emphasis on the education of patients diagnosed with GERD.
CORRESPONDENCE
Naser M. Khan, MD, Advanced Gastroenterology Associates, Doctors Office Building 3, Suite 2300b, 1555 Barrington Road, Hoffman Estates, IL 60169; [email protected]
1. Richter JE. The many manifestations of gastroesophageal reflux disease: presentation, evaluation, and treatment. Gastroenterol Clin North Am. 2007;36:577-599, vii-ix.
2. Kessels RPC. Patients’ memory for medical information. J R Soc Med. 2003;96:219-222.
3. Makaryus AN, Friedman EA. Patients’ understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80:991-994.
4. American Gastroenterological Association. New Nationwide Survey Identifies Need for Increased Dialogue Between Gastroesophageal Reflux Disease or Frequent Heartburn Sufferers and Health Care Providers. Available at: http://www.gastro.org/news/articles/2011/03/23/new-nationwide-survey-identifiesneed-for-increased-dialogue-between-gastroesophageal-reflux-disease-or-frequent-heartburn-sufferers-and-health-careproviders. Accessed July 19, 2012.
5. ClinicalTrials.gov. National Survey on Gastroesophageal Reflux Disease (GERD) Patients (LINEA). Available at: http://clinicaltrials.gov/ct2/show/NCT00695838. Accessed July 19, 2012.
6. Dupont WD, Plummer WD. PS power and sample size program available for free on the internet. Control Clin Trials. 1997;18:274.
7. Kahrilas PJ, Shaheen NJ, Vaezi MF; American Gastroenterological Association Institute; Clinical Practice and Quality Management Committee. American Gastroenterological Association Institute technical review on the management of gastroesophageal reflux disease. Gastroenterology. 2008;135:1392-1413, 1413.e1-e5.
8. El-Serag HB. Time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007;5:17-26.
1. Richter JE. The many manifestations of gastroesophageal reflux disease: presentation, evaluation, and treatment. Gastroenterol Clin North Am. 2007;36:577-599, vii-ix.
2. Kessels RPC. Patients’ memory for medical information. J R Soc Med. 2003;96:219-222.
3. Makaryus AN, Friedman EA. Patients’ understanding of their treatment plans and diagnosis at discharge. Mayo Clin Proc. 2005;80:991-994.
4. American Gastroenterological Association. New Nationwide Survey Identifies Need for Increased Dialogue Between Gastroesophageal Reflux Disease or Frequent Heartburn Sufferers and Health Care Providers. Available at: http://www.gastro.org/news/articles/2011/03/23/new-nationwide-survey-identifiesneed-for-increased-dialogue-between-gastroesophageal-reflux-disease-or-frequent-heartburn-sufferers-and-health-careproviders. Accessed July 19, 2012.
5. ClinicalTrials.gov. National Survey on Gastroesophageal Reflux Disease (GERD) Patients (LINEA). Available at: http://clinicaltrials.gov/ct2/show/NCT00695838. Accessed July 19, 2012.
6. Dupont WD, Plummer WD. PS power and sample size program available for free on the internet. Control Clin Trials. 1997;18:274.
7. Kahrilas PJ, Shaheen NJ, Vaezi MF; American Gastroenterological Association Institute; Clinical Practice and Quality Management Committee. American Gastroenterological Association Institute technical review on the management of gastroesophageal reflux disease. Gastroenterology. 2008;135:1392-1413, 1413.e1-e5.
8. El-Serag HB. Time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007;5:17-26.