User login
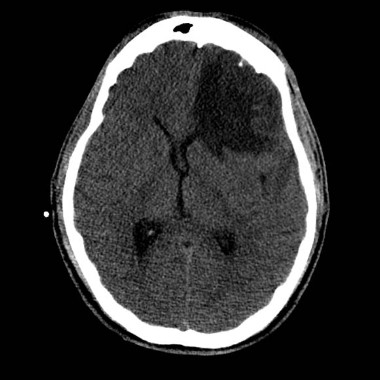
HONOLULU – Cerebral vasospasm and intracranial hypertension may be frequent secondary insults following wartime traumatic brain injury, according to a retrospective study of 122 consecutive veterans.
Transcranial Doppler (TCD) ultrasonography signs of mild, moderate, and severe vasospasm involving anterior circulation vessels were observed in 71%, 42%, and 16% of the veterans with traumatic brain injury (TBI), respectively.
TCD signs involving posterior circulation vessels were observed in 57%, 32%, and 14%, respectively.
Intracranial hypertension was recorded in 43% of patients, lead author Alexander Razumovsky, Ph.D., reported at the International Stroke Conference.
"Cerebral blood flow velocity measurements permit detection of early signs of cerebral vasospasm and allow physicians to better define management strategies," he said.
TCD monitoring is routinely used by the U.S. Army, but it has not been fully embraced elsewhere because many physicians are unaware of how it can be used within the continuum of TBI care to help reverse outcomes, said study coauthor Col. Rocco Armonda, MC, USA.
"There’s this lack of drive to change outcomes because people haven’t seen how you can take someone who is in a comatose state and eventually gain functional independence," said Dr. Armonda, who is the director of cerebrovascular surgery and interventional neuroradiology at the National Naval Medical Center in Bethesda, Md.
A recent study from Walter Reed National Military Medical Center (J. Trauma Acute Care Surg. 2012;73:1525-30), however, reported that 63% of veterans with a penetrating TBI and a mean discharge Glasgow Coma Scale (GCS) score of 6-8 progressed to functional independence – a number twice as high as would be expected, Dr. Armonda remarked.

Dr. Razumovsky said that simple, noninvasive TCD monitoring should be performed in the daily management of hospitalized TBI patients to complement other monitoring strategies, and it can be used alone in emergency situations when intracranial pressure monitoring is contraindicated or not readily available.
TCD monitoring is not necessary during outpatient follow-up of patients with TBI, with the exception of the subset who’ve undergone hemicraniectomy, Dr. Armonda said.
"In those patients who’ve had hemicraniectomy, some of them suffer prolonged duration from atmospheric pressure of the cranial defect, and TCD has actually been helpful to look at the cerebral blood flow dynamics," he said at a press briefing on the study.
The results confirm earlier data that TBI is associated with a high incidence of cerebral vasospasm, particularly in patients with severe TBI, and are applicable to civilian TBI patients because a significant number will experience post-traumatic bleeding that will lead to vasospasm and intracranial hypertension, said Dr. Razumovsky, director of Sentient NeuroCare Services in Hunt Valley, Md., which provides services to the National Naval Medical Hospital.

In the current study, patients were admitted to Walter Reed a mean of 6.7 days after injury from Oct. 1, 2008, to Nov. 30, 2012. Mean cerebral blood flow velocity (CBFV) of 100-139 cm/s was used to define mild vasospasm, 140-199 cm/s moderate vasospasm, and more than 200 cm/s severe vasospasm.
In all, 88 patients had penetrating head injury, of whom 45 (51%) had a secondary diagnosis of blast injury; and 34 patients had a closed head injury, of whom 15 (44%) had a secondary diagnosis of blast injury. Their mean age was 26 years.
In the mild vasospasm group, the mean anterior circulation CBFV was 122.5 cm/s and mean posterior CBFV was 61 cm/s. Their average GCS score changed from 8 at baseline to 6.1 at discharge, Dr. Razumovsky said.
In the moderate vasospasm group, the mean anterior circulation CBFV was 156.6 cm/s and mean posterior CBFV was 77.5 cm/s. Their average GCS score changed from 5.9 at baseline to 5.3 at discharge.
Patients with severe vasospasm had an average anterior circulation CBFV of 241.9 cm/s and a mean posterior CBFV of 101.8 cm/s. Their average GCS score was 4.8 at both time periods.
Eight patients (7%) underwent transluminal angioplasty for post-traumatic symptomatic vasospasm, he said at the meeting, sponsored by the American Heart Association.
Dr. Larry Goldstein, director of the Duke Stroke Center in Durham, N.C., said in an interview that the detection of vasospasm by TCD was potentially important because there is an increased risk of vasospasm after subarachnoid hemorrhage that can lead to delayed ischemic neurological deficits. Although it was unclear from the data how many patients had traumatic subarachnoid hemorrhage associated with their brain injury, he noted that the risk of vasospasm seems to be similar for traumatic and nontraumatic subarachnoid hemorrhage.
"In many centers, both groups of patients are routinely monitored with transcranial Dopplers over the first couple of weeks or so, which is when the peak period of vasospasm develops," Dr. Goldstein said. "Showing that monitoring leads to interventions that then change outcome, that’s not so straightforward."
The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
posterior circulation vessels, Alexander Razumovsky, Ph.D., the International Stroke Conference, Cerebral blood flow velocity, U.S. Army, Col. Rocco Armonda, MC, USA,
HONOLULU – Cerebral vasospasm and intracranial hypertension may be frequent secondary insults following wartime traumatic brain injury, according to a retrospective study of 122 consecutive veterans.
Transcranial Doppler (TCD) ultrasonography signs of mild, moderate, and severe vasospasm involving anterior circulation vessels were observed in 71%, 42%, and 16% of the veterans with traumatic brain injury (TBI), respectively.
TCD signs involving posterior circulation vessels were observed in 57%, 32%, and 14%, respectively.
Intracranial hypertension was recorded in 43% of patients, lead author Alexander Razumovsky, Ph.D., reported at the International Stroke Conference.
"Cerebral blood flow velocity measurements permit detection of early signs of cerebral vasospasm and allow physicians to better define management strategies," he said.
TCD monitoring is routinely used by the U.S. Army, but it has not been fully embraced elsewhere because many physicians are unaware of how it can be used within the continuum of TBI care to help reverse outcomes, said study coauthor Col. Rocco Armonda, MC, USA.
"There’s this lack of drive to change outcomes because people haven’t seen how you can take someone who is in a comatose state and eventually gain functional independence," said Dr. Armonda, who is the director of cerebrovascular surgery and interventional neuroradiology at the National Naval Medical Center in Bethesda, Md.
A recent study from Walter Reed National Military Medical Center (J. Trauma Acute Care Surg. 2012;73:1525-30), however, reported that 63% of veterans with a penetrating TBI and a mean discharge Glasgow Coma Scale (GCS) score of 6-8 progressed to functional independence – a number twice as high as would be expected, Dr. Armonda remarked.
Dr. Razumovsky said that simple, noninvasive TCD monitoring should be performed in the daily management of hospitalized TBI patients to complement other monitoring strategies, and it can be used alone in emergency situations when intracranial pressure monitoring is contraindicated or not readily available.
TCD monitoring is not necessary during outpatient follow-up of patients with TBI, with the exception of the subset who’ve undergone hemicraniectomy, Dr. Armonda said.
"In those patients who’ve had hemicraniectomy, some of them suffer prolonged duration from atmospheric pressure of the cranial defect, and TCD has actually been helpful to look at the cerebral blood flow dynamics," he said at a press briefing on the study.
The results confirm earlier data that TBI is associated with a high incidence of cerebral vasospasm, particularly in patients with severe TBI, and are applicable to civilian TBI patients because a significant number will experience post-traumatic bleeding that will lead to vasospasm and intracranial hypertension, said Dr. Razumovsky, director of Sentient NeuroCare Services in Hunt Valley, Md., which provides services to the National Naval Medical Hospital.
In the current study, patients were admitted to Walter Reed a mean of 6.7 days after injury from Oct. 1, 2008, to Nov. 30, 2012. Mean cerebral blood flow velocity (CBFV) of 100-139 cm/s was used to define mild vasospasm, 140-199 cm/s moderate vasospasm, and more than 200 cm/s severe vasospasm.
In all, 88 patients had penetrating head injury, of whom 45 (51%) had a secondary diagnosis of blast injury; and 34 patients had a closed head injury, of whom 15 (44%) had a secondary diagnosis of blast injury. Their mean age was 26 years.
In the mild vasospasm group, the mean anterior circulation CBFV was 122.5 cm/s and mean posterior CBFV was 61 cm/s. Their average GCS score changed from 8 at baseline to 6.1 at discharge, Dr. Razumovsky said.
In the moderate vasospasm group, the mean anterior circulation CBFV was 156.6 cm/s and mean posterior CBFV was 77.5 cm/s. Their average GCS score changed from 5.9 at baseline to 5.3 at discharge.
Patients with severe vasospasm had an average anterior circulation CBFV of 241.9 cm/s and a mean posterior CBFV of 101.8 cm/s. Their average GCS score was 4.8 at both time periods.
Eight patients (7%) underwent transluminal angioplasty for post-traumatic symptomatic vasospasm, he said at the meeting, sponsored by the American Heart Association.
Dr. Larry Goldstein, director of the Duke Stroke Center in Durham, N.C., said in an interview that the detection of vasospasm by TCD was potentially important because there is an increased risk of vasospasm after subarachnoid hemorrhage that can lead to delayed ischemic neurological deficits. Although it was unclear from the data how many patients had traumatic subarachnoid hemorrhage associated with their brain injury, he noted that the risk of vasospasm seems to be similar for traumatic and nontraumatic subarachnoid hemorrhage.
"In many centers, both groups of patients are routinely monitored with transcranial Dopplers over the first couple of weeks or so, which is when the peak period of vasospasm develops," Dr. Goldstein said. "Showing that monitoring leads to interventions that then change outcome, that’s not so straightforward."
The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
HONOLULU – Cerebral vasospasm and intracranial hypertension may be frequent secondary insults following wartime traumatic brain injury, according to a retrospective study of 122 consecutive veterans.
Transcranial Doppler (TCD) ultrasonography signs of mild, moderate, and severe vasospasm involving anterior circulation vessels were observed in 71%, 42%, and 16% of the veterans with traumatic brain injury (TBI), respectively.
TCD signs involving posterior circulation vessels were observed in 57%, 32%, and 14%, respectively.
Intracranial hypertension was recorded in 43% of patients, lead author Alexander Razumovsky, Ph.D., reported at the International Stroke Conference.
"Cerebral blood flow velocity measurements permit detection of early signs of cerebral vasospasm and allow physicians to better define management strategies," he said.
TCD monitoring is routinely used by the U.S. Army, but it has not been fully embraced elsewhere because many physicians are unaware of how it can be used within the continuum of TBI care to help reverse outcomes, said study coauthor Col. Rocco Armonda, MC, USA.
"There’s this lack of drive to change outcomes because people haven’t seen how you can take someone who is in a comatose state and eventually gain functional independence," said Dr. Armonda, who is the director of cerebrovascular surgery and interventional neuroradiology at the National Naval Medical Center in Bethesda, Md.
A recent study from Walter Reed National Military Medical Center (J. Trauma Acute Care Surg. 2012;73:1525-30), however, reported that 63% of veterans with a penetrating TBI and a mean discharge Glasgow Coma Scale (GCS) score of 6-8 progressed to functional independence – a number twice as high as would be expected, Dr. Armonda remarked.
Dr. Razumovsky said that simple, noninvasive TCD monitoring should be performed in the daily management of hospitalized TBI patients to complement other monitoring strategies, and it can be used alone in emergency situations when intracranial pressure monitoring is contraindicated or not readily available.
TCD monitoring is not necessary during outpatient follow-up of patients with TBI, with the exception of the subset who’ve undergone hemicraniectomy, Dr. Armonda said.
"In those patients who’ve had hemicraniectomy, some of them suffer prolonged duration from atmospheric pressure of the cranial defect, and TCD has actually been helpful to look at the cerebral blood flow dynamics," he said at a press briefing on the study.
The results confirm earlier data that TBI is associated with a high incidence of cerebral vasospasm, particularly in patients with severe TBI, and are applicable to civilian TBI patients because a significant number will experience post-traumatic bleeding that will lead to vasospasm and intracranial hypertension, said Dr. Razumovsky, director of Sentient NeuroCare Services in Hunt Valley, Md., which provides services to the National Naval Medical Hospital.
In the current study, patients were admitted to Walter Reed a mean of 6.7 days after injury from Oct. 1, 2008, to Nov. 30, 2012. Mean cerebral blood flow velocity (CBFV) of 100-139 cm/s was used to define mild vasospasm, 140-199 cm/s moderate vasospasm, and more than 200 cm/s severe vasospasm.
In all, 88 patients had penetrating head injury, of whom 45 (51%) had a secondary diagnosis of blast injury; and 34 patients had a closed head injury, of whom 15 (44%) had a secondary diagnosis of blast injury. Their mean age was 26 years.
In the mild vasospasm group, the mean anterior circulation CBFV was 122.5 cm/s and mean posterior CBFV was 61 cm/s. Their average GCS score changed from 8 at baseline to 6.1 at discharge, Dr. Razumovsky said.
In the moderate vasospasm group, the mean anterior circulation CBFV was 156.6 cm/s and mean posterior CBFV was 77.5 cm/s. Their average GCS score changed from 5.9 at baseline to 5.3 at discharge.
Patients with severe vasospasm had an average anterior circulation CBFV of 241.9 cm/s and a mean posterior CBFV of 101.8 cm/s. Their average GCS score was 4.8 at both time periods.
Eight patients (7%) underwent transluminal angioplasty for post-traumatic symptomatic vasospasm, he said at the meeting, sponsored by the American Heart Association.
Dr. Larry Goldstein, director of the Duke Stroke Center in Durham, N.C., said in an interview that the detection of vasospasm by TCD was potentially important because there is an increased risk of vasospasm after subarachnoid hemorrhage that can lead to delayed ischemic neurological deficits. Although it was unclear from the data how many patients had traumatic subarachnoid hemorrhage associated with their brain injury, he noted that the risk of vasospasm seems to be similar for traumatic and nontraumatic subarachnoid hemorrhage.
"In many centers, both groups of patients are routinely monitored with transcranial Dopplers over the first couple of weeks or so, which is when the peak period of vasospasm develops," Dr. Goldstein said. "Showing that monitoring leads to interventions that then change outcome, that’s not so straightforward."
The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.
posterior circulation vessels, Alexander Razumovsky, Ph.D., the International Stroke Conference, Cerebral blood flow velocity, U.S. Army, Col. Rocco Armonda, MC, USA,
posterior circulation vessels, Alexander Razumovsky, Ph.D., the International Stroke Conference, Cerebral blood flow velocity, U.S. Army, Col. Rocco Armonda, MC, USA,
AT THE INTERNATIONAL STROKE CONFERENCE
Major finding: Transcranial Doppler ultrasonography revealed signs of mild, moderate, and severe vasospasm involving anterior circulation vessels in 71%, 42%, and 16% of patients, respectively, but slightly less often in posterior circulation vessels (57%, 32%, and 14%).
Data source: A retrospective study of 122 consecutive patients with combat-related traumatic brain injury.
Disclosures: The study was supported in part by the U.S. Army Medical Research and Materiel Command’s Telemedicine and Advanced Technology Research Center. Dr. Razumovsky and two of his coauthors reported financial remuneration from private practice.