User login
OBJECTIVE: The chasm theory of marketing states that fundamental differences exist between early adopters of technology and the mainstream marketplace, making it difficult for technology to transition to the mainstream market. We investigated possible differences in attitudes and beliefs about electronic medical records (EMRs) between current EMR users (early market) and nonusers (mainstream market).
STUDY DESIGN: Cross-sectional mail survey.
POPULATION: Active members in the Indiana Academy of Family Physicians 2000–2001 membership database (N = 1328).
OUTCOMES MEASURED: Differences in attitudes, beliefs, and demographic characteristics of EMR users and nonusers.
RESULTS: The overall return rate was 51.7%; 14.4% of respondents currently use an EMR. Electronic medical record users were more likely to practice in urban areas or to be hospital-based and reported seeing fewer patients. Nonusers were less likely to believe that (1) physicians should computerize their medical records; (2) current EMRs are a useful tool for physicians; (3) EMRs improve quality of medical records and decrease errors; and (4) it is easy to enter data into current EMRs. Nonusers were more likely to believe that paper records are more secure and more confidential than EMRs. Both users and nonusers believed that current EMRs are too expensive.
CONCLUSIONS: A chasm exists between EMR users and nonusers regarding issues that affect EMR implementation, including necessity, usefulness, data entry, cost, security and confidentiality. To reach full implementation of EMRs in family medicine, organizations should use these data to target their research, education, and marketing efforts.
- Physicians have major concerns about data entry, cost, security, and confidentiality of current electronic medical records (EMRs), resulting in their questioning the need for EMRs and the usefulness of existing EMRS.
- There are large differences in the perceptions of physicians who do and do not use EMRs.
- Before EMRs will be accepted by a majority of family physicians, EMR companies must balance cost against the needs of mainstream family physicians.
—Clement J. McDonald, MD1
The benefits of using electronic medical records (EMRs) instead of paper records have been well documented.1-6 However, the current use (5% to 10%) falls very short of the 100% by the year 2000 recommended by a 1991 Institute of Medicine (IOM) report7; furthermore, the rate of EMR use has remained relatively unchanged (5% to 10%) over the past decade. Given this stagnant rate of growth despite the IOM’s support, it is important to analyze the needs and perceptions of physicians with regard to EMRs.
There are few articles on the use of EMRs in out-patient settings.1-20 Only 2 studies have analyzed the perceived needs and preferences for use of EMRs and family physicians.11,12 The first study found significant concerns about the ease of data entry, data confidentiality, data sharing, and initial EMR train-ing.11 The other article rated user requirements in rank order, but was limited by a 24% response rate.12 Most of the literature and information on the Internet about EMRs focuses on the needs and perceptions of current EMR users.1-20
The chasm theory of marketing (Figure) states that the early market of new product adopters (the first 5% to 10%) often has different concerns than the mainstream market. This group leaps ahead of the mainstream, creating a chasm.21 Early market adopters are more willing to endure technical difficulties and poor service to make a product work if it promises a competitive advantage, while mainstream users are more likely to look for widely used products that are inexpensive and easily assimilated into their current work environment with little organizational discomfort.21 Products engineered for the needs of the early market are often too complex to meet the needs of mainstream users; therefore, many products are unable to cross the chasm from early markets to mainstream markets because they fail to meet the needs of the mainstream users.21
This theory may explain the slow adoption of EMRs by family physicians. The purpose of this study was to investigate differences in attitudes and beliefs about EMRs between current EMR users (early market) and nonusers (mainstream market).
FIGURE 1
Chasm theory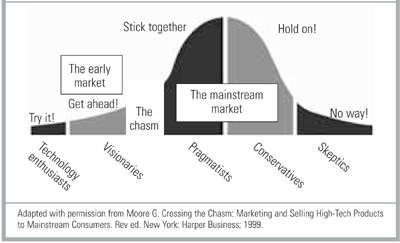
Methods
The study population comprised active members of the Indiana Academy of Family Physicians (IAFP) listed in the 2000–2001 IAFP Membership Database. IAFP members who were practicing outside of Indiana or who spent less than 4 hours per week seeing patients were excluded from the study, leaving a study population of 1398 participants.
The authors designed a 53-item questionnaire based on the principles outlined in the 1991 Institute of Medicine report.7,18,19 Six physicians with expertise in medical informatics screened the questionnaire for content validity. Twelve academic family physicians reviewed the instrument for structure, clarity, and relevance to test face validity. Ten resident physicians generated a test–retest reliability rate of >80% for each item over a 2-week interval.
The questionnaire consisted of 3 parts. The first section included questions about physician demographics, use of computer aided technology, practice location and type, and volume of patients. The second section contained questions about respondents’ attitudes, beliefs, and concerns regarding current and emerging technologic issues related to EMRs using a 4-point Likert scale ranging from “strongly agree” to “strongly disagree.” The Likert Scale also contained a “Don’t Know” option. The third section included multiple-choice questions to evaluate specific computer technology needs and preferences of family physicians. The final item was an open-ended question inviting a written response about any issues the respondent felt were not adequately addressed by the questionnaire.
Questionnaires were mailed in January 2001, with a followup mailing to nonrespondents 3 weeks later.22 Of the 726 (51.7%) responses, 45 (6.2%) were excluded because they did not indicate user or nonuser EMR status and 63 (8.8%) were excluded because half or more of the questions were unanswered. There were 618 (44.2%) usable surveys. The questionnaires were scanned into an electronic database and verified for accuracy using TELEform® software; the data were analyzed using SPSS® (Version 10.0). The Likert scales were collapsed to a dichotomous variable, “agree” (strongly agree and agree) and “disagree” (strongly disagree, disagree, and unsure) for this analysis. Differences in demographic characteristics and attitudes, beliefs, and concerns were tested for significance using chi-square tests and the z-test of proportions. Statistical significance was determined by P < .05.
Results
Demographic and practice characteristics of the respondents are presented in Table 1. Of the 618 respondents, 89 (14.4%) were EMR users. A comparison of the users and nonusers revealed that there were no statistically significant differences in age or sex. EMR nonusers were more likely to practice in a suburban or rural location and were more often in a solo or small practice (2–6 physicians). Nonusers also tended to see an average of 31 more patients per week (116 vs 85).
Table 2 presents responses to questions about respondents’ experience with computer technology. A significantly greater proportion of EMR users use the Internet at home (98.9% vs 89.3%), at work (88.6% vs 62.8%), e-mail at work (78.4% vs 48.2%), and personal digital assistants (PDAs) (49.4% vs 26.1%). Other differences in technology use were not statistically significant.
Responses to questions about perceived EMR need and usefulness are summarized in Table 3. Nonusers were significantly less likely than users to believe that (1) physicians should computerize their medical records (67.7% vs 92.1%); (2) current EMRs are useful (51.5% vs 92.0%); (3) EMRs will reduce their risk of making medical errors (56.6% vs 78.7%); and (4) EMRs will improve health care quality in their office (52.4% vs 80.9%) or in the United States overall (54.3% vs 78.4%). Most respondents (77.6%) expressed an interest in an EMR system that would connect all physician practices, laboratories, radiography facilities, and hospitals for the secure exchange of patient data (85.4% user vs 76.2% nonuser; P = .076).
Table 4 summarizes the attitudes and beliefs of respondents about previously reported potential obstacles to EMR use, including: (1) data input; (2) cost; and (3) confidentiality and security.1,11,12,14,17-20,23,24 Few respondents (55.1% users vs 13.4% nonusers) stated that it is easy to enter data into current EMRs. Many respondents in both groups (61.8% vs 68.0%) responded that EMRs are too costly. Users tend to consider a relatively higher price as affordable for setting up an EMR system (66% would pay more than $5000) and are willing to pay a slightly higher monthly fee for the ongoing use of an EMR (65% would pay more than $100 per month). Users consider EMRs as more secure (54.5% users vs 21.2% nonusers) and more confidential (62.5% users vs 21.9% nonusers) than paper records. Few respondents stated they would object to sharing their EMR data with other physicians (24.9% nonusers vs 13.6% users).
TABLE 1
Demographic characteristics of respondents
| Characteristic | User n (%) | Nonuser n (%) | P |
|---|---|---|---|
| Female | 23 (26.1) | 131 (25.0) | .925 |
| Mean age (y) | 44.1 (8.84 SD) | 44.6 (9.29 SD) | .059 |
| Mean number of outpatient visits per week | 85.1 (51.4 SD) | 116.1 (55.2 SD) | <.001 |
| County type | |||
| Rural | 26 (29.5) | 194 (37.2) | .013 |
| Suburban | 28 (31.8) | 204 (39.1) | |
| Urban | 34 (38.6) | 124 (23.8) | |
| Practice setting | |||
| Solo | 12 (13.6) | 101 (19.3) | .003 |
| Small FP (2–6) | 21 (23.9) | 191 (36.5) | |
| Large FP (>6) | 8 (9.1) | 55 (10.5) | |
| Multispecialty group | 9 (10.2) | 54 (10.3) | |
| Hospital employee | 25 (28.4) | 91 (17.4) | |
| Other | 13 (14.8) | 31 (5.9) | |
| 89 users and 529 nonusers responded. | |||
| The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
| FP, family practice; SD, standard deviation. | |||
TABLE 2
Technology use by respondents
| User n (%) | Nonuser n (%) | P | |
|---|---|---|---|
| Computer use at home | |||
| Computer | 89/89 (100.0) | 507/527 (96.2) | .122 |
| Internet | 88/89 (98.9) | 467/523 (89.3) | .007 |
| 83/89 (93.3) | 451/521 (86.6) | .111 | |
| Computer use at work | |||
| Computer | 86/87 (98.9) | 467/506 (92.3) | .043 |
| Internet | 78/88 (88.6) | 318/506 (62.8) | <.001 |
| 69/88 (78.4) | 242/502 (48.2) | <.001 | |
| Computerized scheduling | 83/89 (93.3) | 420/526 (79.8) | .004 |
| Computerized billing | 79/84 (94.0) | 458/489 (93.7) | .999 |
| Handheld computer user | 44/89 (49.4) | 137/525 (26.1) | <.001 |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
TABLE 3
Attitudes and beliefs regarding electronic medical records
| Number (%) agreeing with statement | P | ||
|---|---|---|---|
| User | Nonuser | ||
| Physicians should computerize their medical records | 82/89 (92.1) | 354/523 (67.7) | <.001 |
| Currently available EMRs are a useful tool for physicians (92.0) (51.5) | 81/88 | 269/522 | <.001 |
| EMRs will improve the quality of care in physicians’ offices | 72/89 (80.9) | 274/523 (52.4) | <.001 |
| Widespread use of EMRs would improve healthcare quality in the United States | 69/88 (78.4) | 283/521 (54.3) | <.001 |
| EMRs will reduce my risk of making medical errors | 70/89 (78.7) | 297/525 (56.6) | <.001 |
| I am interested in an EMR that would connect all physician practices, labs, x-ray facilities, and hospitals in my area securely for the exchange of patient data | 76/89 (85.4) | 398/522 (76.2) | .076 |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
| EMR, electronic medical records. | |||
TABLE 4
Possible barriers to electronic medical record use
| Number (%) agreeing with statement | P | ||
|---|---|---|---|
| User | Nonuser | ||
| Security and confidentiality | |||
| EMRs are more secure | 48/88 (54.5) | 111/523 (21.2) | <.001 |
| EMRs are more confidential | 55/88 (62.5) | 115/524 (21.9) | <.001 |
| Object to sharing EMR data with other physicians | 11/81 (13.6) | 121/486 (24.9) | .037 |
| Usefulness | |||
| Easy to enter data | 49/89 (55.1) | 70/521 (13.4) | <.001 |
| Ability to use an EMR with minimal training | 79/87 (90.8) | 479/522 (91.8) | .929 |
| Would like direct link to Medline | 73/88 (83.0) | 298/522 (57.1) | <.001 |
| Would like direct links to updated treatment guidelines | 73/87 (83.9) | 360/521 (69.1) | .007 |
| Would like direct link to patient education materials | 83/88 (94.3) | 421/520 (81.0) | .003 |
| EMR data should be available without patient or physician identifiers for use in clinical and health care services research | 46/89 (51.7) | 263/521 (50.5) | .924 |
| Costs | |||
| Current EMRs are too costly | 55/89 (61.8) | 355/522 (68.0) | <.001 |
| Affordable price per physician to set up an EMR system | |||
| <$1000 | 5/77 (6.5) | 65/464 (14.0) | <.001 |
| $1000–$4999 | 21/77 (27.3) | 202/464 (43.5) | |
| $5000–$9999 | 27/77 (35.1) | 147/464 (31.7) | |
| $10,000–$19,999 | 17/77 (22.1) | 42/464 (9.1) | |
| >$20,000 | 7/77 (9.1) | 8/464 (1.7) | |
| Willing to spend monthly for ongoing use of an EMR | |||
| <$50 | 3 (3.9) | 89 (19.7) | .013 |
| $50–$99 | 23 (30.3) | 101 (22.4) | |
| $100–$149 | 25 (32.9) | 139 (30.8) | |
| $150–$199 | 14 (18.4) | 79 (17.5) | |
| >$200 | 11 (14.5) | 43 (9.5) | |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. EMR, electronic medical records. | |||
Discussion
Despite the low penetration of EMRs (14.4%), family physicians in Indiana are interested in using EMRs. Most users (85.4%) and nonusers (76.2%) expressed interest in a system that would securely connect all physician practices, laboratories, radiography facilities, and hospitals in their area for exchanging patient data. Many family physicians are currently using the Internet (67%), e-mail (53%), computers (93%), and PDAs (30%) in their practice.
Despite this expressed interest, only two thirds of nonusers believe that physicians should computerize their medical records. This may be related to the fact that only half of the responding nonusers perceive that current EMRs are useful for physicians. There was also a considerable lack of belief that EMRs will improve quality or reduce medical errors. Replies to the open-ended question indicated that 5% to 10% of respondents, for a variety of reasons, have strong feelings about computerizing their offices. A targeted, educational effort to show the advantages of EMRs may be useful for improving physician perceptions of EMRs.
The demographic profile of the nonusers may indicate that current EMRs are not perceived as being well adapted for use in rural, solo, or small-group practice. EMRs may be thought of as more feasible for larger organizations with larger capital budgets and robust information technology support systems. The differences in the volume of patients treated between users and nonusers suggest that productivity concerns may also be important.
Both EMR users and nonusers believe current EMRs are too costly. The data suggests that family physicians are willing to pay a relatively low set-up charge <$5000 would be accepted by more than 87% of respondents) and a very low monthly fee (<$100 would be accepted by more than 81% of respondents) for the use of an EMR. Few current EMRs can be installed and operated within these price specifications. This supports the previously published view that physicians believe current EMRs are not cost effective.17 Lower prices or greater perceived value is needed for physicians to consider EMRs a wise business choice.
Data entry is a concern for both users and nonusers. Practicing family medicine requires varied skills, a fast pace, treating patients from multiple age groups, diagnosing conditions from a myriad of potentially unrelated complaints, and keeping a comprehensive record from multiple sources. These factors make data entry the largest potential obstacle to the effective use of computers in family medi-cine.1,14,18-20 Our data indicate that only 55% of users and 13.4% of nonusers believe data entry is easy for current EMRs. Perceived and actual ease of data entry must be improved before widespread adoption of EMRs by family physicians can be realized.
Concerns about security and confidentiality generated the largest number of written comments. Despite evidence to the contrary,9,23,24,28,29 nonusers believe that there are more security and confidentiality risks involved with EMRs than paper records. A small group emphatically expressed dismay at the possibility of subjecting their office to a “Big Brother”-type system. The Health Insurance Portability and Accountability Act (HIPAA) sets the standards for medical record (electronic and written) confidentiality and security, and the creation of an EMR that is HIPAA compliant may give providers greater confidence in its security and confidentiality.23,24 Educating physicians about the security and confidentiality risks of paper records and the safeguards built into EMR programs may help alleviate these concerns.
It is encouraging that both users and nonusers seem to understand the potential usefulness of EMRs. Over half of the nonusers believe an EMR is a useful way to provide patient education materials, participate in clinical and health services research, launch a literature search (eg, Medline), or obtain up-to-date treatment guidelines. To increase the number of physicians using EMRs, vendors should maximize and promote the use of EMR features.
The results of this study are limited by the response rate. Although this rate introduces the possibility of a nonresponse bias, it is comparable to or exceeds the response rate in other physician EMR surveys.11,12,23-27 Evidence of nonresponse bias includes the high rate of EMR use by Indiana family physicians (14.4%) compared to previous studies, suggesting users were more likely to respond than nonusers. Questionnaires that were returned early in the survey showed an EMR use rate of 40%, but this number dropped quickly after the first 2 weeks. A very small percentage of questionnaires returned near the end of the study were from EMR users. The nonresponse bias of the study is likely toward EMR users and nonusers who have seriously considered using EMRs; since this is the segment of the physician market most likely to adopt EMRs, the sample is likely adequate for the attempted analysis. The study is also limited by its focus on family physicians in Indiana, and may differ from the views of physicians in other specialties or states.
Conclusions
Our data demonstrate the existence of a chasm between EMR users (early adopters) and nonusers (mainstream market) regarding attitudes and perceptions that impact the implementation of EMRs by family physicians. Specifically, EMR nonusers exhibit the following important differences from users: (1) less perceived need for EMRs; (2) greater concerns about EMR data entry; (3) less confidence in the security and confidentiality of EMRs; and (4) more concerns about the cost for installation and ongoing use of EMRs.
Further studies are needed to examine nonusers in more detail and to discover if current EMRs can meet the needs of the mainstream physician user. Our research suggests that data entry, cost, security and confidentiality, and connectivity issues are important starting points. A qualitative study of nonusers is desirable to better understand the true needs of the mainstream physician. Broadening this study to include all specialties throughout the country would also be useful.
The IOM has repeatedly called for the computerization of the US medical system.7,28,29 Government, industry, and physician organizations should use the results of this study to target their research, education, and marketing efforts regarding EMRs, and to develop EMRs that meet the needs of most practicing family physicians, especially family physicians in small group, high-volume, rural or suburban practices.
Acknowledgments
This study was undertaken as part of the faculty development fellowship at the University of North Carolina Department of Family Medicine and funded by the Bureau of Health Professions grant no. HRSA#1-D14-HP00019. We thank the Indiana Academy of Family Physicians, St. Francis Family Practice Residency, Indiana University Department of Family Medicine, Bowen Research Center, UNC Faculty Development Fellowship 2000–2001 fellows, Nancy Loomis, and Jenny Kirby for their support.
1. McDonald CJ. The barriers to electronic medical record systems and how to overcome them. J Am Med Inform Assoc 1997;4:213-21.
2. Wager KA, SM Ornstein, Jenkins RG. Perceived value of computer-based patient records among clinician users. MD Comput 1997;14:334-6,338-340.
3. Wager KA, Lee FW, White AW, Ward DM, Ornstein SM. Impact of an electronic medical record system on community-based primary care practices. J Am Board Fam Pract 2000;13:338-48.
4. Spann SJ. Should the complete medical record be computerized in family practice? An affirmative view. J Fam Pract 1990;30:457-60.
5. Ornstein SM. Electronic medical records in family practice: the time is now. J Fam Pract 1997;44:45-8.
6. Rodnick JE. Should the complete medical record be computerized in family practice? An opposing view. J Fam Pract 1990;30:460-4.
7. Dick RS. The Institute of Medicine’s patient record study and its implications for record administrators. Top Health Rec Manage 1991;11:67-72.
8. Swanson T, Dostal J, Eichhorst B, Jernigan C, Knox M, Roper K. Recent implementations of electronic medical records in four family practice residency programs. Acad Med 1997;72:607-12.
9. Woodward B. The computer-based patient record and confidentiality. N Engl J Med 1995;333:1419-22.
10. Wager KA, Heda S, Austin CJ. Developing a health information network within an integrated delivery system: a case study. Top Health Inf Manage 1997;17:20-31.
11. Strasberg HR, Tudiver F, Holbrook AM, Geiger G, Keshavjee KK, Troyan S. Moving towards an electronic patient record: a survey to assess the needs of community family physicians. Proc AMIA Symp 1998;230-4.
12. Smith WR, Zastrow R. User requirements for the computerized patient record: physician opinions. Proc Annu Symp Comput Appl Med Care 1994;994.-
13. Powsner SM, Wyatt JC, Wright P. Opportunities for and challenges of computerisation. Lancet 1998;352:1617-22.
14. Musham C, Orstein SM, Jenkins RG. Family practice educators’ perceptions of computer-based patient records. Fam Med 1995;27:571-5.
15. Arias-Vimarlund V, Ljunggren M, Timpka T. Implementation of computer-based patient records in primary care: the societal health economic effects. Proc AMIA Annu Fall Symp 1996;503-7.
16. Lawler F, Cacy JR, Viviani N, Hamm RM, Cobb SW. Implementation and termination of a computerized medical information system. J Fam Pract 1996;42:233-6.
17. Lindberg DA, Humpreys BL. Medical informatics. JAMA 1996;275:1821-2.
18. Levitt JI. Why physicians continue to reject the computerized medical record. Minn Med 1994;7(8):17-21.
19. Lenhart JG, Honess K, Covington D, Johnson KE. An analysis of trends, perceptions, and use patterns of electronic medical records among US family practice residency programs. Fam Med 2000;32:109-14.
20. Bernstein RM, Hollingworth GR, Viner G, Lemelin J. Family practice informatics: research issues in computerized medical records. Proc Annu Symp Comput Appl Med Care 1993;93-7.
21. Moore G. Crossing the Chasm: Marketing and Selling High-Tech Products to Mainstream Consumers. Rev ed. New York: Harper Business; 1999.
22. Dillman DA. Mail and Internet Surveys: The Tailored Design Method. 2nd ed. New York: John Wiley & Sons; 1999.
23. Kibbe DC. A problem-oriented approach to the HIPAA security standards. Fam Pract Manag 2001;8(7):37-43.
24. Kibbe DC. What you need to know about HIPAA now. Fam Pract Manag 2001;8(3):43-7.
25. Bomba D. A comparative study of computerised medical records usage among general practitioners in Australia and Sweden. Medinfo 1998;(Pt 1):55-9.
26. Ebell MH, Gaspar DL, Khurana S. Family physicians’ p for computerized decision-support hardware and software. J Fam Pract 1997;45:137-41.
27. Kalsman MW, Acosta DA. Use of the Internet as a medical resource by rural physicians. J Am Board Fam Pract 2000;13:349-52.
28. Committee on Quality Healthcare in America, eds. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
29. Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
OBJECTIVE: The chasm theory of marketing states that fundamental differences exist between early adopters of technology and the mainstream marketplace, making it difficult for technology to transition to the mainstream market. We investigated possible differences in attitudes and beliefs about electronic medical records (EMRs) between current EMR users (early market) and nonusers (mainstream market).
STUDY DESIGN: Cross-sectional mail survey.
POPULATION: Active members in the Indiana Academy of Family Physicians 2000–2001 membership database (N = 1328).
OUTCOMES MEASURED: Differences in attitudes, beliefs, and demographic characteristics of EMR users and nonusers.
RESULTS: The overall return rate was 51.7%; 14.4% of respondents currently use an EMR. Electronic medical record users were more likely to practice in urban areas or to be hospital-based and reported seeing fewer patients. Nonusers were less likely to believe that (1) physicians should computerize their medical records; (2) current EMRs are a useful tool for physicians; (3) EMRs improve quality of medical records and decrease errors; and (4) it is easy to enter data into current EMRs. Nonusers were more likely to believe that paper records are more secure and more confidential than EMRs. Both users and nonusers believed that current EMRs are too expensive.
CONCLUSIONS: A chasm exists between EMR users and nonusers regarding issues that affect EMR implementation, including necessity, usefulness, data entry, cost, security and confidentiality. To reach full implementation of EMRs in family medicine, organizations should use these data to target their research, education, and marketing efforts.
- Physicians have major concerns about data entry, cost, security, and confidentiality of current electronic medical records (EMRs), resulting in their questioning the need for EMRs and the usefulness of existing EMRS.
- There are large differences in the perceptions of physicians who do and do not use EMRs.
- Before EMRs will be accepted by a majority of family physicians, EMR companies must balance cost against the needs of mainstream family physicians.
—Clement J. McDonald, MD1
The benefits of using electronic medical records (EMRs) instead of paper records have been well documented.1-6 However, the current use (5% to 10%) falls very short of the 100% by the year 2000 recommended by a 1991 Institute of Medicine (IOM) report7; furthermore, the rate of EMR use has remained relatively unchanged (5% to 10%) over the past decade. Given this stagnant rate of growth despite the IOM’s support, it is important to analyze the needs and perceptions of physicians with regard to EMRs.
There are few articles on the use of EMRs in out-patient settings.1-20 Only 2 studies have analyzed the perceived needs and preferences for use of EMRs and family physicians.11,12 The first study found significant concerns about the ease of data entry, data confidentiality, data sharing, and initial EMR train-ing.11 The other article rated user requirements in rank order, but was limited by a 24% response rate.12 Most of the literature and information on the Internet about EMRs focuses on the needs and perceptions of current EMR users.1-20
The chasm theory of marketing (Figure) states that the early market of new product adopters (the first 5% to 10%) often has different concerns than the mainstream market. This group leaps ahead of the mainstream, creating a chasm.21 Early market adopters are more willing to endure technical difficulties and poor service to make a product work if it promises a competitive advantage, while mainstream users are more likely to look for widely used products that are inexpensive and easily assimilated into their current work environment with little organizational discomfort.21 Products engineered for the needs of the early market are often too complex to meet the needs of mainstream users; therefore, many products are unable to cross the chasm from early markets to mainstream markets because they fail to meet the needs of the mainstream users.21
This theory may explain the slow adoption of EMRs by family physicians. The purpose of this study was to investigate differences in attitudes and beliefs about EMRs between current EMR users (early market) and nonusers (mainstream market).
FIGURE 1
Chasm theory
Methods
The study population comprised active members of the Indiana Academy of Family Physicians (IAFP) listed in the 2000–2001 IAFP Membership Database. IAFP members who were practicing outside of Indiana or who spent less than 4 hours per week seeing patients were excluded from the study, leaving a study population of 1398 participants.
The authors designed a 53-item questionnaire based on the principles outlined in the 1991 Institute of Medicine report.7,18,19 Six physicians with expertise in medical informatics screened the questionnaire for content validity. Twelve academic family physicians reviewed the instrument for structure, clarity, and relevance to test face validity. Ten resident physicians generated a test–retest reliability rate of >80% for each item over a 2-week interval.
The questionnaire consisted of 3 parts. The first section included questions about physician demographics, use of computer aided technology, practice location and type, and volume of patients. The second section contained questions about respondents’ attitudes, beliefs, and concerns regarding current and emerging technologic issues related to EMRs using a 4-point Likert scale ranging from “strongly agree” to “strongly disagree.” The Likert Scale also contained a “Don’t Know” option. The third section included multiple-choice questions to evaluate specific computer technology needs and preferences of family physicians. The final item was an open-ended question inviting a written response about any issues the respondent felt were not adequately addressed by the questionnaire.
Questionnaires were mailed in January 2001, with a followup mailing to nonrespondents 3 weeks later.22 Of the 726 (51.7%) responses, 45 (6.2%) were excluded because they did not indicate user or nonuser EMR status and 63 (8.8%) were excluded because half or more of the questions were unanswered. There were 618 (44.2%) usable surveys. The questionnaires were scanned into an electronic database and verified for accuracy using TELEform® software; the data were analyzed using SPSS® (Version 10.0). The Likert scales were collapsed to a dichotomous variable, “agree” (strongly agree and agree) and “disagree” (strongly disagree, disagree, and unsure) for this analysis. Differences in demographic characteristics and attitudes, beliefs, and concerns were tested for significance using chi-square tests and the z-test of proportions. Statistical significance was determined by P < .05.
Results
Demographic and practice characteristics of the respondents are presented in Table 1. Of the 618 respondents, 89 (14.4%) were EMR users. A comparison of the users and nonusers revealed that there were no statistically significant differences in age or sex. EMR nonusers were more likely to practice in a suburban or rural location and were more often in a solo or small practice (2–6 physicians). Nonusers also tended to see an average of 31 more patients per week (116 vs 85).
Table 2 presents responses to questions about respondents’ experience with computer technology. A significantly greater proportion of EMR users use the Internet at home (98.9% vs 89.3%), at work (88.6% vs 62.8%), e-mail at work (78.4% vs 48.2%), and personal digital assistants (PDAs) (49.4% vs 26.1%). Other differences in technology use were not statistically significant.
Responses to questions about perceived EMR need and usefulness are summarized in Table 3. Nonusers were significantly less likely than users to believe that (1) physicians should computerize their medical records (67.7% vs 92.1%); (2) current EMRs are useful (51.5% vs 92.0%); (3) EMRs will reduce their risk of making medical errors (56.6% vs 78.7%); and (4) EMRs will improve health care quality in their office (52.4% vs 80.9%) or in the United States overall (54.3% vs 78.4%). Most respondents (77.6%) expressed an interest in an EMR system that would connect all physician practices, laboratories, radiography facilities, and hospitals for the secure exchange of patient data (85.4% user vs 76.2% nonuser; P = .076).
Table 4 summarizes the attitudes and beliefs of respondents about previously reported potential obstacles to EMR use, including: (1) data input; (2) cost; and (3) confidentiality and security.1,11,12,14,17-20,23,24 Few respondents (55.1% users vs 13.4% nonusers) stated that it is easy to enter data into current EMRs. Many respondents in both groups (61.8% vs 68.0%) responded that EMRs are too costly. Users tend to consider a relatively higher price as affordable for setting up an EMR system (66% would pay more than $5000) and are willing to pay a slightly higher monthly fee for the ongoing use of an EMR (65% would pay more than $100 per month). Users consider EMRs as more secure (54.5% users vs 21.2% nonusers) and more confidential (62.5% users vs 21.9% nonusers) than paper records. Few respondents stated they would object to sharing their EMR data with other physicians (24.9% nonusers vs 13.6% users).
TABLE 1
Demographic characteristics of respondents
| Characteristic | User n (%) | Nonuser n (%) | P |
|---|---|---|---|
| Female | 23 (26.1) | 131 (25.0) | .925 |
| Mean age (y) | 44.1 (8.84 SD) | 44.6 (9.29 SD) | .059 |
| Mean number of outpatient visits per week | 85.1 (51.4 SD) | 116.1 (55.2 SD) | <.001 |
| County type | |||
| Rural | 26 (29.5) | 194 (37.2) | .013 |
| Suburban | 28 (31.8) | 204 (39.1) | |
| Urban | 34 (38.6) | 124 (23.8) | |
| Practice setting | |||
| Solo | 12 (13.6) | 101 (19.3) | .003 |
| Small FP (2–6) | 21 (23.9) | 191 (36.5) | |
| Large FP (>6) | 8 (9.1) | 55 (10.5) | |
| Multispecialty group | 9 (10.2) | 54 (10.3) | |
| Hospital employee | 25 (28.4) | 91 (17.4) | |
| Other | 13 (14.8) | 31 (5.9) | |
| 89 users and 529 nonusers responded. | |||
| The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
| FP, family practice; SD, standard deviation. | |||
TABLE 2
Technology use by respondents
| User n (%) | Nonuser n (%) | P | |
|---|---|---|---|
| Computer use at home | |||
| Computer | 89/89 (100.0) | 507/527 (96.2) | .122 |
| Internet | 88/89 (98.9) | 467/523 (89.3) | .007 |
| 83/89 (93.3) | 451/521 (86.6) | .111 | |
| Computer use at work | |||
| Computer | 86/87 (98.9) | 467/506 (92.3) | .043 |
| Internet | 78/88 (88.6) | 318/506 (62.8) | <.001 |
| 69/88 (78.4) | 242/502 (48.2) | <.001 | |
| Computerized scheduling | 83/89 (93.3) | 420/526 (79.8) | .004 |
| Computerized billing | 79/84 (94.0) | 458/489 (93.7) | .999 |
| Handheld computer user | 44/89 (49.4) | 137/525 (26.1) | <.001 |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
TABLE 3
Attitudes and beliefs regarding electronic medical records
| Number (%) agreeing with statement | P | ||
|---|---|---|---|
| User | Nonuser | ||
| Physicians should computerize their medical records | 82/89 (92.1) | 354/523 (67.7) | <.001 |
| Currently available EMRs are a useful tool for physicians (92.0) (51.5) | 81/88 | 269/522 | <.001 |
| EMRs will improve the quality of care in physicians’ offices | 72/89 (80.9) | 274/523 (52.4) | <.001 |
| Widespread use of EMRs would improve healthcare quality in the United States | 69/88 (78.4) | 283/521 (54.3) | <.001 |
| EMRs will reduce my risk of making medical errors | 70/89 (78.7) | 297/525 (56.6) | <.001 |
| I am interested in an EMR that would connect all physician practices, labs, x-ray facilities, and hospitals in my area securely for the exchange of patient data | 76/89 (85.4) | 398/522 (76.2) | .076 |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
| EMR, electronic medical records. | |||
TABLE 4
Possible barriers to electronic medical record use
| Number (%) agreeing with statement | P | ||
|---|---|---|---|
| User | Nonuser | ||
| Security and confidentiality | |||
| EMRs are more secure | 48/88 (54.5) | 111/523 (21.2) | <.001 |
| EMRs are more confidential | 55/88 (62.5) | 115/524 (21.9) | <.001 |
| Object to sharing EMR data with other physicians | 11/81 (13.6) | 121/486 (24.9) | .037 |
| Usefulness | |||
| Easy to enter data | 49/89 (55.1) | 70/521 (13.4) | <.001 |
| Ability to use an EMR with minimal training | 79/87 (90.8) | 479/522 (91.8) | .929 |
| Would like direct link to Medline | 73/88 (83.0) | 298/522 (57.1) | <.001 |
| Would like direct links to updated treatment guidelines | 73/87 (83.9) | 360/521 (69.1) | .007 |
| Would like direct link to patient education materials | 83/88 (94.3) | 421/520 (81.0) | .003 |
| EMR data should be available without patient or physician identifiers for use in clinical and health care services research | 46/89 (51.7) | 263/521 (50.5) | .924 |
| Costs | |||
| Current EMRs are too costly | 55/89 (61.8) | 355/522 (68.0) | <.001 |
| Affordable price per physician to set up an EMR system | |||
| <$1000 | 5/77 (6.5) | 65/464 (14.0) | <.001 |
| $1000–$4999 | 21/77 (27.3) | 202/464 (43.5) | |
| $5000–$9999 | 27/77 (35.1) | 147/464 (31.7) | |
| $10,000–$19,999 | 17/77 (22.1) | 42/464 (9.1) | |
| >$20,000 | 7/77 (9.1) | 8/464 (1.7) | |
| Willing to spend monthly for ongoing use of an EMR | |||
| <$50 | 3 (3.9) | 89 (19.7) | .013 |
| $50–$99 | 23 (30.3) | 101 (22.4) | |
| $100–$149 | 25 (32.9) | 139 (30.8) | |
| $150–$199 | 14 (18.4) | 79 (17.5) | |
| >$200 | 11 (14.5) | 43 (9.5) | |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. EMR, electronic medical records. | |||
Discussion
Despite the low penetration of EMRs (14.4%), family physicians in Indiana are interested in using EMRs. Most users (85.4%) and nonusers (76.2%) expressed interest in a system that would securely connect all physician practices, laboratories, radiography facilities, and hospitals in their area for exchanging patient data. Many family physicians are currently using the Internet (67%), e-mail (53%), computers (93%), and PDAs (30%) in their practice.
Despite this expressed interest, only two thirds of nonusers believe that physicians should computerize their medical records. This may be related to the fact that only half of the responding nonusers perceive that current EMRs are useful for physicians. There was also a considerable lack of belief that EMRs will improve quality or reduce medical errors. Replies to the open-ended question indicated that 5% to 10% of respondents, for a variety of reasons, have strong feelings about computerizing their offices. A targeted, educational effort to show the advantages of EMRs may be useful for improving physician perceptions of EMRs.
The demographic profile of the nonusers may indicate that current EMRs are not perceived as being well adapted for use in rural, solo, or small-group practice. EMRs may be thought of as more feasible for larger organizations with larger capital budgets and robust information technology support systems. The differences in the volume of patients treated between users and nonusers suggest that productivity concerns may also be important.
Both EMR users and nonusers believe current EMRs are too costly. The data suggests that family physicians are willing to pay a relatively low set-up charge <$5000 would be accepted by more than 87% of respondents) and a very low monthly fee (<$100 would be accepted by more than 81% of respondents) for the use of an EMR. Few current EMRs can be installed and operated within these price specifications. This supports the previously published view that physicians believe current EMRs are not cost effective.17 Lower prices or greater perceived value is needed for physicians to consider EMRs a wise business choice.
Data entry is a concern for both users and nonusers. Practicing family medicine requires varied skills, a fast pace, treating patients from multiple age groups, diagnosing conditions from a myriad of potentially unrelated complaints, and keeping a comprehensive record from multiple sources. These factors make data entry the largest potential obstacle to the effective use of computers in family medi-cine.1,14,18-20 Our data indicate that only 55% of users and 13.4% of nonusers believe data entry is easy for current EMRs. Perceived and actual ease of data entry must be improved before widespread adoption of EMRs by family physicians can be realized.
Concerns about security and confidentiality generated the largest number of written comments. Despite evidence to the contrary,9,23,24,28,29 nonusers believe that there are more security and confidentiality risks involved with EMRs than paper records. A small group emphatically expressed dismay at the possibility of subjecting their office to a “Big Brother”-type system. The Health Insurance Portability and Accountability Act (HIPAA) sets the standards for medical record (electronic and written) confidentiality and security, and the creation of an EMR that is HIPAA compliant may give providers greater confidence in its security and confidentiality.23,24 Educating physicians about the security and confidentiality risks of paper records and the safeguards built into EMR programs may help alleviate these concerns.
It is encouraging that both users and nonusers seem to understand the potential usefulness of EMRs. Over half of the nonusers believe an EMR is a useful way to provide patient education materials, participate in clinical and health services research, launch a literature search (eg, Medline), or obtain up-to-date treatment guidelines. To increase the number of physicians using EMRs, vendors should maximize and promote the use of EMR features.
The results of this study are limited by the response rate. Although this rate introduces the possibility of a nonresponse bias, it is comparable to or exceeds the response rate in other physician EMR surveys.11,12,23-27 Evidence of nonresponse bias includes the high rate of EMR use by Indiana family physicians (14.4%) compared to previous studies, suggesting users were more likely to respond than nonusers. Questionnaires that were returned early in the survey showed an EMR use rate of 40%, but this number dropped quickly after the first 2 weeks. A very small percentage of questionnaires returned near the end of the study were from EMR users. The nonresponse bias of the study is likely toward EMR users and nonusers who have seriously considered using EMRs; since this is the segment of the physician market most likely to adopt EMRs, the sample is likely adequate for the attempted analysis. The study is also limited by its focus on family physicians in Indiana, and may differ from the views of physicians in other specialties or states.
Conclusions
Our data demonstrate the existence of a chasm between EMR users (early adopters) and nonusers (mainstream market) regarding attitudes and perceptions that impact the implementation of EMRs by family physicians. Specifically, EMR nonusers exhibit the following important differences from users: (1) less perceived need for EMRs; (2) greater concerns about EMR data entry; (3) less confidence in the security and confidentiality of EMRs; and (4) more concerns about the cost for installation and ongoing use of EMRs.
Further studies are needed to examine nonusers in more detail and to discover if current EMRs can meet the needs of the mainstream physician user. Our research suggests that data entry, cost, security and confidentiality, and connectivity issues are important starting points. A qualitative study of nonusers is desirable to better understand the true needs of the mainstream physician. Broadening this study to include all specialties throughout the country would also be useful.
The IOM has repeatedly called for the computerization of the US medical system.7,28,29 Government, industry, and physician organizations should use the results of this study to target their research, education, and marketing efforts regarding EMRs, and to develop EMRs that meet the needs of most practicing family physicians, especially family physicians in small group, high-volume, rural or suburban practices.
Acknowledgments
This study was undertaken as part of the faculty development fellowship at the University of North Carolina Department of Family Medicine and funded by the Bureau of Health Professions grant no. HRSA#1-D14-HP00019. We thank the Indiana Academy of Family Physicians, St. Francis Family Practice Residency, Indiana University Department of Family Medicine, Bowen Research Center, UNC Faculty Development Fellowship 2000–2001 fellows, Nancy Loomis, and Jenny Kirby for their support.
OBJECTIVE: The chasm theory of marketing states that fundamental differences exist between early adopters of technology and the mainstream marketplace, making it difficult for technology to transition to the mainstream market. We investigated possible differences in attitudes and beliefs about electronic medical records (EMRs) between current EMR users (early market) and nonusers (mainstream market).
STUDY DESIGN: Cross-sectional mail survey.
POPULATION: Active members in the Indiana Academy of Family Physicians 2000–2001 membership database (N = 1328).
OUTCOMES MEASURED: Differences in attitudes, beliefs, and demographic characteristics of EMR users and nonusers.
RESULTS: The overall return rate was 51.7%; 14.4% of respondents currently use an EMR. Electronic medical record users were more likely to practice in urban areas or to be hospital-based and reported seeing fewer patients. Nonusers were less likely to believe that (1) physicians should computerize their medical records; (2) current EMRs are a useful tool for physicians; (3) EMRs improve quality of medical records and decrease errors; and (4) it is easy to enter data into current EMRs. Nonusers were more likely to believe that paper records are more secure and more confidential than EMRs. Both users and nonusers believed that current EMRs are too expensive.
CONCLUSIONS: A chasm exists between EMR users and nonusers regarding issues that affect EMR implementation, including necessity, usefulness, data entry, cost, security and confidentiality. To reach full implementation of EMRs in family medicine, organizations should use these data to target their research, education, and marketing efforts.
- Physicians have major concerns about data entry, cost, security, and confidentiality of current electronic medical records (EMRs), resulting in their questioning the need for EMRs and the usefulness of existing EMRS.
- There are large differences in the perceptions of physicians who do and do not use EMRs.
- Before EMRs will be accepted by a majority of family physicians, EMR companies must balance cost against the needs of mainstream family physicians.
—Clement J. McDonald, MD1
The benefits of using electronic medical records (EMRs) instead of paper records have been well documented.1-6 However, the current use (5% to 10%) falls very short of the 100% by the year 2000 recommended by a 1991 Institute of Medicine (IOM) report7; furthermore, the rate of EMR use has remained relatively unchanged (5% to 10%) over the past decade. Given this stagnant rate of growth despite the IOM’s support, it is important to analyze the needs and perceptions of physicians with regard to EMRs.
There are few articles on the use of EMRs in out-patient settings.1-20 Only 2 studies have analyzed the perceived needs and preferences for use of EMRs and family physicians.11,12 The first study found significant concerns about the ease of data entry, data confidentiality, data sharing, and initial EMR train-ing.11 The other article rated user requirements in rank order, but was limited by a 24% response rate.12 Most of the literature and information on the Internet about EMRs focuses on the needs and perceptions of current EMR users.1-20
The chasm theory of marketing (Figure) states that the early market of new product adopters (the first 5% to 10%) often has different concerns than the mainstream market. This group leaps ahead of the mainstream, creating a chasm.21 Early market adopters are more willing to endure technical difficulties and poor service to make a product work if it promises a competitive advantage, while mainstream users are more likely to look for widely used products that are inexpensive and easily assimilated into their current work environment with little organizational discomfort.21 Products engineered for the needs of the early market are often too complex to meet the needs of mainstream users; therefore, many products are unable to cross the chasm from early markets to mainstream markets because they fail to meet the needs of the mainstream users.21
This theory may explain the slow adoption of EMRs by family physicians. The purpose of this study was to investigate differences in attitudes and beliefs about EMRs between current EMR users (early market) and nonusers (mainstream market).
FIGURE 1
Chasm theory
Methods
The study population comprised active members of the Indiana Academy of Family Physicians (IAFP) listed in the 2000–2001 IAFP Membership Database. IAFP members who were practicing outside of Indiana or who spent less than 4 hours per week seeing patients were excluded from the study, leaving a study population of 1398 participants.
The authors designed a 53-item questionnaire based on the principles outlined in the 1991 Institute of Medicine report.7,18,19 Six physicians with expertise in medical informatics screened the questionnaire for content validity. Twelve academic family physicians reviewed the instrument for structure, clarity, and relevance to test face validity. Ten resident physicians generated a test–retest reliability rate of >80% for each item over a 2-week interval.
The questionnaire consisted of 3 parts. The first section included questions about physician demographics, use of computer aided technology, practice location and type, and volume of patients. The second section contained questions about respondents’ attitudes, beliefs, and concerns regarding current and emerging technologic issues related to EMRs using a 4-point Likert scale ranging from “strongly agree” to “strongly disagree.” The Likert Scale also contained a “Don’t Know” option. The third section included multiple-choice questions to evaluate specific computer technology needs and preferences of family physicians. The final item was an open-ended question inviting a written response about any issues the respondent felt were not adequately addressed by the questionnaire.
Questionnaires were mailed in January 2001, with a followup mailing to nonrespondents 3 weeks later.22 Of the 726 (51.7%) responses, 45 (6.2%) were excluded because they did not indicate user or nonuser EMR status and 63 (8.8%) were excluded because half or more of the questions were unanswered. There were 618 (44.2%) usable surveys. The questionnaires were scanned into an electronic database and verified for accuracy using TELEform® software; the data were analyzed using SPSS® (Version 10.0). The Likert scales were collapsed to a dichotomous variable, “agree” (strongly agree and agree) and “disagree” (strongly disagree, disagree, and unsure) for this analysis. Differences in demographic characteristics and attitudes, beliefs, and concerns were tested for significance using chi-square tests and the z-test of proportions. Statistical significance was determined by P < .05.
Results
Demographic and practice characteristics of the respondents are presented in Table 1. Of the 618 respondents, 89 (14.4%) were EMR users. A comparison of the users and nonusers revealed that there were no statistically significant differences in age or sex. EMR nonusers were more likely to practice in a suburban or rural location and were more often in a solo or small practice (2–6 physicians). Nonusers also tended to see an average of 31 more patients per week (116 vs 85).
Table 2 presents responses to questions about respondents’ experience with computer technology. A significantly greater proportion of EMR users use the Internet at home (98.9% vs 89.3%), at work (88.6% vs 62.8%), e-mail at work (78.4% vs 48.2%), and personal digital assistants (PDAs) (49.4% vs 26.1%). Other differences in technology use were not statistically significant.
Responses to questions about perceived EMR need and usefulness are summarized in Table 3. Nonusers were significantly less likely than users to believe that (1) physicians should computerize their medical records (67.7% vs 92.1%); (2) current EMRs are useful (51.5% vs 92.0%); (3) EMRs will reduce their risk of making medical errors (56.6% vs 78.7%); and (4) EMRs will improve health care quality in their office (52.4% vs 80.9%) or in the United States overall (54.3% vs 78.4%). Most respondents (77.6%) expressed an interest in an EMR system that would connect all physician practices, laboratories, radiography facilities, and hospitals for the secure exchange of patient data (85.4% user vs 76.2% nonuser; P = .076).
Table 4 summarizes the attitudes and beliefs of respondents about previously reported potential obstacles to EMR use, including: (1) data input; (2) cost; and (3) confidentiality and security.1,11,12,14,17-20,23,24 Few respondents (55.1% users vs 13.4% nonusers) stated that it is easy to enter data into current EMRs. Many respondents in both groups (61.8% vs 68.0%) responded that EMRs are too costly. Users tend to consider a relatively higher price as affordable for setting up an EMR system (66% would pay more than $5000) and are willing to pay a slightly higher monthly fee for the ongoing use of an EMR (65% would pay more than $100 per month). Users consider EMRs as more secure (54.5% users vs 21.2% nonusers) and more confidential (62.5% users vs 21.9% nonusers) than paper records. Few respondents stated they would object to sharing their EMR data with other physicians (24.9% nonusers vs 13.6% users).
TABLE 1
Demographic characteristics of respondents
| Characteristic | User n (%) | Nonuser n (%) | P |
|---|---|---|---|
| Female | 23 (26.1) | 131 (25.0) | .925 |
| Mean age (y) | 44.1 (8.84 SD) | 44.6 (9.29 SD) | .059 |
| Mean number of outpatient visits per week | 85.1 (51.4 SD) | 116.1 (55.2 SD) | <.001 |
| County type | |||
| Rural | 26 (29.5) | 194 (37.2) | .013 |
| Suburban | 28 (31.8) | 204 (39.1) | |
| Urban | 34 (38.6) | 124 (23.8) | |
| Practice setting | |||
| Solo | 12 (13.6) | 101 (19.3) | .003 |
| Small FP (2–6) | 21 (23.9) | 191 (36.5) | |
| Large FP (>6) | 8 (9.1) | 55 (10.5) | |
| Multispecialty group | 9 (10.2) | 54 (10.3) | |
| Hospital employee | 25 (28.4) | 91 (17.4) | |
| Other | 13 (14.8) | 31 (5.9) | |
| 89 users and 529 nonusers responded. | |||
| The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
| FP, family practice; SD, standard deviation. | |||
TABLE 2
Technology use by respondents
| User n (%) | Nonuser n (%) | P | |
|---|---|---|---|
| Computer use at home | |||
| Computer | 89/89 (100.0) | 507/527 (96.2) | .122 |
| Internet | 88/89 (98.9) | 467/523 (89.3) | .007 |
| 83/89 (93.3) | 451/521 (86.6) | .111 | |
| Computer use at work | |||
| Computer | 86/87 (98.9) | 467/506 (92.3) | .043 |
| Internet | 78/88 (88.6) | 318/506 (62.8) | <.001 |
| 69/88 (78.4) | 242/502 (48.2) | <.001 | |
| Computerized scheduling | 83/89 (93.3) | 420/526 (79.8) | .004 |
| Computerized billing | 79/84 (94.0) | 458/489 (93.7) | .999 |
| Handheld computer user | 44/89 (49.4) | 137/525 (26.1) | <.001 |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
TABLE 3
Attitudes and beliefs regarding electronic medical records
| Number (%) agreeing with statement | P | ||
|---|---|---|---|
| User | Nonuser | ||
| Physicians should computerize their medical records | 82/89 (92.1) | 354/523 (67.7) | <.001 |
| Currently available EMRs are a useful tool for physicians (92.0) (51.5) | 81/88 | 269/522 | <.001 |
| EMRs will improve the quality of care in physicians’ offices | 72/89 (80.9) | 274/523 (52.4) | <.001 |
| Widespread use of EMRs would improve healthcare quality in the United States | 69/88 (78.4) | 283/521 (54.3) | <.001 |
| EMRs will reduce my risk of making medical errors | 70/89 (78.7) | 297/525 (56.6) | <.001 |
| I am interested in an EMR that would connect all physician practices, labs, x-ray facilities, and hospitals in my area securely for the exchange of patient data | 76/89 (85.4) | 398/522 (76.2) | .076 |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. | |||
| EMR, electronic medical records. | |||
TABLE 4
Possible barriers to electronic medical record use
| Number (%) agreeing with statement | P | ||
|---|---|---|---|
| User | Nonuser | ||
| Security and confidentiality | |||
| EMRs are more secure | 48/88 (54.5) | 111/523 (21.2) | <.001 |
| EMRs are more confidential | 55/88 (62.5) | 115/524 (21.9) | <.001 |
| Object to sharing EMR data with other physicians | 11/81 (13.6) | 121/486 (24.9) | .037 |
| Usefulness | |||
| Easy to enter data | 49/89 (55.1) | 70/521 (13.4) | <.001 |
| Ability to use an EMR with minimal training | 79/87 (90.8) | 479/522 (91.8) | .929 |
| Would like direct link to Medline | 73/88 (83.0) | 298/522 (57.1) | <.001 |
| Would like direct links to updated treatment guidelines | 73/87 (83.9) | 360/521 (69.1) | .007 |
| Would like direct link to patient education materials | 83/88 (94.3) | 421/520 (81.0) | .003 |
| EMR data should be available without patient or physician identifiers for use in clinical and health care services research | 46/89 (51.7) | 263/521 (50.5) | .924 |
| Costs | |||
| Current EMRs are too costly | 55/89 (61.8) | 355/522 (68.0) | <.001 |
| Affordable price per physician to set up an EMR system | |||
| <$1000 | 5/77 (6.5) | 65/464 (14.0) | <.001 |
| $1000–$4999 | 21/77 (27.3) | 202/464 (43.5) | |
| $5000–$9999 | 27/77 (35.1) | 147/464 (31.7) | |
| $10,000–$19,999 | 17/77 (22.1) | 42/464 (9.1) | |
| >$20,000 | 7/77 (9.1) | 8/464 (1.7) | |
| Willing to spend monthly for ongoing use of an EMR | |||
| <$50 | 3 (3.9) | 89 (19.7) | .013 |
| $50–$99 | 23 (30.3) | 101 (22.4) | |
| $100–$149 | 25 (32.9) | 139 (30.8) | |
| $150–$199 | 14 (18.4) | 79 (17.5) | |
| >$200 | 11 (14.5) | 43 (9.5) | |
| 89 users and 529 nonusers responded. The number of users or nonusers for a given variable may be less than the total due to missing responses. EMR, electronic medical records. | |||
Discussion
Despite the low penetration of EMRs (14.4%), family physicians in Indiana are interested in using EMRs. Most users (85.4%) and nonusers (76.2%) expressed interest in a system that would securely connect all physician practices, laboratories, radiography facilities, and hospitals in their area for exchanging patient data. Many family physicians are currently using the Internet (67%), e-mail (53%), computers (93%), and PDAs (30%) in their practice.
Despite this expressed interest, only two thirds of nonusers believe that physicians should computerize their medical records. This may be related to the fact that only half of the responding nonusers perceive that current EMRs are useful for physicians. There was also a considerable lack of belief that EMRs will improve quality or reduce medical errors. Replies to the open-ended question indicated that 5% to 10% of respondents, for a variety of reasons, have strong feelings about computerizing their offices. A targeted, educational effort to show the advantages of EMRs may be useful for improving physician perceptions of EMRs.
The demographic profile of the nonusers may indicate that current EMRs are not perceived as being well adapted for use in rural, solo, or small-group practice. EMRs may be thought of as more feasible for larger organizations with larger capital budgets and robust information technology support systems. The differences in the volume of patients treated between users and nonusers suggest that productivity concerns may also be important.
Both EMR users and nonusers believe current EMRs are too costly. The data suggests that family physicians are willing to pay a relatively low set-up charge <$5000 would be accepted by more than 87% of respondents) and a very low monthly fee (<$100 would be accepted by more than 81% of respondents) for the use of an EMR. Few current EMRs can be installed and operated within these price specifications. This supports the previously published view that physicians believe current EMRs are not cost effective.17 Lower prices or greater perceived value is needed for physicians to consider EMRs a wise business choice.
Data entry is a concern for both users and nonusers. Practicing family medicine requires varied skills, a fast pace, treating patients from multiple age groups, diagnosing conditions from a myriad of potentially unrelated complaints, and keeping a comprehensive record from multiple sources. These factors make data entry the largest potential obstacle to the effective use of computers in family medi-cine.1,14,18-20 Our data indicate that only 55% of users and 13.4% of nonusers believe data entry is easy for current EMRs. Perceived and actual ease of data entry must be improved before widespread adoption of EMRs by family physicians can be realized.
Concerns about security and confidentiality generated the largest number of written comments. Despite evidence to the contrary,9,23,24,28,29 nonusers believe that there are more security and confidentiality risks involved with EMRs than paper records. A small group emphatically expressed dismay at the possibility of subjecting their office to a “Big Brother”-type system. The Health Insurance Portability and Accountability Act (HIPAA) sets the standards for medical record (electronic and written) confidentiality and security, and the creation of an EMR that is HIPAA compliant may give providers greater confidence in its security and confidentiality.23,24 Educating physicians about the security and confidentiality risks of paper records and the safeguards built into EMR programs may help alleviate these concerns.
It is encouraging that both users and nonusers seem to understand the potential usefulness of EMRs. Over half of the nonusers believe an EMR is a useful way to provide patient education materials, participate in clinical and health services research, launch a literature search (eg, Medline), or obtain up-to-date treatment guidelines. To increase the number of physicians using EMRs, vendors should maximize and promote the use of EMR features.
The results of this study are limited by the response rate. Although this rate introduces the possibility of a nonresponse bias, it is comparable to or exceeds the response rate in other physician EMR surveys.11,12,23-27 Evidence of nonresponse bias includes the high rate of EMR use by Indiana family physicians (14.4%) compared to previous studies, suggesting users were more likely to respond than nonusers. Questionnaires that were returned early in the survey showed an EMR use rate of 40%, but this number dropped quickly after the first 2 weeks. A very small percentage of questionnaires returned near the end of the study were from EMR users. The nonresponse bias of the study is likely toward EMR users and nonusers who have seriously considered using EMRs; since this is the segment of the physician market most likely to adopt EMRs, the sample is likely adequate for the attempted analysis. The study is also limited by its focus on family physicians in Indiana, and may differ from the views of physicians in other specialties or states.
Conclusions
Our data demonstrate the existence of a chasm between EMR users (early adopters) and nonusers (mainstream market) regarding attitudes and perceptions that impact the implementation of EMRs by family physicians. Specifically, EMR nonusers exhibit the following important differences from users: (1) less perceived need for EMRs; (2) greater concerns about EMR data entry; (3) less confidence in the security and confidentiality of EMRs; and (4) more concerns about the cost for installation and ongoing use of EMRs.
Further studies are needed to examine nonusers in more detail and to discover if current EMRs can meet the needs of the mainstream physician user. Our research suggests that data entry, cost, security and confidentiality, and connectivity issues are important starting points. A qualitative study of nonusers is desirable to better understand the true needs of the mainstream physician. Broadening this study to include all specialties throughout the country would also be useful.
The IOM has repeatedly called for the computerization of the US medical system.7,28,29 Government, industry, and physician organizations should use the results of this study to target their research, education, and marketing efforts regarding EMRs, and to develop EMRs that meet the needs of most practicing family physicians, especially family physicians in small group, high-volume, rural or suburban practices.
Acknowledgments
This study was undertaken as part of the faculty development fellowship at the University of North Carolina Department of Family Medicine and funded by the Bureau of Health Professions grant no. HRSA#1-D14-HP00019. We thank the Indiana Academy of Family Physicians, St. Francis Family Practice Residency, Indiana University Department of Family Medicine, Bowen Research Center, UNC Faculty Development Fellowship 2000–2001 fellows, Nancy Loomis, and Jenny Kirby for their support.
1. McDonald CJ. The barriers to electronic medical record systems and how to overcome them. J Am Med Inform Assoc 1997;4:213-21.
2. Wager KA, SM Ornstein, Jenkins RG. Perceived value of computer-based patient records among clinician users. MD Comput 1997;14:334-6,338-340.
3. Wager KA, Lee FW, White AW, Ward DM, Ornstein SM. Impact of an electronic medical record system on community-based primary care practices. J Am Board Fam Pract 2000;13:338-48.
4. Spann SJ. Should the complete medical record be computerized in family practice? An affirmative view. J Fam Pract 1990;30:457-60.
5. Ornstein SM. Electronic medical records in family practice: the time is now. J Fam Pract 1997;44:45-8.
6. Rodnick JE. Should the complete medical record be computerized in family practice? An opposing view. J Fam Pract 1990;30:460-4.
7. Dick RS. The Institute of Medicine’s patient record study and its implications for record administrators. Top Health Rec Manage 1991;11:67-72.
8. Swanson T, Dostal J, Eichhorst B, Jernigan C, Knox M, Roper K. Recent implementations of electronic medical records in four family practice residency programs. Acad Med 1997;72:607-12.
9. Woodward B. The computer-based patient record and confidentiality. N Engl J Med 1995;333:1419-22.
10. Wager KA, Heda S, Austin CJ. Developing a health information network within an integrated delivery system: a case study. Top Health Inf Manage 1997;17:20-31.
11. Strasberg HR, Tudiver F, Holbrook AM, Geiger G, Keshavjee KK, Troyan S. Moving towards an electronic patient record: a survey to assess the needs of community family physicians. Proc AMIA Symp 1998;230-4.
12. Smith WR, Zastrow R. User requirements for the computerized patient record: physician opinions. Proc Annu Symp Comput Appl Med Care 1994;994.-
13. Powsner SM, Wyatt JC, Wright P. Opportunities for and challenges of computerisation. Lancet 1998;352:1617-22.
14. Musham C, Orstein SM, Jenkins RG. Family practice educators’ perceptions of computer-based patient records. Fam Med 1995;27:571-5.
15. Arias-Vimarlund V, Ljunggren M, Timpka T. Implementation of computer-based patient records in primary care: the societal health economic effects. Proc AMIA Annu Fall Symp 1996;503-7.
16. Lawler F, Cacy JR, Viviani N, Hamm RM, Cobb SW. Implementation and termination of a computerized medical information system. J Fam Pract 1996;42:233-6.
17. Lindberg DA, Humpreys BL. Medical informatics. JAMA 1996;275:1821-2.
18. Levitt JI. Why physicians continue to reject the computerized medical record. Minn Med 1994;7(8):17-21.
19. Lenhart JG, Honess K, Covington D, Johnson KE. An analysis of trends, perceptions, and use patterns of electronic medical records among US family practice residency programs. Fam Med 2000;32:109-14.
20. Bernstein RM, Hollingworth GR, Viner G, Lemelin J. Family practice informatics: research issues in computerized medical records. Proc Annu Symp Comput Appl Med Care 1993;93-7.
21. Moore G. Crossing the Chasm: Marketing and Selling High-Tech Products to Mainstream Consumers. Rev ed. New York: Harper Business; 1999.
22. Dillman DA. Mail and Internet Surveys: The Tailored Design Method. 2nd ed. New York: John Wiley & Sons; 1999.
23. Kibbe DC. A problem-oriented approach to the HIPAA security standards. Fam Pract Manag 2001;8(7):37-43.
24. Kibbe DC. What you need to know about HIPAA now. Fam Pract Manag 2001;8(3):43-7.
25. Bomba D. A comparative study of computerised medical records usage among general practitioners in Australia and Sweden. Medinfo 1998;(Pt 1):55-9.
26. Ebell MH, Gaspar DL, Khurana S. Family physicians’ p for computerized decision-support hardware and software. J Fam Pract 1997;45:137-41.
27. Kalsman MW, Acosta DA. Use of the Internet as a medical resource by rural physicians. J Am Board Fam Pract 2000;13:349-52.
28. Committee on Quality Healthcare in America, eds. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
29. Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.
1. McDonald CJ. The barriers to electronic medical record systems and how to overcome them. J Am Med Inform Assoc 1997;4:213-21.
2. Wager KA, SM Ornstein, Jenkins RG. Perceived value of computer-based patient records among clinician users. MD Comput 1997;14:334-6,338-340.
3. Wager KA, Lee FW, White AW, Ward DM, Ornstein SM. Impact of an electronic medical record system on community-based primary care practices. J Am Board Fam Pract 2000;13:338-48.
4. Spann SJ. Should the complete medical record be computerized in family practice? An affirmative view. J Fam Pract 1990;30:457-60.
5. Ornstein SM. Electronic medical records in family practice: the time is now. J Fam Pract 1997;44:45-8.
6. Rodnick JE. Should the complete medical record be computerized in family practice? An opposing view. J Fam Pract 1990;30:460-4.
7. Dick RS. The Institute of Medicine’s patient record study and its implications for record administrators. Top Health Rec Manage 1991;11:67-72.
8. Swanson T, Dostal J, Eichhorst B, Jernigan C, Knox M, Roper K. Recent implementations of electronic medical records in four family practice residency programs. Acad Med 1997;72:607-12.
9. Woodward B. The computer-based patient record and confidentiality. N Engl J Med 1995;333:1419-22.
10. Wager KA, Heda S, Austin CJ. Developing a health information network within an integrated delivery system: a case study. Top Health Inf Manage 1997;17:20-31.
11. Strasberg HR, Tudiver F, Holbrook AM, Geiger G, Keshavjee KK, Troyan S. Moving towards an electronic patient record: a survey to assess the needs of community family physicians. Proc AMIA Symp 1998;230-4.
12. Smith WR, Zastrow R. User requirements for the computerized patient record: physician opinions. Proc Annu Symp Comput Appl Med Care 1994;994.-
13. Powsner SM, Wyatt JC, Wright P. Opportunities for and challenges of computerisation. Lancet 1998;352:1617-22.
14. Musham C, Orstein SM, Jenkins RG. Family practice educators’ perceptions of computer-based patient records. Fam Med 1995;27:571-5.
15. Arias-Vimarlund V, Ljunggren M, Timpka T. Implementation of computer-based patient records in primary care: the societal health economic effects. Proc AMIA Annu Fall Symp 1996;503-7.
16. Lawler F, Cacy JR, Viviani N, Hamm RM, Cobb SW. Implementation and termination of a computerized medical information system. J Fam Pract 1996;42:233-6.
17. Lindberg DA, Humpreys BL. Medical informatics. JAMA 1996;275:1821-2.
18. Levitt JI. Why physicians continue to reject the computerized medical record. Minn Med 1994;7(8):17-21.
19. Lenhart JG, Honess K, Covington D, Johnson KE. An analysis of trends, perceptions, and use patterns of electronic medical records among US family practice residency programs. Fam Med 2000;32:109-14.
20. Bernstein RM, Hollingworth GR, Viner G, Lemelin J. Family practice informatics: research issues in computerized medical records. Proc Annu Symp Comput Appl Med Care 1993;93-7.
21. Moore G. Crossing the Chasm: Marketing and Selling High-Tech Products to Mainstream Consumers. Rev ed. New York: Harper Business; 1999.
22. Dillman DA. Mail and Internet Surveys: The Tailored Design Method. 2nd ed. New York: John Wiley & Sons; 1999.
23. Kibbe DC. A problem-oriented approach to the HIPAA security standards. Fam Pract Manag 2001;8(7):37-43.
24. Kibbe DC. What you need to know about HIPAA now. Fam Pract Manag 2001;8(3):43-7.
25. Bomba D. A comparative study of computerised medical records usage among general practitioners in Australia and Sweden. Medinfo 1998;(Pt 1):55-9.
26. Ebell MH, Gaspar DL, Khurana S. Family physicians’ p for computerized decision-support hardware and software. J Fam Pract 1997;45:137-41.
27. Kalsman MW, Acosta DA. Use of the Internet as a medical resource by rural physicians. J Am Board Fam Pract 2000;13:349-52.
28. Committee on Quality Healthcare in America, eds. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
29. Kohn L, Corrigan J, Donaldson M, eds. To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; 2000.