User login
Also known as “domestic violence” and “spouse abuse,” intimate partner violence (IPV) is now the term defined by the US Centers for Disease Control and Prevention to include physical violence, sexual violence, threats of physical or sexual violence, and psychological or emotional abuse by a current or former spouse, common-law spouse, nonmarital dating partner, or boyfriend or girlfriend of the same or opposite sex.1 Although IPV is often hidden or kept secret by those affected, it is a highly prevalent issue, especially in women. Knowing how to broach the subject and provide appropriate support in a caring and nonjudgmental manner are the keys to helping a woman move forward in her readiness and ability to improve her situation.
See related patient information
ONE IN THREE WOMEN EXPERIENCES IPV IN HER LIFE
As clinicians, we have all seen patients who have been affected by IPV—even if we did not realize it at the time. Indeed, 36% of women in the United States (approximately 42.4 million) have experienced rape, physical violence, or stalking by an intimate partner in their lifetime, and 6% (approximately 7 million) have experienced these forms of IPV within the past 12 months.2
ASSOCIATION WITH MURDER
From 30% to 70% of women who are murdered are killed by a current or former intimate partner.3,4 Of those killed by their partner, two-thirds had previously reported physical assault, and 83% had been threatened by the man who eventually killed them.4 In another study, 44% of IPV murder victims had presented to an emergency department within 2 years of their murder.5
PHYSICAL EFFECTS NOT ALWAYS APPARENT
Although 41% of women who experience IPV suffer physical injury from their attacks, only 28% of those who are injured seek medical care.6 Because injuries are often absent or no longer apparent when an IPV victim decides to get help, it is important to be aware of the clinical signs associated with IPV:
- Gastrointestinal disorders7
- Depression8
- Anxiety
- Chronic pain syndromes9
- Substance abuse
- Suicidal ideation.10
In women of childbearing age, IPV is associated with unintended pregnancy, sexually transmitted infections, condom non-use,11,12 inconsistent condom use,13 and fear of talking about condom use.11,12 Coerced sexual experiences (eg, sexual intercourse that was not wanted or consented to) are common, with 28% to 42% of college women reporting at least one such experience. In more than three quarters of women who have been sexually assaulted, the first experience occurred before age 25.14,15
One-quarter of women ages 16 to 29 have experienced reproductive coercion, which includes birth control sabotage or pregnancy coercion by the active male partner.16 Among women reporting birth control sabotage, 79% had also been victims of physical or sexual IPV.16
The cost of providing health care to women experiencing IPV is 1.4 to 2.5 times higher than that of the nonabused population. Studies have shown that female victims of both physical and nonphysical (eg, emotional or verbal) IPV are more likely to use emergency, mental health, and outpatient health care services. The economic toll of IPV, including health care and costs from lost productivity and premature death, ranges from $2.3 to $8.3 billion per year.17,18
ASK FEMALE PATIENTS ABOUT IPV
In the early 1990s, various medical organizations began issuing policy statements that endorsed screening for IPV.19–22 Since 1992, the Joint Commission on Accreditation of Healthcare Organizations has required hospitals and clinics to provide assistance to those experiencing IPV.23 Although the United States Preventive Services Task Force initially found insufficient evidence to support regular IPV screening in health care settings,24–27 the group reversed its position in 2012 after a review of more recent studies. The group now recommends that clinicians address IPV with all women of childbearing age.28
A Cochrane review found that IPV screening increased identification of IPV survivors.29 Female participants in many studies wanted clinicians to ask routinely about violence and to provide information on community and legal resources.30,31
How should we ask about IPV?
Although various sets of screening questions and tools are available, no one instrument is considered better than the others. However, women experiencing IPV have specific preferences regarding how they want clinicians to ask and talk about the topic. In one survey, women who had experienced IPV preferred that clinicians ask about it as part of the complete medical history, as long as it did not create “an atmosphere of interrogation.”32
The style in which a clinician asks about IPV may make a difference as well. In focus groups, immigrant Latina and Asian women who had experienced IPV stated that clinicians could facilitate open communication by initiating the discussion and exhibiting compassionate and supportive behavior during the visit.33 Being able to see the same clinician at each visit also enhanced clinician-patient communication.33
In a study of IPV screening in emergency room settings, most clinicians asked about IPV in a perfunctory, direct manner—generally some variant of, “Are you a victim of domestic violence?” In this study, patient IPV disclosure occurred more often when clinicians used an open-ended approach such as, “Tell me what happened,” or when clinicians probed for possible IPV (eg, “What do you think may be causing some of this stress?”).34
In a focus group, female IPV survivors described feeling stigmatized or invalidated when clinicians were condescending, judgmental, or dismissive.35 Nonjudgmental and supportive communication decreased the women’s sense of isolation and led to positive outcomes such as increased awareness of IPV as a problem, decreased isolation, and feeling that the clinician cared.35
When addressing IPV, clinicians should explain why they are asking about it because it allows the woman to understand the context of the inquiry and to feel more comfortable about disclosing IPV. If the query is a regular part of a general screening or history-taking, for example, they should frame the question to make that point apparent. For example, “Because we know that many women in the United States experience physical, sexual or emotional violence from their romantic partners, I like to ask all of my patients whether they have been hurt or have felt threatened or afraid in a current or past relationship.”
In situations in which clinicians are concerned about IPV with a particular patient, they should explicitly share their concerns and desire to help the patient. One IPV survivor offered this advice: “Just look at the patient like she is your friend. Call her by her name. For instance, say ‘Sally, is he hurting you? Are you having problems? If you need help, I have some [phone] numbers.’ Personalize the encounter.”
It is also important to address IPV in a manner that ensures the patient’s safety, confidentiality, and dignity. When having this type of sensitive conversation, the patient should ideally be clothed and alone—without others present, particularly her partner. Professional interpreters should be available to women who do not speak English. The clinician should maintain eye contact, smile to communicate friendliness, and use a supportive tone.36
Just asking may be an intervention
Qualitative studies have suggested that just the act of asking about IPV in a nonjudgmental and compassionate manner is helpful to women experiencing IPV.35,37 Doing so not only helps women recognize the abuse, but also begins to decrease their sense of isolation and increase their awareness of helpful resources. It also gives the patient a sense that the clinician cares about her situation.35 As a result, experts have begun to recommend that health clinicians view asking about IPV not merely as a screening tool, but as a potentially therapeutic intervention in and of itself.35,37,38
HOW TO HELP
What to do when a woman discloses IPV
Female survivors, advocates, and health care clinicians who care for abused women suggest responding to a positive disclosure of IPV by providing the following:
Validation. The IPV perpetrator will often attempt to justify the violence and abuse by shifting some of the blame or responsibility for the violence onto the victim. This “brainwashing” leads to self-blame and a diminished sense of self-worth. However, clinicians can help reverse this mindset by acknowledging the woman’s disclosure and emphasizing that she did not deserve the abuse or violence. An example of such a statement is, “I am so very sorry that you went through that with your partner. You definitely did not deserve that. No one should ever be hurt by or afraid of the people who are supposed to love them.” Providing validation helps women recognize that the violence was a problem they did not deserve.38,39
Support. Women who have experienced IPV appreciate feeling supported and cared for by their health care clinician. Even if the patient is not ready to take any definitive action regarding her relationship or situation, knowing that her clinician and the health care setting are resources and sources of support is both comforting and empowering.35,40 Clinicians can communicate this support by stating, “I want you to know that whatever happens and whatever you decide, we are here for you.”
Respect for autonomy. Women experiencing IPV best understand their own situation and its various complexities and so they know best what they can do, cannot do, or need to do. As such, clinicians must respect a woman’s autonomy and preserve her ability to express her own needs and desires and make her own decisions. Prescribing a plan of action or giving commands to IPV victims could further perpetuate their sense of disempowerment and lack of control over their life.
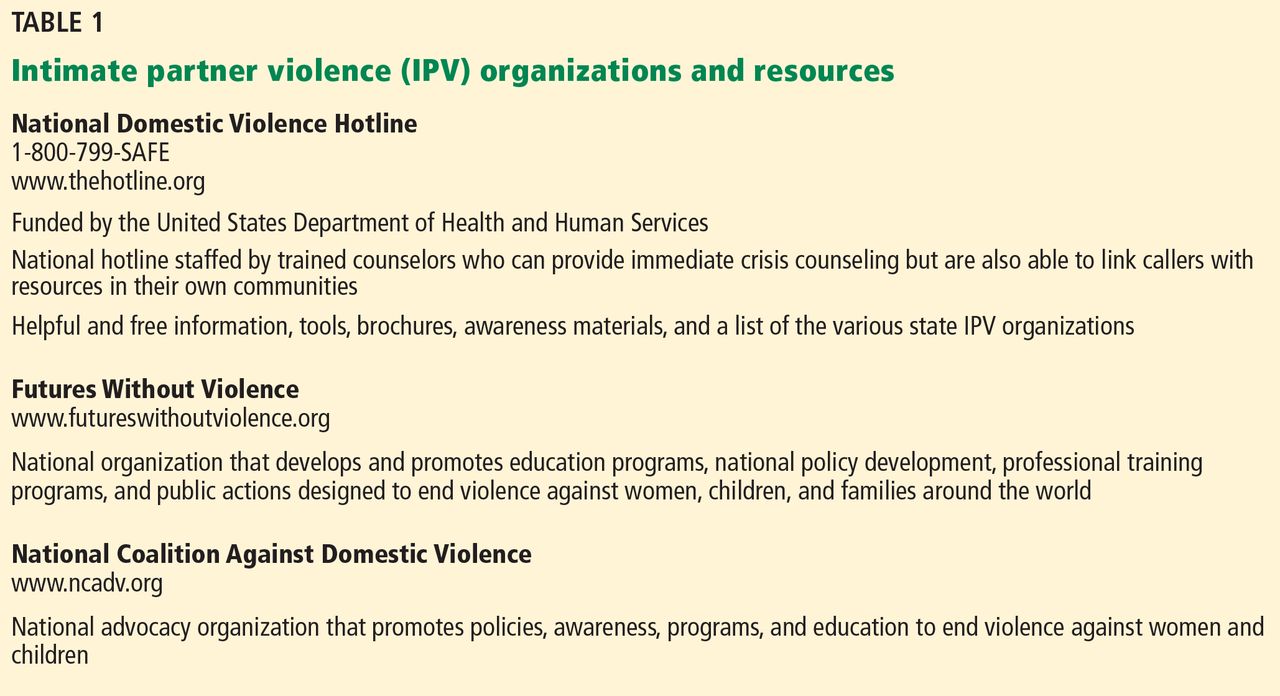
Information. Providing referral information or hotline numbers to community domestic violence programs is helpful. However, not all women feel safe or comfortable taking printed brochures or written information with them because their abusive partner may find it. Thus, clinicians should ask if the patient can take the information safely or offer to write the numbers down without labeling them if she is afraid. The National Domestic Violence hotline is a 24-hour toll-free resource that will help women locate and contact shelters and other support services in their own community. The number, 1-800-799-SAFE (7233), is easy to memorize and thus is an easy resource to pass along quickly and safely. Other national organizations such as Futures Without Violence (formerly known as the Family Violence Prevention Fund) and the National Coalition Against Violence also provide links to local resources (Table 1).
Safety planning. Discussing the need for a safety plan will help the patient prepare for future abusive episodes. Even women who report that they are no longer in an abusive relationship should be asked about their current safety needs and concerns because they often remain in contact with abusive partners even after a relationship has ended.
When discussing safety planning, clinicians should ask the woman if she is currently safe or if she needs shelter. If she intends to return to or is still in contact with her batterer, ask if she has a plan for what to do or how to escape if the violence occurs again. Advise the patient to:
- Hide money so that she can leave quickly
- Make copies of birth certificates, immunization records, Social Security Number, and other important documents and keep them hidden and accessible
- Make a spare car key
- Have a list of hotline numbers
- Develop a code with friends, family, and neighbors that will let them know she needs immediate help.
Studies show that discussing safety-promoting behaviors increases the number of them that are used by IPV victims.41 A detailed list that can be shared with patients is provided in the patient information page that accompanies this article.42 Examples of personalized safety plans are available from the National Center on Domestic and Sexual Violence at its website, www.ncdsv.org/images/NCDSV_DVSafetyPlan_updated2013.pdf.
Danger assessment. Several researchers have examined potential risk factors associated with increased risk of homicide.43 Table 2 lists some of the characteristics associated with an increased risk of homicide in IPV situations.42 From this work, a danger assessment tool and scoring system has been developed. This tool and training on how to use it are available for free at www.dangerassessment.org. Although there are currently no outcome data on the benefits or risks of using this instrument, its objective is to increase women’s awareness of their danger level and individualize their safety counseling.
Proper documentation. Victim advocates and lawyers working on behalf of IPV victims emphasize that documentation by a medical provider can help a woman with her legal case. This documentation should be clear, legible, and as detailed as possible. These details should include a patient’s own words set off by quotation marks, a description or body map illustrating associated injuries or physical signs corroborating the violence, and a description of the patient’s demeanor or signs of emotion. Clinicians should avoid legal terms such as “alleges” or “alleged perpetrator” and should either define or avoid abbreviations that may be considered ambiguous in a legal proceeding (eg, clinicians should write out the words “domestic violence” or “intimate partner violence” rather than using “DV” or “IPV”).44 Most states have passed laws that prevent insurance companies from discriminating against IPV victims; insurance companies can no longer deny women coverage for seeking care related to IPV.45
A nonthreatening physical examination. Women who have experienced physical or sexual violence may feel anxious or experience added trauma during certain portions of the physical examination. Women who have been raped or otherwise sexually abused may have difficulty tolerating a pelvic examination, for example. Others who have been choked or grabbed by the neck may experience distress during palpation of the thyroid or cervical lymph nodes. The oropharyngeal examination may be challenging for women who have experienced forced oral sex or who may have had objects such as the barrel of a gun forced into their mouth. Asking women who have experienced IPV what aspects of the physical examination they may find difficult and how this could be made easier allows the patient and clinician to work together to develop strategies for or alternatives to necessary examinations or testing.
Before starting an examination, clinicians should explain what will happen and then ask the patient for her permission before moving on to the next step. Doing so creates a sense of control in an otherwise challenging and potentially traumatizing examination.
Disclosure of mandatory IPV reporting. Many states require health care providers to report any injuries caused by a weapon or criminal act to police or other official institutions.45,46 Several of these states specify that this reporting should occur during an IPV evaluation.
Mandatory reporting of IPV to police is highly controversial.47–49 Opponents of these laws argue that they do not benefit victims because they do not respect autonomy, they violate patient-clinician confidentiality, and they violate informed consent.47 Female IPV victims indicate that they would be less likely to disclose IPV and seek help if they knew it had to be reported.50–53 In a survey of California physicians, 59% stated that they might not comply with reporting laws if the patient objected.54
In states with mandatory reporting laws, clinicians can advocate for their patients by disclosing whether IPV must be reported before beginning their examination. The Michigan Coalition Against Domestic Violence devised this sample statement:
“I do have to let you know that under state law, I am obligated to make a police report to (name police agency with jurisdiction over the facility), if I/we are treating someone for any injury sustained by means of violence (tailor this information to the specifics of your state law). So, if you would have any concerns about that, I would encourage you to speak with one of the domestic violence advocates/counselors at (DV agency), who are able to provide confidential services and help without being required to make a police report.”55
The Compendium of State Statutes and Polices on Domestic Violence and Health Care by Futures Without Violence is an excellent reference that describes current state laws and policies regarding domestic violence and includes descriptions of the specific characteristics of each state’s mandatory reporting laws and their implications for health care providers. A copy can be downloaded from www.futureswithout-violence.org/content/features/detail/1584/.
What not to do
Clinicians should not ignore or minimize the extent of IPV, make excuses for the batterer, or blame the woman.32,56,57 They also should not inadvertently blame or criticize the woman by asking her, “What did you do to deserve this?” or “Why don’t you just leave?”57
While leaving a violent relationship is an obvious solution, many women experiencing IPV are either unwilling or unable to do so. In fact, leaving the batterer can be just as dangerous as staying. In a North Carolina study, half of all women killed by their partner had divorced or broken up with the partner immediately before the murder.4
What to do when a woman does not disclose IPV
Women who have experienced IPV often deny the violence to others out of fear. So a denial of violence, even in highly suspicious cases, can be expected. Abused patients often want help but are confused and afraid to ask for it.58,59 Providing easy and anonymous access to IPV information and resources through posters, flyers, brochures, and booklets will allow any woman—regardless of disclosure—to obtain help.36
In one IPV trial, all women in a family planning clinic who were in the intervention group were given information about IPV and how it can affect sexual and reproductive health, whether or not they disclosed. Compared with women in the control group, women who received the intervention—both those who did and did not experience IPV—were 63% more likely than those in the control group to end a relationship because they perceived it to be unhealthy or unsafe. In this case, all women—not just those who were victims—benefited from receiving information about IPV.60
PROVIDERS’ SUPPORT MAKES A DIFFERENCE, IMPROVES OUTCOMES
Patients may seek help for and find safety from IPV in stages or steps, and it may take them several months or even years to do so.61–63 In this sense, then, IPV is an issue that is not likely to be “cured” or changed in a single medical visit. In addition, a single visit may not be associated with direct health and safety outcomes. However, a patient is more likely to make changes if she has supportive and informative interaction with a caring, nonjudgmental clinician who can increase her awareness of IPV and IPV resources and promote an improved sense of self-efficacy or perceived power.40
For example, in a study in which health clinicians expressed concern about potential IPV health effects and offered support services such as counseling, 67% of women used one of those resources at least once.40 In another study, women who talked to a health care provider about their abuse were almost four times more likely to use an IPV intervention (eg, advocacy, shelter, restraining order) than women who did not talk to their provider. Those who used an IPV intervention were 2.6 times more likely to leave their abusive relationship, and those who left reported improved physical health.64
Thus, health care providers can have a positive effect by addressing this complex and difficult issue. The power and influence of a provider’s kindness, empathy, and support cannot be overestimated in their ability to improve the safety and well-being of women dealing with IPV.
- Saltzman LE, Fanslow JL, McMahon PM, Shelley GA; National Center for Injury Prevention and Control; Centers for Disease Control and Prevention. Intimate partner violence surveillance: uniform definitions and recommended data elements, Version 1.0. Atlanta, GA; 1999. www.cdc.gov/ncipc/pub-res/ipv_surveillance/intimate%20partner%20violence.pdf. Accessed June 3, 2014.
- Black MC, Basile KC, Breiding MJ, et al; Center for Injury Prevention and Control; Centers for Disease Control and Prevention. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta, GA. www.cdc.gov/violenceprevention/pdf/nisvs_executive_summary-a.pdf. Accessed June 3, 2014.
- Kellermann AL, Mercy JA. Men, women, and murder: gender-specific differences in rates of fatal violence and victimization. J Trauma 1992; 33:1–5.
- Moracco KE, Runywan CW, Butts JD. Femicide in North Carolina, 1991–1993: a statewide study of patterns and precursors. Homicide Studies 1998; 4:422–446.
- Wadman MC, Muelleman RL. Domestic violence homicides: ED use before victimization. Am J Emerg Med 1999; 17:689–691.
- Catalano SM; United States Bureau of Justice Statistics. Intimate partner violence in the United States: 2007. http://bjs.ojp.usdoj.gov/index.cfm?ty=pbdetail&iid=1000. Accessed February 19, 2014.
- Drossman DA, Talley NJ, Leserman J, Olden KW, Barreiro MA. Sexual and physical abuse and gastrointestinal illness. Review and recommendations. Ann Intern Med 1995; 123:782–794.
- Scholle SH, Rost KM, Golding JM. Physical abuse among depressed women. J Gen Intern Med 1998; 13:607–613.
- Walling MK, O’Hara MW, Reiter RC, Milburn AK, Lilly G, Vincent SD. Abuse history and chronic pain in women: II. A multivariate analysis of abuse and psychological morbidity. Obstet Gynecol 1994; 84:200–206.
- McCauley J, Kern DE, Kolodner K, Derogatis LR, Bass EB. Relation of low-severity violence to women’s health. J Gen Intern Med 1998; 13:687–691.
- Wingood GM, DiClemente RJ. The effects of an abusive primary partner on the condom use and sexual negotiation practices of African-American women. Am J Public Health 1997; 87:1016–1018.
- Sales JM, Salazar LF, Wingood GM, DiClemente RJ, Rose E, Crosby RA. The mediating role of partner communication skills on HIV/STD-associated risk behaviors in young African American females with a history of sexual violence. Arch Pediatr Adolesc Med 2008; 162:432–438.
- Davila YR, Brackley MH. Mexican and Mexican American women in a battered women’s shelter: barriers to condom negotiation for HIV/AIDS prevention. Issues Ment Health Nurs 1999; 20:333–355.
- Tjaden P, Thoennes N; National Institute of Justice; Centers for Disease Control and Prevention. Prevalence, incidence and consequences of violence against women: findings from the national violence against women survey. Washington, DC; 1998. https://www.ncjrs.gov/pdffiles/172837.pdf. Accessed June 3, 2014.
- Masho SW, Odor RK, Adera T. Sexual assault in Virginia: a population-based study. Womens Health Issues 2005; 15:157–166.
- Miller E, Decker MR, McCauley HL, et al. Pregnancy coercion, intimate partner violence and unintended pregnancy. Contraception 2010; 81:316–322.
- Bonomi AE, Anderson ML, Rivara FP, Thompson RS. Health care utilization and costs associated with physical and nonphysical-only intimate partner violence. Health Serv Res 2009; 44:1052–1067.
- Rivara FP, Anderson ML, Fishman P, et al. Healthcare utilization and costs for women with a history of intimate partner violence. Am J Prev Med 2007; 32:89–96.
- American Nurses Association. Position statement on physical violence against women. Washington, DC; 1991.
- Physicians and domestic violence. Ethical considerations. Council on Ethical and Judicial Affairs, American Medical Association. JAMA 1992; 267:3190–3193.
- The American College of Obstetricians and Gynecologists. Screening tools: domestic violence. http://www.acog.org/About_ACOG/ACOG_Departments/Violence_Against_Women/Screening_Tools__Domestic_Violence. Accessed June 3, 2014.
- Lee D, James L, Sawires P; The Family Violence Prevention Fund. Preventing domestic violence: clinical guidelines on routine screening. San Francisco, CA; 1999. http://new.vawnet.org/Assoc_Files_VAWnet/screpol.pdf. Accessed June 3, 2014.
- Joint Commission on Accreditation of Healthcare Organizations. Accreditation manual for hospitals. Chicago, IL; 1992.
- US Department of Health and Human Services. US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd ed. Washington, DC; 1996.
- Ramsay J, Richardson J, Carter YH, Davidson LL, Feder G. Should health professionals screen women for domestic violence? Systematic review. BMJ 2002; 325:314.
- Nelson HD, Nygren P, McInerney Y, Klein J; US Preventive Services Task Force. Screening women and elderly adults for family and intimate partner violence: a review of the evidence for the US Preventive Services Task Force. Ann Intern Med 2004; 140:387–396.
- Chamberlain L. The USPSTF recommendation on intimate partner violence: what we can learn from it and what we can do about it. Fam Viol Prev Health Pract 2005; 1:1–24.
- Moyer VA; US Preventive Services Task Force. Screening for intimate partner violence and abuse of elderly and vulnerable adults: US Preventive Services Task Force recommendation statement. Ann Intern Med 2013; 158:478–486.
- Taft A, O’Doherty L, Hegarty K, Ramsay J, Davidson L, Feder G. Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev 2013; 4:CD007007.
- McNutt LA, Carlson BE, Gagen D, Winterbauer N. Reproductive violence screening in primary care: perspectives and experiences of patients and battered women. J Am Med Womens Assoc 1999; 54:85–90.
- Friedman LS, Samet JH, Roberts MS, Hudlin M, Hans P. Inquiry about victimization experiences. A survey of patient p and physician practices. Arch Intern Med 1992; 152:1186–1190.
- Hamberger LK, Ambuel B, Marbella A, Donze J. Physician interaction with battered women: the women’s perspective. Arch Fam Med 1998; 7:575–582.
- Rodriguez MA, Bauer HM, Flores-Ortiz Y, Szkupinski-Quiroga S. Factors affecting patient-physician communication for abused Latina and Asian immigrant women. J Fam Pract 1998; 47:309–311.
- Rhodes KV, Frankel RM, Levinthal N, Prenoveau E, Bailey J, Levinson W. “You’re not a victim of domestic violence, are you?” Provider patient communication about domestic violence”. Ann Intern Med 2007; 147:620–627.
- Chang JC, Decker M, Moracco KE, Martin SL, Petersen R, Frasier PY. What happens when health care providers ask about intimate partner violence? A description of consequences from the perspectives of female survivors. J Am Med Womens Assoc 2003; 58:76–81.
- Chang JC, Decker MR, Moracco KE, Martin SL, Petersen R, Frasier PY. Asking about intimate partner violence: advice from female survivors to health care providers. Patient Educ Couns 2005; 59:141–147.
- Hathaway JE, Willis G, Zimmer B. Listening to survivors’ voices: addressing partner abuse in the health care setting. Violence Against Women 2002; 8:687–716.
- Gerbert B, Caspers N, Bronstone A, Moe J, Abercrombie P. A qualitative analysis of how physicians with expertise in domestic violence approach the identification of victims. Ann Intern Med 1999; 131:578–584.
- Gerbert B, Caspers N, Milliken N, Berlin M, Bronstone A, Moe J. Interventions that help victims of domestic violence. A qualitative analysis of physicians’ experiences. J Fam Pract 2000; 49:889–895.
- McCaw B, Bauer HM, Berman WH, Mooney L, Holmberg M, Hunkeler E. Women referred for on-site domestic violence services in a managed care organization. Women Health 2002; 35:23–40.
- McFarlane J, Malecha A, Gist J, et al. An intervention to increase safety behaviors of abused women: results of a randomized clinical trial. Nurs Res 2002; 51:347–354.
- Chang JC. Domestic violence. In:Bieber EJ, Sanfilippo JS, Horowitz IR, editors. Clinical Gynecology. Philadelphia, PA; Elsevier, Inc; 2006:79–89.
- Campbell JC, Webster D, Koziol-McLain J, et al. Risk factors for femicide in abusive relationships: results from a multisite case control study. Am J Public Health 2003; 93:1089–1097.
- Isaac NE, Enos V; National Institute of Justice. Documenting domestic violence: how health care providers can help victims. Research in Brief, 2001. https://www.ncjrs.gov/pdffiles1/nij/188564.pdf. Accessed June 3, 2014.
- Durborow N, Lizdas KC, O’Flaherty A, Marjavi A; Futures Without Violence. Compendium of state and US terrritory statutes and policies on domestic violence and health care, 2010. www.futureswithoutviolence.org/content/features/detail/1584/. Accessed June 3, 2014.
- Hyman A, Schillinger D, Lo B. Laws mandating reporting of domestic violence. Do they promote patient well-being? JAMA 1995; 273:1781–1787.
- Hyman A, Chez RA. Mandatory reporting of domestic violence by health care providers: a misguided approach. Womens Health Issues 1995; 5:208–213.
- Knight MA. Ethical debate: should doctors be more proactive as advocates for victims of violence? The police surgeon’s view: medical paternalism is unacceptable. BMJ 1995; 311:1620–1621.
- Hyman A; Futures Without Violence. Mandatory reporting of domestic violence by healthcare providers: a policy paper. San Francisco, CA; 1997. www.futureswithoutviolence.org/userfiles/file/HealthCare/mandatory_policypaper.pdf. Accessed June 3, 2014.
- Rodriguez MA, Craig AM, Mooney DR, Bauer HM. Patient attitudes about mandatory reporting of domestic violence. Implications for health care professionals. West J Med 1998; 169:337–341.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997; 90:1075–1080.
- Sachs CJ, Koziol-McLain J, Glass N, Webster D, Campbell J. A population-based survey assessing support for mandatory domestic violence reporting by health care personnel. Women Health 2002; 35:121–133.
- Sullivan CM, Hagen LA. Survivors’ opinions about mandatory reporting of domestic violence and sexual assault by medical professionals. Affilia 2005; 20:1–16.
- Rodriguez MA, McLoughlin E, Bauer HM, Paredes V, Grumbach K. Mandatory reporting of intimate partner violence to police: views of physicians in California. Am J Public Health 1999; 89:575–578.
- Futures Without Violence. Mandatory reporting of domestic violence to law enforcement by health care providers: a guide for advocates working to respond to or amend reporting laws related to domestic violence. www.healthcaresaboutipv.org/wp-content/blogs.dir/3/files/2012/09/Mandatory_Reporting_of_DV_to_Law-Enforcement_by_HCP.pdf. Accessed June 3, 2014.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997; 90:1075–1080.
- Gerbert B, Johnston K, Caspers N, Bleecker T, Woods A, Rosenbaum A. Experiences of battered women in health care settings: a qualitative study. Women Health 1996; 24:1–17.
- Chang JC, Cluss PA, Ranieri L, et al. Health care interventions for intimate partner violence: what women want. Womens Health Issues 2005; 15:21–30.
- Rodriguez MA, Quiroga SS, Bauer HM. Breaking the silence. Battered women’s perspectives on medical care. Arch Fam Med 1996; 5:153–158.
- Miller E, Decker MR, McCauley HL, et al. A family planning clinic partner violence intervention to reduce risk associated with reproductive coercion. Contraception 2011; 83:274–280.
- Landenburger K. A process of entrapment in and recovery from an abusive relationship. Issues Ment Health Nurs 1989; 10:209–227.
- Cluss PA, Chang JC, Hawker L, et al. The process of change for victims of intimate partner violence: support for a psychosocial readiness model. Womens Health Issues 2006; 16:262–274.
- Gerbert B, Abercrombie P, Caspers N, Love C, Bronstone A. How health care providers help battered women: the survivor’s perspective. Women Health 1999; 29:115–135.
- McCloskey LA, Lichter E, Williams C, Gerber M, Wittenberg E, Ganz M. Assessing intimate partner violence in health care settings leads to women’s receipt of interventions and improved health. Public Health Rep 2006; 121:435–444.
Also known as “domestic violence” and “spouse abuse,” intimate partner violence (IPV) is now the term defined by the US Centers for Disease Control and Prevention to include physical violence, sexual violence, threats of physical or sexual violence, and psychological or emotional abuse by a current or former spouse, common-law spouse, nonmarital dating partner, or boyfriend or girlfriend of the same or opposite sex.1 Although IPV is often hidden or kept secret by those affected, it is a highly prevalent issue, especially in women. Knowing how to broach the subject and provide appropriate support in a caring and nonjudgmental manner are the keys to helping a woman move forward in her readiness and ability to improve her situation.
See related patient information
ONE IN THREE WOMEN EXPERIENCES IPV IN HER LIFE
As clinicians, we have all seen patients who have been affected by IPV—even if we did not realize it at the time. Indeed, 36% of women in the United States (approximately 42.4 million) have experienced rape, physical violence, or stalking by an intimate partner in their lifetime, and 6% (approximately 7 million) have experienced these forms of IPV within the past 12 months.2
ASSOCIATION WITH MURDER
From 30% to 70% of women who are murdered are killed by a current or former intimate partner.3,4 Of those killed by their partner, two-thirds had previously reported physical assault, and 83% had been threatened by the man who eventually killed them.4 In another study, 44% of IPV murder victims had presented to an emergency department within 2 years of their murder.5
PHYSICAL EFFECTS NOT ALWAYS APPARENT
Although 41% of women who experience IPV suffer physical injury from their attacks, only 28% of those who are injured seek medical care.6 Because injuries are often absent or no longer apparent when an IPV victim decides to get help, it is important to be aware of the clinical signs associated with IPV:
- Gastrointestinal disorders7
- Depression8
- Anxiety
- Chronic pain syndromes9
- Substance abuse
- Suicidal ideation.10
In women of childbearing age, IPV is associated with unintended pregnancy, sexually transmitted infections, condom non-use,11,12 inconsistent condom use,13 and fear of talking about condom use.11,12 Coerced sexual experiences (eg, sexual intercourse that was not wanted or consented to) are common, with 28% to 42% of college women reporting at least one such experience. In more than three quarters of women who have been sexually assaulted, the first experience occurred before age 25.14,15
One-quarter of women ages 16 to 29 have experienced reproductive coercion, which includes birth control sabotage or pregnancy coercion by the active male partner.16 Among women reporting birth control sabotage, 79% had also been victims of physical or sexual IPV.16
The cost of providing health care to women experiencing IPV is 1.4 to 2.5 times higher than that of the nonabused population. Studies have shown that female victims of both physical and nonphysical (eg, emotional or verbal) IPV are more likely to use emergency, mental health, and outpatient health care services. The economic toll of IPV, including health care and costs from lost productivity and premature death, ranges from $2.3 to $8.3 billion per year.17,18
ASK FEMALE PATIENTS ABOUT IPV
In the early 1990s, various medical organizations began issuing policy statements that endorsed screening for IPV.19–22 Since 1992, the Joint Commission on Accreditation of Healthcare Organizations has required hospitals and clinics to provide assistance to those experiencing IPV.23 Although the United States Preventive Services Task Force initially found insufficient evidence to support regular IPV screening in health care settings,24–27 the group reversed its position in 2012 after a review of more recent studies. The group now recommends that clinicians address IPV with all women of childbearing age.28
A Cochrane review found that IPV screening increased identification of IPV survivors.29 Female participants in many studies wanted clinicians to ask routinely about violence and to provide information on community and legal resources.30,31
How should we ask about IPV?
Although various sets of screening questions and tools are available, no one instrument is considered better than the others. However, women experiencing IPV have specific preferences regarding how they want clinicians to ask and talk about the topic. In one survey, women who had experienced IPV preferred that clinicians ask about it as part of the complete medical history, as long as it did not create “an atmosphere of interrogation.”32
The style in which a clinician asks about IPV may make a difference as well. In focus groups, immigrant Latina and Asian women who had experienced IPV stated that clinicians could facilitate open communication by initiating the discussion and exhibiting compassionate and supportive behavior during the visit.33 Being able to see the same clinician at each visit also enhanced clinician-patient communication.33
In a study of IPV screening in emergency room settings, most clinicians asked about IPV in a perfunctory, direct manner—generally some variant of, “Are you a victim of domestic violence?” In this study, patient IPV disclosure occurred more often when clinicians used an open-ended approach such as, “Tell me what happened,” or when clinicians probed for possible IPV (eg, “What do you think may be causing some of this stress?”).34
In a focus group, female IPV survivors described feeling stigmatized or invalidated when clinicians were condescending, judgmental, or dismissive.35 Nonjudgmental and supportive communication decreased the women’s sense of isolation and led to positive outcomes such as increased awareness of IPV as a problem, decreased isolation, and feeling that the clinician cared.35
When addressing IPV, clinicians should explain why they are asking about it because it allows the woman to understand the context of the inquiry and to feel more comfortable about disclosing IPV. If the query is a regular part of a general screening or history-taking, for example, they should frame the question to make that point apparent. For example, “Because we know that many women in the United States experience physical, sexual or emotional violence from their romantic partners, I like to ask all of my patients whether they have been hurt or have felt threatened or afraid in a current or past relationship.”
In situations in which clinicians are concerned about IPV with a particular patient, they should explicitly share their concerns and desire to help the patient. One IPV survivor offered this advice: “Just look at the patient like she is your friend. Call her by her name. For instance, say ‘Sally, is he hurting you? Are you having problems? If you need help, I have some [phone] numbers.’ Personalize the encounter.”
It is also important to address IPV in a manner that ensures the patient’s safety, confidentiality, and dignity. When having this type of sensitive conversation, the patient should ideally be clothed and alone—without others present, particularly her partner. Professional interpreters should be available to women who do not speak English. The clinician should maintain eye contact, smile to communicate friendliness, and use a supportive tone.36
Just asking may be an intervention
Qualitative studies have suggested that just the act of asking about IPV in a nonjudgmental and compassionate manner is helpful to women experiencing IPV.35,37 Doing so not only helps women recognize the abuse, but also begins to decrease their sense of isolation and increase their awareness of helpful resources. It also gives the patient a sense that the clinician cares about her situation.35 As a result, experts have begun to recommend that health clinicians view asking about IPV not merely as a screening tool, but as a potentially therapeutic intervention in and of itself.35,37,38
HOW TO HELP
What to do when a woman discloses IPV
Female survivors, advocates, and health care clinicians who care for abused women suggest responding to a positive disclosure of IPV by providing the following:
Validation. The IPV perpetrator will often attempt to justify the violence and abuse by shifting some of the blame or responsibility for the violence onto the victim. This “brainwashing” leads to self-blame and a diminished sense of self-worth. However, clinicians can help reverse this mindset by acknowledging the woman’s disclosure and emphasizing that she did not deserve the abuse or violence. An example of such a statement is, “I am so very sorry that you went through that with your partner. You definitely did not deserve that. No one should ever be hurt by or afraid of the people who are supposed to love them.” Providing validation helps women recognize that the violence was a problem they did not deserve.38,39
Support. Women who have experienced IPV appreciate feeling supported and cared for by their health care clinician. Even if the patient is not ready to take any definitive action regarding her relationship or situation, knowing that her clinician and the health care setting are resources and sources of support is both comforting and empowering.35,40 Clinicians can communicate this support by stating, “I want you to know that whatever happens and whatever you decide, we are here for you.”
Respect for autonomy. Women experiencing IPV best understand their own situation and its various complexities and so they know best what they can do, cannot do, or need to do. As such, clinicians must respect a woman’s autonomy and preserve her ability to express her own needs and desires and make her own decisions. Prescribing a plan of action or giving commands to IPV victims could further perpetuate their sense of disempowerment and lack of control over their life.
Information. Providing referral information or hotline numbers to community domestic violence programs is helpful. However, not all women feel safe or comfortable taking printed brochures or written information with them because their abusive partner may find it. Thus, clinicians should ask if the patient can take the information safely or offer to write the numbers down without labeling them if she is afraid. The National Domestic Violence hotline is a 24-hour toll-free resource that will help women locate and contact shelters and other support services in their own community. The number, 1-800-799-SAFE (7233), is easy to memorize and thus is an easy resource to pass along quickly and safely. Other national organizations such as Futures Without Violence (formerly known as the Family Violence Prevention Fund) and the National Coalition Against Violence also provide links to local resources (Table 1).
Safety planning. Discussing the need for a safety plan will help the patient prepare for future abusive episodes. Even women who report that they are no longer in an abusive relationship should be asked about their current safety needs and concerns because they often remain in contact with abusive partners even after a relationship has ended.
When discussing safety planning, clinicians should ask the woman if she is currently safe or if she needs shelter. If she intends to return to or is still in contact with her batterer, ask if she has a plan for what to do or how to escape if the violence occurs again. Advise the patient to:
- Hide money so that she can leave quickly
- Make copies of birth certificates, immunization records, Social Security Number, and other important documents and keep them hidden and accessible
- Make a spare car key
- Have a list of hotline numbers
- Develop a code with friends, family, and neighbors that will let them know she needs immediate help.
Studies show that discussing safety-promoting behaviors increases the number of them that are used by IPV victims.41 A detailed list that can be shared with patients is provided in the patient information page that accompanies this article.42 Examples of personalized safety plans are available from the National Center on Domestic and Sexual Violence at its website, www.ncdsv.org/images/NCDSV_DVSafetyPlan_updated2013.pdf.
Danger assessment. Several researchers have examined potential risk factors associated with increased risk of homicide.43 Table 2 lists some of the characteristics associated with an increased risk of homicide in IPV situations.42 From this work, a danger assessment tool and scoring system has been developed. This tool and training on how to use it are available for free at www.dangerassessment.org. Although there are currently no outcome data on the benefits or risks of using this instrument, its objective is to increase women’s awareness of their danger level and individualize their safety counseling.
Proper documentation. Victim advocates and lawyers working on behalf of IPV victims emphasize that documentation by a medical provider can help a woman with her legal case. This documentation should be clear, legible, and as detailed as possible. These details should include a patient’s own words set off by quotation marks, a description or body map illustrating associated injuries or physical signs corroborating the violence, and a description of the patient’s demeanor or signs of emotion. Clinicians should avoid legal terms such as “alleges” or “alleged perpetrator” and should either define or avoid abbreviations that may be considered ambiguous in a legal proceeding (eg, clinicians should write out the words “domestic violence” or “intimate partner violence” rather than using “DV” or “IPV”).44 Most states have passed laws that prevent insurance companies from discriminating against IPV victims; insurance companies can no longer deny women coverage for seeking care related to IPV.45
A nonthreatening physical examination. Women who have experienced physical or sexual violence may feel anxious or experience added trauma during certain portions of the physical examination. Women who have been raped or otherwise sexually abused may have difficulty tolerating a pelvic examination, for example. Others who have been choked or grabbed by the neck may experience distress during palpation of the thyroid or cervical lymph nodes. The oropharyngeal examination may be challenging for women who have experienced forced oral sex or who may have had objects such as the barrel of a gun forced into their mouth. Asking women who have experienced IPV what aspects of the physical examination they may find difficult and how this could be made easier allows the patient and clinician to work together to develop strategies for or alternatives to necessary examinations or testing.
Before starting an examination, clinicians should explain what will happen and then ask the patient for her permission before moving on to the next step. Doing so creates a sense of control in an otherwise challenging and potentially traumatizing examination.
Disclosure of mandatory IPV reporting. Many states require health care providers to report any injuries caused by a weapon or criminal act to police or other official institutions.45,46 Several of these states specify that this reporting should occur during an IPV evaluation.
Mandatory reporting of IPV to police is highly controversial.47–49 Opponents of these laws argue that they do not benefit victims because they do not respect autonomy, they violate patient-clinician confidentiality, and they violate informed consent.47 Female IPV victims indicate that they would be less likely to disclose IPV and seek help if they knew it had to be reported.50–53 In a survey of California physicians, 59% stated that they might not comply with reporting laws if the patient objected.54
In states with mandatory reporting laws, clinicians can advocate for their patients by disclosing whether IPV must be reported before beginning their examination. The Michigan Coalition Against Domestic Violence devised this sample statement:
“I do have to let you know that under state law, I am obligated to make a police report to (name police agency with jurisdiction over the facility), if I/we are treating someone for any injury sustained by means of violence (tailor this information to the specifics of your state law). So, if you would have any concerns about that, I would encourage you to speak with one of the domestic violence advocates/counselors at (DV agency), who are able to provide confidential services and help without being required to make a police report.”55
The Compendium of State Statutes and Polices on Domestic Violence and Health Care by Futures Without Violence is an excellent reference that describes current state laws and policies regarding domestic violence and includes descriptions of the specific characteristics of each state’s mandatory reporting laws and their implications for health care providers. A copy can be downloaded from www.futureswithout-violence.org/content/features/detail/1584/.
What not to do
Clinicians should not ignore or minimize the extent of IPV, make excuses for the batterer, or blame the woman.32,56,57 They also should not inadvertently blame or criticize the woman by asking her, “What did you do to deserve this?” or “Why don’t you just leave?”57
While leaving a violent relationship is an obvious solution, many women experiencing IPV are either unwilling or unable to do so. In fact, leaving the batterer can be just as dangerous as staying. In a North Carolina study, half of all women killed by their partner had divorced or broken up with the partner immediately before the murder.4
What to do when a woman does not disclose IPV
Women who have experienced IPV often deny the violence to others out of fear. So a denial of violence, even in highly suspicious cases, can be expected. Abused patients often want help but are confused and afraid to ask for it.58,59 Providing easy and anonymous access to IPV information and resources through posters, flyers, brochures, and booklets will allow any woman—regardless of disclosure—to obtain help.36
In one IPV trial, all women in a family planning clinic who were in the intervention group were given information about IPV and how it can affect sexual and reproductive health, whether or not they disclosed. Compared with women in the control group, women who received the intervention—both those who did and did not experience IPV—were 63% more likely than those in the control group to end a relationship because they perceived it to be unhealthy or unsafe. In this case, all women—not just those who were victims—benefited from receiving information about IPV.60
PROVIDERS’ SUPPORT MAKES A DIFFERENCE, IMPROVES OUTCOMES
Patients may seek help for and find safety from IPV in stages or steps, and it may take them several months or even years to do so.61–63 In this sense, then, IPV is an issue that is not likely to be “cured” or changed in a single medical visit. In addition, a single visit may not be associated with direct health and safety outcomes. However, a patient is more likely to make changes if she has supportive and informative interaction with a caring, nonjudgmental clinician who can increase her awareness of IPV and IPV resources and promote an improved sense of self-efficacy or perceived power.40
For example, in a study in which health clinicians expressed concern about potential IPV health effects and offered support services such as counseling, 67% of women used one of those resources at least once.40 In another study, women who talked to a health care provider about their abuse were almost four times more likely to use an IPV intervention (eg, advocacy, shelter, restraining order) than women who did not talk to their provider. Those who used an IPV intervention were 2.6 times more likely to leave their abusive relationship, and those who left reported improved physical health.64
Thus, health care providers can have a positive effect by addressing this complex and difficult issue. The power and influence of a provider’s kindness, empathy, and support cannot be overestimated in their ability to improve the safety and well-being of women dealing with IPV.
Also known as “domestic violence” and “spouse abuse,” intimate partner violence (IPV) is now the term defined by the US Centers for Disease Control and Prevention to include physical violence, sexual violence, threats of physical or sexual violence, and psychological or emotional abuse by a current or former spouse, common-law spouse, nonmarital dating partner, or boyfriend or girlfriend of the same or opposite sex.1 Although IPV is often hidden or kept secret by those affected, it is a highly prevalent issue, especially in women. Knowing how to broach the subject and provide appropriate support in a caring and nonjudgmental manner are the keys to helping a woman move forward in her readiness and ability to improve her situation.
See related patient information
ONE IN THREE WOMEN EXPERIENCES IPV IN HER LIFE
As clinicians, we have all seen patients who have been affected by IPV—even if we did not realize it at the time. Indeed, 36% of women in the United States (approximately 42.4 million) have experienced rape, physical violence, or stalking by an intimate partner in their lifetime, and 6% (approximately 7 million) have experienced these forms of IPV within the past 12 months.2
ASSOCIATION WITH MURDER
From 30% to 70% of women who are murdered are killed by a current or former intimate partner.3,4 Of those killed by their partner, two-thirds had previously reported physical assault, and 83% had been threatened by the man who eventually killed them.4 In another study, 44% of IPV murder victims had presented to an emergency department within 2 years of their murder.5
PHYSICAL EFFECTS NOT ALWAYS APPARENT
Although 41% of women who experience IPV suffer physical injury from their attacks, only 28% of those who are injured seek medical care.6 Because injuries are often absent or no longer apparent when an IPV victim decides to get help, it is important to be aware of the clinical signs associated with IPV:
- Gastrointestinal disorders7
- Depression8
- Anxiety
- Chronic pain syndromes9
- Substance abuse
- Suicidal ideation.10
In women of childbearing age, IPV is associated with unintended pregnancy, sexually transmitted infections, condom non-use,11,12 inconsistent condom use,13 and fear of talking about condom use.11,12 Coerced sexual experiences (eg, sexual intercourse that was not wanted or consented to) are common, with 28% to 42% of college women reporting at least one such experience. In more than three quarters of women who have been sexually assaulted, the first experience occurred before age 25.14,15
One-quarter of women ages 16 to 29 have experienced reproductive coercion, which includes birth control sabotage or pregnancy coercion by the active male partner.16 Among women reporting birth control sabotage, 79% had also been victims of physical or sexual IPV.16
The cost of providing health care to women experiencing IPV is 1.4 to 2.5 times higher than that of the nonabused population. Studies have shown that female victims of both physical and nonphysical (eg, emotional or verbal) IPV are more likely to use emergency, mental health, and outpatient health care services. The economic toll of IPV, including health care and costs from lost productivity and premature death, ranges from $2.3 to $8.3 billion per year.17,18
ASK FEMALE PATIENTS ABOUT IPV
In the early 1990s, various medical organizations began issuing policy statements that endorsed screening for IPV.19–22 Since 1992, the Joint Commission on Accreditation of Healthcare Organizations has required hospitals and clinics to provide assistance to those experiencing IPV.23 Although the United States Preventive Services Task Force initially found insufficient evidence to support regular IPV screening in health care settings,24–27 the group reversed its position in 2012 after a review of more recent studies. The group now recommends that clinicians address IPV with all women of childbearing age.28
A Cochrane review found that IPV screening increased identification of IPV survivors.29 Female participants in many studies wanted clinicians to ask routinely about violence and to provide information on community and legal resources.30,31
How should we ask about IPV?
Although various sets of screening questions and tools are available, no one instrument is considered better than the others. However, women experiencing IPV have specific preferences regarding how they want clinicians to ask and talk about the topic. In one survey, women who had experienced IPV preferred that clinicians ask about it as part of the complete medical history, as long as it did not create “an atmosphere of interrogation.”32
The style in which a clinician asks about IPV may make a difference as well. In focus groups, immigrant Latina and Asian women who had experienced IPV stated that clinicians could facilitate open communication by initiating the discussion and exhibiting compassionate and supportive behavior during the visit.33 Being able to see the same clinician at each visit also enhanced clinician-patient communication.33
In a study of IPV screening in emergency room settings, most clinicians asked about IPV in a perfunctory, direct manner—generally some variant of, “Are you a victim of domestic violence?” In this study, patient IPV disclosure occurred more often when clinicians used an open-ended approach such as, “Tell me what happened,” or when clinicians probed for possible IPV (eg, “What do you think may be causing some of this stress?”).34
In a focus group, female IPV survivors described feeling stigmatized or invalidated when clinicians were condescending, judgmental, or dismissive.35 Nonjudgmental and supportive communication decreased the women’s sense of isolation and led to positive outcomes such as increased awareness of IPV as a problem, decreased isolation, and feeling that the clinician cared.35
When addressing IPV, clinicians should explain why they are asking about it because it allows the woman to understand the context of the inquiry and to feel more comfortable about disclosing IPV. If the query is a regular part of a general screening or history-taking, for example, they should frame the question to make that point apparent. For example, “Because we know that many women in the United States experience physical, sexual or emotional violence from their romantic partners, I like to ask all of my patients whether they have been hurt or have felt threatened or afraid in a current or past relationship.”
In situations in which clinicians are concerned about IPV with a particular patient, they should explicitly share their concerns and desire to help the patient. One IPV survivor offered this advice: “Just look at the patient like she is your friend. Call her by her name. For instance, say ‘Sally, is he hurting you? Are you having problems? If you need help, I have some [phone] numbers.’ Personalize the encounter.”
It is also important to address IPV in a manner that ensures the patient’s safety, confidentiality, and dignity. When having this type of sensitive conversation, the patient should ideally be clothed and alone—without others present, particularly her partner. Professional interpreters should be available to women who do not speak English. The clinician should maintain eye contact, smile to communicate friendliness, and use a supportive tone.36
Just asking may be an intervention
Qualitative studies have suggested that just the act of asking about IPV in a nonjudgmental and compassionate manner is helpful to women experiencing IPV.35,37 Doing so not only helps women recognize the abuse, but also begins to decrease their sense of isolation and increase their awareness of helpful resources. It also gives the patient a sense that the clinician cares about her situation.35 As a result, experts have begun to recommend that health clinicians view asking about IPV not merely as a screening tool, but as a potentially therapeutic intervention in and of itself.35,37,38
HOW TO HELP
What to do when a woman discloses IPV
Female survivors, advocates, and health care clinicians who care for abused women suggest responding to a positive disclosure of IPV by providing the following:
Validation. The IPV perpetrator will often attempt to justify the violence and abuse by shifting some of the blame or responsibility for the violence onto the victim. This “brainwashing” leads to self-blame and a diminished sense of self-worth. However, clinicians can help reverse this mindset by acknowledging the woman’s disclosure and emphasizing that she did not deserve the abuse or violence. An example of such a statement is, “I am so very sorry that you went through that with your partner. You definitely did not deserve that. No one should ever be hurt by or afraid of the people who are supposed to love them.” Providing validation helps women recognize that the violence was a problem they did not deserve.38,39
Support. Women who have experienced IPV appreciate feeling supported and cared for by their health care clinician. Even if the patient is not ready to take any definitive action regarding her relationship or situation, knowing that her clinician and the health care setting are resources and sources of support is both comforting and empowering.35,40 Clinicians can communicate this support by stating, “I want you to know that whatever happens and whatever you decide, we are here for you.”
Respect for autonomy. Women experiencing IPV best understand their own situation and its various complexities and so they know best what they can do, cannot do, or need to do. As such, clinicians must respect a woman’s autonomy and preserve her ability to express her own needs and desires and make her own decisions. Prescribing a plan of action or giving commands to IPV victims could further perpetuate their sense of disempowerment and lack of control over their life.
Information. Providing referral information or hotline numbers to community domestic violence programs is helpful. However, not all women feel safe or comfortable taking printed brochures or written information with them because their abusive partner may find it. Thus, clinicians should ask if the patient can take the information safely or offer to write the numbers down without labeling them if she is afraid. The National Domestic Violence hotline is a 24-hour toll-free resource that will help women locate and contact shelters and other support services in their own community. The number, 1-800-799-SAFE (7233), is easy to memorize and thus is an easy resource to pass along quickly and safely. Other national organizations such as Futures Without Violence (formerly known as the Family Violence Prevention Fund) and the National Coalition Against Violence also provide links to local resources (Table 1).
Safety planning. Discussing the need for a safety plan will help the patient prepare for future abusive episodes. Even women who report that they are no longer in an abusive relationship should be asked about their current safety needs and concerns because they often remain in contact with abusive partners even after a relationship has ended.
When discussing safety planning, clinicians should ask the woman if she is currently safe or if she needs shelter. If she intends to return to or is still in contact with her batterer, ask if she has a plan for what to do or how to escape if the violence occurs again. Advise the patient to:
- Hide money so that she can leave quickly
- Make copies of birth certificates, immunization records, Social Security Number, and other important documents and keep them hidden and accessible
- Make a spare car key
- Have a list of hotline numbers
- Develop a code with friends, family, and neighbors that will let them know she needs immediate help.
Studies show that discussing safety-promoting behaviors increases the number of them that are used by IPV victims.41 A detailed list that can be shared with patients is provided in the patient information page that accompanies this article.42 Examples of personalized safety plans are available from the National Center on Domestic and Sexual Violence at its website, www.ncdsv.org/images/NCDSV_DVSafetyPlan_updated2013.pdf.
Danger assessment. Several researchers have examined potential risk factors associated with increased risk of homicide.43 Table 2 lists some of the characteristics associated with an increased risk of homicide in IPV situations.42 From this work, a danger assessment tool and scoring system has been developed. This tool and training on how to use it are available for free at www.dangerassessment.org. Although there are currently no outcome data on the benefits or risks of using this instrument, its objective is to increase women’s awareness of their danger level and individualize their safety counseling.
Proper documentation. Victim advocates and lawyers working on behalf of IPV victims emphasize that documentation by a medical provider can help a woman with her legal case. This documentation should be clear, legible, and as detailed as possible. These details should include a patient’s own words set off by quotation marks, a description or body map illustrating associated injuries or physical signs corroborating the violence, and a description of the patient’s demeanor or signs of emotion. Clinicians should avoid legal terms such as “alleges” or “alleged perpetrator” and should either define or avoid abbreviations that may be considered ambiguous in a legal proceeding (eg, clinicians should write out the words “domestic violence” or “intimate partner violence” rather than using “DV” or “IPV”).44 Most states have passed laws that prevent insurance companies from discriminating against IPV victims; insurance companies can no longer deny women coverage for seeking care related to IPV.45
A nonthreatening physical examination. Women who have experienced physical or sexual violence may feel anxious or experience added trauma during certain portions of the physical examination. Women who have been raped or otherwise sexually abused may have difficulty tolerating a pelvic examination, for example. Others who have been choked or grabbed by the neck may experience distress during palpation of the thyroid or cervical lymph nodes. The oropharyngeal examination may be challenging for women who have experienced forced oral sex or who may have had objects such as the barrel of a gun forced into their mouth. Asking women who have experienced IPV what aspects of the physical examination they may find difficult and how this could be made easier allows the patient and clinician to work together to develop strategies for or alternatives to necessary examinations or testing.
Before starting an examination, clinicians should explain what will happen and then ask the patient for her permission before moving on to the next step. Doing so creates a sense of control in an otherwise challenging and potentially traumatizing examination.
Disclosure of mandatory IPV reporting. Many states require health care providers to report any injuries caused by a weapon or criminal act to police or other official institutions.45,46 Several of these states specify that this reporting should occur during an IPV evaluation.
Mandatory reporting of IPV to police is highly controversial.47–49 Opponents of these laws argue that they do not benefit victims because they do not respect autonomy, they violate patient-clinician confidentiality, and they violate informed consent.47 Female IPV victims indicate that they would be less likely to disclose IPV and seek help if they knew it had to be reported.50–53 In a survey of California physicians, 59% stated that they might not comply with reporting laws if the patient objected.54
In states with mandatory reporting laws, clinicians can advocate for their patients by disclosing whether IPV must be reported before beginning their examination. The Michigan Coalition Against Domestic Violence devised this sample statement:
“I do have to let you know that under state law, I am obligated to make a police report to (name police agency with jurisdiction over the facility), if I/we are treating someone for any injury sustained by means of violence (tailor this information to the specifics of your state law). So, if you would have any concerns about that, I would encourage you to speak with one of the domestic violence advocates/counselors at (DV agency), who are able to provide confidential services and help without being required to make a police report.”55
The Compendium of State Statutes and Polices on Domestic Violence and Health Care by Futures Without Violence is an excellent reference that describes current state laws and policies regarding domestic violence and includes descriptions of the specific characteristics of each state’s mandatory reporting laws and their implications for health care providers. A copy can be downloaded from www.futureswithout-violence.org/content/features/detail/1584/.
What not to do
Clinicians should not ignore or minimize the extent of IPV, make excuses for the batterer, or blame the woman.32,56,57 They also should not inadvertently blame or criticize the woman by asking her, “What did you do to deserve this?” or “Why don’t you just leave?”57
While leaving a violent relationship is an obvious solution, many women experiencing IPV are either unwilling or unable to do so. In fact, leaving the batterer can be just as dangerous as staying. In a North Carolina study, half of all women killed by their partner had divorced or broken up with the partner immediately before the murder.4
What to do when a woman does not disclose IPV
Women who have experienced IPV often deny the violence to others out of fear. So a denial of violence, even in highly suspicious cases, can be expected. Abused patients often want help but are confused and afraid to ask for it.58,59 Providing easy and anonymous access to IPV information and resources through posters, flyers, brochures, and booklets will allow any woman—regardless of disclosure—to obtain help.36
In one IPV trial, all women in a family planning clinic who were in the intervention group were given information about IPV and how it can affect sexual and reproductive health, whether or not they disclosed. Compared with women in the control group, women who received the intervention—both those who did and did not experience IPV—were 63% more likely than those in the control group to end a relationship because they perceived it to be unhealthy or unsafe. In this case, all women—not just those who were victims—benefited from receiving information about IPV.60
PROVIDERS’ SUPPORT MAKES A DIFFERENCE, IMPROVES OUTCOMES
Patients may seek help for and find safety from IPV in stages or steps, and it may take them several months or even years to do so.61–63 In this sense, then, IPV is an issue that is not likely to be “cured” or changed in a single medical visit. In addition, a single visit may not be associated with direct health and safety outcomes. However, a patient is more likely to make changes if she has supportive and informative interaction with a caring, nonjudgmental clinician who can increase her awareness of IPV and IPV resources and promote an improved sense of self-efficacy or perceived power.40
For example, in a study in which health clinicians expressed concern about potential IPV health effects and offered support services such as counseling, 67% of women used one of those resources at least once.40 In another study, women who talked to a health care provider about their abuse were almost four times more likely to use an IPV intervention (eg, advocacy, shelter, restraining order) than women who did not talk to their provider. Those who used an IPV intervention were 2.6 times more likely to leave their abusive relationship, and those who left reported improved physical health.64
Thus, health care providers can have a positive effect by addressing this complex and difficult issue. The power and influence of a provider’s kindness, empathy, and support cannot be overestimated in their ability to improve the safety and well-being of women dealing with IPV.
- Saltzman LE, Fanslow JL, McMahon PM, Shelley GA; National Center for Injury Prevention and Control; Centers for Disease Control and Prevention. Intimate partner violence surveillance: uniform definitions and recommended data elements, Version 1.0. Atlanta, GA; 1999. www.cdc.gov/ncipc/pub-res/ipv_surveillance/intimate%20partner%20violence.pdf. Accessed June 3, 2014.
- Black MC, Basile KC, Breiding MJ, et al; Center for Injury Prevention and Control; Centers for Disease Control and Prevention. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta, GA. www.cdc.gov/violenceprevention/pdf/nisvs_executive_summary-a.pdf. Accessed June 3, 2014.
- Kellermann AL, Mercy JA. Men, women, and murder: gender-specific differences in rates of fatal violence and victimization. J Trauma 1992; 33:1–5.
- Moracco KE, Runywan CW, Butts JD. Femicide in North Carolina, 1991–1993: a statewide study of patterns and precursors. Homicide Studies 1998; 4:422–446.
- Wadman MC, Muelleman RL. Domestic violence homicides: ED use before victimization. Am J Emerg Med 1999; 17:689–691.
- Catalano SM; United States Bureau of Justice Statistics. Intimate partner violence in the United States: 2007. http://bjs.ojp.usdoj.gov/index.cfm?ty=pbdetail&iid=1000. Accessed February 19, 2014.
- Drossman DA, Talley NJ, Leserman J, Olden KW, Barreiro MA. Sexual and physical abuse and gastrointestinal illness. Review and recommendations. Ann Intern Med 1995; 123:782–794.
- Scholle SH, Rost KM, Golding JM. Physical abuse among depressed women. J Gen Intern Med 1998; 13:607–613.
- Walling MK, O’Hara MW, Reiter RC, Milburn AK, Lilly G, Vincent SD. Abuse history and chronic pain in women: II. A multivariate analysis of abuse and psychological morbidity. Obstet Gynecol 1994; 84:200–206.
- McCauley J, Kern DE, Kolodner K, Derogatis LR, Bass EB. Relation of low-severity violence to women’s health. J Gen Intern Med 1998; 13:687–691.
- Wingood GM, DiClemente RJ. The effects of an abusive primary partner on the condom use and sexual negotiation practices of African-American women. Am J Public Health 1997; 87:1016–1018.
- Sales JM, Salazar LF, Wingood GM, DiClemente RJ, Rose E, Crosby RA. The mediating role of partner communication skills on HIV/STD-associated risk behaviors in young African American females with a history of sexual violence. Arch Pediatr Adolesc Med 2008; 162:432–438.
- Davila YR, Brackley MH. Mexican and Mexican American women in a battered women’s shelter: barriers to condom negotiation for HIV/AIDS prevention. Issues Ment Health Nurs 1999; 20:333–355.
- Tjaden P, Thoennes N; National Institute of Justice; Centers for Disease Control and Prevention. Prevalence, incidence and consequences of violence against women: findings from the national violence against women survey. Washington, DC; 1998. https://www.ncjrs.gov/pdffiles/172837.pdf. Accessed June 3, 2014.
- Masho SW, Odor RK, Adera T. Sexual assault in Virginia: a population-based study. Womens Health Issues 2005; 15:157–166.
- Miller E, Decker MR, McCauley HL, et al. Pregnancy coercion, intimate partner violence and unintended pregnancy. Contraception 2010; 81:316–322.
- Bonomi AE, Anderson ML, Rivara FP, Thompson RS. Health care utilization and costs associated with physical and nonphysical-only intimate partner violence. Health Serv Res 2009; 44:1052–1067.
- Rivara FP, Anderson ML, Fishman P, et al. Healthcare utilization and costs for women with a history of intimate partner violence. Am J Prev Med 2007; 32:89–96.
- American Nurses Association. Position statement on physical violence against women. Washington, DC; 1991.
- Physicians and domestic violence. Ethical considerations. Council on Ethical and Judicial Affairs, American Medical Association. JAMA 1992; 267:3190–3193.
- The American College of Obstetricians and Gynecologists. Screening tools: domestic violence. http://www.acog.org/About_ACOG/ACOG_Departments/Violence_Against_Women/Screening_Tools__Domestic_Violence. Accessed June 3, 2014.
- Lee D, James L, Sawires P; The Family Violence Prevention Fund. Preventing domestic violence: clinical guidelines on routine screening. San Francisco, CA; 1999. http://new.vawnet.org/Assoc_Files_VAWnet/screpol.pdf. Accessed June 3, 2014.
- Joint Commission on Accreditation of Healthcare Organizations. Accreditation manual for hospitals. Chicago, IL; 1992.
- US Department of Health and Human Services. US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd ed. Washington, DC; 1996.
- Ramsay J, Richardson J, Carter YH, Davidson LL, Feder G. Should health professionals screen women for domestic violence? Systematic review. BMJ 2002; 325:314.
- Nelson HD, Nygren P, McInerney Y, Klein J; US Preventive Services Task Force. Screening women and elderly adults for family and intimate partner violence: a review of the evidence for the US Preventive Services Task Force. Ann Intern Med 2004; 140:387–396.
- Chamberlain L. The USPSTF recommendation on intimate partner violence: what we can learn from it and what we can do about it. Fam Viol Prev Health Pract 2005; 1:1–24.
- Moyer VA; US Preventive Services Task Force. Screening for intimate partner violence and abuse of elderly and vulnerable adults: US Preventive Services Task Force recommendation statement. Ann Intern Med 2013; 158:478–486.
- Taft A, O’Doherty L, Hegarty K, Ramsay J, Davidson L, Feder G. Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev 2013; 4:CD007007.
- McNutt LA, Carlson BE, Gagen D, Winterbauer N. Reproductive violence screening in primary care: perspectives and experiences of patients and battered women. J Am Med Womens Assoc 1999; 54:85–90.
- Friedman LS, Samet JH, Roberts MS, Hudlin M, Hans P. Inquiry about victimization experiences. A survey of patient p and physician practices. Arch Intern Med 1992; 152:1186–1190.
- Hamberger LK, Ambuel B, Marbella A, Donze J. Physician interaction with battered women: the women’s perspective. Arch Fam Med 1998; 7:575–582.
- Rodriguez MA, Bauer HM, Flores-Ortiz Y, Szkupinski-Quiroga S. Factors affecting patient-physician communication for abused Latina and Asian immigrant women. J Fam Pract 1998; 47:309–311.
- Rhodes KV, Frankel RM, Levinthal N, Prenoveau E, Bailey J, Levinson W. “You’re not a victim of domestic violence, are you?” Provider patient communication about domestic violence”. Ann Intern Med 2007; 147:620–627.
- Chang JC, Decker M, Moracco KE, Martin SL, Petersen R, Frasier PY. What happens when health care providers ask about intimate partner violence? A description of consequences from the perspectives of female survivors. J Am Med Womens Assoc 2003; 58:76–81.
- Chang JC, Decker MR, Moracco KE, Martin SL, Petersen R, Frasier PY. Asking about intimate partner violence: advice from female survivors to health care providers. Patient Educ Couns 2005; 59:141–147.
- Hathaway JE, Willis G, Zimmer B. Listening to survivors’ voices: addressing partner abuse in the health care setting. Violence Against Women 2002; 8:687–716.
- Gerbert B, Caspers N, Bronstone A, Moe J, Abercrombie P. A qualitative analysis of how physicians with expertise in domestic violence approach the identification of victims. Ann Intern Med 1999; 131:578–584.
- Gerbert B, Caspers N, Milliken N, Berlin M, Bronstone A, Moe J. Interventions that help victims of domestic violence. A qualitative analysis of physicians’ experiences. J Fam Pract 2000; 49:889–895.
- McCaw B, Bauer HM, Berman WH, Mooney L, Holmberg M, Hunkeler E. Women referred for on-site domestic violence services in a managed care organization. Women Health 2002; 35:23–40.
- McFarlane J, Malecha A, Gist J, et al. An intervention to increase safety behaviors of abused women: results of a randomized clinical trial. Nurs Res 2002; 51:347–354.
- Chang JC. Domestic violence. In:Bieber EJ, Sanfilippo JS, Horowitz IR, editors. Clinical Gynecology. Philadelphia, PA; Elsevier, Inc; 2006:79–89.
- Campbell JC, Webster D, Koziol-McLain J, et al. Risk factors for femicide in abusive relationships: results from a multisite case control study. Am J Public Health 2003; 93:1089–1097.
- Isaac NE, Enos V; National Institute of Justice. Documenting domestic violence: how health care providers can help victims. Research in Brief, 2001. https://www.ncjrs.gov/pdffiles1/nij/188564.pdf. Accessed June 3, 2014.
- Durborow N, Lizdas KC, O’Flaherty A, Marjavi A; Futures Without Violence. Compendium of state and US terrritory statutes and policies on domestic violence and health care, 2010. www.futureswithoutviolence.org/content/features/detail/1584/. Accessed June 3, 2014.
- Hyman A, Schillinger D, Lo B. Laws mandating reporting of domestic violence. Do they promote patient well-being? JAMA 1995; 273:1781–1787.
- Hyman A, Chez RA. Mandatory reporting of domestic violence by health care providers: a misguided approach. Womens Health Issues 1995; 5:208–213.
- Knight MA. Ethical debate: should doctors be more proactive as advocates for victims of violence? The police surgeon’s view: medical paternalism is unacceptable. BMJ 1995; 311:1620–1621.
- Hyman A; Futures Without Violence. Mandatory reporting of domestic violence by healthcare providers: a policy paper. San Francisco, CA; 1997. www.futureswithoutviolence.org/userfiles/file/HealthCare/mandatory_policypaper.pdf. Accessed June 3, 2014.
- Rodriguez MA, Craig AM, Mooney DR, Bauer HM. Patient attitudes about mandatory reporting of domestic violence. Implications for health care professionals. West J Med 1998; 169:337–341.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997; 90:1075–1080.
- Sachs CJ, Koziol-McLain J, Glass N, Webster D, Campbell J. A population-based survey assessing support for mandatory domestic violence reporting by health care personnel. Women Health 2002; 35:121–133.
- Sullivan CM, Hagen LA. Survivors’ opinions about mandatory reporting of domestic violence and sexual assault by medical professionals. Affilia 2005; 20:1–16.
- Rodriguez MA, McLoughlin E, Bauer HM, Paredes V, Grumbach K. Mandatory reporting of intimate partner violence to police: views of physicians in California. Am J Public Health 1999; 89:575–578.
- Futures Without Violence. Mandatory reporting of domestic violence to law enforcement by health care providers: a guide for advocates working to respond to or amend reporting laws related to domestic violence. www.healthcaresaboutipv.org/wp-content/blogs.dir/3/files/2012/09/Mandatory_Reporting_of_DV_to_Law-Enforcement_by_HCP.pdf. Accessed June 3, 2014.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997; 90:1075–1080.
- Gerbert B, Johnston K, Caspers N, Bleecker T, Woods A, Rosenbaum A. Experiences of battered women in health care settings: a qualitative study. Women Health 1996; 24:1–17.
- Chang JC, Cluss PA, Ranieri L, et al. Health care interventions for intimate partner violence: what women want. Womens Health Issues 2005; 15:21–30.
- Rodriguez MA, Quiroga SS, Bauer HM. Breaking the silence. Battered women’s perspectives on medical care. Arch Fam Med 1996; 5:153–158.
- Miller E, Decker MR, McCauley HL, et al. A family planning clinic partner violence intervention to reduce risk associated with reproductive coercion. Contraception 2011; 83:274–280.
- Landenburger K. A process of entrapment in and recovery from an abusive relationship. Issues Ment Health Nurs 1989; 10:209–227.
- Cluss PA, Chang JC, Hawker L, et al. The process of change for victims of intimate partner violence: support for a psychosocial readiness model. Womens Health Issues 2006; 16:262–274.
- Gerbert B, Abercrombie P, Caspers N, Love C, Bronstone A. How health care providers help battered women: the survivor’s perspective. Women Health 1999; 29:115–135.
- McCloskey LA, Lichter E, Williams C, Gerber M, Wittenberg E, Ganz M. Assessing intimate partner violence in health care settings leads to women’s receipt of interventions and improved health. Public Health Rep 2006; 121:435–444.
- Saltzman LE, Fanslow JL, McMahon PM, Shelley GA; National Center for Injury Prevention and Control; Centers for Disease Control and Prevention. Intimate partner violence surveillance: uniform definitions and recommended data elements, Version 1.0. Atlanta, GA; 1999. www.cdc.gov/ncipc/pub-res/ipv_surveillance/intimate%20partner%20violence.pdf. Accessed June 3, 2014.
- Black MC, Basile KC, Breiding MJ, et al; Center for Injury Prevention and Control; Centers for Disease Control and Prevention. The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Summary Report. Atlanta, GA. www.cdc.gov/violenceprevention/pdf/nisvs_executive_summary-a.pdf. Accessed June 3, 2014.
- Kellermann AL, Mercy JA. Men, women, and murder: gender-specific differences in rates of fatal violence and victimization. J Trauma 1992; 33:1–5.
- Moracco KE, Runywan CW, Butts JD. Femicide in North Carolina, 1991–1993: a statewide study of patterns and precursors. Homicide Studies 1998; 4:422–446.
- Wadman MC, Muelleman RL. Domestic violence homicides: ED use before victimization. Am J Emerg Med 1999; 17:689–691.
- Catalano SM; United States Bureau of Justice Statistics. Intimate partner violence in the United States: 2007. http://bjs.ojp.usdoj.gov/index.cfm?ty=pbdetail&iid=1000. Accessed February 19, 2014.
- Drossman DA, Talley NJ, Leserman J, Olden KW, Barreiro MA. Sexual and physical abuse and gastrointestinal illness. Review and recommendations. Ann Intern Med 1995; 123:782–794.
- Scholle SH, Rost KM, Golding JM. Physical abuse among depressed women. J Gen Intern Med 1998; 13:607–613.
- Walling MK, O’Hara MW, Reiter RC, Milburn AK, Lilly G, Vincent SD. Abuse history and chronic pain in women: II. A multivariate analysis of abuse and psychological morbidity. Obstet Gynecol 1994; 84:200–206.
- McCauley J, Kern DE, Kolodner K, Derogatis LR, Bass EB. Relation of low-severity violence to women’s health. J Gen Intern Med 1998; 13:687–691.
- Wingood GM, DiClemente RJ. The effects of an abusive primary partner on the condom use and sexual negotiation practices of African-American women. Am J Public Health 1997; 87:1016–1018.
- Sales JM, Salazar LF, Wingood GM, DiClemente RJ, Rose E, Crosby RA. The mediating role of partner communication skills on HIV/STD-associated risk behaviors in young African American females with a history of sexual violence. Arch Pediatr Adolesc Med 2008; 162:432–438.
- Davila YR, Brackley MH. Mexican and Mexican American women in a battered women’s shelter: barriers to condom negotiation for HIV/AIDS prevention. Issues Ment Health Nurs 1999; 20:333–355.
- Tjaden P, Thoennes N; National Institute of Justice; Centers for Disease Control and Prevention. Prevalence, incidence and consequences of violence against women: findings from the national violence against women survey. Washington, DC; 1998. https://www.ncjrs.gov/pdffiles/172837.pdf. Accessed June 3, 2014.
- Masho SW, Odor RK, Adera T. Sexual assault in Virginia: a population-based study. Womens Health Issues 2005; 15:157–166.
- Miller E, Decker MR, McCauley HL, et al. Pregnancy coercion, intimate partner violence and unintended pregnancy. Contraception 2010; 81:316–322.
- Bonomi AE, Anderson ML, Rivara FP, Thompson RS. Health care utilization and costs associated with physical and nonphysical-only intimate partner violence. Health Serv Res 2009; 44:1052–1067.
- Rivara FP, Anderson ML, Fishman P, et al. Healthcare utilization and costs for women with a history of intimate partner violence. Am J Prev Med 2007; 32:89–96.
- American Nurses Association. Position statement on physical violence against women. Washington, DC; 1991.
- Physicians and domestic violence. Ethical considerations. Council on Ethical and Judicial Affairs, American Medical Association. JAMA 1992; 267:3190–3193.
- The American College of Obstetricians and Gynecologists. Screening tools: domestic violence. http://www.acog.org/About_ACOG/ACOG_Departments/Violence_Against_Women/Screening_Tools__Domestic_Violence. Accessed June 3, 2014.
- Lee D, James L, Sawires P; The Family Violence Prevention Fund. Preventing domestic violence: clinical guidelines on routine screening. San Francisco, CA; 1999. http://new.vawnet.org/Assoc_Files_VAWnet/screpol.pdf. Accessed June 3, 2014.
- Joint Commission on Accreditation of Healthcare Organizations. Accreditation manual for hospitals. Chicago, IL; 1992.
- US Department of Health and Human Services. US Preventive Services Task Force. Guide to Clinical Preventive Services. 2nd ed. Washington, DC; 1996.
- Ramsay J, Richardson J, Carter YH, Davidson LL, Feder G. Should health professionals screen women for domestic violence? Systematic review. BMJ 2002; 325:314.
- Nelson HD, Nygren P, McInerney Y, Klein J; US Preventive Services Task Force. Screening women and elderly adults for family and intimate partner violence: a review of the evidence for the US Preventive Services Task Force. Ann Intern Med 2004; 140:387–396.
- Chamberlain L. The USPSTF recommendation on intimate partner violence: what we can learn from it and what we can do about it. Fam Viol Prev Health Pract 2005; 1:1–24.
- Moyer VA; US Preventive Services Task Force. Screening for intimate partner violence and abuse of elderly and vulnerable adults: US Preventive Services Task Force recommendation statement. Ann Intern Med 2013; 158:478–486.
- Taft A, O’Doherty L, Hegarty K, Ramsay J, Davidson L, Feder G. Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev 2013; 4:CD007007.
- McNutt LA, Carlson BE, Gagen D, Winterbauer N. Reproductive violence screening in primary care: perspectives and experiences of patients and battered women. J Am Med Womens Assoc 1999; 54:85–90.
- Friedman LS, Samet JH, Roberts MS, Hudlin M, Hans P. Inquiry about victimization experiences. A survey of patient p and physician practices. Arch Intern Med 1992; 152:1186–1190.
- Hamberger LK, Ambuel B, Marbella A, Donze J. Physician interaction with battered women: the women’s perspective. Arch Fam Med 1998; 7:575–582.
- Rodriguez MA, Bauer HM, Flores-Ortiz Y, Szkupinski-Quiroga S. Factors affecting patient-physician communication for abused Latina and Asian immigrant women. J Fam Pract 1998; 47:309–311.
- Rhodes KV, Frankel RM, Levinthal N, Prenoveau E, Bailey J, Levinson W. “You’re not a victim of domestic violence, are you?” Provider patient communication about domestic violence”. Ann Intern Med 2007; 147:620–627.
- Chang JC, Decker M, Moracco KE, Martin SL, Petersen R, Frasier PY. What happens when health care providers ask about intimate partner violence? A description of consequences from the perspectives of female survivors. J Am Med Womens Assoc 2003; 58:76–81.
- Chang JC, Decker MR, Moracco KE, Martin SL, Petersen R, Frasier PY. Asking about intimate partner violence: advice from female survivors to health care providers. Patient Educ Couns 2005; 59:141–147.
- Hathaway JE, Willis G, Zimmer B. Listening to survivors’ voices: addressing partner abuse in the health care setting. Violence Against Women 2002; 8:687–716.
- Gerbert B, Caspers N, Bronstone A, Moe J, Abercrombie P. A qualitative analysis of how physicians with expertise in domestic violence approach the identification of victims. Ann Intern Med 1999; 131:578–584.
- Gerbert B, Caspers N, Milliken N, Berlin M, Bronstone A, Moe J. Interventions that help victims of domestic violence. A qualitative analysis of physicians’ experiences. J Fam Pract 2000; 49:889–895.
- McCaw B, Bauer HM, Berman WH, Mooney L, Holmberg M, Hunkeler E. Women referred for on-site domestic violence services in a managed care organization. Women Health 2002; 35:23–40.
- McFarlane J, Malecha A, Gist J, et al. An intervention to increase safety behaviors of abused women: results of a randomized clinical trial. Nurs Res 2002; 51:347–354.
- Chang JC. Domestic violence. In:Bieber EJ, Sanfilippo JS, Horowitz IR, editors. Clinical Gynecology. Philadelphia, PA; Elsevier, Inc; 2006:79–89.
- Campbell JC, Webster D, Koziol-McLain J, et al. Risk factors for femicide in abusive relationships: results from a multisite case control study. Am J Public Health 2003; 93:1089–1097.
- Isaac NE, Enos V; National Institute of Justice. Documenting domestic violence: how health care providers can help victims. Research in Brief, 2001. https://www.ncjrs.gov/pdffiles1/nij/188564.pdf. Accessed June 3, 2014.
- Durborow N, Lizdas KC, O’Flaherty A, Marjavi A; Futures Without Violence. Compendium of state and US terrritory statutes and policies on domestic violence and health care, 2010. www.futureswithoutviolence.org/content/features/detail/1584/. Accessed June 3, 2014.
- Hyman A, Schillinger D, Lo B. Laws mandating reporting of domestic violence. Do they promote patient well-being? JAMA 1995; 273:1781–1787.
- Hyman A, Chez RA. Mandatory reporting of domestic violence by health care providers: a misguided approach. Womens Health Issues 1995; 5:208–213.
- Knight MA. Ethical debate: should doctors be more proactive as advocates for victims of violence? The police surgeon’s view: medical paternalism is unacceptable. BMJ 1995; 311:1620–1621.
- Hyman A; Futures Without Violence. Mandatory reporting of domestic violence by healthcare providers: a policy paper. San Francisco, CA; 1997. www.futureswithoutviolence.org/userfiles/file/HealthCare/mandatory_policypaper.pdf. Accessed June 3, 2014.
- Rodriguez MA, Craig AM, Mooney DR, Bauer HM. Patient attitudes about mandatory reporting of domestic violence. Implications for health care professionals. West J Med 1998; 169:337–341.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997; 90:1075–1080.
- Sachs CJ, Koziol-McLain J, Glass N, Webster D, Campbell J. A population-based survey assessing support for mandatory domestic violence reporting by health care personnel. Women Health 2002; 35:121–133.
- Sullivan CM, Hagen LA. Survivors’ opinions about mandatory reporting of domestic violence and sexual assault by medical professionals. Affilia 2005; 20:1–16.
- Rodriguez MA, McLoughlin E, Bauer HM, Paredes V, Grumbach K. Mandatory reporting of intimate partner violence to police: views of physicians in California. Am J Public Health 1999; 89:575–578.
- Futures Without Violence. Mandatory reporting of domestic violence to law enforcement by health care providers: a guide for advocates working to respond to or amend reporting laws related to domestic violence. www.healthcaresaboutipv.org/wp-content/blogs.dir/3/files/2012/09/Mandatory_Reporting_of_DV_to_Law-Enforcement_by_HCP.pdf. Accessed June 3, 2014.
- Caralis PV, Musialowski R. Women’s experiences with domestic violence and their attitudes and expectations regarding medical care of abuse victims. South Med J 1997; 90:1075–1080.
- Gerbert B, Johnston K, Caspers N, Bleecker T, Woods A, Rosenbaum A. Experiences of battered women in health care settings: a qualitative study. Women Health 1996; 24:1–17.
- Chang JC, Cluss PA, Ranieri L, et al. Health care interventions for intimate partner violence: what women want. Womens Health Issues 2005; 15:21–30.
- Rodriguez MA, Quiroga SS, Bauer HM. Breaking the silence. Battered women’s perspectives on medical care. Arch Fam Med 1996; 5:153–158.
- Miller E, Decker MR, McCauley HL, et al. A family planning clinic partner violence intervention to reduce risk associated with reproductive coercion. Contraception 2011; 83:274–280.
- Landenburger K. A process of entrapment in and recovery from an abusive relationship. Issues Ment Health Nurs 1989; 10:209–227.
- Cluss PA, Chang JC, Hawker L, et al. The process of change for victims of intimate partner violence: support for a psychosocial readiness model. Womens Health Issues 2006; 16:262–274.
- Gerbert B, Abercrombie P, Caspers N, Love C, Bronstone A. How health care providers help battered women: the survivor’s perspective. Women Health 1999; 29:115–135.
- McCloskey LA, Lichter E, Williams C, Gerber M, Wittenberg E, Ganz M. Assessing intimate partner violence in health care settings leads to women’s receipt of interventions and improved health. Public Health Rep 2006; 121:435–444.
KEY POINTS
- Many victims of IPV will not present with injuries but may have medical or mental health issues related to their IPV experiences.
- Addressing IPV with female patients not only results in increased identification of survivors but is also associated with cognitive and emotional benefits.
- IPV information and resources should be provided to all women, regardless of IPV disclosure.
- Clinicians should respond to a patient’s IPV disclosure with validation, support, respect, and information.
- Clinicians must respect patients’ autonomy, as they are the ones who best understand their situation and know what they need. In some cases, leaving an abusive relationship can be more dangerous than staying.