User login
› Evaluate patients for movement disorders before initiating or adjusting antipsychotic therapy, then weekly until the dose is stabilized. A
› Use nonpharmacologic interventions—eg, positive reinforcement, music, light exercise—as first-line therapy for neuropsychiatric symptoms of dementia; consider antipsychotic therapy only if they fail. A
› Obtain a fasting glucose level before initiating or adjusting antipsychotic therapy, then at 12 weeks, and annually if the patient is taking a second-generation agent. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 › Steve B is a 43-year-old patient with bipolar disorder and a history of hypertension and high cholesterol. His body mass index (BMI) is 29. During a checkup, he tells you his psychiatrist recently started him on olanzapine. He reports that the medication is working, but he’s concerned about adverse effects, and asks whether he should be monitored for signs of diabetes.
CASE 2 › Mary F, an 83-year-old with Alzheimer’s disease and a history of stable coronary artery disease, is a resident in a long-term care facility, where staff members report that she is increasingly combative. The floor nurse says Ms. F has been striking out at the nurses’ aides who attempt to dress her and asks that you prescribe an antipsychotic to “calm her down.”
If Mr. B and Ms. F were your patients, what would you do?
In 1951, the chance discovery of an anesthetic’s calming properties was the first step in the development of the medications that came to be known as antipsychotics.1 In recent years, we have seen an expansion in both the number of antipsychotic agents on the market and the scope of their use, for conditions as varied as chronic pain, dementia, nausea and vomiting, and Tourette syndrome.
While antipsychotics often are prescribed by psychiatrists or other specialists, primary care physicians are increasingly likely to be involved in the management of patients who take them—and, at times, to prescribe antipsychotic agents themselves. We developed this guide to increase awareness of safe prescribing practices and principles guiding the initiation and management of antipsychotic agents. We start with a review of the mechanism of action of first- and second-generation antipsychotics (SGAs).

In the last decade, research has called into question whether second-generation antipsychotics really are more effective than first-generation agents
First- and second-generation agents: How they work and differ
Antipsychotics act at the level of the dopaminergic pathways in the central nervous system by blocking the D2 receptors. Action on the mesolimbic pathway is thought to be responsible for their effects on schizophrenia symptoms,2 while action at receptor sites in other dopaminergic pathways leads to common adverse effects, primarily the extrapyramidal symptoms (EPS) associated with first-generation antipsychotics (FGAs).
The distinction between first- and second-generation agents relates to SGAs’ blockage of serotonin receptors (thought to better relieve schizophrenia symptoms) and increased specificity for the mesolimbic pathway (which reduces the action on other dopamine pathways and is less likely to produce EPS).3 These differences largely accounted for the belief that SGAs were more effective and provided the rationale for their designation as atypical antipsychotics.
Are SGAs really better?
In the last decade, research has called such claims into question. Trials such as the Clinical Antipsychotic Trials of Intervention Effectiveness4 and Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia study,5 as well as a meta-analysis,6 found that SGAs as a class are no more effective than FGAs. That said, 2 SGAs—clozapine and olanzapine—were found to be superior to FGAs for the treatment of schizophrenia. The studies also raised doubts about SGAs’ advantages regarding tolerability, as the time to discontinuation due to intolerable adverse effects was similar for first- and second-generation drugs.4-6
Approved and off-label indications: A look at the evidence
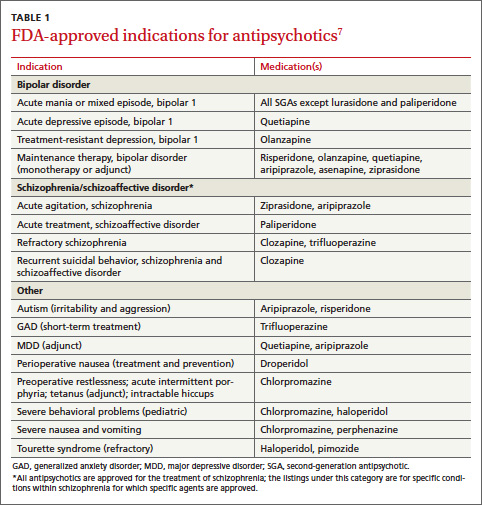
In addition to schizophrenia, many antipsychotics have US Food and Drug Administration (FDA) approval to treat various psychiatric and nonpsychiatric conditions (TABLE 1).7 Several are approved for use in bipolar disorder, 2 are approved as adjunctive treatment of major depressive disorder (MDD), and one is approved for the short-term treatment of generalized anxiety disorder (GAD). Porphyria, tetanus, and intractable hiccups are among the nonpsychiatric conditions for which some antipsychotics are approved.7
Evidence ranging from anecdotal to randomized controlled trials (RCTs) is steadily emerging about off-label uses of antipsychotics, with risperidone, quetiapine, and olanzapine foremost among them.8,9 Use of antipsychotics in the treatment of neuropsychiatric symptoms (NPS) of dementia has become particularly widespread, with off-label use of antipsychotics more prevalent in long-term care facilities than in outpatient settings.9
NPS. Antipsychotics’ efficacy in controlling dementia-related agitation, aggression, and psychosis has consistently shown a modest but statistically significant benefit. A Cochrane review found evidence that the use of risperidone and olanzapine resulted in improvements in agitation scale scores; risperidone was linked to improved scores on a psychosis scale, as well.10 A second meta-analysis showed small but statistically significant improvements in NPS with risperidone, olanzapine, and aripiprazole.8 Another study showed that nearly half (48%) of patients who had a positive response to risperidone relapsed when they stopped taking the drug.11
A rapidly aging population is expected to further increase the need for pharmacologic interventions to control NPS. Yet safety concerns about the use of antipsychotics in the elderly (more on this in a bit) call this practice into question.
Chronic pain. A 2008 Cochrane review analyzed the efficacy of antipsychotics for acute and chronic pain, pooling results of 11 studies of the treatment of conditions such as postherpetic neuralgia, tension headache, acute myocardial infarction (MI), and terminal cancer. Results from the pooled trials were described as mixed, although an overall statistically significant decrease in pain intensity was found.12
Polypharmacy. The simultaneous use of 2 or more antipsychotic agents is also increasingly prevalent,13 with levels exceeding 50% in one study of patients with schizophrenia.14 Because there is little data on the safety and efficacy of antipsychotic polypharmacy, this off-label approach should be considered only as a last resort.15
Off-label treatment of psychiatric conditions
GAD. In comparative effectiveness trials, quetiapine was found to be equal to both paroxetine and escitalopram for the treatment of GAD, with a favorable effect on symptoms 8 weeks after its initiation.8 Trials of other antipsychotics for the treatment of GAD have not demonstrated clear efficacy. Trifluoperazine is approved for GAD, as a short-term treatment.
MDD. Antipsychotics have been shown to be beneficial in the treatment of MDD, although only quetiapine and aripiprazole are approved (and only as adjunctive treatment). Evidence supports the use of both agents, as well as risperidone, as augmentation to selective serotonin reuptake inhibitors (SSRIs), and in pooled results from 5 placebo-controlled trials, quetiapine was found to be effective as monotherapy for MDD.9
Obsessive-compulsive disorder (OCD). Compared with placebo, risperidone showed a 4-fold increase in the likelihood of a favorable response (number needed to treat [NNT]=4) in patients with OCD,8 but the drug remains off-label for this purpose.
Posttraumatic stress disorder (PTSD). A meta-analysis of 7 studies demonstrated risperidone’s efficacy in the treatment of combat-related PTSD.9 In a large Veterans Administration study of patients with combat-related PTSD resistant to treatment with SSRIs, however, risperidone showed no benefit after 6 months of therapy.16 Antipsychotics have not been found beneficial for substance abuse, eating disorders, or insomnia.9
Identifying risk factos, monitoring for adverse effects
While FGAs carry an increased risk of EPS, SGAs increase the risk of obesity, hyperlipidemia, hypertension, and diabetes mellitus. The average life expectancy of patients with schizophrenia is 2 to 3 decades lower than that of age-matched controls,17 a finding largely attributed to the increased rate of cardiovascular disease. While this can be partly explained by differences in lifestyle and access to care, the metabolic effects of SGAs are a likely contributing factor.
Because of the adverse effects of FGAs and SGAs, the American Diabetes Association and American Psychiatric Association jointly issued guidelines addressing both the type and optimal frequency of monitoring for patients on antipsychotics (TABLE 2).18,19 Following them is critical, as both the initiation of an antipsychotic agent and any change in regimen can lead to the development—or exacerbation—of a number of diseases.
Before initiating antipsychotic therapy—or the first time you see a patient like Mr. B, whose care you will be monitoring—a thorough assessment of risk factors is needed. Foremost among them are overweight or obesity, insulin resistance or diabetes, a history of heart disease, and EPS.
In some cases, preexisting conditions and the potential harm of a specific drug must be weighed in determining which antipsychotic to prescribe. When adverse effects develop after drug therapy has been initiated, decisions about further actions should be based on both the degree of the unfavorable response and the availability of other treatments—and made, as appropriate, in consultation with the specialist who prescribed the drug.
CASE 1 › You tell Mr. B that metabolic side effects like weight gain, impaired glucose tolerance, and increased low-density lipoprotein cholesterol are common with SGAs like the one he is taking, and that you will monitor his fasting glucose levels to evaluate his risk for developing diabetes—starting with this visit. (Olanzapine, the drug he is taking, is 4 times more likely than an FGA to lead to diabetes.18)
You talk to him, too, about the importance of weight control and note that if his BMI increases by ≥1 point you will refer him to a nutritionist and recommend a structured exercise program. Finally, you schedule an appointment in 3 months.
Risks associated with older age and dementia
In 2010, there were 84,842 visits to US emergency departments (EDs) due to adverse drug events involving antipsychotic agents—a 110% increase since 2005. Nearly 30% of these ED visits involved patients 65 years or older.20
Among patients with dementia, use of antipsychotics has been found to dramatically increase the risk of stroke (rate ratio, 3.26 for FGAs and 5.86 for SGAs).21 The risk was greatest in the first 35 days of treatment, but persisted throughout the 175-day study period.
The rate of MI also was elevated in dementia patients (hazard ratio of 2.19 for the first 30 days of treatment, then falling to 1.15 for the first year).22 The risk of pulmonary embolism and deep vein thrombosis also rose for patients who had been on antipsychotics during the previous 24 months (odds ratio=1.32), with the highest risk within the first 90 days of treatment.23
Risk of death varies with agent and dose. Multiple studies have shown that the mortality risk associated with antipsychotics varies greatly among individual drugs, with haloperidol carrying the highest risk and quetiapine the lowest.24-26 The hazard ratio for death within the first 30 days was 3.2 for haloperidol, 1.6 for risperidone, and 1.5 for olanzapine; quetiapine had no statistically significant increase. The increased mortality risk was statistically significant only at higher doses.24
The FDA weighs in
Evidence of the elevated risk of death led the FDA to require black-box warnings on SGAs (in 2005)27 and FGAs (in 2008),28 stating that “antipsychotics are not indicated for the treatment of dementia-related psychosis.”28 More recently (in 2012), the American Geriatrics Society (AGS) published a guide on the management of NPS in patients with dementia.29 In it, the AGS acknowledges that despite FDA warnings, antipsychotics may be necessary for the treatment of NPS.
The AGS stresses the importance of nonpharmacologic interventions (eg, positive reinforcement, orientation to time and place, music, light exercise, pet therapy) as a first-line approach. If these measures fail and antipsychotics are necessary, the AGS calls for obtaining informed consent from a family member, using the lowest effective dose, and regularly attempting to wean the patient off the antipsychotic as the standard of care.28
CASE 2 › New or worsening aggressive behavior in an elderly patient with dementia requires a prompt assessment. You start with a complete medical evaluation of Ms. F, ruling out common causes of agitation such as infection, pain, constipation, and an adverse reaction to medication.
You also ask about the incidents of aggression: Does the same aide dress Ms. F daily? Does the aide introduce herself and explain what she’s about to do before attempting to dress the patient?
Next, you recommend nonpharmacologic therapies, such as calming music, participation in group activities, and pet therapy. You tell the floor nurse that if these measures fail and Ms. F’s threatening behavior continues, an antipsychotic may be considered.
Guard against abuse of antipsychotics
As antipsychotic use increases, so, too, does misuse and abuse, particularly of quetiapine. The drug has a reported street value of $3 to $8 for a 25- to 100-mg dose and is known as “quell,” “Susie-Q,” “and “baby heroin”; “Q-ball” is the name used for a combination of cocaine and quetiapine.30,31
The Drug Abuse Warning Network reported a 115% increase in ED visits related to the misuse or abuse of pharmaceuticals between 2004 and 2010.32 In 2010, 57,199 drug abuse cases—including 28,618 suicide attempts—were linked to antipsychotics.20

To optimize the benefit of antipsychotics and minimize the likelihood of abuse, ensure that every patient taking them has a clearly documented indication for an antipsychotic and a single responsible prescriber of the antipsychotic, often a psychiatrist. Your responsibilities: Schedule visits for monitoring, do a medication review to identify potential drug-drug interactions, and assess efficacy, all on a regular basis.
CASE 1 › At Mr. B’s next visit, you retest his fasting glucose (which is now 105 mg/dL) and recheck his BMI, which has climbed to 30. You tell him you will speak with his psychiatrist about his weight gain and your concern about the development of insulin resistance.
Meanwhile, you refer the patient to a nutritionist and encourage a healthy lifestyle. Because the medication has been effective, you schedule a follow-up visit in 6 weeks to see if the lifestyle interventions have been successful before consulting with the patient’s psychiatrist about a change in medication.
CASE 2 › When you return to the long-term care facility one week later, you find that Ms. F’s NPS have not abated. You realize an antipsychotic agent may be needed. Because she has a history of heart disease, however, she has a higher risk for cardiovascular events.
You meet with her son to review the benefits and risks of antipsychotic therapy, explaining that risperidone is a reasonable agent and that a low starting dose (0.25-0.5 mg) will reduce the risk. You obtain his informed consent, document your treatment goals—a decrease in threatening behavior and the ability of the staff to work with Ms. F to get her up and out of bed—and establish a plan to review in 2 weeks.
CORRESPONDENCE
Daniel DeJoseph, MD, Drexel Family Medicine, 3401 Market Street, Suite 105-B, Philadelphia, PA 19104; [email protected]
1. Shen WW. A history of antipsychotic drug development. Compr Psychiatry. 1999;40:407-414.
2. Miller R. Mechanism of action of antipsychotic drugs of different classes, refractoriness to therapeutic effects of classical neuroleptics, and individual variation in sensitivity to their actions. Curr Neuropharmacol. 2009;7:302-314.
3. Seeman P. Atypical antipsychotics: mechanism of action. Can J Psychiatry. 2002;47:27-38.
4. Lieberman JA, Stroup TS, McEvoy JP, et al; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209-1223.
5. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of the effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63:1079-1087.
6. Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373:31-41.
7. Christian R, Saavedra L, Gaynes BN, et al. Future research needs for first- and second-generation antipsychotics for children and young adults [Internet]. Agency for Healthcare Research and Quality. 2012:12-EHC042-EF.
8. Maher AR, Maglione M, Bagley S, et al. Efficacy and comparative effectiveness of atypical antipsychotic medications for off-label uses in adults: a systematic review and meta-analysis. JAMA. 2011;306:1359-1369.
9. Maglione M, Maher AR, Hu J, et al. Off-label use of atypical antipsychotics: An update [Internet]. Agency for Healthcare Research and Quality. 2011:11-EHC087-EF.
10. Ballard CG, Waite J. Atypical antipsychotics for aggression and psychosis in Alzheimer’s disease. Cochrane Database Syst Rev. 2006;(1):CD003476.
11. Devanand DP, Mintzer J, Schultz SK, et al. Relapse risk after discontinuation of risperidone in Alzheimer’s disease. N Engl J Med. 2012;367:1497-1507.
12. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. Cochrane Database Syst Rev. 2008;(4):CD004844.
13. Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26-36.
14. Faries D, Ascher-Svanum H, Zhu B, et al. Antipsychotic monotherapy and polypharmacy in the naturalistic treatment of schizophrenia with atypical antipsychotics. BMC Psychiatry. 2005;5:26.
15. Ballon J, Stroup TS. Polypharmacy for schizophrenia. Curr Opin Psychiatry. 2013;26:208-213.
16. Krystal JH, Rosenheck RA, Cramer JA, et al; Veterans Affairs Cooperative Study No. 504 Group. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: a randomized trial. JAMA. 2011;306:493-502.
17. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: National Academy of Sciences; 2008.
18. Marder SR, Essock SM, Miller AL, et al. Physical health monitoring of patients with schizophrenia. Am J Psychiatry. 2004;161:1334-1349.
19. Barrett E, Blonde L, Clement S, et al. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
20. Drug Abuse Warning Network, 2010: National Estimates of Drug-Related Emergency Department Visits. HHS Publication No. (SMA) 12-4733, DAWN Series D-38. Substance Abuse and Mental Health Services Administration Web site. Available at: http://www.samhsa.gov/data/2k13/DAWN2k10ED/DAWN2k10ED.htm. Accessed May 1, 2013.
21. Douglas IJ, Smeeth L. Exposure to antipsychotics and risk of stroke: self controlled case series study. BMJ. 2008;337:a1227.
22. Pariente A, Fourrier-Réglat A, Ducruet T, et al. Antipsychotic use and myocardial infarction in older patients with treated dementia. Arch Intern Med. 2012;172:648-653.
23. Parker C, Coupland C, Hippisley-Cox J. Antipsychotic drugs and risk of venous thromboembolism: nested case-control study. BMJ. 2010;341:c4245.
24. Rossom RC, Rector TS, Lederle FA, et al. Are all commonly prescribed antipsychotics associated with greater mortality in elderly male veterans with dementia? J Am Geriatr Soc. 2010;58:1027-1034.
25. Kales HC, Kim HM, Zivin K, et al. Risk of mortality among individual antipsychotics in patients with dementia. Am J Psychiatry. 2012;169:71-79.
26. Huybrechts KF, Gerhard T, Crystal S, et al. Differential risk of death in older residents in nursing homes prescribed specific antipsychotic drugs: population based cohort study. BMJ. 2012;344:e977.
27. US Food and Drug Public Health Advisory: Deaths with antipsychotics in elderly patients with behavioral disturbances. US Food and Drug Administration Web site Available at: http://1.usa.gov/1plsxPk. Accessed February 5, 2014.
28. Information for healthcare professionals: conventional antipsychotics. US Food and Drug Administration Web site. Available at: http://www.fda.gov/drugs/drugsafety/postmarketdrugsafetyinformationforpatientsandproviders/ucm124830.htm. Accessed February 5, 2014.
29. Guide to the management of psychotic disorders and neuropsychiatric symptoms of dementia in older adults. American Geriatric Society Web site. Available at: http://dementia.americangeriatrics.org/GeriPsych_index.php. Accessed April 15, 2013.
30. Bogart GT, Ott CA. Abuse of second-generation antipsychotics: What prescribers need to know. Curr Psychiatr. 2011;10:77-79.
31. Tarosoff G, Osti K. Black-market value of antipsychotics, antidepressants, and hypnotics in Las Vegas, Nevada. Am J Psychiatry. 2007;164:350.
32. Highlights of the 2010 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality Web site. Available at: http://www.samhsa.gov/data/2k12/DAWN096/SR096EDHighlights2010.htm. Accessed May 1, 2013.
› Evaluate patients for movement disorders before initiating or adjusting antipsychotic therapy, then weekly until the dose is stabilized. A
› Use nonpharmacologic interventions—eg, positive reinforcement, music, light exercise—as first-line therapy for neuropsychiatric symptoms of dementia; consider antipsychotic therapy only if they fail. A
› Obtain a fasting glucose level before initiating or adjusting antipsychotic therapy, then at 12 weeks, and annually if the patient is taking a second-generation agent. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 › Steve B is a 43-year-old patient with bipolar disorder and a history of hypertension and high cholesterol. His body mass index (BMI) is 29. During a checkup, he tells you his psychiatrist recently started him on olanzapine. He reports that the medication is working, but he’s concerned about adverse effects, and asks whether he should be monitored for signs of diabetes.
CASE 2 › Mary F, an 83-year-old with Alzheimer’s disease and a history of stable coronary artery disease, is a resident in a long-term care facility, where staff members report that she is increasingly combative. The floor nurse says Ms. F has been striking out at the nurses’ aides who attempt to dress her and asks that you prescribe an antipsychotic to “calm her down.”
If Mr. B and Ms. F were your patients, what would you do?
In 1951, the chance discovery of an anesthetic’s calming properties was the first step in the development of the medications that came to be known as antipsychotics.1 In recent years, we have seen an expansion in both the number of antipsychotic agents on the market and the scope of their use, for conditions as varied as chronic pain, dementia, nausea and vomiting, and Tourette syndrome.
While antipsychotics often are prescribed by psychiatrists or other specialists, primary care physicians are increasingly likely to be involved in the management of patients who take them—and, at times, to prescribe antipsychotic agents themselves. We developed this guide to increase awareness of safe prescribing practices and principles guiding the initiation and management of antipsychotic agents. We start with a review of the mechanism of action of first- and second-generation antipsychotics (SGAs).
In the last decade, research has called into question whether second-generation antipsychotics really are more effective than first-generation agents
First- and second-generation agents: How they work and differ
Antipsychotics act at the level of the dopaminergic pathways in the central nervous system by blocking the D2 receptors. Action on the mesolimbic pathway is thought to be responsible for their effects on schizophrenia symptoms,2 while action at receptor sites in other dopaminergic pathways leads to common adverse effects, primarily the extrapyramidal symptoms (EPS) associated with first-generation antipsychotics (FGAs).
The distinction between first- and second-generation agents relates to SGAs’ blockage of serotonin receptors (thought to better relieve schizophrenia symptoms) and increased specificity for the mesolimbic pathway (which reduces the action on other dopamine pathways and is less likely to produce EPS).3 These differences largely accounted for the belief that SGAs were more effective and provided the rationale for their designation as atypical antipsychotics.
Are SGAs really better?
In the last decade, research has called such claims into question. Trials such as the Clinical Antipsychotic Trials of Intervention Effectiveness4 and Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia study,5 as well as a meta-analysis,6 found that SGAs as a class are no more effective than FGAs. That said, 2 SGAs—clozapine and olanzapine—were found to be superior to FGAs for the treatment of schizophrenia. The studies also raised doubts about SGAs’ advantages regarding tolerability, as the time to discontinuation due to intolerable adverse effects was similar for first- and second-generation drugs.4-6
Approved and off-label indications: A look at the evidence
In addition to schizophrenia, many antipsychotics have US Food and Drug Administration (FDA) approval to treat various psychiatric and nonpsychiatric conditions (TABLE 1).7 Several are approved for use in bipolar disorder, 2 are approved as adjunctive treatment of major depressive disorder (MDD), and one is approved for the short-term treatment of generalized anxiety disorder (GAD). Porphyria, tetanus, and intractable hiccups are among the nonpsychiatric conditions for which some antipsychotics are approved.7
Evidence ranging from anecdotal to randomized controlled trials (RCTs) is steadily emerging about off-label uses of antipsychotics, with risperidone, quetiapine, and olanzapine foremost among them.8,9 Use of antipsychotics in the treatment of neuropsychiatric symptoms (NPS) of dementia has become particularly widespread, with off-label use of antipsychotics more prevalent in long-term care facilities than in outpatient settings.9
NPS. Antipsychotics’ efficacy in controlling dementia-related agitation, aggression, and psychosis has consistently shown a modest but statistically significant benefit. A Cochrane review found evidence that the use of risperidone and olanzapine resulted in improvements in agitation scale scores; risperidone was linked to improved scores on a psychosis scale, as well.10 A second meta-analysis showed small but statistically significant improvements in NPS with risperidone, olanzapine, and aripiprazole.8 Another study showed that nearly half (48%) of patients who had a positive response to risperidone relapsed when they stopped taking the drug.11
A rapidly aging population is expected to further increase the need for pharmacologic interventions to control NPS. Yet safety concerns about the use of antipsychotics in the elderly (more on this in a bit) call this practice into question.
Chronic pain. A 2008 Cochrane review analyzed the efficacy of antipsychotics for acute and chronic pain, pooling results of 11 studies of the treatment of conditions such as postherpetic neuralgia, tension headache, acute myocardial infarction (MI), and terminal cancer. Results from the pooled trials were described as mixed, although an overall statistically significant decrease in pain intensity was found.12
Polypharmacy. The simultaneous use of 2 or more antipsychotic agents is also increasingly prevalent,13 with levels exceeding 50% in one study of patients with schizophrenia.14 Because there is little data on the safety and efficacy of antipsychotic polypharmacy, this off-label approach should be considered only as a last resort.15
Off-label treatment of psychiatric conditions
GAD. In comparative effectiveness trials, quetiapine was found to be equal to both paroxetine and escitalopram for the treatment of GAD, with a favorable effect on symptoms 8 weeks after its initiation.8 Trials of other antipsychotics for the treatment of GAD have not demonstrated clear efficacy. Trifluoperazine is approved for GAD, as a short-term treatment.
MDD. Antipsychotics have been shown to be beneficial in the treatment of MDD, although only quetiapine and aripiprazole are approved (and only as adjunctive treatment). Evidence supports the use of both agents, as well as risperidone, as augmentation to selective serotonin reuptake inhibitors (SSRIs), and in pooled results from 5 placebo-controlled trials, quetiapine was found to be effective as monotherapy for MDD.9
Obsessive-compulsive disorder (OCD). Compared with placebo, risperidone showed a 4-fold increase in the likelihood of a favorable response (number needed to treat [NNT]=4) in patients with OCD,8 but the drug remains off-label for this purpose.
Posttraumatic stress disorder (PTSD). A meta-analysis of 7 studies demonstrated risperidone’s efficacy in the treatment of combat-related PTSD.9 In a large Veterans Administration study of patients with combat-related PTSD resistant to treatment with SSRIs, however, risperidone showed no benefit after 6 months of therapy.16 Antipsychotics have not been found beneficial for substance abuse, eating disorders, or insomnia.9
Identifying risk factos, monitoring for adverse effects
While FGAs carry an increased risk of EPS, SGAs increase the risk of obesity, hyperlipidemia, hypertension, and diabetes mellitus. The average life expectancy of patients with schizophrenia is 2 to 3 decades lower than that of age-matched controls,17 a finding largely attributed to the increased rate of cardiovascular disease. While this can be partly explained by differences in lifestyle and access to care, the metabolic effects of SGAs are a likely contributing factor.
Because of the adverse effects of FGAs and SGAs, the American Diabetes Association and American Psychiatric Association jointly issued guidelines addressing both the type and optimal frequency of monitoring for patients on antipsychotics (TABLE 2).18,19 Following them is critical, as both the initiation of an antipsychotic agent and any change in regimen can lead to the development—or exacerbation—of a number of diseases.
Before initiating antipsychotic therapy—or the first time you see a patient like Mr. B, whose care you will be monitoring—a thorough assessment of risk factors is needed. Foremost among them are overweight or obesity, insulin resistance or diabetes, a history of heart disease, and EPS.
In some cases, preexisting conditions and the potential harm of a specific drug must be weighed in determining which antipsychotic to prescribe. When adverse effects develop after drug therapy has been initiated, decisions about further actions should be based on both the degree of the unfavorable response and the availability of other treatments—and made, as appropriate, in consultation with the specialist who prescribed the drug.
CASE 1 › You tell Mr. B that metabolic side effects like weight gain, impaired glucose tolerance, and increased low-density lipoprotein cholesterol are common with SGAs like the one he is taking, and that you will monitor his fasting glucose levels to evaluate his risk for developing diabetes—starting with this visit. (Olanzapine, the drug he is taking, is 4 times more likely than an FGA to lead to diabetes.18)
You talk to him, too, about the importance of weight control and note that if his BMI increases by ≥1 point you will refer him to a nutritionist and recommend a structured exercise program. Finally, you schedule an appointment in 3 months.
Risks associated with older age and dementia
In 2010, there were 84,842 visits to US emergency departments (EDs) due to adverse drug events involving antipsychotic agents—a 110% increase since 2005. Nearly 30% of these ED visits involved patients 65 years or older.20
Among patients with dementia, use of antipsychotics has been found to dramatically increase the risk of stroke (rate ratio, 3.26 for FGAs and 5.86 for SGAs).21 The risk was greatest in the first 35 days of treatment, but persisted throughout the 175-day study period.
The rate of MI also was elevated in dementia patients (hazard ratio of 2.19 for the first 30 days of treatment, then falling to 1.15 for the first year).22 The risk of pulmonary embolism and deep vein thrombosis also rose for patients who had been on antipsychotics during the previous 24 months (odds ratio=1.32), with the highest risk within the first 90 days of treatment.23
Risk of death varies with agent and dose. Multiple studies have shown that the mortality risk associated with antipsychotics varies greatly among individual drugs, with haloperidol carrying the highest risk and quetiapine the lowest.24-26 The hazard ratio for death within the first 30 days was 3.2 for haloperidol, 1.6 for risperidone, and 1.5 for olanzapine; quetiapine had no statistically significant increase. The increased mortality risk was statistically significant only at higher doses.24
The FDA weighs in
Evidence of the elevated risk of death led the FDA to require black-box warnings on SGAs (in 2005)27 and FGAs (in 2008),28 stating that “antipsychotics are not indicated for the treatment of dementia-related psychosis.”28 More recently (in 2012), the American Geriatrics Society (AGS) published a guide on the management of NPS in patients with dementia.29 In it, the AGS acknowledges that despite FDA warnings, antipsychotics may be necessary for the treatment of NPS.
The AGS stresses the importance of nonpharmacologic interventions (eg, positive reinforcement, orientation to time and place, music, light exercise, pet therapy) as a first-line approach. If these measures fail and antipsychotics are necessary, the AGS calls for obtaining informed consent from a family member, using the lowest effective dose, and regularly attempting to wean the patient off the antipsychotic as the standard of care.28
CASE 2 › New or worsening aggressive behavior in an elderly patient with dementia requires a prompt assessment. You start with a complete medical evaluation of Ms. F, ruling out common causes of agitation such as infection, pain, constipation, and an adverse reaction to medication.
You also ask about the incidents of aggression: Does the same aide dress Ms. F daily? Does the aide introduce herself and explain what she’s about to do before attempting to dress the patient?
Next, you recommend nonpharmacologic therapies, such as calming music, participation in group activities, and pet therapy. You tell the floor nurse that if these measures fail and Ms. F’s threatening behavior continues, an antipsychotic may be considered.
Guard against abuse of antipsychotics
As antipsychotic use increases, so, too, does misuse and abuse, particularly of quetiapine. The drug has a reported street value of $3 to $8 for a 25- to 100-mg dose and is known as “quell,” “Susie-Q,” “and “baby heroin”; “Q-ball” is the name used for a combination of cocaine and quetiapine.30,31
The Drug Abuse Warning Network reported a 115% increase in ED visits related to the misuse or abuse of pharmaceuticals between 2004 and 2010.32 In 2010, 57,199 drug abuse cases—including 28,618 suicide attempts—were linked to antipsychotics.20
To optimize the benefit of antipsychotics and minimize the likelihood of abuse, ensure that every patient taking them has a clearly documented indication for an antipsychotic and a single responsible prescriber of the antipsychotic, often a psychiatrist. Your responsibilities: Schedule visits for monitoring, do a medication review to identify potential drug-drug interactions, and assess efficacy, all on a regular basis.
CASE 1 › At Mr. B’s next visit, you retest his fasting glucose (which is now 105 mg/dL) and recheck his BMI, which has climbed to 30. You tell him you will speak with his psychiatrist about his weight gain and your concern about the development of insulin resistance.
Meanwhile, you refer the patient to a nutritionist and encourage a healthy lifestyle. Because the medication has been effective, you schedule a follow-up visit in 6 weeks to see if the lifestyle interventions have been successful before consulting with the patient’s psychiatrist about a change in medication.
CASE 2 › When you return to the long-term care facility one week later, you find that Ms. F’s NPS have not abated. You realize an antipsychotic agent may be needed. Because she has a history of heart disease, however, she has a higher risk for cardiovascular events.
You meet with her son to review the benefits and risks of antipsychotic therapy, explaining that risperidone is a reasonable agent and that a low starting dose (0.25-0.5 mg) will reduce the risk. You obtain his informed consent, document your treatment goals—a decrease in threatening behavior and the ability of the staff to work with Ms. F to get her up and out of bed—and establish a plan to review in 2 weeks.
CORRESPONDENCE
Daniel DeJoseph, MD, Drexel Family Medicine, 3401 Market Street, Suite 105-B, Philadelphia, PA 19104; [email protected]
› Evaluate patients for movement disorders before initiating or adjusting antipsychotic therapy, then weekly until the dose is stabilized. A
› Use nonpharmacologic interventions—eg, positive reinforcement, music, light exercise—as first-line therapy for neuropsychiatric symptoms of dementia; consider antipsychotic therapy only if they fail. A
› Obtain a fasting glucose level before initiating or adjusting antipsychotic therapy, then at 12 weeks, and annually if the patient is taking a second-generation agent. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 › Steve B is a 43-year-old patient with bipolar disorder and a history of hypertension and high cholesterol. His body mass index (BMI) is 29. During a checkup, he tells you his psychiatrist recently started him on olanzapine. He reports that the medication is working, but he’s concerned about adverse effects, and asks whether he should be monitored for signs of diabetes.
CASE 2 › Mary F, an 83-year-old with Alzheimer’s disease and a history of stable coronary artery disease, is a resident in a long-term care facility, where staff members report that she is increasingly combative. The floor nurse says Ms. F has been striking out at the nurses’ aides who attempt to dress her and asks that you prescribe an antipsychotic to “calm her down.”
If Mr. B and Ms. F were your patients, what would you do?
In 1951, the chance discovery of an anesthetic’s calming properties was the first step in the development of the medications that came to be known as antipsychotics.1 In recent years, we have seen an expansion in both the number of antipsychotic agents on the market and the scope of their use, for conditions as varied as chronic pain, dementia, nausea and vomiting, and Tourette syndrome.
While antipsychotics often are prescribed by psychiatrists or other specialists, primary care physicians are increasingly likely to be involved in the management of patients who take them—and, at times, to prescribe antipsychotic agents themselves. We developed this guide to increase awareness of safe prescribing practices and principles guiding the initiation and management of antipsychotic agents. We start with a review of the mechanism of action of first- and second-generation antipsychotics (SGAs).
In the last decade, research has called into question whether second-generation antipsychotics really are more effective than first-generation agents
First- and second-generation agents: How they work and differ
Antipsychotics act at the level of the dopaminergic pathways in the central nervous system by blocking the D2 receptors. Action on the mesolimbic pathway is thought to be responsible for their effects on schizophrenia symptoms,2 while action at receptor sites in other dopaminergic pathways leads to common adverse effects, primarily the extrapyramidal symptoms (EPS) associated with first-generation antipsychotics (FGAs).
The distinction between first- and second-generation agents relates to SGAs’ blockage of serotonin receptors (thought to better relieve schizophrenia symptoms) and increased specificity for the mesolimbic pathway (which reduces the action on other dopamine pathways and is less likely to produce EPS).3 These differences largely accounted for the belief that SGAs were more effective and provided the rationale for their designation as atypical antipsychotics.
Are SGAs really better?
In the last decade, research has called such claims into question. Trials such as the Clinical Antipsychotic Trials of Intervention Effectiveness4 and Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia study,5 as well as a meta-analysis,6 found that SGAs as a class are no more effective than FGAs. That said, 2 SGAs—clozapine and olanzapine—were found to be superior to FGAs for the treatment of schizophrenia. The studies also raised doubts about SGAs’ advantages regarding tolerability, as the time to discontinuation due to intolerable adverse effects was similar for first- and second-generation drugs.4-6
Approved and off-label indications: A look at the evidence
In addition to schizophrenia, many antipsychotics have US Food and Drug Administration (FDA) approval to treat various psychiatric and nonpsychiatric conditions (TABLE 1).7 Several are approved for use in bipolar disorder, 2 are approved as adjunctive treatment of major depressive disorder (MDD), and one is approved for the short-term treatment of generalized anxiety disorder (GAD). Porphyria, tetanus, and intractable hiccups are among the nonpsychiatric conditions for which some antipsychotics are approved.7
Evidence ranging from anecdotal to randomized controlled trials (RCTs) is steadily emerging about off-label uses of antipsychotics, with risperidone, quetiapine, and olanzapine foremost among them.8,9 Use of antipsychotics in the treatment of neuropsychiatric symptoms (NPS) of dementia has become particularly widespread, with off-label use of antipsychotics more prevalent in long-term care facilities than in outpatient settings.9
NPS. Antipsychotics’ efficacy in controlling dementia-related agitation, aggression, and psychosis has consistently shown a modest but statistically significant benefit. A Cochrane review found evidence that the use of risperidone and olanzapine resulted in improvements in agitation scale scores; risperidone was linked to improved scores on a psychosis scale, as well.10 A second meta-analysis showed small but statistically significant improvements in NPS with risperidone, olanzapine, and aripiprazole.8 Another study showed that nearly half (48%) of patients who had a positive response to risperidone relapsed when they stopped taking the drug.11
A rapidly aging population is expected to further increase the need for pharmacologic interventions to control NPS. Yet safety concerns about the use of antipsychotics in the elderly (more on this in a bit) call this practice into question.
Chronic pain. A 2008 Cochrane review analyzed the efficacy of antipsychotics for acute and chronic pain, pooling results of 11 studies of the treatment of conditions such as postherpetic neuralgia, tension headache, acute myocardial infarction (MI), and terminal cancer. Results from the pooled trials were described as mixed, although an overall statistically significant decrease in pain intensity was found.12
Polypharmacy. The simultaneous use of 2 or more antipsychotic agents is also increasingly prevalent,13 with levels exceeding 50% in one study of patients with schizophrenia.14 Because there is little data on the safety and efficacy of antipsychotic polypharmacy, this off-label approach should be considered only as a last resort.15
Off-label treatment of psychiatric conditions
GAD. In comparative effectiveness trials, quetiapine was found to be equal to both paroxetine and escitalopram for the treatment of GAD, with a favorable effect on symptoms 8 weeks after its initiation.8 Trials of other antipsychotics for the treatment of GAD have not demonstrated clear efficacy. Trifluoperazine is approved for GAD, as a short-term treatment.
MDD. Antipsychotics have been shown to be beneficial in the treatment of MDD, although only quetiapine and aripiprazole are approved (and only as adjunctive treatment). Evidence supports the use of both agents, as well as risperidone, as augmentation to selective serotonin reuptake inhibitors (SSRIs), and in pooled results from 5 placebo-controlled trials, quetiapine was found to be effective as monotherapy for MDD.9
Obsessive-compulsive disorder (OCD). Compared with placebo, risperidone showed a 4-fold increase in the likelihood of a favorable response (number needed to treat [NNT]=4) in patients with OCD,8 but the drug remains off-label for this purpose.
Posttraumatic stress disorder (PTSD). A meta-analysis of 7 studies demonstrated risperidone’s efficacy in the treatment of combat-related PTSD.9 In a large Veterans Administration study of patients with combat-related PTSD resistant to treatment with SSRIs, however, risperidone showed no benefit after 6 months of therapy.16 Antipsychotics have not been found beneficial for substance abuse, eating disorders, or insomnia.9
Identifying risk factos, monitoring for adverse effects
While FGAs carry an increased risk of EPS, SGAs increase the risk of obesity, hyperlipidemia, hypertension, and diabetes mellitus. The average life expectancy of patients with schizophrenia is 2 to 3 decades lower than that of age-matched controls,17 a finding largely attributed to the increased rate of cardiovascular disease. While this can be partly explained by differences in lifestyle and access to care, the metabolic effects of SGAs are a likely contributing factor.
Because of the adverse effects of FGAs and SGAs, the American Diabetes Association and American Psychiatric Association jointly issued guidelines addressing both the type and optimal frequency of monitoring for patients on antipsychotics (TABLE 2).18,19 Following them is critical, as both the initiation of an antipsychotic agent and any change in regimen can lead to the development—or exacerbation—of a number of diseases.
Before initiating antipsychotic therapy—or the first time you see a patient like Mr. B, whose care you will be monitoring—a thorough assessment of risk factors is needed. Foremost among them are overweight or obesity, insulin resistance or diabetes, a history of heart disease, and EPS.
In some cases, preexisting conditions and the potential harm of a specific drug must be weighed in determining which antipsychotic to prescribe. When adverse effects develop after drug therapy has been initiated, decisions about further actions should be based on both the degree of the unfavorable response and the availability of other treatments—and made, as appropriate, in consultation with the specialist who prescribed the drug.
CASE 1 › You tell Mr. B that metabolic side effects like weight gain, impaired glucose tolerance, and increased low-density lipoprotein cholesterol are common with SGAs like the one he is taking, and that you will monitor his fasting glucose levels to evaluate his risk for developing diabetes—starting with this visit. (Olanzapine, the drug he is taking, is 4 times more likely than an FGA to lead to diabetes.18)
You talk to him, too, about the importance of weight control and note that if his BMI increases by ≥1 point you will refer him to a nutritionist and recommend a structured exercise program. Finally, you schedule an appointment in 3 months.
Risks associated with older age and dementia
In 2010, there were 84,842 visits to US emergency departments (EDs) due to adverse drug events involving antipsychotic agents—a 110% increase since 2005. Nearly 30% of these ED visits involved patients 65 years or older.20
Among patients with dementia, use of antipsychotics has been found to dramatically increase the risk of stroke (rate ratio, 3.26 for FGAs and 5.86 for SGAs).21 The risk was greatest in the first 35 days of treatment, but persisted throughout the 175-day study period.
The rate of MI also was elevated in dementia patients (hazard ratio of 2.19 for the first 30 days of treatment, then falling to 1.15 for the first year).22 The risk of pulmonary embolism and deep vein thrombosis also rose for patients who had been on antipsychotics during the previous 24 months (odds ratio=1.32), with the highest risk within the first 90 days of treatment.23
Risk of death varies with agent and dose. Multiple studies have shown that the mortality risk associated with antipsychotics varies greatly among individual drugs, with haloperidol carrying the highest risk and quetiapine the lowest.24-26 The hazard ratio for death within the first 30 days was 3.2 for haloperidol, 1.6 for risperidone, and 1.5 for olanzapine; quetiapine had no statistically significant increase. The increased mortality risk was statistically significant only at higher doses.24
The FDA weighs in
Evidence of the elevated risk of death led the FDA to require black-box warnings on SGAs (in 2005)27 and FGAs (in 2008),28 stating that “antipsychotics are not indicated for the treatment of dementia-related psychosis.”28 More recently (in 2012), the American Geriatrics Society (AGS) published a guide on the management of NPS in patients with dementia.29 In it, the AGS acknowledges that despite FDA warnings, antipsychotics may be necessary for the treatment of NPS.
The AGS stresses the importance of nonpharmacologic interventions (eg, positive reinforcement, orientation to time and place, music, light exercise, pet therapy) as a first-line approach. If these measures fail and antipsychotics are necessary, the AGS calls for obtaining informed consent from a family member, using the lowest effective dose, and regularly attempting to wean the patient off the antipsychotic as the standard of care.28
CASE 2 › New or worsening aggressive behavior in an elderly patient with dementia requires a prompt assessment. You start with a complete medical evaluation of Ms. F, ruling out common causes of agitation such as infection, pain, constipation, and an adverse reaction to medication.
You also ask about the incidents of aggression: Does the same aide dress Ms. F daily? Does the aide introduce herself and explain what she’s about to do before attempting to dress the patient?
Next, you recommend nonpharmacologic therapies, such as calming music, participation in group activities, and pet therapy. You tell the floor nurse that if these measures fail and Ms. F’s threatening behavior continues, an antipsychotic may be considered.
Guard against abuse of antipsychotics
As antipsychotic use increases, so, too, does misuse and abuse, particularly of quetiapine. The drug has a reported street value of $3 to $8 for a 25- to 100-mg dose and is known as “quell,” “Susie-Q,” “and “baby heroin”; “Q-ball” is the name used for a combination of cocaine and quetiapine.30,31
The Drug Abuse Warning Network reported a 115% increase in ED visits related to the misuse or abuse of pharmaceuticals between 2004 and 2010.32 In 2010, 57,199 drug abuse cases—including 28,618 suicide attempts—were linked to antipsychotics.20
To optimize the benefit of antipsychotics and minimize the likelihood of abuse, ensure that every patient taking them has a clearly documented indication for an antipsychotic and a single responsible prescriber of the antipsychotic, often a psychiatrist. Your responsibilities: Schedule visits for monitoring, do a medication review to identify potential drug-drug interactions, and assess efficacy, all on a regular basis.
CASE 1 › At Mr. B’s next visit, you retest his fasting glucose (which is now 105 mg/dL) and recheck his BMI, which has climbed to 30. You tell him you will speak with his psychiatrist about his weight gain and your concern about the development of insulin resistance.
Meanwhile, you refer the patient to a nutritionist and encourage a healthy lifestyle. Because the medication has been effective, you schedule a follow-up visit in 6 weeks to see if the lifestyle interventions have been successful before consulting with the patient’s psychiatrist about a change in medication.
CASE 2 › When you return to the long-term care facility one week later, you find that Ms. F’s NPS have not abated. You realize an antipsychotic agent may be needed. Because she has a history of heart disease, however, she has a higher risk for cardiovascular events.
You meet with her son to review the benefits and risks of antipsychotic therapy, explaining that risperidone is a reasonable agent and that a low starting dose (0.25-0.5 mg) will reduce the risk. You obtain his informed consent, document your treatment goals—a decrease in threatening behavior and the ability of the staff to work with Ms. F to get her up and out of bed—and establish a plan to review in 2 weeks.
CORRESPONDENCE
Daniel DeJoseph, MD, Drexel Family Medicine, 3401 Market Street, Suite 105-B, Philadelphia, PA 19104; [email protected]
1. Shen WW. A history of antipsychotic drug development. Compr Psychiatry. 1999;40:407-414.
2. Miller R. Mechanism of action of antipsychotic drugs of different classes, refractoriness to therapeutic effects of classical neuroleptics, and individual variation in sensitivity to their actions. Curr Neuropharmacol. 2009;7:302-314.
3. Seeman P. Atypical antipsychotics: mechanism of action. Can J Psychiatry. 2002;47:27-38.
4. Lieberman JA, Stroup TS, McEvoy JP, et al; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209-1223.
5. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of the effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63:1079-1087.
6. Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373:31-41.
7. Christian R, Saavedra L, Gaynes BN, et al. Future research needs for first- and second-generation antipsychotics for children and young adults [Internet]. Agency for Healthcare Research and Quality. 2012:12-EHC042-EF.
8. Maher AR, Maglione M, Bagley S, et al. Efficacy and comparative effectiveness of atypical antipsychotic medications for off-label uses in adults: a systematic review and meta-analysis. JAMA. 2011;306:1359-1369.
9. Maglione M, Maher AR, Hu J, et al. Off-label use of atypical antipsychotics: An update [Internet]. Agency for Healthcare Research and Quality. 2011:11-EHC087-EF.
10. Ballard CG, Waite J. Atypical antipsychotics for aggression and psychosis in Alzheimer’s disease. Cochrane Database Syst Rev. 2006;(1):CD003476.
11. Devanand DP, Mintzer J, Schultz SK, et al. Relapse risk after discontinuation of risperidone in Alzheimer’s disease. N Engl J Med. 2012;367:1497-1507.
12. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. Cochrane Database Syst Rev. 2008;(4):CD004844.
13. Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26-36.
14. Faries D, Ascher-Svanum H, Zhu B, et al. Antipsychotic monotherapy and polypharmacy in the naturalistic treatment of schizophrenia with atypical antipsychotics. BMC Psychiatry. 2005;5:26.
15. Ballon J, Stroup TS. Polypharmacy for schizophrenia. Curr Opin Psychiatry. 2013;26:208-213.
16. Krystal JH, Rosenheck RA, Cramer JA, et al; Veterans Affairs Cooperative Study No. 504 Group. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: a randomized trial. JAMA. 2011;306:493-502.
17. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: National Academy of Sciences; 2008.
18. Marder SR, Essock SM, Miller AL, et al. Physical health monitoring of patients with schizophrenia. Am J Psychiatry. 2004;161:1334-1349.
19. Barrett E, Blonde L, Clement S, et al. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
20. Drug Abuse Warning Network, 2010: National Estimates of Drug-Related Emergency Department Visits. HHS Publication No. (SMA) 12-4733, DAWN Series D-38. Substance Abuse and Mental Health Services Administration Web site. Available at: http://www.samhsa.gov/data/2k13/DAWN2k10ED/DAWN2k10ED.htm. Accessed May 1, 2013.
21. Douglas IJ, Smeeth L. Exposure to antipsychotics and risk of stroke: self controlled case series study. BMJ. 2008;337:a1227.
22. Pariente A, Fourrier-Réglat A, Ducruet T, et al. Antipsychotic use and myocardial infarction in older patients with treated dementia. Arch Intern Med. 2012;172:648-653.
23. Parker C, Coupland C, Hippisley-Cox J. Antipsychotic drugs and risk of venous thromboembolism: nested case-control study. BMJ. 2010;341:c4245.
24. Rossom RC, Rector TS, Lederle FA, et al. Are all commonly prescribed antipsychotics associated with greater mortality in elderly male veterans with dementia? J Am Geriatr Soc. 2010;58:1027-1034.
25. Kales HC, Kim HM, Zivin K, et al. Risk of mortality among individual antipsychotics in patients with dementia. Am J Psychiatry. 2012;169:71-79.
26. Huybrechts KF, Gerhard T, Crystal S, et al. Differential risk of death in older residents in nursing homes prescribed specific antipsychotic drugs: population based cohort study. BMJ. 2012;344:e977.
27. US Food and Drug Public Health Advisory: Deaths with antipsychotics in elderly patients with behavioral disturbances. US Food and Drug Administration Web site Available at: http://1.usa.gov/1plsxPk. Accessed February 5, 2014.
28. Information for healthcare professionals: conventional antipsychotics. US Food and Drug Administration Web site. Available at: http://www.fda.gov/drugs/drugsafety/postmarketdrugsafetyinformationforpatientsandproviders/ucm124830.htm. Accessed February 5, 2014.
29. Guide to the management of psychotic disorders and neuropsychiatric symptoms of dementia in older adults. American Geriatric Society Web site. Available at: http://dementia.americangeriatrics.org/GeriPsych_index.php. Accessed April 15, 2013.
30. Bogart GT, Ott CA. Abuse of second-generation antipsychotics: What prescribers need to know. Curr Psychiatr. 2011;10:77-79.
31. Tarosoff G, Osti K. Black-market value of antipsychotics, antidepressants, and hypnotics in Las Vegas, Nevada. Am J Psychiatry. 2007;164:350.
32. Highlights of the 2010 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality Web site. Available at: http://www.samhsa.gov/data/2k12/DAWN096/SR096EDHighlights2010.htm. Accessed May 1, 2013.
1. Shen WW. A history of antipsychotic drug development. Compr Psychiatry. 1999;40:407-414.
2. Miller R. Mechanism of action of antipsychotic drugs of different classes, refractoriness to therapeutic effects of classical neuroleptics, and individual variation in sensitivity to their actions. Curr Neuropharmacol. 2009;7:302-314.
3. Seeman P. Atypical antipsychotics: mechanism of action. Can J Psychiatry. 2002;47:27-38.
4. Lieberman JA, Stroup TS, McEvoy JP, et al; Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) Investigators. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209-1223.
5. Jones PB, Barnes TR, Davies L, et al. Randomized controlled trial of the effect on quality of life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1). Arch Gen Psychiatry. 2006;63:1079-1087.
6. Leucht S, Corves C, Arbter D, et al. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373:31-41.
7. Christian R, Saavedra L, Gaynes BN, et al. Future research needs for first- and second-generation antipsychotics for children and young adults [Internet]. Agency for Healthcare Research and Quality. 2012:12-EHC042-EF.
8. Maher AR, Maglione M, Bagley S, et al. Efficacy and comparative effectiveness of atypical antipsychotic medications for off-label uses in adults: a systematic review and meta-analysis. JAMA. 2011;306:1359-1369.
9. Maglione M, Maher AR, Hu J, et al. Off-label use of atypical antipsychotics: An update [Internet]. Agency for Healthcare Research and Quality. 2011:11-EHC087-EF.
10. Ballard CG, Waite J. Atypical antipsychotics for aggression and psychosis in Alzheimer’s disease. Cochrane Database Syst Rev. 2006;(1):CD003476.
11. Devanand DP, Mintzer J, Schultz SK, et al. Relapse risk after discontinuation of risperidone in Alzheimer’s disease. N Engl J Med. 2012;367:1497-1507.
12. Seidel S, Aigner M, Ossege M, et al. Antipsychotics for acute and chronic pain in adults. Cochrane Database Syst Rev. 2008;(4):CD004844.
13. Mojtabai R, Olfson M. National trends in psychotropic medication polypharmacy in office-based psychiatry. Arch Gen Psychiatry. 2010;67:26-36.
14. Faries D, Ascher-Svanum H, Zhu B, et al. Antipsychotic monotherapy and polypharmacy in the naturalistic treatment of schizophrenia with atypical antipsychotics. BMC Psychiatry. 2005;5:26.
15. Ballon J, Stroup TS. Polypharmacy for schizophrenia. Curr Opin Psychiatry. 2013;26:208-213.
16. Krystal JH, Rosenheck RA, Cramer JA, et al; Veterans Affairs Cooperative Study No. 504 Group. Adjunctive risperidone treatment for antidepressant-resistant symptoms of chronic military service-related PTSD: a randomized trial. JAMA. 2011;306:493-502.
17. Institute of Medicine. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: National Academy of Sciences; 2008.
18. Marder SR, Essock SM, Miller AL, et al. Physical health monitoring of patients with schizophrenia. Am J Psychiatry. 2004;161:1334-1349.
19. Barrett E, Blonde L, Clement S, et al. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27:596-601.
20. Drug Abuse Warning Network, 2010: National Estimates of Drug-Related Emergency Department Visits. HHS Publication No. (SMA) 12-4733, DAWN Series D-38. Substance Abuse and Mental Health Services Administration Web site. Available at: http://www.samhsa.gov/data/2k13/DAWN2k10ED/DAWN2k10ED.htm. Accessed May 1, 2013.
21. Douglas IJ, Smeeth L. Exposure to antipsychotics and risk of stroke: self controlled case series study. BMJ. 2008;337:a1227.
22. Pariente A, Fourrier-Réglat A, Ducruet T, et al. Antipsychotic use and myocardial infarction in older patients with treated dementia. Arch Intern Med. 2012;172:648-653.
23. Parker C, Coupland C, Hippisley-Cox J. Antipsychotic drugs and risk of venous thromboembolism: nested case-control study. BMJ. 2010;341:c4245.
24. Rossom RC, Rector TS, Lederle FA, et al. Are all commonly prescribed antipsychotics associated with greater mortality in elderly male veterans with dementia? J Am Geriatr Soc. 2010;58:1027-1034.
25. Kales HC, Kim HM, Zivin K, et al. Risk of mortality among individual antipsychotics in patients with dementia. Am J Psychiatry. 2012;169:71-79.
26. Huybrechts KF, Gerhard T, Crystal S, et al. Differential risk of death in older residents in nursing homes prescribed specific antipsychotic drugs: population based cohort study. BMJ. 2012;344:e977.
27. US Food and Drug Public Health Advisory: Deaths with antipsychotics in elderly patients with behavioral disturbances. US Food and Drug Administration Web site Available at: http://1.usa.gov/1plsxPk. Accessed February 5, 2014.
28. Information for healthcare professionals: conventional antipsychotics. US Food and Drug Administration Web site. Available at: http://www.fda.gov/drugs/drugsafety/postmarketdrugsafetyinformationforpatientsandproviders/ucm124830.htm. Accessed February 5, 2014.
29. Guide to the management of psychotic disorders and neuropsychiatric symptoms of dementia in older adults. American Geriatric Society Web site. Available at: http://dementia.americangeriatrics.org/GeriPsych_index.php. Accessed April 15, 2013.
30. Bogart GT, Ott CA. Abuse of second-generation antipsychotics: What prescribers need to know. Curr Psychiatr. 2011;10:77-79.
31. Tarosoff G, Osti K. Black-market value of antipsychotics, antidepressants, and hypnotics in Las Vegas, Nevada. Am J Psychiatry. 2007;164:350.
32. Highlights of the 2010 Drug Abuse Warning Network (DAWN) findings on drug-related emergency department visits. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality Web site. Available at: http://www.samhsa.gov/data/2k12/DAWN096/SR096EDHighlights2010.htm. Accessed May 1, 2013.
