User login
OBJECTIVES: Our objectives were to determine how patients who make frequent use of the medical system (high users) with medically unexplained symptoms met our chart-rating criteria for somatization and minor acute illness and what the stability of such diagnoses were over time.
STUDY DESIGN: A chart review was performed at baseline and 1 and 2 years; we re-rated the charts of patients initially rated as having somatization, as well as a 15% sample of those with minor acute illness.
POPULATION: We obtained a random sample of high-use patients (6 visits/year) aged 21 to 55 years who were identified from the management information system.
OUTCOMES: We measured chart review designations as organic disease, somatization, or minor acute illness.
RESULTS: Among 883 high users at baseline, 35% had organic diseases; 14% had somatization; and 51% had minor acute illness as their primary problems. No patients with initial minor acute diagnoses were reclassified as having somatization 1 or 2 years later, and all but 2 patients had minor acute illness in 1 or both follow-up years.
CONCLUSIONS: Minor acute illness was more common among high users than somatization and organic diseases combined. It has not previously been studied but probably has been recognized by clinicians as the “worried well.” Diagnoses of somatization were unstable over 2 years’ follow-up, while minor acute diagnoses were stable, supporting the latter as a valid entity.
- Many high-use patients with medically unexplained symptoms have a syndrome characterized by minor but recurring symptoms that we call minor acute illness.
- Minor acute illness has not been previously described as a research entity, but there are some similarities to what is referred to as the “worried well” in the nonresearch literature.
Using this preliminary research, we report on patients with medically unexplained physical symptoms, who have what we call “minor acute illness.” In contrast to the well-studied chronic somatizing patient in whom medically unexplained symptoms1,2 are of at least 6 months’ duration,3 we define minor acute illness as unexplained symptoms of any type (eg, sore throats, minor sprains, “sinuses”) that resolve completely in less than 6 months (usually days or weeks). Although most patients would not seek care for these minor complaints, some patients with minor acute illness have exaggerated responses to common symptoms and become high users of medical care.4-8 These are probably recognized by many physicians as the “worried well.”
Our review of the literature and discussion with several experts reveal that no research group has given consideration to defining the diagnostic features of minor acute illness or to describing it over time.9,10 Not surprisingly, studies of treatment are nonexistent, and reported treatments are ineffective.5,6,11 We present preliminary research defining minor acute illness, distinguishing it from somatization and organic disease, and evaluating its persistence over time among high-use patients.
Methods
Subjects
All patients were members of a largely primary care, staff model health maintenance organization (HMO) in Lansing, Michigan (Blue Cross Network). Only computerized descriptive information in the HMO’s management information system (MIS) and data in patients’ clinical charts were involved in our study. The MIS includes administrative information on age, sex, all patient encounters with the system, primary diagnoses made at each physician/nurse practitioner/physician assistant visit (International Classification of Diseases—Ninth Revision codes), revenue codes, and charges for services. Subjects whose visits for the year were primarily because of pregnancy, substance abuse, or other recognized psychiatric problems/diagnoses (eg, bipolar disorder, eating disorder) were excluded.
Screening to identify somatizing and minor acute illness patients
We first identified all patients aged 21 to 55 years in the Lansing, Michigan, area who had at least 1 visit during 1995 to a physician, physician assistant, nurse practitioner, specialist, or emergency room; each hospitalization was counted as 1 visit. We did not use older patients, because our goal for another project was to identify chronic somatizing patients with minimal organic disease; the discovery of minor acute illness patients was an unexpected byproduct. Of 15,505 members in 1995, 5423 had 6 or more visits, and 1000 of these patients were randomly selected for further evaluation; to obtain the greatest possible sample, we arbitrarily defined 6 or more visits (65th percentile) as high users. Of the 1000, 94 were excluded because of pregnancy, substance abuse, visits for psychiatric care, or because they were employees of the HMO, and 23 were excluded because of incomplete data. We excluded patients under regular psychiatric care, because we wanted to obtain (for a treatment intervention) patients not receiving psychologic attention. The remaining 883 patients constituted the study population. Excluded patients differed from those in the study group in age, sex, and employer group but not on the amount of copay (P =.58) and relationship to the subscriber (P =.23). Excluded patients were on average younger (35.7 years vs 40.3 years, P <.001), and 88% were women as opposed to 68% for patients included in the overall study (P <.001).
Reference standard diagnoses were established by a resident physician (emergency medicine) rating the 883 charts according to specific criteria, reported previously12 and summarized in the report’s Appendix.* The rater classified patients by their primary/predominant problem for the entire year as organic disease, somatization, or minor acute illness. The designation of the primary problem was based on the largest number of visits for a problem. For example, a patient with a documented urinary infection at the first visit with 1 follow-up visit, documented pneumonia at the third visit with 2 follow-up visits, 1 visit for chronic low back pain with a negative computed tomography scan, and 2 visits for minor ligamentous strain, with no objective manifestations and no investigation, would be rated as organic for this year; similarly, a patient would be considered to have minor acute illness with 6 visits for minor complaints with no work-up and no objective manifestations of disease on examination, as well as 1 visit for documented urinary infection and 3 for diabetes mellitus. The same rule was used for follow-up ratings 1 and 2 years later, and the rater for follow-up ratings was unaware of the baseline ratings.
Organic disease was diagnosed by standard medical criteria and based on clear physical signs of disease (eg, laceration, enlarged liver) or, almost always, definitive laboratory investigation; the rater relied on expert judgment and referred to text material as needed.13 Somatization was rated when, following objectively based diagnostic evaluation (definitive testing), patients were free of organic disease that contributed significantly to at least 1 physical symptom of at least 6 months’ duration. Minor acute illness was rated when all physical symptoms were of less than 6 months’ duration, as judged by the rater from explicit mention in the chart or from observation that symptoms cleared and did not recur, and there was no documentation of an organic disease explanation for the symptom or its degree of severity. Because minor acute problems typically were not severe or disabling (in contrast to somatization), definitive testing often had not been performed. From the 1995 baseline sample of 122 somatizers and 450 minor acute patients identified by our rating procedure, we re-rated a sample of all available somatizers (N=104; 85%) and a 15% random sample of minor acute illness patients (N=66) both 1 and 2 years later.
After 10 hours of initial training, including practice rating on nonstudy charts, the rater rated 20 charts of non-study high-utilizing patients. A priori, we set an agreement rate with the trainer (one of the authors [R.C.S.]) for primary diagnosis of 90% (18 of 20 charts) before the rater began rating study patients. During the study, the trainer rated sets of 20 study charts already evaluated by the rater, once each during 1995, 1996, and 1997. The rater had high levels of agreement with the trainer throughout, varying from 90% to 95%. This level of agreement is not surprising, because the trainer trained the rater, which was also reflected in the of 0.93.
Statistical analysis
We also reviewed the 1996 and 1997 use for the same 104 somatizers identified in our initial 1995 baseline chart review of high-utilizing patients. Again, the same 15% random sample (N=66) was selected from those classified as having minor acute illness in 1995. In the follow-up years, some patients had relocated or were no longer receiving their medical care at our HMO. However, nearly 85% of the patients in our selected sample were continuously enrolled in the HMO in the 2 subsequent years of our study. Similar to chart rating, the final sample consisted of 104 somatizers and 66 patients with minor acute illness. For these patients we ascertained their status (somatization, organic disease, or minor acute illness) and their use (<6 visits; 6 visits) in 1996 and 1997. The 2 groups of patients were compared using chi-square tests for categoric variables and by t tests for continuous variables. Confidence intervals for binomial proportions were calculated by the exact method.
Results
The characteristics of 170 patients (104 somatization; 66 minor acute) studied at all data collection points are shown in Table 1. The mean age (as of 1995) was 41.3 years among somatizers versus 39.7 years among patients with minor acute illness (P =.19) The 2 groups differed only by sex, with nearly 83% of the somatizers being women, compared with 65% among minor acute illness patients (P=.009).
Among 883 high-use patients at baseline, 311 had organic diseases (35%); 122 had somatization (14%); and 450 had minor acute illness (51%) as their primary problems. No patients with initial minor acute illness diagnoses were reclassified as somatization 1 and 2 years later, and all but 2 patients had minor acute illness in 1 or both follow-up years.
The follow-up status in 1996 and 1997 of the 104 somatizers and the 66 minor acute illness patients initially rated in 1995 appears in Figure 1. It shows the (percentage) distribution of organic diseases, somatization, and minor acute illness diagnoses for 1995, 1996, and 1997, using all available data in each year. Because our rating of patients in 1 of the 3 categories followed a strict protocol (for 13 patients in 1996 and 40 patients in 1997), and because of insufficient information in their charts, we were unable to definitely ascertain their status. None of the patients with minor acute illness were reclassified as somatizers in the follow-up years, and 83% of these patients continued to have minor acute illness in 1996. All but 2 patients had minor acute illness either in 1996 or 1997 or both. Approximately 27% of the somatizers remained somatizers in 1996, 54% were rated as having minor acute illness, and 13% had organic disease. In 27% of these somatizers minor acute illness developed in the 2 subsequent years. Among patients in 1995, the probabilities of somatization for 2 and 3 consecutive years were 3.7% and 1.1%, respectively. In contrast, for minor acute illness these probabilities were 42.5% and 27%, respectively.
Use status of the groups (somatization, minor acute illness) combined is shown in Figure 2. It shows the (percentage) distribution of use (<6 visits; 6 visits) for 1996 and 1997. Approximately 57% of the somatizers were high users in 1996, compared with 29% of the minor acute illness patients. High use in either 1996 or 1997 was more prevalent among somatizers (70%) than in minor acute illness patients (45%). Persistent high use in both years among minor acute illness patients was 16.7% (95% confidence interval [CI], 8.6%-27.9%) and among somatizers 32.7% (95% CI, 23.8%-42.6%).
TABLE 1
CHARACTERISTICS OF FOLLOW-UP STUDY (N=70)
| Characteristic | Subgroup | Somatizers % (N) | Minor Acute % (N) |
|---|---|---|---|
| Age, years | 20-29 | 13.5 (14) | 9.1 (6) |
| 30-39 | 24.0 (25) | 43.9 (29) | |
| 40-49 | 51.0 (53) | 36.4 (24) | |
| 50+ | 11.5 (12) | 10.6 (7) | |
| Sex | Men | 17.3 (18) | 34.9 (23) |
| Women | 82.7 (86) | 65.2 (43) | |
| Employer | MSU | 6.7 (7) | 4.6 (3) |
| State | 28.9 (30) | 24.2 (16) | |
| GM | 22.1 (23) | 30.3 (20) | |
| Other | 42.3 (44) | 41.0 (27) | |
| Copay, $ | 0 | 58.7 (61) | 57.6 (38) |
| 5 | 28.9 (30) | 25.8 (17) | |
| 7 | 11.5 (12) | 10.6 (7) | |
| 10 | 1.0 (1) | 6.1 (4) | |
| Relationship to subscriber | Self | 59.6 (62) | 62.1 (41) |
| Spouse | 37.5 (39) | 34.9 (23) | |
| Dependent | 2.9 (3) | 3.0 (2) | |
| MSU denotes Michigan State University; GM, General Motors. | |||
FIGURE 1
FOLLOW-UP DIAGNOSES IN INTIALLY IDENTIFIED MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS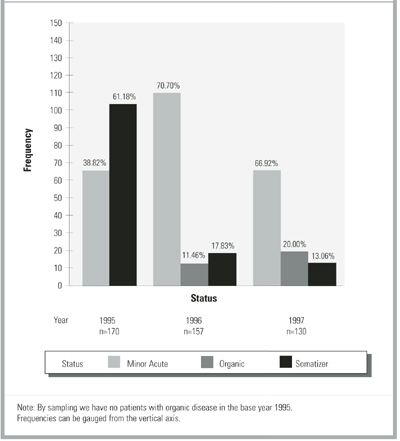
FIGURE 2
FOLLOW-UP USE PATTERNS OF INTIALLY HIGH-USE PATIENTS WITH MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS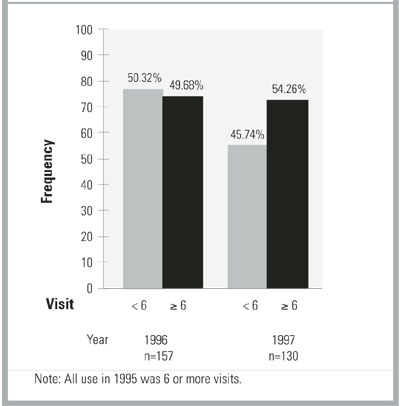
Discussion
Among high users of care, patients with minor acute symptoms were more common than those with symptoms of somatization and organic diseases combined. On follow-up study, diagnoses of somatization often changed to minor acute status, while minor acute illness diagnoses were more persistent. Although use did not remain high in either group, regression to the mean must be considered, because we sampled only on high use in 1995.
We found no research data to compare with our results in patients with minor acute illness. However, the presumed stability and chronicity of somatization diagnoses3,14 have been questioned.14-16 For example, great variability in symptoms was seen in repeated hospitalizations of somatizers, as judged by chart review.17 Others found that only 21 of 70 cases identified as somatization disorder at baseline had the same diagnosis 12 months later and that only approximately one half of all somatization symptoms were present 1 year later.16,18
Limitations
This first preliminary study of high users with minor acute illness was limited by the shortcomings of any retrospective chart review. These include the facts that: (1) We depended on how aggressively a physician attempted to diagnose organic disease and on how completely clinicians recorded their findings; (2) Without access to patients, we were unable to identify their unique perspective or to diagnose specific somatoform disorders3 using, for example, the Diagnostic Interview Schedule,19 the World Health Organization Composite Diagnostic Interview,20 or direct patient interviews; (3) Our designation of somatization depended on identifying symptoms of 6 or more months’ duration, the minimum criterion specified for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) somatoform diagnoses3; if busy clinicians did not record duration, overcoding of minor acute status could have occurred.4 We cannot be certain that patients in either the medically unexplained group (ie, somatization, minor acute illness) did not in fact have organic diseases, because we were unable to investigate each patient ourselves from a biomedical perspective. However, during follow-up chart review, we observed no instances of an important organic disease having been missed when a diagnosis of minor acute illness or somatization status was made initially.15,21
In spite of these expected problems when chart review is the only available source of data, this research on previously unstudied patients provides a starting point for further research. Based on clinical descriptions, our observations on somatizing patients did in fact indicate that we had studied a typical chronic somatizing population (eg, those with low back pain, pelvic pain, irritable bowel syndrome). Also, others have found that chart review may be superior in identifying somatizing patients17,18 and that the DSM-IV has important shortcomings, notwithstanding the latter’s prominent present role in diagnosing conditions with medically unexplained symptoms.22,23 Further, because minor acute illness symptoms are short term, it is arguable that few minor acute patients will receive DSM-IV somatoform diagnoses. Still, as the next research step DSM-IV diagnoses should be sought to better delineate this new group, as should other standard psychiatric measures, especially for depression, anxiety, and unique personality traits.
Although psychiatric measures are needed to better define this high-use population, their absence in this initial study does not negate the importance of our findings from medical patients’ charts. They presumably reflect what patients actually reported to providers as their major reasons for seeking care, in contrast to questionnaire and lay interviewer data obtained unrelated to care seeking. Complementing our chart-based data with these standard psychiatric measures is the necessary next step.
Others have considered the problem of minor symptoms. Barsky and Borus7 seemed to distinguish short-term symptoms from the chronic symptoms of somatization and somatoform disorders by including many symptoms that often are brief and self-limited in what they called functional somatic syndromes (eg, palpitations, dizziness, lightheadedness, sore throat, and dry mouth). To avoid compounding the severe nosology problem in somatization24,25 and because the term functional somatic syndromes has been used by others to encompass all types of somatization,26,27 we are using the purely descriptive term “minor acute illness” to identify the patients reported here with short-term symptoms, recognizing that there may be considerable overlap with the group of patients identified by Barsky and Borus,7 Katon and colleagues,28 the acute and subacute somatizers of Kleinman,8 and the somatoform “not otherwise specified” category in DSM-IV.29 We prefer minor acute illness also to the common but pejorative term “worried well,” which we believe has never been defined. The “minor acute” label also has been used previously in a closely related context.30 Similar to Katon and coworkers,28 we propose that minor acute illness fits into the mild end of a multidimensional classification scheme for patients with medically unexplained symptoms—with abridged somatization disorder31 as moderate and full somatization disorder as severe.3 The latter 2 diagnoses are based on DSM-IV criteria only.
CONCLUSIONS
More research is needed to assist the field in better addressing patients with medically unexplained symptoms. The long-range goal for minor acute illness (as well as somatization) is to determine if it is a distinct and valid entity. In what is a complex task for psychiatric epidemiologists in the absence of organic disease and pathophysiologic changes,32-37 we can use the recommendations of Guze and colleagues38,39 for establishing the validity of a psychiatric diagnosis to guide us (Table 2). At this point, we can say only that there is evidence from our initial research study that we can use to describe and define minor acute illness and that it persists over 2 years (criteria 1 and 4 from Table 2). These are key determinants of validity, but they require much confirmation.38,39 Extensive work lies ahead in achieving our ultimate goal, providing effective treatment for a group that often receives inappropriate treatment, such as unnecessary antibiotics.
TABLE 2
VALIDITY CRITERIA FOR PSYCHIATRIC ENTITIES
|
| NOTE: From Guze and colleagues,38,39 who comment that we often know little about criteria 2 and 3, and a careful description must focus on criteria 4 and 5, follow-up studies, and family studies. |
Acknowledgments
Our work was supported by a generous grant from the Institute for Managed Care, Michigan State University, East Lansing.
1. Lipowski ZJ. Somatization: the concept and its clinical application. Am J Psychiatry 1988;145:1358-68.
2. Kirmayer LJ, Robbins JM. Introduction: concepts of somatization. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;1-19.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
4. Komaroff AL. ‘Minor’ illness symptoms—the magnitude of their burden and of our ignorance. Arch Intern Med 1990;150:1586-87.
5. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-66.
6. Connelly JE, Smith GR, Philbrick JT, Kaiser DL. Healthy patients who perceive poor health and their use of primary care services. J Gen Int Med 1991;6:47-51.
7. Barsky AJ, Borus JF. Functional somatic syndromes. Ann Intern Med 1999;130:910-21.
8. Kleinman A. Social origins of distress and disease—depression, neurasthenia, and pain in modern China. New Haven, Conn: Yale University Press; 1986.
9. Andersson S-O, Mattsson B, Lynoe N. Patients frequently consulting general practitioners at a primary health care centre in Sweden—a comparative study. Scand J Soc Med 1995;23:251-57.
10. Verbrugge LM, Ascione FJ. Exploring the iceberg—common symptoms and how people care for them. Med Care 1987;25:539-69.
11. Kroenke K, Arrington ME, Mangelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med 1990;150:1685-89.
12. Smith RC, Gardiner JC, Armatti S, et al. Screening for high utilizing somatizing patients using a prediction rule derived from the management information system of an HMO—a preliminary study. In press.
13. Humes HD, DuPont HL, Gardner LB, et al, eds. Kelley’s textbook of internal medicine. 4th ed. Philadelphia, Pa: Lippincott Williams and Wilkins; 2000.
14. Cloninger CR, Martin RL, Guze SB, Clayton PJ. A prospective follow-up and family study of somatization in men and women. Am J Psychiatry 1986;143:873-78.
15. Rief W, Hiller W, Geissner E, Fichter MM. A two-year follow-up study of patients with somatoform disorders. Psychosomatics 1995;36:376-86.
16. Gara MA, Escobar JI. The stability of somatization syndromes over time. Arch Gen Psychiatry 2001;58:94.-
17. Fink P. Physical complaints and symptoms of somatizing patients. J Psychosom Res 1992;36:125-36.
18. Simon GE, Gureje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry 1999;56:90-95.
19. Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health Diagnostic Interview Schedule: its history, characteristics, and validity. Arch Gen Psychiatry 1981;38:381-89.
20. Sartorius N. Composite International Diagnostic Interview (CIDI)—core version 1.1. Geneva, Switzerland: World Health Organization.
21. Kroenke K, Spitzer RL, deGruy FV, Hahn SR, Linzer M, Williams JBW, Brody D, Davies M. Multisomatoform disorder—an alternative to undifferentiated somatoform disorder for the somatizing patient in primary care. Arch Gen Psychiatry 1997;54:352-58.
22. Norquist G, Hyman SE. Advances in understanding and treating mental illness: implications for policy. Health Aff 1999;18:32-47.
23. Krueger RF. The structure of common mental disorders. Arch Gen Psychiatry 1999;56:921-26.
24. Murphy MR. Classification of the somatoform disorders. In: Bass CM, ed. Somatization: physical symptoms and psychological illness. Oxford, England: Blackwell; 1990;10-39.
25. Mayou R, Bass C, Sharpe M. Overview of epidemiology, classification, and aetiology. In: Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms. Oxford, England: Oxford University Press, 1995;42-65.
26. Kirmayer LJ, Robbins JM. Functional somatic syndromes. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;79-106.
27. Sharpe M, Mayou R, Bass C. Concepts, theories, and terminology. In: Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms. Oxford, England: Oxford University Press; 1995;1-16.
28. Katon W, Lin E, von Korff M, Russo J, Lipscomb P, Bush T. Somatization: a spectrum of severity. Am J Psychiatry 1991;148:34-40.
29. Kroenke K, Spitzer RL, deGruy FV, Swindle R. A symptom checklist to screen for somatoform disorders in primary care. Psychosomatics 1998;39:263-72.
30. Weiner JP, Starfield BH, Steinwachs DM, Mumford LM. Development and application of a population-oriented measure of ambulatory care case-mix. Med Care 1991;29:452-72.
31. Escobar JI, Swartz M, Rubio-Stipec M, Manu P. Medically unexplained symptoms: distribution, risk factors, and comorbidity. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;63-78.
32. Kovacs M, Gatsonis C. Stability and change in childhood-onset depressive disorders: longitudinal course as a diagnostic validator. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnosis. New York, NY: Raven Press, Ltd; 1989;57-73.
33. Tyrer P, Alexander J, Remington M, Riley P. Relationship between neurotic symptoms and neurotic diagnosis: a longitudinal study. J Affect Dis 1987;13:13-21.
34. Beiser M, Iacono WG, Erickson D. Temporal stability in the major mental disorders. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnosis. New York, NY: Raven Press, Ltd; 1989;77-97.
35. Andreason NC. The validation of psychiatric diagnosis: new models and approaches. Am J Psychiatry 1995;152:161-62.
36. Cloninger CR. Establishment of diagnostic validity in psychiatric illness: Robins and Guze’s method revisited. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnoses. New York, NY: Raven Press; 1989;9-16.
37. Grove WM, Andreasen NC. Quantitative and qualitative distinctions between psychiatric disorders. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnoses. New York, NY: Raven Press; 1989;127-39.
38. Guze SB. The diagnosis of hysteria: what are we trying to do? Am J Psychiatry 1967;124:491-98.
39. Robins E, Guze SB. Establishment of diagnostic validity in psychiatric illness: its application to schizophrenia. Am J Psychiatry 1970;126:983-87.
OBJECTIVES: Our objectives were to determine how patients who make frequent use of the medical system (high users) with medically unexplained symptoms met our chart-rating criteria for somatization and minor acute illness and what the stability of such diagnoses were over time.
STUDY DESIGN: A chart review was performed at baseline and 1 and 2 years; we re-rated the charts of patients initially rated as having somatization, as well as a 15% sample of those with minor acute illness.
POPULATION: We obtained a random sample of high-use patients (6 visits/year) aged 21 to 55 years who were identified from the management information system.
OUTCOMES: We measured chart review designations as organic disease, somatization, or minor acute illness.
RESULTS: Among 883 high users at baseline, 35% had organic diseases; 14% had somatization; and 51% had minor acute illness as their primary problems. No patients with initial minor acute diagnoses were reclassified as having somatization 1 or 2 years later, and all but 2 patients had minor acute illness in 1 or both follow-up years.
CONCLUSIONS: Minor acute illness was more common among high users than somatization and organic diseases combined. It has not previously been studied but probably has been recognized by clinicians as the “worried well.” Diagnoses of somatization were unstable over 2 years’ follow-up, while minor acute diagnoses were stable, supporting the latter as a valid entity.
- Many high-use patients with medically unexplained symptoms have a syndrome characterized by minor but recurring symptoms that we call minor acute illness.
- Minor acute illness has not been previously described as a research entity, but there are some similarities to what is referred to as the “worried well” in the nonresearch literature.
Using this preliminary research, we report on patients with medically unexplained physical symptoms, who have what we call “minor acute illness.” In contrast to the well-studied chronic somatizing patient in whom medically unexplained symptoms1,2 are of at least 6 months’ duration,3 we define minor acute illness as unexplained symptoms of any type (eg, sore throats, minor sprains, “sinuses”) that resolve completely in less than 6 months (usually days or weeks). Although most patients would not seek care for these minor complaints, some patients with minor acute illness have exaggerated responses to common symptoms and become high users of medical care.4-8 These are probably recognized by many physicians as the “worried well.”
Our review of the literature and discussion with several experts reveal that no research group has given consideration to defining the diagnostic features of minor acute illness or to describing it over time.9,10 Not surprisingly, studies of treatment are nonexistent, and reported treatments are ineffective.5,6,11 We present preliminary research defining minor acute illness, distinguishing it from somatization and organic disease, and evaluating its persistence over time among high-use patients.
Methods
Subjects
All patients were members of a largely primary care, staff model health maintenance organization (HMO) in Lansing, Michigan (Blue Cross Network). Only computerized descriptive information in the HMO’s management information system (MIS) and data in patients’ clinical charts were involved in our study. The MIS includes administrative information on age, sex, all patient encounters with the system, primary diagnoses made at each physician/nurse practitioner/physician assistant visit (International Classification of Diseases—Ninth Revision codes), revenue codes, and charges for services. Subjects whose visits for the year were primarily because of pregnancy, substance abuse, or other recognized psychiatric problems/diagnoses (eg, bipolar disorder, eating disorder) were excluded.
Screening to identify somatizing and minor acute illness patients
We first identified all patients aged 21 to 55 years in the Lansing, Michigan, area who had at least 1 visit during 1995 to a physician, physician assistant, nurse practitioner, specialist, or emergency room; each hospitalization was counted as 1 visit. We did not use older patients, because our goal for another project was to identify chronic somatizing patients with minimal organic disease; the discovery of minor acute illness patients was an unexpected byproduct. Of 15,505 members in 1995, 5423 had 6 or more visits, and 1000 of these patients were randomly selected for further evaluation; to obtain the greatest possible sample, we arbitrarily defined 6 or more visits (65th percentile) as high users. Of the 1000, 94 were excluded because of pregnancy, substance abuse, visits for psychiatric care, or because they were employees of the HMO, and 23 were excluded because of incomplete data. We excluded patients under regular psychiatric care, because we wanted to obtain (for a treatment intervention) patients not receiving psychologic attention. The remaining 883 patients constituted the study population. Excluded patients differed from those in the study group in age, sex, and employer group but not on the amount of copay (P =.58) and relationship to the subscriber (P =.23). Excluded patients were on average younger (35.7 years vs 40.3 years, P <.001), and 88% were women as opposed to 68% for patients included in the overall study (P <.001).
Reference standard diagnoses were established by a resident physician (emergency medicine) rating the 883 charts according to specific criteria, reported previously12 and summarized in the report’s Appendix.* The rater classified patients by their primary/predominant problem for the entire year as organic disease, somatization, or minor acute illness. The designation of the primary problem was based on the largest number of visits for a problem. For example, a patient with a documented urinary infection at the first visit with 1 follow-up visit, documented pneumonia at the third visit with 2 follow-up visits, 1 visit for chronic low back pain with a negative computed tomography scan, and 2 visits for minor ligamentous strain, with no objective manifestations and no investigation, would be rated as organic for this year; similarly, a patient would be considered to have minor acute illness with 6 visits for minor complaints with no work-up and no objective manifestations of disease on examination, as well as 1 visit for documented urinary infection and 3 for diabetes mellitus. The same rule was used for follow-up ratings 1 and 2 years later, and the rater for follow-up ratings was unaware of the baseline ratings.
Organic disease was diagnosed by standard medical criteria and based on clear physical signs of disease (eg, laceration, enlarged liver) or, almost always, definitive laboratory investigation; the rater relied on expert judgment and referred to text material as needed.13 Somatization was rated when, following objectively based diagnostic evaluation (definitive testing), patients were free of organic disease that contributed significantly to at least 1 physical symptom of at least 6 months’ duration. Minor acute illness was rated when all physical symptoms were of less than 6 months’ duration, as judged by the rater from explicit mention in the chart or from observation that symptoms cleared and did not recur, and there was no documentation of an organic disease explanation for the symptom or its degree of severity. Because minor acute problems typically were not severe or disabling (in contrast to somatization), definitive testing often had not been performed. From the 1995 baseline sample of 122 somatizers and 450 minor acute patients identified by our rating procedure, we re-rated a sample of all available somatizers (N=104; 85%) and a 15% random sample of minor acute illness patients (N=66) both 1 and 2 years later.
After 10 hours of initial training, including practice rating on nonstudy charts, the rater rated 20 charts of non-study high-utilizing patients. A priori, we set an agreement rate with the trainer (one of the authors [R.C.S.]) for primary diagnosis of 90% (18 of 20 charts) before the rater began rating study patients. During the study, the trainer rated sets of 20 study charts already evaluated by the rater, once each during 1995, 1996, and 1997. The rater had high levels of agreement with the trainer throughout, varying from 90% to 95%. This level of agreement is not surprising, because the trainer trained the rater, which was also reflected in the of 0.93.
Statistical analysis
We also reviewed the 1996 and 1997 use for the same 104 somatizers identified in our initial 1995 baseline chart review of high-utilizing patients. Again, the same 15% random sample (N=66) was selected from those classified as having minor acute illness in 1995. In the follow-up years, some patients had relocated or were no longer receiving their medical care at our HMO. However, nearly 85% of the patients in our selected sample were continuously enrolled in the HMO in the 2 subsequent years of our study. Similar to chart rating, the final sample consisted of 104 somatizers and 66 patients with minor acute illness. For these patients we ascertained their status (somatization, organic disease, or minor acute illness) and their use (<6 visits; 6 visits) in 1996 and 1997. The 2 groups of patients were compared using chi-square tests for categoric variables and by t tests for continuous variables. Confidence intervals for binomial proportions were calculated by the exact method.
Results
The characteristics of 170 patients (104 somatization; 66 minor acute) studied at all data collection points are shown in Table 1. The mean age (as of 1995) was 41.3 years among somatizers versus 39.7 years among patients with minor acute illness (P =.19) The 2 groups differed only by sex, with nearly 83% of the somatizers being women, compared with 65% among minor acute illness patients (P=.009).
Among 883 high-use patients at baseline, 311 had organic diseases (35%); 122 had somatization (14%); and 450 had minor acute illness (51%) as their primary problems. No patients with initial minor acute illness diagnoses were reclassified as somatization 1 and 2 years later, and all but 2 patients had minor acute illness in 1 or both follow-up years.
The follow-up status in 1996 and 1997 of the 104 somatizers and the 66 minor acute illness patients initially rated in 1995 appears in Figure 1. It shows the (percentage) distribution of organic diseases, somatization, and minor acute illness diagnoses for 1995, 1996, and 1997, using all available data in each year. Because our rating of patients in 1 of the 3 categories followed a strict protocol (for 13 patients in 1996 and 40 patients in 1997), and because of insufficient information in their charts, we were unable to definitely ascertain their status. None of the patients with minor acute illness were reclassified as somatizers in the follow-up years, and 83% of these patients continued to have minor acute illness in 1996. All but 2 patients had minor acute illness either in 1996 or 1997 or both. Approximately 27% of the somatizers remained somatizers in 1996, 54% were rated as having minor acute illness, and 13% had organic disease. In 27% of these somatizers minor acute illness developed in the 2 subsequent years. Among patients in 1995, the probabilities of somatization for 2 and 3 consecutive years were 3.7% and 1.1%, respectively. In contrast, for minor acute illness these probabilities were 42.5% and 27%, respectively.
Use status of the groups (somatization, minor acute illness) combined is shown in Figure 2. It shows the (percentage) distribution of use (<6 visits; 6 visits) for 1996 and 1997. Approximately 57% of the somatizers were high users in 1996, compared with 29% of the minor acute illness patients. High use in either 1996 or 1997 was more prevalent among somatizers (70%) than in minor acute illness patients (45%). Persistent high use in both years among minor acute illness patients was 16.7% (95% confidence interval [CI], 8.6%-27.9%) and among somatizers 32.7% (95% CI, 23.8%-42.6%).
TABLE 1
CHARACTERISTICS OF FOLLOW-UP STUDY (N=70)
| Characteristic | Subgroup | Somatizers % (N) | Minor Acute % (N) |
|---|---|---|---|
| Age, years | 20-29 | 13.5 (14) | 9.1 (6) |
| 30-39 | 24.0 (25) | 43.9 (29) | |
| 40-49 | 51.0 (53) | 36.4 (24) | |
| 50+ | 11.5 (12) | 10.6 (7) | |
| Sex | Men | 17.3 (18) | 34.9 (23) |
| Women | 82.7 (86) | 65.2 (43) | |
| Employer | MSU | 6.7 (7) | 4.6 (3) |
| State | 28.9 (30) | 24.2 (16) | |
| GM | 22.1 (23) | 30.3 (20) | |
| Other | 42.3 (44) | 41.0 (27) | |
| Copay, $ | 0 | 58.7 (61) | 57.6 (38) |
| 5 | 28.9 (30) | 25.8 (17) | |
| 7 | 11.5 (12) | 10.6 (7) | |
| 10 | 1.0 (1) | 6.1 (4) | |
| Relationship to subscriber | Self | 59.6 (62) | 62.1 (41) |
| Spouse | 37.5 (39) | 34.9 (23) | |
| Dependent | 2.9 (3) | 3.0 (2) | |
| MSU denotes Michigan State University; GM, General Motors. | |||
FIGURE 1
FOLLOW-UP DIAGNOSES IN INTIALLY IDENTIFIED MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS
FIGURE 2
FOLLOW-UP USE PATTERNS OF INTIALLY HIGH-USE PATIENTS WITH MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS
Discussion
Among high users of care, patients with minor acute symptoms were more common than those with symptoms of somatization and organic diseases combined. On follow-up study, diagnoses of somatization often changed to minor acute status, while minor acute illness diagnoses were more persistent. Although use did not remain high in either group, regression to the mean must be considered, because we sampled only on high use in 1995.
We found no research data to compare with our results in patients with minor acute illness. However, the presumed stability and chronicity of somatization diagnoses3,14 have been questioned.14-16 For example, great variability in symptoms was seen in repeated hospitalizations of somatizers, as judged by chart review.17 Others found that only 21 of 70 cases identified as somatization disorder at baseline had the same diagnosis 12 months later and that only approximately one half of all somatization symptoms were present 1 year later.16,18
Limitations
This first preliminary study of high users with minor acute illness was limited by the shortcomings of any retrospective chart review. These include the facts that: (1) We depended on how aggressively a physician attempted to diagnose organic disease and on how completely clinicians recorded their findings; (2) Without access to patients, we were unable to identify their unique perspective or to diagnose specific somatoform disorders3 using, for example, the Diagnostic Interview Schedule,19 the World Health Organization Composite Diagnostic Interview,20 or direct patient interviews; (3) Our designation of somatization depended on identifying symptoms of 6 or more months’ duration, the minimum criterion specified for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) somatoform diagnoses3; if busy clinicians did not record duration, overcoding of minor acute status could have occurred.4 We cannot be certain that patients in either the medically unexplained group (ie, somatization, minor acute illness) did not in fact have organic diseases, because we were unable to investigate each patient ourselves from a biomedical perspective. However, during follow-up chart review, we observed no instances of an important organic disease having been missed when a diagnosis of minor acute illness or somatization status was made initially.15,21
In spite of these expected problems when chart review is the only available source of data, this research on previously unstudied patients provides a starting point for further research. Based on clinical descriptions, our observations on somatizing patients did in fact indicate that we had studied a typical chronic somatizing population (eg, those with low back pain, pelvic pain, irritable bowel syndrome). Also, others have found that chart review may be superior in identifying somatizing patients17,18 and that the DSM-IV has important shortcomings, notwithstanding the latter’s prominent present role in diagnosing conditions with medically unexplained symptoms.22,23 Further, because minor acute illness symptoms are short term, it is arguable that few minor acute patients will receive DSM-IV somatoform diagnoses. Still, as the next research step DSM-IV diagnoses should be sought to better delineate this new group, as should other standard psychiatric measures, especially for depression, anxiety, and unique personality traits.
Although psychiatric measures are needed to better define this high-use population, their absence in this initial study does not negate the importance of our findings from medical patients’ charts. They presumably reflect what patients actually reported to providers as their major reasons for seeking care, in contrast to questionnaire and lay interviewer data obtained unrelated to care seeking. Complementing our chart-based data with these standard psychiatric measures is the necessary next step.
Others have considered the problem of minor symptoms. Barsky and Borus7 seemed to distinguish short-term symptoms from the chronic symptoms of somatization and somatoform disorders by including many symptoms that often are brief and self-limited in what they called functional somatic syndromes (eg, palpitations, dizziness, lightheadedness, sore throat, and dry mouth). To avoid compounding the severe nosology problem in somatization24,25 and because the term functional somatic syndromes has been used by others to encompass all types of somatization,26,27 we are using the purely descriptive term “minor acute illness” to identify the patients reported here with short-term symptoms, recognizing that there may be considerable overlap with the group of patients identified by Barsky and Borus,7 Katon and colleagues,28 the acute and subacute somatizers of Kleinman,8 and the somatoform “not otherwise specified” category in DSM-IV.29 We prefer minor acute illness also to the common but pejorative term “worried well,” which we believe has never been defined. The “minor acute” label also has been used previously in a closely related context.30 Similar to Katon and coworkers,28 we propose that minor acute illness fits into the mild end of a multidimensional classification scheme for patients with medically unexplained symptoms—with abridged somatization disorder31 as moderate and full somatization disorder as severe.3 The latter 2 diagnoses are based on DSM-IV criteria only.
CONCLUSIONS
More research is needed to assist the field in better addressing patients with medically unexplained symptoms. The long-range goal for minor acute illness (as well as somatization) is to determine if it is a distinct and valid entity. In what is a complex task for psychiatric epidemiologists in the absence of organic disease and pathophysiologic changes,32-37 we can use the recommendations of Guze and colleagues38,39 for establishing the validity of a psychiatric diagnosis to guide us (Table 2). At this point, we can say only that there is evidence from our initial research study that we can use to describe and define minor acute illness and that it persists over 2 years (criteria 1 and 4 from Table 2). These are key determinants of validity, but they require much confirmation.38,39 Extensive work lies ahead in achieving our ultimate goal, providing effective treatment for a group that often receives inappropriate treatment, such as unnecessary antibiotics.
TABLE 2
VALIDITY CRITERIA FOR PSYCHIATRIC ENTITIES
|
| NOTE: From Guze and colleagues,38,39 who comment that we often know little about criteria 2 and 3, and a careful description must focus on criteria 4 and 5, follow-up studies, and family studies. |
Acknowledgments
Our work was supported by a generous grant from the Institute for Managed Care, Michigan State University, East Lansing.
OBJECTIVES: Our objectives were to determine how patients who make frequent use of the medical system (high users) with medically unexplained symptoms met our chart-rating criteria for somatization and minor acute illness and what the stability of such diagnoses were over time.
STUDY DESIGN: A chart review was performed at baseline and 1 and 2 years; we re-rated the charts of patients initially rated as having somatization, as well as a 15% sample of those with minor acute illness.
POPULATION: We obtained a random sample of high-use patients (6 visits/year) aged 21 to 55 years who were identified from the management information system.
OUTCOMES: We measured chart review designations as organic disease, somatization, or minor acute illness.
RESULTS: Among 883 high users at baseline, 35% had organic diseases; 14% had somatization; and 51% had minor acute illness as their primary problems. No patients with initial minor acute diagnoses were reclassified as having somatization 1 or 2 years later, and all but 2 patients had minor acute illness in 1 or both follow-up years.
CONCLUSIONS: Minor acute illness was more common among high users than somatization and organic diseases combined. It has not previously been studied but probably has been recognized by clinicians as the “worried well.” Diagnoses of somatization were unstable over 2 years’ follow-up, while minor acute diagnoses were stable, supporting the latter as a valid entity.
- Many high-use patients with medically unexplained symptoms have a syndrome characterized by minor but recurring symptoms that we call minor acute illness.
- Minor acute illness has not been previously described as a research entity, but there are some similarities to what is referred to as the “worried well” in the nonresearch literature.
Using this preliminary research, we report on patients with medically unexplained physical symptoms, who have what we call “minor acute illness.” In contrast to the well-studied chronic somatizing patient in whom medically unexplained symptoms1,2 are of at least 6 months’ duration,3 we define minor acute illness as unexplained symptoms of any type (eg, sore throats, minor sprains, “sinuses”) that resolve completely in less than 6 months (usually days or weeks). Although most patients would not seek care for these minor complaints, some patients with minor acute illness have exaggerated responses to common symptoms and become high users of medical care.4-8 These are probably recognized by many physicians as the “worried well.”
Our review of the literature and discussion with several experts reveal that no research group has given consideration to defining the diagnostic features of minor acute illness or to describing it over time.9,10 Not surprisingly, studies of treatment are nonexistent, and reported treatments are ineffective.5,6,11 We present preliminary research defining minor acute illness, distinguishing it from somatization and organic disease, and evaluating its persistence over time among high-use patients.
Methods
Subjects
All patients were members of a largely primary care, staff model health maintenance organization (HMO) in Lansing, Michigan (Blue Cross Network). Only computerized descriptive information in the HMO’s management information system (MIS) and data in patients’ clinical charts were involved in our study. The MIS includes administrative information on age, sex, all patient encounters with the system, primary diagnoses made at each physician/nurse practitioner/physician assistant visit (International Classification of Diseases—Ninth Revision codes), revenue codes, and charges for services. Subjects whose visits for the year were primarily because of pregnancy, substance abuse, or other recognized psychiatric problems/diagnoses (eg, bipolar disorder, eating disorder) were excluded.
Screening to identify somatizing and minor acute illness patients
We first identified all patients aged 21 to 55 years in the Lansing, Michigan, area who had at least 1 visit during 1995 to a physician, physician assistant, nurse practitioner, specialist, or emergency room; each hospitalization was counted as 1 visit. We did not use older patients, because our goal for another project was to identify chronic somatizing patients with minimal organic disease; the discovery of minor acute illness patients was an unexpected byproduct. Of 15,505 members in 1995, 5423 had 6 or more visits, and 1000 of these patients were randomly selected for further evaluation; to obtain the greatest possible sample, we arbitrarily defined 6 or more visits (65th percentile) as high users. Of the 1000, 94 were excluded because of pregnancy, substance abuse, visits for psychiatric care, or because they were employees of the HMO, and 23 were excluded because of incomplete data. We excluded patients under regular psychiatric care, because we wanted to obtain (for a treatment intervention) patients not receiving psychologic attention. The remaining 883 patients constituted the study population. Excluded patients differed from those in the study group in age, sex, and employer group but not on the amount of copay (P =.58) and relationship to the subscriber (P =.23). Excluded patients were on average younger (35.7 years vs 40.3 years, P <.001), and 88% were women as opposed to 68% for patients included in the overall study (P <.001).
Reference standard diagnoses were established by a resident physician (emergency medicine) rating the 883 charts according to specific criteria, reported previously12 and summarized in the report’s Appendix.* The rater classified patients by their primary/predominant problem for the entire year as organic disease, somatization, or minor acute illness. The designation of the primary problem was based on the largest number of visits for a problem. For example, a patient with a documented urinary infection at the first visit with 1 follow-up visit, documented pneumonia at the third visit with 2 follow-up visits, 1 visit for chronic low back pain with a negative computed tomography scan, and 2 visits for minor ligamentous strain, with no objective manifestations and no investigation, would be rated as organic for this year; similarly, a patient would be considered to have minor acute illness with 6 visits for minor complaints with no work-up and no objective manifestations of disease on examination, as well as 1 visit for documented urinary infection and 3 for diabetes mellitus. The same rule was used for follow-up ratings 1 and 2 years later, and the rater for follow-up ratings was unaware of the baseline ratings.
Organic disease was diagnosed by standard medical criteria and based on clear physical signs of disease (eg, laceration, enlarged liver) or, almost always, definitive laboratory investigation; the rater relied on expert judgment and referred to text material as needed.13 Somatization was rated when, following objectively based diagnostic evaluation (definitive testing), patients were free of organic disease that contributed significantly to at least 1 physical symptom of at least 6 months’ duration. Minor acute illness was rated when all physical symptoms were of less than 6 months’ duration, as judged by the rater from explicit mention in the chart or from observation that symptoms cleared and did not recur, and there was no documentation of an organic disease explanation for the symptom or its degree of severity. Because minor acute problems typically were not severe or disabling (in contrast to somatization), definitive testing often had not been performed. From the 1995 baseline sample of 122 somatizers and 450 minor acute patients identified by our rating procedure, we re-rated a sample of all available somatizers (N=104; 85%) and a 15% random sample of minor acute illness patients (N=66) both 1 and 2 years later.
After 10 hours of initial training, including practice rating on nonstudy charts, the rater rated 20 charts of non-study high-utilizing patients. A priori, we set an agreement rate with the trainer (one of the authors [R.C.S.]) for primary diagnosis of 90% (18 of 20 charts) before the rater began rating study patients. During the study, the trainer rated sets of 20 study charts already evaluated by the rater, once each during 1995, 1996, and 1997. The rater had high levels of agreement with the trainer throughout, varying from 90% to 95%. This level of agreement is not surprising, because the trainer trained the rater, which was also reflected in the of 0.93.
Statistical analysis
We also reviewed the 1996 and 1997 use for the same 104 somatizers identified in our initial 1995 baseline chart review of high-utilizing patients. Again, the same 15% random sample (N=66) was selected from those classified as having minor acute illness in 1995. In the follow-up years, some patients had relocated or were no longer receiving their medical care at our HMO. However, nearly 85% of the patients in our selected sample were continuously enrolled in the HMO in the 2 subsequent years of our study. Similar to chart rating, the final sample consisted of 104 somatizers and 66 patients with minor acute illness. For these patients we ascertained their status (somatization, organic disease, or minor acute illness) and their use (<6 visits; 6 visits) in 1996 and 1997. The 2 groups of patients were compared using chi-square tests for categoric variables and by t tests for continuous variables. Confidence intervals for binomial proportions were calculated by the exact method.
Results
The characteristics of 170 patients (104 somatization; 66 minor acute) studied at all data collection points are shown in Table 1. The mean age (as of 1995) was 41.3 years among somatizers versus 39.7 years among patients with minor acute illness (P =.19) The 2 groups differed only by sex, with nearly 83% of the somatizers being women, compared with 65% among minor acute illness patients (P=.009).
Among 883 high-use patients at baseline, 311 had organic diseases (35%); 122 had somatization (14%); and 450 had minor acute illness (51%) as their primary problems. No patients with initial minor acute illness diagnoses were reclassified as somatization 1 and 2 years later, and all but 2 patients had minor acute illness in 1 or both follow-up years.
The follow-up status in 1996 and 1997 of the 104 somatizers and the 66 minor acute illness patients initially rated in 1995 appears in Figure 1. It shows the (percentage) distribution of organic diseases, somatization, and minor acute illness diagnoses for 1995, 1996, and 1997, using all available data in each year. Because our rating of patients in 1 of the 3 categories followed a strict protocol (for 13 patients in 1996 and 40 patients in 1997), and because of insufficient information in their charts, we were unable to definitely ascertain their status. None of the patients with minor acute illness were reclassified as somatizers in the follow-up years, and 83% of these patients continued to have minor acute illness in 1996. All but 2 patients had minor acute illness either in 1996 or 1997 or both. Approximately 27% of the somatizers remained somatizers in 1996, 54% were rated as having minor acute illness, and 13% had organic disease. In 27% of these somatizers minor acute illness developed in the 2 subsequent years. Among patients in 1995, the probabilities of somatization for 2 and 3 consecutive years were 3.7% and 1.1%, respectively. In contrast, for minor acute illness these probabilities were 42.5% and 27%, respectively.
Use status of the groups (somatization, minor acute illness) combined is shown in Figure 2. It shows the (percentage) distribution of use (<6 visits; 6 visits) for 1996 and 1997. Approximately 57% of the somatizers were high users in 1996, compared with 29% of the minor acute illness patients. High use in either 1996 or 1997 was more prevalent among somatizers (70%) than in minor acute illness patients (45%). Persistent high use in both years among minor acute illness patients was 16.7% (95% confidence interval [CI], 8.6%-27.9%) and among somatizers 32.7% (95% CI, 23.8%-42.6%).
TABLE 1
CHARACTERISTICS OF FOLLOW-UP STUDY (N=70)
| Characteristic | Subgroup | Somatizers % (N) | Minor Acute % (N) |
|---|---|---|---|
| Age, years | 20-29 | 13.5 (14) | 9.1 (6) |
| 30-39 | 24.0 (25) | 43.9 (29) | |
| 40-49 | 51.0 (53) | 36.4 (24) | |
| 50+ | 11.5 (12) | 10.6 (7) | |
| Sex | Men | 17.3 (18) | 34.9 (23) |
| Women | 82.7 (86) | 65.2 (43) | |
| Employer | MSU | 6.7 (7) | 4.6 (3) |
| State | 28.9 (30) | 24.2 (16) | |
| GM | 22.1 (23) | 30.3 (20) | |
| Other | 42.3 (44) | 41.0 (27) | |
| Copay, $ | 0 | 58.7 (61) | 57.6 (38) |
| 5 | 28.9 (30) | 25.8 (17) | |
| 7 | 11.5 (12) | 10.6 (7) | |
| 10 | 1.0 (1) | 6.1 (4) | |
| Relationship to subscriber | Self | 59.6 (62) | 62.1 (41) |
| Spouse | 37.5 (39) | 34.9 (23) | |
| Dependent | 2.9 (3) | 3.0 (2) | |
| MSU denotes Michigan State University; GM, General Motors. | |||
FIGURE 1
FOLLOW-UP DIAGNOSES IN INTIALLY IDENTIFIED MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS
FIGURE 2
FOLLOW-UP USE PATTERNS OF INTIALLY HIGH-USE PATIENTS WITH MINOR ACUTE ILLNESS AND SOMATIZATION PATIENTS
Discussion
Among high users of care, patients with minor acute symptoms were more common than those with symptoms of somatization and organic diseases combined. On follow-up study, diagnoses of somatization often changed to minor acute status, while minor acute illness diagnoses were more persistent. Although use did not remain high in either group, regression to the mean must be considered, because we sampled only on high use in 1995.
We found no research data to compare with our results in patients with minor acute illness. However, the presumed stability and chronicity of somatization diagnoses3,14 have been questioned.14-16 For example, great variability in symptoms was seen in repeated hospitalizations of somatizers, as judged by chart review.17 Others found that only 21 of 70 cases identified as somatization disorder at baseline had the same diagnosis 12 months later and that only approximately one half of all somatization symptoms were present 1 year later.16,18
Limitations
This first preliminary study of high users with minor acute illness was limited by the shortcomings of any retrospective chart review. These include the facts that: (1) We depended on how aggressively a physician attempted to diagnose organic disease and on how completely clinicians recorded their findings; (2) Without access to patients, we were unable to identify their unique perspective or to diagnose specific somatoform disorders3 using, for example, the Diagnostic Interview Schedule,19 the World Health Organization Composite Diagnostic Interview,20 or direct patient interviews; (3) Our designation of somatization depended on identifying symptoms of 6 or more months’ duration, the minimum criterion specified for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) somatoform diagnoses3; if busy clinicians did not record duration, overcoding of minor acute status could have occurred.4 We cannot be certain that patients in either the medically unexplained group (ie, somatization, minor acute illness) did not in fact have organic diseases, because we were unable to investigate each patient ourselves from a biomedical perspective. However, during follow-up chart review, we observed no instances of an important organic disease having been missed when a diagnosis of minor acute illness or somatization status was made initially.15,21
In spite of these expected problems when chart review is the only available source of data, this research on previously unstudied patients provides a starting point for further research. Based on clinical descriptions, our observations on somatizing patients did in fact indicate that we had studied a typical chronic somatizing population (eg, those with low back pain, pelvic pain, irritable bowel syndrome). Also, others have found that chart review may be superior in identifying somatizing patients17,18 and that the DSM-IV has important shortcomings, notwithstanding the latter’s prominent present role in diagnosing conditions with medically unexplained symptoms.22,23 Further, because minor acute illness symptoms are short term, it is arguable that few minor acute patients will receive DSM-IV somatoform diagnoses. Still, as the next research step DSM-IV diagnoses should be sought to better delineate this new group, as should other standard psychiatric measures, especially for depression, anxiety, and unique personality traits.
Although psychiatric measures are needed to better define this high-use population, their absence in this initial study does not negate the importance of our findings from medical patients’ charts. They presumably reflect what patients actually reported to providers as their major reasons for seeking care, in contrast to questionnaire and lay interviewer data obtained unrelated to care seeking. Complementing our chart-based data with these standard psychiatric measures is the necessary next step.
Others have considered the problem of minor symptoms. Barsky and Borus7 seemed to distinguish short-term symptoms from the chronic symptoms of somatization and somatoform disorders by including many symptoms that often are brief and self-limited in what they called functional somatic syndromes (eg, palpitations, dizziness, lightheadedness, sore throat, and dry mouth). To avoid compounding the severe nosology problem in somatization24,25 and because the term functional somatic syndromes has been used by others to encompass all types of somatization,26,27 we are using the purely descriptive term “minor acute illness” to identify the patients reported here with short-term symptoms, recognizing that there may be considerable overlap with the group of patients identified by Barsky and Borus,7 Katon and colleagues,28 the acute and subacute somatizers of Kleinman,8 and the somatoform “not otherwise specified” category in DSM-IV.29 We prefer minor acute illness also to the common but pejorative term “worried well,” which we believe has never been defined. The “minor acute” label also has been used previously in a closely related context.30 Similar to Katon and coworkers,28 we propose that minor acute illness fits into the mild end of a multidimensional classification scheme for patients with medically unexplained symptoms—with abridged somatization disorder31 as moderate and full somatization disorder as severe.3 The latter 2 diagnoses are based on DSM-IV criteria only.
CONCLUSIONS
More research is needed to assist the field in better addressing patients with medically unexplained symptoms. The long-range goal for minor acute illness (as well as somatization) is to determine if it is a distinct and valid entity. In what is a complex task for psychiatric epidemiologists in the absence of organic disease and pathophysiologic changes,32-37 we can use the recommendations of Guze and colleagues38,39 for establishing the validity of a psychiatric diagnosis to guide us (Table 2). At this point, we can say only that there is evidence from our initial research study that we can use to describe and define minor acute illness and that it persists over 2 years (criteria 1 and 4 from Table 2). These are key determinants of validity, but they require much confirmation.38,39 Extensive work lies ahead in achieving our ultimate goal, providing effective treatment for a group that often receives inappropriate treatment, such as unnecessary antibiotics.
TABLE 2
VALIDITY CRITERIA FOR PSYCHIATRIC ENTITIES
|
| NOTE: From Guze and colleagues,38,39 who comment that we often know little about criteria 2 and 3, and a careful description must focus on criteria 4 and 5, follow-up studies, and family studies. |
Acknowledgments
Our work was supported by a generous grant from the Institute for Managed Care, Michigan State University, East Lansing.
1. Lipowski ZJ. Somatization: the concept and its clinical application. Am J Psychiatry 1988;145:1358-68.
2. Kirmayer LJ, Robbins JM. Introduction: concepts of somatization. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;1-19.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
4. Komaroff AL. ‘Minor’ illness symptoms—the magnitude of their burden and of our ignorance. Arch Intern Med 1990;150:1586-87.
5. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-66.
6. Connelly JE, Smith GR, Philbrick JT, Kaiser DL. Healthy patients who perceive poor health and their use of primary care services. J Gen Int Med 1991;6:47-51.
7. Barsky AJ, Borus JF. Functional somatic syndromes. Ann Intern Med 1999;130:910-21.
8. Kleinman A. Social origins of distress and disease—depression, neurasthenia, and pain in modern China. New Haven, Conn: Yale University Press; 1986.
9. Andersson S-O, Mattsson B, Lynoe N. Patients frequently consulting general practitioners at a primary health care centre in Sweden—a comparative study. Scand J Soc Med 1995;23:251-57.
10. Verbrugge LM, Ascione FJ. Exploring the iceberg—common symptoms and how people care for them. Med Care 1987;25:539-69.
11. Kroenke K, Arrington ME, Mangelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med 1990;150:1685-89.
12. Smith RC, Gardiner JC, Armatti S, et al. Screening for high utilizing somatizing patients using a prediction rule derived from the management information system of an HMO—a preliminary study. In press.
13. Humes HD, DuPont HL, Gardner LB, et al, eds. Kelley’s textbook of internal medicine. 4th ed. Philadelphia, Pa: Lippincott Williams and Wilkins; 2000.
14. Cloninger CR, Martin RL, Guze SB, Clayton PJ. A prospective follow-up and family study of somatization in men and women. Am J Psychiatry 1986;143:873-78.
15. Rief W, Hiller W, Geissner E, Fichter MM. A two-year follow-up study of patients with somatoform disorders. Psychosomatics 1995;36:376-86.
16. Gara MA, Escobar JI. The stability of somatization syndromes over time. Arch Gen Psychiatry 2001;58:94.-
17. Fink P. Physical complaints and symptoms of somatizing patients. J Psychosom Res 1992;36:125-36.
18. Simon GE, Gureje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry 1999;56:90-95.
19. Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health Diagnostic Interview Schedule: its history, characteristics, and validity. Arch Gen Psychiatry 1981;38:381-89.
20. Sartorius N. Composite International Diagnostic Interview (CIDI)—core version 1.1. Geneva, Switzerland: World Health Organization.
21. Kroenke K, Spitzer RL, deGruy FV, Hahn SR, Linzer M, Williams JBW, Brody D, Davies M. Multisomatoform disorder—an alternative to undifferentiated somatoform disorder for the somatizing patient in primary care. Arch Gen Psychiatry 1997;54:352-58.
22. Norquist G, Hyman SE. Advances in understanding and treating mental illness: implications for policy. Health Aff 1999;18:32-47.
23. Krueger RF. The structure of common mental disorders. Arch Gen Psychiatry 1999;56:921-26.
24. Murphy MR. Classification of the somatoform disorders. In: Bass CM, ed. Somatization: physical symptoms and psychological illness. Oxford, England: Blackwell; 1990;10-39.
25. Mayou R, Bass C, Sharpe M. Overview of epidemiology, classification, and aetiology. In: Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms. Oxford, England: Oxford University Press, 1995;42-65.
26. Kirmayer LJ, Robbins JM. Functional somatic syndromes. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;79-106.
27. Sharpe M, Mayou R, Bass C. Concepts, theories, and terminology. In: Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms. Oxford, England: Oxford University Press; 1995;1-16.
28. Katon W, Lin E, von Korff M, Russo J, Lipscomb P, Bush T. Somatization: a spectrum of severity. Am J Psychiatry 1991;148:34-40.
29. Kroenke K, Spitzer RL, deGruy FV, Swindle R. A symptom checklist to screen for somatoform disorders in primary care. Psychosomatics 1998;39:263-72.
30. Weiner JP, Starfield BH, Steinwachs DM, Mumford LM. Development and application of a population-oriented measure of ambulatory care case-mix. Med Care 1991;29:452-72.
31. Escobar JI, Swartz M, Rubio-Stipec M, Manu P. Medically unexplained symptoms: distribution, risk factors, and comorbidity. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;63-78.
32. Kovacs M, Gatsonis C. Stability and change in childhood-onset depressive disorders: longitudinal course as a diagnostic validator. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnosis. New York, NY: Raven Press, Ltd; 1989;57-73.
33. Tyrer P, Alexander J, Remington M, Riley P. Relationship between neurotic symptoms and neurotic diagnosis: a longitudinal study. J Affect Dis 1987;13:13-21.
34. Beiser M, Iacono WG, Erickson D. Temporal stability in the major mental disorders. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnosis. New York, NY: Raven Press, Ltd; 1989;77-97.
35. Andreason NC. The validation of psychiatric diagnosis: new models and approaches. Am J Psychiatry 1995;152:161-62.
36. Cloninger CR. Establishment of diagnostic validity in psychiatric illness: Robins and Guze’s method revisited. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnoses. New York, NY: Raven Press; 1989;9-16.
37. Grove WM, Andreasen NC. Quantitative and qualitative distinctions between psychiatric disorders. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnoses. New York, NY: Raven Press; 1989;127-39.
38. Guze SB. The diagnosis of hysteria: what are we trying to do? Am J Psychiatry 1967;124:491-98.
39. Robins E, Guze SB. Establishment of diagnostic validity in psychiatric illness: its application to schizophrenia. Am J Psychiatry 1970;126:983-87.
1. Lipowski ZJ. Somatization: the concept and its clinical application. Am J Psychiatry 1988;145:1358-68.
2. Kirmayer LJ, Robbins JM. Introduction: concepts of somatization. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;1-19.
3. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
4. Komaroff AL. ‘Minor’ illness symptoms—the magnitude of their burden and of our ignorance. Arch Intern Med 1990;150:1586-87.
5. Kroenke K, Mangelsdorff AD. Common symptoms in ambulatory care: incidence, evaluation, therapy, and outcome. Am J Med 1989;86:262-66.
6. Connelly JE, Smith GR, Philbrick JT, Kaiser DL. Healthy patients who perceive poor health and their use of primary care services. J Gen Int Med 1991;6:47-51.
7. Barsky AJ, Borus JF. Functional somatic syndromes. Ann Intern Med 1999;130:910-21.
8. Kleinman A. Social origins of distress and disease—depression, neurasthenia, and pain in modern China. New Haven, Conn: Yale University Press; 1986.
9. Andersson S-O, Mattsson B, Lynoe N. Patients frequently consulting general practitioners at a primary health care centre in Sweden—a comparative study. Scand J Soc Med 1995;23:251-57.
10. Verbrugge LM, Ascione FJ. Exploring the iceberg—common symptoms and how people care for them. Med Care 1987;25:539-69.
11. Kroenke K, Arrington ME, Mangelsdorff AD. The prevalence of symptoms in medical outpatients and the adequacy of therapy. Arch Intern Med 1990;150:1685-89.
12. Smith RC, Gardiner JC, Armatti S, et al. Screening for high utilizing somatizing patients using a prediction rule derived from the management information system of an HMO—a preliminary study. In press.
13. Humes HD, DuPont HL, Gardner LB, et al, eds. Kelley’s textbook of internal medicine. 4th ed. Philadelphia, Pa: Lippincott Williams and Wilkins; 2000.
14. Cloninger CR, Martin RL, Guze SB, Clayton PJ. A prospective follow-up and family study of somatization in men and women. Am J Psychiatry 1986;143:873-78.
15. Rief W, Hiller W, Geissner E, Fichter MM. A two-year follow-up study of patients with somatoform disorders. Psychosomatics 1995;36:376-86.
16. Gara MA, Escobar JI. The stability of somatization syndromes over time. Arch Gen Psychiatry 2001;58:94.-
17. Fink P. Physical complaints and symptoms of somatizing patients. J Psychosom Res 1992;36:125-36.
18. Simon GE, Gureje O. Stability of somatization disorder and somatization symptoms among primary care patients. Arch Gen Psychiatry 1999;56:90-95.
19. Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health Diagnostic Interview Schedule: its history, characteristics, and validity. Arch Gen Psychiatry 1981;38:381-89.
20. Sartorius N. Composite International Diagnostic Interview (CIDI)—core version 1.1. Geneva, Switzerland: World Health Organization.
21. Kroenke K, Spitzer RL, deGruy FV, Hahn SR, Linzer M, Williams JBW, Brody D, Davies M. Multisomatoform disorder—an alternative to undifferentiated somatoform disorder for the somatizing patient in primary care. Arch Gen Psychiatry 1997;54:352-58.
22. Norquist G, Hyman SE. Advances in understanding and treating mental illness: implications for policy. Health Aff 1999;18:32-47.
23. Krueger RF. The structure of common mental disorders. Arch Gen Psychiatry 1999;56:921-26.
24. Murphy MR. Classification of the somatoform disorders. In: Bass CM, ed. Somatization: physical symptoms and psychological illness. Oxford, England: Blackwell; 1990;10-39.
25. Mayou R, Bass C, Sharpe M. Overview of epidemiology, classification, and aetiology. In: Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms. Oxford, England: Oxford University Press, 1995;42-65.
26. Kirmayer LJ, Robbins JM. Functional somatic syndromes. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;79-106.
27. Sharpe M, Mayou R, Bass C. Concepts, theories, and terminology. In: Mayou R, Bass C, Sharpe M, eds. Treatment of functional somatic symptoms. Oxford, England: Oxford University Press; 1995;1-16.
28. Katon W, Lin E, von Korff M, Russo J, Lipscomb P, Bush T. Somatization: a spectrum of severity. Am J Psychiatry 1991;148:34-40.
29. Kroenke K, Spitzer RL, deGruy FV, Swindle R. A symptom checklist to screen for somatoform disorders in primary care. Psychosomatics 1998;39:263-72.
30. Weiner JP, Starfield BH, Steinwachs DM, Mumford LM. Development and application of a population-oriented measure of ambulatory care case-mix. Med Care 1991;29:452-72.
31. Escobar JI, Swartz M, Rubio-Stipec M, Manu P. Medically unexplained symptoms: distribution, risk factors, and comorbidity. In: Kirmayer LJ, Robbins JM, eds. Current concepts of somatization: research and clinical perspectives. Washington, DC: American Psychiatric Press, Inc; 1991;63-78.
32. Kovacs M, Gatsonis C. Stability and change in childhood-onset depressive disorders: longitudinal course as a diagnostic validator. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnosis. New York, NY: Raven Press, Ltd; 1989;57-73.
33. Tyrer P, Alexander J, Remington M, Riley P. Relationship between neurotic symptoms and neurotic diagnosis: a longitudinal study. J Affect Dis 1987;13:13-21.
34. Beiser M, Iacono WG, Erickson D. Temporal stability in the major mental disorders. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnosis. New York, NY: Raven Press, Ltd; 1989;77-97.
35. Andreason NC. The validation of psychiatric diagnosis: new models and approaches. Am J Psychiatry 1995;152:161-62.
36. Cloninger CR. Establishment of diagnostic validity in psychiatric illness: Robins and Guze’s method revisited. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnoses. New York, NY: Raven Press; 1989;9-16.
37. Grove WM, Andreasen NC. Quantitative and qualitative distinctions between psychiatric disorders. In: Robins LN, Barrett JE, eds. The validity of psychiatric diagnoses. New York, NY: Raven Press; 1989;127-39.
38. Guze SB. The diagnosis of hysteria: what are we trying to do? Am J Psychiatry 1967;124:491-98.
39. Robins E, Guze SB. Establishment of diagnostic validity in psychiatric illness: its application to schizophrenia. Am J Psychiatry 1970;126:983-87.