User login
From the Department of Neurology, University of Maryland School of Medicine, Baltimore, MD.
Abstracts
- Objective: To provide a review of psychogenic nonepileptic seizures, including a discussion of the diagnosis, treatment, and clinical significance of the disorder.
- Methods: Review of the relevant literature.
- Results: Psychogenic nonepileptic seizures are a common and potentially disabling neurologic disorder. They are most prevalent in young adults, and more commonly seen in women versus men. Certain psychosocial variables may impact the development of the condition. The diagnosis is made through a detailed history and observation of clinical events in conjunction with video EEG monitoring. Neuropsychological testing is an important component in the evaluation. Treatment includes establishment of an accurate diagnosis, management of any underlying psychiatric diagnoses, and regular follow-up with a neurologist or trained care provider.
- Conclusion: Psychogenic nonepileptic seizures represent a complex interaction between neurologic and psychological factors. Obtaining an accurate diagnosis through the use of video EEG monitoring and clinical observation is an important initial step in treatment and improved quality of life in this patient population.
Psychogenic nonepileptic seizures (PNES) are commonly encountered in outpatient specialty epilepsy clinics as well as inpatient epilepsy monitoring units. They comprise approximately 20% of all refractory seizure disorders referred to specialty epilepsy centers [1–4]. PNES are thought to be psychological in origin as opposed to arising from abnormal electrical discharges as in epileptic seizures. PNES may be more frequent and disabling than epileptic seizures, and patients with PNES may report worse outcomes [5,6]. Increased utilization of long-term video EEG monitoring along with greater recognition of psychogenic neurologic disorders has allowed for improved diagnosis of PNES. However, many diagnostic and therapeutic challenges remain. There are often delays in obtaining an accurate diagnosis, and optimal management remains challenging, often leading to inappropriate, ineffective, and costly treatment, sometimes for many years [6–8].
Epidemiology
PNES are seen across the spectrum of age-groups, from children [9,10] to elderly persons, but they most often occur in young adults between the ages of 15 to 35 years [1,8]. Caution should be used when considering this diagnosis in infants or young children, in whom it is more common to see physiologic events that may mimic epileptic seizures, including gastroesophageal reflux, shuddering, night terrors, or breath holding spells [1,9,10].
PNES are prevalent within epilepsy practices. Patients with PNES comprise approximately 5% to 20% patients thought to have intractable epilepsy seen in outpatient centers, and within epilepsy monitoring units they account for 10% to 40% of patients [1,2,6,8]. A population-based study approximates the incidence of PNES at 1.4 per 100,000 people and 3.4 per 100,000 people between the ages of 15 to 24 years [4].
There is a female preponderance in PNES, which is similar to other conversion and somatoform disorders. Overall, women comprise approximately 70% to 80% of patients with the PNES diagnosis [1,2,6]. There are psychosocial variables that are seen in some patients with this disorder. An important factor that has been described is past history of sexual or physical abuse. In one series, there was a history of sexual abuse in almost 25% of patients with PNES, and history of either sexual abuse, physical abuse, or both in 32% of patients [11]. A history of sexual and/or physical abuse is not exclusive to these patients, and can certainly be seen in patients with epilepsy as well. For example, in a control population of epilepsy patients, there was a reported rate of past sexual or physical abuse approaching 9% [12].
A prior history of head trauma, often of a relatively mild degree, has been described as a potential inciting factor for some cases of PNES [6,13]. In the literature, studies report that as many as 20% of PNES patients attributed their seizures to head trauma, often rather mild head trauma [6,14].
Historcial Context
Historically, what today are called PNES originate with the concept of hysteria, a medical diagnosis in women that can be traced to antiquity [15,16]. By the late 1800s, one of the founders of neurology, Jean Charcot, established hysterical seizures as an important clinical entity with his detailed, elegant descriptions of patients. Charcot formulated clinical methods for distinguishing hysteria and particularly hysterical seizures from epilepsy. He presumed that hysteria and epilepsy were closely related, and he termed seizures due to hysteria as “hysteroepilepsy” or “epileptiform” hysteria. Charcot proposed that hysterical seizures were organic disorders of the brain, like other forms of seizures and epilepsy, and emphasized their relation to disturbance of the female reproductive system [17,18]. Charcot utilized techniques such as manipulation of “hysterogenic zones” and ovarian compression as well as suggestion to both treat and provoke hysteria and hysterical seizures, which he described and documented [17,18]. One of Charcot’s most celebrated students, Sigmund Freud, observed Charcot’s demonstrations but drew different conclusions. He theorized that hysteria and hysterical seizures were not organic disorders of the brain as Charcot proposed, but were rather emotional disorders of the unconscious mind due to repressed energies or drives. Based largely the theories of Freud and Charcot, individuals with hysteria were distinguished from those with epilepsy, with hysterical seizures related to psychological dysfunction while epileptic seizures were associated with physical or organic brain disorders [15,16].
With the introduction of EEG recording in the 1930s, it became possible to characterize epilepsy as an electrical disorder of the brain with associated EEG changes and more effectively distinguish it from hysterical seizures, which did not have such abnormalities. In addition, in the first half of the 20th century, the nature of hysteria as seen and diagnosed by physicians seemed to change. The dramatic, theatrical convulsions described by Charcot and his contemporaries appeared less commonly, while disorders such as chronic pain seemed to increase [1,19].
However, by the 1960s, several reports confirmed that hysterical seizures were actually still prevalent. Newer terms like “pseudoseizures” were used to describe these disorders because the term “hysteria” was thought to be somewhat derogatory, anti-feminist, and antiquated [20,21]. In the 1970s and thereafter, with the increasing availability of video EEG monitoring and growth of inpatient epilepsy monitoring units, it was discovered that these hysterical, pseudo-, or what were also by then termed psychogenic seizures, were actually still common [1,22].
More recently, it has been recognized that the pendulum in some cases may have swung too far in regard to the diagnosis of this disorder. Some rare patients with seizures initially diagnosed as PNES may actually have forms of epileptic seizures such as frontal lobe epilepsy or related physiological disorders rather than psychogenic causes for their episodes [1,23]. These types of epileptic seizures can be very difficult to diagnose properly unless one appreciates how they present and manifest and remains vigilant for them during evaluation [1,23].
Terminology
There is an ongoing debate regarding the appropriate terminology for psychogenic events, and there is no uniform standardized definition or classification at this time. The term that is currently preferred within the epilepsy community for seizures of psychological origin that are thought to be associated with conversion, somatization, or dissociative disorders is “psychogenic nonepileptic seizures” (PNES). This terminology is felt to be non-disparaging and more neutral as compared with other terms such as pseudoseizures, which were previously favored. Nonepileptic seizures or nonepileptic events are broader terms meant to incorporate both physiologic and psychological causes for disorders that are mistaken for epilepsy. PNES are widely defined as paroxysmal events that appear similar to epileptic seizures but are not due to abnormal electrical discharges in the brain and as noted, are typically thought to be related or caused by conversion, somatization, or dissociative disorders.
Physiologic nonepileptic events are another category of physical disorders that may be mistaken for epilepsy. The underlying causes differ between age-groups, and can include conditions such as cardiac arrhythmias, migraine variants, syncope, or metabolic abnormalities. Physiologic nonepileptic seizures account for only a small proportion of all patients with nonepileptic seizures or events [1]. In general, any patient with a psychological disorder that causes symptoms that are mistaken for epilepsy can be said to have PNES.
Clinical Characteristics And Presentation
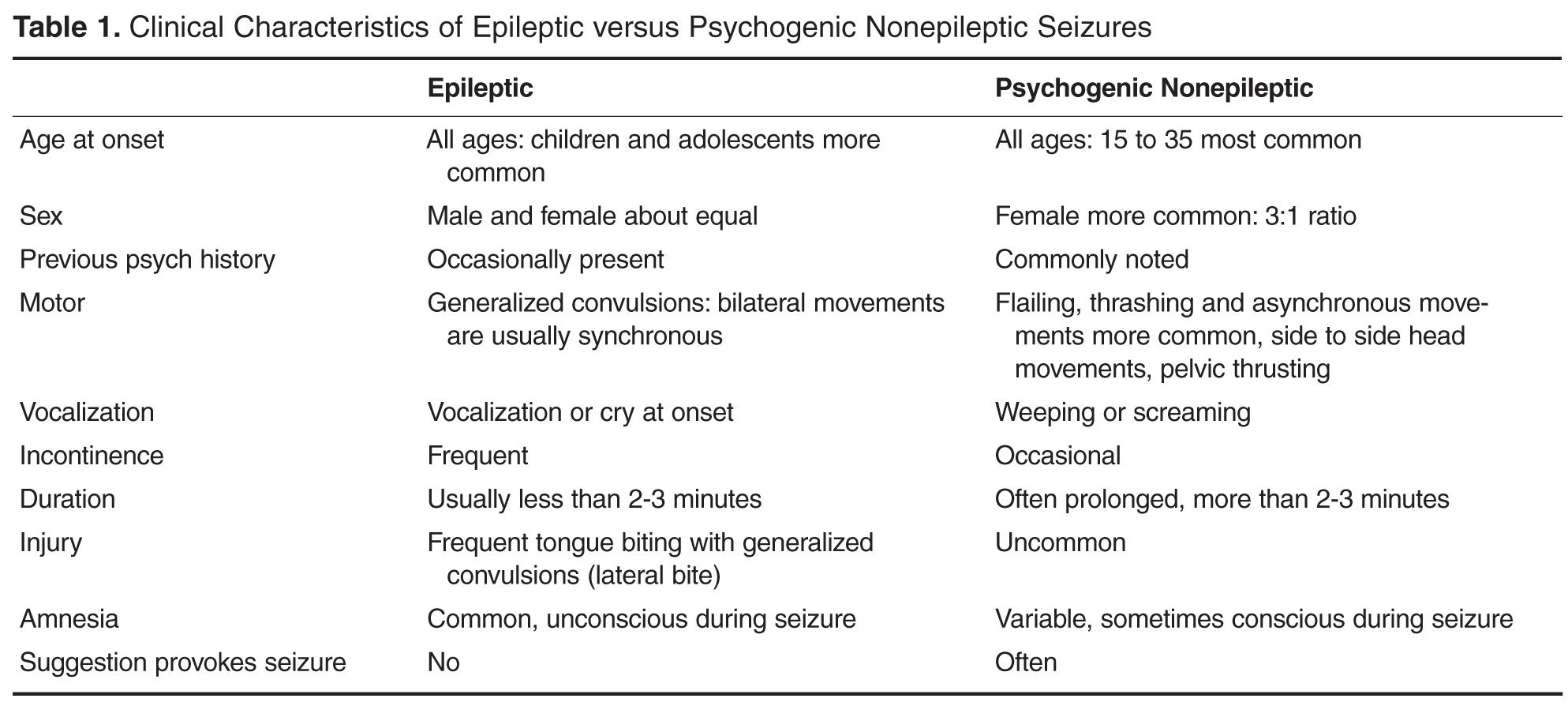
The duration of PNES is often significantly longer than that seen in epileptic seizures, which usually last less than 3 minutes, excluding the postictal period. PNES may also exhibit waxing and waning convulsive activity, although this finding can certainly be seen in epileptic seizures as well. PNES may be shown to have distractibility with external stimuli. Additionally, the movements in PNES may appear asymmetric, asynchronous, or purposeful, although this is not diagnostic for this disorder. This may contrast with the well-defined, synchronous tonic-clonic activity typically seen in epileptic seizures [1,24,25]. Back arching and pelvic thrusting movements can also be seen in PNES. Despite these differences, it may still be challenging to distinguish the semi-purposeful behaviors of PNES from the automatisms of certain focal epileptic seizures. The often bizarre-appearing, hypermotor activity that can be seen in frontal lobe seizures is often especially difficult to differentiate from PNES [1,23].
Another important consideration is that consciousness is preserved in PNES, while consciousness and responsiveness are frequently impaired in epileptic seizures. Patients with PNES are often apparently unresponsive during events, although there is no true impairment of awareness. Other characteristics that are more commonly seen in PNES are crying and eye closure [26]. Self-injury and incontinence may be reported, but they are less often clearly witnessed or documented [27,28]. Additionally, although patients may at times appear to be asleep at seizure onset, EEG recordings document the patient to actually be asleep in less than 1% of cases [29]. While epileptic seizures often respond well to antiepileptic medications, PNES characteristically do not [1,3,6,8].
In certain situations, provocation maneuvers may be utilized in order to reproduce PNES in patients undergoing EEG monitoring. In comparison to epileptic seizures, suggestion and emotional stimuli are more likely to trigger psychogenic events [1]. Methods utilized to provoke PNES may include saline injections, placement of a tuning fork on the head or body, or even hypnosis, when a suggestion is concurrently provided that such maneuvers can trigger the patient’s seizures [1,30,31]. When evaluating seizures that are provoked in such a manner, it is important to consider whether or not the event captured is in fact a typical event for the patient, or whether the provocation has uncovered a different, atypical event. Given that PNES and epileptic seizures can co-exist within the same patient, care should be taken to avoid making a diagnosis based on capturing an atypical event, or capturing only a subset of a patient’s seizure types. This could result in failure to make an accurate and thorough diagnosis [23]. There is debate regarding the ethics of provoking seizures by way of suggestion. Some members of the epilepsy community feel that provoking seizures through suggestion is inherently deceitful, and therefore can damage the physician-patient relationship. Others assert that such provocative testing can be undertaken in an honest manner, and can ultimately help achieve an accurate diagnosis for the patient [32].
As previously mentioned, there is a proportion of patients who have co-existing epileptic seizures and PNES, and obtaining an accurate diagnosis can be especially challenging in this group. Studies have reported that around 10% to 40% of patients with PNES also have epilepsy [1,22,23,33]. Care must be taken to distinguish between differences in seizure types and if necessary, video EEG monitoring may be needed to capture both seizure types for an accurate diagnosis. This testing can then be useful in education with families and caregivers who may be shown the videos with consent from the patient in order to guide future care.
Evaluation And Diagnosis
As in much of neurology, a thorough history, along with detailed clinical observation remains essential in the diagnosis of patients with PNES and for distinguishing these events from epilepsy. Video EEG monitoring of seizures is a key adjunct to the history and clinical observation in diagnosing this condition [1,2]. Long-term video EEG monitoring is considered the “gold standard” in the characterization and differential diagnosis of seizures. Additional potentially helpful diagnostic techniques include video EEG-monitored seizure provocation, serum prolactin levels, single photon emission computed tomography, and neuropsychological testing.
Video EEG Monitoring
![]()
EEG monitoring for characterization of clinical events can be conducted on an ambulatory or outpatient basis or in dedicated inpatient epilepsy monitoring units. Ambulatory monitoring can be useful in the case of patients who report seizures that are more frequent in their home environment or in patients with frequent events. If events are infrequent, then inpatient monitoring may be more efficacious [1]. With longer-term inpatient monitoring, antiepileptic medications can be withdrawn in a supervised setting, in order to lower the seizure threshold as well as to safely discontinue medications that may not be necessary. Such medication titrations are typically not safe in an unsupervised outpatient setting. Some ambulatory EEG monitoring systems do allow for simultaneous video and EEG recording. However, an advantage to inpatient monitoring, which is not afforded in the outpatient setting, is the ability for nursing staff or physicians to perform clinical testing during events to assess for patient responsiveness and other features. Additionally, with inpatient monitoring, EEG technicians can routinely assess for any technical problems with the electrodes or recording system.
Another benefit of video EEG monitoring is that the state (waking, drowsy, or asleep) of the patient at the onset of an event can be established. While epileptic seizures can arise from any state, PNES most often occur from wakefulness. Patients with PNES may appear to be asleep at the onset of events, and they may report seizures from sleep. Video EEG monitoring can help to establish the waking or sleep state of the patient that may aid in diagnosis [29].
Prolactin Levels
Serum prolactin levels may be helpful in the diagnosis of PNES [35,36]. Following generalized tonic-clonic or complex partial epileptic seizures, the serum prolactin can rise from two to threefold to five to tenfold [37]. The maximal rise in serum prolactin occurs in the initial 20 to 60 minutes after the seizure [35–37]. A similar rise in serum prolactin would not be expected in PNES. Although prolactin levels may have some utility in diagnosis, they are not currently routinely ordered as part of a standard admission to most inpatient epilepsy monitoring units. This may be due in part to the fact that false-positive and false-negative results can occur with these levels [37–39]. For example, there may not be a rise in the prolactin level after a simple partial seizure or more subtle complex partial seizure.
Neuropsychological Testing
Neuropsychological testing is also a key component in the evaluation and diagnosis of PNES. Ideally, a mental health provider with a background in psychological assessment and neuropsychological intervention for patients with psychogenic disorders would perform the evaluation [40,41].
The goal of the evaluation should not solely focused on whether the patient suffers from nonepileptic or epileptic seizures. An epileptologist upon review of clinical, electrographic, and neuropsychological data better makes this determination. Moreover, neuropsychological testing cannot in itself either diagnose or exclude the possibility that a seizure disorder is nonepileptic because of the considerable overlap between epileptic and nonepileptic test results [40,41]. Neuropsychological evaluations aid this assessment by (1) determining the potential or likelihood of significant contributing psychopathology or cognitive difficulties, (2) defining the nature of the associated psychological or psychosocial issues, and (3) assessing how a patient might benefit from various psychologically based interventions [1]. The testing may identify psychological problems that can guide treatment after diagnosis.
Delays in Diagnosis
Correct and prompt diagnosis is essential for patients with PNES as is appropriate referral to a knowledgeable trained mental health professional. On average, patients with PNES are diagnosed 7.2 years after manifestation (SD 9.3 years), with mean delay of 5 to 7 years. Younger age, interictal epileptiform potentials in the EEG, and anticonvulsant treatment are associated with longer delays [42,43]. Delays are also thought to occur because of problems with “ownership” of these patients. Although typically neurologists are involved in the diagnosis of PNES, often using video EEG monitoring done in an inpatient setting, the next step is often a referral to a psychiatrist or mental health care provider. There are sometimes delays in the initial referral to the neurologist, delays in referral to specialists for video EEG testing, and also to the physicians, psychologists or social workers who may provide treatment. Another disconnect can occur if patients are “lost to follow-up” if they receive a referral for mental health care and either do not follow up on this on their own, or if the reason for this care is not fully explained. In addition, many mental health professionals are not trained in the evaluation and treatment of psychogenic symptoms and may even feel uncomfortable in dealing with these patients [13,44].
Many studies have been suggestive that delays in diagnosis may result in poorer outcomes [45,46], while other studies have suggested that patients who have an acute diagnosis of PNES upon presentation may do particularly well [8,47–49]. Some of the most recent large outcome studies suggest that there may be no worsening of outcome associated with delays in diagnosis and that outcome was predicted by other factors [50–52].
Management
Management of patients with PNES is similar to that for patients with other types of so-called abnormal illness behavior, although there remains a relative paucity of evidence for specific treatment strategies for PNES [1]. The first consideration should be the manner in which the diagnosis of PNES is presented to the patient and family. It is important to be honest with the patient and demonstrate a positive approach to the diagnosis [53]. The physician should emphasize as favorable or good news the fact that the patient does not have epilepsy, and should also stress that the disorder, although serious and "real," does not require treatment with antiepileptic medications and that once stress or emotional issues are resolved, the patient has the potential to gain better control of these events [1,54,55]. Nevertheless, not all patients readily accept the diagnosis or this type of approach. Some patients may seek other opinions, and this should not be discouraged. An adversarial relationship with the patient should be avoided. The patient should be encouraged to return if desired, and records should be made available to other health care providers to avoid duplication of services.
After the diagnosis of PNES is presented, supportive measures should be initiated. PNES patients may benefit from education and support that can be provided by the neurologist or primary care physician [1]. If the neuropsychological assessment suggests a clinical profile that requires a professional mental health intervention, then an appropriate referral should be made. Regular follow-up visits for the patient with the neurologist are useful even if a mental health professional is involved [49,56]. This allows the patient to get medical attention without demonstrating illness behavior. Patient education and support are stressed at these visits. Because family issues are often important contributing factors, physicians should consider involving family members in visits with consent of the patient [1].
A variety of treatment strategies are employed for the management of PNES including cognitive behavioral therapy (CBT), group and family therapy, antidepressant medication, and other forms of rehabilitation [5,57,58]. A 2007 Cochrane review that identified 608 references for non-medication PNES treatments found that only 3 studies met criteria for a randomized controlled trial. One of the more recently favored treatment options for PNES that has been applied to the treatment of various somatoform disorders and other psychiatric disorders in the past is CBT [57,59,60]. This form of psychotherapy can be administered by trained personnel in a time-limited fashion using defined protocols. The basis of this treatment is that the patient learns to increase awareness of their dysfunctional thoughts and learns new ways to respond to them [57,58]. To date, several groups have reported results of nonrandomized trials as well as case reports and case series which have established the utility of this treatment. There have been reports of significant reductions in seizure frequency and this treatment strategy appears very promising [61–65]. Preliminary randomized controlled trials have also been piloted and are also suggestive that this may be a validated treatment approach [66].
Prognosis
The outcomes of patients with PNES vary. Long-term follow-up studies show that about half of all patients with PNES function reasonably well following their diagnosis. However, only approximately one-third of patients will completely stop having seizures or related problems, and approximately 50% percent have poor functional outcomes [1,2,50]. When the diagnosis of PNES is based on reliable criteria such a video EEG monitoring, misdiagnosis is unlikely. Instead, the usual cause for a poor outcome is related to a patient’s chronic psychological and social problems[1,8,22,50].
It is noteworthy that children with PNES appear to have a much better prognosis than adults [9,10]. In fact, the etiology in children may be related more to transient stress and coping disorders, while adults are more likely to have PNES within the context of more chronic psychological maladjustment, such as personality disorders [10]. Another factor that accounts for the better outcomes in children is that they are usually properly diagnosed earlier in the course of their disorder [9,10].
Patients with milder psychopathology respond better to supportive educational or behavioral therapeutic approaches. In contrast, patients with more severe psychopathology and factitious disorders more often have associated chronic personality problems and correspondingly, a poorer prognosis [1,50]. Also it appears that patients who continue to be followed by the diagnosing neurologist or center do better than patients who are not seen after diagnosis [49,67]. As knowledge about the nature of PNES and their associated psychopathology is gained, better treatment strategies can be developed that will improve the care and prognosis of these difficult and challenging patients.
A large study of 164 patients who were followed for 10 years were considered to have “poor outcome” in general but favorable factors included higher education, younger age of onset and diagnosis, and less “dramatic” attacks, defined as lack of “positive motor features, no ictal incontinence or tongue biting.” These findings were consistent with prior studies [52,68].
In addition, the patients who tended to have less seizures and do better long term, had less somatoform and dissociative symptoms on psychometric testing [51]. These findings are often explained by the theory that patients who do not do well have poor coping strategies to deal with stress and anxiety and that in a sense, these patients have emotional dysregulation.
Special Issues
Coexisting Epileptic and Psychogenic Nonepileptic Seizures
A complicating factor in diagnosis is that both PNES and epileptic seizures may occur in a single patient. Indeed, approximately 10% to 40% of patients identified to have PNES also have been reported to have epileptic seizures [1,23,33,56]. There are several possible explanations for this. Some patients with epilepsy may learn that seizures result in attention and fill certain psychological needs. Alternatively, they may have concomitant neurologic problems, personality disorders, cognitive deficits, or impaired coping mechanisms that predispose them to psychogenic symptoms [69–71]. Fortunately, in such patients with combined seizure disorders, the epileptic seizures are usually well controlled or of only historical relevance at the time a patient develops PNES [1,22,23,33,72–74].
In other patients, both epileptic and PNES may start simultaneously, making management even more complex. In such patients, we have found it particularly helpful to focus on the semiology of seizure manifestations as recorded by video EEG monitoring to distinguish PNES from the epileptic seizures. We then direct our treatment of the patient according to the semiology manifesting at that time. We also have found it useful to show the videos of seizures to family members or caregivers with patient consent to help them understand how to respond best to a patient’s symptoms when epileptic and PNES co-exist.
Misdiagnosis of Psychogenic Nonepileptic Seizures
Sometimes events that are initially diagnosed as nonepileptic actually prove to be epileptic. Such events can be called “pseudo-pseudo” or “epileptic-nonepileptic” seizures [1]. Frontal lobe seizures in particular may not be associated with significant EEG changes ictally and therefore misdiagnosed as PNES [23,75,76]. Clinical presentation and proper diagnosis of these types of events warrant emphasis.
Notable manifestations of frontal lobe seizures that may easily be confused with hysterical behavior include shouting, laughing, cursing, clapping, snapping, genital manipulation, pelvic thrusting, pedaling, running, kicking, and thrashing [23,75–77]. Not all of these behaviors are specific for frontal lobe seizures. For example, bicycling leg movements have also been reported in seizures originating from the temporal lobe [78].
Summary
PNES represent a common yet challenging problem within neurology. This is due to the difficulty in diagnosis as well as lack of effective and widely available treatment options. Overall outcomes of patients with PNES vary, and may relate to an individual patient’s chronic psychological and social problems. However, an accurate and timely diagnosis remains critical and can help provide direction for implementing appropriate treatment.
Corresponding author: Jennifer Hopp, MD, Department of Neurology, University of Maryland Medical Center, Room S12C09, 22 South Greene Street, Baltimore, MD 21201, [email protected].
Financial disclosures: None.
1. Krumholz A. Nonepileptic seizures: diagnosis and management. Neurology 1999;S76–83.
2. Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–6.
3. Lesser RP. Psychogenic seizures. Neurology 1996;46:1499–1507.
4. Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:857–62.
5. Szaflarski JP, Szaflarski M, Hughes C, et al. Psychopathology and quality of life: psychogenic non-epileptic seizures versus epilepsy. Med Sci Monit 2003 9:CR113–8.
6. Barry E, Krumholz A, Bergey C, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31.
7. Pakalnis A, Drake ME, Phillips B. Neuropsychiatric aspects of psychogenic status epilepticus. Neurology 1991;41;1104–6.
8. Walzack TS, Papacostas S, Williams DT, et al. Outcome after the diagnosis of psychogenic nonepileptic seizures. Epilepsia 1995;36:1131–7.
9. Metrick ME, Ritter FJ, Gates JR, et al. Nonepileptic events in childhood. Epilepsia 1991;32:322–8.
10. Wyllie E, Friedman D, Luders H, et al. Outcome of psychogenic seizures in children and adolescents compared to adults. Neurology 1991;41:742–4.
11. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5.
12. Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993; 43:1950–3.
13. LaFrance WC Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45 Suppl 2:15–21.
14. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82.
15. Slavney PR. Perspectives on hysteria. Baltimore: Johns Hopkins University Press; 1990.
16. Veith I. Hysteria: the history of a disease. Chicago: University of Chicago Press; 1965.
17. Goetz CG. Charcot the clinician. The Tuesday lessons. New York: Raven Press; 1987.
18. Massey EW, McHenry LC. Hysteroepilepsy in the nineteenth century: Charcot and Gowers. Neurology 1986;36:65–7.
19. Zeigler FJ, Imboden JB, Meyer E. Contemporary conversion reactions: a clinical study. Am J Psychiatry 1960;116:901–10.
20. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology 1964;14:41–9.
21. Diagnostic and statistical manual of mental disorders. DSM-IV 4th ed. American Psychiatric Association. Washington, DC; 1995.
22. Krumholz A, Niedermeyer, E. Psychogenic seizures: a clinical study with follow-up data. Neurology 1983; 33:498-502.
23. Krumholz A, Ting T. Co-existing epileptic and nonepileptic seizures. in imitators of epilepsy. 2nd ed. In: Kaplan PW, Fisher RS, editors. New York: Demos Medical Publishing; 2005:261–76.
24. Gates JR, Ramani V, Whalen S, Loewenson R. Ictal characteristics of pseudoseizures. Arch Neurol 1985;42:1183–87.
25. Leis AA, Ross MA, Summers AK. Psychogenic seizures: Ictal characteristics and diagnostic pitfalls. Neurology 1992;42:95–9.
26. Walczak TS, Bogolioubov. Weeping during psychogenic nonepileptic seizures. Epilepsia 1996;37:207–10.
27. Bergen D, Ristanovic R. Weeping is a common element during psychogenic nonepileptic seizures. Arch Neurol 1993;50:1059–60.
28. Peguero E, Abou-Khalil B, Fakhoury, Mathews G. Self-injury and incontinence in psychogenic seizures. Epilepsia 1995;36:586–91.
29. Orbach D, Ritaccio A, Devinsky O. Psychogenic, nonepileptic seizures associated with video-EEG-verified sleep. Epilepsia 2003;44:64–8.
30. Walczak TS, Williams DT, Berton W. Utility and reliability of placebo infusion in the evaluation of patients with seizures. Neurology 1994;44:394–99.
31. Bazil CW, Kothari M, Luciano D, et al. Provocation of nonepileptic seizures by suggestion in a general seizure population. Epilepsia 1994;35:768–70.
32. Devinsky O, Fisher RS. Ethical use of placebos and provocative testing in diagnosing nonepileptic seizures. Neurology 1996;47:866–70.
33. Lesser RP, Lueders H, Dinner DS. Evidence for epilepsy is rare in patients with psychogenic seizures. Neurology 1983; 33:502–4.
34. Barre MA, Burnstine TH, Fisher RS, Lesser RP. Electroencephalographic changes during simple partial seizures. Epilepsia 1994;35:715–20.
35. Trimble MR. Serum prolactin levels in epilepsy and hysteria. BMJ 1978;2:1682.
36. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985; 35:31–5.
37. Pritchard PB, Wannamaker BB, Sagel J, et al. Endocrine function following complex partial seizures. Ann Neurol 1983;14:27–32.
38. Malkowicz DE, Legido A, Jackel RA, et al. Prolactin secretion following repetitive seizures. Neurology 1995;45:448–52.
39. Oribe E, Rohullah A, Nissenbaum E, Boal B. Serum prolactin concentrations are elevated after syncope. Neurology 1996;47:60–2.
40. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184–8.
41. Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI and neuropsychological assessments of psychogenic and epileptic seizure patients. Epilepsia 1989;30:339–47.
42. DeTimary P, Fouchet P, Sylin M, et al. Non–epileptic seizures: delayed diagnosis in patients presenting with electroencephalographic (EEG) or clinical signs of epileptic seizures. Seizure 2002;11:193–7.
43. Reuber M, Fernandez G, et al. Diagnostic delay in psychogenic nonepileptic seizures. Neurology 2002;58:493–5.
44. Rosenbaum DH, et al. Outpatient multidisciplinary management of non-epileptic seizures. In: Rowan AJ, Gates Jr, editors. Non-epileptic seizures. 1st ed. Stoneham, MA: Butterworth-Heinemann; 1993:275–83.
45. Lempert T, Schmidt D. Natural history and outcome of psychogenic seizures: a clinical study in 50 patients. J Neurol 1990;237:35–8.
46. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41:1330–4.
47. Buchanan N, Snars J. Pseudoseizures (non epileptic attack disorder): clinical management and outcome in 50 patients. Seizure 1993;2:141–6.
48. Kanner AM. More controversies on the treatment of psychogenic pseudoseizures: an addendum. Epilepsy Behav 2003;4:360–4.
49. Aboukasm A, Mahr G, Gahry BR, et al. Retrospective analysis of the effects of psychotherapeutic interventions on outcomes of psychogenic nonepileptic seizures. Epilepsia 1998;39:470–3.
50. Reuber M, Pukrop T, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11.
51. McKenzie P, Oto M, Russell A, Pelosi A, Duncan R. Early outcomes and predictors in 260 patients with psychogenic nonepileptic seizures (PNES). Neurology 2010;74:64–9.
52. Kanner AM, Parra J, Frey M, et al. Psychiatric and neurologic predictors of psychogenic pseudoseizure outcome. Neurology 1999;53:933–8.
53. Shen W, Bowman ES, Markand ON. Presenting the diagnosis of pseudoseizure. Neurology 1990; 40:756–9.
54. Friedman JH, LaFrance Jr WC. Psychogenic disorders: the need to speak plainly. Arch Neurol 2010;67:753–5.
55. LaFrance Jr WC. Psychogenic nonepileptic “seizures” or “attacks”? It’s not just semantics: “Seizures.” Neurology 2010;75: 87–8.
56. Ramsay RE, Cohen A, Brown MC. Coexisting epilepsy and non-epileptic seizures. In: Non-epileptic seizures. Butterworth-Heinemann; 1998:47–54.
57. Stone J, Carson A, Sharpe M. Functional symptoms in neurology: management. J Neurol Neurosurg Psychiatry. 2005;6(Suppl 1):i13–i21.
58. LaFrance WC Jr, Bjornaes H. Designing treatment plans based on etiology of psychogenic nonepileptic seizures. In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s nonepileptic seizures. 3rd ed. New York: Cambridge University Press; 2010:266–80.
59. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 200;69:205–15.
60. Kroenke K. Efficacy of treatment of somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007:69:881–8.
61. LaFrance WC Jr, Miller IW, Ryan CE, et al. Cognitive behavioral therapy for psychogenic nonepileptic seizures. Epilepsy Behav 2009;14:591–6.
62. Chalder T. Non-epileptic attacks: a cognitive behavioral approach in a single case with a four-year follow-up. Clin Psychol Psychother 1996;3:291–7.
63. Betts T, Duffy N. Non-epileptic attack disorder (pseudoseizures) and sexual abuse: a review. In: Gram L, Johannessen SI, Osterman PE, et al, editors. Pseudo-epileptic seizures. Petersfield, UK: Wrightson Biomedical Publishing; 1993:55–66.
64. Lesser RP. Treatment and outcome of psychogenic nonepileptic seizures. Epilepsy Currents 2003;3:198–200.
65. Ramani V. Review of psychiatric treatment strategies in non-epileptic seizures. In: Rowan AJ, Gates JR, eds. Non-epileptic Seizures. 1st ed. Stoneham, MA: Butterworth Heinemann; 1993:259–67.
66. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94.
67. Bennet C, So NM, Smith WB, Thompson K. Structured treatment improves the outcome of nonepileptic events. Epilepsia 1997;38(Suppl 8):214.
68. McDade G, Brown SW. Non-epileptic seizures: management and predictive factors of outcome. Seizure 1992;1:7–10.
69. Bowman ES. Etiology and clinical course of pseudoseizures: relationship to trauma, depression, and dissociation. Psychosomatics 1993;34:333–42.
70. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63.
71. Vanderzant CW, Giordani B, Berent S, et al. Personality of patients with pseudoseizures. Neurology 1986;36:664–8.
72. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001; 57:915–7.
73. Glosser G, Roberts D, et al. Nonepileptic seizures after resective epilepsy surgery. Epilepsia 1999; 40:1750–4.
74. Reuber M, Kral T. New-onset psychogenic seizures after intracranial neurosurgery. Acta Neurochir (Wien) 2002; 144:901–7.
75. Williamson P, Spencer D, Spencer S, et al. Complex partial seizures of frontal lobe origin. Ann Neurol 1985;18:497–504.
76. Saygi S, Katz A, Marks D, et al. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology 1992;42:1274–7.
77. Waterman K, Purves S, Kosaka B, et al. An epileptic syndrome caused by mesial frontal lobe seizure foci. Neurology 1987; 37:577–82.
78. Sussman N, Jackel R, Kaplan L, et al. Bicycling movements as a manifestation of complex partial seizures of temporal lobe origin. Epilepsia 1989;30:527–31.
From the Department of Neurology, University of Maryland School of Medicine, Baltimore, MD.
Abstracts
- Objective: To provide a review of psychogenic nonepileptic seizures, including a discussion of the diagnosis, treatment, and clinical significance of the disorder.
- Methods: Review of the relevant literature.
- Results: Psychogenic nonepileptic seizures are a common and potentially disabling neurologic disorder. They are most prevalent in young adults, and more commonly seen in women versus men. Certain psychosocial variables may impact the development of the condition. The diagnosis is made through a detailed history and observation of clinical events in conjunction with video EEG monitoring. Neuropsychological testing is an important component in the evaluation. Treatment includes establishment of an accurate diagnosis, management of any underlying psychiatric diagnoses, and regular follow-up with a neurologist or trained care provider.
- Conclusion: Psychogenic nonepileptic seizures represent a complex interaction between neurologic and psychological factors. Obtaining an accurate diagnosis through the use of video EEG monitoring and clinical observation is an important initial step in treatment and improved quality of life in this patient population.
Psychogenic nonepileptic seizures (PNES) are commonly encountered in outpatient specialty epilepsy clinics as well as inpatient epilepsy monitoring units. They comprise approximately 20% of all refractory seizure disorders referred to specialty epilepsy centers [1–4]. PNES are thought to be psychological in origin as opposed to arising from abnormal electrical discharges as in epileptic seizures. PNES may be more frequent and disabling than epileptic seizures, and patients with PNES may report worse outcomes [5,6]. Increased utilization of long-term video EEG monitoring along with greater recognition of psychogenic neurologic disorders has allowed for improved diagnosis of PNES. However, many diagnostic and therapeutic challenges remain. There are often delays in obtaining an accurate diagnosis, and optimal management remains challenging, often leading to inappropriate, ineffective, and costly treatment, sometimes for many years [6–8].
Epidemiology
PNES are seen across the spectrum of age-groups, from children [9,10] to elderly persons, but they most often occur in young adults between the ages of 15 to 35 years [1,8]. Caution should be used when considering this diagnosis in infants or young children, in whom it is more common to see physiologic events that may mimic epileptic seizures, including gastroesophageal reflux, shuddering, night terrors, or breath holding spells [1,9,10].
PNES are prevalent within epilepsy practices. Patients with PNES comprise approximately 5% to 20% patients thought to have intractable epilepsy seen in outpatient centers, and within epilepsy monitoring units they account for 10% to 40% of patients [1,2,6,8]. A population-based study approximates the incidence of PNES at 1.4 per 100,000 people and 3.4 per 100,000 people between the ages of 15 to 24 years [4].
There is a female preponderance in PNES, which is similar to other conversion and somatoform disorders. Overall, women comprise approximately 70% to 80% of patients with the PNES diagnosis [1,2,6]. There are psychosocial variables that are seen in some patients with this disorder. An important factor that has been described is past history of sexual or physical abuse. In one series, there was a history of sexual abuse in almost 25% of patients with PNES, and history of either sexual abuse, physical abuse, or both in 32% of patients [11]. A history of sexual and/or physical abuse is not exclusive to these patients, and can certainly be seen in patients with epilepsy as well. For example, in a control population of epilepsy patients, there was a reported rate of past sexual or physical abuse approaching 9% [12].
A prior history of head trauma, often of a relatively mild degree, has been described as a potential inciting factor for some cases of PNES [6,13]. In the literature, studies report that as many as 20% of PNES patients attributed their seizures to head trauma, often rather mild head trauma [6,14].
Historcial Context
Historically, what today are called PNES originate with the concept of hysteria, a medical diagnosis in women that can be traced to antiquity [15,16]. By the late 1800s, one of the founders of neurology, Jean Charcot, established hysterical seizures as an important clinical entity with his detailed, elegant descriptions of patients. Charcot formulated clinical methods for distinguishing hysteria and particularly hysterical seizures from epilepsy. He presumed that hysteria and epilepsy were closely related, and he termed seizures due to hysteria as “hysteroepilepsy” or “epileptiform” hysteria. Charcot proposed that hysterical seizures were organic disorders of the brain, like other forms of seizures and epilepsy, and emphasized their relation to disturbance of the female reproductive system [17,18]. Charcot utilized techniques such as manipulation of “hysterogenic zones” and ovarian compression as well as suggestion to both treat and provoke hysteria and hysterical seizures, which he described and documented [17,18]. One of Charcot’s most celebrated students, Sigmund Freud, observed Charcot’s demonstrations but drew different conclusions. He theorized that hysteria and hysterical seizures were not organic disorders of the brain as Charcot proposed, but were rather emotional disorders of the unconscious mind due to repressed energies or drives. Based largely the theories of Freud and Charcot, individuals with hysteria were distinguished from those with epilepsy, with hysterical seizures related to psychological dysfunction while epileptic seizures were associated with physical or organic brain disorders [15,16].
With the introduction of EEG recording in the 1930s, it became possible to characterize epilepsy as an electrical disorder of the brain with associated EEG changes and more effectively distinguish it from hysterical seizures, which did not have such abnormalities. In addition, in the first half of the 20th century, the nature of hysteria as seen and diagnosed by physicians seemed to change. The dramatic, theatrical convulsions described by Charcot and his contemporaries appeared less commonly, while disorders such as chronic pain seemed to increase [1,19].
However, by the 1960s, several reports confirmed that hysterical seizures were actually still prevalent. Newer terms like “pseudoseizures” were used to describe these disorders because the term “hysteria” was thought to be somewhat derogatory, anti-feminist, and antiquated [20,21]. In the 1970s and thereafter, with the increasing availability of video EEG monitoring and growth of inpatient epilepsy monitoring units, it was discovered that these hysterical, pseudo-, or what were also by then termed psychogenic seizures, were actually still common [1,22].
More recently, it has been recognized that the pendulum in some cases may have swung too far in regard to the diagnosis of this disorder. Some rare patients with seizures initially diagnosed as PNES may actually have forms of epileptic seizures such as frontal lobe epilepsy or related physiological disorders rather than psychogenic causes for their episodes [1,23]. These types of epileptic seizures can be very difficult to diagnose properly unless one appreciates how they present and manifest and remains vigilant for them during evaluation [1,23].
Terminology
There is an ongoing debate regarding the appropriate terminology for psychogenic events, and there is no uniform standardized definition or classification at this time. The term that is currently preferred within the epilepsy community for seizures of psychological origin that are thought to be associated with conversion, somatization, or dissociative disorders is “psychogenic nonepileptic seizures” (PNES). This terminology is felt to be non-disparaging and more neutral as compared with other terms such as pseudoseizures, which were previously favored. Nonepileptic seizures or nonepileptic events are broader terms meant to incorporate both physiologic and psychological causes for disorders that are mistaken for epilepsy. PNES are widely defined as paroxysmal events that appear similar to epileptic seizures but are not due to abnormal electrical discharges in the brain and as noted, are typically thought to be related or caused by conversion, somatization, or dissociative disorders.
Physiologic nonepileptic events are another category of physical disorders that may be mistaken for epilepsy. The underlying causes differ between age-groups, and can include conditions such as cardiac arrhythmias, migraine variants, syncope, or metabolic abnormalities. Physiologic nonepileptic seizures account for only a small proportion of all patients with nonepileptic seizures or events [1]. In general, any patient with a psychological disorder that causes symptoms that are mistaken for epilepsy can be said to have PNES.
Clinical Characteristics And Presentation
The duration of PNES is often significantly longer than that seen in epileptic seizures, which usually last less than 3 minutes, excluding the postictal period. PNES may also exhibit waxing and waning convulsive activity, although this finding can certainly be seen in epileptic seizures as well. PNES may be shown to have distractibility with external stimuli. Additionally, the movements in PNES may appear asymmetric, asynchronous, or purposeful, although this is not diagnostic for this disorder. This may contrast with the well-defined, synchronous tonic-clonic activity typically seen in epileptic seizures [1,24,25]. Back arching and pelvic thrusting movements can also be seen in PNES. Despite these differences, it may still be challenging to distinguish the semi-purposeful behaviors of PNES from the automatisms of certain focal epileptic seizures. The often bizarre-appearing, hypermotor activity that can be seen in frontal lobe seizures is often especially difficult to differentiate from PNES [1,23].
Another important consideration is that consciousness is preserved in PNES, while consciousness and responsiveness are frequently impaired in epileptic seizures. Patients with PNES are often apparently unresponsive during events, although there is no true impairment of awareness. Other characteristics that are more commonly seen in PNES are crying and eye closure [26]. Self-injury and incontinence may be reported, but they are less often clearly witnessed or documented [27,28]. Additionally, although patients may at times appear to be asleep at seizure onset, EEG recordings document the patient to actually be asleep in less than 1% of cases [29]. While epileptic seizures often respond well to antiepileptic medications, PNES characteristically do not [1,3,6,8].
In certain situations, provocation maneuvers may be utilized in order to reproduce PNES in patients undergoing EEG monitoring. In comparison to epileptic seizures, suggestion and emotional stimuli are more likely to trigger psychogenic events [1]. Methods utilized to provoke PNES may include saline injections, placement of a tuning fork on the head or body, or even hypnosis, when a suggestion is concurrently provided that such maneuvers can trigger the patient’s seizures [1,30,31]. When evaluating seizures that are provoked in such a manner, it is important to consider whether or not the event captured is in fact a typical event for the patient, or whether the provocation has uncovered a different, atypical event. Given that PNES and epileptic seizures can co-exist within the same patient, care should be taken to avoid making a diagnosis based on capturing an atypical event, or capturing only a subset of a patient’s seizure types. This could result in failure to make an accurate and thorough diagnosis [23]. There is debate regarding the ethics of provoking seizures by way of suggestion. Some members of the epilepsy community feel that provoking seizures through suggestion is inherently deceitful, and therefore can damage the physician-patient relationship. Others assert that such provocative testing can be undertaken in an honest manner, and can ultimately help achieve an accurate diagnosis for the patient [32].
As previously mentioned, there is a proportion of patients who have co-existing epileptic seizures and PNES, and obtaining an accurate diagnosis can be especially challenging in this group. Studies have reported that around 10% to 40% of patients with PNES also have epilepsy [1,22,23,33]. Care must be taken to distinguish between differences in seizure types and if necessary, video EEG monitoring may be needed to capture both seizure types for an accurate diagnosis. This testing can then be useful in education with families and caregivers who may be shown the videos with consent from the patient in order to guide future care.
Evaluation And Diagnosis
As in much of neurology, a thorough history, along with detailed clinical observation remains essential in the diagnosis of patients with PNES and for distinguishing these events from epilepsy. Video EEG monitoring of seizures is a key adjunct to the history and clinical observation in diagnosing this condition [1,2]. Long-term video EEG monitoring is considered the “gold standard” in the characterization and differential diagnosis of seizures. Additional potentially helpful diagnostic techniques include video EEG-monitored seizure provocation, serum prolactin levels, single photon emission computed tomography, and neuropsychological testing.
Video EEG Monitoring
![]()
EEG monitoring for characterization of clinical events can be conducted on an ambulatory or outpatient basis or in dedicated inpatient epilepsy monitoring units. Ambulatory monitoring can be useful in the case of patients who report seizures that are more frequent in their home environment or in patients with frequent events. If events are infrequent, then inpatient monitoring may be more efficacious [1]. With longer-term inpatient monitoring, antiepileptic medications can be withdrawn in a supervised setting, in order to lower the seizure threshold as well as to safely discontinue medications that may not be necessary. Such medication titrations are typically not safe in an unsupervised outpatient setting. Some ambulatory EEG monitoring systems do allow for simultaneous video and EEG recording. However, an advantage to inpatient monitoring, which is not afforded in the outpatient setting, is the ability for nursing staff or physicians to perform clinical testing during events to assess for patient responsiveness and other features. Additionally, with inpatient monitoring, EEG technicians can routinely assess for any technical problems with the electrodes or recording system.
Another benefit of video EEG monitoring is that the state (waking, drowsy, or asleep) of the patient at the onset of an event can be established. While epileptic seizures can arise from any state, PNES most often occur from wakefulness. Patients with PNES may appear to be asleep at the onset of events, and they may report seizures from sleep. Video EEG monitoring can help to establish the waking or sleep state of the patient that may aid in diagnosis [29].
Prolactin Levels
Serum prolactin levels may be helpful in the diagnosis of PNES [35,36]. Following generalized tonic-clonic or complex partial epileptic seizures, the serum prolactin can rise from two to threefold to five to tenfold [37]. The maximal rise in serum prolactin occurs in the initial 20 to 60 minutes after the seizure [35–37]. A similar rise in serum prolactin would not be expected in PNES. Although prolactin levels may have some utility in diagnosis, they are not currently routinely ordered as part of a standard admission to most inpatient epilepsy monitoring units. This may be due in part to the fact that false-positive and false-negative results can occur with these levels [37–39]. For example, there may not be a rise in the prolactin level after a simple partial seizure or more subtle complex partial seizure.
Neuropsychological Testing
Neuropsychological testing is also a key component in the evaluation and diagnosis of PNES. Ideally, a mental health provider with a background in psychological assessment and neuropsychological intervention for patients with psychogenic disorders would perform the evaluation [40,41].
The goal of the evaluation should not solely focused on whether the patient suffers from nonepileptic or epileptic seizures. An epileptologist upon review of clinical, electrographic, and neuropsychological data better makes this determination. Moreover, neuropsychological testing cannot in itself either diagnose or exclude the possibility that a seizure disorder is nonepileptic because of the considerable overlap between epileptic and nonepileptic test results [40,41]. Neuropsychological evaluations aid this assessment by (1) determining the potential or likelihood of significant contributing psychopathology or cognitive difficulties, (2) defining the nature of the associated psychological or psychosocial issues, and (3) assessing how a patient might benefit from various psychologically based interventions [1]. The testing may identify psychological problems that can guide treatment after diagnosis.
Delays in Diagnosis
Correct and prompt diagnosis is essential for patients with PNES as is appropriate referral to a knowledgeable trained mental health professional. On average, patients with PNES are diagnosed 7.2 years after manifestation (SD 9.3 years), with mean delay of 5 to 7 years. Younger age, interictal epileptiform potentials in the EEG, and anticonvulsant treatment are associated with longer delays [42,43]. Delays are also thought to occur because of problems with “ownership” of these patients. Although typically neurologists are involved in the diagnosis of PNES, often using video EEG monitoring done in an inpatient setting, the next step is often a referral to a psychiatrist or mental health care provider. There are sometimes delays in the initial referral to the neurologist, delays in referral to specialists for video EEG testing, and also to the physicians, psychologists or social workers who may provide treatment. Another disconnect can occur if patients are “lost to follow-up” if they receive a referral for mental health care and either do not follow up on this on their own, or if the reason for this care is not fully explained. In addition, many mental health professionals are not trained in the evaluation and treatment of psychogenic symptoms and may even feel uncomfortable in dealing with these patients [13,44].
Many studies have been suggestive that delays in diagnosis may result in poorer outcomes [45,46], while other studies have suggested that patients who have an acute diagnosis of PNES upon presentation may do particularly well [8,47–49]. Some of the most recent large outcome studies suggest that there may be no worsening of outcome associated with delays in diagnosis and that outcome was predicted by other factors [50–52].
Management
Management of patients with PNES is similar to that for patients with other types of so-called abnormal illness behavior, although there remains a relative paucity of evidence for specific treatment strategies for PNES [1]. The first consideration should be the manner in which the diagnosis of PNES is presented to the patient and family. It is important to be honest with the patient and demonstrate a positive approach to the diagnosis [53]. The physician should emphasize as favorable or good news the fact that the patient does not have epilepsy, and should also stress that the disorder, although serious and "real," does not require treatment with antiepileptic medications and that once stress or emotional issues are resolved, the patient has the potential to gain better control of these events [1,54,55]. Nevertheless, not all patients readily accept the diagnosis or this type of approach. Some patients may seek other opinions, and this should not be discouraged. An adversarial relationship with the patient should be avoided. The patient should be encouraged to return if desired, and records should be made available to other health care providers to avoid duplication of services.
After the diagnosis of PNES is presented, supportive measures should be initiated. PNES patients may benefit from education and support that can be provided by the neurologist or primary care physician [1]. If the neuropsychological assessment suggests a clinical profile that requires a professional mental health intervention, then an appropriate referral should be made. Regular follow-up visits for the patient with the neurologist are useful even if a mental health professional is involved [49,56]. This allows the patient to get medical attention without demonstrating illness behavior. Patient education and support are stressed at these visits. Because family issues are often important contributing factors, physicians should consider involving family members in visits with consent of the patient [1].
A variety of treatment strategies are employed for the management of PNES including cognitive behavioral therapy (CBT), group and family therapy, antidepressant medication, and other forms of rehabilitation [5,57,58]. A 2007 Cochrane review that identified 608 references for non-medication PNES treatments found that only 3 studies met criteria for a randomized controlled trial. One of the more recently favored treatment options for PNES that has been applied to the treatment of various somatoform disorders and other psychiatric disorders in the past is CBT [57,59,60]. This form of psychotherapy can be administered by trained personnel in a time-limited fashion using defined protocols. The basis of this treatment is that the patient learns to increase awareness of their dysfunctional thoughts and learns new ways to respond to them [57,58]. To date, several groups have reported results of nonrandomized trials as well as case reports and case series which have established the utility of this treatment. There have been reports of significant reductions in seizure frequency and this treatment strategy appears very promising [61–65]. Preliminary randomized controlled trials have also been piloted and are also suggestive that this may be a validated treatment approach [66].
Prognosis
The outcomes of patients with PNES vary. Long-term follow-up studies show that about half of all patients with PNES function reasonably well following their diagnosis. However, only approximately one-third of patients will completely stop having seizures or related problems, and approximately 50% percent have poor functional outcomes [1,2,50]. When the diagnosis of PNES is based on reliable criteria such a video EEG monitoring, misdiagnosis is unlikely. Instead, the usual cause for a poor outcome is related to a patient’s chronic psychological and social problems[1,8,22,50].
It is noteworthy that children with PNES appear to have a much better prognosis than adults [9,10]. In fact, the etiology in children may be related more to transient stress and coping disorders, while adults are more likely to have PNES within the context of more chronic psychological maladjustment, such as personality disorders [10]. Another factor that accounts for the better outcomes in children is that they are usually properly diagnosed earlier in the course of their disorder [9,10].
Patients with milder psychopathology respond better to supportive educational or behavioral therapeutic approaches. In contrast, patients with more severe psychopathology and factitious disorders more often have associated chronic personality problems and correspondingly, a poorer prognosis [1,50]. Also it appears that patients who continue to be followed by the diagnosing neurologist or center do better than patients who are not seen after diagnosis [49,67]. As knowledge about the nature of PNES and their associated psychopathology is gained, better treatment strategies can be developed that will improve the care and prognosis of these difficult and challenging patients.
A large study of 164 patients who were followed for 10 years were considered to have “poor outcome” in general but favorable factors included higher education, younger age of onset and diagnosis, and less “dramatic” attacks, defined as lack of “positive motor features, no ictal incontinence or tongue biting.” These findings were consistent with prior studies [52,68].
In addition, the patients who tended to have less seizures and do better long term, had less somatoform and dissociative symptoms on psychometric testing [51]. These findings are often explained by the theory that patients who do not do well have poor coping strategies to deal with stress and anxiety and that in a sense, these patients have emotional dysregulation.
Special Issues
Coexisting Epileptic and Psychogenic Nonepileptic Seizures
A complicating factor in diagnosis is that both PNES and epileptic seizures may occur in a single patient. Indeed, approximately 10% to 40% of patients identified to have PNES also have been reported to have epileptic seizures [1,23,33,56]. There are several possible explanations for this. Some patients with epilepsy may learn that seizures result in attention and fill certain psychological needs. Alternatively, they may have concomitant neurologic problems, personality disorders, cognitive deficits, or impaired coping mechanisms that predispose them to psychogenic symptoms [69–71]. Fortunately, in such patients with combined seizure disorders, the epileptic seizures are usually well controlled or of only historical relevance at the time a patient develops PNES [1,22,23,33,72–74].
In other patients, both epileptic and PNES may start simultaneously, making management even more complex. In such patients, we have found it particularly helpful to focus on the semiology of seizure manifestations as recorded by video EEG monitoring to distinguish PNES from the epileptic seizures. We then direct our treatment of the patient according to the semiology manifesting at that time. We also have found it useful to show the videos of seizures to family members or caregivers with patient consent to help them understand how to respond best to a patient’s symptoms when epileptic and PNES co-exist.
Misdiagnosis of Psychogenic Nonepileptic Seizures
Sometimes events that are initially diagnosed as nonepileptic actually prove to be epileptic. Such events can be called “pseudo-pseudo” or “epileptic-nonepileptic” seizures [1]. Frontal lobe seizures in particular may not be associated with significant EEG changes ictally and therefore misdiagnosed as PNES [23,75,76]. Clinical presentation and proper diagnosis of these types of events warrant emphasis.
Notable manifestations of frontal lobe seizures that may easily be confused with hysterical behavior include shouting, laughing, cursing, clapping, snapping, genital manipulation, pelvic thrusting, pedaling, running, kicking, and thrashing [23,75–77]. Not all of these behaviors are specific for frontal lobe seizures. For example, bicycling leg movements have also been reported in seizures originating from the temporal lobe [78].
Summary
PNES represent a common yet challenging problem within neurology. This is due to the difficulty in diagnosis as well as lack of effective and widely available treatment options. Overall outcomes of patients with PNES vary, and may relate to an individual patient’s chronic psychological and social problems. However, an accurate and timely diagnosis remains critical and can help provide direction for implementing appropriate treatment.
Corresponding author: Jennifer Hopp, MD, Department of Neurology, University of Maryland Medical Center, Room S12C09, 22 South Greene Street, Baltimore, MD 21201, [email protected].
Financial disclosures: None.
From the Department of Neurology, University of Maryland School of Medicine, Baltimore, MD.
Abstracts
- Objective: To provide a review of psychogenic nonepileptic seizures, including a discussion of the diagnosis, treatment, and clinical significance of the disorder.
- Methods: Review of the relevant literature.
- Results: Psychogenic nonepileptic seizures are a common and potentially disabling neurologic disorder. They are most prevalent in young adults, and more commonly seen in women versus men. Certain psychosocial variables may impact the development of the condition. The diagnosis is made through a detailed history and observation of clinical events in conjunction with video EEG monitoring. Neuropsychological testing is an important component in the evaluation. Treatment includes establishment of an accurate diagnosis, management of any underlying psychiatric diagnoses, and regular follow-up with a neurologist or trained care provider.
- Conclusion: Psychogenic nonepileptic seizures represent a complex interaction between neurologic and psychological factors. Obtaining an accurate diagnosis through the use of video EEG monitoring and clinical observation is an important initial step in treatment and improved quality of life in this patient population.
Psychogenic nonepileptic seizures (PNES) are commonly encountered in outpatient specialty epilepsy clinics as well as inpatient epilepsy monitoring units. They comprise approximately 20% of all refractory seizure disorders referred to specialty epilepsy centers [1–4]. PNES are thought to be psychological in origin as opposed to arising from abnormal electrical discharges as in epileptic seizures. PNES may be more frequent and disabling than epileptic seizures, and patients with PNES may report worse outcomes [5,6]. Increased utilization of long-term video EEG monitoring along with greater recognition of psychogenic neurologic disorders has allowed for improved diagnosis of PNES. However, many diagnostic and therapeutic challenges remain. There are often delays in obtaining an accurate diagnosis, and optimal management remains challenging, often leading to inappropriate, ineffective, and costly treatment, sometimes for many years [6–8].
Epidemiology
PNES are seen across the spectrum of age-groups, from children [9,10] to elderly persons, but they most often occur in young adults between the ages of 15 to 35 years [1,8]. Caution should be used when considering this diagnosis in infants or young children, in whom it is more common to see physiologic events that may mimic epileptic seizures, including gastroesophageal reflux, shuddering, night terrors, or breath holding spells [1,9,10].
PNES are prevalent within epilepsy practices. Patients with PNES comprise approximately 5% to 20% patients thought to have intractable epilepsy seen in outpatient centers, and within epilepsy monitoring units they account for 10% to 40% of patients [1,2,6,8]. A population-based study approximates the incidence of PNES at 1.4 per 100,000 people and 3.4 per 100,000 people between the ages of 15 to 24 years [4].
There is a female preponderance in PNES, which is similar to other conversion and somatoform disorders. Overall, women comprise approximately 70% to 80% of patients with the PNES diagnosis [1,2,6]. There are psychosocial variables that are seen in some patients with this disorder. An important factor that has been described is past history of sexual or physical abuse. In one series, there was a history of sexual abuse in almost 25% of patients with PNES, and history of either sexual abuse, physical abuse, or both in 32% of patients [11]. A history of sexual and/or physical abuse is not exclusive to these patients, and can certainly be seen in patients with epilepsy as well. For example, in a control population of epilepsy patients, there was a reported rate of past sexual or physical abuse approaching 9% [12].
A prior history of head trauma, often of a relatively mild degree, has been described as a potential inciting factor for some cases of PNES [6,13]. In the literature, studies report that as many as 20% of PNES patients attributed their seizures to head trauma, often rather mild head trauma [6,14].
Historcial Context
Historically, what today are called PNES originate with the concept of hysteria, a medical diagnosis in women that can be traced to antiquity [15,16]. By the late 1800s, one of the founders of neurology, Jean Charcot, established hysterical seizures as an important clinical entity with his detailed, elegant descriptions of patients. Charcot formulated clinical methods for distinguishing hysteria and particularly hysterical seizures from epilepsy. He presumed that hysteria and epilepsy were closely related, and he termed seizures due to hysteria as “hysteroepilepsy” or “epileptiform” hysteria. Charcot proposed that hysterical seizures were organic disorders of the brain, like other forms of seizures and epilepsy, and emphasized their relation to disturbance of the female reproductive system [17,18]. Charcot utilized techniques such as manipulation of “hysterogenic zones” and ovarian compression as well as suggestion to both treat and provoke hysteria and hysterical seizures, which he described and documented [17,18]. One of Charcot’s most celebrated students, Sigmund Freud, observed Charcot’s demonstrations but drew different conclusions. He theorized that hysteria and hysterical seizures were not organic disorders of the brain as Charcot proposed, but were rather emotional disorders of the unconscious mind due to repressed energies or drives. Based largely the theories of Freud and Charcot, individuals with hysteria were distinguished from those with epilepsy, with hysterical seizures related to psychological dysfunction while epileptic seizures were associated with physical or organic brain disorders [15,16].
With the introduction of EEG recording in the 1930s, it became possible to characterize epilepsy as an electrical disorder of the brain with associated EEG changes and more effectively distinguish it from hysterical seizures, which did not have such abnormalities. In addition, in the first half of the 20th century, the nature of hysteria as seen and diagnosed by physicians seemed to change. The dramatic, theatrical convulsions described by Charcot and his contemporaries appeared less commonly, while disorders such as chronic pain seemed to increase [1,19].
However, by the 1960s, several reports confirmed that hysterical seizures were actually still prevalent. Newer terms like “pseudoseizures” were used to describe these disorders because the term “hysteria” was thought to be somewhat derogatory, anti-feminist, and antiquated [20,21]. In the 1970s and thereafter, with the increasing availability of video EEG monitoring and growth of inpatient epilepsy monitoring units, it was discovered that these hysterical, pseudo-, or what were also by then termed psychogenic seizures, were actually still common [1,22].
More recently, it has been recognized that the pendulum in some cases may have swung too far in regard to the diagnosis of this disorder. Some rare patients with seizures initially diagnosed as PNES may actually have forms of epileptic seizures such as frontal lobe epilepsy or related physiological disorders rather than psychogenic causes for their episodes [1,23]. These types of epileptic seizures can be very difficult to diagnose properly unless one appreciates how they present and manifest and remains vigilant for them during evaluation [1,23].
Terminology
There is an ongoing debate regarding the appropriate terminology for psychogenic events, and there is no uniform standardized definition or classification at this time. The term that is currently preferred within the epilepsy community for seizures of psychological origin that are thought to be associated with conversion, somatization, or dissociative disorders is “psychogenic nonepileptic seizures” (PNES). This terminology is felt to be non-disparaging and more neutral as compared with other terms such as pseudoseizures, which were previously favored. Nonepileptic seizures or nonepileptic events are broader terms meant to incorporate both physiologic and psychological causes for disorders that are mistaken for epilepsy. PNES are widely defined as paroxysmal events that appear similar to epileptic seizures but are not due to abnormal electrical discharges in the brain and as noted, are typically thought to be related or caused by conversion, somatization, or dissociative disorders.
Physiologic nonepileptic events are another category of physical disorders that may be mistaken for epilepsy. The underlying causes differ between age-groups, and can include conditions such as cardiac arrhythmias, migraine variants, syncope, or metabolic abnormalities. Physiologic nonepileptic seizures account for only a small proportion of all patients with nonepileptic seizures or events [1]. In general, any patient with a psychological disorder that causes symptoms that are mistaken for epilepsy can be said to have PNES.
Clinical Characteristics And Presentation
The duration of PNES is often significantly longer than that seen in epileptic seizures, which usually last less than 3 minutes, excluding the postictal period. PNES may also exhibit waxing and waning convulsive activity, although this finding can certainly be seen in epileptic seizures as well. PNES may be shown to have distractibility with external stimuli. Additionally, the movements in PNES may appear asymmetric, asynchronous, or purposeful, although this is not diagnostic for this disorder. This may contrast with the well-defined, synchronous tonic-clonic activity typically seen in epileptic seizures [1,24,25]. Back arching and pelvic thrusting movements can also be seen in PNES. Despite these differences, it may still be challenging to distinguish the semi-purposeful behaviors of PNES from the automatisms of certain focal epileptic seizures. The often bizarre-appearing, hypermotor activity that can be seen in frontal lobe seizures is often especially difficult to differentiate from PNES [1,23].
Another important consideration is that consciousness is preserved in PNES, while consciousness and responsiveness are frequently impaired in epileptic seizures. Patients with PNES are often apparently unresponsive during events, although there is no true impairment of awareness. Other characteristics that are more commonly seen in PNES are crying and eye closure [26]. Self-injury and incontinence may be reported, but they are less often clearly witnessed or documented [27,28]. Additionally, although patients may at times appear to be asleep at seizure onset, EEG recordings document the patient to actually be asleep in less than 1% of cases [29]. While epileptic seizures often respond well to antiepileptic medications, PNES characteristically do not [1,3,6,8].
In certain situations, provocation maneuvers may be utilized in order to reproduce PNES in patients undergoing EEG monitoring. In comparison to epileptic seizures, suggestion and emotional stimuli are more likely to trigger psychogenic events [1]. Methods utilized to provoke PNES may include saline injections, placement of a tuning fork on the head or body, or even hypnosis, when a suggestion is concurrently provided that such maneuvers can trigger the patient’s seizures [1,30,31]. When evaluating seizures that are provoked in such a manner, it is important to consider whether or not the event captured is in fact a typical event for the patient, or whether the provocation has uncovered a different, atypical event. Given that PNES and epileptic seizures can co-exist within the same patient, care should be taken to avoid making a diagnosis based on capturing an atypical event, or capturing only a subset of a patient’s seizure types. This could result in failure to make an accurate and thorough diagnosis [23]. There is debate regarding the ethics of provoking seizures by way of suggestion. Some members of the epilepsy community feel that provoking seizures through suggestion is inherently deceitful, and therefore can damage the physician-patient relationship. Others assert that such provocative testing can be undertaken in an honest manner, and can ultimately help achieve an accurate diagnosis for the patient [32].
As previously mentioned, there is a proportion of patients who have co-existing epileptic seizures and PNES, and obtaining an accurate diagnosis can be especially challenging in this group. Studies have reported that around 10% to 40% of patients with PNES also have epilepsy [1,22,23,33]. Care must be taken to distinguish between differences in seizure types and if necessary, video EEG monitoring may be needed to capture both seizure types for an accurate diagnosis. This testing can then be useful in education with families and caregivers who may be shown the videos with consent from the patient in order to guide future care.
Evaluation And Diagnosis
As in much of neurology, a thorough history, along with detailed clinical observation remains essential in the diagnosis of patients with PNES and for distinguishing these events from epilepsy. Video EEG monitoring of seizures is a key adjunct to the history and clinical observation in diagnosing this condition [1,2]. Long-term video EEG monitoring is considered the “gold standard” in the characterization and differential diagnosis of seizures. Additional potentially helpful diagnostic techniques include video EEG-monitored seizure provocation, serum prolactin levels, single photon emission computed tomography, and neuropsychological testing.
Video EEG Monitoring
![]()
EEG monitoring for characterization of clinical events can be conducted on an ambulatory or outpatient basis or in dedicated inpatient epilepsy monitoring units. Ambulatory monitoring can be useful in the case of patients who report seizures that are more frequent in their home environment or in patients with frequent events. If events are infrequent, then inpatient monitoring may be more efficacious [1]. With longer-term inpatient monitoring, antiepileptic medications can be withdrawn in a supervised setting, in order to lower the seizure threshold as well as to safely discontinue medications that may not be necessary. Such medication titrations are typically not safe in an unsupervised outpatient setting. Some ambulatory EEG monitoring systems do allow for simultaneous video and EEG recording. However, an advantage to inpatient monitoring, which is not afforded in the outpatient setting, is the ability for nursing staff or physicians to perform clinical testing during events to assess for patient responsiveness and other features. Additionally, with inpatient monitoring, EEG technicians can routinely assess for any technical problems with the electrodes or recording system.
Another benefit of video EEG monitoring is that the state (waking, drowsy, or asleep) of the patient at the onset of an event can be established. While epileptic seizures can arise from any state, PNES most often occur from wakefulness. Patients with PNES may appear to be asleep at the onset of events, and they may report seizures from sleep. Video EEG monitoring can help to establish the waking or sleep state of the patient that may aid in diagnosis [29].
Prolactin Levels
Serum prolactin levels may be helpful in the diagnosis of PNES [35,36]. Following generalized tonic-clonic or complex partial epileptic seizures, the serum prolactin can rise from two to threefold to five to tenfold [37]. The maximal rise in serum prolactin occurs in the initial 20 to 60 minutes after the seizure [35–37]. A similar rise in serum prolactin would not be expected in PNES. Although prolactin levels may have some utility in diagnosis, they are not currently routinely ordered as part of a standard admission to most inpatient epilepsy monitoring units. This may be due in part to the fact that false-positive and false-negative results can occur with these levels [37–39]. For example, there may not be a rise in the prolactin level after a simple partial seizure or more subtle complex partial seizure.
Neuropsychological Testing
Neuropsychological testing is also a key component in the evaluation and diagnosis of PNES. Ideally, a mental health provider with a background in psychological assessment and neuropsychological intervention for patients with psychogenic disorders would perform the evaluation [40,41].
The goal of the evaluation should not solely focused on whether the patient suffers from nonepileptic or epileptic seizures. An epileptologist upon review of clinical, electrographic, and neuropsychological data better makes this determination. Moreover, neuropsychological testing cannot in itself either diagnose or exclude the possibility that a seizure disorder is nonepileptic because of the considerable overlap between epileptic and nonepileptic test results [40,41]. Neuropsychological evaluations aid this assessment by (1) determining the potential or likelihood of significant contributing psychopathology or cognitive difficulties, (2) defining the nature of the associated psychological or psychosocial issues, and (3) assessing how a patient might benefit from various psychologically based interventions [1]. The testing may identify psychological problems that can guide treatment after diagnosis.
Delays in Diagnosis
Correct and prompt diagnosis is essential for patients with PNES as is appropriate referral to a knowledgeable trained mental health professional. On average, patients with PNES are diagnosed 7.2 years after manifestation (SD 9.3 years), with mean delay of 5 to 7 years. Younger age, interictal epileptiform potentials in the EEG, and anticonvulsant treatment are associated with longer delays [42,43]. Delays are also thought to occur because of problems with “ownership” of these patients. Although typically neurologists are involved in the diagnosis of PNES, often using video EEG monitoring done in an inpatient setting, the next step is often a referral to a psychiatrist or mental health care provider. There are sometimes delays in the initial referral to the neurologist, delays in referral to specialists for video EEG testing, and also to the physicians, psychologists or social workers who may provide treatment. Another disconnect can occur if patients are “lost to follow-up” if they receive a referral for mental health care and either do not follow up on this on their own, or if the reason for this care is not fully explained. In addition, many mental health professionals are not trained in the evaluation and treatment of psychogenic symptoms and may even feel uncomfortable in dealing with these patients [13,44].
Many studies have been suggestive that delays in diagnosis may result in poorer outcomes [45,46], while other studies have suggested that patients who have an acute diagnosis of PNES upon presentation may do particularly well [8,47–49]. Some of the most recent large outcome studies suggest that there may be no worsening of outcome associated with delays in diagnosis and that outcome was predicted by other factors [50–52].
Management
Management of patients with PNES is similar to that for patients with other types of so-called abnormal illness behavior, although there remains a relative paucity of evidence for specific treatment strategies for PNES [1]. The first consideration should be the manner in which the diagnosis of PNES is presented to the patient and family. It is important to be honest with the patient and demonstrate a positive approach to the diagnosis [53]. The physician should emphasize as favorable or good news the fact that the patient does not have epilepsy, and should also stress that the disorder, although serious and "real," does not require treatment with antiepileptic medications and that once stress or emotional issues are resolved, the patient has the potential to gain better control of these events [1,54,55]. Nevertheless, not all patients readily accept the diagnosis or this type of approach. Some patients may seek other opinions, and this should not be discouraged. An adversarial relationship with the patient should be avoided. The patient should be encouraged to return if desired, and records should be made available to other health care providers to avoid duplication of services.
After the diagnosis of PNES is presented, supportive measures should be initiated. PNES patients may benefit from education and support that can be provided by the neurologist or primary care physician [1]. If the neuropsychological assessment suggests a clinical profile that requires a professional mental health intervention, then an appropriate referral should be made. Regular follow-up visits for the patient with the neurologist are useful even if a mental health professional is involved [49,56]. This allows the patient to get medical attention without demonstrating illness behavior. Patient education and support are stressed at these visits. Because family issues are often important contributing factors, physicians should consider involving family members in visits with consent of the patient [1].
A variety of treatment strategies are employed for the management of PNES including cognitive behavioral therapy (CBT), group and family therapy, antidepressant medication, and other forms of rehabilitation [5,57,58]. A 2007 Cochrane review that identified 608 references for non-medication PNES treatments found that only 3 studies met criteria for a randomized controlled trial. One of the more recently favored treatment options for PNES that has been applied to the treatment of various somatoform disorders and other psychiatric disorders in the past is CBT [57,59,60]. This form of psychotherapy can be administered by trained personnel in a time-limited fashion using defined protocols. The basis of this treatment is that the patient learns to increase awareness of their dysfunctional thoughts and learns new ways to respond to them [57,58]. To date, several groups have reported results of nonrandomized trials as well as case reports and case series which have established the utility of this treatment. There have been reports of significant reductions in seizure frequency and this treatment strategy appears very promising [61–65]. Preliminary randomized controlled trials have also been piloted and are also suggestive that this may be a validated treatment approach [66].
Prognosis
The outcomes of patients with PNES vary. Long-term follow-up studies show that about half of all patients with PNES function reasonably well following their diagnosis. However, only approximately one-third of patients will completely stop having seizures or related problems, and approximately 50% percent have poor functional outcomes [1,2,50]. When the diagnosis of PNES is based on reliable criteria such a video EEG monitoring, misdiagnosis is unlikely. Instead, the usual cause for a poor outcome is related to a patient’s chronic psychological and social problems[1,8,22,50].
It is noteworthy that children with PNES appear to have a much better prognosis than adults [9,10]. In fact, the etiology in children may be related more to transient stress and coping disorders, while adults are more likely to have PNES within the context of more chronic psychological maladjustment, such as personality disorders [10]. Another factor that accounts for the better outcomes in children is that they are usually properly diagnosed earlier in the course of their disorder [9,10].
Patients with milder psychopathology respond better to supportive educational or behavioral therapeutic approaches. In contrast, patients with more severe psychopathology and factitious disorders more often have associated chronic personality problems and correspondingly, a poorer prognosis [1,50]. Also it appears that patients who continue to be followed by the diagnosing neurologist or center do better than patients who are not seen after diagnosis [49,67]. As knowledge about the nature of PNES and their associated psychopathology is gained, better treatment strategies can be developed that will improve the care and prognosis of these difficult and challenging patients.
A large study of 164 patients who were followed for 10 years were considered to have “poor outcome” in general but favorable factors included higher education, younger age of onset and diagnosis, and less “dramatic” attacks, defined as lack of “positive motor features, no ictal incontinence or tongue biting.” These findings were consistent with prior studies [52,68].
In addition, the patients who tended to have less seizures and do better long term, had less somatoform and dissociative symptoms on psychometric testing [51]. These findings are often explained by the theory that patients who do not do well have poor coping strategies to deal with stress and anxiety and that in a sense, these patients have emotional dysregulation.
Special Issues
Coexisting Epileptic and Psychogenic Nonepileptic Seizures
A complicating factor in diagnosis is that both PNES and epileptic seizures may occur in a single patient. Indeed, approximately 10% to 40% of patients identified to have PNES also have been reported to have epileptic seizures [1,23,33,56]. There are several possible explanations for this. Some patients with epilepsy may learn that seizures result in attention and fill certain psychological needs. Alternatively, they may have concomitant neurologic problems, personality disorders, cognitive deficits, or impaired coping mechanisms that predispose them to psychogenic symptoms [69–71]. Fortunately, in such patients with combined seizure disorders, the epileptic seizures are usually well controlled or of only historical relevance at the time a patient develops PNES [1,22,23,33,72–74].
In other patients, both epileptic and PNES may start simultaneously, making management even more complex. In such patients, we have found it particularly helpful to focus on the semiology of seizure manifestations as recorded by video EEG monitoring to distinguish PNES from the epileptic seizures. We then direct our treatment of the patient according to the semiology manifesting at that time. We also have found it useful to show the videos of seizures to family members or caregivers with patient consent to help them understand how to respond best to a patient’s symptoms when epileptic and PNES co-exist.
Misdiagnosis of Psychogenic Nonepileptic Seizures
Sometimes events that are initially diagnosed as nonepileptic actually prove to be epileptic. Such events can be called “pseudo-pseudo” or “epileptic-nonepileptic” seizures [1]. Frontal lobe seizures in particular may not be associated with significant EEG changes ictally and therefore misdiagnosed as PNES [23,75,76]. Clinical presentation and proper diagnosis of these types of events warrant emphasis.
Notable manifestations of frontal lobe seizures that may easily be confused with hysterical behavior include shouting, laughing, cursing, clapping, snapping, genital manipulation, pelvic thrusting, pedaling, running, kicking, and thrashing [23,75–77]. Not all of these behaviors are specific for frontal lobe seizures. For example, bicycling leg movements have also been reported in seizures originating from the temporal lobe [78].
Summary
PNES represent a common yet challenging problem within neurology. This is due to the difficulty in diagnosis as well as lack of effective and widely available treatment options. Overall outcomes of patients with PNES vary, and may relate to an individual patient’s chronic psychological and social problems. However, an accurate and timely diagnosis remains critical and can help provide direction for implementing appropriate treatment.
Corresponding author: Jennifer Hopp, MD, Department of Neurology, University of Maryland Medical Center, Room S12C09, 22 South Greene Street, Baltimore, MD 21201, [email protected].
Financial disclosures: None.
1. Krumholz A. Nonepileptic seizures: diagnosis and management. Neurology 1999;S76–83.
2. Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–6.
3. Lesser RP. Psychogenic seizures. Neurology 1996;46:1499–1507.
4. Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:857–62.
5. Szaflarski JP, Szaflarski M, Hughes C, et al. Psychopathology and quality of life: psychogenic non-epileptic seizures versus epilepsy. Med Sci Monit 2003 9:CR113–8.
6. Barry E, Krumholz A, Bergey C, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31.
7. Pakalnis A, Drake ME, Phillips B. Neuropsychiatric aspects of psychogenic status epilepticus. Neurology 1991;41;1104–6.
8. Walzack TS, Papacostas S, Williams DT, et al. Outcome after the diagnosis of psychogenic nonepileptic seizures. Epilepsia 1995;36:1131–7.
9. Metrick ME, Ritter FJ, Gates JR, et al. Nonepileptic events in childhood. Epilepsia 1991;32:322–8.
10. Wyllie E, Friedman D, Luders H, et al. Outcome of psychogenic seizures in children and adolescents compared to adults. Neurology 1991;41:742–4.
11. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5.
12. Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993; 43:1950–3.
13. LaFrance WC Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45 Suppl 2:15–21.
14. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82.
15. Slavney PR. Perspectives on hysteria. Baltimore: Johns Hopkins University Press; 1990.
16. Veith I. Hysteria: the history of a disease. Chicago: University of Chicago Press; 1965.
17. Goetz CG. Charcot the clinician. The Tuesday lessons. New York: Raven Press; 1987.
18. Massey EW, McHenry LC. Hysteroepilepsy in the nineteenth century: Charcot and Gowers. Neurology 1986;36:65–7.
19. Zeigler FJ, Imboden JB, Meyer E. Contemporary conversion reactions: a clinical study. Am J Psychiatry 1960;116:901–10.
20. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology 1964;14:41–9.
21. Diagnostic and statistical manual of mental disorders. DSM-IV 4th ed. American Psychiatric Association. Washington, DC; 1995.
22. Krumholz A, Niedermeyer, E. Psychogenic seizures: a clinical study with follow-up data. Neurology 1983; 33:498-502.
23. Krumholz A, Ting T. Co-existing epileptic and nonepileptic seizures. in imitators of epilepsy. 2nd ed. In: Kaplan PW, Fisher RS, editors. New York: Demos Medical Publishing; 2005:261–76.
24. Gates JR, Ramani V, Whalen S, Loewenson R. Ictal characteristics of pseudoseizures. Arch Neurol 1985;42:1183–87.
25. Leis AA, Ross MA, Summers AK. Psychogenic seizures: Ictal characteristics and diagnostic pitfalls. Neurology 1992;42:95–9.
26. Walczak TS, Bogolioubov. Weeping during psychogenic nonepileptic seizures. Epilepsia 1996;37:207–10.
27. Bergen D, Ristanovic R. Weeping is a common element during psychogenic nonepileptic seizures. Arch Neurol 1993;50:1059–60.
28. Peguero E, Abou-Khalil B, Fakhoury, Mathews G. Self-injury and incontinence in psychogenic seizures. Epilepsia 1995;36:586–91.
29. Orbach D, Ritaccio A, Devinsky O. Psychogenic, nonepileptic seizures associated with video-EEG-verified sleep. Epilepsia 2003;44:64–8.
30. Walczak TS, Williams DT, Berton W. Utility and reliability of placebo infusion in the evaluation of patients with seizures. Neurology 1994;44:394–99.
31. Bazil CW, Kothari M, Luciano D, et al. Provocation of nonepileptic seizures by suggestion in a general seizure population. Epilepsia 1994;35:768–70.
32. Devinsky O, Fisher RS. Ethical use of placebos and provocative testing in diagnosing nonepileptic seizures. Neurology 1996;47:866–70.
33. Lesser RP, Lueders H, Dinner DS. Evidence for epilepsy is rare in patients with psychogenic seizures. Neurology 1983; 33:502–4.
34. Barre MA, Burnstine TH, Fisher RS, Lesser RP. Electroencephalographic changes during simple partial seizures. Epilepsia 1994;35:715–20.
35. Trimble MR. Serum prolactin levels in epilepsy and hysteria. BMJ 1978;2:1682.
36. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985; 35:31–5.
37. Pritchard PB, Wannamaker BB, Sagel J, et al. Endocrine function following complex partial seizures. Ann Neurol 1983;14:27–32.
38. Malkowicz DE, Legido A, Jackel RA, et al. Prolactin secretion following repetitive seizures. Neurology 1995;45:448–52.
39. Oribe E, Rohullah A, Nissenbaum E, Boal B. Serum prolactin concentrations are elevated after syncope. Neurology 1996;47:60–2.
40. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184–8.
41. Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI and neuropsychological assessments of psychogenic and epileptic seizure patients. Epilepsia 1989;30:339–47.
42. DeTimary P, Fouchet P, Sylin M, et al. Non–epileptic seizures: delayed diagnosis in patients presenting with electroencephalographic (EEG) or clinical signs of epileptic seizures. Seizure 2002;11:193–7.
43. Reuber M, Fernandez G, et al. Diagnostic delay in psychogenic nonepileptic seizures. Neurology 2002;58:493–5.
44. Rosenbaum DH, et al. Outpatient multidisciplinary management of non-epileptic seizures. In: Rowan AJ, Gates Jr, editors. Non-epileptic seizures. 1st ed. Stoneham, MA: Butterworth-Heinemann; 1993:275–83.
45. Lempert T, Schmidt D. Natural history and outcome of psychogenic seizures: a clinical study in 50 patients. J Neurol 1990;237:35–8.
46. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41:1330–4.
47. Buchanan N, Snars J. Pseudoseizures (non epileptic attack disorder): clinical management and outcome in 50 patients. Seizure 1993;2:141–6.
48. Kanner AM. More controversies on the treatment of psychogenic pseudoseizures: an addendum. Epilepsy Behav 2003;4:360–4.
49. Aboukasm A, Mahr G, Gahry BR, et al. Retrospective analysis of the effects of psychotherapeutic interventions on outcomes of psychogenic nonepileptic seizures. Epilepsia 1998;39:470–3.
50. Reuber M, Pukrop T, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11.
51. McKenzie P, Oto M, Russell A, Pelosi A, Duncan R. Early outcomes and predictors in 260 patients with psychogenic nonepileptic seizures (PNES). Neurology 2010;74:64–9.
52. Kanner AM, Parra J, Frey M, et al. Psychiatric and neurologic predictors of psychogenic pseudoseizure outcome. Neurology 1999;53:933–8.
53. Shen W, Bowman ES, Markand ON. Presenting the diagnosis of pseudoseizure. Neurology 1990; 40:756–9.
54. Friedman JH, LaFrance Jr WC. Psychogenic disorders: the need to speak plainly. Arch Neurol 2010;67:753–5.
55. LaFrance Jr WC. Psychogenic nonepileptic “seizures” or “attacks”? It’s not just semantics: “Seizures.” Neurology 2010;75: 87–8.
56. Ramsay RE, Cohen A, Brown MC. Coexisting epilepsy and non-epileptic seizures. In: Non-epileptic seizures. Butterworth-Heinemann; 1998:47–54.
57. Stone J, Carson A, Sharpe M. Functional symptoms in neurology: management. J Neurol Neurosurg Psychiatry. 2005;6(Suppl 1):i13–i21.
58. LaFrance WC Jr, Bjornaes H. Designing treatment plans based on etiology of psychogenic nonepileptic seizures. In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s nonepileptic seizures. 3rd ed. New York: Cambridge University Press; 2010:266–80.
59. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 200;69:205–15.
60. Kroenke K. Efficacy of treatment of somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007:69:881–8.
61. LaFrance WC Jr, Miller IW, Ryan CE, et al. Cognitive behavioral therapy for psychogenic nonepileptic seizures. Epilepsy Behav 2009;14:591–6.
62. Chalder T. Non-epileptic attacks: a cognitive behavioral approach in a single case with a four-year follow-up. Clin Psychol Psychother 1996;3:291–7.
63. Betts T, Duffy N. Non-epileptic attack disorder (pseudoseizures) and sexual abuse: a review. In: Gram L, Johannessen SI, Osterman PE, et al, editors. Pseudo-epileptic seizures. Petersfield, UK: Wrightson Biomedical Publishing; 1993:55–66.
64. Lesser RP. Treatment and outcome of psychogenic nonepileptic seizures. Epilepsy Currents 2003;3:198–200.
65. Ramani V. Review of psychiatric treatment strategies in non-epileptic seizures. In: Rowan AJ, Gates JR, eds. Non-epileptic Seizures. 1st ed. Stoneham, MA: Butterworth Heinemann; 1993:259–67.
66. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94.
67. Bennet C, So NM, Smith WB, Thompson K. Structured treatment improves the outcome of nonepileptic events. Epilepsia 1997;38(Suppl 8):214.
68. McDade G, Brown SW. Non-epileptic seizures: management and predictive factors of outcome. Seizure 1992;1:7–10.
69. Bowman ES. Etiology and clinical course of pseudoseizures: relationship to trauma, depression, and dissociation. Psychosomatics 1993;34:333–42.
70. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63.
71. Vanderzant CW, Giordani B, Berent S, et al. Personality of patients with pseudoseizures. Neurology 1986;36:664–8.
72. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001; 57:915–7.
73. Glosser G, Roberts D, et al. Nonepileptic seizures after resective epilepsy surgery. Epilepsia 1999; 40:1750–4.
74. Reuber M, Kral T. New-onset psychogenic seizures after intracranial neurosurgery. Acta Neurochir (Wien) 2002; 144:901–7.
75. Williamson P, Spencer D, Spencer S, et al. Complex partial seizures of frontal lobe origin. Ann Neurol 1985;18:497–504.
76. Saygi S, Katz A, Marks D, et al. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology 1992;42:1274–7.
77. Waterman K, Purves S, Kosaka B, et al. An epileptic syndrome caused by mesial frontal lobe seizure foci. Neurology 1987; 37:577–82.
78. Sussman N, Jackel R, Kaplan L, et al. Bicycling movements as a manifestation of complex partial seizures of temporal lobe origin. Epilepsia 1989;30:527–31.
1. Krumholz A. Nonepileptic seizures: diagnosis and management. Neurology 1999;S76–83.
2. Meierkord H, Will B, Fish D, Shorvon S. The clinical features and prognosis of pseudoseizures diagnosed using video-EEG telemetry. Neurology 1991;41:1643–6.
3. Lesser RP. Psychogenic seizures. Neurology 1996;46:1499–1507.
4. Sigurdardottir KR, Olafsson E. Incidence of psychogenic seizures in adults: a population-based study in Iceland. Epilepsia 1998;39:857–62.
5. Szaflarski JP, Szaflarski M, Hughes C, et al. Psychopathology and quality of life: psychogenic non-epileptic seizures versus epilepsy. Med Sci Monit 2003 9:CR113–8.
6. Barry E, Krumholz A, Bergey C, et al. Nonepileptic posttraumatic seizures. Epilepsia 1998;39:427–31.
7. Pakalnis A, Drake ME, Phillips B. Neuropsychiatric aspects of psychogenic status epilepticus. Neurology 1991;41;1104–6.
8. Walzack TS, Papacostas S, Williams DT, et al. Outcome after the diagnosis of psychogenic nonepileptic seizures. Epilepsia 1995;36:1131–7.
9. Metrick ME, Ritter FJ, Gates JR, et al. Nonepileptic events in childhood. Epilepsia 1991;32:322–8.
10. Wyllie E, Friedman D, Luders H, et al. Outcome of psychogenic seizures in children and adolescents compared to adults. Neurology 1991;41:742–4.
11. Duncan R, Oto M. Predictors of antecedent factors in psychogenic nonepileptic attacks: multivariate analysis. Neurology 2008;71:1000–5.
12. Alper K, Devinsky O, Perrine K, et al. Nonepileptic seizures and childhood sexual and physical abuse. Neurology 1993; 43:1950–3.
13. LaFrance WC Jr, Devinsky O. The treatment of nonepileptic seizures: historical perspectives and future directions. Epilepsia 2004;45 Suppl 2:15–21.
14. Westbrook LE, Devinsky O, Geocadin R. Nonepileptic seizures after head injury. Epilepsia 1998;39:978–82.
15. Slavney PR. Perspectives on hysteria. Baltimore: Johns Hopkins University Press; 1990.
16. Veith I. Hysteria: the history of a disease. Chicago: University of Chicago Press; 1965.
17. Goetz CG. Charcot the clinician. The Tuesday lessons. New York: Raven Press; 1987.
18. Massey EW, McHenry LC. Hysteroepilepsy in the nineteenth century: Charcot and Gowers. Neurology 1986;36:65–7.
19. Zeigler FJ, Imboden JB, Meyer E. Contemporary conversion reactions: a clinical study. Am J Psychiatry 1960;116:901–10.
20. Liske E, Forster FM. Pseudoseizures: a problem in the diagnosis and management of epileptic patients. Neurology 1964;14:41–9.
21. Diagnostic and statistical manual of mental disorders. DSM-IV 4th ed. American Psychiatric Association. Washington, DC; 1995.
22. Krumholz A, Niedermeyer, E. Psychogenic seizures: a clinical study with follow-up data. Neurology 1983; 33:498-502.
23. Krumholz A, Ting T. Co-existing epileptic and nonepileptic seizures. in imitators of epilepsy. 2nd ed. In: Kaplan PW, Fisher RS, editors. New York: Demos Medical Publishing; 2005:261–76.
24. Gates JR, Ramani V, Whalen S, Loewenson R. Ictal characteristics of pseudoseizures. Arch Neurol 1985;42:1183–87.
25. Leis AA, Ross MA, Summers AK. Psychogenic seizures: Ictal characteristics and diagnostic pitfalls. Neurology 1992;42:95–9.
26. Walczak TS, Bogolioubov. Weeping during psychogenic nonepileptic seizures. Epilepsia 1996;37:207–10.
27. Bergen D, Ristanovic R. Weeping is a common element during psychogenic nonepileptic seizures. Arch Neurol 1993;50:1059–60.
28. Peguero E, Abou-Khalil B, Fakhoury, Mathews G. Self-injury and incontinence in psychogenic seizures. Epilepsia 1995;36:586–91.
29. Orbach D, Ritaccio A, Devinsky O. Psychogenic, nonepileptic seizures associated with video-EEG-verified sleep. Epilepsia 2003;44:64–8.
30. Walczak TS, Williams DT, Berton W. Utility and reliability of placebo infusion in the evaluation of patients with seizures. Neurology 1994;44:394–99.
31. Bazil CW, Kothari M, Luciano D, et al. Provocation of nonepileptic seizures by suggestion in a general seizure population. Epilepsia 1994;35:768–70.
32. Devinsky O, Fisher RS. Ethical use of placebos and provocative testing in diagnosing nonepileptic seizures. Neurology 1996;47:866–70.
33. Lesser RP, Lueders H, Dinner DS. Evidence for epilepsy is rare in patients with psychogenic seizures. Neurology 1983; 33:502–4.
34. Barre MA, Burnstine TH, Fisher RS, Lesser RP. Electroencephalographic changes during simple partial seizures. Epilepsia 1994;35:715–20.
35. Trimble MR. Serum prolactin levels in epilepsy and hysteria. BMJ 1978;2:1682.
36. Laxer KD, Mullooly JP, Howell B. Prolactin changes after seizures classified by EEG monitoring. Neurology 1985; 35:31–5.
37. Pritchard PB, Wannamaker BB, Sagel J, et al. Endocrine function following complex partial seizures. Ann Neurol 1983;14:27–32.
38. Malkowicz DE, Legido A, Jackel RA, et al. Prolactin secretion following repetitive seizures. Neurology 1995;45:448–52.
39. Oribe E, Rohullah A, Nissenbaum E, Boal B. Serum prolactin concentrations are elevated after syncope. Neurology 1996;47:60–2.
40. Henrichs TF, Tucker DM, Farha J, Novelly RA. MMPI indices in the identification of patients evidencing pseudoseizures. Epilepsia 1988;29:184–8.
41. Wilkus RJ, Dodrill CB. Factors affecting the outcome of MMPI and neuropsychological assessments of psychogenic and epileptic seizure patients. Epilepsia 1989;30:339–47.
42. DeTimary P, Fouchet P, Sylin M, et al. Non–epileptic seizures: delayed diagnosis in patients presenting with electroencephalographic (EEG) or clinical signs of epileptic seizures. Seizure 2002;11:193–7.
43. Reuber M, Fernandez G, et al. Diagnostic delay in psychogenic nonepileptic seizures. Neurology 2002;58:493–5.
44. Rosenbaum DH, et al. Outpatient multidisciplinary management of non-epileptic seizures. In: Rowan AJ, Gates Jr, editors. Non-epileptic seizures. 1st ed. Stoneham, MA: Butterworth-Heinemann; 1993:275–83.
45. Lempert T, Schmidt D. Natural history and outcome of psychogenic seizures: a clinical study in 50 patients. J Neurol 1990;237:35–8.
46. Selwa LM, Geyer J, Nikakhtar N, et al. Nonepileptic seizure outcome varies by type of spell and duration of illness. Epilepsia 2000;41:1330–4.
47. Buchanan N, Snars J. Pseudoseizures (non epileptic attack disorder): clinical management and outcome in 50 patients. Seizure 1993;2:141–6.
48. Kanner AM. More controversies on the treatment of psychogenic pseudoseizures: an addendum. Epilepsy Behav 2003;4:360–4.
49. Aboukasm A, Mahr G, Gahry BR, et al. Retrospective analysis of the effects of psychotherapeutic interventions on outcomes of psychogenic nonepileptic seizures. Epilepsia 1998;39:470–3.
50. Reuber M, Pukrop T, Bauer J, et al. Outcome in psychogenic nonepileptic seizures: 1 to 10-year follow-up in 164 patients. Ann Neurol 2003;53:305–11.
51. McKenzie P, Oto M, Russell A, Pelosi A, Duncan R. Early outcomes and predictors in 260 patients with psychogenic nonepileptic seizures (PNES). Neurology 2010;74:64–9.
52. Kanner AM, Parra J, Frey M, et al. Psychiatric and neurologic predictors of psychogenic pseudoseizure outcome. Neurology 1999;53:933–8.
53. Shen W, Bowman ES, Markand ON. Presenting the diagnosis of pseudoseizure. Neurology 1990; 40:756–9.
54. Friedman JH, LaFrance Jr WC. Psychogenic disorders: the need to speak plainly. Arch Neurol 2010;67:753–5.
55. LaFrance Jr WC. Psychogenic nonepileptic “seizures” or “attacks”? It’s not just semantics: “Seizures.” Neurology 2010;75: 87–8.
56. Ramsay RE, Cohen A, Brown MC. Coexisting epilepsy and non-epileptic seizures. In: Non-epileptic seizures. Butterworth-Heinemann; 1998:47–54.
57. Stone J, Carson A, Sharpe M. Functional symptoms in neurology: management. J Neurol Neurosurg Psychiatry. 2005;6(Suppl 1):i13–i21.
58. LaFrance WC Jr, Bjornaes H. Designing treatment plans based on etiology of psychogenic nonepileptic seizures. In: Schachter SC, LaFrance WC Jr, editors. Gates and Rowan’s nonepileptic seizures. 3rd ed. New York: Cambridge University Press; 2010:266–80.
59. Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of controlled clinical trials. Psychother Psychosom 200;69:205–15.
60. Kroenke K. Efficacy of treatment of somatoform disorders: a review of randomized controlled trials. Psychosom Med 2007:69:881–8.
61. LaFrance WC Jr, Miller IW, Ryan CE, et al. Cognitive behavioral therapy for psychogenic nonepileptic seizures. Epilepsy Behav 2009;14:591–6.
62. Chalder T. Non-epileptic attacks: a cognitive behavioral approach in a single case with a four-year follow-up. Clin Psychol Psychother 1996;3:291–7.
63. Betts T, Duffy N. Non-epileptic attack disorder (pseudoseizures) and sexual abuse: a review. In: Gram L, Johannessen SI, Osterman PE, et al, editors. Pseudo-epileptic seizures. Petersfield, UK: Wrightson Biomedical Publishing; 1993:55–66.
64. Lesser RP. Treatment and outcome of psychogenic nonepileptic seizures. Epilepsy Currents 2003;3:198–200.
65. Ramani V. Review of psychiatric treatment strategies in non-epileptic seizures. In: Rowan AJ, Gates JR, eds. Non-epileptic Seizures. 1st ed. Stoneham, MA: Butterworth Heinemann; 1993:259–67.
66. Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for psychogenic nonepileptic seizures: a pilot RCT. Neurology 2010;74:1986–94.
67. Bennet C, So NM, Smith WB, Thompson K. Structured treatment improves the outcome of nonepileptic events. Epilepsia 1997;38(Suppl 8):214.
68. McDade G, Brown SW. Non-epileptic seizures: management and predictive factors of outcome. Seizure 1992;1:7–10.
69. Bowman ES. Etiology and clinical course of pseudoseizures: relationship to trauma, depression, and dissociation. Psychosomatics 1993;34:333–42.
70. Bowman ES, Markand ON. Psychodynamics and psychiatric diagnoses of pseudoseizure subjects. Am J Psychiatry 1996;153:57–63.
71. Vanderzant CW, Giordani B, Berent S, et al. Personality of patients with pseudoseizures. Neurology 1986;36:664–8.
72. Benbadis SR, Agrawal V, Tatum WO. How many patients with psychogenic nonepileptic seizures also have epilepsy? Neurology 2001; 57:915–7.
73. Glosser G, Roberts D, et al. Nonepileptic seizures after resective epilepsy surgery. Epilepsia 1999; 40:1750–4.
74. Reuber M, Kral T. New-onset psychogenic seizures after intracranial neurosurgery. Acta Neurochir (Wien) 2002; 144:901–7.
75. Williamson P, Spencer D, Spencer S, et al. Complex partial seizures of frontal lobe origin. Ann Neurol 1985;18:497–504.
76. Saygi S, Katz A, Marks D, et al. Frontal lobe partial seizures and psychogenic seizures: comparison of clinical and ictal characteristics. Neurology 1992;42:1274–7.
77. Waterman K, Purves S, Kosaka B, et al. An epileptic syndrome caused by mesial frontal lobe seizure foci. Neurology 1987; 37:577–82.
78. Sussman N, Jackel R, Kaplan L, et al. Bicycling movements as a manifestation of complex partial seizures of temporal lobe origin. Epilepsia 1989;30:527–31.