User login
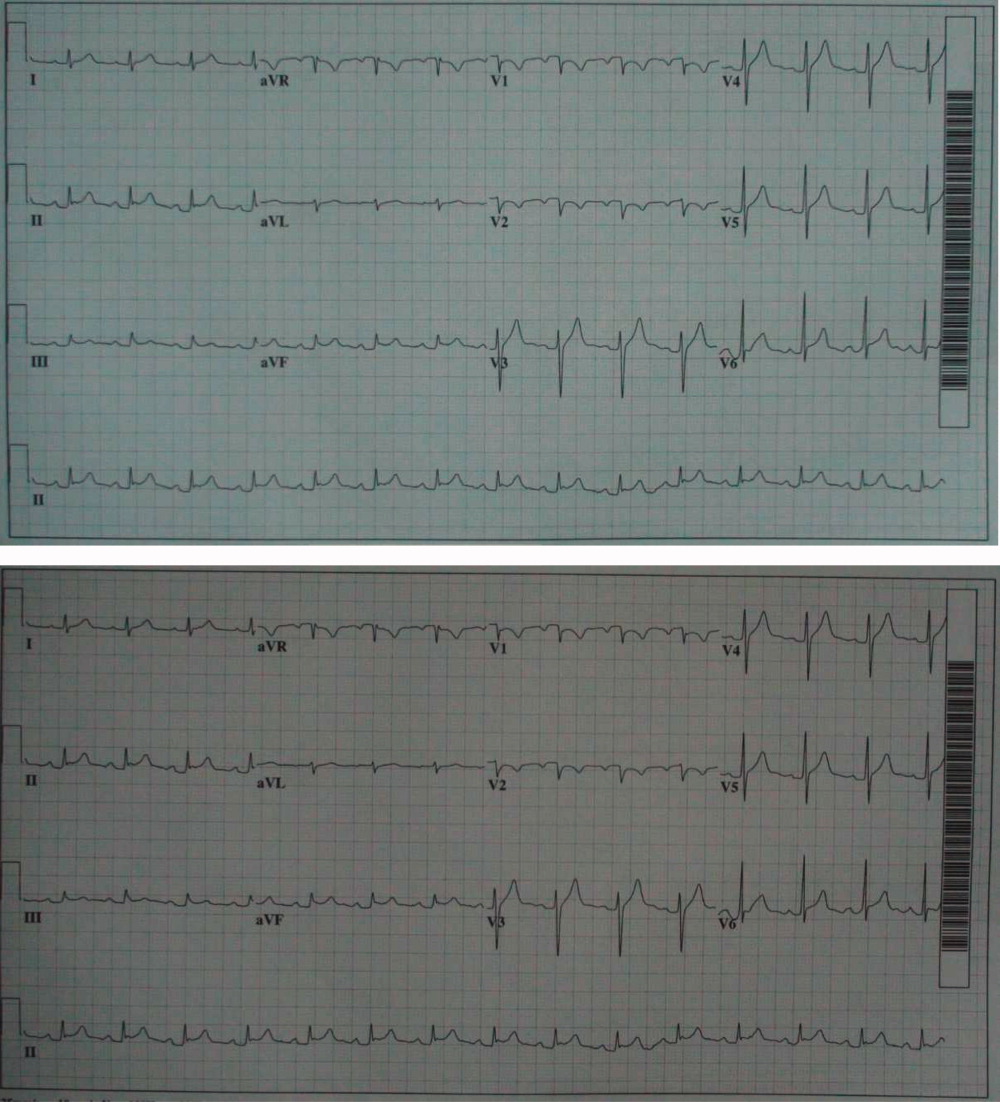
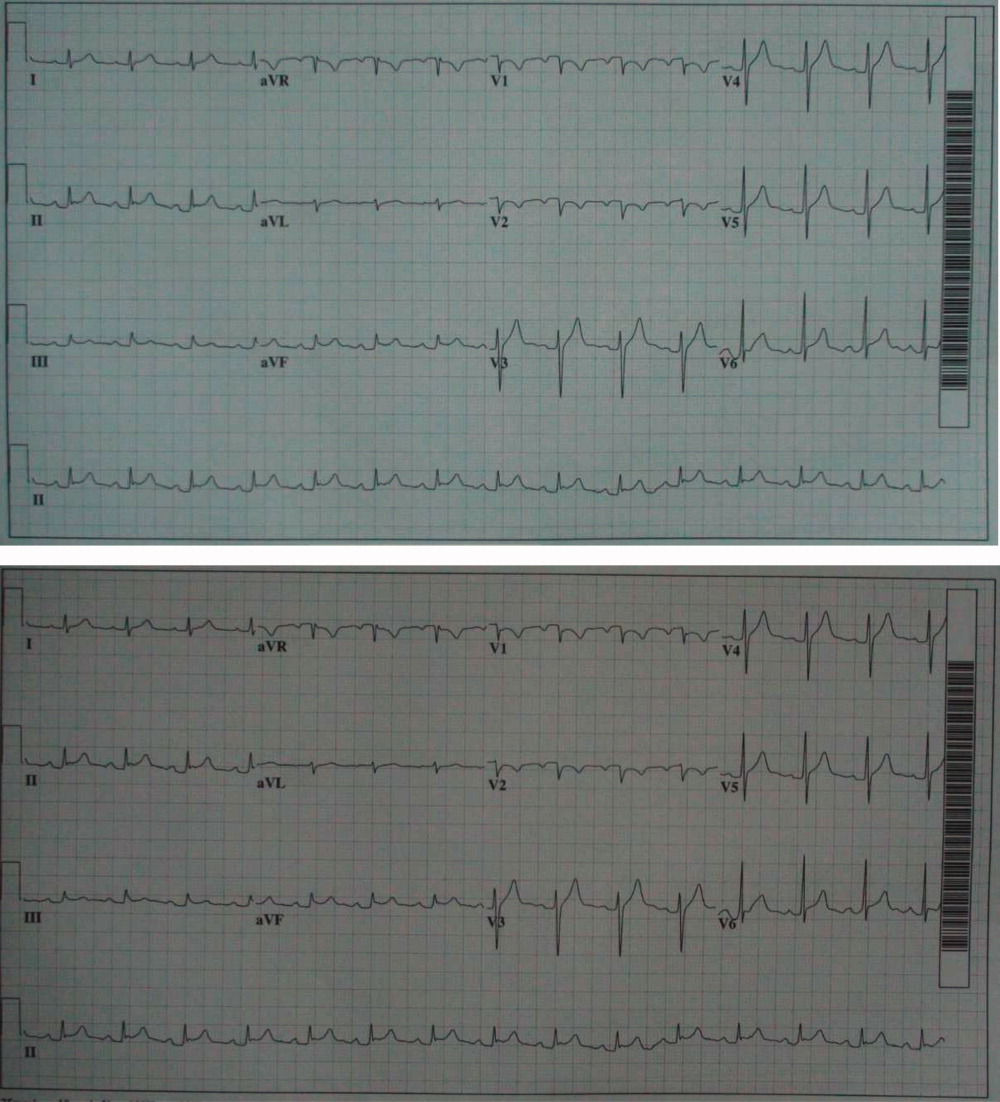
A 57‐year‐old man with Hepatitis B and C was scheduled for an outpatient computed tomography (CT)‐guided biopsy of the left lobe of the liver for grading and staging of his liver disease at an outside hospital. Complete metabolic profile (CMP), complete blood count (CBC) and international normalized ratio (INR) were performed and were normal. Following his liver biopsy, the patient became hypotensive and developed shock. He received fluid resuscitation. Clinical exam and an abdominal x‐ray failed to identify a hepatic or intraperitoneal source of bleeding to explain the cause of hypotension. A chest radiograph showed an enlarged cardiac silhouette with clear lung fields. An electrocardiogram (ECG) demonstrated (Figure 1) 1‐mm ST segment elevation in the anterior leads. An emergent echocardiogram showed a significant pericardial effusion with echocardiographic evidence of cardiac tamponade. The patient underwent emergent pericardiocentesis with removal of 400 mL of hemorrhagic fluid. The etiology of the hemorrhagic fluid was thought to be due to myocardial injury secondary to the liver biopsy. Subsequently, the histopathology of the liver biopsy reported (Figure 2) features suggestive of cirrhosis of the liver. Additional tissues from the biopsy included pericardium, myocardium and coronary artery. The patient was transferred to our institution for a cardiac catheterization and coronary angiogram to evaluate his coronary anatomy. The coronary angiogram was normal without any evidence of dye extravasation. A follow‐up echocardiogram and CT scan of the chest showed residual pericardial and pleural fluid. The remainder of the hospital stay was uneventful and he was discharged on day 7 in good condition. He was doing well a month later at the time of his follow‐up visit.0, 0

Discussion
Serious complications of liver biopsy occur in less than 1% of biopsied patients and include intraperitoneal1 or intrahepatic hemorrhage,2, 3 pneumothorax, hemothorax, hemobilia,1 and injury to the gall bladder, colon, kidney and lung. Other rare complications of percutaneous liver biopsy include biliary ascites, bile pleuritis, bile peritonitis, subcutaneous emphysema, pneumoperitoneum, subphrenic abscess, carcinoid crisis, anaphylaxis after biopsy of an echinococcal cyst, pancreatitis due to hemobilia, and breakage of the biopsy needle.1, 4, 5 Bleeding is more common in the elderly and in patients with cirrhosis and liver cancer.1, 6 The most common cause of shock in a patient after liver biopsy is hypovolemia from intrahepatic or intraperitoneal bleeding. The incidence of such complications may be higher than commonly appreciated as these complications are likely underreported.
Ultrasound (US)‐guided and CT‐guided techniques are 2 common methods for performing liver biopsy. US‐guided and CT‐guided liver biopsy each have their own benefits and limitations. The CT‐guided biopsy provides an excellent resolution of the liver architecture and is done from the epigastric region, but uses a static view. The US‐guided liver biopsy, on the other hand, is done from the mid‐axillary intercostal line and is performed with real‐time images.
Our patient's complication was presumably caused by accidental passage of the biopsy needle from the liver into the pericardium during respiratory movements. The coronary artery tissue was most likely not an epicardial vessel as supported by the normal angiogram without evidence of coronary artery perforation.
Our patient had an inadvertent biopsy of cardiac tissue during a liver biopsy resulting in a hemorrhagic pericardial effusion and tamponade. Cardiac tamponade as a complication of liver biopsy and intrathoracic percutaneous procedures has been described, although this has very rarely been reported.7, 8 Fortunately, the patient's coronary artery anatomy was normal and he did well without surgical intervention.
Unusual procedural complications are reported in the literature with the intention of increasing awareness and improving patient safety. Percutaneous liver biopsy is performed to stage and grade liver disease for assessment and treatment. However, as with any invasive procedure, there are potential risks and complications. In patients who present with hypotension and shock following liver biopsy, myocardial injury with cardiac tamponade should be considered in the differential diagnosis.
- , , , .Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies.J Hepatol.1986;2:165–173.
- , , .Intrahepatic hematoma: a complication of percutaneous liver biopsy.Gastroenterology.1974;67:284–289.
- , , , et al.Intrahepatic hematoma resulting in obstructive jaundice. An unusual complication of liver biopsy.Gastroenterology.1978;74(1):124–127.
- , , , .Liver biopsy: its safety and complications as seen at a liver transplant center.Transplantation.1993;55:1087–1090.
- , .Bile peritonitis after liver biopsy: nonsurgical management of a patient with an acute abdomen: a case report with review of the literature.Am J Gastroenterol.1987;82:265–268.
- , .Outcome of patients hospitalized for complications after outpatient liver biopsy.Ann Intern Med.1993;118:96–98.
- , , .Unusual presentation and course of acute cardiac tamponade.J Cardiothorac Vasc Anesth.2007;21:712–714.
- , , .Cardiac tamponade following fine needle aspiration (FNA) of a mediastinal mass.Clin Radiol.1998;53(2):151–152.
A 57‐year‐old man with Hepatitis B and C was scheduled for an outpatient computed tomography (CT)‐guided biopsy of the left lobe of the liver for grading and staging of his liver disease at an outside hospital. Complete metabolic profile (CMP), complete blood count (CBC) and international normalized ratio (INR) were performed and were normal. Following his liver biopsy, the patient became hypotensive and developed shock. He received fluid resuscitation. Clinical exam and an abdominal x‐ray failed to identify a hepatic or intraperitoneal source of bleeding to explain the cause of hypotension. A chest radiograph showed an enlarged cardiac silhouette with clear lung fields. An electrocardiogram (ECG) demonstrated (Figure 1) 1‐mm ST segment elevation in the anterior leads. An emergent echocardiogram showed a significant pericardial effusion with echocardiographic evidence of cardiac tamponade. The patient underwent emergent pericardiocentesis with removal of 400 mL of hemorrhagic fluid. The etiology of the hemorrhagic fluid was thought to be due to myocardial injury secondary to the liver biopsy. Subsequently, the histopathology of the liver biopsy reported (Figure 2) features suggestive of cirrhosis of the liver. Additional tissues from the biopsy included pericardium, myocardium and coronary artery. The patient was transferred to our institution for a cardiac catheterization and coronary angiogram to evaluate his coronary anatomy. The coronary angiogram was normal without any evidence of dye extravasation. A follow‐up echocardiogram and CT scan of the chest showed residual pericardial and pleural fluid. The remainder of the hospital stay was uneventful and he was discharged on day 7 in good condition. He was doing well a month later at the time of his follow‐up visit.0, 0
Discussion
Serious complications of liver biopsy occur in less than 1% of biopsied patients and include intraperitoneal1 or intrahepatic hemorrhage,2, 3 pneumothorax, hemothorax, hemobilia,1 and injury to the gall bladder, colon, kidney and lung. Other rare complications of percutaneous liver biopsy include biliary ascites, bile pleuritis, bile peritonitis, subcutaneous emphysema, pneumoperitoneum, subphrenic abscess, carcinoid crisis, anaphylaxis after biopsy of an echinococcal cyst, pancreatitis due to hemobilia, and breakage of the biopsy needle.1, 4, 5 Bleeding is more common in the elderly and in patients with cirrhosis and liver cancer.1, 6 The most common cause of shock in a patient after liver biopsy is hypovolemia from intrahepatic or intraperitoneal bleeding. The incidence of such complications may be higher than commonly appreciated as these complications are likely underreported.
Ultrasound (US)‐guided and CT‐guided techniques are 2 common methods for performing liver biopsy. US‐guided and CT‐guided liver biopsy each have their own benefits and limitations. The CT‐guided biopsy provides an excellent resolution of the liver architecture and is done from the epigastric region, but uses a static view. The US‐guided liver biopsy, on the other hand, is done from the mid‐axillary intercostal line and is performed with real‐time images.
Our patient's complication was presumably caused by accidental passage of the biopsy needle from the liver into the pericardium during respiratory movements. The coronary artery tissue was most likely not an epicardial vessel as supported by the normal angiogram without evidence of coronary artery perforation.
Our patient had an inadvertent biopsy of cardiac tissue during a liver biopsy resulting in a hemorrhagic pericardial effusion and tamponade. Cardiac tamponade as a complication of liver biopsy and intrathoracic percutaneous procedures has been described, although this has very rarely been reported.7, 8 Fortunately, the patient's coronary artery anatomy was normal and he did well without surgical intervention.
Unusual procedural complications are reported in the literature with the intention of increasing awareness and improving patient safety. Percutaneous liver biopsy is performed to stage and grade liver disease for assessment and treatment. However, as with any invasive procedure, there are potential risks and complications. In patients who present with hypotension and shock following liver biopsy, myocardial injury with cardiac tamponade should be considered in the differential diagnosis.
A 57‐year‐old man with Hepatitis B and C was scheduled for an outpatient computed tomography (CT)‐guided biopsy of the left lobe of the liver for grading and staging of his liver disease at an outside hospital. Complete metabolic profile (CMP), complete blood count (CBC) and international normalized ratio (INR) were performed and were normal. Following his liver biopsy, the patient became hypotensive and developed shock. He received fluid resuscitation. Clinical exam and an abdominal x‐ray failed to identify a hepatic or intraperitoneal source of bleeding to explain the cause of hypotension. A chest radiograph showed an enlarged cardiac silhouette with clear lung fields. An electrocardiogram (ECG) demonstrated (Figure 1) 1‐mm ST segment elevation in the anterior leads. An emergent echocardiogram showed a significant pericardial effusion with echocardiographic evidence of cardiac tamponade. The patient underwent emergent pericardiocentesis with removal of 400 mL of hemorrhagic fluid. The etiology of the hemorrhagic fluid was thought to be due to myocardial injury secondary to the liver biopsy. Subsequently, the histopathology of the liver biopsy reported (Figure 2) features suggestive of cirrhosis of the liver. Additional tissues from the biopsy included pericardium, myocardium and coronary artery. The patient was transferred to our institution for a cardiac catheterization and coronary angiogram to evaluate his coronary anatomy. The coronary angiogram was normal without any evidence of dye extravasation. A follow‐up echocardiogram and CT scan of the chest showed residual pericardial and pleural fluid. The remainder of the hospital stay was uneventful and he was discharged on day 7 in good condition. He was doing well a month later at the time of his follow‐up visit.0, 0
Discussion
Serious complications of liver biopsy occur in less than 1% of biopsied patients and include intraperitoneal1 or intrahepatic hemorrhage,2, 3 pneumothorax, hemothorax, hemobilia,1 and injury to the gall bladder, colon, kidney and lung. Other rare complications of percutaneous liver biopsy include biliary ascites, bile pleuritis, bile peritonitis, subcutaneous emphysema, pneumoperitoneum, subphrenic abscess, carcinoid crisis, anaphylaxis after biopsy of an echinococcal cyst, pancreatitis due to hemobilia, and breakage of the biopsy needle.1, 4, 5 Bleeding is more common in the elderly and in patients with cirrhosis and liver cancer.1, 6 The most common cause of shock in a patient after liver biopsy is hypovolemia from intrahepatic or intraperitoneal bleeding. The incidence of such complications may be higher than commonly appreciated as these complications are likely underreported.
Ultrasound (US)‐guided and CT‐guided techniques are 2 common methods for performing liver biopsy. US‐guided and CT‐guided liver biopsy each have their own benefits and limitations. The CT‐guided biopsy provides an excellent resolution of the liver architecture and is done from the epigastric region, but uses a static view. The US‐guided liver biopsy, on the other hand, is done from the mid‐axillary intercostal line and is performed with real‐time images.
Our patient's complication was presumably caused by accidental passage of the biopsy needle from the liver into the pericardium during respiratory movements. The coronary artery tissue was most likely not an epicardial vessel as supported by the normal angiogram without evidence of coronary artery perforation.
Our patient had an inadvertent biopsy of cardiac tissue during a liver biopsy resulting in a hemorrhagic pericardial effusion and tamponade. Cardiac tamponade as a complication of liver biopsy and intrathoracic percutaneous procedures has been described, although this has very rarely been reported.7, 8 Fortunately, the patient's coronary artery anatomy was normal and he did well without surgical intervention.
Unusual procedural complications are reported in the literature with the intention of increasing awareness and improving patient safety. Percutaneous liver biopsy is performed to stage and grade liver disease for assessment and treatment. However, as with any invasive procedure, there are potential risks and complications. In patients who present with hypotension and shock following liver biopsy, myocardial injury with cardiac tamponade should be considered in the differential diagnosis.
- , , , .Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies.J Hepatol.1986;2:165–173.
- , , .Intrahepatic hematoma: a complication of percutaneous liver biopsy.Gastroenterology.1974;67:284–289.
- , , , et al.Intrahepatic hematoma resulting in obstructive jaundice. An unusual complication of liver biopsy.Gastroenterology.1978;74(1):124–127.
- , , , .Liver biopsy: its safety and complications as seen at a liver transplant center.Transplantation.1993;55:1087–1090.
- , .Bile peritonitis after liver biopsy: nonsurgical management of a patient with an acute abdomen: a case report with review of the literature.Am J Gastroenterol.1987;82:265–268.
- , .Outcome of patients hospitalized for complications after outpatient liver biopsy.Ann Intern Med.1993;118:96–98.
- , , .Unusual presentation and course of acute cardiac tamponade.J Cardiothorac Vasc Anesth.2007;21:712–714.
- , , .Cardiac tamponade following fine needle aspiration (FNA) of a mediastinal mass.Clin Radiol.1998;53(2):151–152.
- , , , .Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies.J Hepatol.1986;2:165–173.
- , , .Intrahepatic hematoma: a complication of percutaneous liver biopsy.Gastroenterology.1974;67:284–289.
- , , , et al.Intrahepatic hematoma resulting in obstructive jaundice. An unusual complication of liver biopsy.Gastroenterology.1978;74(1):124–127.
- , , , .Liver biopsy: its safety and complications as seen at a liver transplant center.Transplantation.1993;55:1087–1090.
- , .Bile peritonitis after liver biopsy: nonsurgical management of a patient with an acute abdomen: a case report with review of the literature.Am J Gastroenterol.1987;82:265–268.
- , .Outcome of patients hospitalized for complications after outpatient liver biopsy.Ann Intern Med.1993;118:96–98.
- , , .Unusual presentation and course of acute cardiac tamponade.J Cardiothorac Vasc Anesth.2007;21:712–714.
- , , .Cardiac tamponade following fine needle aspiration (FNA) of a mediastinal mass.Clin Radiol.1998;53(2):151–152.