User login
CASE: Unexpectedly high fetal weight, shoulder dystocia
A nurse midwife is managing the labor of a 41-year-old, G3P2 woman who had two prior spontaneous vaginal deliveries. Results of her glucose-loading test were normal. The midwife estimates the fetal weight as 7 lb 8 oz, but the birth weight proves to be 10 lb 6 oz. After delivery of the head, a turtle sign is obvious, and a shoulder dystocia is declared.
An emergency call for help is made to the front desk. The mother is asked to stop pushing. The obstetric nurse and midwife perform a McRoberts maneuver and apply suprapubic pressure without success. The woman is placed in the Gaskin’s all-fours position, but delivery cannot be accomplished.
Roused from your call room, you quickly proceed to help the team. At 3 minutes into the shoulder dystocia, you enter the room. As the emergency responder, what sequence of maneuvers will you use to resolve the shoulder dystocia?
In response to a shoulder dystocia emergency, most of us have practiced a sequence of actions:
- recognize shoulder dystocia early and communicate with staff
- instruct the mother to stop pushing and move the mother’s buttocks to the edge of the birthing bed
- ensure there is not a tight nuchal cord
- commit to avoid using excessive force on the fetal head and neck
- call for emergency help from other expert clinicians
- perform the McRoberts maneuver combined with suprapubic pressure
- consider performing an episiotomy
- use a rotational maneuver such as the Woods screw or Rubin maneuver
- deliver the posterior arm
- consider rarely used “salvage maneuvers,” such as the Zavanelli maneuver with cesarean delivery.1
When you are called to a shoulder dystocia as the emergency responder, the sequence of maneuvers is likely dependent on the actions already attempted by the primary clinician and the length of time from identification of the shoulder dystocia to the responder’s arrival at the patient’s bedside.
Based on my experience, if the primary clinician already has attempted the McRoberts maneuver, suprapubic pressure, and other advanced maneuvers without success, it is best for you to immediately move to the advanced maneuvers with which you are most comfortable. These advanced maneuvers typically include:
- consider an episiotomy and then a rotational maneuver (Woods screw or Rubin maneuver)
- attempt to deliver the posterior arm.
Woods screw and Rubin rotational maneuvers
Woods screw: Removing a well-placed screw requires a rotational maneuver. The Woods screw maneuver is based on the idea that a large baby is like a screw that must maneuver through pelvic threads. You cannot easily directly pull a well-set screw from its threads.
In Woods’ original description of the maneuver, the fetal spine was toward the mother’s right. Woods described a rotational maneuver that is performed by placing the left hand on the mother’s abdomen to provide judicious downward thrust on the fetal buttocks while simultaneously using the fingers of the right hand, placed on the ANTERIOR aspect of the shoulder, to create a clockwise rotational force on the fetus. Using the right hand, the fetal shoulder is moved through >180°, past the 12 o’clock position. At the same time, the fundal pressure and the fingers of the right hand are used to guide the fetus down the birth canal. This maneuver moves the anterior shoulder to the posterior position.
If delivery cannot be completed, a second step in the procedure is to then place the fingers of the right hand on the ANTERIOR aspect of the posterior shoulder (previously the anterior shoulder) and rotate the fetus in a counter-clockwise arc to the 12 o’clock position while gently guiding the fetus down the birth canal.2
Rubin rotational maneuver. Rubin observed that if you adduct the shoulders, the diameter of the shoulders are reduced, thereby easing the passage of the fetus through the birth canal. Adduction is the movement of a body part toward the MIDLINE sagittal plane.
Rubin recommended applying pressure to the POSTERIOR surface of the posterior (6 o’clock) fetal shoulder to help push the shoulder toward the midline of the chest (adduction). If the fetal spine is toward the mother’s left side, you place your right hand on the POSTERIOR surface of the shoulder at the 6 o’clock position, rotating the shoulder in a clockwise arc to the 12 o’clock position while simultaneously guiding the fetus down the birth canal.
Rubin also recommended the use of judicious fundal pressure after the anterior shoulder is disimpacted, if necessary, to facilitate delivery.3 Although both Woods and Rubin recommended the use of judiciously applied fundal pressure, most modern textbooks of obstetrics do not endorse the use of fundal pressure.
Delivery of the posterior arm: My preferred first maneuver
When I arrive as an emergency responder to a shoulder dystocia delivery, my preferred maneuver is to deliver the posterior arm. Many experts recommend prioritizing this maneuver when attempting to resolve a difficult shoulder dystocia.4-7
Delivery of the posterior arm is performed by inserting the hand and forearm into the sacral hollow. The left hand and forearm are used if the fetal spine is toward the mother’s left, and vice-versa. The posterior humerus is identified and followed to the elbow. The fetal forearm is flexed and swept across the fetal chest. The wrist or hand is then grasped and the arm is extended along the fetal trunk and face, which delivers the posterior arm from the vagina. This results in a reduction in the presenting diameter and the anterior shoulder usually can be delivered with minimal force.
If the delivery of the posterior arm does not resolve the shoulder dystocia, gently support the fetal head and posterior arm, and rotate the fetus 180° using pressure on the posterior surface of the shoulder.
When a fetus is macrosomic, the posterior arm can be fully extended in utero, with the hand below the level of the fetal groin. In such situations, it can be difficult to execute the delivery of the posterior arm.8 A back-up technique is to manipulate the posterior axilla to accomplish delivery.
Manipulation of the posterior axilla
When the posterior arm cannot be reached, these maneuvers may be helpful
One of the earliest written descriptions of resolving a severe shoulder dystocia by manipulating the posterior axilla was provided by Percival Willughby (born 1596, died 1685). He wrote:
- “After the head is born, if the child through the greatness of the shoulders, should stick at the neck, let the midwife put her fingers under the child’s armpit and give it a nudge, thrusting it to the other side with her finger, drawing the child or she may quickly bring forth the shoulders, without offering to put it forth by her hands clasped about the neck, which might endanger the breaking of the neck.”9
Manipulation of the posterior axilla can either involve a rotational maneuver (using the axilla to rotate the fetus through 180°) or it can be used to pull the posterior shoulder into the hollow of the sacrum and down the birth canal.
Schramm advocated using the posterior axilla to rotate the fetus. She recommended placing 1 or 2 fingers of the right hand in the posterior axilla and then rotating the posterior shoulder into the 12 o’clock position while simultaneously using the left hand to provide gentle guidance on the fetal neck.10
Menticoglou advocated using manipulation of the posterior axilla to draw the fetal shoulder into the sacral hollow and down the birth canal, thereby releasing the anterior shoulder. In the Menticoglou maneuver the middle fingers of the right and left hand of the obstetrician are hooked into the fetal axilla, one finger from the fetus’ front and the other from the fetus’ back. The fingers overlap each other within the fetal posterior axilla. Downward traction is then exerted on the fetal axilla and the posterior shoulder is pulled outward along the curve of the sacrum (FIGURE).11
Sandmire recommended combining fundal pressure with axillary traction and rotation to facilitate delivery.12
The posterior axillary maneuvers are seldom described in modern textbooks of obstetrics and represent a lost art. I have found that they can be useful when the posterior arm cannot be reached. The fetal posterior axilla is almost always closer to the vaginal introitus than the fetal hand or arm, and if the posterior arm cannot be reached, it is a valuable maneuver to have in your armamentarium.
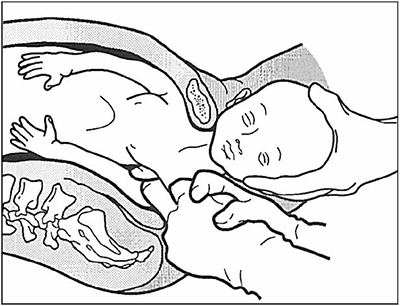
Manipulation of the posterior axilla
The right and left third fingers are locked into the posterior axilla, one finger from the front and one from the back of the fetus. Gentle downward guidance is provided by the fingers to draw the posterior shoulder down and out along the curve of the sacrum, thus releasing the anterior shoulder. In this drawing, an assistant gently holds the head up.
(Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108:755–757. Reprinted with permission from Wolters Kluwer.)
My recommendation
Shoulder dystocia emergencies are an important cause of neonatal injury, including brachial plexus injury, fractures of the humerus, and hypoxic-ischemic encephalopathy. Obstetricians and midwives relentlessly train to resolve shoulder dystocia births with alacrity and minimal fetal trauma. When you are called as an emergency responder in a shoulder dystocia birth, I recommend that you prioritize a rotational maneuver or delivery of the posterior arm, and add manipulation of the posterior axilla to your armamentarium.
1. Burkman RT. Stop all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia. OBG Manage. 2013;25(3):22, 24, 28.
2. Woods CE. A principle of physics as applicable to shoulder dystocia. Am J Obstet Gynecol. 1943;45:796-804.
3. Rubin A. Management of shoulder dystocia. JAMA. 1964;189:835-837.
4. Nocon JJ, McKenzie DK, Thomas LJ, Hansell RS. Shoulder dystocia: an analysis of risks and obstetric maneuvers. Am J Obstet Gynecol. 1993;168(6 pt 1):1732-1737.
5. Poggi SH, Spong CY, Allen RH. Prioritizing posterior arm delivery during severe shoulder dystocia. Obstet Gynecol. 2003;101(5 pt 2):1068-1072.
6. Kung J, Swan AV, Arulkumaran S. Delivery of the posterior arm reduces shoulder dimensions in shoulder dystocia. In J Gynecol Obstet. 2006;93(3):233-237.
7. Hoffman MK, Bailit JL, Branch DW, et al. A comparison of obstetric maneuvers for the acute management of shoulder dystocia. Obstet Gynecol. 2011;117(6):1272-1278.
8. Barnum CG. Dystocia due to the shoulders. Am J Obstet Gynecol. 1945;50:439-442.
9. Willughby P. Observations in midwifery. New York, NY: MW Books; 1972:312–3.
10. Schramm M. Impacted shoulders—a personal experience. Aust N Z J Obstet Gynaecol. 1983;23(1):28-31.
11. Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108(3 pt 2):755-757.
12. Sandmire HF. From Green Bay, a game plan for shoulder dystocia. OBG Manage. 1997;9:15-16.

Robert L. Barbieri, MD
Editor in Chief
[email protected]
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
[email protected]
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
[email protected]
Dr. Barbieri reports no financial relationships relevant to this article.
CASE: Unexpectedly high fetal weight, shoulder dystocia
A nurse midwife is managing the labor of a 41-year-old, G3P2 woman who had two prior spontaneous vaginal deliveries. Results of her glucose-loading test were normal. The midwife estimates the fetal weight as 7 lb 8 oz, but the birth weight proves to be 10 lb 6 oz. After delivery of the head, a turtle sign is obvious, and a shoulder dystocia is declared.
An emergency call for help is made to the front desk. The mother is asked to stop pushing. The obstetric nurse and midwife perform a McRoberts maneuver and apply suprapubic pressure without success. The woman is placed in the Gaskin’s all-fours position, but delivery cannot be accomplished.
Roused from your call room, you quickly proceed to help the team. At 3 minutes into the shoulder dystocia, you enter the room. As the emergency responder, what sequence of maneuvers will you use to resolve the shoulder dystocia?
In response to a shoulder dystocia emergency, most of us have practiced a sequence of actions:
- recognize shoulder dystocia early and communicate with staff
- instruct the mother to stop pushing and move the mother’s buttocks to the edge of the birthing bed
- ensure there is not a tight nuchal cord
- commit to avoid using excessive force on the fetal head and neck
- call for emergency help from other expert clinicians
- perform the McRoberts maneuver combined with suprapubic pressure
- consider performing an episiotomy
- use a rotational maneuver such as the Woods screw or Rubin maneuver
- deliver the posterior arm
- consider rarely used “salvage maneuvers,” such as the Zavanelli maneuver with cesarean delivery.1
When you are called to a shoulder dystocia as the emergency responder, the sequence of maneuvers is likely dependent on the actions already attempted by the primary clinician and the length of time from identification of the shoulder dystocia to the responder’s arrival at the patient’s bedside.
Based on my experience, if the primary clinician already has attempted the McRoberts maneuver, suprapubic pressure, and other advanced maneuvers without success, it is best for you to immediately move to the advanced maneuvers with which you are most comfortable. These advanced maneuvers typically include:
- consider an episiotomy and then a rotational maneuver (Woods screw or Rubin maneuver)
- attempt to deliver the posterior arm.
Woods screw and Rubin rotational maneuvers
Woods screw: Removing a well-placed screw requires a rotational maneuver. The Woods screw maneuver is based on the idea that a large baby is like a screw that must maneuver through pelvic threads. You cannot easily directly pull a well-set screw from its threads.
In Woods’ original description of the maneuver, the fetal spine was toward the mother’s right. Woods described a rotational maneuver that is performed by placing the left hand on the mother’s abdomen to provide judicious downward thrust on the fetal buttocks while simultaneously using the fingers of the right hand, placed on the ANTERIOR aspect of the shoulder, to create a clockwise rotational force on the fetus. Using the right hand, the fetal shoulder is moved through >180°, past the 12 o’clock position. At the same time, the fundal pressure and the fingers of the right hand are used to guide the fetus down the birth canal. This maneuver moves the anterior shoulder to the posterior position.
If delivery cannot be completed, a second step in the procedure is to then place the fingers of the right hand on the ANTERIOR aspect of the posterior shoulder (previously the anterior shoulder) and rotate the fetus in a counter-clockwise arc to the 12 o’clock position while gently guiding the fetus down the birth canal.2
Rubin rotational maneuver. Rubin observed that if you adduct the shoulders, the diameter of the shoulders are reduced, thereby easing the passage of the fetus through the birth canal. Adduction is the movement of a body part toward the MIDLINE sagittal plane.
Rubin recommended applying pressure to the POSTERIOR surface of the posterior (6 o’clock) fetal shoulder to help push the shoulder toward the midline of the chest (adduction). If the fetal spine is toward the mother’s left side, you place your right hand on the POSTERIOR surface of the shoulder at the 6 o’clock position, rotating the shoulder in a clockwise arc to the 12 o’clock position while simultaneously guiding the fetus down the birth canal.
Rubin also recommended the use of judicious fundal pressure after the anterior shoulder is disimpacted, if necessary, to facilitate delivery.3 Although both Woods and Rubin recommended the use of judiciously applied fundal pressure, most modern textbooks of obstetrics do not endorse the use of fundal pressure.
Delivery of the posterior arm: My preferred first maneuver
When I arrive as an emergency responder to a shoulder dystocia delivery, my preferred maneuver is to deliver the posterior arm. Many experts recommend prioritizing this maneuver when attempting to resolve a difficult shoulder dystocia.4-7
Delivery of the posterior arm is performed by inserting the hand and forearm into the sacral hollow. The left hand and forearm are used if the fetal spine is toward the mother’s left, and vice-versa. The posterior humerus is identified and followed to the elbow. The fetal forearm is flexed and swept across the fetal chest. The wrist or hand is then grasped and the arm is extended along the fetal trunk and face, which delivers the posterior arm from the vagina. This results in a reduction in the presenting diameter and the anterior shoulder usually can be delivered with minimal force.
If the delivery of the posterior arm does not resolve the shoulder dystocia, gently support the fetal head and posterior arm, and rotate the fetus 180° using pressure on the posterior surface of the shoulder.
When a fetus is macrosomic, the posterior arm can be fully extended in utero, with the hand below the level of the fetal groin. In such situations, it can be difficult to execute the delivery of the posterior arm.8 A back-up technique is to manipulate the posterior axilla to accomplish delivery.
Manipulation of the posterior axilla
When the posterior arm cannot be reached, these maneuvers may be helpful
One of the earliest written descriptions of resolving a severe shoulder dystocia by manipulating the posterior axilla was provided by Percival Willughby (born 1596, died 1685). He wrote:
- “After the head is born, if the child through the greatness of the shoulders, should stick at the neck, let the midwife put her fingers under the child’s armpit and give it a nudge, thrusting it to the other side with her finger, drawing the child or she may quickly bring forth the shoulders, without offering to put it forth by her hands clasped about the neck, which might endanger the breaking of the neck.”9
Manipulation of the posterior axilla can either involve a rotational maneuver (using the axilla to rotate the fetus through 180°) or it can be used to pull the posterior shoulder into the hollow of the sacrum and down the birth canal.
Schramm advocated using the posterior axilla to rotate the fetus. She recommended placing 1 or 2 fingers of the right hand in the posterior axilla and then rotating the posterior shoulder into the 12 o’clock position while simultaneously using the left hand to provide gentle guidance on the fetal neck.10
Menticoglou advocated using manipulation of the posterior axilla to draw the fetal shoulder into the sacral hollow and down the birth canal, thereby releasing the anterior shoulder. In the Menticoglou maneuver the middle fingers of the right and left hand of the obstetrician are hooked into the fetal axilla, one finger from the fetus’ front and the other from the fetus’ back. The fingers overlap each other within the fetal posterior axilla. Downward traction is then exerted on the fetal axilla and the posterior shoulder is pulled outward along the curve of the sacrum (FIGURE).11
Sandmire recommended combining fundal pressure with axillary traction and rotation to facilitate delivery.12
The posterior axillary maneuvers are seldom described in modern textbooks of obstetrics and represent a lost art. I have found that they can be useful when the posterior arm cannot be reached. The fetal posterior axilla is almost always closer to the vaginal introitus than the fetal hand or arm, and if the posterior arm cannot be reached, it is a valuable maneuver to have in your armamentarium.
Manipulation of the posterior axilla
The right and left third fingers are locked into the posterior axilla, one finger from the front and one from the back of the fetus. Gentle downward guidance is provided by the fingers to draw the posterior shoulder down and out along the curve of the sacrum, thus releasing the anterior shoulder. In this drawing, an assistant gently holds the head up.
(Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108:755–757. Reprinted with permission from Wolters Kluwer.)
My recommendation
Shoulder dystocia emergencies are an important cause of neonatal injury, including brachial plexus injury, fractures of the humerus, and hypoxic-ischemic encephalopathy. Obstetricians and midwives relentlessly train to resolve shoulder dystocia births with alacrity and minimal fetal trauma. When you are called as an emergency responder in a shoulder dystocia birth, I recommend that you prioritize a rotational maneuver or delivery of the posterior arm, and add manipulation of the posterior axilla to your armamentarium.
CASE: Unexpectedly high fetal weight, shoulder dystocia
A nurse midwife is managing the labor of a 41-year-old, G3P2 woman who had two prior spontaneous vaginal deliveries. Results of her glucose-loading test were normal. The midwife estimates the fetal weight as 7 lb 8 oz, but the birth weight proves to be 10 lb 6 oz. After delivery of the head, a turtle sign is obvious, and a shoulder dystocia is declared.
An emergency call for help is made to the front desk. The mother is asked to stop pushing. The obstetric nurse and midwife perform a McRoberts maneuver and apply suprapubic pressure without success. The woman is placed in the Gaskin’s all-fours position, but delivery cannot be accomplished.
Roused from your call room, you quickly proceed to help the team. At 3 minutes into the shoulder dystocia, you enter the room. As the emergency responder, what sequence of maneuvers will you use to resolve the shoulder dystocia?
In response to a shoulder dystocia emergency, most of us have practiced a sequence of actions:
- recognize shoulder dystocia early and communicate with staff
- instruct the mother to stop pushing and move the mother’s buttocks to the edge of the birthing bed
- ensure there is not a tight nuchal cord
- commit to avoid using excessive force on the fetal head and neck
- call for emergency help from other expert clinicians
- perform the McRoberts maneuver combined with suprapubic pressure
- consider performing an episiotomy
- use a rotational maneuver such as the Woods screw or Rubin maneuver
- deliver the posterior arm
- consider rarely used “salvage maneuvers,” such as the Zavanelli maneuver with cesarean delivery.1
When you are called to a shoulder dystocia as the emergency responder, the sequence of maneuvers is likely dependent on the actions already attempted by the primary clinician and the length of time from identification of the shoulder dystocia to the responder’s arrival at the patient’s bedside.
Based on my experience, if the primary clinician already has attempted the McRoberts maneuver, suprapubic pressure, and other advanced maneuvers without success, it is best for you to immediately move to the advanced maneuvers with which you are most comfortable. These advanced maneuvers typically include:
- consider an episiotomy and then a rotational maneuver (Woods screw or Rubin maneuver)
- attempt to deliver the posterior arm.
Woods screw and Rubin rotational maneuvers
Woods screw: Removing a well-placed screw requires a rotational maneuver. The Woods screw maneuver is based on the idea that a large baby is like a screw that must maneuver through pelvic threads. You cannot easily directly pull a well-set screw from its threads.
In Woods’ original description of the maneuver, the fetal spine was toward the mother’s right. Woods described a rotational maneuver that is performed by placing the left hand on the mother’s abdomen to provide judicious downward thrust on the fetal buttocks while simultaneously using the fingers of the right hand, placed on the ANTERIOR aspect of the shoulder, to create a clockwise rotational force on the fetus. Using the right hand, the fetal shoulder is moved through >180°, past the 12 o’clock position. At the same time, the fundal pressure and the fingers of the right hand are used to guide the fetus down the birth canal. This maneuver moves the anterior shoulder to the posterior position.
If delivery cannot be completed, a second step in the procedure is to then place the fingers of the right hand on the ANTERIOR aspect of the posterior shoulder (previously the anterior shoulder) and rotate the fetus in a counter-clockwise arc to the 12 o’clock position while gently guiding the fetus down the birth canal.2
Rubin rotational maneuver. Rubin observed that if you adduct the shoulders, the diameter of the shoulders are reduced, thereby easing the passage of the fetus through the birth canal. Adduction is the movement of a body part toward the MIDLINE sagittal plane.
Rubin recommended applying pressure to the POSTERIOR surface of the posterior (6 o’clock) fetal shoulder to help push the shoulder toward the midline of the chest (adduction). If the fetal spine is toward the mother’s left side, you place your right hand on the POSTERIOR surface of the shoulder at the 6 o’clock position, rotating the shoulder in a clockwise arc to the 12 o’clock position while simultaneously guiding the fetus down the birth canal.
Rubin also recommended the use of judicious fundal pressure after the anterior shoulder is disimpacted, if necessary, to facilitate delivery.3 Although both Woods and Rubin recommended the use of judiciously applied fundal pressure, most modern textbooks of obstetrics do not endorse the use of fundal pressure.
Delivery of the posterior arm: My preferred first maneuver
When I arrive as an emergency responder to a shoulder dystocia delivery, my preferred maneuver is to deliver the posterior arm. Many experts recommend prioritizing this maneuver when attempting to resolve a difficult shoulder dystocia.4-7
Delivery of the posterior arm is performed by inserting the hand and forearm into the sacral hollow. The left hand and forearm are used if the fetal spine is toward the mother’s left, and vice-versa. The posterior humerus is identified and followed to the elbow. The fetal forearm is flexed and swept across the fetal chest. The wrist or hand is then grasped and the arm is extended along the fetal trunk and face, which delivers the posterior arm from the vagina. This results in a reduction in the presenting diameter and the anterior shoulder usually can be delivered with minimal force.
If the delivery of the posterior arm does not resolve the shoulder dystocia, gently support the fetal head and posterior arm, and rotate the fetus 180° using pressure on the posterior surface of the shoulder.
When a fetus is macrosomic, the posterior arm can be fully extended in utero, with the hand below the level of the fetal groin. In such situations, it can be difficult to execute the delivery of the posterior arm.8 A back-up technique is to manipulate the posterior axilla to accomplish delivery.
Manipulation of the posterior axilla
When the posterior arm cannot be reached, these maneuvers may be helpful
One of the earliest written descriptions of resolving a severe shoulder dystocia by manipulating the posterior axilla was provided by Percival Willughby (born 1596, died 1685). He wrote:
- “After the head is born, if the child through the greatness of the shoulders, should stick at the neck, let the midwife put her fingers under the child’s armpit and give it a nudge, thrusting it to the other side with her finger, drawing the child or she may quickly bring forth the shoulders, without offering to put it forth by her hands clasped about the neck, which might endanger the breaking of the neck.”9
Manipulation of the posterior axilla can either involve a rotational maneuver (using the axilla to rotate the fetus through 180°) or it can be used to pull the posterior shoulder into the hollow of the sacrum and down the birth canal.
Schramm advocated using the posterior axilla to rotate the fetus. She recommended placing 1 or 2 fingers of the right hand in the posterior axilla and then rotating the posterior shoulder into the 12 o’clock position while simultaneously using the left hand to provide gentle guidance on the fetal neck.10
Menticoglou advocated using manipulation of the posterior axilla to draw the fetal shoulder into the sacral hollow and down the birth canal, thereby releasing the anterior shoulder. In the Menticoglou maneuver the middle fingers of the right and left hand of the obstetrician are hooked into the fetal axilla, one finger from the fetus’ front and the other from the fetus’ back. The fingers overlap each other within the fetal posterior axilla. Downward traction is then exerted on the fetal axilla and the posterior shoulder is pulled outward along the curve of the sacrum (FIGURE).11
Sandmire recommended combining fundal pressure with axillary traction and rotation to facilitate delivery.12
The posterior axillary maneuvers are seldom described in modern textbooks of obstetrics and represent a lost art. I have found that they can be useful when the posterior arm cannot be reached. The fetal posterior axilla is almost always closer to the vaginal introitus than the fetal hand or arm, and if the posterior arm cannot be reached, it is a valuable maneuver to have in your armamentarium.
Manipulation of the posterior axilla
The right and left third fingers are locked into the posterior axilla, one finger from the front and one from the back of the fetus. Gentle downward guidance is provided by the fingers to draw the posterior shoulder down and out along the curve of the sacrum, thus releasing the anterior shoulder. In this drawing, an assistant gently holds the head up.
(Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108:755–757. Reprinted with permission from Wolters Kluwer.)
My recommendation
Shoulder dystocia emergencies are an important cause of neonatal injury, including brachial plexus injury, fractures of the humerus, and hypoxic-ischemic encephalopathy. Obstetricians and midwives relentlessly train to resolve shoulder dystocia births with alacrity and minimal fetal trauma. When you are called as an emergency responder in a shoulder dystocia birth, I recommend that you prioritize a rotational maneuver or delivery of the posterior arm, and add manipulation of the posterior axilla to your armamentarium.
1. Burkman RT. Stop all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia. OBG Manage. 2013;25(3):22, 24, 28.
2. Woods CE. A principle of physics as applicable to shoulder dystocia. Am J Obstet Gynecol. 1943;45:796-804.
3. Rubin A. Management of shoulder dystocia. JAMA. 1964;189:835-837.
4. Nocon JJ, McKenzie DK, Thomas LJ, Hansell RS. Shoulder dystocia: an analysis of risks and obstetric maneuvers. Am J Obstet Gynecol. 1993;168(6 pt 1):1732-1737.
5. Poggi SH, Spong CY, Allen RH. Prioritizing posterior arm delivery during severe shoulder dystocia. Obstet Gynecol. 2003;101(5 pt 2):1068-1072.
6. Kung J, Swan AV, Arulkumaran S. Delivery of the posterior arm reduces shoulder dimensions in shoulder dystocia. In J Gynecol Obstet. 2006;93(3):233-237.
7. Hoffman MK, Bailit JL, Branch DW, et al. A comparison of obstetric maneuvers for the acute management of shoulder dystocia. Obstet Gynecol. 2011;117(6):1272-1278.
8. Barnum CG. Dystocia due to the shoulders. Am J Obstet Gynecol. 1945;50:439-442.
9. Willughby P. Observations in midwifery. New York, NY: MW Books; 1972:312–3.
10. Schramm M. Impacted shoulders—a personal experience. Aust N Z J Obstet Gynaecol. 1983;23(1):28-31.
11. Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108(3 pt 2):755-757.
12. Sandmire HF. From Green Bay, a game plan for shoulder dystocia. OBG Manage. 1997;9:15-16.
1. Burkman RT. Stop all activities that may lead to further shoulder impaction when you suspect possible shoulder dystocia. OBG Manage. 2013;25(3):22, 24, 28.
2. Woods CE. A principle of physics as applicable to shoulder dystocia. Am J Obstet Gynecol. 1943;45:796-804.
3. Rubin A. Management of shoulder dystocia. JAMA. 1964;189:835-837.
4. Nocon JJ, McKenzie DK, Thomas LJ, Hansell RS. Shoulder dystocia: an analysis of risks and obstetric maneuvers. Am J Obstet Gynecol. 1993;168(6 pt 1):1732-1737.
5. Poggi SH, Spong CY, Allen RH. Prioritizing posterior arm delivery during severe shoulder dystocia. Obstet Gynecol. 2003;101(5 pt 2):1068-1072.
6. Kung J, Swan AV, Arulkumaran S. Delivery of the posterior arm reduces shoulder dimensions in shoulder dystocia. In J Gynecol Obstet. 2006;93(3):233-237.
7. Hoffman MK, Bailit JL, Branch DW, et al. A comparison of obstetric maneuvers for the acute management of shoulder dystocia. Obstet Gynecol. 2011;117(6):1272-1278.
8. Barnum CG. Dystocia due to the shoulders. Am J Obstet Gynecol. 1945;50:439-442.
9. Willughby P. Observations in midwifery. New York, NY: MW Books; 1972:312–3.
10. Schramm M. Impacted shoulders—a personal experience. Aust N Z J Obstet Gynaecol. 1983;23(1):28-31.
11. Menticoglou SM. A modified technique to deliver the posterior arm in severe shoulder dystocia. Obstet Gynecol. 2006;108(3 pt 2):755-757.
12. Sandmire HF. From Green Bay, a game plan for shoulder dystocia. OBG Manage. 1997;9:15-16.