User login
VAM ’17 Will Be a ‘Spectacular Meeting’
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Participants at the Vascular Annual Meeting (VAM) have lots more to look forward to than sunny skies, beaches and palm trees. A number of new program features are planned to add interest and value to the meeting, said Dr. Ron Dalman.
Dr. Dalman chairs the SVS Program Committee, which develops programming and content for VAM, the premiere meeting for vascular specialists.
The 2017 meeting will be May 31-June 3 in beautiful San Diego, with plenaries and exhibits set for June 1-3.
Changes for 2017 include:
• More and potentially longer sessions with collaborative specialty societies, such as the American Venous Forum, the Society for Vascular Ultrasound and the Society of Thoracic Surgeons. “These sessions provide a multi-disciplinary perspective on our common problems and showcase the SVS’ leadership role in vascular health and disease management,” said Dr. Dalman. Members provided positive feedback on last year’s partnership sessions, so this year, these program features will be significantly expanded.
• An educational review course highlighting some of the more frequently missed questions from the latest version of the Vascular Education Self-Assessment Program (VESAP3).
• Guideline summaries, organized by the SVS Document Oversight Committee and presented by the authorship group for each, on critical topics such as abdominal aortic aneurysms, aortic dissection, venous disease and more. These summaries will be incorporated into post-graduate programming. “It makes sense to cover current practice guidelines and consensus documents, as several high-profile efforts are being updated this year,” said Dr. Dalman. “We can give attendees an executive summary of current guidelines by their respective authors, and attendees will come away with unique insights into why the most impactful and significant changes were included in each respective document.”
• Sessions of potential interest to surgeons in community practice environments, marked in the schedule as such by the SVS Community Practice Committee.
“These improvements will increase the value of the Annual Meeting for all attendees,” Dr. Dalman said. “We’re emphasizing interactive education, not simply passive learning. It’s going to be very exciting – and different in both style and substance.”
A Californian himself, Dr. Dalman also is looking forward to showing off his state. “San Diego is a wonderful place to vacation and the meeting venue provides convenient access to the Gaslamp District, the waterfront and the world-famous beaches,” he said.
“We encourage our members to bring their families to San Diego and make a vacation out of it.”
With the programming additions, increased opportunities for participation, the educational activities planned plus the perfect location, he added, “This is going to be a spectacular meeting.”
Ready for post-acute care?
The definition of “hospitalist,” according to the SHM website, is a clinician “dedicated to delivering comprehensive medical care to hospitalized patients.” For years, the hospital setting was the specialties’ identifier. But as hospitalists’ scope has expanded, and post-acute care (PAC) in the United States has grown, more hospitalists are extending their roles into this space.
PAC today is more than the traditional nursing home, according to Manoj K. Mathew, MD, SFHM, national medical director of Agilon Health in Los Angeles.

Many of those expanded settings Dr. Mathew describes emerged as a result of the Affordable Care Act. Since its enactment in 2010, the ACA has heightened providers’ focus on the “Triple Aim” of improving the patient experience (including quality and satisfaction), improving the health of populations, and reducing the per capita cost of healthcare.1 Vishal Kuchaculla, MD, New England regional post-acute medical director of Knoxville,Tenn.-based TeamHealth, says new service lines also developed as Medicare clamped down on long-term inpatient hospital stays by giving financial impetus to discharge patients as soon as possible.
“Over the last few years, there’s been a major shift from fee-for-service to risk-based payment models,” Dr. Kuchaculla says. “The government’s financial incentives are driving outcomes to improve performance initiatives.”

“Today, LTACHs can be used as substitutes for short-term acute care,” says Sean R. Muldoon, MD, MPH, FCCP, chief medical officer of Kindred Healthcare in Louisville, Ky., and former chair of SHM’s Post-Acute Care Committee. “This means that a patient can be directly admitted from their home to an LTACH. In fact, many hospice and home-care patients are referred from physicians’ offices without a preceding hospitalization.”
Hospitalists can fill a need
More hospitalists are working in PACs for a number of reasons. Dr. Mathew says PAC facilities and services have “typically lacked the clinical structure and processes to obtain the results that patients and payors expect.
“These deficits needed to be quickly remedied as patients discharged from hospitals have increased acuity and higher disease burdens,” he adds. “Hospitalists were the natural choice to fill roles requiring their expertise and experience.”
Dr. Muldoon considers the expanded scope of practice into PACs an additional layer to hospital medicine’s value proposition to the healthcare system.
“As experts in the management of inpatient populations, it’s natural for hospitalists to expand to other facilities with inpatient-like populations,” he says, noting SNFs are the most popular choice, with IRFs and LTACHs also being common places to work. Few hospitalists work in home care or hospice.
PAC settings are designed to help patients who are transitioning from an inpatient setting back to their home or other setting.
“Many patients go home after a SNF stay, while others will move to a nursing home or other longer-term care setting for the first time,” says Tiffany Radcliff, PhD, a health economist in the department of health policy and management at Texas A&M University School of Public Health in College Station. “With this in mind, hospitalists working in PAC have the opportunity to address each patient’s ongoing care needs and prepare them for their next setting. Hospitalists can manage medication or other care regimen changes that resulted from an inpatient stay, reinforce discharge instructions to the patient and their caregivers, and identify any other issues with continuing care that need to be addressed before discharge to the next care setting.”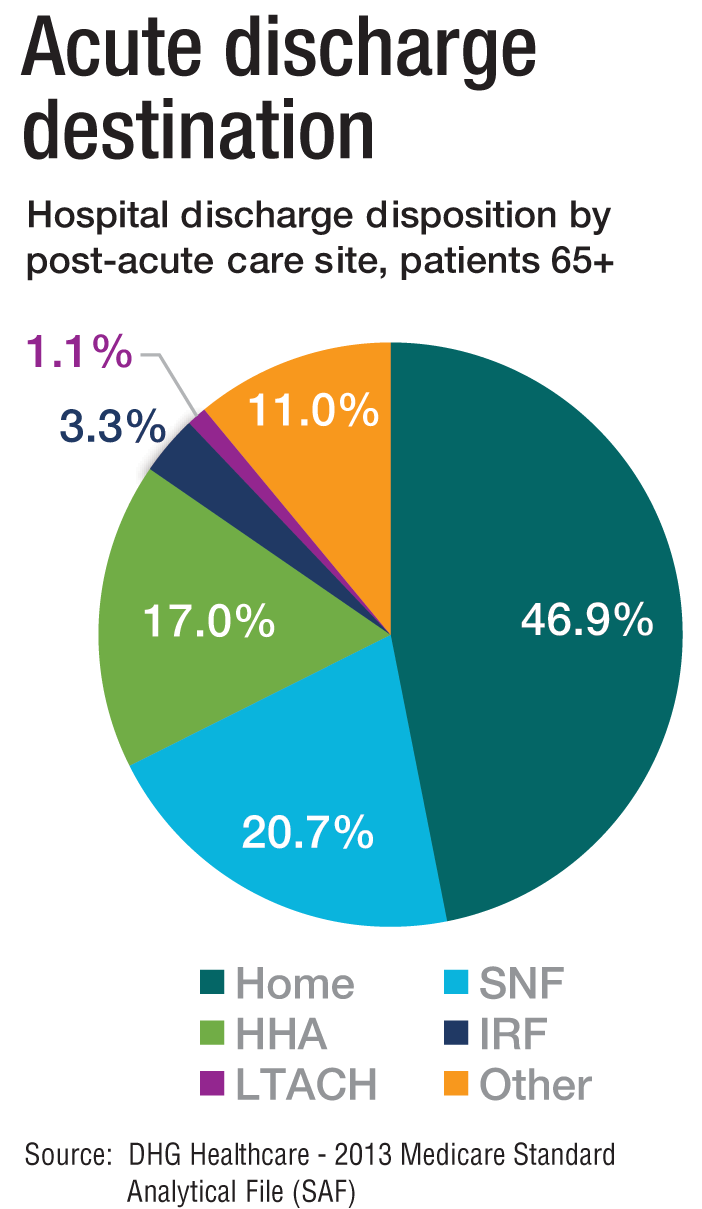
Transitioning Care
Even if a hospitalist is not employed at a PAC, it’s important that they know something about them.
“As patients are moved downstream earlier, hospitalists are being asked to help make a judgment regarding when and where an inpatient is transitioned,” Dr. Muldoon says. As organizations move toward becoming fully risk capable, it is necessary to develop referral networks of high-quality PAC providers to achieve the best clinical outcomes, reduce readmissions, and lower costs.2“Therefore, hospitalists should have a working knowledge of the different sites of service as well as some opinion on the suitability of available options in their community,” Dr. Muldoon says. “The hospitalist can also help to educate the hospitalized patient on what to expect at a PAC.”
If a patient is inappropriately prepared for the PAC setting, it could lead to incomplete management of their condition, which ultimately could lead to readmission.
“When hospitalists know how care is provided in a PAC setting, they are better able to ensure a smoother transition of care between settings,” says Tochi Iroku-Malize, MD, MPH, MBA, FAAFP, SFHM, chair of family medicine at Northwell Health in Long Island, N.Y. “This will ultimately prevent unnecessary readmissions.”
Further, the quality metrics that hospitals and thereby hospitalists are judged by no longer end at the hospital’s exit.
“The ownership of acute-care outcomes requires extending the accountability to outside of the institution’s four walls,” Dr. Mathew says. “The inpatient team needs to place great importance on the transition of care and the subsequent quality of that care when the patient is discharged.”
Robert W. Harrington Jr., MD, SFHM, chief medical officer of Plano, Texas–based Reliant Post-Acute Care Solutions and former SHM president, says the health system landscapes are pushing HM beyond the hospitals’ walls.

How PAC settings differ from hospitals
Practicing in PAC has some important nuances that hospitalists from short-term acute care need to get accustomed to, Dr. Muldoon says. Primarily, the diagnostic capabilities are much more limited, as is the presence of high-level staffing. Further, patients are less resilient to medication changes and interventions, so changes need to be done gradually.
“Hospitalists who try to practice acute-care medicine in a PAC setting may become frustrated by the length of time it takes to do a work-up, get a consultation, and respond to a patient’s change of condition,” Dr. Muldoon says. “Nonetheless, hospitalists can overcome this once recognizing this mind shift.”
According to Dr. Harrington, another challenge hospitalists may face is the inability of the hospital’s and PAC facility’s IT platforms to exchange electronic information.
“The major vendors on both sides need to figure out an interoperability strategy,” he says. “Currently, it often takes 1-3 days to receive a new patient’s discharge summary. The summary may consist of a stack of paper that takes significant time to sort through and requires the PAC facility to perform duplicate data entry. It’s a very highly inefficient process that opens up the doors to mistakes and errors of omission and commission that can result in bad patient outcomes.”
Arif Nazir, MD, CMD, FACP, AGSF, chief medical officer of Signature HealthCARE and president of SHC Medical Partners, both in Louisville, Ky., cites additional reasons the lack of seamless communication between a hospital and PAC facility is problematic. “I see physicians order laboratory tests and investigations that were already done in the hospital because they didn’t know they were already performed or never received the results,” he says. “Similarly, I see patients continue to take medications prescribed in the hospital long term even though they were only supposed to take them short term. I’ve also seen patients come to a PAC setting from a hospital without any formal understanding of their rehabilitative period and expectations for recovery.”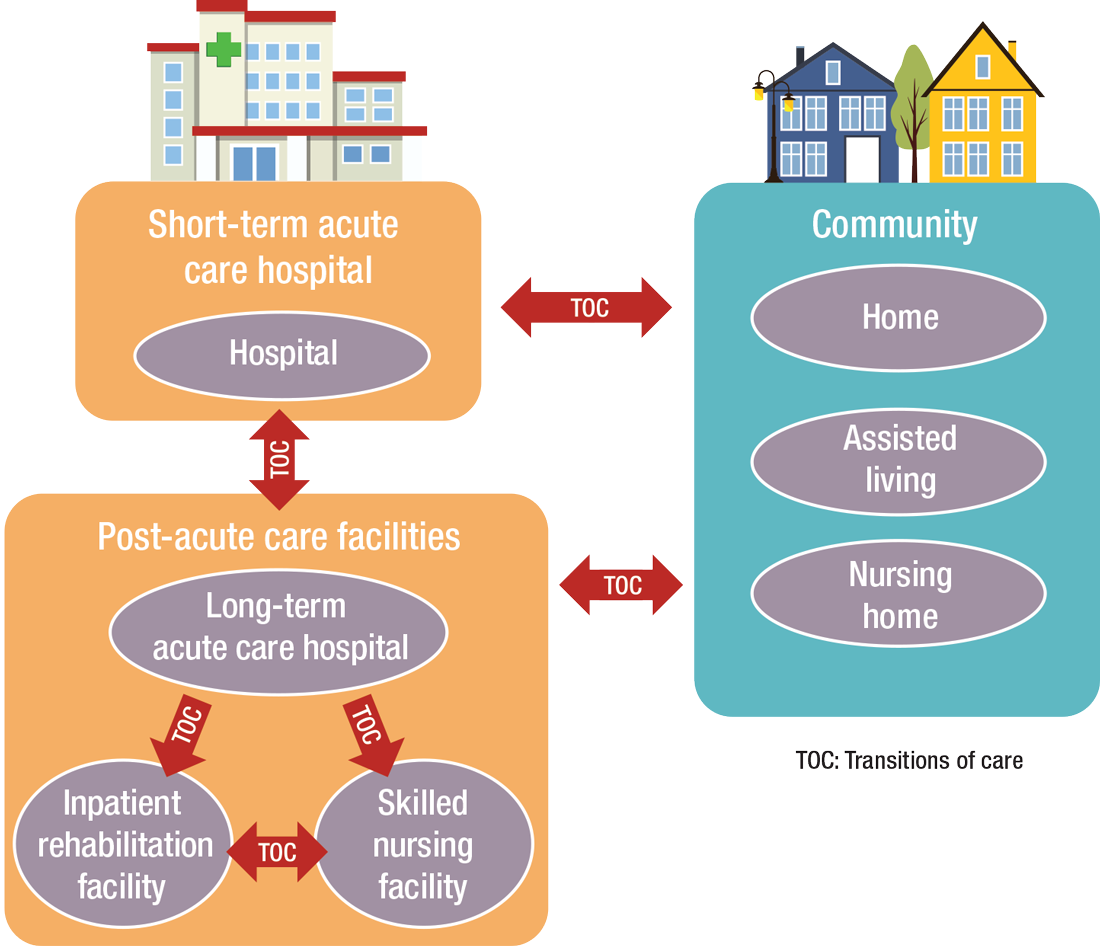
What’s ahead?
Looking to the future, Surafel Tsega, MD, clinical instructor at Mount Sinai Hospital in New York, says he thinks there will be a move toward greater collaboration among inpatient and PAC facilities, particularly in the discharge process, given that hospitals have an added incentive to ensure safe transitions because reimbursement from the Centers for Medicare & Medicaid Services is tied to readmissions and there are penalties for readmission. This involves more comprehensive planning regarding “warm handoffs” (e.g., real-time discussions with PAC providers about a patient’s hospital course and plan of care upon discharge), transferring of information, and so forth.
And while it can still be challenging to identify high-risk patients or determine the intensity and duration of their care, Dr. Mathew says risk-stratification tools and care pathways are continually being refined to maximize value with the limited resources available. In addition, with an increased emphasis on employing a team approach to care, there will be better integration of non-medical services to address the social determinants of health, which play significant roles in overall health and healing.
“Working with community-based organizations for this purpose will be a valuable tool for any of the population health–based initiatives,” he says.
Dr. Muldoon says he believes healthcare reform will increasingly view an inpatient admission as something to be avoided.
“If hospitalization can’t be avoided, then it should be shortened as much as possible,” he says. “This will shift inpatient care into LTACHs, SNFs, and IRFs. Hospitalists would be wise to follow patients into those settings as traditional inpatient census is reduced. This will take a few years, so hospitalists should start now in preparing for that downstream transition of individuals who were previously inpatients.”
The cost of care, and other PAC facts and figures
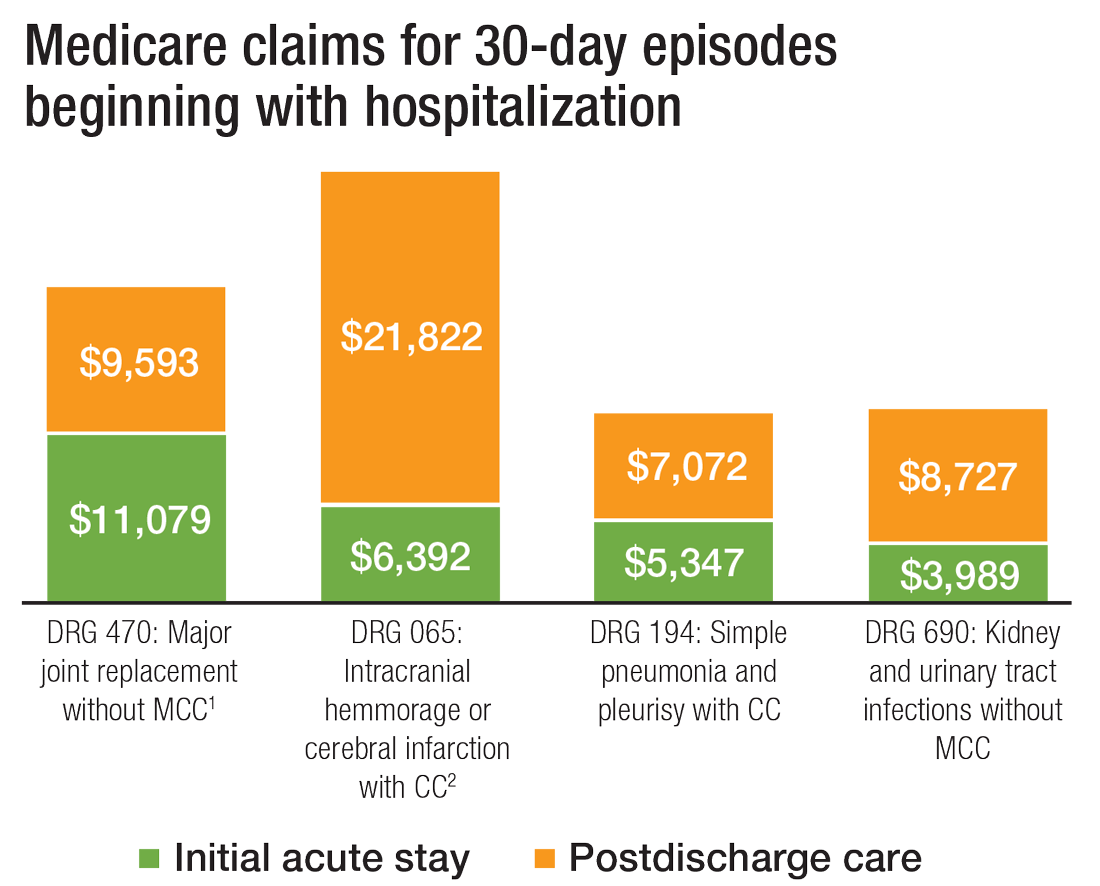
The amount of money that Medicare spends on post-acute care (PAC) has been increasing. In 2012, 12.6% of Medicare beneficiaries used some form of PAC, costing $62 billion.2 That amounts to the Centers for Medicare & Medicaid Services spending close to 25% of Medicare beneficiary expenses on PAC, a 133% increase from 2001 to 2012. Among the different types, $30.4 billion was spent on skilled nursing facilities (SNFs), $18.6 billion on home health, and $13.1 billion on long-term acute care (LTAC) and acute-care rehabilitation.2
It’s also been reported that after short-term acute-care hospitalization, about one in five Medicare beneficiaries requires continued specialized treatment in one of the three typical Medicare PAC settings: inpatient rehabilitation facilities (IRFs), LTAC hospitals, and SNFs.3
What’s more, hospital readmission nearly doubles the cost of an episode, so the financial implications for organizations operating in risk-bearing arrangements are significant. In 2013, 2,213 hospitals were charged $280 million in readmission penalties.2
References
1. The role of post-acute care in new care delivery models. American Hospital Association website. Available at: http://www.aha.org/research/reports/tw/15dec-tw-postacute.pdf. Accessed Nov. 7, 2016.
2. Post-acute care integration: Today and in the future. DHG Healthcare website. Available at: http://www2.dhgllp.com/res_pubs/HCG-Post-Acute-Care-Integration.pdf. Accessed Nov. 7, 2016.
3. Overview: Post-acute care transitions toolkit. Society for Hospital Medicine website. Available at: http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c-8620-46db-a00f-89f07f021958. Accessed Nov. 10, 2016.
The definition of “hospitalist,” according to the SHM website, is a clinician “dedicated to delivering comprehensive medical care to hospitalized patients.” For years, the hospital setting was the specialties’ identifier. But as hospitalists’ scope has expanded, and post-acute care (PAC) in the United States has grown, more hospitalists are extending their roles into this space.
PAC today is more than the traditional nursing home, according to Manoj K. Mathew, MD, SFHM, national medical director of Agilon Health in Los Angeles.
Many of those expanded settings Dr. Mathew describes emerged as a result of the Affordable Care Act. Since its enactment in 2010, the ACA has heightened providers’ focus on the “Triple Aim” of improving the patient experience (including quality and satisfaction), improving the health of populations, and reducing the per capita cost of healthcare.1 Vishal Kuchaculla, MD, New England regional post-acute medical director of Knoxville,Tenn.-based TeamHealth, says new service lines also developed as Medicare clamped down on long-term inpatient hospital stays by giving financial impetus to discharge patients as soon as possible.
“Over the last few years, there’s been a major shift from fee-for-service to risk-based payment models,” Dr. Kuchaculla says. “The government’s financial incentives are driving outcomes to improve performance initiatives.”
“Today, LTACHs can be used as substitutes for short-term acute care,” says Sean R. Muldoon, MD, MPH, FCCP, chief medical officer of Kindred Healthcare in Louisville, Ky., and former chair of SHM’s Post-Acute Care Committee. “This means that a patient can be directly admitted from their home to an LTACH. In fact, many hospice and home-care patients are referred from physicians’ offices without a preceding hospitalization.”
Hospitalists can fill a need
More hospitalists are working in PACs for a number of reasons. Dr. Mathew says PAC facilities and services have “typically lacked the clinical structure and processes to obtain the results that patients and payors expect.
“These deficits needed to be quickly remedied as patients discharged from hospitals have increased acuity and higher disease burdens,” he adds. “Hospitalists were the natural choice to fill roles requiring their expertise and experience.”
Dr. Muldoon considers the expanded scope of practice into PACs an additional layer to hospital medicine’s value proposition to the healthcare system.
“As experts in the management of inpatient populations, it’s natural for hospitalists to expand to other facilities with inpatient-like populations,” he says, noting SNFs are the most popular choice, with IRFs and LTACHs also being common places to work. Few hospitalists work in home care or hospice.
PAC settings are designed to help patients who are transitioning from an inpatient setting back to their home or other setting.
“Many patients go home after a SNF stay, while others will move to a nursing home or other longer-term care setting for the first time,” says Tiffany Radcliff, PhD, a health economist in the department of health policy and management at Texas A&M University School of Public Health in College Station. “With this in mind, hospitalists working in PAC have the opportunity to address each patient’s ongoing care needs and prepare them for their next setting. Hospitalists can manage medication or other care regimen changes that resulted from an inpatient stay, reinforce discharge instructions to the patient and their caregivers, and identify any other issues with continuing care that need to be addressed before discharge to the next care setting.”
Transitioning Care
Even if a hospitalist is not employed at a PAC, it’s important that they know something about them.
“As patients are moved downstream earlier, hospitalists are being asked to help make a judgment regarding when and where an inpatient is transitioned,” Dr. Muldoon says. As organizations move toward becoming fully risk capable, it is necessary to develop referral networks of high-quality PAC providers to achieve the best clinical outcomes, reduce readmissions, and lower costs.2“Therefore, hospitalists should have a working knowledge of the different sites of service as well as some opinion on the suitability of available options in their community,” Dr. Muldoon says. “The hospitalist can also help to educate the hospitalized patient on what to expect at a PAC.”
If a patient is inappropriately prepared for the PAC setting, it could lead to incomplete management of their condition, which ultimately could lead to readmission.
“When hospitalists know how care is provided in a PAC setting, they are better able to ensure a smoother transition of care between settings,” says Tochi Iroku-Malize, MD, MPH, MBA, FAAFP, SFHM, chair of family medicine at Northwell Health in Long Island, N.Y. “This will ultimately prevent unnecessary readmissions.”
Further, the quality metrics that hospitals and thereby hospitalists are judged by no longer end at the hospital’s exit.
“The ownership of acute-care outcomes requires extending the accountability to outside of the institution’s four walls,” Dr. Mathew says. “The inpatient team needs to place great importance on the transition of care and the subsequent quality of that care when the patient is discharged.”
Robert W. Harrington Jr., MD, SFHM, chief medical officer of Plano, Texas–based Reliant Post-Acute Care Solutions and former SHM president, says the health system landscapes are pushing HM beyond the hospitals’ walls.
How PAC settings differ from hospitals
Practicing in PAC has some important nuances that hospitalists from short-term acute care need to get accustomed to, Dr. Muldoon says. Primarily, the diagnostic capabilities are much more limited, as is the presence of high-level staffing. Further, patients are less resilient to medication changes and interventions, so changes need to be done gradually.
“Hospitalists who try to practice acute-care medicine in a PAC setting may become frustrated by the length of time it takes to do a work-up, get a consultation, and respond to a patient’s change of condition,” Dr. Muldoon says. “Nonetheless, hospitalists can overcome this once recognizing this mind shift.”
According to Dr. Harrington, another challenge hospitalists may face is the inability of the hospital’s and PAC facility’s IT platforms to exchange electronic information.
“The major vendors on both sides need to figure out an interoperability strategy,” he says. “Currently, it often takes 1-3 days to receive a new patient’s discharge summary. The summary may consist of a stack of paper that takes significant time to sort through and requires the PAC facility to perform duplicate data entry. It’s a very highly inefficient process that opens up the doors to mistakes and errors of omission and commission that can result in bad patient outcomes.”
Arif Nazir, MD, CMD, FACP, AGSF, chief medical officer of Signature HealthCARE and president of SHC Medical Partners, both in Louisville, Ky., cites additional reasons the lack of seamless communication between a hospital and PAC facility is problematic. “I see physicians order laboratory tests and investigations that were already done in the hospital because they didn’t know they were already performed or never received the results,” he says. “Similarly, I see patients continue to take medications prescribed in the hospital long term even though they were only supposed to take them short term. I’ve also seen patients come to a PAC setting from a hospital without any formal understanding of their rehabilitative period and expectations for recovery.”
What’s ahead?
Looking to the future, Surafel Tsega, MD, clinical instructor at Mount Sinai Hospital in New York, says he thinks there will be a move toward greater collaboration among inpatient and PAC facilities, particularly in the discharge process, given that hospitals have an added incentive to ensure safe transitions because reimbursement from the Centers for Medicare & Medicaid Services is tied to readmissions and there are penalties for readmission. This involves more comprehensive planning regarding “warm handoffs” (e.g., real-time discussions with PAC providers about a patient’s hospital course and plan of care upon discharge), transferring of information, and so forth.
And while it can still be challenging to identify high-risk patients or determine the intensity and duration of their care, Dr. Mathew says risk-stratification tools and care pathways are continually being refined to maximize value with the limited resources available. In addition, with an increased emphasis on employing a team approach to care, there will be better integration of non-medical services to address the social determinants of health, which play significant roles in overall health and healing.
“Working with community-based organizations for this purpose will be a valuable tool for any of the population health–based initiatives,” he says.
Dr. Muldoon says he believes healthcare reform will increasingly view an inpatient admission as something to be avoided.
“If hospitalization can’t be avoided, then it should be shortened as much as possible,” he says. “This will shift inpatient care into LTACHs, SNFs, and IRFs. Hospitalists would be wise to follow patients into those settings as traditional inpatient census is reduced. This will take a few years, so hospitalists should start now in preparing for that downstream transition of individuals who were previously inpatients.”
The cost of care, and other PAC facts and figures
The amount of money that Medicare spends on post-acute care (PAC) has been increasing. In 2012, 12.6% of Medicare beneficiaries used some form of PAC, costing $62 billion.2 That amounts to the Centers for Medicare & Medicaid Services spending close to 25% of Medicare beneficiary expenses on PAC, a 133% increase from 2001 to 2012. Among the different types, $30.4 billion was spent on skilled nursing facilities (SNFs), $18.6 billion on home health, and $13.1 billion on long-term acute care (LTAC) and acute-care rehabilitation.2
It’s also been reported that after short-term acute-care hospitalization, about one in five Medicare beneficiaries requires continued specialized treatment in one of the three typical Medicare PAC settings: inpatient rehabilitation facilities (IRFs), LTAC hospitals, and SNFs.3
What’s more, hospital readmission nearly doubles the cost of an episode, so the financial implications for organizations operating in risk-bearing arrangements are significant. In 2013, 2,213 hospitals were charged $280 million in readmission penalties.2
References
1. The role of post-acute care in new care delivery models. American Hospital Association website. Available at: http://www.aha.org/research/reports/tw/15dec-tw-postacute.pdf. Accessed Nov. 7, 2016.
2. Post-acute care integration: Today and in the future. DHG Healthcare website. Available at: http://www2.dhgllp.com/res_pubs/HCG-Post-Acute-Care-Integration.pdf. Accessed Nov. 7, 2016.
3. Overview: Post-acute care transitions toolkit. Society for Hospital Medicine website. Available at: http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c-8620-46db-a00f-89f07f021958. Accessed Nov. 10, 2016.
The definition of “hospitalist,” according to the SHM website, is a clinician “dedicated to delivering comprehensive medical care to hospitalized patients.” For years, the hospital setting was the specialties’ identifier. But as hospitalists’ scope has expanded, and post-acute care (PAC) in the United States has grown, more hospitalists are extending their roles into this space.
PAC today is more than the traditional nursing home, according to Manoj K. Mathew, MD, SFHM, national medical director of Agilon Health in Los Angeles.
Many of those expanded settings Dr. Mathew describes emerged as a result of the Affordable Care Act. Since its enactment in 2010, the ACA has heightened providers’ focus on the “Triple Aim” of improving the patient experience (including quality and satisfaction), improving the health of populations, and reducing the per capita cost of healthcare.1 Vishal Kuchaculla, MD, New England regional post-acute medical director of Knoxville,Tenn.-based TeamHealth, says new service lines also developed as Medicare clamped down on long-term inpatient hospital stays by giving financial impetus to discharge patients as soon as possible.
“Over the last few years, there’s been a major shift from fee-for-service to risk-based payment models,” Dr. Kuchaculla says. “The government’s financial incentives are driving outcomes to improve performance initiatives.”
“Today, LTACHs can be used as substitutes for short-term acute care,” says Sean R. Muldoon, MD, MPH, FCCP, chief medical officer of Kindred Healthcare in Louisville, Ky., and former chair of SHM’s Post-Acute Care Committee. “This means that a patient can be directly admitted from their home to an LTACH. In fact, many hospice and home-care patients are referred from physicians’ offices without a preceding hospitalization.”
Hospitalists can fill a need
More hospitalists are working in PACs for a number of reasons. Dr. Mathew says PAC facilities and services have “typically lacked the clinical structure and processes to obtain the results that patients and payors expect.
“These deficits needed to be quickly remedied as patients discharged from hospitals have increased acuity and higher disease burdens,” he adds. “Hospitalists were the natural choice to fill roles requiring their expertise and experience.”
Dr. Muldoon considers the expanded scope of practice into PACs an additional layer to hospital medicine’s value proposition to the healthcare system.
“As experts in the management of inpatient populations, it’s natural for hospitalists to expand to other facilities with inpatient-like populations,” he says, noting SNFs are the most popular choice, with IRFs and LTACHs also being common places to work. Few hospitalists work in home care or hospice.
PAC settings are designed to help patients who are transitioning from an inpatient setting back to their home or other setting.
“Many patients go home after a SNF stay, while others will move to a nursing home or other longer-term care setting for the first time,” says Tiffany Radcliff, PhD, a health economist in the department of health policy and management at Texas A&M University School of Public Health in College Station. “With this in mind, hospitalists working in PAC have the opportunity to address each patient’s ongoing care needs and prepare them for their next setting. Hospitalists can manage medication or other care regimen changes that resulted from an inpatient stay, reinforce discharge instructions to the patient and their caregivers, and identify any other issues with continuing care that need to be addressed before discharge to the next care setting.”
Transitioning Care
Even if a hospitalist is not employed at a PAC, it’s important that they know something about them.
“As patients are moved downstream earlier, hospitalists are being asked to help make a judgment regarding when and where an inpatient is transitioned,” Dr. Muldoon says. As organizations move toward becoming fully risk capable, it is necessary to develop referral networks of high-quality PAC providers to achieve the best clinical outcomes, reduce readmissions, and lower costs.2“Therefore, hospitalists should have a working knowledge of the different sites of service as well as some opinion on the suitability of available options in their community,” Dr. Muldoon says. “The hospitalist can also help to educate the hospitalized patient on what to expect at a PAC.”
If a patient is inappropriately prepared for the PAC setting, it could lead to incomplete management of their condition, which ultimately could lead to readmission.
“When hospitalists know how care is provided in a PAC setting, they are better able to ensure a smoother transition of care between settings,” says Tochi Iroku-Malize, MD, MPH, MBA, FAAFP, SFHM, chair of family medicine at Northwell Health in Long Island, N.Y. “This will ultimately prevent unnecessary readmissions.”
Further, the quality metrics that hospitals and thereby hospitalists are judged by no longer end at the hospital’s exit.
“The ownership of acute-care outcomes requires extending the accountability to outside of the institution’s four walls,” Dr. Mathew says. “The inpatient team needs to place great importance on the transition of care and the subsequent quality of that care when the patient is discharged.”
Robert W. Harrington Jr., MD, SFHM, chief medical officer of Plano, Texas–based Reliant Post-Acute Care Solutions and former SHM president, says the health system landscapes are pushing HM beyond the hospitals’ walls.
How PAC settings differ from hospitals
Practicing in PAC has some important nuances that hospitalists from short-term acute care need to get accustomed to, Dr. Muldoon says. Primarily, the diagnostic capabilities are much more limited, as is the presence of high-level staffing. Further, patients are less resilient to medication changes and interventions, so changes need to be done gradually.
“Hospitalists who try to practice acute-care medicine in a PAC setting may become frustrated by the length of time it takes to do a work-up, get a consultation, and respond to a patient’s change of condition,” Dr. Muldoon says. “Nonetheless, hospitalists can overcome this once recognizing this mind shift.”
According to Dr. Harrington, another challenge hospitalists may face is the inability of the hospital’s and PAC facility’s IT platforms to exchange electronic information.
“The major vendors on both sides need to figure out an interoperability strategy,” he says. “Currently, it often takes 1-3 days to receive a new patient’s discharge summary. The summary may consist of a stack of paper that takes significant time to sort through and requires the PAC facility to perform duplicate data entry. It’s a very highly inefficient process that opens up the doors to mistakes and errors of omission and commission that can result in bad patient outcomes.”
Arif Nazir, MD, CMD, FACP, AGSF, chief medical officer of Signature HealthCARE and president of SHC Medical Partners, both in Louisville, Ky., cites additional reasons the lack of seamless communication between a hospital and PAC facility is problematic. “I see physicians order laboratory tests and investigations that were already done in the hospital because they didn’t know they were already performed or never received the results,” he says. “Similarly, I see patients continue to take medications prescribed in the hospital long term even though they were only supposed to take them short term. I’ve also seen patients come to a PAC setting from a hospital without any formal understanding of their rehabilitative period and expectations for recovery.”
What’s ahead?
Looking to the future, Surafel Tsega, MD, clinical instructor at Mount Sinai Hospital in New York, says he thinks there will be a move toward greater collaboration among inpatient and PAC facilities, particularly in the discharge process, given that hospitals have an added incentive to ensure safe transitions because reimbursement from the Centers for Medicare & Medicaid Services is tied to readmissions and there are penalties for readmission. This involves more comprehensive planning regarding “warm handoffs” (e.g., real-time discussions with PAC providers about a patient’s hospital course and plan of care upon discharge), transferring of information, and so forth.
And while it can still be challenging to identify high-risk patients or determine the intensity and duration of their care, Dr. Mathew says risk-stratification tools and care pathways are continually being refined to maximize value with the limited resources available. In addition, with an increased emphasis on employing a team approach to care, there will be better integration of non-medical services to address the social determinants of health, which play significant roles in overall health and healing.
“Working with community-based organizations for this purpose will be a valuable tool for any of the population health–based initiatives,” he says.
Dr. Muldoon says he believes healthcare reform will increasingly view an inpatient admission as something to be avoided.
“If hospitalization can’t be avoided, then it should be shortened as much as possible,” he says. “This will shift inpatient care into LTACHs, SNFs, and IRFs. Hospitalists would be wise to follow patients into those settings as traditional inpatient census is reduced. This will take a few years, so hospitalists should start now in preparing for that downstream transition of individuals who were previously inpatients.”
The cost of care, and other PAC facts and figures
The amount of money that Medicare spends on post-acute care (PAC) has been increasing. In 2012, 12.6% of Medicare beneficiaries used some form of PAC, costing $62 billion.2 That amounts to the Centers for Medicare & Medicaid Services spending close to 25% of Medicare beneficiary expenses on PAC, a 133% increase from 2001 to 2012. Among the different types, $30.4 billion was spent on skilled nursing facilities (SNFs), $18.6 billion on home health, and $13.1 billion on long-term acute care (LTAC) and acute-care rehabilitation.2
It’s also been reported that after short-term acute-care hospitalization, about one in five Medicare beneficiaries requires continued specialized treatment in one of the three typical Medicare PAC settings: inpatient rehabilitation facilities (IRFs), LTAC hospitals, and SNFs.3
What’s more, hospital readmission nearly doubles the cost of an episode, so the financial implications for organizations operating in risk-bearing arrangements are significant. In 2013, 2,213 hospitals were charged $280 million in readmission penalties.2
References
1. The role of post-acute care in new care delivery models. American Hospital Association website. Available at: http://www.aha.org/research/reports/tw/15dec-tw-postacute.pdf. Accessed Nov. 7, 2016.
2. Post-acute care integration: Today and in the future. DHG Healthcare website. Available at: http://www2.dhgllp.com/res_pubs/HCG-Post-Acute-Care-Integration.pdf. Accessed Nov. 7, 2016.
3. Overview: Post-acute care transitions toolkit. Society for Hospital Medicine website. Available at: http://www.hospitalmedicine.org/Web/Quality___Innovation/Implementation_Toolkit/pact/Overview_PACT.aspx?hkey=dea3da3c-8620-46db-a00f-89f07f021958. Accessed Nov. 10, 2016.
Transplantation palliative care: The time is ripe
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3

What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Over 10 years ago, a challenge was made in a surgical publication for increased collaboration between the fields of transplantation and palliative care.1
Since that time not much progress has been made bringing these fields together in a consistent way that would mutually benefit patients and the specialties. However, other progress has been made, particularly in the field of palliative care, which could brighten the prospects and broaden the opportunities to accomplish collaboration between palliative care and transplantation.
Growth of palliative services
During the past decade there has been a robust proliferation of hospital-based palliative care programs in the United States. In all, 67% of U.S. hospitals with 50 or more beds report palliative care teams, up from 63% in 2011 and 53% in 2008.
Only a decade ago, critical care and palliative care were generally considered mutually exclusive. Evidence is trickling in to suggest that this is no longer the case. Although palliative care was not an integral part of critical care at that time, patients, families, and even practitioners began to demand these services. Cook and Rocker have eloquently advocated the rightful place of palliative care in the ICU.2
Studies in recent years have shown that the integration of palliative care into critical care decreases in length of ICU and hospital stay, decreases costs, enhances patient/family satisfaction, and promotes a more rapid consensus about goals of care, without increasing mortality. The ICU experience to date could be considered a reassuring precedent for transplantation palliative care.
Integration of palliative care with transplantation
Early palliative care intervention has been shown to improve symptom burden and depression scores in end-stage liver disease patients awaiting transplant. In addition, early palliative care consultation in conjunction with cancer treatment has been associated with increased survival in non–small-cell lung cancer patients. It has been demonstrated that early integration of palliative care in the surgical ICU alongside disease-directed curative care can be accomplished without change in mortality, while improving end-of-life practice in liver transplant patients.3
What palliative care can do for transplant patients
What does palliative care mean for the person (and family) awaiting transplantation? For the cirrhotic patient with cachexia, ascites, and encephalopathy, it means access to the services of a team trained in the management of these symptoms. Palliative care teams can also provide psychosocial and spiritual support for patients and families who are intimidated by the complex navigation of the health care system and the existential threat that end-stage organ failure presents to them. Skilled palliative care and services can be the difference between failing and extended life with a higher quality of life for these very sick patients
Resuscitation of a patient, whether through restoration of organ function or interdicting the progression of disease, begins with resuscitation of hope. Nothing achieves this more quickly than amelioration of burdensome symptoms for the patient and family.
The barriers for transplant surgeons and teams referring and incorporating palliative care services in their practices are multiple and profound. The unique dilemma facing the transplant team is to balance the treatment of the failing organ, the treatment of the patient (and family and friends), and the best use of the graft, a precious gift of society.
Palliative surgery has been defined as any invasive procedure in which the main intention is to mitigate physical symptoms in patients with noncurable disease without causing premature death. The very success of transplantation over the past 3 decades has obscured our memory of transplantation as a type of palliative surgery. It is a well-known axiom of reconstructive surgery that the reconstructed site should be compared to what was there, not to “normal.” Even in the current era of improved immunosuppression and posttransplant support services, one could hardly describe even a successful transplant patient’s experience as “normal.” These patients’ lives may be extended and/or enhanced but they need palliative care before, during, and after transplantation. The growing availability of trained palliative care clinicians and teams, the increased familiarity of palliative and end-of-life care to surgical residents and fellows, and quality metrics measuring palliative care outcomes will provide reassurance and guidance to address reservations about the convergence of the two seemingly opposite realities.
A modest proposal
We propose that palliative care be presented to the entire spectrum of transplantation care: on the ward, in the ICU, and after transplantation. More specific “triggers” for palliative care for referral of transplant patients should be identified. Wentlandt et al.4 have described a promising model for an ambulatory clinic, which provides early, integrated palliative care to patients awaiting and receiving organ transplantation. In addition, we propose an application for grant funding for a conference and eventual formation of a work group of transplant surgeons and team members, palliative care clinicians, and patient/families who have experienced one of the aspects of the transplant spectrum. We await the subspecialty certification in hospice and palliative medicine of a transplant surgeon. Outside of transplantation, every other surgical specialty in the United States has diplomates certified in hospice and palliative medicine. We await the benefits that will accrue from research about the merging of these fields.
1. Molmenti EP, Dunn GP: Transplantation and palliative care: The convergence of two seemingly opposite realities. Surg Clin North Am. 2005;85:373-82.
2. Cook D, Rocker G. Dying with dignity in the intensive care unit. N Engl J Med. 2014;370:2506-14.
3. Lamba S, Murphy P, McVicker S, Smith JH, and Mosenthal AC. Changing end-of-life care practice for liver transplant patients: structured palliative care intervention in the surgical intensive care unit. J Pain Symptom Manage. 2012; 44(4):508-19.
4. Wentlandt, K., Dall’Osto, A., Freeman, N., Le, L. W., Kaya, E., Ross, H., Singer, L. G., Abbey, S., Clarke, H. and Zimmermann, C. (2016), The Transplant Palliative Care Clinic: An early palliative care model for patients in a transplant program. Clin Transplant. 2016 Nov 4; doi: 10.1111/ctr.12838.
Dr. Azoulay is a transplantation specialist of Assistance Publique – Hôpitaux de Paris, and the University of Paris. Dr. Dunn is medical director of the Palliative Care Consultation Service at the University of Pittsburgh Medical Center Hamot, and vice-chair of the ACS Committee on Surgical Palliative Care.
Best Practices: Protecting Dry Vulnerable Skin with CeraVe® Healing Ointment
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.

- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.
A supplement to Dermatology News. This advertising supplement is sponsored by Valeant Pharmaceuticals.
- Reinforcing the Skin Barrier
- NEA Seal of Acceptance
- A Preventative Approach to Dry, Cracked Skin
- CeraVe Ointment in the Clinical Setting
Faculty/Faculty Disclosure
Sheila Fallon Friedlander, MD
Professor of Clinical Dermatology & Pediatrics
Director, Pediatric Dermatology Fellowship Training Program
University of California at San Diego School of Medicine
Rady Children’s Hospital,
San Diego, California
Dr. Friedlander was compensated for her participation in the development of this article.
CeraVe is a registered trademark of Valeant Pharmaceuticals International, Inc. or its affiliates.

Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
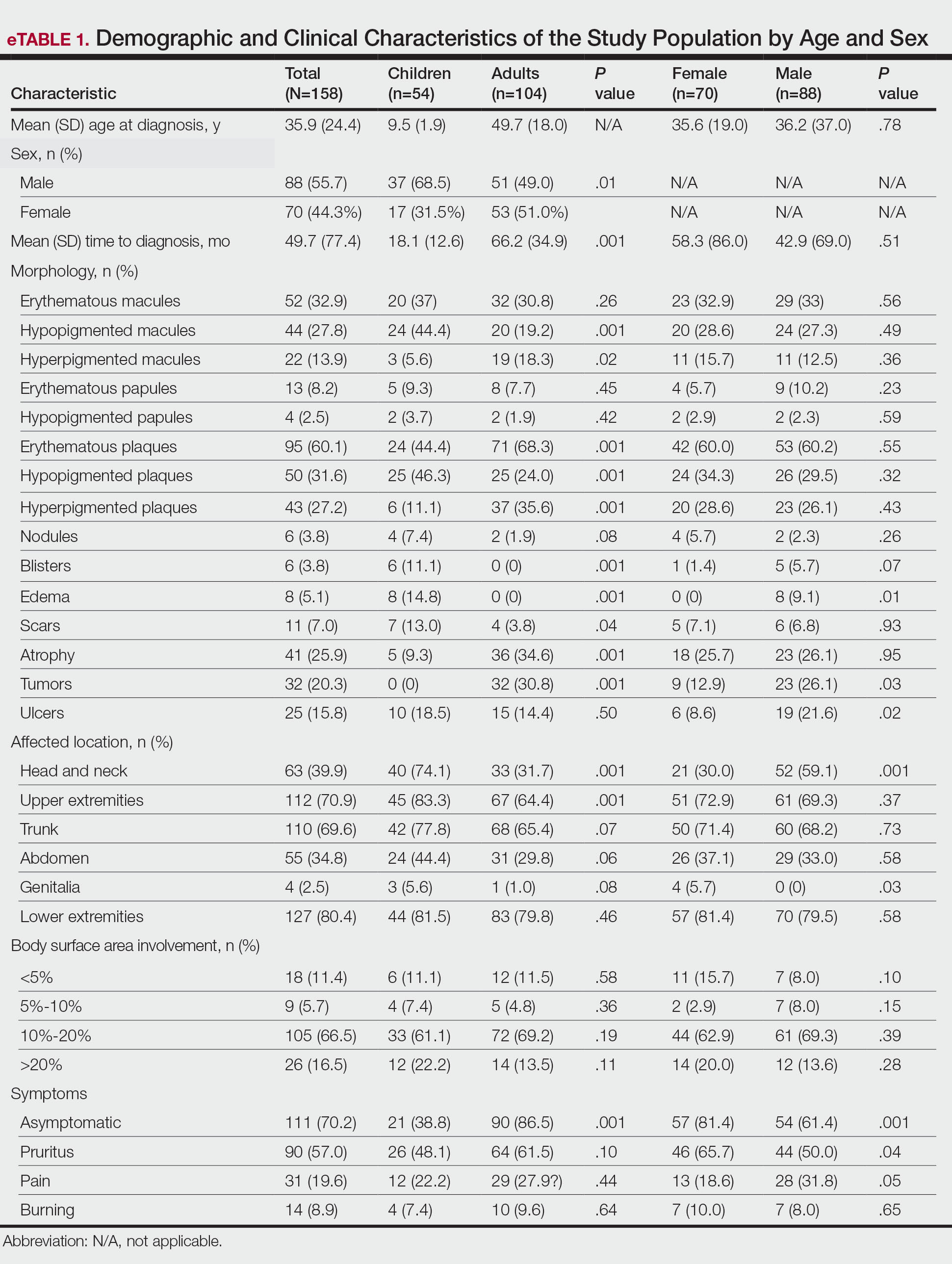
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
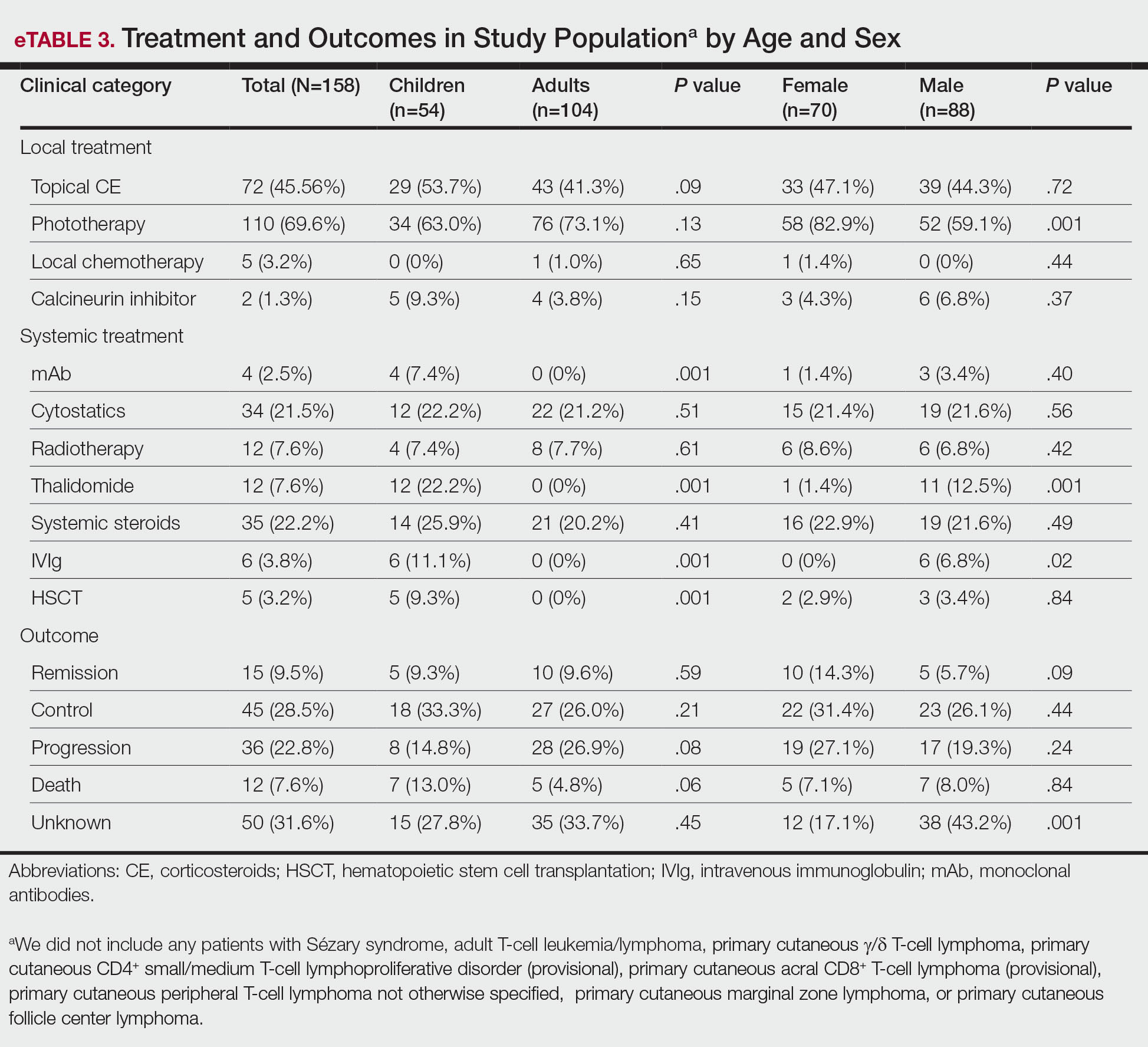
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
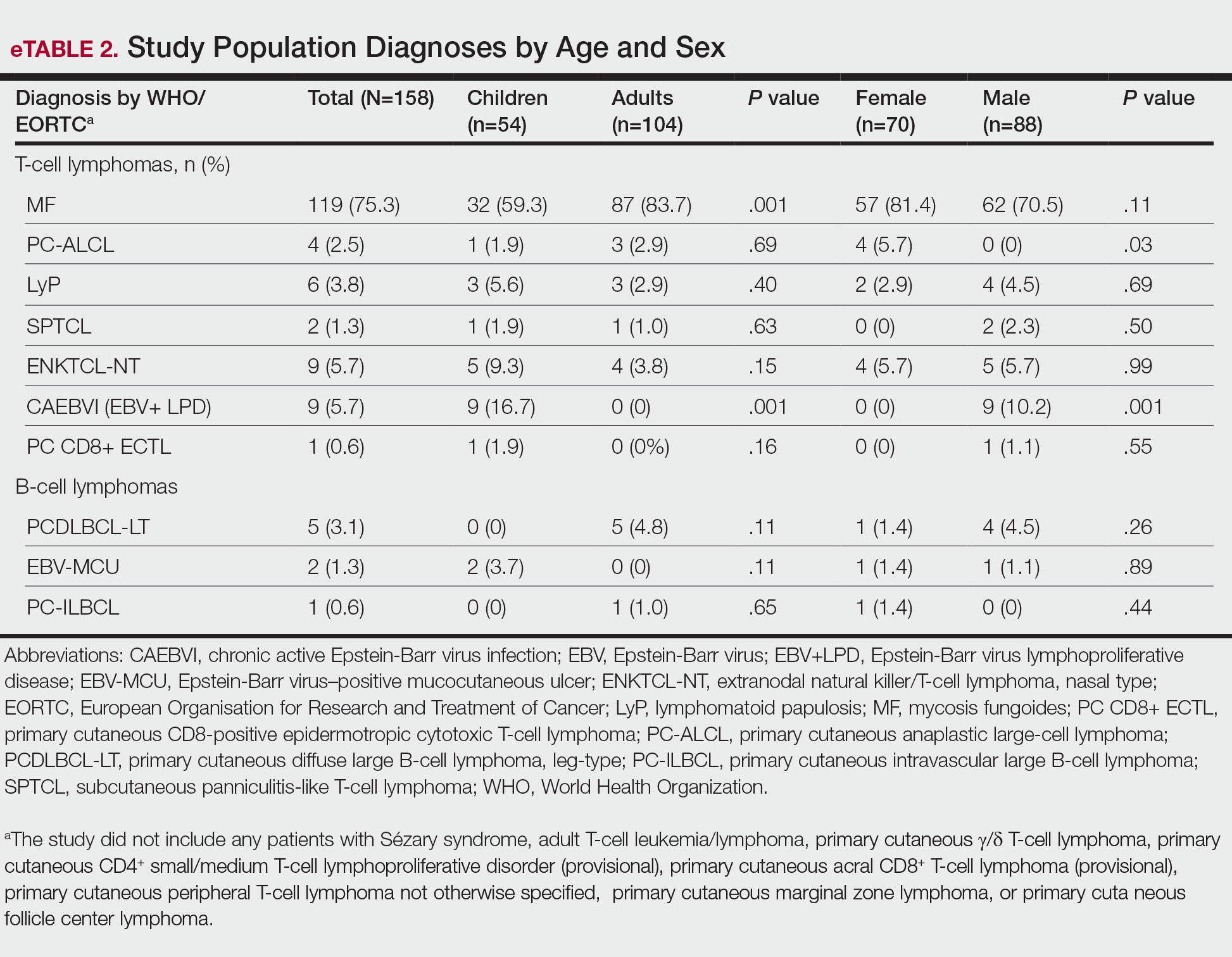
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
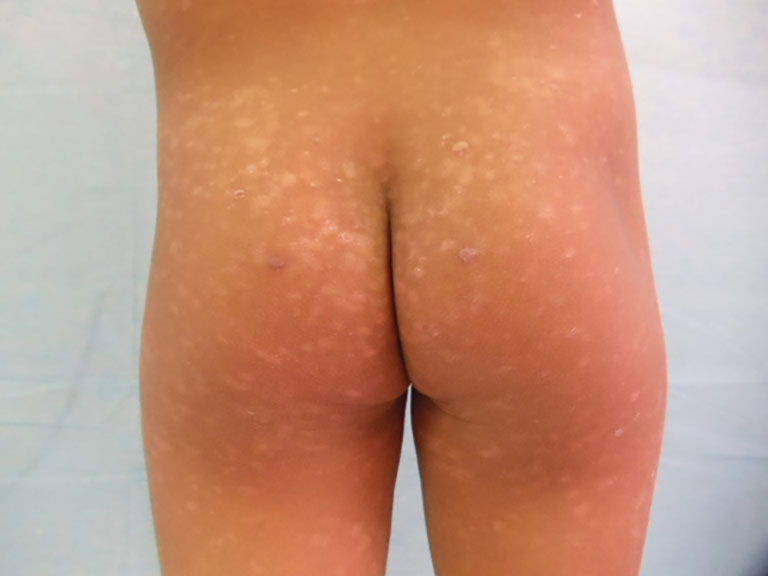
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).

Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).

Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).
Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).
Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Practice Points
- The clinical behavior and incidence of primary cutaneous lymphomas vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.
- Primary cutaneous lymphoma is more common among males, particularly in children.
- Adults experience longer diagnostic delays due to slower symptom progression and overlap with benign skin conditions, whereas children often present with rapidly progressive, severe variants requiring more aggressive therapies.

The Hair-Cut Sign for Scalp Biopsy Site Identification
The Hair-Cut Sign for Scalp Biopsy Site Identification
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
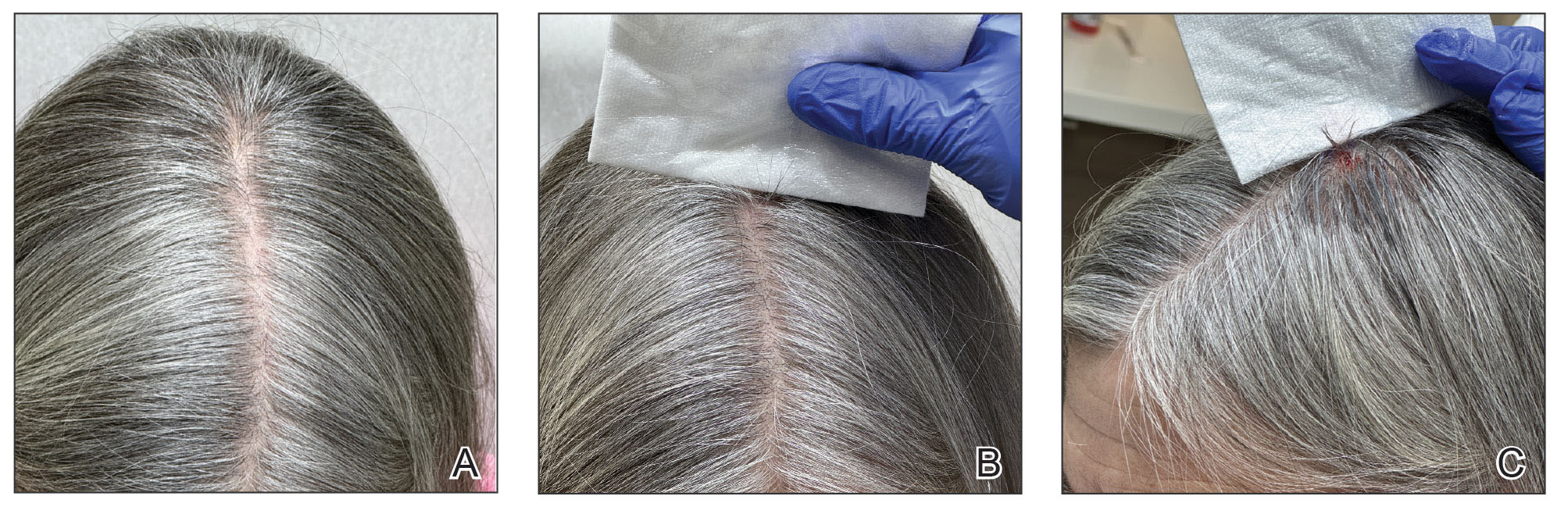
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
Practice Gap
Accurate biopsy site identification prior to Mohs micrographic surgery (MMS) can be challenging, particularly on the scalp, where excellent healing, field cancerization, prior procedures, large surface area, and hair density may complicate localization. Accurate site identification is further hindered when patients are unable to recall the biopsy location, when the biopsy and MMS are performed by different clinicians, or when photographic documentation is absent. Scalp lesions pose an additional challenge because even high-quality photographs may fail to capture subtle landmarks that are obscured by hair.
Wrong-site surgery was the most common serious error reported in a survey of 150 dermatologists, accounting for 19.0% of these errors.1 Research has shown that dermatologists may misidentify biopsy sites in up to 17.6% of cases, and patients (eg, if a patient goes to a dermatologic surgeon and is asked to identify the biopsy site for the surgeon) in up to 25.5% (N=278).2 Additionally, a survey of Mohs surgeons revealed that 14.0% of 42 malpractice cases were due to wrong-site surgery.3 A Delphi consensus study assessing possible preventive interventions found that the best way to document the site is with a photograph in association with landmarks and diagrams.4
The Technique
The hair-cut sign is a simple and effective technique for identifying biopsy sites on the scalp. Hair at the biopsy site typically is cut during biopsy; as the surrounding hair grows, the resulting short tuft serves as an anatomic marker that can persist for weeks to months to facilitate accurate site localization by the Mohs surgeon (Figure). This noninvasive, equipment-free method may be particularly useful when documentation or photography is limited. To maximize its effectiveness, clinical staff should avoid trimming the area before physician verification of the site. The technique is most effective in patients with longer hair and when the interval between biopsy and surgery is less than 3 months, as hair regrowth may reduce contrast with the surrounding scalp.
Practice Implications
Accurate biopsy site identification is a critical component of patient safety in dermatologic surgery, particularly on the scalp, where traditional localization strategies may be unreliable. The hair-cut sign is a simple, reliable, no-cost, and reproducible adjunct to photography, anatomic documentation, and patient verification that may improve site localization and help reduce the risk for wrong-site surgery in select patients to complement standard practices. Incorporating the hair-cut sign into routine scalp surgery workflow represents a low-burden intervention that may improve accuracy when other documentation is limited.
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
- Watson AJ, Redbord K, Taylor JS, et al. Medical error in dermatology practice: development of a classification system to drive priority setting in patient safety efforts. J Am Acad Dermatol. 2013;68:729-737. doi:10.1016/j.jaad.2012.10.058
- Nijhawan RI, Lee EH , Nehal KS. Biopsy site selfies—a quality improvement pilot study to assist with correct surgical site identification. Dermatol Surg. 2015;41:499-504. doi:10.1097/DSS.0000000000000305
- Perlis CS, Campbell RM, Perlis RH, et al. Incidence of and risk factors for medical malpractice lawsuits among Mohs surgeons. Dermatol Surg. 2006;32:79-83. doi:10.1111/1524-4725.2006.32009
- Alam M, Lee A, Ibrahimi OA, et al. A multistep approach to improving biopsy site identification in dermatology: physician, staff, and patient roles based on a Delphi consensus. JAMA Dermatol. 2014;150:550-558. doi:10.1001/jamadermatol.2013.9804
The Hair-Cut Sign for Scalp Biopsy Site Identification
The Hair-Cut Sign for Scalp Biopsy Site Identification

When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
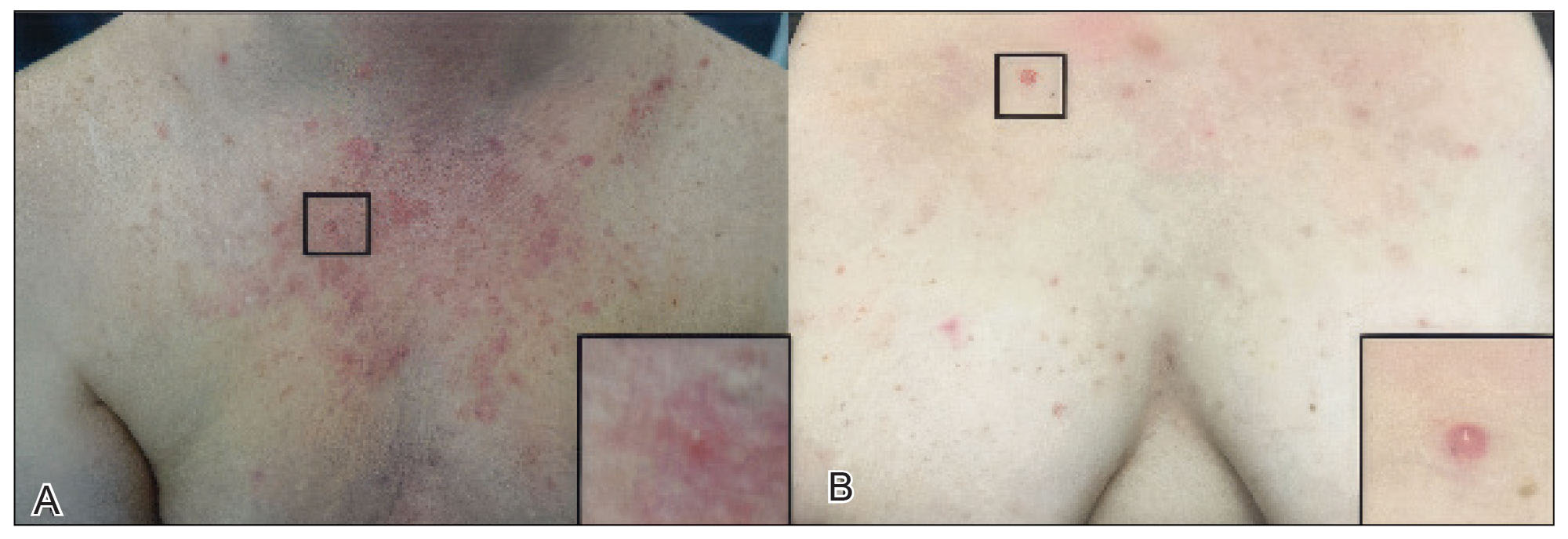
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).

Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
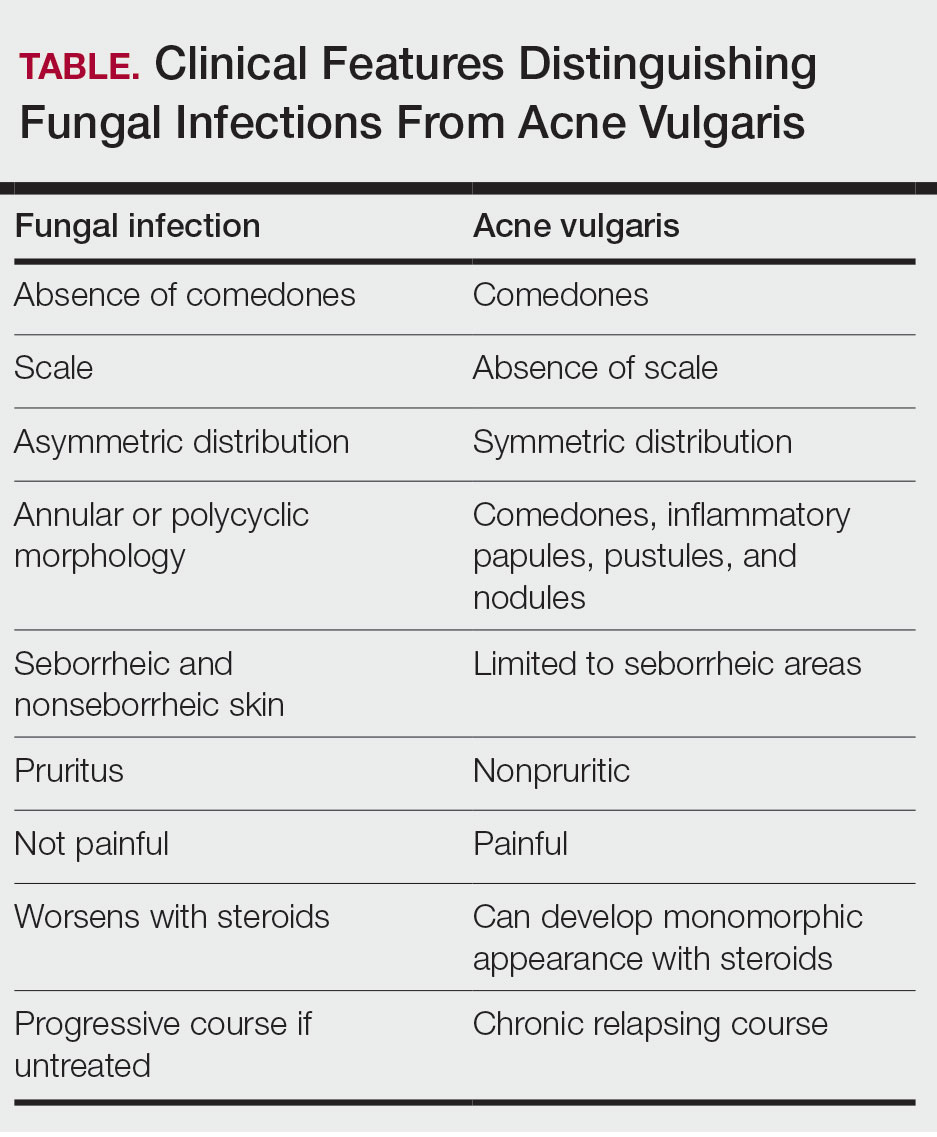
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
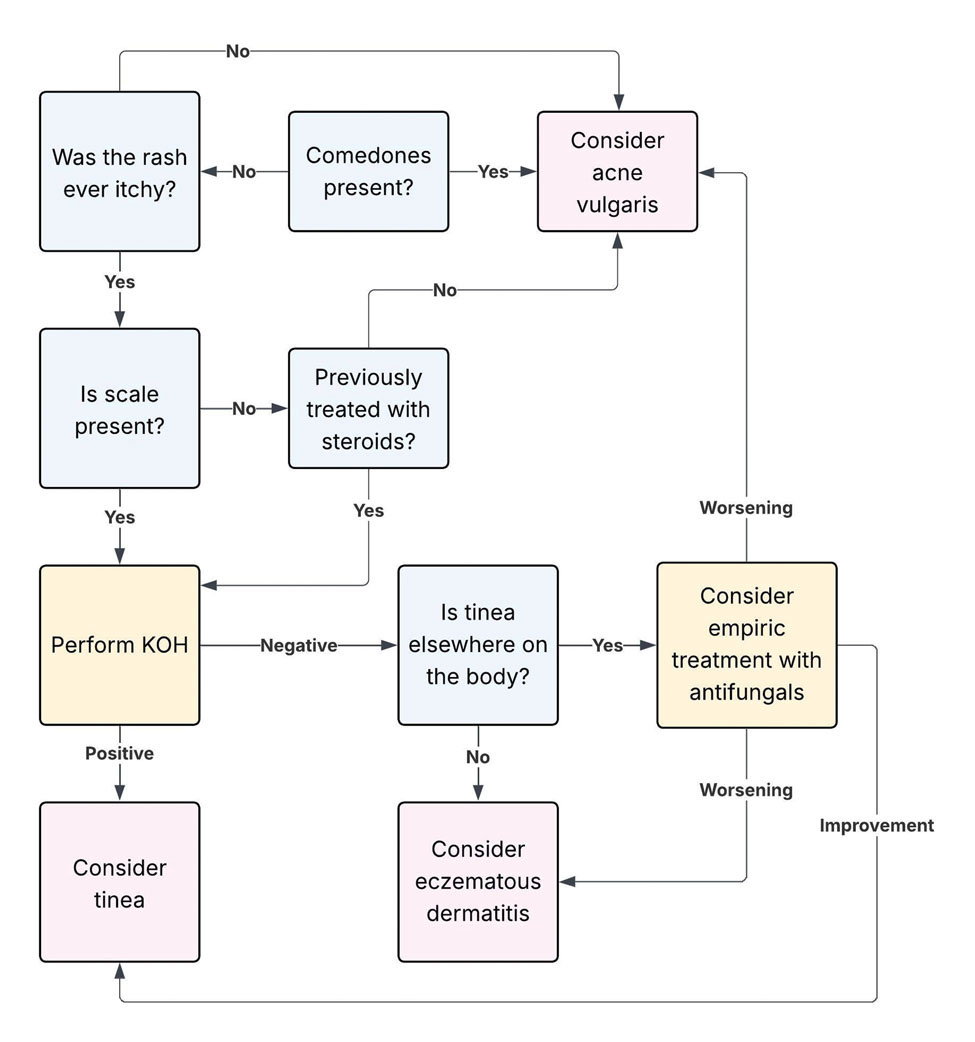
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).
Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
Dermatophyte infections, commonly referred to as tinea, involve the superficial epidermis and are caused by fungi belonging primarily to the genera Trichophyton, Epidermophyton, and Microsporum.1 Malassezia are lipophilic yeasts found in the normal skin flora that can overgrow within hair follicles and trigger an inflammatory response. While both fungal infections are associated with several classic clinical features, they can demonstrate variable clinical morphology, especially when modified by previous topical treatments. In such cases, fungal infections may mimic other forms of inflammatory dermatitis and can be misdiagnosed.
Acne vulgaris is one of the most prevalent dermatologic conditions and typically is diagnosed clinically based on characteristic morphology and distribution. Despite their distinct etiologies, dermatophyte infections and acne vulgaris may manifest with overlapping features, particularly in acne-prone regions such as the face, chest, and back, which may result in diagnostic errors and inappropriate management. This review highlights dermatophyte infections as an underrecognized mimic of acne vulgaris, emphasizing key clinical distinguishing features, common diagnostic pitfalls, and a practical approach to evaluation.
Clinical Overlap of Dermatophyte Infections and Acne
Despite their fundamentally different etiologies, dermatophyte infections and acne may demonstrate overlapping clinical morphology and anatomic distribution, creating diagnostic challenges and increasing misdiagnosis risk. Clinically, acne is characterized by the presence of open and closed comedones as well as inflammatory papules, pustules, nodules, and occasionally cysts.2 In contrast, dermatophyte infections classically manifest as annular erythematous plaques with peripheral scale and central clearing, primarily due to their superficial confinement to the stratum corneum; however, in certain cases the dermatophyte invades the hair follicle, which can lead to the formation of folliculocentric pustules.1 This is known as dermatophyte folliculitis and may closely resemble the pustules observed in acne.
Follicular invasion by dermatophytes is more likely in cases in which infection has been misdiagnosed as a noninfectious inflammatory dermatosis, (eg, atopic dermatitis) and treated with topical corticosteroids. Corticosteroid-induced local immunosuppression facilitates deeper and more extensive proliferation of the invading fungus, including into the hair follicle. Topical corticosteroid use may further obscure the diagnosis of a dermatophyte infection by masking its hallmark features such as scale and annularity.3 This steroid-altered dermatophyte infection is referred to as tinea incognita and may be misdiagnosed as acne or another inflammatory dermatosis. When dermatophytes extend from the stratum corneum into the dermis due to local immunosuppression (eg, corticosteroid use), trauma, shaving, or occlusion, the resulting deep follicular infection is known as Majocchi granuloma.
Further complicating the diagnostic picture is the substantial anatomic and epidemiologic overlap between dermatophyte infections and acne vulgaris. Acne preferentially affects sebum-rich areas, including the face, chest, and back.2 Dermatophytes, by contrast, thrive in keratinized tissue.1 Because areas with a higher density of hair follicles contain abundant keratin, dermatophyte infections often involve the same sebum-rich regions affected by acne. Both acne and tinea are observed frequently in adolescents, possibly due to hormonal changes that increase sebum production and create an environment conducive to fungal growth.4
Pityrosporum Folliculitis Manifesting as Acne Vulgaris
Although it has been widely popularized in lay and social media, the term fungal acne is a misnomer; this entity more accurately represents a fungal folliculitis manifesting as an acneform eruption. In most cases, fungal acne refers to Malassezia folliculitis, also called pityrosporum folliculitis, which is caused by Malassezia species. Malassezia are not dermatophytes but rather lipophilic yeasts found in the normal skin flora. Whereas dermatophytes are drawn to highly keratinized tissue, Malassezia are drawn to lipid-rich environments of the skin. In these conditions, including sweating and hot or humid environments, Malassezia may proliferate to pathogenic levels within the hair follicle.5
Clinically, Malassezia folliculitis manifests as monomorphic, folliculocentric, dome-shaped papules and pustules with occasional progression to nodules or cysts in more severe cases.5 Lesions typically are intensely pruritic, a distinguishing feature that helps differentiate them from acne vulgaris.6 The eruption predominantly involves sebum-rich areas, including the face, hairline, chest, and upper back (Figure 1).5 Overall, the clinical presentation often more closely resembles steroid-induced acne than classic acne vulgaris. Antibiotic exposure is an important risk factor, potentially due to disruption of the normal skin microbiome and subsequent yeast overgrowth; for example, in a retrospective review of 110 patients (age range, 0-21 years) with Malassezia folliculitis, more than 75% had recently received antibiotics for treatment of acne.6 Additional predisposing factors include corticosteroid use and immunosuppression.5
Importantly, Malassezia folliculitis and acne vulgaris may coexist, further complicating diagnosis. In a study of 217 patients with acne vulgaris, cytologic evaluation demonstrated Malassezia overgrowth (defined as >6 spores per high-power field) in approximately 25% of patients, of whom 70% responded to antifungal therapy.7 Similarly, a study of 300 patients with newly diagnosed acne found a prevalence of Malassezia folliculitis of almost 30%. Patients with concurrent Malassezia folliculitis and acne were more likely to report pruritus and have involvement of the scalp, hairline, and upper back compared to those with acne alone.8
Tinea Faciei and Tinea Barbae Manifesting as Facial Acne
Tinea faciei describes a dermatophyte infection of the nonbearded area of the face, whereas infection of the beard-bearing region is known as tinea barbae. In North America, Trichophyton species are the leading cause of tinea faciei.1 Clinically, tinea faciei manifests as one or more erythematous scaly plaques on the face, often associated with pruritus. Lesions often assume an annular shape with an advancing border along which pustules, vesicles, or crusting can be observed. In cases of inappropriate treatment with topical corticosteroids, lesions may lose their characteristic scale and annularity and instead become papular, mimicking the acneform eruptions of facial acne vulgaris (Figure 2).
Like tinea faciei, tinea barbae most commonly develops from infection with Trichophyton species but differs in its clinical presentation. While superficial scaly variants exist, tinea barbae more frequently manifests as a deep, papular, inflammatory folliculitis. This deeper form typically is caused by follicular infiltration by zoophilic dermatophytes such as Trichophyton verrucosum and Microsporum canis. Not surprisingly, infection by these zoophilic dermatophytes is associated with exposure to animals such as cattle, horses, dogs, and cats, and a history of agricultural work may offer a helpful clue to diagnosis.9 The tender, nodular, or nodulocystic lesions of severe tinea barbae infections may closely resemble nodulocystic acne.
Misdiagnosis, inappropriate treatment, and diagnostic delays are common in patients with tinea faciei and tinea barbae. In a retrospective study of 818 cases of tinea faciei, approximately 30% of patients had received prior corticosteroid treatment at the time of diagnosis.10 Similarly, a cross-sectional study of 7 adult patients with tinea barbae in a Portuguese hospital found that 3 cases initially were misdiagnosed and that in 2 cases potent topical steroids were previously applied.11 Finally, in a retrospective review of 38 patients with mycologically confirmed tinea faciei, the mean duration from symptom onset to diagnosis was 3.4 months.10 Notably, nearly 60% of patients had concomitant dermatophyte infections at other body sites, most commonly involving the feet and toes, highlighting that recognition of dermatophyte infections elsewhere on physical examination may provide an important diagnostic clue.12
Tinea Corporis Manifesting as Truncal Acne
Tinea corporis refers to a dermatophyte infection involving the glabrous, or hairless, skin of the trunk and extremities. Trichophyton rubrum accounts for 80% to 90% of the pathogenic strains that cause tinea corporis.1 As with other variants of superficial dermatophyte infections, tinea corporis classically manifests as annular erythematous plaques with peripheral scale and central clearing, distinguished by its involvement of the trunk. Pruritus of lesions is variable.1
Inappropriate treatment of tinea corporis with topical corticosteroids may induce a morphologic change in the infection so that it resembles the lesions of truncal acne, which characteristically involves the chest, upper back, and shoulders, and less frequently the lower back and abdomen.2 As in other forms of acne vulgaris, the lesions are characterized by a mixture of inflammatory papules, pustules, and comedones. When differentiating tinea corporis and truncal acne, consider the distribution and symmetry of the lesions. Dermatophyte infections often are localized to one area of the trunk and are asymmetric. In contrast, acne typically is generalized and manifests more symmetrically.
Additional clinical clues may aid in differentiation. An acneform eruption involving other seborrheic areas of the body (eg, the face) supports a diagnosis of truncal acne. Conversely, the presence of tinea elsewhere, particularly on the hands or feet, may suggest tinea corporis. Finally, although pustules can be seen with tinea corporis, the presence of true comedones is a key distinguishing factor favoring acne vulgaris.
Importantly, resistant dermatophyte infections have emerged as a growing concern among public health experts over the past decade. A recently described species, Trichophyton indotineae, has played a substantial role in driving these cases.13 While early US cases largely were limited to patients who had travelled to Bangladesh, infections now are increasingly reported in individuals without travel history.13 Trichophyton indotineae most commonly involves the trunk, extremities, and groin, which mirrors the distribution of truncal acne. Further complicating the clinical picture is the lack of response to standard antifungal therapies such as oral terbinafine in these patients.13 Failure to consider this diagnosis, particularly given its recent recognition, may lead physicians to empirically switch treatment to topical or systemic corticosteroids. This can further alter lesion morphology and increase the likelihood of misdiagnosis.
Helpful Bedside Diagnostic Tools
When clinical findings are equivocal, bedside diagnostic tools, including dermoscopy, a Wood lamp, potassium hydroxide (KOH) preparation, and histopathology, may be helpful in differentiating cutaneous fungal infections from acne.
Dermoscopy—In an observational study of 81 patients with fungal folliculitis, dermoscopy demonstrated a diagnostic accuracy of 76.5%.14 Dermoscopic findings in a cohort of 45 patients with KOH-confirmed Malassezia folliculitis included folliculocentric lesions and background erythema (100%); dotted, linear, or tortuous vessels (89%); fine white scale (78%); perifollicular hypopigmentation (64%); coiled or looped hairs (58%); and broken hairs (13%).15 Moreover, in a study comparing 36 microscopically confirmed tinea cases with 40 negative cases, peripheral scales (odds ratio [OR], 5.2; 95% CI, 2.0-13.5), moth-eaten scales (OR, 3.9; 95% CI, 1.9-8.1), broken hairs (OR, 5.8; 95% CI, 2.0-16.6), and outward-peeling scales (OR, 14.3; 95% CI, 1.3-155.2) were predictive of tinea.16 Dermoscopic findings in a cross-sectional study of 100 clinically diagnosed tinea cases included diffuse erythema with whitish scars (100.0%), follicular micropustules (36.7%), brown spots with a white-yellow halo (20.0%), wavy or broken hairs (13.0%), and Morse code– like vellus hairs (3.0%).17 In tinea incognito, features such as Morse code–like hairs, deformable translucent hairs, comma and corkscrew hairs, and perifollicular scaling may persist despite corticosteroid use.18,19
Wood Lamp Examination—Wood lamp examination may be a helpful adjunctive tool for diagnosis of Malassezia folliculitis. In a study of 264 patients with folliculitis (49 of whom were diagnosed with Malassezia folliculitis), Wood lamp examination demonstrated yellow-green fluorescence in 66.7% of cases.20 In contrast, this method has limited utility in diagnosing common dermatophyte infections, as only Microsporum and a small subset of Trichophyton species fluoresce.21 In a study of 50 pediatric patients with tinea capitis, Microsporum cases were identified via Wood lamp examination by bright green fluorescence. Wood lamp examination demonstrated 73% sensitivity and 100% specificity for Microsporum canis, confirmed by microscopy and culture, indicating that positive results are highly reliable for this genus, though false negatives may occur.22
Some dermatoscopes incorporate a Wood lamp, enabling UV-induced fluorescence dermoscopy (UVFD). In a study of 208 patients with nonneoplastic dermatoses, UVFD of tinea showed light green hair shaft concretions in 27% (4/15) of patients and no fluorescence in 73% (11/15), whereas Malassezia folliculitis demonstrated blue follicular concretions in 85% (11/13) and acne showed disruption of uniform follicular red fluorescence in 81% (13/16).23 However, these dermatoscopes are not widely available.
KOH Preparation—While the aforementioned tests are useful and require minimal effort, the diagnostic test of choice for cutaneous fungal infections remains the KOH preparation, which is fast and inexpensive and offers immediate results, often while the patient is still in the office. The test should be performed by obtaining scale, ideally from an active lesion border, by gently scraping the stratum corneum, often with a #15 blade. For sampling of pustules or when there is concern for Malassezia folliculitis, optimal technique involves unroofing a pustule and transferring its contents onto a slide for KOH preparation. The specimen then is treated with KOH, a keratolytic agent that dissolves keratinocytes and facilitates visualization of fungal elements under light microscopy. Reported sensitivity and specificity of KOH preparation are approximately 73% and 78%, respectively.24 Notably, sensitivity and specificity of KOH is highly dependent on expertise. A fungal culture also can be collected and sent for microbiologic analysis, although results often are delayed. In one pooled analysis of tinea pedis using clinical assessment as the reference standard, fungal culture demonstrated a sensitivity of 42% and specificity of 78%, though these estimates are highly dependent on study design and sampling technique.24
Histopathology—Finally, histopathologic evaluation may be considered in diagnostically challenging cases. Histology of Malassezia folliculitis demonstrates fungal spores within the follicular lumen, while histology of acne shows irregular keratin plugging, nuclear debris within the follicular lumen, and intrafollicular inflammation. Notably, perifollicular inflammatory infiltrates are histologically similar in acne and Malassezia folliculitis.25
Practical Diagnostic Approach to Differentiating Dermatophyte Infections from Acne
For physicians encountering papulopustular eruptions in acne-prone regions, distinguishing acne vulgaris from dermatophyte infection can be challenging. A stepwise approach incorporating history, morphology, and distribution can improve diagnostic accuracy and guide appropriate management.
First, obtain a thorough treatment history. Presumed acne that has failed to respond to appropriate acne therapies should prompt reconsideration of the diagnosis. Prior treatment with topical corticosteroids should be specifically assessed. Patients may not volunteer this history unless directly asked. Corticosteroid use can alter the clinical appearance of dermatophyte infections, leading to diagnostic confusion.
Second, use morphologic features and lesion distribution as diagnostic clues. The presence of comedones favors acne vulgaris, whereas their absence should raise suspicion for tinea. It is important to note, however, that certain dermatophyte infections may manifest with folliculocentric pustules, which can mimic closed comedones or inflammatory lesions seen in acne. Acne vulgaris also typically demonstrates a bilateral and relatively symmetric distribution, particularly on the face, chest, and upper back. In contrast, dermatophyte infections are more often asymmetric or localized, especially in early stages.
Patient-reported symptoms and a complete skin examination can further aid in differentiation. While acne may occasionally be pruritic, pain or tenderness is more commonly reported. In contrast, dermatophyte infections often will have prominent pruritus, which frequently is the patient’s primary complaint. The presence of tinea on the hands or feet supports a diagnosis of dermatophyte infection, whereas concurrent acneform lesions in classic seborrheic regions favor acne vulgaris. The Table outlines key clinical features that help distinguish dermatophyte infections from acne vulgaris.
When the diagnosis remains unclear after clinical assessment, physicians may utilize both bedside and laboratory tests, including dermoscopy, Wood lamp examination, in-office KOH preparation, and/or fungal culture, as discussed previously. In cases of diagnostic uncertainty, empiric antifungal therapy is preferred over topical corticosteroid therapy, as corticosteroids may exacerbate an underlying dermatophyte infection. In refractory or diagnostically challenging cases, skin biopsy with periodic acid–Schiff staining may be considered to confirm the presence of fungal organisms. Biopsy generally is reserved for cases that fail to respond to empiric therapy or when diagnostic confirmation is strongly desired. Figure 3 provides an algorithmic approach to distinguishing acne vulgaris from dermatophyte infection.
Final Thoughts
Dermatophyte infections are a common but often overlooked mimic of acne vulgaris. Clinically, acne is characterized by comedones, whereas dermatophyte infections typically demonstrate scale, though these features can be less apparent in modified presentations. In cases of diagnostic uncertainty, physicians should keep dermatophyte infections in mind and be comfortable performing bedside KOH preparations to support timely diagnosis. Early recognition is important to reduce morbidity and avoid inappropriate treatments, particularly corticosteroids, which can worsen the infection and delay improvement.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
- Yee G, Syed HA, Al Aboud AM. Tinea corporis. StatPearls (Internet). Updated February 14, 2025. Accessed June 5, 2026. https://www.ncbi. nlm.nih.gov/books/NBK544360/
- Sutaria AH, Masood S, Saleh HM, et al. Acne vulgaris. StatPearls (Internet). Updated August 17, 2023. Accessed June 5, 2026. https://www. ncbi.nlm.nih.gov/books/NBK459173/
- Ive FA, Marks R. Tinea incognito. Br Med J. 1968;3:149-152.
- Zarzeka D, Benedict K, McCloskey M, et al. Current epidemiology of tinea corporis and tinea cruris causative species: analysis of data from a major commercial laboratory, United States. J Am Acad Dermatol. 2024;91:559-562.
- Vlachos C, Henning MAS, Gaitanis G, et al. Critical synthesis of available data in Malassezia folliculitis and a systematic review of treatments. J Eur Acad Dermatol Venereol. 2020;34:1672-1683.
- Prindaville B, Belazarian L, Levin NA, et al. Pityrosporum folliculitis: a retrospective review of 110 cases. J Am Acad Dermatol. 2018;78:511-514.
- Pürnak S, Durdu M, Tekindal MA, et al. The prevalence of Malassezia folliculitis in patients with papulopustular/comedonal acne, and their response to antifungal treatment. Skinmed. 2018;16:99-104.
- Paichitrojjana A, Chalermchai T. The prevalence, associated factors, and clinical characterization of Malassezia folliculitis in patients clinically diagnosed with acne vulgaris. Clin Cosmet Investig Dermatol. 2022;15:2647-2654.
- Kuruvella T, Saleh HM, Pandey S. Tinea barbae. StatPearls (Internet). Updated December 5, 2024. Accessed June 5, 2026. https://www.ncbi .nlm.nih.gov/books/NBK563204/
- del Boz J, Crespo V, de Troya M. Pediatric tinea faciei in southern Spain: a 30-year survey. Pediatr Dermatol. 2012;29:249-253.
- Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079-1083.
- Kwak HB, Lee SK, Yoo HH, et al. Facial tinea incognito: a clinical, dermoscopic and mycological study of 38 cases. Eur J Dermatol. 2023;33:101-108.
- Caplan AS, Todd GC, Zhu Y, et al. Clinical course, antifungal susceptibility, and genomic sequencing of Trichophyton indotineae. JAMA Dermatol. 2024;160:701-709.
- Durdu M, Errichetti E, Eskiocak AH, et al. High accuracy of recognition of common forms of folliculitis by dermoscopy: an observational study. J Am Acad Dermatol. 2019;81:463-471.
- Jakhar D, Bhatia V, Gupta RK, et al. Dermoscopy as an auxiliary tool in the assessment of Malassezia folliculitis: an observational study. Actas Dermosifiliogr. 2022;113:T78-T81.
- Lekkas D, Ioannides D, Lazaridou E, et al. Dermatoscopy of tinea corporis. J Eur Acad Dermatol Venereol. 2020;34:E278-E280.
- Bhat YJ, Keen A, Hassan I, et al. Can dermoscopy serve as a diagnostic tool in dermatophytosis? a pilot study. Indian Dermatol Online J. 2019;10:530-535.
- Gómez Moyano E, Crespo Erchiga V, Martínez Pilar L, et al. Correlation between dermoscopy and direct microscopy of morse code hairs in tinea incognito. J Am Acad Dermatol. 2016;74:E7-E8.
- Sonthalia S, Ankad BS, Goldust M, et al. Dermoscopy—a simple and rapid in vivo diagnostic technique for tinea incognito. An Bras Dermatol. 2019;94:612-614.
- Durdu M, Güran M, Ilkit M. Epidemiological characteristics of Malassezia folliculitis and use of the May-Grünwald-Giemsa stain to diagnose the infection. Diagn Microbiol Infect Dis. 2013;76:450-457.
- Dyer JM, Foy VM. Revealing the unseen: a review of Wood’s lamp in dermatology. J Clin Aesthet Dermatol. 2022;15:25-30.
- Sun D, Lu J, Liu T, Wang J. Wood’s lamp for early detection of Microsporum canis tinea capitis in children. Photodiagnosis Photodyn Ther. 2025;51:104428.
- Errichetti E, Pietkiewicz P, Bhat YJ, et al. Diagnostic accuracy of ultraviolet- induced fluorescence dermoscopy in non-neoplastic dermatoses (general dermatology): a multicentric retrospective comparative study. J Eur Acad Dermatol Venereol. 2025;39:97-108.
- Levitt JO, Levitt BH, Akhavan A, et al. The sensitivity and specificity of potassium hydroxide smear and fungal culture relative to clinical assessment in the evaluation of tinea pedis: a pooled analysis. Dermatol Res Pract. 2010;2010:764843.
- An MK, Hong EH, Cho EB, et al. Clinicopathological differentiation between Pityrosporum folliculitis and acneiform eruption. J Dermatol. 2019;46:978-984.
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
When Fungal Infections Mimic Acne: Diagnostic Pitfalls and Practical Approaches
Practice Points
- Folliculocentric pustules and/or papules from dermatophytes (including tinea incognita and Majocchi granuloma) or Malassezia folliculitis can closely mimic acne, especially following steroid use.
- Key red flags for dermatophyte infection include an absence of comedones, pruritus, and asymmetric or localized lesions in sebum‐rich zones.
- Bedside tools such as dermoscopy, Wood lamp examination, and in-office potassium hydroxide preparation can provide rapid differentiation between dermatophyte infections and acne.
- Prompt antifungal treatment and avoidance of topical steroids can prevent deeper fungal invasion.

Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.

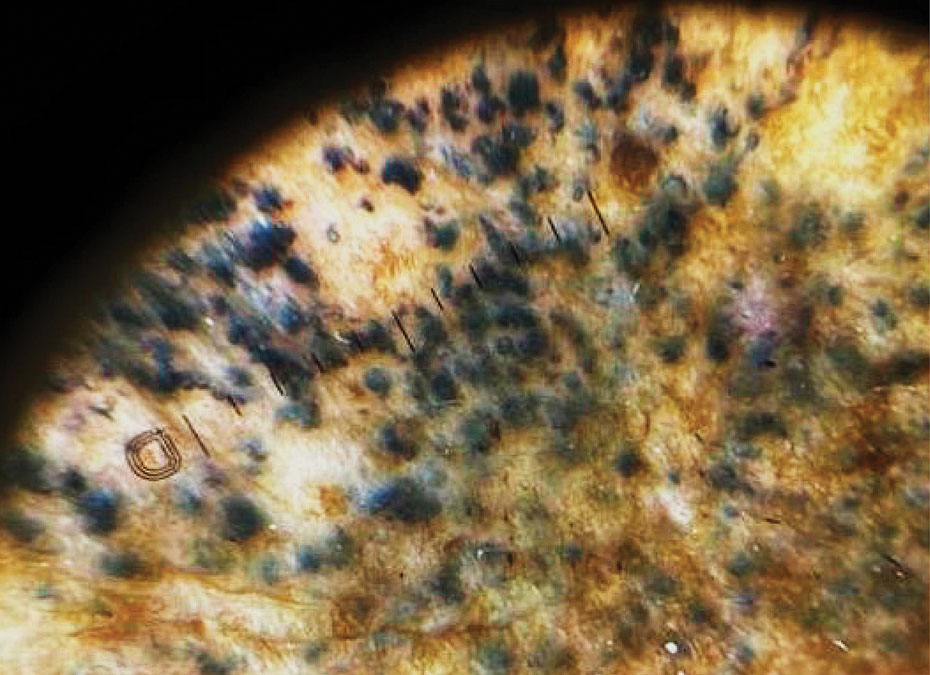
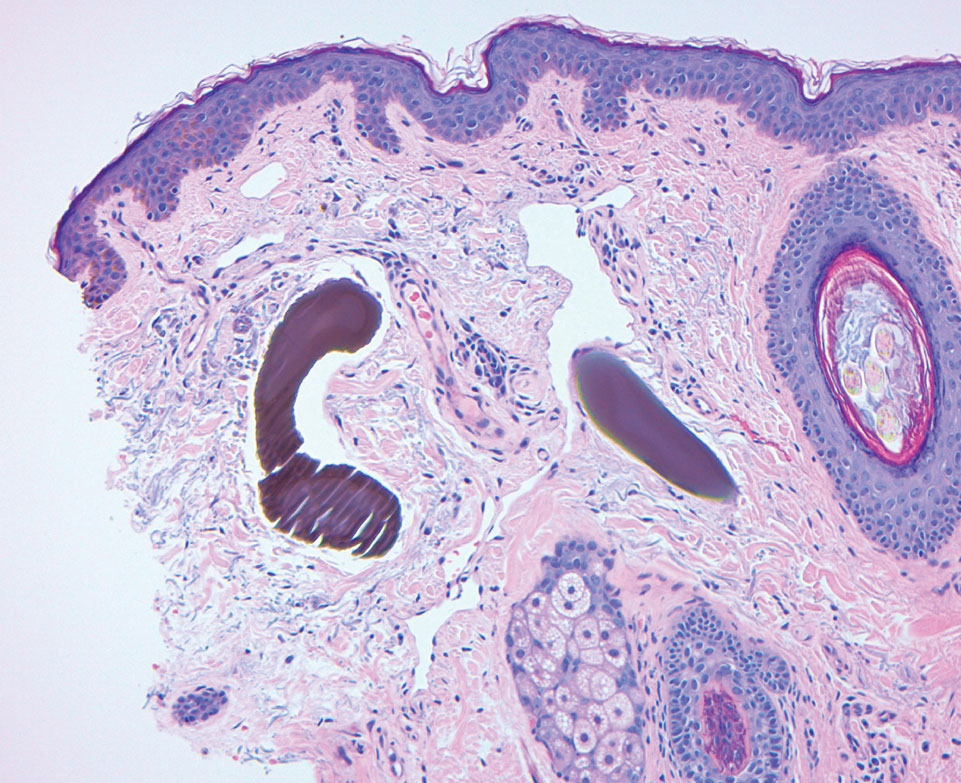
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
To the Editor:
Exogenous ochronosis (EO) is a rare dyschromia that affects individuals with darker skin tones and results from the application of skin-lightening topical agents, most commonly those containing hydroquinone. Hydroquinone-induced EO usually is reported outside the United States, mainly in African and South Asian patients,1 as well as after long-term use of high‑concentration hydroquinone. We report a case of stage II EO that developed in a patient in the United States following 6 months' use of hydroquinone cream 2% that was purchased online.
A 75-year-old Black man presented to the dermatology clinic with dark discoloration on the cheeks of 6 months’ duration. He reported that the hyperpigmentation had developed after 6 months of daily use of an over-the-counter (OTC) cream containing 2% hydroquinone, which he purchased online to treat melasma of the bilateral cheeks and temples that had been present for at least a decade. The patient was otherwise healthy and did not take any other daily medications. He was a landscaper by occupation and spent most days outdoors. He reported a history of recurrent blistering sunburns and reported that he applied sunscreen with a sun protection factor of 30 to the face on most days.
Physical examination revealed gray-black, coarsely textured papules and plaques on a background of brown pigmentation involving the malar cheeks. Reticulated, blue-black, caviarlike papules were present within the plaques (Figure 1). Dermoscopy revealed blue-black globules and globularlike structures on a brown background with the absence of follicular openings (Figure 2). A punch biopsy from the left malar cheek revealed banana-shaped, yellow-brown deposits with heavy elastosis in the superficial dermis (Figure 3). The patient was advised to permanently discontinue hydroquinone and was prescribed topical adapalene. He was evaluated for treatment with a fractional erbium-doped yttrium aluminum garnet laser but ultimately elected not to pursue treatment.
Hydroquinone has long been a first-line topical agent for the treatment of skin dyschromia. It generally is regarded as a safe and effective therapy when used under the supervision of a dermatologist. Prolonged use of topical hydroquinone is known to induce paradoxical EO. This acquired dyschromia is characterized by the development of blue-black or gray-blue pigmented patches as well as caviarlike black papules, papulonodules, and skin atrophy in more severe cases.2 Most cases are documented in African and South Asian countries, with fewer than 100 cases described in the United States.2 Despite the rarity of EO in the United States, concerns regarding the unsupervised use of hydroquinone contributed to regulatory changes. In response to the CARES Act and Over-the-Counter Drug Monograph Reform, the sale of OTC hydroquinone-based products became prohibited in September 2020 in the United States.³ Prior to the CARES Act, an estimated 10 million tubes of OTC hydroquinone were sold, and approximately 330,000 prescriptions were written in 2019.2,4 Subsequently, its availability was converted to prescription only in the United States.
Exogenous ochronosis occurs in 3 clinical stages: (I) erythema and hyperpigmentation, (II) black colloid milia (caviarlike papules) and atrophy, and (III) papulonodules.1 Our patient’s case was unusual, as EO is most commonly described after exposure to high concentrations and prolonged hydroquinone treatment. In a global retrospective review of 126 patients of varied racial and ethnic backgrounds with hydroquinone-induced ochronosis, EO was most frequently reported with concentrations exceeding 4%. The median duration of use was 5 years, and only 12 cases (9.5%) of EO were reported with 1 year of use or less, including 4 cases with 3 months or less of use.1
While large epidemiologic studies from South Africa have reported EO prevalence rates as high as 69% among users of skin-lightening products,6 a search of the PubMed, Scopus, and Web of Science databases using the terms exogenous ochronosis and hydroquinone identified only 39 cases in US-based literature between 1983 and 2020.2 In a retrospective review of 25 cases of EO in the United States, the average length of product use was 9.2 years, and the shortest duration was 1.5 years.7
The pathogenesis of EO is thought to occur due to the inhibitive effect of topical hydroquinone on homogentisic acid oxidase, resulting in the accumulation of homogentisic acid in tissues and ochronotic deposits.1,5 We suspect that our patient’s occupation as a landscaper and associated chronic sun exposure may have accelerated the development of EO, as UV exposure and inadequate photoprotection have been described as risk factors in the development and severity of EO.8 Although the patient reported daily application of sun protection factor 30 sunscreen, the extent of his outdoor occupational exposure may have exceeded the protection afforded.
Treatment of EO is notoriously challenging, and skin changes often are permanent. Of the 25 patients identified in a 10-year retrospective analysis of EO at a single US center, none responded to topical treatment alone.7 Among those who underwent procedural interventions, 3 patients treated with microneedling and 3 patients treated with Q-switched Alexandrite laser demonstrated favorable outcomes; however, this was a retrospective chart review, not a controlled trial with predefined treatment arms.7 Bellew et al9 reported 2 patients with EO who showed progressive lightening in response to Q-switched Alexandrite laser treatments. In this case series, the first patient received 6 treatments at 2-month intervals and the second received 4 treatments at 4-month intervals. Posttreatment biopsies demonstrated decreased dermal pigmentation, and neither patient experienced scarring or textural changes. Méndez Baca et al10 demonstrated successful lightening of pigmentation in a patient with medium-toned skin following 9 sessions with a fractional nonablative picosecond laser. Ceglio et al11 described a stepwise treatment approach in a patient with dark brown skin with EO, beginning with 12 sessions of a 1064-nm Q-switched Nd:YAG laser that yielded slight improvement, followed by 7 sessions of intense pulsed light therapy with partial response, and ultimately achieving marked improvement after 5 bimonthly sessions of fractional 10,600-nm carbon dioxide laser.
This case highlights the potential for EO to develop even with low-concentration (2%) hydroquinone obtained through unregulated online sources, underscoring the need for dermatologist supervision when hydroquinone is used. Despite the 2020 prohibition of OTC hydroquinone sales in the United States, patients continue to access these products online. Clinicians should maintain a high index of suspicion for EO in patients presenting with paradoxical facial hyperpigmentation and a history of unsupervised hydroquinone use.
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
- Ishack S, Lipner SR. Exogenous ochronosis associated with hydroquinone: a systematic review. Int J Dermatol. 2022;61:675-684. doi:10.1111/ijd.15878
- Qorbani A, Mubasher A, Sarantopoulos GP, et al. Exogenous ochronosis (EO): skin lightening cream causing rare caviar-like lesion with banana-like pigments; review of literature and histological comparison with endogenous counterpart. Autops Case Rep. 2020;10:E2020197. doi:10.4322/acr.2020.197
- Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub L No. 116-136, §3851, 134 Stat 281 (2020).
- Hydroquinone, found in skin lightening agents worldwide, linked with increased skin cancer risk. Medscape. August 26, 2022. Accessed June 5, 2026.
- Dogliotti M, Leibowitz M. Granulomatous ochronosis—a cosmetic-induced skin disorder in Blacks. S Afr Med J. 1979;56:757-760.
- Hardwick N, Van Gelder LW, Van der Merwe CA, Van der Merwe MP. Exogenous ochronosis: an epidemiological study. Br J Dermatol. 1989;120:229-238. doi:10.1111/j.1365-2133.1989.tb07787.x
- Lazar M, De La Garza H, Vashi NA. Exogenous ochronosis: characterizing a rare disorder in skin of color. J Clin Med. 2023;12:4341. doi:10.3390/jcm12134341
- Findlay GH, de Beer HA. Chronic hydroquinone poisoning of the skin from skin-lightening cosmetics. A South African epidemic of ochronosis of the face in dark-skinned individuals. S Afr Med J. 1980;57:187-190.
- Bellew SG, Alster TS. Treatment of exogenous ochronosis with a Q-switched alexandrite (755 nm) laser. Dermatol Surg. 2004;30:555-558. doi:10.1111/j.1524-4725.2004.30177.x
- Méndez Baca I, Al-Niaimi F, Colina C, et al. A case of ochronosis successfully treated with the picosecond laser. J Cosmet Dermatol. 2019;18:1322-1325. doi:10.1111/jocd.12834
- Ceglio WW, Careta MF, Patriota R, et al. Exogenous ochronosis successfully treated with the combination of intense pulsed light and fractional CO2 laser. An Bras Dermatol. 2023;98:138-140. doi:10.1016/j.abd.2021.08.013
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Black Malar Papules Following Use of Hydroquinone Cream 2% Purchased Online
Practice Points
- Exogenous ochronosis (EO) is a rare adverse effect of topical hydroquinone characterized by blue-black or gray-blue pigmentation, caviarlike papules, and distinctive banana-shaped dermal deposits on histopathology.
- Most reported cases of hydroquinone-induced EO occur after prolonged use of concentrations exceeding 4%; this case developed after only 6 months of exposure to hydroquinone cream 2% purchased online.
- Available evidence suggests that laser-based therapies may offer greater improvement than topical treatments in affected patients.

Rosacea: We Still Haven’t Found What We’re Looking For
Rosacea: We Still Haven’t Found What We’re Looking For
In May 1987, U2 released “I Still Haven’t Found What I’m Looking For” as a single from their legendary fifth album, The Joshua Tree. The song became their second consecutive #1 hit in the United States to chart on the Billboard Hot 100.1 Here I am, almost 4 decades later, composing an editorial focused on where we are now in dermatology with rosacea. The first thought that came to mind is that U2 was right—and still is—because with rosacea, we still haven’t found what we’re looking for.
In this editorial, I am discussing cutaneous rosacea, not including ocular disease and phymatous changes. The first challenge with cutaneous rosacea is to get the dermatology community on the same page with what the clinical disease state includes, as the individual “dots” that comprise the pathophysiology of rosacea are not similarly connected in each affected patient. This confounds our ability to effectively treat the disease state in many cases, as the clinical manifestations of rosacea are highly variable, reflecting relative contributions from different components of the pathophysiology.2-5
On top of this challenge, the vast majority of US Food and Drug Administration (FDA)–approved therapies for rosacea have been directed at reducing papules and pustules, which are not present in all patients, and their associated perilesional erythema.6,7 We have only had topical alpha agonists as FDA-approved therapies for persistent facial erythema, the superficial vascular component of rosacea that is distinct from the papulopustular component and can intensify during flares with flushing episodes. A major limitation of the alpha-agonist topical approach is the short duration of their effects, which last only hours, and the need for consistent application over time, which can be frustrating for patients. Physical modalities such as lights and lasers offer marked assistance, especially for the superficial vascular component, but may be limited by availability, cost, and differences in expertise. Is the above challenging enough? Keep in mind that I still have not addressed the skin barrier aspects of the disease, symptomatology, and patient education challenges.
I don’t want to sound as if dermatology has been defeated, as we have actually been able to provide marked improvement for many patients with rosacea.6-9 This is especially true in those who present with papules and pustules and also are compliant and patient enough to allow for the integration of the topical and/or physical therapies needed to treat the vascular components including telangiectasias. What has lagged has been the ability to develop a more comprehensive selection of pharmaceutical options, as most have targeted the papulopustular manifestation of the disease. There are many highly effective options in this “papules and pustules of rosacea” space, including topical ivermectin, azelaic acid, and metronidazole, along with the addition of a foam formulation of minocycline, a microencapsulated formulation of benzoyl peroxide, and low-dose oral minocycline. What mostly limits experience with newer FDA-approved therapies is access for patients due to insurance coverage issues and generic substitutions. Overall, the development of newer FDA-approved pharmacologic therapies has become relatively stagnant and remains so at the present time.6-9
So where are we now? Much of the emphasis on rosacea management has transitioned to alternative areas of consideration, including skin care and barrier dysfunction, the role of vitamins and other nutrients, and use of natural compounds.
An algorithm created by a consensus panel of dermatologists has provided foundational measures recommended for use in all patients with rosacea and rosacea-prone skin, including education, behavioral modifications, recognition and avoidance of triggers, avoidance of skin irritants, preventive skin care, and sun photoprotection measures.10 The algorithm emphasizes that assessment of an individual’s facial skin condition and grading of cutaneous rosacea are very important at the first visit and continually thereafter during treatment while the preventive measures continue. Individual dermatology panels have published on skin care nuances suggested for specific patient subgroups such as skin of color and Asian and Latino populations.11-13 While the importance of skin care and skin barrier function in rosacea are well known to the dermatology community, it is essential for clinicians to consistently emphasize this importance to their patients and their staff.
A relatively recent publication has thoroughly addressed the potential roles of vitamins and nutrients in rosacea, discussing both systemic supplementation and topical approaches. A variety of ingredients were evaluated—including vitamin B3, a vitamin A derivative, vitamin C, vitamin D, zinc formulations, and omega-3 fatty acids—demonstrating a range of outcomes.14 There are data that support the potential of vitamins and nutrients as an adjunctive approach; however, at present, this area holds potential for future advancement without any definitive products or well-established recommendations available. More well-designed studies that are targeted for specific rosacea populations are needed.
A large array of natural compounds, primarily botanicals and phytochemicals, have been discussed in the literature for both short- and long-term management of rosacea.15 Many cosmeceutical products are gaining public notoriety, as the concept of “natural” is appealing to the lay population due to the assumption that natural implies greater safety, which is not necessarily true. Semenescu et al15 provided a very comprehensive review of the applicable characteristics of several plant-based agents and potential mechanisms that may be beneficial as adjunctive agents in rosacea. Similar to vitamins and nutrients, there is some scientific basis for the routine integration of natural phytochemicals, but research is needed with well-designed studies used in targeted specific rosacea populations.
Unfortunately, I cannot finish this editorial with ground-breaking news about a new gamechanger approach or product; however, I can tell you that dermatology never gives up. Advances in developing adjunctive therapies and future disease targets such as mast cell activation, microvesicle particles, NLRP3 inflammasome pathway, and Janus kinase inhibition are always in motion, and we continue to try to find what we’re looking for.16
- U2. “I Still Haven’t Found What I’m Looking For.” Wikipedia. Accessed May 17, 2026. https://en.wikipedia.org/wiki/I_Still_Haven%27t_Found_What_I%27m_Looking_For
- Geng RSQ, Bourkas AN, Mufti A, et al. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28:178-189. doi:10.1177/12034754241229365
- Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;16:15:1367994. doi:10.3389/fimmu.2024.1367994
- Andrusiewicz A, Khimuk S, Mijas D, et al. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26:11292. doi:10.3390/ijms262311292
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Del Rosso JQ, Tanghetti E, Webster G, et al. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). Clin Aesthet Dermatol. 2020;13(6 suppl):S17-S24.
- van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22:457-465. doi:10.1007/s40257-021-00595-7
- Tu KY, Jung CJ, Shih YH, et al. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Baldwin H, Alexis A, Andriessen A, et al. Skin barrier deficiency in rosacea: an algorithm integrating OTC skincare products into treatment regimens. Drugs Dermatol. 2022;21:SF3595563-SF35955610. doi:10.36849/JDD.m0922
- Alexis A, Woolery-Lloyd H, Andriessen A, et al. Improving rosacea outcomes in skin of color patients: a review on the nuances in the treatment and the use of cleansers and moisturizers. J Drugs Dermatol. 2022;21:574-580. doi:10.36849/JDD.6838
- Kulthanan K, Andriessen A, Jiang X, et al. A review of the challenges and nuances in treating rosacea in Asian skin types using cleansers and moisturizers as adjuncts. J Drugs Dermatol. 2023;22:45-53. doi:10.36849/JDD.7021
- Gonzalez C, Andriessen A, Antelo D, et al. Treatment and maintenance of cutaneous rosacea in Latino skin types with prescription medications and non-prescription cleansers and moisturizers as adjuncts: a review. J Drugs Dermatol. 2022;21:1111-1118. doi:10.36849/JDD.7010
- Algarin YA, Pulumati A, Jaalouk D, et al. The role of vitamins and nutrients in rosacea. Arch Dermatol Res. 2024;316:142. doi:10.1007/s00403-024-02895-4
- Semenescu J, Similie D, Diaconeasa Z, et al. Recent advances in the management of rosacea through natural compounds. Pharmaceuticals (Basel). 2024;17:212. doi:10.3390/ph17020212
- Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med (Lausanne). 2023;10:1292722. doi:10.3389/fmed.2023.1292722
In May 1987, U2 released “I Still Haven’t Found What I’m Looking For” as a single from their legendary fifth album, The Joshua Tree. The song became their second consecutive #1 hit in the United States to chart on the Billboard Hot 100.1 Here I am, almost 4 decades later, composing an editorial focused on where we are now in dermatology with rosacea. The first thought that came to mind is that U2 was right—and still is—because with rosacea, we still haven’t found what we’re looking for.
In this editorial, I am discussing cutaneous rosacea, not including ocular disease and phymatous changes. The first challenge with cutaneous rosacea is to get the dermatology community on the same page with what the clinical disease state includes, as the individual “dots” that comprise the pathophysiology of rosacea are not similarly connected in each affected patient. This confounds our ability to effectively treat the disease state in many cases, as the clinical manifestations of rosacea are highly variable, reflecting relative contributions from different components of the pathophysiology.2-5
On top of this challenge, the vast majority of US Food and Drug Administration (FDA)–approved therapies for rosacea have been directed at reducing papules and pustules, which are not present in all patients, and their associated perilesional erythema.6,7 We have only had topical alpha agonists as FDA-approved therapies for persistent facial erythema, the superficial vascular component of rosacea that is distinct from the papulopustular component and can intensify during flares with flushing episodes. A major limitation of the alpha-agonist topical approach is the short duration of their effects, which last only hours, and the need for consistent application over time, which can be frustrating for patients. Physical modalities such as lights and lasers offer marked assistance, especially for the superficial vascular component, but may be limited by availability, cost, and differences in expertise. Is the above challenging enough? Keep in mind that I still have not addressed the skin barrier aspects of the disease, symptomatology, and patient education challenges.
I don’t want to sound as if dermatology has been defeated, as we have actually been able to provide marked improvement for many patients with rosacea.6-9 This is especially true in those who present with papules and pustules and also are compliant and patient enough to allow for the integration of the topical and/or physical therapies needed to treat the vascular components including telangiectasias. What has lagged has been the ability to develop a more comprehensive selection of pharmaceutical options, as most have targeted the papulopustular manifestation of the disease. There are many highly effective options in this “papules and pustules of rosacea” space, including topical ivermectin, azelaic acid, and metronidazole, along with the addition of a foam formulation of minocycline, a microencapsulated formulation of benzoyl peroxide, and low-dose oral minocycline. What mostly limits experience with newer FDA-approved therapies is access for patients due to insurance coverage issues and generic substitutions. Overall, the development of newer FDA-approved pharmacologic therapies has become relatively stagnant and remains so at the present time.6-9
So where are we now? Much of the emphasis on rosacea management has transitioned to alternative areas of consideration, including skin care and barrier dysfunction, the role of vitamins and other nutrients, and use of natural compounds.
An algorithm created by a consensus panel of dermatologists has provided foundational measures recommended for use in all patients with rosacea and rosacea-prone skin, including education, behavioral modifications, recognition and avoidance of triggers, avoidance of skin irritants, preventive skin care, and sun photoprotection measures.10 The algorithm emphasizes that assessment of an individual’s facial skin condition and grading of cutaneous rosacea are very important at the first visit and continually thereafter during treatment while the preventive measures continue. Individual dermatology panels have published on skin care nuances suggested for specific patient subgroups such as skin of color and Asian and Latino populations.11-13 While the importance of skin care and skin barrier function in rosacea are well known to the dermatology community, it is essential for clinicians to consistently emphasize this importance to their patients and their staff.
A relatively recent publication has thoroughly addressed the potential roles of vitamins and nutrients in rosacea, discussing both systemic supplementation and topical approaches. A variety of ingredients were evaluated—including vitamin B3, a vitamin A derivative, vitamin C, vitamin D, zinc formulations, and omega-3 fatty acids—demonstrating a range of outcomes.14 There are data that support the potential of vitamins and nutrients as an adjunctive approach; however, at present, this area holds potential for future advancement without any definitive products or well-established recommendations available. More well-designed studies that are targeted for specific rosacea populations are needed.
A large array of natural compounds, primarily botanicals and phytochemicals, have been discussed in the literature for both short- and long-term management of rosacea.15 Many cosmeceutical products are gaining public notoriety, as the concept of “natural” is appealing to the lay population due to the assumption that natural implies greater safety, which is not necessarily true. Semenescu et al15 provided a very comprehensive review of the applicable characteristics of several plant-based agents and potential mechanisms that may be beneficial as adjunctive agents in rosacea. Similar to vitamins and nutrients, there is some scientific basis for the routine integration of natural phytochemicals, but research is needed with well-designed studies used in targeted specific rosacea populations.
Unfortunately, I cannot finish this editorial with ground-breaking news about a new gamechanger approach or product; however, I can tell you that dermatology never gives up. Advances in developing adjunctive therapies and future disease targets such as mast cell activation, microvesicle particles, NLRP3 inflammasome pathway, and Janus kinase inhibition are always in motion, and we continue to try to find what we’re looking for.16
In May 1987, U2 released “I Still Haven’t Found What I’m Looking For” as a single from their legendary fifth album, The Joshua Tree. The song became their second consecutive #1 hit in the United States to chart on the Billboard Hot 100.1 Here I am, almost 4 decades later, composing an editorial focused on where we are now in dermatology with rosacea. The first thought that came to mind is that U2 was right—and still is—because with rosacea, we still haven’t found what we’re looking for.
In this editorial, I am discussing cutaneous rosacea, not including ocular disease and phymatous changes. The first challenge with cutaneous rosacea is to get the dermatology community on the same page with what the clinical disease state includes, as the individual “dots” that comprise the pathophysiology of rosacea are not similarly connected in each affected patient. This confounds our ability to effectively treat the disease state in many cases, as the clinical manifestations of rosacea are highly variable, reflecting relative contributions from different components of the pathophysiology.2-5
On top of this challenge, the vast majority of US Food and Drug Administration (FDA)–approved therapies for rosacea have been directed at reducing papules and pustules, which are not present in all patients, and their associated perilesional erythema.6,7 We have only had topical alpha agonists as FDA-approved therapies for persistent facial erythema, the superficial vascular component of rosacea that is distinct from the papulopustular component and can intensify during flares with flushing episodes. A major limitation of the alpha-agonist topical approach is the short duration of their effects, which last only hours, and the need for consistent application over time, which can be frustrating for patients. Physical modalities such as lights and lasers offer marked assistance, especially for the superficial vascular component, but may be limited by availability, cost, and differences in expertise. Is the above challenging enough? Keep in mind that I still have not addressed the skin barrier aspects of the disease, symptomatology, and patient education challenges.
I don’t want to sound as if dermatology has been defeated, as we have actually been able to provide marked improvement for many patients with rosacea.6-9 This is especially true in those who present with papules and pustules and also are compliant and patient enough to allow for the integration of the topical and/or physical therapies needed to treat the vascular components including telangiectasias. What has lagged has been the ability to develop a more comprehensive selection of pharmaceutical options, as most have targeted the papulopustular manifestation of the disease. There are many highly effective options in this “papules and pustules of rosacea” space, including topical ivermectin, azelaic acid, and metronidazole, along with the addition of a foam formulation of minocycline, a microencapsulated formulation of benzoyl peroxide, and low-dose oral minocycline. What mostly limits experience with newer FDA-approved therapies is access for patients due to insurance coverage issues and generic substitutions. Overall, the development of newer FDA-approved pharmacologic therapies has become relatively stagnant and remains so at the present time.6-9
So where are we now? Much of the emphasis on rosacea management has transitioned to alternative areas of consideration, including skin care and barrier dysfunction, the role of vitamins and other nutrients, and use of natural compounds.
An algorithm created by a consensus panel of dermatologists has provided foundational measures recommended for use in all patients with rosacea and rosacea-prone skin, including education, behavioral modifications, recognition and avoidance of triggers, avoidance of skin irritants, preventive skin care, and sun photoprotection measures.10 The algorithm emphasizes that assessment of an individual’s facial skin condition and grading of cutaneous rosacea are very important at the first visit and continually thereafter during treatment while the preventive measures continue. Individual dermatology panels have published on skin care nuances suggested for specific patient subgroups such as skin of color and Asian and Latino populations.11-13 While the importance of skin care and skin barrier function in rosacea are well known to the dermatology community, it is essential for clinicians to consistently emphasize this importance to their patients and their staff.
A relatively recent publication has thoroughly addressed the potential roles of vitamins and nutrients in rosacea, discussing both systemic supplementation and topical approaches. A variety of ingredients were evaluated—including vitamin B3, a vitamin A derivative, vitamin C, vitamin D, zinc formulations, and omega-3 fatty acids—demonstrating a range of outcomes.14 There are data that support the potential of vitamins and nutrients as an adjunctive approach; however, at present, this area holds potential for future advancement without any definitive products or well-established recommendations available. More well-designed studies that are targeted for specific rosacea populations are needed.
A large array of natural compounds, primarily botanicals and phytochemicals, have been discussed in the literature for both short- and long-term management of rosacea.15 Many cosmeceutical products are gaining public notoriety, as the concept of “natural” is appealing to the lay population due to the assumption that natural implies greater safety, which is not necessarily true. Semenescu et al15 provided a very comprehensive review of the applicable characteristics of several plant-based agents and potential mechanisms that may be beneficial as adjunctive agents in rosacea. Similar to vitamins and nutrients, there is some scientific basis for the routine integration of natural phytochemicals, but research is needed with well-designed studies used in targeted specific rosacea populations.
Unfortunately, I cannot finish this editorial with ground-breaking news about a new gamechanger approach or product; however, I can tell you that dermatology never gives up. Advances in developing adjunctive therapies and future disease targets such as mast cell activation, microvesicle particles, NLRP3 inflammasome pathway, and Janus kinase inhibition are always in motion, and we continue to try to find what we’re looking for.16
- U2. “I Still Haven’t Found What I’m Looking For.” Wikipedia. Accessed May 17, 2026. https://en.wikipedia.org/wiki/I_Still_Haven%27t_Found_What_I%27m_Looking_For
- Geng RSQ, Bourkas AN, Mufti A, et al. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28:178-189. doi:10.1177/12034754241229365
- Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;16:15:1367994. doi:10.3389/fimmu.2024.1367994
- Andrusiewicz A, Khimuk S, Mijas D, et al. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26:11292. doi:10.3390/ijms262311292
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Del Rosso JQ, Tanghetti E, Webster G, et al. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). Clin Aesthet Dermatol. 2020;13(6 suppl):S17-S24.
- van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22:457-465. doi:10.1007/s40257-021-00595-7
- Tu KY, Jung CJ, Shih YH, et al. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Baldwin H, Alexis A, Andriessen A, et al. Skin barrier deficiency in rosacea: an algorithm integrating OTC skincare products into treatment regimens. Drugs Dermatol. 2022;21:SF3595563-SF35955610. doi:10.36849/JDD.m0922
- Alexis A, Woolery-Lloyd H, Andriessen A, et al. Improving rosacea outcomes in skin of color patients: a review on the nuances in the treatment and the use of cleansers and moisturizers. J Drugs Dermatol. 2022;21:574-580. doi:10.36849/JDD.6838
- Kulthanan K, Andriessen A, Jiang X, et al. A review of the challenges and nuances in treating rosacea in Asian skin types using cleansers and moisturizers as adjuncts. J Drugs Dermatol. 2023;22:45-53. doi:10.36849/JDD.7021
- Gonzalez C, Andriessen A, Antelo D, et al. Treatment and maintenance of cutaneous rosacea in Latino skin types with prescription medications and non-prescription cleansers and moisturizers as adjuncts: a review. J Drugs Dermatol. 2022;21:1111-1118. doi:10.36849/JDD.7010
- Algarin YA, Pulumati A, Jaalouk D, et al. The role of vitamins and nutrients in rosacea. Arch Dermatol Res. 2024;316:142. doi:10.1007/s00403-024-02895-4
- Semenescu J, Similie D, Diaconeasa Z, et al. Recent advances in the management of rosacea through natural compounds. Pharmaceuticals (Basel). 2024;17:212. doi:10.3390/ph17020212
- Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med (Lausanne). 2023;10:1292722. doi:10.3389/fmed.2023.1292722
- U2. “I Still Haven’t Found What I’m Looking For.” Wikipedia. Accessed May 17, 2026. https://en.wikipedia.org/wiki/I_Still_Haven%27t_Found_What_I%27m_Looking_For
- Geng RSQ, Bourkas AN, Mufti A, et al. Rosacea: pathogenesis and therapeutic correlates. J Cutan Med Surg. 2024;28:178-189. doi:10.1177/12034754241229365
- Yang F, Wang L, Song D, et al. Signaling pathways and targeted therapy for rosacea. Front Immunol. 2024;16:15:1367994. doi:10.3389/fimmu.2024.1367994
- Andrusiewicz A, Khimuk S, Mijas D, et al. Molecular mechanisms in the etiopathology of rosacea-systematic review. Int J Mol Sci. 2025;26:11292. doi:10.3390/ijms262311292
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Del Rosso JQ, Tanghetti E, Webster G, et al. Update on the management of rosacea from the American Acne & Rosacea Society (AARS). Clin Aesthet Dermatol. 2020;13(6 suppl):S17-S24.
- van Zuuren EJ, Arents BWM, van der Linden MMD, et al. Rosacea: new concepts in classification and treatment. Am J Clin Dermatol. 2021;22:457-465. doi:10.1007/s40257-021-00595-7
- Tu KY, Jung CJ, Shih YH, et al. Therapeutic strategies focusing on immune dysregulation and neuroinflammation in rosacea. Front Immunol. 2024;15:1403798. doi:10.3389/fimmu.2024.1403798
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global ROSacea COnsensus 2019 panel. Br J Dermatol. 2020;182:1269-1276. doi:10.1111/bjd.18420
- Baldwin H, Alexis A, Andriessen A, et al. Skin barrier deficiency in rosacea: an algorithm integrating OTC skincare products into treatment regimens. Drugs Dermatol. 2022;21:SF3595563-SF35955610. doi:10.36849/JDD.m0922
- Alexis A, Woolery-Lloyd H, Andriessen A, et al. Improving rosacea outcomes in skin of color patients: a review on the nuances in the treatment and the use of cleansers and moisturizers. J Drugs Dermatol. 2022;21:574-580. doi:10.36849/JDD.6838
- Kulthanan K, Andriessen A, Jiang X, et al. A review of the challenges and nuances in treating rosacea in Asian skin types using cleansers and moisturizers as adjuncts. J Drugs Dermatol. 2023;22:45-53. doi:10.36849/JDD.7021
- Gonzalez C, Andriessen A, Antelo D, et al. Treatment and maintenance of cutaneous rosacea in Latino skin types with prescription medications and non-prescription cleansers and moisturizers as adjuncts: a review. J Drugs Dermatol. 2022;21:1111-1118. doi:10.36849/JDD.7010
- Algarin YA, Pulumati A, Jaalouk D, et al. The role of vitamins and nutrients in rosacea. Arch Dermatol Res. 2024;316:142. doi:10.1007/s00403-024-02895-4
- Semenescu J, Similie D, Diaconeasa Z, et al. Recent advances in the management of rosacea through natural compounds. Pharmaceuticals (Basel). 2024;17:212. doi:10.3390/ph17020212
- Fisher GW, Travers JB, Rohan CA. Rosacea pathogenesis and therapeutics: current treatments and a look at future targets. Front Med (Lausanne). 2023;10:1292722. doi:10.3389/fmed.2023.1292722
Rosacea: We Still Haven’t Found What We’re Looking For
Rosacea: We Still Haven’t Found What We’re Looking For
