User login
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians
T he US Census Bureau projects that the number of older adults (aged ≥ 65 years) will exceed 49 million by 2030, and an estimated 20% (nearly 10 million) of this population will experience cognitive or mental health disorders.1,2 The mental health workforce is not equipped to address the specialized mental health care needs of many older adults.2,3 For example, geriatric psychiatrists specialize in the diagnosis and treatment of mental illness and cognitive disorders in the later stages of life, but their numbers are few and declining. Only 33.5% of geriatric psychiatry fellowship training slots were filled from 2017 to 2021, and only 62 fellows trained during the 2021-2022 academic year.4 Board-certified geriatric psychiatrists also tend to be concentrated in larger, urban, academically-affiliated medical centers, often leaving rural areas and smaller facilities without access, including facilities in the Veterans Health Administration (VHA).5
The VHA has been optimizing access to specialty geriatric mental health services via regional and national virtual consultation services. Seven of 19 Veterans Integrated Service Network (VISN) Clinical Resource Hubs (CRHs) have geriatric mental health teams.6 These provide interdisciplinary geriatric mental telehealth services, including geriatric psychiatry, for older veterans with complex care needs.7,8 Likewise, the VHA National Expert Consultation & Specialized Services-Mental Health (NEXCSS- MH, formerly known as the National Telemental Health Center) sponsors video teleconsultations with board-certified geriatric psychiatrists and an Ask the Expert email consultation program.
This article describes the Ask the Expert Geriatric Psychiatry email program (one of several similar programs at NEXCSS-MH), building upon a symposium presented at the American Association for Geriatric Psychiatry (AAGP) annual meeting in March 2022.9 The program was initiated in June 2021 as a result of discussions between the National Mental Health Director, Geriatric Mental Health in the VHA Office of Mental Health and Suicide Prevention (now known as the Office of Mental Health [OMH]), and National Telemental Health Center leadership. VHA board certified geriatric psychiatrists were recruited to serve as expert consultants and respond to email questions submitted by VHA clinicians regarding the psychiatric care of older adult veterans. The results of this program identify educational needs among clinical staff and may inform the development of program materials for a range of clinicians.
Program Description
The national geriatric mental health director recruited prospective experts and met with each to assess interest and qualifications, consulting with OMH psychiatrist leaders before making selections. Five experts were initially selected; 1 later stepped down and was replaced by another, who also stepped down. The experts were board certified in psychiatry and geriatric psychiatry and held a variety of local and national leadership positions, including geriatric psychiatry fellowship director, US Department of Veterans Affairs (VA) research and clinical leader, and various roles in the AAGP; some had received teaching awards.
Operations
The national geriatric mental health director announced the program in June 2021 to VHA mental health and geriatric program email groups with reminders sent every few months. The announcement included information about the types of questions appropriate to submit, including examples of general clinical management questions that did not share patient-specific protected health information, and clarified that experts would not be conducting chart reviews because the time required for detailed chart reviews was not feasible for volunteer experts to integrate into their otherwise full-time jobs at their respective VA medical centers. The announcement also included brief biographies of the experts.
The Figure describes the daily operations of the Ask the Expert Geriatric Psychiatry email consultation program. The NEXCSS- MH developed a Microsoft Outlook mailbox and group email address where clinicians from across the VHA could submit questions. The experts, as well as the national geriatric mental health director and NEXCSS-MH staff, had access to this mailbox to track and/or respond to questions. One expert volunteered to be the program’s primary mailbox coordinator. The coordinator checked the inbox daily and assigned each question to one of the experts on a rotating basis using the color-coding feature in Outlook. The other experts were advised to check the email account at least once weekly and reply to any assigned questions.
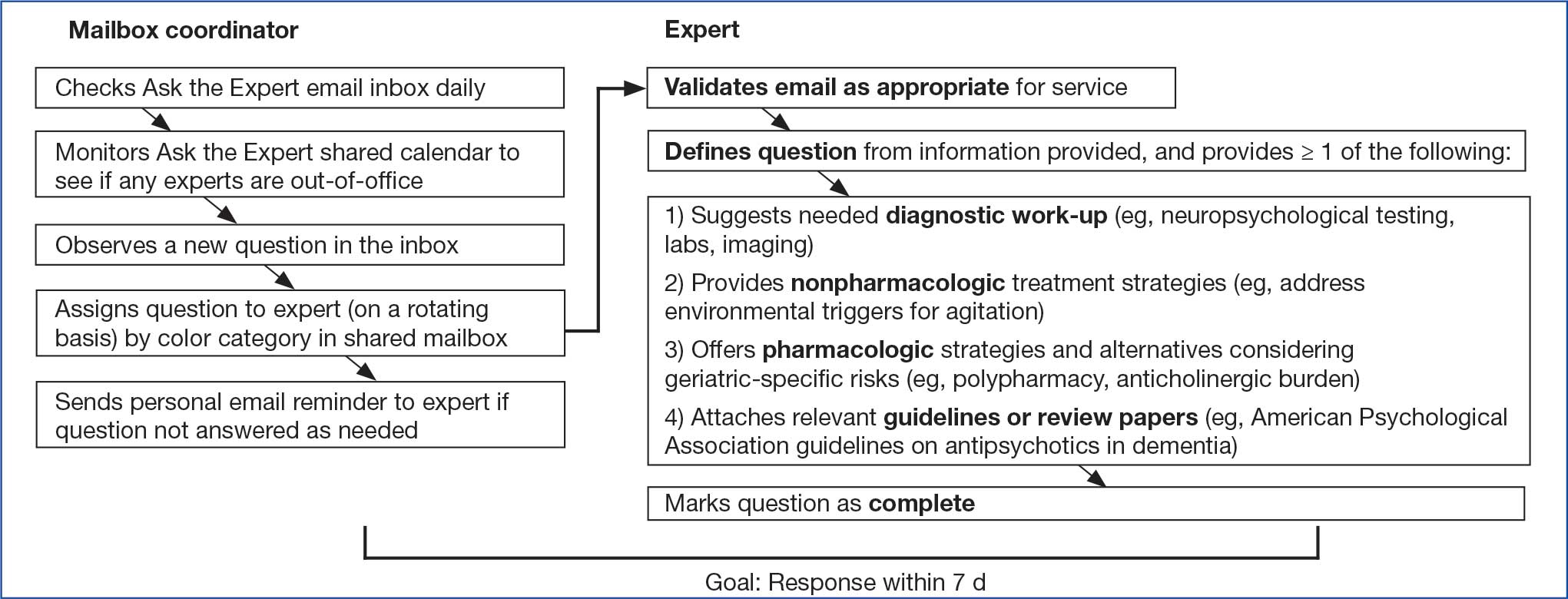
Responding to a question entailed first determining whether the question was appropriate for the service. For example, if a question requested a chart review, the expert replied that experts could not provide chart reviews and requested that the question be reframed. Next, the expert often needed to define a specific clinical question from the information provided, as email questions often touched upon several topics. The expert provided personalized advice on diagnostic testing, nonpharmacologic treatment strategies, and/or pharmacologic treatment options. Experts also often attached relevant guidelines or review articles. The goal was to provide a response within 7 business days.
All email responses included a disclaimer indicating that the program was not intended for urgent or immediate medical advice and that the information provided was for VHA clinician education purposes only. The disclaimer explained that email communication did not establish a doctor-patient relationship between the expert and a specific veteran and that, if desired, a request for a clinical consultation could be submitted on a specific case (ie, a video teleconsultation).
Methods for Reviewing Questions
Descriptive statistics, including frequencies, means, and minimum and maximum ranges, were used to capture the number of questions the program received, type of requester, and length of time prior to response for emailed questions.9 Conventional content analysis procedures were used between January and October 2024 to analyze clinicians’ questions.10 Four subject matter experts (3 geriatric psychiatrists and 1 geropsychologist) served as coders, assigned in groups of 2 to review questions. Each coder independently reviewed assigned questions and identified preliminary themes. Themes were reviewed and revised using an iterative process during regular team meetings with coders to clarify and confirm interpretations. Discrepancies were discussed within team meetings to achieve consensus.
Questions received. Between February 2022 and December 2023, the program received 101 email questions. Requesters included 39 physicians, 17 nurse practitioners or physician assistants, 15 social workers, 14 psychologists, 9 nurses, 5 pharmacists, 1 dietitian, and 1 who was undetermined. Experts responded to the questions an average of 6 days after receipt (range, < 1-19); 73 responses (72%) met the 7-day goal.
Iterative changes to coded themes were made during group discussions. Multiple clinical questions were often posed within the same email. Initially, some coders identified themes solely based on reported symptoms; others identified themes based on reported and/or potential diagnostic conditions attributed to the symptom(s) described within the email. For example, some coders selected a primary theme of behavioral and psychological symptoms of dementia (BPSD) only if a behavior contributing to distress in the veteran or others was described, while others selected this theme when any psychiatric symptom (eg, psychosis) was present in the context of dementia. The group identified 1 primary theme per question based on the main clinical symptom or main concern presented. Co-occurring diagnostic conditions highlighted in the email requests were included as secondary themes, and each question could have > 1 secondary theme.
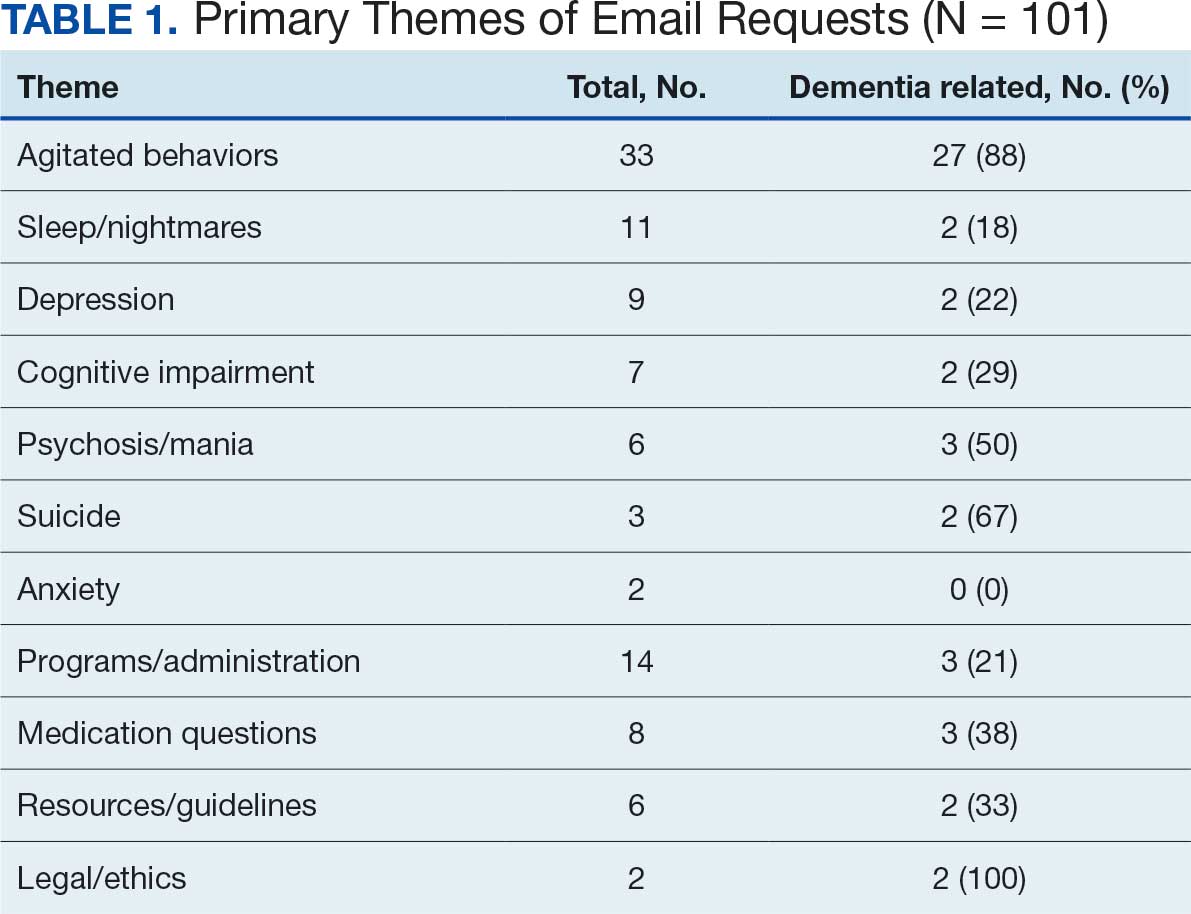
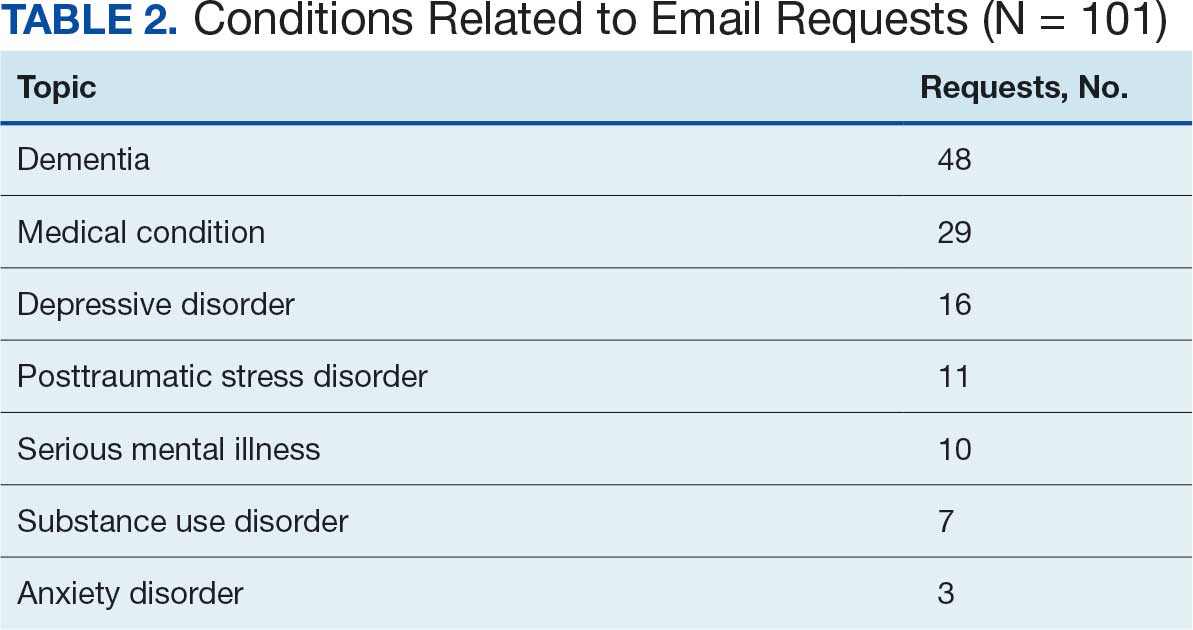
The most frequent requests related to clinical symptoms included questions about agitated behaviors, sleep and/or nightmares, and depression symptoms (Table 1). Twenty-seven of 33 email requests on agitated behaviors were related to a dementia diagnosis, as were several questions about sleep/nightmares, depression, psychosis/mania, and anxiety. Many diagnostic conditions were described in the email requests (Table 2). The most frequent condition was dementia, followed by a medical condition, depressive disorder, posttraumatic stress disorder, and/or serious mental illness.
Request for Feedback. In February 2022, an email request was sent to the 64 clinicians who asked email questions from the start of the program in June 2021 through December 2021. A second request included 11 clinicians who asked questions from January through February 2022. These requests were sent as part of preparations for the symposium on the program presented at the AAGP annual meeting in March 2022.9 In May 2024, feedback was requested from 37 clinicians who submitted questions from May 1, 2023, through May 15, 2024.
Requests for feedback included 6 closed-ended and 1 open-ended question: (1) Did the answer you received help inform clinical practice? (2) Did you receive a timely response? (3) What type of information was useful to you in addressing your question (ie, direct/specific answer to a clinical scenario, guidelines, articles, VA resources)? (4) Do you have access to a geriatric psychiatrist at your facility? (5) Are you likely to use Ask the Expert Geriatric Psychiatry in the future? (6) Would you use a geriatric psychiatry teleconsultation service? (7) Share suggestions for improvement. Frequencies of response selection were obtained for each question. Text responses to the open-ended question asking for suggestions for improvement were reviewed and summarized.
Responses
Thirty users responded to the feedback request (27% response rate). Respondents considered the answers received extremely (n = 14; 47%) or very much (n = 12; 40%) helpful for their clinical practice. Twenty-three respondents (77%) felt an answer was provided promptly, 7 respondents (23%) felt the answer was not timely but still useful, and none felt that the answer was too late. Respondents reported that the most useful type of information in addressing their questions was a direct/specific answer to a clinical scenario (n = 27; 90%), followed by guidelines (n = 12; 40%), articles (n = 7; 23%), and VA resources (n = 4; 13%).
Sixteen respondents (53%) reported that they rarely had ready access to a geriatric psychiatrist at their facility, 3 (10%) had access sometimes, 4 (14%) had access usually, 3 (10%) had access regularly, and 3 (10%) never had access. Twenty-seven respondents (90%) indicated they would be very likely to use the service again. If geriatric psychiatry teleconsultation and/or e-consultation were offered, many respondents indicated they would be extremely (n = 10; 33%) or very (n = 12; 40%) likely to use teleconsultation and/or e-consultation.
Suggestions for improvement included supporting experts to perform chart reviews for email questions, developing a template or consult form, holding a biweekly drop-in meeting to present questions to and discuss cases with a panel of experts, and providing further help addressing complex decisional capacity issues, delirium, and care or placement for veterans with severe behavioral issues in a rural setting.
Discussion
Although many older adults experience cognitive and mental health disorders that may benefit from management by a geriatric psychiatrist, the number of trained geriatric psychiatrists available is insufficient to allow for direct care for each patient. The Ask the Expert Geriatric Psychiatry email consultation program is one aspect of a multicomponent strategy within the VHA to increase access to specialty geriatric mental health services for veterans. A key advantage of the program is that it is not resource intensive. Experts can participate voluntarily, providing timely feedback to clinicians around the country while continuing other duties at their respective VA medical centers. Email replies to the experts’ answers elicited positive feedback on the program, include: “I found this service to be extremely helpful and I have shared the information they sent me with several other coworkers!”, “It was great!”, and “I endorsed the service to our VISN Rehabilitation and Extended Care group.”
The coding of primary and secondary themes from 101 email questions that were retained revealed the range and relative frequencies of clinical and administrative topics with which clinicians needed help. The most common (33%) theme was agitated behaviors. Nearly half of the questions (48%) were related to underlying dementia, and 29% were related to a patient’s medical comorbidities. These findings suggest that the expertise of a geriatric psychiatrist is particularly relevant when caring for older patients experiencing BPSD or patients with complex, overlapping psychiatric and medical conditions.
Despite a 27% response rate, participant feedback has been helpful. The program reached its intended audience of clinicians in rural areas and at smaller facilities with 53% of requesters reporting they rarely had access to a geriatric psychiatrist. Suggestions for improvement indicated that some clinicians desired additional support, including chart reviews, meetings with experts, and a video teleconsultation service (available through NEXCSS-MH).
Many clinicians without training in specialty geriatric mental health may require help with complex clinical presentations. For example, 39 clinicians who submitted questions to the program were physicians. Accreditation Council for Graduate Medical Education program requirements for general psychiatry residency include 4 weeks of geriatric psychiatry.11 The findings of this study suggest that this level of training may not be adequate to independently care for every patient who experiences dementia or multimorbidity. Several training and mentoring initiatives have been developed to address the professional development need for psychiatrists.12-14
The need for geriatric workforce development is significant across health care, including other mental health professions.15,16 The VHA Geriatric Scholars program trains rural primary care practitioners, psychologists, and psychiatrists.17,18 Likewise, consultative geriatric specialty support for primary care practitioners in rural areas is provided via the Geriatric Research Education and Clinical Center Connect program.19 The Ask the Expert Geriatric Psychiatry email program is an additional economical model to support clinician educational development and provide rapid educational responses to inform patient care.
Ask the Expert received fewer email questions than anticipated. Enhanced optimization may require more frequent and widespread announcements about the program. Clinical staff may not be aware of the program due to an overload of email communications. Likewise, it may be challenging for busy clinicians to take the time to seek consultation or recognize a potential gap in their knowledge or skills. Had more questions been submitted, the 5 volunteer experts may have had more difficulty addressing the demand. Feedback from this project may inform development of a frequently asked questions document to share with VHA teams and a drop-in office hour to pose clinical questions of geriatric psychiatry experts, as recommended by a clinician who participated in the program.
Limitations
Not all requesters were sent a request for feedback, and the response rate for the request for feedback was only 27%. As the program has evolved, it began sending a request for feedback immediately after answering each question, which may increase the odds of response. The goal of experts answering questions within 7 business days was met 72% of the time, likely an artifact of experts integrating question answering with many other duties. The mailbox coordinator has since provided email prompts to experts immediately upon being assigned a question with the goal of improving timeliness. The program did not include chart reviews or patient consultations, as neither was feasible for volunteer experts. The email consultation service is a single component of virtual consultative specialty geriatric mental health services within the VHA, including video consultations via NEXCSS-MH and regional geriatric mental health teams.
Conclusions
The need for specialty geriatric mental health services is increasing in the VHA and across the US. However, there are too few board-certified geriatric psychiatrists to provide direct patient care to all older adults with cognitive and mental health disorders. The VHA has leveraged telehealth to improve access to geriatric mental health care. The VHA Ask the Expert Geriatric Psychiatry email consultation program is a low-resource service which provides rapid feedback to clinicians nationwide on challenging clinical scenarios, many of which are dementia-related. Most users of the service who responded to requests for feedback reported that answers to their questions were helpful and timely. The email consultation program should continue to be supplemented by more comprehensive geriatric telemental health services for particularly complex cases to meet the needs of older veterans.
- 2023 population projections for the nation by age, sex, race, Hispanic origin and nativity. United States Census Bureau. November 9, 2023. Accessed December 11, 2025. https://www.census.gov/newsroom/press-kits/2023/population-projections.html
- National Academies of Sciences Engineering and Medicine. Addressing the rising mental health needs of an aging population: proceedings of a workshop. 2024. Accessed December 11, 2025. doi.org:10.17226/27340
- Institute of Medicine. The mental health and substance use workforce for older adults: in whose hands? The National Academies Press; 2012. Accessed December 11, 2025. doi:10.17226/13400
- American Psychiatric Association. 2022 resident/fellow census. November 2023. Accessed December 11, 2025. https://www.psychiatry.org/getmedia/d80438af-f760-40f3-9d33-f91309b09564/APA-Resident-Census-2022.pdf
- Juul D, Colenda CC, Lyness JM, et al. Subspecialty training and certification in geriatric psychiatry: a 25-year overview. Am J Geriatr Psychiatry. 2017;25:445-453. doi:10.1016/j.jagp.2016.12.018
- Jaske E, Wheat CL, Rubenstein LV, et al. Understanding how contingency staffing programs can support mental health services in the Veterans Health Administration. Telemed J E Health. 2024;30:1857-1865. doi:10.1089/tmj.2023.0573
- Gould CE, Carlson C, Alfaro AJ, et al. Supporting veterans, caregivers, and providers in rural regions with tele-geriatric psychiatry consultation: a mixed methods pilot study. Am J Geriatr Psychiatry. 2023;31:279-290. doi:10.1016/j.jagp.2023.01.005
- Gould CE, Paiko L, Carlson C, et al. Implementation of tele-geriatricmental healthcare for rural veterans: factors influencing care models. Front Health Serv. 2024;4:1221899. doi:10.3389/frhs.2024.1221899
- Padala P, Schultz S, Khatkhate G, et al. Ask the expert geriatric psychiatry: VA program to support clinicians. Am J Geriatr Psychiatry. 2022;30:S18. doi:10.1016/j.jagp.2022.01.279
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288. doi:10.1177/1049732305276687
- Accreditation Council for Graduate Medical Education. Program requirements for graduate medical education in psychiatry. Revised September 3, 2025. Accessed December 11, 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/400_psychiatry_2025_reformatted.pdf
- Fernandez J, Agarwal KS, Amspoker AB, et al. Outcomes from an interprofessional, dementia-focused, telementoring program: a brief report. Gerontol Geriatr Educ. 2024;45:601-606. doi:10.1080/02701960.2023.2253175
- Conroy ML, Garcia-Pittman EC, van Dyck LI, et al. The COVID-19 American Association for Geriatric Psychiatry (AAGP) online trainee curriculum: program evaluation and future directions. Am J Geriatr Psychiatry. 2025;33:308-314. doi:10.1016/j.jagp.2024.10.010
- Conroy ML, Garcia-Pittman EC, Ali H, et al. The COVID-19 AAGP online trainee curriculum: development and method of initial evaluation. Am J Geriatr Psychiatry. 2020;28:1004-1008. doi:10.1016/j.jagp.2020.06.003
- Flaherty E, Busby-Whitehead J, Potter J, et al. The geriatric workforce enhancement program: review of the coordinating center and examples of the GWEP in practice. Am J Geriatr Psychiatry. 2019;27:675-686. doi:10.1016/j.jagp.2019.04.010
- Hoge MA, Karel MJ, Zeiss AM, et al. Strengthening psychology’s workforce for older adults: implications of the Institute of Medicine’s report to Congress. Am Psychol. 2015;70:265-278. doi:10.1037/a0038927
- Kramer BJ, Creekmur B, Howe JL, et al. Veterans Affairs geriatric scholars program: enhancing existing primary care clinician skills in caring for older veterans. J Am Geriatr Soc. 2016;64:2343-2348. doi:10.1111/jgs.14382
- Gould CE, Rodriguez RL, Gregg JJ, et al. Preparing Veterans Health Administration psychologists to meet the complex needs of aging veterans. Fed Pract. 2024;41:S10-S15. doi:10.12788/fp.0466
- Pimentel CB, Gately M, Barczi SR, et al. GRECC Connect: Geriatrics telehealth to empower health care providers and improve management of older veterans in rural communities. Fed Pract. 2019;36:464-470.
T he US Census Bureau projects that the number of older adults (aged ≥ 65 years) will exceed 49 million by 2030, and an estimated 20% (nearly 10 million) of this population will experience cognitive or mental health disorders.1,2 The mental health workforce is not equipped to address the specialized mental health care needs of many older adults.2,3 For example, geriatric psychiatrists specialize in the diagnosis and treatment of mental illness and cognitive disorders in the later stages of life, but their numbers are few and declining. Only 33.5% of geriatric psychiatry fellowship training slots were filled from 2017 to 2021, and only 62 fellows trained during the 2021-2022 academic year.4 Board-certified geriatric psychiatrists also tend to be concentrated in larger, urban, academically-affiliated medical centers, often leaving rural areas and smaller facilities without access, including facilities in the Veterans Health Administration (VHA).5
The VHA has been optimizing access to specialty geriatric mental health services via regional and national virtual consultation services. Seven of 19 Veterans Integrated Service Network (VISN) Clinical Resource Hubs (CRHs) have geriatric mental health teams.6 These provide interdisciplinary geriatric mental telehealth services, including geriatric psychiatry, for older veterans with complex care needs.7,8 Likewise, the VHA National Expert Consultation & Specialized Services-Mental Health (NEXCSS- MH, formerly known as the National Telemental Health Center) sponsors video teleconsultations with board-certified geriatric psychiatrists and an Ask the Expert email consultation program.
This article describes the Ask the Expert Geriatric Psychiatry email program (one of several similar programs at NEXCSS-MH), building upon a symposium presented at the American Association for Geriatric Psychiatry (AAGP) annual meeting in March 2022.9 The program was initiated in June 2021 as a result of discussions between the National Mental Health Director, Geriatric Mental Health in the VHA Office of Mental Health and Suicide Prevention (now known as the Office of Mental Health [OMH]), and National Telemental Health Center leadership. VHA board certified geriatric psychiatrists were recruited to serve as expert consultants and respond to email questions submitted by VHA clinicians regarding the psychiatric care of older adult veterans. The results of this program identify educational needs among clinical staff and may inform the development of program materials for a range of clinicians.
Program Description
The national geriatric mental health director recruited prospective experts and met with each to assess interest and qualifications, consulting with OMH psychiatrist leaders before making selections. Five experts were initially selected; 1 later stepped down and was replaced by another, who also stepped down. The experts were board certified in psychiatry and geriatric psychiatry and held a variety of local and national leadership positions, including geriatric psychiatry fellowship director, US Department of Veterans Affairs (VA) research and clinical leader, and various roles in the AAGP; some had received teaching awards.
Operations
The national geriatric mental health director announced the program in June 2021 to VHA mental health and geriatric program email groups with reminders sent every few months. The announcement included information about the types of questions appropriate to submit, including examples of general clinical management questions that did not share patient-specific protected health information, and clarified that experts would not be conducting chart reviews because the time required for detailed chart reviews was not feasible for volunteer experts to integrate into their otherwise full-time jobs at their respective VA medical centers. The announcement also included brief biographies of the experts.
The Figure describes the daily operations of the Ask the Expert Geriatric Psychiatry email consultation program. The NEXCSS- MH developed a Microsoft Outlook mailbox and group email address where clinicians from across the VHA could submit questions. The experts, as well as the national geriatric mental health director and NEXCSS-MH staff, had access to this mailbox to track and/or respond to questions. One expert volunteered to be the program’s primary mailbox coordinator. The coordinator checked the inbox daily and assigned each question to one of the experts on a rotating basis using the color-coding feature in Outlook. The other experts were advised to check the email account at least once weekly and reply to any assigned questions.
Responding to a question entailed first determining whether the question was appropriate for the service. For example, if a question requested a chart review, the expert replied that experts could not provide chart reviews and requested that the question be reframed. Next, the expert often needed to define a specific clinical question from the information provided, as email questions often touched upon several topics. The expert provided personalized advice on diagnostic testing, nonpharmacologic treatment strategies, and/or pharmacologic treatment options. Experts also often attached relevant guidelines or review articles. The goal was to provide a response within 7 business days.
All email responses included a disclaimer indicating that the program was not intended for urgent or immediate medical advice and that the information provided was for VHA clinician education purposes only. The disclaimer explained that email communication did not establish a doctor-patient relationship between the expert and a specific veteran and that, if desired, a request for a clinical consultation could be submitted on a specific case (ie, a video teleconsultation).
Methods for Reviewing Questions
Descriptive statistics, including frequencies, means, and minimum and maximum ranges, were used to capture the number of questions the program received, type of requester, and length of time prior to response for emailed questions.9 Conventional content analysis procedures were used between January and October 2024 to analyze clinicians’ questions.10 Four subject matter experts (3 geriatric psychiatrists and 1 geropsychologist) served as coders, assigned in groups of 2 to review questions. Each coder independently reviewed assigned questions and identified preliminary themes. Themes were reviewed and revised using an iterative process during regular team meetings with coders to clarify and confirm interpretations. Discrepancies were discussed within team meetings to achieve consensus.
Questions received. Between February 2022 and December 2023, the program received 101 email questions. Requesters included 39 physicians, 17 nurse practitioners or physician assistants, 15 social workers, 14 psychologists, 9 nurses, 5 pharmacists, 1 dietitian, and 1 who was undetermined. Experts responded to the questions an average of 6 days after receipt (range, < 1-19); 73 responses (72%) met the 7-day goal.
Iterative changes to coded themes were made during group discussions. Multiple clinical questions were often posed within the same email. Initially, some coders identified themes solely based on reported symptoms; others identified themes based on reported and/or potential diagnostic conditions attributed to the symptom(s) described within the email. For example, some coders selected a primary theme of behavioral and psychological symptoms of dementia (BPSD) only if a behavior contributing to distress in the veteran or others was described, while others selected this theme when any psychiatric symptom (eg, psychosis) was present in the context of dementia. The group identified 1 primary theme per question based on the main clinical symptom or main concern presented. Co-occurring diagnostic conditions highlighted in the email requests were included as secondary themes, and each question could have > 1 secondary theme.
The most frequent requests related to clinical symptoms included questions about agitated behaviors, sleep and/or nightmares, and depression symptoms (Table 1). Twenty-seven of 33 email requests on agitated behaviors were related to a dementia diagnosis, as were several questions about sleep/nightmares, depression, psychosis/mania, and anxiety. Many diagnostic conditions were described in the email requests (Table 2). The most frequent condition was dementia, followed by a medical condition, depressive disorder, posttraumatic stress disorder, and/or serious mental illness.
Request for Feedback. In February 2022, an email request was sent to the 64 clinicians who asked email questions from the start of the program in June 2021 through December 2021. A second request included 11 clinicians who asked questions from January through February 2022. These requests were sent as part of preparations for the symposium on the program presented at the AAGP annual meeting in March 2022.9 In May 2024, feedback was requested from 37 clinicians who submitted questions from May 1, 2023, through May 15, 2024.
Requests for feedback included 6 closed-ended and 1 open-ended question: (1) Did the answer you received help inform clinical practice? (2) Did you receive a timely response? (3) What type of information was useful to you in addressing your question (ie, direct/specific answer to a clinical scenario, guidelines, articles, VA resources)? (4) Do you have access to a geriatric psychiatrist at your facility? (5) Are you likely to use Ask the Expert Geriatric Psychiatry in the future? (6) Would you use a geriatric psychiatry teleconsultation service? (7) Share suggestions for improvement. Frequencies of response selection were obtained for each question. Text responses to the open-ended question asking for suggestions for improvement were reviewed and summarized.
Responses
Thirty users responded to the feedback request (27% response rate). Respondents considered the answers received extremely (n = 14; 47%) or very much (n = 12; 40%) helpful for their clinical practice. Twenty-three respondents (77%) felt an answer was provided promptly, 7 respondents (23%) felt the answer was not timely but still useful, and none felt that the answer was too late. Respondents reported that the most useful type of information in addressing their questions was a direct/specific answer to a clinical scenario (n = 27; 90%), followed by guidelines (n = 12; 40%), articles (n = 7; 23%), and VA resources (n = 4; 13%).
Sixteen respondents (53%) reported that they rarely had ready access to a geriatric psychiatrist at their facility, 3 (10%) had access sometimes, 4 (14%) had access usually, 3 (10%) had access regularly, and 3 (10%) never had access. Twenty-seven respondents (90%) indicated they would be very likely to use the service again. If geriatric psychiatry teleconsultation and/or e-consultation were offered, many respondents indicated they would be extremely (n = 10; 33%) or very (n = 12; 40%) likely to use teleconsultation and/or e-consultation.
Suggestions for improvement included supporting experts to perform chart reviews for email questions, developing a template or consult form, holding a biweekly drop-in meeting to present questions to and discuss cases with a panel of experts, and providing further help addressing complex decisional capacity issues, delirium, and care or placement for veterans with severe behavioral issues in a rural setting.
Discussion
Although many older adults experience cognitive and mental health disorders that may benefit from management by a geriatric psychiatrist, the number of trained geriatric psychiatrists available is insufficient to allow for direct care for each patient. The Ask the Expert Geriatric Psychiatry email consultation program is one aspect of a multicomponent strategy within the VHA to increase access to specialty geriatric mental health services for veterans. A key advantage of the program is that it is not resource intensive. Experts can participate voluntarily, providing timely feedback to clinicians around the country while continuing other duties at their respective VA medical centers. Email replies to the experts’ answers elicited positive feedback on the program, include: “I found this service to be extremely helpful and I have shared the information they sent me with several other coworkers!”, “It was great!”, and “I endorsed the service to our VISN Rehabilitation and Extended Care group.”
The coding of primary and secondary themes from 101 email questions that were retained revealed the range and relative frequencies of clinical and administrative topics with which clinicians needed help. The most common (33%) theme was agitated behaviors. Nearly half of the questions (48%) were related to underlying dementia, and 29% were related to a patient’s medical comorbidities. These findings suggest that the expertise of a geriatric psychiatrist is particularly relevant when caring for older patients experiencing BPSD or patients with complex, overlapping psychiatric and medical conditions.
Despite a 27% response rate, participant feedback has been helpful. The program reached its intended audience of clinicians in rural areas and at smaller facilities with 53% of requesters reporting they rarely had access to a geriatric psychiatrist. Suggestions for improvement indicated that some clinicians desired additional support, including chart reviews, meetings with experts, and a video teleconsultation service (available through NEXCSS-MH).
Many clinicians without training in specialty geriatric mental health may require help with complex clinical presentations. For example, 39 clinicians who submitted questions to the program were physicians. Accreditation Council for Graduate Medical Education program requirements for general psychiatry residency include 4 weeks of geriatric psychiatry.11 The findings of this study suggest that this level of training may not be adequate to independently care for every patient who experiences dementia or multimorbidity. Several training and mentoring initiatives have been developed to address the professional development need for psychiatrists.12-14
The need for geriatric workforce development is significant across health care, including other mental health professions.15,16 The VHA Geriatric Scholars program trains rural primary care practitioners, psychologists, and psychiatrists.17,18 Likewise, consultative geriatric specialty support for primary care practitioners in rural areas is provided via the Geriatric Research Education and Clinical Center Connect program.19 The Ask the Expert Geriatric Psychiatry email program is an additional economical model to support clinician educational development and provide rapid educational responses to inform patient care.
Ask the Expert received fewer email questions than anticipated. Enhanced optimization may require more frequent and widespread announcements about the program. Clinical staff may not be aware of the program due to an overload of email communications. Likewise, it may be challenging for busy clinicians to take the time to seek consultation or recognize a potential gap in their knowledge or skills. Had more questions been submitted, the 5 volunteer experts may have had more difficulty addressing the demand. Feedback from this project may inform development of a frequently asked questions document to share with VHA teams and a drop-in office hour to pose clinical questions of geriatric psychiatry experts, as recommended by a clinician who participated in the program.
Limitations
Not all requesters were sent a request for feedback, and the response rate for the request for feedback was only 27%. As the program has evolved, it began sending a request for feedback immediately after answering each question, which may increase the odds of response. The goal of experts answering questions within 7 business days was met 72% of the time, likely an artifact of experts integrating question answering with many other duties. The mailbox coordinator has since provided email prompts to experts immediately upon being assigned a question with the goal of improving timeliness. The program did not include chart reviews or patient consultations, as neither was feasible for volunteer experts. The email consultation service is a single component of virtual consultative specialty geriatric mental health services within the VHA, including video consultations via NEXCSS-MH and regional geriatric mental health teams.
Conclusions
The need for specialty geriatric mental health services is increasing in the VHA and across the US. However, there are too few board-certified geriatric psychiatrists to provide direct patient care to all older adults with cognitive and mental health disorders. The VHA has leveraged telehealth to improve access to geriatric mental health care. The VHA Ask the Expert Geriatric Psychiatry email consultation program is a low-resource service which provides rapid feedback to clinicians nationwide on challenging clinical scenarios, many of which are dementia-related. Most users of the service who responded to requests for feedback reported that answers to their questions were helpful and timely. The email consultation program should continue to be supplemented by more comprehensive geriatric telemental health services for particularly complex cases to meet the needs of older veterans.
T he US Census Bureau projects that the number of older adults (aged ≥ 65 years) will exceed 49 million by 2030, and an estimated 20% (nearly 10 million) of this population will experience cognitive or mental health disorders.1,2 The mental health workforce is not equipped to address the specialized mental health care needs of many older adults.2,3 For example, geriatric psychiatrists specialize in the diagnosis and treatment of mental illness and cognitive disorders in the later stages of life, but their numbers are few and declining. Only 33.5% of geriatric psychiatry fellowship training slots were filled from 2017 to 2021, and only 62 fellows trained during the 2021-2022 academic year.4 Board-certified geriatric psychiatrists also tend to be concentrated in larger, urban, academically-affiliated medical centers, often leaving rural areas and smaller facilities without access, including facilities in the Veterans Health Administration (VHA).5
The VHA has been optimizing access to specialty geriatric mental health services via regional and national virtual consultation services. Seven of 19 Veterans Integrated Service Network (VISN) Clinical Resource Hubs (CRHs) have geriatric mental health teams.6 These provide interdisciplinary geriatric mental telehealth services, including geriatric psychiatry, for older veterans with complex care needs.7,8 Likewise, the VHA National Expert Consultation & Specialized Services-Mental Health (NEXCSS- MH, formerly known as the National Telemental Health Center) sponsors video teleconsultations with board-certified geriatric psychiatrists and an Ask the Expert email consultation program.
This article describes the Ask the Expert Geriatric Psychiatry email program (one of several similar programs at NEXCSS-MH), building upon a symposium presented at the American Association for Geriatric Psychiatry (AAGP) annual meeting in March 2022.9 The program was initiated in June 2021 as a result of discussions between the National Mental Health Director, Geriatric Mental Health in the VHA Office of Mental Health and Suicide Prevention (now known as the Office of Mental Health [OMH]), and National Telemental Health Center leadership. VHA board certified geriatric psychiatrists were recruited to serve as expert consultants and respond to email questions submitted by VHA clinicians regarding the psychiatric care of older adult veterans. The results of this program identify educational needs among clinical staff and may inform the development of program materials for a range of clinicians.
Program Description
The national geriatric mental health director recruited prospective experts and met with each to assess interest and qualifications, consulting with OMH psychiatrist leaders before making selections. Five experts were initially selected; 1 later stepped down and was replaced by another, who also stepped down. The experts were board certified in psychiatry and geriatric psychiatry and held a variety of local and national leadership positions, including geriatric psychiatry fellowship director, US Department of Veterans Affairs (VA) research and clinical leader, and various roles in the AAGP; some had received teaching awards.
Operations
The national geriatric mental health director announced the program in June 2021 to VHA mental health and geriatric program email groups with reminders sent every few months. The announcement included information about the types of questions appropriate to submit, including examples of general clinical management questions that did not share patient-specific protected health information, and clarified that experts would not be conducting chart reviews because the time required for detailed chart reviews was not feasible for volunteer experts to integrate into their otherwise full-time jobs at their respective VA medical centers. The announcement also included brief biographies of the experts.
The Figure describes the daily operations of the Ask the Expert Geriatric Psychiatry email consultation program. The NEXCSS- MH developed a Microsoft Outlook mailbox and group email address where clinicians from across the VHA could submit questions. The experts, as well as the national geriatric mental health director and NEXCSS-MH staff, had access to this mailbox to track and/or respond to questions. One expert volunteered to be the program’s primary mailbox coordinator. The coordinator checked the inbox daily and assigned each question to one of the experts on a rotating basis using the color-coding feature in Outlook. The other experts were advised to check the email account at least once weekly and reply to any assigned questions.
Responding to a question entailed first determining whether the question was appropriate for the service. For example, if a question requested a chart review, the expert replied that experts could not provide chart reviews and requested that the question be reframed. Next, the expert often needed to define a specific clinical question from the information provided, as email questions often touched upon several topics. The expert provided personalized advice on diagnostic testing, nonpharmacologic treatment strategies, and/or pharmacologic treatment options. Experts also often attached relevant guidelines or review articles. The goal was to provide a response within 7 business days.
All email responses included a disclaimer indicating that the program was not intended for urgent or immediate medical advice and that the information provided was for VHA clinician education purposes only. The disclaimer explained that email communication did not establish a doctor-patient relationship between the expert and a specific veteran and that, if desired, a request for a clinical consultation could be submitted on a specific case (ie, a video teleconsultation).
Methods for Reviewing Questions
Descriptive statistics, including frequencies, means, and minimum and maximum ranges, were used to capture the number of questions the program received, type of requester, and length of time prior to response for emailed questions.9 Conventional content analysis procedures were used between January and October 2024 to analyze clinicians’ questions.10 Four subject matter experts (3 geriatric psychiatrists and 1 geropsychologist) served as coders, assigned in groups of 2 to review questions. Each coder independently reviewed assigned questions and identified preliminary themes. Themes were reviewed and revised using an iterative process during regular team meetings with coders to clarify and confirm interpretations. Discrepancies were discussed within team meetings to achieve consensus.
Questions received. Between February 2022 and December 2023, the program received 101 email questions. Requesters included 39 physicians, 17 nurse practitioners or physician assistants, 15 social workers, 14 psychologists, 9 nurses, 5 pharmacists, 1 dietitian, and 1 who was undetermined. Experts responded to the questions an average of 6 days after receipt (range, < 1-19); 73 responses (72%) met the 7-day goal.
Iterative changes to coded themes were made during group discussions. Multiple clinical questions were often posed within the same email. Initially, some coders identified themes solely based on reported symptoms; others identified themes based on reported and/or potential diagnostic conditions attributed to the symptom(s) described within the email. For example, some coders selected a primary theme of behavioral and psychological symptoms of dementia (BPSD) only if a behavior contributing to distress in the veteran or others was described, while others selected this theme when any psychiatric symptom (eg, psychosis) was present in the context of dementia. The group identified 1 primary theme per question based on the main clinical symptom or main concern presented. Co-occurring diagnostic conditions highlighted in the email requests were included as secondary themes, and each question could have > 1 secondary theme.
The most frequent requests related to clinical symptoms included questions about agitated behaviors, sleep and/or nightmares, and depression symptoms (Table 1). Twenty-seven of 33 email requests on agitated behaviors were related to a dementia diagnosis, as were several questions about sleep/nightmares, depression, psychosis/mania, and anxiety. Many diagnostic conditions were described in the email requests (Table 2). The most frequent condition was dementia, followed by a medical condition, depressive disorder, posttraumatic stress disorder, and/or serious mental illness.
Request for Feedback. In February 2022, an email request was sent to the 64 clinicians who asked email questions from the start of the program in June 2021 through December 2021. A second request included 11 clinicians who asked questions from January through February 2022. These requests were sent as part of preparations for the symposium on the program presented at the AAGP annual meeting in March 2022.9 In May 2024, feedback was requested from 37 clinicians who submitted questions from May 1, 2023, through May 15, 2024.
Requests for feedback included 6 closed-ended and 1 open-ended question: (1) Did the answer you received help inform clinical practice? (2) Did you receive a timely response? (3) What type of information was useful to you in addressing your question (ie, direct/specific answer to a clinical scenario, guidelines, articles, VA resources)? (4) Do you have access to a geriatric psychiatrist at your facility? (5) Are you likely to use Ask the Expert Geriatric Psychiatry in the future? (6) Would you use a geriatric psychiatry teleconsultation service? (7) Share suggestions for improvement. Frequencies of response selection were obtained for each question. Text responses to the open-ended question asking for suggestions for improvement were reviewed and summarized.
Responses
Thirty users responded to the feedback request (27% response rate). Respondents considered the answers received extremely (n = 14; 47%) or very much (n = 12; 40%) helpful for their clinical practice. Twenty-three respondents (77%) felt an answer was provided promptly, 7 respondents (23%) felt the answer was not timely but still useful, and none felt that the answer was too late. Respondents reported that the most useful type of information in addressing their questions was a direct/specific answer to a clinical scenario (n = 27; 90%), followed by guidelines (n = 12; 40%), articles (n = 7; 23%), and VA resources (n = 4; 13%).
Sixteen respondents (53%) reported that they rarely had ready access to a geriatric psychiatrist at their facility, 3 (10%) had access sometimes, 4 (14%) had access usually, 3 (10%) had access regularly, and 3 (10%) never had access. Twenty-seven respondents (90%) indicated they would be very likely to use the service again. If geriatric psychiatry teleconsultation and/or e-consultation were offered, many respondents indicated they would be extremely (n = 10; 33%) or very (n = 12; 40%) likely to use teleconsultation and/or e-consultation.
Suggestions for improvement included supporting experts to perform chart reviews for email questions, developing a template or consult form, holding a biweekly drop-in meeting to present questions to and discuss cases with a panel of experts, and providing further help addressing complex decisional capacity issues, delirium, and care or placement for veterans with severe behavioral issues in a rural setting.
Discussion
Although many older adults experience cognitive and mental health disorders that may benefit from management by a geriatric psychiatrist, the number of trained geriatric psychiatrists available is insufficient to allow for direct care for each patient. The Ask the Expert Geriatric Psychiatry email consultation program is one aspect of a multicomponent strategy within the VHA to increase access to specialty geriatric mental health services for veterans. A key advantage of the program is that it is not resource intensive. Experts can participate voluntarily, providing timely feedback to clinicians around the country while continuing other duties at their respective VA medical centers. Email replies to the experts’ answers elicited positive feedback on the program, include: “I found this service to be extremely helpful and I have shared the information they sent me with several other coworkers!”, “It was great!”, and “I endorsed the service to our VISN Rehabilitation and Extended Care group.”
The coding of primary and secondary themes from 101 email questions that were retained revealed the range and relative frequencies of clinical and administrative topics with which clinicians needed help. The most common (33%) theme was agitated behaviors. Nearly half of the questions (48%) were related to underlying dementia, and 29% were related to a patient’s medical comorbidities. These findings suggest that the expertise of a geriatric psychiatrist is particularly relevant when caring for older patients experiencing BPSD or patients with complex, overlapping psychiatric and medical conditions.
Despite a 27% response rate, participant feedback has been helpful. The program reached its intended audience of clinicians in rural areas and at smaller facilities with 53% of requesters reporting they rarely had access to a geriatric psychiatrist. Suggestions for improvement indicated that some clinicians desired additional support, including chart reviews, meetings with experts, and a video teleconsultation service (available through NEXCSS-MH).
Many clinicians without training in specialty geriatric mental health may require help with complex clinical presentations. For example, 39 clinicians who submitted questions to the program were physicians. Accreditation Council for Graduate Medical Education program requirements for general psychiatry residency include 4 weeks of geriatric psychiatry.11 The findings of this study suggest that this level of training may not be adequate to independently care for every patient who experiences dementia or multimorbidity. Several training and mentoring initiatives have been developed to address the professional development need for psychiatrists.12-14
The need for geriatric workforce development is significant across health care, including other mental health professions.15,16 The VHA Geriatric Scholars program trains rural primary care practitioners, psychologists, and psychiatrists.17,18 Likewise, consultative geriatric specialty support for primary care practitioners in rural areas is provided via the Geriatric Research Education and Clinical Center Connect program.19 The Ask the Expert Geriatric Psychiatry email program is an additional economical model to support clinician educational development and provide rapid educational responses to inform patient care.
Ask the Expert received fewer email questions than anticipated. Enhanced optimization may require more frequent and widespread announcements about the program. Clinical staff may not be aware of the program due to an overload of email communications. Likewise, it may be challenging for busy clinicians to take the time to seek consultation or recognize a potential gap in their knowledge or skills. Had more questions been submitted, the 5 volunteer experts may have had more difficulty addressing the demand. Feedback from this project may inform development of a frequently asked questions document to share with VHA teams and a drop-in office hour to pose clinical questions of geriatric psychiatry experts, as recommended by a clinician who participated in the program.
Limitations
Not all requesters were sent a request for feedback, and the response rate for the request for feedback was only 27%. As the program has evolved, it began sending a request for feedback immediately after answering each question, which may increase the odds of response. The goal of experts answering questions within 7 business days was met 72% of the time, likely an artifact of experts integrating question answering with many other duties. The mailbox coordinator has since provided email prompts to experts immediately upon being assigned a question with the goal of improving timeliness. The program did not include chart reviews or patient consultations, as neither was feasible for volunteer experts. The email consultation service is a single component of virtual consultative specialty geriatric mental health services within the VHA, including video consultations via NEXCSS-MH and regional geriatric mental health teams.
Conclusions
The need for specialty geriatric mental health services is increasing in the VHA and across the US. However, there are too few board-certified geriatric psychiatrists to provide direct patient care to all older adults with cognitive and mental health disorders. The VHA has leveraged telehealth to improve access to geriatric mental health care. The VHA Ask the Expert Geriatric Psychiatry email consultation program is a low-resource service which provides rapid feedback to clinicians nationwide on challenging clinical scenarios, many of which are dementia-related. Most users of the service who responded to requests for feedback reported that answers to their questions were helpful and timely. The email consultation program should continue to be supplemented by more comprehensive geriatric telemental health services for particularly complex cases to meet the needs of older veterans.
- 2023 population projections for the nation by age, sex, race, Hispanic origin and nativity. United States Census Bureau. November 9, 2023. Accessed December 11, 2025. https://www.census.gov/newsroom/press-kits/2023/population-projections.html
- National Academies of Sciences Engineering and Medicine. Addressing the rising mental health needs of an aging population: proceedings of a workshop. 2024. Accessed December 11, 2025. doi.org:10.17226/27340
- Institute of Medicine. The mental health and substance use workforce for older adults: in whose hands? The National Academies Press; 2012. Accessed December 11, 2025. doi:10.17226/13400
- American Psychiatric Association. 2022 resident/fellow census. November 2023. Accessed December 11, 2025. https://www.psychiatry.org/getmedia/d80438af-f760-40f3-9d33-f91309b09564/APA-Resident-Census-2022.pdf
- Juul D, Colenda CC, Lyness JM, et al. Subspecialty training and certification in geriatric psychiatry: a 25-year overview. Am J Geriatr Psychiatry. 2017;25:445-453. doi:10.1016/j.jagp.2016.12.018
- Jaske E, Wheat CL, Rubenstein LV, et al. Understanding how contingency staffing programs can support mental health services in the Veterans Health Administration. Telemed J E Health. 2024;30:1857-1865. doi:10.1089/tmj.2023.0573
- Gould CE, Carlson C, Alfaro AJ, et al. Supporting veterans, caregivers, and providers in rural regions with tele-geriatric psychiatry consultation: a mixed methods pilot study. Am J Geriatr Psychiatry. 2023;31:279-290. doi:10.1016/j.jagp.2023.01.005
- Gould CE, Paiko L, Carlson C, et al. Implementation of tele-geriatricmental healthcare for rural veterans: factors influencing care models. Front Health Serv. 2024;4:1221899. doi:10.3389/frhs.2024.1221899
- Padala P, Schultz S, Khatkhate G, et al. Ask the expert geriatric psychiatry: VA program to support clinicians. Am J Geriatr Psychiatry. 2022;30:S18. doi:10.1016/j.jagp.2022.01.279
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288. doi:10.1177/1049732305276687
- Accreditation Council for Graduate Medical Education. Program requirements for graduate medical education in psychiatry. Revised September 3, 2025. Accessed December 11, 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/400_psychiatry_2025_reformatted.pdf
- Fernandez J, Agarwal KS, Amspoker AB, et al. Outcomes from an interprofessional, dementia-focused, telementoring program: a brief report. Gerontol Geriatr Educ. 2024;45:601-606. doi:10.1080/02701960.2023.2253175
- Conroy ML, Garcia-Pittman EC, van Dyck LI, et al. The COVID-19 American Association for Geriatric Psychiatry (AAGP) online trainee curriculum: program evaluation and future directions. Am J Geriatr Psychiatry. 2025;33:308-314. doi:10.1016/j.jagp.2024.10.010
- Conroy ML, Garcia-Pittman EC, Ali H, et al. The COVID-19 AAGP online trainee curriculum: development and method of initial evaluation. Am J Geriatr Psychiatry. 2020;28:1004-1008. doi:10.1016/j.jagp.2020.06.003
- Flaherty E, Busby-Whitehead J, Potter J, et al. The geriatric workforce enhancement program: review of the coordinating center and examples of the GWEP in practice. Am J Geriatr Psychiatry. 2019;27:675-686. doi:10.1016/j.jagp.2019.04.010
- Hoge MA, Karel MJ, Zeiss AM, et al. Strengthening psychology’s workforce for older adults: implications of the Institute of Medicine’s report to Congress. Am Psychol. 2015;70:265-278. doi:10.1037/a0038927
- Kramer BJ, Creekmur B, Howe JL, et al. Veterans Affairs geriatric scholars program: enhancing existing primary care clinician skills in caring for older veterans. J Am Geriatr Soc. 2016;64:2343-2348. doi:10.1111/jgs.14382
- Gould CE, Rodriguez RL, Gregg JJ, et al. Preparing Veterans Health Administration psychologists to meet the complex needs of aging veterans. Fed Pract. 2024;41:S10-S15. doi:10.12788/fp.0466
- Pimentel CB, Gately M, Barczi SR, et al. GRECC Connect: Geriatrics telehealth to empower health care providers and improve management of older veterans in rural communities. Fed Pract. 2019;36:464-470.
- 2023 population projections for the nation by age, sex, race, Hispanic origin and nativity. United States Census Bureau. November 9, 2023. Accessed December 11, 2025. https://www.census.gov/newsroom/press-kits/2023/population-projections.html
- National Academies of Sciences Engineering and Medicine. Addressing the rising mental health needs of an aging population: proceedings of a workshop. 2024. Accessed December 11, 2025. doi.org:10.17226/27340
- Institute of Medicine. The mental health and substance use workforce for older adults: in whose hands? The National Academies Press; 2012. Accessed December 11, 2025. doi:10.17226/13400
- American Psychiatric Association. 2022 resident/fellow census. November 2023. Accessed December 11, 2025. https://www.psychiatry.org/getmedia/d80438af-f760-40f3-9d33-f91309b09564/APA-Resident-Census-2022.pdf
- Juul D, Colenda CC, Lyness JM, et al. Subspecialty training and certification in geriatric psychiatry: a 25-year overview. Am J Geriatr Psychiatry. 2017;25:445-453. doi:10.1016/j.jagp.2016.12.018
- Jaske E, Wheat CL, Rubenstein LV, et al. Understanding how contingency staffing programs can support mental health services in the Veterans Health Administration. Telemed J E Health. 2024;30:1857-1865. doi:10.1089/tmj.2023.0573
- Gould CE, Carlson C, Alfaro AJ, et al. Supporting veterans, caregivers, and providers in rural regions with tele-geriatric psychiatry consultation: a mixed methods pilot study. Am J Geriatr Psychiatry. 2023;31:279-290. doi:10.1016/j.jagp.2023.01.005
- Gould CE, Paiko L, Carlson C, et al. Implementation of tele-geriatricmental healthcare for rural veterans: factors influencing care models. Front Health Serv. 2024;4:1221899. doi:10.3389/frhs.2024.1221899
- Padala P, Schultz S, Khatkhate G, et al. Ask the expert geriatric psychiatry: VA program to support clinicians. Am J Geriatr Psychiatry. 2022;30:S18. doi:10.1016/j.jagp.2022.01.279
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15:1277-1288. doi:10.1177/1049732305276687
- Accreditation Council for Graduate Medical Education. Program requirements for graduate medical education in psychiatry. Revised September 3, 2025. Accessed December 11, 2025. https://www.acgme.org/globalassets/pfassets/programrequirements/2025-reformatted-requirements/400_psychiatry_2025_reformatted.pdf
- Fernandez J, Agarwal KS, Amspoker AB, et al. Outcomes from an interprofessional, dementia-focused, telementoring program: a brief report. Gerontol Geriatr Educ. 2024;45:601-606. doi:10.1080/02701960.2023.2253175
- Conroy ML, Garcia-Pittman EC, van Dyck LI, et al. The COVID-19 American Association for Geriatric Psychiatry (AAGP) online trainee curriculum: program evaluation and future directions. Am J Geriatr Psychiatry. 2025;33:308-314. doi:10.1016/j.jagp.2024.10.010
- Conroy ML, Garcia-Pittman EC, Ali H, et al. The COVID-19 AAGP online trainee curriculum: development and method of initial evaluation. Am J Geriatr Psychiatry. 2020;28:1004-1008. doi:10.1016/j.jagp.2020.06.003
- Flaherty E, Busby-Whitehead J, Potter J, et al. The geriatric workforce enhancement program: review of the coordinating center and examples of the GWEP in practice. Am J Geriatr Psychiatry. 2019;27:675-686. doi:10.1016/j.jagp.2019.04.010
- Hoge MA, Karel MJ, Zeiss AM, et al. Strengthening psychology’s workforce for older adults: implications of the Institute of Medicine’s report to Congress. Am Psychol. 2015;70:265-278. doi:10.1037/a0038927
- Kramer BJ, Creekmur B, Howe JL, et al. Veterans Affairs geriatric scholars program: enhancing existing primary care clinician skills in caring for older veterans. J Am Geriatr Soc. 2016;64:2343-2348. doi:10.1111/jgs.14382
- Gould CE, Rodriguez RL, Gregg JJ, et al. Preparing Veterans Health Administration psychologists to meet the complex needs of aging veterans. Fed Pract. 2024;41:S10-S15. doi:10.12788/fp.0466
- Pimentel CB, Gately M, Barczi SR, et al. GRECC Connect: Geriatrics telehealth to empower health care providers and improve management of older veterans in rural communities. Fed Pract. 2019;36:464-470.
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians
Ask the Expert Geriatric Psychiatry: A VHA Email Consultation Program to Support Clinicians