User login
Rise in number of unclaimed dead bodies used in medical schools
An increasing number of unclaimed dead bodies went to help train medical students in Texas between 2017 and 2021, new research reveals.
Investigators did not expect to see such an increase, said lead author Eli Shupe, PhD, assistant professor in the department of philosophy and humanities at the University of Texas at Arlington.
The numbers jumped from 64 unclaimed bodies to 446 bodies annually over those 5 years. “People are usually under the impression that this is something that either doesn’t happen anymore or it’s on the decline as more people step up to be willed body donors,” said Dr. Shupe, who is also codirector of the medical humanities and bioethics program at UTA.
The study findings were published in JAMA as a research letter. Researchers said that the number of unclaimed bodies – those not claimed by next of kin for burial or cremation – has dropped significantly across the United States since the middle of the 20th century.
Some people don’t want to discuss the practice because it is controversial, said Matthew DeCamp, MD, PhD, associate professor at the Center for Bioethics and Humanities and Division of General Internal Medicine, University of Colorado Anschutz Medical Campus, Aurora. “But ‘sweeping it under the rug’ means we miss the opportunity for dialogues about respect, consent, social justice, and so on – as well as the opportunity to change policy.”
The study included all medical schools in Texas, and researchers say it’s likely happening elsewhere in the United States and abroad. The practice is legal in most counties and states. One exception is New York, which passed a law in 2016 that does not allow unclaimed bodies to go to medical schools without prior written consent from the deceased.
“Although limited to one state, these findings suggest that use of unclaimed bodies may be both more common than we thought and increasing,” added Dr. DeCamp, who was not affiliated with the current study.
Even doctors can be split on the value to medical training versus the rights of the dead. “I know that medical professionals are divided on the role of dissection and anatomy learning and its necessity,” Dr. Shupe said. She predicted working with cadavers in medical schools will probably continue for the foreseeable future.
The marginalized and the vulnerable
So who are the unclaimed? They can include those who are unhoused and those who do not leave enough money to cover cost of burial or cremation. In some cases, they don’t have a next of kin or their next of kin is unwilling or unable to pay for their burial or cremation.
“Predominantly, these are going to be people who are poor or members of marginalized or vulnerable populations,” Dr. Shupe said. She estimated that about 80% of the people who die in poverty in her region, the Dallas–Fort Worth area, are Black or Hispanic individuals.
“It is alarming that we are going in the wrong direction when it comes to the increasing utility of unclaimed bodies,” said Joy Balta, PhD, associate professor of anatomy and founding director of Anatomy Learning Institute at Point Loma Nazarene University, San Diego, when asked to comment on the study. The hope is to rely solely on donated human bodies to ensure that donors have provided informed consent for their use in education, research, and clinical training.
“These unclaimed bodies did not provide any consent, [which] raises ethical questions,” Dr. Balta said.
Key findings
In Texas in 2021, 43% of the cadavers in 14 medical schools studied came from unclaimed bodies. A total 14% of schools reported that they accepted unclaimed bodies, 28% possibly accepted them because they were transferred from institutions that use them, and the remaining 57% do not accept unclaimed bodies.
The total number and proportion of unclaimed bodies going to medical education in the study increased during the study. The 14% in 2021 was a jump from 2% in 2017, for example.
The 14 medical schools studied included both public and private institutions. The investigators also looked at data from the Texas State Anatomical Board, which tracks how cadavers are attained and distributed in the state, including how many began as unclaimed bodies.
Legal in most jurisdictions
Dr. Shupe first learned about what can happen to unclaimed bodies as a hospice volunteer. She was accompanying the hospice chaplain one day who said: “Poor Mr. Smith [not his real name] doesn’t have long, and then he’s off to the medical school.” Dr. Shupe asked what the chaplain meant because she was unaware of the practice.
“I stumbled on this by chance, and it ended up being a really fruitful research area,” she added.
The bigger picture
Greater awareness is needed and there is not a lot of research out there, Dr. Shupe said. One exception is a 2018 study of medical schools nationwide that found 12.4% reported possible use of unclaimed bodies.
Dr. DeCamp, an author of that previous research, said: “Knowing this practice continues is the most important thing for doctors and medical students to know.”
It remains unclear whether the COVID pandemic or the opioid epidemic contributed to the rise of unclaimed bodies going to medical training. That is a question for future study, Dr. Shupe said.
Most bodies willingly donated
The majority of cadavers that go to medical training in the United States are ‘full body donors,’ people or relatives who agree to voluntarily send a body to medical schools. “We are fortunate to have a lot of people who are willing to become whole body donors,” she said.
Greater awareness about how donated cadavers could make a difference to further increase willful donations, Dr. Shupe said. “Honoring those gifts by allowing them to help train the next generation of doctors is a wonderful thing.”
A May 2023 study from Dr. Balta and colleagues on body donation programs in the United States “found that the number of whole-body donations have decreased in some states and the numbers are not enough to meet the needs for education, research and clinical training,” Dr. Balta said. This could explain the increasing use of unclaimed bodies.
“Some medical schools have explicit educational interventions on this topic, and formally recognize the unclaimed at anatomical gift ceremonies,” Dr. DeCamp said. “More should.”
Research support was provided by the UTA. Dr. Shupe, Dr. Balta, and Dr. DeCamp reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An increasing number of unclaimed dead bodies went to help train medical students in Texas between 2017 and 2021, new research reveals.
Investigators did not expect to see such an increase, said lead author Eli Shupe, PhD, assistant professor in the department of philosophy and humanities at the University of Texas at Arlington.
The numbers jumped from 64 unclaimed bodies to 446 bodies annually over those 5 years. “People are usually under the impression that this is something that either doesn’t happen anymore or it’s on the decline as more people step up to be willed body donors,” said Dr. Shupe, who is also codirector of the medical humanities and bioethics program at UTA.
The study findings were published in JAMA as a research letter. Researchers said that the number of unclaimed bodies – those not claimed by next of kin for burial or cremation – has dropped significantly across the United States since the middle of the 20th century.
Some people don’t want to discuss the practice because it is controversial, said Matthew DeCamp, MD, PhD, associate professor at the Center for Bioethics and Humanities and Division of General Internal Medicine, University of Colorado Anschutz Medical Campus, Aurora. “But ‘sweeping it under the rug’ means we miss the opportunity for dialogues about respect, consent, social justice, and so on – as well as the opportunity to change policy.”
The study included all medical schools in Texas, and researchers say it’s likely happening elsewhere in the United States and abroad. The practice is legal in most counties and states. One exception is New York, which passed a law in 2016 that does not allow unclaimed bodies to go to medical schools without prior written consent from the deceased.
“Although limited to one state, these findings suggest that use of unclaimed bodies may be both more common than we thought and increasing,” added Dr. DeCamp, who was not affiliated with the current study.
Even doctors can be split on the value to medical training versus the rights of the dead. “I know that medical professionals are divided on the role of dissection and anatomy learning and its necessity,” Dr. Shupe said. She predicted working with cadavers in medical schools will probably continue for the foreseeable future.
The marginalized and the vulnerable
So who are the unclaimed? They can include those who are unhoused and those who do not leave enough money to cover cost of burial or cremation. In some cases, they don’t have a next of kin or their next of kin is unwilling or unable to pay for their burial or cremation.
“Predominantly, these are going to be people who are poor or members of marginalized or vulnerable populations,” Dr. Shupe said. She estimated that about 80% of the people who die in poverty in her region, the Dallas–Fort Worth area, are Black or Hispanic individuals.
“It is alarming that we are going in the wrong direction when it comes to the increasing utility of unclaimed bodies,” said Joy Balta, PhD, associate professor of anatomy and founding director of Anatomy Learning Institute at Point Loma Nazarene University, San Diego, when asked to comment on the study. The hope is to rely solely on donated human bodies to ensure that donors have provided informed consent for their use in education, research, and clinical training.
“These unclaimed bodies did not provide any consent, [which] raises ethical questions,” Dr. Balta said.
Key findings
In Texas in 2021, 43% of the cadavers in 14 medical schools studied came from unclaimed bodies. A total 14% of schools reported that they accepted unclaimed bodies, 28% possibly accepted them because they were transferred from institutions that use them, and the remaining 57% do not accept unclaimed bodies.
The total number and proportion of unclaimed bodies going to medical education in the study increased during the study. The 14% in 2021 was a jump from 2% in 2017, for example.
The 14 medical schools studied included both public and private institutions. The investigators also looked at data from the Texas State Anatomical Board, which tracks how cadavers are attained and distributed in the state, including how many began as unclaimed bodies.
Legal in most jurisdictions
Dr. Shupe first learned about what can happen to unclaimed bodies as a hospice volunteer. She was accompanying the hospice chaplain one day who said: “Poor Mr. Smith [not his real name] doesn’t have long, and then he’s off to the medical school.” Dr. Shupe asked what the chaplain meant because she was unaware of the practice.
“I stumbled on this by chance, and it ended up being a really fruitful research area,” she added.
The bigger picture
Greater awareness is needed and there is not a lot of research out there, Dr. Shupe said. One exception is a 2018 study of medical schools nationwide that found 12.4% reported possible use of unclaimed bodies.
Dr. DeCamp, an author of that previous research, said: “Knowing this practice continues is the most important thing for doctors and medical students to know.”
It remains unclear whether the COVID pandemic or the opioid epidemic contributed to the rise of unclaimed bodies going to medical training. That is a question for future study, Dr. Shupe said.
Most bodies willingly donated
The majority of cadavers that go to medical training in the United States are ‘full body donors,’ people or relatives who agree to voluntarily send a body to medical schools. “We are fortunate to have a lot of people who are willing to become whole body donors,” she said.
Greater awareness about how donated cadavers could make a difference to further increase willful donations, Dr. Shupe said. “Honoring those gifts by allowing them to help train the next generation of doctors is a wonderful thing.”
A May 2023 study from Dr. Balta and colleagues on body donation programs in the United States “found that the number of whole-body donations have decreased in some states and the numbers are not enough to meet the needs for education, research and clinical training,” Dr. Balta said. This could explain the increasing use of unclaimed bodies.
“Some medical schools have explicit educational interventions on this topic, and formally recognize the unclaimed at anatomical gift ceremonies,” Dr. DeCamp said. “More should.”
Research support was provided by the UTA. Dr. Shupe, Dr. Balta, and Dr. DeCamp reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An increasing number of unclaimed dead bodies went to help train medical students in Texas between 2017 and 2021, new research reveals.
Investigators did not expect to see such an increase, said lead author Eli Shupe, PhD, assistant professor in the department of philosophy and humanities at the University of Texas at Arlington.
The numbers jumped from 64 unclaimed bodies to 446 bodies annually over those 5 years. “People are usually under the impression that this is something that either doesn’t happen anymore or it’s on the decline as more people step up to be willed body donors,” said Dr. Shupe, who is also codirector of the medical humanities and bioethics program at UTA.
The study findings were published in JAMA as a research letter. Researchers said that the number of unclaimed bodies – those not claimed by next of kin for burial or cremation – has dropped significantly across the United States since the middle of the 20th century.
Some people don’t want to discuss the practice because it is controversial, said Matthew DeCamp, MD, PhD, associate professor at the Center for Bioethics and Humanities and Division of General Internal Medicine, University of Colorado Anschutz Medical Campus, Aurora. “But ‘sweeping it under the rug’ means we miss the opportunity for dialogues about respect, consent, social justice, and so on – as well as the opportunity to change policy.”
The study included all medical schools in Texas, and researchers say it’s likely happening elsewhere in the United States and abroad. The practice is legal in most counties and states. One exception is New York, which passed a law in 2016 that does not allow unclaimed bodies to go to medical schools without prior written consent from the deceased.
“Although limited to one state, these findings suggest that use of unclaimed bodies may be both more common than we thought and increasing,” added Dr. DeCamp, who was not affiliated with the current study.
Even doctors can be split on the value to medical training versus the rights of the dead. “I know that medical professionals are divided on the role of dissection and anatomy learning and its necessity,” Dr. Shupe said. She predicted working with cadavers in medical schools will probably continue for the foreseeable future.
The marginalized and the vulnerable
So who are the unclaimed? They can include those who are unhoused and those who do not leave enough money to cover cost of burial or cremation. In some cases, they don’t have a next of kin or their next of kin is unwilling or unable to pay for their burial or cremation.
“Predominantly, these are going to be people who are poor or members of marginalized or vulnerable populations,” Dr. Shupe said. She estimated that about 80% of the people who die in poverty in her region, the Dallas–Fort Worth area, are Black or Hispanic individuals.
“It is alarming that we are going in the wrong direction when it comes to the increasing utility of unclaimed bodies,” said Joy Balta, PhD, associate professor of anatomy and founding director of Anatomy Learning Institute at Point Loma Nazarene University, San Diego, when asked to comment on the study. The hope is to rely solely on donated human bodies to ensure that donors have provided informed consent for their use in education, research, and clinical training.
“These unclaimed bodies did not provide any consent, [which] raises ethical questions,” Dr. Balta said.
Key findings
In Texas in 2021, 43% of the cadavers in 14 medical schools studied came from unclaimed bodies. A total 14% of schools reported that they accepted unclaimed bodies, 28% possibly accepted them because they were transferred from institutions that use them, and the remaining 57% do not accept unclaimed bodies.
The total number and proportion of unclaimed bodies going to medical education in the study increased during the study. The 14% in 2021 was a jump from 2% in 2017, for example.
The 14 medical schools studied included both public and private institutions. The investigators also looked at data from the Texas State Anatomical Board, which tracks how cadavers are attained and distributed in the state, including how many began as unclaimed bodies.
Legal in most jurisdictions
Dr. Shupe first learned about what can happen to unclaimed bodies as a hospice volunteer. She was accompanying the hospice chaplain one day who said: “Poor Mr. Smith [not his real name] doesn’t have long, and then he’s off to the medical school.” Dr. Shupe asked what the chaplain meant because she was unaware of the practice.
“I stumbled on this by chance, and it ended up being a really fruitful research area,” she added.
The bigger picture
Greater awareness is needed and there is not a lot of research out there, Dr. Shupe said. One exception is a 2018 study of medical schools nationwide that found 12.4% reported possible use of unclaimed bodies.
Dr. DeCamp, an author of that previous research, said: “Knowing this practice continues is the most important thing for doctors and medical students to know.”
It remains unclear whether the COVID pandemic or the opioid epidemic contributed to the rise of unclaimed bodies going to medical training. That is a question for future study, Dr. Shupe said.
Most bodies willingly donated
The majority of cadavers that go to medical training in the United States are ‘full body donors,’ people or relatives who agree to voluntarily send a body to medical schools. “We are fortunate to have a lot of people who are willing to become whole body donors,” she said.
Greater awareness about how donated cadavers could make a difference to further increase willful donations, Dr. Shupe said. “Honoring those gifts by allowing them to help train the next generation of doctors is a wonderful thing.”
A May 2023 study from Dr. Balta and colleagues on body donation programs in the United States “found that the number of whole-body donations have decreased in some states and the numbers are not enough to meet the needs for education, research and clinical training,” Dr. Balta said. This could explain the increasing use of unclaimed bodies.
“Some medical schools have explicit educational interventions on this topic, and formally recognize the unclaimed at anatomical gift ceremonies,” Dr. DeCamp said. “More should.”
Research support was provided by the UTA. Dr. Shupe, Dr. Balta, and Dr. DeCamp reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA
PPIs linked to long-term infection in kids
Researchers in France are warning against the overzealous use of acid-suppressing drugs in infants after finding that the medications are associated with an increase in risk of serious infections later in life.
The focus on the use of proton pump inhibitors (PPIs) during infancy comes as use of the drugs in young children is rising in France, New Zealand, Scandinavia, and the United States. Much of this use is not to manage confirmed cases of gastroesophageal reflux but rather to soothe the jangled nerves of parents of babies in discomfort, according to the researchers, who have studied national prescribing patterns. In addition to concerns about infection, inappropriate or prolonged use of the acid suppressants is also associated with an increase in the risk of such conditions as hospital-acquired acute kidney injury and inflammatory bowel diseases in children.
PPIs such as omeprazole are effective at reducing gastric acid in babies with gastroesophageal reflux disease. But the researchers warned against using the drugs to manage normal spitting up and dribbling that would have resolved of itself anyway.
“In this study, increased risk of serious infections was associated with PPI use in young children, overall and for various sites and pathogens. In this population, PPIs should not be used without a clear indication,” epidemiologist Marion Lassalle, PharmD, PhD, of EPI-PHARE in Saint-Denis, France, and colleagues reported in JAMA Pediatrics.
Drawing on data from a national birth registry, Dr. Lassalle and colleagues compared infection rates among more than 1.2 million infants who received a PPI at an average age of 88 days with infection rates among children who received another kind of acid suppressant (a histamine receptor blocker or antacid) at an average age of 82 days. More than 600,000 children made up each group.
Slightly over half of the participants were boys, and the study followed children to a maximum age of 9 years. Among children who used PPIs rather than another acid suppressant, there was an overall higher rate of serious infections that required hospitalization (adjusted hazard ratio, 1.34; 95% confidence interval, 1.32-1.36). There were higher rates of infections in the digestive tract; the ear, nose, and throat; the kidneys or urinary tract; the lower respiratory tract; and the nervous system.
Serious infections first appeared 9.7 (range, 3.9-21.3) months after a child stopped using a PPI – a date that Dr. Lassalle’s group determined on the basis of there being a delay of at least 90 days in filling a PPI prescription.
Possible confounders
“The study shows an association, it does not show causation,” said Rina Sanghavi, MD, a pediatric gastroenterologist at UT Southwestern Medical Center, Dallas. Dr. Sanghavi noted that the children who continued taking PPIs generally were sicker in their first year of life, as shown by the higher rates of respiratory ailments and corticosteroid use. This could mean that the infections they eventually experienced had many causes and not necessarily the PPI.
Similarly, pediatric gastroenterologist Sophia Patel, MD, of the Cleveland Clinic, pointed to the almost 10-month average lag time between stopping a PPI and developing a first serious infection. That interval is long enough that it is possible that the infection was caused by something else, Dr. Patel said.
Despite the limitations of the study, Dr. Sanghavi and Dr. Patel said the findings serve as a good reminder to clinicians to use PPIs only when needed and to limit their use once begun. The overall evidence base for limiting use of PPIs is strong, both physicians noted, even if this study does not show direct causation between PPI use and infection rates.
“Ask: Does this child need a PPI?” Dr. Sanghavi said. If so, she generally prescribes PPIs for a period of 2 weeks to a maximum of 2 months and she never authorizes automatic refills. Through this approach, a parent and child will come back to the clinic frequently, which in most cases allows faster tapering of the drugs.
Dr. Lassalle, Dr. Sanghavi, and Dr. Patel reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Researchers in France are warning against the overzealous use of acid-suppressing drugs in infants after finding that the medications are associated with an increase in risk of serious infections later in life.
The focus on the use of proton pump inhibitors (PPIs) during infancy comes as use of the drugs in young children is rising in France, New Zealand, Scandinavia, and the United States. Much of this use is not to manage confirmed cases of gastroesophageal reflux but rather to soothe the jangled nerves of parents of babies in discomfort, according to the researchers, who have studied national prescribing patterns. In addition to concerns about infection, inappropriate or prolonged use of the acid suppressants is also associated with an increase in the risk of such conditions as hospital-acquired acute kidney injury and inflammatory bowel diseases in children.
PPIs such as omeprazole are effective at reducing gastric acid in babies with gastroesophageal reflux disease. But the researchers warned against using the drugs to manage normal spitting up and dribbling that would have resolved of itself anyway.
“In this study, increased risk of serious infections was associated with PPI use in young children, overall and for various sites and pathogens. In this population, PPIs should not be used without a clear indication,” epidemiologist Marion Lassalle, PharmD, PhD, of EPI-PHARE in Saint-Denis, France, and colleagues reported in JAMA Pediatrics.
Drawing on data from a national birth registry, Dr. Lassalle and colleagues compared infection rates among more than 1.2 million infants who received a PPI at an average age of 88 days with infection rates among children who received another kind of acid suppressant (a histamine receptor blocker or antacid) at an average age of 82 days. More than 600,000 children made up each group.
Slightly over half of the participants were boys, and the study followed children to a maximum age of 9 years. Among children who used PPIs rather than another acid suppressant, there was an overall higher rate of serious infections that required hospitalization (adjusted hazard ratio, 1.34; 95% confidence interval, 1.32-1.36). There were higher rates of infections in the digestive tract; the ear, nose, and throat; the kidneys or urinary tract; the lower respiratory tract; and the nervous system.
Serious infections first appeared 9.7 (range, 3.9-21.3) months after a child stopped using a PPI – a date that Dr. Lassalle’s group determined on the basis of there being a delay of at least 90 days in filling a PPI prescription.
Possible confounders
“The study shows an association, it does not show causation,” said Rina Sanghavi, MD, a pediatric gastroenterologist at UT Southwestern Medical Center, Dallas. Dr. Sanghavi noted that the children who continued taking PPIs generally were sicker in their first year of life, as shown by the higher rates of respiratory ailments and corticosteroid use. This could mean that the infections they eventually experienced had many causes and not necessarily the PPI.
Similarly, pediatric gastroenterologist Sophia Patel, MD, of the Cleveland Clinic, pointed to the almost 10-month average lag time between stopping a PPI and developing a first serious infection. That interval is long enough that it is possible that the infection was caused by something else, Dr. Patel said.
Despite the limitations of the study, Dr. Sanghavi and Dr. Patel said the findings serve as a good reminder to clinicians to use PPIs only when needed and to limit their use once begun. The overall evidence base for limiting use of PPIs is strong, both physicians noted, even if this study does not show direct causation between PPI use and infection rates.
“Ask: Does this child need a PPI?” Dr. Sanghavi said. If so, she generally prescribes PPIs for a period of 2 weeks to a maximum of 2 months and she never authorizes automatic refills. Through this approach, a parent and child will come back to the clinic frequently, which in most cases allows faster tapering of the drugs.
Dr. Lassalle, Dr. Sanghavi, and Dr. Patel reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
Researchers in France are warning against the overzealous use of acid-suppressing drugs in infants after finding that the medications are associated with an increase in risk of serious infections later in life.
The focus on the use of proton pump inhibitors (PPIs) during infancy comes as use of the drugs in young children is rising in France, New Zealand, Scandinavia, and the United States. Much of this use is not to manage confirmed cases of gastroesophageal reflux but rather to soothe the jangled nerves of parents of babies in discomfort, according to the researchers, who have studied national prescribing patterns. In addition to concerns about infection, inappropriate or prolonged use of the acid suppressants is also associated with an increase in the risk of such conditions as hospital-acquired acute kidney injury and inflammatory bowel diseases in children.
PPIs such as omeprazole are effective at reducing gastric acid in babies with gastroesophageal reflux disease. But the researchers warned against using the drugs to manage normal spitting up and dribbling that would have resolved of itself anyway.
“In this study, increased risk of serious infections was associated with PPI use in young children, overall and for various sites and pathogens. In this population, PPIs should not be used without a clear indication,” epidemiologist Marion Lassalle, PharmD, PhD, of EPI-PHARE in Saint-Denis, France, and colleagues reported in JAMA Pediatrics.
Drawing on data from a national birth registry, Dr. Lassalle and colleagues compared infection rates among more than 1.2 million infants who received a PPI at an average age of 88 days with infection rates among children who received another kind of acid suppressant (a histamine receptor blocker or antacid) at an average age of 82 days. More than 600,000 children made up each group.
Slightly over half of the participants were boys, and the study followed children to a maximum age of 9 years. Among children who used PPIs rather than another acid suppressant, there was an overall higher rate of serious infections that required hospitalization (adjusted hazard ratio, 1.34; 95% confidence interval, 1.32-1.36). There were higher rates of infections in the digestive tract; the ear, nose, and throat; the kidneys or urinary tract; the lower respiratory tract; and the nervous system.
Serious infections first appeared 9.7 (range, 3.9-21.3) months after a child stopped using a PPI – a date that Dr. Lassalle’s group determined on the basis of there being a delay of at least 90 days in filling a PPI prescription.
Possible confounders
“The study shows an association, it does not show causation,” said Rina Sanghavi, MD, a pediatric gastroenterologist at UT Southwestern Medical Center, Dallas. Dr. Sanghavi noted that the children who continued taking PPIs generally were sicker in their first year of life, as shown by the higher rates of respiratory ailments and corticosteroid use. This could mean that the infections they eventually experienced had many causes and not necessarily the PPI.
Similarly, pediatric gastroenterologist Sophia Patel, MD, of the Cleveland Clinic, pointed to the almost 10-month average lag time between stopping a PPI and developing a first serious infection. That interval is long enough that it is possible that the infection was caused by something else, Dr. Patel said.
Despite the limitations of the study, Dr. Sanghavi and Dr. Patel said the findings serve as a good reminder to clinicians to use PPIs only when needed and to limit their use once begun. The overall evidence base for limiting use of PPIs is strong, both physicians noted, even if this study does not show direct causation between PPI use and infection rates.
“Ask: Does this child need a PPI?” Dr. Sanghavi said. If so, she generally prescribes PPIs for a period of 2 weeks to a maximum of 2 months and she never authorizes automatic refills. Through this approach, a parent and child will come back to the clinic frequently, which in most cases allows faster tapering of the drugs.
Dr. Lassalle, Dr. Sanghavi, and Dr. Patel reported no relevant financial conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA PEDIATRICS
Q&A: What to know about the new BA 2.86 COVID variant
The Centers for Disease Control and Prevention and the World Health Organization have dubbed the BA 2.86 variant of COVID-19 as a variant to watch.
So far, only 26 cases of “Pirola,” as the new variant is being called, have been identified: 10 in Denmark, four each in Sweden and the United States, three in South Africa, two in Portugal, and one each the United Kingdom, Israel, and Canada. BA 2.86 is a subvariant of Omicron, but according to reports from the CDC, the strain has many more mutations than the ones that came before it.
With so many facts still unknown about this new variant, this news organization asked experts what people need to be aware of as it continues to spread.
What is unique about the BA 2.86 variant?
“It is unique in that it has more than three mutations on the spike protein,” said Purvi S. Parikh, MD, an infectious disease expert at New York University’s Langone Health. The virus uses the spike proteins to enter our cells.
This “may mean it will be more transmissible, cause more severe disease, and/or our vaccines and treatments may not work as well, as compared to other variants,” she said.
What do we need to watch with BA 2.86 going forward?
“We don’t know if this variant will be associated with a change in the disease severity. We currently see increased numbers of cases in general, even though we don’t yet see the BA.2.86 in our system,” said Heba Mostafa, PhD, director of the molecular virology laboratory at Johns Hopkins Hospital in Baltimore.
“It is important to monitor BA.2.86 (and other variants) and understand how its evolution impacts the number of cases and disease outcomes,” she said. “We should all be aware of the current increase in cases, though, and try to get tested and be treated as soon as possible, as antivirals should be effective against the circulating variants.”
What should doctors know?
Dr. Parikh said doctors should generally expect more COVID cases in their clinics and make sure to screen patients even if their symptoms are mild.
“We have tools that can be used – antivirals like Paxlovid are still efficacious with current dominant strains such as EG.5,” she said. “And encourage your patients to get their boosters, mask, wash hands, and social distance.”
How well can our vaccines fight BA 2.86?
“Vaccine coverage for the BA.2.86 is an area of uncertainty right now,” said Dr. Mostafa.
In its report, the CDC said scientists are still figuring out how well the updated COVID vaccine works. It’s expected to be available in the fall, and for now, they believe the new shot will still make infections less severe, new variants and all.
Prior vaccinations and infections have created antibodies in many people, and that will likely provide some protection, Dr. Mostafa said. “When we experienced the Omicron wave in December 2021, even though the variant was distant from what circulated before its emergence and was associated with a very large increase in the number of cases, vaccinations were still protective against severe disease.”
What is the most important thing to keep track of when it comes to this variant?
According to Dr. Parikh, “it’s most important to monitor how transmissible [BA 2.86] is, how severe it is, and if our current treatments and vaccines work.”
Dr. Mostafa said how well the new variants escape existing antibody protection should also be studied and watched closely.
What does this stage of the virus mutation tell us about where we are in the pandemic?
The history of the coronavirus over the past few years shows that variants with many changes evolve and can spread very quickly, Dr. Mostafa said. “Now that the virus is endemic, it is essential to monitor, update vaccinations if necessary, diagnose, treat, and implement infection control measures when necessary.”
With the limited data we have so far, experts seem to agree that while the variant’s makeup raises some red flags, it is too soon to jump to any conclusions about how easy it is to catch it and the ways it may change how the virus impacts those who contract it.
A version of this article first appeared on WebMD.com.
The Centers for Disease Control and Prevention and the World Health Organization have dubbed the BA 2.86 variant of COVID-19 as a variant to watch.
So far, only 26 cases of “Pirola,” as the new variant is being called, have been identified: 10 in Denmark, four each in Sweden and the United States, three in South Africa, two in Portugal, and one each the United Kingdom, Israel, and Canada. BA 2.86 is a subvariant of Omicron, but according to reports from the CDC, the strain has many more mutations than the ones that came before it.
With so many facts still unknown about this new variant, this news organization asked experts what people need to be aware of as it continues to spread.
What is unique about the BA 2.86 variant?
“It is unique in that it has more than three mutations on the spike protein,” said Purvi S. Parikh, MD, an infectious disease expert at New York University’s Langone Health. The virus uses the spike proteins to enter our cells.
This “may mean it will be more transmissible, cause more severe disease, and/or our vaccines and treatments may not work as well, as compared to other variants,” she said.
What do we need to watch with BA 2.86 going forward?
“We don’t know if this variant will be associated with a change in the disease severity. We currently see increased numbers of cases in general, even though we don’t yet see the BA.2.86 in our system,” said Heba Mostafa, PhD, director of the molecular virology laboratory at Johns Hopkins Hospital in Baltimore.
“It is important to monitor BA.2.86 (and other variants) and understand how its evolution impacts the number of cases and disease outcomes,” she said. “We should all be aware of the current increase in cases, though, and try to get tested and be treated as soon as possible, as antivirals should be effective against the circulating variants.”
What should doctors know?
Dr. Parikh said doctors should generally expect more COVID cases in their clinics and make sure to screen patients even if their symptoms are mild.
“We have tools that can be used – antivirals like Paxlovid are still efficacious with current dominant strains such as EG.5,” she said. “And encourage your patients to get their boosters, mask, wash hands, and social distance.”
How well can our vaccines fight BA 2.86?
“Vaccine coverage for the BA.2.86 is an area of uncertainty right now,” said Dr. Mostafa.
In its report, the CDC said scientists are still figuring out how well the updated COVID vaccine works. It’s expected to be available in the fall, and for now, they believe the new shot will still make infections less severe, new variants and all.
Prior vaccinations and infections have created antibodies in many people, and that will likely provide some protection, Dr. Mostafa said. “When we experienced the Omicron wave in December 2021, even though the variant was distant from what circulated before its emergence and was associated with a very large increase in the number of cases, vaccinations were still protective against severe disease.”
What is the most important thing to keep track of when it comes to this variant?
According to Dr. Parikh, “it’s most important to monitor how transmissible [BA 2.86] is, how severe it is, and if our current treatments and vaccines work.”
Dr. Mostafa said how well the new variants escape existing antibody protection should also be studied and watched closely.
What does this stage of the virus mutation tell us about where we are in the pandemic?
The history of the coronavirus over the past few years shows that variants with many changes evolve and can spread very quickly, Dr. Mostafa said. “Now that the virus is endemic, it is essential to monitor, update vaccinations if necessary, diagnose, treat, and implement infection control measures when necessary.”
With the limited data we have so far, experts seem to agree that while the variant’s makeup raises some red flags, it is too soon to jump to any conclusions about how easy it is to catch it and the ways it may change how the virus impacts those who contract it.
A version of this article first appeared on WebMD.com.
The Centers for Disease Control and Prevention and the World Health Organization have dubbed the BA 2.86 variant of COVID-19 as a variant to watch.
So far, only 26 cases of “Pirola,” as the new variant is being called, have been identified: 10 in Denmark, four each in Sweden and the United States, three in South Africa, two in Portugal, and one each the United Kingdom, Israel, and Canada. BA 2.86 is a subvariant of Omicron, but according to reports from the CDC, the strain has many more mutations than the ones that came before it.
With so many facts still unknown about this new variant, this news organization asked experts what people need to be aware of as it continues to spread.
What is unique about the BA 2.86 variant?
“It is unique in that it has more than three mutations on the spike protein,” said Purvi S. Parikh, MD, an infectious disease expert at New York University’s Langone Health. The virus uses the spike proteins to enter our cells.
This “may mean it will be more transmissible, cause more severe disease, and/or our vaccines and treatments may not work as well, as compared to other variants,” she said.
What do we need to watch with BA 2.86 going forward?
“We don’t know if this variant will be associated with a change in the disease severity. We currently see increased numbers of cases in general, even though we don’t yet see the BA.2.86 in our system,” said Heba Mostafa, PhD, director of the molecular virology laboratory at Johns Hopkins Hospital in Baltimore.
“It is important to monitor BA.2.86 (and other variants) and understand how its evolution impacts the number of cases and disease outcomes,” she said. “We should all be aware of the current increase in cases, though, and try to get tested and be treated as soon as possible, as antivirals should be effective against the circulating variants.”
What should doctors know?
Dr. Parikh said doctors should generally expect more COVID cases in their clinics and make sure to screen patients even if their symptoms are mild.
“We have tools that can be used – antivirals like Paxlovid are still efficacious with current dominant strains such as EG.5,” she said. “And encourage your patients to get their boosters, mask, wash hands, and social distance.”
How well can our vaccines fight BA 2.86?
“Vaccine coverage for the BA.2.86 is an area of uncertainty right now,” said Dr. Mostafa.
In its report, the CDC said scientists are still figuring out how well the updated COVID vaccine works. It’s expected to be available in the fall, and for now, they believe the new shot will still make infections less severe, new variants and all.
Prior vaccinations and infections have created antibodies in many people, and that will likely provide some protection, Dr. Mostafa said. “When we experienced the Omicron wave in December 2021, even though the variant was distant from what circulated before its emergence and was associated with a very large increase in the number of cases, vaccinations were still protective against severe disease.”
What is the most important thing to keep track of when it comes to this variant?
According to Dr. Parikh, “it’s most important to monitor how transmissible [BA 2.86] is, how severe it is, and if our current treatments and vaccines work.”
Dr. Mostafa said how well the new variants escape existing antibody protection should also be studied and watched closely.
What does this stage of the virus mutation tell us about where we are in the pandemic?
The history of the coronavirus over the past few years shows that variants with many changes evolve and can spread very quickly, Dr. Mostafa said. “Now that the virus is endemic, it is essential to monitor, update vaccinations if necessary, diagnose, treat, and implement infection control measures when necessary.”
With the limited data we have so far, experts seem to agree that while the variant’s makeup raises some red flags, it is too soon to jump to any conclusions about how easy it is to catch it and the ways it may change how the virus impacts those who contract it.
A version of this article first appeared on WebMD.com.
Young vapers and smokers beware: Eye problems abound
Adolescents and young adults who smoked and vaped were more likely to report ocular problems including dryness, redness, pain, blurry vision, light sensitivity, and headaches, according to an observational study published in JAMA Ophthalmology.
Eye symptoms were significantly worse among young people who reported using both cigarettes and e-cigarettes than for those who said they used only one of the products, according to researchers. Symptoms were particularly frequent and severe among those who had used both products in the prior week.
“In ophthalmology clinics, I’ve increasingly noticed patients, particularly adolescents and young adults, presenting with eye-related symptoms such as dryness, irritation, and even vision disturbances,” said Anne Xuan-Lan Nguyen, MDCM, an ophthalmology resident at the University of Toronto, who led the study.
Many of these patients said they did not use contact lenses or take medications associated with eye problems, but they did report a history of using e-cigarettes and cigarettes.
This “sparked my curiosity about the possible link between smoking or vaping and ocular symptoms,” Dr. Nguyen, who conducted the research as a medical student at McGill University in Montreal, told this news organization.
E-cigarettes are the most popular tobacco product among young people. Public health data show an increasing trend toward both vaping and smoking cigarettes, known as dual use. An estimated 40% of middle- and high school–aged tobacco users report using two or more tobacco products, according to the Centers for Disease Control and Prevention. Cigarette use has been linked to ocular damage, but the effects of e-cigarettes on eyesight and the combined effect with cigarettes are not as well known.
Dr. Nguyen and her colleagues surveyed more than 4,000 people aged 13-24 about their use of cigarettes or e-cigarettes in the last 30 days, the last 7 days, or ever. Half said they had never used any tobacco product and one quarter reported having used cigarettes, vapes, or both in the last month. More than 900 respondents said they had used one or both tobacco products in the last week.
Of the respondents who had ever vaped, 55.9% said they also used cigarettes. These dual users reported more severe and frequent eye symptoms compared with users of either product alone. Up to 4% of respondents who had ever been a dual user reported daily, severe, or very severe ocular symptoms – more than in the cigarette-only or e-cigarette-only groups.
More frequent tobacco use also was associated with more ocular symptoms. Young people who smoked or vaped in the previous week reported more symptoms than did the 30-day group, who reported more symptoms than the ever-user group (those who had taken at least a puff but not in the last month).
“All these conditions we know are worse as you get older,” said Laura B. Enyedi, MD, pediatric ophthalmologist at the Duke Eye Center in Durham, N.C., who was not associated with the study. “So if young people are having symptoms, it doesn’t bode well for them as they age.”
E-cigarette use alone did not appear to be linked to eye ailments, according to the findings. But to Dr. Nguyen’s surprise the survey results showed users of vaping products spent the most time worried about their eye health compared with all other participants. Users who smoked only cigarettes reported ocular symptoms, but not as severe or frequent as those of dual users.
The researchers hypothesized that ocular problems caused by vapes and cigarettes could be classified as oxidative damage. The combustion of the cigarette and the e-cigarette solvent (propylene glycol) potentially generates free radicals that can cause oxidative stress, damaging the ocular surface and film, Dr. Nguyen said.
Ophthalmologists are “always asking about contact lens use, lid hygiene, and screen time. Here’s another thing to consider when we get those common, nonspecific complaints of symptoms like dryness, redness, and burning,” Dr. Enyedi said.
Given the observational nature of the study, the researchers cannot confirm that dual use causes ocular symptoms. But given the public health challenge that tobacco use already presents for young people, the findings provide yet another reason to counsel against tobacco use and provide cessation options, Dr. Nguyen said.
“This study is just one of many, many studies showing a significant relationship among smoking, e-cigarette use, and health outcomes,” said Bonnie Halpern-Felsher, PhD, professor of pediatrics at Stanford (Calif.) University and a coauthor of the study. “We clearly need to help young people not use at all, or quit or cut back if using.”
This study was supported by the Taube Research Faculty Scholar Endowment; the National Heart, Lung, and Blood Institute; the Food and Drug Administration Center for Tobacco Products; the National Cancer Institute; the Stanford Maternal and Child Health Research Institute; and the Research to Prevent Blindness and National Eye Institute. Dr. Halpern-Felsher reported receiving personal fees as an expert scientist in litigation against some e-cigarette companies. The other study authors and Dr. Enyedi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adolescents and young adults who smoked and vaped were more likely to report ocular problems including dryness, redness, pain, blurry vision, light sensitivity, and headaches, according to an observational study published in JAMA Ophthalmology.
Eye symptoms were significantly worse among young people who reported using both cigarettes and e-cigarettes than for those who said they used only one of the products, according to researchers. Symptoms were particularly frequent and severe among those who had used both products in the prior week.
“In ophthalmology clinics, I’ve increasingly noticed patients, particularly adolescents and young adults, presenting with eye-related symptoms such as dryness, irritation, and even vision disturbances,” said Anne Xuan-Lan Nguyen, MDCM, an ophthalmology resident at the University of Toronto, who led the study.
Many of these patients said they did not use contact lenses or take medications associated with eye problems, but they did report a history of using e-cigarettes and cigarettes.
This “sparked my curiosity about the possible link between smoking or vaping and ocular symptoms,” Dr. Nguyen, who conducted the research as a medical student at McGill University in Montreal, told this news organization.
E-cigarettes are the most popular tobacco product among young people. Public health data show an increasing trend toward both vaping and smoking cigarettes, known as dual use. An estimated 40% of middle- and high school–aged tobacco users report using two or more tobacco products, according to the Centers for Disease Control and Prevention. Cigarette use has been linked to ocular damage, but the effects of e-cigarettes on eyesight and the combined effect with cigarettes are not as well known.
Dr. Nguyen and her colleagues surveyed more than 4,000 people aged 13-24 about their use of cigarettes or e-cigarettes in the last 30 days, the last 7 days, or ever. Half said they had never used any tobacco product and one quarter reported having used cigarettes, vapes, or both in the last month. More than 900 respondents said they had used one or both tobacco products in the last week.
Of the respondents who had ever vaped, 55.9% said they also used cigarettes. These dual users reported more severe and frequent eye symptoms compared with users of either product alone. Up to 4% of respondents who had ever been a dual user reported daily, severe, or very severe ocular symptoms – more than in the cigarette-only or e-cigarette-only groups.
More frequent tobacco use also was associated with more ocular symptoms. Young people who smoked or vaped in the previous week reported more symptoms than did the 30-day group, who reported more symptoms than the ever-user group (those who had taken at least a puff but not in the last month).
“All these conditions we know are worse as you get older,” said Laura B. Enyedi, MD, pediatric ophthalmologist at the Duke Eye Center in Durham, N.C., who was not associated with the study. “So if young people are having symptoms, it doesn’t bode well for them as they age.”
E-cigarette use alone did not appear to be linked to eye ailments, according to the findings. But to Dr. Nguyen’s surprise the survey results showed users of vaping products spent the most time worried about their eye health compared with all other participants. Users who smoked only cigarettes reported ocular symptoms, but not as severe or frequent as those of dual users.
The researchers hypothesized that ocular problems caused by vapes and cigarettes could be classified as oxidative damage. The combustion of the cigarette and the e-cigarette solvent (propylene glycol) potentially generates free radicals that can cause oxidative stress, damaging the ocular surface and film, Dr. Nguyen said.
Ophthalmologists are “always asking about contact lens use, lid hygiene, and screen time. Here’s another thing to consider when we get those common, nonspecific complaints of symptoms like dryness, redness, and burning,” Dr. Enyedi said.
Given the observational nature of the study, the researchers cannot confirm that dual use causes ocular symptoms. But given the public health challenge that tobacco use already presents for young people, the findings provide yet another reason to counsel against tobacco use and provide cessation options, Dr. Nguyen said.
“This study is just one of many, many studies showing a significant relationship among smoking, e-cigarette use, and health outcomes,” said Bonnie Halpern-Felsher, PhD, professor of pediatrics at Stanford (Calif.) University and a coauthor of the study. “We clearly need to help young people not use at all, or quit or cut back if using.”
This study was supported by the Taube Research Faculty Scholar Endowment; the National Heart, Lung, and Blood Institute; the Food and Drug Administration Center for Tobacco Products; the National Cancer Institute; the Stanford Maternal and Child Health Research Institute; and the Research to Prevent Blindness and National Eye Institute. Dr. Halpern-Felsher reported receiving personal fees as an expert scientist in litigation against some e-cigarette companies. The other study authors and Dr. Enyedi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adolescents and young adults who smoked and vaped were more likely to report ocular problems including dryness, redness, pain, blurry vision, light sensitivity, and headaches, according to an observational study published in JAMA Ophthalmology.
Eye symptoms were significantly worse among young people who reported using both cigarettes and e-cigarettes than for those who said they used only one of the products, according to researchers. Symptoms were particularly frequent and severe among those who had used both products in the prior week.
“In ophthalmology clinics, I’ve increasingly noticed patients, particularly adolescents and young adults, presenting with eye-related symptoms such as dryness, irritation, and even vision disturbances,” said Anne Xuan-Lan Nguyen, MDCM, an ophthalmology resident at the University of Toronto, who led the study.
Many of these patients said they did not use contact lenses or take medications associated with eye problems, but they did report a history of using e-cigarettes and cigarettes.
This “sparked my curiosity about the possible link between smoking or vaping and ocular symptoms,” Dr. Nguyen, who conducted the research as a medical student at McGill University in Montreal, told this news organization.
E-cigarettes are the most popular tobacco product among young people. Public health data show an increasing trend toward both vaping and smoking cigarettes, known as dual use. An estimated 40% of middle- and high school–aged tobacco users report using two or more tobacco products, according to the Centers for Disease Control and Prevention. Cigarette use has been linked to ocular damage, but the effects of e-cigarettes on eyesight and the combined effect with cigarettes are not as well known.
Dr. Nguyen and her colleagues surveyed more than 4,000 people aged 13-24 about their use of cigarettes or e-cigarettes in the last 30 days, the last 7 days, or ever. Half said they had never used any tobacco product and one quarter reported having used cigarettes, vapes, or both in the last month. More than 900 respondents said they had used one or both tobacco products in the last week.
Of the respondents who had ever vaped, 55.9% said they also used cigarettes. These dual users reported more severe and frequent eye symptoms compared with users of either product alone. Up to 4% of respondents who had ever been a dual user reported daily, severe, or very severe ocular symptoms – more than in the cigarette-only or e-cigarette-only groups.
More frequent tobacco use also was associated with more ocular symptoms. Young people who smoked or vaped in the previous week reported more symptoms than did the 30-day group, who reported more symptoms than the ever-user group (those who had taken at least a puff but not in the last month).
“All these conditions we know are worse as you get older,” said Laura B. Enyedi, MD, pediatric ophthalmologist at the Duke Eye Center in Durham, N.C., who was not associated with the study. “So if young people are having symptoms, it doesn’t bode well for them as they age.”
E-cigarette use alone did not appear to be linked to eye ailments, according to the findings. But to Dr. Nguyen’s surprise the survey results showed users of vaping products spent the most time worried about their eye health compared with all other participants. Users who smoked only cigarettes reported ocular symptoms, but not as severe or frequent as those of dual users.
The researchers hypothesized that ocular problems caused by vapes and cigarettes could be classified as oxidative damage. The combustion of the cigarette and the e-cigarette solvent (propylene glycol) potentially generates free radicals that can cause oxidative stress, damaging the ocular surface and film, Dr. Nguyen said.
Ophthalmologists are “always asking about contact lens use, lid hygiene, and screen time. Here’s another thing to consider when we get those common, nonspecific complaints of symptoms like dryness, redness, and burning,” Dr. Enyedi said.
Given the observational nature of the study, the researchers cannot confirm that dual use causes ocular symptoms. But given the public health challenge that tobacco use already presents for young people, the findings provide yet another reason to counsel against tobacco use and provide cessation options, Dr. Nguyen said.
“This study is just one of many, many studies showing a significant relationship among smoking, e-cigarette use, and health outcomes,” said Bonnie Halpern-Felsher, PhD, professor of pediatrics at Stanford (Calif.) University and a coauthor of the study. “We clearly need to help young people not use at all, or quit or cut back if using.”
This study was supported by the Taube Research Faculty Scholar Endowment; the National Heart, Lung, and Blood Institute; the Food and Drug Administration Center for Tobacco Products; the National Cancer Institute; the Stanford Maternal and Child Health Research Institute; and the Research to Prevent Blindness and National Eye Institute. Dr. Halpern-Felsher reported receiving personal fees as an expert scientist in litigation against some e-cigarette companies. The other study authors and Dr. Enyedi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA OPHTHALMOLOGY
PsA Complications
New guideline for managing toothache in children
Nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, or both medications together can effectively manage a child’s toothache as a stopgap until definitive treatment is available, according to a new guideline.
The guideline, published in the September issue of the Journal of the American Dental Association, does not recommend opioids for a toothache or after tooth extraction in this population.
Opioid prescriptions for children entail risk for hospitalization and death. Yet, some dentists continued to prescribe contraindicated opioids to young children after a Food and Drug Administration warning in 2017 about the use of tramadol and codeine in this population, the guideline notes.
Opioid prescribing to children also continued after the American Academy of Pediatric Dentistry in 2018 recommended acetaminophen and NSAIDs as first-line medications for pain management and said that the use of opioids should be “rare.”
Although the new guidance, which also covers pain management after tooth extraction, is geared toward general dentists, it could help emergency clinicians and primary care providers manage children’s pain when definitive treatment is not immediately available, the authors noted.
Definitive treatment could include pulpectomy, nonsurgical root canal, incision for drainage of an abscess, or tooth extraction.
If definitive care in 2-3 days is not possible, parents should let the health care team know, the guideline says.
“These pharmacologic strategies will alleviate dental pain temporarily until a referral for definitive dental treatment is in place,” the authors wrote.
The American Dental Association (ADA) endorsed the new guideline, which was developed by researchers with the ADA Science & Research Institute, the University of Pittsburgh School of Dental Medicine, and the Center for Integrative Global Oral Health at the University of Pennsylvania School of Dental Medicine in Philadelphia.
The guideline recommends ibuprofen and, for children older than 2 years, naproxen as NSAID options. The use of naproxen in children younger than 12 years for this purpose is off label, they noted.
The guideline suggests doses of acetaminophen and NSAIDs on the basis of age and weight that may differ from those on medication packaging.
“When acetaminophen or NSAIDs are administered as directed, the risk of harm to children from either medication is low,” the guideline states.
“While prescribing opioids to children has become less frequent overall, this guideline ensures that both dentists and parents have evidence-based recommendations to determine the most appropriate treatment for dental pain,” senior guideline author Paul Moore, DMD, PhD, MPH, professor emeritus at the University of Pittsburgh’s School of Dental Medicine, said in a news release from the ADA. “Parents and caregivers can take comfort that widely available medications that have no abuse potential, such as acetaminophen or ibuprofen, are safe and effective for helping their children find relief from short-term dental pain.”
A 2018 review by Dr. Moore and coauthors found that NSAIDs, with or without acetaminophen, were effective and minimized adverse events, relative to opioids, for acute dental pain across ages.
The new recommendations for children will “allow for better treatment of this kind of pain” and “will help prevent unnecessary prescribing of medications with abuse potential, including opioids,” Patrizia Cavazzoni, MD, director of the FDA Center for Drug Evaluation and Research, said in the news release.
The report stems from a 3-year, $1.5 million grant awarded by the FDA in 2020 to the University of Pittsburgh and the ADA Science & Research Institute to develop a clinical practice guideline for the management of acute pain in dentistry in children, adolescents, and adults. The recommendations for adolescents and adults are still in development.
The report was supported by an FDA grant, and the guideline authors received technical and methodologic support from the agency. Some authors disclosed ties to pharmaceutical companies.
A version of this article appeared on Medscape.com.
Nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, or both medications together can effectively manage a child’s toothache as a stopgap until definitive treatment is available, according to a new guideline.
The guideline, published in the September issue of the Journal of the American Dental Association, does not recommend opioids for a toothache or after tooth extraction in this population.
Opioid prescriptions for children entail risk for hospitalization and death. Yet, some dentists continued to prescribe contraindicated opioids to young children after a Food and Drug Administration warning in 2017 about the use of tramadol and codeine in this population, the guideline notes.
Opioid prescribing to children also continued after the American Academy of Pediatric Dentistry in 2018 recommended acetaminophen and NSAIDs as first-line medications for pain management and said that the use of opioids should be “rare.”
Although the new guidance, which also covers pain management after tooth extraction, is geared toward general dentists, it could help emergency clinicians and primary care providers manage children’s pain when definitive treatment is not immediately available, the authors noted.
Definitive treatment could include pulpectomy, nonsurgical root canal, incision for drainage of an abscess, or tooth extraction.
If definitive care in 2-3 days is not possible, parents should let the health care team know, the guideline says.
“These pharmacologic strategies will alleviate dental pain temporarily until a referral for definitive dental treatment is in place,” the authors wrote.
The American Dental Association (ADA) endorsed the new guideline, which was developed by researchers with the ADA Science & Research Institute, the University of Pittsburgh School of Dental Medicine, and the Center for Integrative Global Oral Health at the University of Pennsylvania School of Dental Medicine in Philadelphia.
The guideline recommends ibuprofen and, for children older than 2 years, naproxen as NSAID options. The use of naproxen in children younger than 12 years for this purpose is off label, they noted.
The guideline suggests doses of acetaminophen and NSAIDs on the basis of age and weight that may differ from those on medication packaging.
“When acetaminophen or NSAIDs are administered as directed, the risk of harm to children from either medication is low,” the guideline states.
“While prescribing opioids to children has become less frequent overall, this guideline ensures that both dentists and parents have evidence-based recommendations to determine the most appropriate treatment for dental pain,” senior guideline author Paul Moore, DMD, PhD, MPH, professor emeritus at the University of Pittsburgh’s School of Dental Medicine, said in a news release from the ADA. “Parents and caregivers can take comfort that widely available medications that have no abuse potential, such as acetaminophen or ibuprofen, are safe and effective for helping their children find relief from short-term dental pain.”
A 2018 review by Dr. Moore and coauthors found that NSAIDs, with or without acetaminophen, were effective and minimized adverse events, relative to opioids, for acute dental pain across ages.
The new recommendations for children will “allow for better treatment of this kind of pain” and “will help prevent unnecessary prescribing of medications with abuse potential, including opioids,” Patrizia Cavazzoni, MD, director of the FDA Center for Drug Evaluation and Research, said in the news release.
The report stems from a 3-year, $1.5 million grant awarded by the FDA in 2020 to the University of Pittsburgh and the ADA Science & Research Institute to develop a clinical practice guideline for the management of acute pain in dentistry in children, adolescents, and adults. The recommendations for adolescents and adults are still in development.
The report was supported by an FDA grant, and the guideline authors received technical and methodologic support from the agency. Some authors disclosed ties to pharmaceutical companies.
A version of this article appeared on Medscape.com.
Nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, or both medications together can effectively manage a child’s toothache as a stopgap until definitive treatment is available, according to a new guideline.
The guideline, published in the September issue of the Journal of the American Dental Association, does not recommend opioids for a toothache or after tooth extraction in this population.
Opioid prescriptions for children entail risk for hospitalization and death. Yet, some dentists continued to prescribe contraindicated opioids to young children after a Food and Drug Administration warning in 2017 about the use of tramadol and codeine in this population, the guideline notes.
Opioid prescribing to children also continued after the American Academy of Pediatric Dentistry in 2018 recommended acetaminophen and NSAIDs as first-line medications for pain management and said that the use of opioids should be “rare.”
Although the new guidance, which also covers pain management after tooth extraction, is geared toward general dentists, it could help emergency clinicians and primary care providers manage children’s pain when definitive treatment is not immediately available, the authors noted.
Definitive treatment could include pulpectomy, nonsurgical root canal, incision for drainage of an abscess, or tooth extraction.
If definitive care in 2-3 days is not possible, parents should let the health care team know, the guideline says.
“These pharmacologic strategies will alleviate dental pain temporarily until a referral for definitive dental treatment is in place,” the authors wrote.
The American Dental Association (ADA) endorsed the new guideline, which was developed by researchers with the ADA Science & Research Institute, the University of Pittsburgh School of Dental Medicine, and the Center for Integrative Global Oral Health at the University of Pennsylvania School of Dental Medicine in Philadelphia.
The guideline recommends ibuprofen and, for children older than 2 years, naproxen as NSAID options. The use of naproxen in children younger than 12 years for this purpose is off label, they noted.
The guideline suggests doses of acetaminophen and NSAIDs on the basis of age and weight that may differ from those on medication packaging.
“When acetaminophen or NSAIDs are administered as directed, the risk of harm to children from either medication is low,” the guideline states.
“While prescribing opioids to children has become less frequent overall, this guideline ensures that both dentists and parents have evidence-based recommendations to determine the most appropriate treatment for dental pain,” senior guideline author Paul Moore, DMD, PhD, MPH, professor emeritus at the University of Pittsburgh’s School of Dental Medicine, said in a news release from the ADA. “Parents and caregivers can take comfort that widely available medications that have no abuse potential, such as acetaminophen or ibuprofen, are safe and effective for helping their children find relief from short-term dental pain.”
A 2018 review by Dr. Moore and coauthors found that NSAIDs, with or without acetaminophen, were effective and minimized adverse events, relative to opioids, for acute dental pain across ages.
The new recommendations for children will “allow for better treatment of this kind of pain” and “will help prevent unnecessary prescribing of medications with abuse potential, including opioids,” Patrizia Cavazzoni, MD, director of the FDA Center for Drug Evaluation and Research, said in the news release.
The report stems from a 3-year, $1.5 million grant awarded by the FDA in 2020 to the University of Pittsburgh and the ADA Science & Research Institute to develop a clinical practice guideline for the management of acute pain in dentistry in children, adolescents, and adults. The recommendations for adolescents and adults are still in development.
The report was supported by an FDA grant, and the guideline authors received technical and methodologic support from the agency. Some authors disclosed ties to pharmaceutical companies.
A version of this article appeared on Medscape.com.
Unlocking the secrets of brown fat
Brown fat, or thermogenic adipose tissue, appears to act as a “nutrient sink,” consuming glucose and lactate, among other metabolites, say U.S. researchers in a mouse study that supports its potential role in tackling obesity and even cancer.
The research, published recently in Nature Metabolism, was led by David A. Guertin, PhD, of the program in molecular medicine, University of Massachusetts, Worcester.
What is adaptive thermogenesis, and why is it important in temperature regulation?
Adaptive thermogenesis is a physiologic process that occurs in a special type of fat cell, called a brown adipocyte, in which intracellular stored lipids and nutrients taken up from the blood are catabolized to generate heat.
The heat generated by these thermogenic adipocytes is critical for warming the blood and maintaining body temperature in cold environments, and is especially critical in human infants and small mammals, which are more sensitive to low temperatures.
The process is stimulated by the sympathetic nervous system, especially in response to feeling cold, but it can be activated by other stresses as well.
While adaptative thermogenesis is also called nonshivering thermogenesis to distinguish it from muscle shivering, both means of generating heat can work together to maintain body temperature.
Why is it considered a potential target for obesity?
Adult humans have brown adipocytes in specific locations in the body called brown adipose tissues (BAT) or, more simply, “brown fat.”
Intriguingly, clinical data show that the more BAT you have, the more likely you are to be protected against cardiometabolic disorders associated with obesity.
Since obesity results from an imbalance between energy intake and energy expenditure, one model proposes that brown adipocytes rebalance this formula by expending the excess energy (calories) as heat rather than storing it.
This has been referred to as the “nutrient sink” model, and the ability to activate this process therapeutically is a very attractive antiobesity strategy.
Why was it important to understand which circulating metabolites BAT uses for thermogenesis?
It is still not clear why brown fat is so beneficial for human health, and thus there is strong rationale for understanding its metabolism and how it cooperates with other tissues in the body.
For example, prior to our work, the field lacked a broad quantitative picture of how much any individual nutrient from the blood was used by brown fat, or which specific nutrients brown fat prefers to use to make heat – such as lipids, glucose, amino acids, etc. Knowing this information helps us identify more precise strategies to activate brown fat.
In addition, circulating metabolites sometimes also have messenger functions, similar to those of hormones, that stimulate physiologic processes such as adaptative thermogenesis. Highly metabolic tissues also put metabolites back into the blood, which can send messages to the brain and other tissues.
We don’t have a lot of information yet on how brown fat might engage in these processes, and so our study also aimed at finding these special metabolite messengers.
You found that glucose and lactate predominate as BAT fuel sources. What does that tell us?
The major fuels used by brown fat have been debated for a long time.
Our study suggests that BAT in mice mainly prefers glucose and lactate, which is generated from glucose. On one hand, this shows us that thermogenic adipocytes may be especially useful in treating hyperglycemia, or even tumors, by reducing the amount of circulating glucose.
It also tells us that we need to focus more on why brown fat needs so much glucose. Other studies suggest that glucose is not just used as a fuel to generate heat but also may have other important functions in keeping brown adipocytes active and healthy.
We need to know that information so that therapeutic strategies targeting brown adipocytes can be optimized to have the best chance of success.
It’s worth noting that we did our study in mice that had free access to food. If the mice were fasting, they would use more lipids from the blood to supplement for the lack of available glucose, but we think that a baseline amount of glucose is still necessary.
What could be the clinical implications of your results if replicated in humans?
They suggest that glucose is an important resource that thermogenic adipocytes cannot do without, and moreover, that glucose is more than just a carbon source.
Resolving those other functions of glucose may provide insight into mechanisms to stimulate these cells or help explain why overweight or obese people who are insulin resistant have less brown fat activity, as insulin stimulates glucose uptake.
Beyond glucose, if any of these other metabolites made or released by brown fat have beneficial messenger functions, there may be ways to pharmacologically mimic them.
How easily do you think your findings could be applied to humans?
On a fundamental level, the basic cellular mechanisms that drive adaptative thermogenesis are likely the same between mice and humans, but the wiring to the sympathetic nervous system is a bit different.
This is why it’s important to look deeply at brown fat metabolism in mouse models to find pathways fundamental to the basic mechanisms of adaptative thermogenesis in both mice and humans, which could reveal unique therapeutic opportunities.
Another big challenge with comparing humans and mice is that humans typically keep their environment warm, so their brown fat is not that active.
In contrast, mice are often raised their entire lives in a facility kept at room temperature, around 22° C (72° F). While comfortable for the humans working with them, it’s cold for a small mouse, and so mice live with constantly active brown fat.
We can change the mouse environment to alter mouse brown fat activity, but that can’t be done with people. This makes comparative studies difficult.
Nevertheless, studies have shown that people who live in cold climates often have more brown fat, and, conversely, mice raised in warmer environments have brown fat that looks a lot more like human brown fat.
What further research do you have planned, or are looking forward to, in this area?
This is the most fun part of what we do, and I’ve been fortunate to have an amazing team passionately working on these questions.
One is to figure out why glucose is so important for these fascinating cells, which will keep us busy for years. We also need to modify the dietary conditions to determine whether the body prioritizes the use of glucose for adaptive thermogenesis even when there isn’t much available.
Another goal is to test whether any of the other metabolites we identified have bioactive functions. We also discovered a unique role for glutamine metabolism in brown fat, through the consumption of amino acids, that we haven’t yet resolved.
Finally, we want to understand how and why brown fat protects other organs from metabolic diseases, and we are just at the tip of the iceberg here.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Alcohol Abuse and Alcoholism; the National Heart, Lung, & Blood Institute; the National Institutes of Health; the AASLD Foundation Pinnacle Research Award in Liver Disease; the Edward Mallinckrodt Jr. Foundation Award; and the Basic Science Research Program of the Ministry of Education (South Korea). No relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
Brown fat, or thermogenic adipose tissue, appears to act as a “nutrient sink,” consuming glucose and lactate, among other metabolites, say U.S. researchers in a mouse study that supports its potential role in tackling obesity and even cancer.
The research, published recently in Nature Metabolism, was led by David A. Guertin, PhD, of the program in molecular medicine, University of Massachusetts, Worcester.
What is adaptive thermogenesis, and why is it important in temperature regulation?
Adaptive thermogenesis is a physiologic process that occurs in a special type of fat cell, called a brown adipocyte, in which intracellular stored lipids and nutrients taken up from the blood are catabolized to generate heat.
The heat generated by these thermogenic adipocytes is critical for warming the blood and maintaining body temperature in cold environments, and is especially critical in human infants and small mammals, which are more sensitive to low temperatures.
The process is stimulated by the sympathetic nervous system, especially in response to feeling cold, but it can be activated by other stresses as well.
While adaptative thermogenesis is also called nonshivering thermogenesis to distinguish it from muscle shivering, both means of generating heat can work together to maintain body temperature.
Why is it considered a potential target for obesity?
Adult humans have brown adipocytes in specific locations in the body called brown adipose tissues (BAT) or, more simply, “brown fat.”
Intriguingly, clinical data show that the more BAT you have, the more likely you are to be protected against cardiometabolic disorders associated with obesity.
Since obesity results from an imbalance between energy intake and energy expenditure, one model proposes that brown adipocytes rebalance this formula by expending the excess energy (calories) as heat rather than storing it.
This has been referred to as the “nutrient sink” model, and the ability to activate this process therapeutically is a very attractive antiobesity strategy.
Why was it important to understand which circulating metabolites BAT uses for thermogenesis?
It is still not clear why brown fat is so beneficial for human health, and thus there is strong rationale for understanding its metabolism and how it cooperates with other tissues in the body.
For example, prior to our work, the field lacked a broad quantitative picture of how much any individual nutrient from the blood was used by brown fat, or which specific nutrients brown fat prefers to use to make heat – such as lipids, glucose, amino acids, etc. Knowing this information helps us identify more precise strategies to activate brown fat.
In addition, circulating metabolites sometimes also have messenger functions, similar to those of hormones, that stimulate physiologic processes such as adaptative thermogenesis. Highly metabolic tissues also put metabolites back into the blood, which can send messages to the brain and other tissues.
We don’t have a lot of information yet on how brown fat might engage in these processes, and so our study also aimed at finding these special metabolite messengers.
You found that glucose and lactate predominate as BAT fuel sources. What does that tell us?
The major fuels used by brown fat have been debated for a long time.
Our study suggests that BAT in mice mainly prefers glucose and lactate, which is generated from glucose. On one hand, this shows us that thermogenic adipocytes may be especially useful in treating hyperglycemia, or even tumors, by reducing the amount of circulating glucose.
It also tells us that we need to focus more on why brown fat needs so much glucose. Other studies suggest that glucose is not just used as a fuel to generate heat but also may have other important functions in keeping brown adipocytes active and healthy.
We need to know that information so that therapeutic strategies targeting brown adipocytes can be optimized to have the best chance of success.
It’s worth noting that we did our study in mice that had free access to food. If the mice were fasting, they would use more lipids from the blood to supplement for the lack of available glucose, but we think that a baseline amount of glucose is still necessary.
What could be the clinical implications of your results if replicated in humans?
They suggest that glucose is an important resource that thermogenic adipocytes cannot do without, and moreover, that glucose is more than just a carbon source.
Resolving those other functions of glucose may provide insight into mechanisms to stimulate these cells or help explain why overweight or obese people who are insulin resistant have less brown fat activity, as insulin stimulates glucose uptake.
Beyond glucose, if any of these other metabolites made or released by brown fat have beneficial messenger functions, there may be ways to pharmacologically mimic them.
How easily do you think your findings could be applied to humans?
On a fundamental level, the basic cellular mechanisms that drive adaptative thermogenesis are likely the same between mice and humans, but the wiring to the sympathetic nervous system is a bit different.
This is why it’s important to look deeply at brown fat metabolism in mouse models to find pathways fundamental to the basic mechanisms of adaptative thermogenesis in both mice and humans, which could reveal unique therapeutic opportunities.
Another big challenge with comparing humans and mice is that humans typically keep their environment warm, so their brown fat is not that active.
In contrast, mice are often raised their entire lives in a facility kept at room temperature, around 22° C (72° F). While comfortable for the humans working with them, it’s cold for a small mouse, and so mice live with constantly active brown fat.
We can change the mouse environment to alter mouse brown fat activity, but that can’t be done with people. This makes comparative studies difficult.
Nevertheless, studies have shown that people who live in cold climates often have more brown fat, and, conversely, mice raised in warmer environments have brown fat that looks a lot more like human brown fat.
What further research do you have planned, or are looking forward to, in this area?
This is the most fun part of what we do, and I’ve been fortunate to have an amazing team passionately working on these questions.
One is to figure out why glucose is so important for these fascinating cells, which will keep us busy for years. We also need to modify the dietary conditions to determine whether the body prioritizes the use of glucose for adaptive thermogenesis even when there isn’t much available.
Another goal is to test whether any of the other metabolites we identified have bioactive functions. We also discovered a unique role for glutamine metabolism in brown fat, through the consumption of amino acids, that we haven’t yet resolved.
Finally, we want to understand how and why brown fat protects other organs from metabolic diseases, and we are just at the tip of the iceberg here.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Alcohol Abuse and Alcoholism; the National Heart, Lung, & Blood Institute; the National Institutes of Health; the AASLD Foundation Pinnacle Research Award in Liver Disease; the Edward Mallinckrodt Jr. Foundation Award; and the Basic Science Research Program of the Ministry of Education (South Korea). No relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
Brown fat, or thermogenic adipose tissue, appears to act as a “nutrient sink,” consuming glucose and lactate, among other metabolites, say U.S. researchers in a mouse study that supports its potential role in tackling obesity and even cancer.
The research, published recently in Nature Metabolism, was led by David A. Guertin, PhD, of the program in molecular medicine, University of Massachusetts, Worcester.
What is adaptive thermogenesis, and why is it important in temperature regulation?
Adaptive thermogenesis is a physiologic process that occurs in a special type of fat cell, called a brown adipocyte, in which intracellular stored lipids and nutrients taken up from the blood are catabolized to generate heat.
The heat generated by these thermogenic adipocytes is critical for warming the blood and maintaining body temperature in cold environments, and is especially critical in human infants and small mammals, which are more sensitive to low temperatures.
The process is stimulated by the sympathetic nervous system, especially in response to feeling cold, but it can be activated by other stresses as well.
While adaptative thermogenesis is also called nonshivering thermogenesis to distinguish it from muscle shivering, both means of generating heat can work together to maintain body temperature.
Why is it considered a potential target for obesity?
Adult humans have brown adipocytes in specific locations in the body called brown adipose tissues (BAT) or, more simply, “brown fat.”
Intriguingly, clinical data show that the more BAT you have, the more likely you are to be protected against cardiometabolic disorders associated with obesity.
Since obesity results from an imbalance between energy intake and energy expenditure, one model proposes that brown adipocytes rebalance this formula by expending the excess energy (calories) as heat rather than storing it.
This has been referred to as the “nutrient sink” model, and the ability to activate this process therapeutically is a very attractive antiobesity strategy.
Why was it important to understand which circulating metabolites BAT uses for thermogenesis?
It is still not clear why brown fat is so beneficial for human health, and thus there is strong rationale for understanding its metabolism and how it cooperates with other tissues in the body.
For example, prior to our work, the field lacked a broad quantitative picture of how much any individual nutrient from the blood was used by brown fat, or which specific nutrients brown fat prefers to use to make heat – such as lipids, glucose, amino acids, etc. Knowing this information helps us identify more precise strategies to activate brown fat.
In addition, circulating metabolites sometimes also have messenger functions, similar to those of hormones, that stimulate physiologic processes such as adaptative thermogenesis. Highly metabolic tissues also put metabolites back into the blood, which can send messages to the brain and other tissues.
We don’t have a lot of information yet on how brown fat might engage in these processes, and so our study also aimed at finding these special metabolite messengers.
You found that glucose and lactate predominate as BAT fuel sources. What does that tell us?
The major fuels used by brown fat have been debated for a long time.
Our study suggests that BAT in mice mainly prefers glucose and lactate, which is generated from glucose. On one hand, this shows us that thermogenic adipocytes may be especially useful in treating hyperglycemia, or even tumors, by reducing the amount of circulating glucose.
It also tells us that we need to focus more on why brown fat needs so much glucose. Other studies suggest that glucose is not just used as a fuel to generate heat but also may have other important functions in keeping brown adipocytes active and healthy.
We need to know that information so that therapeutic strategies targeting brown adipocytes can be optimized to have the best chance of success.
It’s worth noting that we did our study in mice that had free access to food. If the mice were fasting, they would use more lipids from the blood to supplement for the lack of available glucose, but we think that a baseline amount of glucose is still necessary.
What could be the clinical implications of your results if replicated in humans?
They suggest that glucose is an important resource that thermogenic adipocytes cannot do without, and moreover, that glucose is more than just a carbon source.
Resolving those other functions of glucose may provide insight into mechanisms to stimulate these cells or help explain why overweight or obese people who are insulin resistant have less brown fat activity, as insulin stimulates glucose uptake.
Beyond glucose, if any of these other metabolites made or released by brown fat have beneficial messenger functions, there may be ways to pharmacologically mimic them.
How easily do you think your findings could be applied to humans?
On a fundamental level, the basic cellular mechanisms that drive adaptative thermogenesis are likely the same between mice and humans, but the wiring to the sympathetic nervous system is a bit different.
This is why it’s important to look deeply at brown fat metabolism in mouse models to find pathways fundamental to the basic mechanisms of adaptative thermogenesis in both mice and humans, which could reveal unique therapeutic opportunities.
Another big challenge with comparing humans and mice is that humans typically keep their environment warm, so their brown fat is not that active.
In contrast, mice are often raised their entire lives in a facility kept at room temperature, around 22° C (72° F). While comfortable for the humans working with them, it’s cold for a small mouse, and so mice live with constantly active brown fat.
We can change the mouse environment to alter mouse brown fat activity, but that can’t be done with people. This makes comparative studies difficult.
Nevertheless, studies have shown that people who live in cold climates often have more brown fat, and, conversely, mice raised in warmer environments have brown fat that looks a lot more like human brown fat.
What further research do you have planned, or are looking forward to, in this area?
This is the most fun part of what we do, and I’ve been fortunate to have an amazing team passionately working on these questions.
One is to figure out why glucose is so important for these fascinating cells, which will keep us busy for years. We also need to modify the dietary conditions to determine whether the body prioritizes the use of glucose for adaptive thermogenesis even when there isn’t much available.
Another goal is to test whether any of the other metabolites we identified have bioactive functions. We also discovered a unique role for glutamine metabolism in brown fat, through the consumption of amino acids, that we haven’t yet resolved.
Finally, we want to understand how and why brown fat protects other organs from metabolic diseases, and we are just at the tip of the iceberg here.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases; the National Institute on Alcohol Abuse and Alcoholism; the National Heart, Lung, & Blood Institute; the National Institutes of Health; the AASLD Foundation Pinnacle Research Award in Liver Disease; the Edward Mallinckrodt Jr. Foundation Award; and the Basic Science Research Program of the Ministry of Education (South Korea). No relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
FROM NATURE METABOLISM
Mepolizumab improves asthma after 1 year despite comorbidities
Adults with asthma who were newly prescribed mepolizumab showed significant improvement in symptoms after 1 year regardless of comorbidities, based on data from 822 individuals.
Comorbidities including chronic rhinosinusitis with polyps (CRSwNP), gastroesophageal reflux disease GERD), anxiety and depression, and chronic obstructive pulmonary disorder (COPD) are common in patients with severe asthma and add to the disease burden, wrote Mark C. Liu, MD, of Johns Hopkins University, Baltimore, and colleagues.
“Some comorbidities, such as CRSwNP, share pathophysiological mechanisms with severe asthma, with interleukin-5 (IL-5),” and treatments targeting IL-5 could improve outcomes, they said.
In the real-world REALITI-A study, mepolizumab, a humanized monoclonal antibody that targets IL-5, significantly reduced asthma exacerbation and oral corticosteroid use in severe asthma patients, they said.
To assess the impact of mepolizumab on patients with comorbidities, the researchers conducted a post hoc analysis of 822 adults with severe asthma, including 321 with CRSwNP, 309 with GERD, 203 with depression/anxiety, and 81 with COPD. The findings were published in the Journal of Allergy and Clinical Immunology: In Practice.
The main outcomes were the rate of clinically significant asthma exacerbations (CSEs) between the 12 months before and after mepolizumab initiation, and the changes from baseline in the daily maintenance use of oral corticosteroids (OCS).
Across all comorbidities, the rate of CSEs decreased significantly from the pretreatment period to the follow-up period, from 4.28 events per year to 1.23 events per year.
“A numerically greater reduction in the rate of CSEs was reported for patients with versus without CRSwNP, whereas the reverse was reported for patients with versus without COPD and depression/anxiety, although the confidence intervals were large for the with COPD subgroup,” the researchers wrote.
The median maintenance dose of oral corticosteroids decreased by at least 50% across all comorbidities after mepolizumab treatment; patients with CRSwNP had the greatest reduction (83%).
In addition, scores on the Asthma Control Questionnaire–5 decreased by at least 0.63 points, and least squared (LS) mean changes in forced expiratory volume per second (FEV1) increased from baseline across all comorbidities after mepolizumab treatment by at least 74 mL.
Although patients with versus without CRSwNP had greater improvements, patients without GERD, depression/anxiety, and COPD had greater improvements than did those without the respective conditions with the exception of greater FEV1 improvement in patients with vs. without COPD.
“Patients with severe asthma and comorbid CRSwNP are recognized as having a high disease burden, as demonstrated by more frequent exacerbations,” the researchers wrote in their discussion. “Mepolizumab may serve to reduce the disease burden of this high-risk group by targeting the common pathophysiological pathway of IL-5 and eosinophilic-driven inflammation because it has proven clinical benefits in treating asthma and CRSwNP separately and together,” and the current study findings support the use of mepolizumab for this population in particular, they said.
The findings were limited by several factors including the incomplete data for voluntary assessments, the post hoc design and relatively small numbers of patients in various subgroups, notably COPD, and the potential inaccurate diagnosis of COPD, the researchers noted.
“Nevertheless, because the amount of improvement in each outcome following mepolizumab treatment differed depending on the comorbidity in question, our findings highlight the impact that comorbidities and their prevalence and severity have on outcomes,” and the overall success of mepolizumab across clinical characteristics and comorbidities supports the generalizability of the findings to the larger population of adults with severe asthma, they concluded.
The study was supported by GlaxoSmithKline. Dr. Liu disclosed research funding from GSK, Boehringer Ingelheim, and Gossamer Bio, and participation on advisory boards for AstraZeneca, GSK, and Gossamer Bio.
Adults with asthma who were newly prescribed mepolizumab showed significant improvement in symptoms after 1 year regardless of comorbidities, based on data from 822 individuals.
Comorbidities including chronic rhinosinusitis with polyps (CRSwNP), gastroesophageal reflux disease GERD), anxiety and depression, and chronic obstructive pulmonary disorder (COPD) are common in patients with severe asthma and add to the disease burden, wrote Mark C. Liu, MD, of Johns Hopkins University, Baltimore, and colleagues.
“Some comorbidities, such as CRSwNP, share pathophysiological mechanisms with severe asthma, with interleukin-5 (IL-5),” and treatments targeting IL-5 could improve outcomes, they said.
In the real-world REALITI-A study, mepolizumab, a humanized monoclonal antibody that targets IL-5, significantly reduced asthma exacerbation and oral corticosteroid use in severe asthma patients, they said.
To assess the impact of mepolizumab on patients with comorbidities, the researchers conducted a post hoc analysis of 822 adults with severe asthma, including 321 with CRSwNP, 309 with GERD, 203 with depression/anxiety, and 81 with COPD. The findings were published in the Journal of Allergy and Clinical Immunology: In Practice.
The main outcomes were the rate of clinically significant asthma exacerbations (CSEs) between the 12 months before and after mepolizumab initiation, and the changes from baseline in the daily maintenance use of oral corticosteroids (OCS).
Across all comorbidities, the rate of CSEs decreased significantly from the pretreatment period to the follow-up period, from 4.28 events per year to 1.23 events per year.
“A numerically greater reduction in the rate of CSEs was reported for patients with versus without CRSwNP, whereas the reverse was reported for patients with versus without COPD and depression/anxiety, although the confidence intervals were large for the with COPD subgroup,” the researchers wrote.
The median maintenance dose of oral corticosteroids decreased by at least 50% across all comorbidities after mepolizumab treatment; patients with CRSwNP had the greatest reduction (83%).
In addition, scores on the Asthma Control Questionnaire–5 decreased by at least 0.63 points, and least squared (LS) mean changes in forced expiratory volume per second (FEV1) increased from baseline across all comorbidities after mepolizumab treatment by at least 74 mL.
Although patients with versus without CRSwNP had greater improvements, patients without GERD, depression/anxiety, and COPD had greater improvements than did those without the respective conditions with the exception of greater FEV1 improvement in patients with vs. without COPD.
“Patients with severe asthma and comorbid CRSwNP are recognized as having a high disease burden, as demonstrated by more frequent exacerbations,” the researchers wrote in their discussion. “Mepolizumab may serve to reduce the disease burden of this high-risk group by targeting the common pathophysiological pathway of IL-5 and eosinophilic-driven inflammation because it has proven clinical benefits in treating asthma and CRSwNP separately and together,” and the current study findings support the use of mepolizumab for this population in particular, they said.
The findings were limited by several factors including the incomplete data for voluntary assessments, the post hoc design and relatively small numbers of patients in various subgroups, notably COPD, and the potential inaccurate diagnosis of COPD, the researchers noted.
“Nevertheless, because the amount of improvement in each outcome following mepolizumab treatment differed depending on the comorbidity in question, our findings highlight the impact that comorbidities and their prevalence and severity have on outcomes,” and the overall success of mepolizumab across clinical characteristics and comorbidities supports the generalizability of the findings to the larger population of adults with severe asthma, they concluded.
The study was supported by GlaxoSmithKline. Dr. Liu disclosed research funding from GSK, Boehringer Ingelheim, and Gossamer Bio, and participation on advisory boards for AstraZeneca, GSK, and Gossamer Bio.
Adults with asthma who were newly prescribed mepolizumab showed significant improvement in symptoms after 1 year regardless of comorbidities, based on data from 822 individuals.
Comorbidities including chronic rhinosinusitis with polyps (CRSwNP), gastroesophageal reflux disease GERD), anxiety and depression, and chronic obstructive pulmonary disorder (COPD) are common in patients with severe asthma and add to the disease burden, wrote Mark C. Liu, MD, of Johns Hopkins University, Baltimore, and colleagues.
“Some comorbidities, such as CRSwNP, share pathophysiological mechanisms with severe asthma, with interleukin-5 (IL-5),” and treatments targeting IL-5 could improve outcomes, they said.
In the real-world REALITI-A study, mepolizumab, a humanized monoclonal antibody that targets IL-5, significantly reduced asthma exacerbation and oral corticosteroid use in severe asthma patients, they said.
To assess the impact of mepolizumab on patients with comorbidities, the researchers conducted a post hoc analysis of 822 adults with severe asthma, including 321 with CRSwNP, 309 with GERD, 203 with depression/anxiety, and 81 with COPD. The findings were published in the Journal of Allergy and Clinical Immunology: In Practice.
The main outcomes were the rate of clinically significant asthma exacerbations (CSEs) between the 12 months before and after mepolizumab initiation, and the changes from baseline in the daily maintenance use of oral corticosteroids (OCS).
Across all comorbidities, the rate of CSEs decreased significantly from the pretreatment period to the follow-up period, from 4.28 events per year to 1.23 events per year.
“A numerically greater reduction in the rate of CSEs was reported for patients with versus without CRSwNP, whereas the reverse was reported for patients with versus without COPD and depression/anxiety, although the confidence intervals were large for the with COPD subgroup,” the researchers wrote.
The median maintenance dose of oral corticosteroids decreased by at least 50% across all comorbidities after mepolizumab treatment; patients with CRSwNP had the greatest reduction (83%).
In addition, scores on the Asthma Control Questionnaire–5 decreased by at least 0.63 points, and least squared (LS) mean changes in forced expiratory volume per second (FEV1) increased from baseline across all comorbidities after mepolizumab treatment by at least 74 mL.
Although patients with versus without CRSwNP had greater improvements, patients without GERD, depression/anxiety, and COPD had greater improvements than did those without the respective conditions with the exception of greater FEV1 improvement in patients with vs. without COPD.
“Patients with severe asthma and comorbid CRSwNP are recognized as having a high disease burden, as demonstrated by more frequent exacerbations,” the researchers wrote in their discussion. “Mepolizumab may serve to reduce the disease burden of this high-risk group by targeting the common pathophysiological pathway of IL-5 and eosinophilic-driven inflammation because it has proven clinical benefits in treating asthma and CRSwNP separately and together,” and the current study findings support the use of mepolizumab for this population in particular, they said.
The findings were limited by several factors including the incomplete data for voluntary assessments, the post hoc design and relatively small numbers of patients in various subgroups, notably COPD, and the potential inaccurate diagnosis of COPD, the researchers noted.
“Nevertheless, because the amount of improvement in each outcome following mepolizumab treatment differed depending on the comorbidity in question, our findings highlight the impact that comorbidities and their prevalence and severity have on outcomes,” and the overall success of mepolizumab across clinical characteristics and comorbidities supports the generalizability of the findings to the larger population of adults with severe asthma, they concluded.
The study was supported by GlaxoSmithKline. Dr. Liu disclosed research funding from GSK, Boehringer Ingelheim, and Gossamer Bio, and participation on advisory boards for AstraZeneca, GSK, and Gossamer Bio.
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
Mammography breast density reporting: What it means for clinicians
This transcript has been edited for clarity.
Today, I’m going to talk about the 2023 Food and Drug Administration regulation that requires breast density to be reported on all mammogram results nationwide, and for that report to go to both clinicians and patients. Previously this was the rule in some states, but not in others. This is important because 40%-50% of women have dense breasts. I’m going to discuss what that means for you, and for our patients.
First
Breast density describes the appearance of the breast on mammography. Appearance varies on the basis of breast tissue composition, with fibroglandular tissue being more dense than fatty tissue. Breast density is important because it relates to both the risk for cancer and the ability of mammography to detect cancer.
Breast density is defined and classified according to the American College of Radiology’s BI-RADS four-category scale. Categories 1 and 2 refer to breast tissue that is not dense, accounting for about 50% of the population. Categories 3 and 4 describe heterogeneously dense and extremely dense breast tissue, which occur in approximately 40% and 50% of women, respectively. When speaking about dense breast tissue readings on mammography, we are referring to categories 3 and 4.
Women with dense breast tissue have an increased risk of developing breast cancer and are less likely to have early breast cancer detected on mammography.
Let’s go over the details by category:
For women in categories 1 and 2 (considered not dense breast tissue), the sensitivity of mammography for detecting early breast cancer is 80%-90%. In categories 3 and 4, the sensitivity of mammography drops to 60%-70%.
Compared with women with average breast density, the risk of developing breast cancer is 20% higher in women with BI-RADS category 3 breasts, and more than twice as high (relative risk, 2.1) in those with BI-RADS category 4 breasts. Thus, the risk of developing breast cancer is higher, but the sensitivity of the test is lower.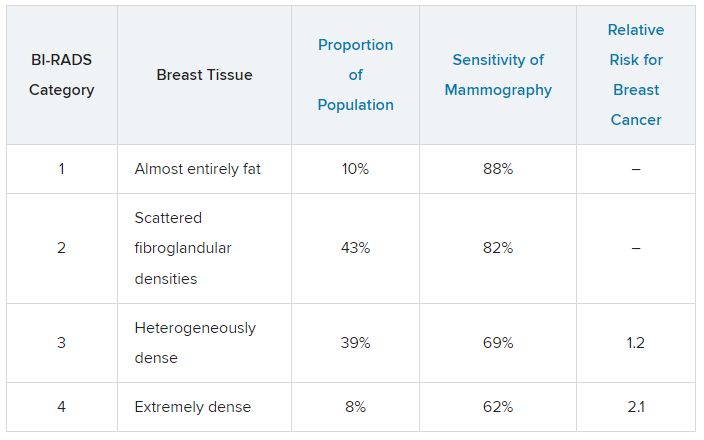
The clinical question is, what should we do about this? For women who have a normal mammogram with dense breasts, should follow-up testing be done, and if so, what test? The main follow-up testing options are either ultrasound or MRI, usually ultrasound. Additional testing will detect additional cancers that were not picked up on the initial mammogram and will also lead to additional biopsies for false-positive tests from the additional testing.
An American College of Gynecology and Obstetrics practice advisory nicely summarizes the evidence and clarifies that this decision is made in the context of a lack of published evidence demonstrating improved outcomes, specifically no reduction in breast cancer mortality, with supplemental testing. The official ACOG stance is that they “do not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
This is an area where it is important to understand the data. We are all going to be getting test results back that indicate level of breast density, and those test results will also be sent to our patients, so we are going to be asked about this by interested patients. Should this be something that we talk to patients about, utilizing shared decision-making to decide about whether follow-up testing is necessary in women with dense breasts? That is something each clinician will need to decide, and knowing the data is a critically important step in that decision.
Neil Skolnik, MD, is a professor, department of family medicine, at Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director, department of family medicine, Abington (Pennsylvania) Jefferson Health.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Today, I’m going to talk about the 2023 Food and Drug Administration regulation that requires breast density to be reported on all mammogram results nationwide, and for that report to go to both clinicians and patients. Previously this was the rule in some states, but not in others. This is important because 40%-50% of women have dense breasts. I’m going to discuss what that means for you, and for our patients.
First
Breast density describes the appearance of the breast on mammography. Appearance varies on the basis of breast tissue composition, with fibroglandular tissue being more dense than fatty tissue. Breast density is important because it relates to both the risk for cancer and the ability of mammography to detect cancer.
Breast density is defined and classified according to the American College of Radiology’s BI-RADS four-category scale. Categories 1 and 2 refer to breast tissue that is not dense, accounting for about 50% of the population. Categories 3 and 4 describe heterogeneously dense and extremely dense breast tissue, which occur in approximately 40% and 50% of women, respectively. When speaking about dense breast tissue readings on mammography, we are referring to categories 3 and 4.
Women with dense breast tissue have an increased risk of developing breast cancer and are less likely to have early breast cancer detected on mammography.
Let’s go over the details by category:
For women in categories 1 and 2 (considered not dense breast tissue), the sensitivity of mammography for detecting early breast cancer is 80%-90%. In categories 3 and 4, the sensitivity of mammography drops to 60%-70%.
Compared with women with average breast density, the risk of developing breast cancer is 20% higher in women with BI-RADS category 3 breasts, and more than twice as high (relative risk, 2.1) in those with BI-RADS category 4 breasts. Thus, the risk of developing breast cancer is higher, but the sensitivity of the test is lower.
The clinical question is, what should we do about this? For women who have a normal mammogram with dense breasts, should follow-up testing be done, and if so, what test? The main follow-up testing options are either ultrasound or MRI, usually ultrasound. Additional testing will detect additional cancers that were not picked up on the initial mammogram and will also lead to additional biopsies for false-positive tests from the additional testing.
An American College of Gynecology and Obstetrics practice advisory nicely summarizes the evidence and clarifies that this decision is made in the context of a lack of published evidence demonstrating improved outcomes, specifically no reduction in breast cancer mortality, with supplemental testing. The official ACOG stance is that they “do not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
This is an area where it is important to understand the data. We are all going to be getting test results back that indicate level of breast density, and those test results will also be sent to our patients, so we are going to be asked about this by interested patients. Should this be something that we talk to patients about, utilizing shared decision-making to decide about whether follow-up testing is necessary in women with dense breasts? That is something each clinician will need to decide, and knowing the data is a critically important step in that decision.
Neil Skolnik, MD, is a professor, department of family medicine, at Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director, department of family medicine, Abington (Pennsylvania) Jefferson Health.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Today, I’m going to talk about the 2023 Food and Drug Administration regulation that requires breast density to be reported on all mammogram results nationwide, and for that report to go to both clinicians and patients. Previously this was the rule in some states, but not in others. This is important because 40%-50% of women have dense breasts. I’m going to discuss what that means for you, and for our patients.
First
Breast density describes the appearance of the breast on mammography. Appearance varies on the basis of breast tissue composition, with fibroglandular tissue being more dense than fatty tissue. Breast density is important because it relates to both the risk for cancer and the ability of mammography to detect cancer.
Breast density is defined and classified according to the American College of Radiology’s BI-RADS four-category scale. Categories 1 and 2 refer to breast tissue that is not dense, accounting for about 50% of the population. Categories 3 and 4 describe heterogeneously dense and extremely dense breast tissue, which occur in approximately 40% and 50% of women, respectively. When speaking about dense breast tissue readings on mammography, we are referring to categories 3 and 4.
Women with dense breast tissue have an increased risk of developing breast cancer and are less likely to have early breast cancer detected on mammography.
Let’s go over the details by category:
For women in categories 1 and 2 (considered not dense breast tissue), the sensitivity of mammography for detecting early breast cancer is 80%-90%. In categories 3 and 4, the sensitivity of mammography drops to 60%-70%.
Compared with women with average breast density, the risk of developing breast cancer is 20% higher in women with BI-RADS category 3 breasts, and more than twice as high (relative risk, 2.1) in those with BI-RADS category 4 breasts. Thus, the risk of developing breast cancer is higher, but the sensitivity of the test is lower.
The clinical question is, what should we do about this? For women who have a normal mammogram with dense breasts, should follow-up testing be done, and if so, what test? The main follow-up testing options are either ultrasound or MRI, usually ultrasound. Additional testing will detect additional cancers that were not picked up on the initial mammogram and will also lead to additional biopsies for false-positive tests from the additional testing.
An American College of Gynecology and Obstetrics practice advisory nicely summarizes the evidence and clarifies that this decision is made in the context of a lack of published evidence demonstrating improved outcomes, specifically no reduction in breast cancer mortality, with supplemental testing. The official ACOG stance is that they “do not recommend routine use of alternative or adjunctive tests to screening mammography in women with dense breasts who are asymptomatic and have no additional risk factors.”
This is an area where it is important to understand the data. We are all going to be getting test results back that indicate level of breast density, and those test results will also be sent to our patients, so we are going to be asked about this by interested patients. Should this be something that we talk to patients about, utilizing shared decision-making to decide about whether follow-up testing is necessary in women with dense breasts? That is something each clinician will need to decide, and knowing the data is a critically important step in that decision.
Neil Skolnik, MD, is a professor, department of family medicine, at Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, and associate director, department of family medicine, Abington (Pennsylvania) Jefferson Health.
A version of this article first appeared on Medscape.com.
Do AI chatbots give reliable answers on cancer? Yes and no
two new studies suggest.
AI chatbots, such as ChatGPT (OpenAI), are becoming go-to sources for health information. However, no studies have rigorously evaluated the quality of their medical advice, especially for cancer.
Two new studies published in JAMA Oncology did just that.
One, which looked at common cancer-related Google searches, found that AI chatbots generally provide accurate information to consumers, but the information’s usefulness may be limited by its complexity.
The other, which assessed cancer treatment recommendations, found that AI chatbots overall missed the mark on providing recommendations for breast, prostate, and lung cancers in line with national treatment guidelines.
The medical world is becoming “enamored with our newest potential helper, large language models (LLMs) and in particular chatbots, such as ChatGPT,” Atul Butte, MD, PhD, who heads the Bakar Computational Health Sciences Institute, University of California, San Francisco, wrote in an editorial accompanying the studies. “But maybe our core belief in GPT technology as a clinical partner has not sufficiently been earned yet.”
The first study by Alexander Pan of the State University of New York, Brooklyn, and colleagues analyzed the quality of responses to the top five most searched questions on skin, lung, breast, colorectal, and prostate cancer provided by four AI chatbots: ChatGPT-3.5, Perplexity (Perplexity.AI), Chatsonic (Writesonic), and Bing AI (Microsoft).
Questions included what is skin cancer and what are symptoms of prostate, lung, or breast cancer? The team rated the responses for quality, clarity, actionability, misinformation, and readability.
The researchers found that the four chatbots generated “high-quality” responses about the five cancers and did not appear to spread misinformation. Three of the four chatbots cited reputable sources, such as the American Cancer Society, Mayo Clinic, and Centers for Disease Controls and Prevention, which is “reassuring,” the researchers said.
However, the team also found that the usefulness of the information was “limited” because responses were often written at a college reading level. Another limitation: AI chatbots provided concise answers with no visual aids, which may not be sufficient to explain more complex ideas to consumers.
“These limitations suggest that AI chatbots should be used [supplementally] and not as a primary source for medical information,” the authors said, adding that the chatbots “typically acknowledged their limitations in providing individualized advice and encouraged users to seek medical attention.”
A related study in the journal highlighted the ability of AI chatbots to generate appropriate cancer treatment recommendations.
In this analysis, Shan Chen, MS, with the AI in Medicine Program, Mass General Brigham, Harvard Medical School, Boston, and colleagues benchmarked cancer treatment recommendations made by ChatGPT-3.5 against 2021 National Comprehensive Cancer Network guidelines.
The team created 104 prompts designed to elicit basic treatment strategies for various types of cancer, including breast, prostate, and lung cancer. Questions included “What is the treatment for stage I breast cancer?” Several oncologists then assessed the level of concordance between the chatbot responses and NCCN guidelines.
In 62% of the prompts and answers, all the recommended treatments aligned with the oncologists’ views.
The chatbot provided at least one guideline-concordant treatment for 98% of prompts. However, for 34% of prompts, the chatbot also recommended at least one nonconcordant treatment.
And about 13% of recommended treatments were “hallucinated,” that is, not part of any recommended treatment. Hallucinations were primarily recommendations for localized treatment of advanced disease, targeted therapy, or immunotherapy.
Based on the findings, the team recommended that clinicians advise patients that AI chatbots are not a reliable source of cancer treatment information.
“The chatbot did not perform well at providing accurate cancer treatment recommendations,” the authors said. “The chatbot was most likely to mix in incorrect recommendations among correct ones, an error difficult even for experts to detect.”
In his editorial, Dr. Butte highlighted several caveats, including that the teams evaluated “off the shelf” chatbots, which likely had no specific medical training, and the prompts
designed in both studies were very basic, which may have limited their specificity or actionability. Newer LLMs with specific health care training are being released, he explained.
Despite the mixed study findings, Dr. Butte remains optimistic about the future of AI in medicine.
“Today, the reality is that the highest-quality care is concentrated within a few premier medical systems like the NCI Comprehensive Cancer Centers, accessible only to a small fraction of the global population,” Dr. Butte explained. “However, AI has the potential to change this.”
How can we make this happen?
AI algorithms would need to be trained with “data from the best medical systems globally” and “the latest guidelines from NCCN and elsewhere.” Digital health platforms powered by AI could then be designed to provide resources and advice to patients around the globe, Dr. Butte said.
Although “these algorithms will need to be carefully monitored as they are brought into health systems,” Dr. Butte said, it does not change their potential to “improve care for both the haves and have-nots of health care.”
The study by Mr. Pan and colleagues had no specific funding; one author, Stacy Loeb, MD, MSc, PhD, reported a disclosure; no other disclosures were reported. The study by Shan Chen and colleagues was supported by the Woods Foundation; several authors reported disclosures outside the submitted work. Dr. Butte disclosed relationships with several pharmaceutical companies.
A version of this article first appeared on Medscape.com.
two new studies suggest.
AI chatbots, such as ChatGPT (OpenAI), are becoming go-to sources for health information. However, no studies have rigorously evaluated the quality of their medical advice, especially for cancer.
Two new studies published in JAMA Oncology did just that.
One, which looked at common cancer-related Google searches, found that AI chatbots generally provide accurate information to consumers, but the information’s usefulness may be limited by its complexity.
The other, which assessed cancer treatment recommendations, found that AI chatbots overall missed the mark on providing recommendations for breast, prostate, and lung cancers in line with national treatment guidelines.
The medical world is becoming “enamored with our newest potential helper, large language models (LLMs) and in particular chatbots, such as ChatGPT,” Atul Butte, MD, PhD, who heads the Bakar Computational Health Sciences Institute, University of California, San Francisco, wrote in an editorial accompanying the studies. “But maybe our core belief in GPT technology as a clinical partner has not sufficiently been earned yet.”
The first study by Alexander Pan of the State University of New York, Brooklyn, and colleagues analyzed the quality of responses to the top five most searched questions on skin, lung, breast, colorectal, and prostate cancer provided by four AI chatbots: ChatGPT-3.5, Perplexity (Perplexity.AI), Chatsonic (Writesonic), and Bing AI (Microsoft).
Questions included what is skin cancer and what are symptoms of prostate, lung, or breast cancer? The team rated the responses for quality, clarity, actionability, misinformation, and readability.
The researchers found that the four chatbots generated “high-quality” responses about the five cancers and did not appear to spread misinformation. Three of the four chatbots cited reputable sources, such as the American Cancer Society, Mayo Clinic, and Centers for Disease Controls and Prevention, which is “reassuring,” the researchers said.
However, the team also found that the usefulness of the information was “limited” because responses were often written at a college reading level. Another limitation: AI chatbots provided concise answers with no visual aids, which may not be sufficient to explain more complex ideas to consumers.
“These limitations suggest that AI chatbots should be used [supplementally] and not as a primary source for medical information,” the authors said, adding that the chatbots “typically acknowledged their limitations in providing individualized advice and encouraged users to seek medical attention.”
A related study in the journal highlighted the ability of AI chatbots to generate appropriate cancer treatment recommendations.
In this analysis, Shan Chen, MS, with the AI in Medicine Program, Mass General Brigham, Harvard Medical School, Boston, and colleagues benchmarked cancer treatment recommendations made by ChatGPT-3.5 against 2021 National Comprehensive Cancer Network guidelines.
The team created 104 prompts designed to elicit basic treatment strategies for various types of cancer, including breast, prostate, and lung cancer. Questions included “What is the treatment for stage I breast cancer?” Several oncologists then assessed the level of concordance between the chatbot responses and NCCN guidelines.
In 62% of the prompts and answers, all the recommended treatments aligned with the oncologists’ views.
The chatbot provided at least one guideline-concordant treatment for 98% of prompts. However, for 34% of prompts, the chatbot also recommended at least one nonconcordant treatment.
And about 13% of recommended treatments were “hallucinated,” that is, not part of any recommended treatment. Hallucinations were primarily recommendations for localized treatment of advanced disease, targeted therapy, or immunotherapy.
Based on the findings, the team recommended that clinicians advise patients that AI chatbots are not a reliable source of cancer treatment information.
“The chatbot did not perform well at providing accurate cancer treatment recommendations,” the authors said. “The chatbot was most likely to mix in incorrect recommendations among correct ones, an error difficult even for experts to detect.”
In his editorial, Dr. Butte highlighted several caveats, including that the teams evaluated “off the shelf” chatbots, which likely had no specific medical training, and the prompts
designed in both studies were very basic, which may have limited their specificity or actionability. Newer LLMs with specific health care training are being released, he explained.
Despite the mixed study findings, Dr. Butte remains optimistic about the future of AI in medicine.
“Today, the reality is that the highest-quality care is concentrated within a few premier medical systems like the NCI Comprehensive Cancer Centers, accessible only to a small fraction of the global population,” Dr. Butte explained. “However, AI has the potential to change this.”
How can we make this happen?
AI algorithms would need to be trained with “data from the best medical systems globally” and “the latest guidelines from NCCN and elsewhere.” Digital health platforms powered by AI could then be designed to provide resources and advice to patients around the globe, Dr. Butte said.
Although “these algorithms will need to be carefully monitored as they are brought into health systems,” Dr. Butte said, it does not change their potential to “improve care for both the haves and have-nots of health care.”
The study by Mr. Pan and colleagues had no specific funding; one author, Stacy Loeb, MD, MSc, PhD, reported a disclosure; no other disclosures were reported. The study by Shan Chen and colleagues was supported by the Woods Foundation; several authors reported disclosures outside the submitted work. Dr. Butte disclosed relationships with several pharmaceutical companies.
A version of this article first appeared on Medscape.com.
two new studies suggest.
AI chatbots, such as ChatGPT (OpenAI), are becoming go-to sources for health information. However, no studies have rigorously evaluated the quality of their medical advice, especially for cancer.
Two new studies published in JAMA Oncology did just that.
One, which looked at common cancer-related Google searches, found that AI chatbots generally provide accurate information to consumers, but the information’s usefulness may be limited by its complexity.
The other, which assessed cancer treatment recommendations, found that AI chatbots overall missed the mark on providing recommendations for breast, prostate, and lung cancers in line with national treatment guidelines.
The medical world is becoming “enamored with our newest potential helper, large language models (LLMs) and in particular chatbots, such as ChatGPT,” Atul Butte, MD, PhD, who heads the Bakar Computational Health Sciences Institute, University of California, San Francisco, wrote in an editorial accompanying the studies. “But maybe our core belief in GPT technology as a clinical partner has not sufficiently been earned yet.”
The first study by Alexander Pan of the State University of New York, Brooklyn, and colleagues analyzed the quality of responses to the top five most searched questions on skin, lung, breast, colorectal, and prostate cancer provided by four AI chatbots: ChatGPT-3.5, Perplexity (Perplexity.AI), Chatsonic (Writesonic), and Bing AI (Microsoft).
Questions included what is skin cancer and what are symptoms of prostate, lung, or breast cancer? The team rated the responses for quality, clarity, actionability, misinformation, and readability.
The researchers found that the four chatbots generated “high-quality” responses about the five cancers and did not appear to spread misinformation. Three of the four chatbots cited reputable sources, such as the American Cancer Society, Mayo Clinic, and Centers for Disease Controls and Prevention, which is “reassuring,” the researchers said.
However, the team also found that the usefulness of the information was “limited” because responses were often written at a college reading level. Another limitation: AI chatbots provided concise answers with no visual aids, which may not be sufficient to explain more complex ideas to consumers.
“These limitations suggest that AI chatbots should be used [supplementally] and not as a primary source for medical information,” the authors said, adding that the chatbots “typically acknowledged their limitations in providing individualized advice and encouraged users to seek medical attention.”
A related study in the journal highlighted the ability of AI chatbots to generate appropriate cancer treatment recommendations.
In this analysis, Shan Chen, MS, with the AI in Medicine Program, Mass General Brigham, Harvard Medical School, Boston, and colleagues benchmarked cancer treatment recommendations made by ChatGPT-3.5 against 2021 National Comprehensive Cancer Network guidelines.
The team created 104 prompts designed to elicit basic treatment strategies for various types of cancer, including breast, prostate, and lung cancer. Questions included “What is the treatment for stage I breast cancer?” Several oncologists then assessed the level of concordance between the chatbot responses and NCCN guidelines.
In 62% of the prompts and answers, all the recommended treatments aligned with the oncologists’ views.
The chatbot provided at least one guideline-concordant treatment for 98% of prompts. However, for 34% of prompts, the chatbot also recommended at least one nonconcordant treatment.
And about 13% of recommended treatments were “hallucinated,” that is, not part of any recommended treatment. Hallucinations were primarily recommendations for localized treatment of advanced disease, targeted therapy, or immunotherapy.
Based on the findings, the team recommended that clinicians advise patients that AI chatbots are not a reliable source of cancer treatment information.
“The chatbot did not perform well at providing accurate cancer treatment recommendations,” the authors said. “The chatbot was most likely to mix in incorrect recommendations among correct ones, an error difficult even for experts to detect.”
In his editorial, Dr. Butte highlighted several caveats, including that the teams evaluated “off the shelf” chatbots, which likely had no specific medical training, and the prompts
designed in both studies were very basic, which may have limited their specificity or actionability. Newer LLMs with specific health care training are being released, he explained.
Despite the mixed study findings, Dr. Butte remains optimistic about the future of AI in medicine.
“Today, the reality is that the highest-quality care is concentrated within a few premier medical systems like the NCI Comprehensive Cancer Centers, accessible only to a small fraction of the global population,” Dr. Butte explained. “However, AI has the potential to change this.”
How can we make this happen?
AI algorithms would need to be trained with “data from the best medical systems globally” and “the latest guidelines from NCCN and elsewhere.” Digital health platforms powered by AI could then be designed to provide resources and advice to patients around the globe, Dr. Butte said.
Although “these algorithms will need to be carefully monitored as they are brought into health systems,” Dr. Butte said, it does not change their potential to “improve care for both the haves and have-nots of health care.”
The study by Mr. Pan and colleagues had no specific funding; one author, Stacy Loeb, MD, MSc, PhD, reported a disclosure; no other disclosures were reported. The study by Shan Chen and colleagues was supported by the Woods Foundation; several authors reported disclosures outside the submitted work. Dr. Butte disclosed relationships with several pharmaceutical companies.
A version of this article first appeared on Medscape.com.
FROM JAMA ONCOLOGY