User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
Powered by CHEST Physician, Clinician Reviews, MDedge Family Medicine, Internal Medicine News, and The Journal of Clinical Outcomes Management.
Flu activity increases after 2 weeks of declines
according to the Centers for Disease Control and Prevention.
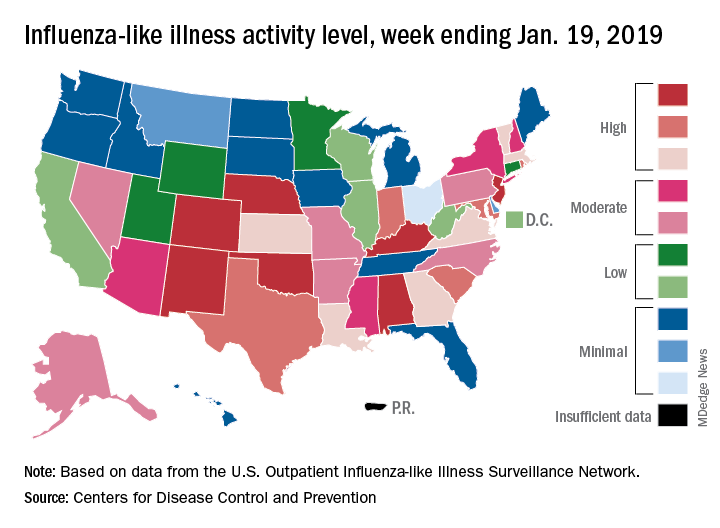
The proportion of outpatient visits for influenza-like illness (ILI) was 3.3% for the most recent measurement period, the CDC’s influenza division reported Jan 25. The previous 2-week decline had seen ILI visits dip down to 3.1% for the week ending Jan. 12 after hitting a season high of 4%.
To go along with the national increase in visits, more states reported high levels of flu activity. For the week ending Jan. 19, seven states were at level 10 on the CDC’s 1-10 scale, compared with four the previous week, and there were 18 states in the high range (levels 8-10), compared with 9 the week before, the CDC said.
Three flu-related pediatric deaths were reported in the week ending Jan. 19, although all three occurred during earlier weeks. The total number of pediatric deaths for the 2018-2019 season is now up to 22. Deaths among all ages, which are reported a week later, totaled 118 for the week ending Jan. 12, with 63% of reporting complete. There were 144 deaths during the week ending Jan. 5, with reporting 86% complete. During the second full week of 2018, in the middle of the very severe 2017-2018 season, there were 1,537 flu-related deaths, CDC data show.
according to the Centers for Disease Control and Prevention.
The proportion of outpatient visits for influenza-like illness (ILI) was 3.3% for the most recent measurement period, the CDC’s influenza division reported Jan 25. The previous 2-week decline had seen ILI visits dip down to 3.1% for the week ending Jan. 12 after hitting a season high of 4%.
To go along with the national increase in visits, more states reported high levels of flu activity. For the week ending Jan. 19, seven states were at level 10 on the CDC’s 1-10 scale, compared with four the previous week, and there were 18 states in the high range (levels 8-10), compared with 9 the week before, the CDC said.
Three flu-related pediatric deaths were reported in the week ending Jan. 19, although all three occurred during earlier weeks. The total number of pediatric deaths for the 2018-2019 season is now up to 22. Deaths among all ages, which are reported a week later, totaled 118 for the week ending Jan. 12, with 63% of reporting complete. There were 144 deaths during the week ending Jan. 5, with reporting 86% complete. During the second full week of 2018, in the middle of the very severe 2017-2018 season, there were 1,537 flu-related deaths, CDC data show.
according to the Centers for Disease Control and Prevention.
The proportion of outpatient visits for influenza-like illness (ILI) was 3.3% for the most recent measurement period, the CDC’s influenza division reported Jan 25. The previous 2-week decline had seen ILI visits dip down to 3.1% for the week ending Jan. 12 after hitting a season high of 4%.
To go along with the national increase in visits, more states reported high levels of flu activity. For the week ending Jan. 19, seven states were at level 10 on the CDC’s 1-10 scale, compared with four the previous week, and there were 18 states in the high range (levels 8-10), compared with 9 the week before, the CDC said.
Three flu-related pediatric deaths were reported in the week ending Jan. 19, although all three occurred during earlier weeks. The total number of pediatric deaths for the 2018-2019 season is now up to 22. Deaths among all ages, which are reported a week later, totaled 118 for the week ending Jan. 12, with 63% of reporting complete. There were 144 deaths during the week ending Jan. 5, with reporting 86% complete. During the second full week of 2018, in the middle of the very severe 2017-2018 season, there were 1,537 flu-related deaths, CDC data show.
SNOT-22 may help identify patients with undiagnosed OSA
CORONADO, CALIF. – results from a retrospective analysis demonstrated.
“We know based on experience and prior studies that there is significant overlap in symptoms for obstructive sleep apnea and chronic rhinosinusitis [CRS], which are two common conditions in the general population,” one of the study authors, David W. Jang, MD, said in an interview in advance of the Triological Society’s Combined Sections Meeting. “Therefore, it is important to identify patients with undiagnosed OSA who may present to the physician with nose- and sinus-related symptoms.”
Dr. Jang, assistant professor of rhinology and endoscopic skull surgery in the department of surgery at Duke University, Durham, N.C., and his colleagues conducted a 3-year retrospective analysis of 165 adults who presented with a rhinologic chief complaint and completed the SNOT-22 survey. The researchers compared SNOT-22 survey results between patients with untreated OSA confirmed on polysomnography without chronic rhinosinusitis and a control group of CRS patients. A chi-square test with Bonferroni correction was used for analysis.
Of the 165 patients, 41 met criteria for untreated OSA, based on a mean apnea-hypopnea index of 29.3, while 124 were included in the CRS control group. Sleep and psychological domain scores were not significantly different between the two groups, although patients in the OSA group were more likely to choose a sleep-related symptom as their most important complaint (MIC) (P less than .001). As for the cardinal symptoms of CRS, nasal discharge and loss of smell were significantly higher in the CRS group (P less than .001), while facial pain and nasal obstruction were not significantly different (P = .117 and P = .198, respectively). Facial pain and nasal obstruction were the most common MICs in the rhinologic domain for OSA patients; thick nasal discharge and postnasal discharge were the most common MICs reported by patients in the CRS group.

“It was surprising that, for the cardinal symptoms of CRS, only two of the four were significantly worse for the CRS group and predictive of CRS [nasal discharge and loss of smell],” Dr. Jang said. “Nasal obstruction and facial pain scores were similar between the two groups. Also, there was no significant difference in each of the sleep-related questions when comparing the CRS and OSA groups.”
He concluded that the findings further underscore the “significant overlap in symptoms between CRS and OSA. The SNOT-22 questionnaire may help identify patients with undiagnosed OSA.”
Dr. Jang acknowledged certain limitations of the study, including its retrospective design and relatively small sample size. He reported receiving research funding from Olympus.
The meeting was jointly sponsored by the Triological Society and the American College of Surgeons.
CORONADO, CALIF. – results from a retrospective analysis demonstrated.
“We know based on experience and prior studies that there is significant overlap in symptoms for obstructive sleep apnea and chronic rhinosinusitis [CRS], which are two common conditions in the general population,” one of the study authors, David W. Jang, MD, said in an interview in advance of the Triological Society’s Combined Sections Meeting. “Therefore, it is important to identify patients with undiagnosed OSA who may present to the physician with nose- and sinus-related symptoms.”
Dr. Jang, assistant professor of rhinology and endoscopic skull surgery in the department of surgery at Duke University, Durham, N.C., and his colleagues conducted a 3-year retrospective analysis of 165 adults who presented with a rhinologic chief complaint and completed the SNOT-22 survey. The researchers compared SNOT-22 survey results between patients with untreated OSA confirmed on polysomnography without chronic rhinosinusitis and a control group of CRS patients. A chi-square test with Bonferroni correction was used for analysis.
Of the 165 patients, 41 met criteria for untreated OSA, based on a mean apnea-hypopnea index of 29.3, while 124 were included in the CRS control group. Sleep and psychological domain scores were not significantly different between the two groups, although patients in the OSA group were more likely to choose a sleep-related symptom as their most important complaint (MIC) (P less than .001). As for the cardinal symptoms of CRS, nasal discharge and loss of smell were significantly higher in the CRS group (P less than .001), while facial pain and nasal obstruction were not significantly different (P = .117 and P = .198, respectively). Facial pain and nasal obstruction were the most common MICs in the rhinologic domain for OSA patients; thick nasal discharge and postnasal discharge were the most common MICs reported by patients in the CRS group.
“It was surprising that, for the cardinal symptoms of CRS, only two of the four were significantly worse for the CRS group and predictive of CRS [nasal discharge and loss of smell],” Dr. Jang said. “Nasal obstruction and facial pain scores were similar between the two groups. Also, there was no significant difference in each of the sleep-related questions when comparing the CRS and OSA groups.”
He concluded that the findings further underscore the “significant overlap in symptoms between CRS and OSA. The SNOT-22 questionnaire may help identify patients with undiagnosed OSA.”
Dr. Jang acknowledged certain limitations of the study, including its retrospective design and relatively small sample size. He reported receiving research funding from Olympus.
The meeting was jointly sponsored by the Triological Society and the American College of Surgeons.
CORONADO, CALIF. – results from a retrospective analysis demonstrated.
“We know based on experience and prior studies that there is significant overlap in symptoms for obstructive sleep apnea and chronic rhinosinusitis [CRS], which are two common conditions in the general population,” one of the study authors, David W. Jang, MD, said in an interview in advance of the Triological Society’s Combined Sections Meeting. “Therefore, it is important to identify patients with undiagnosed OSA who may present to the physician with nose- and sinus-related symptoms.”
Dr. Jang, assistant professor of rhinology and endoscopic skull surgery in the department of surgery at Duke University, Durham, N.C., and his colleagues conducted a 3-year retrospective analysis of 165 adults who presented with a rhinologic chief complaint and completed the SNOT-22 survey. The researchers compared SNOT-22 survey results between patients with untreated OSA confirmed on polysomnography without chronic rhinosinusitis and a control group of CRS patients. A chi-square test with Bonferroni correction was used for analysis.
Of the 165 patients, 41 met criteria for untreated OSA, based on a mean apnea-hypopnea index of 29.3, while 124 were included in the CRS control group. Sleep and psychological domain scores were not significantly different between the two groups, although patients in the OSA group were more likely to choose a sleep-related symptom as their most important complaint (MIC) (P less than .001). As for the cardinal symptoms of CRS, nasal discharge and loss of smell were significantly higher in the CRS group (P less than .001), while facial pain and nasal obstruction were not significantly different (P = .117 and P = .198, respectively). Facial pain and nasal obstruction were the most common MICs in the rhinologic domain for OSA patients; thick nasal discharge and postnasal discharge were the most common MICs reported by patients in the CRS group.
“It was surprising that, for the cardinal symptoms of CRS, only two of the four were significantly worse for the CRS group and predictive of CRS [nasal discharge and loss of smell],” Dr. Jang said. “Nasal obstruction and facial pain scores were similar between the two groups. Also, there was no significant difference in each of the sleep-related questions when comparing the CRS and OSA groups.”
He concluded that the findings further underscore the “significant overlap in symptoms between CRS and OSA. The SNOT-22 questionnaire may help identify patients with undiagnosed OSA.”
Dr. Jang acknowledged certain limitations of the study, including its retrospective design and relatively small sample size. He reported receiving research funding from Olympus.
The meeting was jointly sponsored by the Triological Society and the American College of Surgeons.
REPORTING FROM THE TRIOLOGICAL CSM
Key clinical point: Obstructive sleep apnea (OSA) should be suspected in patients with sleep dysfunction as their primary complaint without the significant nasal drainage and anosmia that characterizes chronic rhinosinusitis.
Major finding: Sleep and psychological domain scores on the SNOT-22 were not significantly different between patients with chronic rhinosinusitis and those with OSA, although OSA patients were more likely to choose a sleep-related symptom as their most important complaint (P less than .001).
Study details: A retrospective analysis of 165 adults who presented with a rhinologic chief complaint and completed the SNOT-22 survey.
Disclosures: Dr. Jang reported receiving research funding from Olympus.
New study determines factors that can send flu patients to the ICU
Numerous independent factors – including a history of obstructive/central sleep apnea syndrome (OSAS/CSAS) or myocardial infarction, along with a body mass index greater than 30 g/m2 – could be related to ICU admission and subsequent high mortality rates in influenza patients, according to an analysis of patients in the Netherlands who were treated during the influenza epidemic of 2015-2016.

Along with determining these factors, lead author M.C. Beumer, of Radboud University Medical Center, the Netherlands, and his coauthors found that “coinfections with bacterial, fungal, and viral pathogens developed more often in patients who were admitted to the ICU.” The study was published in the Journal of Critical Care.
The coauthors reviewed 199 influenza patients who were admitted to two medical centers in the Netherlands during October 2015–April 2016. Of those patients, 45 (23%) were admitted to the ICU, primarily because of respiratory failure, and their mortality rate was 17/45 (38%) versus an overall mortality rate of 18/199 (9%).
Compared with patients in the normal ward, patients admitted to the ICU more frequently had a history of OSAS/CSAS (11% vs. 3%; P = .03) and MI (20% vs. 6%; P = .007), along with a BMI higher than 30 g/m2 (30% vs. 15%; P = .04) and dyspnea as a symptom (77% vs. 48%,; P = .001). In addition, more ICU-admitted patients had influenza A rather than influenza B, compared with those not admitted (87% vs. 66%; P = .009).
Pulmonary coinfections – including bacterial, fungal, and viral pathogens – were also proportionally higher among the 45 ICU patients (56% vs. 20%; P less than .0001). The most common bacterial pathogens were Staphylococcus aureus (11%) and Streptococcus pneumoniae (7%) while Aspergillus fumigatus (18%) and Pneumocystis jirovecii (7%) topped the fungal pathogens.
Mr. Beumer and his colleagues noted potential limitations of their work, including the selection of patients from among the “most severely ill” contributing to an ICU admission rate that surpassed the 5%-10% described elsewhere. They also admitted that their study relied on a “relatively small sample size,” focusing on one seasonal influenza outbreak. However, “despite the limited validity,” they reiterated that “the identified factors may contribute to a complicated disease course and could represent a tool for early recognition of the influenza patients at risk for a complicated disease course.”
The authors reported no conflicts of interest.
SOURCE: Beumer MC et al. J Crit Care. 2019;50:59-65.
.
Numerous independent factors – including a history of obstructive/central sleep apnea syndrome (OSAS/CSAS) or myocardial infarction, along with a body mass index greater than 30 g/m2 – could be related to ICU admission and subsequent high mortality rates in influenza patients, according to an analysis of patients in the Netherlands who were treated during the influenza epidemic of 2015-2016.
Along with determining these factors, lead author M.C. Beumer, of Radboud University Medical Center, the Netherlands, and his coauthors found that “coinfections with bacterial, fungal, and viral pathogens developed more often in patients who were admitted to the ICU.” The study was published in the Journal of Critical Care.
The coauthors reviewed 199 influenza patients who were admitted to two medical centers in the Netherlands during October 2015–April 2016. Of those patients, 45 (23%) were admitted to the ICU, primarily because of respiratory failure, and their mortality rate was 17/45 (38%) versus an overall mortality rate of 18/199 (9%).
Compared with patients in the normal ward, patients admitted to the ICU more frequently had a history of OSAS/CSAS (11% vs. 3%; P = .03) and MI (20% vs. 6%; P = .007), along with a BMI higher than 30 g/m2 (30% vs. 15%; P = .04) and dyspnea as a symptom (77% vs. 48%,; P = .001). In addition, more ICU-admitted patients had influenza A rather than influenza B, compared with those not admitted (87% vs. 66%; P = .009).
Pulmonary coinfections – including bacterial, fungal, and viral pathogens – were also proportionally higher among the 45 ICU patients (56% vs. 20%; P less than .0001). The most common bacterial pathogens were Staphylococcus aureus (11%) and Streptococcus pneumoniae (7%) while Aspergillus fumigatus (18%) and Pneumocystis jirovecii (7%) topped the fungal pathogens.
Mr. Beumer and his colleagues noted potential limitations of their work, including the selection of patients from among the “most severely ill” contributing to an ICU admission rate that surpassed the 5%-10% described elsewhere. They also admitted that their study relied on a “relatively small sample size,” focusing on one seasonal influenza outbreak. However, “despite the limited validity,” they reiterated that “the identified factors may contribute to a complicated disease course and could represent a tool for early recognition of the influenza patients at risk for a complicated disease course.”
The authors reported no conflicts of interest.
SOURCE: Beumer MC et al. J Crit Care. 2019;50:59-65.
.
Numerous independent factors – including a history of obstructive/central sleep apnea syndrome (OSAS/CSAS) or myocardial infarction, along with a body mass index greater than 30 g/m2 – could be related to ICU admission and subsequent high mortality rates in influenza patients, according to an analysis of patients in the Netherlands who were treated during the influenza epidemic of 2015-2016.
Along with determining these factors, lead author M.C. Beumer, of Radboud University Medical Center, the Netherlands, and his coauthors found that “coinfections with bacterial, fungal, and viral pathogens developed more often in patients who were admitted to the ICU.” The study was published in the Journal of Critical Care.
The coauthors reviewed 199 influenza patients who were admitted to two medical centers in the Netherlands during October 2015–April 2016. Of those patients, 45 (23%) were admitted to the ICU, primarily because of respiratory failure, and their mortality rate was 17/45 (38%) versus an overall mortality rate of 18/199 (9%).
Compared with patients in the normal ward, patients admitted to the ICU more frequently had a history of OSAS/CSAS (11% vs. 3%; P = .03) and MI (20% vs. 6%; P = .007), along with a BMI higher than 30 g/m2 (30% vs. 15%; P = .04) and dyspnea as a symptom (77% vs. 48%,; P = .001). In addition, more ICU-admitted patients had influenza A rather than influenza B, compared with those not admitted (87% vs. 66%; P = .009).
Pulmonary coinfections – including bacterial, fungal, and viral pathogens – were also proportionally higher among the 45 ICU patients (56% vs. 20%; P less than .0001). The most common bacterial pathogens were Staphylococcus aureus (11%) and Streptococcus pneumoniae (7%) while Aspergillus fumigatus (18%) and Pneumocystis jirovecii (7%) topped the fungal pathogens.
Mr. Beumer and his colleagues noted potential limitations of their work, including the selection of patients from among the “most severely ill” contributing to an ICU admission rate that surpassed the 5%-10% described elsewhere. They also admitted that their study relied on a “relatively small sample size,” focusing on one seasonal influenza outbreak. However, “despite the limited validity,” they reiterated that “the identified factors may contribute to a complicated disease course and could represent a tool for early recognition of the influenza patients at risk for a complicated disease course.”
The authors reported no conflicts of interest.
SOURCE: Beumer MC et al. J Crit Care. 2019;50:59-65.
.
FROM THE JOURNAL OF CRITICAL CARE
Key clinical point:
Major finding: Flu patients in the ICU more frequently had a history of obstructive/central sleep apnea syndrome (11% vs. 3%; P = .03) and MI (20% vs. 6%; P = .007), compared with non-ICU flu patients.
Study details: A retrospective cohort study of 199 flu patients who were admitted to two academic hospitals in the Netherlands.
Disclosures: The authors reported no conflicts of interest.
Source: Beumer MC et al. J Crit Care. 2019; 50:59-65.
Prescribed opioids increase pneumonia risk in patients with, without HIV
Prescribed opioids were associated with an increase in community-acquired pneumonia in patients with and without HIV infection, according to results of a large database study.
People living with HIV (PLWH) appeared to have a greater community-acquired pneumonia (CAP) risk at lower opioid doses and particularly with immunosuppressive opioids compared with uninfected patients, although the difference was not significant, E. Jennifer Edelman, MD, of Yale University, New Haven, Conn., and her colleagues wrote in JAMA Internal Medicine.
The researchers performed a nested case-control study comprising 25,392 participants (98.9% men; mean age, 55 years) in the Veterans Aging Cohort Study from Jan. 1, 2000, through Dec. 31, 2012.
Dr. Edelman and her colleagues compared the characteristics of 4,246 CAP cases with those of 21,146 uninfected controls in the sample. They also compared cases and controls by HIV status. They ran bivariate and multivariate analysis to estimate odds ratios for CAP risk associated with opioid exposure. In addition, the researchers ran models stratified by HIV status and formally checked for an interaction between prescribed opioid characteristics and HIV status.
In unadjusted logistic regression, prescribed opioids were associated with increased odds of CAP, with the greatest risk observed with currently prescribed opioids, compared with past prescribed opioids or no opioids.
Prescribed opioids remained associated with CAP in the adjusted models for past unknown or nonimmunosuppressive (adjusted OR, 1.24; 95% confidence interval, 1.09-1.40) and past immunosuppressive opioid use (aOR, 1.42; 95% CI, 1.21-1.67).
For currently prescribed opioids, nonimmunosuppressive or unknown, the aOR was 1.23 (95% CI, 1.03-1.48). For currently prescribed immunosuppressive opioids, the aOR was 3.18 (95% CI, 2.44-4.14).
The researchers also found evidence of a dose-response effect such that currently prescribed high-dose opioids were associated with the greatest CAP risk, followed by medium- and then by low-dose opioids, whether immunosuppressive or not.
With regard to the effect of HIV status in stratified, adjusted analyses, CAP risk tended to be greater among PLWH with current prescribed opioids, especially immunosuppressive opioids, compared with uninfected patients. However, the overall interaction term for opioid × HIV status was not significant (P = .36).
Although the researchers stated that a limitation of their study was an inability to prove causality or rule out respiratory depression (vs. immunosuppression) as the cause of the increased CAP risk, “the observed effects of opioid immunosuppressive properties and CAP risk lend support to our hypothesis that opioids have clinically relevant immunosuppressive properties.”
Dr. Edelman and her colleagues cited several limitations. For example, they were not able to determine whether patients took their prescribed medications appropriately and assess whether the patients took nonmedically prescribed opioids. Also, because men made up such a large portion of the study population, it is unclear whether the results are generalizable to women.
Nevertheless, the study “adds to growing evidence of potential medical harms associated with prescribed opioids,” they wrote.
“Health care professionals should be aware of this additional CAP risk when they prescribe opioids, and future studies should investigate the effects of opioids prescribed for longer durations and on other immune-related outcomes,” wrote Dr. Edelman and her colleagues. “Understanding whether mitigating the risk of prescribed opioids for CAP is possible by using a lower dose and nonimmunosuppressive opioids awaits further study.”
However, without such data, when prescribed opioids are warranted, physicians should attempt to modify other factors known to affect CAP risk, including smoking and lack of vaccination, Dr. Edelman and her colleagues concluded.
Several U.S. government agencies and Yale University provided funding for the study. The authors reported that they had no conflicts.
SOURCE: Edelman EJ et al. JAMA Intern Med. 2019 Jan 7. doi: 10.1001/jamainternmed.2018.6101.
Prescribed opioids were associated with an increase in community-acquired pneumonia in patients with and without HIV infection, according to results of a large database study.
People living with HIV (PLWH) appeared to have a greater community-acquired pneumonia (CAP) risk at lower opioid doses and particularly with immunosuppressive opioids compared with uninfected patients, although the difference was not significant, E. Jennifer Edelman, MD, of Yale University, New Haven, Conn., and her colleagues wrote in JAMA Internal Medicine.
The researchers performed a nested case-control study comprising 25,392 participants (98.9% men; mean age, 55 years) in the Veterans Aging Cohort Study from Jan. 1, 2000, through Dec. 31, 2012.
Dr. Edelman and her colleagues compared the characteristics of 4,246 CAP cases with those of 21,146 uninfected controls in the sample. They also compared cases and controls by HIV status. They ran bivariate and multivariate analysis to estimate odds ratios for CAP risk associated with opioid exposure. In addition, the researchers ran models stratified by HIV status and formally checked for an interaction between prescribed opioid characteristics and HIV status.
In unadjusted logistic regression, prescribed opioids were associated with increased odds of CAP, with the greatest risk observed with currently prescribed opioids, compared with past prescribed opioids or no opioids.
Prescribed opioids remained associated with CAP in the adjusted models for past unknown or nonimmunosuppressive (adjusted OR, 1.24; 95% confidence interval, 1.09-1.40) and past immunosuppressive opioid use (aOR, 1.42; 95% CI, 1.21-1.67).
For currently prescribed opioids, nonimmunosuppressive or unknown, the aOR was 1.23 (95% CI, 1.03-1.48). For currently prescribed immunosuppressive opioids, the aOR was 3.18 (95% CI, 2.44-4.14).
The researchers also found evidence of a dose-response effect such that currently prescribed high-dose opioids were associated with the greatest CAP risk, followed by medium- and then by low-dose opioids, whether immunosuppressive or not.
With regard to the effect of HIV status in stratified, adjusted analyses, CAP risk tended to be greater among PLWH with current prescribed opioids, especially immunosuppressive opioids, compared with uninfected patients. However, the overall interaction term for opioid × HIV status was not significant (P = .36).
Although the researchers stated that a limitation of their study was an inability to prove causality or rule out respiratory depression (vs. immunosuppression) as the cause of the increased CAP risk, “the observed effects of opioid immunosuppressive properties and CAP risk lend support to our hypothesis that opioids have clinically relevant immunosuppressive properties.”
Dr. Edelman and her colleagues cited several limitations. For example, they were not able to determine whether patients took their prescribed medications appropriately and assess whether the patients took nonmedically prescribed opioids. Also, because men made up such a large portion of the study population, it is unclear whether the results are generalizable to women.
Nevertheless, the study “adds to growing evidence of potential medical harms associated with prescribed opioids,” they wrote.
“Health care professionals should be aware of this additional CAP risk when they prescribe opioids, and future studies should investigate the effects of opioids prescribed for longer durations and on other immune-related outcomes,” wrote Dr. Edelman and her colleagues. “Understanding whether mitigating the risk of prescribed opioids for CAP is possible by using a lower dose and nonimmunosuppressive opioids awaits further study.”
However, without such data, when prescribed opioids are warranted, physicians should attempt to modify other factors known to affect CAP risk, including smoking and lack of vaccination, Dr. Edelman and her colleagues concluded.
Several U.S. government agencies and Yale University provided funding for the study. The authors reported that they had no conflicts.
SOURCE: Edelman EJ et al. JAMA Intern Med. 2019 Jan 7. doi: 10.1001/jamainternmed.2018.6101.
Prescribed opioids were associated with an increase in community-acquired pneumonia in patients with and without HIV infection, according to results of a large database study.
People living with HIV (PLWH) appeared to have a greater community-acquired pneumonia (CAP) risk at lower opioid doses and particularly with immunosuppressive opioids compared with uninfected patients, although the difference was not significant, E. Jennifer Edelman, MD, of Yale University, New Haven, Conn., and her colleagues wrote in JAMA Internal Medicine.
The researchers performed a nested case-control study comprising 25,392 participants (98.9% men; mean age, 55 years) in the Veterans Aging Cohort Study from Jan. 1, 2000, through Dec. 31, 2012.
Dr. Edelman and her colleagues compared the characteristics of 4,246 CAP cases with those of 21,146 uninfected controls in the sample. They also compared cases and controls by HIV status. They ran bivariate and multivariate analysis to estimate odds ratios for CAP risk associated with opioid exposure. In addition, the researchers ran models stratified by HIV status and formally checked for an interaction between prescribed opioid characteristics and HIV status.
In unadjusted logistic regression, prescribed opioids were associated with increased odds of CAP, with the greatest risk observed with currently prescribed opioids, compared with past prescribed opioids or no opioids.
Prescribed opioids remained associated with CAP in the adjusted models for past unknown or nonimmunosuppressive (adjusted OR, 1.24; 95% confidence interval, 1.09-1.40) and past immunosuppressive opioid use (aOR, 1.42; 95% CI, 1.21-1.67).
For currently prescribed opioids, nonimmunosuppressive or unknown, the aOR was 1.23 (95% CI, 1.03-1.48). For currently prescribed immunosuppressive opioids, the aOR was 3.18 (95% CI, 2.44-4.14).
The researchers also found evidence of a dose-response effect such that currently prescribed high-dose opioids were associated with the greatest CAP risk, followed by medium- and then by low-dose opioids, whether immunosuppressive or not.
With regard to the effect of HIV status in stratified, adjusted analyses, CAP risk tended to be greater among PLWH with current prescribed opioids, especially immunosuppressive opioids, compared with uninfected patients. However, the overall interaction term for opioid × HIV status was not significant (P = .36).
Although the researchers stated that a limitation of their study was an inability to prove causality or rule out respiratory depression (vs. immunosuppression) as the cause of the increased CAP risk, “the observed effects of opioid immunosuppressive properties and CAP risk lend support to our hypothesis that opioids have clinically relevant immunosuppressive properties.”
Dr. Edelman and her colleagues cited several limitations. For example, they were not able to determine whether patients took their prescribed medications appropriately and assess whether the patients took nonmedically prescribed opioids. Also, because men made up such a large portion of the study population, it is unclear whether the results are generalizable to women.
Nevertheless, the study “adds to growing evidence of potential medical harms associated with prescribed opioids,” they wrote.
“Health care professionals should be aware of this additional CAP risk when they prescribe opioids, and future studies should investigate the effects of opioids prescribed for longer durations and on other immune-related outcomes,” wrote Dr. Edelman and her colleagues. “Understanding whether mitigating the risk of prescribed opioids for CAP is possible by using a lower dose and nonimmunosuppressive opioids awaits further study.”
However, without such data, when prescribed opioids are warranted, physicians should attempt to modify other factors known to affect CAP risk, including smoking and lack of vaccination, Dr. Edelman and her colleagues concluded.
Several U.S. government agencies and Yale University provided funding for the study. The authors reported that they had no conflicts.
SOURCE: Edelman EJ et al. JAMA Intern Med. 2019 Jan 7. doi: 10.1001/jamainternmed.2018.6101.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Prescribed opioids, especially those with immunosuppressive properties, are associated with increased community-acquired pneumonia risk.
Major finding: For currently prescribed immunosuppressive opioids, the adjusted odds ratio for community-acquired pneumonia was 3.18 (95% confidence interval, 2.44-4.14).
Study details: A nested case-control study of 25,392 patients in the Veterans Aging Cohort Study from Jan. 1, 2000, through Dec. 31, 2012.
Disclosures: Funding was provided by a variety of government organizations and Yale University, New Haven, Conn. The authors reported that they had no conflicts.
Source: Edelman EJ et al. JAMA Intern Med. 2019 Jan 7. doi: 10.1001/jamainternmed.2018.6101.
COPD linked to higher in-hospital death rates in patients with PAD
A growing body of evidence suggests that, along with other vascular beds, smoking and chronic obstructive pulmonary disease (COPD) affect the arteries of the lower limbs in terms of the development of peripheral arterial disease (PAD), reported Karsten Keller, MD, of the Johannes Gutenberg-University Mainz (Germany) and his colleagues.

This provided the rationale for their large database analysis of inpatients with concomitant COPD and PAD. They found that the additional presence of COPD was associated with increased in-hospital mortality in patients with PAD.
“Our data suggest that COPD increased the mortality of PAD patients by the factor 1.2-fold,” they wrote in Respiratory Medicine. “Unexpectedly, this increase was not driven by [myocardial infarction] as the life-threatening acute presentation of [coronary artery disease], but rather related to an increased risk for [pulmonary embolism] and a higher coprevalence of cancer.”
Dr. Keller and his colleagues inspected the German inpatient national database based on ICD codes. They identified 5,611,827 adult inpatients (64.8% men) diagnosed with PAD between January 2005 and December 2015, and of those, 13.6% also were coded for COPD. Overall, 277,894 PAD patients (5.0%) died in the hospital, Dr. Keller and his colleagues wrote.
The all-cause, in-hospital mortality was significantly higher in PAD patients with COPD, compared with those without COPD (6.5% vs. 4.7%, respectively; P less than .001), and cardiovascular events comprising pulmonary embolism (PE), deep vein thrombosis (DVT), and myocardial infarction (MI) occurred more often in coprevalence with PAD and COPD than in PAD without COPD.
In PAD patients, COPD was an independent predictor of in-hospital death (odds ratio, 1.16; 95% confidence interval, 1.15-1.17; P less than .001) as well as an independent predictor for PE (OR, 1.44; 95% CI, 1.40-1.49; P less than .001).
Overall, PAD patients with COPD were of similar age as (73 years), but stayed slightly longer in the hospital than (9 vs. 8 days), those without COPD. PAD patients without COPD revealed more often cardiovascular risk factors like essential arterial hypertension and diabetes, but the prevalence of cardiovascular diseases such as coronary artery disease and heart failure were more often found in PAD patients with COPD. In addition, cancer and renal insufficiency also were more common in PAD patients with COPD, according to the authors.
“Remarkably, PAD patients with COPD showed more frequently lower PAD stages than those without COPD. Especially, PAD stage IV was more prevalent in PAD patients without COPD (19.6% vs. 13.8%; P less than 0.001),” the authors stated. In addition, amputations were more often performed in PAD patients without COPD.
Dr. Keller and his colleagues had the following conclusions regarding the clinical implications of their study: “I) PAD patients with long-standing tobacco use might benefit from COPD screening and treatment. II) PAD patients with additional COPD should be monitored more intensively, and the treatment for COPD should be optimized. III) COPD increases the risk for PE, and it is critical not to overlook this life-threatening disease. IV) MI and PE are important causes of in-hospital death in PAD patients with and without COPD.”
The German Federal Ministry of Education and Research funded the study, and the authors reported having no conflicts.
SOURCE: Keller K et al. Respir Med. 2019 Feb;147:1-6.
A growing body of evidence suggests that, along with other vascular beds, smoking and chronic obstructive pulmonary disease (COPD) affect the arteries of the lower limbs in terms of the development of peripheral arterial disease (PAD), reported Karsten Keller, MD, of the Johannes Gutenberg-University Mainz (Germany) and his colleagues.
This provided the rationale for their large database analysis of inpatients with concomitant COPD and PAD. They found that the additional presence of COPD was associated with increased in-hospital mortality in patients with PAD.
“Our data suggest that COPD increased the mortality of PAD patients by the factor 1.2-fold,” they wrote in Respiratory Medicine. “Unexpectedly, this increase was not driven by [myocardial infarction] as the life-threatening acute presentation of [coronary artery disease], but rather related to an increased risk for [pulmonary embolism] and a higher coprevalence of cancer.”
Dr. Keller and his colleagues inspected the German inpatient national database based on ICD codes. They identified 5,611,827 adult inpatients (64.8% men) diagnosed with PAD between January 2005 and December 2015, and of those, 13.6% also were coded for COPD. Overall, 277,894 PAD patients (5.0%) died in the hospital, Dr. Keller and his colleagues wrote.
The all-cause, in-hospital mortality was significantly higher in PAD patients with COPD, compared with those without COPD (6.5% vs. 4.7%, respectively; P less than .001), and cardiovascular events comprising pulmonary embolism (PE), deep vein thrombosis (DVT), and myocardial infarction (MI) occurred more often in coprevalence with PAD and COPD than in PAD without COPD.
In PAD patients, COPD was an independent predictor of in-hospital death (odds ratio, 1.16; 95% confidence interval, 1.15-1.17; P less than .001) as well as an independent predictor for PE (OR, 1.44; 95% CI, 1.40-1.49; P less than .001).
Overall, PAD patients with COPD were of similar age as (73 years), but stayed slightly longer in the hospital than (9 vs. 8 days), those without COPD. PAD patients without COPD revealed more often cardiovascular risk factors like essential arterial hypertension and diabetes, but the prevalence of cardiovascular diseases such as coronary artery disease and heart failure were more often found in PAD patients with COPD. In addition, cancer and renal insufficiency also were more common in PAD patients with COPD, according to the authors.
“Remarkably, PAD patients with COPD showed more frequently lower PAD stages than those without COPD. Especially, PAD stage IV was more prevalent in PAD patients without COPD (19.6% vs. 13.8%; P less than 0.001),” the authors stated. In addition, amputations were more often performed in PAD patients without COPD.
Dr. Keller and his colleagues had the following conclusions regarding the clinical implications of their study: “I) PAD patients with long-standing tobacco use might benefit from COPD screening and treatment. II) PAD patients with additional COPD should be monitored more intensively, and the treatment for COPD should be optimized. III) COPD increases the risk for PE, and it is critical not to overlook this life-threatening disease. IV) MI and PE are important causes of in-hospital death in PAD patients with and without COPD.”
The German Federal Ministry of Education and Research funded the study, and the authors reported having no conflicts.
SOURCE: Keller K et al. Respir Med. 2019 Feb;147:1-6.
A growing body of evidence suggests that, along with other vascular beds, smoking and chronic obstructive pulmonary disease (COPD) affect the arteries of the lower limbs in terms of the development of peripheral arterial disease (PAD), reported Karsten Keller, MD, of the Johannes Gutenberg-University Mainz (Germany) and his colleagues.
This provided the rationale for their large database analysis of inpatients with concomitant COPD and PAD. They found that the additional presence of COPD was associated with increased in-hospital mortality in patients with PAD.
“Our data suggest that COPD increased the mortality of PAD patients by the factor 1.2-fold,” they wrote in Respiratory Medicine. “Unexpectedly, this increase was not driven by [myocardial infarction] as the life-threatening acute presentation of [coronary artery disease], but rather related to an increased risk for [pulmonary embolism] and a higher coprevalence of cancer.”
Dr. Keller and his colleagues inspected the German inpatient national database based on ICD codes. They identified 5,611,827 adult inpatients (64.8% men) diagnosed with PAD between January 2005 and December 2015, and of those, 13.6% also were coded for COPD. Overall, 277,894 PAD patients (5.0%) died in the hospital, Dr. Keller and his colleagues wrote.
The all-cause, in-hospital mortality was significantly higher in PAD patients with COPD, compared with those without COPD (6.5% vs. 4.7%, respectively; P less than .001), and cardiovascular events comprising pulmonary embolism (PE), deep vein thrombosis (DVT), and myocardial infarction (MI) occurred more often in coprevalence with PAD and COPD than in PAD without COPD.
In PAD patients, COPD was an independent predictor of in-hospital death (odds ratio, 1.16; 95% confidence interval, 1.15-1.17; P less than .001) as well as an independent predictor for PE (OR, 1.44; 95% CI, 1.40-1.49; P less than .001).
Overall, PAD patients with COPD were of similar age as (73 years), but stayed slightly longer in the hospital than (9 vs. 8 days), those without COPD. PAD patients without COPD revealed more often cardiovascular risk factors like essential arterial hypertension and diabetes, but the prevalence of cardiovascular diseases such as coronary artery disease and heart failure were more often found in PAD patients with COPD. In addition, cancer and renal insufficiency also were more common in PAD patients with COPD, according to the authors.
“Remarkably, PAD patients with COPD showed more frequently lower PAD stages than those without COPD. Especially, PAD stage IV was more prevalent in PAD patients without COPD (19.6% vs. 13.8%; P less than 0.001),” the authors stated. In addition, amputations were more often performed in PAD patients without COPD.
Dr. Keller and his colleagues had the following conclusions regarding the clinical implications of their study: “I) PAD patients with long-standing tobacco use might benefit from COPD screening and treatment. II) PAD patients with additional COPD should be monitored more intensively, and the treatment for COPD should be optimized. III) COPD increases the risk for PE, and it is critical not to overlook this life-threatening disease. IV) MI and PE are important causes of in-hospital death in PAD patients with and without COPD.”
The German Federal Ministry of Education and Research funded the study, and the authors reported having no conflicts.
SOURCE: Keller K et al. Respir Med. 2019 Feb;147:1-6.
FROM RESPIRATORY MEDICINE
Key clinical point:
Major finding: All-cause, in-hospital mortality was significantly higher in PAD patients with COPD, compared with those without (6.5% vs. 4.7%; P less than 0.001).
Study details: Database analysis of 5.6 million German PAD inpatients stratified for COPD.
Disclosures: The German Federal Ministry of Education and Research funded the study, and the authors reported having no conflicts.
Source: Keller K et al. Respir Med. 2019 Feb;147:1-6.
Flu activity down for second consecutive week
The second week of the new year brought a second straight week of declining activity for the 2018-2019 flu season, according to the Centers for Disease Control and Prevention.
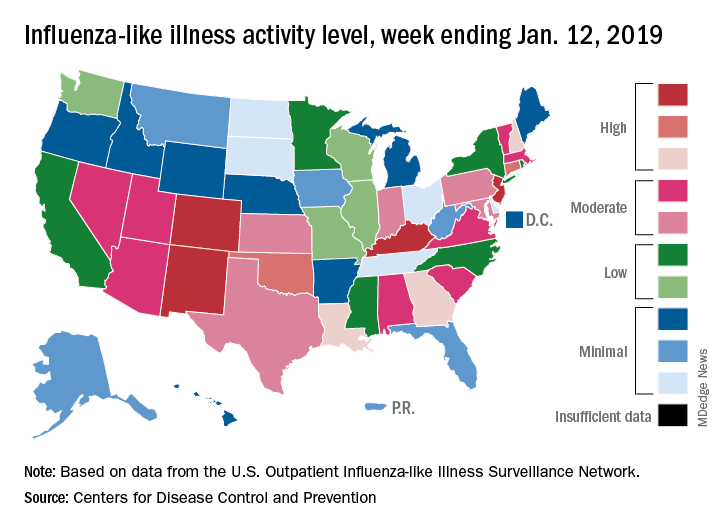
The proportion of outpatient visits for influenza-like illness (ILI) was 3.1% for the week ending Jan. 12, 2019, down from 3.5% the previous week but still above the national baseline level of 2.2%, the CDC’s influenza division reported Jan. 18.
Activity was also down at the state level. There were 4 states – Colorado, Kentucky, New Jersey, and New Mexico – at level 10 on the CDC’s 1-10 scale for ILI activity, compared with 10 the week before, and a total of 9 were in the high range from 8 to 10, compared with 15 the previous week, data from the influenza division show.
Reports of total influenza deaths, which lag a week behind other measures, continue to rise: 111 for the week ending Jan. 5, although reporting is only 72% complete. There were 89 deaths during the previous week, with reporting 82% complete so far. Total flu-related deaths among children are up to 19 for the 2018-2019 season after three more were reported during the week ending Jan. 12, the CDC said. Influenza deaths from the comparable weeks of the much more severe 2017-2018 season were 1,163 for all ages and 10 for children.
The second week of the new year brought a second straight week of declining activity for the 2018-2019 flu season, according to the Centers for Disease Control and Prevention.
The proportion of outpatient visits for influenza-like illness (ILI) was 3.1% for the week ending Jan. 12, 2019, down from 3.5% the previous week but still above the national baseline level of 2.2%, the CDC’s influenza division reported Jan. 18.
Activity was also down at the state level. There were 4 states – Colorado, Kentucky, New Jersey, and New Mexico – at level 10 on the CDC’s 1-10 scale for ILI activity, compared with 10 the week before, and a total of 9 were in the high range from 8 to 10, compared with 15 the previous week, data from the influenza division show.
Reports of total influenza deaths, which lag a week behind other measures, continue to rise: 111 for the week ending Jan. 5, although reporting is only 72% complete. There were 89 deaths during the previous week, with reporting 82% complete so far. Total flu-related deaths among children are up to 19 for the 2018-2019 season after three more were reported during the week ending Jan. 12, the CDC said. Influenza deaths from the comparable weeks of the much more severe 2017-2018 season were 1,163 for all ages and 10 for children.
The second week of the new year brought a second straight week of declining activity for the 2018-2019 flu season, according to the Centers for Disease Control and Prevention.
The proportion of outpatient visits for influenza-like illness (ILI) was 3.1% for the week ending Jan. 12, 2019, down from 3.5% the previous week but still above the national baseline level of 2.2%, the CDC’s influenza division reported Jan. 18.
Activity was also down at the state level. There were 4 states – Colorado, Kentucky, New Jersey, and New Mexico – at level 10 on the CDC’s 1-10 scale for ILI activity, compared with 10 the week before, and a total of 9 were in the high range from 8 to 10, compared with 15 the previous week, data from the influenza division show.
Reports of total influenza deaths, which lag a week behind other measures, continue to rise: 111 for the week ending Jan. 5, although reporting is only 72% complete. There were 89 deaths during the previous week, with reporting 82% complete so far. Total flu-related deaths among children are up to 19 for the 2018-2019 season after three more were reported during the week ending Jan. 12, the CDC said. Influenza deaths from the comparable weeks of the much more severe 2017-2018 season were 1,163 for all ages and 10 for children.
FDA approves Adacel for repeat Tdap vaccinations
The Food and Drug Administration has approved the expanded use of Adacel (Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis (Tdap) Vaccine Adsorbed) to include repeat vaccinations 8 years or more after the first vaccination in people aged 10-64 years.

The expanded indication was based on results of a randomized, controlled trial, published in the Journal of the Pediatric Infectious Diseases Society, in which more than 1,300 adults aged 18-64 years received either Adacel or a Td (tetanus-diphtheria) vaccine 8-12 years after receiving a previous dose of Adacel.
Over the course of the study, no significant difference in adverse event incidence was observed between groups. Injection-site reaction was the most common adverse event during the study, occurring in 87.7% of those who received Adacel and 88.0% of those who received the Td vaccine. Other common adverse events associated with Adacel include headache, body ache or muscle weakness, tiredness, muscle aches, and general discomfort.
“While strong vaccination programs are in place for young adolescents, a single Tdap immunization does not offer lifetime protection against pertussis due to waning immunity. The licensure of Adacel as the first Tdap vaccine in the U.S. for repeat vaccination is an important step for eligible patients and offers flexibility for health care providers to help manage their immunization schedules,” said David P. Greenberg, MD, regional medical head North America at Sanofi Pasteur, in the press release.
Find the full press release on the Sanofi website.
The Food and Drug Administration has approved the expanded use of Adacel (Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis (Tdap) Vaccine Adsorbed) to include repeat vaccinations 8 years or more after the first vaccination in people aged 10-64 years.
The expanded indication was based on results of a randomized, controlled trial, published in the Journal of the Pediatric Infectious Diseases Society, in which more than 1,300 adults aged 18-64 years received either Adacel or a Td (tetanus-diphtheria) vaccine 8-12 years after receiving a previous dose of Adacel.
Over the course of the study, no significant difference in adverse event incidence was observed between groups. Injection-site reaction was the most common adverse event during the study, occurring in 87.7% of those who received Adacel and 88.0% of those who received the Td vaccine. Other common adverse events associated with Adacel include headache, body ache or muscle weakness, tiredness, muscle aches, and general discomfort.
“While strong vaccination programs are in place for young adolescents, a single Tdap immunization does not offer lifetime protection against pertussis due to waning immunity. The licensure of Adacel as the first Tdap vaccine in the U.S. for repeat vaccination is an important step for eligible patients and offers flexibility for health care providers to help manage their immunization schedules,” said David P. Greenberg, MD, regional medical head North America at Sanofi Pasteur, in the press release.
Find the full press release on the Sanofi website.
The Food and Drug Administration has approved the expanded use of Adacel (Tetanus Toxoid, Reduced Diphtheria Toxoid and Acellular Pertussis (Tdap) Vaccine Adsorbed) to include repeat vaccinations 8 years or more after the first vaccination in people aged 10-64 years.
The expanded indication was based on results of a randomized, controlled trial, published in the Journal of the Pediatric Infectious Diseases Society, in which more than 1,300 adults aged 18-64 years received either Adacel or a Td (tetanus-diphtheria) vaccine 8-12 years after receiving a previous dose of Adacel.
Over the course of the study, no significant difference in adverse event incidence was observed between groups. Injection-site reaction was the most common adverse event during the study, occurring in 87.7% of those who received Adacel and 88.0% of those who received the Td vaccine. Other common adverse events associated with Adacel include headache, body ache or muscle weakness, tiredness, muscle aches, and general discomfort.
“While strong vaccination programs are in place for young adolescents, a single Tdap immunization does not offer lifetime protection against pertussis due to waning immunity. The licensure of Adacel as the first Tdap vaccine in the U.S. for repeat vaccination is an important step for eligible patients and offers flexibility for health care providers to help manage their immunization schedules,” said David P. Greenberg, MD, regional medical head North America at Sanofi Pasteur, in the press release.
Find the full press release on the Sanofi website.
INPULSIS-ON: Nintedanib shows manageable long-term safety for IPF
For patients with showed acceptable safety and tolerability and might have slowed disease progression, according to the results of the open-label INPULSIS-ON trial.

No new safety signals were identified among patients who continued nintedanib or switched from placebo to the medication after completing one of the two 52-week phase 3 INPULSIS trials, reported Bruno Crestani, MD, of H
Idiopathic pulmonary fibrosis has had a poor prognosis – before antifibrotic therapy became available in the United States, median survival after diagnosis was estimated at 3-5 years, the researchers noted. Patients often die or deteriorate because of acute declines in respiratory function, often from unknown causes. Nintedanib (Ofev) is an intracellular tyrosine kinase inhibitor first approved for idiopathic pulmonary fibrosis in the United States in 2014, based on the results of the replicate randomized, placebo-controlled, double-blind, phase 3 INPULSIS trials, in which nintedanib (150 mg twice daily) was usually tolerable, showed an acceptable overall toxicity profile, and significantly lessened the annual rate of decline in forced vital capacity (FVC), compared with placebo.
Because idiopathic pulmonary fibrosis has a chronic trajectory, data on long-term safety and efficacy were clearly desirable. “Results from the open-label extension of the [foundational] phase 2 TOMORROW trial [also] identified no new safety signals and suggested an effect of nintedanib on slowing the progression of idiopathic pulmonary fibrosis beyond 52 weeks; however, only 35 patients treated with nintedanib 150 mg twice daily entered the extension study,” Dr. Crestani and his associates noted.
The open-label INPULSIS-ON extension trial included 734 patients, which was 91% of the population that completed the INPULSIS trials. A total of 59% patients in the open-label trial continued nintedanib while the rest switched to nintedanib from placebo. When considering both cohorts, the median duration of exposure to nintedanib was 44.7 months (range, 1.9-68.3 months).
Rates of major adverse cardiovascular events were 2.4 per 100 person-years of drug exposure among treatment initiators and 3.6 per 100 person-years among continuers, the researchers reported. Rates of bleeding were 6.7 and 8.4 events per 100 person-years, respectively, while rates of myocardial infarction, using the broadest possible definition, were 0.7 and 1.3 events per 100 person-years, respectively. The most common adverse event was diarrhea, with 60.1 and 71.2 events per 100 person-years among treatment initiators and continuers, respectively. In all, 10% of treatment initiators and 5% of continuers stopped nintedanib because of diarrhea. A total of 14% of treatment initiators and 12% of continuers stopped treatment because they experienced progression of idiopathic pulmonary fibrosis, making this adverse event the most common reason to stop treatment.
The adjusted annual rate of decline in FVC was −135.1 mL overall, –145 mL in nintedanib continuers, and –119.7 mL in nintedanib initiators, which resembled the findings of the INPULSIS trials, the researcher said. They added that the difference in FVC decline between INPULSIS-ON nintedanib initiators and continuers does not seem clinically meaningful, especially given that the average FVC decline in the INPULSIS placebo group was −223.5 mL per year, and the minimal clinically important difference in FVC is thought to be 2%-6% predicted, a difference of at least 75 mL-80 mL.
Boehringer Ingelheim funded the study. Dr. Crestani disclosed grants and personal fees from Boehringer Ingelheim and Roche, grants from Apellis and MedImmune, and personal fees from AstraZeneca and Sanofi.
SOURCE: Crestani B et al. Lancet Respir Med. 2018 Sep 14. doi: 10.1016/S2213-2600(18)30339-4.
The study provides “invaluable safety data, including a very low incidence of cardiovascular events” among patients who received long-term nintedanib therapy for idiopathic pulmonary fibrosis, wrote Athol U. Wells, MD, in an editorial published alongside the study.
But the efficacy data were substantially more problematic, he said. “At first sight, the data seem to show that treatment benefits are sustained during long-term follow-up. However, this finding applied to patients completing 4 years of treatment. Approximately 70% of patients discontinued nintedanib [during the open-label extension trial].”
Death, probable treatment failure, or adverse events unrelated to idiopathic pulmonary fibrosis accounted for 62% of withdrawals from this study, and the investigators did not present FVC trends for these patients, he noted. This makes it difficult to know whether bias affected the efficacy results. Long-term stability or slow progression was seen in 30%-40% of patients, exceeding results from previous IPF cohorts, but “this finding, although encouraging, is clearly non-definitive.”
The mortality data also were problematic because the trial excluded patients with major comorbidities and severe disease, and the researchers only tracked vital status for 6 weeks after patients withdrew from INPULSIS-ON, he said. “One cannot help but feel that a major opportunity was lost in this study and, equally, in the pirfenidone extension study. An intention-to-treat study design would have provided invaluable long-term efficacy data and should be prioritized in future.”
Dr. Wells is with Royal Brompton Hospital in London. He disclosed personal fees from Boehringer Ingelheim, Intermune/Roche, Bayer, Actelion, and Raffo, outside the submitted work (Lancet Respir Med. 2018 Sep 14. doi: 10.1016/S2213-2600[18]30385-0).
The study provides “invaluable safety data, including a very low incidence of cardiovascular events” among patients who received long-term nintedanib therapy for idiopathic pulmonary fibrosis, wrote Athol U. Wells, MD, in an editorial published alongside the study.
But the efficacy data were substantially more problematic, he said. “At first sight, the data seem to show that treatment benefits are sustained during long-term follow-up. However, this finding applied to patients completing 4 years of treatment. Approximately 70% of patients discontinued nintedanib [during the open-label extension trial].”
Death, probable treatment failure, or adverse events unrelated to idiopathic pulmonary fibrosis accounted for 62% of withdrawals from this study, and the investigators did not present FVC trends for these patients, he noted. This makes it difficult to know whether bias affected the efficacy results. Long-term stability or slow progression was seen in 30%-40% of patients, exceeding results from previous IPF cohorts, but “this finding, although encouraging, is clearly non-definitive.”
The mortality data also were problematic because the trial excluded patients with major comorbidities and severe disease, and the researchers only tracked vital status for 6 weeks after patients withdrew from INPULSIS-ON, he said. “One cannot help but feel that a major opportunity was lost in this study and, equally, in the pirfenidone extension study. An intention-to-treat study design would have provided invaluable long-term efficacy data and should be prioritized in future.”
Dr. Wells is with Royal Brompton Hospital in London. He disclosed personal fees from Boehringer Ingelheim, Intermune/Roche, Bayer, Actelion, and Raffo, outside the submitted work (Lancet Respir Med. 2018 Sep 14. doi: 10.1016/S2213-2600[18]30385-0).
The study provides “invaluable safety data, including a very low incidence of cardiovascular events” among patients who received long-term nintedanib therapy for idiopathic pulmonary fibrosis, wrote Athol U. Wells, MD, in an editorial published alongside the study.
But the efficacy data were substantially more problematic, he said. “At first sight, the data seem to show that treatment benefits are sustained during long-term follow-up. However, this finding applied to patients completing 4 years of treatment. Approximately 70% of patients discontinued nintedanib [during the open-label extension trial].”
Death, probable treatment failure, or adverse events unrelated to idiopathic pulmonary fibrosis accounted for 62% of withdrawals from this study, and the investigators did not present FVC trends for these patients, he noted. This makes it difficult to know whether bias affected the efficacy results. Long-term stability or slow progression was seen in 30%-40% of patients, exceeding results from previous IPF cohorts, but “this finding, although encouraging, is clearly non-definitive.”
The mortality data also were problematic because the trial excluded patients with major comorbidities and severe disease, and the researchers only tracked vital status for 6 weeks after patients withdrew from INPULSIS-ON, he said. “One cannot help but feel that a major opportunity was lost in this study and, equally, in the pirfenidone extension study. An intention-to-treat study design would have provided invaluable long-term efficacy data and should be prioritized in future.”
Dr. Wells is with Royal Brompton Hospital in London. He disclosed personal fees from Boehringer Ingelheim, Intermune/Roche, Bayer, Actelion, and Raffo, outside the submitted work (Lancet Respir Med. 2018 Sep 14. doi: 10.1016/S2213-2600[18]30385-0).
For patients with showed acceptable safety and tolerability and might have slowed disease progression, according to the results of the open-label INPULSIS-ON trial.
No new safety signals were identified among patients who continued nintedanib or switched from placebo to the medication after completing one of the two 52-week phase 3 INPULSIS trials, reported Bruno Crestani, MD, of H
Idiopathic pulmonary fibrosis has had a poor prognosis – before antifibrotic therapy became available in the United States, median survival after diagnosis was estimated at 3-5 years, the researchers noted. Patients often die or deteriorate because of acute declines in respiratory function, often from unknown causes. Nintedanib (Ofev) is an intracellular tyrosine kinase inhibitor first approved for idiopathic pulmonary fibrosis in the United States in 2014, based on the results of the replicate randomized, placebo-controlled, double-blind, phase 3 INPULSIS trials, in which nintedanib (150 mg twice daily) was usually tolerable, showed an acceptable overall toxicity profile, and significantly lessened the annual rate of decline in forced vital capacity (FVC), compared with placebo.
Because idiopathic pulmonary fibrosis has a chronic trajectory, data on long-term safety and efficacy were clearly desirable. “Results from the open-label extension of the [foundational] phase 2 TOMORROW trial [also] identified no new safety signals and suggested an effect of nintedanib on slowing the progression of idiopathic pulmonary fibrosis beyond 52 weeks; however, only 35 patients treated with nintedanib 150 mg twice daily entered the extension study,” Dr. Crestani and his associates noted.
The open-label INPULSIS-ON extension trial included 734 patients, which was 91% of the population that completed the INPULSIS trials. A total of 59% patients in the open-label trial continued nintedanib while the rest switched to nintedanib from placebo. When considering both cohorts, the median duration of exposure to nintedanib was 44.7 months (range, 1.9-68.3 months).
Rates of major adverse cardiovascular events were 2.4 per 100 person-years of drug exposure among treatment initiators and 3.6 per 100 person-years among continuers, the researchers reported. Rates of bleeding were 6.7 and 8.4 events per 100 person-years, respectively, while rates of myocardial infarction, using the broadest possible definition, were 0.7 and 1.3 events per 100 person-years, respectively. The most common adverse event was diarrhea, with 60.1 and 71.2 events per 100 person-years among treatment initiators and continuers, respectively. In all, 10% of treatment initiators and 5% of continuers stopped nintedanib because of diarrhea. A total of 14% of treatment initiators and 12% of continuers stopped treatment because they experienced progression of idiopathic pulmonary fibrosis, making this adverse event the most common reason to stop treatment.
The adjusted annual rate of decline in FVC was −135.1 mL overall, –145 mL in nintedanib continuers, and –119.7 mL in nintedanib initiators, which resembled the findings of the INPULSIS trials, the researcher said. They added that the difference in FVC decline between INPULSIS-ON nintedanib initiators and continuers does not seem clinically meaningful, especially given that the average FVC decline in the INPULSIS placebo group was −223.5 mL per year, and the minimal clinically important difference in FVC is thought to be 2%-6% predicted, a difference of at least 75 mL-80 mL.
Boehringer Ingelheim funded the study. Dr. Crestani disclosed grants and personal fees from Boehringer Ingelheim and Roche, grants from Apellis and MedImmune, and personal fees from AstraZeneca and Sanofi.
SOURCE: Crestani B et al. Lancet Respir Med. 2018 Sep 14. doi: 10.1016/S2213-2600(18)30339-4.
For patients with showed acceptable safety and tolerability and might have slowed disease progression, according to the results of the open-label INPULSIS-ON trial.
No new safety signals were identified among patients who continued nintedanib or switched from placebo to the medication after completing one of the two 52-week phase 3 INPULSIS trials, reported Bruno Crestani, MD, of H
Idiopathic pulmonary fibrosis has had a poor prognosis – before antifibrotic therapy became available in the United States, median survival after diagnosis was estimated at 3-5 years, the researchers noted. Patients often die or deteriorate because of acute declines in respiratory function, often from unknown causes. Nintedanib (Ofev) is an intracellular tyrosine kinase inhibitor first approved for idiopathic pulmonary fibrosis in the United States in 2014, based on the results of the replicate randomized, placebo-controlled, double-blind, phase 3 INPULSIS trials, in which nintedanib (150 mg twice daily) was usually tolerable, showed an acceptable overall toxicity profile, and significantly lessened the annual rate of decline in forced vital capacity (FVC), compared with placebo.
Because idiopathic pulmonary fibrosis has a chronic trajectory, data on long-term safety and efficacy were clearly desirable. “Results from the open-label extension of the [foundational] phase 2 TOMORROW trial [also] identified no new safety signals and suggested an effect of nintedanib on slowing the progression of idiopathic pulmonary fibrosis beyond 52 weeks; however, only 35 patients treated with nintedanib 150 mg twice daily entered the extension study,” Dr. Crestani and his associates noted.
The open-label INPULSIS-ON extension trial included 734 patients, which was 91% of the population that completed the INPULSIS trials. A total of 59% patients in the open-label trial continued nintedanib while the rest switched to nintedanib from placebo. When considering both cohorts, the median duration of exposure to nintedanib was 44.7 months (range, 1.9-68.3 months).
Rates of major adverse cardiovascular events were 2.4 per 100 person-years of drug exposure among treatment initiators and 3.6 per 100 person-years among continuers, the researchers reported. Rates of bleeding were 6.7 and 8.4 events per 100 person-years, respectively, while rates of myocardial infarction, using the broadest possible definition, were 0.7 and 1.3 events per 100 person-years, respectively. The most common adverse event was diarrhea, with 60.1 and 71.2 events per 100 person-years among treatment initiators and continuers, respectively. In all, 10% of treatment initiators and 5% of continuers stopped nintedanib because of diarrhea. A total of 14% of treatment initiators and 12% of continuers stopped treatment because they experienced progression of idiopathic pulmonary fibrosis, making this adverse event the most common reason to stop treatment.
The adjusted annual rate of decline in FVC was −135.1 mL overall, –145 mL in nintedanib continuers, and –119.7 mL in nintedanib initiators, which resembled the findings of the INPULSIS trials, the researcher said. They added that the difference in FVC decline between INPULSIS-ON nintedanib initiators and continuers does not seem clinically meaningful, especially given that the average FVC decline in the INPULSIS placebo group was −223.5 mL per year, and the minimal clinically important difference in FVC is thought to be 2%-6% predicted, a difference of at least 75 mL-80 mL.
Boehringer Ingelheim funded the study. Dr. Crestani disclosed grants and personal fees from Boehringer Ingelheim and Roche, grants from Apellis and MedImmune, and personal fees from AstraZeneca and Sanofi.
SOURCE: Crestani B et al. Lancet Respir Med. 2018 Sep 14. doi: 10.1016/S2213-2600(18)30339-4.
FROM THE LANCET RESPIRATORY MEDICINE
Key clinical point: Nintedanib showed manageable safety and tolerability and might have helped conserve forced vital capacity during long-term use for the treatment of IPF.
Major finding: No new safety signals were found over up to 68 months of treatment.
Study details: Open-label extension study of nintedanib initiation or continuation in 734 patients with idiopathic pulmonary fibrosis (median drug exposure 44.7 months; range, 11.9-68.3 months).
Disclosures: Boehringer Ingelheim funded the study. Dr. Crestani disclosed grants and personal fees from Boehringer Ingelheim and Roche, grants from Apellis and MedImmune, and personal fees from AstraZeneca and Sanofi.
Source: Crestani B et al. Lancet Respir Med. 2018 Sep 14.
In pediatric asthma, jet nebulizers beat breath enhanced
In children with moderate to severe acute asthma, albuterol delivered by a conventional jet nebulizer led to more improvement in forced expiratory volume in 1 second (FEV1) than delivery via a breath-enhanced nebulizer.

Only one previous study has compared the two types of nebulizers in children with acute asthma. It showed that the new technology is noninferior to the older device, but it had a small sample size and did not examine spirometry data.
Mike Gardiner, MD, of the department of pediatrics, University of California, San Diego, and Matthew H. Wilkinson, MD, of the department of pediatrics, University of Texas at Austin, conducted a randomized, observer-blind study to look at effectiveness of these two nebulizers in a larger population of pediatric users. The results were published in the Journal of Pediatrics.
At a large, urban pediatric emergency department, researchers randomized 107 children (aged 6-18 years) presenting with a moderate to severe asthma exacerbation to receive one or the other nebulizer.
Children treated with the conventional jet nebulizer had a greater improvement in FEV1 (+13.8% vs. +9.1% of predicted; P = .04). The improvements were similar in a subgroup analysis of 57 subjects who met ATS/ERS (American Thoracic Society/ European Respiratory Society) spirometry guidelines (+14.5% vs. +8.5% of predicted; P = .03).
The researchers found no significant differences in changes in Pediatric Asthma Score, Pediatric Asthma Severity Score, ED length of stay, or admission rate. There was no significant difference in side effects between the two groups.
Breath-enhanced nebulizers use a holding chamber to store continuously nebulized medication, and one-way valves that direct exhaled air away from the holding chamber. The system reduces medication loss during exhalation and delivers a bolus of medication.
In lung models and healthy adult controls, breath-enhanced nebulizers achieved more effective lung deposition of aerosol. The authors speculate that the reduced clinical effect of the breath-enhanced nebulizer could be because the design of the mouthpiece, which allows a nonaerosolized “dead space” volume to be inhaled first. This volume may have a greater clinical impact in children than in adults.
Children experiencing asthma also have a rapid and shallow breathing pattern, which could also lead to a larger contribution of “dead space” to the overall dose, thus reducing drug exposure.
The study, Comparison of Breath-Enhanced and T-Piece Nebulizers in Children With Acute Asthma (NCT02566902) was funded by the University of Texas Southwestern, Austin. The authors declared no conflicts of interest.
SOURCE: Gardiner M, Wilkinson M. J Pediatr. 2019;204:245-9.
In children with moderate to severe acute asthma, albuterol delivered by a conventional jet nebulizer led to more improvement in forced expiratory volume in 1 second (FEV1) than delivery via a breath-enhanced nebulizer.
Only one previous study has compared the two types of nebulizers in children with acute asthma. It showed that the new technology is noninferior to the older device, but it had a small sample size and did not examine spirometry data.
Mike Gardiner, MD, of the department of pediatrics, University of California, San Diego, and Matthew H. Wilkinson, MD, of the department of pediatrics, University of Texas at Austin, conducted a randomized, observer-blind study to look at effectiveness of these two nebulizers in a larger population of pediatric users. The results were published in the Journal of Pediatrics.
At a large, urban pediatric emergency department, researchers randomized 107 children (aged 6-18 years) presenting with a moderate to severe asthma exacerbation to receive one or the other nebulizer.
Children treated with the conventional jet nebulizer had a greater improvement in FEV1 (+13.8% vs. +9.1% of predicted; P = .04). The improvements were similar in a subgroup analysis of 57 subjects who met ATS/ERS (American Thoracic Society/ European Respiratory Society) spirometry guidelines (+14.5% vs. +8.5% of predicted; P = .03).
The researchers found no significant differences in changes in Pediatric Asthma Score, Pediatric Asthma Severity Score, ED length of stay, or admission rate. There was no significant difference in side effects between the two groups.
Breath-enhanced nebulizers use a holding chamber to store continuously nebulized medication, and one-way valves that direct exhaled air away from the holding chamber. The system reduces medication loss during exhalation and delivers a bolus of medication.
In lung models and healthy adult controls, breath-enhanced nebulizers achieved more effective lung deposition of aerosol. The authors speculate that the reduced clinical effect of the breath-enhanced nebulizer could be because the design of the mouthpiece, which allows a nonaerosolized “dead space” volume to be inhaled first. This volume may have a greater clinical impact in children than in adults.
Children experiencing asthma also have a rapid and shallow breathing pattern, which could also lead to a larger contribution of “dead space” to the overall dose, thus reducing drug exposure.
The study, Comparison of Breath-Enhanced and T-Piece Nebulizers in Children With Acute Asthma (NCT02566902) was funded by the University of Texas Southwestern, Austin. The authors declared no conflicts of interest.
SOURCE: Gardiner M, Wilkinson M. J Pediatr. 2019;204:245-9.
In children with moderate to severe acute asthma, albuterol delivered by a conventional jet nebulizer led to more improvement in forced expiratory volume in 1 second (FEV1) than delivery via a breath-enhanced nebulizer.
Only one previous study has compared the two types of nebulizers in children with acute asthma. It showed that the new technology is noninferior to the older device, but it had a small sample size and did not examine spirometry data.
Mike Gardiner, MD, of the department of pediatrics, University of California, San Diego, and Matthew H. Wilkinson, MD, of the department of pediatrics, University of Texas at Austin, conducted a randomized, observer-blind study to look at effectiveness of these two nebulizers in a larger population of pediatric users. The results were published in the Journal of Pediatrics.
At a large, urban pediatric emergency department, researchers randomized 107 children (aged 6-18 years) presenting with a moderate to severe asthma exacerbation to receive one or the other nebulizer.
Children treated with the conventional jet nebulizer had a greater improvement in FEV1 (+13.8% vs. +9.1% of predicted; P = .04). The improvements were similar in a subgroup analysis of 57 subjects who met ATS/ERS (American Thoracic Society/ European Respiratory Society) spirometry guidelines (+14.5% vs. +8.5% of predicted; P = .03).
The researchers found no significant differences in changes in Pediatric Asthma Score, Pediatric Asthma Severity Score, ED length of stay, or admission rate. There was no significant difference in side effects between the two groups.
Breath-enhanced nebulizers use a holding chamber to store continuously nebulized medication, and one-way valves that direct exhaled air away from the holding chamber. The system reduces medication loss during exhalation and delivers a bolus of medication.
In lung models and healthy adult controls, breath-enhanced nebulizers achieved more effective lung deposition of aerosol. The authors speculate that the reduced clinical effect of the breath-enhanced nebulizer could be because the design of the mouthpiece, which allows a nonaerosolized “dead space” volume to be inhaled first. This volume may have a greater clinical impact in children than in adults.
Children experiencing asthma also have a rapid and shallow breathing pattern, which could also lead to a larger contribution of “dead space” to the overall dose, thus reducing drug exposure.
The study, Comparison of Breath-Enhanced and T-Piece Nebulizers in Children With Acute Asthma (NCT02566902) was funded by the University of Texas Southwestern, Austin. The authors declared no conflicts of interest.
SOURCE: Gardiner M, Wilkinson M. J Pediatr. 2019;204:245-9.
FROM THE JOURNAL OF PEDIATRICS
Key clinical point: New nebulizers worked better in adults, but pediatric populations may pose a challenge.
Major finding: FEV1 improved +13.8% in standard inhalers vs. +9.1% in breath-enhanced analyzers.
Study details: Randomized, controlled trial (n = 107).
Disclosures: The study was funded by the University of Texas Southwestern, Austin. The authors declared no conflicts of interest.
Source: Gardiner M, Wilkinson M. J Pediatr. 2019;204:245-9.
Flu season showing signs of decline
The 2018-2019 flu season may have peaked as measures of influenza-like illness (ILI) activity dropped in the first week of the new year, according to the U.S. Centers for Disease Control and Prevention.

The proportion of outpatients visits for ILI dropped to 3.5% for the week ending Jan. 5, 2019, after reaching 4.0% the previous week. Outpatient ILI visits first topped the national baseline of 2.2% during the week ending Dec. 8, 2018, and have remained above that value for 5 consecutive weeks, the CDC’s influenza division said on Jan. 11.
Flu activity reported by the states reflects the national drop: 10 states came in at level 10 on the CDC’s 1-10 scale of activity for the week ending Jan. 5 – down from 12 the week before – and a total of 15 were in the high range from 8 to 10, compared with 19 the previous week, the CDC said. Two states, Mississippi and Texas, dropped from level 10 to level 7, which the CDC categorizes as moderate activity.
A total of 73 ILI-related deaths were reported during the week ending Dec. 29 (the latest with data available; reporting less than 68% complete), which already exceeds the 71 deaths reported for the week ending Dec. 22 (reporting 85% complete). Flu deaths totaled 437 through the first 13 weeks of the 2018-2019 season, compared with the 1,659 that occurred during weeks 1-13 of the very severe 2017-2018 season, CDC data show.
For the week ending Jan. 5, the CDC received reports of three flu-related pediatric deaths, all of which occurred the previous week. For the season so far, there have been 16 pediatric deaths, compared with 20 at this point in the 2017-2018 season.
Estimates released during the flu season for the first time show that between 6 and 7 million Americans have been infected since Oct. 1, 2018, and that 69,000-84,000 people have been hospitalized with the flu through Jan. 5, 2019. These cumulative totals have previously been available only at the end of the season, the CDC noted.
The 2018-2019 flu season may have peaked as measures of influenza-like illness (ILI) activity dropped in the first week of the new year, according to the U.S. Centers for Disease Control and Prevention.
The proportion of outpatients visits for ILI dropped to 3.5% for the week ending Jan. 5, 2019, after reaching 4.0% the previous week. Outpatient ILI visits first topped the national baseline of 2.2% during the week ending Dec. 8, 2018, and have remained above that value for 5 consecutive weeks, the CDC’s influenza division said on Jan. 11.
Flu activity reported by the states reflects the national drop: 10 states came in at level 10 on the CDC’s 1-10 scale of activity for the week ending Jan. 5 – down from 12 the week before – and a total of 15 were in the high range from 8 to 10, compared with 19 the previous week, the CDC said. Two states, Mississippi and Texas, dropped from level 10 to level 7, which the CDC categorizes as moderate activity.
A total of 73 ILI-related deaths were reported during the week ending Dec. 29 (the latest with data available; reporting less than 68% complete), which already exceeds the 71 deaths reported for the week ending Dec. 22 (reporting 85% complete). Flu deaths totaled 437 through the first 13 weeks of the 2018-2019 season, compared with the 1,659 that occurred during weeks 1-13 of the very severe 2017-2018 season, CDC data show.
For the week ending Jan. 5, the CDC received reports of three flu-related pediatric deaths, all of which occurred the previous week. For the season so far, there have been 16 pediatric deaths, compared with 20 at this point in the 2017-2018 season.
Estimates released during the flu season for the first time show that between 6 and 7 million Americans have been infected since Oct. 1, 2018, and that 69,000-84,000 people have been hospitalized with the flu through Jan. 5, 2019. These cumulative totals have previously been available only at the end of the season, the CDC noted.
The 2018-2019 flu season may have peaked as measures of influenza-like illness (ILI) activity dropped in the first week of the new year, according to the U.S. Centers for Disease Control and Prevention.
The proportion of outpatients visits for ILI dropped to 3.5% for the week ending Jan. 5, 2019, after reaching 4.0% the previous week. Outpatient ILI visits first topped the national baseline of 2.2% during the week ending Dec. 8, 2018, and have remained above that value for 5 consecutive weeks, the CDC’s influenza division said on Jan. 11.
Flu activity reported by the states reflects the national drop: 10 states came in at level 10 on the CDC’s 1-10 scale of activity for the week ending Jan. 5 – down from 12 the week before – and a total of 15 were in the high range from 8 to 10, compared with 19 the previous week, the CDC said. Two states, Mississippi and Texas, dropped from level 10 to level 7, which the CDC categorizes as moderate activity.
A total of 73 ILI-related deaths were reported during the week ending Dec. 29 (the latest with data available; reporting less than 68% complete), which already exceeds the 71 deaths reported for the week ending Dec. 22 (reporting 85% complete). Flu deaths totaled 437 through the first 13 weeks of the 2018-2019 season, compared with the 1,659 that occurred during weeks 1-13 of the very severe 2017-2018 season, CDC data show.
For the week ending Jan. 5, the CDC received reports of three flu-related pediatric deaths, all of which occurred the previous week. For the season so far, there have been 16 pediatric deaths, compared with 20 at this point in the 2017-2018 season.
Estimates released during the flu season for the first time show that between 6 and 7 million Americans have been infected since Oct. 1, 2018, and that 69,000-84,000 people have been hospitalized with the flu through Jan. 5, 2019. These cumulative totals have previously been available only at the end of the season, the CDC noted.