User login
Seasonal affective disorder: How to help patients beat the winter blues
All of us see patients whose recurrent depressions seem to have a seasonal component. Should we treat them differently than patients whose recurrent depressions are not related to seasons? Is there adequate evidence for the existence of seasonal affective disorder (SAD), or—as it is called in DSM-IV-TR—mood disorder with a seasonal pattern? Is bright light therapy supported by the literature, or is it just some sort of fad?
As December brings the shortest days of the year, we shine the spotlight on SAD and examine the latest evidence on its causes, diagnosis, and treatment.
Moods with a seasonal rhythm
Moods have been observed to change with the seasons since ancient times (Box 1).1 As recently as 25 years ago, however, seasonal affective disorder was not recognized as a psychiatric diagnosis.
In the early 1980s, when researchers at the National Institute of Mental Health (NIMH) were studying the effect of bright light on melatonin secretion, they were contacted by Herbert E. Kern, a research engineer who suffered from recurrent depression. A methodical person, Kern had kept a journal of his mood variations and noticed a pattern that appeared to follow the seasons. His depression worsened in the fall and winter and improved in the spring and summer. Kern subsequently participated in an NIMH trial with phototherapy, his mood improved, and the results were published in 1982.2
Hippocrates, with his knack for keen observation, observed the variation of moods with the seasons. Aretaeus went a step further in the 2nd century by proposing that “lethargics are to be laid in the light and exposed to the rays of the sun.”
More recently, the physicist Angstrom—for whom the unit of light wavelength is named—was one of the first to mention the Swedish word “Lappsjuka,” which means “Lapp sickness” (Lapp refers to Scandinavian aborigines). He wrote, “Many people are sensitive to the lack of light, while others are less so. The former will in arctic winters suffer from Lappsjuka.”1
Two years later, the researchers published the first paper that described SAD as a psychiatric diagnosis.3 Criteria for the diagnosis included:
- presence of a major affective disorder
- affective episodes occurring during fall or winter and remitting in spring or summer for at least 2 consecutive years.
The paper also discussed treatment of winter depression with phototherapy.
DSM-IV-TR describes SAD as a course specifier for mood disorders, including major depressive episodes in bipolar I and II disorders and major depressive disorder (Box 2). In other words, as used in DSM-IV-TR and this article, SAD is not an independent disorder but a type of major affective disorder.
Characteristics of SAD
Symptoms. Patients with SAD suffer the typical symptoms of depression—decreased energy, guilt, and decreased libido—as well as atypical symptoms—carbohydrate craving, hypersomnia, and weight gain. They also appear less likely to exhibit psychotic symptoms and may be at lower risk for suicide than persons with major mood disorders but without SAD.1
Changes in sleep patterns also have been observed. Rosenthal et al4 found increased sleep latency and increased total sleep time in patients with SAD. Delta or slow-wave sleep—the restorative part of the sleep cycle—decreased by nearly one-half (mean 46%). REM latency did not change, contrary to typical findings in depressed patients. Anderson et al5 also reported no change in REM latency in patients with SAD.
Comorbid conditions. Eating disorders—particularly bulimia nervosa—are more prevalent in patients with SAD.1 Binge eating tends to worsen in the fall and winter.
Personality disorders are also common in these patients, with cluster C over-represented. Avoidant personality disorder is most common. In a sample of 45 patients with SAD, Reichborn-Kjennerud et al6 found any personality disorder in 58% and avoidant personality disorder in 31%. Patients with comorbid personality disorders were less likely to respond to bright light therapy.
Prevalence. The prevalence of SAD in North America is approximately 1 to 6 %, with four times as many women affected as men.1 Data on the effect of latitude on prevalence of SAD are inconclusive.7
Making the diagnosis
For patients with depression, clinicians should ask about seasonality of symptoms. Onset of major depressive symptoms in the fall or winter for at least two consecutive years or remission of depressive symptoms in the spring for two consecutive years (without onset of depressive syndromes during the spring or summer) probably merits a diagnosis of SAD. The diagnosis is confirmed if seasonal patterns of depressive symptoms substantially outnumber nonseasonal occurrences over the patient’s lifetime. The diagnosis may not be appropriate if there are obvious seasonal psychosocial stressors, such as anniversary reactions in posttraumatic stress disorder.
Some patients have sub-syndromal depressive symptoms that occur seasonally. DSM-IV would probably classify them as “mood disorder, not otherwise specified,” and that group has not been studied extensively.
Specify if:
With seasonal pattern (can be applied to the pattern of major depressive episodes in bipolar I disorder, bipolar II disorder, or major depressive disorder, recurrent)
- There has been a regular temporal relationship between the onset of major depressive episodes in bipolar I or bipolar II disorder or major depressive disorder, recurrent, and a particular time of the year (e.g., regular appearance of the major depressive episode in the fall or winter). Note: Do not include cases in which seasonal-related psychosocial stressors (e.g., regularly being unemployed every winter) create an obvious effect.
- Full remissions (or a change from depression to mania or hypomania) also occur at a characteristic time of the year (e.g., depression disappears in the spring).
- In the past 2 years, two major depressive episodes have occurred that demonstrate the temporal seasonal relationships defined in criteria A and B, and no nonseasonal major depressive episodes have occurred during that same period.
- Seasonal major depressive episodes (as described above) substantially outnumber the nonseasonal major depressive episodes that may have occurred over the individual’s lifetime.
Source: DSM-IV-TR
What causes SAD?
Research is ongoing, but the cause of SAD is not yet fully understood, although hypotheses have been developed. The four main hypotheses relate to duration of sunlight, changes in the circadian cycle, and secretion of the “hormone of darkness,” melatonin.
Photoperiod hypothesis. The shortening of the photoperiod—duration of sunlight—during autumn and winter may explain winter depression. Some research suggests that patients with SAD have an exaggerated melatonin response to shorter days and longer nights. For example, Wehr et al8 found that SAD patients secrete melatonin approximately 30 minutes longer per day in the winter, compared with controls.
Phase-delay hypothesis. Core body temperature is considered one of the most reliable markers of circadian rhythm. The nadir core body temperature occurs earlier than normal in a person whose circadian rhythm is “phase-advanced” and later than usual in those with “phase-delayed” circadian rhythms. Patients with seasonal affective symptoms generally reach their lowest body temperature of the day earlier than do controls.
Lewy et al,9 who proposed the phase-delay hypothesis, observed that melatonin secretion appeared to be delayed in patients with SAD. Some studies have supported this hypothesis, demonstrating greater benefit of bright light treatment when administered early in the morning than later in the day. Other studies, however, have shown benefit from light exposure late in the day.10
Reduced-amplitude hypothesis. SAD sufferers have dampened circadian rhythms, and bright light may increase the amplitude of the rhythms. There is little evidence for this hypothesis.
Melatonin hypothesis. Melatonin does not appear to cause depression. Looking at melatonin secretion patterns in conjunction with circadian phases, however, may offer new insights.8 Several studies have shown that manipulating the timing of melatonin secretion affects mood.
Cryptochrome, a photoreceptor in the retina, may be responsible for transmitting the photosignal to the elements of the circadian clock that regulate melatonin secretion. The pineal gland modifies its secretion of melatonin in response to the amount of light exposure (Box 3).8,11
Light therapy
Bright light therapy has been supported by placebo-controlled trials and is first-line treatment for patients with SAD.1 Bright light therapy is usually dosed at 2,500 lux for 2 hr/day or 10,000 lux for 30 min/day at eye level.12 The best evidence supports administering light therapy in the morning, generally between 6 and 10 AM. As described by Terman,13 “larks”—people who go to bed early and get up early—need earlier light than “owls”—people who stay up later and sleep later.
When light strikes the eye, it is well known that vitamin A-based photo pigments, cones, and rods receive the signal and transmit it via the optic tracts to the occipital cortex. But if light plays a role in the pathophysiology of seasonal affective disorder, how does light signal the other elements of the circadian system?

Cryptochrome, a photoreceptor in the retina, may be responsible for transmitting the photosignal to the circadian clock.11 Cryptochrome is a vitamin B2-based pigment found in the ganglion cells and on cells in the inner nuclear layer of the retina. It is thought to transmit light through the optic nerve to the suprachiasmatic nucleus, the circadian pacemaker in the hypothalamus. The signal is then transmitted through the paraventricular nucleus, down the sympathetic chain, through the superior cervical ganglion, up the nervi canarii, to its final destination—the pineal gland.8 The pineal gland then modifies its secretion of melatonin in response to the amount of light exposure.
Although mammals have an intrinsic rhythmicity, the circadian clock must be entrained by exogenous light. The retinohypothalamic tract is believed to be the vehicle that sets the circadian clock. If the optic nerve is cut, a person becomes blind and unable to entrain the circadian rhythm.
Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously wellcontrolled depressive symptoms worsen in the fall or winter. Light therapy also can be used as prophylaxis—starting in early fall—in patients with a history of a seasonal pattern of depression. Either way, light treatments generally should continue until early spring.
Given the relatively few side effects, light therapy may be used as monotherapy in patients with mild, subsyndromal mood symptoms occurring on a seasonal basis. Light therapy should not be used without pharmacotherapy to treat a full-blown major depressive episode.
Light boxes can be found via the Internet at an average cost of $180 to $300 for a 10,000-lux unit. The boxes are small enough to be placed on a table while the patient reads or eats breakfast. Artificial lights for this therapy do not emit ultraviolet rays, which have been associated with skin cancers.
Light visors also have shown some promise in SAD treatment, as demonstrated by a 2-week, randomized, controlled trial by Joffe et al.14 Compared with light boxes, light visors are more portable, so the patient can move around during treatment. Generally, the patient wears the visor 30 minutes in the morning.
Light visors appear to be as effective as table models, although no studies have compared the two devices. A visor costs $250 to $300.
Dawn simulation in SAD treatment has been examined in a few small studies and one placebo-controlled trial with 95 patients.10 In dawn simulation, a white light gradually increases between 4:30 and 6 AM to a peak intensity of 250 lux. Dawn simulation can be done while the patient is sleeping, whereas other light treatments require the patient to wake up early enough each morning to sit before a light box for 30 minutes. More study is needed to assess this modality’s efficacy.
Light therapy precautions. Review the patient’s medications before starting light therapy. Drugs that can magnify the effects of short wave-length light—leading to severe sunburns or rashes—include tetracycline, sulfonamides, and some older antipsychotics such as chlorpromazine. Some authors recommend an ophthalmologic examination before starting light therapy and every 2 to 3 years afterwards if no complications are apparent.1 Others believe that no ophthalmologic examination is necessary unless the patient is older than 70 or has a history of retinal disease.
Side effects of bright light therapy are usually few and mild and include headaches, eye irritation, and nausea. In some anecdotal cases, patients with bipolar disorder appear to have switched from depression to mania upon starting light therapy,1 but such switches appear to be rare. Still, patients with bipolar disorder and their family members should be advised to watch out for switches when using light therapy.
Pharmacologic therapy
Drug therapy in SAD has not been well studied, and many of the placebo-controlled trials that have examined this mode of treatment have been small. Serotonergic agents have been most studied because serotonin, with its effects on sleep and appetite, is thought to be related to SAD pathogenesis. The largest study of a selective serotonin reuptake inhibitor for SAD15 compared sertraline with placebo. Patients who received sertraline at a mean dosage of 111 mg/d had significantly fewer depressive symptoms than did the placebo group.
A placebo-controlled, double-blind study by Thorell16 found that adding citalopram to light therapy improved measures of depressed mood, compared with light therapy alone. This study is limited by small sample size but provides direction for further research.
An open trial of reboxetine—a noradrenaline reuptake inhibitor not available in the United States—suggests that further research of agents affecting catecholamines may be worthwhile in SAD treatment.17
Psychotherapy
Psychotherapy has not been researched sufficiently to be considered a proven treatment for SAD. However, some have observed that SAD patients have a negative cognitive style that may benefit from cognitive therapy. Thus, behavioral therapy may alter a patient’s response to light.1
Related resources
- National Organization for Seasonal Affective Disorder www.nosad.org
- Dr. Ivan’s (Ivan Goldberg, MD) Depression Central www.psycom.net/depression.central.seasonal.html
- Columbia/Presbyterian Hospital Program in Clinical Chronobiology www.light-and-iontherapy.org
Drug brand names
- Citalopram • Celexa
- Sertraline • Zoloft
Disclosure
Dr. Paradies reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Hillard reports that he is a consultant to Pfizer Inc. and Janssen Pharmaceutica, and serves on the speakers bureau of Pfizer Inc., Janssen Pharmaceutica, and Eli Lilly and Co.
1. Partonen T, Magnusson A. Seasonal affective disorder New York: Oxford University Press, 2001;3-134.
2. Lewy AJ, Kern HA, Rosenthal NE, Wehr TA. Bright artificial light treatment of a manic-depressive patient with a seasonal mood cycle. Am J Psychiatry 1982;139(11):1496-8.
3. Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder: A description of the syndrome and preliminary findings with light therapy. Arch Gen Psychiatry 1984;41(1):72-80.
4. Rosenthal NE, Jacobsen FM, Sack DA, et al. Atenolol in seasonal affective disorder: a test of the melatonin hypothesis. Am J Psychiatry 1988;145:52-6.
5. Anderson JL, Rosen LN, Mendelson WB, et al. Sleep in fall/winter seasonal affective disorder: effects of light and changing seasons. J Psychosom Res 1994;38:323-37.
6. Reichborn-Kjennerud T, Lingjaerde O, Dahl AA. Personality disorders in patients with winter depression. Acta Psychiatrica Scand 1994;90:413-19.
7. Mersch PPA, Middendorp HM, Bouhuys AL, Beersma DGM, van den Hoofdakker RH. Seasonal affective disorder and latitude: a review of the literature. J Affect Disord 1999;53:35-48.
8. Wehr TA, Duncan WC, Sher L, et al. A circadian signal of change in patients with seasonal affective disorder. Arch Gen Psychiatry 2001;58:1108-14.
9. Lewy AJ, Sack RL, Singer CM, White DM, Hoban TM. Winter depression and the phase-shift hypothesis for bright light’s therapeutic effects: history, theory, and experimental evidence. J Biolog Rhythms 1988;3:121-34.
10. Avery DH, Kizer D, Bolte MA, Hellekson C. Bright light therapy of subsyndromal seasonal affective disorder in the workplace: morning vs. afternoon exposure. Acta Psychiatrica Scand 2000;103:267-74.
11. Sancar A. Cryptochrome: the second photoactive pigment in the eye and its role in circadian photoreception. Ann Rev Biochemistry 2000;69:31-67.
12. Meesters Y, Jansen JHC, Beersma DGM, Bouhuys AL, van den Hoofdakker RH. Light therapy for seasonal affective disorder: the effects of timing. Br J Psychiatry 1995;166:607-12.
13. Terman M. Internal night. Arch Gen Psychiatry 2001;58:1115-6.
14. Joffe RT, Moul DE, Lam RW, et al. Light visor treatment for seasonal affective disorder: a multicenter study. Psychiatry Res 1993;46(1):29-39.
15. Blashko CA, Moscovitch A, Eagles JM, Darcourt G, Thompson C, Kasper S. A placebo-controlled study of sertraline in the treatment of outpatients with seasonal affective disorder (unpublished data on file with Pfizer Inc.)
16. Thorell LH, Kjellman B, Arned M, Lindwall-Sundel K, Walinder J, Wetterberg L. Light treatment of seasonal affective disorder in combination with citalopram or placebo with 1-year follow-up. Int Clin Psychopharmacol 1999;14(suppl 2):S7-S11.
17. Hilger E. Reboxetine in seasonal affective disorder: an open trial. Eur Neuropsychopharmacology 2001;11(1):1-5.
All of us see patients whose recurrent depressions seem to have a seasonal component. Should we treat them differently than patients whose recurrent depressions are not related to seasons? Is there adequate evidence for the existence of seasonal affective disorder (SAD), or—as it is called in DSM-IV-TR—mood disorder with a seasonal pattern? Is bright light therapy supported by the literature, or is it just some sort of fad?
As December brings the shortest days of the year, we shine the spotlight on SAD and examine the latest evidence on its causes, diagnosis, and treatment.
Moods with a seasonal rhythm
Moods have been observed to change with the seasons since ancient times (Box 1).1 As recently as 25 years ago, however, seasonal affective disorder was not recognized as a psychiatric diagnosis.
In the early 1980s, when researchers at the National Institute of Mental Health (NIMH) were studying the effect of bright light on melatonin secretion, they were contacted by Herbert E. Kern, a research engineer who suffered from recurrent depression. A methodical person, Kern had kept a journal of his mood variations and noticed a pattern that appeared to follow the seasons. His depression worsened in the fall and winter and improved in the spring and summer. Kern subsequently participated in an NIMH trial with phototherapy, his mood improved, and the results were published in 1982.2
Hippocrates, with his knack for keen observation, observed the variation of moods with the seasons. Aretaeus went a step further in the 2nd century by proposing that “lethargics are to be laid in the light and exposed to the rays of the sun.”
More recently, the physicist Angstrom—for whom the unit of light wavelength is named—was one of the first to mention the Swedish word “Lappsjuka,” which means “Lapp sickness” (Lapp refers to Scandinavian aborigines). He wrote, “Many people are sensitive to the lack of light, while others are less so. The former will in arctic winters suffer from Lappsjuka.”1
Two years later, the researchers published the first paper that described SAD as a psychiatric diagnosis.3 Criteria for the diagnosis included:
- presence of a major affective disorder
- affective episodes occurring during fall or winter and remitting in spring or summer for at least 2 consecutive years.
The paper also discussed treatment of winter depression with phototherapy.
DSM-IV-TR describes SAD as a course specifier for mood disorders, including major depressive episodes in bipolar I and II disorders and major depressive disorder (Box 2). In other words, as used in DSM-IV-TR and this article, SAD is not an independent disorder but a type of major affective disorder.
Characteristics of SAD
Symptoms. Patients with SAD suffer the typical symptoms of depression—decreased energy, guilt, and decreased libido—as well as atypical symptoms—carbohydrate craving, hypersomnia, and weight gain. They also appear less likely to exhibit psychotic symptoms and may be at lower risk for suicide than persons with major mood disorders but without SAD.1
Changes in sleep patterns also have been observed. Rosenthal et al4 found increased sleep latency and increased total sleep time in patients with SAD. Delta or slow-wave sleep—the restorative part of the sleep cycle—decreased by nearly one-half (mean 46%). REM latency did not change, contrary to typical findings in depressed patients. Anderson et al5 also reported no change in REM latency in patients with SAD.
Comorbid conditions. Eating disorders—particularly bulimia nervosa—are more prevalent in patients with SAD.1 Binge eating tends to worsen in the fall and winter.
Personality disorders are also common in these patients, with cluster C over-represented. Avoidant personality disorder is most common. In a sample of 45 patients with SAD, Reichborn-Kjennerud et al6 found any personality disorder in 58% and avoidant personality disorder in 31%. Patients with comorbid personality disorders were less likely to respond to bright light therapy.
Prevalence. The prevalence of SAD in North America is approximately 1 to 6 %, with four times as many women affected as men.1 Data on the effect of latitude on prevalence of SAD are inconclusive.7
Making the diagnosis
For patients with depression, clinicians should ask about seasonality of symptoms. Onset of major depressive symptoms in the fall or winter for at least two consecutive years or remission of depressive symptoms in the spring for two consecutive years (without onset of depressive syndromes during the spring or summer) probably merits a diagnosis of SAD. The diagnosis is confirmed if seasonal patterns of depressive symptoms substantially outnumber nonseasonal occurrences over the patient’s lifetime. The diagnosis may not be appropriate if there are obvious seasonal psychosocial stressors, such as anniversary reactions in posttraumatic stress disorder.
Some patients have sub-syndromal depressive symptoms that occur seasonally. DSM-IV would probably classify them as “mood disorder, not otherwise specified,” and that group has not been studied extensively.
Specify if:
With seasonal pattern (can be applied to the pattern of major depressive episodes in bipolar I disorder, bipolar II disorder, or major depressive disorder, recurrent)
- There has been a regular temporal relationship between the onset of major depressive episodes in bipolar I or bipolar II disorder or major depressive disorder, recurrent, and a particular time of the year (e.g., regular appearance of the major depressive episode in the fall or winter). Note: Do not include cases in which seasonal-related psychosocial stressors (e.g., regularly being unemployed every winter) create an obvious effect.
- Full remissions (or a change from depression to mania or hypomania) also occur at a characteristic time of the year (e.g., depression disappears in the spring).
- In the past 2 years, two major depressive episodes have occurred that demonstrate the temporal seasonal relationships defined in criteria A and B, and no nonseasonal major depressive episodes have occurred during that same period.
- Seasonal major depressive episodes (as described above) substantially outnumber the nonseasonal major depressive episodes that may have occurred over the individual’s lifetime.
Source: DSM-IV-TR
What causes SAD?
Research is ongoing, but the cause of SAD is not yet fully understood, although hypotheses have been developed. The four main hypotheses relate to duration of sunlight, changes in the circadian cycle, and secretion of the “hormone of darkness,” melatonin.
Photoperiod hypothesis. The shortening of the photoperiod—duration of sunlight—during autumn and winter may explain winter depression. Some research suggests that patients with SAD have an exaggerated melatonin response to shorter days and longer nights. For example, Wehr et al8 found that SAD patients secrete melatonin approximately 30 minutes longer per day in the winter, compared with controls.
Phase-delay hypothesis. Core body temperature is considered one of the most reliable markers of circadian rhythm. The nadir core body temperature occurs earlier than normal in a person whose circadian rhythm is “phase-advanced” and later than usual in those with “phase-delayed” circadian rhythms. Patients with seasonal affective symptoms generally reach their lowest body temperature of the day earlier than do controls.
Lewy et al,9 who proposed the phase-delay hypothesis, observed that melatonin secretion appeared to be delayed in patients with SAD. Some studies have supported this hypothesis, demonstrating greater benefit of bright light treatment when administered early in the morning than later in the day. Other studies, however, have shown benefit from light exposure late in the day.10
Reduced-amplitude hypothesis. SAD sufferers have dampened circadian rhythms, and bright light may increase the amplitude of the rhythms. There is little evidence for this hypothesis.
Melatonin hypothesis. Melatonin does not appear to cause depression. Looking at melatonin secretion patterns in conjunction with circadian phases, however, may offer new insights.8 Several studies have shown that manipulating the timing of melatonin secretion affects mood.
Cryptochrome, a photoreceptor in the retina, may be responsible for transmitting the photosignal to the elements of the circadian clock that regulate melatonin secretion. The pineal gland modifies its secretion of melatonin in response to the amount of light exposure (Box 3).8,11
Light therapy
Bright light therapy has been supported by placebo-controlled trials and is first-line treatment for patients with SAD.1 Bright light therapy is usually dosed at 2,500 lux for 2 hr/day or 10,000 lux for 30 min/day at eye level.12 The best evidence supports administering light therapy in the morning, generally between 6 and 10 AM. As described by Terman,13 “larks”—people who go to bed early and get up early—need earlier light than “owls”—people who stay up later and sleep later.
When light strikes the eye, it is well known that vitamin A-based photo pigments, cones, and rods receive the signal and transmit it via the optic tracts to the occipital cortex. But if light plays a role in the pathophysiology of seasonal affective disorder, how does light signal the other elements of the circadian system?
Cryptochrome, a photoreceptor in the retina, may be responsible for transmitting the photosignal to the circadian clock.11 Cryptochrome is a vitamin B2-based pigment found in the ganglion cells and on cells in the inner nuclear layer of the retina. It is thought to transmit light through the optic nerve to the suprachiasmatic nucleus, the circadian pacemaker in the hypothalamus. The signal is then transmitted through the paraventricular nucleus, down the sympathetic chain, through the superior cervical ganglion, up the nervi canarii, to its final destination—the pineal gland.8 The pineal gland then modifies its secretion of melatonin in response to the amount of light exposure.
Although mammals have an intrinsic rhythmicity, the circadian clock must be entrained by exogenous light. The retinohypothalamic tract is believed to be the vehicle that sets the circadian clock. If the optic nerve is cut, a person becomes blind and unable to entrain the circadian rhythm.
Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously wellcontrolled depressive symptoms worsen in the fall or winter. Light therapy also can be used as prophylaxis—starting in early fall—in patients with a history of a seasonal pattern of depression. Either way, light treatments generally should continue until early spring.
Given the relatively few side effects, light therapy may be used as monotherapy in patients with mild, subsyndromal mood symptoms occurring on a seasonal basis. Light therapy should not be used without pharmacotherapy to treat a full-blown major depressive episode.
Light boxes can be found via the Internet at an average cost of $180 to $300 for a 10,000-lux unit. The boxes are small enough to be placed on a table while the patient reads or eats breakfast. Artificial lights for this therapy do not emit ultraviolet rays, which have been associated with skin cancers.
Light visors also have shown some promise in SAD treatment, as demonstrated by a 2-week, randomized, controlled trial by Joffe et al.14 Compared with light boxes, light visors are more portable, so the patient can move around during treatment. Generally, the patient wears the visor 30 minutes in the morning.
Light visors appear to be as effective as table models, although no studies have compared the two devices. A visor costs $250 to $300.
Dawn simulation in SAD treatment has been examined in a few small studies and one placebo-controlled trial with 95 patients.10 In dawn simulation, a white light gradually increases between 4:30 and 6 AM to a peak intensity of 250 lux. Dawn simulation can be done while the patient is sleeping, whereas other light treatments require the patient to wake up early enough each morning to sit before a light box for 30 minutes. More study is needed to assess this modality’s efficacy.
Light therapy precautions. Review the patient’s medications before starting light therapy. Drugs that can magnify the effects of short wave-length light—leading to severe sunburns or rashes—include tetracycline, sulfonamides, and some older antipsychotics such as chlorpromazine. Some authors recommend an ophthalmologic examination before starting light therapy and every 2 to 3 years afterwards if no complications are apparent.1 Others believe that no ophthalmologic examination is necessary unless the patient is older than 70 or has a history of retinal disease.
Side effects of bright light therapy are usually few and mild and include headaches, eye irritation, and nausea. In some anecdotal cases, patients with bipolar disorder appear to have switched from depression to mania upon starting light therapy,1 but such switches appear to be rare. Still, patients with bipolar disorder and their family members should be advised to watch out for switches when using light therapy.
Pharmacologic therapy
Drug therapy in SAD has not been well studied, and many of the placebo-controlled trials that have examined this mode of treatment have been small. Serotonergic agents have been most studied because serotonin, with its effects on sleep and appetite, is thought to be related to SAD pathogenesis. The largest study of a selective serotonin reuptake inhibitor for SAD15 compared sertraline with placebo. Patients who received sertraline at a mean dosage of 111 mg/d had significantly fewer depressive symptoms than did the placebo group.
A placebo-controlled, double-blind study by Thorell16 found that adding citalopram to light therapy improved measures of depressed mood, compared with light therapy alone. This study is limited by small sample size but provides direction for further research.
An open trial of reboxetine—a noradrenaline reuptake inhibitor not available in the United States—suggests that further research of agents affecting catecholamines may be worthwhile in SAD treatment.17
Psychotherapy
Psychotherapy has not been researched sufficiently to be considered a proven treatment for SAD. However, some have observed that SAD patients have a negative cognitive style that may benefit from cognitive therapy. Thus, behavioral therapy may alter a patient’s response to light.1
Related resources
- National Organization for Seasonal Affective Disorder www.nosad.org
- Dr. Ivan’s (Ivan Goldberg, MD) Depression Central www.psycom.net/depression.central.seasonal.html
- Columbia/Presbyterian Hospital Program in Clinical Chronobiology www.light-and-iontherapy.org
Drug brand names
- Citalopram • Celexa
- Sertraline • Zoloft
Disclosure
Dr. Paradies reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Hillard reports that he is a consultant to Pfizer Inc. and Janssen Pharmaceutica, and serves on the speakers bureau of Pfizer Inc., Janssen Pharmaceutica, and Eli Lilly and Co.
All of us see patients whose recurrent depressions seem to have a seasonal component. Should we treat them differently than patients whose recurrent depressions are not related to seasons? Is there adequate evidence for the existence of seasonal affective disorder (SAD), or—as it is called in DSM-IV-TR—mood disorder with a seasonal pattern? Is bright light therapy supported by the literature, or is it just some sort of fad?
As December brings the shortest days of the year, we shine the spotlight on SAD and examine the latest evidence on its causes, diagnosis, and treatment.
Moods with a seasonal rhythm
Moods have been observed to change with the seasons since ancient times (Box 1).1 As recently as 25 years ago, however, seasonal affective disorder was not recognized as a psychiatric diagnosis.
In the early 1980s, when researchers at the National Institute of Mental Health (NIMH) were studying the effect of bright light on melatonin secretion, they were contacted by Herbert E. Kern, a research engineer who suffered from recurrent depression. A methodical person, Kern had kept a journal of his mood variations and noticed a pattern that appeared to follow the seasons. His depression worsened in the fall and winter and improved in the spring and summer. Kern subsequently participated in an NIMH trial with phototherapy, his mood improved, and the results were published in 1982.2
Hippocrates, with his knack for keen observation, observed the variation of moods with the seasons. Aretaeus went a step further in the 2nd century by proposing that “lethargics are to be laid in the light and exposed to the rays of the sun.”
More recently, the physicist Angstrom—for whom the unit of light wavelength is named—was one of the first to mention the Swedish word “Lappsjuka,” which means “Lapp sickness” (Lapp refers to Scandinavian aborigines). He wrote, “Many people are sensitive to the lack of light, while others are less so. The former will in arctic winters suffer from Lappsjuka.”1
Two years later, the researchers published the first paper that described SAD as a psychiatric diagnosis.3 Criteria for the diagnosis included:
- presence of a major affective disorder
- affective episodes occurring during fall or winter and remitting in spring or summer for at least 2 consecutive years.
The paper also discussed treatment of winter depression with phototherapy.
DSM-IV-TR describes SAD as a course specifier for mood disorders, including major depressive episodes in bipolar I and II disorders and major depressive disorder (Box 2). In other words, as used in DSM-IV-TR and this article, SAD is not an independent disorder but a type of major affective disorder.
Characteristics of SAD
Symptoms. Patients with SAD suffer the typical symptoms of depression—decreased energy, guilt, and decreased libido—as well as atypical symptoms—carbohydrate craving, hypersomnia, and weight gain. They also appear less likely to exhibit psychotic symptoms and may be at lower risk for suicide than persons with major mood disorders but without SAD.1
Changes in sleep patterns also have been observed. Rosenthal et al4 found increased sleep latency and increased total sleep time in patients with SAD. Delta or slow-wave sleep—the restorative part of the sleep cycle—decreased by nearly one-half (mean 46%). REM latency did not change, contrary to typical findings in depressed patients. Anderson et al5 also reported no change in REM latency in patients with SAD.
Comorbid conditions. Eating disorders—particularly bulimia nervosa—are more prevalent in patients with SAD.1 Binge eating tends to worsen in the fall and winter.
Personality disorders are also common in these patients, with cluster C over-represented. Avoidant personality disorder is most common. In a sample of 45 patients with SAD, Reichborn-Kjennerud et al6 found any personality disorder in 58% and avoidant personality disorder in 31%. Patients with comorbid personality disorders were less likely to respond to bright light therapy.
Prevalence. The prevalence of SAD in North America is approximately 1 to 6 %, with four times as many women affected as men.1 Data on the effect of latitude on prevalence of SAD are inconclusive.7
Making the diagnosis
For patients with depression, clinicians should ask about seasonality of symptoms. Onset of major depressive symptoms in the fall or winter for at least two consecutive years or remission of depressive symptoms in the spring for two consecutive years (without onset of depressive syndromes during the spring or summer) probably merits a diagnosis of SAD. The diagnosis is confirmed if seasonal patterns of depressive symptoms substantially outnumber nonseasonal occurrences over the patient’s lifetime. The diagnosis may not be appropriate if there are obvious seasonal psychosocial stressors, such as anniversary reactions in posttraumatic stress disorder.
Some patients have sub-syndromal depressive symptoms that occur seasonally. DSM-IV would probably classify them as “mood disorder, not otherwise specified,” and that group has not been studied extensively.
Specify if:
With seasonal pattern (can be applied to the pattern of major depressive episodes in bipolar I disorder, bipolar II disorder, or major depressive disorder, recurrent)
- There has been a regular temporal relationship between the onset of major depressive episodes in bipolar I or bipolar II disorder or major depressive disorder, recurrent, and a particular time of the year (e.g., regular appearance of the major depressive episode in the fall or winter). Note: Do not include cases in which seasonal-related psychosocial stressors (e.g., regularly being unemployed every winter) create an obvious effect.
- Full remissions (or a change from depression to mania or hypomania) also occur at a characteristic time of the year (e.g., depression disappears in the spring).
- In the past 2 years, two major depressive episodes have occurred that demonstrate the temporal seasonal relationships defined in criteria A and B, and no nonseasonal major depressive episodes have occurred during that same period.
- Seasonal major depressive episodes (as described above) substantially outnumber the nonseasonal major depressive episodes that may have occurred over the individual’s lifetime.
Source: DSM-IV-TR
What causes SAD?
Research is ongoing, but the cause of SAD is not yet fully understood, although hypotheses have been developed. The four main hypotheses relate to duration of sunlight, changes in the circadian cycle, and secretion of the “hormone of darkness,” melatonin.
Photoperiod hypothesis. The shortening of the photoperiod—duration of sunlight—during autumn and winter may explain winter depression. Some research suggests that patients with SAD have an exaggerated melatonin response to shorter days and longer nights. For example, Wehr et al8 found that SAD patients secrete melatonin approximately 30 minutes longer per day in the winter, compared with controls.
Phase-delay hypothesis. Core body temperature is considered one of the most reliable markers of circadian rhythm. The nadir core body temperature occurs earlier than normal in a person whose circadian rhythm is “phase-advanced” and later than usual in those with “phase-delayed” circadian rhythms. Patients with seasonal affective symptoms generally reach their lowest body temperature of the day earlier than do controls.
Lewy et al,9 who proposed the phase-delay hypothesis, observed that melatonin secretion appeared to be delayed in patients with SAD. Some studies have supported this hypothesis, demonstrating greater benefit of bright light treatment when administered early in the morning than later in the day. Other studies, however, have shown benefit from light exposure late in the day.10
Reduced-amplitude hypothesis. SAD sufferers have dampened circadian rhythms, and bright light may increase the amplitude of the rhythms. There is little evidence for this hypothesis.
Melatonin hypothesis. Melatonin does not appear to cause depression. Looking at melatonin secretion patterns in conjunction with circadian phases, however, may offer new insights.8 Several studies have shown that manipulating the timing of melatonin secretion affects mood.
Cryptochrome, a photoreceptor in the retina, may be responsible for transmitting the photosignal to the elements of the circadian clock that regulate melatonin secretion. The pineal gland modifies its secretion of melatonin in response to the amount of light exposure (Box 3).8,11
Light therapy
Bright light therapy has been supported by placebo-controlled trials and is first-line treatment for patients with SAD.1 Bright light therapy is usually dosed at 2,500 lux for 2 hr/day or 10,000 lux for 30 min/day at eye level.12 The best evidence supports administering light therapy in the morning, generally between 6 and 10 AM. As described by Terman,13 “larks”—people who go to bed early and get up early—need earlier light than “owls”—people who stay up later and sleep later.
When light strikes the eye, it is well known that vitamin A-based photo pigments, cones, and rods receive the signal and transmit it via the optic tracts to the occipital cortex. But if light plays a role in the pathophysiology of seasonal affective disorder, how does light signal the other elements of the circadian system?
Cryptochrome, a photoreceptor in the retina, may be responsible for transmitting the photosignal to the circadian clock.11 Cryptochrome is a vitamin B2-based pigment found in the ganglion cells and on cells in the inner nuclear layer of the retina. It is thought to transmit light through the optic nerve to the suprachiasmatic nucleus, the circadian pacemaker in the hypothalamus. The signal is then transmitted through the paraventricular nucleus, down the sympathetic chain, through the superior cervical ganglion, up the nervi canarii, to its final destination—the pineal gland.8 The pineal gland then modifies its secretion of melatonin in response to the amount of light exposure.
Although mammals have an intrinsic rhythmicity, the circadian clock must be entrained by exogenous light. The retinohypothalamic tract is believed to be the vehicle that sets the circadian clock. If the optic nerve is cut, a person becomes blind and unable to entrain the circadian rhythm.
Light therapy can be used alone or in addition to pharmacotherapy in patients whose previously wellcontrolled depressive symptoms worsen in the fall or winter. Light therapy also can be used as prophylaxis—starting in early fall—in patients with a history of a seasonal pattern of depression. Either way, light treatments generally should continue until early spring.
Given the relatively few side effects, light therapy may be used as monotherapy in patients with mild, subsyndromal mood symptoms occurring on a seasonal basis. Light therapy should not be used without pharmacotherapy to treat a full-blown major depressive episode.
Light boxes can be found via the Internet at an average cost of $180 to $300 for a 10,000-lux unit. The boxes are small enough to be placed on a table while the patient reads or eats breakfast. Artificial lights for this therapy do not emit ultraviolet rays, which have been associated with skin cancers.
Light visors also have shown some promise in SAD treatment, as demonstrated by a 2-week, randomized, controlled trial by Joffe et al.14 Compared with light boxes, light visors are more portable, so the patient can move around during treatment. Generally, the patient wears the visor 30 minutes in the morning.
Light visors appear to be as effective as table models, although no studies have compared the two devices. A visor costs $250 to $300.
Dawn simulation in SAD treatment has been examined in a few small studies and one placebo-controlled trial with 95 patients.10 In dawn simulation, a white light gradually increases between 4:30 and 6 AM to a peak intensity of 250 lux. Dawn simulation can be done while the patient is sleeping, whereas other light treatments require the patient to wake up early enough each morning to sit before a light box for 30 minutes. More study is needed to assess this modality’s efficacy.
Light therapy precautions. Review the patient’s medications before starting light therapy. Drugs that can magnify the effects of short wave-length light—leading to severe sunburns or rashes—include tetracycline, sulfonamides, and some older antipsychotics such as chlorpromazine. Some authors recommend an ophthalmologic examination before starting light therapy and every 2 to 3 years afterwards if no complications are apparent.1 Others believe that no ophthalmologic examination is necessary unless the patient is older than 70 or has a history of retinal disease.
Side effects of bright light therapy are usually few and mild and include headaches, eye irritation, and nausea. In some anecdotal cases, patients with bipolar disorder appear to have switched from depression to mania upon starting light therapy,1 but such switches appear to be rare. Still, patients with bipolar disorder and their family members should be advised to watch out for switches when using light therapy.
Pharmacologic therapy
Drug therapy in SAD has not been well studied, and many of the placebo-controlled trials that have examined this mode of treatment have been small. Serotonergic agents have been most studied because serotonin, with its effects on sleep and appetite, is thought to be related to SAD pathogenesis. The largest study of a selective serotonin reuptake inhibitor for SAD15 compared sertraline with placebo. Patients who received sertraline at a mean dosage of 111 mg/d had significantly fewer depressive symptoms than did the placebo group.
A placebo-controlled, double-blind study by Thorell16 found that adding citalopram to light therapy improved measures of depressed mood, compared with light therapy alone. This study is limited by small sample size but provides direction for further research.
An open trial of reboxetine—a noradrenaline reuptake inhibitor not available in the United States—suggests that further research of agents affecting catecholamines may be worthwhile in SAD treatment.17
Psychotherapy
Psychotherapy has not been researched sufficiently to be considered a proven treatment for SAD. However, some have observed that SAD patients have a negative cognitive style that may benefit from cognitive therapy. Thus, behavioral therapy may alter a patient’s response to light.1
Related resources
- National Organization for Seasonal Affective Disorder www.nosad.org
- Dr. Ivan’s (Ivan Goldberg, MD) Depression Central www.psycom.net/depression.central.seasonal.html
- Columbia/Presbyterian Hospital Program in Clinical Chronobiology www.light-and-iontherapy.org
Drug brand names
- Citalopram • Celexa
- Sertraline • Zoloft
Disclosure
Dr. Paradies reports no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
Dr. Hillard reports that he is a consultant to Pfizer Inc. and Janssen Pharmaceutica, and serves on the speakers bureau of Pfizer Inc., Janssen Pharmaceutica, and Eli Lilly and Co.
1. Partonen T, Magnusson A. Seasonal affective disorder New York: Oxford University Press, 2001;3-134.
2. Lewy AJ, Kern HA, Rosenthal NE, Wehr TA. Bright artificial light treatment of a manic-depressive patient with a seasonal mood cycle. Am J Psychiatry 1982;139(11):1496-8.
3. Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder: A description of the syndrome and preliminary findings with light therapy. Arch Gen Psychiatry 1984;41(1):72-80.
4. Rosenthal NE, Jacobsen FM, Sack DA, et al. Atenolol in seasonal affective disorder: a test of the melatonin hypothesis. Am J Psychiatry 1988;145:52-6.
5. Anderson JL, Rosen LN, Mendelson WB, et al. Sleep in fall/winter seasonal affective disorder: effects of light and changing seasons. J Psychosom Res 1994;38:323-37.
6. Reichborn-Kjennerud T, Lingjaerde O, Dahl AA. Personality disorders in patients with winter depression. Acta Psychiatrica Scand 1994;90:413-19.
7. Mersch PPA, Middendorp HM, Bouhuys AL, Beersma DGM, van den Hoofdakker RH. Seasonal affective disorder and latitude: a review of the literature. J Affect Disord 1999;53:35-48.
8. Wehr TA, Duncan WC, Sher L, et al. A circadian signal of change in patients with seasonal affective disorder. Arch Gen Psychiatry 2001;58:1108-14.
9. Lewy AJ, Sack RL, Singer CM, White DM, Hoban TM. Winter depression and the phase-shift hypothesis for bright light’s therapeutic effects: history, theory, and experimental evidence. J Biolog Rhythms 1988;3:121-34.
10. Avery DH, Kizer D, Bolte MA, Hellekson C. Bright light therapy of subsyndromal seasonal affective disorder in the workplace: morning vs. afternoon exposure. Acta Psychiatrica Scand 2000;103:267-74.
11. Sancar A. Cryptochrome: the second photoactive pigment in the eye and its role in circadian photoreception. Ann Rev Biochemistry 2000;69:31-67.
12. Meesters Y, Jansen JHC, Beersma DGM, Bouhuys AL, van den Hoofdakker RH. Light therapy for seasonal affective disorder: the effects of timing. Br J Psychiatry 1995;166:607-12.
13. Terman M. Internal night. Arch Gen Psychiatry 2001;58:1115-6.
14. Joffe RT, Moul DE, Lam RW, et al. Light visor treatment for seasonal affective disorder: a multicenter study. Psychiatry Res 1993;46(1):29-39.
15. Blashko CA, Moscovitch A, Eagles JM, Darcourt G, Thompson C, Kasper S. A placebo-controlled study of sertraline in the treatment of outpatients with seasonal affective disorder (unpublished data on file with Pfizer Inc.)
16. Thorell LH, Kjellman B, Arned M, Lindwall-Sundel K, Walinder J, Wetterberg L. Light treatment of seasonal affective disorder in combination with citalopram or placebo with 1-year follow-up. Int Clin Psychopharmacol 1999;14(suppl 2):S7-S11.
17. Hilger E. Reboxetine in seasonal affective disorder: an open trial. Eur Neuropsychopharmacology 2001;11(1):1-5.
1. Partonen T, Magnusson A. Seasonal affective disorder New York: Oxford University Press, 2001;3-134.
2. Lewy AJ, Kern HA, Rosenthal NE, Wehr TA. Bright artificial light treatment of a manic-depressive patient with a seasonal mood cycle. Am J Psychiatry 1982;139(11):1496-8.
3. Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder: A description of the syndrome and preliminary findings with light therapy. Arch Gen Psychiatry 1984;41(1):72-80.
4. Rosenthal NE, Jacobsen FM, Sack DA, et al. Atenolol in seasonal affective disorder: a test of the melatonin hypothesis. Am J Psychiatry 1988;145:52-6.
5. Anderson JL, Rosen LN, Mendelson WB, et al. Sleep in fall/winter seasonal affective disorder: effects of light and changing seasons. J Psychosom Res 1994;38:323-37.
6. Reichborn-Kjennerud T, Lingjaerde O, Dahl AA. Personality disorders in patients with winter depression. Acta Psychiatrica Scand 1994;90:413-19.
7. Mersch PPA, Middendorp HM, Bouhuys AL, Beersma DGM, van den Hoofdakker RH. Seasonal affective disorder and latitude: a review of the literature. J Affect Disord 1999;53:35-48.
8. Wehr TA, Duncan WC, Sher L, et al. A circadian signal of change in patients with seasonal affective disorder. Arch Gen Psychiatry 2001;58:1108-14.
9. Lewy AJ, Sack RL, Singer CM, White DM, Hoban TM. Winter depression and the phase-shift hypothesis for bright light’s therapeutic effects: history, theory, and experimental evidence. J Biolog Rhythms 1988;3:121-34.
10. Avery DH, Kizer D, Bolte MA, Hellekson C. Bright light therapy of subsyndromal seasonal affective disorder in the workplace: morning vs. afternoon exposure. Acta Psychiatrica Scand 2000;103:267-74.
11. Sancar A. Cryptochrome: the second photoactive pigment in the eye and its role in circadian photoreception. Ann Rev Biochemistry 2000;69:31-67.
12. Meesters Y, Jansen JHC, Beersma DGM, Bouhuys AL, van den Hoofdakker RH. Light therapy for seasonal affective disorder: the effects of timing. Br J Psychiatry 1995;166:607-12.
13. Terman M. Internal night. Arch Gen Psychiatry 2001;58:1115-6.
14. Joffe RT, Moul DE, Lam RW, et al. Light visor treatment for seasonal affective disorder: a multicenter study. Psychiatry Res 1993;46(1):29-39.
15. Blashko CA, Moscovitch A, Eagles JM, Darcourt G, Thompson C, Kasper S. A placebo-controlled study of sertraline in the treatment of outpatients with seasonal affective disorder (unpublished data on file with Pfizer Inc.)
16. Thorell LH, Kjellman B, Arned M, Lindwall-Sundel K, Walinder J, Wetterberg L. Light treatment of seasonal affective disorder in combination with citalopram or placebo with 1-year follow-up. Int Clin Psychopharmacol 1999;14(suppl 2):S7-S11.
17. Hilger E. Reboxetine in seasonal affective disorder: an open trial. Eur Neuropsychopharmacology 2001;11(1):1-5.
Late-onset schizophrenia: Make the right diagnosis when psychosis emerges after age 60
Mr. B, age 73, repeatedly complained to his landlord that people were trying to poison him by pumping noxious gas into his apartment. He barricaded himself inside, taped up all air vents and windows, and left only when absolutely necessary. At night, he could hear people working the “apparatus” that pumped the gas, and could “smell” the vapors.
On examination, he was physically well but suffered from mild neural deafness and myopia. He was suspicious and guarded but oriented and not cognitively impaired. He expressed paranoid beliefs and experienced auditory and olfactory hallucinations. There was no evidence of affective disturbance.
At first he refused psychiatric care but eventually agreed to take risperidone, 0.5 mg at night. He tolerated the agent well, and his psychotic symptoms slowly resolved.
As Mr. B’s case illustrates, schizophrenia—once thought to be strictly an early-onset disorder—commonly manifests late in life (Box). Too often, however, very late-onset schizophrenia goes undiagnosed because older patients with the disorder tend to be socially isolated. Their symptoms of paranoia and reluctance by family members to intervene also can prevent them from receiving treatment that could control psychotic symptoms and improve their quality of life.
Most clinical samples of patients with schizophrenia cite few cases of onset after age 60, reflecting the confused and changing nosology of very late-onset schizophrenia.
DSM-III (1980) stated that the schizophrenia label could apply only if onset occurred before age 45. This stipulation was dropped in DSM-III-R (1987), but it undoubtedly led psychiatrists to believe that schizophrenia simply did not begin in late life. The International Late-Onset Schizophrenia Group1 today recognizes the disorder’s late-onset version as “verylate-onset schizophrenia-like psychosis.”
General population studies report rates of “late paraphrenia” of around 1%, but these studies probably underestimate the true prevalence. One presumes that persons with paranoia are less likely than those without to participate in such a study.
The Camberwell Register First Episode Study,2 performed in London, is one of the few to determine rates of nonaffective psychosis across all ages of onset. In this study, 12% of the 513 patients studied across 20 years had illness onset after age 60. Researchers suspect a similar incidence in the U.S. population.
Psychosis presenting at any age, but especially in later life, requires careful evaluation to exclude organic pathology. Very late-onset schizophrenia differs substantially from psychosis associated with dementia, as in Alzheimer’s disease, both in terms of neuropsychological and brain imaging findings.
Although limited, data on late-life psychosis offer clues to its diagnosis and treatment. This article will address:
- risk factors and clinical presentations associated with late-onset schizophrenia
- pharmacologic and psychosocial treatment options based on available evidence.
Clinical presentation
Clinical presentation of schizophrenia with onset after age 60 differs from that of early-onset schizophrenia (Table 1). To those familiar with early-onset cases, the most obvious differences in late-onset patients are negligible rates of primary negative symptoms and formal thought disorder.
Persecutory delusions are common in both types and often are elaborate. The so-called “partition” delusion, which leads the patient to believe that people or objects can transgress impermeable barriers and access his or her home with malign intent, is more common in late-onset than in early-onset schizophrenia.3
Hallucinations in very late-onset schizophrenia are often prominent and can occur in multiple modalities, including auditory, visual, and olfactory. Sometimes the hallucination and delusion are clearly linked; for example, a patient claims to smell the noxious gas he believes is being pumped into his home.
Does the difference in presentation between early- and very late-onset schizophrenia reflect distinct disease processes or the disorder’s impact at different stages of brain maturation and degeneration? To answer that question, researchers have compared late-onset patients with young early-onset patents and with older patients who developed schizophrenia in their youth. Similar phenomena have been found in both early-onset groups,4 suggesting that age of onset causes the differences in clinical presentation.
Risk factors
As with early-onset schizophrenia, family history is the most common cause of very late-onset schizophrenia. Despite their limitations, family history studies almost all show a familial risk of very late-onset schizophrenia lower than that of early-onset patients but greater than that of the general population.5 Published studies do not tell us whether age of onset is genetically determined, in part because not all patients at risk for very late-onset schizophrenia live long enough to manifest its symptoms.
Family history has been associated with affective disorder in some patients with very late-onset schizophrenia. One casecontrolled series of family interviews6 found an approximate 1.3% rate of schizophrenia in relatives —about the same rate as that of the control group. The rate of depression among relatives of patients with very late-onset schizophrenia was 16.3%, compared with only 4.4% for controls (p = 0.003). Thus, late-onset psychosis and affective disorders may have etiologic links.7
Other possible risk factors for very late-onset schizophrenia include sensory deficits, premorbid personality disorder, social isolation, neuropsychological abnormalities, and female gender.
Sensory deficits. Several studies have reported that hearing and vision loss is more prevalent in older patients with very late-onset schizophrenia than in similarly aged controls. Most of these studies have associated either auditory or sensory impairment with very late-onset schizophrenia,8 but most did not include appropriate controls.
One case-control study (of younger patients)8 found that only uncorrected sensory deficits were over-represented in late-onset cases. This finding implies that one should find out if the patient is willing or able to get medical help for the sensory deficit, as well as whether that treatment has been adequate, before calling the sensory deficit a sequela of late-onset schizophrenia.
Premorbid personality disorder. Patients with very late-onset schizophrenia are widely reported to have gone through life reclusive and paranoid.5 Of interest is that unlike many of their early-onset counterparts, late-onset patients tend to have achieved fairly well in the workplace. Whether this success reflects a later onset of illness cannot be determined.
Social isolation is common among older persons and even more so among those with very late-onset schizophrenia.9 Whether this finding reflects patients’ premorbid personalities, the illness itself, or a risk factor for the disorder is open to conjecture.
Neuropsychological abnormalities. Assessments of patients with very late-onset schizophrenia reveal cognitive impairment patterns similar to those reported in patients with an earlier onset10 but distinct from those reported in patients with psychosis associated with dementia. CTand MRIstudies reveal focal (reduced left temporal lobe volume) and nonspecific (increased ventricular-to-brain ratios) structural abnormalities similar to those in younger patients.11
Table 1
CLINICAL FEATURES OF SCHIZOPHRENIA: EARLY- VS. VERY LATE-ONSET TYPES
| Clinical feature | Early onset | Very late onset |
|---|---|---|
| Persecutory delusions | Common (often elaborate) | Common (often elaborate) |
| Partition delusions | Rare | Common |
| Negative symptoms | Common | Rare |
| Formal thought disorder | Common | Rare |
| Hallucinations | Common, especially auditory | Often prominent (can manifest in multiple modalities) |
| Gender differences | Equally common in men, women | More common in women |
| Family history of schizophrenia | Common | Less common |
| Uncorrected auditory, visual impairments | No consistent relationship | Common; excessive in some patients |
| Premorbid personality | Maybe schizoid/schizotypal | Reclusive, suspicious |
| Social abilities | Social isolation | Social isolation |
| Marital status | Usually unmarried | Usually unmarried |
| Cognitive deficits, structural brain abnormalities | Similar for both groups | Similar for both groups |
Researchers previously reported excessive white-matter abnormalities in late-onset patients compared with healthy controls—a consistent finding in patients with late-life depression. More recent studies that carefully excluded organic cerebral disorders have not replicated this finding, however.11
Female gender. Very late-onset schizophrenia is more common in women than in men.12 Female-to-male ratios ranging from 2.2:1 to 22.5:1 have been calculated. Although women generally live longer than men, this predominance is still greater than one would expect. It might also hide important clues regarding schizophrenia and related disorders across the life span, including the fact that the brains of men and women show sex-specific patterns of aging.12
Managing very late-onset schizophrenia
Initial assessment. Patients who present with a new-onset psychotic disorder at any age require careful evaluation to exclude an underlying organic cause. The following are strongly suggested in older patients with new-onset psychoses:
- comprehensive history (including medications)
- physical (including neurologic) examination
- laboratory investigations
- CTneuroimaging
- and cognitive screening, such as the Mini Mental State Examination.
Drug treatment. Despite the wealth of published data on the psychopharmacologic management of schizophrenia, few randomized, controlled trials have examined the use of drugs to treat the disorder’s very late-onset form. Case reports or small open studies comprise the available literature. Significant flaws in treatment studies have included diagnostic heterogeneity, mixing of early- and late-onset patients, inadequate outcome criteria, and lack of control groups.13
As with early-onset schizophrenia, however, antipsychotics appear to improve the acute symptoms of very late-onset schizophrenia and reduce the risk of relapse.14 Pearlson et al4 reported at least partial remission in 76% of patients with late-onset schizophrenia after neuroleptic regimens (complete remission occurred in 48%). The presence of thought disorder or a premorbid schizoid personality predicted poor response to treatment, whereas gender, family history, and first-rank symptoms (auditory hallucinations, delusions, social withdrawal) did not significantly affect outcome.
Very late-onset patients respond to about one-half the antipsychotic dosage required for younger patients.13 Sweet and Pollock15 found an average dosage of chlorpromazine equivalents, 148 mg/d, to be effective in older patients, compared with >300 mg/d in younger cohorts.
Neuroleptic side effects. Older patients are more susceptible than their younger counterparts to side effects and adverse reactions from typical neuroleptics, even at low dosages. Age-related differences in pharmacokinetics and pharmacodynamics, combined with the increased incidence of comorbid physical disease and polypharmacy among older patients, often complicate pharmacotherapy for late-onset schizophrenia.
Older patients taking antipsychotics face an increased risk of extrapyramidal symptoms (EPS), especially parkinsonism and akathisia.16 Anticholinergics are poorly tolerated and may cause urinary retention, constipation, blurred vision, exacerbation of glaucoma, and delirium. Cardiovascular side effects, especially orthostatic hypotension, may lead to falls and significant injury and may exacerbate coexisting cardiovascular disease.
Neuroleptic-induced tardive dyskinesia (TD) is another potential complication. Jeste et al found the cumulative annual incidence of drug-induced TD to be five times greater among older psychotic patients than among younger ones (26% vs. 5% after 1 year).17 Duration of exposure and total cumulative amount of prescribed neuroleptics remain significant risk factors for TD in older patients.
Atypical antipsychotics, with their less-adverse side-effect profiles and lower risk of EPS (and probably TD as well) are the preferred first-line drugs for late-onset schizophrenia. These agents also have been associated with improved cognition in younger patients with schizophrenia, a potentially significant benefit in the older patient.
Table 2
ANTIPSYCHOTIC DOSAGES RECOMMENDED FOR VERY LATE-ONSET SCHIZOPHRENIA
| Drugs | Initial dosages | Maintenance dosages |
|---|---|---|
| Olanzapine | 1 to 5 mg/d | 2.5 to 15 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 0.5 to 3 mg/d |
| Quetiapine | 12.5 to 25 mg/d | 75 to 150 mg/d |
No well-controlled trials of clozapine in very late-onset schizophrenia have been performed. According to one literature review,18 most older psychotic patients showed moderate to marked improvement at relatively low dosages (mean dosage 134 mg/d). The reviewers concluded that clozapine was safe and well tolerated but suggested that agranulocytosis may occur at higher rates in this group than in younger patients. Clozapine’s potent anticholinergic action and its marked sedative effects limit its use in very late-onset schizophrenia to treatmentresistant patients or those with severe TD.
Data on the use of other atypical agents in very late-onset schizophrenia are limited. Risperidone has been associated with significant improvements in older patients with schizophrenia.16 Risperidone, olanzapine, and quetiapine have all been found to be safe, well-tolerated, and effective in managing late-life psychotic disorders.16,19,20 As with neuroleptics, recommended starting and maintenance dosages of the atypicals are lower than those used in younger patients (Table 2).13
A “start low, go slow” approach is warranted, and dosages should be adjusted according to clinical response. Communicate with the patient’s primary care physician to learn of any potential drug-drug interactions with medications being given for comorbid illnesses.
Electroconvulsive therapy has been reported to be useful in several studies, but data on its use in very late-onset schizophrenia are limited.21
Psychosocial interventions. One review of the role of non-biological treatment in very late-onset schizophrenia22 stressed the need to develop trust between patient and psychiatrist, so that the patient clearly views the treatment team as allies (Table 3). To that end, look for thoughts, feelings, or situations that may have precipitated the onset of psychosis, and explore their subjective meaning with the patient. Address any clear losses that are identified, such as the recent death of a spouse or other family member.
Table 3
DOs AND DON’Ts OF MANAGING AN OLDER PATIENT WITH SCHIZOPHRENIA
| Do | Don’t |
|---|---|
|
|
Find out if the patient is isolated and to what degree he or she feels lonely. Encourage the patient to engage in activities that he or she once enjoyed, and subtly introduce the patient to an appropriate community support group. Suggesting participation in group leisure activities may also help. Ascertain the patient’s living arrangements and basic needs. You may need to refer the patient to a social agency for assistance with housing, finances, nutrition/diet, and transportation.
Reminiscence therapy, through which patients are encouraged to reflect on their lives, can be useful for patients with very late-onset schizophrenia. Through reflection, patients can review past successes and painful experiences and move toward ultimate resolution of conflict and current difficulties.22
As in younger patients with schizophrenia, cognitivebehavioral therapy can help to modify delusional beliefs, gain control over hallucinations, and identify high-risk situations and appropriate coping strategies.23
Include family members in the treatment plan, and offer them support, education, and practical assistance (e.g., strategies for dealing with delusions). Informed families can help patients comply with prescriptions and appointments and can also detect relapse in its early stages.
In some cases, the patient’s longstanding paranoia and paranoid personality can lead to resentment and conflict within the family. Before treatment can begin, you may also need to address this conflict by educating family members on how a loved one’s schizophrenia affects them. Counseling the family as a group may be appropriate in some cases.
Related resources
- Howard R, Rabins PV, Castle DJ, eds. Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical; 1999.
- Howard R, Rabins PV, Seeman MV, et al. Late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: an international consensus. Am J Psychiatry 2000; 157:172-8.
Drug brand names
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no affiliation or financial arrangement with any of the companies whose products are mentioned in this article, or with manufacturers of competing products.
Acknowledgements
Dr. Lubman wishes to thank the Nauma Licht Fellowship, a bequest supporting schizophrenia research, for its support.
1. Howard R, Rabins PV, Seeman MV, et al. Consensus statement of the International Late Onset Schizophrenia Group. In: Howard R, Rabins PV, Castle DJ, (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;263-6.
2. Castle DJ, Wessely S, Van Os J, et al. Psychosis in the inner city: The Camberwell First Episode Study. Maudsley Monograph 40. Hove, UK: Psychology Press, 1998.
3. Howard R, Castle DJ, O’Brien J, et al. Permeable walls, floors, ceilings and doors: partition delusions in late paraphrenia. Int J Geriatr Psychiatry 1992;7:719-24.
4. Pearlson GD, Kreger L, Rabins PV, et al. A chart review study of late-onset and early-onset schizophrenia. Am J Psychiatry 1989;146:1568-74.
5. Castle DJ, Howard R. What do we know about the aetiology of late onset schizophrenia? Eur Psychiatry 1992;7:99-108.
6. Howard R, Graham C, Sham P, et al. A controlled family study of late-onset non-affective psychosis (late paraphrenia). Br J Psychiatry 1997;170:511-4.
7. Murray RM, O’Callaghan E, Castle DJ, et al. A neurodevelopmental approach to the classification of schizophrenia. Schizophr Bull 1992;18:319-32.
8. Prager S, Jeste DV. Sensory impairment in late life schizophrenia. Schizophr Bull 1993;19:755-71.
9. Kay DWK. The English language literature on late paraphrenia from the 1950s. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;17-43.
10. Jeste DV, Harris MJ, Krull A, et al. Clinical and neuropsychological characteristics of patients with late-onset schizophrenia. Am J Psychiatry 1995;152:722-30.
11. Pearlson GD. Brain imaging in late onset schizophrenia. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;191-204.
12. Castle DJ. Gender and age at onset in schizophrenia. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;147-64.
13. Salzman C, Tune L. Neuroleptic treatment of late-life schizophrenia. Harvard Rev Psychiatry 2001;9:77-83.
14. Harris MJ, Jeste DV. Late-onset schizophrenia: an overview. Schizophr Bull 1988;14:39-55.
15. Sweet RA, Pollock BG. Neuroleptics in the elderly: guidelines for monitoring. Harvard Rev Psychiatry 1995;2:327-35.
16. Sciolla A, Jeste DV. Use of antipsychotics in the elderly. Int J Psych Clin Pract 1998;2(suppl 1):S27-S34.
17. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients: a prospective longitudinal study of 266 patients. Arch Gen Psychiatry 1995;52:756-65.
18. Barak Y, Wittenberg N, Naor S, et al. Clozapine in elderly psychiatric patients: tolerability, safety and efficacy. Compr Psychiatry 1999;40:320-5.
19. Madhusoodanan S, Suresh P, et al. Experience with the atypical antipsychotics—risperidone and olanzapine in the elderly. Ann Clin Psychiatry 1999;11(3):113-8.
20. Arvanitis LA, Miller BG. Multiple fixed doses of “Seroquel” (quetiapine) in patients with acute exacerbation of schizophrenia: a comparison with haloperidol and placebo. Biol Psychiatry 1997;42(4):233-46.
21. Kay DWK, Roth M. Environmental and hereditary factors in the schizophrenias of old age (‘late paraphrenia’) and their bearing on the general problem of causation in schizophrenia. J Mental Sci 1961;107:649-86.
22. Aguera-Ortiz L, Reneses-Prieto B. The place of non-biological treatments. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;233:60.-
23. Fowler D, Garety P, Kuipers E. Cognitive behavioural therapy for psychosis: theory and practice. Chichester, UK: Wiley, 1995.
Mr. B, age 73, repeatedly complained to his landlord that people were trying to poison him by pumping noxious gas into his apartment. He barricaded himself inside, taped up all air vents and windows, and left only when absolutely necessary. At night, he could hear people working the “apparatus” that pumped the gas, and could “smell” the vapors.
On examination, he was physically well but suffered from mild neural deafness and myopia. He was suspicious and guarded but oriented and not cognitively impaired. He expressed paranoid beliefs and experienced auditory and olfactory hallucinations. There was no evidence of affective disturbance.
At first he refused psychiatric care but eventually agreed to take risperidone, 0.5 mg at night. He tolerated the agent well, and his psychotic symptoms slowly resolved.
As Mr. B’s case illustrates, schizophrenia—once thought to be strictly an early-onset disorder—commonly manifests late in life (Box). Too often, however, very late-onset schizophrenia goes undiagnosed because older patients with the disorder tend to be socially isolated. Their symptoms of paranoia and reluctance by family members to intervene also can prevent them from receiving treatment that could control psychotic symptoms and improve their quality of life.
Most clinical samples of patients with schizophrenia cite few cases of onset after age 60, reflecting the confused and changing nosology of very late-onset schizophrenia.
DSM-III (1980) stated that the schizophrenia label could apply only if onset occurred before age 45. This stipulation was dropped in DSM-III-R (1987), but it undoubtedly led psychiatrists to believe that schizophrenia simply did not begin in late life. The International Late-Onset Schizophrenia Group1 today recognizes the disorder’s late-onset version as “verylate-onset schizophrenia-like psychosis.”
General population studies report rates of “late paraphrenia” of around 1%, but these studies probably underestimate the true prevalence. One presumes that persons with paranoia are less likely than those without to participate in such a study.
The Camberwell Register First Episode Study,2 performed in London, is one of the few to determine rates of nonaffective psychosis across all ages of onset. In this study, 12% of the 513 patients studied across 20 years had illness onset after age 60. Researchers suspect a similar incidence in the U.S. population.
Psychosis presenting at any age, but especially in later life, requires careful evaluation to exclude organic pathology. Very late-onset schizophrenia differs substantially from psychosis associated with dementia, as in Alzheimer’s disease, both in terms of neuropsychological and brain imaging findings.
Although limited, data on late-life psychosis offer clues to its diagnosis and treatment. This article will address:
- risk factors and clinical presentations associated with late-onset schizophrenia
- pharmacologic and psychosocial treatment options based on available evidence.
Clinical presentation
Clinical presentation of schizophrenia with onset after age 60 differs from that of early-onset schizophrenia (Table 1). To those familiar with early-onset cases, the most obvious differences in late-onset patients are negligible rates of primary negative symptoms and formal thought disorder.
Persecutory delusions are common in both types and often are elaborate. The so-called “partition” delusion, which leads the patient to believe that people or objects can transgress impermeable barriers and access his or her home with malign intent, is more common in late-onset than in early-onset schizophrenia.3
Hallucinations in very late-onset schizophrenia are often prominent and can occur in multiple modalities, including auditory, visual, and olfactory. Sometimes the hallucination and delusion are clearly linked; for example, a patient claims to smell the noxious gas he believes is being pumped into his home.
Does the difference in presentation between early- and very late-onset schizophrenia reflect distinct disease processes or the disorder’s impact at different stages of brain maturation and degeneration? To answer that question, researchers have compared late-onset patients with young early-onset patents and with older patients who developed schizophrenia in their youth. Similar phenomena have been found in both early-onset groups,4 suggesting that age of onset causes the differences in clinical presentation.
Risk factors
As with early-onset schizophrenia, family history is the most common cause of very late-onset schizophrenia. Despite their limitations, family history studies almost all show a familial risk of very late-onset schizophrenia lower than that of early-onset patients but greater than that of the general population.5 Published studies do not tell us whether age of onset is genetically determined, in part because not all patients at risk for very late-onset schizophrenia live long enough to manifest its symptoms.
Family history has been associated with affective disorder in some patients with very late-onset schizophrenia. One casecontrolled series of family interviews6 found an approximate 1.3% rate of schizophrenia in relatives —about the same rate as that of the control group. The rate of depression among relatives of patients with very late-onset schizophrenia was 16.3%, compared with only 4.4% for controls (p = 0.003). Thus, late-onset psychosis and affective disorders may have etiologic links.7
Other possible risk factors for very late-onset schizophrenia include sensory deficits, premorbid personality disorder, social isolation, neuropsychological abnormalities, and female gender.
Sensory deficits. Several studies have reported that hearing and vision loss is more prevalent in older patients with very late-onset schizophrenia than in similarly aged controls. Most of these studies have associated either auditory or sensory impairment with very late-onset schizophrenia,8 but most did not include appropriate controls.
One case-control study (of younger patients)8 found that only uncorrected sensory deficits were over-represented in late-onset cases. This finding implies that one should find out if the patient is willing or able to get medical help for the sensory deficit, as well as whether that treatment has been adequate, before calling the sensory deficit a sequela of late-onset schizophrenia.
Premorbid personality disorder. Patients with very late-onset schizophrenia are widely reported to have gone through life reclusive and paranoid.5 Of interest is that unlike many of their early-onset counterparts, late-onset patients tend to have achieved fairly well in the workplace. Whether this success reflects a later onset of illness cannot be determined.
Social isolation is common among older persons and even more so among those with very late-onset schizophrenia.9 Whether this finding reflects patients’ premorbid personalities, the illness itself, or a risk factor for the disorder is open to conjecture.
Neuropsychological abnormalities. Assessments of patients with very late-onset schizophrenia reveal cognitive impairment patterns similar to those reported in patients with an earlier onset10 but distinct from those reported in patients with psychosis associated with dementia. CTand MRIstudies reveal focal (reduced left temporal lobe volume) and nonspecific (increased ventricular-to-brain ratios) structural abnormalities similar to those in younger patients.11
Table 1
CLINICAL FEATURES OF SCHIZOPHRENIA: EARLY- VS. VERY LATE-ONSET TYPES
| Clinical feature | Early onset | Very late onset |
|---|---|---|
| Persecutory delusions | Common (often elaborate) | Common (often elaborate) |
| Partition delusions | Rare | Common |
| Negative symptoms | Common | Rare |
| Formal thought disorder | Common | Rare |
| Hallucinations | Common, especially auditory | Often prominent (can manifest in multiple modalities) |
| Gender differences | Equally common in men, women | More common in women |
| Family history of schizophrenia | Common | Less common |
| Uncorrected auditory, visual impairments | No consistent relationship | Common; excessive in some patients |
| Premorbid personality | Maybe schizoid/schizotypal | Reclusive, suspicious |
| Social abilities | Social isolation | Social isolation |
| Marital status | Usually unmarried | Usually unmarried |
| Cognitive deficits, structural brain abnormalities | Similar for both groups | Similar for both groups |
Researchers previously reported excessive white-matter abnormalities in late-onset patients compared with healthy controls—a consistent finding in patients with late-life depression. More recent studies that carefully excluded organic cerebral disorders have not replicated this finding, however.11
Female gender. Very late-onset schizophrenia is more common in women than in men.12 Female-to-male ratios ranging from 2.2:1 to 22.5:1 have been calculated. Although women generally live longer than men, this predominance is still greater than one would expect. It might also hide important clues regarding schizophrenia and related disorders across the life span, including the fact that the brains of men and women show sex-specific patterns of aging.12
Managing very late-onset schizophrenia
Initial assessment. Patients who present with a new-onset psychotic disorder at any age require careful evaluation to exclude an underlying organic cause. The following are strongly suggested in older patients with new-onset psychoses:
- comprehensive history (including medications)
- physical (including neurologic) examination
- laboratory investigations
- CTneuroimaging
- and cognitive screening, such as the Mini Mental State Examination.
Drug treatment. Despite the wealth of published data on the psychopharmacologic management of schizophrenia, few randomized, controlled trials have examined the use of drugs to treat the disorder’s very late-onset form. Case reports or small open studies comprise the available literature. Significant flaws in treatment studies have included diagnostic heterogeneity, mixing of early- and late-onset patients, inadequate outcome criteria, and lack of control groups.13
As with early-onset schizophrenia, however, antipsychotics appear to improve the acute symptoms of very late-onset schizophrenia and reduce the risk of relapse.14 Pearlson et al4 reported at least partial remission in 76% of patients with late-onset schizophrenia after neuroleptic regimens (complete remission occurred in 48%). The presence of thought disorder or a premorbid schizoid personality predicted poor response to treatment, whereas gender, family history, and first-rank symptoms (auditory hallucinations, delusions, social withdrawal) did not significantly affect outcome.
Very late-onset patients respond to about one-half the antipsychotic dosage required for younger patients.13 Sweet and Pollock15 found an average dosage of chlorpromazine equivalents, 148 mg/d, to be effective in older patients, compared with >300 mg/d in younger cohorts.
Neuroleptic side effects. Older patients are more susceptible than their younger counterparts to side effects and adverse reactions from typical neuroleptics, even at low dosages. Age-related differences in pharmacokinetics and pharmacodynamics, combined with the increased incidence of comorbid physical disease and polypharmacy among older patients, often complicate pharmacotherapy for late-onset schizophrenia.
Older patients taking antipsychotics face an increased risk of extrapyramidal symptoms (EPS), especially parkinsonism and akathisia.16 Anticholinergics are poorly tolerated and may cause urinary retention, constipation, blurred vision, exacerbation of glaucoma, and delirium. Cardiovascular side effects, especially orthostatic hypotension, may lead to falls and significant injury and may exacerbate coexisting cardiovascular disease.
Neuroleptic-induced tardive dyskinesia (TD) is another potential complication. Jeste et al found the cumulative annual incidence of drug-induced TD to be five times greater among older psychotic patients than among younger ones (26% vs. 5% after 1 year).17 Duration of exposure and total cumulative amount of prescribed neuroleptics remain significant risk factors for TD in older patients.
Atypical antipsychotics, with their less-adverse side-effect profiles and lower risk of EPS (and probably TD as well) are the preferred first-line drugs for late-onset schizophrenia. These agents also have been associated with improved cognition in younger patients with schizophrenia, a potentially significant benefit in the older patient.
Table 2
ANTIPSYCHOTIC DOSAGES RECOMMENDED FOR VERY LATE-ONSET SCHIZOPHRENIA
| Drugs | Initial dosages | Maintenance dosages |
|---|---|---|
| Olanzapine | 1 to 5 mg/d | 2.5 to 15 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 0.5 to 3 mg/d |
| Quetiapine | 12.5 to 25 mg/d | 75 to 150 mg/d |
No well-controlled trials of clozapine in very late-onset schizophrenia have been performed. According to one literature review,18 most older psychotic patients showed moderate to marked improvement at relatively low dosages (mean dosage 134 mg/d). The reviewers concluded that clozapine was safe and well tolerated but suggested that agranulocytosis may occur at higher rates in this group than in younger patients. Clozapine’s potent anticholinergic action and its marked sedative effects limit its use in very late-onset schizophrenia to treatmentresistant patients or those with severe TD.
Data on the use of other atypical agents in very late-onset schizophrenia are limited. Risperidone has been associated with significant improvements in older patients with schizophrenia.16 Risperidone, olanzapine, and quetiapine have all been found to be safe, well-tolerated, and effective in managing late-life psychotic disorders.16,19,20 As with neuroleptics, recommended starting and maintenance dosages of the atypicals are lower than those used in younger patients (Table 2).13
A “start low, go slow” approach is warranted, and dosages should be adjusted according to clinical response. Communicate with the patient’s primary care physician to learn of any potential drug-drug interactions with medications being given for comorbid illnesses.
Electroconvulsive therapy has been reported to be useful in several studies, but data on its use in very late-onset schizophrenia are limited.21
Psychosocial interventions. One review of the role of non-biological treatment in very late-onset schizophrenia22 stressed the need to develop trust between patient and psychiatrist, so that the patient clearly views the treatment team as allies (Table 3). To that end, look for thoughts, feelings, or situations that may have precipitated the onset of psychosis, and explore their subjective meaning with the patient. Address any clear losses that are identified, such as the recent death of a spouse or other family member.
Table 3
DOs AND DON’Ts OF MANAGING AN OLDER PATIENT WITH SCHIZOPHRENIA
| Do | Don’t |
|---|---|
|
|
Find out if the patient is isolated and to what degree he or she feels lonely. Encourage the patient to engage in activities that he or she once enjoyed, and subtly introduce the patient to an appropriate community support group. Suggesting participation in group leisure activities may also help. Ascertain the patient’s living arrangements and basic needs. You may need to refer the patient to a social agency for assistance with housing, finances, nutrition/diet, and transportation.
Reminiscence therapy, through which patients are encouraged to reflect on their lives, can be useful for patients with very late-onset schizophrenia. Through reflection, patients can review past successes and painful experiences and move toward ultimate resolution of conflict and current difficulties.22
As in younger patients with schizophrenia, cognitivebehavioral therapy can help to modify delusional beliefs, gain control over hallucinations, and identify high-risk situations and appropriate coping strategies.23
Include family members in the treatment plan, and offer them support, education, and practical assistance (e.g., strategies for dealing with delusions). Informed families can help patients comply with prescriptions and appointments and can also detect relapse in its early stages.
In some cases, the patient’s longstanding paranoia and paranoid personality can lead to resentment and conflict within the family. Before treatment can begin, you may also need to address this conflict by educating family members on how a loved one’s schizophrenia affects them. Counseling the family as a group may be appropriate in some cases.
Related resources
- Howard R, Rabins PV, Castle DJ, eds. Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical; 1999.
- Howard R, Rabins PV, Seeman MV, et al. Late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: an international consensus. Am J Psychiatry 2000; 157:172-8.
Drug brand names
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no affiliation or financial arrangement with any of the companies whose products are mentioned in this article, or with manufacturers of competing products.
Acknowledgements
Dr. Lubman wishes to thank the Nauma Licht Fellowship, a bequest supporting schizophrenia research, for its support.
Mr. B, age 73, repeatedly complained to his landlord that people were trying to poison him by pumping noxious gas into his apartment. He barricaded himself inside, taped up all air vents and windows, and left only when absolutely necessary. At night, he could hear people working the “apparatus” that pumped the gas, and could “smell” the vapors.
On examination, he was physically well but suffered from mild neural deafness and myopia. He was suspicious and guarded but oriented and not cognitively impaired. He expressed paranoid beliefs and experienced auditory and olfactory hallucinations. There was no evidence of affective disturbance.
At first he refused psychiatric care but eventually agreed to take risperidone, 0.5 mg at night. He tolerated the agent well, and his psychotic symptoms slowly resolved.
As Mr. B’s case illustrates, schizophrenia—once thought to be strictly an early-onset disorder—commonly manifests late in life (Box). Too often, however, very late-onset schizophrenia goes undiagnosed because older patients with the disorder tend to be socially isolated. Their symptoms of paranoia and reluctance by family members to intervene also can prevent them from receiving treatment that could control psychotic symptoms and improve their quality of life.
Most clinical samples of patients with schizophrenia cite few cases of onset after age 60, reflecting the confused and changing nosology of very late-onset schizophrenia.
DSM-III (1980) stated that the schizophrenia label could apply only if onset occurred before age 45. This stipulation was dropped in DSM-III-R (1987), but it undoubtedly led psychiatrists to believe that schizophrenia simply did not begin in late life. The International Late-Onset Schizophrenia Group1 today recognizes the disorder’s late-onset version as “verylate-onset schizophrenia-like psychosis.”
General population studies report rates of “late paraphrenia” of around 1%, but these studies probably underestimate the true prevalence. One presumes that persons with paranoia are less likely than those without to participate in such a study.
The Camberwell Register First Episode Study,2 performed in London, is one of the few to determine rates of nonaffective psychosis across all ages of onset. In this study, 12% of the 513 patients studied across 20 years had illness onset after age 60. Researchers suspect a similar incidence in the U.S. population.
Psychosis presenting at any age, but especially in later life, requires careful evaluation to exclude organic pathology. Very late-onset schizophrenia differs substantially from psychosis associated with dementia, as in Alzheimer’s disease, both in terms of neuropsychological and brain imaging findings.
Although limited, data on late-life psychosis offer clues to its diagnosis and treatment. This article will address:
- risk factors and clinical presentations associated with late-onset schizophrenia
- pharmacologic and psychosocial treatment options based on available evidence.
Clinical presentation
Clinical presentation of schizophrenia with onset after age 60 differs from that of early-onset schizophrenia (Table 1). To those familiar with early-onset cases, the most obvious differences in late-onset patients are negligible rates of primary negative symptoms and formal thought disorder.
Persecutory delusions are common in both types and often are elaborate. The so-called “partition” delusion, which leads the patient to believe that people or objects can transgress impermeable barriers and access his or her home with malign intent, is more common in late-onset than in early-onset schizophrenia.3
Hallucinations in very late-onset schizophrenia are often prominent and can occur in multiple modalities, including auditory, visual, and olfactory. Sometimes the hallucination and delusion are clearly linked; for example, a patient claims to smell the noxious gas he believes is being pumped into his home.
Does the difference in presentation between early- and very late-onset schizophrenia reflect distinct disease processes or the disorder’s impact at different stages of brain maturation and degeneration? To answer that question, researchers have compared late-onset patients with young early-onset patents and with older patients who developed schizophrenia in their youth. Similar phenomena have been found in both early-onset groups,4 suggesting that age of onset causes the differences in clinical presentation.
Risk factors
As with early-onset schizophrenia, family history is the most common cause of very late-onset schizophrenia. Despite their limitations, family history studies almost all show a familial risk of very late-onset schizophrenia lower than that of early-onset patients but greater than that of the general population.5 Published studies do not tell us whether age of onset is genetically determined, in part because not all patients at risk for very late-onset schizophrenia live long enough to manifest its symptoms.
Family history has been associated with affective disorder in some patients with very late-onset schizophrenia. One casecontrolled series of family interviews6 found an approximate 1.3% rate of schizophrenia in relatives —about the same rate as that of the control group. The rate of depression among relatives of patients with very late-onset schizophrenia was 16.3%, compared with only 4.4% for controls (p = 0.003). Thus, late-onset psychosis and affective disorders may have etiologic links.7
Other possible risk factors for very late-onset schizophrenia include sensory deficits, premorbid personality disorder, social isolation, neuropsychological abnormalities, and female gender.
Sensory deficits. Several studies have reported that hearing and vision loss is more prevalent in older patients with very late-onset schizophrenia than in similarly aged controls. Most of these studies have associated either auditory or sensory impairment with very late-onset schizophrenia,8 but most did not include appropriate controls.
One case-control study (of younger patients)8 found that only uncorrected sensory deficits were over-represented in late-onset cases. This finding implies that one should find out if the patient is willing or able to get medical help for the sensory deficit, as well as whether that treatment has been adequate, before calling the sensory deficit a sequela of late-onset schizophrenia.
Premorbid personality disorder. Patients with very late-onset schizophrenia are widely reported to have gone through life reclusive and paranoid.5 Of interest is that unlike many of their early-onset counterparts, late-onset patients tend to have achieved fairly well in the workplace. Whether this success reflects a later onset of illness cannot be determined.
Social isolation is common among older persons and even more so among those with very late-onset schizophrenia.9 Whether this finding reflects patients’ premorbid personalities, the illness itself, or a risk factor for the disorder is open to conjecture.
Neuropsychological abnormalities. Assessments of patients with very late-onset schizophrenia reveal cognitive impairment patterns similar to those reported in patients with an earlier onset10 but distinct from those reported in patients with psychosis associated with dementia. CTand MRIstudies reveal focal (reduced left temporal lobe volume) and nonspecific (increased ventricular-to-brain ratios) structural abnormalities similar to those in younger patients.11
Table 1
CLINICAL FEATURES OF SCHIZOPHRENIA: EARLY- VS. VERY LATE-ONSET TYPES
| Clinical feature | Early onset | Very late onset |
|---|---|---|
| Persecutory delusions | Common (often elaborate) | Common (often elaborate) |
| Partition delusions | Rare | Common |
| Negative symptoms | Common | Rare |
| Formal thought disorder | Common | Rare |
| Hallucinations | Common, especially auditory | Often prominent (can manifest in multiple modalities) |
| Gender differences | Equally common in men, women | More common in women |
| Family history of schizophrenia | Common | Less common |
| Uncorrected auditory, visual impairments | No consistent relationship | Common; excessive in some patients |
| Premorbid personality | Maybe schizoid/schizotypal | Reclusive, suspicious |
| Social abilities | Social isolation | Social isolation |
| Marital status | Usually unmarried | Usually unmarried |
| Cognitive deficits, structural brain abnormalities | Similar for both groups | Similar for both groups |
Researchers previously reported excessive white-matter abnormalities in late-onset patients compared with healthy controls—a consistent finding in patients with late-life depression. More recent studies that carefully excluded organic cerebral disorders have not replicated this finding, however.11
Female gender. Very late-onset schizophrenia is more common in women than in men.12 Female-to-male ratios ranging from 2.2:1 to 22.5:1 have been calculated. Although women generally live longer than men, this predominance is still greater than one would expect. It might also hide important clues regarding schizophrenia and related disorders across the life span, including the fact that the brains of men and women show sex-specific patterns of aging.12
Managing very late-onset schizophrenia
Initial assessment. Patients who present with a new-onset psychotic disorder at any age require careful evaluation to exclude an underlying organic cause. The following are strongly suggested in older patients with new-onset psychoses:
- comprehensive history (including medications)
- physical (including neurologic) examination
- laboratory investigations
- CTneuroimaging
- and cognitive screening, such as the Mini Mental State Examination.
Drug treatment. Despite the wealth of published data on the psychopharmacologic management of schizophrenia, few randomized, controlled trials have examined the use of drugs to treat the disorder’s very late-onset form. Case reports or small open studies comprise the available literature. Significant flaws in treatment studies have included diagnostic heterogeneity, mixing of early- and late-onset patients, inadequate outcome criteria, and lack of control groups.13
As with early-onset schizophrenia, however, antipsychotics appear to improve the acute symptoms of very late-onset schizophrenia and reduce the risk of relapse.14 Pearlson et al4 reported at least partial remission in 76% of patients with late-onset schizophrenia after neuroleptic regimens (complete remission occurred in 48%). The presence of thought disorder or a premorbid schizoid personality predicted poor response to treatment, whereas gender, family history, and first-rank symptoms (auditory hallucinations, delusions, social withdrawal) did not significantly affect outcome.
Very late-onset patients respond to about one-half the antipsychotic dosage required for younger patients.13 Sweet and Pollock15 found an average dosage of chlorpromazine equivalents, 148 mg/d, to be effective in older patients, compared with >300 mg/d in younger cohorts.
Neuroleptic side effects. Older patients are more susceptible than their younger counterparts to side effects and adverse reactions from typical neuroleptics, even at low dosages. Age-related differences in pharmacokinetics and pharmacodynamics, combined with the increased incidence of comorbid physical disease and polypharmacy among older patients, often complicate pharmacotherapy for late-onset schizophrenia.
Older patients taking antipsychotics face an increased risk of extrapyramidal symptoms (EPS), especially parkinsonism and akathisia.16 Anticholinergics are poorly tolerated and may cause urinary retention, constipation, blurred vision, exacerbation of glaucoma, and delirium. Cardiovascular side effects, especially orthostatic hypotension, may lead to falls and significant injury and may exacerbate coexisting cardiovascular disease.
Neuroleptic-induced tardive dyskinesia (TD) is another potential complication. Jeste et al found the cumulative annual incidence of drug-induced TD to be five times greater among older psychotic patients than among younger ones (26% vs. 5% after 1 year).17 Duration of exposure and total cumulative amount of prescribed neuroleptics remain significant risk factors for TD in older patients.
Atypical antipsychotics, with their less-adverse side-effect profiles and lower risk of EPS (and probably TD as well) are the preferred first-line drugs for late-onset schizophrenia. These agents also have been associated with improved cognition in younger patients with schizophrenia, a potentially significant benefit in the older patient.
Table 2
ANTIPSYCHOTIC DOSAGES RECOMMENDED FOR VERY LATE-ONSET SCHIZOPHRENIA
| Drugs | Initial dosages | Maintenance dosages |
|---|---|---|
| Olanzapine | 1 to 5 mg/d | 2.5 to 15 mg/d |
| Risperidone | 0.25 to 0.5 mg/d | 0.5 to 3 mg/d |
| Quetiapine | 12.5 to 25 mg/d | 75 to 150 mg/d |
No well-controlled trials of clozapine in very late-onset schizophrenia have been performed. According to one literature review,18 most older psychotic patients showed moderate to marked improvement at relatively low dosages (mean dosage 134 mg/d). The reviewers concluded that clozapine was safe and well tolerated but suggested that agranulocytosis may occur at higher rates in this group than in younger patients. Clozapine’s potent anticholinergic action and its marked sedative effects limit its use in very late-onset schizophrenia to treatmentresistant patients or those with severe TD.
Data on the use of other atypical agents in very late-onset schizophrenia are limited. Risperidone has been associated with significant improvements in older patients with schizophrenia.16 Risperidone, olanzapine, and quetiapine have all been found to be safe, well-tolerated, and effective in managing late-life psychotic disorders.16,19,20 As with neuroleptics, recommended starting and maintenance dosages of the atypicals are lower than those used in younger patients (Table 2).13
A “start low, go slow” approach is warranted, and dosages should be adjusted according to clinical response. Communicate with the patient’s primary care physician to learn of any potential drug-drug interactions with medications being given for comorbid illnesses.
Electroconvulsive therapy has been reported to be useful in several studies, but data on its use in very late-onset schizophrenia are limited.21
Psychosocial interventions. One review of the role of non-biological treatment in very late-onset schizophrenia22 stressed the need to develop trust between patient and psychiatrist, so that the patient clearly views the treatment team as allies (Table 3). To that end, look for thoughts, feelings, or situations that may have precipitated the onset of psychosis, and explore their subjective meaning with the patient. Address any clear losses that are identified, such as the recent death of a spouse or other family member.
Table 3
DOs AND DON’Ts OF MANAGING AN OLDER PATIENT WITH SCHIZOPHRENIA
| Do | Don’t |
|---|---|
|
|
Find out if the patient is isolated and to what degree he or she feels lonely. Encourage the patient to engage in activities that he or she once enjoyed, and subtly introduce the patient to an appropriate community support group. Suggesting participation in group leisure activities may also help. Ascertain the patient’s living arrangements and basic needs. You may need to refer the patient to a social agency for assistance with housing, finances, nutrition/diet, and transportation.
Reminiscence therapy, through which patients are encouraged to reflect on their lives, can be useful for patients with very late-onset schizophrenia. Through reflection, patients can review past successes and painful experiences and move toward ultimate resolution of conflict and current difficulties.22
As in younger patients with schizophrenia, cognitivebehavioral therapy can help to modify delusional beliefs, gain control over hallucinations, and identify high-risk situations and appropriate coping strategies.23
Include family members in the treatment plan, and offer them support, education, and practical assistance (e.g., strategies for dealing with delusions). Informed families can help patients comply with prescriptions and appointments and can also detect relapse in its early stages.
In some cases, the patient’s longstanding paranoia and paranoid personality can lead to resentment and conflict within the family. Before treatment can begin, you may also need to address this conflict by educating family members on how a loved one’s schizophrenia affects them. Counseling the family as a group may be appropriate in some cases.
Related resources
- Howard R, Rabins PV, Castle DJ, eds. Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical; 1999.
- Howard R, Rabins PV, Seeman MV, et al. Late-onset schizophrenia and very-late-onset schizophrenia-like psychosis: an international consensus. Am J Psychiatry 2000; 157:172-8.
Drug brand names
- Clozapine • Clozaril
- Olanzapine • Zyprexa
- Quetiapine • Seroquel
- Risperidone • Risperdal
Disclosure
The authors report no affiliation or financial arrangement with any of the companies whose products are mentioned in this article, or with manufacturers of competing products.
Acknowledgements
Dr. Lubman wishes to thank the Nauma Licht Fellowship, a bequest supporting schizophrenia research, for its support.
1. Howard R, Rabins PV, Seeman MV, et al. Consensus statement of the International Late Onset Schizophrenia Group. In: Howard R, Rabins PV, Castle DJ, (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;263-6.
2. Castle DJ, Wessely S, Van Os J, et al. Psychosis in the inner city: The Camberwell First Episode Study. Maudsley Monograph 40. Hove, UK: Psychology Press, 1998.
3. Howard R, Castle DJ, O’Brien J, et al. Permeable walls, floors, ceilings and doors: partition delusions in late paraphrenia. Int J Geriatr Psychiatry 1992;7:719-24.
4. Pearlson GD, Kreger L, Rabins PV, et al. A chart review study of late-onset and early-onset schizophrenia. Am J Psychiatry 1989;146:1568-74.
5. Castle DJ, Howard R. What do we know about the aetiology of late onset schizophrenia? Eur Psychiatry 1992;7:99-108.
6. Howard R, Graham C, Sham P, et al. A controlled family study of late-onset non-affective psychosis (late paraphrenia). Br J Psychiatry 1997;170:511-4.
7. Murray RM, O’Callaghan E, Castle DJ, et al. A neurodevelopmental approach to the classification of schizophrenia. Schizophr Bull 1992;18:319-32.
8. Prager S, Jeste DV. Sensory impairment in late life schizophrenia. Schizophr Bull 1993;19:755-71.
9. Kay DWK. The English language literature on late paraphrenia from the 1950s. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;17-43.
10. Jeste DV, Harris MJ, Krull A, et al. Clinical and neuropsychological characteristics of patients with late-onset schizophrenia. Am J Psychiatry 1995;152:722-30.
11. Pearlson GD. Brain imaging in late onset schizophrenia. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;191-204.
12. Castle DJ. Gender and age at onset in schizophrenia. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;147-64.
13. Salzman C, Tune L. Neuroleptic treatment of late-life schizophrenia. Harvard Rev Psychiatry 2001;9:77-83.
14. Harris MJ, Jeste DV. Late-onset schizophrenia: an overview. Schizophr Bull 1988;14:39-55.
15. Sweet RA, Pollock BG. Neuroleptics in the elderly: guidelines for monitoring. Harvard Rev Psychiatry 1995;2:327-35.
16. Sciolla A, Jeste DV. Use of antipsychotics in the elderly. Int J Psych Clin Pract 1998;2(suppl 1):S27-S34.
17. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients: a prospective longitudinal study of 266 patients. Arch Gen Psychiatry 1995;52:756-65.
18. Barak Y, Wittenberg N, Naor S, et al. Clozapine in elderly psychiatric patients: tolerability, safety and efficacy. Compr Psychiatry 1999;40:320-5.
19. Madhusoodanan S, Suresh P, et al. Experience with the atypical antipsychotics—risperidone and olanzapine in the elderly. Ann Clin Psychiatry 1999;11(3):113-8.
20. Arvanitis LA, Miller BG. Multiple fixed doses of “Seroquel” (quetiapine) in patients with acute exacerbation of schizophrenia: a comparison with haloperidol and placebo. Biol Psychiatry 1997;42(4):233-46.
21. Kay DWK, Roth M. Environmental and hereditary factors in the schizophrenias of old age (‘late paraphrenia’) and their bearing on the general problem of causation in schizophrenia. J Mental Sci 1961;107:649-86.
22. Aguera-Ortiz L, Reneses-Prieto B. The place of non-biological treatments. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;233:60.-
23. Fowler D, Garety P, Kuipers E. Cognitive behavioural therapy for psychosis: theory and practice. Chichester, UK: Wiley, 1995.
1. Howard R, Rabins PV, Seeman MV, et al. Consensus statement of the International Late Onset Schizophrenia Group. In: Howard R, Rabins PV, Castle DJ, (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;263-6.
2. Castle DJ, Wessely S, Van Os J, et al. Psychosis in the inner city: The Camberwell First Episode Study. Maudsley Monograph 40. Hove, UK: Psychology Press, 1998.
3. Howard R, Castle DJ, O’Brien J, et al. Permeable walls, floors, ceilings and doors: partition delusions in late paraphrenia. Int J Geriatr Psychiatry 1992;7:719-24.
4. Pearlson GD, Kreger L, Rabins PV, et al. A chart review study of late-onset and early-onset schizophrenia. Am J Psychiatry 1989;146:1568-74.
5. Castle DJ, Howard R. What do we know about the aetiology of late onset schizophrenia? Eur Psychiatry 1992;7:99-108.
6. Howard R, Graham C, Sham P, et al. A controlled family study of late-onset non-affective psychosis (late paraphrenia). Br J Psychiatry 1997;170:511-4.
7. Murray RM, O’Callaghan E, Castle DJ, et al. A neurodevelopmental approach to the classification of schizophrenia. Schizophr Bull 1992;18:319-32.
8. Prager S, Jeste DV. Sensory impairment in late life schizophrenia. Schizophr Bull 1993;19:755-71.
9. Kay DWK. The English language literature on late paraphrenia from the 1950s. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;17-43.
10. Jeste DV, Harris MJ, Krull A, et al. Clinical and neuropsychological characteristics of patients with late-onset schizophrenia. Am J Psychiatry 1995;152:722-30.
11. Pearlson GD. Brain imaging in late onset schizophrenia. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;191-204.
12. Castle DJ. Gender and age at onset in schizophrenia. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;147-64.
13. Salzman C, Tune L. Neuroleptic treatment of late-life schizophrenia. Harvard Rev Psychiatry 2001;9:77-83.
14. Harris MJ, Jeste DV. Late-onset schizophrenia: an overview. Schizophr Bull 1988;14:39-55.
15. Sweet RA, Pollock BG. Neuroleptics in the elderly: guidelines for monitoring. Harvard Rev Psychiatry 1995;2:327-35.
16. Sciolla A, Jeste DV. Use of antipsychotics in the elderly. Int J Psych Clin Pract 1998;2(suppl 1):S27-S34.
17. Jeste DV, Caligiuri MP, Paulsen JS, et al. Risk of tardive dyskinesia in older patients: a prospective longitudinal study of 266 patients. Arch Gen Psychiatry 1995;52:756-65.
18. Barak Y, Wittenberg N, Naor S, et al. Clozapine in elderly psychiatric patients: tolerability, safety and efficacy. Compr Psychiatry 1999;40:320-5.
19. Madhusoodanan S, Suresh P, et al. Experience with the atypical antipsychotics—risperidone and olanzapine in the elderly. Ann Clin Psychiatry 1999;11(3):113-8.
20. Arvanitis LA, Miller BG. Multiple fixed doses of “Seroquel” (quetiapine) in patients with acute exacerbation of schizophrenia: a comparison with haloperidol and placebo. Biol Psychiatry 1997;42(4):233-46.
21. Kay DWK, Roth M. Environmental and hereditary factors in the schizophrenias of old age (‘late paraphrenia’) and their bearing on the general problem of causation in schizophrenia. J Mental Sci 1961;107:649-86.
22. Aguera-Ortiz L, Reneses-Prieto B. The place of non-biological treatments. In: Howard R, Rabins PV, Castle DJ (eds). Late onset schizophrenia. Petersfield, UK: Wrightson Biomedical, 1999;233:60.-
23. Fowler D, Garety P, Kuipers E. Cognitive behavioural therapy for psychosis: theory and practice. Chichester, UK: Wiley, 1995.
Personal digital assistants: Which one is right for your practice?
Personal digital assistants (PDAs) are becoming more commonplace in practice because they immediately provide critical information at the point of care.
If you’re in the market for a handheld computer, chances are you’re fazed by the multitude of available models, upgrades, and extras. Choosing a PDA is not that difficult, however, if you take the time to assess your needs and do a little homework. Start by answering these four questions:
1. Why do I need a PDA? Look at your work patterns and see how a PDA would fit in. Do you frequently look up DSM-IV criteria and other reference information? Are you constantly writing prescriptions, giving presentations, or assessing drug-drug interactions? Do you find yourself regularly checking your schedule?
Also try to envision:
- where you would carry the device
- where, when, and how you would charge it when needed
- what connections to computers for data exchange are available
- with whom you would share data
- and from whom you could get technical support.
You may have trouble thinking that far ahead, but doing so will help you narrow your PDA choices.
2. Which operating system should I use? A PDA operates on one of four main operating systems:
- Palm OS, the most popular world wide
- EPOC OS, which is more popular in Europe
- Pocket PC, which is rapidly gaining popularity
- and Linux OS, which recently entered the PDA market.
Choosing a PDA platform is much like deciding between Macintosh and Windows. The differences between PDAs based on Pocket PC or Palm OS have been diminishing in the last year. All PDAs have similar basic personal information manager functions, but available software, hardware features, and accessories set them apart. Pocket PC-based PDAs generally have much more memory and more diverse multimedia capabilities-but also lower battery life (1 day with average use) and compatibility with fewer software titles-than do Palm OS devices.
Because of their higher memory capacity, Pocket PC PDAs may generally be better suited to:
- large groups or organizations
- and users who rely heavily on multimedia, large data sets, or interface with Microsoft Office documents.
However, newer PDAs that are based on Palm OS 5 and employ the StrongARM processor (as do Pocket PC devices) offer greatly improved function in these areas. Compared with Pocket PC PDAs, Palm OS devices are much more intuitive and easier to use, offer longer battery life (1 week or more for average use), and are compatible with more medical software titles. More physicians use Palm OS PDAs because of their simplicity and reliability.
Consider either a Palm or Pocket PC PDA. EPOC PDAs are good devices, but Psion, a major manufacturer, has ceased development of EPOC devices to focus on specific markets. Linux PDAs are only recommended to users who are familiar with Linux or UNIX and are capable of writing their own software.
3. Where should I purchase my PDA? Visit any major computer, office supply, or electronics or chain retailer and check out the different models and manufacturers. Consider your priorities on features such as size, screen resolution, color, weight, memory, wireless capability, and accessory options. Consider purchasing there or online.
The level of support you need should dictate your point of purchase. Online retailers usually charge less for PDAs, but devices may be back-ordered and support often is offered only through the manufacturer. Beginners are probably wise to purchase locally and obtain support through the store.
4. How can I avoid purchasing a soon-to-be-obsolete model? Because PDA technology is improving so rapidly, new devices are frequently reaching the market. This can be frustrating to someone who has just purchased what he or she thought was the latest model.
If you are a beginner, plan to keep your PDA device for at least 1 year while you gradually learn to use it to its full potential. Consider spending about $200 for a device, then upgrade only when newer devices provide more features that you can use. Avid users may upgrade more frequently and spend $500 or more for a device.
Palm vs. Pocket PC: Finer points
Palm OS PDAs. If you are new to PDAs, start with a Palm OS-based PDA from Palm, Sony, or Handspring. The Sony models make more sense if you have or plan to purchase other Sony products (e.g., digital cameras, digital camcorders, computers) because the PDA’s external memory stick can be shared among the products.
Handspring offers models integrated with a cellular phone if you prefer a combined device. The Palm Tungsten T has built-in Bluetooth wireless mobile capability and offers portable keyboards that fold out to full size.
Pocket PC PDAs. Not long ago, Pocket PC PDAs were only compatible with software specific to the device’s processor. Today, the StrongARM processor is standard in any device running on Pocket PC 2002. Therefore, stick with Pocket PC 2002 devices only, as many of the earlier devices cannot be upgraded.
Because Pocket PC devices offer such a short battery life, consider a device with interchangeable lithium batteries or purchase a portable charger. If you choose a Pocket PC with integrated wireless connectivity, be aware that your battery life will be about 2 to 3 hours. Avoid the Jornada line of handhelds, as these will be phased out in the merger of Compaq and Hewlett Packard.
To learn more about PDAs
The Internet has a wealth of information on these devices. PDABuzz, Handango, and PDAGeek offer reviews, user opinions, and useful links. Two excellent magazines, Handheld Computing Magazine (www.hhcmag.com) and Pocket PC Magazine (www.pocketpcmag.com), are devoted to PDA/handheld computers. Manufacturers also post extensive information about their PDA devices on their Web sites (Box).
If you have any questions about PDAs or comments about Psyber Psychiatry, click here to contact Dr. Luo or send an e-mail to [email protected].
Palm OS
Manufacturer URL
Palm www.palm.com
Handspring www.handspring.com
HandEra www.handera.com
Sony http://www.sonystyle.com/
Acer global.acer.com/products/pda/index.htm
Pocket PC OS
Audiovox www.audiovox.com/pda
Casio www.casio.com
Toshiba pda.toshiba.com
HP www.compaq.com/products/handhelds/pocketpc/index.html
NEC www.neccomp.com/v2/products/MobilePro/P300/
Zayo (Asus) usa.asus.com/PDA/a600/overview.htm
ViewSonic www.viewsonic.com/products/pocket_pc_pocketpcv35.htm
URThere www.urthere.com
Related Resources
Carlson J. Palm organizers: visual quick start guide (2nd ed). Berkeley, CA: Peachpit Press, 2001.
Chan C, Luo J, Kennedy R. Concise guide to computers in clinical psychiatry (1st ed). Washington, DC: American Psychiatric Press, 2002.
Dyzsel B. Palm for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Underdahl B. Pocket PCs for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Personal digital assistants (PDAs) are becoming more commonplace in practice because they immediately provide critical information at the point of care.
If you’re in the market for a handheld computer, chances are you’re fazed by the multitude of available models, upgrades, and extras. Choosing a PDA is not that difficult, however, if you take the time to assess your needs and do a little homework. Start by answering these four questions:
1. Why do I need a PDA? Look at your work patterns and see how a PDA would fit in. Do you frequently look up DSM-IV criteria and other reference information? Are you constantly writing prescriptions, giving presentations, or assessing drug-drug interactions? Do you find yourself regularly checking your schedule?
Also try to envision:
- where you would carry the device
- where, when, and how you would charge it when needed
- what connections to computers for data exchange are available
- with whom you would share data
- and from whom you could get technical support.
You may have trouble thinking that far ahead, but doing so will help you narrow your PDA choices.
2. Which operating system should I use? A PDA operates on one of four main operating systems:
- Palm OS, the most popular world wide
- EPOC OS, which is more popular in Europe
- Pocket PC, which is rapidly gaining popularity
- and Linux OS, which recently entered the PDA market.
Choosing a PDA platform is much like deciding between Macintosh and Windows. The differences between PDAs based on Pocket PC or Palm OS have been diminishing in the last year. All PDAs have similar basic personal information manager functions, but available software, hardware features, and accessories set them apart. Pocket PC-based PDAs generally have much more memory and more diverse multimedia capabilities-but also lower battery life (1 day with average use) and compatibility with fewer software titles-than do Palm OS devices.
Because of their higher memory capacity, Pocket PC PDAs may generally be better suited to:
- large groups or organizations
- and users who rely heavily on multimedia, large data sets, or interface with Microsoft Office documents.
However, newer PDAs that are based on Palm OS 5 and employ the StrongARM processor (as do Pocket PC devices) offer greatly improved function in these areas. Compared with Pocket PC PDAs, Palm OS devices are much more intuitive and easier to use, offer longer battery life (1 week or more for average use), and are compatible with more medical software titles. More physicians use Palm OS PDAs because of their simplicity and reliability.
Consider either a Palm or Pocket PC PDA. EPOC PDAs are good devices, but Psion, a major manufacturer, has ceased development of EPOC devices to focus on specific markets. Linux PDAs are only recommended to users who are familiar with Linux or UNIX and are capable of writing their own software.
3. Where should I purchase my PDA? Visit any major computer, office supply, or electronics or chain retailer and check out the different models and manufacturers. Consider your priorities on features such as size, screen resolution, color, weight, memory, wireless capability, and accessory options. Consider purchasing there or online.
The level of support you need should dictate your point of purchase. Online retailers usually charge less for PDAs, but devices may be back-ordered and support often is offered only through the manufacturer. Beginners are probably wise to purchase locally and obtain support through the store.
4. How can I avoid purchasing a soon-to-be-obsolete model? Because PDA technology is improving so rapidly, new devices are frequently reaching the market. This can be frustrating to someone who has just purchased what he or she thought was the latest model.
If you are a beginner, plan to keep your PDA device for at least 1 year while you gradually learn to use it to its full potential. Consider spending about $200 for a device, then upgrade only when newer devices provide more features that you can use. Avid users may upgrade more frequently and spend $500 or more for a device.
Palm vs. Pocket PC: Finer points
Palm OS PDAs. If you are new to PDAs, start with a Palm OS-based PDA from Palm, Sony, or Handspring. The Sony models make more sense if you have or plan to purchase other Sony products (e.g., digital cameras, digital camcorders, computers) because the PDA’s external memory stick can be shared among the products.
Handspring offers models integrated with a cellular phone if you prefer a combined device. The Palm Tungsten T has built-in Bluetooth wireless mobile capability and offers portable keyboards that fold out to full size.
Pocket PC PDAs. Not long ago, Pocket PC PDAs were only compatible with software specific to the device’s processor. Today, the StrongARM processor is standard in any device running on Pocket PC 2002. Therefore, stick with Pocket PC 2002 devices only, as many of the earlier devices cannot be upgraded.
Because Pocket PC devices offer such a short battery life, consider a device with interchangeable lithium batteries or purchase a portable charger. If you choose a Pocket PC with integrated wireless connectivity, be aware that your battery life will be about 2 to 3 hours. Avoid the Jornada line of handhelds, as these will be phased out in the merger of Compaq and Hewlett Packard.
To learn more about PDAs
The Internet has a wealth of information on these devices. PDABuzz, Handango, and PDAGeek offer reviews, user opinions, and useful links. Two excellent magazines, Handheld Computing Magazine (www.hhcmag.com) and Pocket PC Magazine (www.pocketpcmag.com), are devoted to PDA/handheld computers. Manufacturers also post extensive information about their PDA devices on their Web sites (Box).
If you have any questions about PDAs or comments about Psyber Psychiatry, click here to contact Dr. Luo or send an e-mail to [email protected].
Palm OS
Manufacturer URL
Palm www.palm.com
Handspring www.handspring.com
HandEra www.handera.com
Sony http://www.sonystyle.com/
Acer global.acer.com/products/pda/index.htm
Pocket PC OS
Audiovox www.audiovox.com/pda
Casio www.casio.com
Toshiba pda.toshiba.com
HP www.compaq.com/products/handhelds/pocketpc/index.html
NEC www.neccomp.com/v2/products/MobilePro/P300/
Zayo (Asus) usa.asus.com/PDA/a600/overview.htm
ViewSonic www.viewsonic.com/products/pocket_pc_pocketpcv35.htm
URThere www.urthere.com
Related Resources
Carlson J. Palm organizers: visual quick start guide (2nd ed). Berkeley, CA: Peachpit Press, 2001.
Chan C, Luo J, Kennedy R. Concise guide to computers in clinical psychiatry (1st ed). Washington, DC: American Psychiatric Press, 2002.
Dyzsel B. Palm for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Underdahl B. Pocket PCs for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Personal digital assistants (PDAs) are becoming more commonplace in practice because they immediately provide critical information at the point of care.
If you’re in the market for a handheld computer, chances are you’re fazed by the multitude of available models, upgrades, and extras. Choosing a PDA is not that difficult, however, if you take the time to assess your needs and do a little homework. Start by answering these four questions:
1. Why do I need a PDA? Look at your work patterns and see how a PDA would fit in. Do you frequently look up DSM-IV criteria and other reference information? Are you constantly writing prescriptions, giving presentations, or assessing drug-drug interactions? Do you find yourself regularly checking your schedule?
Also try to envision:
- where you would carry the device
- where, when, and how you would charge it when needed
- what connections to computers for data exchange are available
- with whom you would share data
- and from whom you could get technical support.
You may have trouble thinking that far ahead, but doing so will help you narrow your PDA choices.
2. Which operating system should I use? A PDA operates on one of four main operating systems:
- Palm OS, the most popular world wide
- EPOC OS, which is more popular in Europe
- Pocket PC, which is rapidly gaining popularity
- and Linux OS, which recently entered the PDA market.
Choosing a PDA platform is much like deciding between Macintosh and Windows. The differences between PDAs based on Pocket PC or Palm OS have been diminishing in the last year. All PDAs have similar basic personal information manager functions, but available software, hardware features, and accessories set them apart. Pocket PC-based PDAs generally have much more memory and more diverse multimedia capabilities-but also lower battery life (1 day with average use) and compatibility with fewer software titles-than do Palm OS devices.
Because of their higher memory capacity, Pocket PC PDAs may generally be better suited to:
- large groups or organizations
- and users who rely heavily on multimedia, large data sets, or interface with Microsoft Office documents.
However, newer PDAs that are based on Palm OS 5 and employ the StrongARM processor (as do Pocket PC devices) offer greatly improved function in these areas. Compared with Pocket PC PDAs, Palm OS devices are much more intuitive and easier to use, offer longer battery life (1 week or more for average use), and are compatible with more medical software titles. More physicians use Palm OS PDAs because of their simplicity and reliability.
Consider either a Palm or Pocket PC PDA. EPOC PDAs are good devices, but Psion, a major manufacturer, has ceased development of EPOC devices to focus on specific markets. Linux PDAs are only recommended to users who are familiar with Linux or UNIX and are capable of writing their own software.
3. Where should I purchase my PDA? Visit any major computer, office supply, or electronics or chain retailer and check out the different models and manufacturers. Consider your priorities on features such as size, screen resolution, color, weight, memory, wireless capability, and accessory options. Consider purchasing there or online.
The level of support you need should dictate your point of purchase. Online retailers usually charge less for PDAs, but devices may be back-ordered and support often is offered only through the manufacturer. Beginners are probably wise to purchase locally and obtain support through the store.
4. How can I avoid purchasing a soon-to-be-obsolete model? Because PDA technology is improving so rapidly, new devices are frequently reaching the market. This can be frustrating to someone who has just purchased what he or she thought was the latest model.
If you are a beginner, plan to keep your PDA device for at least 1 year while you gradually learn to use it to its full potential. Consider spending about $200 for a device, then upgrade only when newer devices provide more features that you can use. Avid users may upgrade more frequently and spend $500 or more for a device.
Palm vs. Pocket PC: Finer points
Palm OS PDAs. If you are new to PDAs, start with a Palm OS-based PDA from Palm, Sony, or Handspring. The Sony models make more sense if you have or plan to purchase other Sony products (e.g., digital cameras, digital camcorders, computers) because the PDA’s external memory stick can be shared among the products.
Handspring offers models integrated with a cellular phone if you prefer a combined device. The Palm Tungsten T has built-in Bluetooth wireless mobile capability and offers portable keyboards that fold out to full size.
Pocket PC PDAs. Not long ago, Pocket PC PDAs were only compatible with software specific to the device’s processor. Today, the StrongARM processor is standard in any device running on Pocket PC 2002. Therefore, stick with Pocket PC 2002 devices only, as many of the earlier devices cannot be upgraded.
Because Pocket PC devices offer such a short battery life, consider a device with interchangeable lithium batteries or purchase a portable charger. If you choose a Pocket PC with integrated wireless connectivity, be aware that your battery life will be about 2 to 3 hours. Avoid the Jornada line of handhelds, as these will be phased out in the merger of Compaq and Hewlett Packard.
To learn more about PDAs
The Internet has a wealth of information on these devices. PDABuzz, Handango, and PDAGeek offer reviews, user opinions, and useful links. Two excellent magazines, Handheld Computing Magazine (www.hhcmag.com) and Pocket PC Magazine (www.pocketpcmag.com), are devoted to PDA/handheld computers. Manufacturers also post extensive information about their PDA devices on their Web sites (Box).
If you have any questions about PDAs or comments about Psyber Psychiatry, click here to contact Dr. Luo or send an e-mail to [email protected].
Palm OS
Manufacturer URL
Palm www.palm.com
Handspring www.handspring.com
HandEra www.handera.com
Sony http://www.sonystyle.com/
Acer global.acer.com/products/pda/index.htm
Pocket PC OS
Audiovox www.audiovox.com/pda
Casio www.casio.com
Toshiba pda.toshiba.com
HP www.compaq.com/products/handhelds/pocketpc/index.html
NEC www.neccomp.com/v2/products/MobilePro/P300/
Zayo (Asus) usa.asus.com/PDA/a600/overview.htm
ViewSonic www.viewsonic.com/products/pocket_pc_pocketpcv35.htm
URThere www.urthere.com
Related Resources
Carlson J. Palm organizers: visual quick start guide (2nd ed). Berkeley, CA: Peachpit Press, 2001.
Chan C, Luo J, Kennedy R. Concise guide to computers in clinical psychiatry (1st ed). Washington, DC: American Psychiatric Press, 2002.
Dyzsel B. Palm for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Underdahl B. Pocket PCs for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Personal digital assistants: Which one is right for your practice?
Personal digital assistants (PDAs) are becoming more commonplace in practice because they immediately provide critical information at the point of care.
If you’re in the market for a handheld computer, chances are you’re fazed by the multitude of available models, upgrades, and extras. Choosing a PDA is not that difficult, however, if you take the time to assess your needs and do a little homework. Start by answering these four questions:
1. Why do I need a PDA? Look at your work patterns and see how a PDA would fit in. Do you frequently look up DSM-IV criteria and other reference information? Are you constantly writing prescriptions, giving presentations, or assessing drug-drug interactions? Do you find yourself regularly checking your schedule?
Also try to envision:
- where you would carry the device
- where, when, and how you would charge it when needed
- what connections to computers for data exchange are available
- with whom you would share data
- and from whom you could get technical support.
You may have trouble thinking that far ahead, but doing so will help you narrow your PDA choices.
2. Which operating system should I use? A PDA operates on one of four main operating systems:
- Palm OS, the most popular world wide
- EPOC OS, which is more popular in Europe
- Pocket PC, which is rapidly gaining popularity
- and Linux OS, which recently entered the PDA market.
Choosing a PDA platform is much like deciding between Macintosh and Windows. The differences between PDAs based on Pocket PC or Palm OS have been diminishing in the last year. All PDAs have similar basic personal information manager functions, but available software, hardware features, and accessories set them apart. Pocket PC-based PDAs generally have much more memory and more diverse multimedia capabilities-but also lower battery life (1 day with average use) and compatibility with fewer software titles-than do Palm OS devices.
Because of their higher memory capacity, Pocket PC PDAs may generally be better suited to:
- large groups or organizations
- and users who rely heavily on multimedia, large data sets, or interface with Microsoft Office documents.
However, newer PDAs that are based on Palm OS 5 and employ the StrongARM processor (as do Pocket PC devices) offer greatly improved function in these areas. Compared with Pocket PC PDAs, Palm OS devices are much more intuitive and easier to use, offer longer battery life (1 week or more for average use), and are compatible with more medical software titles. More physicians use Palm OS PDAs because of their simplicity and reliability.
Consider either a Palm or Pocket PC PDA. EPOC PDAs are good devices, but Psion, a major manufacturer, has ceased development of EPOC devices to focus on specific markets. Linux PDAs are only recommended to users who are familiar with Linux or UNIX and are capable of writing their own software.
3. Where should I purchase my PDA? Visit any major computer, office supply, or electronics or chain retailer and check out the different models and manufacturers. Consider your priorities on features such as size, screen resolution, color, weight, memory, wireless capability, and accessory options. Consider purchasing there or online.
The level of support you need should dictate your point of purchase. Online retailers usually charge less for PDAs, but devices may be back-ordered and support often is offered only through the manufacturer. Beginners are probably wise to purchase locally and obtain support through the store.
4. How can I avoid purchasing a soon-to-be-obsolete model? Because PDA technology is improving so rapidly, new devices are frequently reaching the market. This can be frustrating to someone who has just purchased what he or she thought was the latest model.
If you are a beginner, plan to keep your PDA device for at least 1 year while you gradually learn to use it to its full potential. Consider spending about $200 for a device, then upgrade only when newer devices provide more features that you can use. Avid users may upgrade more frequently and spend $500 or more for a device.
Palm vs. Pocket PC: Finer points
Palm OS PDAs. If you are new to PDAs, start with a Palm OS-based PDA from Palm, Sony, or Handspring. The Sony models make more sense if you have or plan to purchase other Sony products (e.g., digital cameras, digital camcorders, computers) because the PDA’s external memory stick can be shared among the products.
Handspring offers models integrated with a cellular phone if you prefer a combined device. The Palm Tungsten T has built-in Bluetooth wireless mobile capability and offers portable keyboards that fold out to full size.
Pocket PC PDAs. Not long ago, Pocket PC PDAs were only compatible with software specific to the device’s processor. Today, the StrongARM processor is standard in any device running on Pocket PC 2002. Therefore, stick with Pocket PC 2002 devices only, as many of the earlier devices cannot be upgraded.
Because Pocket PC devices offer such a short battery life, consider a device with interchangeable lithium batteries or purchase a portable charger. If you choose a Pocket PC with integrated wireless connectivity, be aware that your battery life will be about 2 to 3 hours. Avoid the Jornada line of handhelds, as these will be phased out in the merger of Compaq and Hewlett Packard.
To learn more about PDAs
The Internet has a wealth of information on these devices. PDABuzz, Handango, and PDAGeek offer reviews, user opinions, and useful links. Two excellent magazines, Handheld Computing Magazine (www.hhcmag.com) and Pocket PC Magazine (www.pocketpcmag.com), are devoted to PDA/handheld computers. Manufacturers also post extensive information about their PDA devices on their Web sites (Box).
If you have any questions about PDAs or comments about Psyber Psychiatry, click here to contact Dr. Luo or send an e-mail to [email protected].
Palm OS
Manufacturer URL
Palm www.palm.com
Handspring www.handspring.com
HandEra www.handera.com
Sony http://www.sonystyle.com/
Acer global.acer.com/products/pda/index.htm
Pocket PC OS
Audiovox www.audiovox.com/pda
Casio www.casio.com
Toshiba pda.toshiba.com
HP www.compaq.com/products/handhelds/pocketpc/index.html
NEC www.neccomp.com/v2/products/MobilePro/P300/
Zayo (Asus) usa.asus.com/PDA/a600/overview.htm
ViewSonic www.viewsonic.com/products/pocket_pc_pocketpcv35.htm
URThere www.urthere.com
Related Resources
Carlson J. Palm organizers: visual quick start guide (2nd ed). Berkeley, CA: Peachpit Press, 2001.
Chan C, Luo J, Kennedy R. Concise guide to computers in clinical psychiatry (1st ed). Washington, DC: American Psychiatric Press, 2002.
Dyzsel B. Palm for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Underdahl B. Pocket PCs for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Personal digital assistants (PDAs) are becoming more commonplace in practice because they immediately provide critical information at the point of care.
If you’re in the market for a handheld computer, chances are you’re fazed by the multitude of available models, upgrades, and extras. Choosing a PDA is not that difficult, however, if you take the time to assess your needs and do a little homework. Start by answering these four questions:
1. Why do I need a PDA? Look at your work patterns and see how a PDA would fit in. Do you frequently look up DSM-IV criteria and other reference information? Are you constantly writing prescriptions, giving presentations, or assessing drug-drug interactions? Do you find yourself regularly checking your schedule?
Also try to envision:
- where you would carry the device
- where, when, and how you would charge it when needed
- what connections to computers for data exchange are available
- with whom you would share data
- and from whom you could get technical support.
You may have trouble thinking that far ahead, but doing so will help you narrow your PDA choices.
2. Which operating system should I use? A PDA operates on one of four main operating systems:
- Palm OS, the most popular world wide
- EPOC OS, which is more popular in Europe
- Pocket PC, which is rapidly gaining popularity
- and Linux OS, which recently entered the PDA market.
Choosing a PDA platform is much like deciding between Macintosh and Windows. The differences between PDAs based on Pocket PC or Palm OS have been diminishing in the last year. All PDAs have similar basic personal information manager functions, but available software, hardware features, and accessories set them apart. Pocket PC-based PDAs generally have much more memory and more diverse multimedia capabilities-but also lower battery life (1 day with average use) and compatibility with fewer software titles-than do Palm OS devices.
Because of their higher memory capacity, Pocket PC PDAs may generally be better suited to:
- large groups or organizations
- and users who rely heavily on multimedia, large data sets, or interface with Microsoft Office documents.
However, newer PDAs that are based on Palm OS 5 and employ the StrongARM processor (as do Pocket PC devices) offer greatly improved function in these areas. Compared with Pocket PC PDAs, Palm OS devices are much more intuitive and easier to use, offer longer battery life (1 week or more for average use), and are compatible with more medical software titles. More physicians use Palm OS PDAs because of their simplicity and reliability.
Consider either a Palm or Pocket PC PDA. EPOC PDAs are good devices, but Psion, a major manufacturer, has ceased development of EPOC devices to focus on specific markets. Linux PDAs are only recommended to users who are familiar with Linux or UNIX and are capable of writing their own software.
3. Where should I purchase my PDA? Visit any major computer, office supply, or electronics or chain retailer and check out the different models and manufacturers. Consider your priorities on features such as size, screen resolution, color, weight, memory, wireless capability, and accessory options. Consider purchasing there or online.
The level of support you need should dictate your point of purchase. Online retailers usually charge less for PDAs, but devices may be back-ordered and support often is offered only through the manufacturer. Beginners are probably wise to purchase locally and obtain support through the store.
4. How can I avoid purchasing a soon-to-be-obsolete model? Because PDA technology is improving so rapidly, new devices are frequently reaching the market. This can be frustrating to someone who has just purchased what he or she thought was the latest model.
If you are a beginner, plan to keep your PDA device for at least 1 year while you gradually learn to use it to its full potential. Consider spending about $200 for a device, then upgrade only when newer devices provide more features that you can use. Avid users may upgrade more frequently and spend $500 or more for a device.
Palm vs. Pocket PC: Finer points
Palm OS PDAs. If you are new to PDAs, start with a Palm OS-based PDA from Palm, Sony, or Handspring. The Sony models make more sense if you have or plan to purchase other Sony products (e.g., digital cameras, digital camcorders, computers) because the PDA’s external memory stick can be shared among the products.
Handspring offers models integrated with a cellular phone if you prefer a combined device. The Palm Tungsten T has built-in Bluetooth wireless mobile capability and offers portable keyboards that fold out to full size.
Pocket PC PDAs. Not long ago, Pocket PC PDAs were only compatible with software specific to the device’s processor. Today, the StrongARM processor is standard in any device running on Pocket PC 2002. Therefore, stick with Pocket PC 2002 devices only, as many of the earlier devices cannot be upgraded.
Because Pocket PC devices offer such a short battery life, consider a device with interchangeable lithium batteries or purchase a portable charger. If you choose a Pocket PC with integrated wireless connectivity, be aware that your battery life will be about 2 to 3 hours. Avoid the Jornada line of handhelds, as these will be phased out in the merger of Compaq and Hewlett Packard.
To learn more about PDAs
The Internet has a wealth of information on these devices. PDABuzz, Handango, and PDAGeek offer reviews, user opinions, and useful links. Two excellent magazines, Handheld Computing Magazine (www.hhcmag.com) and Pocket PC Magazine (www.pocketpcmag.com), are devoted to PDA/handheld computers. Manufacturers also post extensive information about their PDA devices on their Web sites (Box).
If you have any questions about PDAs or comments about Psyber Psychiatry, click here to contact Dr. Luo or send an e-mail to [email protected].
Palm OS
Manufacturer URL
Palm www.palm.com
Handspring www.handspring.com
HandEra www.handera.com
Sony http://www.sonystyle.com/
Acer global.acer.com/products/pda/index.htm
Pocket PC OS
Audiovox www.audiovox.com/pda
Casio www.casio.com
Toshiba pda.toshiba.com
HP www.compaq.com/products/handhelds/pocketpc/index.html
NEC www.neccomp.com/v2/products/MobilePro/P300/
Zayo (Asus) usa.asus.com/PDA/a600/overview.htm
ViewSonic www.viewsonic.com/products/pocket_pc_pocketpcv35.htm
URThere www.urthere.com
Related Resources
Carlson J. Palm organizers: visual quick start guide (2nd ed). Berkeley, CA: Peachpit Press, 2001.
Chan C, Luo J, Kennedy R. Concise guide to computers in clinical psychiatry (1st ed). Washington, DC: American Psychiatric Press, 2002.
Dyzsel B. Palm for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Underdahl B. Pocket PCs for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Personal digital assistants (PDAs) are becoming more commonplace in practice because they immediately provide critical information at the point of care.
If you’re in the market for a handheld computer, chances are you’re fazed by the multitude of available models, upgrades, and extras. Choosing a PDA is not that difficult, however, if you take the time to assess your needs and do a little homework. Start by answering these four questions:
1. Why do I need a PDA? Look at your work patterns and see how a PDA would fit in. Do you frequently look up DSM-IV criteria and other reference information? Are you constantly writing prescriptions, giving presentations, or assessing drug-drug interactions? Do you find yourself regularly checking your schedule?
Also try to envision:
- where you would carry the device
- where, when, and how you would charge it when needed
- what connections to computers for data exchange are available
- with whom you would share data
- and from whom you could get technical support.
You may have trouble thinking that far ahead, but doing so will help you narrow your PDA choices.
2. Which operating system should I use? A PDA operates on one of four main operating systems:
- Palm OS, the most popular world wide
- EPOC OS, which is more popular in Europe
- Pocket PC, which is rapidly gaining popularity
- and Linux OS, which recently entered the PDA market.
Choosing a PDA platform is much like deciding between Macintosh and Windows. The differences between PDAs based on Pocket PC or Palm OS have been diminishing in the last year. All PDAs have similar basic personal information manager functions, but available software, hardware features, and accessories set them apart. Pocket PC-based PDAs generally have much more memory and more diverse multimedia capabilities-but also lower battery life (1 day with average use) and compatibility with fewer software titles-than do Palm OS devices.
Because of their higher memory capacity, Pocket PC PDAs may generally be better suited to:
- large groups or organizations
- and users who rely heavily on multimedia, large data sets, or interface with Microsoft Office documents.
However, newer PDAs that are based on Palm OS 5 and employ the StrongARM processor (as do Pocket PC devices) offer greatly improved function in these areas. Compared with Pocket PC PDAs, Palm OS devices are much more intuitive and easier to use, offer longer battery life (1 week or more for average use), and are compatible with more medical software titles. More physicians use Palm OS PDAs because of their simplicity and reliability.
Consider either a Palm or Pocket PC PDA. EPOC PDAs are good devices, but Psion, a major manufacturer, has ceased development of EPOC devices to focus on specific markets. Linux PDAs are only recommended to users who are familiar with Linux or UNIX and are capable of writing their own software.
3. Where should I purchase my PDA? Visit any major computer, office supply, or electronics or chain retailer and check out the different models and manufacturers. Consider your priorities on features such as size, screen resolution, color, weight, memory, wireless capability, and accessory options. Consider purchasing there or online.
The level of support you need should dictate your point of purchase. Online retailers usually charge less for PDAs, but devices may be back-ordered and support often is offered only through the manufacturer. Beginners are probably wise to purchase locally and obtain support through the store.
4. How can I avoid purchasing a soon-to-be-obsolete model? Because PDA technology is improving so rapidly, new devices are frequently reaching the market. This can be frustrating to someone who has just purchased what he or she thought was the latest model.
If you are a beginner, plan to keep your PDA device for at least 1 year while you gradually learn to use it to its full potential. Consider spending about $200 for a device, then upgrade only when newer devices provide more features that you can use. Avid users may upgrade more frequently and spend $500 or more for a device.
Palm vs. Pocket PC: Finer points
Palm OS PDAs. If you are new to PDAs, start with a Palm OS-based PDA from Palm, Sony, or Handspring. The Sony models make more sense if you have or plan to purchase other Sony products (e.g., digital cameras, digital camcorders, computers) because the PDA’s external memory stick can be shared among the products.
Handspring offers models integrated with a cellular phone if you prefer a combined device. The Palm Tungsten T has built-in Bluetooth wireless mobile capability and offers portable keyboards that fold out to full size.
Pocket PC PDAs. Not long ago, Pocket PC PDAs were only compatible with software specific to the device’s processor. Today, the StrongARM processor is standard in any device running on Pocket PC 2002. Therefore, stick with Pocket PC 2002 devices only, as many of the earlier devices cannot be upgraded.
Because Pocket PC devices offer such a short battery life, consider a device with interchangeable lithium batteries or purchase a portable charger. If you choose a Pocket PC with integrated wireless connectivity, be aware that your battery life will be about 2 to 3 hours. Avoid the Jornada line of handhelds, as these will be phased out in the merger of Compaq and Hewlett Packard.
To learn more about PDAs
The Internet has a wealth of information on these devices. PDABuzz, Handango, and PDAGeek offer reviews, user opinions, and useful links. Two excellent magazines, Handheld Computing Magazine (www.hhcmag.com) and Pocket PC Magazine (www.pocketpcmag.com), are devoted to PDA/handheld computers. Manufacturers also post extensive information about their PDA devices on their Web sites (Box).
If you have any questions about PDAs or comments about Psyber Psychiatry, click here to contact Dr. Luo or send an e-mail to [email protected].
Palm OS
Manufacturer URL
Palm www.palm.com
Handspring www.handspring.com
HandEra www.handera.com
Sony http://www.sonystyle.com/
Acer global.acer.com/products/pda/index.htm
Pocket PC OS
Audiovox www.audiovox.com/pda
Casio www.casio.com
Toshiba pda.toshiba.com
HP www.compaq.com/products/handhelds/pocketpc/index.html
NEC www.neccomp.com/v2/products/MobilePro/P300/
Zayo (Asus) usa.asus.com/PDA/a600/overview.htm
ViewSonic www.viewsonic.com/products/pocket_pc_pocketpcv35.htm
URThere www.urthere.com
Related Resources
Carlson J. Palm organizers: visual quick start guide (2nd ed). Berkeley, CA: Peachpit Press, 2001.
Chan C, Luo J, Kennedy R. Concise guide to computers in clinical psychiatry (1st ed). Washington, DC: American Psychiatric Press, 2002.
Dyzsel B. Palm for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Underdahl B. Pocket PCs for dummies (2nd ed). Hoboken, NJ: Wiley Publishing, 2002.
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Rediscovering the art of lithium therapy
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
Rediscovering the art of lithium therapy
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
As a mood stabilizer for patients with bipolar disorder, lithium was the darling of U.S. psychiatry from the 1970s to well into the 1990s. It then began an ill-deserved, gradual fall from grace and today could be considered a pharmaceutical endangered species. But why?
Did lithium lose effectiveness? Is it too toxic? Is its side effect burden too heavy? Does it interact adversely with too many medicines? Is it too cumbersome to use? Was it just a fad whose time came and went—a psychiatric pet rock? Did it fall prey to the marketing might behind patent-protected drugs? Was it replaced by more effective and safer drugs?
You are partially correct if you checked “all of the above,” because all contain a kernel of truth. At the same time, each is an exaggeration that does grave injustice to a remarkable medication. In addition, psychiatry appears to pay only lip service to convincing evidence that lithium is the only mood stabilizer that reduces the risk of suicide during long-term treatment.1
Some psychiatrists rationalize that “lithium is too difficult to use, so I never prescribe it.”2,3 My response is simply, “try it, and I think you’ll like it.” Measuring serum lithium concentrations is simple, accurate, and inexpensive. And we know quite a bit about how lithium dosage and blood level relate to response and tolerability.
Where does lithium stand?
Lithium is the first solid element in the periodic table (atomic number 3, atomic weight 6.94) (Box 1). As a treatment for bipolar disorder, lithium’s rise to prominence in the United States was far from rapid. Its antimanic properties were described by John Cade in Australia in 1949 in an open-label case series, but it was not FDA-approved for 20 years—for acute manic episodes in 1970 and for maintenance therapy “in those manic depressive patients with a history of mania” in 1974. Today, lithium shares FDA-approved manic episode billing with chlorpromazine (1973), divalproex (1995), and olanzapine (2000), but it remains the only FDA-approved drug for maintenance (although the FDA is considering a bipolar depression maintenance indication for lamotrigine).
Lithium has no meaningful protein binding and no metabolites, being excreted almost entirely by the kidneys. Its elimination half-life of 18 to 24 hours may be longer in the elderly and shorter in youth because of age-dependent variations in glomerular filtration rate. For unclear reasons, renal lithium clearance appears to be more rapid in obese persons.
Lithium preparations available in the United States include standard-release (150, 300, 600 mg), slow-release (Lithobid and generic 300 mg), and controlled-release (Eskalith CR 450 mg) forms of lithium carbonate and a lithium citrate liquid. Lithium carbonate, 300 mg, and lithium citrate, 5 cc, each contain about 8 mmols of lithium. Lithium and lithium carbonate are not the same—there are 56.36 mg of lithium in 300 mg of lithium carbonate. The correct formula for lithium carbonate is Li2CO3, not LiCO3 as is commonly and erroneously written.
With the standard-release preparation, peak serum levels are reached in about 1 1/2 hours and with the slow- and controlled-release forms in about 4 to 4 1/2 hours. At times, the slower-release forms may be better tolerated, but they are also a bit more costly (although all forms of lithium are inexpensive, compared with other mood stabilizers).
If you examine lithium’s status relative to other bipolar medications, you’ll find some inconsistencies. For example:
- Clinical practice guidelines from the Department of Veterans Affairs (January 1999) recommended lithium as the first-line agent for acute and prophylactic treatment of manic and mixed states, bipolar depression, and rapid cycling.4
- The Expert Consensus Guidelines (April 2000) gave at least equal billing—if not preferred status—to divalproex for those indications.5
- The American Psychiatric Association’s (APA) revised guidelines (April 2002) gave the nod to lithium for classic elated mania and bipolar depression but to divalproex for mixed mania and rapid cycling.6 Divalproex was rated comparable to lithium for maintenance therapy, despite the lack of convincing data.
- The European perspective (January 2002) is most similar to that of the Department of Veterans Affairs, favoring lithium for acute mania, bipolar depression, and long-term treatment.7
There is no clear winner (or loser) in the battle for bipolar marketplace supremacy. The belief that one drug does everything is a fantasy for all but a small minority of patients with bipolar disorder. Polypharmacy is the rule, and rational polypharmacy the goal. To exclude lithium from the arsenal of bipolar drugs would be folly, yet lithium prescribing seems to have become a vanishing art. One of my psychopharmacologist colleagues recently expressed bewilderment at the number of “treatment-resistant” bipolar patients referred to him who had never been treated with lithium.
Diagnosis matters
Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning. Its potential benefits, however, clearly extend to all other aspects of bipolar disorder, to augmentation for treatment-resistant major depressive disorder, to schizoaffective disorder, and—at times—to aggressive states. As the bipolar spectrum expands, it is hardly surprising that the effectiveness of lithium (or any other drug) lessens as we approach the periphery of the spectrum.
Blood levels and dosing
Recommended lithium serum concentrations are given as ranges, realizing that individual variability makes exact numbers impractical. Package inserts for lithium products list serum concentrations between 1.0 and 1.5 mEq/L for acute mania and 0.6 and 1.2 mEq/L for maintenance therapy. The APA’s revised guidelines are a bit more conservative, recommending 0.5 to 1.2 mEq/L for acute mania and waffling somewhat on maintenance.4 Many patients on maintenance therapy do well at levels between 0.6 and 0.8 mEq/L, and some prosper at even lower levels.
To avoid obtaining a misleading blood level:
- Samples should be drawn in the morning as close as possible to 12 hours after the last dose.
- Steady state conditions should exist, usually meaning 4 or 5 days on the same dosage without any missed or extra doses (Box 2).
Start treatment using divided dosages, but—following stabilization—once-daily dosing is possible for many patients. If lithium is taken as a single daily dose, 12-hour blood levels will be somewhat higher than with multiple daily dosing. Single and multiple daily dosing are similarly effective, but once-daily dosing may have a compliance and tolerability edge in some patients.
Considering individual patient variability, a lithium carbonate dosage of 1,200 to 1,800 mg/d is likely to be therapeutic for mania and 900 to 1,200 mg/d for maintenance in otherwise healthy, nongeriatric adults.
Starting and maintaining lithium
Medical history. Assuming that lithium theapy is indicated, obtain a detailed medical history. Focus on findings that increase the risk of lithium toxicity, such as renal impairment, drug interactions, and unstable fluid-electrolyte balance.
Although lithium is not contraindicated in patients with renal disease, using an alternate drug is probably preferable. On the other hand, because lithium does not adversely affect the liver or pancreas, it may be preferred to some other mood stabilizers if these organs are diseased.
A thorough diet and drug history is also important. Because low-sodium diets reduce renal lithium clearance, lower doses may be required to reach a given serum concentration. Some drugs alter lithium excretion and can increase or decrease blood levels (see “Drug combinations,”).
Advise women of childbearing age about lithium’s teratogenic potential (which is considerably less than that of carbamazepine or valproate). The risk of cardiovascular malformation of the fetus has been estimated at 1/1,000 to 1/2,000 births among women who took lithium during the first trimester of pregnancy.8
- Draw samples in the morning, as close as possible to 12 hours after the last dose.
- Measure serum levels at steady state, at least 4 or 5 days on the same dosage without any missed or extra doses.
Baseline lab tests. Assessing renal function is essential. A serum creatinine level will usually suffice, unless a history of renal disease suggests the need for a more extensive evaluation, such as creatinine clearance, renal ultrasound, or nephrology consultation.
A urinalysis is often part of the package. Because thyroid dysfunction can alter mood and lithium can disrupt thyroid function, baseline TSH and T4 tests are recommended. CBC is optional (lithium can cause leukocytosis). The medical history should determine whether additional blood work is necessary. An ECG is sometimes advised in older patients, especially if the history suggests cardiovascular disease. Finally, don’t forget a pregnancy test in women of childbearing potential (Box 3).
Monitoring. Early in the course of therapy, lithium blood levels are usually obtained at 5- to 7-day intervals until the patient is stabilized. After that, assuming all is well, routine monitoring can occur every 3, 4, or even 6 months, depending on the individual’s reliability and stability. Because ongoing assessment of renal and thyroid function is also important, it makes sense to obtain:
- a serum creatinine measurement linked to each lithium level
- and a serum TSH yearly or at the slightest indication of thyroid dysfunction, such as fatigue, weight gain, cognitive impairment, cold intolerance, or depression.
Stopping lithium. Lithium can be discontinued abruptly without side effects if it is ineffective or not tolerated. Stopping lithium after successful long-term use is another story. There is a high likelihood of illness recurrence and a small but real possibility that lithium will be ineffective when restarted. Also, abrupt or rapid discontinuation (within 1 to 14 days) is believed to increase the likelihood of earlier recurrence, compared with more gradual discontinuation.9
Side effects and toxicity
One reason for lithium’s slide in popularity is its perceived side-effect profile. Toxic amounts can be lethal, and therapeutic amounts can be bothersome. Yet concerns are often exaggerated because of lack of familiarity with the drug.10,11
Intoxication. Lithium does have a narrow therapeutic index, with toxicity related to serum concentration and duration of exposure. Acute overdoses, while not benign, are often better tolerated than gradual, more tissue-saturating exposures. Idiosyncratic factors are also involved, as evidenced by documented toxicity at “therapeutic” levels and tolerability despite very high levels.
Early warnings of impending toxicity include:
- neurologic findings such as dysarthria, new or worsening tremor, and ataxia
- gastrointestinal symptoms such as anorexia, nausea, vomiting, and diarrhea.
Severe toxicity can be fatal or cause permanent neurologic (often cerebellar) damage. Causes of intoxication range from deliberate overdose to renal impairment, low-sodium diets, drug interactions, and dehydration. At particular risk are patients with lithium-induced polyuria whose access to fluid replacement is compromised.
Treatment involves reducing absorption, increasing excretion, and restoring fluid-electrolyte balance. Severe intoxication, especially if renal function is impaired, is best treated with hemodialysis.
| Test | Indication |
|---|---|
| Serum creatinine, urinalysis | To screen for renal function |
| TSH and T4 | To establish baseline thyroid function |
| CBC (optional) | If indicated by patient’s overall medical condition or because some doctors prefer to do more general screening |
| ECG (optional) | For patients with risk factors for heart disease |
| Pregnancy test | For at-risk women because of lithium’s teratogenic potential |
Neurologic. Mild neurologic complaints such as memory impairment, slow reaction time, lack of spontaneity, and lost creativity have been ascribed to lithium and may lead to noncompliance. Under such circumstances, other diagnostic considerations include breakthrough depression, hypothyroidism, other illness, hypercalcemia, other medications, and absence of hypomania.
Like valproate, lithium can cause a benign postural tremor that is usually tolerable and often transient. Should the tremor be problematic, treatment considerations include dosage reduction, switching to a slow-release preparation, reducing caffeine intake, avoiding other tremor-causing drugs such as theophylline or stimulants, and treating associated anxiety. If an anti-tremor drug is needed, a beta-blocker such as propranolol is used most commonly; other options to consider are primidone and gabapentin. Don’t forget that a worsening tremor may indicate impending toxicity.
Very rarely, lithium has been associated with pseudotumor cerebri (benign intracranial hypertension), peripheral neuropathy, and a myasthenia gravis-like syndrome.
Cardiovascular. Like many drugs, lithium can cause benign ST-T wave changes on ECG.
More serious, but fortunately quite uncommon, is lithium-induced sinus node dysfunction manifesting as a variety of bradyarrhythmias and, at times, syncopal episodes. Since normal aging is associated with a gradual loss of sinus node pacemaker cells, the elderly may be especially sensitive to this problem. Unless a pacemaker is implanted, sinus node dysfunction usually requires lithium discontinuation.
Endocrine. The association between lithium and goiter and hypothyroidism is well-recognized, with elevated risk in women and in patients with pre-existing thyroid disease. Both clinical and symptomatic subclinical hypothyroidism will improve with supplemental thyroid hormone. Less well appreciated are reports of hyperthyroidism occurring during lithium therapy or shortly after its discontinuation. Because subclinical hyperthyroidism may not be benign, careful attention must be paid to maintaining thyroid function well within the normal range.
Reports continue to accrue of lithium-related hypercalcemia and increased parathyroid hormone levels, with an occasional patient developing parathyroid hyperplasia or adenoma requiring surgical intervention.12 No specific guidelines have been established for monitoring serum calcium, but some authors have recommended periodic testing.
Weight. At least one-third of patients on lithium gain weight for a variety of reasons, such as altered lipid and carbohydrate metabolism, use of high-calorie fluids to combat polydipsia and polyuria, hypothyroidism, and the use of other drugs associated with weight gain. If weight gain occurs, recognize it early (weigh your patients) and institute appropriate dietary and exercise measures.
Hematologic. A mild, benign leukocytosis is seen sometimes during treatment with lithium. This effect has been harnessed to treat some neutropenic conditions. Lithium does not increase the risk of blood dyscrasias.
Dermatologic. Acne, psoriasis, and follicular keratosis may first appear or worsen during lithium therapy. Occasionally, otherwise successful lithium therapy has been rendered impossible by a dramatic dermatologic flare-up. Hair loss has also been associated with lithium use for unclear reasons, although hypothyroidism is occasionally a factor.
Renal. Impaired urinary concentrating ability and polyuria are common adverse effects. Both may be reversed with timely treatment discontinuation, but they may persist even after discontinuation in patients on long-term lithium treatment.12
Polyuria is largely nephrogenic in origin and, at times, can be voluminous, cause great inconvenience, and pose a risk of dehydration and lithium intoxication. Patients sometimes believe that thirst drives the polyuria and attempt to deal with it by restricting fluid intake, which can be quite dangerous. More appropriate interventions include dosage reduction (if possible) and the use of a thiazide and/or potassium-sparing diuretic. If diuretics are used, serum lithium concentrations may rise. Debate remains as to whether slow-or controlled-release preparations or single daily dosing are “kinder to the kidney.”
- Lithium is most effective in patients with euphoric mania, full remission between episodes, and normal interepisode functioning.
- Lithium is the only mood stabilizer that has been shown to reduce the risk of suicide during long-term treatment.
- Renal impairment, drug interactions, and unstable fluid-electrolyte balance increase the risk of lithium toxicity.
- Lithium does not adversely affect the liver or pancreas and may be the preferred mood stabilizer if these organs are diseased.
- Lithium has teratogenic potential but less than that of carbamazepine or valproate.
- Because lithium can disrupt thyroid function, baseline and ongoing thyroid function tests are recommended.
In recent years, there has been a disturbing increase in reports of elevated serum creatinine and reduced creatinine clearance associated with long-term lithium use.13 Because renal impairment has many causes, evaluation by a nephrologist is strongly advised. Then if the finger of causation points strongly at lithium, a careful risk/benefit analysis is in order. Even if lithium is discontinued—and especially if it is continued—regular renal function assessment is essential.
Rarely, lithium can cause a nephrotic syndrome (proteinuria, edema, decreased serum albumin, and increased serum lipids) that tends to be reversible with drug discontinuation.
Drug combinations
First the good news. Lithium tends to combine well with all the anticonvulsant mood stabilizers, making it the favored drug for combination therapies. Lithium/antidepressant combinations can be useful for treatment-resistant depression, although serotonin syndrome occasionally has been reported when lithium is combined with selective serotonin reuptake inhibitors.10,11 Using lithium with atypical antipsychotics is common, often effective, and usually well-tolerated.
Drug-drug interactions. Some nonpsychiatric drugs are associated with reduced renal lithium clearance and potential lithium toxicity. Because nonpsychiatrists usually prescribe these drugs, encourage patients taking lithium to ask their doctors about the possibility of interactions whenever a new drug is prescribed. Pharmacists can be particularly helpful in avoiding drug-drug interactions.
In patients taking diuretics, serum lithium concentrations are definitely increased by thiazides, possibly by potassium-sparing types, and occasionally by loop types. Osmotic and xanthine diuretics do just the opposite. Because diuretics are often used in medically unstable patients, assume that all can disrupt lithium balance.
Most nonsteroidal anti-inflammatory drugs can increase serum lithium levels, although dose and treatment duration are important variables. Aspirin and acetaminophen should not cause problems. The effect of COX-2 inhibitors on lithium levels has not been studied adequately, so these drugs should remain under suspicion.14
Lithium toxicity has been reported with angiotensin-converting enzyme (ACE) inhibitors, and their package inserts caution about this possibility. More recently, a few cases of lithium toxicity have been reported in patients taking angiotensin II receptor type-1 (AT-1) antagonists (e.g., candesartan, losartan, valsartan).15
Other, less well-substantiated pharmacokinetic and pharmacodynamic interactions that have been reported with lithium and other drugs can be researched, by using a computer-based drug interaction program or consulting with a drug information center.
Patient and clinician education
Both patients and clinicians have an obligation to ensure that lithium (or any other drug) is used safely and effectively (Box 4). Excellent sources of continuing education are listed below in “Related resources.” Rather than fall prey to the illusion that lithium therapy is a “vanishing art,” it would be better for clinicians to heed these words from the APA’s 2002 practice guidelines for bipolar disorder:
“No other treatment has performed as well as lithium in as many aspects of long-term care of bipolar disorder patients, and despite some risks and limitations lithium remains the standard against which all proposed alternatives are compared.”6
- Depression and Bipolar Support Alliance. www.dbsalliance.org
- Lithium Information Center. www.miminc.org
Drug brand names
- Chlorpromazine • Thorazine
- Divalproex • Depakote
- Gabapentin • Neurontin
- Lamotrigine • Lamictal
- Olanzapine • Zyprexa
- Primidone • Mysoline
- Propranolol • Inderal
Disclosure
Dr. Jefferson receives grant/research support from Abbott Laboratories, Bristol-Myers Squibb Co., Forest Laboratories Inc., GlaxoSmithKline, Eli Lilly and Co., Novartis Pharmaceuticals Corp., Organon, Janssen Pharmaceutica, Pfizer Inc., Solvay, and Wyeth Pharmaceuticals. He also serves as a consultant to GlaxoSmithKline, Novartis Pharmaceuticals Corp., Solvay, and UCB Pharma.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
1. Tondo L, Hennen J, Baldessarini RJ, et al. Lower suicide risk with long-term lithium treatment in major affective illness: a meta-analysis. Acta Psychiatr Scand 2001;104:163-72.
2. Baldessarini RJ, Tondo L, Hennen J, et al. Is lithium still worth using? An update of selected recent research. Harvard Rev Psychiatry 2002;10(2):59-75.
3. Sadock BJ. Sadock VA (eds). Kaplan & Sadock’s comprehensive textbook of psychiatry. Philadelphia: Lippincott Williams & Wilkins, 2000;2377-90.
4. Bauer MS, Callahan AM, Jampala C, et al. Clinical practice guidelines for bipolar disorder from the Department of Veterans Affairs. J Clin Psychiatry 1999;60(1):9-21.
5. Sachs GS, Printz DJ, Kahn DA, et al. Medication treatment of bipolar disorder. Postgrad Med Special Report 2000;Apr:1-104.
6. American Psychiatric Association. Practice guidelines for the treatment of patients with bipolar disorder (revision). Am J Psychiatry 2002;159:1.-
7. Müller-Oerlinghausen B, Berghöfer A, Bauer M. Bipolar disorder. Lancet 2002;356:241-7.
8. Cohen LS, Rosenbaum JP. Psychotropic drug use during pregnancy: weighing the risks. J Clin Psychiatry 1998;59(suppl 2):18-28.
9. Baldessarini RJ, Tondo L. Recurrence risk in bipolar manic-depressive disorders after discontinuing lithium maintenance treatment: an overview. Clin Drug Invest 1998;15(4):337-51.
10. Jefferson JW. Lithium. In: Dukes MNG, Aronson JK (eds). Meyler’s side effects of drugs (14th ed). Amsterdam: Elsevier Science BV, 2001;86-94.
11. Jefferson JW. Lithium. In: Aronson JK (ed). Side effects of drugs, annual 24. Amsterdam: Elsevier Science BV, 2001;22-31.
12. Abdull H, Bliss R, Guinea AE, et al. Pathology and outcome of surgical treatment for lithium-associated hyperparathyroidism. Br J Surg 1999;86:91-3.
13. Gitlin M. Lithium and the kidney. An updated review. Drug Safety 1999;20(3):231-43.
14. Lundmark J, Gunnarsson T, Bengtsson F. A possible interaction between lithium and rofecoxib (letter to the editor). Br J Clin Pharmacol 2002;53(4):403-4.
15. Zwanzger P, Marcuse A, Boerner RJ, et al. Lithium intoxication after administration of AT1 blockers. J Clin Psychiatry 2001;62(3):208-9.
Teachable moments: Turning alcohol and drug emergencies into catalysts for change
Mrs. R, age 43, is agitated and confused, and her husband has brought her to the hospital’s emergency department. He reports that she has a history of denying alcohol abuse and told him during an argument yesterday that she could stop drinking any time she wanted to.
You are the psychiatrist on call. As the emergency medical team treats the apparent withdrawal episode, you tell Mrs. R’s husband: “We’ll take good care of your wife because alcohol withdrawal is dangerous and painful. But after detoxification, it’s important to prevent her from getting sick again. She needs to enter a rehabilitation program, and then outpatient treatment. When she comes around, maybe you could remind her about how much pain she was in and bring her to the rehab center yourself…”
Addicts face potentially life-threatening consequences from their behavior, which—when handled skillfully in the emergency room—can start them on the road to recovery. Some say the addict must “hit bottom” before making the changes necessary for a sober life. You can help the addict define his or her bottom as an unpleasant trip to the hospital—instead of death or loss of a job or spouse—by realistically assessing the physical consequences of continued drug or alcohol use (Table 1).
Emergencies related to alcohol or drug use accounted for 601,563 visits to U.S. emergency departments in 2000, according to the government-sponsored Drug Abuse Warning Network (DAWN).2 Alcohol in combination with any illegal or illicit drug accounted for 34% of emergency visits, cocaine for 29%, and heroin for 16%.
Mortality rates vary by region. In Los Angeles, for instance, heroin and cocaine each caused approximately the same number of deaths when compared with alcohol in combination (Figure).3 Most deaths (73%) were considered accidental/unexpected, with 19% coded as suicide. New York City showed similar percentages of deaths called accidental/unexpected, but heroin as the cause of death ran a distant fourth to cocaine alone, narcotic analgesics alone, and alcohol in combination.2
Addiction crises bring more than a half-million Americans to hospital emergency rooms each year (Box 1,Figure).2,3 This article describes teachable moments—suicide attempts, accidental overdose, intoxication, and withdrawal—that you can use to bundle acute treatment with referral for addiction treatment.
Suicide
Suicide is the addict’s most immediate life-threatening emergency. Psychiatric and addictive disorders often coexist,4 but some substances can trigger suicidal behavior even in the absence of another diagnosable psychiatric disorder. The addicted person who jumps off a roof, believing he can fly, may think perfectly clearly when not using crack cocaine.
Addiction to any substance greatly increases the risk for suicide. An alcohol-dependent person is 32 times more likely to commit suicide than the nonaddicted individual.5 And the suicidal addict often has the means to end his life when he feels most suicidal.
Figure DRUG-RELATED DEATHS IN LOS ANGELES, 20022
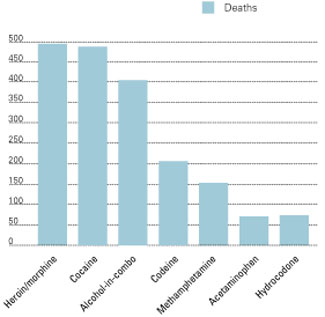
Diagnosing and treating suicidality require a high degree of vigilance for subtle clues of suicidal behavior. Because suicide risk has no pathognomonic signs, clinical judgment is required. Though addiction itself can be viewed as a slow form of suicide,6 signs that suggest an immediate threat to life include:
- the addict’s assertion that he intends to kill himself
- serious comorbid mental illness (psychosis, depression)7
- prior suicide attempts
- hopelessness.8
Some addicts feign suicidal thoughts or use them as a cry for help. Any mention or hint regarding suicide marks a severely disturbed patient who needs a complete psychiatric evaluation. This includes a formal mental status examination and exploring whether the patient has access to lethal means.
We cannot consistently predict our patients’ behavior, but a careful examination often reveals the seriousness of a suicidal threat, method, and intention, as well as support systems for keeping the patient safe. Consulting with a colleague can offer a “fresh look,” allowing two clinicians to balance the need for treatment against concerns such as bed availability and possible malingering.
Table 1
EMERGENCY AND LONG-TERM MEDICAL CONSEQUENCES OF ADDICTION
| Addictive substance | Intoxication symptoms | Withdrawal symptoms | Longer-term problems |
|---|---|---|---|
| Alcohol | Slowed respiration, impaired thinking and coordination, coma, death | Seizures, death | Dementia, liver damage |
| Barbiturates | Slowed respiration, impaired thinking and coordination, coma, death | Seizures | Rebound pain, hepatotoxicity |
| Benzodiazepines | Slowed respiration, impaired thinking and coordination | Seizures | |
| Hallucinogens | Paranoia, impaired thinking and coordination | Amotivational syndrome; possession is grounds for arrest | |
| MDMA(‘ecstasy’) | Impaired thinking and coordination, stroke, hyperthymia, dehydration, death | Cognitive impairment; possession is grounds for arrest | |
| Nicotine | Tachycardia, arrhythmia | Lung cancer, chronic-obstructive pulmonary disease | |
| Opiates | Slowed respiration, impaired thinking and coordination, coma, death | Skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Phencyclidine (PCP, ‘angel dust’) | Impaired thinking and coordination, violent behavior | Possession is grounds for arrest | |
| Stimulants | Impaired thinking and coordination, myocardial infarction, stroke | Nasal damage (if snorted); skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Inhalants | Impaired thinking and coordination, headache, coma | Neurologic damage |
Suicidal thoughts are unassailable grounds for comprehensive evaluation and treatment—regardless of the suicide evaluation’s outcome. The addict who even hints at suicide should undergo a thorough medical and psychiatric evaluation and then engage in whatever treatment is indicated.
Emphasize the seriousness of suicidal thoughts to the patient, his family, third-party payers, and whomever else has influence in bringing the patient to treatment. Suicidal behaviors or intentions remain one of the few legal justifications for involuntary hospitalization.
Accidental overdose
An accidental overdose provides another teachable moment to convince the addict to enter treatment. Patients who try to make a statement by overdosing on a substance they consider benign, such as oxycodone with acetaminophen, can inadvertently kill or badly injure themselves. Conversely, patients who clearly intend to harm themselves may misconstrue a substance’s lethality and ingest a large amount of a relatively nonlethal substance such as clonazepam. Either case:
- is a true psychiatric emergency
- bodes poorly for the patient’s future
- provides a strong rationale for addiction treatment.
Whether the means or the intent were deadly or benign, the overdose can be used as a convincing argument for treatment.
Intoxication
Intoxication with any addictive substance impairs judgment and increases the danger of injury. Specific medical dangers include alcohol’s powerful CNS depression in the nontolerant individual and the possibility for heart attack and stroke in the cocaine-intoxicated patient.
Attempts to convince an intoxicated person of the need for addiction treatment are usually futile. But the acute treatment represents a golden opportunity to reach out to friends and family members, who often escort the intoxicated addict to the emergency room. A medical record documenting the patient’s impaired behavior serves as evidence for (later) convincing the addict to go into treatment or for legal coercion of that treatment.
Table 2
MANAGING SYMPTOMS OF ALCOHOL WITHDRAWAL AND DELIRIUM TREMENS
| Alcohol withdrawal | Delirium tremens |
|---|---|
| Begins 4 hours to 2 days after cessation of alcohol or precipitous drop in blood alcohol level | Begins 1 to 2 days after cessation of alcohol or precipitous drop in blood alcohol level |
| Symptoms | Symptoms |
| Anxiety Agitation Tremor Autonomic instability Insomnia Confusion | Agitation Severe autonomic instability Seizure Severe confusion Hallucinations |
| Treatment Treatment of co-occurring medical illness Parenteral thiamine Tapering doses of CNS depressants, most often benzodiazepines | |
Withdrawal
Withdrawal, like intoxication, presents emergency conditions specific to the abused substance. Unlike the intoxicated patient, however, a patient experiencing the unpleasant symptoms of withdrawal may understand the need for addiction treatment. Because alcohol withdrawal often requires sedative/hypnotic treatment, the wise clinician can design a treatment plan that combines the anti-withdrawal medication with:
- attending Alcoholics Anonymous meetings
- taking disulfiram 12 hours after the last alcohol use and then daily
- and participation in relapse prevention psychotherapy.
Emergency treatments
Psychiatrists often have close contact with addicted patients in the hospital, clinic, or emergency department and therefore need to be familiar with basic techniques for managing addiction emergencies. Although addiction-trained psychiatrists manage emergencies at many institutions, general psychiatrists who have learned the following guidelines can form quick and solid therapeutic alliances with their addicted patients in the emergency department.
Alcohol
People live dangerously when intoxicated; about 40% of fatal U.S. car accidents involve a drunken driver.9 Alcohol also can incite physical violence and self-damaging sexual behavior and cause respiratory depression and death.
Acute effects of alcohol intoxication must be treated while guarding against potentially lethal withdrawal. Dangerous intoxication states with respiratory compromise may require aggressive supportive care, including intubation and mechanical ventilation. For agitated, intoxicated persons who represent a threat to themselves or others, chemical sedation with benzodiazepines—as opposed to physical restraint—is the preferred treatment.
Alcohol withdrawal requires immediate, definitive treatment (Table 2). Although mild withdrawal is common among alcoholics who cut back on or abruptly stop drinking, it can devolve quickly into delirium tremens (DTs). Serious medical problems—including severe autonomic instability and seizures—occur with DTs, which are associated with mortality rates of 5 to 15%.10 The adroit emergency department clinician can use the alcohol withdrawal/delirium episode to encourage the patient to begin addiction treatment (Box 2).11
Cocaine
Stimulants—most commonly cocaine and smoked methamphetamine—can cause myocardial infarction, cardiac arrhythmia, cerebral hemorrhage, hyperpyrexia, and status epilepticus.12 These emergencies occurring in a young person indicate the need to screen for cocaine use. Because no antidote exists for stimulant intoxication, we can only deliver supportive care while remaining vigilant for other sequelae of stimulant use, such as agitation and hypertension.13
Opiates
Overdoses leading to coma and death are the most devastating physical consequence of opiate abuse. Contrary to popular belief, orally ingested and inhaled opiates can depress respiration enough to cause death, just as injected opiates can. Because even appropriately prescribed opioid medications can lead to overdose or addiction, emergency treaters should be prepared to refer patients for pain management.
High-potency heroin often causes overdose in the novice user or in the addict who is surprised by a sudden increase in the heroin’s purity. Adulterants used by dealers to “cut” heroin also can cause illness and death. Quinine, for instance, can cause cardiac arrhythmias. Contaminants such as fentanyl and cholinergic agents such as scopolamine added to enhance the “high” associated with heroin can increase the risk of toxicity or death.
Opioid overdose is characterized by cyanosis and pulmonary edema: slowed breathing, altered mental status, blue lips and fingernail beds, pinpoint pupils, hypothermia, and gasping respirations. In addition to respiratory and cardiac support, treatment with the narcotic antagonist naloxone immediately reverses opioid overdose.
To what level of care should you refer the addicted patient from the emergency department—an inpatient medical unit, psychiatric unit/detoxification facility, residential treatment, partial hospitalization, or other model of care? The American Society of Addiction Medicine (ASAM) manual lists disposition recommendations to match individual patients’ clinical criteria. The criteria and levels are listed here as reminders of the issues involved in referring the addicted patient.
ASAM patient criteria
- Alcohol intoxication and/or withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Relapse, continued use, or continued problem potential
- Recovery environment
ASAM levels of care
- Early intervention
- Opioid maintenance therapy
- Outpatient treatment
- Intensive outpatient treatment
- Partial hospitalization
- Clinically managed low-intensity residential services
- Clinically managed high-intensity residential services
- Medically monitored intensive inpatient treatment
- Medically managed intensive inpatient treatment
Source: Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001:27-33.
Ecstasy
The drug 3,4-methylenedioxymethamphetamine (MDMA)—also known as Ecstasy, X, and XTC3 —provokes release of dopamine and serotonin into the synapse, causing a sense of blissful open-mindedness, closeness to others, and the ability to “break down (mental) barriers.”14 In the context of “rave” dance parties, MDMA also causes dehydration and hyperthermia, which can lead to rhabdomyolysis, kidney failure, and death.
Life-threatening consequences generally occur only when adequate water is unavailable to a group of intoxicated, dancing teenagers.15 The more common emergency presentations include sudden hypertension, tachycardia, vomiting, depersonalization, panic attacks, and psychosis.16
Immediate treatment includes restoration of normal fluid levels and body temperature, plus reassurance for the non-life-threatening, more common, presentations.
Phencyclidine
Phencyclidine (PCP) and its analogue ketamine—originally developed as anesthetic agents—are no longer used therapeutically because they can cause dissociation, anxiety, and even psychosis. Panic can change to hyperactive behavior, aggressiveness, and violent acts, so the first treatment goal must be to secure the safety of the intoxicated person and others. Chemical restraints such as benzodiazepines are preferred to physical restraints, although some situations may require physical restraint, at least initially.17
PCP affects memory, and often the user is unaware of the agent’s consequences unless he hears descriptions of his behavior from family and friends unfortunate enough to witness the intoxicated state. Coaching by emergency personnel can help the family confront the user with evidence that he needs treatment.
Barbiturates
Physicians prescribe barbiturates such as pentobarbital, phenobarbital, and secobarbital for pain, insomnia, alcohol withdrawal, and anxiety states. Although sometimes useful for acute pain, these drugs can also cause physical dependence, intoxication in overdose, withdrawal seizures, and rebound pain.18
The withdrawal associated with barbiturates—as with withdrawal from other CNS depressants such as alcohol and benzodiazepines—consists of autonomic hyperactivity, confusion, and occasionally seizures.
Overdose, often in combination with alcohol, accounts for most emergency presentations of barbiturate addiction. Supportive treatment—from reassurance and observation to airway support and mechanical ventilation—is required. Since obtundation and coma commonly occur with alcohol/barbiturate combinations, treatment includes monitoring for alcohol intoxication or withdrawal. No antidote exists for barbiturate intoxication.
Alternate medications. If the patient has become addicted to barbiturates prescribed for one of the common indications such as migraine headache, the emergency treater can promote use of a more effective treatment by acknowledging the need to control the headache pain. In managing this pain, the emergency worker can arrange referral:
- to an addiction specialist for treatment of the (now addictive) barbiturate use
- and to a neurologist who can evaluate the patient and prescribe one of many highly effective, nonaddicting headache remedies.
By taking the addiction and the pain seriously, the treater forms an alliance with the patient against the unhealthy consequences of both migraine headaches and addiction.
Benzodiazepines
Often prescribed for anxiety and insomnia, benzodiazepines cause emergency syndromes directly related to their potency, serum half-lives, and lipophilicity. For instance, alprazolam—which is potent, short-acting,19 and highly lipophilic—causes a severe withdrawal syndrome when high doses are stopped abruptly. This withdrawal state includes anxiety, agitation, and autonomic instability and can progress to frank seizures.
Withdrawal is treated by tapering the benzodiazepine dosage or substituting another benzodiazepine such as clonazepam. Benzodiazepine intoxication usually occurs only with large overdoses, although intoxication can last for days in a patient with hepatic disease. Lorazepam and oxazepam are not metabolized by the liver and can be prescribed to the patient in liver failure without causing an overdose.
Intoxication is usually treated with supportive measures and close observation for signs of withdrawal. Parenteral flumazenil immediately reverses benzodiazepine intoxication—which may assist both diagnosis and treatment—but its potential to cause seizures20 decreases this antagonist’s clinical usefulness.
Because benzodiazepine addiction often begins with prescribed medication, emergency department personnel can educate both patients and prescribers. Medications such as diazepam, lorazepam, and alprazolam are relatively safe short-term soporific agents, but use for more than a few weeks often leads to physical dependence and/or addiction. Emergency personnel can help the patient and prescriber switch to a treatment with fewer side effects and less danger of addiction.
Summary
Addicts do often change their destructive behavior when faced with increasing consequences such as job loss, relationship problems, financial difficulties, and physical deterioration. Emergencies related to drug and alcohol abuse can serve as learning experiences. Emergency department psychiatrists and other clinicians can use these crises as opportunities to help the addict:
- examine the consequences of substance use
- and change the destructive behaviors that lead to medical and social consequences.
Related resources
- American Academy of Addiction Psychiatry. www.aaap.org
- Galanter M, Kleber HD (eds). Textbook of substance abuse treatment (2nd ed). Washington, DC: American Psychiatric Press, 1999.
- Graham AW, Schultz TK (eds). Principles of addiction medicine (2nd ed). Chevy Chase, MD: American Society of Addiction Medicine, Inc., 1998.
- National Clearinghouse on Alcohol and Drug Issues. www.ncadi.org
Drug brand names
- Alprazolam • Xanax
- Diazepam • Valium
- Disulfiram • Antabuse
- Flumazenil • Romazicon
- Lorazepan • Ativan
- Oxazepam • Serax
- Secobarbital • Seconal
Disclosure
Dr. Westreich reports that he serves on the speakers’ bureaus of Pfizer Inc. and Bristol-Myers Squibb Company.
1. John F. Kennedy (speech). Indianapolis: April 12, 1959.
2. Office of Applied Studies Emergency department trends from the Drug Abuse Warning Network. Preliminary estimates, January-June 2001, with revised estimates, 1994-2000. Rockville, MD: Department of Health and Human Services, February 2002:40.
3. Office of Applied Studies. Mortality data from the Drug Abuse Warning Network, 2000. Rockville, MD: Department of Health and Human Services. January 2002:56-68.
4. Rosenthal RN, Westreich L. Treatment of persons with dual diagnoses of substance use disorder and other psychological problems. In: McCrady BS, Epstein EE (eds). Addictions: a comprehensive textbook. New York: Oxford University Press, 1999;439-76.
5. Sexia FA. Criteria for the diagnosis of alcoholism. In: Estes NJ, Heinemann ME (eds). Alcoholism: development, consequences and intervention. St. Louis: CV Mosby, 1982;49-66.
6. Menninger K. Man against himself. New York: Harcourt, Brace and World, 1938:147.
7. Hirschfeld RM. When to hospitalize the addict at risk for suicide. Ann NY Acad Sci 2001;932:188-96.
8. Malone KM, Oquendo MA, Haas GL, et al. Protective factors against suicidal acts in major depression: reasons for living. Am J Psychiatry 2000;157:1084-8.
9. Sixth Special Report to the United States Congress on Alcohol and Health Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1987.
10. Erwin WE, Williams DB, Speir WA. Delirium tremens. South Med J 1998;91(5):425-32.
11. Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001;27-33.
12. Weiss RD, Mirin SM, Bartell RL. Cocaine (2nd ed). Washington, DC: American Psychiatric Press, 1994;31-3.
13. Catravas JD, Waters IW, Walz MA, et al. Antidotes for cocaine poisoning. N Engl J Med 1977;301:1238.-
14. Stimmel B. Alcoholism, drug addiction, and the road to recovery. New York: Haworth Medical Press, 2002;142.-
15. Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine (“ecstasy”). Lancet 1992;340:384-7.
16. Cohen RS. The love drug: marching to the beat of ecstasy. Binghamton, NY: Haworth Medical Press, 1998.
17. Baldridge EB, Bessen HA. Phencyclidine. Emerg Med Clin North Am 1990;8(3):541-50.
18. Silberstein SD. Drug-induced headache. Neurol Clin North Am 1998;16(1):114.-
19. Arana G, Rosenbaum JF. Handbook of psychiatric drug therapy (4th ed). New York: Lippincott Williams & Wilkins; 2000;179.-
20. Roche Laboratories Romazicon (package insert).
Mrs. R, age 43, is agitated and confused, and her husband has brought her to the hospital’s emergency department. He reports that she has a history of denying alcohol abuse and told him during an argument yesterday that she could stop drinking any time she wanted to.
You are the psychiatrist on call. As the emergency medical team treats the apparent withdrawal episode, you tell Mrs. R’s husband: “We’ll take good care of your wife because alcohol withdrawal is dangerous and painful. But after detoxification, it’s important to prevent her from getting sick again. She needs to enter a rehabilitation program, and then outpatient treatment. When she comes around, maybe you could remind her about how much pain she was in and bring her to the rehab center yourself…”
Addicts face potentially life-threatening consequences from their behavior, which—when handled skillfully in the emergency room—can start them on the road to recovery. Some say the addict must “hit bottom” before making the changes necessary for a sober life. You can help the addict define his or her bottom as an unpleasant trip to the hospital—instead of death or loss of a job or spouse—by realistically assessing the physical consequences of continued drug or alcohol use (Table 1).
Emergencies related to alcohol or drug use accounted for 601,563 visits to U.S. emergency departments in 2000, according to the government-sponsored Drug Abuse Warning Network (DAWN).2 Alcohol in combination with any illegal or illicit drug accounted for 34% of emergency visits, cocaine for 29%, and heroin for 16%.
Mortality rates vary by region. In Los Angeles, for instance, heroin and cocaine each caused approximately the same number of deaths when compared with alcohol in combination (Figure).3 Most deaths (73%) were considered accidental/unexpected, with 19% coded as suicide. New York City showed similar percentages of deaths called accidental/unexpected, but heroin as the cause of death ran a distant fourth to cocaine alone, narcotic analgesics alone, and alcohol in combination.2
Addiction crises bring more than a half-million Americans to hospital emergency rooms each year (Box 1,Figure).2,3 This article describes teachable moments—suicide attempts, accidental overdose, intoxication, and withdrawal—that you can use to bundle acute treatment with referral for addiction treatment.
Suicide
Suicide is the addict’s most immediate life-threatening emergency. Psychiatric and addictive disorders often coexist,4 but some substances can trigger suicidal behavior even in the absence of another diagnosable psychiatric disorder. The addicted person who jumps off a roof, believing he can fly, may think perfectly clearly when not using crack cocaine.
Addiction to any substance greatly increases the risk for suicide. An alcohol-dependent person is 32 times more likely to commit suicide than the nonaddicted individual.5 And the suicidal addict often has the means to end his life when he feels most suicidal.
Figure DRUG-RELATED DEATHS IN LOS ANGELES, 20022
Diagnosing and treating suicidality require a high degree of vigilance for subtle clues of suicidal behavior. Because suicide risk has no pathognomonic signs, clinical judgment is required. Though addiction itself can be viewed as a slow form of suicide,6 signs that suggest an immediate threat to life include:
- the addict’s assertion that he intends to kill himself
- serious comorbid mental illness (psychosis, depression)7
- prior suicide attempts
- hopelessness.8
Some addicts feign suicidal thoughts or use them as a cry for help. Any mention or hint regarding suicide marks a severely disturbed patient who needs a complete psychiatric evaluation. This includes a formal mental status examination and exploring whether the patient has access to lethal means.
We cannot consistently predict our patients’ behavior, but a careful examination often reveals the seriousness of a suicidal threat, method, and intention, as well as support systems for keeping the patient safe. Consulting with a colleague can offer a “fresh look,” allowing two clinicians to balance the need for treatment against concerns such as bed availability and possible malingering.
Table 1
EMERGENCY AND LONG-TERM MEDICAL CONSEQUENCES OF ADDICTION
| Addictive substance | Intoxication symptoms | Withdrawal symptoms | Longer-term problems |
|---|---|---|---|
| Alcohol | Slowed respiration, impaired thinking and coordination, coma, death | Seizures, death | Dementia, liver damage |
| Barbiturates | Slowed respiration, impaired thinking and coordination, coma, death | Seizures | Rebound pain, hepatotoxicity |
| Benzodiazepines | Slowed respiration, impaired thinking and coordination | Seizures | |
| Hallucinogens | Paranoia, impaired thinking and coordination | Amotivational syndrome; possession is grounds for arrest | |
| MDMA(‘ecstasy’) | Impaired thinking and coordination, stroke, hyperthymia, dehydration, death | Cognitive impairment; possession is grounds for arrest | |
| Nicotine | Tachycardia, arrhythmia | Lung cancer, chronic-obstructive pulmonary disease | |
| Opiates | Slowed respiration, impaired thinking and coordination, coma, death | Skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Phencyclidine (PCP, ‘angel dust’) | Impaired thinking and coordination, violent behavior | Possession is grounds for arrest | |
| Stimulants | Impaired thinking and coordination, myocardial infarction, stroke | Nasal damage (if snorted); skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Inhalants | Impaired thinking and coordination, headache, coma | Neurologic damage |
Suicidal thoughts are unassailable grounds for comprehensive evaluation and treatment—regardless of the suicide evaluation’s outcome. The addict who even hints at suicide should undergo a thorough medical and psychiatric evaluation and then engage in whatever treatment is indicated.
Emphasize the seriousness of suicidal thoughts to the patient, his family, third-party payers, and whomever else has influence in bringing the patient to treatment. Suicidal behaviors or intentions remain one of the few legal justifications for involuntary hospitalization.
Accidental overdose
An accidental overdose provides another teachable moment to convince the addict to enter treatment. Patients who try to make a statement by overdosing on a substance they consider benign, such as oxycodone with acetaminophen, can inadvertently kill or badly injure themselves. Conversely, patients who clearly intend to harm themselves may misconstrue a substance’s lethality and ingest a large amount of a relatively nonlethal substance such as clonazepam. Either case:
- is a true psychiatric emergency
- bodes poorly for the patient’s future
- provides a strong rationale for addiction treatment.
Whether the means or the intent were deadly or benign, the overdose can be used as a convincing argument for treatment.
Intoxication
Intoxication with any addictive substance impairs judgment and increases the danger of injury. Specific medical dangers include alcohol’s powerful CNS depression in the nontolerant individual and the possibility for heart attack and stroke in the cocaine-intoxicated patient.
Attempts to convince an intoxicated person of the need for addiction treatment are usually futile. But the acute treatment represents a golden opportunity to reach out to friends and family members, who often escort the intoxicated addict to the emergency room. A medical record documenting the patient’s impaired behavior serves as evidence for (later) convincing the addict to go into treatment or for legal coercion of that treatment.
Table 2
MANAGING SYMPTOMS OF ALCOHOL WITHDRAWAL AND DELIRIUM TREMENS
| Alcohol withdrawal | Delirium tremens |
|---|---|
| Begins 4 hours to 2 days after cessation of alcohol or precipitous drop in blood alcohol level | Begins 1 to 2 days after cessation of alcohol or precipitous drop in blood alcohol level |
| Symptoms | Symptoms |
| Anxiety Agitation Tremor Autonomic instability Insomnia Confusion | Agitation Severe autonomic instability Seizure Severe confusion Hallucinations |
| Treatment Treatment of co-occurring medical illness Parenteral thiamine Tapering doses of CNS depressants, most often benzodiazepines | |
Withdrawal
Withdrawal, like intoxication, presents emergency conditions specific to the abused substance. Unlike the intoxicated patient, however, a patient experiencing the unpleasant symptoms of withdrawal may understand the need for addiction treatment. Because alcohol withdrawal often requires sedative/hypnotic treatment, the wise clinician can design a treatment plan that combines the anti-withdrawal medication with:
- attending Alcoholics Anonymous meetings
- taking disulfiram 12 hours after the last alcohol use and then daily
- and participation in relapse prevention psychotherapy.
Emergency treatments
Psychiatrists often have close contact with addicted patients in the hospital, clinic, or emergency department and therefore need to be familiar with basic techniques for managing addiction emergencies. Although addiction-trained psychiatrists manage emergencies at many institutions, general psychiatrists who have learned the following guidelines can form quick and solid therapeutic alliances with their addicted patients in the emergency department.
Alcohol
People live dangerously when intoxicated; about 40% of fatal U.S. car accidents involve a drunken driver.9 Alcohol also can incite physical violence and self-damaging sexual behavior and cause respiratory depression and death.
Acute effects of alcohol intoxication must be treated while guarding against potentially lethal withdrawal. Dangerous intoxication states with respiratory compromise may require aggressive supportive care, including intubation and mechanical ventilation. For agitated, intoxicated persons who represent a threat to themselves or others, chemical sedation with benzodiazepines—as opposed to physical restraint—is the preferred treatment.
Alcohol withdrawal requires immediate, definitive treatment (Table 2). Although mild withdrawal is common among alcoholics who cut back on or abruptly stop drinking, it can devolve quickly into delirium tremens (DTs). Serious medical problems—including severe autonomic instability and seizures—occur with DTs, which are associated with mortality rates of 5 to 15%.10 The adroit emergency department clinician can use the alcohol withdrawal/delirium episode to encourage the patient to begin addiction treatment (Box 2).11
Cocaine
Stimulants—most commonly cocaine and smoked methamphetamine—can cause myocardial infarction, cardiac arrhythmia, cerebral hemorrhage, hyperpyrexia, and status epilepticus.12 These emergencies occurring in a young person indicate the need to screen for cocaine use. Because no antidote exists for stimulant intoxication, we can only deliver supportive care while remaining vigilant for other sequelae of stimulant use, such as agitation and hypertension.13
Opiates
Overdoses leading to coma and death are the most devastating physical consequence of opiate abuse. Contrary to popular belief, orally ingested and inhaled opiates can depress respiration enough to cause death, just as injected opiates can. Because even appropriately prescribed opioid medications can lead to overdose or addiction, emergency treaters should be prepared to refer patients for pain management.
High-potency heroin often causes overdose in the novice user or in the addict who is surprised by a sudden increase in the heroin’s purity. Adulterants used by dealers to “cut” heroin also can cause illness and death. Quinine, for instance, can cause cardiac arrhythmias. Contaminants such as fentanyl and cholinergic agents such as scopolamine added to enhance the “high” associated with heroin can increase the risk of toxicity or death.
Opioid overdose is characterized by cyanosis and pulmonary edema: slowed breathing, altered mental status, blue lips and fingernail beds, pinpoint pupils, hypothermia, and gasping respirations. In addition to respiratory and cardiac support, treatment with the narcotic antagonist naloxone immediately reverses opioid overdose.
To what level of care should you refer the addicted patient from the emergency department—an inpatient medical unit, psychiatric unit/detoxification facility, residential treatment, partial hospitalization, or other model of care? The American Society of Addiction Medicine (ASAM) manual lists disposition recommendations to match individual patients’ clinical criteria. The criteria and levels are listed here as reminders of the issues involved in referring the addicted patient.
ASAM patient criteria
- Alcohol intoxication and/or withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Relapse, continued use, or continued problem potential
- Recovery environment
ASAM levels of care
- Early intervention
- Opioid maintenance therapy
- Outpatient treatment
- Intensive outpatient treatment
- Partial hospitalization
- Clinically managed low-intensity residential services
- Clinically managed high-intensity residential services
- Medically monitored intensive inpatient treatment
- Medically managed intensive inpatient treatment
Source: Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001:27-33.
Ecstasy
The drug 3,4-methylenedioxymethamphetamine (MDMA)—also known as Ecstasy, X, and XTC3 —provokes release of dopamine and serotonin into the synapse, causing a sense of blissful open-mindedness, closeness to others, and the ability to “break down (mental) barriers.”14 In the context of “rave” dance parties, MDMA also causes dehydration and hyperthermia, which can lead to rhabdomyolysis, kidney failure, and death.
Life-threatening consequences generally occur only when adequate water is unavailable to a group of intoxicated, dancing teenagers.15 The more common emergency presentations include sudden hypertension, tachycardia, vomiting, depersonalization, panic attacks, and psychosis.16
Immediate treatment includes restoration of normal fluid levels and body temperature, plus reassurance for the non-life-threatening, more common, presentations.
Phencyclidine
Phencyclidine (PCP) and its analogue ketamine—originally developed as anesthetic agents—are no longer used therapeutically because they can cause dissociation, anxiety, and even psychosis. Panic can change to hyperactive behavior, aggressiveness, and violent acts, so the first treatment goal must be to secure the safety of the intoxicated person and others. Chemical restraints such as benzodiazepines are preferred to physical restraints, although some situations may require physical restraint, at least initially.17
PCP affects memory, and often the user is unaware of the agent’s consequences unless he hears descriptions of his behavior from family and friends unfortunate enough to witness the intoxicated state. Coaching by emergency personnel can help the family confront the user with evidence that he needs treatment.
Barbiturates
Physicians prescribe barbiturates such as pentobarbital, phenobarbital, and secobarbital for pain, insomnia, alcohol withdrawal, and anxiety states. Although sometimes useful for acute pain, these drugs can also cause physical dependence, intoxication in overdose, withdrawal seizures, and rebound pain.18
The withdrawal associated with barbiturates—as with withdrawal from other CNS depressants such as alcohol and benzodiazepines—consists of autonomic hyperactivity, confusion, and occasionally seizures.
Overdose, often in combination with alcohol, accounts for most emergency presentations of barbiturate addiction. Supportive treatment—from reassurance and observation to airway support and mechanical ventilation—is required. Since obtundation and coma commonly occur with alcohol/barbiturate combinations, treatment includes monitoring for alcohol intoxication or withdrawal. No antidote exists for barbiturate intoxication.
Alternate medications. If the patient has become addicted to barbiturates prescribed for one of the common indications such as migraine headache, the emergency treater can promote use of a more effective treatment by acknowledging the need to control the headache pain. In managing this pain, the emergency worker can arrange referral:
- to an addiction specialist for treatment of the (now addictive) barbiturate use
- and to a neurologist who can evaluate the patient and prescribe one of many highly effective, nonaddicting headache remedies.
By taking the addiction and the pain seriously, the treater forms an alliance with the patient against the unhealthy consequences of both migraine headaches and addiction.
Benzodiazepines
Often prescribed for anxiety and insomnia, benzodiazepines cause emergency syndromes directly related to their potency, serum half-lives, and lipophilicity. For instance, alprazolam—which is potent, short-acting,19 and highly lipophilic—causes a severe withdrawal syndrome when high doses are stopped abruptly. This withdrawal state includes anxiety, agitation, and autonomic instability and can progress to frank seizures.
Withdrawal is treated by tapering the benzodiazepine dosage or substituting another benzodiazepine such as clonazepam. Benzodiazepine intoxication usually occurs only with large overdoses, although intoxication can last for days in a patient with hepatic disease. Lorazepam and oxazepam are not metabolized by the liver and can be prescribed to the patient in liver failure without causing an overdose.
Intoxication is usually treated with supportive measures and close observation for signs of withdrawal. Parenteral flumazenil immediately reverses benzodiazepine intoxication—which may assist both diagnosis and treatment—but its potential to cause seizures20 decreases this antagonist’s clinical usefulness.
Because benzodiazepine addiction often begins with prescribed medication, emergency department personnel can educate both patients and prescribers. Medications such as diazepam, lorazepam, and alprazolam are relatively safe short-term soporific agents, but use for more than a few weeks often leads to physical dependence and/or addiction. Emergency personnel can help the patient and prescriber switch to a treatment with fewer side effects and less danger of addiction.
Summary
Addicts do often change their destructive behavior when faced with increasing consequences such as job loss, relationship problems, financial difficulties, and physical deterioration. Emergencies related to drug and alcohol abuse can serve as learning experiences. Emergency department psychiatrists and other clinicians can use these crises as opportunities to help the addict:
- examine the consequences of substance use
- and change the destructive behaviors that lead to medical and social consequences.
Related resources
- American Academy of Addiction Psychiatry. www.aaap.org
- Galanter M, Kleber HD (eds). Textbook of substance abuse treatment (2nd ed). Washington, DC: American Psychiatric Press, 1999.
- Graham AW, Schultz TK (eds). Principles of addiction medicine (2nd ed). Chevy Chase, MD: American Society of Addiction Medicine, Inc., 1998.
- National Clearinghouse on Alcohol and Drug Issues. www.ncadi.org
Drug brand names
- Alprazolam • Xanax
- Diazepam • Valium
- Disulfiram • Antabuse
- Flumazenil • Romazicon
- Lorazepan • Ativan
- Oxazepam • Serax
- Secobarbital • Seconal
Disclosure
Dr. Westreich reports that he serves on the speakers’ bureaus of Pfizer Inc. and Bristol-Myers Squibb Company.
Mrs. R, age 43, is agitated and confused, and her husband has brought her to the hospital’s emergency department. He reports that she has a history of denying alcohol abuse and told him during an argument yesterday that she could stop drinking any time she wanted to.
You are the psychiatrist on call. As the emergency medical team treats the apparent withdrawal episode, you tell Mrs. R’s husband: “We’ll take good care of your wife because alcohol withdrawal is dangerous and painful. But after detoxification, it’s important to prevent her from getting sick again. She needs to enter a rehabilitation program, and then outpatient treatment. When she comes around, maybe you could remind her about how much pain she was in and bring her to the rehab center yourself…”
Addicts face potentially life-threatening consequences from their behavior, which—when handled skillfully in the emergency room—can start them on the road to recovery. Some say the addict must “hit bottom” before making the changes necessary for a sober life. You can help the addict define his or her bottom as an unpleasant trip to the hospital—instead of death or loss of a job or spouse—by realistically assessing the physical consequences of continued drug or alcohol use (Table 1).
Emergencies related to alcohol or drug use accounted for 601,563 visits to U.S. emergency departments in 2000, according to the government-sponsored Drug Abuse Warning Network (DAWN).2 Alcohol in combination with any illegal or illicit drug accounted for 34% of emergency visits, cocaine for 29%, and heroin for 16%.
Mortality rates vary by region. In Los Angeles, for instance, heroin and cocaine each caused approximately the same number of deaths when compared with alcohol in combination (Figure).3 Most deaths (73%) were considered accidental/unexpected, with 19% coded as suicide. New York City showed similar percentages of deaths called accidental/unexpected, but heroin as the cause of death ran a distant fourth to cocaine alone, narcotic analgesics alone, and alcohol in combination.2
Addiction crises bring more than a half-million Americans to hospital emergency rooms each year (Box 1,Figure).2,3 This article describes teachable moments—suicide attempts, accidental overdose, intoxication, and withdrawal—that you can use to bundle acute treatment with referral for addiction treatment.
Suicide
Suicide is the addict’s most immediate life-threatening emergency. Psychiatric and addictive disorders often coexist,4 but some substances can trigger suicidal behavior even in the absence of another diagnosable psychiatric disorder. The addicted person who jumps off a roof, believing he can fly, may think perfectly clearly when not using crack cocaine.
Addiction to any substance greatly increases the risk for suicide. An alcohol-dependent person is 32 times more likely to commit suicide than the nonaddicted individual.5 And the suicidal addict often has the means to end his life when he feels most suicidal.
Figure DRUG-RELATED DEATHS IN LOS ANGELES, 20022
Diagnosing and treating suicidality require a high degree of vigilance for subtle clues of suicidal behavior. Because suicide risk has no pathognomonic signs, clinical judgment is required. Though addiction itself can be viewed as a slow form of suicide,6 signs that suggest an immediate threat to life include:
- the addict’s assertion that he intends to kill himself
- serious comorbid mental illness (psychosis, depression)7
- prior suicide attempts
- hopelessness.8
Some addicts feign suicidal thoughts or use them as a cry for help. Any mention or hint regarding suicide marks a severely disturbed patient who needs a complete psychiatric evaluation. This includes a formal mental status examination and exploring whether the patient has access to lethal means.
We cannot consistently predict our patients’ behavior, but a careful examination often reveals the seriousness of a suicidal threat, method, and intention, as well as support systems for keeping the patient safe. Consulting with a colleague can offer a “fresh look,” allowing two clinicians to balance the need for treatment against concerns such as bed availability and possible malingering.
Table 1
EMERGENCY AND LONG-TERM MEDICAL CONSEQUENCES OF ADDICTION
| Addictive substance | Intoxication symptoms | Withdrawal symptoms | Longer-term problems |
|---|---|---|---|
| Alcohol | Slowed respiration, impaired thinking and coordination, coma, death | Seizures, death | Dementia, liver damage |
| Barbiturates | Slowed respiration, impaired thinking and coordination, coma, death | Seizures | Rebound pain, hepatotoxicity |
| Benzodiazepines | Slowed respiration, impaired thinking and coordination | Seizures | |
| Hallucinogens | Paranoia, impaired thinking and coordination | Amotivational syndrome; possession is grounds for arrest | |
| MDMA(‘ecstasy’) | Impaired thinking and coordination, stroke, hyperthymia, dehydration, death | Cognitive impairment; possession is grounds for arrest | |
| Nicotine | Tachycardia, arrhythmia | Lung cancer, chronic-obstructive pulmonary disease | |
| Opiates | Slowed respiration, impaired thinking and coordination, coma, death | Skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Phencyclidine (PCP, ‘angel dust’) | Impaired thinking and coordination, violent behavior | Possession is grounds for arrest | |
| Stimulants | Impaired thinking and coordination, myocardial infarction, stroke | Nasal damage (if snorted); skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Inhalants | Impaired thinking and coordination, headache, coma | Neurologic damage |
Suicidal thoughts are unassailable grounds for comprehensive evaluation and treatment—regardless of the suicide evaluation’s outcome. The addict who even hints at suicide should undergo a thorough medical and psychiatric evaluation and then engage in whatever treatment is indicated.
Emphasize the seriousness of suicidal thoughts to the patient, his family, third-party payers, and whomever else has influence in bringing the patient to treatment. Suicidal behaviors or intentions remain one of the few legal justifications for involuntary hospitalization.
Accidental overdose
An accidental overdose provides another teachable moment to convince the addict to enter treatment. Patients who try to make a statement by overdosing on a substance they consider benign, such as oxycodone with acetaminophen, can inadvertently kill or badly injure themselves. Conversely, patients who clearly intend to harm themselves may misconstrue a substance’s lethality and ingest a large amount of a relatively nonlethal substance such as clonazepam. Either case:
- is a true psychiatric emergency
- bodes poorly for the patient’s future
- provides a strong rationale for addiction treatment.
Whether the means or the intent were deadly or benign, the overdose can be used as a convincing argument for treatment.
Intoxication
Intoxication with any addictive substance impairs judgment and increases the danger of injury. Specific medical dangers include alcohol’s powerful CNS depression in the nontolerant individual and the possibility for heart attack and stroke in the cocaine-intoxicated patient.
Attempts to convince an intoxicated person of the need for addiction treatment are usually futile. But the acute treatment represents a golden opportunity to reach out to friends and family members, who often escort the intoxicated addict to the emergency room. A medical record documenting the patient’s impaired behavior serves as evidence for (later) convincing the addict to go into treatment or for legal coercion of that treatment.
Table 2
MANAGING SYMPTOMS OF ALCOHOL WITHDRAWAL AND DELIRIUM TREMENS
| Alcohol withdrawal | Delirium tremens |
|---|---|
| Begins 4 hours to 2 days after cessation of alcohol or precipitous drop in blood alcohol level | Begins 1 to 2 days after cessation of alcohol or precipitous drop in blood alcohol level |
| Symptoms | Symptoms |
| Anxiety Agitation Tremor Autonomic instability Insomnia Confusion | Agitation Severe autonomic instability Seizure Severe confusion Hallucinations |
| Treatment Treatment of co-occurring medical illness Parenteral thiamine Tapering doses of CNS depressants, most often benzodiazepines | |
Withdrawal
Withdrawal, like intoxication, presents emergency conditions specific to the abused substance. Unlike the intoxicated patient, however, a patient experiencing the unpleasant symptoms of withdrawal may understand the need for addiction treatment. Because alcohol withdrawal often requires sedative/hypnotic treatment, the wise clinician can design a treatment plan that combines the anti-withdrawal medication with:
- attending Alcoholics Anonymous meetings
- taking disulfiram 12 hours after the last alcohol use and then daily
- and participation in relapse prevention psychotherapy.
Emergency treatments
Psychiatrists often have close contact with addicted patients in the hospital, clinic, or emergency department and therefore need to be familiar with basic techniques for managing addiction emergencies. Although addiction-trained psychiatrists manage emergencies at many institutions, general psychiatrists who have learned the following guidelines can form quick and solid therapeutic alliances with their addicted patients in the emergency department.
Alcohol
People live dangerously when intoxicated; about 40% of fatal U.S. car accidents involve a drunken driver.9 Alcohol also can incite physical violence and self-damaging sexual behavior and cause respiratory depression and death.
Acute effects of alcohol intoxication must be treated while guarding against potentially lethal withdrawal. Dangerous intoxication states with respiratory compromise may require aggressive supportive care, including intubation and mechanical ventilation. For agitated, intoxicated persons who represent a threat to themselves or others, chemical sedation with benzodiazepines—as opposed to physical restraint—is the preferred treatment.
Alcohol withdrawal requires immediate, definitive treatment (Table 2). Although mild withdrawal is common among alcoholics who cut back on or abruptly stop drinking, it can devolve quickly into delirium tremens (DTs). Serious medical problems—including severe autonomic instability and seizures—occur with DTs, which are associated with mortality rates of 5 to 15%.10 The adroit emergency department clinician can use the alcohol withdrawal/delirium episode to encourage the patient to begin addiction treatment (Box 2).11
Cocaine
Stimulants—most commonly cocaine and smoked methamphetamine—can cause myocardial infarction, cardiac arrhythmia, cerebral hemorrhage, hyperpyrexia, and status epilepticus.12 These emergencies occurring in a young person indicate the need to screen for cocaine use. Because no antidote exists for stimulant intoxication, we can only deliver supportive care while remaining vigilant for other sequelae of stimulant use, such as agitation and hypertension.13
Opiates
Overdoses leading to coma and death are the most devastating physical consequence of opiate abuse. Contrary to popular belief, orally ingested and inhaled opiates can depress respiration enough to cause death, just as injected opiates can. Because even appropriately prescribed opioid medications can lead to overdose or addiction, emergency treaters should be prepared to refer patients for pain management.
High-potency heroin often causes overdose in the novice user or in the addict who is surprised by a sudden increase in the heroin’s purity. Adulterants used by dealers to “cut” heroin also can cause illness and death. Quinine, for instance, can cause cardiac arrhythmias. Contaminants such as fentanyl and cholinergic agents such as scopolamine added to enhance the “high” associated with heroin can increase the risk of toxicity or death.
Opioid overdose is characterized by cyanosis and pulmonary edema: slowed breathing, altered mental status, blue lips and fingernail beds, pinpoint pupils, hypothermia, and gasping respirations. In addition to respiratory and cardiac support, treatment with the narcotic antagonist naloxone immediately reverses opioid overdose.
To what level of care should you refer the addicted patient from the emergency department—an inpatient medical unit, psychiatric unit/detoxification facility, residential treatment, partial hospitalization, or other model of care? The American Society of Addiction Medicine (ASAM) manual lists disposition recommendations to match individual patients’ clinical criteria. The criteria and levels are listed here as reminders of the issues involved in referring the addicted patient.
ASAM patient criteria
- Alcohol intoxication and/or withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Relapse, continued use, or continued problem potential
- Recovery environment
ASAM levels of care
- Early intervention
- Opioid maintenance therapy
- Outpatient treatment
- Intensive outpatient treatment
- Partial hospitalization
- Clinically managed low-intensity residential services
- Clinically managed high-intensity residential services
- Medically monitored intensive inpatient treatment
- Medically managed intensive inpatient treatment
Source: Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001:27-33.
Ecstasy
The drug 3,4-methylenedioxymethamphetamine (MDMA)—also known as Ecstasy, X, and XTC3 —provokes release of dopamine and serotonin into the synapse, causing a sense of blissful open-mindedness, closeness to others, and the ability to “break down (mental) barriers.”14 In the context of “rave” dance parties, MDMA also causes dehydration and hyperthermia, which can lead to rhabdomyolysis, kidney failure, and death.
Life-threatening consequences generally occur only when adequate water is unavailable to a group of intoxicated, dancing teenagers.15 The more common emergency presentations include sudden hypertension, tachycardia, vomiting, depersonalization, panic attacks, and psychosis.16
Immediate treatment includes restoration of normal fluid levels and body temperature, plus reassurance for the non-life-threatening, more common, presentations.
Phencyclidine
Phencyclidine (PCP) and its analogue ketamine—originally developed as anesthetic agents—are no longer used therapeutically because they can cause dissociation, anxiety, and even psychosis. Panic can change to hyperactive behavior, aggressiveness, and violent acts, so the first treatment goal must be to secure the safety of the intoxicated person and others. Chemical restraints such as benzodiazepines are preferred to physical restraints, although some situations may require physical restraint, at least initially.17
PCP affects memory, and often the user is unaware of the agent’s consequences unless he hears descriptions of his behavior from family and friends unfortunate enough to witness the intoxicated state. Coaching by emergency personnel can help the family confront the user with evidence that he needs treatment.
Barbiturates
Physicians prescribe barbiturates such as pentobarbital, phenobarbital, and secobarbital for pain, insomnia, alcohol withdrawal, and anxiety states. Although sometimes useful for acute pain, these drugs can also cause physical dependence, intoxication in overdose, withdrawal seizures, and rebound pain.18
The withdrawal associated with barbiturates—as with withdrawal from other CNS depressants such as alcohol and benzodiazepines—consists of autonomic hyperactivity, confusion, and occasionally seizures.
Overdose, often in combination with alcohol, accounts for most emergency presentations of barbiturate addiction. Supportive treatment—from reassurance and observation to airway support and mechanical ventilation—is required. Since obtundation and coma commonly occur with alcohol/barbiturate combinations, treatment includes monitoring for alcohol intoxication or withdrawal. No antidote exists for barbiturate intoxication.
Alternate medications. If the patient has become addicted to barbiturates prescribed for one of the common indications such as migraine headache, the emergency treater can promote use of a more effective treatment by acknowledging the need to control the headache pain. In managing this pain, the emergency worker can arrange referral:
- to an addiction specialist for treatment of the (now addictive) barbiturate use
- and to a neurologist who can evaluate the patient and prescribe one of many highly effective, nonaddicting headache remedies.
By taking the addiction and the pain seriously, the treater forms an alliance with the patient against the unhealthy consequences of both migraine headaches and addiction.
Benzodiazepines
Often prescribed for anxiety and insomnia, benzodiazepines cause emergency syndromes directly related to their potency, serum half-lives, and lipophilicity. For instance, alprazolam—which is potent, short-acting,19 and highly lipophilic—causes a severe withdrawal syndrome when high doses are stopped abruptly. This withdrawal state includes anxiety, agitation, and autonomic instability and can progress to frank seizures.
Withdrawal is treated by tapering the benzodiazepine dosage or substituting another benzodiazepine such as clonazepam. Benzodiazepine intoxication usually occurs only with large overdoses, although intoxication can last for days in a patient with hepatic disease. Lorazepam and oxazepam are not metabolized by the liver and can be prescribed to the patient in liver failure without causing an overdose.
Intoxication is usually treated with supportive measures and close observation for signs of withdrawal. Parenteral flumazenil immediately reverses benzodiazepine intoxication—which may assist both diagnosis and treatment—but its potential to cause seizures20 decreases this antagonist’s clinical usefulness.
Because benzodiazepine addiction often begins with prescribed medication, emergency department personnel can educate both patients and prescribers. Medications such as diazepam, lorazepam, and alprazolam are relatively safe short-term soporific agents, but use for more than a few weeks often leads to physical dependence and/or addiction. Emergency personnel can help the patient and prescriber switch to a treatment with fewer side effects and less danger of addiction.
Summary
Addicts do often change their destructive behavior when faced with increasing consequences such as job loss, relationship problems, financial difficulties, and physical deterioration. Emergencies related to drug and alcohol abuse can serve as learning experiences. Emergency department psychiatrists and other clinicians can use these crises as opportunities to help the addict:
- examine the consequences of substance use
- and change the destructive behaviors that lead to medical and social consequences.
Related resources
- American Academy of Addiction Psychiatry. www.aaap.org
- Galanter M, Kleber HD (eds). Textbook of substance abuse treatment (2nd ed). Washington, DC: American Psychiatric Press, 1999.
- Graham AW, Schultz TK (eds). Principles of addiction medicine (2nd ed). Chevy Chase, MD: American Society of Addiction Medicine, Inc., 1998.
- National Clearinghouse on Alcohol and Drug Issues. www.ncadi.org
Drug brand names
- Alprazolam • Xanax
- Diazepam • Valium
- Disulfiram • Antabuse
- Flumazenil • Romazicon
- Lorazepan • Ativan
- Oxazepam • Serax
- Secobarbital • Seconal
Disclosure
Dr. Westreich reports that he serves on the speakers’ bureaus of Pfizer Inc. and Bristol-Myers Squibb Company.
1. John F. Kennedy (speech). Indianapolis: April 12, 1959.
2. Office of Applied Studies Emergency department trends from the Drug Abuse Warning Network. Preliminary estimates, January-June 2001, with revised estimates, 1994-2000. Rockville, MD: Department of Health and Human Services, February 2002:40.
3. Office of Applied Studies. Mortality data from the Drug Abuse Warning Network, 2000. Rockville, MD: Department of Health and Human Services. January 2002:56-68.
4. Rosenthal RN, Westreich L. Treatment of persons with dual diagnoses of substance use disorder and other psychological problems. In: McCrady BS, Epstein EE (eds). Addictions: a comprehensive textbook. New York: Oxford University Press, 1999;439-76.
5. Sexia FA. Criteria for the diagnosis of alcoholism. In: Estes NJ, Heinemann ME (eds). Alcoholism: development, consequences and intervention. St. Louis: CV Mosby, 1982;49-66.
6. Menninger K. Man against himself. New York: Harcourt, Brace and World, 1938:147.
7. Hirschfeld RM. When to hospitalize the addict at risk for suicide. Ann NY Acad Sci 2001;932:188-96.
8. Malone KM, Oquendo MA, Haas GL, et al. Protective factors against suicidal acts in major depression: reasons for living. Am J Psychiatry 2000;157:1084-8.
9. Sixth Special Report to the United States Congress on Alcohol and Health Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1987.
10. Erwin WE, Williams DB, Speir WA. Delirium tremens. South Med J 1998;91(5):425-32.
11. Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001;27-33.
12. Weiss RD, Mirin SM, Bartell RL. Cocaine (2nd ed). Washington, DC: American Psychiatric Press, 1994;31-3.
13. Catravas JD, Waters IW, Walz MA, et al. Antidotes for cocaine poisoning. N Engl J Med 1977;301:1238.-
14. Stimmel B. Alcoholism, drug addiction, and the road to recovery. New York: Haworth Medical Press, 2002;142.-
15. Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine (“ecstasy”). Lancet 1992;340:384-7.
16. Cohen RS. The love drug: marching to the beat of ecstasy. Binghamton, NY: Haworth Medical Press, 1998.
17. Baldridge EB, Bessen HA. Phencyclidine. Emerg Med Clin North Am 1990;8(3):541-50.
18. Silberstein SD. Drug-induced headache. Neurol Clin North Am 1998;16(1):114.-
19. Arana G, Rosenbaum JF. Handbook of psychiatric drug therapy (4th ed). New York: Lippincott Williams & Wilkins; 2000;179.-
20. Roche Laboratories Romazicon (package insert).
1. John F. Kennedy (speech). Indianapolis: April 12, 1959.
2. Office of Applied Studies Emergency department trends from the Drug Abuse Warning Network. Preliminary estimates, January-June 2001, with revised estimates, 1994-2000. Rockville, MD: Department of Health and Human Services, February 2002:40.
3. Office of Applied Studies. Mortality data from the Drug Abuse Warning Network, 2000. Rockville, MD: Department of Health and Human Services. January 2002:56-68.
4. Rosenthal RN, Westreich L. Treatment of persons with dual diagnoses of substance use disorder and other psychological problems. In: McCrady BS, Epstein EE (eds). Addictions: a comprehensive textbook. New York: Oxford University Press, 1999;439-76.
5. Sexia FA. Criteria for the diagnosis of alcoholism. In: Estes NJ, Heinemann ME (eds). Alcoholism: development, consequences and intervention. St. Louis: CV Mosby, 1982;49-66.
6. Menninger K. Man against himself. New York: Harcourt, Brace and World, 1938:147.
7. Hirschfeld RM. When to hospitalize the addict at risk for suicide. Ann NY Acad Sci 2001;932:188-96.
8. Malone KM, Oquendo MA, Haas GL, et al. Protective factors against suicidal acts in major depression: reasons for living. Am J Psychiatry 2000;157:1084-8.
9. Sixth Special Report to the United States Congress on Alcohol and Health Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1987.
10. Erwin WE, Williams DB, Speir WA. Delirium tremens. South Med J 1998;91(5):425-32.
11. Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001;27-33.
12. Weiss RD, Mirin SM, Bartell RL. Cocaine (2nd ed). Washington, DC: American Psychiatric Press, 1994;31-3.
13. Catravas JD, Waters IW, Walz MA, et al. Antidotes for cocaine poisoning. N Engl J Med 1977;301:1238.-
14. Stimmel B. Alcoholism, drug addiction, and the road to recovery. New York: Haworth Medical Press, 2002;142.-
15. Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine (“ecstasy”). Lancet 1992;340:384-7.
16. Cohen RS. The love drug: marching to the beat of ecstasy. Binghamton, NY: Haworth Medical Press, 1998.
17. Baldridge EB, Bessen HA. Phencyclidine. Emerg Med Clin North Am 1990;8(3):541-50.
18. Silberstein SD. Drug-induced headache. Neurol Clin North Am 1998;16(1):114.-
19. Arana G, Rosenbaum JF. Handbook of psychiatric drug therapy (4th ed). New York: Lippincott Williams & Wilkins; 2000;179.-
20. Roche Laboratories Romazicon (package insert).
Teachable moments: Turning alcohol and drug emergencies into catalysts for change
Mrs. R, age 43, is agitated and confused, and her husband has brought her to the hospital’s emergency department. He reports that she has a history of denying alcohol abuse and told him during an argument yesterday that she could stop drinking any time she wanted to.
You are the psychiatrist on call. As the emergency medical team treats the apparent withdrawal episode, you tell Mrs. R’s husband: “We’ll take good care of your wife because alcohol withdrawal is dangerous and painful. But after detoxification, it’s important to prevent her from getting sick again. She needs to enter a rehabilitation program, and then outpatient treatment. When she comes around, maybe you could remind her about how much pain she was in and bring her to the rehab center yourself…”
Addicts face potentially life-threatening consequences from their behavior, which—when handled skillfully in the emergency room—can start them on the road to recovery. Some say the addict must “hit bottom” before making the changes necessary for a sober life. You can help the addict define his or her bottom as an unpleasant trip to the hospital—instead of death or loss of a job or spouse—by realistically assessing the physical consequences of continued drug or alcohol use (Table 1).
Emergencies related to alcohol or drug use accounted for 601,563 visits to U.S. emergency departments in 2000, according to the government-sponsored Drug Abuse Warning Network (DAWN).2 Alcohol in combination with any illegal or illicit drug accounted for 34% of emergency visits, cocaine for 29%, and heroin for 16%.
Mortality rates vary by region. In Los Angeles, for instance, heroin and cocaine each caused approximately the same number of deaths when compared with alcohol in combination (Figure).3 Most deaths (73%) were considered accidental/unexpected, with 19% coded as suicide. New York City showed similar percentages of deaths called accidental/unexpected, but heroin as the cause of death ran a distant fourth to cocaine alone, narcotic analgesics alone, and alcohol in combination.2
Addiction crises bring more than a half-million Americans to hospital emergency rooms each year (Box 1,Figure).2,3 This article describes teachable moments—suicide attempts, accidental overdose, intoxication, and withdrawal—that you can use to bundle acute treatment with referral for addiction treatment.
Suicide
Suicide is the addict’s most immediate life-threatening emergency. Psychiatric and addictive disorders often coexist,4 but some substances can trigger suicidal behavior even in the absence of another diagnosable psychiatric disorder. The addicted person who jumps off a roof, believing he can fly, may think perfectly clearly when not using crack cocaine.
Addiction to any substance greatly increases the risk for suicide. An alcohol-dependent person is 32 times more likely to commit suicide than the nonaddicted individual.5 And the suicidal addict often has the means to end his life when he feels most suicidal.
Figure DRUG-RELATED DEATHS IN LOS ANGELES, 20022
Diagnosing and treating suicidality require a high degree of vigilance for subtle clues of suicidal behavior. Because suicide risk has no pathognomonic signs, clinical judgment is required. Though addiction itself can be viewed as a slow form of suicide,6 signs that suggest an immediate threat to life include:
- the addict’s assertion that he intends to kill himself
- serious comorbid mental illness (psychosis, depression)7
- prior suicide attempts
- hopelessness.8
Some addicts feign suicidal thoughts or use them as a cry for help. Any mention or hint regarding suicide marks a severely disturbed patient who needs a complete psychiatric evaluation. This includes a formal mental status examination and exploring whether the patient has access to lethal means.
We cannot consistently predict our patients’ behavior, but a careful examination often reveals the seriousness of a suicidal threat, method, and intention, as well as support systems for keeping the patient safe. Consulting with a colleague can offer a “fresh look,” allowing two clinicians to balance the need for treatment against concerns such as bed availability and possible malingering.
Table 1
EMERGENCY AND LONG-TERM MEDICAL CONSEQUENCES OF ADDICTION
| Addictive substance | Intoxication symptoms | Withdrawal symptoms | Longer-term problems |
|---|---|---|---|
| Alcohol | Slowed respiration, impaired thinking and coordination, coma, death | Seizures, death | Dementia, liver damage |
| Barbiturates | Slowed respiration, impaired thinking and coordination, coma, death | Seizures | Rebound pain, hepatotoxicity |
| Benzodiazepines | Slowed respiration, impaired thinking and coordination | Seizures | |
| Hallucinogens | Paranoia, impaired thinking and coordination | Amotivational syndrome; possession is grounds for arrest | |
| MDMA(‘ecstasy’) | Impaired thinking and coordination, stroke, hyperthymia, dehydration, death | Cognitive impairment; possession is grounds for arrest | |
| Nicotine | Tachycardia, arrhythmia | Lung cancer, chronic-obstructive pulmonary disease | |
| Opiates | Slowed respiration, impaired thinking and coordination, coma, death | Skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Phencyclidine (PCP, ‘angel dust’) | Impaired thinking and coordination, violent behavior | Possession is grounds for arrest | |
| Stimulants | Impaired thinking and coordination, myocardial infarction, stroke | Nasal damage (if snorted); skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Inhalants | Impaired thinking and coordination, headache, coma | Neurologic damage |
Suicidal thoughts are unassailable grounds for comprehensive evaluation and treatment—regardless of the suicide evaluation’s outcome. The addict who even hints at suicide should undergo a thorough medical and psychiatric evaluation and then engage in whatever treatment is indicated.
Emphasize the seriousness of suicidal thoughts to the patient, his family, third-party payers, and whomever else has influence in bringing the patient to treatment. Suicidal behaviors or intentions remain one of the few legal justifications for involuntary hospitalization.
Accidental overdose
An accidental overdose provides another teachable moment to convince the addict to enter treatment. Patients who try to make a statement by overdosing on a substance they consider benign, such as oxycodone with acetaminophen, can inadvertently kill or badly injure themselves. Conversely, patients who clearly intend to harm themselves may misconstrue a substance’s lethality and ingest a large amount of a relatively nonlethal substance such as clonazepam. Either case:
- is a true psychiatric emergency
- bodes poorly for the patient’s future
- provides a strong rationale for addiction treatment.
Whether the means or the intent were deadly or benign, the overdose can be used as a convincing argument for treatment.
Intoxication
Intoxication with any addictive substance impairs judgment and increases the danger of injury. Specific medical dangers include alcohol’s powerful CNS depression in the nontolerant individual and the possibility for heart attack and stroke in the cocaine-intoxicated patient.
Attempts to convince an intoxicated person of the need for addiction treatment are usually futile. But the acute treatment represents a golden opportunity to reach out to friends and family members, who often escort the intoxicated addict to the emergency room. A medical record documenting the patient’s impaired behavior serves as evidence for (later) convincing the addict to go into treatment or for legal coercion of that treatment.
Table 2
MANAGING SYMPTOMS OF ALCOHOL WITHDRAWAL AND DELIRIUM TREMENS
| Alcohol withdrawal | Delirium tremens |
|---|---|
| Begins 4 hours to 2 days after cessation of alcohol or precipitous drop in blood alcohol level | Begins 1 to 2 days after cessation of alcohol or precipitous drop in blood alcohol level |
| Symptoms | Symptoms |
| Anxiety Agitation Tremor Autonomic instability Insomnia Confusion | Agitation Severe autonomic instability Seizure Severe confusion Hallucinations |
| Treatment Treatment of co-occurring medical illness Parenteral thiamine Tapering doses of CNS depressants, most often benzodiazepines | |
Withdrawal
Withdrawal, like intoxication, presents emergency conditions specific to the abused substance. Unlike the intoxicated patient, however, a patient experiencing the unpleasant symptoms of withdrawal may understand the need for addiction treatment. Because alcohol withdrawal often requires sedative/hypnotic treatment, the wise clinician can design a treatment plan that combines the anti-withdrawal medication with:
- attending Alcoholics Anonymous meetings
- taking disulfiram 12 hours after the last alcohol use and then daily
- and participation in relapse prevention psychotherapy.
Emergency treatments
Psychiatrists often have close contact with addicted patients in the hospital, clinic, or emergency department and therefore need to be familiar with basic techniques for managing addiction emergencies. Although addiction-trained psychiatrists manage emergencies at many institutions, general psychiatrists who have learned the following guidelines can form quick and solid therapeutic alliances with their addicted patients in the emergency department.
Alcohol
People live dangerously when intoxicated; about 40% of fatal U.S. car accidents involve a drunken driver.9 Alcohol also can incite physical violence and self-damaging sexual behavior and cause respiratory depression and death.
Acute effects of alcohol intoxication must be treated while guarding against potentially lethal withdrawal. Dangerous intoxication states with respiratory compromise may require aggressive supportive care, including intubation and mechanical ventilation. For agitated, intoxicated persons who represent a threat to themselves or others, chemical sedation with benzodiazepines—as opposed to physical restraint—is the preferred treatment.
Alcohol withdrawal requires immediate, definitive treatment (Table 2). Although mild withdrawal is common among alcoholics who cut back on or abruptly stop drinking, it can devolve quickly into delirium tremens (DTs). Serious medical problems—including severe autonomic instability and seizures—occur with DTs, which are associated with mortality rates of 5 to 15%.10 The adroit emergency department clinician can use the alcohol withdrawal/delirium episode to encourage the patient to begin addiction treatment (Box 2).11
Cocaine
Stimulants—most commonly cocaine and smoked methamphetamine—can cause myocardial infarction, cardiac arrhythmia, cerebral hemorrhage, hyperpyrexia, and status epilepticus.12 These emergencies occurring in a young person indicate the need to screen for cocaine use. Because no antidote exists for stimulant intoxication, we can only deliver supportive care while remaining vigilant for other sequelae of stimulant use, such as agitation and hypertension.13
Opiates
Overdoses leading to coma and death are the most devastating physical consequence of opiate abuse. Contrary to popular belief, orally ingested and inhaled opiates can depress respiration enough to cause death, just as injected opiates can. Because even appropriately prescribed opioid medications can lead to overdose or addiction, emergency treaters should be prepared to refer patients for pain management.
High-potency heroin often causes overdose in the novice user or in the addict who is surprised by a sudden increase in the heroin’s purity. Adulterants used by dealers to “cut” heroin also can cause illness and death. Quinine, for instance, can cause cardiac arrhythmias. Contaminants such as fentanyl and cholinergic agents such as scopolamine added to enhance the “high” associated with heroin can increase the risk of toxicity or death.
Opioid overdose is characterized by cyanosis and pulmonary edema: slowed breathing, altered mental status, blue lips and fingernail beds, pinpoint pupils, hypothermia, and gasping respirations. In addition to respiratory and cardiac support, treatment with the narcotic antagonist naloxone immediately reverses opioid overdose.
To what level of care should you refer the addicted patient from the emergency department—an inpatient medical unit, psychiatric unit/detoxification facility, residential treatment, partial hospitalization, or other model of care? The American Society of Addiction Medicine (ASAM) manual lists disposition recommendations to match individual patients’ clinical criteria. The criteria and levels are listed here as reminders of the issues involved in referring the addicted patient.
ASAM patient criteria
- Alcohol intoxication and/or withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Relapse, continued use, or continued problem potential
- Recovery environment
ASAM levels of care
- Early intervention
- Opioid maintenance therapy
- Outpatient treatment
- Intensive outpatient treatment
- Partial hospitalization
- Clinically managed low-intensity residential services
- Clinically managed high-intensity residential services
- Medically monitored intensive inpatient treatment
- Medically managed intensive inpatient treatment
Source: Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001:27-33.
Ecstasy
The drug 3,4-methylenedioxymethamphetamine (MDMA)—also known as Ecstasy, X, and XTC3 —provokes release of dopamine and serotonin into the synapse, causing a sense of blissful open-mindedness, closeness to others, and the ability to “break down (mental) barriers.”14 In the context of “rave” dance parties, MDMA also causes dehydration and hyperthermia, which can lead to rhabdomyolysis, kidney failure, and death.
Life-threatening consequences generally occur only when adequate water is unavailable to a group of intoxicated, dancing teenagers.15 The more common emergency presentations include sudden hypertension, tachycardia, vomiting, depersonalization, panic attacks, and psychosis.16
Immediate treatment includes restoration of normal fluid levels and body temperature, plus reassurance for the non-life-threatening, more common, presentations.
Phencyclidine
Phencyclidine (PCP) and its analogue ketamine—originally developed as anesthetic agents—are no longer used therapeutically because they can cause dissociation, anxiety, and even psychosis. Panic can change to hyperactive behavior, aggressiveness, and violent acts, so the first treatment goal must be to secure the safety of the intoxicated person and others. Chemical restraints such as benzodiazepines are preferred to physical restraints, although some situations may require physical restraint, at least initially.17
PCP affects memory, and often the user is unaware of the agent’s consequences unless he hears descriptions of his behavior from family and friends unfortunate enough to witness the intoxicated state. Coaching by emergency personnel can help the family confront the user with evidence that he needs treatment.
Barbiturates
Physicians prescribe barbiturates such as pentobarbital, phenobarbital, and secobarbital for pain, insomnia, alcohol withdrawal, and anxiety states. Although sometimes useful for acute pain, these drugs can also cause physical dependence, intoxication in overdose, withdrawal seizures, and rebound pain.18
The withdrawal associated with barbiturates—as with withdrawal from other CNS depressants such as alcohol and benzodiazepines—consists of autonomic hyperactivity, confusion, and occasionally seizures.
Overdose, often in combination with alcohol, accounts for most emergency presentations of barbiturate addiction. Supportive treatment—from reassurance and observation to airway support and mechanical ventilation—is required. Since obtundation and coma commonly occur with alcohol/barbiturate combinations, treatment includes monitoring for alcohol intoxication or withdrawal. No antidote exists for barbiturate intoxication.
Alternate medications. If the patient has become addicted to barbiturates prescribed for one of the common indications such as migraine headache, the emergency treater can promote use of a more effective treatment by acknowledging the need to control the headache pain. In managing this pain, the emergency worker can arrange referral:
- to an addiction specialist for treatment of the (now addictive) barbiturate use
- and to a neurologist who can evaluate the patient and prescribe one of many highly effective, nonaddicting headache remedies.
By taking the addiction and the pain seriously, the treater forms an alliance with the patient against the unhealthy consequences of both migraine headaches and addiction.
Benzodiazepines
Often prescribed for anxiety and insomnia, benzodiazepines cause emergency syndromes directly related to their potency, serum half-lives, and lipophilicity. For instance, alprazolam—which is potent, short-acting,19 and highly lipophilic—causes a severe withdrawal syndrome when high doses are stopped abruptly. This withdrawal state includes anxiety, agitation, and autonomic instability and can progress to frank seizures.
Withdrawal is treated by tapering the benzodiazepine dosage or substituting another benzodiazepine such as clonazepam. Benzodiazepine intoxication usually occurs only with large overdoses, although intoxication can last for days in a patient with hepatic disease. Lorazepam and oxazepam are not metabolized by the liver and can be prescribed to the patient in liver failure without causing an overdose.
Intoxication is usually treated with supportive measures and close observation for signs of withdrawal. Parenteral flumazenil immediately reverses benzodiazepine intoxication—which may assist both diagnosis and treatment—but its potential to cause seizures20 decreases this antagonist’s clinical usefulness.
Because benzodiazepine addiction often begins with prescribed medication, emergency department personnel can educate both patients and prescribers. Medications such as diazepam, lorazepam, and alprazolam are relatively safe short-term soporific agents, but use for more than a few weeks often leads to physical dependence and/or addiction. Emergency personnel can help the patient and prescriber switch to a treatment with fewer side effects and less danger of addiction.
Summary
Addicts do often change their destructive behavior when faced with increasing consequences such as job loss, relationship problems, financial difficulties, and physical deterioration. Emergencies related to drug and alcohol abuse can serve as learning experiences. Emergency department psychiatrists and other clinicians can use these crises as opportunities to help the addict:
- examine the consequences of substance use
- and change the destructive behaviors that lead to medical and social consequences.
Related resources
- American Academy of Addiction Psychiatry. www.aaap.org
- Galanter M, Kleber HD (eds). Textbook of substance abuse treatment (2nd ed). Washington, DC: American Psychiatric Press, 1999.
- Graham AW, Schultz TK (eds). Principles of addiction medicine (2nd ed). Chevy Chase, MD: American Society of Addiction Medicine, Inc., 1998.
- National Clearinghouse on Alcohol and Drug Issues. www.ncadi.org
Drug brand names
- Alprazolam • Xanax
- Diazepam • Valium
- Disulfiram • Antabuse
- Flumazenil • Romazicon
- Lorazepan • Ativan
- Oxazepam • Serax
- Secobarbital • Seconal
Disclosure
Dr. Westreich reports that he serves on the speakers’ bureaus of Pfizer Inc. and Bristol-Myers Squibb Company.
1. John F. Kennedy (speech). Indianapolis: April 12, 1959.
2. Office of Applied Studies Emergency department trends from the Drug Abuse Warning Network. Preliminary estimates, January-June 2001, with revised estimates, 1994-2000. Rockville, MD: Department of Health and Human Services, February 2002:40.
3. Office of Applied Studies. Mortality data from the Drug Abuse Warning Network, 2000. Rockville, MD: Department of Health and Human Services. January 2002:56-68.
4. Rosenthal RN, Westreich L. Treatment of persons with dual diagnoses of substance use disorder and other psychological problems. In: McCrady BS, Epstein EE (eds). Addictions: a comprehensive textbook. New York: Oxford University Press, 1999;439-76.
5. Sexia FA. Criteria for the diagnosis of alcoholism. In: Estes NJ, Heinemann ME (eds). Alcoholism: development, consequences and intervention. St. Louis: CV Mosby, 1982;49-66.
6. Menninger K. Man against himself. New York: Harcourt, Brace and World, 1938:147.
7. Hirschfeld RM. When to hospitalize the addict at risk for suicide. Ann NY Acad Sci 2001;932:188-96.
8. Malone KM, Oquendo MA, Haas GL, et al. Protective factors against suicidal acts in major depression: reasons for living. Am J Psychiatry 2000;157:1084-8.
9. Sixth Special Report to the United States Congress on Alcohol and Health Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1987.
10. Erwin WE, Williams DB, Speir WA. Delirium tremens. South Med J 1998;91(5):425-32.
11. Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001;27-33.
12. Weiss RD, Mirin SM, Bartell RL. Cocaine (2nd ed). Washington, DC: American Psychiatric Press, 1994;31-3.
13. Catravas JD, Waters IW, Walz MA, et al. Antidotes for cocaine poisoning. N Engl J Med 1977;301:1238.-
14. Stimmel B. Alcoholism, drug addiction, and the road to recovery. New York: Haworth Medical Press, 2002;142.-
15. Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine (“ecstasy”). Lancet 1992;340:384-7.
16. Cohen RS. The love drug: marching to the beat of ecstasy. Binghamton, NY: Haworth Medical Press, 1998.
17. Baldridge EB, Bessen HA. Phencyclidine. Emerg Med Clin North Am 1990;8(3):541-50.
18. Silberstein SD. Drug-induced headache. Neurol Clin North Am 1998;16(1):114.-
19. Arana G, Rosenbaum JF. Handbook of psychiatric drug therapy (4th ed). New York: Lippincott Williams & Wilkins; 2000;179.-
20. Roche Laboratories Romazicon (package insert).
Mrs. R, age 43, is agitated and confused, and her husband has brought her to the hospital’s emergency department. He reports that she has a history of denying alcohol abuse and told him during an argument yesterday that she could stop drinking any time she wanted to.
You are the psychiatrist on call. As the emergency medical team treats the apparent withdrawal episode, you tell Mrs. R’s husband: “We’ll take good care of your wife because alcohol withdrawal is dangerous and painful. But after detoxification, it’s important to prevent her from getting sick again. She needs to enter a rehabilitation program, and then outpatient treatment. When she comes around, maybe you could remind her about how much pain she was in and bring her to the rehab center yourself…”
Addicts face potentially life-threatening consequences from their behavior, which—when handled skillfully in the emergency room—can start them on the road to recovery. Some say the addict must “hit bottom” before making the changes necessary for a sober life. You can help the addict define his or her bottom as an unpleasant trip to the hospital—instead of death or loss of a job or spouse—by realistically assessing the physical consequences of continued drug or alcohol use (Table 1).
Emergencies related to alcohol or drug use accounted for 601,563 visits to U.S. emergency departments in 2000, according to the government-sponsored Drug Abuse Warning Network (DAWN).2 Alcohol in combination with any illegal or illicit drug accounted for 34% of emergency visits, cocaine for 29%, and heroin for 16%.
Mortality rates vary by region. In Los Angeles, for instance, heroin and cocaine each caused approximately the same number of deaths when compared with alcohol in combination (Figure).3 Most deaths (73%) were considered accidental/unexpected, with 19% coded as suicide. New York City showed similar percentages of deaths called accidental/unexpected, but heroin as the cause of death ran a distant fourth to cocaine alone, narcotic analgesics alone, and alcohol in combination.2
Addiction crises bring more than a half-million Americans to hospital emergency rooms each year (Box 1,Figure).2,3 This article describes teachable moments—suicide attempts, accidental overdose, intoxication, and withdrawal—that you can use to bundle acute treatment with referral for addiction treatment.
Suicide
Suicide is the addict’s most immediate life-threatening emergency. Psychiatric and addictive disorders often coexist,4 but some substances can trigger suicidal behavior even in the absence of another diagnosable psychiatric disorder. The addicted person who jumps off a roof, believing he can fly, may think perfectly clearly when not using crack cocaine.
Addiction to any substance greatly increases the risk for suicide. An alcohol-dependent person is 32 times more likely to commit suicide than the nonaddicted individual.5 And the suicidal addict often has the means to end his life when he feels most suicidal.
Figure DRUG-RELATED DEATHS IN LOS ANGELES, 20022
Diagnosing and treating suicidality require a high degree of vigilance for subtle clues of suicidal behavior. Because suicide risk has no pathognomonic signs, clinical judgment is required. Though addiction itself can be viewed as a slow form of suicide,6 signs that suggest an immediate threat to life include:
- the addict’s assertion that he intends to kill himself
- serious comorbid mental illness (psychosis, depression)7
- prior suicide attempts
- hopelessness.8
Some addicts feign suicidal thoughts or use them as a cry for help. Any mention or hint regarding suicide marks a severely disturbed patient who needs a complete psychiatric evaluation. This includes a formal mental status examination and exploring whether the patient has access to lethal means.
We cannot consistently predict our patients’ behavior, but a careful examination often reveals the seriousness of a suicidal threat, method, and intention, as well as support systems for keeping the patient safe. Consulting with a colleague can offer a “fresh look,” allowing two clinicians to balance the need for treatment against concerns such as bed availability and possible malingering.
Table 1
EMERGENCY AND LONG-TERM MEDICAL CONSEQUENCES OF ADDICTION
| Addictive substance | Intoxication symptoms | Withdrawal symptoms | Longer-term problems |
|---|---|---|---|
| Alcohol | Slowed respiration, impaired thinking and coordination, coma, death | Seizures, death | Dementia, liver damage |
| Barbiturates | Slowed respiration, impaired thinking and coordination, coma, death | Seizures | Rebound pain, hepatotoxicity |
| Benzodiazepines | Slowed respiration, impaired thinking and coordination | Seizures | |
| Hallucinogens | Paranoia, impaired thinking and coordination | Amotivational syndrome; possession is grounds for arrest | |
| MDMA(‘ecstasy’) | Impaired thinking and coordination, stroke, hyperthymia, dehydration, death | Cognitive impairment; possession is grounds for arrest | |
| Nicotine | Tachycardia, arrhythmia | Lung cancer, chronic-obstructive pulmonary disease | |
| Opiates | Slowed respiration, impaired thinking and coordination, coma, death | Skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Phencyclidine (PCP, ‘angel dust’) | Impaired thinking and coordination, violent behavior | Possession is grounds for arrest | |
| Stimulants | Impaired thinking and coordination, myocardial infarction, stroke | Nasal damage (if snorted); skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Inhalants | Impaired thinking and coordination, headache, coma | Neurologic damage |
Suicidal thoughts are unassailable grounds for comprehensive evaluation and treatment—regardless of the suicide evaluation’s outcome. The addict who even hints at suicide should undergo a thorough medical and psychiatric evaluation and then engage in whatever treatment is indicated.
Emphasize the seriousness of suicidal thoughts to the patient, his family, third-party payers, and whomever else has influence in bringing the patient to treatment. Suicidal behaviors or intentions remain one of the few legal justifications for involuntary hospitalization.
Accidental overdose
An accidental overdose provides another teachable moment to convince the addict to enter treatment. Patients who try to make a statement by overdosing on a substance they consider benign, such as oxycodone with acetaminophen, can inadvertently kill or badly injure themselves. Conversely, patients who clearly intend to harm themselves may misconstrue a substance’s lethality and ingest a large amount of a relatively nonlethal substance such as clonazepam. Either case:
- is a true psychiatric emergency
- bodes poorly for the patient’s future
- provides a strong rationale for addiction treatment.
Whether the means or the intent were deadly or benign, the overdose can be used as a convincing argument for treatment.
Intoxication
Intoxication with any addictive substance impairs judgment and increases the danger of injury. Specific medical dangers include alcohol’s powerful CNS depression in the nontolerant individual and the possibility for heart attack and stroke in the cocaine-intoxicated patient.
Attempts to convince an intoxicated person of the need for addiction treatment are usually futile. But the acute treatment represents a golden opportunity to reach out to friends and family members, who often escort the intoxicated addict to the emergency room. A medical record documenting the patient’s impaired behavior serves as evidence for (later) convincing the addict to go into treatment or for legal coercion of that treatment.
Table 2
MANAGING SYMPTOMS OF ALCOHOL WITHDRAWAL AND DELIRIUM TREMENS
| Alcohol withdrawal | Delirium tremens |
|---|---|
| Begins 4 hours to 2 days after cessation of alcohol or precipitous drop in blood alcohol level | Begins 1 to 2 days after cessation of alcohol or precipitous drop in blood alcohol level |
| Symptoms | Symptoms |
| Anxiety Agitation Tremor Autonomic instability Insomnia Confusion | Agitation Severe autonomic instability Seizure Severe confusion Hallucinations |
| Treatment Treatment of co-occurring medical illness Parenteral thiamine Tapering doses of CNS depressants, most often benzodiazepines | |
Withdrawal
Withdrawal, like intoxication, presents emergency conditions specific to the abused substance. Unlike the intoxicated patient, however, a patient experiencing the unpleasant symptoms of withdrawal may understand the need for addiction treatment. Because alcohol withdrawal often requires sedative/hypnotic treatment, the wise clinician can design a treatment plan that combines the anti-withdrawal medication with:
- attending Alcoholics Anonymous meetings
- taking disulfiram 12 hours after the last alcohol use and then daily
- and participation in relapse prevention psychotherapy.
Emergency treatments
Psychiatrists often have close contact with addicted patients in the hospital, clinic, or emergency department and therefore need to be familiar with basic techniques for managing addiction emergencies. Although addiction-trained psychiatrists manage emergencies at many institutions, general psychiatrists who have learned the following guidelines can form quick and solid therapeutic alliances with their addicted patients in the emergency department.
Alcohol
People live dangerously when intoxicated; about 40% of fatal U.S. car accidents involve a drunken driver.9 Alcohol also can incite physical violence and self-damaging sexual behavior and cause respiratory depression and death.
Acute effects of alcohol intoxication must be treated while guarding against potentially lethal withdrawal. Dangerous intoxication states with respiratory compromise may require aggressive supportive care, including intubation and mechanical ventilation. For agitated, intoxicated persons who represent a threat to themselves or others, chemical sedation with benzodiazepines—as opposed to physical restraint—is the preferred treatment.
Alcohol withdrawal requires immediate, definitive treatment (Table 2). Although mild withdrawal is common among alcoholics who cut back on or abruptly stop drinking, it can devolve quickly into delirium tremens (DTs). Serious medical problems—including severe autonomic instability and seizures—occur with DTs, which are associated with mortality rates of 5 to 15%.10 The adroit emergency department clinician can use the alcohol withdrawal/delirium episode to encourage the patient to begin addiction treatment (Box 2).11
Cocaine
Stimulants—most commonly cocaine and smoked methamphetamine—can cause myocardial infarction, cardiac arrhythmia, cerebral hemorrhage, hyperpyrexia, and status epilepticus.12 These emergencies occurring in a young person indicate the need to screen for cocaine use. Because no antidote exists for stimulant intoxication, we can only deliver supportive care while remaining vigilant for other sequelae of stimulant use, such as agitation and hypertension.13
Opiates
Overdoses leading to coma and death are the most devastating physical consequence of opiate abuse. Contrary to popular belief, orally ingested and inhaled opiates can depress respiration enough to cause death, just as injected opiates can. Because even appropriately prescribed opioid medications can lead to overdose or addiction, emergency treaters should be prepared to refer patients for pain management.
High-potency heroin often causes overdose in the novice user or in the addict who is surprised by a sudden increase in the heroin’s purity. Adulterants used by dealers to “cut” heroin also can cause illness and death. Quinine, for instance, can cause cardiac arrhythmias. Contaminants such as fentanyl and cholinergic agents such as scopolamine added to enhance the “high” associated with heroin can increase the risk of toxicity or death.
Opioid overdose is characterized by cyanosis and pulmonary edema: slowed breathing, altered mental status, blue lips and fingernail beds, pinpoint pupils, hypothermia, and gasping respirations. In addition to respiratory and cardiac support, treatment with the narcotic antagonist naloxone immediately reverses opioid overdose.
To what level of care should you refer the addicted patient from the emergency department—an inpatient medical unit, psychiatric unit/detoxification facility, residential treatment, partial hospitalization, or other model of care? The American Society of Addiction Medicine (ASAM) manual lists disposition recommendations to match individual patients’ clinical criteria. The criteria and levels are listed here as reminders of the issues involved in referring the addicted patient.
ASAM patient criteria
- Alcohol intoxication and/or withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Relapse, continued use, or continued problem potential
- Recovery environment
ASAM levels of care
- Early intervention
- Opioid maintenance therapy
- Outpatient treatment
- Intensive outpatient treatment
- Partial hospitalization
- Clinically managed low-intensity residential services
- Clinically managed high-intensity residential services
- Medically monitored intensive inpatient treatment
- Medically managed intensive inpatient treatment
Source: Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001:27-33.
Ecstasy
The drug 3,4-methylenedioxymethamphetamine (MDMA)—also known as Ecstasy, X, and XTC3 —provokes release of dopamine and serotonin into the synapse, causing a sense of blissful open-mindedness, closeness to others, and the ability to “break down (mental) barriers.”14 In the context of “rave” dance parties, MDMA also causes dehydration and hyperthermia, which can lead to rhabdomyolysis, kidney failure, and death.
Life-threatening consequences generally occur only when adequate water is unavailable to a group of intoxicated, dancing teenagers.15 The more common emergency presentations include sudden hypertension, tachycardia, vomiting, depersonalization, panic attacks, and psychosis.16
Immediate treatment includes restoration of normal fluid levels and body temperature, plus reassurance for the non-life-threatening, more common, presentations.
Phencyclidine
Phencyclidine (PCP) and its analogue ketamine—originally developed as anesthetic agents—are no longer used therapeutically because they can cause dissociation, anxiety, and even psychosis. Panic can change to hyperactive behavior, aggressiveness, and violent acts, so the first treatment goal must be to secure the safety of the intoxicated person and others. Chemical restraints such as benzodiazepines are preferred to physical restraints, although some situations may require physical restraint, at least initially.17
PCP affects memory, and often the user is unaware of the agent’s consequences unless he hears descriptions of his behavior from family and friends unfortunate enough to witness the intoxicated state. Coaching by emergency personnel can help the family confront the user with evidence that he needs treatment.
Barbiturates
Physicians prescribe barbiturates such as pentobarbital, phenobarbital, and secobarbital for pain, insomnia, alcohol withdrawal, and anxiety states. Although sometimes useful for acute pain, these drugs can also cause physical dependence, intoxication in overdose, withdrawal seizures, and rebound pain.18
The withdrawal associated with barbiturates—as with withdrawal from other CNS depressants such as alcohol and benzodiazepines—consists of autonomic hyperactivity, confusion, and occasionally seizures.
Overdose, often in combination with alcohol, accounts for most emergency presentations of barbiturate addiction. Supportive treatment—from reassurance and observation to airway support and mechanical ventilation—is required. Since obtundation and coma commonly occur with alcohol/barbiturate combinations, treatment includes monitoring for alcohol intoxication or withdrawal. No antidote exists for barbiturate intoxication.
Alternate medications. If the patient has become addicted to barbiturates prescribed for one of the common indications such as migraine headache, the emergency treater can promote use of a more effective treatment by acknowledging the need to control the headache pain. In managing this pain, the emergency worker can arrange referral:
- to an addiction specialist for treatment of the (now addictive) barbiturate use
- and to a neurologist who can evaluate the patient and prescribe one of many highly effective, nonaddicting headache remedies.
By taking the addiction and the pain seriously, the treater forms an alliance with the patient against the unhealthy consequences of both migraine headaches and addiction.
Benzodiazepines
Often prescribed for anxiety and insomnia, benzodiazepines cause emergency syndromes directly related to their potency, serum half-lives, and lipophilicity. For instance, alprazolam—which is potent, short-acting,19 and highly lipophilic—causes a severe withdrawal syndrome when high doses are stopped abruptly. This withdrawal state includes anxiety, agitation, and autonomic instability and can progress to frank seizures.
Withdrawal is treated by tapering the benzodiazepine dosage or substituting another benzodiazepine such as clonazepam. Benzodiazepine intoxication usually occurs only with large overdoses, although intoxication can last for days in a patient with hepatic disease. Lorazepam and oxazepam are not metabolized by the liver and can be prescribed to the patient in liver failure without causing an overdose.
Intoxication is usually treated with supportive measures and close observation for signs of withdrawal. Parenteral flumazenil immediately reverses benzodiazepine intoxication—which may assist both diagnosis and treatment—but its potential to cause seizures20 decreases this antagonist’s clinical usefulness.
Because benzodiazepine addiction often begins with prescribed medication, emergency department personnel can educate both patients and prescribers. Medications such as diazepam, lorazepam, and alprazolam are relatively safe short-term soporific agents, but use for more than a few weeks often leads to physical dependence and/or addiction. Emergency personnel can help the patient and prescriber switch to a treatment with fewer side effects and less danger of addiction.
Summary
Addicts do often change their destructive behavior when faced with increasing consequences such as job loss, relationship problems, financial difficulties, and physical deterioration. Emergencies related to drug and alcohol abuse can serve as learning experiences. Emergency department psychiatrists and other clinicians can use these crises as opportunities to help the addict:
- examine the consequences of substance use
- and change the destructive behaviors that lead to medical and social consequences.
Related resources
- American Academy of Addiction Psychiatry. www.aaap.org
- Galanter M, Kleber HD (eds). Textbook of substance abuse treatment (2nd ed). Washington, DC: American Psychiatric Press, 1999.
- Graham AW, Schultz TK (eds). Principles of addiction medicine (2nd ed). Chevy Chase, MD: American Society of Addiction Medicine, Inc., 1998.
- National Clearinghouse on Alcohol and Drug Issues. www.ncadi.org
Drug brand names
- Alprazolam • Xanax
- Diazepam • Valium
- Disulfiram • Antabuse
- Flumazenil • Romazicon
- Lorazepan • Ativan
- Oxazepam • Serax
- Secobarbital • Seconal
Disclosure
Dr. Westreich reports that he serves on the speakers’ bureaus of Pfizer Inc. and Bristol-Myers Squibb Company.
Mrs. R, age 43, is agitated and confused, and her husband has brought her to the hospital’s emergency department. He reports that she has a history of denying alcohol abuse and told him during an argument yesterday that she could stop drinking any time she wanted to.
You are the psychiatrist on call. As the emergency medical team treats the apparent withdrawal episode, you tell Mrs. R’s husband: “We’ll take good care of your wife because alcohol withdrawal is dangerous and painful. But after detoxification, it’s important to prevent her from getting sick again. She needs to enter a rehabilitation program, and then outpatient treatment. When she comes around, maybe you could remind her about how much pain she was in and bring her to the rehab center yourself…”
Addicts face potentially life-threatening consequences from their behavior, which—when handled skillfully in the emergency room—can start them on the road to recovery. Some say the addict must “hit bottom” before making the changes necessary for a sober life. You can help the addict define his or her bottom as an unpleasant trip to the hospital—instead of death or loss of a job or spouse—by realistically assessing the physical consequences of continued drug or alcohol use (Table 1).
Emergencies related to alcohol or drug use accounted for 601,563 visits to U.S. emergency departments in 2000, according to the government-sponsored Drug Abuse Warning Network (DAWN).2 Alcohol in combination with any illegal or illicit drug accounted for 34% of emergency visits, cocaine for 29%, and heroin for 16%.
Mortality rates vary by region. In Los Angeles, for instance, heroin and cocaine each caused approximately the same number of deaths when compared with alcohol in combination (Figure).3 Most deaths (73%) were considered accidental/unexpected, with 19% coded as suicide. New York City showed similar percentages of deaths called accidental/unexpected, but heroin as the cause of death ran a distant fourth to cocaine alone, narcotic analgesics alone, and alcohol in combination.2
Addiction crises bring more than a half-million Americans to hospital emergency rooms each year (Box 1,Figure).2,3 This article describes teachable moments—suicide attempts, accidental overdose, intoxication, and withdrawal—that you can use to bundle acute treatment with referral for addiction treatment.
Suicide
Suicide is the addict’s most immediate life-threatening emergency. Psychiatric and addictive disorders often coexist,4 but some substances can trigger suicidal behavior even in the absence of another diagnosable psychiatric disorder. The addicted person who jumps off a roof, believing he can fly, may think perfectly clearly when not using crack cocaine.
Addiction to any substance greatly increases the risk for suicide. An alcohol-dependent person is 32 times more likely to commit suicide than the nonaddicted individual.5 And the suicidal addict often has the means to end his life when he feels most suicidal.
Figure DRUG-RELATED DEATHS IN LOS ANGELES, 20022
Diagnosing and treating suicidality require a high degree of vigilance for subtle clues of suicidal behavior. Because suicide risk has no pathognomonic signs, clinical judgment is required. Though addiction itself can be viewed as a slow form of suicide,6 signs that suggest an immediate threat to life include:
- the addict’s assertion that he intends to kill himself
- serious comorbid mental illness (psychosis, depression)7
- prior suicide attempts
- hopelessness.8
Some addicts feign suicidal thoughts or use them as a cry for help. Any mention or hint regarding suicide marks a severely disturbed patient who needs a complete psychiatric evaluation. This includes a formal mental status examination and exploring whether the patient has access to lethal means.
We cannot consistently predict our patients’ behavior, but a careful examination often reveals the seriousness of a suicidal threat, method, and intention, as well as support systems for keeping the patient safe. Consulting with a colleague can offer a “fresh look,” allowing two clinicians to balance the need for treatment against concerns such as bed availability and possible malingering.
Table 1
EMERGENCY AND LONG-TERM MEDICAL CONSEQUENCES OF ADDICTION
| Addictive substance | Intoxication symptoms | Withdrawal symptoms | Longer-term problems |
|---|---|---|---|
| Alcohol | Slowed respiration, impaired thinking and coordination, coma, death | Seizures, death | Dementia, liver damage |
| Barbiturates | Slowed respiration, impaired thinking and coordination, coma, death | Seizures | Rebound pain, hepatotoxicity |
| Benzodiazepines | Slowed respiration, impaired thinking and coordination | Seizures | |
| Hallucinogens | Paranoia, impaired thinking and coordination | Amotivational syndrome; possession is grounds for arrest | |
| MDMA(‘ecstasy’) | Impaired thinking and coordination, stroke, hyperthymia, dehydration, death | Cognitive impairment; possession is grounds for arrest | |
| Nicotine | Tachycardia, arrhythmia | Lung cancer, chronic-obstructive pulmonary disease | |
| Opiates | Slowed respiration, impaired thinking and coordination, coma, death | Skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Phencyclidine (PCP, ‘angel dust’) | Impaired thinking and coordination, violent behavior | Possession is grounds for arrest | |
| Stimulants | Impaired thinking and coordination, myocardial infarction, stroke | Nasal damage (if snorted); skin infections, HIV, hepatitis (if injected); possession is grounds for arrest | |
| Inhalants | Impaired thinking and coordination, headache, coma | Neurologic damage |
Suicidal thoughts are unassailable grounds for comprehensive evaluation and treatment—regardless of the suicide evaluation’s outcome. The addict who even hints at suicide should undergo a thorough medical and psychiatric evaluation and then engage in whatever treatment is indicated.
Emphasize the seriousness of suicidal thoughts to the patient, his family, third-party payers, and whomever else has influence in bringing the patient to treatment. Suicidal behaviors or intentions remain one of the few legal justifications for involuntary hospitalization.
Accidental overdose
An accidental overdose provides another teachable moment to convince the addict to enter treatment. Patients who try to make a statement by overdosing on a substance they consider benign, such as oxycodone with acetaminophen, can inadvertently kill or badly injure themselves. Conversely, patients who clearly intend to harm themselves may misconstrue a substance’s lethality and ingest a large amount of a relatively nonlethal substance such as clonazepam. Either case:
- is a true psychiatric emergency
- bodes poorly for the patient’s future
- provides a strong rationale for addiction treatment.
Whether the means or the intent were deadly or benign, the overdose can be used as a convincing argument for treatment.
Intoxication
Intoxication with any addictive substance impairs judgment and increases the danger of injury. Specific medical dangers include alcohol’s powerful CNS depression in the nontolerant individual and the possibility for heart attack and stroke in the cocaine-intoxicated patient.
Attempts to convince an intoxicated person of the need for addiction treatment are usually futile. But the acute treatment represents a golden opportunity to reach out to friends and family members, who often escort the intoxicated addict to the emergency room. A medical record documenting the patient’s impaired behavior serves as evidence for (later) convincing the addict to go into treatment or for legal coercion of that treatment.
Table 2
MANAGING SYMPTOMS OF ALCOHOL WITHDRAWAL AND DELIRIUM TREMENS
| Alcohol withdrawal | Delirium tremens |
|---|---|
| Begins 4 hours to 2 days after cessation of alcohol or precipitous drop in blood alcohol level | Begins 1 to 2 days after cessation of alcohol or precipitous drop in blood alcohol level |
| Symptoms | Symptoms |
| Anxiety Agitation Tremor Autonomic instability Insomnia Confusion | Agitation Severe autonomic instability Seizure Severe confusion Hallucinations |
| Treatment Treatment of co-occurring medical illness Parenteral thiamine Tapering doses of CNS depressants, most often benzodiazepines | |
Withdrawal
Withdrawal, like intoxication, presents emergency conditions specific to the abused substance. Unlike the intoxicated patient, however, a patient experiencing the unpleasant symptoms of withdrawal may understand the need for addiction treatment. Because alcohol withdrawal often requires sedative/hypnotic treatment, the wise clinician can design a treatment plan that combines the anti-withdrawal medication with:
- attending Alcoholics Anonymous meetings
- taking disulfiram 12 hours after the last alcohol use and then daily
- and participation in relapse prevention psychotherapy.
Emergency treatments
Psychiatrists often have close contact with addicted patients in the hospital, clinic, or emergency department and therefore need to be familiar with basic techniques for managing addiction emergencies. Although addiction-trained psychiatrists manage emergencies at many institutions, general psychiatrists who have learned the following guidelines can form quick and solid therapeutic alliances with their addicted patients in the emergency department.
Alcohol
People live dangerously when intoxicated; about 40% of fatal U.S. car accidents involve a drunken driver.9 Alcohol also can incite physical violence and self-damaging sexual behavior and cause respiratory depression and death.
Acute effects of alcohol intoxication must be treated while guarding against potentially lethal withdrawal. Dangerous intoxication states with respiratory compromise may require aggressive supportive care, including intubation and mechanical ventilation. For agitated, intoxicated persons who represent a threat to themselves or others, chemical sedation with benzodiazepines—as opposed to physical restraint—is the preferred treatment.
Alcohol withdrawal requires immediate, definitive treatment (Table 2). Although mild withdrawal is common among alcoholics who cut back on or abruptly stop drinking, it can devolve quickly into delirium tremens (DTs). Serious medical problems—including severe autonomic instability and seizures—occur with DTs, which are associated with mortality rates of 5 to 15%.10 The adroit emergency department clinician can use the alcohol withdrawal/delirium episode to encourage the patient to begin addiction treatment (Box 2).11
Cocaine
Stimulants—most commonly cocaine and smoked methamphetamine—can cause myocardial infarction, cardiac arrhythmia, cerebral hemorrhage, hyperpyrexia, and status epilepticus.12 These emergencies occurring in a young person indicate the need to screen for cocaine use. Because no antidote exists for stimulant intoxication, we can only deliver supportive care while remaining vigilant for other sequelae of stimulant use, such as agitation and hypertension.13
Opiates
Overdoses leading to coma and death are the most devastating physical consequence of opiate abuse. Contrary to popular belief, orally ingested and inhaled opiates can depress respiration enough to cause death, just as injected opiates can. Because even appropriately prescribed opioid medications can lead to overdose or addiction, emergency treaters should be prepared to refer patients for pain management.
High-potency heroin often causes overdose in the novice user or in the addict who is surprised by a sudden increase in the heroin’s purity. Adulterants used by dealers to “cut” heroin also can cause illness and death. Quinine, for instance, can cause cardiac arrhythmias. Contaminants such as fentanyl and cholinergic agents such as scopolamine added to enhance the “high” associated with heroin can increase the risk of toxicity or death.
Opioid overdose is characterized by cyanosis and pulmonary edema: slowed breathing, altered mental status, blue lips and fingernail beds, pinpoint pupils, hypothermia, and gasping respirations. In addition to respiratory and cardiac support, treatment with the narcotic antagonist naloxone immediately reverses opioid overdose.
To what level of care should you refer the addicted patient from the emergency department—an inpatient medical unit, psychiatric unit/detoxification facility, residential treatment, partial hospitalization, or other model of care? The American Society of Addiction Medicine (ASAM) manual lists disposition recommendations to match individual patients’ clinical criteria. The criteria and levels are listed here as reminders of the issues involved in referring the addicted patient.
ASAM patient criteria
- Alcohol intoxication and/or withdrawal potential
- Biomedical conditions and complications
- Emotional, behavioral, or cognitive conditions and complications
- Readiness to change
- Relapse, continued use, or continued problem potential
- Recovery environment
ASAM levels of care
- Early intervention
- Opioid maintenance therapy
- Outpatient treatment
- Intensive outpatient treatment
- Partial hospitalization
- Clinically managed low-intensity residential services
- Clinically managed high-intensity residential services
- Medically monitored intensive inpatient treatment
- Medically managed intensive inpatient treatment
Source: Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001:27-33.
Ecstasy
The drug 3,4-methylenedioxymethamphetamine (MDMA)—also known as Ecstasy, X, and XTC3 —provokes release of dopamine and serotonin into the synapse, causing a sense of blissful open-mindedness, closeness to others, and the ability to “break down (mental) barriers.”14 In the context of “rave” dance parties, MDMA also causes dehydration and hyperthermia, which can lead to rhabdomyolysis, kidney failure, and death.
Life-threatening consequences generally occur only when adequate water is unavailable to a group of intoxicated, dancing teenagers.15 The more common emergency presentations include sudden hypertension, tachycardia, vomiting, depersonalization, panic attacks, and psychosis.16
Immediate treatment includes restoration of normal fluid levels and body temperature, plus reassurance for the non-life-threatening, more common, presentations.
Phencyclidine
Phencyclidine (PCP) and its analogue ketamine—originally developed as anesthetic agents—are no longer used therapeutically because they can cause dissociation, anxiety, and even psychosis. Panic can change to hyperactive behavior, aggressiveness, and violent acts, so the first treatment goal must be to secure the safety of the intoxicated person and others. Chemical restraints such as benzodiazepines are preferred to physical restraints, although some situations may require physical restraint, at least initially.17
PCP affects memory, and often the user is unaware of the agent’s consequences unless he hears descriptions of his behavior from family and friends unfortunate enough to witness the intoxicated state. Coaching by emergency personnel can help the family confront the user with evidence that he needs treatment.
Barbiturates
Physicians prescribe barbiturates such as pentobarbital, phenobarbital, and secobarbital for pain, insomnia, alcohol withdrawal, and anxiety states. Although sometimes useful for acute pain, these drugs can also cause physical dependence, intoxication in overdose, withdrawal seizures, and rebound pain.18
The withdrawal associated with barbiturates—as with withdrawal from other CNS depressants such as alcohol and benzodiazepines—consists of autonomic hyperactivity, confusion, and occasionally seizures.
Overdose, often in combination with alcohol, accounts for most emergency presentations of barbiturate addiction. Supportive treatment—from reassurance and observation to airway support and mechanical ventilation—is required. Since obtundation and coma commonly occur with alcohol/barbiturate combinations, treatment includes monitoring for alcohol intoxication or withdrawal. No antidote exists for barbiturate intoxication.
Alternate medications. If the patient has become addicted to barbiturates prescribed for one of the common indications such as migraine headache, the emergency treater can promote use of a more effective treatment by acknowledging the need to control the headache pain. In managing this pain, the emergency worker can arrange referral:
- to an addiction specialist for treatment of the (now addictive) barbiturate use
- and to a neurologist who can evaluate the patient and prescribe one of many highly effective, nonaddicting headache remedies.
By taking the addiction and the pain seriously, the treater forms an alliance with the patient against the unhealthy consequences of both migraine headaches and addiction.
Benzodiazepines
Often prescribed for anxiety and insomnia, benzodiazepines cause emergency syndromes directly related to their potency, serum half-lives, and lipophilicity. For instance, alprazolam—which is potent, short-acting,19 and highly lipophilic—causes a severe withdrawal syndrome when high doses are stopped abruptly. This withdrawal state includes anxiety, agitation, and autonomic instability and can progress to frank seizures.
Withdrawal is treated by tapering the benzodiazepine dosage or substituting another benzodiazepine such as clonazepam. Benzodiazepine intoxication usually occurs only with large overdoses, although intoxication can last for days in a patient with hepatic disease. Lorazepam and oxazepam are not metabolized by the liver and can be prescribed to the patient in liver failure without causing an overdose.
Intoxication is usually treated with supportive measures and close observation for signs of withdrawal. Parenteral flumazenil immediately reverses benzodiazepine intoxication—which may assist both diagnosis and treatment—but its potential to cause seizures20 decreases this antagonist’s clinical usefulness.
Because benzodiazepine addiction often begins with prescribed medication, emergency department personnel can educate both patients and prescribers. Medications such as diazepam, lorazepam, and alprazolam are relatively safe short-term soporific agents, but use for more than a few weeks often leads to physical dependence and/or addiction. Emergency personnel can help the patient and prescriber switch to a treatment with fewer side effects and less danger of addiction.
Summary
Addicts do often change their destructive behavior when faced with increasing consequences such as job loss, relationship problems, financial difficulties, and physical deterioration. Emergencies related to drug and alcohol abuse can serve as learning experiences. Emergency department psychiatrists and other clinicians can use these crises as opportunities to help the addict:
- examine the consequences of substance use
- and change the destructive behaviors that lead to medical and social consequences.
Related resources
- American Academy of Addiction Psychiatry. www.aaap.org
- Galanter M, Kleber HD (eds). Textbook of substance abuse treatment (2nd ed). Washington, DC: American Psychiatric Press, 1999.
- Graham AW, Schultz TK (eds). Principles of addiction medicine (2nd ed). Chevy Chase, MD: American Society of Addiction Medicine, Inc., 1998.
- National Clearinghouse on Alcohol and Drug Issues. www.ncadi.org
Drug brand names
- Alprazolam • Xanax
- Diazepam • Valium
- Disulfiram • Antabuse
- Flumazenil • Romazicon
- Lorazepan • Ativan
- Oxazepam • Serax
- Secobarbital • Seconal
Disclosure
Dr. Westreich reports that he serves on the speakers’ bureaus of Pfizer Inc. and Bristol-Myers Squibb Company.
1. John F. Kennedy (speech). Indianapolis: April 12, 1959.
2. Office of Applied Studies Emergency department trends from the Drug Abuse Warning Network. Preliminary estimates, January-June 2001, with revised estimates, 1994-2000. Rockville, MD: Department of Health and Human Services, February 2002:40.
3. Office of Applied Studies. Mortality data from the Drug Abuse Warning Network, 2000. Rockville, MD: Department of Health and Human Services. January 2002:56-68.
4. Rosenthal RN, Westreich L. Treatment of persons with dual diagnoses of substance use disorder and other psychological problems. In: McCrady BS, Epstein EE (eds). Addictions: a comprehensive textbook. New York: Oxford University Press, 1999;439-76.
5. Sexia FA. Criteria for the diagnosis of alcoholism. In: Estes NJ, Heinemann ME (eds). Alcoholism: development, consequences and intervention. St. Louis: CV Mosby, 1982;49-66.
6. Menninger K. Man against himself. New York: Harcourt, Brace and World, 1938:147.
7. Hirschfeld RM. When to hospitalize the addict at risk for suicide. Ann NY Acad Sci 2001;932:188-96.
8. Malone KM, Oquendo MA, Haas GL, et al. Protective factors against suicidal acts in major depression: reasons for living. Am J Psychiatry 2000;157:1084-8.
9. Sixth Special Report to the United States Congress on Alcohol and Health Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1987.
10. Erwin WE, Williams DB, Speir WA. Delirium tremens. South Med J 1998;91(5):425-32.
11. Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001;27-33.
12. Weiss RD, Mirin SM, Bartell RL. Cocaine (2nd ed). Washington, DC: American Psychiatric Press, 1994;31-3.
13. Catravas JD, Waters IW, Walz MA, et al. Antidotes for cocaine poisoning. N Engl J Med 1977;301:1238.-
14. Stimmel B. Alcoholism, drug addiction, and the road to recovery. New York: Haworth Medical Press, 2002;142.-
15. Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine (“ecstasy”). Lancet 1992;340:384-7.
16. Cohen RS. The love drug: marching to the beat of ecstasy. Binghamton, NY: Haworth Medical Press, 1998.
17. Baldridge EB, Bessen HA. Phencyclidine. Emerg Med Clin North Am 1990;8(3):541-50.
18. Silberstein SD. Drug-induced headache. Neurol Clin North Am 1998;16(1):114.-
19. Arana G, Rosenbaum JF. Handbook of psychiatric drug therapy (4th ed). New York: Lippincott Williams & Wilkins; 2000;179.-
20. Roche Laboratories Romazicon (package insert).
1. John F. Kennedy (speech). Indianapolis: April 12, 1959.
2. Office of Applied Studies Emergency department trends from the Drug Abuse Warning Network. Preliminary estimates, January-June 2001, with revised estimates, 1994-2000. Rockville, MD: Department of Health and Human Services, February 2002:40.
3. Office of Applied Studies. Mortality data from the Drug Abuse Warning Network, 2000. Rockville, MD: Department of Health and Human Services. January 2002:56-68.
4. Rosenthal RN, Westreich L. Treatment of persons with dual diagnoses of substance use disorder and other psychological problems. In: McCrady BS, Epstein EE (eds). Addictions: a comprehensive textbook. New York: Oxford University Press, 1999;439-76.
5. Sexia FA. Criteria for the diagnosis of alcoholism. In: Estes NJ, Heinemann ME (eds). Alcoholism: development, consequences and intervention. St. Louis: CV Mosby, 1982;49-66.
6. Menninger K. Man against himself. New York: Harcourt, Brace and World, 1938:147.
7. Hirschfeld RM. When to hospitalize the addict at risk for suicide. Ann NY Acad Sci 2001;932:188-96.
8. Malone KM, Oquendo MA, Haas GL, et al. Protective factors against suicidal acts in major depression: reasons for living. Am J Psychiatry 2000;157:1084-8.
9. Sixth Special Report to the United States Congress on Alcohol and Health Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, 1987.
10. Erwin WE, Williams DB, Speir WA. Delirium tremens. South Med J 1998;91(5):425-32.
11. Mee-Lee D, Shulman GD, Fishman M, et al. ASAM patient placement criteria for the treatment of substance-related disorders (2nd ed, rev). Chevy Chase, MD: American Society of Addiction Medicine, 2001;27-33.
12. Weiss RD, Mirin SM, Bartell RL. Cocaine (2nd ed). Washington, DC: American Psychiatric Press, 1994;31-3.
13. Catravas JD, Waters IW, Walz MA, et al. Antidotes for cocaine poisoning. N Engl J Med 1977;301:1238.-
14. Stimmel B. Alcoholism, drug addiction, and the road to recovery. New York: Haworth Medical Press, 2002;142.-
15. Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from 3,4 methylenedioxymethamphetamine (“ecstasy”). Lancet 1992;340:384-7.
16. Cohen RS. The love drug: marching to the beat of ecstasy. Binghamton, NY: Haworth Medical Press, 1998.
17. Baldridge EB, Bessen HA. Phencyclidine. Emerg Med Clin North Am 1990;8(3):541-50.
18. Silberstein SD. Drug-induced headache. Neurol Clin North Am 1998;16(1):114.-
19. Arana G, Rosenbaum JF. Handbook of psychiatric drug therapy (4th ed). New York: Lippincott Williams & Wilkins; 2000;179.-
20. Roche Laboratories Romazicon (package insert).
Pastoral counseling: What is it, and when can it help?
Pastoral counselors represent a valuable resource for psychiatric referrals as they are uniquely qualified to address certain mental health issues—including bereavement and coping with terminal illness. Pastoral counselors trained in behavioral sciences can help assess and treat patients who prefer psychotherapy that reflects their spiritual beliefs.
Ministers have been counseling members of their congregations since ancient times. As many psychiatrists may not be aware of the skills and services offered by pastoral counselors, this article:
- describes their background and credentialing
- identifies clinical scenarios in which splitting care with a pastoral counselor may benefit the patient.
Short- or long-term counseling
Pastoral counselors practice in a variety of settings, including pastoral counseling centers, inpatient and outpatient mental health facilities, and in private practice. Individuals generally seek therapy from a pastoral counselor because of their connection with a particular faith, whether Christian, Jewish, Native American, or others. Pastoral counselors— with training in both a religious tradition and the basics of psychology and psychotherapy—can challenge rigid, defensive, or misinformed spiritual beliefs that might contribute to a patient’s psychological distress and dysfunction.1
- In the Torah, the word for counsel, etsah, is used 84 times. Its verb, yaatz, is the root of the Hebrew word for counselor.3
- In the Bible, pastoral counseling prototypes include ministers assigned by Moses to guide the Hebrew people in family, community, and religious life; the prophets Samuel, Jeremiah, and Ezekiel; Jesus of Nazareth; and the apostle, Paul.
- In the 6th century, manuals for Christian priests on assigning penance during confessions (the “Penitentials”) were also intended to reconstruct the personality.3
- Sixteenth-century documents detail steps to “growth in holiness” and prayer and meditation for persons aspiring to greater “perfection.”4
- Martin Luther, leader of the Protestant Reformation in the 16th century, emphasized reasoning and individual freedom rather than doctrine in the Christian church.
Some forms of pastoral counseling are short-term and problem-focused, whereas others address long-standing conflicts and require a long-term relationship with the therapist. For this reason, some therapists prefer the term “pastoral psychotherapy,” feeling it better reflects the work and goals of the counseling they do.
Pastoral counseling and psychotherapy are predominantly insight-oriented but include other therapeutic models as well. Clinebell recommends that pastoral counselors be familiar with four types of therapy:
- behavioral
- human potential (e.g., transactional analysis and Gestalt psychology)
- relational
- and spiritual growth (e.g., based on theories and practices of Carl Jung).2
Integration of religion and science
Examples of pastoral counseling can be traced throughout Judeo-Christian history (Box 1).3,4 As early as 1861, Congregational minister Horace Bushnell of Hartford, Conn., advised parents of the importance of the first 3 years of life in the development of a child’s character.5
Pastoral couseling was shaped by the scientific exploration of the human mind in the late 19th century. William James’ 1890 work, The Principles of Psychology, described the nature of human consciousness and contributed significantly to what became the profession of psychology.6 At the same time, Sigmund Freud was developing his theories of the unconscious. Whereas James explored the dynamics of the individual mind, Freud explored interactions with significant persons at critical periods of development, bringing out the importance of relationships in psychological organization.
The study of the psychology of religion was well underway by the turn of the 20th century, with the publication of E. D. Starbuck’s The Psychology of Religion (1899) and James’ The Varieties of Religious Experience (1902). Ministerial training programs introduced courses in the psychology of religion to help clergy educate and counsel parishioners. Rollo May’s The Art of Counseling (1939), which was presented as a series of lectures to Methodist student workers, is regarded as the first systematic study of counseling techniques. It incorporated the theories of Freud, Jung, Otto Rank, and Alfred Adler.3
Physicians also helped to nurture pastoral psychotherapy by providing clinical experience to seminarians:
- William Keller, MD, of Cincinnati supervised five students from Bexley Hall, an Episcopal seminary in central Ohio, in 1923.
- Richard C. Cabot, MD, then on the faculty of Harvard Medical School, collaborated with minister Anton T. Boisen to develop a clinical pastoral training program at Worcester State Hospital in Massachusetts in 1925.3
- Psychiatrist Smiley Blanton, MD, collaborated with the Rev. Norman Vincent Peale in the 1930s to form the American Foundation of Religion and Psychiatry. The New York-based organization—now called the Blanton-Peale Institute—provides clinical training for pastors and pastoral counselors.
Clinical pastoral education has allowed clergy to practice counseling under the supervision of experienced professionals and has laid the foundation for the pastoral counseling profession.
A ‘theology of relationship’
The theological and community focus of modern pastoral counseling have led some to describe it as a “theology of relationship.”7 Extending from Freud’s understanding of the impact of relationships during infancy on subsequent personality development and Erik Eriksons’s work on the formation of identity through relationships later in life, pastoral counseling considers the individual’s relationship to the community of humankind to be a significant determinant in mental health and illness.
Ministry views all persons as related to one another as creatures of God’s creation. In this fellowship, it is believed that individuals can find meaning, wholeness, and the ability to transcend the pain of life’s experience.
Contrary to James’ view of individual consciousness as finite and Freud’s limited focus on relationships within the immediate family, ministry asserts that all persons are connected, and this connection can be a route to healing. Responsibility to other human beings and to the world is seen as a component of these healing connections. As such, pastoral counseling includes an ethical dimension in the psychotherapy process.
A goal of pastoral counseling is to guide individuals towards greater wholeness within themselves and in their relationships with others. Six dimensions of this growth have been described:
- enlivening the mind
- revitalizing the body
- renewing and enriching intimate relationships
- deepening one’s relationship with nature and the biosphere
- growth in relation to significant institutions
- deepening and vitalizing one’s relationship with God.2
Credentialing of pastoral counselors
Pastors of any religious congregation can function as pastoral counselors. Clergy generally do not counsel outside their parishes, although they may do so even if they lack training beyond seminary. Some clergy have developed excellent skills in counseling and psychotherapy through mentorship, self-directed study, and their own psychotherapy and are competent pastoral counselors. However, certification by the American Association of Pastoral Counselors (AAPC) provides assurance that a counselor has met certain minimum training requirements.
Most pastoral counselors who practice in mental health agencies have obtained AAPC certification. The AAPC accredits pastoral counseling centers, approves training programs, determines credentialing criteria, and ascertains whether an individual has met educational and experiential requirements. It also offers a referral service for persons seeking a pastoral counselor (Box 2).8
- American Association of Pastoral Counselors (AAPC) referral service
- Pastoral counseling centers can be found in the Yellow Pages or on the Internet. Many centers are accredited by the AAPC.
To be certified, a pastoral counselor must have a theology-based master’s or doctoral degree or a comparable degree in pastoral counseling. An AAPC member supervises one-third of the required hours of pastoral counseling experience. A supervised, self-reflective pastoral experience is also required, usually through clinical pastoral education (CPE). This training promotes the integration of theology and behavioral science that is central to pastoral counseling.
CPE generally involves closely supervised work as a hospital chaplain, with classroom instruction and small-group discussion of cases that students encounter on their rounds. These discussions help students:
- identify clinical and theological issues in patients with physical and mental illness
- become aware of their own issues when dealing with patients (i.e., sources of potential counter-transference)
- work toward a mature personal theology.
To receive AAPC credentials, a pastoral counselor must be recognized by a religious organization. Although ordination is not required, the individual must work within a local religious community and be endorsed by its leaders. This requirement helps ensure that the candidate conforms to a generally accepted interpretation of religious experience and not some idiosyncratic personal theology.
Interviews. After the candidate’s training documents have been received and approved, the candidate meets with a three- to four-person certification committee. This 90-minute interview is intended to educate the candidate and promote clarity of purpose within the profession, as credentialing is based solely on the written documents. The committee:
- reviews an audio- or videotape of a therapy session that reflects the candidate’s work
- talks with the candidate about integrating basic theologic concepts and theories of psychology and behavioral science, both professionally and in therapy
- attempts to determine the sophistication and maturity of the candidate’s personal theology
- explores the candidate’s awareness of his or her own psychodynamic characteristics and tendencies.
Appropriate
- To obtain a standard spiritual assessment
- Loss or bereavement
- Chronic or terminal illness
- Guilt, vocational confusion, or lack of direction
- Conflicts regarding patients’ own religious beliefs or those of their families
- Conflicts related to patients’ interpretation of the Bible or other religious texts
- To help patients re-enter the community after institutionalization
- For patients who believe their mental illness is a punishment for having insufficient faith
- As a segue into the mental health system
Not appropriate
- Patient rejects religion or spirituality
- Patient views pastoral counseling as a means to deny the need for psychiatric treatment
- Treatment by another clinician might “dilute” therapy
- Patient uses religion to obtain special privileges or to feign health and functioning
- Role confusion exists because the counselor is the patient’s seminary teacher or pastor
Source: Adapted from Oates WE. The religious care of the psychiatric patient. Philadelphia: The Westminster Press, 1978.
Psychotherapy is no longer required for AAPC certification, but candidates are asked what they have done to ensure that their personal conflicts do not interfere with their ability to provide psychotherapy and counseling. The interview concludes with suggestions to encourage the candidate’s personal growth and professional development.
Working with pastoral counselors
Pastoral counselors are especially well-qualified to address certain types of mental health problems (Box 3).9 A psychiatrist who can identify these problems and make the appropriate referral will provide an important service to the patient.
When to refer. Patients experiencing loss or dealing with bereavement are often struggling with theological questions and can benefit from therapy from a pastoral counselor. Chronic or terminal illness likewise can bring up existential questions, and pastoral counselors can explore with the patient the meaning of suffering, providing spiritual healing when medicine offers no cure.
Some patients frame their mental illness as punishment for a past wrongdoing or sin, and standard psychotherapy is limited in its ability to confront this religious belief. Misinterpretation of biblical or other religious texts can support dysfunctional views of illness, and pastoral counselors can help guide patients to more informed and healthy views of the role of religion and spirituality in health. To help with this, they might bring into therapy such spiritual concepts as faith, forgiveness, reverence, stewardship, evil, suffering, and repentance.
The position of many pastoral counselors as pastors of religious congregations can help some patients make the transition from institutionalization to community life. These counselors can help patients connect with community resources and social groups associated with the patients’ religious affiliations. Some patients newly-diagnosed with a psychiatric illness may be reluctant at first to see a psychiatrist but will see a clergy member. In these cases, pastoral counselors can provide a pathway into the mental health system.
When not to refer. Referrals to pastoral counselors should be avoided when patients are perceived to be using clergy involvement to avoid psychiatric treatment. Some patients might use religion to get special privileges in treatment or to try to look healthier or more functional than they are.
Pastoral counseling is also contraindicated:
- when role confusion might result, such as when the pastoral counselor is also the patient’s pastor or seminary instructor
- in patients who denounce religious involvement or beliefs.
Split treatment As is done with psychologists or social workers, psychiatrists can split treatment with pastoral counselors and prescribe psychotropic medications. Regular communication among all clinicians ensures consistent treatment goals and reduces the risk of splitting dynamics and behaviors.
Certified pastoral counselors are trained in mental health assessment and are educated regarding safety concerns, including warning signs of suicidal or homicidal tendencies and symptoms of psychosis, such as delusions. Pastoral counselors who work in mental health agencies may be best able to respond to these psychiatric emergencies appropriately and expeditiously.
Related resources
- Friedman EH. Generation to generation: Family process in church and synagogue. New York: The Guilford Press, 1985.
- Fowler JW. Stages of faith: the psychology of human development and the quest for meaning. San Franscisco: Harper and Row, 1981.
- Pruyser PW. The minister as diagnostician: personal problems in pastoral perspective. Philadelphia: The Westminster Press, 1976.
- International Center for the Integration of Health and Spirituality. www.icihs.org
1. Bollinger RA. Differences between pastoral counseling and psychotherapy. Bull Menninger Clinic 1985;49(4):371-86.
2. Clinebell H. Basic types of pastoral care and counseling: resources for the ministry of healing and growth. Nashville: Abington Press, 1984.
3. Meiburg AL. The heritage of the pastoral counselor. In: Oates WE (ed). An introduction to pastoral counseling. Nashville: Broadview Press, 1959.
4. Stafford JW. Pastoral counseling. In: Weitzel EJ (ed). Contemporary pastoral counseling. New York: The Bruce Publishing Co., 1969.
5. Bushnell H. Christian nurture. Grand Rapids, MI: Baker Book House, 1979: 248-9 (original work published 1861).
6. James W. Principles of psychology (vols. 1-2). New York: Henry Holt and Co., 1890.
7. Johnson PE. Person and counselor. Nashville: Abington Press, 1967;55.-
8. American Association of Pastoral Counselors. Categories of membership available at http://www.aapc.org/membership.htm. Accessed July 25, 2002,
9. Oates WE. The religious care of the psychiatric patient. Philadelphia: The Westminster Press, 1978.
Pastoral counselors represent a valuable resource for psychiatric referrals as they are uniquely qualified to address certain mental health issues—including bereavement and coping with terminal illness. Pastoral counselors trained in behavioral sciences can help assess and treat patients who prefer psychotherapy that reflects their spiritual beliefs.
Ministers have been counseling members of their congregations since ancient times. As many psychiatrists may not be aware of the skills and services offered by pastoral counselors, this article:
- describes their background and credentialing
- identifies clinical scenarios in which splitting care with a pastoral counselor may benefit the patient.
Short- or long-term counseling
Pastoral counselors practice in a variety of settings, including pastoral counseling centers, inpatient and outpatient mental health facilities, and in private practice. Individuals generally seek therapy from a pastoral counselor because of their connection with a particular faith, whether Christian, Jewish, Native American, or others. Pastoral counselors— with training in both a religious tradition and the basics of psychology and psychotherapy—can challenge rigid, defensive, or misinformed spiritual beliefs that might contribute to a patient’s psychological distress and dysfunction.1
- In the Torah, the word for counsel, etsah, is used 84 times. Its verb, yaatz, is the root of the Hebrew word for counselor.3
- In the Bible, pastoral counseling prototypes include ministers assigned by Moses to guide the Hebrew people in family, community, and religious life; the prophets Samuel, Jeremiah, and Ezekiel; Jesus of Nazareth; and the apostle, Paul.
- In the 6th century, manuals for Christian priests on assigning penance during confessions (the “Penitentials”) were also intended to reconstruct the personality.3
- Sixteenth-century documents detail steps to “growth in holiness” and prayer and meditation for persons aspiring to greater “perfection.”4
- Martin Luther, leader of the Protestant Reformation in the 16th century, emphasized reasoning and individual freedom rather than doctrine in the Christian church.
Some forms of pastoral counseling are short-term and problem-focused, whereas others address long-standing conflicts and require a long-term relationship with the therapist. For this reason, some therapists prefer the term “pastoral psychotherapy,” feeling it better reflects the work and goals of the counseling they do.
Pastoral counseling and psychotherapy are predominantly insight-oriented but include other therapeutic models as well. Clinebell recommends that pastoral counselors be familiar with four types of therapy:
- behavioral
- human potential (e.g., transactional analysis and Gestalt psychology)
- relational
- and spiritual growth (e.g., based on theories and practices of Carl Jung).2
Integration of religion and science
Examples of pastoral counseling can be traced throughout Judeo-Christian history (Box 1).3,4 As early as 1861, Congregational minister Horace Bushnell of Hartford, Conn., advised parents of the importance of the first 3 years of life in the development of a child’s character.5
Pastoral couseling was shaped by the scientific exploration of the human mind in the late 19th century. William James’ 1890 work, The Principles of Psychology, described the nature of human consciousness and contributed significantly to what became the profession of psychology.6 At the same time, Sigmund Freud was developing his theories of the unconscious. Whereas James explored the dynamics of the individual mind, Freud explored interactions with significant persons at critical periods of development, bringing out the importance of relationships in psychological organization.
The study of the psychology of religion was well underway by the turn of the 20th century, with the publication of E. D. Starbuck’s The Psychology of Religion (1899) and James’ The Varieties of Religious Experience (1902). Ministerial training programs introduced courses in the psychology of religion to help clergy educate and counsel parishioners. Rollo May’s The Art of Counseling (1939), which was presented as a series of lectures to Methodist student workers, is regarded as the first systematic study of counseling techniques. It incorporated the theories of Freud, Jung, Otto Rank, and Alfred Adler.3
Physicians also helped to nurture pastoral psychotherapy by providing clinical experience to seminarians:
- William Keller, MD, of Cincinnati supervised five students from Bexley Hall, an Episcopal seminary in central Ohio, in 1923.
- Richard C. Cabot, MD, then on the faculty of Harvard Medical School, collaborated with minister Anton T. Boisen to develop a clinical pastoral training program at Worcester State Hospital in Massachusetts in 1925.3
- Psychiatrist Smiley Blanton, MD, collaborated with the Rev. Norman Vincent Peale in the 1930s to form the American Foundation of Religion and Psychiatry. The New York-based organization—now called the Blanton-Peale Institute—provides clinical training for pastors and pastoral counselors.
Clinical pastoral education has allowed clergy to practice counseling under the supervision of experienced professionals and has laid the foundation for the pastoral counseling profession.
A ‘theology of relationship’
The theological and community focus of modern pastoral counseling have led some to describe it as a “theology of relationship.”7 Extending from Freud’s understanding of the impact of relationships during infancy on subsequent personality development and Erik Eriksons’s work on the formation of identity through relationships later in life, pastoral counseling considers the individual’s relationship to the community of humankind to be a significant determinant in mental health and illness.
Ministry views all persons as related to one another as creatures of God’s creation. In this fellowship, it is believed that individuals can find meaning, wholeness, and the ability to transcend the pain of life’s experience.
Contrary to James’ view of individual consciousness as finite and Freud’s limited focus on relationships within the immediate family, ministry asserts that all persons are connected, and this connection can be a route to healing. Responsibility to other human beings and to the world is seen as a component of these healing connections. As such, pastoral counseling includes an ethical dimension in the psychotherapy process.
A goal of pastoral counseling is to guide individuals towards greater wholeness within themselves and in their relationships with others. Six dimensions of this growth have been described:
- enlivening the mind
- revitalizing the body
- renewing and enriching intimate relationships
- deepening one’s relationship with nature and the biosphere
- growth in relation to significant institutions
- deepening and vitalizing one’s relationship with God.2
Credentialing of pastoral counselors
Pastors of any religious congregation can function as pastoral counselors. Clergy generally do not counsel outside their parishes, although they may do so even if they lack training beyond seminary. Some clergy have developed excellent skills in counseling and psychotherapy through mentorship, self-directed study, and their own psychotherapy and are competent pastoral counselors. However, certification by the American Association of Pastoral Counselors (AAPC) provides assurance that a counselor has met certain minimum training requirements.
Most pastoral counselors who practice in mental health agencies have obtained AAPC certification. The AAPC accredits pastoral counseling centers, approves training programs, determines credentialing criteria, and ascertains whether an individual has met educational and experiential requirements. It also offers a referral service for persons seeking a pastoral counselor (Box 2).8
- American Association of Pastoral Counselors (AAPC) referral service
- Pastoral counseling centers can be found in the Yellow Pages or on the Internet. Many centers are accredited by the AAPC.
To be certified, a pastoral counselor must have a theology-based master’s or doctoral degree or a comparable degree in pastoral counseling. An AAPC member supervises one-third of the required hours of pastoral counseling experience. A supervised, self-reflective pastoral experience is also required, usually through clinical pastoral education (CPE). This training promotes the integration of theology and behavioral science that is central to pastoral counseling.
CPE generally involves closely supervised work as a hospital chaplain, with classroom instruction and small-group discussion of cases that students encounter on their rounds. These discussions help students:
- identify clinical and theological issues in patients with physical and mental illness
- become aware of their own issues when dealing with patients (i.e., sources of potential counter-transference)
- work toward a mature personal theology.
To receive AAPC credentials, a pastoral counselor must be recognized by a religious organization. Although ordination is not required, the individual must work within a local religious community and be endorsed by its leaders. This requirement helps ensure that the candidate conforms to a generally accepted interpretation of religious experience and not some idiosyncratic personal theology.
Interviews. After the candidate’s training documents have been received and approved, the candidate meets with a three- to four-person certification committee. This 90-minute interview is intended to educate the candidate and promote clarity of purpose within the profession, as credentialing is based solely on the written documents. The committee:
- reviews an audio- or videotape of a therapy session that reflects the candidate’s work
- talks with the candidate about integrating basic theologic concepts and theories of psychology and behavioral science, both professionally and in therapy
- attempts to determine the sophistication and maturity of the candidate’s personal theology
- explores the candidate’s awareness of his or her own psychodynamic characteristics and tendencies.
Appropriate
- To obtain a standard spiritual assessment
- Loss or bereavement
- Chronic or terminal illness
- Guilt, vocational confusion, or lack of direction
- Conflicts regarding patients’ own religious beliefs or those of their families
- Conflicts related to patients’ interpretation of the Bible or other religious texts
- To help patients re-enter the community after institutionalization
- For patients who believe their mental illness is a punishment for having insufficient faith
- As a segue into the mental health system
Not appropriate
- Patient rejects religion or spirituality
- Patient views pastoral counseling as a means to deny the need for psychiatric treatment
- Treatment by another clinician might “dilute” therapy
- Patient uses religion to obtain special privileges or to feign health and functioning
- Role confusion exists because the counselor is the patient’s seminary teacher or pastor
Source: Adapted from Oates WE. The religious care of the psychiatric patient. Philadelphia: The Westminster Press, 1978.
Psychotherapy is no longer required for AAPC certification, but candidates are asked what they have done to ensure that their personal conflicts do not interfere with their ability to provide psychotherapy and counseling. The interview concludes with suggestions to encourage the candidate’s personal growth and professional development.
Working with pastoral counselors
Pastoral counselors are especially well-qualified to address certain types of mental health problems (Box 3).9 A psychiatrist who can identify these problems and make the appropriate referral will provide an important service to the patient.
When to refer. Patients experiencing loss or dealing with bereavement are often struggling with theological questions and can benefit from therapy from a pastoral counselor. Chronic or terminal illness likewise can bring up existential questions, and pastoral counselors can explore with the patient the meaning of suffering, providing spiritual healing when medicine offers no cure.
Some patients frame their mental illness as punishment for a past wrongdoing or sin, and standard psychotherapy is limited in its ability to confront this religious belief. Misinterpretation of biblical or other religious texts can support dysfunctional views of illness, and pastoral counselors can help guide patients to more informed and healthy views of the role of religion and spirituality in health. To help with this, they might bring into therapy such spiritual concepts as faith, forgiveness, reverence, stewardship, evil, suffering, and repentance.
The position of many pastoral counselors as pastors of religious congregations can help some patients make the transition from institutionalization to community life. These counselors can help patients connect with community resources and social groups associated with the patients’ religious affiliations. Some patients newly-diagnosed with a psychiatric illness may be reluctant at first to see a psychiatrist but will see a clergy member. In these cases, pastoral counselors can provide a pathway into the mental health system.
When not to refer. Referrals to pastoral counselors should be avoided when patients are perceived to be using clergy involvement to avoid psychiatric treatment. Some patients might use religion to get special privileges in treatment or to try to look healthier or more functional than they are.
Pastoral counseling is also contraindicated:
- when role confusion might result, such as when the pastoral counselor is also the patient’s pastor or seminary instructor
- in patients who denounce religious involvement or beliefs.
Split treatment As is done with psychologists or social workers, psychiatrists can split treatment with pastoral counselors and prescribe psychotropic medications. Regular communication among all clinicians ensures consistent treatment goals and reduces the risk of splitting dynamics and behaviors.
Certified pastoral counselors are trained in mental health assessment and are educated regarding safety concerns, including warning signs of suicidal or homicidal tendencies and symptoms of psychosis, such as delusions. Pastoral counselors who work in mental health agencies may be best able to respond to these psychiatric emergencies appropriately and expeditiously.
Related resources
- Friedman EH. Generation to generation: Family process in church and synagogue. New York: The Guilford Press, 1985.
- Fowler JW. Stages of faith: the psychology of human development and the quest for meaning. San Franscisco: Harper and Row, 1981.
- Pruyser PW. The minister as diagnostician: personal problems in pastoral perspective. Philadelphia: The Westminster Press, 1976.
- International Center for the Integration of Health and Spirituality. www.icihs.org
Pastoral counselors represent a valuable resource for psychiatric referrals as they are uniquely qualified to address certain mental health issues—including bereavement and coping with terminal illness. Pastoral counselors trained in behavioral sciences can help assess and treat patients who prefer psychotherapy that reflects their spiritual beliefs.
Ministers have been counseling members of their congregations since ancient times. As many psychiatrists may not be aware of the skills and services offered by pastoral counselors, this article:
- describes their background and credentialing
- identifies clinical scenarios in which splitting care with a pastoral counselor may benefit the patient.
Short- or long-term counseling
Pastoral counselors practice in a variety of settings, including pastoral counseling centers, inpatient and outpatient mental health facilities, and in private practice. Individuals generally seek therapy from a pastoral counselor because of their connection with a particular faith, whether Christian, Jewish, Native American, or others. Pastoral counselors— with training in both a religious tradition and the basics of psychology and psychotherapy—can challenge rigid, defensive, or misinformed spiritual beliefs that might contribute to a patient’s psychological distress and dysfunction.1
- In the Torah, the word for counsel, etsah, is used 84 times. Its verb, yaatz, is the root of the Hebrew word for counselor.3
- In the Bible, pastoral counseling prototypes include ministers assigned by Moses to guide the Hebrew people in family, community, and religious life; the prophets Samuel, Jeremiah, and Ezekiel; Jesus of Nazareth; and the apostle, Paul.
- In the 6th century, manuals for Christian priests on assigning penance during confessions (the “Penitentials”) were also intended to reconstruct the personality.3
- Sixteenth-century documents detail steps to “growth in holiness” and prayer and meditation for persons aspiring to greater “perfection.”4
- Martin Luther, leader of the Protestant Reformation in the 16th century, emphasized reasoning and individual freedom rather than doctrine in the Christian church.
Some forms of pastoral counseling are short-term and problem-focused, whereas others address long-standing conflicts and require a long-term relationship with the therapist. For this reason, some therapists prefer the term “pastoral psychotherapy,” feeling it better reflects the work and goals of the counseling they do.
Pastoral counseling and psychotherapy are predominantly insight-oriented but include other therapeutic models as well. Clinebell recommends that pastoral counselors be familiar with four types of therapy:
- behavioral
- human potential (e.g., transactional analysis and Gestalt psychology)
- relational
- and spiritual growth (e.g., based on theories and practices of Carl Jung).2
Integration of religion and science
Examples of pastoral counseling can be traced throughout Judeo-Christian history (Box 1).3,4 As early as 1861, Congregational minister Horace Bushnell of Hartford, Conn., advised parents of the importance of the first 3 years of life in the development of a child’s character.5
Pastoral couseling was shaped by the scientific exploration of the human mind in the late 19th century. William James’ 1890 work, The Principles of Psychology, described the nature of human consciousness and contributed significantly to what became the profession of psychology.6 At the same time, Sigmund Freud was developing his theories of the unconscious. Whereas James explored the dynamics of the individual mind, Freud explored interactions with significant persons at critical periods of development, bringing out the importance of relationships in psychological organization.
The study of the psychology of religion was well underway by the turn of the 20th century, with the publication of E. D. Starbuck’s The Psychology of Religion (1899) and James’ The Varieties of Religious Experience (1902). Ministerial training programs introduced courses in the psychology of religion to help clergy educate and counsel parishioners. Rollo May’s The Art of Counseling (1939), which was presented as a series of lectures to Methodist student workers, is regarded as the first systematic study of counseling techniques. It incorporated the theories of Freud, Jung, Otto Rank, and Alfred Adler.3
Physicians also helped to nurture pastoral psychotherapy by providing clinical experience to seminarians:
- William Keller, MD, of Cincinnati supervised five students from Bexley Hall, an Episcopal seminary in central Ohio, in 1923.
- Richard C. Cabot, MD, then on the faculty of Harvard Medical School, collaborated with minister Anton T. Boisen to develop a clinical pastoral training program at Worcester State Hospital in Massachusetts in 1925.3
- Psychiatrist Smiley Blanton, MD, collaborated with the Rev. Norman Vincent Peale in the 1930s to form the American Foundation of Religion and Psychiatry. The New York-based organization—now called the Blanton-Peale Institute—provides clinical training for pastors and pastoral counselors.
Clinical pastoral education has allowed clergy to practice counseling under the supervision of experienced professionals and has laid the foundation for the pastoral counseling profession.
A ‘theology of relationship’
The theological and community focus of modern pastoral counseling have led some to describe it as a “theology of relationship.”7 Extending from Freud’s understanding of the impact of relationships during infancy on subsequent personality development and Erik Eriksons’s work on the formation of identity through relationships later in life, pastoral counseling considers the individual’s relationship to the community of humankind to be a significant determinant in mental health and illness.
Ministry views all persons as related to one another as creatures of God’s creation. In this fellowship, it is believed that individuals can find meaning, wholeness, and the ability to transcend the pain of life’s experience.
Contrary to James’ view of individual consciousness as finite and Freud’s limited focus on relationships within the immediate family, ministry asserts that all persons are connected, and this connection can be a route to healing. Responsibility to other human beings and to the world is seen as a component of these healing connections. As such, pastoral counseling includes an ethical dimension in the psychotherapy process.
A goal of pastoral counseling is to guide individuals towards greater wholeness within themselves and in their relationships with others. Six dimensions of this growth have been described:
- enlivening the mind
- revitalizing the body
- renewing and enriching intimate relationships
- deepening one’s relationship with nature and the biosphere
- growth in relation to significant institutions
- deepening and vitalizing one’s relationship with God.2
Credentialing of pastoral counselors
Pastors of any religious congregation can function as pastoral counselors. Clergy generally do not counsel outside their parishes, although they may do so even if they lack training beyond seminary. Some clergy have developed excellent skills in counseling and psychotherapy through mentorship, self-directed study, and their own psychotherapy and are competent pastoral counselors. However, certification by the American Association of Pastoral Counselors (AAPC) provides assurance that a counselor has met certain minimum training requirements.
Most pastoral counselors who practice in mental health agencies have obtained AAPC certification. The AAPC accredits pastoral counseling centers, approves training programs, determines credentialing criteria, and ascertains whether an individual has met educational and experiential requirements. It also offers a referral service for persons seeking a pastoral counselor (Box 2).8
- American Association of Pastoral Counselors (AAPC) referral service
- Pastoral counseling centers can be found in the Yellow Pages or on the Internet. Many centers are accredited by the AAPC.
To be certified, a pastoral counselor must have a theology-based master’s or doctoral degree or a comparable degree in pastoral counseling. An AAPC member supervises one-third of the required hours of pastoral counseling experience. A supervised, self-reflective pastoral experience is also required, usually through clinical pastoral education (CPE). This training promotes the integration of theology and behavioral science that is central to pastoral counseling.
CPE generally involves closely supervised work as a hospital chaplain, with classroom instruction and small-group discussion of cases that students encounter on their rounds. These discussions help students:
- identify clinical and theological issues in patients with physical and mental illness
- become aware of their own issues when dealing with patients (i.e., sources of potential counter-transference)
- work toward a mature personal theology.
To receive AAPC credentials, a pastoral counselor must be recognized by a religious organization. Although ordination is not required, the individual must work within a local religious community and be endorsed by its leaders. This requirement helps ensure that the candidate conforms to a generally accepted interpretation of religious experience and not some idiosyncratic personal theology.
Interviews. After the candidate’s training documents have been received and approved, the candidate meets with a three- to four-person certification committee. This 90-minute interview is intended to educate the candidate and promote clarity of purpose within the profession, as credentialing is based solely on the written documents. The committee:
- reviews an audio- or videotape of a therapy session that reflects the candidate’s work
- talks with the candidate about integrating basic theologic concepts and theories of psychology and behavioral science, both professionally and in therapy
- attempts to determine the sophistication and maturity of the candidate’s personal theology
- explores the candidate’s awareness of his or her own psychodynamic characteristics and tendencies.
Appropriate
- To obtain a standard spiritual assessment
- Loss or bereavement
- Chronic or terminal illness
- Guilt, vocational confusion, or lack of direction
- Conflicts regarding patients’ own religious beliefs or those of their families
- Conflicts related to patients’ interpretation of the Bible or other religious texts
- To help patients re-enter the community after institutionalization
- For patients who believe their mental illness is a punishment for having insufficient faith
- As a segue into the mental health system
Not appropriate
- Patient rejects religion or spirituality
- Patient views pastoral counseling as a means to deny the need for psychiatric treatment
- Treatment by another clinician might “dilute” therapy
- Patient uses religion to obtain special privileges or to feign health and functioning
- Role confusion exists because the counselor is the patient’s seminary teacher or pastor
Source: Adapted from Oates WE. The religious care of the psychiatric patient. Philadelphia: The Westminster Press, 1978.
Psychotherapy is no longer required for AAPC certification, but candidates are asked what they have done to ensure that their personal conflicts do not interfere with their ability to provide psychotherapy and counseling. The interview concludes with suggestions to encourage the candidate’s personal growth and professional development.
Working with pastoral counselors
Pastoral counselors are especially well-qualified to address certain types of mental health problems (Box 3).9 A psychiatrist who can identify these problems and make the appropriate referral will provide an important service to the patient.
When to refer. Patients experiencing loss or dealing with bereavement are often struggling with theological questions and can benefit from therapy from a pastoral counselor. Chronic or terminal illness likewise can bring up existential questions, and pastoral counselors can explore with the patient the meaning of suffering, providing spiritual healing when medicine offers no cure.
Some patients frame their mental illness as punishment for a past wrongdoing or sin, and standard psychotherapy is limited in its ability to confront this religious belief. Misinterpretation of biblical or other religious texts can support dysfunctional views of illness, and pastoral counselors can help guide patients to more informed and healthy views of the role of religion and spirituality in health. To help with this, they might bring into therapy such spiritual concepts as faith, forgiveness, reverence, stewardship, evil, suffering, and repentance.
The position of many pastoral counselors as pastors of religious congregations can help some patients make the transition from institutionalization to community life. These counselors can help patients connect with community resources and social groups associated with the patients’ religious affiliations. Some patients newly-diagnosed with a psychiatric illness may be reluctant at first to see a psychiatrist but will see a clergy member. In these cases, pastoral counselors can provide a pathway into the mental health system.
When not to refer. Referrals to pastoral counselors should be avoided when patients are perceived to be using clergy involvement to avoid psychiatric treatment. Some patients might use religion to get special privileges in treatment or to try to look healthier or more functional than they are.
Pastoral counseling is also contraindicated:
- when role confusion might result, such as when the pastoral counselor is also the patient’s pastor or seminary instructor
- in patients who denounce religious involvement or beliefs.
Split treatment As is done with psychologists or social workers, psychiatrists can split treatment with pastoral counselors and prescribe psychotropic medications. Regular communication among all clinicians ensures consistent treatment goals and reduces the risk of splitting dynamics and behaviors.
Certified pastoral counselors are trained in mental health assessment and are educated regarding safety concerns, including warning signs of suicidal or homicidal tendencies and symptoms of psychosis, such as delusions. Pastoral counselors who work in mental health agencies may be best able to respond to these psychiatric emergencies appropriately and expeditiously.
Related resources
- Friedman EH. Generation to generation: Family process in church and synagogue. New York: The Guilford Press, 1985.
- Fowler JW. Stages of faith: the psychology of human development and the quest for meaning. San Franscisco: Harper and Row, 1981.
- Pruyser PW. The minister as diagnostician: personal problems in pastoral perspective. Philadelphia: The Westminster Press, 1976.
- International Center for the Integration of Health and Spirituality. www.icihs.org
1. Bollinger RA. Differences between pastoral counseling and psychotherapy. Bull Menninger Clinic 1985;49(4):371-86.
2. Clinebell H. Basic types of pastoral care and counseling: resources for the ministry of healing and growth. Nashville: Abington Press, 1984.
3. Meiburg AL. The heritage of the pastoral counselor. In: Oates WE (ed). An introduction to pastoral counseling. Nashville: Broadview Press, 1959.
4. Stafford JW. Pastoral counseling. In: Weitzel EJ (ed). Contemporary pastoral counseling. New York: The Bruce Publishing Co., 1969.
5. Bushnell H. Christian nurture. Grand Rapids, MI: Baker Book House, 1979: 248-9 (original work published 1861).
6. James W. Principles of psychology (vols. 1-2). New York: Henry Holt and Co., 1890.
7. Johnson PE. Person and counselor. Nashville: Abington Press, 1967;55.-
8. American Association of Pastoral Counselors. Categories of membership available at http://www.aapc.org/membership.htm. Accessed July 25, 2002,
9. Oates WE. The religious care of the psychiatric patient. Philadelphia: The Westminster Press, 1978.
1. Bollinger RA. Differences between pastoral counseling and psychotherapy. Bull Menninger Clinic 1985;49(4):371-86.
2. Clinebell H. Basic types of pastoral care and counseling: resources for the ministry of healing and growth. Nashville: Abington Press, 1984.
3. Meiburg AL. The heritage of the pastoral counselor. In: Oates WE (ed). An introduction to pastoral counseling. Nashville: Broadview Press, 1959.
4. Stafford JW. Pastoral counseling. In: Weitzel EJ (ed). Contemporary pastoral counseling. New York: The Bruce Publishing Co., 1969.
5. Bushnell H. Christian nurture. Grand Rapids, MI: Baker Book House, 1979: 248-9 (original work published 1861).
6. James W. Principles of psychology (vols. 1-2). New York: Henry Holt and Co., 1890.
7. Johnson PE. Person and counselor. Nashville: Abington Press, 1967;55.-
8. American Association of Pastoral Counselors. Categories of membership available at http://www.aapc.org/membership.htm. Accessed July 25, 2002,
9. Oates WE. The religious care of the psychiatric patient. Philadelphia: The Westminster Press, 1978.
Beware cytochrome P450 inducers: Prescribing tips to prevent drug-drug interactions
Psychiatrists know that common psychotropic medications can inhibit the liver’s cytochrome P450 enzyme system, increasing both plasma levels and the toxicity of co-administered drugs. Less well-known, perhaps, is that the opposite process—hepatic enzyme induction—can accelerate the liver’s meolism of co-administered drugs, resulting in abnormally low plasma levels.
Hepatic enzyme-inducing agents may appear in a patient’s regimen by prescription or self-administration (e.g., cigarette smoking, use of St. John’s wort, etc.) (Table 1). Most psychotropics are metabolized by the liver, and co-administering them with a hepatic enzyme inducer may cause pharmacokinetic consequences, including lowered plasma levels of the parent compound and elevated plasma levels of its metabolites. These plasma level changes may result in:
- reduced efficacy (e.g., if the parent drug alone is responsible for clinical benefit)
- greater efficacy (e.g., with the prodrug codeine, where the analgesic effect may be amplified by accelerated metabolism into its active drug, morphine)
- or no change in clinical effect (e.g., if the metabolite of the parent drug is active and its increased plasma level sufficiently compensates for the decreased plasma level of the parent compound).
This article offers an overview of common inducers and the drugs they affect, as well as five principles that can help you anticipate and manage potential drug-drug interactions.
Table 1
COMMON AGENTS ASSOCIATED WITH HEPATIC ENZYME INDUCTION
| Prescription | Nonprescription |
|---|---|
| Carbamazepine | Chronic cigarette smoking |
| Dexamethasone | Chronic ethanol use |
| Isoniazid | Chronic marijuana smoking |
| Modafinil | St. John’s wort |
| Omeprazole | |
| Oxcarbazepine | |
| Phenobarbital | |
| Phenytoin | |
| Prednisone | |
| Primidone | |
| Rifampin |
Carbamazepine
Carbamazepine is the best-known and most-thoroughly documented agent that can induce hepatic enzymes and lower plasma levels of co-administered drugs, both psychiatric and nonpsychiatric. This anticonvulsant also shows evidence of autoinduction, the unusual property of inducing its own accelerated hepatic metabolism.1
Carbamazepine is a powerful inducer of CYP3A, the most abundant family of cytochrome P450 enzymes.2 With initial carbamazepine therapy, hepatic enzyme induction begins within 3 to 5 days and is complete within 21 to 28 days.3 Because any co-administered drug requires some (often unknown) minimum plasma concentration for efficacy—and sometimes requires a “therapeutic window” level4— an inducing agent such as carbamazepine may compromise the other drug’s effectiveness.
Effect on neuroleptics. Drugs and classes of psychotropics whose levels and/or efficacies may be reduced in the presence of enzyme-inducing agents are listed in Table 2. For example, when carbamazepine and haloperidol are co-administered, haloperidol plasma levels may be reduced by 60%.5 The literature also shows a 50% reduction in fluphenazine levels6 and substantially reduced levels of valproic acid,7 clozapine,8 and perphenazine9 when co-administered with carbamazepine. Data on how these changes alter the drugs’ clinical effects are mixed: some patients have improved, and some have worsened.
It is unclear whether carbamazepine’s presence may lower drug levels into or below a neuroleptic plasma “therapeutic window,” or whether some observed patient improvement might occur as an independent augmenting effect of carbamazepine. Clearly, however, the presence or addition of the inducing agent—carbamazepine—substantially lowers neuroleptic plasma levels.
Effect on antidepressants. Carbamazepine has similar plasma level-reducing effects on antidepressants:
- amitriptyline and nortriptyline levels have been shown to be reduced by 40%10
- bupropion peak levels are decreased by 87%11
- levels of clomipramine,12 imipramine,13 and doxepin show marked reductions.10
Table 2
PSYCHOTROPICS AFFECTED* BY HEPATIC ENZYME INDUCERS
| Antidepressants (tricyclics and potentially SSRIs) |
| Antipsychotics (neuroleptics and atypicals) |
| Benzodiazepines |
| Bupropion |
| Valproate |
| * Exhibit reduced plasma levels and/or impaired efficacy when co-administered |
Other anticonvulsants
For unclear reasons, anticonvulsants are often hepatic enzyme inducers. Phenobarbitol, primidone, and phenytoin have been associated with reduced plasma levels of numerous drugs.16 For example, phenytoin has been reported to increase clearance of the atypical antipsychotic quetiapine. In one report, phenytoin cessation resulted in a 24-fold increase in plasma quetiapine levels. Similarly, carbamazepine cessation increased quetiapine plasma levels 14-fold.17
Oxcarbazepine. Oxcarbazepine is a newer anticonvulsant—a keto-analogue of carbamazepine—that offers improved safety in overdose, no cardiotoxic effect, and no known risk of agranulocytosis. Like older anticonvulsants, oxcarbazepine is being used to treat mood disorders.
Oxcarbazepine has been described as exhibiting “mild induction” of hepatic enzymes.18 The drug’s manufacturer reports that the agent can induce the 3A4 hepatic enzyme, reduce levels of oral contraceptives by 50%, and decrease calcium channel blocker levels by 28%.16 In two patients recently treated by the author:
- adding oxcarbazepine, 600 mg bid, to the regimen of a male patient, age 46, with schizophrenia and obsessive-compulsive disorder resulted in a 100% reduction in the plasma level of clomipramine.
- adding oxcarbazepine, 600 mg in the morning and 900 mg at bedtime, to the regimen of a woman, age 44, with bipolar disorder led to a 71% decrease in the plasma level of valproate.
Topiramate. Topiramate—which is used as an antiepileptic and to treat mood disorders—has been shown to decrease digoxin levels by 11% and the estrogenic component of oral contraceptives by 30%. Topiramate may both induce and inhibit hepatic enzyme metabolism and has been associated with a 25% increase in phenytoin levels in some patients.
Other known inducers
Lesser-known hepatic enzyme inducers include chronic cigarette smoking,19 marijuana smoking,20 chronic ethanol use,21 modafinil,22 St. John’s wort,23 prednisone,16 dexamethasone,16 omeprazole,16 rifampin,16 and isoniazid.16 Unfortunately, the doses and duration required for induction are undocumented. The effect of these agents can only be detected by the astute clinician or perhaps by measuring plasma levels of co-prescribed drugs.
Among more than 20 known CYP450 isoenzymes, the six that metabolize most clinically useful medications are 1A2, 2C9, 2C19, 2D6, 2E1, and the 3A family. The 3A isoenzymes metabolize the widest range of drugs, so any agent that induces them is likely to have many interactions.
Inducing agents affect numerous specific enzymes (Table 3). For example:
- cigarette smoking induces at least 1A2
- carbamazepine and other anticonvulsants induce at least 3A4, 1A2, 2C9, 2C19, and 2D6
- alcohol induces at least 3A4 and 2E1.
The catalogue of hepatic enzymes, inducers, and specific enzymes and substrates (affected drugs) is poorly documented, inadequately studied, and difficult to commit to memory. It is much simpler to assume that any inducing agent in a patient’s regimen may lower plasma levels and alter the efficacy of co-administered drugs that are also metabolized by the liver.
Compensating for induction
A careful patient history and monitoring of clinical effect and plasma levels can compensate for the effects of hepatic enzyme inducers.4 Dosages of affected drugs may need to be adjusted to achieve desired therapeutic levels.
Table 3
HEPATIC INDUCERS1, AFFECTED ISOENZYMES2, AND SOME AFFECTED MEDICATIONS3
| Hepatic enzyme inducer | CYP1A2 | CYP2C19 | CYP2C9 | CYP2D6 | CYP3A family | CYP2E1 |
|---|---|---|---|---|---|---|
| Carbamazepine | Clozapine4 Amitriptyline Fluoxetine Haloperidol | Citalopram Diazepam Imipramine Fluoxetine | Warfarin | Risperidone Paroxetine Amphetamine Perphenazine | OCP5 Alprazolam Quetiapine | |
| Oxcarbazepine | Clomipramine | Clomipramine Risperidone | OCP | |||
| Phenytoin | Clozapine | Diazepam | OCP Quetiapine | |||
| Phenobarbital | Haloperidol Paroxetine Fluvoxamine | |||||
| Topiramate 6 | OCP | |||||
| Omeprazole | Clozapine | Phenytoin | ||||
| Rifampin | Phenytoin | Fluoxetine | ||||
| Prednisone | OCP | |||||
| Dexamethasone | Paroxetine | OCP | ||||
| Hypericum (St. John’s wort) | OCP Cyclosporine7 Haloperidol Pimozide | |||||
| Ethanol (chronic) | Tricyclics Neuroleptics | Alprazolam Trazodone Zaleplon | Ethanol Acetaminophen8 | |||
| Cigarette smoking | Haloperidol Clozapine | |||||
| OCP: Oral contraceptives 1 Only clinically relevant inducing agents listed 2 Cited by manufacturer or in literature 3 Examples of drugs known to be affected 4 Induction effect known, concomitant use not advisable due to possible addictive agranulocytosis risk 5 Among numerous medications metabolized by 3A isoenzymes 6 Acts as an inducer but also inhibits isoenzyme 2C19 7 St. John’s wort use has been associated with reduced cyclosporine levels and acute transplant rejection. 8 Chronic alcohol intake has been associated with accelerated acetaminophen metabolism and toxic metabolite levels. | ||||||
When an inducing agent is halted during psychotropic treatment, expect higher plasma levels, side effects, or even toxicity related to the psychotropic. This medication effect is likely as the inducing agent is tapered, discontinued, and cleared from the body (across approximately 5.5 times its half-life), and the induction process is gradually reversed.
Cessation of inducing agents has amplified the effects of clozapine8 and tricyclic antidepressants.10 Anecdotally, the taper and cessation of oxcarbazepine in the author’s bipolar patient resulted in a 40% increase in plasma risperidone level and an 118% increase in valproic acid level, without any increase in the dosage of either psychotropic. At baseline, the patient’s risperidone plasma level was 58 ng/ml (all parent compound). After oxcarbazepine was tapered and discontinued across 1 month, a repeat measurement of risperidone yielded a higher total plasma level (76 ng/ml) but an altered parent drug-to-metabolite ratio (risperidone 68 ng/ml, metabolite 8 ng/ml). This suggests that induction reversal was incomplete 2 weeks after oxcarbazepine was discontinued.
The literature offers little data on timelines for the onset and reversal of hepatic enzyme induction. Induction probably begins and becomes complete within days or weeks after drug therapy is initiated and steady-state levels are achieved. Similarly, the reversal likely occurs within days or weeks after clearance of the inducer.
How plasma levels correlate with clinical findings is the key, of course, and one must account for other possible influences, such as the presence of other hepatic enzyme inducers and inhibitors, dosage adjustments, cigarette smoking, chronic alcohol abuse, and other factors.
- Prescription or nonprescription agents (e.g., cigarette smoking, St. John’s wort) may induce hepatic enzymes.
- Inducing agents can lower plasma levels of co-administered medications that are also metabolized by the liver.
- Most psychotropics are metabolized by the liver, and their therapeutic effect requires a minimum plasma concentration.
- Hepatic enzyme induction can result in subtherapeutic plasma levels and inadequate drug trials of prescribed psychotropics.
- Assume that any inducing agent may lower plasma levels and alter the efficacy of co-administered drugs that are also metabolized by the liver. Observe carefully, monitor plasma levels, and use incremental dosing to assess and compensate for induction effects.
Five principles
When prescribing psychotropics, careful attention to five principles for managing the effects of hepatic enzyme induction (Box ) can result in:
- fewer patients with refractory symptoms
- less polypharmacy
- fewer sequelae of undertreated serious psychiatric illness
- improved therapy of comorbid medical conditions whose therapeutic agents may be metabolized by the liver and are therefore vulnerable to the effects of hepatic enzyme induction.
- Flockhart D. Indiana University Department of Medicine. Cytochrome P450 drug interaction table. http://www.Drug-Interactions.com
- DePiro JT, Talbert RL, Yee, GC, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002.
- Bernstein JG. Handbook of drug therapy in psychiatry. New York: Mosby-Year Book, 1995.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clomipramine • Anafranil
- Citalopram • Celexa
- Clozapine • Clozaril
- Diazepam • Valium
- Doxepin • Sinequan
- Dexamethasone • Decadron
- Fluphenazine • Prolixin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Isoniazid • Rifamate
- Modafinil • Provigil
- Nortriptyline • Pamelor
- Omeprazole • Prilosec
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Phenytoin • Dilantin
- Pimozide • Orap
- Primidone • Mysoline
- Quetiapine • Seroquel
- Rifampin • Rifadin
- Risperidone • Risperdal
- Trazodone • Desyrel
- Valproate • Depakote
- Warfarin • Coumadin
- Zaleplon • Sonata
Dr. Baird reports that he has served as a consultant to Eli Lilly and Co.
1. Rosenbaum JF. Drug treatment of resistant depression: reviewing options. Boston: Harvard Psychopharmacology Review, October 21, 1990.
2. Steffens DC, Krishnan RR, Doraiswamy PM. Psychotropic drug interactions. New York: MBL Communications, 1997.
3. Gidal BE, Garnett WR, Graves N. Epilepsy. In: DiPiro JT, Talbert RL, Yee GE, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002;1031-59.
4. Preskorn SH, Burke MJ, Fast GA. Therapeutic drug monitoring: principles and practice. Psychiatric Clin North Am 1993;16(3):611-41.
5. Arana GW, Goff DC, Friedman H, et al. Does carbamazepine-induced reduction of plasma haloperidol levels worsen psychotic symptoms? Am J Psychiatry 1986;143:650-1.
6. Jann MW, Fidone GS, Hernandez JM, et al. Clinical implications of increased antipsychotic plasma concentrations upon anticonvulsant cessation. Psychiatry Res 1989;28:153-9.
7. Wilder BJ. Pharmacokinetics of valproate and carbamazepine. J Clin Psychopharmacol 1992;12(1):64S-67S.
8. Raitasuo V, Lehtovarra R, Huttunen MO. Carbamazepine and plasma levels of clozapine. Am J Psychiatry 1993;150(1):169.-
9. Nelson JC. Combined treatment strategies in psychiatry. J Clin Psychiatry 1993;54 (suppl 9):42-9.
10. Leinonen E, Lillsunde P, Laukkanen V, et al. Effects of carbamazepine on serum antidepressant concentration in psychiatric patients. J Clin Psychopharmacology 1991;11:313-18.
11. Ketter TA, Jenkins JB, Schroeder DH, et al. Carbamazepine but not valproate induces buproprion metabolism. J Clin Psychopharmacology 1995;15:327-33.
12. De la Fuente JM, Mendlewicz J. Carbamazepine addition in tricyclic antidepressant-resistant unipolar depression. Biol Psychiatry 1992;32:369-74.
13. Brown CS, Wells BG, Cold JA. Possible influence of carbamazepine on plasma imipramine concentration in children with attention deficit hyperactivity disorder. J Clin Psychopharmacol 1990;10:359-62.
14. Arana GW, Epstein S, Molloy M, et al. Carbamazepine-induced reduction of plasma alprazolam concentrations: a clinical case report. J Clin Psychiatry 1988;49:448-9.
15. Callahan AM, Fava M, Rosenbaum JF. Drug interactions in psychopharmacology. Psychiatric Clin North Am 1993;16:647-71.
16. Physician’s Desk Reference. Montvale, NJ: Medical Economics, 2002.
17. Savasi I, Millson RC, Owen JA. Quetiapine blood level variability. Can J Psychiatry 2002;47:94.-
18. Ghaemi S, Ko J. Oxcarbazepine treatment of bipolar disorder: a review of the literature. Primary Psychiatry 2002;9:55-9.
19. Brown RA, Goldstein MG, Niaura R, et al. Nicotine dependence: assessment and management. In: Stoudemire A, Fogel BS (eds). Psychiatric care of the medical patient. New York: Oxford University Press, 1993;877-901.
20. Bauer LA. Clinical pharmacokinetics and pharmacodynamics. In: DiPiro JT, Talbert RL, Yee GC, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill, 2002;33-54.
21. Franklin JE, Frances RJ. Substance-related disorders. In: Rundell JR, Wise MG (eds). Textbook of consultation-liaison psychiatry. Washington, DC: American Psychiatric Press, 1996;427-65.
22. Flockhart D. Indiana University Department of Medicine. Cytochrome P450 drug interaction table. http://www.drug-interactions.com.
23. Crisman ML, Dorson PG. Schizophrenia. In: DiPiro JT, Talbert RL, Yee GE, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002;1219-42.
Psychiatrists know that common psychotropic medications can inhibit the liver’s cytochrome P450 enzyme system, increasing both plasma levels and the toxicity of co-administered drugs. Less well-known, perhaps, is that the opposite process—hepatic enzyme induction—can accelerate the liver’s meolism of co-administered drugs, resulting in abnormally low plasma levels.
Hepatic enzyme-inducing agents may appear in a patient’s regimen by prescription or self-administration (e.g., cigarette smoking, use of St. John’s wort, etc.) (Table 1). Most psychotropics are metabolized by the liver, and co-administering them with a hepatic enzyme inducer may cause pharmacokinetic consequences, including lowered plasma levels of the parent compound and elevated plasma levels of its metabolites. These plasma level changes may result in:
- reduced efficacy (e.g., if the parent drug alone is responsible for clinical benefit)
- greater efficacy (e.g., with the prodrug codeine, where the analgesic effect may be amplified by accelerated metabolism into its active drug, morphine)
- or no change in clinical effect (e.g., if the metabolite of the parent drug is active and its increased plasma level sufficiently compensates for the decreased plasma level of the parent compound).
This article offers an overview of common inducers and the drugs they affect, as well as five principles that can help you anticipate and manage potential drug-drug interactions.
Table 1
COMMON AGENTS ASSOCIATED WITH HEPATIC ENZYME INDUCTION
| Prescription | Nonprescription |
|---|---|
| Carbamazepine | Chronic cigarette smoking |
| Dexamethasone | Chronic ethanol use |
| Isoniazid | Chronic marijuana smoking |
| Modafinil | St. John’s wort |
| Omeprazole | |
| Oxcarbazepine | |
| Phenobarbital | |
| Phenytoin | |
| Prednisone | |
| Primidone | |
| Rifampin |
Carbamazepine
Carbamazepine is the best-known and most-thoroughly documented agent that can induce hepatic enzymes and lower plasma levels of co-administered drugs, both psychiatric and nonpsychiatric. This anticonvulsant also shows evidence of autoinduction, the unusual property of inducing its own accelerated hepatic metabolism.1
Carbamazepine is a powerful inducer of CYP3A, the most abundant family of cytochrome P450 enzymes.2 With initial carbamazepine therapy, hepatic enzyme induction begins within 3 to 5 days and is complete within 21 to 28 days.3 Because any co-administered drug requires some (often unknown) minimum plasma concentration for efficacy—and sometimes requires a “therapeutic window” level4— an inducing agent such as carbamazepine may compromise the other drug’s effectiveness.
Effect on neuroleptics. Drugs and classes of psychotropics whose levels and/or efficacies may be reduced in the presence of enzyme-inducing agents are listed in Table 2. For example, when carbamazepine and haloperidol are co-administered, haloperidol plasma levels may be reduced by 60%.5 The literature also shows a 50% reduction in fluphenazine levels6 and substantially reduced levels of valproic acid,7 clozapine,8 and perphenazine9 when co-administered with carbamazepine. Data on how these changes alter the drugs’ clinical effects are mixed: some patients have improved, and some have worsened.
It is unclear whether carbamazepine’s presence may lower drug levels into or below a neuroleptic plasma “therapeutic window,” or whether some observed patient improvement might occur as an independent augmenting effect of carbamazepine. Clearly, however, the presence or addition of the inducing agent—carbamazepine—substantially lowers neuroleptic plasma levels.
Effect on antidepressants. Carbamazepine has similar plasma level-reducing effects on antidepressants:
- amitriptyline and nortriptyline levels have been shown to be reduced by 40%10
- bupropion peak levels are decreased by 87%11
- levels of clomipramine,12 imipramine,13 and doxepin show marked reductions.10
Table 2
PSYCHOTROPICS AFFECTED* BY HEPATIC ENZYME INDUCERS
| Antidepressants (tricyclics and potentially SSRIs) |
| Antipsychotics (neuroleptics and atypicals) |
| Benzodiazepines |
| Bupropion |
| Valproate |
| * Exhibit reduced plasma levels and/or impaired efficacy when co-administered |
Other anticonvulsants
For unclear reasons, anticonvulsants are often hepatic enzyme inducers. Phenobarbitol, primidone, and phenytoin have been associated with reduced plasma levels of numerous drugs.16 For example, phenytoin has been reported to increase clearance of the atypical antipsychotic quetiapine. In one report, phenytoin cessation resulted in a 24-fold increase in plasma quetiapine levels. Similarly, carbamazepine cessation increased quetiapine plasma levels 14-fold.17
Oxcarbazepine. Oxcarbazepine is a newer anticonvulsant—a keto-analogue of carbamazepine—that offers improved safety in overdose, no cardiotoxic effect, and no known risk of agranulocytosis. Like older anticonvulsants, oxcarbazepine is being used to treat mood disorders.
Oxcarbazepine has been described as exhibiting “mild induction” of hepatic enzymes.18 The drug’s manufacturer reports that the agent can induce the 3A4 hepatic enzyme, reduce levels of oral contraceptives by 50%, and decrease calcium channel blocker levels by 28%.16 In two patients recently treated by the author:
- adding oxcarbazepine, 600 mg bid, to the regimen of a male patient, age 46, with schizophrenia and obsessive-compulsive disorder resulted in a 100% reduction in the plasma level of clomipramine.
- adding oxcarbazepine, 600 mg in the morning and 900 mg at bedtime, to the regimen of a woman, age 44, with bipolar disorder led to a 71% decrease in the plasma level of valproate.
Topiramate. Topiramate—which is used as an antiepileptic and to treat mood disorders—has been shown to decrease digoxin levels by 11% and the estrogenic component of oral contraceptives by 30%. Topiramate may both induce and inhibit hepatic enzyme metabolism and has been associated with a 25% increase in phenytoin levels in some patients.
Other known inducers
Lesser-known hepatic enzyme inducers include chronic cigarette smoking,19 marijuana smoking,20 chronic ethanol use,21 modafinil,22 St. John’s wort,23 prednisone,16 dexamethasone,16 omeprazole,16 rifampin,16 and isoniazid.16 Unfortunately, the doses and duration required for induction are undocumented. The effect of these agents can only be detected by the astute clinician or perhaps by measuring plasma levels of co-prescribed drugs.
Among more than 20 known CYP450 isoenzymes, the six that metabolize most clinically useful medications are 1A2, 2C9, 2C19, 2D6, 2E1, and the 3A family. The 3A isoenzymes metabolize the widest range of drugs, so any agent that induces them is likely to have many interactions.
Inducing agents affect numerous specific enzymes (Table 3). For example:
- cigarette smoking induces at least 1A2
- carbamazepine and other anticonvulsants induce at least 3A4, 1A2, 2C9, 2C19, and 2D6
- alcohol induces at least 3A4 and 2E1.
The catalogue of hepatic enzymes, inducers, and specific enzymes and substrates (affected drugs) is poorly documented, inadequately studied, and difficult to commit to memory. It is much simpler to assume that any inducing agent in a patient’s regimen may lower plasma levels and alter the efficacy of co-administered drugs that are also metabolized by the liver.
Compensating for induction
A careful patient history and monitoring of clinical effect and plasma levels can compensate for the effects of hepatic enzyme inducers.4 Dosages of affected drugs may need to be adjusted to achieve desired therapeutic levels.
Table 3
HEPATIC INDUCERS1, AFFECTED ISOENZYMES2, AND SOME AFFECTED MEDICATIONS3
| Hepatic enzyme inducer | CYP1A2 | CYP2C19 | CYP2C9 | CYP2D6 | CYP3A family | CYP2E1 |
|---|---|---|---|---|---|---|
| Carbamazepine | Clozapine4 Amitriptyline Fluoxetine Haloperidol | Citalopram Diazepam Imipramine Fluoxetine | Warfarin | Risperidone Paroxetine Amphetamine Perphenazine | OCP5 Alprazolam Quetiapine | |
| Oxcarbazepine | Clomipramine | Clomipramine Risperidone | OCP | |||
| Phenytoin | Clozapine | Diazepam | OCP Quetiapine | |||
| Phenobarbital | Haloperidol Paroxetine Fluvoxamine | |||||
| Topiramate 6 | OCP | |||||
| Omeprazole | Clozapine | Phenytoin | ||||
| Rifampin | Phenytoin | Fluoxetine | ||||
| Prednisone | OCP | |||||
| Dexamethasone | Paroxetine | OCP | ||||
| Hypericum (St. John’s wort) | OCP Cyclosporine7 Haloperidol Pimozide | |||||
| Ethanol (chronic) | Tricyclics Neuroleptics | Alprazolam Trazodone Zaleplon | Ethanol Acetaminophen8 | |||
| Cigarette smoking | Haloperidol Clozapine | |||||
| OCP: Oral contraceptives 1 Only clinically relevant inducing agents listed 2 Cited by manufacturer or in literature 3 Examples of drugs known to be affected 4 Induction effect known, concomitant use not advisable due to possible addictive agranulocytosis risk 5 Among numerous medications metabolized by 3A isoenzymes 6 Acts as an inducer but also inhibits isoenzyme 2C19 7 St. John’s wort use has been associated with reduced cyclosporine levels and acute transplant rejection. 8 Chronic alcohol intake has been associated with accelerated acetaminophen metabolism and toxic metabolite levels. | ||||||
When an inducing agent is halted during psychotropic treatment, expect higher plasma levels, side effects, or even toxicity related to the psychotropic. This medication effect is likely as the inducing agent is tapered, discontinued, and cleared from the body (across approximately 5.5 times its half-life), and the induction process is gradually reversed.
Cessation of inducing agents has amplified the effects of clozapine8 and tricyclic antidepressants.10 Anecdotally, the taper and cessation of oxcarbazepine in the author’s bipolar patient resulted in a 40% increase in plasma risperidone level and an 118% increase in valproic acid level, without any increase in the dosage of either psychotropic. At baseline, the patient’s risperidone plasma level was 58 ng/ml (all parent compound). After oxcarbazepine was tapered and discontinued across 1 month, a repeat measurement of risperidone yielded a higher total plasma level (76 ng/ml) but an altered parent drug-to-metabolite ratio (risperidone 68 ng/ml, metabolite 8 ng/ml). This suggests that induction reversal was incomplete 2 weeks after oxcarbazepine was discontinued.
The literature offers little data on timelines for the onset and reversal of hepatic enzyme induction. Induction probably begins and becomes complete within days or weeks after drug therapy is initiated and steady-state levels are achieved. Similarly, the reversal likely occurs within days or weeks after clearance of the inducer.
How plasma levels correlate with clinical findings is the key, of course, and one must account for other possible influences, such as the presence of other hepatic enzyme inducers and inhibitors, dosage adjustments, cigarette smoking, chronic alcohol abuse, and other factors.
- Prescription or nonprescription agents (e.g., cigarette smoking, St. John’s wort) may induce hepatic enzymes.
- Inducing agents can lower plasma levels of co-administered medications that are also metabolized by the liver.
- Most psychotropics are metabolized by the liver, and their therapeutic effect requires a minimum plasma concentration.
- Hepatic enzyme induction can result in subtherapeutic plasma levels and inadequate drug trials of prescribed psychotropics.
- Assume that any inducing agent may lower plasma levels and alter the efficacy of co-administered drugs that are also metabolized by the liver. Observe carefully, monitor plasma levels, and use incremental dosing to assess and compensate for induction effects.
Five principles
When prescribing psychotropics, careful attention to five principles for managing the effects of hepatic enzyme induction (Box ) can result in:
- fewer patients with refractory symptoms
- less polypharmacy
- fewer sequelae of undertreated serious psychiatric illness
- improved therapy of comorbid medical conditions whose therapeutic agents may be metabolized by the liver and are therefore vulnerable to the effects of hepatic enzyme induction.
- Flockhart D. Indiana University Department of Medicine. Cytochrome P450 drug interaction table. http://www.Drug-Interactions.com
- DePiro JT, Talbert RL, Yee, GC, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002.
- Bernstein JG. Handbook of drug therapy in psychiatry. New York: Mosby-Year Book, 1995.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clomipramine • Anafranil
- Citalopram • Celexa
- Clozapine • Clozaril
- Diazepam • Valium
- Doxepin • Sinequan
- Dexamethasone • Decadron
- Fluphenazine • Prolixin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Isoniazid • Rifamate
- Modafinil • Provigil
- Nortriptyline • Pamelor
- Omeprazole • Prilosec
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Phenytoin • Dilantin
- Pimozide • Orap
- Primidone • Mysoline
- Quetiapine • Seroquel
- Rifampin • Rifadin
- Risperidone • Risperdal
- Trazodone • Desyrel
- Valproate • Depakote
- Warfarin • Coumadin
- Zaleplon • Sonata
Dr. Baird reports that he has served as a consultant to Eli Lilly and Co.
Psychiatrists know that common psychotropic medications can inhibit the liver’s cytochrome P450 enzyme system, increasing both plasma levels and the toxicity of co-administered drugs. Less well-known, perhaps, is that the opposite process—hepatic enzyme induction—can accelerate the liver’s meolism of co-administered drugs, resulting in abnormally low plasma levels.
Hepatic enzyme-inducing agents may appear in a patient’s regimen by prescription or self-administration (e.g., cigarette smoking, use of St. John’s wort, etc.) (Table 1). Most psychotropics are metabolized by the liver, and co-administering them with a hepatic enzyme inducer may cause pharmacokinetic consequences, including lowered plasma levels of the parent compound and elevated plasma levels of its metabolites. These plasma level changes may result in:
- reduced efficacy (e.g., if the parent drug alone is responsible for clinical benefit)
- greater efficacy (e.g., with the prodrug codeine, where the analgesic effect may be amplified by accelerated metabolism into its active drug, morphine)
- or no change in clinical effect (e.g., if the metabolite of the parent drug is active and its increased plasma level sufficiently compensates for the decreased plasma level of the parent compound).
This article offers an overview of common inducers and the drugs they affect, as well as five principles that can help you anticipate and manage potential drug-drug interactions.
Table 1
COMMON AGENTS ASSOCIATED WITH HEPATIC ENZYME INDUCTION
| Prescription | Nonprescription |
|---|---|
| Carbamazepine | Chronic cigarette smoking |
| Dexamethasone | Chronic ethanol use |
| Isoniazid | Chronic marijuana smoking |
| Modafinil | St. John’s wort |
| Omeprazole | |
| Oxcarbazepine | |
| Phenobarbital | |
| Phenytoin | |
| Prednisone | |
| Primidone | |
| Rifampin |
Carbamazepine
Carbamazepine is the best-known and most-thoroughly documented agent that can induce hepatic enzymes and lower plasma levels of co-administered drugs, both psychiatric and nonpsychiatric. This anticonvulsant also shows evidence of autoinduction, the unusual property of inducing its own accelerated hepatic metabolism.1
Carbamazepine is a powerful inducer of CYP3A, the most abundant family of cytochrome P450 enzymes.2 With initial carbamazepine therapy, hepatic enzyme induction begins within 3 to 5 days and is complete within 21 to 28 days.3 Because any co-administered drug requires some (often unknown) minimum plasma concentration for efficacy—and sometimes requires a “therapeutic window” level4— an inducing agent such as carbamazepine may compromise the other drug’s effectiveness.
Effect on neuroleptics. Drugs and classes of psychotropics whose levels and/or efficacies may be reduced in the presence of enzyme-inducing agents are listed in Table 2. For example, when carbamazepine and haloperidol are co-administered, haloperidol plasma levels may be reduced by 60%.5 The literature also shows a 50% reduction in fluphenazine levels6 and substantially reduced levels of valproic acid,7 clozapine,8 and perphenazine9 when co-administered with carbamazepine. Data on how these changes alter the drugs’ clinical effects are mixed: some patients have improved, and some have worsened.
It is unclear whether carbamazepine’s presence may lower drug levels into or below a neuroleptic plasma “therapeutic window,” or whether some observed patient improvement might occur as an independent augmenting effect of carbamazepine. Clearly, however, the presence or addition of the inducing agent—carbamazepine—substantially lowers neuroleptic plasma levels.
Effect on antidepressants. Carbamazepine has similar plasma level-reducing effects on antidepressants:
- amitriptyline and nortriptyline levels have been shown to be reduced by 40%10
- bupropion peak levels are decreased by 87%11
- levels of clomipramine,12 imipramine,13 and doxepin show marked reductions.10
Table 2
PSYCHOTROPICS AFFECTED* BY HEPATIC ENZYME INDUCERS
| Antidepressants (tricyclics and potentially SSRIs) |
| Antipsychotics (neuroleptics and atypicals) |
| Benzodiazepines |
| Bupropion |
| Valproate |
| * Exhibit reduced plasma levels and/or impaired efficacy when co-administered |
Other anticonvulsants
For unclear reasons, anticonvulsants are often hepatic enzyme inducers. Phenobarbitol, primidone, and phenytoin have been associated with reduced plasma levels of numerous drugs.16 For example, phenytoin has been reported to increase clearance of the atypical antipsychotic quetiapine. In one report, phenytoin cessation resulted in a 24-fold increase in plasma quetiapine levels. Similarly, carbamazepine cessation increased quetiapine plasma levels 14-fold.17
Oxcarbazepine. Oxcarbazepine is a newer anticonvulsant—a keto-analogue of carbamazepine—that offers improved safety in overdose, no cardiotoxic effect, and no known risk of agranulocytosis. Like older anticonvulsants, oxcarbazepine is being used to treat mood disorders.
Oxcarbazepine has been described as exhibiting “mild induction” of hepatic enzymes.18 The drug’s manufacturer reports that the agent can induce the 3A4 hepatic enzyme, reduce levels of oral contraceptives by 50%, and decrease calcium channel blocker levels by 28%.16 In two patients recently treated by the author:
- adding oxcarbazepine, 600 mg bid, to the regimen of a male patient, age 46, with schizophrenia and obsessive-compulsive disorder resulted in a 100% reduction in the plasma level of clomipramine.
- adding oxcarbazepine, 600 mg in the morning and 900 mg at bedtime, to the regimen of a woman, age 44, with bipolar disorder led to a 71% decrease in the plasma level of valproate.
Topiramate. Topiramate—which is used as an antiepileptic and to treat mood disorders—has been shown to decrease digoxin levels by 11% and the estrogenic component of oral contraceptives by 30%. Topiramate may both induce and inhibit hepatic enzyme metabolism and has been associated with a 25% increase in phenytoin levels in some patients.
Other known inducers
Lesser-known hepatic enzyme inducers include chronic cigarette smoking,19 marijuana smoking,20 chronic ethanol use,21 modafinil,22 St. John’s wort,23 prednisone,16 dexamethasone,16 omeprazole,16 rifampin,16 and isoniazid.16 Unfortunately, the doses and duration required for induction are undocumented. The effect of these agents can only be detected by the astute clinician or perhaps by measuring plasma levels of co-prescribed drugs.
Among more than 20 known CYP450 isoenzymes, the six that metabolize most clinically useful medications are 1A2, 2C9, 2C19, 2D6, 2E1, and the 3A family. The 3A isoenzymes metabolize the widest range of drugs, so any agent that induces them is likely to have many interactions.
Inducing agents affect numerous specific enzymes (Table 3). For example:
- cigarette smoking induces at least 1A2
- carbamazepine and other anticonvulsants induce at least 3A4, 1A2, 2C9, 2C19, and 2D6
- alcohol induces at least 3A4 and 2E1.
The catalogue of hepatic enzymes, inducers, and specific enzymes and substrates (affected drugs) is poorly documented, inadequately studied, and difficult to commit to memory. It is much simpler to assume that any inducing agent in a patient’s regimen may lower plasma levels and alter the efficacy of co-administered drugs that are also metabolized by the liver.
Compensating for induction
A careful patient history and monitoring of clinical effect and plasma levels can compensate for the effects of hepatic enzyme inducers.4 Dosages of affected drugs may need to be adjusted to achieve desired therapeutic levels.
Table 3
HEPATIC INDUCERS1, AFFECTED ISOENZYMES2, AND SOME AFFECTED MEDICATIONS3
| Hepatic enzyme inducer | CYP1A2 | CYP2C19 | CYP2C9 | CYP2D6 | CYP3A family | CYP2E1 |
|---|---|---|---|---|---|---|
| Carbamazepine | Clozapine4 Amitriptyline Fluoxetine Haloperidol | Citalopram Diazepam Imipramine Fluoxetine | Warfarin | Risperidone Paroxetine Amphetamine Perphenazine | OCP5 Alprazolam Quetiapine | |
| Oxcarbazepine | Clomipramine | Clomipramine Risperidone | OCP | |||
| Phenytoin | Clozapine | Diazepam | OCP Quetiapine | |||
| Phenobarbital | Haloperidol Paroxetine Fluvoxamine | |||||
| Topiramate 6 | OCP | |||||
| Omeprazole | Clozapine | Phenytoin | ||||
| Rifampin | Phenytoin | Fluoxetine | ||||
| Prednisone | OCP | |||||
| Dexamethasone | Paroxetine | OCP | ||||
| Hypericum (St. John’s wort) | OCP Cyclosporine7 Haloperidol Pimozide | |||||
| Ethanol (chronic) | Tricyclics Neuroleptics | Alprazolam Trazodone Zaleplon | Ethanol Acetaminophen8 | |||
| Cigarette smoking | Haloperidol Clozapine | |||||
| OCP: Oral contraceptives 1 Only clinically relevant inducing agents listed 2 Cited by manufacturer or in literature 3 Examples of drugs known to be affected 4 Induction effect known, concomitant use not advisable due to possible addictive agranulocytosis risk 5 Among numerous medications metabolized by 3A isoenzymes 6 Acts as an inducer but also inhibits isoenzyme 2C19 7 St. John’s wort use has been associated with reduced cyclosporine levels and acute transplant rejection. 8 Chronic alcohol intake has been associated with accelerated acetaminophen metabolism and toxic metabolite levels. | ||||||
When an inducing agent is halted during psychotropic treatment, expect higher plasma levels, side effects, or even toxicity related to the psychotropic. This medication effect is likely as the inducing agent is tapered, discontinued, and cleared from the body (across approximately 5.5 times its half-life), and the induction process is gradually reversed.
Cessation of inducing agents has amplified the effects of clozapine8 and tricyclic antidepressants.10 Anecdotally, the taper and cessation of oxcarbazepine in the author’s bipolar patient resulted in a 40% increase in plasma risperidone level and an 118% increase in valproic acid level, without any increase in the dosage of either psychotropic. At baseline, the patient’s risperidone plasma level was 58 ng/ml (all parent compound). After oxcarbazepine was tapered and discontinued across 1 month, a repeat measurement of risperidone yielded a higher total plasma level (76 ng/ml) but an altered parent drug-to-metabolite ratio (risperidone 68 ng/ml, metabolite 8 ng/ml). This suggests that induction reversal was incomplete 2 weeks after oxcarbazepine was discontinued.
The literature offers little data on timelines for the onset and reversal of hepatic enzyme induction. Induction probably begins and becomes complete within days or weeks after drug therapy is initiated and steady-state levels are achieved. Similarly, the reversal likely occurs within days or weeks after clearance of the inducer.
How plasma levels correlate with clinical findings is the key, of course, and one must account for other possible influences, such as the presence of other hepatic enzyme inducers and inhibitors, dosage adjustments, cigarette smoking, chronic alcohol abuse, and other factors.
- Prescription or nonprescription agents (e.g., cigarette smoking, St. John’s wort) may induce hepatic enzymes.
- Inducing agents can lower plasma levels of co-administered medications that are also metabolized by the liver.
- Most psychotropics are metabolized by the liver, and their therapeutic effect requires a minimum plasma concentration.
- Hepatic enzyme induction can result in subtherapeutic plasma levels and inadequate drug trials of prescribed psychotropics.
- Assume that any inducing agent may lower plasma levels and alter the efficacy of co-administered drugs that are also metabolized by the liver. Observe carefully, monitor plasma levels, and use incremental dosing to assess and compensate for induction effects.
Five principles
When prescribing psychotropics, careful attention to five principles for managing the effects of hepatic enzyme induction (Box ) can result in:
- fewer patients with refractory symptoms
- less polypharmacy
- fewer sequelae of undertreated serious psychiatric illness
- improved therapy of comorbid medical conditions whose therapeutic agents may be metabolized by the liver and are therefore vulnerable to the effects of hepatic enzyme induction.
- Flockhart D. Indiana University Department of Medicine. Cytochrome P450 drug interaction table. http://www.Drug-Interactions.com
- DePiro JT, Talbert RL, Yee, GC, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002.
- Bernstein JG. Handbook of drug therapy in psychiatry. New York: Mosby-Year Book, 1995.
- Alprazolam • Xanax
- Amitriptyline • Elavil
- Buproprion • Wellbutrin
- Carbamazepine • Tegretol
- Clomipramine • Anafranil
- Citalopram • Celexa
- Clozapine • Clozaril
- Diazepam • Valium
- Doxepin • Sinequan
- Dexamethasone • Decadron
- Fluphenazine • Prolixin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Haloperidol • Haldol
- Imipramine • Tofranil
- Isoniazid • Rifamate
- Modafinil • Provigil
- Nortriptyline • Pamelor
- Omeprazole • Prilosec
- Oxcarbazepine • Trileptal
- Paroxetine • Paxil
- Perphenazine • Trilafon
- Phenytoin • Dilantin
- Pimozide • Orap
- Primidone • Mysoline
- Quetiapine • Seroquel
- Rifampin • Rifadin
- Risperidone • Risperdal
- Trazodone • Desyrel
- Valproate • Depakote
- Warfarin • Coumadin
- Zaleplon • Sonata
Dr. Baird reports that he has served as a consultant to Eli Lilly and Co.
1. Rosenbaum JF. Drug treatment of resistant depression: reviewing options. Boston: Harvard Psychopharmacology Review, October 21, 1990.
2. Steffens DC, Krishnan RR, Doraiswamy PM. Psychotropic drug interactions. New York: MBL Communications, 1997.
3. Gidal BE, Garnett WR, Graves N. Epilepsy. In: DiPiro JT, Talbert RL, Yee GE, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002;1031-59.
4. Preskorn SH, Burke MJ, Fast GA. Therapeutic drug monitoring: principles and practice. Psychiatric Clin North Am 1993;16(3):611-41.
5. Arana GW, Goff DC, Friedman H, et al. Does carbamazepine-induced reduction of plasma haloperidol levels worsen psychotic symptoms? Am J Psychiatry 1986;143:650-1.
6. Jann MW, Fidone GS, Hernandez JM, et al. Clinical implications of increased antipsychotic plasma concentrations upon anticonvulsant cessation. Psychiatry Res 1989;28:153-9.
7. Wilder BJ. Pharmacokinetics of valproate and carbamazepine. J Clin Psychopharmacol 1992;12(1):64S-67S.
8. Raitasuo V, Lehtovarra R, Huttunen MO. Carbamazepine and plasma levels of clozapine. Am J Psychiatry 1993;150(1):169.-
9. Nelson JC. Combined treatment strategies in psychiatry. J Clin Psychiatry 1993;54 (suppl 9):42-9.
10. Leinonen E, Lillsunde P, Laukkanen V, et al. Effects of carbamazepine on serum antidepressant concentration in psychiatric patients. J Clin Psychopharmacology 1991;11:313-18.
11. Ketter TA, Jenkins JB, Schroeder DH, et al. Carbamazepine but not valproate induces buproprion metabolism. J Clin Psychopharmacology 1995;15:327-33.
12. De la Fuente JM, Mendlewicz J. Carbamazepine addition in tricyclic antidepressant-resistant unipolar depression. Biol Psychiatry 1992;32:369-74.
13. Brown CS, Wells BG, Cold JA. Possible influence of carbamazepine on plasma imipramine concentration in children with attention deficit hyperactivity disorder. J Clin Psychopharmacol 1990;10:359-62.
14. Arana GW, Epstein S, Molloy M, et al. Carbamazepine-induced reduction of plasma alprazolam concentrations: a clinical case report. J Clin Psychiatry 1988;49:448-9.
15. Callahan AM, Fava M, Rosenbaum JF. Drug interactions in psychopharmacology. Psychiatric Clin North Am 1993;16:647-71.
16. Physician’s Desk Reference. Montvale, NJ: Medical Economics, 2002.
17. Savasi I, Millson RC, Owen JA. Quetiapine blood level variability. Can J Psychiatry 2002;47:94.-
18. Ghaemi S, Ko J. Oxcarbazepine treatment of bipolar disorder: a review of the literature. Primary Psychiatry 2002;9:55-9.
19. Brown RA, Goldstein MG, Niaura R, et al. Nicotine dependence: assessment and management. In: Stoudemire A, Fogel BS (eds). Psychiatric care of the medical patient. New York: Oxford University Press, 1993;877-901.
20. Bauer LA. Clinical pharmacokinetics and pharmacodynamics. In: DiPiro JT, Talbert RL, Yee GC, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill, 2002;33-54.
21. Franklin JE, Frances RJ. Substance-related disorders. In: Rundell JR, Wise MG (eds). Textbook of consultation-liaison psychiatry. Washington, DC: American Psychiatric Press, 1996;427-65.
22. Flockhart D. Indiana University Department of Medicine. Cytochrome P450 drug interaction table. http://www.drug-interactions.com.
23. Crisman ML, Dorson PG. Schizophrenia. In: DiPiro JT, Talbert RL, Yee GE, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002;1219-42.
1. Rosenbaum JF. Drug treatment of resistant depression: reviewing options. Boston: Harvard Psychopharmacology Review, October 21, 1990.
2. Steffens DC, Krishnan RR, Doraiswamy PM. Psychotropic drug interactions. New York: MBL Communications, 1997.
3. Gidal BE, Garnett WR, Graves N. Epilepsy. In: DiPiro JT, Talbert RL, Yee GE, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002;1031-59.
4. Preskorn SH, Burke MJ, Fast GA. Therapeutic drug monitoring: principles and practice. Psychiatric Clin North Am 1993;16(3):611-41.
5. Arana GW, Goff DC, Friedman H, et al. Does carbamazepine-induced reduction of plasma haloperidol levels worsen psychotic symptoms? Am J Psychiatry 1986;143:650-1.
6. Jann MW, Fidone GS, Hernandez JM, et al. Clinical implications of increased antipsychotic plasma concentrations upon anticonvulsant cessation. Psychiatry Res 1989;28:153-9.
7. Wilder BJ. Pharmacokinetics of valproate and carbamazepine. J Clin Psychopharmacol 1992;12(1):64S-67S.
8. Raitasuo V, Lehtovarra R, Huttunen MO. Carbamazepine and plasma levels of clozapine. Am J Psychiatry 1993;150(1):169.-
9. Nelson JC. Combined treatment strategies in psychiatry. J Clin Psychiatry 1993;54 (suppl 9):42-9.
10. Leinonen E, Lillsunde P, Laukkanen V, et al. Effects of carbamazepine on serum antidepressant concentration in psychiatric patients. J Clin Psychopharmacology 1991;11:313-18.
11. Ketter TA, Jenkins JB, Schroeder DH, et al. Carbamazepine but not valproate induces buproprion metabolism. J Clin Psychopharmacology 1995;15:327-33.
12. De la Fuente JM, Mendlewicz J. Carbamazepine addition in tricyclic antidepressant-resistant unipolar depression. Biol Psychiatry 1992;32:369-74.
13. Brown CS, Wells BG, Cold JA. Possible influence of carbamazepine on plasma imipramine concentration in children with attention deficit hyperactivity disorder. J Clin Psychopharmacol 1990;10:359-62.
14. Arana GW, Epstein S, Molloy M, et al. Carbamazepine-induced reduction of plasma alprazolam concentrations: a clinical case report. J Clin Psychiatry 1988;49:448-9.
15. Callahan AM, Fava M, Rosenbaum JF. Drug interactions in psychopharmacology. Psychiatric Clin North Am 1993;16:647-71.
16. Physician’s Desk Reference. Montvale, NJ: Medical Economics, 2002.
17. Savasi I, Millson RC, Owen JA. Quetiapine blood level variability. Can J Psychiatry 2002;47:94.-
18. Ghaemi S, Ko J. Oxcarbazepine treatment of bipolar disorder: a review of the literature. Primary Psychiatry 2002;9:55-9.
19. Brown RA, Goldstein MG, Niaura R, et al. Nicotine dependence: assessment and management. In: Stoudemire A, Fogel BS (eds). Psychiatric care of the medical patient. New York: Oxford University Press, 1993;877-901.
20. Bauer LA. Clinical pharmacokinetics and pharmacodynamics. In: DiPiro JT, Talbert RL, Yee GC, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw Hill, 2002;33-54.
21. Franklin JE, Frances RJ. Substance-related disorders. In: Rundell JR, Wise MG (eds). Textbook of consultation-liaison psychiatry. Washington, DC: American Psychiatric Press, 1996;427-65.
22. Flockhart D. Indiana University Department of Medicine. Cytochrome P450 drug interaction table. http://www.drug-interactions.com.
23. Crisman ML, Dorson PG. Schizophrenia. In: DiPiro JT, Talbert RL, Yee GE, et al (eds). Pharmacotherapy: A pathophysiologic approach. New York: McGraw-Hill, 2002;1219-42.