User login
Algorithms and guidelines: Superhighway road maps for treatment
Online algorithms and guidelines offer fast access to evidence-based, clinically applicable information on treating a range of psychiatric disorders (Current Psychiatry 2004;3(2):22-40.
Disclosure
Drs. Kung and Lapid report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
To comment on this article or share an algorithm that works in your practice, click here.
Online algorithms and guidelines offer fast access to evidence-based, clinically applicable information on treating a range of psychiatric disorders (Current Psychiatry 2004;3(2):22-40.
Disclosure
Drs. Kung and Lapid report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
To comment on this article or share an algorithm that works in your practice, click here.
Online algorithms and guidelines offer fast access to evidence-based, clinically applicable information on treating a range of psychiatric disorders (Current Psychiatry 2004;3(2):22-40.
Disclosure
Drs. Kung and Lapid report no financial relationship with any company whose products are mentioned in this article, or with manufacturers of competing products.
To comment on this article or share an algorithm that works in your practice, click here.
Get serotonin syndrome down cold with SHIVERS
Critical initial treatment of serotonin syndrome (SS) depends on its swift and accurate identification. But the diagnosis can be complicated by nonspecific laboratory markers and physical symptoms similar to other hyperthermic disorders, such as neuroleptic malignant syndrome and anticholinergic toxicity.
You can recall SS’s hallmark physical symptoms with the acronym SHIVERS (Box).
Differentiating SS from other hyperthermic states requires a thorough review of the patient’s medical and drug history, clinical findings, and laboratory results. If diagnosed shortly after symptom onset and before muscular hypertonicity and hyperthermia develop, most uncomplicated SS cases resolve uneventfully over 24 hours. The key is to discontinue the causative agents, monitor vital signs, and administer IV fluids.1
Cyproheptadine, 4 mg every 4 hours as needed, is the recommended therapy, but further investigation is needed to confirm its effectiveness in alleviating SS or preventing a more-severe, potentially fatal course.2 Try benzodiazepines such as lorazepam (1 to 2 mg slow IV push) to moderate temperature, control agitation, and blunt the syndrome’s hyperadrenergic component. Intensive care is warranted in severe cases involving hypertonicity, rhabdomyolosis, and hyperthermia (temperature >41°C).
S hivering, one of the neuromuscular symptoms unique to SS, helps distinguish it from other hyperthermic syndromes
H yperreflexia and myoclonus are frequently seen in mild to moderate cases and are especially notable in the lower extremities; muscular rigidity occurs only in more severe cases
I ncreased temperature, although variable in SS and usually observed in severe cases, is likely caused by muscular hypertonicity
V ital sign instability can present as tachycardia, tachypnea, and/or labile blood pressure
E ncephalopathy—characterized by mental status changes such as agitation, delirium, confusion, and to a lesser extent obtundation—can develop from hyperthermia
R estlessness and incoordination are common because of excess serotonin activity
S weating (diaphoresis) is an autonomic response to excessive serotonin stimulation; by comparison, anticholinergic toxicity usually manifests with hot, dry skin
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;353(11):1112-20.
2. Sternbach H. Serotonin syndrome: How to avoid, identify and treat dangerous drug interactions. Current Psychiatry 2003;2(5):15-24.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Critical initial treatment of serotonin syndrome (SS) depends on its swift and accurate identification. But the diagnosis can be complicated by nonspecific laboratory markers and physical symptoms similar to other hyperthermic disorders, such as neuroleptic malignant syndrome and anticholinergic toxicity.
You can recall SS’s hallmark physical symptoms with the acronym SHIVERS (Box).
Differentiating SS from other hyperthermic states requires a thorough review of the patient’s medical and drug history, clinical findings, and laboratory results. If diagnosed shortly after symptom onset and before muscular hypertonicity and hyperthermia develop, most uncomplicated SS cases resolve uneventfully over 24 hours. The key is to discontinue the causative agents, monitor vital signs, and administer IV fluids.1
Cyproheptadine, 4 mg every 4 hours as needed, is the recommended therapy, but further investigation is needed to confirm its effectiveness in alleviating SS or preventing a more-severe, potentially fatal course.2 Try benzodiazepines such as lorazepam (1 to 2 mg slow IV push) to moderate temperature, control agitation, and blunt the syndrome’s hyperadrenergic component. Intensive care is warranted in severe cases involving hypertonicity, rhabdomyolosis, and hyperthermia (temperature >41°C).
S hivering, one of the neuromuscular symptoms unique to SS, helps distinguish it from other hyperthermic syndromes
H yperreflexia and myoclonus are frequently seen in mild to moderate cases and are especially notable in the lower extremities; muscular rigidity occurs only in more severe cases
I ncreased temperature, although variable in SS and usually observed in severe cases, is likely caused by muscular hypertonicity
V ital sign instability can present as tachycardia, tachypnea, and/or labile blood pressure
E ncephalopathy—characterized by mental status changes such as agitation, delirium, confusion, and to a lesser extent obtundation—can develop from hyperthermia
R estlessness and incoordination are common because of excess serotonin activity
S weating (diaphoresis) is an autonomic response to excessive serotonin stimulation; by comparison, anticholinergic toxicity usually manifests with hot, dry skin
Critical initial treatment of serotonin syndrome (SS) depends on its swift and accurate identification. But the diagnosis can be complicated by nonspecific laboratory markers and physical symptoms similar to other hyperthermic disorders, such as neuroleptic malignant syndrome and anticholinergic toxicity.
You can recall SS’s hallmark physical symptoms with the acronym SHIVERS (Box).
Differentiating SS from other hyperthermic states requires a thorough review of the patient’s medical and drug history, clinical findings, and laboratory results. If diagnosed shortly after symptom onset and before muscular hypertonicity and hyperthermia develop, most uncomplicated SS cases resolve uneventfully over 24 hours. The key is to discontinue the causative agents, monitor vital signs, and administer IV fluids.1
Cyproheptadine, 4 mg every 4 hours as needed, is the recommended therapy, but further investigation is needed to confirm its effectiveness in alleviating SS or preventing a more-severe, potentially fatal course.2 Try benzodiazepines such as lorazepam (1 to 2 mg slow IV push) to moderate temperature, control agitation, and blunt the syndrome’s hyperadrenergic component. Intensive care is warranted in severe cases involving hypertonicity, rhabdomyolosis, and hyperthermia (temperature >41°C).
S hivering, one of the neuromuscular symptoms unique to SS, helps distinguish it from other hyperthermic syndromes
H yperreflexia and myoclonus are frequently seen in mild to moderate cases and are especially notable in the lower extremities; muscular rigidity occurs only in more severe cases
I ncreased temperature, although variable in SS and usually observed in severe cases, is likely caused by muscular hypertonicity
V ital sign instability can present as tachycardia, tachypnea, and/or labile blood pressure
E ncephalopathy—characterized by mental status changes such as agitation, delirium, confusion, and to a lesser extent obtundation—can develop from hyperthermia
R estlessness and incoordination are common because of excess serotonin activity
S weating (diaphoresis) is an autonomic response to excessive serotonin stimulation; by comparison, anticholinergic toxicity usually manifests with hot, dry skin
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;353(11):1112-20.
2. Sternbach H. Serotonin syndrome: How to avoid, identify and treat dangerous drug interactions. Current Psychiatry 2003;2(5):15-24.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
1. Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med 2005;353(11):1112-20.
2. Sternbach H. Serotonin syndrome: How to avoid, identify and treat dangerous drug interactions. Current Psychiatry 2003;2(5):15-24.
Dr. Christensen is associate professor of psychiatry, University of Florida College of Medicine, Jacksonville, and director of the university’s community psychiatry program.
Make tardive dyskinesia passé with PASST principle
Often disfiguring and irreversible, tardive dyskinesia (TD) remains a problem for patients on maintenance antipsychotics. Central dopamine blockade is believed to contribute to TD’s pathology, but the exact cause remains unknown and treatment results are variable.1,2
To optimally manage TD, remember the PASST principle—an acronym that includes strategies to prevent, assess, switch, suppress, and treat TD. This principle—based on clinical practice, colleague experiences, and literature reviews—has been helpful for training residents how best to manage this difficult condition.
Prevent. To lower your patient’s risk of developing TD:
- reconsider whether an antipsychotic is needed, especially in high-risk patients who are older, have negative symptoms of schizophrenia, experience acute extrapyramidal symptoms, or have affective disorders3
- prescribe atypical antipsychotics, which are less likely than the typical agents to produce TD
- use the minimum effective dosage and duration.
Assess. Screen for dyskinetic movements before you start an antipsychotic and approximately every 6 months, using the Abnormal Involuntary Movement Scale (AIMS). The AIMS is easy to administer and score and can detect subtle dyskinesias at an early stage.
Switch. If you identify TD, stop the offending antipsychotic. Switch to a different drug class if psychotic relapse is not an issue (for example, in a patient taking an antipsychotic for treatment-resistant depression).
For patients who require maintenance treatment with antipsychotics, switch from a first-generation antipsychotic to an atypical. Second-generation agents such as olanzapine carry less TD risk than conventionals such as perphenazine. There may be differential risk among atypicals as well (for example, quetiapine is probably less likely to cause TD than risperidone).1 Also, TD triggered by one atypical may respond to another.4
Suppress. It may take time for a medication switch to decrease TD symptoms, if it happens at all. If a patient experiences dangerous or bothersome symptoms such as difficulty breathing or eating, increasing the antipsychotic dosage for a few weeks often provides short-term relief; reserve this approach for urgent clinical situations where switching antipsychotics would take too long or would otherwise be impractical.
Treat. Clozapine is first-line treatment for TD.5 A variety of non-antipsychotic medications have been used to reduce TD symptoms with inconsistent results (Table). Most carry mild side-effect risks and could be considered for patients who wish to try something to help alleviate symptoms.
Informed consent and collaborative decision-making are essential to managing TD. Inform patients of TD risk before starting an antipsychotic. If TD occurs, include them in decisions by explaining the risks, benefits, and reasons for switches and treatments. Some patients choose to tolerate mild TD so they can keep taking a medication that helps them stay well. Extensively document these discussions—along with your thought processes—in the medical record.
Table
Non-antipsychotic treatments that may reduce TD symptoms
| Class | Agent | Comments |
|---|---|---|
| Antioxidants | Vitamin E | >1,200 IU/d may be best to prevent deterioration, but cardiac risks increase at dosages >400 IU/d |
| GABA agonists | Benzodiazepines | Helps some patients, but may have nonspecific sedative effect; abuse potential |
| Gabapentin | >1,200 mg/d may help TD and/or blepharospasm | |
| 5HT agonists | Buspirone | >120 mg/d |
| Calcium channel blockers | Verapamil | 160 mg/d |
| Anticholinergics | Benztropine | Worsens TD initially, may help later; recommended for tardive dystonia |
| Others | Chelated manganese | 50 mg/d, especially when combined with vitamin E |
| Vitamin B6 | 300 mg/d | |
| Melatonin | 10 mg/d | |
| Branched chain amino acid mix (Tarvil) | 222 mg/kg tid superior to placebo in one study6 |
1. Simpson GM. The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 2000;61(Suppl 4):39-44.
2. Kulkarni SK, Naidu PS. Pathophysiology and drug therapy of tardive dyskinesia: Current concepts and future perspectives. Drugs Today 2003;39:19-49.
3. Gardos G. Tardive dyskinesia: How to prevent and treat a lingering nemesis. Current Psychiatry 2003;2(10):59-66.
4. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159(11):1948.-
5. Louzã MR, Bassitt DP. Maintenance treatment of severe tardive dyskinesia with clozapine: 5 years’ follow-up. J Clin Psychopharmacol 2005;25(2):180-2.
6. Richardson MA, Bevans ML, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
Dr. Rosenstock is director of medical student education, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pennsylvania.
Often disfiguring and irreversible, tardive dyskinesia (TD) remains a problem for patients on maintenance antipsychotics. Central dopamine blockade is believed to contribute to TD’s pathology, but the exact cause remains unknown and treatment results are variable.1,2
To optimally manage TD, remember the PASST principle—an acronym that includes strategies to prevent, assess, switch, suppress, and treat TD. This principle—based on clinical practice, colleague experiences, and literature reviews—has been helpful for training residents how best to manage this difficult condition.
Prevent. To lower your patient’s risk of developing TD:
- reconsider whether an antipsychotic is needed, especially in high-risk patients who are older, have negative symptoms of schizophrenia, experience acute extrapyramidal symptoms, or have affective disorders3
- prescribe atypical antipsychotics, which are less likely than the typical agents to produce TD
- use the minimum effective dosage and duration.
Assess. Screen for dyskinetic movements before you start an antipsychotic and approximately every 6 months, using the Abnormal Involuntary Movement Scale (AIMS). The AIMS is easy to administer and score and can detect subtle dyskinesias at an early stage.
Switch. If you identify TD, stop the offending antipsychotic. Switch to a different drug class if psychotic relapse is not an issue (for example, in a patient taking an antipsychotic for treatment-resistant depression).
For patients who require maintenance treatment with antipsychotics, switch from a first-generation antipsychotic to an atypical. Second-generation agents such as olanzapine carry less TD risk than conventionals such as perphenazine. There may be differential risk among atypicals as well (for example, quetiapine is probably less likely to cause TD than risperidone).1 Also, TD triggered by one atypical may respond to another.4
Suppress. It may take time for a medication switch to decrease TD symptoms, if it happens at all. If a patient experiences dangerous or bothersome symptoms such as difficulty breathing or eating, increasing the antipsychotic dosage for a few weeks often provides short-term relief; reserve this approach for urgent clinical situations where switching antipsychotics would take too long or would otherwise be impractical.
Treat. Clozapine is first-line treatment for TD.5 A variety of non-antipsychotic medications have been used to reduce TD symptoms with inconsistent results (Table). Most carry mild side-effect risks and could be considered for patients who wish to try something to help alleviate symptoms.
Informed consent and collaborative decision-making are essential to managing TD. Inform patients of TD risk before starting an antipsychotic. If TD occurs, include them in decisions by explaining the risks, benefits, and reasons for switches and treatments. Some patients choose to tolerate mild TD so they can keep taking a medication that helps them stay well. Extensively document these discussions—along with your thought processes—in the medical record.
Table
Non-antipsychotic treatments that may reduce TD symptoms
| Class | Agent | Comments |
|---|---|---|
| Antioxidants | Vitamin E | >1,200 IU/d may be best to prevent deterioration, but cardiac risks increase at dosages >400 IU/d |
| GABA agonists | Benzodiazepines | Helps some patients, but may have nonspecific sedative effect; abuse potential |
| Gabapentin | >1,200 mg/d may help TD and/or blepharospasm | |
| 5HT agonists | Buspirone | >120 mg/d |
| Calcium channel blockers | Verapamil | 160 mg/d |
| Anticholinergics | Benztropine | Worsens TD initially, may help later; recommended for tardive dystonia |
| Others | Chelated manganese | 50 mg/d, especially when combined with vitamin E |
| Vitamin B6 | 300 mg/d | |
| Melatonin | 10 mg/d | |
| Branched chain amino acid mix (Tarvil) | 222 mg/kg tid superior to placebo in one study6 |
Often disfiguring and irreversible, tardive dyskinesia (TD) remains a problem for patients on maintenance antipsychotics. Central dopamine blockade is believed to contribute to TD’s pathology, but the exact cause remains unknown and treatment results are variable.1,2
To optimally manage TD, remember the PASST principle—an acronym that includes strategies to prevent, assess, switch, suppress, and treat TD. This principle—based on clinical practice, colleague experiences, and literature reviews—has been helpful for training residents how best to manage this difficult condition.
Prevent. To lower your patient’s risk of developing TD:
- reconsider whether an antipsychotic is needed, especially in high-risk patients who are older, have negative symptoms of schizophrenia, experience acute extrapyramidal symptoms, or have affective disorders3
- prescribe atypical antipsychotics, which are less likely than the typical agents to produce TD
- use the minimum effective dosage and duration.
Assess. Screen for dyskinetic movements before you start an antipsychotic and approximately every 6 months, using the Abnormal Involuntary Movement Scale (AIMS). The AIMS is easy to administer and score and can detect subtle dyskinesias at an early stage.
Switch. If you identify TD, stop the offending antipsychotic. Switch to a different drug class if psychotic relapse is not an issue (for example, in a patient taking an antipsychotic for treatment-resistant depression).
For patients who require maintenance treatment with antipsychotics, switch from a first-generation antipsychotic to an atypical. Second-generation agents such as olanzapine carry less TD risk than conventionals such as perphenazine. There may be differential risk among atypicals as well (for example, quetiapine is probably less likely to cause TD than risperidone).1 Also, TD triggered by one atypical may respond to another.4
Suppress. It may take time for a medication switch to decrease TD symptoms, if it happens at all. If a patient experiences dangerous or bothersome symptoms such as difficulty breathing or eating, increasing the antipsychotic dosage for a few weeks often provides short-term relief; reserve this approach for urgent clinical situations where switching antipsychotics would take too long or would otherwise be impractical.
Treat. Clozapine is first-line treatment for TD.5 A variety of non-antipsychotic medications have been used to reduce TD symptoms with inconsistent results (Table). Most carry mild side-effect risks and could be considered for patients who wish to try something to help alleviate symptoms.
Informed consent and collaborative decision-making are essential to managing TD. Inform patients of TD risk before starting an antipsychotic. If TD occurs, include them in decisions by explaining the risks, benefits, and reasons for switches and treatments. Some patients choose to tolerate mild TD so they can keep taking a medication that helps them stay well. Extensively document these discussions—along with your thought processes—in the medical record.
Table
Non-antipsychotic treatments that may reduce TD symptoms
| Class | Agent | Comments |
|---|---|---|
| Antioxidants | Vitamin E | >1,200 IU/d may be best to prevent deterioration, but cardiac risks increase at dosages >400 IU/d |
| GABA agonists | Benzodiazepines | Helps some patients, but may have nonspecific sedative effect; abuse potential |
| Gabapentin | >1,200 mg/d may help TD and/or blepharospasm | |
| 5HT agonists | Buspirone | >120 mg/d |
| Calcium channel blockers | Verapamil | 160 mg/d |
| Anticholinergics | Benztropine | Worsens TD initially, may help later; recommended for tardive dystonia |
| Others | Chelated manganese | 50 mg/d, especially when combined with vitamin E |
| Vitamin B6 | 300 mg/d | |
| Melatonin | 10 mg/d | |
| Branched chain amino acid mix (Tarvil) | 222 mg/kg tid superior to placebo in one study6 |
1. Simpson GM. The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 2000;61(Suppl 4):39-44.
2. Kulkarni SK, Naidu PS. Pathophysiology and drug therapy of tardive dyskinesia: Current concepts and future perspectives. Drugs Today 2003;39:19-49.
3. Gardos G. Tardive dyskinesia: How to prevent and treat a lingering nemesis. Current Psychiatry 2003;2(10):59-66.
4. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159(11):1948.-
5. Louzã MR, Bassitt DP. Maintenance treatment of severe tardive dyskinesia with clozapine: 5 years’ follow-up. J Clin Psychopharmacol 2005;25(2):180-2.
6. Richardson MA, Bevans ML, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
Dr. Rosenstock is director of medical student education, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pennsylvania.
1. Simpson GM. The treatment of tardive dyskinesia and tardive dystonia. J Clin Psychiatry 2000;61(Suppl 4):39-44.
2. Kulkarni SK, Naidu PS. Pathophysiology and drug therapy of tardive dyskinesia: Current concepts and future perspectives. Drugs Today 2003;39:19-49.
3. Gardos G. Tardive dyskinesia: How to prevent and treat a lingering nemesis. Current Psychiatry 2003;2(10):59-66.
4. Suzuki E, Obata M, Yoshida Y, Miyaoka H. Tardive dyskinesia with risperidone and anticholinergics. Am J Psychiatry 2002;159(11):1948.-
5. Louzã MR, Bassitt DP. Maintenance treatment of severe tardive dyskinesia with clozapine: 5 years’ follow-up. J Clin Psychopharmacol 2005;25(2):180-2.
6. Richardson MA, Bevans ML, Read LL, et al. Efficacy of the branched-chain amino acids in the treatment of tardive dyskinesia in men. Am J Psychiatry 2003;160:1117-24.
Dr. Rosenstock is director of medical student education, Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, Pennsylvania.
How to adjust drug dosing after bariatric surgery
Bariatric surgery has increased 10-fold in the United States over the past decade.1 Because one-third of bariatric candidates take psychiatric medications, psychiatric input on postoperative management is in demand.2
Despite this surgery’s rising popularity, no data exist to guide psychotropic dosing in patients with altered GI environments and who experience massive postoperative weight loss. Evidence and clinical experience support these recommendations:
Managing changes in psychotropic absorption. The most common procedure, the Roux-en-Y gastric bypass (RYGB), bypasses the duodenum, proximal jejunum, and all of the stomach except the cardia (Figure). Because ingested food is normally absorbed in the duodenum and jejunum, a bypass results in relative malabsorption of food. Orally ingested food and medications pass into the cardia, where they are not exposed to acid.
One novel in vitro study2 examined the dissolution of 22 psychotropics in a simulated GI environment of control and post-RYGB states. Twelve medications dissolved differently in a postoperative environment than in the control state; 10 dissolved much less than expected.
The effect of bariatric surgery on in vivo absorption of commonly used psychotropics has not been studied. For safe yet effective dosing immediately after surgery, try:
- Using immediate-release psychotropics.3 Time-released medications are designed to dissolve gradually within the full intestinal tract. Extended-release formulations will probably have markedly different pharmacokinetics after RYGB. Coated pills require stomach acid to release active ingredients, so crush oral medications in the immediate postoperative period.
- Monitoring serum drug levels of medications with a narrow therapeutic index. Also measure preoperative blood levels while the patient feels well. This baseline will provide a target to aim for if the patient has a postoperative relapse.
Figure Roux-en-Y gastric bypass
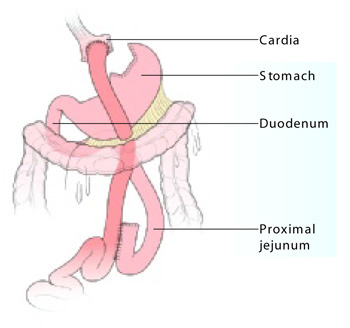
Vertical stapling of the upper stomach creates a small pouch, and a Y-shaped section of small intestine attached to the pouch allows food to bypass the duodenum and part of the jejunum.
Illustration: Jennifer Fairman
Postoperative weight loss. Many physiologic factors influence drug absorption, such as gastric emptying time and the integrity and surface area of the epithelium. The gut has an impressive capacity to compensate for loss of function, so absorption after surgery may eventually normalize. By that time, however, marked weight loss can complicate the clinical picture.
Compared with nonobese persons, obese persons have an increased proportion of adipose tissue, as well as increased total body water, lean body mass, visceral organ mass, and higher glomerular filtration rate.
Postoperative bariatric patients often lose more than 100 pounds of adipose tissue. This type of weight loss mostly affects lipid-soluble drugs with a large volume of distribution (Vd) that readily cross cell membranes, such as fluoxetine. Drugs with a large Vd, such as fluoxetine (Table), reach all major compartments of distribution, which in a normal weight individual include: plasma (5%), interstitial fluid (16%), intracellular fluid (35%), transcellular fluid (2%), and fat (20%). Because the amount of fat in an overweight patient is initially very high but rapidly decreases after bariatric surgery, drugs with a large Vd can shift into other compartments.
For drugs with a small Vd, such as lithium, a lower maintenance dosage may be required because of decreased glomerular filtration following marked weight loss.4
Table
Common drugs’ volume of distribution (Vd)
| Drug | Extent of distribution | Volume of distribution |
|---|---|---|
| Fluoxetine | Large | 10 to 103 L/kg |
| Citalopram | Moderate | 14 to 17 L/kg |
| Venlafaxine | Moderate | 6 to 7 L/kg |
| Oxcarbazepine | Small | 0.7 L/kg |
| Lithium | Small | 0.4 to 0.6 L/kg |
| Valproic acid | Small | 0.1 to 0.4 L/kg |
1. Tsao A. Weighing bariatric surgery’s risks. BusinessWeek Online. Available at: http://www.businessweek.com/bwdaily/dnflash/oct2004/nf20041028_0264_db092.htm. Accessed Nov. 28, 2005.
2. Seaman JS, Bowers SP, Dixon P, Schindler L. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics 2005;46(3):250-3.
3. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract 2003;18(2):131-5.
4. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging 2000;16(3):165-77.
Dr. McAlpine is assistant professor of psychiatry and director of eating disorders services, Mayo Clinic, Rochester, MN.
Bariatric surgery has increased 10-fold in the United States over the past decade.1 Because one-third of bariatric candidates take psychiatric medications, psychiatric input on postoperative management is in demand.2
Despite this surgery’s rising popularity, no data exist to guide psychotropic dosing in patients with altered GI environments and who experience massive postoperative weight loss. Evidence and clinical experience support these recommendations:
Managing changes in psychotropic absorption. The most common procedure, the Roux-en-Y gastric bypass (RYGB), bypasses the duodenum, proximal jejunum, and all of the stomach except the cardia (Figure). Because ingested food is normally absorbed in the duodenum and jejunum, a bypass results in relative malabsorption of food. Orally ingested food and medications pass into the cardia, where they are not exposed to acid.
One novel in vitro study2 examined the dissolution of 22 psychotropics in a simulated GI environment of control and post-RYGB states. Twelve medications dissolved differently in a postoperative environment than in the control state; 10 dissolved much less than expected.
The effect of bariatric surgery on in vivo absorption of commonly used psychotropics has not been studied. For safe yet effective dosing immediately after surgery, try:
- Using immediate-release psychotropics.3 Time-released medications are designed to dissolve gradually within the full intestinal tract. Extended-release formulations will probably have markedly different pharmacokinetics after RYGB. Coated pills require stomach acid to release active ingredients, so crush oral medications in the immediate postoperative period.
- Monitoring serum drug levels of medications with a narrow therapeutic index. Also measure preoperative blood levels while the patient feels well. This baseline will provide a target to aim for if the patient has a postoperative relapse.
Figure Roux-en-Y gastric bypass
Vertical stapling of the upper stomach creates a small pouch, and a Y-shaped section of small intestine attached to the pouch allows food to bypass the duodenum and part of the jejunum.
Illustration: Jennifer Fairman
Postoperative weight loss. Many physiologic factors influence drug absorption, such as gastric emptying time and the integrity and surface area of the epithelium. The gut has an impressive capacity to compensate for loss of function, so absorption after surgery may eventually normalize. By that time, however, marked weight loss can complicate the clinical picture.
Compared with nonobese persons, obese persons have an increased proportion of adipose tissue, as well as increased total body water, lean body mass, visceral organ mass, and higher glomerular filtration rate.
Postoperative bariatric patients often lose more than 100 pounds of adipose tissue. This type of weight loss mostly affects lipid-soluble drugs with a large volume of distribution (Vd) that readily cross cell membranes, such as fluoxetine. Drugs with a large Vd, such as fluoxetine (Table), reach all major compartments of distribution, which in a normal weight individual include: plasma (5%), interstitial fluid (16%), intracellular fluid (35%), transcellular fluid (2%), and fat (20%). Because the amount of fat in an overweight patient is initially very high but rapidly decreases after bariatric surgery, drugs with a large Vd can shift into other compartments.
For drugs with a small Vd, such as lithium, a lower maintenance dosage may be required because of decreased glomerular filtration following marked weight loss.4
Table
Common drugs’ volume of distribution (Vd)
| Drug | Extent of distribution | Volume of distribution |
|---|---|---|
| Fluoxetine | Large | 10 to 103 L/kg |
| Citalopram | Moderate | 14 to 17 L/kg |
| Venlafaxine | Moderate | 6 to 7 L/kg |
| Oxcarbazepine | Small | 0.7 L/kg |
| Lithium | Small | 0.4 to 0.6 L/kg |
| Valproic acid | Small | 0.1 to 0.4 L/kg |
Bariatric surgery has increased 10-fold in the United States over the past decade.1 Because one-third of bariatric candidates take psychiatric medications, psychiatric input on postoperative management is in demand.2
Despite this surgery’s rising popularity, no data exist to guide psychotropic dosing in patients with altered GI environments and who experience massive postoperative weight loss. Evidence and clinical experience support these recommendations:
Managing changes in psychotropic absorption. The most common procedure, the Roux-en-Y gastric bypass (RYGB), bypasses the duodenum, proximal jejunum, and all of the stomach except the cardia (Figure). Because ingested food is normally absorbed in the duodenum and jejunum, a bypass results in relative malabsorption of food. Orally ingested food and medications pass into the cardia, where they are not exposed to acid.
One novel in vitro study2 examined the dissolution of 22 psychotropics in a simulated GI environment of control and post-RYGB states. Twelve medications dissolved differently in a postoperative environment than in the control state; 10 dissolved much less than expected.
The effect of bariatric surgery on in vivo absorption of commonly used psychotropics has not been studied. For safe yet effective dosing immediately after surgery, try:
- Using immediate-release psychotropics.3 Time-released medications are designed to dissolve gradually within the full intestinal tract. Extended-release formulations will probably have markedly different pharmacokinetics after RYGB. Coated pills require stomach acid to release active ingredients, so crush oral medications in the immediate postoperative period.
- Monitoring serum drug levels of medications with a narrow therapeutic index. Also measure preoperative blood levels while the patient feels well. This baseline will provide a target to aim for if the patient has a postoperative relapse.
Figure Roux-en-Y gastric bypass
Vertical stapling of the upper stomach creates a small pouch, and a Y-shaped section of small intestine attached to the pouch allows food to bypass the duodenum and part of the jejunum.
Illustration: Jennifer Fairman
Postoperative weight loss. Many physiologic factors influence drug absorption, such as gastric emptying time and the integrity and surface area of the epithelium. The gut has an impressive capacity to compensate for loss of function, so absorption after surgery may eventually normalize. By that time, however, marked weight loss can complicate the clinical picture.
Compared with nonobese persons, obese persons have an increased proportion of adipose tissue, as well as increased total body water, lean body mass, visceral organ mass, and higher glomerular filtration rate.
Postoperative bariatric patients often lose more than 100 pounds of adipose tissue. This type of weight loss mostly affects lipid-soluble drugs with a large volume of distribution (Vd) that readily cross cell membranes, such as fluoxetine. Drugs with a large Vd, such as fluoxetine (Table), reach all major compartments of distribution, which in a normal weight individual include: plasma (5%), interstitial fluid (16%), intracellular fluid (35%), transcellular fluid (2%), and fat (20%). Because the amount of fat in an overweight patient is initially very high but rapidly decreases after bariatric surgery, drugs with a large Vd can shift into other compartments.
For drugs with a small Vd, such as lithium, a lower maintenance dosage may be required because of decreased glomerular filtration following marked weight loss.4
Table
Common drugs’ volume of distribution (Vd)
| Drug | Extent of distribution | Volume of distribution |
|---|---|---|
| Fluoxetine | Large | 10 to 103 L/kg |
| Citalopram | Moderate | 14 to 17 L/kg |
| Venlafaxine | Moderate | 6 to 7 L/kg |
| Oxcarbazepine | Small | 0.7 L/kg |
| Lithium | Small | 0.4 to 0.6 L/kg |
| Valproic acid | Small | 0.1 to 0.4 L/kg |
1. Tsao A. Weighing bariatric surgery’s risks. BusinessWeek Online. Available at: http://www.businessweek.com/bwdaily/dnflash/oct2004/nf20041028_0264_db092.htm. Accessed Nov. 28, 2005.
2. Seaman JS, Bowers SP, Dixon P, Schindler L. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics 2005;46(3):250-3.
3. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract 2003;18(2):131-5.
4. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging 2000;16(3):165-77.
Dr. McAlpine is assistant professor of psychiatry and director of eating disorders services, Mayo Clinic, Rochester, MN.
1. Tsao A. Weighing bariatric surgery’s risks. BusinessWeek Online. Available at: http://www.businessweek.com/bwdaily/dnflash/oct2004/nf20041028_0264_db092.htm. Accessed Nov. 28, 2005.
2. Seaman JS, Bowers SP, Dixon P, Schindler L. Dissolution of common psychiatric medications in a Roux-en-Y gastric bypass model. Psychosomatics 2005;46(3):250-3.
3. Malone M. Altered drug disposition in obesity and after bariatric surgery. Nutr Clin Pract 2003;18(2):131-5.
4. Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging 2000;16(3):165-77.
Dr. McAlpine is assistant professor of psychiatry and director of eating disorders services, Mayo Clinic, Rochester, MN.
Think PLANT to recall vegetative symptoms
Obvious positive symptoms of schizophrenia—such as hallucinations and delusions—typically prompt treatment, but positive symptoms may be absent or clouded by the rationalizations and minimization often seen in paranoia. Negative symptoms can also escape detection because of their subtlety.
Andreasen and Olson’s criteria for negative symptoms1 provide the basis for the Schedule for the Assessment of Negative Symptoms (SANS) that includes the five As: avolition/apathy, alogia, affective flattening, anhedonia/asociality, and attentional impairment.
Many remember Bleuler’s four As of schizophrenia—autism, loosening of associations, affective disturbances, and ambivalence—but may have a harder time remembering the SANS’ five As. I find the pseudo-acronym PLANT (for the vegetative changes manifested with negative symptoms) helpful for recalling all five As (Table).
Table
Use PLANT pseudo-acronym to recall vegetative symptoms
| Symptom | Meaning | Examples |
|---|---|---|
| aPathy/avolition | Lack of drive | Poor grooming |
| Anergia | ||
| Impersistence | ||
| aLogia | Marked impairment in thought processing and/or content | Poverty of speech |
| Poverty of content | ||
| Thought blocking | ||
| Latency of response | ||
| Poor abstracting | ||
| Affective disturbances | Altered expressiveness | Poor eye contact |
| Aprosodic speech | ||
| Lack of expression | ||
| Poverty of gestures | ||
| aNhedonia/ asociality | Loss of interests and pleasures | Little interest in sex |
| Lack of closeness | ||
| Few friends | ||
| Poor capacity for rapport | ||
| aTtentional impairment | Inattentiveness | Poor concentration |
| Stereotyped thought |
1. Andreasen N, Olson SC. Negative versus positive schizophrenia: definition and validation. Arch Gen Psych 1982;39:789-94.
Dr. Wagner is assistant clinical professor, Indiana University School of Medicine, and staff psychiatrist, Richard L Roudebush VA Medical Center, Indianapolis.
Obvious positive symptoms of schizophrenia—such as hallucinations and delusions—typically prompt treatment, but positive symptoms may be absent or clouded by the rationalizations and minimization often seen in paranoia. Negative symptoms can also escape detection because of their subtlety.
Andreasen and Olson’s criteria for negative symptoms1 provide the basis for the Schedule for the Assessment of Negative Symptoms (SANS) that includes the five As: avolition/apathy, alogia, affective flattening, anhedonia/asociality, and attentional impairment.
Many remember Bleuler’s four As of schizophrenia—autism, loosening of associations, affective disturbances, and ambivalence—but may have a harder time remembering the SANS’ five As. I find the pseudo-acronym PLANT (for the vegetative changes manifested with negative symptoms) helpful for recalling all five As (Table).
Table
Use PLANT pseudo-acronym to recall vegetative symptoms
| Symptom | Meaning | Examples |
|---|---|---|
| aPathy/avolition | Lack of drive | Poor grooming |
| Anergia | ||
| Impersistence | ||
| aLogia | Marked impairment in thought processing and/or content | Poverty of speech |
| Poverty of content | ||
| Thought blocking | ||
| Latency of response | ||
| Poor abstracting | ||
| Affective disturbances | Altered expressiveness | Poor eye contact |
| Aprosodic speech | ||
| Lack of expression | ||
| Poverty of gestures | ||
| aNhedonia/ asociality | Loss of interests and pleasures | Little interest in sex |
| Lack of closeness | ||
| Few friends | ||
| Poor capacity for rapport | ||
| aTtentional impairment | Inattentiveness | Poor concentration |
| Stereotyped thought |
Obvious positive symptoms of schizophrenia—such as hallucinations and delusions—typically prompt treatment, but positive symptoms may be absent or clouded by the rationalizations and minimization often seen in paranoia. Negative symptoms can also escape detection because of their subtlety.
Andreasen and Olson’s criteria for negative symptoms1 provide the basis for the Schedule for the Assessment of Negative Symptoms (SANS) that includes the five As: avolition/apathy, alogia, affective flattening, anhedonia/asociality, and attentional impairment.
Many remember Bleuler’s four As of schizophrenia—autism, loosening of associations, affective disturbances, and ambivalence—but may have a harder time remembering the SANS’ five As. I find the pseudo-acronym PLANT (for the vegetative changes manifested with negative symptoms) helpful for recalling all five As (Table).
Table
Use PLANT pseudo-acronym to recall vegetative symptoms
| Symptom | Meaning | Examples |
|---|---|---|
| aPathy/avolition | Lack of drive | Poor grooming |
| Anergia | ||
| Impersistence | ||
| aLogia | Marked impairment in thought processing and/or content | Poverty of speech |
| Poverty of content | ||
| Thought blocking | ||
| Latency of response | ||
| Poor abstracting | ||
| Affective disturbances | Altered expressiveness | Poor eye contact |
| Aprosodic speech | ||
| Lack of expression | ||
| Poverty of gestures | ||
| aNhedonia/ asociality | Loss of interests and pleasures | Little interest in sex |
| Lack of closeness | ||
| Few friends | ||
| Poor capacity for rapport | ||
| aTtentional impairment | Inattentiveness | Poor concentration |
| Stereotyped thought |
1. Andreasen N, Olson SC. Negative versus positive schizophrenia: definition and validation. Arch Gen Psych 1982;39:789-94.
Dr. Wagner is assistant clinical professor, Indiana University School of Medicine, and staff psychiatrist, Richard L Roudebush VA Medical Center, Indianapolis.
1. Andreasen N, Olson SC. Negative versus positive schizophrenia: definition and validation. Arch Gen Psych 1982;39:789-94.
Dr. Wagner is assistant clinical professor, Indiana University School of Medicine, and staff psychiatrist, Richard L Roudebush VA Medical Center, Indianapolis.
Blogs: Personal and professional
Text:
Once reserved for personal diaries, the Web log or “blog” has become a powerful cybertool for self-expression, news, and debate. Physicians are increasingly using blogs to communicate and stay abreast, and advances in search engine technology make blogs easy to find and easier to start.
This article reviews numerous uses for blogs, plus information on starting your own.
The birth of the blog
Blogs started as public online diaries that provided a forum for self-expression and support. Blogs are similar to personal home pages and newsletters, except that authors update the content more frequently—daily in many cases—and readers can post comments for public viewing. Blogs combine elements of individual and group psychotherapy with a public journal.
Patients and families, for example, use schizophrenia.com to list their favorite blogs or create their own. Moodswing.org lists blogs for persons with bipolar disorder and their families.
Medical professionals also have discovered the therapeutic benefits of blog writing. Crazy Tracy features a psychiatric nurse’s musings about her work and personal life. Physicians post their experiences with patients and their thoughts about health care on blogs such as Intueri.org and Shrinkette.
Although blogs are public, many if not most authors keep identifying information out of their author profiles. Posting your e-mail address on a blog, for example, may open the door to viruses, spamming, or identity theft.
Also, recounting a specific case on a blog could breach patient confidentiality. Instead, post abstract case information to protect the patient’s anonymity.
Blog evolution
Blogs are also becoming well entrenched in business. Most corporate Web sites include blogs for employees to make announcements about products and services. Compared with discussion forums such as Invision Power Board, a blog helps create a sense of community without the constraints of defined topic headings seen in a bulletin board.
Google’s 2003 purchase of Pyra Labs—which developed Blogger, the easy-to-use blog creation site—helped push blogs into the mainstream. Even the CIA is using enterprise-based blog software to collect, organize, and publish information on its Intranet. (See “Psyber Psychiatry. Web logs: Blogging into the future,” January 2003.)
Medical blogs. A growing number of blogs, such as PsychNotes, AATP Interactive, and CodeBlueBlog, disseminate medical news. Authors cull information from clinical journals and Web sites to discuss their opinions and draw attention to new findings. Many medical blogs link to others, using pieces of code from blogLinker or Blogroller, so finding medical blogs is easy.
Some search engines and directories allow users to search exclusively for blogs. Technorati, a well-known blog search engine, searches based on links to sites and keyword tags. The blog sites’ authors choose the keywords, such as “schizophrenia” or “psychiatry.” Keyword tags can be linked to Web sites offering other services, such as photo sharing and listing favorite Web sites.
Social tagging
Even search engines cannot keep up with the growing number of sites proliferating on the Web. Enter social tagging, through which users can share common interests by storing links to Web sites. Blog users can use social tagging to consolidate links to other blogs.
Social tagging sites such as del.icio.us, Furl, and Shadows allow users to store URLs of sites they want to save and share. After creating an account, the user adds URLs with keyword tags into a database. Users can search the database for sites of interest. Using the keyword “psychiatry” on del.icio.us, for example, I found the Virtual Hospital Emergency Services Handbook and other mental health references. Each site found under the keyword also lists the number of users who have added that site to their “favorites” list.
Flickr and Buzznet offer a similar service to help users find photos related to keywords; these photos can be linked to blogs.
Rollyo and Wink are similar to social tagging sites, but with a twist. After establishing an account, users create a specialized search using a keyword tag but specify which Web sites to search. This type of keyword search could be more productive than conventional Web searches if the user knows which sites may produce useful results.
Although the Internet continues to grow almost exponentially, social tagging helps create a sense of community and a shared knowledge base. At SuprGlu, users gather content from other social tagging sites where they have an account. Ning expands upon this process, providing a free online service for building social blogs and connecting blog users based on common interests. These sites and services help make the Internet a much smaller and more useful place.
Starting your own blog
Not long ago, bloggers needed special software to post links to other blogs and comments from readers. Also, archiving previous posts required some skill, as this process was not automated.
Today, blog creation sites take the technical difficulty out of creating and hosting blogs, allowing authors to use the Web browser to edit and then publish the blog. These services, however, may have limited ‘skins’ or templates to customize your site’s look, and your URL will be based on the host name, such as boredhousewife.blogspot.com. You can circumvent this problem by registering your own URL and purchasing blog creation software such as Movable Type.
Send questions about blogs or this column to Dr. Luo or e-mail to [email protected].
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions he expresses in this column are his own and do not necessarily reflect those of Current Psychiatry.
Text:
Once reserved for personal diaries, the Web log or “blog” has become a powerful cybertool for self-expression, news, and debate. Physicians are increasingly using blogs to communicate and stay abreast, and advances in search engine technology make blogs easy to find and easier to start.
This article reviews numerous uses for blogs, plus information on starting your own.
The birth of the blog
Blogs started as public online diaries that provided a forum for self-expression and support. Blogs are similar to personal home pages and newsletters, except that authors update the content more frequently—daily in many cases—and readers can post comments for public viewing. Blogs combine elements of individual and group psychotherapy with a public journal.
Patients and families, for example, use schizophrenia.com to list their favorite blogs or create their own. Moodswing.org lists blogs for persons with bipolar disorder and their families.
Medical professionals also have discovered the therapeutic benefits of blog writing. Crazy Tracy features a psychiatric nurse’s musings about her work and personal life. Physicians post their experiences with patients and their thoughts about health care on blogs such as Intueri.org and Shrinkette.
Although blogs are public, many if not most authors keep identifying information out of their author profiles. Posting your e-mail address on a blog, for example, may open the door to viruses, spamming, or identity theft.
Also, recounting a specific case on a blog could breach patient confidentiality. Instead, post abstract case information to protect the patient’s anonymity.
Blog evolution
Blogs are also becoming well entrenched in business. Most corporate Web sites include blogs for employees to make announcements about products and services. Compared with discussion forums such as Invision Power Board, a blog helps create a sense of community without the constraints of defined topic headings seen in a bulletin board.
Google’s 2003 purchase of Pyra Labs—which developed Blogger, the easy-to-use blog creation site—helped push blogs into the mainstream. Even the CIA is using enterprise-based blog software to collect, organize, and publish information on its Intranet. (See “Psyber Psychiatry. Web logs: Blogging into the future,” January 2003.)
Medical blogs. A growing number of blogs, such as PsychNotes, AATP Interactive, and CodeBlueBlog, disseminate medical news. Authors cull information from clinical journals and Web sites to discuss their opinions and draw attention to new findings. Many medical blogs link to others, using pieces of code from blogLinker or Blogroller, so finding medical blogs is easy.
Some search engines and directories allow users to search exclusively for blogs. Technorati, a well-known blog search engine, searches based on links to sites and keyword tags. The blog sites’ authors choose the keywords, such as “schizophrenia” or “psychiatry.” Keyword tags can be linked to Web sites offering other services, such as photo sharing and listing favorite Web sites.
Social tagging
Even search engines cannot keep up with the growing number of sites proliferating on the Web. Enter social tagging, through which users can share common interests by storing links to Web sites. Blog users can use social tagging to consolidate links to other blogs.
Social tagging sites such as del.icio.us, Furl, and Shadows allow users to store URLs of sites they want to save and share. After creating an account, the user adds URLs with keyword tags into a database. Users can search the database for sites of interest. Using the keyword “psychiatry” on del.icio.us, for example, I found the Virtual Hospital Emergency Services Handbook and other mental health references. Each site found under the keyword also lists the number of users who have added that site to their “favorites” list.
Flickr and Buzznet offer a similar service to help users find photos related to keywords; these photos can be linked to blogs.
Rollyo and Wink are similar to social tagging sites, but with a twist. After establishing an account, users create a specialized search using a keyword tag but specify which Web sites to search. This type of keyword search could be more productive than conventional Web searches if the user knows which sites may produce useful results.
Although the Internet continues to grow almost exponentially, social tagging helps create a sense of community and a shared knowledge base. At SuprGlu, users gather content from other social tagging sites where they have an account. Ning expands upon this process, providing a free online service for building social blogs and connecting blog users based on common interests. These sites and services help make the Internet a much smaller and more useful place.
Starting your own blog
Not long ago, bloggers needed special software to post links to other blogs and comments from readers. Also, archiving previous posts required some skill, as this process was not automated.
Today, blog creation sites take the technical difficulty out of creating and hosting blogs, allowing authors to use the Web browser to edit and then publish the blog. These services, however, may have limited ‘skins’ or templates to customize your site’s look, and your URL will be based on the host name, such as boredhousewife.blogspot.com. You can circumvent this problem by registering your own URL and purchasing blog creation software such as Movable Type.
Send questions about blogs or this column to Dr. Luo or e-mail to [email protected].
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions he expresses in this column are his own and do not necessarily reflect those of Current Psychiatry.
Text:
Once reserved for personal diaries, the Web log or “blog” has become a powerful cybertool for self-expression, news, and debate. Physicians are increasingly using blogs to communicate and stay abreast, and advances in search engine technology make blogs easy to find and easier to start.
This article reviews numerous uses for blogs, plus information on starting your own.
The birth of the blog
Blogs started as public online diaries that provided a forum for self-expression and support. Blogs are similar to personal home pages and newsletters, except that authors update the content more frequently—daily in many cases—and readers can post comments for public viewing. Blogs combine elements of individual and group psychotherapy with a public journal.
Patients and families, for example, use schizophrenia.com to list their favorite blogs or create their own. Moodswing.org lists blogs for persons with bipolar disorder and their families.
Medical professionals also have discovered the therapeutic benefits of blog writing. Crazy Tracy features a psychiatric nurse’s musings about her work and personal life. Physicians post their experiences with patients and their thoughts about health care on blogs such as Intueri.org and Shrinkette.
Although blogs are public, many if not most authors keep identifying information out of their author profiles. Posting your e-mail address on a blog, for example, may open the door to viruses, spamming, or identity theft.
Also, recounting a specific case on a blog could breach patient confidentiality. Instead, post abstract case information to protect the patient’s anonymity.
Blog evolution
Blogs are also becoming well entrenched in business. Most corporate Web sites include blogs for employees to make announcements about products and services. Compared with discussion forums such as Invision Power Board, a blog helps create a sense of community without the constraints of defined topic headings seen in a bulletin board.
Google’s 2003 purchase of Pyra Labs—which developed Blogger, the easy-to-use blog creation site—helped push blogs into the mainstream. Even the CIA is using enterprise-based blog software to collect, organize, and publish information on its Intranet. (See “Psyber Psychiatry. Web logs: Blogging into the future,” January 2003.)
Medical blogs. A growing number of blogs, such as PsychNotes, AATP Interactive, and CodeBlueBlog, disseminate medical news. Authors cull information from clinical journals and Web sites to discuss their opinions and draw attention to new findings. Many medical blogs link to others, using pieces of code from blogLinker or Blogroller, so finding medical blogs is easy.
Some search engines and directories allow users to search exclusively for blogs. Technorati, a well-known blog search engine, searches based on links to sites and keyword tags. The blog sites’ authors choose the keywords, such as “schizophrenia” or “psychiatry.” Keyword tags can be linked to Web sites offering other services, such as photo sharing and listing favorite Web sites.
Social tagging
Even search engines cannot keep up with the growing number of sites proliferating on the Web. Enter social tagging, through which users can share common interests by storing links to Web sites. Blog users can use social tagging to consolidate links to other blogs.
Social tagging sites such as del.icio.us, Furl, and Shadows allow users to store URLs of sites they want to save and share. After creating an account, the user adds URLs with keyword tags into a database. Users can search the database for sites of interest. Using the keyword “psychiatry” on del.icio.us, for example, I found the Virtual Hospital Emergency Services Handbook and other mental health references. Each site found under the keyword also lists the number of users who have added that site to their “favorites” list.
Flickr and Buzznet offer a similar service to help users find photos related to keywords; these photos can be linked to blogs.
Rollyo and Wink are similar to social tagging sites, but with a twist. After establishing an account, users create a specialized search using a keyword tag but specify which Web sites to search. This type of keyword search could be more productive than conventional Web searches if the user knows which sites may produce useful results.
Although the Internet continues to grow almost exponentially, social tagging helps create a sense of community and a shared knowledge base. At SuprGlu, users gather content from other social tagging sites where they have an account. Ning expands upon this process, providing a free online service for building social blogs and connecting blog users based on common interests. These sites and services help make the Internet a much smaller and more useful place.
Starting your own blog
Not long ago, bloggers needed special software to post links to other blogs and comments from readers. Also, archiving previous posts required some skill, as this process was not automated.
Today, blog creation sites take the technical difficulty out of creating and hosting blogs, allowing authors to use the Web browser to edit and then publish the blog. These services, however, may have limited ‘skins’ or templates to customize your site’s look, and your URL will be based on the host name, such as boredhousewife.blogspot.com. You can circumvent this problem by registering your own URL and purchasing blog creation software such as Movable Type.
Send questions about blogs or this column to Dr. Luo or e-mail to [email protected].
Disclosure:
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions he expresses in this column are his own and do not necessarily reflect those of Current Psychiatry.
Remember the kids when parents are ill
When evaluating and treating adults, keep in mind that mental disorders may cause functional impairment that hinders parents’ ability to care for dependent children. Certain disorders—such as schizophrenia, bipolar disorder, and major depressive disorder—are often associated with substantial functional impairment.1 Failure to consider the impact of the functional impairment on a parent’s caretaking responsibilities can place dependent children at risk.
Don’t forget the kids. Ask adult patients with psychiatric conditions if they have dependent children in their care. If they do, determine if any functional impairment resulting from the mental disorder is impacting the patient’s ability to care for the children or places children at imminent risk of harm.
Keep in mind that parents who are experiencing delusions or suicidal ideation may harbor thoughts of filicide.2 Maintain a high degree of suspicion when evaluating and managing such patients, and inquire directly about filicidal thoughts.
Use techniques similar to those for assessing suicidal thoughts. Begin with a normalizing statement such as, “Sometimes, when people have symptoms like those you are describing, they have thoughts of harming their children.” Then follow up with a direct question using unambiguous language: “Have you had any thoughts of hurting or killing your children?” When patients endorse such thoughts, explore whether they have formulated a plan and assess whether they intend to follow through with it.3
When a patient with dependent children requires hospital admission or admits to caretaking inability, ensure that proper arrangements are made for his or her children’s care. Contact the spouse, grandparent, guardian, or social services agency.
Remember that not all dependents are children. An increasing number of elderly persons are being cared for by their adult children. Caretaking can be a major psychosocial stressor that triggers the onset or exacerbation of a psychiatric disorder—such as a major depressive episode—that leads to functional impairment.4
1. Hales RE, Yudofsky SC, eds. Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing; 2003.
2. Jennings KD, Ross S, Popper S, Elmore M. Thoughts of harming infants in depressed and nondepressed mothers. J Affect Disord 1999;54:21-8.
3. Shea SC. Psychiatric interviewing: the art of understanding (2nd ed). Philadelphia: WB Saunders; 1998.
4. Sadock BJ, Sadock VA, eds. Kaplan & Sadock’s comprehensive textbook of psychiatry (8th ed). New York: Lippincott Williams & Wilkins; 2004.
Dr. Campbell is assistant professor, department of psychiatry, Case Western Reserve University School of Medicine, Cleveland, OH, and is residency program director and director of clinical services, department of psychiatry, University Hospitals of Cleveland.
When evaluating and treating adults, keep in mind that mental disorders may cause functional impairment that hinders parents’ ability to care for dependent children. Certain disorders—such as schizophrenia, bipolar disorder, and major depressive disorder—are often associated with substantial functional impairment.1 Failure to consider the impact of the functional impairment on a parent’s caretaking responsibilities can place dependent children at risk.
Don’t forget the kids. Ask adult patients with psychiatric conditions if they have dependent children in their care. If they do, determine if any functional impairment resulting from the mental disorder is impacting the patient’s ability to care for the children or places children at imminent risk of harm.
Keep in mind that parents who are experiencing delusions or suicidal ideation may harbor thoughts of filicide.2 Maintain a high degree of suspicion when evaluating and managing such patients, and inquire directly about filicidal thoughts.
Use techniques similar to those for assessing suicidal thoughts. Begin with a normalizing statement such as, “Sometimes, when people have symptoms like those you are describing, they have thoughts of harming their children.” Then follow up with a direct question using unambiguous language: “Have you had any thoughts of hurting or killing your children?” When patients endorse such thoughts, explore whether they have formulated a plan and assess whether they intend to follow through with it.3
When a patient with dependent children requires hospital admission or admits to caretaking inability, ensure that proper arrangements are made for his or her children’s care. Contact the spouse, grandparent, guardian, or social services agency.
Remember that not all dependents are children. An increasing number of elderly persons are being cared for by their adult children. Caretaking can be a major psychosocial stressor that triggers the onset or exacerbation of a psychiatric disorder—such as a major depressive episode—that leads to functional impairment.4
When evaluating and treating adults, keep in mind that mental disorders may cause functional impairment that hinders parents’ ability to care for dependent children. Certain disorders—such as schizophrenia, bipolar disorder, and major depressive disorder—are often associated with substantial functional impairment.1 Failure to consider the impact of the functional impairment on a parent’s caretaking responsibilities can place dependent children at risk.
Don’t forget the kids. Ask adult patients with psychiatric conditions if they have dependent children in their care. If they do, determine if any functional impairment resulting from the mental disorder is impacting the patient’s ability to care for the children or places children at imminent risk of harm.
Keep in mind that parents who are experiencing delusions or suicidal ideation may harbor thoughts of filicide.2 Maintain a high degree of suspicion when evaluating and managing such patients, and inquire directly about filicidal thoughts.
Use techniques similar to those for assessing suicidal thoughts. Begin with a normalizing statement such as, “Sometimes, when people have symptoms like those you are describing, they have thoughts of harming their children.” Then follow up with a direct question using unambiguous language: “Have you had any thoughts of hurting or killing your children?” When patients endorse such thoughts, explore whether they have formulated a plan and assess whether they intend to follow through with it.3
When a patient with dependent children requires hospital admission or admits to caretaking inability, ensure that proper arrangements are made for his or her children’s care. Contact the spouse, grandparent, guardian, or social services agency.
Remember that not all dependents are children. An increasing number of elderly persons are being cared for by their adult children. Caretaking can be a major psychosocial stressor that triggers the onset or exacerbation of a psychiatric disorder—such as a major depressive episode—that leads to functional impairment.4
1. Hales RE, Yudofsky SC, eds. Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing; 2003.
2. Jennings KD, Ross S, Popper S, Elmore M. Thoughts of harming infants in depressed and nondepressed mothers. J Affect Disord 1999;54:21-8.
3. Shea SC. Psychiatric interviewing: the art of understanding (2nd ed). Philadelphia: WB Saunders; 1998.
4. Sadock BJ, Sadock VA, eds. Kaplan & Sadock’s comprehensive textbook of psychiatry (8th ed). New York: Lippincott Williams & Wilkins; 2004.
Dr. Campbell is assistant professor, department of psychiatry, Case Western Reserve University School of Medicine, Cleveland, OH, and is residency program director and director of clinical services, department of psychiatry, University Hospitals of Cleveland.
1. Hales RE, Yudofsky SC, eds. Textbook of clinical psychiatry (4th ed). Washington, DC: American Psychiatric Publishing; 2003.
2. Jennings KD, Ross S, Popper S, Elmore M. Thoughts of harming infants in depressed and nondepressed mothers. J Affect Disord 1999;54:21-8.
3. Shea SC. Psychiatric interviewing: the art of understanding (2nd ed). Philadelphia: WB Saunders; 1998.
4. Sadock BJ, Sadock VA, eds. Kaplan & Sadock’s comprehensive textbook of psychiatry (8th ed). New York: Lippincott Williams & Wilkins; 2004.
Dr. Campbell is assistant professor, department of psychiatry, Case Western Reserve University School of Medicine, Cleveland, OH, and is residency program director and director of clinical services, department of psychiatry, University Hospitals of Cleveland.
Be prepared, not panicked, when served with a subpoena
On Friday morning, Dr. G receives a subpoena requesting one of her patient’s records be available for court the following Monday. This is Dr. G’s first subpoena. The timetable is short, and she is uncertain about what to do and whom to ask for advice.
If you experience circumstances similar to Dr. G’s, these suggestions can acquaint you with the legal system, its processes, and jargon.
Subpoena or summons? A summons may mean a lawsuit was filed against you. A subpoena means you’re called to appear as a witness and/or provide the court with records or information.1 Inform your personal attorney or your facility’s legal team about the subpoena and provide a copy.
Identify the sender. Find out if a judge, attorney, or prosecutor issued the legal notice. Ask the issuer for information such as the case details and type of information expected from you. Confirm that you treated this particular patient or saw him or her in consultation.
Don’t ignore it. Subpoenas and summonses are court orders. You can be served twice, and if you disregard these notices you can be held in contempt of court. You could be fined or imprisoned, but judges usually are more interested in having witnesses comply than in inflicting punishment.
If the date, time, or location of the court appearance is not convenient, work with the court to reschedule and obtain these arrangements in writing. If you experience difficulty, contact the judge’s clerk directly.
Privacy concerns. Your attorney and the American Psychiatric Association’s legal consultation plan (available at www.psych.org/ecp/membership.cfm) can help you act in accordance with Health Insurance Portability and Accountability Act (HIPAA) regulations and applicable state laws. Your malpractice insurer can also offer guidance.
Request your patient’s consent to release your records to the court. If the patient refuses to consent, clearly explain to the court your inability to release confidential records. If your records or testimony are crucial for the case, the judge may still order you to comply.
Some subpoenas have exclusion criteria that exempt psychiatric and/or psychotherapeutic notes. If you believe your records qualify as exempt, you must submit a letter to the court explaining the reasons.
Requirements to comply. A subpoena may require testimony only, records only, or both. If you are required to testify, clarify whether you are to appear at trial, deposition, or both. In court, discuss only facts pertaining to the case, not your opinion.
1. Reiley DG, Guldner GT, Leinen AL. “You are commanded to appear:” The subpoena and the emergency medicine resident. Ann Emerg Med 2003;42(6):843-6.
Mariam Bekhit, MD, is child psychiatry fellow, New Jersey Medical School, University of Medicine and Dentistry of New Jersey, Newark.
Anwar Ghali, MD, is chairman, psychiatric department, Trinitas Hospital, Elizabeth, NJ.
On Friday morning, Dr. G receives a subpoena requesting one of her patient’s records be available for court the following Monday. This is Dr. G’s first subpoena. The timetable is short, and she is uncertain about what to do and whom to ask for advice.
If you experience circumstances similar to Dr. G’s, these suggestions can acquaint you with the legal system, its processes, and jargon.
Subpoena or summons? A summons may mean a lawsuit was filed against you. A subpoena means you’re called to appear as a witness and/or provide the court with records or information.1 Inform your personal attorney or your facility’s legal team about the subpoena and provide a copy.
Identify the sender. Find out if a judge, attorney, or prosecutor issued the legal notice. Ask the issuer for information such as the case details and type of information expected from you. Confirm that you treated this particular patient or saw him or her in consultation.
Don’t ignore it. Subpoenas and summonses are court orders. You can be served twice, and if you disregard these notices you can be held in contempt of court. You could be fined or imprisoned, but judges usually are more interested in having witnesses comply than in inflicting punishment.
If the date, time, or location of the court appearance is not convenient, work with the court to reschedule and obtain these arrangements in writing. If you experience difficulty, contact the judge’s clerk directly.
Privacy concerns. Your attorney and the American Psychiatric Association’s legal consultation plan (available at www.psych.org/ecp/membership.cfm) can help you act in accordance with Health Insurance Portability and Accountability Act (HIPAA) regulations and applicable state laws. Your malpractice insurer can also offer guidance.
Request your patient’s consent to release your records to the court. If the patient refuses to consent, clearly explain to the court your inability to release confidential records. If your records or testimony are crucial for the case, the judge may still order you to comply.
Some subpoenas have exclusion criteria that exempt psychiatric and/or psychotherapeutic notes. If you believe your records qualify as exempt, you must submit a letter to the court explaining the reasons.
Requirements to comply. A subpoena may require testimony only, records only, or both. If you are required to testify, clarify whether you are to appear at trial, deposition, or both. In court, discuss only facts pertaining to the case, not your opinion.
On Friday morning, Dr. G receives a subpoena requesting one of her patient’s records be available for court the following Monday. This is Dr. G’s first subpoena. The timetable is short, and she is uncertain about what to do and whom to ask for advice.
If you experience circumstances similar to Dr. G’s, these suggestions can acquaint you with the legal system, its processes, and jargon.
Subpoena or summons? A summons may mean a lawsuit was filed against you. A subpoena means you’re called to appear as a witness and/or provide the court with records or information.1 Inform your personal attorney or your facility’s legal team about the subpoena and provide a copy.
Identify the sender. Find out if a judge, attorney, or prosecutor issued the legal notice. Ask the issuer for information such as the case details and type of information expected from you. Confirm that you treated this particular patient or saw him or her in consultation.
Don’t ignore it. Subpoenas and summonses are court orders. You can be served twice, and if you disregard these notices you can be held in contempt of court. You could be fined or imprisoned, but judges usually are more interested in having witnesses comply than in inflicting punishment.
If the date, time, or location of the court appearance is not convenient, work with the court to reschedule and obtain these arrangements in writing. If you experience difficulty, contact the judge’s clerk directly.
Privacy concerns. Your attorney and the American Psychiatric Association’s legal consultation plan (available at www.psych.org/ecp/membership.cfm) can help you act in accordance with Health Insurance Portability and Accountability Act (HIPAA) regulations and applicable state laws. Your malpractice insurer can also offer guidance.
Request your patient’s consent to release your records to the court. If the patient refuses to consent, clearly explain to the court your inability to release confidential records. If your records or testimony are crucial for the case, the judge may still order you to comply.
Some subpoenas have exclusion criteria that exempt psychiatric and/or psychotherapeutic notes. If you believe your records qualify as exempt, you must submit a letter to the court explaining the reasons.
Requirements to comply. A subpoena may require testimony only, records only, or both. If you are required to testify, clarify whether you are to appear at trial, deposition, or both. In court, discuss only facts pertaining to the case, not your opinion.
1. Reiley DG, Guldner GT, Leinen AL. “You are commanded to appear:” The subpoena and the emergency medicine resident. Ann Emerg Med 2003;42(6):843-6.
Mariam Bekhit, MD, is child psychiatry fellow, New Jersey Medical School, University of Medicine and Dentistry of New Jersey, Newark.
Anwar Ghali, MD, is chairman, psychiatric department, Trinitas Hospital, Elizabeth, NJ.
1. Reiley DG, Guldner GT, Leinen AL. “You are commanded to appear:” The subpoena and the emergency medicine resident. Ann Emerg Med 2003;42(6):843-6.
Mariam Bekhit, MD, is child psychiatry fellow, New Jersey Medical School, University of Medicine and Dentistry of New Jersey, Newark.
Anwar Ghali, MD, is chairman, psychiatric department, Trinitas Hospital, Elizabeth, NJ.
PRN medications: Are you using them safely?
Prescribing PRN medications to manage agitation and psychotic behavior may expose psychiatric inpatients to unnecessary psychotropics or overmedication.1 Moreover, nurses’ documentation of “as needed” administration is often inadequate2 because of the volume of required documentation, nursing shortages in inpatient settings, and nurses’ differing opinions on how to pharmacologically manage difficult behaviors and persistent pain.3
In the absence of evidence-based guidelines,4 the following recommendations can help you ensure that PRNs are used safely and documented thoroughly.
Document the rationale for ordering a PRN in your progress notes. Note the behaviors you wish to target, and specify when nurses should administer the drug.
Review nursing progress notes to determine whether the drug rectified the targeted behavior(s). For partial response, consider increasing the dosage. For nonresponse after 2 doses of one agent, try switching to another.
Review medication administration sheets to determine how often a drug is being used. Frequent PRN use suggests a need to re-evaluate the patient and drug regimen. You may need to increase or add to the patient’s standing medications. Consider combining similar medications into a standing order for more-reliable administration.
Request staff education. One study suggests that PRN orders can benefit staff more than patients.1 Advocating for the education of direct-care staff may be psychiatrists’ most effective method of combating PRN medication overuse.
Improper charting or misestimation of PRN use could result in liability. For example, medication that is not immediately documented may be re-administered by another nurse, resulting in overdose. A physician’s clinical judgment is impaired if he or she relies on inaccurate documentation or verbal report when evaluating a patient’s PRN use and standing order.
Education, auditing of records, and corrective action can help maintain charting accuracy and reduce the risk of litigation.3
1. Thapa P, Palmer SL, Owen RR, et al. PRN (as-needed) orders and exposure of psychiatric inpatients to unnecessary psychotropic medications. Psychiatr Serv 2003;54(9):1282-6.
2. Curtis J, Capp K. Administration of “as needed” psychotropic medication: a retrospective study. Int J Ment Health Nurs 2003;12(3):229-34.
3. LaFerney M. To give or not to give: challenging the use of PRN medication for pain and behaviors in long-term care. Advance Nurses 205;7(9):35.
4. Usher K, Holmes C, Lindsay D, Luck L. PRN psychotropic medications: The need for nursing research. Contemp Nurse 2003;14(3):248-57.
Michael C. LaFerney is an advanced practice nurse at Arbour SeniorCare, Rockland, MA.
Prescribing PRN medications to manage agitation and psychotic behavior may expose psychiatric inpatients to unnecessary psychotropics or overmedication.1 Moreover, nurses’ documentation of “as needed” administration is often inadequate2 because of the volume of required documentation, nursing shortages in inpatient settings, and nurses’ differing opinions on how to pharmacologically manage difficult behaviors and persistent pain.3
In the absence of evidence-based guidelines,4 the following recommendations can help you ensure that PRNs are used safely and documented thoroughly.
Document the rationale for ordering a PRN in your progress notes. Note the behaviors you wish to target, and specify when nurses should administer the drug.
Review nursing progress notes to determine whether the drug rectified the targeted behavior(s). For partial response, consider increasing the dosage. For nonresponse after 2 doses of one agent, try switching to another.
Review medication administration sheets to determine how often a drug is being used. Frequent PRN use suggests a need to re-evaluate the patient and drug regimen. You may need to increase or add to the patient’s standing medications. Consider combining similar medications into a standing order for more-reliable administration.
Request staff education. One study suggests that PRN orders can benefit staff more than patients.1 Advocating for the education of direct-care staff may be psychiatrists’ most effective method of combating PRN medication overuse.
Improper charting or misestimation of PRN use could result in liability. For example, medication that is not immediately documented may be re-administered by another nurse, resulting in overdose. A physician’s clinical judgment is impaired if he or she relies on inaccurate documentation or verbal report when evaluating a patient’s PRN use and standing order.
Education, auditing of records, and corrective action can help maintain charting accuracy and reduce the risk of litigation.3
Prescribing PRN medications to manage agitation and psychotic behavior may expose psychiatric inpatients to unnecessary psychotropics or overmedication.1 Moreover, nurses’ documentation of “as needed” administration is often inadequate2 because of the volume of required documentation, nursing shortages in inpatient settings, and nurses’ differing opinions on how to pharmacologically manage difficult behaviors and persistent pain.3
In the absence of evidence-based guidelines,4 the following recommendations can help you ensure that PRNs are used safely and documented thoroughly.
Document the rationale for ordering a PRN in your progress notes. Note the behaviors you wish to target, and specify when nurses should administer the drug.
Review nursing progress notes to determine whether the drug rectified the targeted behavior(s). For partial response, consider increasing the dosage. For nonresponse after 2 doses of one agent, try switching to another.
Review medication administration sheets to determine how often a drug is being used. Frequent PRN use suggests a need to re-evaluate the patient and drug regimen. You may need to increase or add to the patient’s standing medications. Consider combining similar medications into a standing order for more-reliable administration.
Request staff education. One study suggests that PRN orders can benefit staff more than patients.1 Advocating for the education of direct-care staff may be psychiatrists’ most effective method of combating PRN medication overuse.
Improper charting or misestimation of PRN use could result in liability. For example, medication that is not immediately documented may be re-administered by another nurse, resulting in overdose. A physician’s clinical judgment is impaired if he or she relies on inaccurate documentation or verbal report when evaluating a patient’s PRN use and standing order.
Education, auditing of records, and corrective action can help maintain charting accuracy and reduce the risk of litigation.3
1. Thapa P, Palmer SL, Owen RR, et al. PRN (as-needed) orders and exposure of psychiatric inpatients to unnecessary psychotropic medications. Psychiatr Serv 2003;54(9):1282-6.
2. Curtis J, Capp K. Administration of “as needed” psychotropic medication: a retrospective study. Int J Ment Health Nurs 2003;12(3):229-34.
3. LaFerney M. To give or not to give: challenging the use of PRN medication for pain and behaviors in long-term care. Advance Nurses 205;7(9):35.
4. Usher K, Holmes C, Lindsay D, Luck L. PRN psychotropic medications: The need for nursing research. Contemp Nurse 2003;14(3):248-57.
Michael C. LaFerney is an advanced practice nurse at Arbour SeniorCare, Rockland, MA.
1. Thapa P, Palmer SL, Owen RR, et al. PRN (as-needed) orders and exposure of psychiatric inpatients to unnecessary psychotropic medications. Psychiatr Serv 2003;54(9):1282-6.
2. Curtis J, Capp K. Administration of “as needed” psychotropic medication: a retrospective study. Int J Ment Health Nurs 2003;12(3):229-34.
3. LaFerney M. To give or not to give: challenging the use of PRN medication for pain and behaviors in long-term care. Advance Nurses 205;7(9):35.
4. Usher K, Holmes C, Lindsay D, Luck L. PRN psychotropic medications: The need for nursing research. Contemp Nurse 2003;14(3):248-57.
Michael C. LaFerney is an advanced practice nurse at Arbour SeniorCare, Rockland, MA.
VoIP: The right call for your practice?
Voice-over Internet protocol (VoIP), once a cutting-edge telecommunications innovation, has quickly reached the information age mainstream (See Fast facts). Homes and businesses are increasingly using broadband Internet connections to make inexpensive long-distance telephone calls.
Can VoIP help you communicate efficiently and cost-effectively with patients, staff, and colleagues? Read on.
How VoIP works
VoIP lets you make telephone calls using your Internet connection or other computer network. Calls from one PC to another are free, while calls from a PC to a landline or mobile phone are not.
In the most basic VoIP, a user at a computer with a microphone headset calls a similarly equipped user by entering an e-mail address or user name on a network, such as Skype’s “SkypeOut” program. Software transmits the audio signal over the Internet. The technology is similar to that of a mobile phone, which requires cellular towers to send packets of your audio signal.
eBay recently purchased Skype for $1.3 billion in cash and $1.3 billion in eBay stock. VoIP use will likely become more widespread after the eBay takeover, industry observers predict. For more information, see http://news.bbc.co.uk/1/hi/technology/4238258.stm.
For as little as 17 cents per minute, you can call from your computer to a regular telephone number anywhere in the world. Skype, SunRocket, and Vonage are among the more popular and inexpensive VoIP providers (Table). In addition to “SkypeOut,” Google, Yahoo, and MSN also offer free PC-to-PC calling with voice conferencing.
Another Skype service, “SkypeIn,” offers portable local numbers that allow callers—using a computer or a regular phone—to reach you wherever you go. You can be traveling in Paris and receive a phone call at a local Internet café with your notebook computer, yet the caller pays only the regular rate to call your number.
Only Skype offers software that allows telecommunication via Pocket PC. Blackberry is not supported for VoIP communication and SunRocket and Vonage do not offer PDA support.
Table
VoIP Providers
| Provider | Service within USA and Canada | Service to India–New Delhi |
|---|---|---|
| Skype | $0.021/minute | $0.154/minute |
| SunRocket | $24.95/month unlimited | $0.12/minute |
| Vonage | $24.95/month unlimited | $0.17/minute |
VoIP advantages
The ability to make free or low-cost calls to any location worldwide is an obvious advantage. For clinical use, VoIP can help psychiatrists reach patients who travel frequently and have Internet access.
For the psychiatrist who shuttles between offices, a portable number offers flexibility. Psychiatrists attending national meetings or CME courses can use VoIP to contact colleagues or communicate with patients or staff back home.
Online phone communication is also secure, because VoIP data packets are encrypted as they are sent over the Internet.
VoIP users may be able to eliminate their local telephone service and pay only for broadband Internet access. For emergencies when the Internet is not working, a mobile phone may be sufficient backup.
If you prefer a traditional phone to a microphone headset, you can use a phone equipped with a universal serial bus (USB) connector to make online calls. Skype offers phones with built-in USB connectors, while Vonage and SunRocket offer adapters that connect to regular phones and specialized phone adapters that connect to a phone, computer, or fax machine.
Skype, SunRocket, and Vonage offer call waiting and voice mail functions. Many VoIP software clients also offer text messaging and conference calling, allowing you to use your computer to type notes or send files while making a VoIP call. Some VoIP providers, such as Yahoo! Messenger, offer a video signal as well.
Skype offers a Pocket PC software client that lets you make telephone calls while connected to the Internet with a Pocket PC personal digital assistant (PDA). Having a Pocket PC with unlimited monthly wireless Internet data service and using SkypeOut to make mobile telephone calls for 2.4 cents per minute within the continental United States can help control combined PDA/phone charges. Skype will release a Palm OS version of this software sometime this month.1
Drawbacks
When your Internet access is down, you cannot make or receive VoIP calls. Also, as with mobile phones, the connection at times may be dropped or sound somewhat muffled. Overall, VoIP sound quality is on par with mobile phones, but not as good as conventional landline phones.
If traffic over your Internet connection is heavy—with downloads and other applications competing for bandwidth—connection quality can suffer. One solution is to use a router that gives priority to the VoIP application and its data. A router, similar to a “traffic cop” on a shared Internet connection, knows which data to send to and from the different computers/devices and the Internet connection.2 The D-Link Broadband Phone Service VoIP Router, for example, enables VoIP calls and Internet sharing.
VoIP inboxes theoretically are vulnerable to spam attacks because of e-mail addresses associated with accounts. Qovia is seeking a patent for technology designed to guard against VoIP spam, but VoIP spam attacks have not yet been reported because VoIP has only recently become popular.2
As mentioned, VoIP could eliminate the need for a regular telephone line, but if you use a digital subscriber line (DSL) for Internet access, you will need to keep at least a local telephone service.
Telecommunication: the future
The development of faster Internet access with Internet2 could lead to consolidation in the communications industry, allowing voice, data, video and other media to be managed via one connection. Internet2 is a consortium of universities working with industry and government to develop and deploy advanced network applications and technologies for the creation of tomorrow’s Internet.
Related resources
- 1. Federal Communications Commission. Voice-over Internet protocol: frequently asked questions. http://www.fcc.gov/voip/
- 2. Internet2. http://www.internet2.edu/
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed Oct. 3, 2005)
1. Rojas P. Skype coming to Palm next month? Engadget Sept. 14, 2005. Available at: http://www.engadget.com/entry/1016803924623324/.
2. Qovia files patents for voice spam blocking technology. Available at: http://www.qovia.com/company/news/06.28.2004_voip_spam_patent_app_final.htm.
Voice-over Internet protocol (VoIP), once a cutting-edge telecommunications innovation, has quickly reached the information age mainstream (See Fast facts). Homes and businesses are increasingly using broadband Internet connections to make inexpensive long-distance telephone calls.
Can VoIP help you communicate efficiently and cost-effectively with patients, staff, and colleagues? Read on.
How VoIP works
VoIP lets you make telephone calls using your Internet connection or other computer network. Calls from one PC to another are free, while calls from a PC to a landline or mobile phone are not.
In the most basic VoIP, a user at a computer with a microphone headset calls a similarly equipped user by entering an e-mail address or user name on a network, such as Skype’s “SkypeOut” program. Software transmits the audio signal over the Internet. The technology is similar to that of a mobile phone, which requires cellular towers to send packets of your audio signal.
eBay recently purchased Skype for $1.3 billion in cash and $1.3 billion in eBay stock. VoIP use will likely become more widespread after the eBay takeover, industry observers predict. For more information, see http://news.bbc.co.uk/1/hi/technology/4238258.stm.
For as little as 17 cents per minute, you can call from your computer to a regular telephone number anywhere in the world. Skype, SunRocket, and Vonage are among the more popular and inexpensive VoIP providers (Table). In addition to “SkypeOut,” Google, Yahoo, and MSN also offer free PC-to-PC calling with voice conferencing.
Another Skype service, “SkypeIn,” offers portable local numbers that allow callers—using a computer or a regular phone—to reach you wherever you go. You can be traveling in Paris and receive a phone call at a local Internet café with your notebook computer, yet the caller pays only the regular rate to call your number.
Only Skype offers software that allows telecommunication via Pocket PC. Blackberry is not supported for VoIP communication and SunRocket and Vonage do not offer PDA support.
Table
VoIP Providers
| Provider | Service within USA and Canada | Service to India–New Delhi |
|---|---|---|
| Skype | $0.021/minute | $0.154/minute |
| SunRocket | $24.95/month unlimited | $0.12/minute |
| Vonage | $24.95/month unlimited | $0.17/minute |
VoIP advantages
The ability to make free or low-cost calls to any location worldwide is an obvious advantage. For clinical use, VoIP can help psychiatrists reach patients who travel frequently and have Internet access.
For the psychiatrist who shuttles between offices, a portable number offers flexibility. Psychiatrists attending national meetings or CME courses can use VoIP to contact colleagues or communicate with patients or staff back home.
Online phone communication is also secure, because VoIP data packets are encrypted as they are sent over the Internet.
VoIP users may be able to eliminate their local telephone service and pay only for broadband Internet access. For emergencies when the Internet is not working, a mobile phone may be sufficient backup.
If you prefer a traditional phone to a microphone headset, you can use a phone equipped with a universal serial bus (USB) connector to make online calls. Skype offers phones with built-in USB connectors, while Vonage and SunRocket offer adapters that connect to regular phones and specialized phone adapters that connect to a phone, computer, or fax machine.
Skype, SunRocket, and Vonage offer call waiting and voice mail functions. Many VoIP software clients also offer text messaging and conference calling, allowing you to use your computer to type notes or send files while making a VoIP call. Some VoIP providers, such as Yahoo! Messenger, offer a video signal as well.
Skype offers a Pocket PC software client that lets you make telephone calls while connected to the Internet with a Pocket PC personal digital assistant (PDA). Having a Pocket PC with unlimited monthly wireless Internet data service and using SkypeOut to make mobile telephone calls for 2.4 cents per minute within the continental United States can help control combined PDA/phone charges. Skype will release a Palm OS version of this software sometime this month.1
Drawbacks
When your Internet access is down, you cannot make or receive VoIP calls. Also, as with mobile phones, the connection at times may be dropped or sound somewhat muffled. Overall, VoIP sound quality is on par with mobile phones, but not as good as conventional landline phones.
If traffic over your Internet connection is heavy—with downloads and other applications competing for bandwidth—connection quality can suffer. One solution is to use a router that gives priority to the VoIP application and its data. A router, similar to a “traffic cop” on a shared Internet connection, knows which data to send to and from the different computers/devices and the Internet connection.2 The D-Link Broadband Phone Service VoIP Router, for example, enables VoIP calls and Internet sharing.
VoIP inboxes theoretically are vulnerable to spam attacks because of e-mail addresses associated with accounts. Qovia is seeking a patent for technology designed to guard against VoIP spam, but VoIP spam attacks have not yet been reported because VoIP has only recently become popular.2
As mentioned, VoIP could eliminate the need for a regular telephone line, but if you use a digital subscriber line (DSL) for Internet access, you will need to keep at least a local telephone service.
Telecommunication: the future
The development of faster Internet access with Internet2 could lead to consolidation in the communications industry, allowing voice, data, video and other media to be managed via one connection. Internet2 is a consortium of universities working with industry and government to develop and deploy advanced network applications and technologies for the creation of tomorrow’s Internet.
Related resources
- 1. Federal Communications Commission. Voice-over Internet protocol: frequently asked questions. http://www.fcc.gov/voip/
- 2. Internet2. http://www.internet2.edu/
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
Voice-over Internet protocol (VoIP), once a cutting-edge telecommunications innovation, has quickly reached the information age mainstream (See Fast facts). Homes and businesses are increasingly using broadband Internet connections to make inexpensive long-distance telephone calls.
Can VoIP help you communicate efficiently and cost-effectively with patients, staff, and colleagues? Read on.
How VoIP works
VoIP lets you make telephone calls using your Internet connection or other computer network. Calls from one PC to another are free, while calls from a PC to a landline or mobile phone are not.
In the most basic VoIP, a user at a computer with a microphone headset calls a similarly equipped user by entering an e-mail address or user name on a network, such as Skype’s “SkypeOut” program. Software transmits the audio signal over the Internet. The technology is similar to that of a mobile phone, which requires cellular towers to send packets of your audio signal.
eBay recently purchased Skype for $1.3 billion in cash and $1.3 billion in eBay stock. VoIP use will likely become more widespread after the eBay takeover, industry observers predict. For more information, see http://news.bbc.co.uk/1/hi/technology/4238258.stm.
For as little as 17 cents per minute, you can call from your computer to a regular telephone number anywhere in the world. Skype, SunRocket, and Vonage are among the more popular and inexpensive VoIP providers (Table). In addition to “SkypeOut,” Google, Yahoo, and MSN also offer free PC-to-PC calling with voice conferencing.
Another Skype service, “SkypeIn,” offers portable local numbers that allow callers—using a computer or a regular phone—to reach you wherever you go. You can be traveling in Paris and receive a phone call at a local Internet café with your notebook computer, yet the caller pays only the regular rate to call your number.
Only Skype offers software that allows telecommunication via Pocket PC. Blackberry is not supported for VoIP communication and SunRocket and Vonage do not offer PDA support.
Table
VoIP Providers
| Provider | Service within USA and Canada | Service to India–New Delhi |
|---|---|---|
| Skype | $0.021/minute | $0.154/minute |
| SunRocket | $24.95/month unlimited | $0.12/minute |
| Vonage | $24.95/month unlimited | $0.17/minute |
VoIP advantages
The ability to make free or low-cost calls to any location worldwide is an obvious advantage. For clinical use, VoIP can help psychiatrists reach patients who travel frequently and have Internet access.
For the psychiatrist who shuttles between offices, a portable number offers flexibility. Psychiatrists attending national meetings or CME courses can use VoIP to contact colleagues or communicate with patients or staff back home.
Online phone communication is also secure, because VoIP data packets are encrypted as they are sent over the Internet.
VoIP users may be able to eliminate their local telephone service and pay only for broadband Internet access. For emergencies when the Internet is not working, a mobile phone may be sufficient backup.
If you prefer a traditional phone to a microphone headset, you can use a phone equipped with a universal serial bus (USB) connector to make online calls. Skype offers phones with built-in USB connectors, while Vonage and SunRocket offer adapters that connect to regular phones and specialized phone adapters that connect to a phone, computer, or fax machine.
Skype, SunRocket, and Vonage offer call waiting and voice mail functions. Many VoIP software clients also offer text messaging and conference calling, allowing you to use your computer to type notes or send files while making a VoIP call. Some VoIP providers, such as Yahoo! Messenger, offer a video signal as well.
Skype offers a Pocket PC software client that lets you make telephone calls while connected to the Internet with a Pocket PC personal digital assistant (PDA). Having a Pocket PC with unlimited monthly wireless Internet data service and using SkypeOut to make mobile telephone calls for 2.4 cents per minute within the continental United States can help control combined PDA/phone charges. Skype will release a Palm OS version of this software sometime this month.1
Drawbacks
When your Internet access is down, you cannot make or receive VoIP calls. Also, as with mobile phones, the connection at times may be dropped or sound somewhat muffled. Overall, VoIP sound quality is on par with mobile phones, but not as good as conventional landline phones.
If traffic over your Internet connection is heavy—with downloads and other applications competing for bandwidth—connection quality can suffer. One solution is to use a router that gives priority to the VoIP application and its data. A router, similar to a “traffic cop” on a shared Internet connection, knows which data to send to and from the different computers/devices and the Internet connection.2 The D-Link Broadband Phone Service VoIP Router, for example, enables VoIP calls and Internet sharing.
VoIP inboxes theoretically are vulnerable to spam attacks because of e-mail addresses associated with accounts. Qovia is seeking a patent for technology designed to guard against VoIP spam, but VoIP spam attacks have not yet been reported because VoIP has only recently become popular.2
As mentioned, VoIP could eliminate the need for a regular telephone line, but if you use a digital subscriber line (DSL) for Internet access, you will need to keep at least a local telephone service.
Telecommunication: the future
The development of faster Internet access with Internet2 could lead to consolidation in the communications industry, allowing voice, data, video and other media to be managed via one connection. Internet2 is a consortium of universities working with industry and government to develop and deploy advanced network applications and technologies for the creation of tomorrow’s Internet.
Related resources
- 1. Federal Communications Commission. Voice-over Internet protocol: frequently asked questions. http://www.fcc.gov/voip/
- 2. Internet2. http://www.internet2.edu/
Disclosure
Dr. Luo reports no financial relationship with any company whose products are mentioned in this article. The opinions expressed by Dr. Luo in this column are his own and do not necessarily reflect those of Current Psychiatry.
(accessed Oct. 3, 2005)
1. Rojas P. Skype coming to Palm next month? Engadget Sept. 14, 2005. Available at: http://www.engadget.com/entry/1016803924623324/.
2. Qovia files patents for voice spam blocking technology. Available at: http://www.qovia.com/company/news/06.28.2004_voip_spam_patent_app_final.htm.
(accessed Oct. 3, 2005)
1. Rojas P. Skype coming to Palm next month? Engadget Sept. 14, 2005. Available at: http://www.engadget.com/entry/1016803924623324/.
2. Qovia files patents for voice spam blocking technology. Available at: http://www.qovia.com/company/news/06.28.2004_voip_spam_patent_app_final.htm.