User login
Primary vs secondary: A review of pneumothorax management
THORACIC ONCOLOGY AND CHEST PROCEDURES NETWORK
Pleural Disease Section

The consensus for treatment of PSP depends on the size of the pneumothorax; if smaller than 2-3 cm, the patient can be observed for 3-6 hours and if radiographically stable, can discharge home with close (within 48 hours) follow-up and repeat chest radiograph (CXR).1,2 If symptomatic or large, an intervention is recommended or home discharge with a Heimlich valve and close follow up (48 hours) with interval CXR.1 For the management of SSP, it is recommended that the patient remain hospitalized, with a lower threshold to intervene with chest tube placement.1,2

Both the 2001 CHEST guidelines and 2010 BTS guidelines recommend the use of a small bore pigtail catheter (<14 Fr) for management of PSP.1,2 Expert consensus and retrospective studies recommend the use of a large bore chest tube (>28 French) in patients with secondary spontaneous pneumothorax and concomitant hemothorax, empyema, large air leaks, or mechanical ventilation.3,4
For patients requiring pleurodesis, talc slurry is frequently used due to it being widely available and inexpensive.5 However, talc is associated with impurities and has been associated with severe pain, fever, dyspnea, and pneumonitis.6,7 Other agents such as doxycycline have been studied but overall data is lacking. One study comparing doxycycline solution with talc slurry showed less recurrence of pneumothorax with talc as compared with doxycycline with no difference in side effects.8

– Praneet Iyer, MD
Member-at-Large
– Cristina Salmon, MD
Fellow-in-Training
– John N. Shumar, DO
Member-at-Large
References
1. Baumann MH, AACP Pneumothorax Consensus Group, et al. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. CHEST. 2001;119:590-602. doi: 10.1378/chest.119.2.590
2. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ; BTS Pleural Disease Guideline Group Management of a malignant pleural effusion: British Thoracic Society pleural disease guideline 2010. Thorax. 2010;65:ii32-ii40. doi: 10.1136/thx.2010.136994
3. Lin YC, Tu CY, Liang SJ, et al. Pigtail catheter for the management of pneumothorax in mechanically ventilated patients. Am J Emerg Med. 2010;28(4):466-471. doi: 10.1016/j.ajem.2009.01.033. Epub 2010 Jan 28. PMID: 20466227.4. Baumann MH. Pleural Disease: An International Textbook. London: Arnold Publishers; 2003.
5. How CH, Hsu HH, Chen JS. Chemical pleurodesis for spontaneous pneumothorax. J Formos Med Assoc. 2013;112:749-755. 10.1016/j.jfma.2013.10.016
6. Rehse DH, Aye RW, Florence MG. Respiratory failure following talc pleurodesis. Am J Surg. 1999;177:437-440. Doi: 10.1016/S0002-9610(99)00075-6
7. Ferrer J, Villarino MA, Tura JM, et al. Talc preparations used for pleurodesis vary markedly from one preparation to another. CHEST. 2001;119:1901-1905. doi: 10.1378/chest.119.6.1901
8. Park EH, Kim JH, Yee J, et al. Comparisons of doxycycline solution with talc slurry for chemical pleurodesis and risk factors for recurrence in South Korean patients with spontaneous pneumothorax. Eur J Hosp Pharm. 2019;26(5):275-279. doi: 10.1136/ejhpharm-2017-001465. Epub 2018 Apr 18. PMID: 31656615; PMCID: PMC6788261.
THORACIC ONCOLOGY AND CHEST PROCEDURES NETWORK
Pleural Disease Section
The consensus for treatment of PSP depends on the size of the pneumothorax; if smaller than 2-3 cm, the patient can be observed for 3-6 hours and if radiographically stable, can discharge home with close (within 48 hours) follow-up and repeat chest radiograph (CXR).1,2 If symptomatic or large, an intervention is recommended or home discharge with a Heimlich valve and close follow up (48 hours) with interval CXR.1 For the management of SSP, it is recommended that the patient remain hospitalized, with a lower threshold to intervene with chest tube placement.1,2
Both the 2001 CHEST guidelines and 2010 BTS guidelines recommend the use of a small bore pigtail catheter (<14 Fr) for management of PSP.1,2 Expert consensus and retrospective studies recommend the use of a large bore chest tube (>28 French) in patients with secondary spontaneous pneumothorax and concomitant hemothorax, empyema, large air leaks, or mechanical ventilation.3,4
For patients requiring pleurodesis, talc slurry is frequently used due to it being widely available and inexpensive.5 However, talc is associated with impurities and has been associated with severe pain, fever, dyspnea, and pneumonitis.6,7 Other agents such as doxycycline have been studied but overall data is lacking. One study comparing doxycycline solution with talc slurry showed less recurrence of pneumothorax with talc as compared with doxycycline with no difference in side effects.8
– Praneet Iyer, MD
Member-at-Large
– Cristina Salmon, MD
Fellow-in-Training
– John N. Shumar, DO
Member-at-Large
References
1. Baumann MH, AACP Pneumothorax Consensus Group, et al. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. CHEST. 2001;119:590-602. doi: 10.1378/chest.119.2.590
2. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ; BTS Pleural Disease Guideline Group Management of a malignant pleural effusion: British Thoracic Society pleural disease guideline 2010. Thorax. 2010;65:ii32-ii40. doi: 10.1136/thx.2010.136994
3. Lin YC, Tu CY, Liang SJ, et al. Pigtail catheter for the management of pneumothorax in mechanically ventilated patients. Am J Emerg Med. 2010;28(4):466-471. doi: 10.1016/j.ajem.2009.01.033. Epub 2010 Jan 28. PMID: 20466227.4. Baumann MH. Pleural Disease: An International Textbook. London: Arnold Publishers; 2003.
5. How CH, Hsu HH, Chen JS. Chemical pleurodesis for spontaneous pneumothorax. J Formos Med Assoc. 2013;112:749-755. 10.1016/j.jfma.2013.10.016
6. Rehse DH, Aye RW, Florence MG. Respiratory failure following talc pleurodesis. Am J Surg. 1999;177:437-440. Doi: 10.1016/S0002-9610(99)00075-6
7. Ferrer J, Villarino MA, Tura JM, et al. Talc preparations used for pleurodesis vary markedly from one preparation to another. CHEST. 2001;119:1901-1905. doi: 10.1378/chest.119.6.1901
8. Park EH, Kim JH, Yee J, et al. Comparisons of doxycycline solution with talc slurry for chemical pleurodesis and risk factors for recurrence in South Korean patients with spontaneous pneumothorax. Eur J Hosp Pharm. 2019;26(5):275-279. doi: 10.1136/ejhpharm-2017-001465. Epub 2018 Apr 18. PMID: 31656615; PMCID: PMC6788261.
THORACIC ONCOLOGY AND CHEST PROCEDURES NETWORK
Pleural Disease Section
The consensus for treatment of PSP depends on the size of the pneumothorax; if smaller than 2-3 cm, the patient can be observed for 3-6 hours and if radiographically stable, can discharge home with close (within 48 hours) follow-up and repeat chest radiograph (CXR).1,2 If symptomatic or large, an intervention is recommended or home discharge with a Heimlich valve and close follow up (48 hours) with interval CXR.1 For the management of SSP, it is recommended that the patient remain hospitalized, with a lower threshold to intervene with chest tube placement.1,2
Both the 2001 CHEST guidelines and 2010 BTS guidelines recommend the use of a small bore pigtail catheter (<14 Fr) for management of PSP.1,2 Expert consensus and retrospective studies recommend the use of a large bore chest tube (>28 French) in patients with secondary spontaneous pneumothorax and concomitant hemothorax, empyema, large air leaks, or mechanical ventilation.3,4
For patients requiring pleurodesis, talc slurry is frequently used due to it being widely available and inexpensive.5 However, talc is associated with impurities and has been associated with severe pain, fever, dyspnea, and pneumonitis.6,7 Other agents such as doxycycline have been studied but overall data is lacking. One study comparing doxycycline solution with talc slurry showed less recurrence of pneumothorax with talc as compared with doxycycline with no difference in side effects.8
– Praneet Iyer, MD
Member-at-Large
– Cristina Salmon, MD
Fellow-in-Training
– John N. Shumar, DO
Member-at-Large
References
1. Baumann MH, AACP Pneumothorax Consensus Group, et al. Management of spontaneous pneumothorax: an American College of Chest Physicians Delphi consensus statement. CHEST. 2001;119:590-602. doi: 10.1378/chest.119.2.590
2. Roberts ME, Neville E, Berrisford RG, Antunes G, Ali NJ; BTS Pleural Disease Guideline Group Management of a malignant pleural effusion: British Thoracic Society pleural disease guideline 2010. Thorax. 2010;65:ii32-ii40. doi: 10.1136/thx.2010.136994
3. Lin YC, Tu CY, Liang SJ, et al. Pigtail catheter for the management of pneumothorax in mechanically ventilated patients. Am J Emerg Med. 2010;28(4):466-471. doi: 10.1016/j.ajem.2009.01.033. Epub 2010 Jan 28. PMID: 20466227.4. Baumann MH. Pleural Disease: An International Textbook. London: Arnold Publishers; 2003.
5. How CH, Hsu HH, Chen JS. Chemical pleurodesis for spontaneous pneumothorax. J Formos Med Assoc. 2013;112:749-755. 10.1016/j.jfma.2013.10.016
6. Rehse DH, Aye RW, Florence MG. Respiratory failure following talc pleurodesis. Am J Surg. 1999;177:437-440. Doi: 10.1016/S0002-9610(99)00075-6
7. Ferrer J, Villarino MA, Tura JM, et al. Talc preparations used for pleurodesis vary markedly from one preparation to another. CHEST. 2001;119:1901-1905. doi: 10.1378/chest.119.6.1901
8. Park EH, Kim JH, Yee J, et al. Comparisons of doxycycline solution with talc slurry for chemical pleurodesis and risk factors for recurrence in South Korean patients with spontaneous pneumothorax. Eur J Hosp Pharm. 2019;26(5):275-279. doi: 10.1136/ejhpharm-2017-001465. Epub 2018 Apr 18. PMID: 31656615; PMCID: PMC6788261.
Severe early-life respiratory infections heighten pediatric OSA risk
AIRWAYS DISORDERS NETWORK
Pediatric Chest Medicine Section
Children with severe lower respiratory tract infections (LRTIs) within the first 2 years of life had a 2.06-fold increased risk of developing pediatric OSA by age 5, according to a study comparing patients hospitalized with LRTI to controls without severe LRTI.1 Prior studies linked LRTI and OSA, but the impact of LRTI severity was unknown.2,3,4 They used Kaplan-Meier survival estimates and Cox proportional hazards models to evaluate the risk of OSA.
Compared with patients with severe LRTIs, controls were more likely to have been full-term births, delivered vaginally, and breastfed. The OSA rate was significantly higher among children with severe LRTIs compared with controls (14.7% vs 6.8%). In the adjusted model controlling for relevant maternal and infant covariables, severe LRTI was significantly associated with increased OSA risk (HR, 2.06; 95% CI, 1.41-3.02; P < .001). Other factors such as prematurity (HR, 1.34; 95% CI, 1.01-1.77; P = .039) and maternal obesity (HR, 1.82; 95% CI, 1.32-2.52; P < .001) were also associated with increased OSA risk.
Maria Gutierrez, MD, of the Division of Pediatric Allergy, Immunology, and Rheumatology at Johns Hopkins University School of Medicine in Baltimore led the research. The study was published in Pediatric Pulmonology (2023 Dec 2. doi: 10.1002/ppul.26810). Study limitations included the use of electronic medical record data and potential lack of generalizability. The BBC is supported by the NIH.
– Agnes S. Montgomery, MD
Fellow-in-Training
References
1. Gayoso-Liviac MG, Nino G, Montgomery AS, Hong X, Wang X, Gutierrez MJ. Infants hospitalized with lower respiratory tract infections during the first two years of life have increased risk of pediatric obstructive sleep apnea. Pediatr Pulmonol. 2024;59:679-687.
2. Snow A, Dayyat E, Montgomery‐Downs HE, Kheirandish‐Gozal L, Gozal D. Pediatric obstructive sleep apnea: a potential late consequence of respiratory syncytial virus bronchiolitis. Pediatr Pulmonol. 2009;44(12):1186‐1191.
3. Chen VC‐H, Yang Y‐H, Kuo T‐Y, et al. Increased incidence of obstructive sleep apnea in hospitalized children after enterovirus infection: a nationwide population‐based cohort study. Pediatr Infect Dis J. 2018;37(9):872‐879.
4. Gutierrez MJ, Nino G, Landeo‐Gutierrez JS, et al. Lower respiratory tract infections in early life are associated with obstructive sleep apnea diagnosis during childhood in a large birth cohort. Sleep. 2021;44:12.
AIRWAYS DISORDERS NETWORK
Pediatric Chest Medicine Section
Children with severe lower respiratory tract infections (LRTIs) within the first 2 years of life had a 2.06-fold increased risk of developing pediatric OSA by age 5, according to a study comparing patients hospitalized with LRTI to controls without severe LRTI.1 Prior studies linked LRTI and OSA, but the impact of LRTI severity was unknown.2,3,4 They used Kaplan-Meier survival estimates and Cox proportional hazards models to evaluate the risk of OSA.
Compared with patients with severe LRTIs, controls were more likely to have been full-term births, delivered vaginally, and breastfed. The OSA rate was significantly higher among children with severe LRTIs compared with controls (14.7% vs 6.8%). In the adjusted model controlling for relevant maternal and infant covariables, severe LRTI was significantly associated with increased OSA risk (HR, 2.06; 95% CI, 1.41-3.02; P < .001). Other factors such as prematurity (HR, 1.34; 95% CI, 1.01-1.77; P = .039) and maternal obesity (HR, 1.82; 95% CI, 1.32-2.52; P < .001) were also associated with increased OSA risk.
Maria Gutierrez, MD, of the Division of Pediatric Allergy, Immunology, and Rheumatology at Johns Hopkins University School of Medicine in Baltimore led the research. The study was published in Pediatric Pulmonology (2023 Dec 2. doi: 10.1002/ppul.26810). Study limitations included the use of electronic medical record data and potential lack of generalizability. The BBC is supported by the NIH.
– Agnes S. Montgomery, MD
Fellow-in-Training
References
1. Gayoso-Liviac MG, Nino G, Montgomery AS, Hong X, Wang X, Gutierrez MJ. Infants hospitalized with lower respiratory tract infections during the first two years of life have increased risk of pediatric obstructive sleep apnea. Pediatr Pulmonol. 2024;59:679-687.
2. Snow A, Dayyat E, Montgomery‐Downs HE, Kheirandish‐Gozal L, Gozal D. Pediatric obstructive sleep apnea: a potential late consequence of respiratory syncytial virus bronchiolitis. Pediatr Pulmonol. 2009;44(12):1186‐1191.
3. Chen VC‐H, Yang Y‐H, Kuo T‐Y, et al. Increased incidence of obstructive sleep apnea in hospitalized children after enterovirus infection: a nationwide population‐based cohort study. Pediatr Infect Dis J. 2018;37(9):872‐879.
4. Gutierrez MJ, Nino G, Landeo‐Gutierrez JS, et al. Lower respiratory tract infections in early life are associated with obstructive sleep apnea diagnosis during childhood in a large birth cohort. Sleep. 2021;44:12.
AIRWAYS DISORDERS NETWORK
Pediatric Chest Medicine Section
Children with severe lower respiratory tract infections (LRTIs) within the first 2 years of life had a 2.06-fold increased risk of developing pediatric OSA by age 5, according to a study comparing patients hospitalized with LRTI to controls without severe LRTI.1 Prior studies linked LRTI and OSA, but the impact of LRTI severity was unknown.2,3,4 They used Kaplan-Meier survival estimates and Cox proportional hazards models to evaluate the risk of OSA.
Compared with patients with severe LRTIs, controls were more likely to have been full-term births, delivered vaginally, and breastfed. The OSA rate was significantly higher among children with severe LRTIs compared with controls (14.7% vs 6.8%). In the adjusted model controlling for relevant maternal and infant covariables, severe LRTI was significantly associated with increased OSA risk (HR, 2.06; 95% CI, 1.41-3.02; P < .001). Other factors such as prematurity (HR, 1.34; 95% CI, 1.01-1.77; P = .039) and maternal obesity (HR, 1.82; 95% CI, 1.32-2.52; P < .001) were also associated with increased OSA risk.
Maria Gutierrez, MD, of the Division of Pediatric Allergy, Immunology, and Rheumatology at Johns Hopkins University School of Medicine in Baltimore led the research. The study was published in Pediatric Pulmonology (2023 Dec 2. doi: 10.1002/ppul.26810). Study limitations included the use of electronic medical record data and potential lack of generalizability. The BBC is supported by the NIH.
– Agnes S. Montgomery, MD
Fellow-in-Training
References
1. Gayoso-Liviac MG, Nino G, Montgomery AS, Hong X, Wang X, Gutierrez MJ. Infants hospitalized with lower respiratory tract infections during the first two years of life have increased risk of pediatric obstructive sleep apnea. Pediatr Pulmonol. 2024;59:679-687.
2. Snow A, Dayyat E, Montgomery‐Downs HE, Kheirandish‐Gozal L, Gozal D. Pediatric obstructive sleep apnea: a potential late consequence of respiratory syncytial virus bronchiolitis. Pediatr Pulmonol. 2009;44(12):1186‐1191.
3. Chen VC‐H, Yang Y‐H, Kuo T‐Y, et al. Increased incidence of obstructive sleep apnea in hospitalized children after enterovirus infection: a nationwide population‐based cohort study. Pediatr Infect Dis J. 2018;37(9):872‐879.
4. Gutierrez MJ, Nino G, Landeo‐Gutierrez JS, et al. Lower respiratory tract infections in early life are associated with obstructive sleep apnea diagnosis during childhood in a large birth cohort. Sleep. 2021;44:12.
Electrical impedance tomography: Visualization and integration of the impact of mechanical ventilation
CRITICAL CARE NETWORK
Mechanical Ventilation and Airways Management Section
1,2,3 Continuous monitoring of the tidal volume, plateau pressure, and positive end-expiratory pressure (PEEP) is crucial to maintain LPV. Electrical impedance tomography (EIT) is a noninvasive, radiation-free, imaging method of the electrical conductivity distribution inside the human body.4 Integrating EIT into invasive mechanical ventilation allows imaging of the regional lung ventilation as affected by the mechanical ventilation settings as well as the patient position. It can also provide a personalized approach to determining the optimum ventilatory settings based on individual patient conditions.5,6
Optimum PEEP titration is crucial to prevent lung collapse as well as overdistension. In a single-center, randomized, crossover pilot study of 12 patients, optimum PEEP titration was carried out using a high PEEP/FiO2 table vs EIT in moderate to severe ARDS. The primary endpoint was the reduction of mechanical power, which was consistently lower in the EIT group.7 EIT also allows the assessment of regional compliance of the lungs. There are reports regarding the superiority of regional compliance of lung over global compliance in achieving better gas exchange, lung compliance, and weaning of mechanical ventilation.8 EIT could assess the patient’s response to prone positioning by illustrating the change in the functional residual capacity between supine and prone positioning.9 In addition, by visualization of the ventilated areas during spontaneous breathing and reduction of pressure support, EIT could help in weaning off the mechanical ventilation.10

In conclusion, EIT can be a tool to provide safe and personalized mechanical ventilation in patients with respiratory failure. However, there are limited data regarding its use and application, which might become an interesting subject for future clinical research.
– Akram M. Zaaqoq, MD, MPH
Member-at-Large
References
1. Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):347-354.
2. Brower RG, Matthay MA, Morris A, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308.
3. Neto AS, Simonis FD, Barbas CSV, et al. Lung-protective ventilation with low tidal volumes and the occurrence of pulmonary complications in patients without acute respiratory distress syndrome: a systematic review and individual patient data analysis. Crit Care Med. 2015;43(10):2155-2163.
4. Adler A, Boyle A. Electrical impedance tomography: tissue properties to image measures. IEEE Trans Biomed Eng. 2017;64(11):2494-2504.
5. Jang GY, Ayoub G, Kim YE, et al. Integrated EIT system for functional lung ventilation imaging. Biomed Eng Online. 2019;18(1):83.
6. Sella N, Pettenuzzo T, Zarantonello F, et al. Electrical impedance tomography: a compass for the safe route to optimal PEEP. Respir Med. 2021;187:106555.
7. Jimenez JV, Munroe E, Weirauch AJ, et al. Electric impedance tomography-guided PEEP titration reduces mechanical power in ARDS: a randomized crossover pilot trial. Crit Care. 2023;27(1):21.
8. Costa ELV, Borges JB, Melo A, et al. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. 2009;35(6):1132-1137.9. Riera J, Pérez P, Cortés J, Roca O, Masclans JR, Rello J. Effect of high-flow nasal cannula and body position on end-expiratory lung volume: a cohort study using electrical impedance tomography. Respir Care. 2013;58(4):589-596.10. Wisse JJ, Goos TG, Jonkman AH, et al. Electrical impedance tomography as a monitoring tool during weaning from mechanical ventilation: an observational study during the spontaneous breathing trial. Respir Res. 2024;25(1):179.
CRITICAL CARE NETWORK
Mechanical Ventilation and Airways Management Section
1,2,3 Continuous monitoring of the tidal volume, plateau pressure, and positive end-expiratory pressure (PEEP) is crucial to maintain LPV. Electrical impedance tomography (EIT) is a noninvasive, radiation-free, imaging method of the electrical conductivity distribution inside the human body.4 Integrating EIT into invasive mechanical ventilation allows imaging of the regional lung ventilation as affected by the mechanical ventilation settings as well as the patient position. It can also provide a personalized approach to determining the optimum ventilatory settings based on individual patient conditions.5,6
Optimum PEEP titration is crucial to prevent lung collapse as well as overdistension. In a single-center, randomized, crossover pilot study of 12 patients, optimum PEEP titration was carried out using a high PEEP/FiO2 table vs EIT in moderate to severe ARDS. The primary endpoint was the reduction of mechanical power, which was consistently lower in the EIT group.7 EIT also allows the assessment of regional compliance of the lungs. There are reports regarding the superiority of regional compliance of lung over global compliance in achieving better gas exchange, lung compliance, and weaning of mechanical ventilation.8 EIT could assess the patient’s response to prone positioning by illustrating the change in the functional residual capacity between supine and prone positioning.9 In addition, by visualization of the ventilated areas during spontaneous breathing and reduction of pressure support, EIT could help in weaning off the mechanical ventilation.10
In conclusion, EIT can be a tool to provide safe and personalized mechanical ventilation in patients with respiratory failure. However, there are limited data regarding its use and application, which might become an interesting subject for future clinical research.
– Akram M. Zaaqoq, MD, MPH
Member-at-Large
References
1. Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):347-354.
2. Brower RG, Matthay MA, Morris A, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308.
3. Neto AS, Simonis FD, Barbas CSV, et al. Lung-protective ventilation with low tidal volumes and the occurrence of pulmonary complications in patients without acute respiratory distress syndrome: a systematic review and individual patient data analysis. Crit Care Med. 2015;43(10):2155-2163.
4. Adler A, Boyle A. Electrical impedance tomography: tissue properties to image measures. IEEE Trans Biomed Eng. 2017;64(11):2494-2504.
5. Jang GY, Ayoub G, Kim YE, et al. Integrated EIT system for functional lung ventilation imaging. Biomed Eng Online. 2019;18(1):83.
6. Sella N, Pettenuzzo T, Zarantonello F, et al. Electrical impedance tomography: a compass for the safe route to optimal PEEP. Respir Med. 2021;187:106555.
7. Jimenez JV, Munroe E, Weirauch AJ, et al. Electric impedance tomography-guided PEEP titration reduces mechanical power in ARDS: a randomized crossover pilot trial. Crit Care. 2023;27(1):21.
8. Costa ELV, Borges JB, Melo A, et al. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. 2009;35(6):1132-1137.9. Riera J, Pérez P, Cortés J, Roca O, Masclans JR, Rello J. Effect of high-flow nasal cannula and body position on end-expiratory lung volume: a cohort study using electrical impedance tomography. Respir Care. 2013;58(4):589-596.10. Wisse JJ, Goos TG, Jonkman AH, et al. Electrical impedance tomography as a monitoring tool during weaning from mechanical ventilation: an observational study during the spontaneous breathing trial. Respir Res. 2024;25(1):179.
CRITICAL CARE NETWORK
Mechanical Ventilation and Airways Management Section
1,2,3 Continuous monitoring of the tidal volume, plateau pressure, and positive end-expiratory pressure (PEEP) is crucial to maintain LPV. Electrical impedance tomography (EIT) is a noninvasive, radiation-free, imaging method of the electrical conductivity distribution inside the human body.4 Integrating EIT into invasive mechanical ventilation allows imaging of the regional lung ventilation as affected by the mechanical ventilation settings as well as the patient position. It can also provide a personalized approach to determining the optimum ventilatory settings based on individual patient conditions.5,6
Optimum PEEP titration is crucial to prevent lung collapse as well as overdistension. In a single-center, randomized, crossover pilot study of 12 patients, optimum PEEP titration was carried out using a high PEEP/FiO2 table vs EIT in moderate to severe ARDS. The primary endpoint was the reduction of mechanical power, which was consistently lower in the EIT group.7 EIT also allows the assessment of regional compliance of the lungs. There are reports regarding the superiority of regional compliance of lung over global compliance in achieving better gas exchange, lung compliance, and weaning of mechanical ventilation.8 EIT could assess the patient’s response to prone positioning by illustrating the change in the functional residual capacity between supine and prone positioning.9 In addition, by visualization of the ventilated areas during spontaneous breathing and reduction of pressure support, EIT could help in weaning off the mechanical ventilation.10
In conclusion, EIT can be a tool to provide safe and personalized mechanical ventilation in patients with respiratory failure. However, there are limited data regarding its use and application, which might become an interesting subject for future clinical research.
– Akram M. Zaaqoq, MD, MPH
Member-at-Large
References
1. Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):347-354.
2. Brower RG, Matthay MA, Morris A, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301-1308.
3. Neto AS, Simonis FD, Barbas CSV, et al. Lung-protective ventilation with low tidal volumes and the occurrence of pulmonary complications in patients without acute respiratory distress syndrome: a systematic review and individual patient data analysis. Crit Care Med. 2015;43(10):2155-2163.
4. Adler A, Boyle A. Electrical impedance tomography: tissue properties to image measures. IEEE Trans Biomed Eng. 2017;64(11):2494-2504.
5. Jang GY, Ayoub G, Kim YE, et al. Integrated EIT system for functional lung ventilation imaging. Biomed Eng Online. 2019;18(1):83.
6. Sella N, Pettenuzzo T, Zarantonello F, et al. Electrical impedance tomography: a compass for the safe route to optimal PEEP. Respir Med. 2021;187:106555.
7. Jimenez JV, Munroe E, Weirauch AJ, et al. Electric impedance tomography-guided PEEP titration reduces mechanical power in ARDS: a randomized crossover pilot trial. Crit Care. 2023;27(1):21.
8. Costa ELV, Borges JB, Melo A, et al. Bedside estimation of recruitable alveolar collapse and hyperdistension by electrical impedance tomography. Intensive Care Med. 2009;35(6):1132-1137.9. Riera J, Pérez P, Cortés J, Roca O, Masclans JR, Rello J. Effect of high-flow nasal cannula and body position on end-expiratory lung volume: a cohort study using electrical impedance tomography. Respir Care. 2013;58(4):589-596.10. Wisse JJ, Goos TG, Jonkman AH, et al. Electrical impedance tomography as a monitoring tool during weaning from mechanical ventilation: an observational study during the spontaneous breathing trial. Respir Res. 2024;25(1):179.
Nurse practitioners as advocates for health policy and patient care
APP INTERSECTION
In the intricate tapestry of health care, the roles of advanced practice registered nurses, also known as nurse practitioners (NPs), have evolved beyond the confines of clinical settings.
The journey into the realm of nursing often begins with a passion for healing and caring for others. However, for many, this path frequently leads to overcoming barriers to patient care, restrictions to practice, and lengthy red tape in the face of care teams that do not fully understand the scope and role of the NP.

Delving into health policy intricacies, efforts focus on understanding how legislative decisions directly impact patient care. Involvement in advocacy aims to improve health care access, promote patient-centered policies, and reduce disparities in the workforce and patient care.
Achieving sound primary care for people with multiple comorbid conditions requires the skills and abilities of all members of the health care workforce, including NPs.1 NPs have assumed an increasing role in recent decades as primary care providers for people with chronic diseases, while national trends show few physicians entering and staying in primary care.2,3,4,5 NPs are the nation’s fastest-growing primary care workforce, with nearly 90% of them trained to deliver primary care.6,7 Yet, NPs continue to experience reduced reimbursement for services compared with their physician counterparts.
Barriers to practice reduce the productivity and capacity of these health care professionals. Not permitting NPs to practice to the full extent of their licensure and education decreases the types and amounts of health care services that can be provided for people who need care.8 As noted in the Future of Nursing 2020-2030 report, this restriction also has significant implications for addressing the disparities in access to health care between rural and urban areas. A recent systemic review revealed that full practice authority is associated with higher numbers of NPs in rural areas and in primary care where there is a shortage of physicians. Full practice authority is associated with increased access to care and utilization of health care services, lower cost of care, and no decrease in quality of care.9,10 As stated in the National Council of State Boards of Nursing 2022 Environmental Scan, regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as ensuring that standards of care are met and patients are protected.11
Of equal importance is regulator awareness of the degree to which barriers continue to impact NP practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict NP practice. In turn, regulators can support efforts to remove unnecessary barriers to NP practice.
Fueled by experience in reduced practice, NPs become catalysts for change, transcending the role of health care providers. At the core of the NP role lies a commitment to patient advocacy. Beyond diagnosing and treating illnesses, NPs champion patients’ rights, ensuring their voices in health care decision-making. Advocacy efforts range from expanding access to essential services to promoting preventive care and fighting discrimination. By embracing roles as caregivers and agents of change, NPs can help the health care system emerge equitable, accessible, and patient-centric.
Ms. Kavanaugh is Assistant Dean of Graduate Nursing, University of Mount Saint Vincent, Pulmonary Critical Care Nurse Practitioner, Stamford Hospital.
References
1. McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A Systematic Review of Outcomes Related to Nurse Practitioner-Delivered Primary Care for Multiple Chronic Conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
2. Fraze T, Briggs A, Whitcomb E, Peck K, & Meara E (2020). Role of nurse practitioners in caring for patients with complex health needs. Medical Care, 58(10), 853–860. 10.1097/mlr.0000000000001364
3. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
4. Buerhaus P (2018). Nurse practitioners: A solution to America’s primary care crisis. American Enterprise Institute. https://www.aei.org/research-products/report/nurse-practitioners-a-solution-to-americas-primary-care-crisis/
5. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
6. American Association of Nurse Practitioners. (2022). Nurse practitioners in primary care. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioners-in-primary-care
7. Auerbach, D. I. (2012). Will the NP workforce grow in the future? New forecasts and implications for healthcare delivery. Medical Care, 50(7), 606-610. doi: http://dx.doi.org/10.1097/MLR.0b013e318249d6e7
8. National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity.
9. Yang BK, Trinkoff AM, Zito JM, Burcu M, Safer DJ, Storr CL, Johantgen ME, & Idzik S (2017). Nurse practitioner independent practice authority and mental health service delivery in U.S. Community Health Centers. Psychiatric Services, 68(10), 1032–1038. 10.1176/appi.ps.201600495
10. Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X.
11. National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1.
APP INTERSECTION
In the intricate tapestry of health care, the roles of advanced practice registered nurses, also known as nurse practitioners (NPs), have evolved beyond the confines of clinical settings.
The journey into the realm of nursing often begins with a passion for healing and caring for others. However, for many, this path frequently leads to overcoming barriers to patient care, restrictions to practice, and lengthy red tape in the face of care teams that do not fully understand the scope and role of the NP.
Delving into health policy intricacies, efforts focus on understanding how legislative decisions directly impact patient care. Involvement in advocacy aims to improve health care access, promote patient-centered policies, and reduce disparities in the workforce and patient care.
Achieving sound primary care for people with multiple comorbid conditions requires the skills and abilities of all members of the health care workforce, including NPs.1 NPs have assumed an increasing role in recent decades as primary care providers for people with chronic diseases, while national trends show few physicians entering and staying in primary care.2,3,4,5 NPs are the nation’s fastest-growing primary care workforce, with nearly 90% of them trained to deliver primary care.6,7 Yet, NPs continue to experience reduced reimbursement for services compared with their physician counterparts.
Barriers to practice reduce the productivity and capacity of these health care professionals. Not permitting NPs to practice to the full extent of their licensure and education decreases the types and amounts of health care services that can be provided for people who need care.8 As noted in the Future of Nursing 2020-2030 report, this restriction also has significant implications for addressing the disparities in access to health care between rural and urban areas. A recent systemic review revealed that full practice authority is associated with higher numbers of NPs in rural areas and in primary care where there is a shortage of physicians. Full practice authority is associated with increased access to care and utilization of health care services, lower cost of care, and no decrease in quality of care.9,10 As stated in the National Council of State Boards of Nursing 2022 Environmental Scan, regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as ensuring that standards of care are met and patients are protected.11
Of equal importance is regulator awareness of the degree to which barriers continue to impact NP practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict NP practice. In turn, regulators can support efforts to remove unnecessary barriers to NP practice.
Fueled by experience in reduced practice, NPs become catalysts for change, transcending the role of health care providers. At the core of the NP role lies a commitment to patient advocacy. Beyond diagnosing and treating illnesses, NPs champion patients’ rights, ensuring their voices in health care decision-making. Advocacy efforts range from expanding access to essential services to promoting preventive care and fighting discrimination. By embracing roles as caregivers and agents of change, NPs can help the health care system emerge equitable, accessible, and patient-centric.
Ms. Kavanaugh is Assistant Dean of Graduate Nursing, University of Mount Saint Vincent, Pulmonary Critical Care Nurse Practitioner, Stamford Hospital.
References
1. McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A Systematic Review of Outcomes Related to Nurse Practitioner-Delivered Primary Care for Multiple Chronic Conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
2. Fraze T, Briggs A, Whitcomb E, Peck K, & Meara E (2020). Role of nurse practitioners in caring for patients with complex health needs. Medical Care, 58(10), 853–860. 10.1097/mlr.0000000000001364
3. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
4. Buerhaus P (2018). Nurse practitioners: A solution to America’s primary care crisis. American Enterprise Institute. https://www.aei.org/research-products/report/nurse-practitioners-a-solution-to-americas-primary-care-crisis/
5. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
6. American Association of Nurse Practitioners. (2022). Nurse practitioners in primary care. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioners-in-primary-care
7. Auerbach, D. I. (2012). Will the NP workforce grow in the future? New forecasts and implications for healthcare delivery. Medical Care, 50(7), 606-610. doi: http://dx.doi.org/10.1097/MLR.0b013e318249d6e7
8. National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity.
9. Yang BK, Trinkoff AM, Zito JM, Burcu M, Safer DJ, Storr CL, Johantgen ME, & Idzik S (2017). Nurse practitioner independent practice authority and mental health service delivery in U.S. Community Health Centers. Psychiatric Services, 68(10), 1032–1038. 10.1176/appi.ps.201600495
10. Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X.
11. National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1.
APP INTERSECTION
In the intricate tapestry of health care, the roles of advanced practice registered nurses, also known as nurse practitioners (NPs), have evolved beyond the confines of clinical settings.
The journey into the realm of nursing often begins with a passion for healing and caring for others. However, for many, this path frequently leads to overcoming barriers to patient care, restrictions to practice, and lengthy red tape in the face of care teams that do not fully understand the scope and role of the NP.
Delving into health policy intricacies, efforts focus on understanding how legislative decisions directly impact patient care. Involvement in advocacy aims to improve health care access, promote patient-centered policies, and reduce disparities in the workforce and patient care.
Achieving sound primary care for people with multiple comorbid conditions requires the skills and abilities of all members of the health care workforce, including NPs.1 NPs have assumed an increasing role in recent decades as primary care providers for people with chronic diseases, while national trends show few physicians entering and staying in primary care.2,3,4,5 NPs are the nation’s fastest-growing primary care workforce, with nearly 90% of them trained to deliver primary care.6,7 Yet, NPs continue to experience reduced reimbursement for services compared with their physician counterparts.
Barriers to practice reduce the productivity and capacity of these health care professionals. Not permitting NPs to practice to the full extent of their licensure and education decreases the types and amounts of health care services that can be provided for people who need care.8 As noted in the Future of Nursing 2020-2030 report, this restriction also has significant implications for addressing the disparities in access to health care between rural and urban areas. A recent systemic review revealed that full practice authority is associated with higher numbers of NPs in rural areas and in primary care where there is a shortage of physicians. Full practice authority is associated with increased access to care and utilization of health care services, lower cost of care, and no decrease in quality of care.9,10 As stated in the National Council of State Boards of Nursing 2022 Environmental Scan, regulators and nurse leaders are responsible for upholding rules and regulations of nursing practice as well as ensuring that standards of care are met and patients are protected.11
Of equal importance is regulator awareness of the degree to which barriers continue to impact NP practice and limit aspects of care that directly influence care quality and access. Nursing leaders can have a significant impact on removing nonregulatory barriers to practice, such as changing outdated hospital bylaws that restrict NP practice. In turn, regulators can support efforts to remove unnecessary barriers to NP practice.
Fueled by experience in reduced practice, NPs become catalysts for change, transcending the role of health care providers. At the core of the NP role lies a commitment to patient advocacy. Beyond diagnosing and treating illnesses, NPs champion patients’ rights, ensuring their voices in health care decision-making. Advocacy efforts range from expanding access to essential services to promoting preventive care and fighting discrimination. By embracing roles as caregivers and agents of change, NPs can help the health care system emerge equitable, accessible, and patient-centric.
Ms. Kavanaugh is Assistant Dean of Graduate Nursing, University of Mount Saint Vincent, Pulmonary Critical Care Nurse Practitioner, Stamford Hospital.
References
1. McMenamin, A., Turi, E., Schlak, A., & Poghosyan, L. (2023). A Systematic Review of Outcomes Related to Nurse Practitioner-Delivered Primary Care for Multiple Chronic Conditions. Medical care research and review: MCRR, 80(6), 563–581. https://doi.org/10.1177/10775587231186720
2. Fraze T, Briggs A, Whitcomb E, Peck K, & Meara E (2020). Role of nurse practitioners in caring for patients with complex health needs. Medical Care, 58(10), 853–860. 10.1097/mlr.0000000000001364
3. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
4. Buerhaus P (2018). Nurse practitioners: A solution to America’s primary care crisis. American Enterprise Institute. https://www.aei.org/research-products/report/nurse-practitioners-a-solution-to-americas-primary-care-crisis/
5. Xue Y, Goodwin J, Adhikari D, Raji M, & Kuo Y (2017). Trends in primary care provision to medicare beneficiaries by physicians, nurse practitioners, or physician assistants: 2008–2014. Journal of Primary Care & Community Health, 8(4), 256–263. 10.1177/2150131917736634
6. American Association of Nurse Practitioners. (2022). Nurse practitioners in primary care. https://www.aanp.org/advocacy/advocacy-resource/position-statements/nurse-practitioners-in-primary-care
7. Auerbach, D. I. (2012). Will the NP workforce grow in the future? New forecasts and implications for healthcare delivery. Medical Care, 50(7), 606-610. doi: http://dx.doi.org/10.1097/MLR.0b013e318249d6e7
8. National Academy of Medicine . The National Academies Press; 2021. The future of nursing 2020-2030: Charting a path to achieve health equity.
9. Yang BK, Trinkoff AM, Zito JM, Burcu M, Safer DJ, Storr CL, Johantgen ME, & Idzik S (2017). Nurse practitioner independent practice authority and mental health service delivery in U.S. Community Health Centers. Psychiatric Services, 68(10), 1032–1038. 10.1176/appi.ps.201600495
10. Xue Y., Kannan V., Greener E., Smith J.A., Brasch J., Johnson B.A., Spetz J. Full scope-of-practice regulation is associated with higher supply of nurse practitioners in rural and primary care health professional shortage counties. Journal of Nursing Regulation. 2018;8(4):5–13. doi: 10.1016/S2155-8256(17)30176-X.
11. National Council of State Boards of Nursing The NCSBN 2022 environmental scan: Resiliency, achievement, and public protection. Journal of Nursing Regulation. 2022;12:S3–S55. doi: 10.1016/S2155-8256(22)00015-1.

Military burn pits: Their evidence and implications for respiratory health
Military service is a hazard-ridden profession. It’s easy to recognize the direct dangers from warfighting, such as gunfire and explosions, but the risks from environmental, chemical, and other occupational exposures can be harder to see.
Combustion-based waste management systems, otherwise known as “burn pits,” were used in deployed environments by the US military from the 1990s to the early 2010s. These burn pits were commonly used to eliminate plastics, electronics, munitions, metals, wood, chemicals, and even human waste. At the height of the recent conflicts in Afghanistan, Iraq, and other southwest Asia locations, more than 70% of military installations employed at least one, and nearly 4 million service members were exposed to some degree to their emissions.

Reports of burn pits being related to organic disease have garnered widespread media attention. Initially, this came through anecdotal reports of post-deployment respiratory symptoms. Over time, the conditions attributed to burn pits expanded to include newly diagnosed respiratory diseases and malignancies.
Ultimately, Congress passed the 2022 Promise to Address Comprehensive Toxins (PACT) Act, presumptively linking more than 20 diagnoses to burn pits. The PACT Act provides countless veterans access to low-cost or free medical care for their respective conditions.
What do we know about burn pits and deployment-related respiratory disease?
Data from the Millennium Cohort Study noted an approximately 40% increase in respiratory symptoms among individuals returning from deployment but no increase in the frequency of diagnosed respiratory diseases.1 This study and others definitively established a temporal relationship between deployment and respiratory symptoms. Soon after, a retrospective, observational study of service members with post-deployment respiratory symptoms found a high prevalence of constrictive bronchiolitis (CB) identified by lung biopsy.2 Patients in this group reported exposure to burn pits and a sulfur mine fire in the Mosul area while deployed. Most had normal imaging and pulmonary function testing before biopsy, confounding the clinical significance of the CB finding. The publication of this report led to increased investigation of respiratory function during and after deployment.

In a series of prospective studies that included full pulmonary function testing, impulse oscillometry, cardiopulmonary exercise testing, bronchoscopy, and, occasionally, lung biopsy to evaluate post-deployment dyspnea, only a small minority received a diagnosis of clinically significant lung disease.3,4 Additionally, when comparing spirometry and impulse oscillometry results from before and after deployment, no decline in lung function was observed in a population of service members reporting regular burn pit exposure.5 These studies suggest that at the population level, deployment does not lead to abnormalities in the structure and function of the respiratory system.
The National Academies of Sciences published two separate reviews of burn pit exposure and outcomes in 2011 and 2020.6,7 They found insufficient evidence to support a causal relationship between burn pit exposure and pulmonary disease. They highlighted studies on the composition of emissions from the area surrounding the largest military burn pit in Iraq. Levels of particulate matter, volatile organic compounds, and polycyclic aromatic hydrocarbons were elevated when compared with those of a typical American city but were similar to the pollution levels seen in the region at the time. Given these findings, they suggested ambient air pollution may have contributed more to clinically significant disease than burn pit emissions.
How do we interpret this mixed data?
At the population level, we have yet to find conclusive data directly linking burn pit exposure to the development of any respiratory disease. Does this mean that burn pits are not harmful?
Not necessarily. Research on outcomes related to burn pit exposure is challenging given the heterogeneity in exposure volume. Much of the research is retrospective and subject to recall bias. Relationships may be distorted, and the precision of reported symptoms and exposure levels is altered. Given these challenges, it’s unsurprising that evidence of causality has yet to be proven. In addition, some portion of service members has been diagnosed with respiratory disease that could be related to burn pit exposure.
What is now indisputable is that deployment to southwest Asia leads to an increase in respiratory complaints. Whether veteran respiratory symptoms are due to burn pits, ambient pollution, environmental particulate matter, or dust storms is less clinically relevant. These symptoms require attention, investigation, and management.
What does this mean for the future medical care of service members and veterans?
Many veterans with post-deployment respiratory symptoms undergo extensive evaluations without obtaining a definitive diagnosis. A recent consensus statement on deployment-related respiratory symptoms provides a framework for evaluation in such cases.8 In keeping with that statement, we recommend veterans be referred to centers with expertise in this field, such as the Department of Veterans Affairs (VA) or military health centers, when deployment-related respiratory symptoms are reported. When the evaluation does not lead to a treatable diagnosis, these centers can provide multidisciplinary care to address the symptoms of dyspnea, cough, fatigue, and exercise intolerance to improve functional status.
Despite uncertainty in the evidence or challenges in diagnosis, both the Department of Defense (DoD) and VA remain fully committed to addressing the health concerns of service members and veterans. Notably, the VA has already screened more than 5 million veterans for toxic military exposures in accordance with the PACT Act and is providing ongoing screening and care for veterans with post-deployment respiratory symptoms. Furthermore, the DoD and VA have dedicated large portions of their research budgets to investigating the impacts of exposures during military service and optimizing the care of those with respiratory symptoms. With these commitments to patient care and research, our veterans’ respiratory health can now be optimized, and future risks can be mitigated.
Dr. Haynes is Fellow, Pulmonary and Critical Care Medicine, Walter Reed National Military Medical Center, Assistant Professor of Medicine, Uniformed Services University. Dr. Nations is Pulmonary and Critical Care Medicine, Deputy Chief of Staff for Operations, Washington DC VA Medical Center, Associate Professor of Medicine, Uniformed Services University.
References
1. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. Preprint. Posted online October 22, 2009. PMID: 19850627. doi: 10.1093/aje/kwp287
2. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. Erratum in: N Engl J Med. 2011;365(18):1749. PMID: 21774710; PMCID: PMC3296566. doi: 10.1056/NEJMoa1101388
3. Morris MJ, Dodson DW, Lucero PF, et al. Study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE). Am J Respir Crit Care Med. 2014;190(1):77-84. PMID: 24922562. doi: 10.1164/rccm.201402-0372OC
4. Morris MJ, Walter RJ, McCann ET, et al. Clinical evaluation of deployed military personnel with chronic respiratory symptoms: study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE) III. Chest. 2020;157(6):1559-1567. Preprint. Posted online February 1, 2020. PMID: 32017933. doi: 10.1016/j.chest.2020.01.024
5. Morris MJ, Skabelund AJ, Rawlins FA 3rd, Gallup RA, Aden JK, Holley AB. Study of active duty military personnel for environmental deployment exposures: pre- and post-deployment spirometry (STAMPEDE II). Respir Care. 2019;64(5):536-544. Preprint. Posted online January 8, 2019.PMID: 30622173. doi: 10.4187/respcare.06396
6. Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. https://doi.org/10.17226/13209
7. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. https://doi.org/10.17226/25837
8. Falvo MJ, Sotolongo AM, Osterholzer JJ, et al. Consensus statements on deployment-related respiratory disease, inclusive of constrictive bronchiolitis: a modified Delphi study. Chest. 2023;163(3):599-609. Preprint. Posted November 4, 2022. PMID: 36343686; PMCID: PMC10154857. doi: 10.1016/j.chest.2022.10.031
Military service is a hazard-ridden profession. It’s easy to recognize the direct dangers from warfighting, such as gunfire and explosions, but the risks from environmental, chemical, and other occupational exposures can be harder to see.
Combustion-based waste management systems, otherwise known as “burn pits,” were used in deployed environments by the US military from the 1990s to the early 2010s. These burn pits were commonly used to eliminate plastics, electronics, munitions, metals, wood, chemicals, and even human waste. At the height of the recent conflicts in Afghanistan, Iraq, and other southwest Asia locations, more than 70% of military installations employed at least one, and nearly 4 million service members were exposed to some degree to their emissions.
Reports of burn pits being related to organic disease have garnered widespread media attention. Initially, this came through anecdotal reports of post-deployment respiratory symptoms. Over time, the conditions attributed to burn pits expanded to include newly diagnosed respiratory diseases and malignancies.
Ultimately, Congress passed the 2022 Promise to Address Comprehensive Toxins (PACT) Act, presumptively linking more than 20 diagnoses to burn pits. The PACT Act provides countless veterans access to low-cost or free medical care for their respective conditions.
What do we know about burn pits and deployment-related respiratory disease?
Data from the Millennium Cohort Study noted an approximately 40% increase in respiratory symptoms among individuals returning from deployment but no increase in the frequency of diagnosed respiratory diseases.1 This study and others definitively established a temporal relationship between deployment and respiratory symptoms. Soon after, a retrospective, observational study of service members with post-deployment respiratory symptoms found a high prevalence of constrictive bronchiolitis (CB) identified by lung biopsy.2 Patients in this group reported exposure to burn pits and a sulfur mine fire in the Mosul area while deployed. Most had normal imaging and pulmonary function testing before biopsy, confounding the clinical significance of the CB finding. The publication of this report led to increased investigation of respiratory function during and after deployment.
In a series of prospective studies that included full pulmonary function testing, impulse oscillometry, cardiopulmonary exercise testing, bronchoscopy, and, occasionally, lung biopsy to evaluate post-deployment dyspnea, only a small minority received a diagnosis of clinically significant lung disease.3,4 Additionally, when comparing spirometry and impulse oscillometry results from before and after deployment, no decline in lung function was observed in a population of service members reporting regular burn pit exposure.5 These studies suggest that at the population level, deployment does not lead to abnormalities in the structure and function of the respiratory system.
The National Academies of Sciences published two separate reviews of burn pit exposure and outcomes in 2011 and 2020.6,7 They found insufficient evidence to support a causal relationship between burn pit exposure and pulmonary disease. They highlighted studies on the composition of emissions from the area surrounding the largest military burn pit in Iraq. Levels of particulate matter, volatile organic compounds, and polycyclic aromatic hydrocarbons were elevated when compared with those of a typical American city but were similar to the pollution levels seen in the region at the time. Given these findings, they suggested ambient air pollution may have contributed more to clinically significant disease than burn pit emissions.
How do we interpret this mixed data?
At the population level, we have yet to find conclusive data directly linking burn pit exposure to the development of any respiratory disease. Does this mean that burn pits are not harmful?
Not necessarily. Research on outcomes related to burn pit exposure is challenging given the heterogeneity in exposure volume. Much of the research is retrospective and subject to recall bias. Relationships may be distorted, and the precision of reported symptoms and exposure levels is altered. Given these challenges, it’s unsurprising that evidence of causality has yet to be proven. In addition, some portion of service members has been diagnosed with respiratory disease that could be related to burn pit exposure.
What is now indisputable is that deployment to southwest Asia leads to an increase in respiratory complaints. Whether veteran respiratory symptoms are due to burn pits, ambient pollution, environmental particulate matter, or dust storms is less clinically relevant. These symptoms require attention, investigation, and management.
What does this mean for the future medical care of service members and veterans?
Many veterans with post-deployment respiratory symptoms undergo extensive evaluations without obtaining a definitive diagnosis. A recent consensus statement on deployment-related respiratory symptoms provides a framework for evaluation in such cases.8 In keeping with that statement, we recommend veterans be referred to centers with expertise in this field, such as the Department of Veterans Affairs (VA) or military health centers, when deployment-related respiratory symptoms are reported. When the evaluation does not lead to a treatable diagnosis, these centers can provide multidisciplinary care to address the symptoms of dyspnea, cough, fatigue, and exercise intolerance to improve functional status.
Despite uncertainty in the evidence or challenges in diagnosis, both the Department of Defense (DoD) and VA remain fully committed to addressing the health concerns of service members and veterans. Notably, the VA has already screened more than 5 million veterans for toxic military exposures in accordance with the PACT Act and is providing ongoing screening and care for veterans with post-deployment respiratory symptoms. Furthermore, the DoD and VA have dedicated large portions of their research budgets to investigating the impacts of exposures during military service and optimizing the care of those with respiratory symptoms. With these commitments to patient care and research, our veterans’ respiratory health can now be optimized, and future risks can be mitigated.
Dr. Haynes is Fellow, Pulmonary and Critical Care Medicine, Walter Reed National Military Medical Center, Assistant Professor of Medicine, Uniformed Services University. Dr. Nations is Pulmonary and Critical Care Medicine, Deputy Chief of Staff for Operations, Washington DC VA Medical Center, Associate Professor of Medicine, Uniformed Services University.
References
1. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. Preprint. Posted online October 22, 2009. PMID: 19850627. doi: 10.1093/aje/kwp287
2. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. Erratum in: N Engl J Med. 2011;365(18):1749. PMID: 21774710; PMCID: PMC3296566. doi: 10.1056/NEJMoa1101388
3. Morris MJ, Dodson DW, Lucero PF, et al. Study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE). Am J Respir Crit Care Med. 2014;190(1):77-84. PMID: 24922562. doi: 10.1164/rccm.201402-0372OC
4. Morris MJ, Walter RJ, McCann ET, et al. Clinical evaluation of deployed military personnel with chronic respiratory symptoms: study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE) III. Chest. 2020;157(6):1559-1567. Preprint. Posted online February 1, 2020. PMID: 32017933. doi: 10.1016/j.chest.2020.01.024
5. Morris MJ, Skabelund AJ, Rawlins FA 3rd, Gallup RA, Aden JK, Holley AB. Study of active duty military personnel for environmental deployment exposures: pre- and post-deployment spirometry (STAMPEDE II). Respir Care. 2019;64(5):536-544. Preprint. Posted online January 8, 2019.PMID: 30622173. doi: 10.4187/respcare.06396
6. Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. https://doi.org/10.17226/13209
7. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. https://doi.org/10.17226/25837
8. Falvo MJ, Sotolongo AM, Osterholzer JJ, et al. Consensus statements on deployment-related respiratory disease, inclusive of constrictive bronchiolitis: a modified Delphi study. Chest. 2023;163(3):599-609. Preprint. Posted November 4, 2022. PMID: 36343686; PMCID: PMC10154857. doi: 10.1016/j.chest.2022.10.031
Military service is a hazard-ridden profession. It’s easy to recognize the direct dangers from warfighting, such as gunfire and explosions, but the risks from environmental, chemical, and other occupational exposures can be harder to see.
Combustion-based waste management systems, otherwise known as “burn pits,” were used in deployed environments by the US military from the 1990s to the early 2010s. These burn pits were commonly used to eliminate plastics, electronics, munitions, metals, wood, chemicals, and even human waste. At the height of the recent conflicts in Afghanistan, Iraq, and other southwest Asia locations, more than 70% of military installations employed at least one, and nearly 4 million service members were exposed to some degree to their emissions.
Reports of burn pits being related to organic disease have garnered widespread media attention. Initially, this came through anecdotal reports of post-deployment respiratory symptoms. Over time, the conditions attributed to burn pits expanded to include newly diagnosed respiratory diseases and malignancies.
Ultimately, Congress passed the 2022 Promise to Address Comprehensive Toxins (PACT) Act, presumptively linking more than 20 diagnoses to burn pits. The PACT Act provides countless veterans access to low-cost or free medical care for their respective conditions.
What do we know about burn pits and deployment-related respiratory disease?
Data from the Millennium Cohort Study noted an approximately 40% increase in respiratory symptoms among individuals returning from deployment but no increase in the frequency of diagnosed respiratory diseases.1 This study and others definitively established a temporal relationship between deployment and respiratory symptoms. Soon after, a retrospective, observational study of service members with post-deployment respiratory symptoms found a high prevalence of constrictive bronchiolitis (CB) identified by lung biopsy.2 Patients in this group reported exposure to burn pits and a sulfur mine fire in the Mosul area while deployed. Most had normal imaging and pulmonary function testing before biopsy, confounding the clinical significance of the CB finding. The publication of this report led to increased investigation of respiratory function during and after deployment.
In a series of prospective studies that included full pulmonary function testing, impulse oscillometry, cardiopulmonary exercise testing, bronchoscopy, and, occasionally, lung biopsy to evaluate post-deployment dyspnea, only a small minority received a diagnosis of clinically significant lung disease.3,4 Additionally, when comparing spirometry and impulse oscillometry results from before and after deployment, no decline in lung function was observed in a population of service members reporting regular burn pit exposure.5 These studies suggest that at the population level, deployment does not lead to abnormalities in the structure and function of the respiratory system.
The National Academies of Sciences published two separate reviews of burn pit exposure and outcomes in 2011 and 2020.6,7 They found insufficient evidence to support a causal relationship between burn pit exposure and pulmonary disease. They highlighted studies on the composition of emissions from the area surrounding the largest military burn pit in Iraq. Levels of particulate matter, volatile organic compounds, and polycyclic aromatic hydrocarbons were elevated when compared with those of a typical American city but were similar to the pollution levels seen in the region at the time. Given these findings, they suggested ambient air pollution may have contributed more to clinically significant disease than burn pit emissions.
How do we interpret this mixed data?
At the population level, we have yet to find conclusive data directly linking burn pit exposure to the development of any respiratory disease. Does this mean that burn pits are not harmful?
Not necessarily. Research on outcomes related to burn pit exposure is challenging given the heterogeneity in exposure volume. Much of the research is retrospective and subject to recall bias. Relationships may be distorted, and the precision of reported symptoms and exposure levels is altered. Given these challenges, it’s unsurprising that evidence of causality has yet to be proven. In addition, some portion of service members has been diagnosed with respiratory disease that could be related to burn pit exposure.
What is now indisputable is that deployment to southwest Asia leads to an increase in respiratory complaints. Whether veteran respiratory symptoms are due to burn pits, ambient pollution, environmental particulate matter, or dust storms is less clinically relevant. These symptoms require attention, investigation, and management.
What does this mean for the future medical care of service members and veterans?
Many veterans with post-deployment respiratory symptoms undergo extensive evaluations without obtaining a definitive diagnosis. A recent consensus statement on deployment-related respiratory symptoms provides a framework for evaluation in such cases.8 In keeping with that statement, we recommend veterans be referred to centers with expertise in this field, such as the Department of Veterans Affairs (VA) or military health centers, when deployment-related respiratory symptoms are reported. When the evaluation does not lead to a treatable diagnosis, these centers can provide multidisciplinary care to address the symptoms of dyspnea, cough, fatigue, and exercise intolerance to improve functional status.
Despite uncertainty in the evidence or challenges in diagnosis, both the Department of Defense (DoD) and VA remain fully committed to addressing the health concerns of service members and veterans. Notably, the VA has already screened more than 5 million veterans for toxic military exposures in accordance with the PACT Act and is providing ongoing screening and care for veterans with post-deployment respiratory symptoms. Furthermore, the DoD and VA have dedicated large portions of their research budgets to investigating the impacts of exposures during military service and optimizing the care of those with respiratory symptoms. With these commitments to patient care and research, our veterans’ respiratory health can now be optimized, and future risks can be mitigated.
Dr. Haynes is Fellow, Pulmonary and Critical Care Medicine, Walter Reed National Military Medical Center, Assistant Professor of Medicine, Uniformed Services University. Dr. Nations is Pulmonary and Critical Care Medicine, Deputy Chief of Staff for Operations, Washington DC VA Medical Center, Associate Professor of Medicine, Uniformed Services University.
References
1. Smith B, Wong CA, Smith TC, Boyko EJ, Gackstetter GD; Margaret A. K. Ryan for the Millennium Cohort Study Team. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan: a prospective population-based study. Am J Epidemiol. 2009;170(11):1433-1442. Preprint. Posted online October 22, 2009. PMID: 19850627. doi: 10.1093/aje/kwp287
2. King MS, Eisenberg R, Newman JH, et al. Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. N Engl J Med. 2011;365(3):222-230. Erratum in: N Engl J Med. 2011;365(18):1749. PMID: 21774710; PMCID: PMC3296566. doi: 10.1056/NEJMoa1101388
3. Morris MJ, Dodson DW, Lucero PF, et al. Study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE). Am J Respir Crit Care Med. 2014;190(1):77-84. PMID: 24922562. doi: 10.1164/rccm.201402-0372OC
4. Morris MJ, Walter RJ, McCann ET, et al. Clinical evaluation of deployed military personnel with chronic respiratory symptoms: study of active duty military for pulmonary disease related to environmental deployment exposures (STAMPEDE) III. Chest. 2020;157(6):1559-1567. Preprint. Posted online February 1, 2020. PMID: 32017933. doi: 10.1016/j.chest.2020.01.024
5. Morris MJ, Skabelund AJ, Rawlins FA 3rd, Gallup RA, Aden JK, Holley AB. Study of active duty military personnel for environmental deployment exposures: pre- and post-deployment spirometry (STAMPEDE II). Respir Care. 2019;64(5):536-544. Preprint. Posted online January 8, 2019.PMID: 30622173. doi: 10.4187/respcare.06396
6. Institute of Medicine. Long-Term Health Consequences of Exposure to Burn Pits in Iraq and Afghanistan. The National Academies Press; 2011. https://doi.org/10.17226/13209
7. National Academies of Sciences, Engineering, and Medicine. Respiratory Health Effects of Airborne Hazards Exposures in the Southwest Asia Theater of Military Operations. The National Academies Press; 2020. https://doi.org/10.17226/25837
8. Falvo MJ, Sotolongo AM, Osterholzer JJ, et al. Consensus statements on deployment-related respiratory disease, inclusive of constrictive bronchiolitis: a modified Delphi study. Chest. 2023;163(3):599-609. Preprint. Posted November 4, 2022. PMID: 36343686; PMCID: PMC10154857. doi: 10.1016/j.chest.2022.10.031
Hospital-onset sepsis: Why the brouhaha?
A 47-year-old woman with a history of cirrhosis is admitted with an acute kidney injury and altered mental status. On the initial workup, there are no signs of infection, and dehydration is determined to be the cause of the kidney injury. There are signs of improvement in the kidney injury with hydration. On hospital day 3, the patient develops a fever (101.9 o F) with accompanying leukocytosis to 14,000. Concerned for infection, the team starts empiric broad spectrum antibiotics for presumed spontaneous bacterial peritonitis. The next day (hospital day 4), a rapid response evaluation is activated as the patient is demonstrating increasing confusion, hypotension with a systolic blood pressure of 70 mm Hg, and elevated lactic acid. The patient receives 1 L of normal saline and transfers to the ICU. The new critical care fellow, who has just read up on sepsis early management bundles, and specifically the Severe Sepsis and Septic Shock Management Bundle (SEP-1), is reviewing the chart and notices a history of multidrug-resistant organisms in her urine cultures from an admission 2 months ago. They ask of the transferring team, “When was time zero, and was the 3-hour bundle completed?”
1 The excessive cost, both of human life and monetary, has led to the commitment of significant resources to sepsis care. Improved recognition and timely intervention for sepsis have led to noteworthy improvement in mortality. Most of this effort has been directed toward patients with sepsis diagnosed in the emergency department (ED) who are presenting with community-onset sepsis (COS). A new entity, called hospital-onset sepsis (HOS), has been described recently, defined by the Centers for Disease Control and Prevention (CDC) as both infection and organ dysfunction developing more than 48 hours after hospital admission.2

A systematic review of 51 studies found approximately 23.6% of all sepsis cases are HOS. The proportion of HOS is even higher (more than 45%) in patients admitted to the ICU with sepsis.3 The outcome for this group remains comparatively poor. The hospital mortality among patients with HOS is 35%, which increases to 52% with progression to septic shock compared with 25% with COS.3 Even after adjusting for baseline factors that make one prone to developing infection in the hospital, a patient developing HOS has three-times a higher risk of dying compared with a patient who never developed sepsis and two-times a higher risk of dying compared with patients with COS.4 Furthermore, HOS utilizes more resources with significantly longer ICU and hospital stays and has five-times the hospital cost compared with COS.4
The two most crucial factors in improving sepsis outcomes, as identified by the Surviving Sepsis Campaign guidelines, are: 1) prompt identification and treatment within the first few hours of onset and 2) regular reevaluation of the patient’s response to treatment.

Prompt identification
Diagnosing sepsis in the patient who is hospitalized is challenging. Patients admitted to the hospital often have competing comorbidities, have existing organ failure, or are in a postoperative/intervention state that clouds the application and interpretation of vital sign triggers customarily used to identify sepsis. The positive predictive value for all existing sepsis definitions and diagnostic criteria is dismally low. 5 And while automated electronic sepsis alerts may improve processes of care, they still have poor positive predictive value and have not impacted patient-centered outcomes (mortality or length of stay). Furthermore, the causative microorganisms often associated with hospital-acquired infections are complex, are drug-resistant, and can have courses which further delay identification. Finally, cognitive errors, such as anchoring biases or premature diagnosis closure, can contribute to provider-level identification delays that are only further exacerbated by system issues, such as capacity constraints, staffing issues, and differing paces between wards that tend to impede time-sensitive evaluations and interventions. 4,6,7
Management
The SEP-1 core measure uses a framework of early recognition of infection and completion of the sepsis bundles in a timely manner to improve outcomes. Patients with HOS are less likely than those with COS to receive Centers for Medicare & Medicaid Services SEP-1-compliant care, including timely blood culture collection, initial and repeat lactate testing, and fluid resuscitation.8 The Surviving Sepsis Campaign has explored barriers to managing HOS. Among caregivers, these include delay in recognition, poor communication regarding change in patient status, not prioritizing treatment for sepsis, failure to measure lactate, delayed or no antimicrobial administration, and inadequate fluid resuscitation. In one study, the adherence to SEP-1 for HOS was reported at 13% compared with 39.9% in COS. The differences in initial sepsis management included timing of antimicrobials and fluid resuscitation, which accounted for 23% of observed greater mortality risk among patients with HOS compared with COS.6,8 It remains unclear how these recommendations should be applied and whether some of these recommendations confer the same benefits for patients with HOS as for those with COS. For example, administration of fluids conferred no additional benefit to patients with HOS, while rapid antimicrobial administration was shown to be associated with improved mortality in patients with HOS. Although, the optimal timing for treatment initiation and microbial coverage has not been established.

The path forward
Effective HOS management requires both individual and systematic approaches. How clinicians identify a patient with sepsis must be context-dependent. Although standard criteria exist for defining sepsis, the approach to a patient presenting to the ED from home should differ from that of a patient who has been hospitalized for several days, is postoperative, or is in the ICU on multiple forms of life support. Clinical medicine is context-dependent, and the same principles apply to sepsis management. To address the diagnostic uncertainty of the syndrome, providers must remain vigilant and maintain a clinical “iterative urgency” in diagnosing and managing sepsis. While machine learning algorithms have potential, they still rely on human intervention and interaction to navigate the complexities of HOS diagnosis.
At the system level, survival from sepsis is determined by the speed with which complex medical care is delivered and the effectiveness with which resources and personnel are mobilized and coordinated. The Hospital Sepsis Program Core Elements, released by the CDC, serves as an initial playbook to aid hospitals in establishing comprehensive sepsis improvement programs.
A second invaluable resource for hospitals in sepsis management is the rapid response team (RRT). Studies have shown that resolute RRTs can enhance patient outcomes and compliance with sepsis bundles; though, the composition and scope of these teams are crucial to their effectiveness. Responding to in-hospital emergencies and urgencies without conflicting responsibilities is an essential feature of a successful RRT. Often, they are familiar with bundles, protocols, and documentation, and members of these teams can offer clinical and/or technical expertise as well as support active participation and reengagement with bedside staff, which fosters trust and collaboration. This partnership is key, as these interactions instill a common mission and foster a culture of sepsis improvement that is required to achieve sustained success and improved patient outcomes.
Dr. Dugar is Director, Point-of-Care Ultrasound, Department of Critical Care, Respiratory Institute, Assistant Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH. Dr. Jayaprakash is Associate Medical Director, Quality, Emergency Medicine, Physician Lead, Henry Ford Health Sepsis Program. Dr. Reilkoff is Executive Medical Director of Critical Care, M Health Fairview Intensive Care Units, Director of Acting Internship in Critical Care, University of Minnesota Medical School, Associate Professor of Medicine and Surgery, University of Minnesota. Dr. Duggal is Vice-Chair, Department of Critical Care, Respiratory Institute, Director, Critical Care Clinical Research, Associate Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
2. Ginestra JC, Coz Yataco AO, Dugar SP, Dettmer MR. Hospital-onset sepsis warrants expanded investigation and consideration as a unique clinical entity. Chest. 2024;S0012-3692(24):00039-4.
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551.
4. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169-1176.
5. Wong A, Otles E, Donnelly JP, et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern Med. 2021;181(8):1065-1070.
6. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707-716.
7. Baghdadi JD, Wong MD, Uslan DZ, et al. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: a multicenter retrospective cohort study. J Gen Intern Med. 2020;35(4):1153-1160.
8. Basheer A. Patients with hospital-onset sepsis are less likely to receive sepsis bundle care than those with community-onset sepsis. Evid Based Nurs. 2021;24(3):99.
A 47-year-old woman with a history of cirrhosis is admitted with an acute kidney injury and altered mental status. On the initial workup, there are no signs of infection, and dehydration is determined to be the cause of the kidney injury. There are signs of improvement in the kidney injury with hydration. On hospital day 3, the patient develops a fever (101.9 o F) with accompanying leukocytosis to 14,000. Concerned for infection, the team starts empiric broad spectrum antibiotics for presumed spontaneous bacterial peritonitis. The next day (hospital day 4), a rapid response evaluation is activated as the patient is demonstrating increasing confusion, hypotension with a systolic blood pressure of 70 mm Hg, and elevated lactic acid. The patient receives 1 L of normal saline and transfers to the ICU. The new critical care fellow, who has just read up on sepsis early management bundles, and specifically the Severe Sepsis and Septic Shock Management Bundle (SEP-1), is reviewing the chart and notices a history of multidrug-resistant organisms in her urine cultures from an admission 2 months ago. They ask of the transferring team, “When was time zero, and was the 3-hour bundle completed?”
1 The excessive cost, both of human life and monetary, has led to the commitment of significant resources to sepsis care. Improved recognition and timely intervention for sepsis have led to noteworthy improvement in mortality. Most of this effort has been directed toward patients with sepsis diagnosed in the emergency department (ED) who are presenting with community-onset sepsis (COS). A new entity, called hospital-onset sepsis (HOS), has been described recently, defined by the Centers for Disease Control and Prevention (CDC) as both infection and organ dysfunction developing more than 48 hours after hospital admission.2
A systematic review of 51 studies found approximately 23.6% of all sepsis cases are HOS. The proportion of HOS is even higher (more than 45%) in patients admitted to the ICU with sepsis.3 The outcome for this group remains comparatively poor. The hospital mortality among patients with HOS is 35%, which increases to 52% with progression to septic shock compared with 25% with COS.3 Even after adjusting for baseline factors that make one prone to developing infection in the hospital, a patient developing HOS has three-times a higher risk of dying compared with a patient who never developed sepsis and two-times a higher risk of dying compared with patients with COS.4 Furthermore, HOS utilizes more resources with significantly longer ICU and hospital stays and has five-times the hospital cost compared with COS.4
The two most crucial factors in improving sepsis outcomes, as identified by the Surviving Sepsis Campaign guidelines, are: 1) prompt identification and treatment within the first few hours of onset and 2) regular reevaluation of the patient’s response to treatment.
Prompt identification
Diagnosing sepsis in the patient who is hospitalized is challenging. Patients admitted to the hospital often have competing comorbidities, have existing organ failure, or are in a postoperative/intervention state that clouds the application and interpretation of vital sign triggers customarily used to identify sepsis. The positive predictive value for all existing sepsis definitions and diagnostic criteria is dismally low. 5 And while automated electronic sepsis alerts may improve processes of care, they still have poor positive predictive value and have not impacted patient-centered outcomes (mortality or length of stay). Furthermore, the causative microorganisms often associated with hospital-acquired infections are complex, are drug-resistant, and can have courses which further delay identification. Finally, cognitive errors, such as anchoring biases or premature diagnosis closure, can contribute to provider-level identification delays that are only further exacerbated by system issues, such as capacity constraints, staffing issues, and differing paces between wards that tend to impede time-sensitive evaluations and interventions. 4,6,7
Management
The SEP-1 core measure uses a framework of early recognition of infection and completion of the sepsis bundles in a timely manner to improve outcomes. Patients with HOS are less likely than those with COS to receive Centers for Medicare & Medicaid Services SEP-1-compliant care, including timely blood culture collection, initial and repeat lactate testing, and fluid resuscitation.8 The Surviving Sepsis Campaign has explored barriers to managing HOS. Among caregivers, these include delay in recognition, poor communication regarding change in patient status, not prioritizing treatment for sepsis, failure to measure lactate, delayed or no antimicrobial administration, and inadequate fluid resuscitation. In one study, the adherence to SEP-1 for HOS was reported at 13% compared with 39.9% in COS. The differences in initial sepsis management included timing of antimicrobials and fluid resuscitation, which accounted for 23% of observed greater mortality risk among patients with HOS compared with COS.6,8 It remains unclear how these recommendations should be applied and whether some of these recommendations confer the same benefits for patients with HOS as for those with COS. For example, administration of fluids conferred no additional benefit to patients with HOS, while rapid antimicrobial administration was shown to be associated with improved mortality in patients with HOS. Although, the optimal timing for treatment initiation and microbial coverage has not been established.
The path forward
Effective HOS management requires both individual and systematic approaches. How clinicians identify a patient with sepsis must be context-dependent. Although standard criteria exist for defining sepsis, the approach to a patient presenting to the ED from home should differ from that of a patient who has been hospitalized for several days, is postoperative, or is in the ICU on multiple forms of life support. Clinical medicine is context-dependent, and the same principles apply to sepsis management. To address the diagnostic uncertainty of the syndrome, providers must remain vigilant and maintain a clinical “iterative urgency” in diagnosing and managing sepsis. While machine learning algorithms have potential, they still rely on human intervention and interaction to navigate the complexities of HOS diagnosis.
At the system level, survival from sepsis is determined by the speed with which complex medical care is delivered and the effectiveness with which resources and personnel are mobilized and coordinated. The Hospital Sepsis Program Core Elements, released by the CDC, serves as an initial playbook to aid hospitals in establishing comprehensive sepsis improvement programs.
A second invaluable resource for hospitals in sepsis management is the rapid response team (RRT). Studies have shown that resolute RRTs can enhance patient outcomes and compliance with sepsis bundles; though, the composition and scope of these teams are crucial to their effectiveness. Responding to in-hospital emergencies and urgencies without conflicting responsibilities is an essential feature of a successful RRT. Often, they are familiar with bundles, protocols, and documentation, and members of these teams can offer clinical and/or technical expertise as well as support active participation and reengagement with bedside staff, which fosters trust and collaboration. This partnership is key, as these interactions instill a common mission and foster a culture of sepsis improvement that is required to achieve sustained success and improved patient outcomes.
Dr. Dugar is Director, Point-of-Care Ultrasound, Department of Critical Care, Respiratory Institute, Assistant Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH. Dr. Jayaprakash is Associate Medical Director, Quality, Emergency Medicine, Physician Lead, Henry Ford Health Sepsis Program. Dr. Reilkoff is Executive Medical Director of Critical Care, M Health Fairview Intensive Care Units, Director of Acting Internship in Critical Care, University of Minnesota Medical School, Associate Professor of Medicine and Surgery, University of Minnesota. Dr. Duggal is Vice-Chair, Department of Critical Care, Respiratory Institute, Director, Critical Care Clinical Research, Associate Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
2. Ginestra JC, Coz Yataco AO, Dugar SP, Dettmer MR. Hospital-onset sepsis warrants expanded investigation and consideration as a unique clinical entity. Chest. 2024;S0012-3692(24):00039-4.
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551.
4. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169-1176.
5. Wong A, Otles E, Donnelly JP, et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern Med. 2021;181(8):1065-1070.
6. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707-716.
7. Baghdadi JD, Wong MD, Uslan DZ, et al. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: a multicenter retrospective cohort study. J Gen Intern Med. 2020;35(4):1153-1160.
8. Basheer A. Patients with hospital-onset sepsis are less likely to receive sepsis bundle care than those with community-onset sepsis. Evid Based Nurs. 2021;24(3):99.
A 47-year-old woman with a history of cirrhosis is admitted with an acute kidney injury and altered mental status. On the initial workup, there are no signs of infection, and dehydration is determined to be the cause of the kidney injury. There are signs of improvement in the kidney injury with hydration. On hospital day 3, the patient develops a fever (101.9 o F) with accompanying leukocytosis to 14,000. Concerned for infection, the team starts empiric broad spectrum antibiotics for presumed spontaneous bacterial peritonitis. The next day (hospital day 4), a rapid response evaluation is activated as the patient is demonstrating increasing confusion, hypotension with a systolic blood pressure of 70 mm Hg, and elevated lactic acid. The patient receives 1 L of normal saline and transfers to the ICU. The new critical care fellow, who has just read up on sepsis early management bundles, and specifically the Severe Sepsis and Septic Shock Management Bundle (SEP-1), is reviewing the chart and notices a history of multidrug-resistant organisms in her urine cultures from an admission 2 months ago. They ask of the transferring team, “When was time zero, and was the 3-hour bundle completed?”
1 The excessive cost, both of human life and monetary, has led to the commitment of significant resources to sepsis care. Improved recognition and timely intervention for sepsis have led to noteworthy improvement in mortality. Most of this effort has been directed toward patients with sepsis diagnosed in the emergency department (ED) who are presenting with community-onset sepsis (COS). A new entity, called hospital-onset sepsis (HOS), has been described recently, defined by the Centers for Disease Control and Prevention (CDC) as both infection and organ dysfunction developing more than 48 hours after hospital admission.2
A systematic review of 51 studies found approximately 23.6% of all sepsis cases are HOS. The proportion of HOS is even higher (more than 45%) in patients admitted to the ICU with sepsis.3 The outcome for this group remains comparatively poor. The hospital mortality among patients with HOS is 35%, which increases to 52% with progression to septic shock compared with 25% with COS.3 Even after adjusting for baseline factors that make one prone to developing infection in the hospital, a patient developing HOS has three-times a higher risk of dying compared with a patient who never developed sepsis and two-times a higher risk of dying compared with patients with COS.4 Furthermore, HOS utilizes more resources with significantly longer ICU and hospital stays and has five-times the hospital cost compared with COS.4
The two most crucial factors in improving sepsis outcomes, as identified by the Surviving Sepsis Campaign guidelines, are: 1) prompt identification and treatment within the first few hours of onset and 2) regular reevaluation of the patient’s response to treatment.
Prompt identification
Diagnosing sepsis in the patient who is hospitalized is challenging. Patients admitted to the hospital often have competing comorbidities, have existing organ failure, or are in a postoperative/intervention state that clouds the application and interpretation of vital sign triggers customarily used to identify sepsis. The positive predictive value for all existing sepsis definitions and diagnostic criteria is dismally low. 5 And while automated electronic sepsis alerts may improve processes of care, they still have poor positive predictive value and have not impacted patient-centered outcomes (mortality or length of stay). Furthermore, the causative microorganisms often associated with hospital-acquired infections are complex, are drug-resistant, and can have courses which further delay identification. Finally, cognitive errors, such as anchoring biases or premature diagnosis closure, can contribute to provider-level identification delays that are only further exacerbated by system issues, such as capacity constraints, staffing issues, and differing paces between wards that tend to impede time-sensitive evaluations and interventions. 4,6,7
Management
The SEP-1 core measure uses a framework of early recognition of infection and completion of the sepsis bundles in a timely manner to improve outcomes. Patients with HOS are less likely than those with COS to receive Centers for Medicare & Medicaid Services SEP-1-compliant care, including timely blood culture collection, initial and repeat lactate testing, and fluid resuscitation.8 The Surviving Sepsis Campaign has explored barriers to managing HOS. Among caregivers, these include delay in recognition, poor communication regarding change in patient status, not prioritizing treatment for sepsis, failure to measure lactate, delayed or no antimicrobial administration, and inadequate fluid resuscitation. In one study, the adherence to SEP-1 for HOS was reported at 13% compared with 39.9% in COS. The differences in initial sepsis management included timing of antimicrobials and fluid resuscitation, which accounted for 23% of observed greater mortality risk among patients with HOS compared with COS.6,8 It remains unclear how these recommendations should be applied and whether some of these recommendations confer the same benefits for patients with HOS as for those with COS. For example, administration of fluids conferred no additional benefit to patients with HOS, while rapid antimicrobial administration was shown to be associated with improved mortality in patients with HOS. Although, the optimal timing for treatment initiation and microbial coverage has not been established.
The path forward
Effective HOS management requires both individual and systematic approaches. How clinicians identify a patient with sepsis must be context-dependent. Although standard criteria exist for defining sepsis, the approach to a patient presenting to the ED from home should differ from that of a patient who has been hospitalized for several days, is postoperative, or is in the ICU on multiple forms of life support. Clinical medicine is context-dependent, and the same principles apply to sepsis management. To address the diagnostic uncertainty of the syndrome, providers must remain vigilant and maintain a clinical “iterative urgency” in diagnosing and managing sepsis. While machine learning algorithms have potential, they still rely on human intervention and interaction to navigate the complexities of HOS diagnosis.
At the system level, survival from sepsis is determined by the speed with which complex medical care is delivered and the effectiveness with which resources and personnel are mobilized and coordinated. The Hospital Sepsis Program Core Elements, released by the CDC, serves as an initial playbook to aid hospitals in establishing comprehensive sepsis improvement programs.
A second invaluable resource for hospitals in sepsis management is the rapid response team (RRT). Studies have shown that resolute RRTs can enhance patient outcomes and compliance with sepsis bundles; though, the composition and scope of these teams are crucial to their effectiveness. Responding to in-hospital emergencies and urgencies without conflicting responsibilities is an essential feature of a successful RRT. Often, they are familiar with bundles, protocols, and documentation, and members of these teams can offer clinical and/or technical expertise as well as support active participation and reengagement with bedside staff, which fosters trust and collaboration. This partnership is key, as these interactions instill a common mission and foster a culture of sepsis improvement that is required to achieve sustained success and improved patient outcomes.
Dr. Dugar is Director, Point-of-Care Ultrasound, Department of Critical Care, Respiratory Institute, Assistant Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH. Dr. Jayaprakash is Associate Medical Director, Quality, Emergency Medicine, Physician Lead, Henry Ford Health Sepsis Program. Dr. Reilkoff is Executive Medical Director of Critical Care, M Health Fairview Intensive Care Units, Director of Acting Internship in Critical Care, University of Minnesota Medical School, Associate Professor of Medicine and Surgery, University of Minnesota. Dr. Duggal is Vice-Chair, Department of Critical Care, Respiratory Institute, Director, Critical Care Clinical Research, Associate Professor, Cleveland Clinic Lerner College of Medicine, Cleveland, OH
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
2. Ginestra JC, Coz Yataco AO, Dugar SP, Dettmer MR. Hospital-onset sepsis warrants expanded investigation and consideration as a unique clinical entity. Chest. 2024;S0012-3692(24):00039-4.
3. Markwart R, Saito H, Harder T, et al. Epidemiology and burden of sepsis acquired in hospitals and intensive care units: a systematic review and meta-analysis. Intensive Care Med. 2020;46(8):1536-1551.
4. Rhee C, Wang R, Zhang Z, et al. Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med. 2019;47(9):1169-1176.
5. Wong A, Otles E, Donnelly JP, et al. External validation of a widely implemented proprietary sepsis prediction model in hospitalized patients. JAMA Intern Med. 2021;181(8):1065-1070.
6. Baghdadi JD, Brook RH, Uslan DZ, et al. Association of a care bundle for early sepsis management with mortality among patients with hospital-onset or community-onset sepsis. JAMA Intern Med. 2020;180(5):707-716.
7. Baghdadi JD, Wong MD, Uslan DZ, et al. Adherence to the SEP-1 sepsis bundle in hospital-onset v. community-onset sepsis: a multicenter retrospective cohort study. J Gen Intern Med. 2020;35(4):1153-1160.
8. Basheer A. Patients with hospital-onset sepsis are less likely to receive sepsis bundle care than those with community-onset sepsis. Evid Based Nurs. 2021;24(3):99.
Home ventilation consult
Specialist input on a sudden shift in device availability
Philips Respironics released a public statement on January 25, 2024, that would dramatically change the landscape of home mechanical ventilation and sleep-disordered breathing management in the United States. The company announced that, effective immediately in the US and US territories, Philips Respironics would stop production and sale of all hospital and home mechanical ventilation products, home and hospital ventilation devices, and oxygen concentrators.
There are many unknowns and uncertainties about how to proceed with care for patients requiring these devices. So we gathered an expert panel of clinicians from CHEST’s Home-Based Mechanical Ventilation and Neuromuscular Section within the Sleep Medicine Network to explain the current situation and offer suggestions on moving forward in caring for these patients.
Why is this happening?

John M. Coleman III, MD, FCCP: To understand the current Philips Respironics announcement, we must go back to June 2021. At that time, Philips recalled certain home mechanical ventilators, CPAP machines, and BiPAP machines due to potential health risks related to breakdown of the polyester-based polyurethane (PE-PUR) foam placed in these devices for noise reduction. Small and microscopic particles of this foam were at risk for being inhaled or ingested by patients using these devices. It was suspected that inhalation of these particles could potentially result in temporary or permanent injury. Machines in hot temperatures or using ozone cleaning were at increased risk. The US Food and Drug Administration (FDA) issued a class 1 recall, defined as “a situation in which there is reasonable probability that the use of or exposure to a violative product will cause serious adverse health consequences or death.”
In the months following the initial recall, there were additional recalls of both in-hospital and home ventilators related to the potential of these foam particles to move and block the air path, reducing airflow and causing the device to alarm.
Over the next few years, tens of thousands of medical device reports were filed about PE-PUR foam-related injuries, with some cases resulting in death. At this time, the Department of Justice began collaborating with the FDA on a consent decree. There were ongoing recalls of the CoughAssist T70 device, as well as the newest generation of Philips Respironics home ventilators, the Trilogy EVO.
Ultimately, after years of ongoing recalls and reports of numerous deaths and injuries, with multiple class action lawsuits, the consent decree was finalized. Philips Respironics agreed to stop production of all respiratory-related products in the US and US territories.
What devices does this apply to?

Jason Ackrivo, MD: This notice affects the devices shown in Table 1. All sales and device shipments have been discontinued as of January 25, 2024. Philips Respironics will continue to service the devices, subject to part availability, up to 5 years after sales discontinuation. However, Philips Respironics will continue to sell consumables and accessories, including masks.
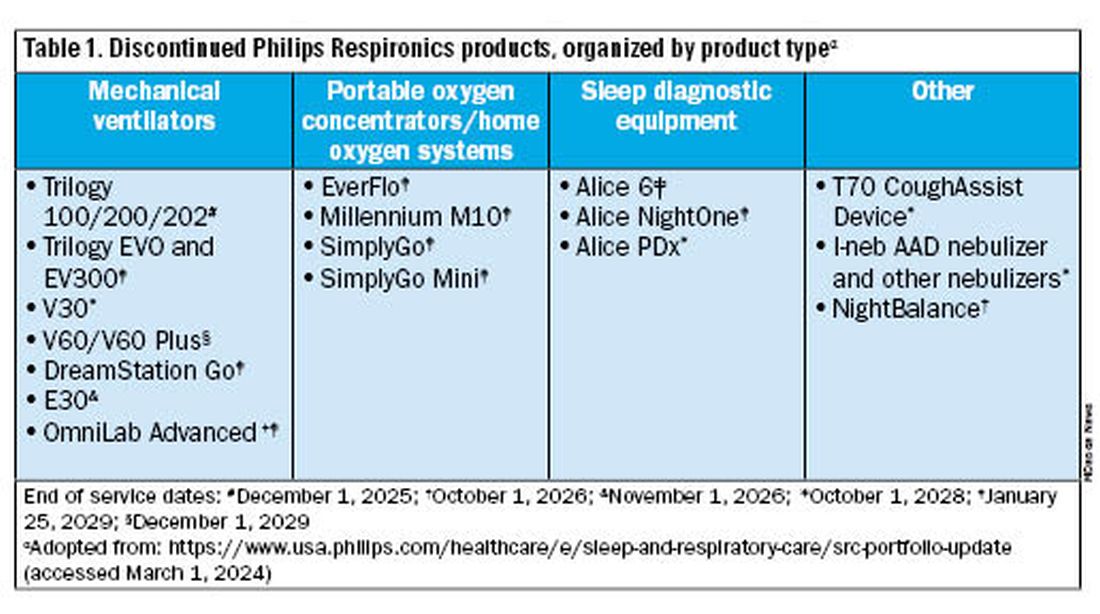
What are my options for home mechanical ventilators?
Bethany L. Lussier, MD, FCCP: In the US, alternative approved home mechanical ventilator (HMV) devices include Astral by ResMed, Vivo 45 and Vivo 65 by Breas, and VOCSN by Ventec. Additional options made available through emergency use authorization by the FDA between 2020 and 2022 included Luisa by Löwenstein Medical, the V+ by Ventec, and Life2000 by Baxter. Many of us expedite disposition from the hospital by prescribing HMVs rather than respiratory assist devices (RADs) because it is easier to meet qualifying criteria for insurance. In efforts to promote just allocation of resources, now might be the ideal time to reconsider higher utilization of RADs over HMVs. Reasonable RAD candidates are those who do not need autotitration of EPAP, dual mode therapy, or invasive ventilation. In these cases, the qualifying criteria and patient needs may be met with a RAD capable of VAPS or BPAP-ST mode.
How are these alternative devices similar to and different from the Trilogy EVO?
Dr. Ackrivo:All these devices are portable ventilators that can deliver noninvasive or invasive ventilation. They have internal batteries for enabling portability. They offer multiple programmable presets and mouthpiece ventilation, and some offer both oxygenation and CO2 monitoring (both TcCO2 and EtCO2).
All alternative portable ventilators include a proprietary ventilation mode analogous to the Trilogy AVAPS algorithm (Table 2). The ResMed Astral has a safety tidal volume feature that targets a minimum tidal volume in PS, S/T, or P(A)C modes. The ResMed iVAPS algorithm adjusts inspiratory pressure and respiratory rate to target an alveolar ventilation based on patient-entered height. The Breas Vivo can target a tidal volume (TgV) in either PSV or PCV mode.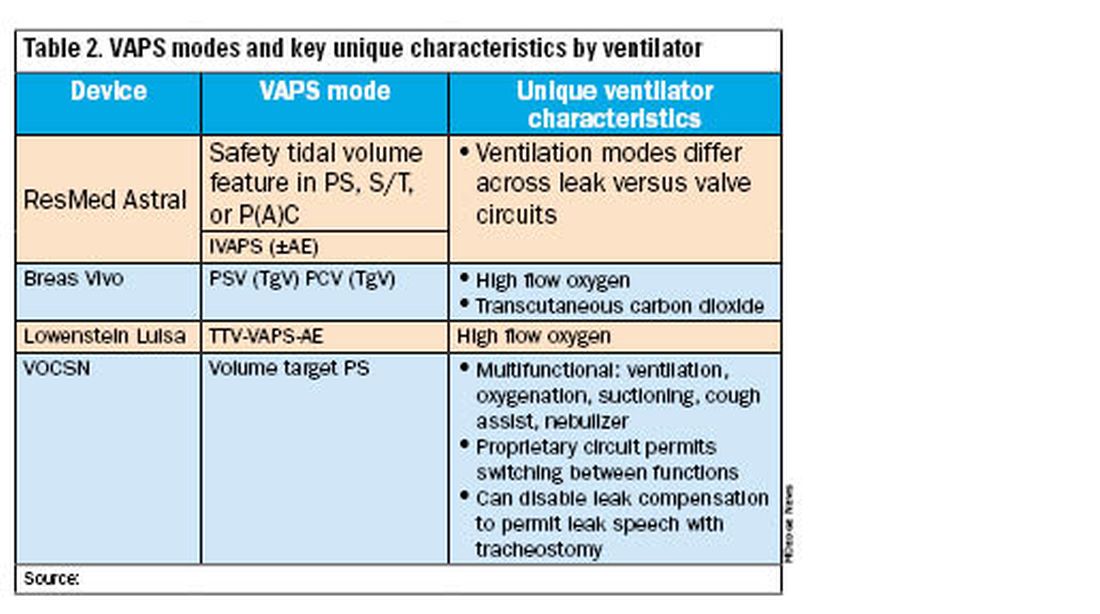
Unique ventilator characteristics are shown in Table 2. ResMed Astral mode options will differ between leak (passive) or valve (active) circuits. Both the Breas Vivo and Löwenstein Luisa enable high-flow oxygen delivery. Only the Breas Vivo enables connecting to a transcutaneous carbon dioxide monitor. The VOCSN name is an acronym for its multifunctional capabilities: ventilation, oxygenation, cough assist, suction, and nebulizer treatments. Lastly, the VOCSN can disable leak compensation, which may be advantageous for enabling leak speech with a tracheostomy.
I just provided my patient with a Trilogy EVO. Do I need to change this immediately?
Dr. Coleman: No, but you should start conversations with your patient/caregiving support and with your durable medical equipment (DME) provider about alternative options. The ripple effects of the Philips Respironics recall will be ongoing for years. The silver lining of this situation is that there are numerous HMV options on the market currently. It is important to review the differences between these new devices and consider what will work best for your patient and your practice. In addition, it is critical that your DME provider is familiar with these new devices, both for support and education, and is taking steps to make alternate devices available. We anticipate a push in coming months to switch patients off Trilogy EVO, so it important to get this process started.
For patients not interested in switching just yet, Philips Respironics will continue to service and offer supplies for these devices for up to 5 years, depending on part availability (Table 1). Refer to the Philips Respironics Sleep & Respiratory Product Portfolio Changes website for the most up-to-date information.
I have a patient on AVAPS, and I must change to iVAPS. What now?
Dr. Lussier: As mentioned previously by Dr. Ackrivo, the ResMed iVAPS algorithm adjusts inspiratory pressure and respiratory rate to target an alveolar ventilation based on patient-entered height. A download from a current VAPS setting can be helpful in defining target ventilation and pressure ranges for a tailored prescription. ResMed has an online iVAPS calculator (resmed.com) to assist in making this switch. Close clinical monitoring with data downloads is recommended to assure desired targets are still achieved.
What will happen to Philips Respironics’ cloud patient data?
Dr. Lussier: Representatives have reported that both providers and DME companies will have continued access to Care Orchestrator going forward. Currently, the logistics of data maintenance and ownership remain unclear, which poses additional questions about global access to patients’ data downloads.
----------
The recent discontinuation of Philips Respironics ventilation devices will induce a dramatic shift in home ventilation options in the US. Clinicians and DME companies should begin familiarizing themselves with alternative ventilators and their unique features. While significant uncertainty exists, we encourage a proactive approach to education and communication to ensure a smooth transition for patients on home ventilation.
John M. Coleman III, MD, FCCP, is Associate Professor, Division of Pulmonary & Critical Care Medicine, Department of Neurology, Northwestern University Feinberg School of Medicine. Bethany L. Lussier, MD, FCCP, is in the Department of Internal Medicine, Division of Pulmonary & Critical Care Medicine, Department of Neurology, Division of Neurocritical Care, UT Southwestern Medical Center. Jason Ackrivo, MD, is Assistant Professor of Medicine and Neurology, and Associate Director, Jay and Randy Fishman Program for Home Assisted Ventilation, Pulmonary, Allergy, and Critical Care Division, Perelman School of Medicine, University of Pennsylvania.
Specialist input on a sudden shift in device availability
Specialist input on a sudden shift in device availability
Philips Respironics released a public statement on January 25, 2024, that would dramatically change the landscape of home mechanical ventilation and sleep-disordered breathing management in the United States. The company announced that, effective immediately in the US and US territories, Philips Respironics would stop production and sale of all hospital and home mechanical ventilation products, home and hospital ventilation devices, and oxygen concentrators.
There are many unknowns and uncertainties about how to proceed with care for patients requiring these devices. So we gathered an expert panel of clinicians from CHEST’s Home-Based Mechanical Ventilation and Neuromuscular Section within the Sleep Medicine Network to explain the current situation and offer suggestions on moving forward in caring for these patients.
Why is this happening?
John M. Coleman III, MD, FCCP: To understand the current Philips Respironics announcement, we must go back to June 2021. At that time, Philips recalled certain home mechanical ventilators, CPAP machines, and BiPAP machines due to potential health risks related to breakdown of the polyester-based polyurethane (PE-PUR) foam placed in these devices for noise reduction. Small and microscopic particles of this foam were at risk for being inhaled or ingested by patients using these devices. It was suspected that inhalation of these particles could potentially result in temporary or permanent injury. Machines in hot temperatures or using ozone cleaning were at increased risk. The US Food and Drug Administration (FDA) issued a class 1 recall, defined as “a situation in which there is reasonable probability that the use of or exposure to a violative product will cause serious adverse health consequences or death.”
In the months following the initial recall, there were additional recalls of both in-hospital and home ventilators related to the potential of these foam particles to move and block the air path, reducing airflow and causing the device to alarm.
Over the next few years, tens of thousands of medical device reports were filed about PE-PUR foam-related injuries, with some cases resulting in death. At this time, the Department of Justice began collaborating with the FDA on a consent decree. There were ongoing recalls of the CoughAssist T70 device, as well as the newest generation of Philips Respironics home ventilators, the Trilogy EVO.
Ultimately, after years of ongoing recalls and reports of numerous deaths and injuries, with multiple class action lawsuits, the consent decree was finalized. Philips Respironics agreed to stop production of all respiratory-related products in the US and US territories.
What devices does this apply to?
Jason Ackrivo, MD: This notice affects the devices shown in Table 1. All sales and device shipments have been discontinued as of January 25, 2024. Philips Respironics will continue to service the devices, subject to part availability, up to 5 years after sales discontinuation. However, Philips Respironics will continue to sell consumables and accessories, including masks.
What are my options for home mechanical ventilators?
Bethany L. Lussier, MD, FCCP: In the US, alternative approved home mechanical ventilator (HMV) devices include Astral by ResMed, Vivo 45 and Vivo 65 by Breas, and VOCSN by Ventec. Additional options made available through emergency use authorization by the FDA between 2020 and 2022 included Luisa by Löwenstein Medical, the V+ by Ventec, and Life2000 by Baxter. Many of us expedite disposition from the hospital by prescribing HMVs rather than respiratory assist devices (RADs) because it is easier to meet qualifying criteria for insurance. In efforts to promote just allocation of resources, now might be the ideal time to reconsider higher utilization of RADs over HMVs. Reasonable RAD candidates are those who do not need autotitration of EPAP, dual mode therapy, or invasive ventilation. In these cases, the qualifying criteria and patient needs may be met with a RAD capable of VAPS or BPAP-ST mode.
How are these alternative devices similar to and different from the Trilogy EVO?
Dr. Ackrivo:All these devices are portable ventilators that can deliver noninvasive or invasive ventilation. They have internal batteries for enabling portability. They offer multiple programmable presets and mouthpiece ventilation, and some offer both oxygenation and CO2 monitoring (both TcCO2 and EtCO2).
All alternative portable ventilators include a proprietary ventilation mode analogous to the Trilogy AVAPS algorithm (Table 2). The ResMed Astral has a safety tidal volume feature that targets a minimum tidal volume in PS, S/T, or P(A)C modes. The ResMed iVAPS algorithm adjusts inspiratory pressure and respiratory rate to target an alveolar ventilation based on patient-entered height. The Breas Vivo can target a tidal volume (TgV) in either PSV or PCV mode.
Unique ventilator characteristics are shown in Table 2. ResMed Astral mode options will differ between leak (passive) or valve (active) circuits. Both the Breas Vivo and Löwenstein Luisa enable high-flow oxygen delivery. Only the Breas Vivo enables connecting to a transcutaneous carbon dioxide monitor. The VOCSN name is an acronym for its multifunctional capabilities: ventilation, oxygenation, cough assist, suction, and nebulizer treatments. Lastly, the VOCSN can disable leak compensation, which may be advantageous for enabling leak speech with a tracheostomy.
I just provided my patient with a Trilogy EVO. Do I need to change this immediately?
Dr. Coleman: No, but you should start conversations with your patient/caregiving support and with your durable medical equipment (DME) provider about alternative options. The ripple effects of the Philips Respironics recall will be ongoing for years. The silver lining of this situation is that there are numerous HMV options on the market currently. It is important to review the differences between these new devices and consider what will work best for your patient and your practice. In addition, it is critical that your DME provider is familiar with these new devices, both for support and education, and is taking steps to make alternate devices available. We anticipate a push in coming months to switch patients off Trilogy EVO, so it important to get this process started.
For patients not interested in switching just yet, Philips Respironics will continue to service and offer supplies for these devices for up to 5 years, depending on part availability (Table 1). Refer to the Philips Respironics Sleep & Respiratory Product Portfolio Changes website for the most up-to-date information.
I have a patient on AVAPS, and I must change to iVAPS. What now?
Dr. Lussier: As mentioned previously by Dr. Ackrivo, the ResMed iVAPS algorithm adjusts inspiratory pressure and respiratory rate to target an alveolar ventilation based on patient-entered height. A download from a current VAPS setting can be helpful in defining target ventilation and pressure ranges for a tailored prescription. ResMed has an online iVAPS calculator (resmed.com) to assist in making this switch. Close clinical monitoring with data downloads is recommended to assure desired targets are still achieved.
What will happen to Philips Respironics’ cloud patient data?
Dr. Lussier: Representatives have reported that both providers and DME companies will have continued access to Care Orchestrator going forward. Currently, the logistics of data maintenance and ownership remain unclear, which poses additional questions about global access to patients’ data downloads.
----------
The recent discontinuation of Philips Respironics ventilation devices will induce a dramatic shift in home ventilation options in the US. Clinicians and DME companies should begin familiarizing themselves with alternative ventilators and their unique features. While significant uncertainty exists, we encourage a proactive approach to education and communication to ensure a smooth transition for patients on home ventilation.
John M. Coleman III, MD, FCCP, is Associate Professor, Division of Pulmonary & Critical Care Medicine, Department of Neurology, Northwestern University Feinberg School of Medicine. Bethany L. Lussier, MD, FCCP, is in the Department of Internal Medicine, Division of Pulmonary & Critical Care Medicine, Department of Neurology, Division of Neurocritical Care, UT Southwestern Medical Center. Jason Ackrivo, MD, is Assistant Professor of Medicine and Neurology, and Associate Director, Jay and Randy Fishman Program for Home Assisted Ventilation, Pulmonary, Allergy, and Critical Care Division, Perelman School of Medicine, University of Pennsylvania.
Philips Respironics released a public statement on January 25, 2024, that would dramatically change the landscape of home mechanical ventilation and sleep-disordered breathing management in the United States. The company announced that, effective immediately in the US and US territories, Philips Respironics would stop production and sale of all hospital and home mechanical ventilation products, home and hospital ventilation devices, and oxygen concentrators.
There are many unknowns and uncertainties about how to proceed with care for patients requiring these devices. So we gathered an expert panel of clinicians from CHEST’s Home-Based Mechanical Ventilation and Neuromuscular Section within the Sleep Medicine Network to explain the current situation and offer suggestions on moving forward in caring for these patients.
Why is this happening?
John M. Coleman III, MD, FCCP: To understand the current Philips Respironics announcement, we must go back to June 2021. At that time, Philips recalled certain home mechanical ventilators, CPAP machines, and BiPAP machines due to potential health risks related to breakdown of the polyester-based polyurethane (PE-PUR) foam placed in these devices for noise reduction. Small and microscopic particles of this foam were at risk for being inhaled or ingested by patients using these devices. It was suspected that inhalation of these particles could potentially result in temporary or permanent injury. Machines in hot temperatures or using ozone cleaning were at increased risk. The US Food and Drug Administration (FDA) issued a class 1 recall, defined as “a situation in which there is reasonable probability that the use of or exposure to a violative product will cause serious adverse health consequences or death.”
In the months following the initial recall, there were additional recalls of both in-hospital and home ventilators related to the potential of these foam particles to move and block the air path, reducing airflow and causing the device to alarm.
Over the next few years, tens of thousands of medical device reports were filed about PE-PUR foam-related injuries, with some cases resulting in death. At this time, the Department of Justice began collaborating with the FDA on a consent decree. There were ongoing recalls of the CoughAssist T70 device, as well as the newest generation of Philips Respironics home ventilators, the Trilogy EVO.
Ultimately, after years of ongoing recalls and reports of numerous deaths and injuries, with multiple class action lawsuits, the consent decree was finalized. Philips Respironics agreed to stop production of all respiratory-related products in the US and US territories.
What devices does this apply to?
Jason Ackrivo, MD: This notice affects the devices shown in Table 1. All sales and device shipments have been discontinued as of January 25, 2024. Philips Respironics will continue to service the devices, subject to part availability, up to 5 years after sales discontinuation. However, Philips Respironics will continue to sell consumables and accessories, including masks.
What are my options for home mechanical ventilators?
Bethany L. Lussier, MD, FCCP: In the US, alternative approved home mechanical ventilator (HMV) devices include Astral by ResMed, Vivo 45 and Vivo 65 by Breas, and VOCSN by Ventec. Additional options made available through emergency use authorization by the FDA between 2020 and 2022 included Luisa by Löwenstein Medical, the V+ by Ventec, and Life2000 by Baxter. Many of us expedite disposition from the hospital by prescribing HMVs rather than respiratory assist devices (RADs) because it is easier to meet qualifying criteria for insurance. In efforts to promote just allocation of resources, now might be the ideal time to reconsider higher utilization of RADs over HMVs. Reasonable RAD candidates are those who do not need autotitration of EPAP, dual mode therapy, or invasive ventilation. In these cases, the qualifying criteria and patient needs may be met with a RAD capable of VAPS or BPAP-ST mode.
How are these alternative devices similar to and different from the Trilogy EVO?
Dr. Ackrivo:All these devices are portable ventilators that can deliver noninvasive or invasive ventilation. They have internal batteries for enabling portability. They offer multiple programmable presets and mouthpiece ventilation, and some offer both oxygenation and CO2 monitoring (both TcCO2 and EtCO2).
All alternative portable ventilators include a proprietary ventilation mode analogous to the Trilogy AVAPS algorithm (Table 2). The ResMed Astral has a safety tidal volume feature that targets a minimum tidal volume in PS, S/T, or P(A)C modes. The ResMed iVAPS algorithm adjusts inspiratory pressure and respiratory rate to target an alveolar ventilation based on patient-entered height. The Breas Vivo can target a tidal volume (TgV) in either PSV or PCV mode.
Unique ventilator characteristics are shown in Table 2. ResMed Astral mode options will differ between leak (passive) or valve (active) circuits. Both the Breas Vivo and Löwenstein Luisa enable high-flow oxygen delivery. Only the Breas Vivo enables connecting to a transcutaneous carbon dioxide monitor. The VOCSN name is an acronym for its multifunctional capabilities: ventilation, oxygenation, cough assist, suction, and nebulizer treatments. Lastly, the VOCSN can disable leak compensation, which may be advantageous for enabling leak speech with a tracheostomy.
I just provided my patient with a Trilogy EVO. Do I need to change this immediately?
Dr. Coleman: No, but you should start conversations with your patient/caregiving support and with your durable medical equipment (DME) provider about alternative options. The ripple effects of the Philips Respironics recall will be ongoing for years. The silver lining of this situation is that there are numerous HMV options on the market currently. It is important to review the differences between these new devices and consider what will work best for your patient and your practice. In addition, it is critical that your DME provider is familiar with these new devices, both for support and education, and is taking steps to make alternate devices available. We anticipate a push in coming months to switch patients off Trilogy EVO, so it important to get this process started.
For patients not interested in switching just yet, Philips Respironics will continue to service and offer supplies for these devices for up to 5 years, depending on part availability (Table 1). Refer to the Philips Respironics Sleep & Respiratory Product Portfolio Changes website for the most up-to-date information.
I have a patient on AVAPS, and I must change to iVAPS. What now?
Dr. Lussier: As mentioned previously by Dr. Ackrivo, the ResMed iVAPS algorithm adjusts inspiratory pressure and respiratory rate to target an alveolar ventilation based on patient-entered height. A download from a current VAPS setting can be helpful in defining target ventilation and pressure ranges for a tailored prescription. ResMed has an online iVAPS calculator (resmed.com) to assist in making this switch. Close clinical monitoring with data downloads is recommended to assure desired targets are still achieved.
What will happen to Philips Respironics’ cloud patient data?
Dr. Lussier: Representatives have reported that both providers and DME companies will have continued access to Care Orchestrator going forward. Currently, the logistics of data maintenance and ownership remain unclear, which poses additional questions about global access to patients’ data downloads.
----------
The recent discontinuation of Philips Respironics ventilation devices will induce a dramatic shift in home ventilation options in the US. Clinicians and DME companies should begin familiarizing themselves with alternative ventilators and their unique features. While significant uncertainty exists, we encourage a proactive approach to education and communication to ensure a smooth transition for patients on home ventilation.
John M. Coleman III, MD, FCCP, is Associate Professor, Division of Pulmonary & Critical Care Medicine, Department of Neurology, Northwestern University Feinberg School of Medicine. Bethany L. Lussier, MD, FCCP, is in the Department of Internal Medicine, Division of Pulmonary & Critical Care Medicine, Department of Neurology, Division of Neurocritical Care, UT Southwestern Medical Center. Jason Ackrivo, MD, is Assistant Professor of Medicine and Neurology, and Associate Director, Jay and Randy Fishman Program for Home Assisted Ventilation, Pulmonary, Allergy, and Critical Care Division, Perelman School of Medicine, University of Pennsylvania.
Fighting for fresh air: RSV’s connection to environmental pollution
Diffuse Lung Disease and Lung Transplant Network
Occupational and Environmental Health Section

Poor air quality has numerous health hazards for patients with chronic lung disease. Now mounting evidence from pediatric studies suggests a concerning link between air pollution and viral infections, specifically respiratory syncytial virus (RSV).

Multiple studies have shown increased incidence and severity of disease in children with exposure to air pollutants such as particulate matter and nitrogen dioxide.1,2,3 Researchers speculate that these pollutants potentiate viral entry to airway epithelium, increase viral load, and dysregulate the immune response.4 Air pollution, increasingly worsened by climate change, is also associated with acute respiratory infections in adults, though adult research remains sparse.5
The adoption of viral testing during the pandemic has revealed a previously under-recognized prevalence of RSV in adults.

RSV accounts for an estimated 60,000 to 160,000 hospitalizations and 6,000 to 10,000 deaths annually among elderly adults. This newfound awareness coincides with the exciting development of a new RSV vaccine that has shown around 85% efficacy at preventing symptomatic RSV infection in the first year, and new data suggest benefits persisting even into the second year after vaccination.6 With an estimated 60 million adults at high risk for RSV in the US, RSV prevention has become an increasingly important aspect of respiratory care.
While more research is needed to definitively quantify the link between air pollution and RSV in adults, the existing data offer valuable insights for all pulmonologists. These findings suggest a benefit in counseling patients with chronic lung conditions on taking steps to mitigate exposure to air pollutants, either through avoidance of outdoor activities or mask-wearing when air quality levels exceed healthy ranges, as well as promoting RSV vaccination for patients who are at risk.7
References
1. Milani GP, Cafora M, Favero C, et al. PM2.5, PM10 and bronchiolitis severity: a cohort study. Pediatr Allergy Immunol. 2022;33(10). https://doi.org/10.1111/pai.13853
2. Wrotek A, Badyda A, Czechowski PO, Owczarek T, Dąbrowiecki P, Jackowska T. Air pollutants’ concentrations are associated with increased number of RSV hospitalizations in Polish children. J Clin Med. 2021;10(15):3224. https://doi.org/10.3390/jcm10153224
3. Horne BD, Joy EA, Hofmann MG, et al. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am J Respir Crit Care Med. 2018;198(6):759-766. https://doi.org/10.1164/rccm.201709-1883oc
4. Wrotek A, Jackowska T. Molecular mechanisms of RSV and air pollution interaction: a scoping review. Int J Mol Sci. 2022;23(20):12704. https://doi.org/10.3390/ijms232012704
5. Kirwa K, Eckert CM, Vedal S, Hajat A, Kaufman JD. Ambient air pollution and risk of respiratory infection among adults: evidence from the multiethnic study of atherosclerosis (MESA). BMJ Open Respir Res. 2021;8(1). https://doi.org/10.1136/bmjresp-2020-000866
6. Melgar M, Britton A, Roper LE, et al. Use of respiratory syncytial virus vaccines in older adults: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(29):793-801. http://dx.doi.org/10.15585/mmwr.mm7229a4
7. Kodros JK, O’Dell K, Samet JM, L’Orange C, Pierce JR, Volckens J. Quantifying the health benefits of face masks and respirators to mitigate exposure to severe air pollution. GeoHealth. 2021;5(9). https://doi.org/10.1029/2021gh000482
Diffuse Lung Disease and Lung Transplant Network
Occupational and Environmental Health Section
Poor air quality has numerous health hazards for patients with chronic lung disease. Now mounting evidence from pediatric studies suggests a concerning link between air pollution and viral infections, specifically respiratory syncytial virus (RSV).
Multiple studies have shown increased incidence and severity of disease in children with exposure to air pollutants such as particulate matter and nitrogen dioxide.1,2,3 Researchers speculate that these pollutants potentiate viral entry to airway epithelium, increase viral load, and dysregulate the immune response.4 Air pollution, increasingly worsened by climate change, is also associated with acute respiratory infections in adults, though adult research remains sparse.5
The adoption of viral testing during the pandemic has revealed a previously under-recognized prevalence of RSV in adults.
RSV accounts for an estimated 60,000 to 160,000 hospitalizations and 6,000 to 10,000 deaths annually among elderly adults. This newfound awareness coincides with the exciting development of a new RSV vaccine that has shown around 85% efficacy at preventing symptomatic RSV infection in the first year, and new data suggest benefits persisting even into the second year after vaccination.6 With an estimated 60 million adults at high risk for RSV in the US, RSV prevention has become an increasingly important aspect of respiratory care.
While more research is needed to definitively quantify the link between air pollution and RSV in adults, the existing data offer valuable insights for all pulmonologists. These findings suggest a benefit in counseling patients with chronic lung conditions on taking steps to mitigate exposure to air pollutants, either through avoidance of outdoor activities or mask-wearing when air quality levels exceed healthy ranges, as well as promoting RSV vaccination for patients who are at risk.7
References
1. Milani GP, Cafora M, Favero C, et al. PM2.5, PM10 and bronchiolitis severity: a cohort study. Pediatr Allergy Immunol. 2022;33(10). https://doi.org/10.1111/pai.13853
2. Wrotek A, Badyda A, Czechowski PO, Owczarek T, Dąbrowiecki P, Jackowska T. Air pollutants’ concentrations are associated with increased number of RSV hospitalizations in Polish children. J Clin Med. 2021;10(15):3224. https://doi.org/10.3390/jcm10153224
3. Horne BD, Joy EA, Hofmann MG, et al. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am J Respir Crit Care Med. 2018;198(6):759-766. https://doi.org/10.1164/rccm.201709-1883oc
4. Wrotek A, Jackowska T. Molecular mechanisms of RSV and air pollution interaction: a scoping review. Int J Mol Sci. 2022;23(20):12704. https://doi.org/10.3390/ijms232012704
5. Kirwa K, Eckert CM, Vedal S, Hajat A, Kaufman JD. Ambient air pollution and risk of respiratory infection among adults: evidence from the multiethnic study of atherosclerosis (MESA). BMJ Open Respir Res. 2021;8(1). https://doi.org/10.1136/bmjresp-2020-000866
6. Melgar M, Britton A, Roper LE, et al. Use of respiratory syncytial virus vaccines in older adults: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(29):793-801. http://dx.doi.org/10.15585/mmwr.mm7229a4
7. Kodros JK, O’Dell K, Samet JM, L’Orange C, Pierce JR, Volckens J. Quantifying the health benefits of face masks and respirators to mitigate exposure to severe air pollution. GeoHealth. 2021;5(9). https://doi.org/10.1029/2021gh000482
Diffuse Lung Disease and Lung Transplant Network
Occupational and Environmental Health Section
Poor air quality has numerous health hazards for patients with chronic lung disease. Now mounting evidence from pediatric studies suggests a concerning link between air pollution and viral infections, specifically respiratory syncytial virus (RSV).
Multiple studies have shown increased incidence and severity of disease in children with exposure to air pollutants such as particulate matter and nitrogen dioxide.1,2,3 Researchers speculate that these pollutants potentiate viral entry to airway epithelium, increase viral load, and dysregulate the immune response.4 Air pollution, increasingly worsened by climate change, is also associated with acute respiratory infections in adults, though adult research remains sparse.5
The adoption of viral testing during the pandemic has revealed a previously under-recognized prevalence of RSV in adults.
RSV accounts for an estimated 60,000 to 160,000 hospitalizations and 6,000 to 10,000 deaths annually among elderly adults. This newfound awareness coincides with the exciting development of a new RSV vaccine that has shown around 85% efficacy at preventing symptomatic RSV infection in the first year, and new data suggest benefits persisting even into the second year after vaccination.6 With an estimated 60 million adults at high risk for RSV in the US, RSV prevention has become an increasingly important aspect of respiratory care.
While more research is needed to definitively quantify the link between air pollution and RSV in adults, the existing data offer valuable insights for all pulmonologists. These findings suggest a benefit in counseling patients with chronic lung conditions on taking steps to mitigate exposure to air pollutants, either through avoidance of outdoor activities or mask-wearing when air quality levels exceed healthy ranges, as well as promoting RSV vaccination for patients who are at risk.7
References
1. Milani GP, Cafora M, Favero C, et al. PM2.5, PM10 and bronchiolitis severity: a cohort study. Pediatr Allergy Immunol. 2022;33(10). https://doi.org/10.1111/pai.13853
2. Wrotek A, Badyda A, Czechowski PO, Owczarek T, Dąbrowiecki P, Jackowska T. Air pollutants’ concentrations are associated with increased number of RSV hospitalizations in Polish children. J Clin Med. 2021;10(15):3224. https://doi.org/10.3390/jcm10153224
3. Horne BD, Joy EA, Hofmann MG, et al. Short-term elevation of fine particulate matter air pollution and acute lower respiratory infection. Am J Respir Crit Care Med. 2018;198(6):759-766. https://doi.org/10.1164/rccm.201709-1883oc
4. Wrotek A, Jackowska T. Molecular mechanisms of RSV and air pollution interaction: a scoping review. Int J Mol Sci. 2022;23(20):12704. https://doi.org/10.3390/ijms232012704
5. Kirwa K, Eckert CM, Vedal S, Hajat A, Kaufman JD. Ambient air pollution and risk of respiratory infection among adults: evidence from the multiethnic study of atherosclerosis (MESA). BMJ Open Respir Res. 2021;8(1). https://doi.org/10.1136/bmjresp-2020-000866
6. Melgar M, Britton A, Roper LE, et al. Use of respiratory syncytial virus vaccines in older adults: recommendations of the Advisory Committee on Immunization Practices — United States, 2023. MMWR Morb Mortal Wkly Rep. 2023;72(29):793-801. http://dx.doi.org/10.15585/mmwr.mm7229a4
7. Kodros JK, O’Dell K, Samet JM, L’Orange C, Pierce JR, Volckens J. Quantifying the health benefits of face masks and respirators to mitigate exposure to severe air pollution. GeoHealth. 2021;5(9). https://doi.org/10.1029/2021gh000482
Transesophageal ultrasound: The future of ultrasound in the ICU
Thoracic Oncology and Chest Procedures Network
Ultrasound and Chest Imaging Section

Historically, transesophageal ultrasound (TEE) has been regarded as a diagnostic and management tool for structural heart disease in relatively stable patients. However, TEE is more commonly being utilized by intensivists as a first-line tool in the diagnostics and management of patients in the ICU.

TEE, with its unobstructed superior cardiac views, facilitates rapid diagnosis in undifferentiated shock and guides appropriate resuscitation efforts. Studies have shown that TEE alters management strategies in 40% of cases, following transthoracic echocardiography with an extremely low complication rate of 2% to 3% (primarily in the form of self-limited gastrointestinal bleeding).1,2,3,4
TEE also provides ultrasonographic evaluation of the lungs through transesophageal lung ultrasound (TELUS). TELUS allows for visualization of all six traditional lung zones utilized in traditional lung ultrasound.5 Patients with severe acute respiratory distress syndrome may greatly benefit from TEE utilization. TEE enables early detection of right ventricular dysfunction, aids in fluid management, and assesses the severity of lung consolidation, thereby facilitating prompt utilization of prone positioning or adjustments in positive end-expiratory pressure.
Cardiac arrest is another unique opportunity for TEE utilization by providing real-time cardiac visualization during active cardiopulmonary resuscitation. This facilitates optimal chest compression positioning, early recognition of arrhythmia, timely identification of reversible cause, and procedural guidance for ECMO-assisted CPR.6 TEE is an invaluable tool for the modern-day intensivist, providing rapid and accurate assessments, and therefore holds the potential to become standard of care in the ICU.
References
1. Prager R, Bowdridge J, Pratte M, Cheng J, McInnes MD, Arntfield R. Indications, clinical impact, and complications of critical care transesophageal echocardiography: a scoping review. J Intensive Care Med. 2023;38(3):245-272. Preprint. Posted online July 19, 2022. PMID: 35854414; PMCID: PMC9806486. doi: 10.1177/08850666221115348
2. Hüttemann E, Schelenz C, Kara F, Chatzinikolaou K, Reinhart K. The use and safety of transoesophageal echocardiography in the general ICU – a minireview. Acta Anaesthesiol Scand. 2004;48(7):827-36. PMID: 15242426. doi: 10.1111/j.0001-5172.2004.00423.x
3. Mayo PH, Narasimhan M, Koenig S. Critical care transesophageal echocardiography. Chest. 2015;148(5):1323-1332. PMID: 26204465. doi: 10.1378/chest.15-0260
4. Prager R, Ainsworth C, Arntfield R. Critical care transesophageal echocardiography for the resuscitation of shock: an important diagnostic skill for the modern intensivist. Chest. 2023;163(2):268-269. PMID: 36759112. doi: 10.1016/j.chest.2022.09.001
5. Cavayas YA, Girard M, Desjardins G, Denault AY. Transesophageal lung ultrasonography: a novel technique for investigating hypoxemia. Can J Anaesth. 2016;63(11):1266-76. Preprint. Posted online July 29, 2016. PMID: 27473720. doi: 10.1007/s12630-016-0702-2
6. Teran F, Prats MI, Nelson BP, et al. Focused transesophageal echocardiography during cardiac arrest resuscitation: JACC review wopic of the Week. J Am Coll Cardiol. 2020;76(6):745-754. PMID: 32762909. doi: 10.1016/j.jacc.2020.05.074
Thoracic Oncology and Chest Procedures Network
Ultrasound and Chest Imaging Section
Historically, transesophageal ultrasound (TEE) has been regarded as a diagnostic and management tool for structural heart disease in relatively stable patients. However, TEE is more commonly being utilized by intensivists as a first-line tool in the diagnostics and management of patients in the ICU.
TEE, with its unobstructed superior cardiac views, facilitates rapid diagnosis in undifferentiated shock and guides appropriate resuscitation efforts. Studies have shown that TEE alters management strategies in 40% of cases, following transthoracic echocardiography with an extremely low complication rate of 2% to 3% (primarily in the form of self-limited gastrointestinal bleeding).1,2,3,4
TEE also provides ultrasonographic evaluation of the lungs through transesophageal lung ultrasound (TELUS). TELUS allows for visualization of all six traditional lung zones utilized in traditional lung ultrasound.5 Patients with severe acute respiratory distress syndrome may greatly benefit from TEE utilization. TEE enables early detection of right ventricular dysfunction, aids in fluid management, and assesses the severity of lung consolidation, thereby facilitating prompt utilization of prone positioning or adjustments in positive end-expiratory pressure.
Cardiac arrest is another unique opportunity for TEE utilization by providing real-time cardiac visualization during active cardiopulmonary resuscitation. This facilitates optimal chest compression positioning, early recognition of arrhythmia, timely identification of reversible cause, and procedural guidance for ECMO-assisted CPR.6 TEE is an invaluable tool for the modern-day intensivist, providing rapid and accurate assessments, and therefore holds the potential to become standard of care in the ICU.
References
1. Prager R, Bowdridge J, Pratte M, Cheng J, McInnes MD, Arntfield R. Indications, clinical impact, and complications of critical care transesophageal echocardiography: a scoping review. J Intensive Care Med. 2023;38(3):245-272. Preprint. Posted online July 19, 2022. PMID: 35854414; PMCID: PMC9806486. doi: 10.1177/08850666221115348
2. Hüttemann E, Schelenz C, Kara F, Chatzinikolaou K, Reinhart K. The use and safety of transoesophageal echocardiography in the general ICU – a minireview. Acta Anaesthesiol Scand. 2004;48(7):827-36. PMID: 15242426. doi: 10.1111/j.0001-5172.2004.00423.x
3. Mayo PH, Narasimhan M, Koenig S. Critical care transesophageal echocardiography. Chest. 2015;148(5):1323-1332. PMID: 26204465. doi: 10.1378/chest.15-0260
4. Prager R, Ainsworth C, Arntfield R. Critical care transesophageal echocardiography for the resuscitation of shock: an important diagnostic skill for the modern intensivist. Chest. 2023;163(2):268-269. PMID: 36759112. doi: 10.1016/j.chest.2022.09.001
5. Cavayas YA, Girard M, Desjardins G, Denault AY. Transesophageal lung ultrasonography: a novel technique for investigating hypoxemia. Can J Anaesth. 2016;63(11):1266-76. Preprint. Posted online July 29, 2016. PMID: 27473720. doi: 10.1007/s12630-016-0702-2
6. Teran F, Prats MI, Nelson BP, et al. Focused transesophageal echocardiography during cardiac arrest resuscitation: JACC review wopic of the Week. J Am Coll Cardiol. 2020;76(6):745-754. PMID: 32762909. doi: 10.1016/j.jacc.2020.05.074
Thoracic Oncology and Chest Procedures Network
Ultrasound and Chest Imaging Section
Historically, transesophageal ultrasound (TEE) has been regarded as a diagnostic and management tool for structural heart disease in relatively stable patients. However, TEE is more commonly being utilized by intensivists as a first-line tool in the diagnostics and management of patients in the ICU.
TEE, with its unobstructed superior cardiac views, facilitates rapid diagnosis in undifferentiated shock and guides appropriate resuscitation efforts. Studies have shown that TEE alters management strategies in 40% of cases, following transthoracic echocardiography with an extremely low complication rate of 2% to 3% (primarily in the form of self-limited gastrointestinal bleeding).1,2,3,4
TEE also provides ultrasonographic evaluation of the lungs through transesophageal lung ultrasound (TELUS). TELUS allows for visualization of all six traditional lung zones utilized in traditional lung ultrasound.5 Patients with severe acute respiratory distress syndrome may greatly benefit from TEE utilization. TEE enables early detection of right ventricular dysfunction, aids in fluid management, and assesses the severity of lung consolidation, thereby facilitating prompt utilization of prone positioning or adjustments in positive end-expiratory pressure.
Cardiac arrest is another unique opportunity for TEE utilization by providing real-time cardiac visualization during active cardiopulmonary resuscitation. This facilitates optimal chest compression positioning, early recognition of arrhythmia, timely identification of reversible cause, and procedural guidance for ECMO-assisted CPR.6 TEE is an invaluable tool for the modern-day intensivist, providing rapid and accurate assessments, and therefore holds the potential to become standard of care in the ICU.
References
1. Prager R, Bowdridge J, Pratte M, Cheng J, McInnes MD, Arntfield R. Indications, clinical impact, and complications of critical care transesophageal echocardiography: a scoping review. J Intensive Care Med. 2023;38(3):245-272. Preprint. Posted online July 19, 2022. PMID: 35854414; PMCID: PMC9806486. doi: 10.1177/08850666221115348
2. Hüttemann E, Schelenz C, Kara F, Chatzinikolaou K, Reinhart K. The use and safety of transoesophageal echocardiography in the general ICU – a minireview. Acta Anaesthesiol Scand. 2004;48(7):827-36. PMID: 15242426. doi: 10.1111/j.0001-5172.2004.00423.x
3. Mayo PH, Narasimhan M, Koenig S. Critical care transesophageal echocardiography. Chest. 2015;148(5):1323-1332. PMID: 26204465. doi: 10.1378/chest.15-0260
4. Prager R, Ainsworth C, Arntfield R. Critical care transesophageal echocardiography for the resuscitation of shock: an important diagnostic skill for the modern intensivist. Chest. 2023;163(2):268-269. PMID: 36759112. doi: 10.1016/j.chest.2022.09.001
5. Cavayas YA, Girard M, Desjardins G, Denault AY. Transesophageal lung ultrasonography: a novel technique for investigating hypoxemia. Can J Anaesth. 2016;63(11):1266-76. Preprint. Posted online July 29, 2016. PMID: 27473720. doi: 10.1007/s12630-016-0702-2
6. Teran F, Prats MI, Nelson BP, et al. Focused transesophageal echocardiography during cardiac arrest resuscitation: JACC review wopic of the Week. J Am Coll Cardiol. 2020;76(6):745-754. PMID: 32762909. doi: 10.1016/j.jacc.2020.05.074
The pendulum swings in favor of corticosteroids


Critical Care Network
Sepsis/Shock Section
The pendulum swings in favor of corticosteroids and endorses the colloquialism among intensivists that no patient shall die without steroids, especially as it relates to sepsis and septic shock.
In 2018, we saw divergence among randomized controlled trials in the use of glucocorticoids for adults with septic shock such that hydrocortisone without the use of fludrocortisone showed no 90-day mortality benefit; however, hydrocortisone with fludrocortisone showed a 90-day mortality benefit.1,2 The Surviving Sepsis Guidelines in 2021 favored using low-dose corticosteroids in those with persistent vasopressor requirements in whom other core interventions had been instituted.
In 2023, a patient-level meta-analysis of low-dose hydrocortisone in adults with septic shock included seven trials and failed to demonstrate a mortality benefit by relative risk in those who received hydrocortisone compared with placebo. Separately, a network meta-analysis with hydrocortisone plus enteral fludrocortisone was associated with a 90-day all-cause mortality. Of the secondary outcomes, these results offered a possible association of hydrocortisone with a decreased risk of ICU mortality and with increased vasopressor-free days.3
The 2024 Society of Critical Care Medicine recently shared an update of focused guidelines on the use of corticosteroids in sepsis, acute respiratory distress syndrome, and community-acquired pneumonia. These included a conditional recommendation to administer corticosteroids for patients with septic shock but recommended against high-dose/short-duration administration of corticosteroids in these patients. These guidelines were supported by data from 46 randomized controlled trials, which showed that corticosteroid use may reduce hospital/long-term mortality and ICU/short-term mortality, as well as result in higher rates of shock reversal and reduced organ dysfunction.
With the results of these meta-analyses and randomized controlled trials, clinicians should consider low-dose corticosteroids paired with fludrocortisone as a tool in treating patients with septic shock given that the short- and long-term benefits may exceed any risks.
References
1. Venkatesh B, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378:797-808.
2. Annane D, et al. Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med. 2018;378:809-818.
3. Pirracchio R, et al. Patient-level meta-analysis of low-dose hydrocortisone in adults with septic shock. NEJM Evid. 2023;2(6).
Critical Care Network
Sepsis/Shock Section
The pendulum swings in favor of corticosteroids and endorses the colloquialism among intensivists that no patient shall die without steroids, especially as it relates to sepsis and septic shock.
In 2018, we saw divergence among randomized controlled trials in the use of glucocorticoids for adults with septic shock such that hydrocortisone without the use of fludrocortisone showed no 90-day mortality benefit; however, hydrocortisone with fludrocortisone showed a 90-day mortality benefit.1,2 The Surviving Sepsis Guidelines in 2021 favored using low-dose corticosteroids in those with persistent vasopressor requirements in whom other core interventions had been instituted.
In 2023, a patient-level meta-analysis of low-dose hydrocortisone in adults with septic shock included seven trials and failed to demonstrate a mortality benefit by relative risk in those who received hydrocortisone compared with placebo. Separately, a network meta-analysis with hydrocortisone plus enteral fludrocortisone was associated with a 90-day all-cause mortality. Of the secondary outcomes, these results offered a possible association of hydrocortisone with a decreased risk of ICU mortality and with increased vasopressor-free days.3
The 2024 Society of Critical Care Medicine recently shared an update of focused guidelines on the use of corticosteroids in sepsis, acute respiratory distress syndrome, and community-acquired pneumonia. These included a conditional recommendation to administer corticosteroids for patients with septic shock but recommended against high-dose/short-duration administration of corticosteroids in these patients. These guidelines were supported by data from 46 randomized controlled trials, which showed that corticosteroid use may reduce hospital/long-term mortality and ICU/short-term mortality, as well as result in higher rates of shock reversal and reduced organ dysfunction.
With the results of these meta-analyses and randomized controlled trials, clinicians should consider low-dose corticosteroids paired with fludrocortisone as a tool in treating patients with septic shock given that the short- and long-term benefits may exceed any risks.
References
1. Venkatesh B, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378:797-808.
2. Annane D, et al. Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med. 2018;378:809-818.
3. Pirracchio R, et al. Patient-level meta-analysis of low-dose hydrocortisone in adults with septic shock. NEJM Evid. 2023;2(6).
Critical Care Network
Sepsis/Shock Section
The pendulum swings in favor of corticosteroids and endorses the colloquialism among intensivists that no patient shall die without steroids, especially as it relates to sepsis and septic shock.
In 2018, we saw divergence among randomized controlled trials in the use of glucocorticoids for adults with septic shock such that hydrocortisone without the use of fludrocortisone showed no 90-day mortality benefit; however, hydrocortisone with fludrocortisone showed a 90-day mortality benefit.1,2 The Surviving Sepsis Guidelines in 2021 favored using low-dose corticosteroids in those with persistent vasopressor requirements in whom other core interventions had been instituted.
In 2023, a patient-level meta-analysis of low-dose hydrocortisone in adults with septic shock included seven trials and failed to demonstrate a mortality benefit by relative risk in those who received hydrocortisone compared with placebo. Separately, a network meta-analysis with hydrocortisone plus enteral fludrocortisone was associated with a 90-day all-cause mortality. Of the secondary outcomes, these results offered a possible association of hydrocortisone with a decreased risk of ICU mortality and with increased vasopressor-free days.3
The 2024 Society of Critical Care Medicine recently shared an update of focused guidelines on the use of corticosteroids in sepsis, acute respiratory distress syndrome, and community-acquired pneumonia. These included a conditional recommendation to administer corticosteroids for patients with septic shock but recommended against high-dose/short-duration administration of corticosteroids in these patients. These guidelines were supported by data from 46 randomized controlled trials, which showed that corticosteroid use may reduce hospital/long-term mortality and ICU/short-term mortality, as well as result in higher rates of shock reversal and reduced organ dysfunction.
With the results of these meta-analyses and randomized controlled trials, clinicians should consider low-dose corticosteroids paired with fludrocortisone as a tool in treating patients with septic shock given that the short- and long-term benefits may exceed any risks.
References
1. Venkatesh B, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378:797-808.
2. Annane D, et al. Hydrocortisone plus fludrocortisone for adults with septic shock. N Engl J Med. 2018;378:809-818.
3. Pirracchio R, et al. Patient-level meta-analysis of low-dose hydrocortisone in adults with septic shock. NEJM Evid. 2023;2(6).