User login
FDA issues safety alert for loperamide
The Food and Drug Administration announced Jan. 30 that is has issued a MedWatch safety alert on the use of the over-the-counter (OTC) antidiarrhea drug, loperamide.
Currently, the FDA is working with manufacturers to use blister packs or other single-dose packaging and to limit the number of doses in a package.
The alert comes after receiving continuous reports of serious heart problems and deaths with the use of much higher than recommended doses of loperamide, mainly among people who are intentionally misusing or abusing the product, regardless of the addition of a warning to the medicine label and a previous communication. The FDA states that loperamide is a safe drug when used as directed.
Loperamide is approved to help control symptoms of diarrhea. The maximum recommended daily dose for adults is 8 mg per day for OTC use and 16 mg per day for prescription use. It acts on opioid receptors in the gut to slow the movement in the intestines and decrease the number of bowel movements.
It is noted that much higher than recommended doses of loperamide, either intentionally or unintentionally, can result in serious cardiac adverse events, including QT interval prolongation, torsade de pointes or other ventricular arrhythmias, syncope, and cardiac arrest. Health care professionals and patients can report adverse events or side effects related to the use of these products to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
In 2016, the FDA issued a Drug Safety Communication and added warnings about serious heart problems to the drug label of prescription loperamide and to the Drug Facts label of OTC loperamide products. The FDA is working to evaluate this safety issue and will update the public when more information is available.
Read the full safety alert here.
The Food and Drug Administration announced Jan. 30 that is has issued a MedWatch safety alert on the use of the over-the-counter (OTC) antidiarrhea drug, loperamide.
Currently, the FDA is working with manufacturers to use blister packs or other single-dose packaging and to limit the number of doses in a package.
The alert comes after receiving continuous reports of serious heart problems and deaths with the use of much higher than recommended doses of loperamide, mainly among people who are intentionally misusing or abusing the product, regardless of the addition of a warning to the medicine label and a previous communication. The FDA states that loperamide is a safe drug when used as directed.
Loperamide is approved to help control symptoms of diarrhea. The maximum recommended daily dose for adults is 8 mg per day for OTC use and 16 mg per day for prescription use. It acts on opioid receptors in the gut to slow the movement in the intestines and decrease the number of bowel movements.
It is noted that much higher than recommended doses of loperamide, either intentionally or unintentionally, can result in serious cardiac adverse events, including QT interval prolongation, torsade de pointes or other ventricular arrhythmias, syncope, and cardiac arrest. Health care professionals and patients can report adverse events or side effects related to the use of these products to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
In 2016, the FDA issued a Drug Safety Communication and added warnings about serious heart problems to the drug label of prescription loperamide and to the Drug Facts label of OTC loperamide products. The FDA is working to evaluate this safety issue and will update the public when more information is available.
Read the full safety alert here.
The Food and Drug Administration announced Jan. 30 that is has issued a MedWatch safety alert on the use of the over-the-counter (OTC) antidiarrhea drug, loperamide.
Currently, the FDA is working with manufacturers to use blister packs or other single-dose packaging and to limit the number of doses in a package.
The alert comes after receiving continuous reports of serious heart problems and deaths with the use of much higher than recommended doses of loperamide, mainly among people who are intentionally misusing or abusing the product, regardless of the addition of a warning to the medicine label and a previous communication. The FDA states that loperamide is a safe drug when used as directed.
Loperamide is approved to help control symptoms of diarrhea. The maximum recommended daily dose for adults is 8 mg per day for OTC use and 16 mg per day for prescription use. It acts on opioid receptors in the gut to slow the movement in the intestines and decrease the number of bowel movements.
It is noted that much higher than recommended doses of loperamide, either intentionally or unintentionally, can result in serious cardiac adverse events, including QT interval prolongation, torsade de pointes or other ventricular arrhythmias, syncope, and cardiac arrest. Health care professionals and patients can report adverse events or side effects related to the use of these products to the FDA’s MedWatch Safety Information and Adverse Event Reporting Program.
In 2016, the FDA issued a Drug Safety Communication and added warnings about serious heart problems to the drug label of prescription loperamide and to the Drug Facts label of OTC loperamide products. The FDA is working to evaluate this safety issue and will update the public when more information is available.
Read the full safety alert here.
FDA approves irritable bowel syndrome treatment
(IBS-C).
Plecanatide had previously been approved to treat adults with chronic idiopathic constipation (CIC).
Plecanatide was approved on the findings of two randomized, double-blind, 12-week, placebo-controlled clinical trials. More than 2,100 adult patients across both trials received either a 3-mg or 6-mg once-daily tablet of plecanatide, or a placebo. The primary endpoints of both studies were greater than 30% reduction in worst abdominal pain and an increase of at least one complete spontaneous bowel movement (CSBM) for at least half of the 12 treatment weeks.
Plecanatide met both of its primary endpoints, with reductions in abdominal pain in both studies, compared with placebo (30.2% vs. 17.8% in study 1, P < .001; 21.5% vs. 14.2% in study 2, P = .009).
Plecanatide is the only prescription, once-daily medication that treats both CIC and IBS-C in adults. The drug should be available in the first quarter of 2018.
AGA offers free patient education materials to help your patients better understand how to live with and manage their IBS. Visit www.gastro.org/ibs.
(IBS-C).
Plecanatide had previously been approved to treat adults with chronic idiopathic constipation (CIC).
Plecanatide was approved on the findings of two randomized, double-blind, 12-week, placebo-controlled clinical trials. More than 2,100 adult patients across both trials received either a 3-mg or 6-mg once-daily tablet of plecanatide, or a placebo. The primary endpoints of both studies were greater than 30% reduction in worst abdominal pain and an increase of at least one complete spontaneous bowel movement (CSBM) for at least half of the 12 treatment weeks.
Plecanatide met both of its primary endpoints, with reductions in abdominal pain in both studies, compared with placebo (30.2% vs. 17.8% in study 1, P < .001; 21.5% vs. 14.2% in study 2, P = .009).
Plecanatide is the only prescription, once-daily medication that treats both CIC and IBS-C in adults. The drug should be available in the first quarter of 2018.
AGA offers free patient education materials to help your patients better understand how to live with and manage their IBS. Visit www.gastro.org/ibs.
(IBS-C).
Plecanatide had previously been approved to treat adults with chronic idiopathic constipation (CIC).
Plecanatide was approved on the findings of two randomized, double-blind, 12-week, placebo-controlled clinical trials. More than 2,100 adult patients across both trials received either a 3-mg or 6-mg once-daily tablet of plecanatide, or a placebo. The primary endpoints of both studies were greater than 30% reduction in worst abdominal pain and an increase of at least one complete spontaneous bowel movement (CSBM) for at least half of the 12 treatment weeks.
Plecanatide met both of its primary endpoints, with reductions in abdominal pain in both studies, compared with placebo (30.2% vs. 17.8% in study 1, P < .001; 21.5% vs. 14.2% in study 2, P = .009).
Plecanatide is the only prescription, once-daily medication that treats both CIC and IBS-C in adults. The drug should be available in the first quarter of 2018.
AGA offers free patient education materials to help your patients better understand how to live with and manage their IBS. Visit www.gastro.org/ibs.

‘Smoker’s paradox’ found in study of IBD patients
Las Vegas – Smoking is more prevalent in Crohn’s disease (CD) patients than in patients with ulcerative colitis (UC), results from a retrospective analysis of national data showed. In addition, , a so-called “smoker’s paradox.”
“This paradox seems to be real, because we know that it has been shown in some heart diseases, that the patients who were smokers had better outcomes,” Zubair Khan, MD, said in an interview at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. In fact, a recent analysis of a nationwide cohort of patients who underwent primary percutaneous coronary intervention for ST-segment elevation myocardial infarction found that smokers had significantly lower risk‐adjusted in‐hospital mortality, compared with nonsmokers (J Am Heart Assoc. 2016 Apr 22;5:e003370. doi: 10.1161/JAHA.116.003370).
Between 2002 and 2014, a higher proportion of CD patients than UC patients were smokers (25.1% vs. 17.2%; P less than .001), while CD patients who smoked were more likely to be younger than age 50 years, compared with UC patients who smoked (53.9% vs. 36.9%; P less than .001). The researchers also found that African Americans with CD were more likely than were those with UC to smoke (10% vs. 7.8%, respectively; P less than .001). On the other hand, both Hispanics and Asians with UC were more likely to be smokers than were their counterparts with CD (5% vs. 2.9% and 3.4% vs. 2.5%, respectively). From a geographical standpoint, UC patients in the Northeast and Western United States were more likely to be smokers, compared with CD patients in those regions (20.7% vs. 18.3% and 21.4% vs. 15%, respectively). Meanwhile, CD patients in the Midwest and South were more likely to be smokers, compared with UC patients in those regions (29.3% vs 26% and 37.2% vs. 31.9%, respectively).
Dr. Khan and his associates also found that a higher proportion of female CD patients were smokers, compared with female UC patients (57% vs. 47.3%; P less than .001), and that mortality among UC and CD patients with no smoking history was higher than that of their counterparts who had a smoking history (2.5% vs. 1.2% and 1.2% vs. 0.7%, respectively; P less than .001 for both associations).
“I would certainly not encourage IBD patients to smoke, but maybe we need to so some more prospective studies to better understand this smoker’s paradox,” Dr. Khan said. He reported having no financial disclosures.
*This story was updated on 3/26.
SOURCE: Khan et al. Crohn’s & Colitis Congress, Poster 213.
Las Vegas – Smoking is more prevalent in Crohn’s disease (CD) patients than in patients with ulcerative colitis (UC), results from a retrospective analysis of national data showed. In addition, , a so-called “smoker’s paradox.”
“This paradox seems to be real, because we know that it has been shown in some heart diseases, that the patients who were smokers had better outcomes,” Zubair Khan, MD, said in an interview at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. In fact, a recent analysis of a nationwide cohort of patients who underwent primary percutaneous coronary intervention for ST-segment elevation myocardial infarction found that smokers had significantly lower risk‐adjusted in‐hospital mortality, compared with nonsmokers (J Am Heart Assoc. 2016 Apr 22;5:e003370. doi: 10.1161/JAHA.116.003370).
Between 2002 and 2014, a higher proportion of CD patients than UC patients were smokers (25.1% vs. 17.2%; P less than .001), while CD patients who smoked were more likely to be younger than age 50 years, compared with UC patients who smoked (53.9% vs. 36.9%; P less than .001). The researchers also found that African Americans with CD were more likely than were those with UC to smoke (10% vs. 7.8%, respectively; P less than .001). On the other hand, both Hispanics and Asians with UC were more likely to be smokers than were their counterparts with CD (5% vs. 2.9% and 3.4% vs. 2.5%, respectively). From a geographical standpoint, UC patients in the Northeast and Western United States were more likely to be smokers, compared with CD patients in those regions (20.7% vs. 18.3% and 21.4% vs. 15%, respectively). Meanwhile, CD patients in the Midwest and South were more likely to be smokers, compared with UC patients in those regions (29.3% vs 26% and 37.2% vs. 31.9%, respectively).
Dr. Khan and his associates also found that a higher proportion of female CD patients were smokers, compared with female UC patients (57% vs. 47.3%; P less than .001), and that mortality among UC and CD patients with no smoking history was higher than that of their counterparts who had a smoking history (2.5% vs. 1.2% and 1.2% vs. 0.7%, respectively; P less than .001 for both associations).
“I would certainly not encourage IBD patients to smoke, but maybe we need to so some more prospective studies to better understand this smoker’s paradox,” Dr. Khan said. He reported having no financial disclosures.
*This story was updated on 3/26.
SOURCE: Khan et al. Crohn’s & Colitis Congress, Poster 213.
Las Vegas – Smoking is more prevalent in Crohn’s disease (CD) patients than in patients with ulcerative colitis (UC), results from a retrospective analysis of national data showed. In addition, , a so-called “smoker’s paradox.”
“This paradox seems to be real, because we know that it has been shown in some heart diseases, that the patients who were smokers had better outcomes,” Zubair Khan, MD, said in an interview at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. In fact, a recent analysis of a nationwide cohort of patients who underwent primary percutaneous coronary intervention for ST-segment elevation myocardial infarction found that smokers had significantly lower risk‐adjusted in‐hospital mortality, compared with nonsmokers (J Am Heart Assoc. 2016 Apr 22;5:e003370. doi: 10.1161/JAHA.116.003370).
Between 2002 and 2014, a higher proportion of CD patients than UC patients were smokers (25.1% vs. 17.2%; P less than .001), while CD patients who smoked were more likely to be younger than age 50 years, compared with UC patients who smoked (53.9% vs. 36.9%; P less than .001). The researchers also found that African Americans with CD were more likely than were those with UC to smoke (10% vs. 7.8%, respectively; P less than .001). On the other hand, both Hispanics and Asians with UC were more likely to be smokers than were their counterparts with CD (5% vs. 2.9% and 3.4% vs. 2.5%, respectively). From a geographical standpoint, UC patients in the Northeast and Western United States were more likely to be smokers, compared with CD patients in those regions (20.7% vs. 18.3% and 21.4% vs. 15%, respectively). Meanwhile, CD patients in the Midwest and South were more likely to be smokers, compared with UC patients in those regions (29.3% vs 26% and 37.2% vs. 31.9%, respectively).
Dr. Khan and his associates also found that a higher proportion of female CD patients were smokers, compared with female UC patients (57% vs. 47.3%; P less than .001), and that mortality among UC and CD patients with no smoking history was higher than that of their counterparts who had a smoking history (2.5% vs. 1.2% and 1.2% vs. 0.7%, respectively; P less than .001 for both associations).
“I would certainly not encourage IBD patients to smoke, but maybe we need to so some more prospective studies to better understand this smoker’s paradox,” Dr. Khan said. He reported having no financial disclosures.
*This story was updated on 3/26.
SOURCE: Khan et al. Crohn’s & Colitis Congress, Poster 213.
REPORTING FROM THE CROHN’S & COLITIS CONGRESS
Key clinical point: In IBD patients, smoker status was paradoxically associated with mortality and other outcomes.
Major finding: Mortality among UC and CD patients with no smoking history was higher than that of their counterparts who had a smoking history (2.5% vs. 1.2% and 1.2% vs. 0.7%, respectively; P less than .001 for both associations).
Study details: An analysis of 22,620 patients with a primary or secondary discharge diagnosis of IBD during 2002-2014.
Disclosures: Dr. Khan reported having no financial disclosures.
Source: Khan et al. Crohn’s & Colitis Congress, Poster 213.
Higher BMI linked to problems for IBD patients
LAS VEGAS – Higher body mass index among inflammatory bowel disease patients is independently associated with an increased risk of treatment failure and IBD-related surgery or hospitalization, a single-center, retrospective cohort study demonstrated.
“The problem of IBD and obesity is on the rise,” Soumya Kurnool said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Today, 15%-40% of IBD patients are obese. This is significant because there is a decreased prevalence of remission and an increased risk of relapse in obese IBD patients. These patients also have a higher annual burden of hospitalization.”

She and her associates set out to evaluate the effect of obesity on response to biologic therapy in patients with ulcerative colitis (UC). They conducted a single-center, retrospective cohort study of biologic-treated adults with UC who started therapy during 2011-2016. The researchers excluded patients who had undergone a prior colectomy, as well as those who were underweight at the time of starting a biologic agent and those who had fewer than 6 months of follow-up data.
The primary outcome was time to treatment failure, defined as a composite of IBD-related surgery, hospitalization, and/or treatment modification. Secondary outcomes were time to IBD-related surgery and/or hospitalization and whether the patient achieved endoscopic remission within 1 year of starting biologic therapy. They conducted multivariate Cox proportional hazard analyses after adjusting for key confounders.
Ms. Kurnool reported results from 160 patients with a median age of 36 years. Half were male, and the mean follow-up was 24 months. The median BMI of the cohort was 24.3 kg/m2; 26% were overweight and 18% were obese. More than half of patients (55%) were on infliximab with weight-based dosing and 45% were on other fixed-dosing regimens, including 19% on vedolizumab. In terms of outcomes, 68% of patients experienced treatment failure. All who failed treatment underwent treatment modifications; 15% had IBD-related surgery, and 19% had IBD-related hospitalization.
After adjusting for age, sex, disease duration, prior hospitalization, prior anti-TNF therapy, steroid use, and albumin level, Ms. Kurnool and her associates found that every 1-kg/m2 increase in BMI was associated with a 4% higher risk of treatment failure (adjusted hazard ratio, 1.04), an 8% higher risk of surgery or hospitalization (adjusted HR, 1.08), and a 6% lower risk of achieving endoscopic remission (adjusted HR, 0.94).
“This increase in the risk of treatment failure and IBD-related surgery or hospitalization was consistent across strata of patients treated with infliximab and fixed-dosing regimens,” she said. “Based on these findings, physicians should consider proactive monitoring in obese patients treated with biologic agents.”
Ms. Kurnool reported having received a National Institutes of Health Short Term Training Grant from the University of California, San Diego.
*This story was updated on 3/26.
SOURCE: Kurnool S et al. Crohn’s & Colitis Congress, Clinical Abstract 24.
LAS VEGAS – Higher body mass index among inflammatory bowel disease patients is independently associated with an increased risk of treatment failure and IBD-related surgery or hospitalization, a single-center, retrospective cohort study demonstrated.
“The problem of IBD and obesity is on the rise,” Soumya Kurnool said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Today, 15%-40% of IBD patients are obese. This is significant because there is a decreased prevalence of remission and an increased risk of relapse in obese IBD patients. These patients also have a higher annual burden of hospitalization.”
She and her associates set out to evaluate the effect of obesity on response to biologic therapy in patients with ulcerative colitis (UC). They conducted a single-center, retrospective cohort study of biologic-treated adults with UC who started therapy during 2011-2016. The researchers excluded patients who had undergone a prior colectomy, as well as those who were underweight at the time of starting a biologic agent and those who had fewer than 6 months of follow-up data.
The primary outcome was time to treatment failure, defined as a composite of IBD-related surgery, hospitalization, and/or treatment modification. Secondary outcomes were time to IBD-related surgery and/or hospitalization and whether the patient achieved endoscopic remission within 1 year of starting biologic therapy. They conducted multivariate Cox proportional hazard analyses after adjusting for key confounders.
Ms. Kurnool reported results from 160 patients with a median age of 36 years. Half were male, and the mean follow-up was 24 months. The median BMI of the cohort was 24.3 kg/m2; 26% were overweight and 18% were obese. More than half of patients (55%) were on infliximab with weight-based dosing and 45% were on other fixed-dosing regimens, including 19% on vedolizumab. In terms of outcomes, 68% of patients experienced treatment failure. All who failed treatment underwent treatment modifications; 15% had IBD-related surgery, and 19% had IBD-related hospitalization.
After adjusting for age, sex, disease duration, prior hospitalization, prior anti-TNF therapy, steroid use, and albumin level, Ms. Kurnool and her associates found that every 1-kg/m2 increase in BMI was associated with a 4% higher risk of treatment failure (adjusted hazard ratio, 1.04), an 8% higher risk of surgery or hospitalization (adjusted HR, 1.08), and a 6% lower risk of achieving endoscopic remission (adjusted HR, 0.94).
“This increase in the risk of treatment failure and IBD-related surgery or hospitalization was consistent across strata of patients treated with infliximab and fixed-dosing regimens,” she said. “Based on these findings, physicians should consider proactive monitoring in obese patients treated with biologic agents.”
Ms. Kurnool reported having received a National Institutes of Health Short Term Training Grant from the University of California, San Diego.
*This story was updated on 3/26.
SOURCE: Kurnool S et al. Crohn’s & Colitis Congress, Clinical Abstract 24.
LAS VEGAS – Higher body mass index among inflammatory bowel disease patients is independently associated with an increased risk of treatment failure and IBD-related surgery or hospitalization, a single-center, retrospective cohort study demonstrated.
“The problem of IBD and obesity is on the rise,” Soumya Kurnool said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Today, 15%-40% of IBD patients are obese. This is significant because there is a decreased prevalence of remission and an increased risk of relapse in obese IBD patients. These patients also have a higher annual burden of hospitalization.”
She and her associates set out to evaluate the effect of obesity on response to biologic therapy in patients with ulcerative colitis (UC). They conducted a single-center, retrospective cohort study of biologic-treated adults with UC who started therapy during 2011-2016. The researchers excluded patients who had undergone a prior colectomy, as well as those who were underweight at the time of starting a biologic agent and those who had fewer than 6 months of follow-up data.
The primary outcome was time to treatment failure, defined as a composite of IBD-related surgery, hospitalization, and/or treatment modification. Secondary outcomes were time to IBD-related surgery and/or hospitalization and whether the patient achieved endoscopic remission within 1 year of starting biologic therapy. They conducted multivariate Cox proportional hazard analyses after adjusting for key confounders.
Ms. Kurnool reported results from 160 patients with a median age of 36 years. Half were male, and the mean follow-up was 24 months. The median BMI of the cohort was 24.3 kg/m2; 26% were overweight and 18% were obese. More than half of patients (55%) were on infliximab with weight-based dosing and 45% were on other fixed-dosing regimens, including 19% on vedolizumab. In terms of outcomes, 68% of patients experienced treatment failure. All who failed treatment underwent treatment modifications; 15% had IBD-related surgery, and 19% had IBD-related hospitalization.
After adjusting for age, sex, disease duration, prior hospitalization, prior anti-TNF therapy, steroid use, and albumin level, Ms. Kurnool and her associates found that every 1-kg/m2 increase in BMI was associated with a 4% higher risk of treatment failure (adjusted hazard ratio, 1.04), an 8% higher risk of surgery or hospitalization (adjusted HR, 1.08), and a 6% lower risk of achieving endoscopic remission (adjusted HR, 0.94).
“This increase in the risk of treatment failure and IBD-related surgery or hospitalization was consistent across strata of patients treated with infliximab and fixed-dosing regimens,” she said. “Based on these findings, physicians should consider proactive monitoring in obese patients treated with biologic agents.”
Ms. Kurnool reported having received a National Institutes of Health Short Term Training Grant from the University of California, San Diego.
*This story was updated on 3/26.
SOURCE: Kurnool S et al. Crohn’s & Colitis Congress, Clinical Abstract 24.
REPORTING FROM THE CROHN’S & COLITIS CONGRESS
Key clinical point: Consider proactive monitoring in obese patients treated with biologic agents.
Major finding: Every 1-kg/m2 increase in BMI was associated with a 4% higher risk of treatment failure (adjusted HR, 1.04).
Study details: A single-center retrospective analysis of 160 IBD patients.
Disclosures: Ms. Kurnool reported having received a National Institutes of Health Short-Term Training Grant from the University of California, San Diego.
Source: Kurnool S et al. Crohn’s & Colitis Congress, Clinical Abstract 24.
Chronic constipation: Practical approaches and novel therapies
While constipation is one of the most common symptoms managed by practicing gastroenterologists, it can also be among the most challenging. As a presenting complaint, constipation manifests with widely varying degrees of severity and may be seen in all age groups, ethnicities, and socioeconomic backgrounds. Its implications can include chronic and serious functional impairment as well as protracted and often excessive health care utilization. A growing number of pharmacologic and nonpharmacologic interventions have become available and proven to be effective when appropriately deployed. As such, health care providers and particularly gastroenterologists should strive to develop logical and efficient strategies for addressing this common disorder.
Clinical importance
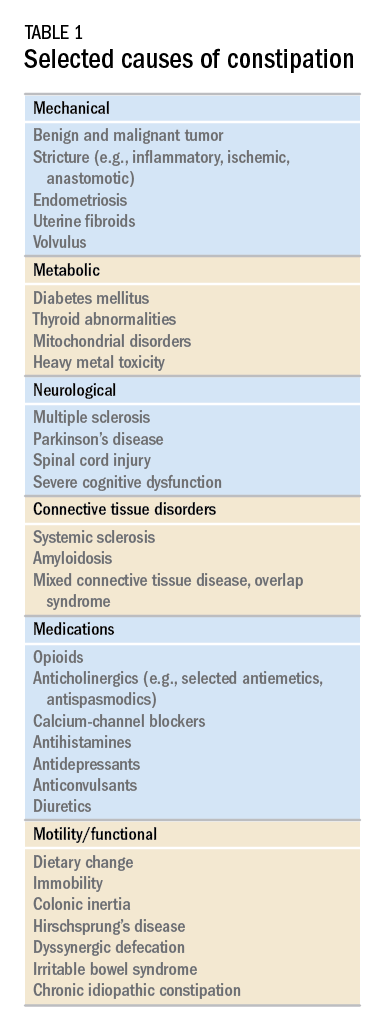
While there are a variety of etiologies for constipation (Table 1), a large proportion of chronic cases fall within the framework of functional gastrointestinal disorders, a category with a substantial burden of disease across the population. Prevalence estimates vary, but constipation likely affects between 12% and 20% of the North American population.1 Research has demonstrated significant health care expenditures associated with chronic constipation management; U.S. estimates suggest direct costs on the order of hundreds of millions of dollars per year, roughly half of which are attributable to inpatient care.2 The financial burden of constipation also includes indirect costs associated with absenteeism as well as the risks of hospitalization and invasive procedures.3

Physical and emotional complications can be likewise significant and affect all age groups, from newborns to patients in the last days of life. Hirschsprung’s disease, for example, can lead to life-threatening sequelae in infancy, such as spontaneous perforation or enterocolitis, or more prolonged functional impairments when it remains undiagnosed. Severe constipation in childhood can lead to encopresis, translating in turn into ostracism and impaired social functioning. Fecal incontinence associated with overflow diarrhea is common and debilitating, particularly in the elderly population.
The potential mechanical complications of constipation lead to its overlap with a variety of other gastrointestinal complaints. For example, the difficulties of passing inspissated stool can provoke lower gastrointestinal bleeding from irritated hemorrhoids, anal fissures, stercoral ulcers, or prolapsed rectal tissue. Retained stool can also lead to upper gastrointestinal symptoms such as postprandial bloating or early satiety.4 Delayed fecal discharge can promote an increase in fermentative microbiota, associated in turn with the production of short-chain fatty acids, methane, and other gaseous byproducts.
The initial assessment
History
Taking an appropriate history is an essential step toward achieving a successful outcome. Presenting concerns related to constipation can range from hard, infrequent, or small-volume stools; abdominal or rectal pain associated with the process of elimination; and bloating, nausea, or early satiety. A sound diagnosis requires a keen understanding of what patients mean when they indicate that they are constipated, an accurate assessment of its impact on quality of life, and a careful inventory of potentially associated complications.
It is critical to define the duration of the problem. Not infrequently, patients will focus on recent events while failing to reveal that altered bowel habits or other functional symptoms have been problematic for years. Reminding the patients to “begin at the beginning” can aid enormously in contextualizing their complaints. Individuals with longstanding symptoms and previously negative evaluations are much less likely to present with a new organic disease than are those in whom symptoms have truly arisen de novo.
Defining constipation by frequency of bowel eliminations alone has proved inaccurate at predicting actual severity. This is in part because the bowel movement frequency varies widely in healthy individuals (anywhere from thrice daily to once every 3 days) and in part because the primary indicator of effective evacuation is not frequency but volume – a much more difficult quantity for patients to gauge.5 The Bristol Stool Scale is a simple, standardized tool that more accurately evaluates the presence or absence of colonic dysfunction. For example, patients passing Type 1-2 (hard or lumpy) stools often have an element of constipation that needs to be addressed.6 However, the interpretation of stool consistency assessments is still aided by awareness of both frequency and volume. A patient passing multiple small-volume Type 6-7 (loose or watery) stools may be the most constipated, presenting with overflow or paradoxical diarrhea attributable to fecal impaction.
Physical examination
An expert physical exam is another essential aspect of the initial assessment. Alarm features can be elicited in this context as well via signs of pallor, weight loss, blood in the stool, physical abuse, or advanced psychological distress. Attention should also be paid to signs of a systemic disorder that might be associated with gastrointestinal dysmotility including previously unrecognized signs of Raynaud’s syndrome, sclerodactyly, amyloidosis, surgical scars, and joint hypermobility.7,8 Abdominal bloating, a frequently vague symptomatic complaint, can be correlated with the presence or absence of distention as perceived by the patient and/or the examiner.9
Any initial evaluation of constipation should also include a detailed digital rectal exam. A complete examination should include a careful visual assessment of the perianal region for external lesions and of the degree and directional appropriateness of pelvic floor excursion (perineal elevation and descent) during squeeze and simulated defecation maneuvers, respectively. Digital examination should include palpation for the presence or absence of pain as well as stool, blood, or masses in the rectal vault, as well as an assessment of sphincter tone at baseline, with squeeze, and with simulated defecation. Rectal pressure generation with the latter maneuver can also be qualitatively assessed. Research has suggested moderate agreement between the digital rectal examination and formal manometric evaluation in diagnosing dyssynergic defecation, underscoring the former’s utility in guiding initial management decisions.10
Testing
It is reasonable to exclude metabolic, inflammatory, or other secondary etiologies of constipation in patients in whom history or examination raises suspicion. Likewise, colonoscopy should be considered in patients with alarm features or who are due for age-appropriate screening. That said, in the absence of risk factors or ancillary signs and symptoms, a detailed diagnostic work-up is often unnecessary. The AGA’s Medical Position Statement on Constipation recommends a complete blood count as the only test to be ordered on a standard basis in the work-up of constipation.11
In patients new to one’s practice, the diligent retrieval of prior records is one of the most efficient ways to avoid wasting health care resources. Locating an old abdominal radiograph that demonstrates extensive retained stool can not only secure the diagnosis for vague symptomatic complaints but also obviate the need for more extensive testing. One should instead consider how symptom duration and the associated changes in objectives measures such as weight and laboratory parameters can be used to justify or refute the need for repeating costly or invasive studies.
It is important to consider the potential contribution of defecatory dyssynergy to chronic constipation early in a patient’s presentation, and to return to this possibility in the future if initial therapeutic interventions are unsuccessful. An abnormal qualitative assessment on digital rectal examination should trigger a more formal characterization of the patient’s defecatory mechanics via anorectal manometry (ARM) and balloon expulsion testing (BET). Likewise, a lack of response to initial pharmacotherapy should prompt suspicion for outlet dysfunction, which can be queried with functional testing even if a rectal examination is qualitatively unrevealing.
Initial approach to the chronically constipated patient
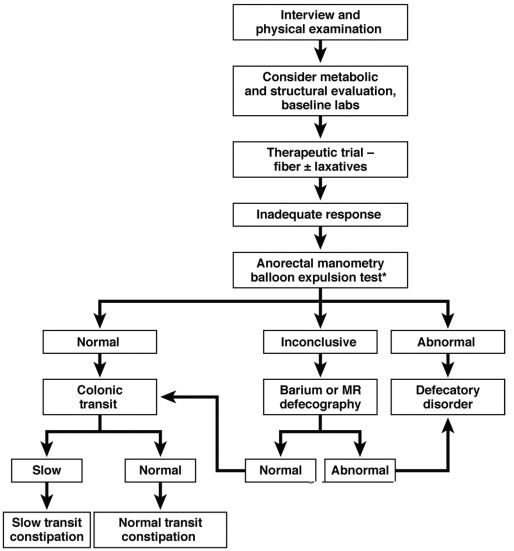
The aforementioned AGA Medical Position Statement provides a helpful algorithm regarding the diagnostic approach to constipation (Figure 1). In the absence of concern for secondary etiologies of constipation, an initial therapeutic trial of dietary, lifestyle, and medication-based intervention is reasonable for mild symptoms. Patients should be encouraged to strive for 25-30 grams of dietary fiber intake per day. For patients unable to reach this goal via high-fiber foods alone, psyllium husk is a popular supplement, but it should be initiated at modest doses to mitigate the risk of bloating. Fiber may be supplemented with the use of osmotic laxatives (e.g., polyethylene glycol) with instructions that the initial dose may be modified as needed to optimal effectiveness. Selective response to rectal therapies (e.g., bisacodyl or glycerin suppositories) over osmotic laxatives may also suggest utility in early queries of outlet dysfunction.
An abdominal radiograph can be helpful not only to diagnose constipation but also to assess the stool burden present at the time of beginning treatment. For patients presenting with a significant degree of fecal loading, an initial bowel cleanse with four liters of osmotically balanced polyethylene glycol can be a useful means of eliminating background fecal impactions that might have mitigated the effectiveness of initial therapies in the past or that might reduce the effectiveness of daily laxative therapy moving forward.
Patients with a diagnosis of defecatory dyssynergy made via ARM/BET should be referred to pelvic floor physical therapy with biofeedback. Recognizing that courses of therapy are highly individualized in practice, randomized controlled trials suggest symptom improvement in 70%-80% of patients, with the majority also demonstrating maintenance of response.12 Biofeedback appears to be an essential component of this modality based on meta-analysis data and should be requested specifically by the referring provider.13
Pharmacologic agents

For those patients with more severe initial presentations or whose symptoms persist despite initial medical management, there are several pharmacologic agents that may be considered on a prescription basis (Table 2). Linaclotide, a minimally absorbed guanylate cyclase agonist, is approved by the Food and Drug Administration for patients with irritable bowel syndrome with constipation (IBS-C) and chronic idiopathic constipation (CIC). Improvements in constipation tend to occur over a slightly shorter timeline than in abdominal pain, though both have been demonstrated in comparison to placebo.14,15 Plecanatide, a newer agent with a similar mechanism of action, has demonstrated improvements in bowel movement frequency and was recently approved for CIC.16 Lubiprostone, a chloride channel agonist, has demonstrated benefit for IBS-C and CIC as well, though its side effect profile is more varied, including dose-related nausea in up to 30% of patients.17
For patients with opioid-induced constipation who cannot wean from the opioid medications, the peripheral acting mu-opioid receptor antagonists may be quite helpful. These include injectable as well as oral formulations (e.g., methylnaltrexone and naloxegol, respectively) with additional agents under active investigation in particular clinical subsets (e.g., naldemedine for patients with cancer-related pain).18,19 Prucalopride, a selective serotonin receptor agonist, has also demonstrated benefit for constipation; it is available abroad but not yet approved for use in the United States.20 Prucalopride shares its primary mechanism of action (selective agonism of the 5HT4 serotonin receptor) with cisapride, a previously quite popular gastrointestinal motility agent that was subsequently withdrawn from the U.S. market because of arrhythmia risk.21 This risk is likely attributable to cisapride’s dual binding affinity for potassium channels, a feature that prucalopride does not share; as such, cardiotoxicity is not an active concern with the latter agent.22
Still other pharmacologic agents with novel mechanisms of action are currently under investigation. Tenapanor, an inhibitor of a particular sodium/potassium exchanger in the gut lumen, mitigates intestinal sodium absorption, which increases fluid volume and transit. A recent phase 2 study demonstrated significantly increased stool frequency relative to placebo in patients with IBS-C.23 Elobixibat, an ileal bile acid transport inhibitor, promotes colonic retention of bile acids and, in placebo-controlled studies, has led to accelerated colonic transit and an increased number of spontaneous bowel movements in patients with CIC.24
Persistent constipation
In cases of refractory constipation (in practical terms, symptoms that persist despite trials of escalating medical therapy over at least 6 weeks), it is worth revisiting the question of etiology. Querying defecatory dyssynergy via ARM/BET, if not pursued prior to trials of newer pharmacologic agents, should certainly be explored in the event that such trials fail. Inconclusive results of ARM and BET testing, or BET abnormalities that persist despite a course of physical therapy with biofeedback, may raise suspicion for pelvic organ prolapse, which may be formally evaluated with defecography. Additional testing for metabolic or structural predispositions toward constipation may also be reasonable at this juncture.
Formal colonic transit testing via radio-opaque markers, scintigraphy, or the wireless motility capsule is often inaccurate in the setting of dyssynergic defecation and should be pursued only after this entity has been excluded or successfully treated.25 While there are not many practical distinctions at present in the therapeutic management of slow-transit versus normal-transit constipation, the use of novel medications with an explicitly prokinetic mechanism of action may be reasonable to consider in the setting of a document delay in colonic transit. Such delays can also help justify further specialized diagnostic testing (e.g., colonic manometry), and, in rare refractory cases, surgical intervention.
Consideration of colectomy should be reserved for highly selected patients with delayed colonic transit, normal defecatory mechanics, and the absence of potentially explanatory background conditions (e.g., connective tissue disease). Clear evidence of an underlying colonic myopathy or neuropathy may militate in favor of a more targeted surgical intervention (e.g., subtotal colectomy) or guide one’s clinical evaluation toward alternative systemic diagnoses. A diverting loop ileostomy with interval assessment of symptoms may be useful to clarify the potential benefits of colectomy while preserving the option of operative reversal. Proximal transit delays should be definitively excluded before pursuing colonic resections given evidence that multisegment transit delays portend significantly worse postoperative outcomes.26
Conclusion
Constipation is a common, sometimes confusing presenting complaint and the variety of established and emergent options for diagnosis and therapy can lend themselves to haphazard application. Patients and providers both are well served by a clinical approach, rooted in a comprehensive history and examination, that begins to organize these options in thoughtful sequence.
Dr. Ahuja is assistant professor of clinical medicine, division of gastroenterology; Dr. Reynolds is professor of clinical medicine, and director of the program in neurogastroenterology and motility, division of gastroenterology, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
References
1. Higgins P.D., Johanson J.F. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004 Apr;99(4):750-9. PubMed PMID: 15089911.
2. Martin B.C., Barghout V., Cerulli A. Direct medical costs of constipation in the United States. Manage Care Interface. 2006 Dec;19(12):43-9. PubMed PMID: 17274481.
3. Sun S.X., Dibonaventura M., Purayidathil F.W., et al. Impact of chronic constipation on health-related quality of life, work productivity, and healthcare resource use: an analysis of the National Health and Wellness Survey. Dig Dis Sc. 2011 Sep;56(9):2688-95. PubMed PMID: 21380761.
4. Heidelbaugh J.J., Stelwagon M., Miller S.A., et al. The spectrum of constipation-predominant irritable bowel syndrome and chronic idiopathic constipation: US survey assessing symptoms, care seeking, and disease burden. Am J Gastroenterol. 2015 Apr;110(4):580-7.
5. Mitsuhashi S., Ballou S., Jiang Z.G., et al. Characterizing normal bowel frequency and consistency in a representative sample of adults in the United States (NHANES). Am J Gastroenterol. 2017 Aug 01. PubMed PMID: 28762379.
6. Saad R.J., Rao S.S., Koch K.L., et al. Do stool form and frequency correlate with whole-gut and colonic transit? Results from a multicenter study in constipated individuals and healthy controls. Am J Gastroenterol. 2010 Feb;105(2):403-11. PubMed PMID: 19888202.
7. Castori M., Morlino S., Pascolini G., et al. Gastrointestinal and nutritional issues in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type. American Journal of Medical Genetics Part C, Semin Med Genet. 2015 Mar;169C(1):54-75. PubMed PMID: 25821092.
8. Nagaraja V., McMahan Z.H., Getzug T., Khanna D. Management of gastrointestinal involvement in scleroderma. Curr Treatm Opt Rheumatol. 2015 Mar 01;1(1):82-105. PubMed PMID: 26005632. Pubmed Central PMCID: 4437639.
9. Malagelada J.R., Accarino A., Azpiroz F. Bloating and abdominal distension: Old misconceptions and current knowledge. Am J Gastroenterol. 2017 Aug;112(8):1221-31. PubMed PMID: 28508867.
10. Soh J.S., Lee H.J., Jung K.W., et al. The diagnostic value of a digital rectal examination compared with high-resolution anorectal manometry in patients with chronic constipation and fecal incontinence. Am J Gastroenterol. 2015 Aug;110(8):1197-204. PubMed PMID: 26032152.
11. American Gastroenterological Association, Bharucha A.E., Dorn S.D., Lembo A., Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013 Jan;144(1):211-7. PubMed PMID: 23261064.
12. Skardoon G.R., Khera A.J., Emmanuel A.V., Burgell R.E. Review article: dyssynergic defaecation and biofeedback therapy in the pathophysiology and management of functional constipation. Aliment Pharmacol Therapeut. 2017 Aug;46(4):410-23. PubMed PMID: 28660663.
13. Koh C.E., Young C.J., Young J.M., Solomon M.J. Systematic review of randomized controlled trials of the effectiveness of biofeedback for pelvic floor dysfunction. Br J Surg. 2008 Sep;95(9):1079-87. PubMed PMID: 18655219.
14. Rao S., Lembo A.J., Shiff S.J., et al. A 12-week, randomized, controlled trial with a 4-week randomized withdrawal period to evaluate the efficacy and safety of linaclotide in irritable bowel syndrome with constipation. Am J Gastroenterol. 2012 Nov;107(11):1714-24; quiz p 25. PubMed PMID: 22986440. Pubmed Central PMCID: 3504311.
15. Lacy B.E., Schey R., Shiff S.J., et al. Linaclotide in chronic idiopathic constipation patients with moderate to severe abdominal bloating: A randomized, controlled trial. PloS One. 2015;10(7):e0134349. PubMed PMID: 26222318. Pubmed Central PMCID: 4519259.
16. Miner P.B., Jr., Koltun W.D., Wiener G.J., et al. A randomized phase III clinical trial of plecanatide, a uroguanylin analog, in patients with chronic idiopathic constipation. Am J Gastroenterol. 2017 Apr;112(4):613-21. PubMed PMID: 28169285. Pubmed Central PMCID: 5415706.
17. Johanson J.F., Drossman D.A., Panas R., Wahle A., Ueno R. Clinical trial: phase 2 study of lubiprostone for irritable bowel syndrome with constipation. Aliment Pharmacol Therapeut. 2008 Apr;27(8):685-96. PubMed PMID: 18248656.
18. Chey W.D., Webster L., Sostek M., Lappalainen J., Barker P.N., Tack J. Naloxegol for opioid-induced constipation in patients with noncancer pain. N Engl J Med. 2014 Jun 19;370(25):2387-96. PubMed PMID: 24896818.
19. Katakami N., Oda K., Tauchi K., et al. Phase IIb, randomized, double-blind, placebo-controlled study of naldemedine for the treatment of opioid-induced constipation in patients with cancer. J Clin Oncol. 2017 Jun 10;35(17):1921-8. PubMed PMID: 28445097.
20. Sajid M.S., Hebbar M., Baig M.K., Li A., Philipose Z. Use of prucalopride for chronic constipation: A systematic review and meta-analysis of published randomized, controlled trials. J Neurogastroenterol Motil. 2016 Jul 30;22(3):412-22. PubMed PMID: 27127190. Pubmed Central PMCID: 4930296.
21. Quigley E.M. Cisapride: What can we learn from the rise and fall of a prokinetic? J Dig Dis. 2011 Jun;12(3):147-56. PubMed PMID: 21615867.
22. Conlon K., De Maeyer J.H., Bruce C., et al. Nonclinical cardiovascular studies of prucalopride, a highly selective 5-hydroxytryptamine 4 receptor agonist. J Pharmacol Exp Therapeut. 2017 Nov; doi: 10.1124/jpet.117.244079 [epub ahead of print].
23. Chey W.D., Lembo A.J., Rosenbaum D.P. Tenapanor treatment of patients with constipation-predominant irritable bowel syndrome: a phase 2, randomized, placebo-controlled efficacy and safety trial. Am J Gastroenterol. 2017;112:763-74.
24. Simren M., Bajor A., Gillberg P-G, Rudling M., Abrahamsson H. Randomised clinical trial: the ileal bile acid transporter inhibitor A3309 vs. placebo in patients with chronic idiopathic constipation – a double-blind study. Aliment Pharmacol Ther. 2011 Jul;34(1):41-50.
25. Zarate N., Knowles C.H., Newell M., et al. In patients with slow transit constipation, the pattern of colonic transit delay does not differentiate between those with and without impaired rectal evacuation. Am J Gastroenterol. 2008 Feb;103(2):427-34. PubMed PMID: 18070233.
26. Redmond J.M., Smith G.W., Barofsky I., et al. Physiological tests to predict long-term outcome of total abdominal colectomy for intractable constipation. Am J Gastroenterol. 1995 May;90(5):748-53. PubMed PMID: 7733081.
While constipation is one of the most common symptoms managed by practicing gastroenterologists, it can also be among the most challenging. As a presenting complaint, constipation manifests with widely varying degrees of severity and may be seen in all age groups, ethnicities, and socioeconomic backgrounds. Its implications can include chronic and serious functional impairment as well as protracted and often excessive health care utilization. A growing number of pharmacologic and nonpharmacologic interventions have become available and proven to be effective when appropriately deployed. As such, health care providers and particularly gastroenterologists should strive to develop logical and efficient strategies for addressing this common disorder.
Clinical importance
While there are a variety of etiologies for constipation (Table 1), a large proportion of chronic cases fall within the framework of functional gastrointestinal disorders, a category with a substantial burden of disease across the population. Prevalence estimates vary, but constipation likely affects between 12% and 20% of the North American population.1 Research has demonstrated significant health care expenditures associated with chronic constipation management; U.S. estimates suggest direct costs on the order of hundreds of millions of dollars per year, roughly half of which are attributable to inpatient care.2 The financial burden of constipation also includes indirect costs associated with absenteeism as well as the risks of hospitalization and invasive procedures.3
Physical and emotional complications can be likewise significant and affect all age groups, from newborns to patients in the last days of life. Hirschsprung’s disease, for example, can lead to life-threatening sequelae in infancy, such as spontaneous perforation or enterocolitis, or more prolonged functional impairments when it remains undiagnosed. Severe constipation in childhood can lead to encopresis, translating in turn into ostracism and impaired social functioning. Fecal incontinence associated with overflow diarrhea is common and debilitating, particularly in the elderly population.
The potential mechanical complications of constipation lead to its overlap with a variety of other gastrointestinal complaints. For example, the difficulties of passing inspissated stool can provoke lower gastrointestinal bleeding from irritated hemorrhoids, anal fissures, stercoral ulcers, or prolapsed rectal tissue. Retained stool can also lead to upper gastrointestinal symptoms such as postprandial bloating or early satiety.4 Delayed fecal discharge can promote an increase in fermentative microbiota, associated in turn with the production of short-chain fatty acids, methane, and other gaseous byproducts.
The initial assessment
History
Taking an appropriate history is an essential step toward achieving a successful outcome. Presenting concerns related to constipation can range from hard, infrequent, or small-volume stools; abdominal or rectal pain associated with the process of elimination; and bloating, nausea, or early satiety. A sound diagnosis requires a keen understanding of what patients mean when they indicate that they are constipated, an accurate assessment of its impact on quality of life, and a careful inventory of potentially associated complications.
It is critical to define the duration of the problem. Not infrequently, patients will focus on recent events while failing to reveal that altered bowel habits or other functional symptoms have been problematic for years. Reminding the patients to “begin at the beginning” can aid enormously in contextualizing their complaints. Individuals with longstanding symptoms and previously negative evaluations are much less likely to present with a new organic disease than are those in whom symptoms have truly arisen de novo.
Defining constipation by frequency of bowel eliminations alone has proved inaccurate at predicting actual severity. This is in part because the bowel movement frequency varies widely in healthy individuals (anywhere from thrice daily to once every 3 days) and in part because the primary indicator of effective evacuation is not frequency but volume – a much more difficult quantity for patients to gauge.5 The Bristol Stool Scale is a simple, standardized tool that more accurately evaluates the presence or absence of colonic dysfunction. For example, patients passing Type 1-2 (hard or lumpy) stools often have an element of constipation that needs to be addressed.6 However, the interpretation of stool consistency assessments is still aided by awareness of both frequency and volume. A patient passing multiple small-volume Type 6-7 (loose or watery) stools may be the most constipated, presenting with overflow or paradoxical diarrhea attributable to fecal impaction.
Physical examination
An expert physical exam is another essential aspect of the initial assessment. Alarm features can be elicited in this context as well via signs of pallor, weight loss, blood in the stool, physical abuse, or advanced psychological distress. Attention should also be paid to signs of a systemic disorder that might be associated with gastrointestinal dysmotility including previously unrecognized signs of Raynaud’s syndrome, sclerodactyly, amyloidosis, surgical scars, and joint hypermobility.7,8 Abdominal bloating, a frequently vague symptomatic complaint, can be correlated with the presence or absence of distention as perceived by the patient and/or the examiner.9
Any initial evaluation of constipation should also include a detailed digital rectal exam. A complete examination should include a careful visual assessment of the perianal region for external lesions and of the degree and directional appropriateness of pelvic floor excursion (perineal elevation and descent) during squeeze and simulated defecation maneuvers, respectively. Digital examination should include palpation for the presence or absence of pain as well as stool, blood, or masses in the rectal vault, as well as an assessment of sphincter tone at baseline, with squeeze, and with simulated defecation. Rectal pressure generation with the latter maneuver can also be qualitatively assessed. Research has suggested moderate agreement between the digital rectal examination and formal manometric evaluation in diagnosing dyssynergic defecation, underscoring the former’s utility in guiding initial management decisions.10
Testing
It is reasonable to exclude metabolic, inflammatory, or other secondary etiologies of constipation in patients in whom history or examination raises suspicion. Likewise, colonoscopy should be considered in patients with alarm features or who are due for age-appropriate screening. That said, in the absence of risk factors or ancillary signs and symptoms, a detailed diagnostic work-up is often unnecessary. The AGA’s Medical Position Statement on Constipation recommends a complete blood count as the only test to be ordered on a standard basis in the work-up of constipation.11
In patients new to one’s practice, the diligent retrieval of prior records is one of the most efficient ways to avoid wasting health care resources. Locating an old abdominal radiograph that demonstrates extensive retained stool can not only secure the diagnosis for vague symptomatic complaints but also obviate the need for more extensive testing. One should instead consider how symptom duration and the associated changes in objectives measures such as weight and laboratory parameters can be used to justify or refute the need for repeating costly or invasive studies.
It is important to consider the potential contribution of defecatory dyssynergy to chronic constipation early in a patient’s presentation, and to return to this possibility in the future if initial therapeutic interventions are unsuccessful. An abnormal qualitative assessment on digital rectal examination should trigger a more formal characterization of the patient’s defecatory mechanics via anorectal manometry (ARM) and balloon expulsion testing (BET). Likewise, a lack of response to initial pharmacotherapy should prompt suspicion for outlet dysfunction, which can be queried with functional testing even if a rectal examination is qualitatively unrevealing.
Initial approach to the chronically constipated patient
The aforementioned AGA Medical Position Statement provides a helpful algorithm regarding the diagnostic approach to constipation (Figure 1). In the absence of concern for secondary etiologies of constipation, an initial therapeutic trial of dietary, lifestyle, and medication-based intervention is reasonable for mild symptoms. Patients should be encouraged to strive for 25-30 grams of dietary fiber intake per day. For patients unable to reach this goal via high-fiber foods alone, psyllium husk is a popular supplement, but it should be initiated at modest doses to mitigate the risk of bloating. Fiber may be supplemented with the use of osmotic laxatives (e.g., polyethylene glycol) with instructions that the initial dose may be modified as needed to optimal effectiveness. Selective response to rectal therapies (e.g., bisacodyl or glycerin suppositories) over osmotic laxatives may also suggest utility in early queries of outlet dysfunction.
An abdominal radiograph can be helpful not only to diagnose constipation but also to assess the stool burden present at the time of beginning treatment. For patients presenting with a significant degree of fecal loading, an initial bowel cleanse with four liters of osmotically balanced polyethylene glycol can be a useful means of eliminating background fecal impactions that might have mitigated the effectiveness of initial therapies in the past or that might reduce the effectiveness of daily laxative therapy moving forward.
Patients with a diagnosis of defecatory dyssynergy made via ARM/BET should be referred to pelvic floor physical therapy with biofeedback. Recognizing that courses of therapy are highly individualized in practice, randomized controlled trials suggest symptom improvement in 70%-80% of patients, with the majority also demonstrating maintenance of response.12 Biofeedback appears to be an essential component of this modality based on meta-analysis data and should be requested specifically by the referring provider.13
Pharmacologic agents
For those patients with more severe initial presentations or whose symptoms persist despite initial medical management, there are several pharmacologic agents that may be considered on a prescription basis (Table 2). Linaclotide, a minimally absorbed guanylate cyclase agonist, is approved by the Food and Drug Administration for patients with irritable bowel syndrome with constipation (IBS-C) and chronic idiopathic constipation (CIC). Improvements in constipation tend to occur over a slightly shorter timeline than in abdominal pain, though both have been demonstrated in comparison to placebo.14,15 Plecanatide, a newer agent with a similar mechanism of action, has demonstrated improvements in bowel movement frequency and was recently approved for CIC.16 Lubiprostone, a chloride channel agonist, has demonstrated benefit for IBS-C and CIC as well, though its side effect profile is more varied, including dose-related nausea in up to 30% of patients.17
For patients with opioid-induced constipation who cannot wean from the opioid medications, the peripheral acting mu-opioid receptor antagonists may be quite helpful. These include injectable as well as oral formulations (e.g., methylnaltrexone and naloxegol, respectively) with additional agents under active investigation in particular clinical subsets (e.g., naldemedine for patients with cancer-related pain).18,19 Prucalopride, a selective serotonin receptor agonist, has also demonstrated benefit for constipation; it is available abroad but not yet approved for use in the United States.20 Prucalopride shares its primary mechanism of action (selective agonism of the 5HT4 serotonin receptor) with cisapride, a previously quite popular gastrointestinal motility agent that was subsequently withdrawn from the U.S. market because of arrhythmia risk.21 This risk is likely attributable to cisapride’s dual binding affinity for potassium channels, a feature that prucalopride does not share; as such, cardiotoxicity is not an active concern with the latter agent.22
Still other pharmacologic agents with novel mechanisms of action are currently under investigation. Tenapanor, an inhibitor of a particular sodium/potassium exchanger in the gut lumen, mitigates intestinal sodium absorption, which increases fluid volume and transit. A recent phase 2 study demonstrated significantly increased stool frequency relative to placebo in patients with IBS-C.23 Elobixibat, an ileal bile acid transport inhibitor, promotes colonic retention of bile acids and, in placebo-controlled studies, has led to accelerated colonic transit and an increased number of spontaneous bowel movements in patients with CIC.24
Persistent constipation
In cases of refractory constipation (in practical terms, symptoms that persist despite trials of escalating medical therapy over at least 6 weeks), it is worth revisiting the question of etiology. Querying defecatory dyssynergy via ARM/BET, if not pursued prior to trials of newer pharmacologic agents, should certainly be explored in the event that such trials fail. Inconclusive results of ARM and BET testing, or BET abnormalities that persist despite a course of physical therapy with biofeedback, may raise suspicion for pelvic organ prolapse, which may be formally evaluated with defecography. Additional testing for metabolic or structural predispositions toward constipation may also be reasonable at this juncture.
Formal colonic transit testing via radio-opaque markers, scintigraphy, or the wireless motility capsule is often inaccurate in the setting of dyssynergic defecation and should be pursued only after this entity has been excluded or successfully treated.25 While there are not many practical distinctions at present in the therapeutic management of slow-transit versus normal-transit constipation, the use of novel medications with an explicitly prokinetic mechanism of action may be reasonable to consider in the setting of a document delay in colonic transit. Such delays can also help justify further specialized diagnostic testing (e.g., colonic manometry), and, in rare refractory cases, surgical intervention.
Consideration of colectomy should be reserved for highly selected patients with delayed colonic transit, normal defecatory mechanics, and the absence of potentially explanatory background conditions (e.g., connective tissue disease). Clear evidence of an underlying colonic myopathy or neuropathy may militate in favor of a more targeted surgical intervention (e.g., subtotal colectomy) or guide one’s clinical evaluation toward alternative systemic diagnoses. A diverting loop ileostomy with interval assessment of symptoms may be useful to clarify the potential benefits of colectomy while preserving the option of operative reversal. Proximal transit delays should be definitively excluded before pursuing colonic resections given evidence that multisegment transit delays portend significantly worse postoperative outcomes.26
Conclusion
Constipation is a common, sometimes confusing presenting complaint and the variety of established and emergent options for diagnosis and therapy can lend themselves to haphazard application. Patients and providers both are well served by a clinical approach, rooted in a comprehensive history and examination, that begins to organize these options in thoughtful sequence.
Dr. Ahuja is assistant professor of clinical medicine, division of gastroenterology; Dr. Reynolds is professor of clinical medicine, and director of the program in neurogastroenterology and motility, division of gastroenterology, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
References
1. Higgins P.D., Johanson J.F. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004 Apr;99(4):750-9. PubMed PMID: 15089911.
2. Martin B.C., Barghout V., Cerulli A. Direct medical costs of constipation in the United States. Manage Care Interface. 2006 Dec;19(12):43-9. PubMed PMID: 17274481.
3. Sun S.X., Dibonaventura M., Purayidathil F.W., et al. Impact of chronic constipation on health-related quality of life, work productivity, and healthcare resource use: an analysis of the National Health and Wellness Survey. Dig Dis Sc. 2011 Sep;56(9):2688-95. PubMed PMID: 21380761.
4. Heidelbaugh J.J., Stelwagon M., Miller S.A., et al. The spectrum of constipation-predominant irritable bowel syndrome and chronic idiopathic constipation: US survey assessing symptoms, care seeking, and disease burden. Am J Gastroenterol. 2015 Apr;110(4):580-7.
5. Mitsuhashi S., Ballou S., Jiang Z.G., et al. Characterizing normal bowel frequency and consistency in a representative sample of adults in the United States (NHANES). Am J Gastroenterol. 2017 Aug 01. PubMed PMID: 28762379.
6. Saad R.J., Rao S.S., Koch K.L., et al. Do stool form and frequency correlate with whole-gut and colonic transit? Results from a multicenter study in constipated individuals and healthy controls. Am J Gastroenterol. 2010 Feb;105(2):403-11. PubMed PMID: 19888202.
7. Castori M., Morlino S., Pascolini G., et al. Gastrointestinal and nutritional issues in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type. American Journal of Medical Genetics Part C, Semin Med Genet. 2015 Mar;169C(1):54-75. PubMed PMID: 25821092.
8. Nagaraja V., McMahan Z.H., Getzug T., Khanna D. Management of gastrointestinal involvement in scleroderma. Curr Treatm Opt Rheumatol. 2015 Mar 01;1(1):82-105. PubMed PMID: 26005632. Pubmed Central PMCID: 4437639.
9. Malagelada J.R., Accarino A., Azpiroz F. Bloating and abdominal distension: Old misconceptions and current knowledge. Am J Gastroenterol. 2017 Aug;112(8):1221-31. PubMed PMID: 28508867.
10. Soh J.S., Lee H.J., Jung K.W., et al. The diagnostic value of a digital rectal examination compared with high-resolution anorectal manometry in patients with chronic constipation and fecal incontinence. Am J Gastroenterol. 2015 Aug;110(8):1197-204. PubMed PMID: 26032152.
11. American Gastroenterological Association, Bharucha A.E., Dorn S.D., Lembo A., Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013 Jan;144(1):211-7. PubMed PMID: 23261064.
12. Skardoon G.R., Khera A.J., Emmanuel A.V., Burgell R.E. Review article: dyssynergic defaecation and biofeedback therapy in the pathophysiology and management of functional constipation. Aliment Pharmacol Therapeut. 2017 Aug;46(4):410-23. PubMed PMID: 28660663.
13. Koh C.E., Young C.J., Young J.M., Solomon M.J. Systematic review of randomized controlled trials of the effectiveness of biofeedback for pelvic floor dysfunction. Br J Surg. 2008 Sep;95(9):1079-87. PubMed PMID: 18655219.
14. Rao S., Lembo A.J., Shiff S.J., et al. A 12-week, randomized, controlled trial with a 4-week randomized withdrawal period to evaluate the efficacy and safety of linaclotide in irritable bowel syndrome with constipation. Am J Gastroenterol. 2012 Nov;107(11):1714-24; quiz p 25. PubMed PMID: 22986440. Pubmed Central PMCID: 3504311.
15. Lacy B.E., Schey R., Shiff S.J., et al. Linaclotide in chronic idiopathic constipation patients with moderate to severe abdominal bloating: A randomized, controlled trial. PloS One. 2015;10(7):e0134349. PubMed PMID: 26222318. Pubmed Central PMCID: 4519259.
16. Miner P.B., Jr., Koltun W.D., Wiener G.J., et al. A randomized phase III clinical trial of plecanatide, a uroguanylin analog, in patients with chronic idiopathic constipation. Am J Gastroenterol. 2017 Apr;112(4):613-21. PubMed PMID: 28169285. Pubmed Central PMCID: 5415706.
17. Johanson J.F., Drossman D.A., Panas R., Wahle A., Ueno R. Clinical trial: phase 2 study of lubiprostone for irritable bowel syndrome with constipation. Aliment Pharmacol Therapeut. 2008 Apr;27(8):685-96. PubMed PMID: 18248656.
18. Chey W.D., Webster L., Sostek M., Lappalainen J., Barker P.N., Tack J. Naloxegol for opioid-induced constipation in patients with noncancer pain. N Engl J Med. 2014 Jun 19;370(25):2387-96. PubMed PMID: 24896818.
19. Katakami N., Oda K., Tauchi K., et al. Phase IIb, randomized, double-blind, placebo-controlled study of naldemedine for the treatment of opioid-induced constipation in patients with cancer. J Clin Oncol. 2017 Jun 10;35(17):1921-8. PubMed PMID: 28445097.
20. Sajid M.S., Hebbar M., Baig M.K., Li A., Philipose Z. Use of prucalopride for chronic constipation: A systematic review and meta-analysis of published randomized, controlled trials. J Neurogastroenterol Motil. 2016 Jul 30;22(3):412-22. PubMed PMID: 27127190. Pubmed Central PMCID: 4930296.
21. Quigley E.M. Cisapride: What can we learn from the rise and fall of a prokinetic? J Dig Dis. 2011 Jun;12(3):147-56. PubMed PMID: 21615867.
22. Conlon K., De Maeyer J.H., Bruce C., et al. Nonclinical cardiovascular studies of prucalopride, a highly selective 5-hydroxytryptamine 4 receptor agonist. J Pharmacol Exp Therapeut. 2017 Nov; doi: 10.1124/jpet.117.244079 [epub ahead of print].
23. Chey W.D., Lembo A.J., Rosenbaum D.P. Tenapanor treatment of patients with constipation-predominant irritable bowel syndrome: a phase 2, randomized, placebo-controlled efficacy and safety trial. Am J Gastroenterol. 2017;112:763-74.
24. Simren M., Bajor A., Gillberg P-G, Rudling M., Abrahamsson H. Randomised clinical trial: the ileal bile acid transporter inhibitor A3309 vs. placebo in patients with chronic idiopathic constipation – a double-blind study. Aliment Pharmacol Ther. 2011 Jul;34(1):41-50.
25. Zarate N., Knowles C.H., Newell M., et al. In patients with slow transit constipation, the pattern of colonic transit delay does not differentiate between those with and without impaired rectal evacuation. Am J Gastroenterol. 2008 Feb;103(2):427-34. PubMed PMID: 18070233.
26. Redmond J.M., Smith G.W., Barofsky I., et al. Physiological tests to predict long-term outcome of total abdominal colectomy for intractable constipation. Am J Gastroenterol. 1995 May;90(5):748-53. PubMed PMID: 7733081.
While constipation is one of the most common symptoms managed by practicing gastroenterologists, it can also be among the most challenging. As a presenting complaint, constipation manifests with widely varying degrees of severity and may be seen in all age groups, ethnicities, and socioeconomic backgrounds. Its implications can include chronic and serious functional impairment as well as protracted and often excessive health care utilization. A growing number of pharmacologic and nonpharmacologic interventions have become available and proven to be effective when appropriately deployed. As such, health care providers and particularly gastroenterologists should strive to develop logical and efficient strategies for addressing this common disorder.
Clinical importance
While there are a variety of etiologies for constipation (Table 1), a large proportion of chronic cases fall within the framework of functional gastrointestinal disorders, a category with a substantial burden of disease across the population. Prevalence estimates vary, but constipation likely affects between 12% and 20% of the North American population.1 Research has demonstrated significant health care expenditures associated with chronic constipation management; U.S. estimates suggest direct costs on the order of hundreds of millions of dollars per year, roughly half of which are attributable to inpatient care.2 The financial burden of constipation also includes indirect costs associated with absenteeism as well as the risks of hospitalization and invasive procedures.3
Physical and emotional complications can be likewise significant and affect all age groups, from newborns to patients in the last days of life. Hirschsprung’s disease, for example, can lead to life-threatening sequelae in infancy, such as spontaneous perforation or enterocolitis, or more prolonged functional impairments when it remains undiagnosed. Severe constipation in childhood can lead to encopresis, translating in turn into ostracism and impaired social functioning. Fecal incontinence associated with overflow diarrhea is common and debilitating, particularly in the elderly population.
The potential mechanical complications of constipation lead to its overlap with a variety of other gastrointestinal complaints. For example, the difficulties of passing inspissated stool can provoke lower gastrointestinal bleeding from irritated hemorrhoids, anal fissures, stercoral ulcers, or prolapsed rectal tissue. Retained stool can also lead to upper gastrointestinal symptoms such as postprandial bloating or early satiety.4 Delayed fecal discharge can promote an increase in fermentative microbiota, associated in turn with the production of short-chain fatty acids, methane, and other gaseous byproducts.
The initial assessment
History
Taking an appropriate history is an essential step toward achieving a successful outcome. Presenting concerns related to constipation can range from hard, infrequent, or small-volume stools; abdominal or rectal pain associated with the process of elimination; and bloating, nausea, or early satiety. A sound diagnosis requires a keen understanding of what patients mean when they indicate that they are constipated, an accurate assessment of its impact on quality of life, and a careful inventory of potentially associated complications.
It is critical to define the duration of the problem. Not infrequently, patients will focus on recent events while failing to reveal that altered bowel habits or other functional symptoms have been problematic for years. Reminding the patients to “begin at the beginning” can aid enormously in contextualizing their complaints. Individuals with longstanding symptoms and previously negative evaluations are much less likely to present with a new organic disease than are those in whom symptoms have truly arisen de novo.
Defining constipation by frequency of bowel eliminations alone has proved inaccurate at predicting actual severity. This is in part because the bowel movement frequency varies widely in healthy individuals (anywhere from thrice daily to once every 3 days) and in part because the primary indicator of effective evacuation is not frequency but volume – a much more difficult quantity for patients to gauge.5 The Bristol Stool Scale is a simple, standardized tool that more accurately evaluates the presence or absence of colonic dysfunction. For example, patients passing Type 1-2 (hard or lumpy) stools often have an element of constipation that needs to be addressed.6 However, the interpretation of stool consistency assessments is still aided by awareness of both frequency and volume. A patient passing multiple small-volume Type 6-7 (loose or watery) stools may be the most constipated, presenting with overflow or paradoxical diarrhea attributable to fecal impaction.
Physical examination
An expert physical exam is another essential aspect of the initial assessment. Alarm features can be elicited in this context as well via signs of pallor, weight loss, blood in the stool, physical abuse, or advanced psychological distress. Attention should also be paid to signs of a systemic disorder that might be associated with gastrointestinal dysmotility including previously unrecognized signs of Raynaud’s syndrome, sclerodactyly, amyloidosis, surgical scars, and joint hypermobility.7,8 Abdominal bloating, a frequently vague symptomatic complaint, can be correlated with the presence or absence of distention as perceived by the patient and/or the examiner.9
Any initial evaluation of constipation should also include a detailed digital rectal exam. A complete examination should include a careful visual assessment of the perianal region for external lesions and of the degree and directional appropriateness of pelvic floor excursion (perineal elevation and descent) during squeeze and simulated defecation maneuvers, respectively. Digital examination should include palpation for the presence or absence of pain as well as stool, blood, or masses in the rectal vault, as well as an assessment of sphincter tone at baseline, with squeeze, and with simulated defecation. Rectal pressure generation with the latter maneuver can also be qualitatively assessed. Research has suggested moderate agreement between the digital rectal examination and formal manometric evaluation in diagnosing dyssynergic defecation, underscoring the former’s utility in guiding initial management decisions.10
Testing
It is reasonable to exclude metabolic, inflammatory, or other secondary etiologies of constipation in patients in whom history or examination raises suspicion. Likewise, colonoscopy should be considered in patients with alarm features or who are due for age-appropriate screening. That said, in the absence of risk factors or ancillary signs and symptoms, a detailed diagnostic work-up is often unnecessary. The AGA’s Medical Position Statement on Constipation recommends a complete blood count as the only test to be ordered on a standard basis in the work-up of constipation.11
In patients new to one’s practice, the diligent retrieval of prior records is one of the most efficient ways to avoid wasting health care resources. Locating an old abdominal radiograph that demonstrates extensive retained stool can not only secure the diagnosis for vague symptomatic complaints but also obviate the need for more extensive testing. One should instead consider how symptom duration and the associated changes in objectives measures such as weight and laboratory parameters can be used to justify or refute the need for repeating costly or invasive studies.
It is important to consider the potential contribution of defecatory dyssynergy to chronic constipation early in a patient’s presentation, and to return to this possibility in the future if initial therapeutic interventions are unsuccessful. An abnormal qualitative assessment on digital rectal examination should trigger a more formal characterization of the patient’s defecatory mechanics via anorectal manometry (ARM) and balloon expulsion testing (BET). Likewise, a lack of response to initial pharmacotherapy should prompt suspicion for outlet dysfunction, which can be queried with functional testing even if a rectal examination is qualitatively unrevealing.
Initial approach to the chronically constipated patient
The aforementioned AGA Medical Position Statement provides a helpful algorithm regarding the diagnostic approach to constipation (Figure 1). In the absence of concern for secondary etiologies of constipation, an initial therapeutic trial of dietary, lifestyle, and medication-based intervention is reasonable for mild symptoms. Patients should be encouraged to strive for 25-30 grams of dietary fiber intake per day. For patients unable to reach this goal via high-fiber foods alone, psyllium husk is a popular supplement, but it should be initiated at modest doses to mitigate the risk of bloating. Fiber may be supplemented with the use of osmotic laxatives (e.g., polyethylene glycol) with instructions that the initial dose may be modified as needed to optimal effectiveness. Selective response to rectal therapies (e.g., bisacodyl or glycerin suppositories) over osmotic laxatives may also suggest utility in early queries of outlet dysfunction.
An abdominal radiograph can be helpful not only to diagnose constipation but also to assess the stool burden present at the time of beginning treatment. For patients presenting with a significant degree of fecal loading, an initial bowel cleanse with four liters of osmotically balanced polyethylene glycol can be a useful means of eliminating background fecal impactions that might have mitigated the effectiveness of initial therapies in the past or that might reduce the effectiveness of daily laxative therapy moving forward.
Patients with a diagnosis of defecatory dyssynergy made via ARM/BET should be referred to pelvic floor physical therapy with biofeedback. Recognizing that courses of therapy are highly individualized in practice, randomized controlled trials suggest symptom improvement in 70%-80% of patients, with the majority also demonstrating maintenance of response.12 Biofeedback appears to be an essential component of this modality based on meta-analysis data and should be requested specifically by the referring provider.13
Pharmacologic agents
For those patients with more severe initial presentations or whose symptoms persist despite initial medical management, there are several pharmacologic agents that may be considered on a prescription basis (Table 2). Linaclotide, a minimally absorbed guanylate cyclase agonist, is approved by the Food and Drug Administration for patients with irritable bowel syndrome with constipation (IBS-C) and chronic idiopathic constipation (CIC). Improvements in constipation tend to occur over a slightly shorter timeline than in abdominal pain, though both have been demonstrated in comparison to placebo.14,15 Plecanatide, a newer agent with a similar mechanism of action, has demonstrated improvements in bowel movement frequency and was recently approved for CIC.16 Lubiprostone, a chloride channel agonist, has demonstrated benefit for IBS-C and CIC as well, though its side effect profile is more varied, including dose-related nausea in up to 30% of patients.17
For patients with opioid-induced constipation who cannot wean from the opioid medications, the peripheral acting mu-opioid receptor antagonists may be quite helpful. These include injectable as well as oral formulations (e.g., methylnaltrexone and naloxegol, respectively) with additional agents under active investigation in particular clinical subsets (e.g., naldemedine for patients with cancer-related pain).18,19 Prucalopride, a selective serotonin receptor agonist, has also demonstrated benefit for constipation; it is available abroad but not yet approved for use in the United States.20 Prucalopride shares its primary mechanism of action (selective agonism of the 5HT4 serotonin receptor) with cisapride, a previously quite popular gastrointestinal motility agent that was subsequently withdrawn from the U.S. market because of arrhythmia risk.21 This risk is likely attributable to cisapride’s dual binding affinity for potassium channels, a feature that prucalopride does not share; as such, cardiotoxicity is not an active concern with the latter agent.22
Still other pharmacologic agents with novel mechanisms of action are currently under investigation. Tenapanor, an inhibitor of a particular sodium/potassium exchanger in the gut lumen, mitigates intestinal sodium absorption, which increases fluid volume and transit. A recent phase 2 study demonstrated significantly increased stool frequency relative to placebo in patients with IBS-C.23 Elobixibat, an ileal bile acid transport inhibitor, promotes colonic retention of bile acids and, in placebo-controlled studies, has led to accelerated colonic transit and an increased number of spontaneous bowel movements in patients with CIC.24
Persistent constipation
In cases of refractory constipation (in practical terms, symptoms that persist despite trials of escalating medical therapy over at least 6 weeks), it is worth revisiting the question of etiology. Querying defecatory dyssynergy via ARM/BET, if not pursued prior to trials of newer pharmacologic agents, should certainly be explored in the event that such trials fail. Inconclusive results of ARM and BET testing, or BET abnormalities that persist despite a course of physical therapy with biofeedback, may raise suspicion for pelvic organ prolapse, which may be formally evaluated with defecography. Additional testing for metabolic or structural predispositions toward constipation may also be reasonable at this juncture.
Formal colonic transit testing via radio-opaque markers, scintigraphy, or the wireless motility capsule is often inaccurate in the setting of dyssynergic defecation and should be pursued only after this entity has been excluded or successfully treated.25 While there are not many practical distinctions at present in the therapeutic management of slow-transit versus normal-transit constipation, the use of novel medications with an explicitly prokinetic mechanism of action may be reasonable to consider in the setting of a document delay in colonic transit. Such delays can also help justify further specialized diagnostic testing (e.g., colonic manometry), and, in rare refractory cases, surgical intervention.
Consideration of colectomy should be reserved for highly selected patients with delayed colonic transit, normal defecatory mechanics, and the absence of potentially explanatory background conditions (e.g., connective tissue disease). Clear evidence of an underlying colonic myopathy or neuropathy may militate in favor of a more targeted surgical intervention (e.g., subtotal colectomy) or guide one’s clinical evaluation toward alternative systemic diagnoses. A diverting loop ileostomy with interval assessment of symptoms may be useful to clarify the potential benefits of colectomy while preserving the option of operative reversal. Proximal transit delays should be definitively excluded before pursuing colonic resections given evidence that multisegment transit delays portend significantly worse postoperative outcomes.26
Conclusion
Constipation is a common, sometimes confusing presenting complaint and the variety of established and emergent options for diagnosis and therapy can lend themselves to haphazard application. Patients and providers both are well served by a clinical approach, rooted in a comprehensive history and examination, that begins to organize these options in thoughtful sequence.
Dr. Ahuja is assistant professor of clinical medicine, division of gastroenterology; Dr. Reynolds is professor of clinical medicine, and director of the program in neurogastroenterology and motility, division of gastroenterology, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
References
1. Higgins P.D., Johanson J.F. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol. 2004 Apr;99(4):750-9. PubMed PMID: 15089911.
2. Martin B.C., Barghout V., Cerulli A. Direct medical costs of constipation in the United States. Manage Care Interface. 2006 Dec;19(12):43-9. PubMed PMID: 17274481.
3. Sun S.X., Dibonaventura M., Purayidathil F.W., et al. Impact of chronic constipation on health-related quality of life, work productivity, and healthcare resource use: an analysis of the National Health and Wellness Survey. Dig Dis Sc. 2011 Sep;56(9):2688-95. PubMed PMID: 21380761.
4. Heidelbaugh J.J., Stelwagon M., Miller S.A., et al. The spectrum of constipation-predominant irritable bowel syndrome and chronic idiopathic constipation: US survey assessing symptoms, care seeking, and disease burden. Am J Gastroenterol. 2015 Apr;110(4):580-7.
5. Mitsuhashi S., Ballou S., Jiang Z.G., et al. Characterizing normal bowel frequency and consistency in a representative sample of adults in the United States (NHANES). Am J Gastroenterol. 2017 Aug 01. PubMed PMID: 28762379.
6. Saad R.J., Rao S.S., Koch K.L., et al. Do stool form and frequency correlate with whole-gut and colonic transit? Results from a multicenter study in constipated individuals and healthy controls. Am J Gastroenterol. 2010 Feb;105(2):403-11. PubMed PMID: 19888202.
7. Castori M., Morlino S., Pascolini G., et al. Gastrointestinal and nutritional issues in joint hypermobility syndrome/Ehlers-Danlos syndrome, hypermobility type. American Journal of Medical Genetics Part C, Semin Med Genet. 2015 Mar;169C(1):54-75. PubMed PMID: 25821092.
8. Nagaraja V., McMahan Z.H., Getzug T., Khanna D. Management of gastrointestinal involvement in scleroderma. Curr Treatm Opt Rheumatol. 2015 Mar 01;1(1):82-105. PubMed PMID: 26005632. Pubmed Central PMCID: 4437639.
9. Malagelada J.R., Accarino A., Azpiroz F. Bloating and abdominal distension: Old misconceptions and current knowledge. Am J Gastroenterol. 2017 Aug;112(8):1221-31. PubMed PMID: 28508867.
10. Soh J.S., Lee H.J., Jung K.W., et al. The diagnostic value of a digital rectal examination compared with high-resolution anorectal manometry in patients with chronic constipation and fecal incontinence. Am J Gastroenterol. 2015 Aug;110(8):1197-204. PubMed PMID: 26032152.
11. American Gastroenterological Association, Bharucha A.E., Dorn S.D., Lembo A., Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology. 2013 Jan;144(1):211-7. PubMed PMID: 23261064.
12. Skardoon G.R., Khera A.J., Emmanuel A.V., Burgell R.E. Review article: dyssynergic defaecation and biofeedback therapy in the pathophysiology and management of functional constipation. Aliment Pharmacol Therapeut. 2017 Aug;46(4):410-23. PubMed PMID: 28660663.
13. Koh C.E., Young C.J., Young J.M., Solomon M.J. Systematic review of randomized controlled trials of the effectiveness of biofeedback for pelvic floor dysfunction. Br J Surg. 2008 Sep;95(9):1079-87. PubMed PMID: 18655219.
14. Rao S., Lembo A.J., Shiff S.J., et al. A 12-week, randomized, controlled trial with a 4-week randomized withdrawal period to evaluate the efficacy and safety of linaclotide in irritable bowel syndrome with constipation. Am J Gastroenterol. 2012 Nov;107(11):1714-24; quiz p 25. PubMed PMID: 22986440. Pubmed Central PMCID: 3504311.
15. Lacy B.E., Schey R., Shiff S.J., et al. Linaclotide in chronic idiopathic constipation patients with moderate to severe abdominal bloating: A randomized, controlled trial. PloS One. 2015;10(7):e0134349. PubMed PMID: 26222318. Pubmed Central PMCID: 4519259.
16. Miner P.B., Jr., Koltun W.D., Wiener G.J., et al. A randomized phase III clinical trial of plecanatide, a uroguanylin analog, in patients with chronic idiopathic constipation. Am J Gastroenterol. 2017 Apr;112(4):613-21. PubMed PMID: 28169285. Pubmed Central PMCID: 5415706.
17. Johanson J.F., Drossman D.A., Panas R., Wahle A., Ueno R. Clinical trial: phase 2 study of lubiprostone for irritable bowel syndrome with constipation. Aliment Pharmacol Therapeut. 2008 Apr;27(8):685-96. PubMed PMID: 18248656.
18. Chey W.D., Webster L., Sostek M., Lappalainen J., Barker P.N., Tack J. Naloxegol for opioid-induced constipation in patients with noncancer pain. N Engl J Med. 2014 Jun 19;370(25):2387-96. PubMed PMID: 24896818.
19. Katakami N., Oda K., Tauchi K., et al. Phase IIb, randomized, double-blind, placebo-controlled study of naldemedine for the treatment of opioid-induced constipation in patients with cancer. J Clin Oncol. 2017 Jun 10;35(17):1921-8. PubMed PMID: 28445097.
20. Sajid M.S., Hebbar M., Baig M.K., Li A., Philipose Z. Use of prucalopride for chronic constipation: A systematic review and meta-analysis of published randomized, controlled trials. J Neurogastroenterol Motil. 2016 Jul 30;22(3):412-22. PubMed PMID: 27127190. Pubmed Central PMCID: 4930296.
21. Quigley E.M. Cisapride: What can we learn from the rise and fall of a prokinetic? J Dig Dis. 2011 Jun;12(3):147-56. PubMed PMID: 21615867.
22. Conlon K., De Maeyer J.H., Bruce C., et al. Nonclinical cardiovascular studies of prucalopride, a highly selective 5-hydroxytryptamine 4 receptor agonist. J Pharmacol Exp Therapeut. 2017 Nov; doi: 10.1124/jpet.117.244079 [epub ahead of print].
23. Chey W.D., Lembo A.J., Rosenbaum D.P. Tenapanor treatment of patients with constipation-predominant irritable bowel syndrome: a phase 2, randomized, placebo-controlled efficacy and safety trial. Am J Gastroenterol. 2017;112:763-74.
24. Simren M., Bajor A., Gillberg P-G, Rudling M., Abrahamsson H. Randomised clinical trial: the ileal bile acid transporter inhibitor A3309 vs. placebo in patients with chronic idiopathic constipation – a double-blind study. Aliment Pharmacol Ther. 2011 Jul;34(1):41-50.
25. Zarate N., Knowles C.H., Newell M., et al. In patients with slow transit constipation, the pattern of colonic transit delay does not differentiate between those with and without impaired rectal evacuation. Am J Gastroenterol. 2008 Feb;103(2):427-34. PubMed PMID: 18070233.
26. Redmond J.M., Smith G.W., Barofsky I., et al. Physiological tests to predict long-term outcome of total abdominal colectomy for intractable constipation. Am J Gastroenterol. 1995 May;90(5):748-53. PubMed PMID: 7733081.
Delayed ileal pouch anal anastomosis creation linked to lower 30-day adverse events
LAS VEGAS – compared with creating the pouch at the time of initial surgery, results from an analysis of national data demonstrated.
“More than 600,000 Americans have UC, and 20%-30% of them require surgical management,” Bharati Kochar, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “The surgical procedure of choice for many UC patients is total proctocolectomy with ileal pouch anal anastomosis creation.”
According to Dr. Kochar, an advanced fellow in inflammatory bowel diseases at the University of North Carolina at Chapel Hill, existing American medical literature regarding ileal pouch anal anastomosis (IPAA) comes mostly from quaternary care centers and compares one-stage procedures with multistage procedures.
“The risks between two- to three-stage procedures are not described, and there are no prospective national reports of postoperative adverse events after IPAA creation,” she said.
Using data from the National Surgical Quality Improvement Program, Dr. Kochar and her associates conducted an observational cohort analysis of 2,390 adult patients with a postoperative diagnosis of UC who underwent IPAA procedures between 2011 and 2015. Their aims were to evaluate adverse events within 30 days after an IPAA creation and to compare adverse events between pouch creation at the time of colectomy and delayed pouch creation.
They also performed a subanalysis of total abdominal colectomy with ileostomy (TAC), the first stage in the delayed pouch procedures, versus pouch creation at the time of colectomy. Multivariable modified Poisson regression models were used to estimate risk ratios adjusted for age, sex, race, body mass index, smoking status, diabetes, preoperative albumin, and American Society of Anesthesiologists class.
Of the 2,390 patients, 1,571 had pouches created at the time of colectomy (group A), and 819 had delayed pouch creation (group B).
Compared with patients in group B, those in group A were older (a median age of 40 years vs. 37 years, respectively; P less than .01), were more likely to be on an immunosuppressant (51% vs. 15%; P less than .01), have a lower median preoperative albumin level (3.9 vs. 4.2; P less than .01), and a longer median length of stay (6 days vs. 5 days; P less than .01).
On unadjusted analyses, the researchers also observed that, at 30 days, patients in group A had significantly more major complications, such as mortality and cardiac arrest (12.4% vs. 8.7%; P less than .01); minor complications, such as superficial surgical site infections and pneumonia (11.8% vs. 6.1%; P less than .01); unplanned readmissions (statistically similar at 23.3% vs. 21.3%), and unplanned reoperations (7.7% vs. 3.8%; P less than .01).
After controlling for confounders, patients in group B were significantly less likely to have major complications (relative risk, 0.72), minor complications (RR, 0.48), unplanned readmissions (RR, 0.95), and unplanned reoperations (RR, 0.42).
In the subgroup analysis, Dr. Kochar and her associates observed that patients who underwent TAC were significantly older, compared with patients in group A (a median of 46 years vs. 40 years, respectively; P less than .01), and a higher proportion were on immunosuppressants (69% vs. 51%; P less than .01). “Despite these factors, the risk of adverse events after TAC was lower,” Dr. Kochar said.
She acknowledged certain limitations of the study, including the inability to accurately determine the risk of linked surgeries together and the inability to assess institution and operator factors. Also, data were not collected for the purposes of studying inflammatory bowel disease.
“This is the first prospective assessment of morbidity following IPAA creation in UC patients from a national database,” Dr. Kochar concluded. “Delayed pouch procedures are associated with a lower risk of unplanned reoperations and major and minor complications. Immunosuppression at the time of pouch creation may result in an increased risk of adverse events postoperatively. The findings can be valuable for preoperative risk assessment and postoperative management.”
Dr. Kochar reported having no financial disclosures.
*This story was updated on 3/26.
SOURCE: Kochar et al. Crohn’s & Colitis Congress 2018 Clinical Abstract 11.
LAS VEGAS – compared with creating the pouch at the time of initial surgery, results from an analysis of national data demonstrated.
“More than 600,000 Americans have UC, and 20%-30% of them require surgical management,” Bharati Kochar, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “The surgical procedure of choice for many UC patients is total proctocolectomy with ileal pouch anal anastomosis creation.”
According to Dr. Kochar, an advanced fellow in inflammatory bowel diseases at the University of North Carolina at Chapel Hill, existing American medical literature regarding ileal pouch anal anastomosis (IPAA) comes mostly from quaternary care centers and compares one-stage procedures with multistage procedures.
“The risks between two- to three-stage procedures are not described, and there are no prospective national reports of postoperative adverse events after IPAA creation,” she said.
Using data from the National Surgical Quality Improvement Program, Dr. Kochar and her associates conducted an observational cohort analysis of 2,390 adult patients with a postoperative diagnosis of UC who underwent IPAA procedures between 2011 and 2015. Their aims were to evaluate adverse events within 30 days after an IPAA creation and to compare adverse events between pouch creation at the time of colectomy and delayed pouch creation.
They also performed a subanalysis of total abdominal colectomy with ileostomy (TAC), the first stage in the delayed pouch procedures, versus pouch creation at the time of colectomy. Multivariable modified Poisson regression models were used to estimate risk ratios adjusted for age, sex, race, body mass index, smoking status, diabetes, preoperative albumin, and American Society of Anesthesiologists class.
Of the 2,390 patients, 1,571 had pouches created at the time of colectomy (group A), and 819 had delayed pouch creation (group B).
Compared with patients in group B, those in group A were older (a median age of 40 years vs. 37 years, respectively; P less than .01), were more likely to be on an immunosuppressant (51% vs. 15%; P less than .01), have a lower median preoperative albumin level (3.9 vs. 4.2; P less than .01), and a longer median length of stay (6 days vs. 5 days; P less than .01).
On unadjusted analyses, the researchers also observed that, at 30 days, patients in group A had significantly more major complications, such as mortality and cardiac arrest (12.4% vs. 8.7%; P less than .01); minor complications, such as superficial surgical site infections and pneumonia (11.8% vs. 6.1%; P less than .01); unplanned readmissions (statistically similar at 23.3% vs. 21.3%), and unplanned reoperations (7.7% vs. 3.8%; P less than .01).
After controlling for confounders, patients in group B were significantly less likely to have major complications (relative risk, 0.72), minor complications (RR, 0.48), unplanned readmissions (RR, 0.95), and unplanned reoperations (RR, 0.42).
In the subgroup analysis, Dr. Kochar and her associates observed that patients who underwent TAC were significantly older, compared with patients in group A (a median of 46 years vs. 40 years, respectively; P less than .01), and a higher proportion were on immunosuppressants (69% vs. 51%; P less than .01). “Despite these factors, the risk of adverse events after TAC was lower,” Dr. Kochar said.
She acknowledged certain limitations of the study, including the inability to accurately determine the risk of linked surgeries together and the inability to assess institution and operator factors. Also, data were not collected for the purposes of studying inflammatory bowel disease.
“This is the first prospective assessment of morbidity following IPAA creation in UC patients from a national database,” Dr. Kochar concluded. “Delayed pouch procedures are associated with a lower risk of unplanned reoperations and major and minor complications. Immunosuppression at the time of pouch creation may result in an increased risk of adverse events postoperatively. The findings can be valuable for preoperative risk assessment and postoperative management.”
Dr. Kochar reported having no financial disclosures.
*This story was updated on 3/26.
SOURCE: Kochar et al. Crohn’s & Colitis Congress 2018 Clinical Abstract 11.
LAS VEGAS – compared with creating the pouch at the time of initial surgery, results from an analysis of national data demonstrated.
“More than 600,000 Americans have UC, and 20%-30% of them require surgical management,” Bharati Kochar, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “The surgical procedure of choice for many UC patients is total proctocolectomy with ileal pouch anal anastomosis creation.”
According to Dr. Kochar, an advanced fellow in inflammatory bowel diseases at the University of North Carolina at Chapel Hill, existing American medical literature regarding ileal pouch anal anastomosis (IPAA) comes mostly from quaternary care centers and compares one-stage procedures with multistage procedures.
“The risks between two- to three-stage procedures are not described, and there are no prospective national reports of postoperative adverse events after IPAA creation,” she said.
Using data from the National Surgical Quality Improvement Program, Dr. Kochar and her associates conducted an observational cohort analysis of 2,390 adult patients with a postoperative diagnosis of UC who underwent IPAA procedures between 2011 and 2015. Their aims were to evaluate adverse events within 30 days after an IPAA creation and to compare adverse events between pouch creation at the time of colectomy and delayed pouch creation.
They also performed a subanalysis of total abdominal colectomy with ileostomy (TAC), the first stage in the delayed pouch procedures, versus pouch creation at the time of colectomy. Multivariable modified Poisson regression models were used to estimate risk ratios adjusted for age, sex, race, body mass index, smoking status, diabetes, preoperative albumin, and American Society of Anesthesiologists class.
Of the 2,390 patients, 1,571 had pouches created at the time of colectomy (group A), and 819 had delayed pouch creation (group B).
Compared with patients in group B, those in group A were older (a median age of 40 years vs. 37 years, respectively; P less than .01), were more likely to be on an immunosuppressant (51% vs. 15%; P less than .01), have a lower median preoperative albumin level (3.9 vs. 4.2; P less than .01), and a longer median length of stay (6 days vs. 5 days; P less than .01).
On unadjusted analyses, the researchers also observed that, at 30 days, patients in group A had significantly more major complications, such as mortality and cardiac arrest (12.4% vs. 8.7%; P less than .01); minor complications, such as superficial surgical site infections and pneumonia (11.8% vs. 6.1%; P less than .01); unplanned readmissions (statistically similar at 23.3% vs. 21.3%), and unplanned reoperations (7.7% vs. 3.8%; P less than .01).
After controlling for confounders, patients in group B were significantly less likely to have major complications (relative risk, 0.72), minor complications (RR, 0.48), unplanned readmissions (RR, 0.95), and unplanned reoperations (RR, 0.42).
In the subgroup analysis, Dr. Kochar and her associates observed that patients who underwent TAC were significantly older, compared with patients in group A (a median of 46 years vs. 40 years, respectively; P less than .01), and a higher proportion were on immunosuppressants (69% vs. 51%; P less than .01). “Despite these factors, the risk of adverse events after TAC was lower,” Dr. Kochar said.
She acknowledged certain limitations of the study, including the inability to accurately determine the risk of linked surgeries together and the inability to assess institution and operator factors. Also, data were not collected for the purposes of studying inflammatory bowel disease.
“This is the first prospective assessment of morbidity following IPAA creation in UC patients from a national database,” Dr. Kochar concluded. “Delayed pouch procedures are associated with a lower risk of unplanned reoperations and major and minor complications. Immunosuppression at the time of pouch creation may result in an increased risk of adverse events postoperatively. The findings can be valuable for preoperative risk assessment and postoperative management.”
Dr. Kochar reported having no financial disclosures.
*This story was updated on 3/26.
SOURCE: Kochar et al. Crohn’s & Colitis Congress 2018 Clinical Abstract 11.
REPORTING FROM THE CROHN’S & COLITIS CONGRESS
Key clinical point: Delayed ileal pouch anal anastomosis procedures are associated with a lower 30-day adverse-event rate.
Major finding: After controlling for confounders, patients who underwent delayed IPAA procedures were significantly less likely to have major complications (relative risk, 0.72), minor complications (RR, 0.48), unplanned readmissions (RR, 0.95), and unplanned reoperations (RR, 0.42) at 30 days, compared with those who underwent pouch creation at the time of initial surgery.
Study details: An observational cohort analysis of 2,390 adult patients with a postoperative diagnosis of UC.
Disclosures: Dr. Kochar reported having no financial disclosures.
Source: Kochar et al. Crohn’s & Colitis Congress 2018 Clinical Abstract 11. Gastroenterology. 2018;154(1)Suppl:S1-S114.
Emergent colectomies for ulcerative colitis declining
LAS VEGAS – , a large database analysis has shown.
“Despite advances in medical therapy for ulcerative colitis (UC), many patients still need surgery,” Ryan C. Ungaro, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Prior epidemiologic studies have demonstrated a decline in colectomy rates over time, particularly comparing the pre- and postbiologic eras, but less is known about rates of emergent colectomy over time,” he said. In particular, he continued, data on UC colectomy and ileal pouch anal anastomosis (IPAA) surgery rates in the United States are limited.
In an effort to examine UC emergent colectomy rates and IPAA over time, Dr. Ungaro, of the division of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York, and his associates analyzed data from the U.S. Nationwide Inpatient Sample from 2000 through 2014. They defined emergent colectomy cases as admission through the emergency department and used the ICD-9-CM code for subtotal colectomy (45.8) as the outcome variable, and defined a second cohort of UC patients admitted electively with an outcome variable of ICD-9-CM code for IPAA (45.95). To evaluate temporal trends of colectomy and IPAA, the researchers used joinpoint regression analysis with calculation of annual percentage change.

They also observed disparities in IPAA surgery rates based on race and insurance type. Specifically, whites had higher rates of elective IPAA during the study period, compared with black or Hispanic patients (P less than .01), while patients with private insurance had higher rates of elective IPAA, compared with those insured by Medicare or Medicaid (P less than .01). Dr. Ungaro acknowledged certain limitations of the study, including the fact that the Nationwide Inpatient Sample relies on administrative codes, “which may increase risk of misclassification bias,” he said. They were also unable to track individual patients across time and lacked data on medication use and disease severity.
“There has been a significant decline in emergency colectomy for ulcerative colitis in the United States,” Dr. Ungaro concluded. “We expect that this is due to more effective inpatient care. However, the overall need for surgery in UC appears to be stable given unchanged IPAA rates. This suggests a limited impact on overall surgery rates with a shift from emergent to elective procedures.” He reported having no relevant financial disclosures.
*This story was updated on 3/26.
SOURCE: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
LAS VEGAS – , a large database analysis has shown.
“Despite advances in medical therapy for ulcerative colitis (UC), many patients still need surgery,” Ryan C. Ungaro, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Prior epidemiologic studies have demonstrated a decline in colectomy rates over time, particularly comparing the pre- and postbiologic eras, but less is known about rates of emergent colectomy over time,” he said. In particular, he continued, data on UC colectomy and ileal pouch anal anastomosis (IPAA) surgery rates in the United States are limited.
In an effort to examine UC emergent colectomy rates and IPAA over time, Dr. Ungaro, of the division of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York, and his associates analyzed data from the U.S. Nationwide Inpatient Sample from 2000 through 2014. They defined emergent colectomy cases as admission through the emergency department and used the ICD-9-CM code for subtotal colectomy (45.8) as the outcome variable, and defined a second cohort of UC patients admitted electively with an outcome variable of ICD-9-CM code for IPAA (45.95). To evaluate temporal trends of colectomy and IPAA, the researchers used joinpoint regression analysis with calculation of annual percentage change.
They also observed disparities in IPAA surgery rates based on race and insurance type. Specifically, whites had higher rates of elective IPAA during the study period, compared with black or Hispanic patients (P less than .01), while patients with private insurance had higher rates of elective IPAA, compared with those insured by Medicare or Medicaid (P less than .01). Dr. Ungaro acknowledged certain limitations of the study, including the fact that the Nationwide Inpatient Sample relies on administrative codes, “which may increase risk of misclassification bias,” he said. They were also unable to track individual patients across time and lacked data on medication use and disease severity.
“There has been a significant decline in emergency colectomy for ulcerative colitis in the United States,” Dr. Ungaro concluded. “We expect that this is due to more effective inpatient care. However, the overall need for surgery in UC appears to be stable given unchanged IPAA rates. This suggests a limited impact on overall surgery rates with a shift from emergent to elective procedures.” He reported having no relevant financial disclosures.
*This story was updated on 3/26.
SOURCE: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
LAS VEGAS – , a large database analysis has shown.
“Despite advances in medical therapy for ulcerative colitis (UC), many patients still need surgery,” Ryan C. Ungaro, MD, said at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association. “Prior epidemiologic studies have demonstrated a decline in colectomy rates over time, particularly comparing the pre- and postbiologic eras, but less is known about rates of emergent colectomy over time,” he said. In particular, he continued, data on UC colectomy and ileal pouch anal anastomosis (IPAA) surgery rates in the United States are limited.
In an effort to examine UC emergent colectomy rates and IPAA over time, Dr. Ungaro, of the division of gastroenterology at the Icahn School of Medicine at Mount Sinai, New York, and his associates analyzed data from the U.S. Nationwide Inpatient Sample from 2000 through 2014. They defined emergent colectomy cases as admission through the emergency department and used the ICD-9-CM code for subtotal colectomy (45.8) as the outcome variable, and defined a second cohort of UC patients admitted electively with an outcome variable of ICD-9-CM code for IPAA (45.95). To evaluate temporal trends of colectomy and IPAA, the researchers used joinpoint regression analysis with calculation of annual percentage change.
They also observed disparities in IPAA surgery rates based on race and insurance type. Specifically, whites had higher rates of elective IPAA during the study period, compared with black or Hispanic patients (P less than .01), while patients with private insurance had higher rates of elective IPAA, compared with those insured by Medicare or Medicaid (P less than .01). Dr. Ungaro acknowledged certain limitations of the study, including the fact that the Nationwide Inpatient Sample relies on administrative codes, “which may increase risk of misclassification bias,” he said. They were also unable to track individual patients across time and lacked data on medication use and disease severity.
“There has been a significant decline in emergency colectomy for ulcerative colitis in the United States,” Dr. Ungaro concluded. “We expect that this is due to more effective inpatient care. However, the overall need for surgery in UC appears to be stable given unchanged IPAA rates. This suggests a limited impact on overall surgery rates with a shift from emergent to elective procedures.” He reported having no relevant financial disclosures.
*This story was updated on 3/26.
SOURCE: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
REPORTING FROM THE CROHN’S & COLITIS CONGRESS
Key clinical point: There has been a significant decline in emergent ulcerative colitis colectomies in the United States.
Major finding: Between 2000 and 2014, the colectomy rate among patients emergently admitted to the hospital declined more than 7% annually (P less than .05).
Study details: An analysis of 470,720 hospital admissions from the Nationwide Inpatient Sample.
Disclosures: Dr. Ungaro reported having no financial disclosures.
Source: Ungaro RC et al. Crohn’s & Colitis Congress, Clinical Abstract 23.
Five reasons to pursue a career in IBD research or patient care
A career in inflammatory bowel disease promises to be challenging, exciting, at times frustrating, and always educational. We asked our expert faculty at the inaugural Crohn’s & Colitis Congress, which took place Jan. 18-20 in Las Vegas, to reflect on why a career in IBD is an excellent path to take.
Why pursue a career in IBD
1. “IBD is the fastest moving area of GI to integrate science (genomics, microbiome, immunology) into care that will change the natural history of disease. The physicians and scientists have an unusually collegial culture, and the patients really care.” – Jonathan G. Braun, MD, PhD
2. “Managing patients with IBD is becoming ever more complex. When patients move beyond having mild disease, complex decisions need to be made. Choosing the right medication at the right time for the right patient will lead to the best outcomes for patients with IBD. I have every reason to believe that specializing in the clinical care of patients with IBD will be intellectually challenging while offering great personal satisfaction in taking care of these ill patients.” – Francis A. Farraye, MD, MSc
3. “IBD research findings and the implications for patient care are evolving rapidly. Many recommendations that we made 5-10 years ago have changed as we are learning more about IBD every day. There are so many opportunities to participate in the expansion of that knowledge base and help us reach our goal of a cure for IBD in the lifetime of many of our patients. Take the challenge.” – Teri Lynn Jackson, MSN, ARNP
4. “IBD is an outstanding field led by great people who want to see fellows and junior faculty succeed. Identify a mentor and listen to them, meet and engage with new people, be curious, think big, and work hard!” – Michael J. Rosen, MD, MSCI
5. “The best career in the world! Such variety. A home for everyone with any interest. It won’t always be smooth, but it will be incredibly rewarding with hardly a dull moment.” – Dermot McGovern, MD, PhD, FRCP
For additional tips and advice, visit the AGA Community.
A career in inflammatory bowel disease promises to be challenging, exciting, at times frustrating, and always educational. We asked our expert faculty at the inaugural Crohn’s & Colitis Congress, which took place Jan. 18-20 in Las Vegas, to reflect on why a career in IBD is an excellent path to take.
Why pursue a career in IBD
1. “IBD is the fastest moving area of GI to integrate science (genomics, microbiome, immunology) into care that will change the natural history of disease. The physicians and scientists have an unusually collegial culture, and the patients really care.” – Jonathan G. Braun, MD, PhD
2. “Managing patients with IBD is becoming ever more complex. When patients move beyond having mild disease, complex decisions need to be made. Choosing the right medication at the right time for the right patient will lead to the best outcomes for patients with IBD. I have every reason to believe that specializing in the clinical care of patients with IBD will be intellectually challenging while offering great personal satisfaction in taking care of these ill patients.” – Francis A. Farraye, MD, MSc
3. “IBD research findings and the implications for patient care are evolving rapidly. Many recommendations that we made 5-10 years ago have changed as we are learning more about IBD every day. There are so many opportunities to participate in the expansion of that knowledge base and help us reach our goal of a cure for IBD in the lifetime of many of our patients. Take the challenge.” – Teri Lynn Jackson, MSN, ARNP
4. “IBD is an outstanding field led by great people who want to see fellows and junior faculty succeed. Identify a mentor and listen to them, meet and engage with new people, be curious, think big, and work hard!” – Michael J. Rosen, MD, MSCI
5. “The best career in the world! Such variety. A home for everyone with any interest. It won’t always be smooth, but it will be incredibly rewarding with hardly a dull moment.” – Dermot McGovern, MD, PhD, FRCP
For additional tips and advice, visit the AGA Community.
A career in inflammatory bowel disease promises to be challenging, exciting, at times frustrating, and always educational. We asked our expert faculty at the inaugural Crohn’s & Colitis Congress, which took place Jan. 18-20 in Las Vegas, to reflect on why a career in IBD is an excellent path to take.
Why pursue a career in IBD
1. “IBD is the fastest moving area of GI to integrate science (genomics, microbiome, immunology) into care that will change the natural history of disease. The physicians and scientists have an unusually collegial culture, and the patients really care.” – Jonathan G. Braun, MD, PhD
2. “Managing patients with IBD is becoming ever more complex. When patients move beyond having mild disease, complex decisions need to be made. Choosing the right medication at the right time for the right patient will lead to the best outcomes for patients with IBD. I have every reason to believe that specializing in the clinical care of patients with IBD will be intellectually challenging while offering great personal satisfaction in taking care of these ill patients.” – Francis A. Farraye, MD, MSc
3. “IBD research findings and the implications for patient care are evolving rapidly. Many recommendations that we made 5-10 years ago have changed as we are learning more about IBD every day. There are so many opportunities to participate in the expansion of that knowledge base and help us reach our goal of a cure for IBD in the lifetime of many of our patients. Take the challenge.” – Teri Lynn Jackson, MSN, ARNP
4. “IBD is an outstanding field led by great people who want to see fellows and junior faculty succeed. Identify a mentor and listen to them, meet and engage with new people, be curious, think big, and work hard!” – Michael J. Rosen, MD, MSCI
5. “The best career in the world! Such variety. A home for everyone with any interest. It won’t always be smooth, but it will be incredibly rewarding with hardly a dull moment.” – Dermot McGovern, MD, PhD, FRCP
For additional tips and advice, visit the AGA Community.
Common food additive makes C. difficile more virulent
, a study showed.
“Out of several carbon sources identified that supported CD2015 growth [epidemic RT027 isolate], we found the disaccharide trehalose increased the growth yield of CD2015 by approximately fivefold, compared with a non-RT027 strain,” according to James Collins, PhD, of Baylor University, Houston, and his colleagues. The increased growth of the epidemic strain of C. difficile observed by Dr. Collins and his team demonstrates that trehalose is a robust carbon source for C. difficile bacterium.

In one experiment, mice with humanized microbiota were infected with two strains of RT027, either R20291 (n = 27) or R20291-delta treA (n = 28), a phosphotrehalase enzyme (TreA) deletion mutant that cannot metabolize trehalose. Mice were then given 5 mM of trehalose ad libitum in their drinking water. Researchers observed that the mice infected with R20291-delta treA had much lower mortality rates than the R20291 group (33.3% vs.78.6%). These findings were then reinforced with a second experiment using mice with humanized microbiota, in which trehalose addition increased mortality in RT027 mice, compared with RT027-infected mice that were not given dietary trehalose.
While Dr. Collins and his team demonstrated the effect of trehalose on C. difficile in mice, they also conducted a limited analysis of ileostomy effluent from three human donors. The researchers found that in two of three samples, treA was strongly induced in CD2015, but not in another ribotype, CD2048. This demonstrates that amounts of trehalose found in food are high enough to be metabolized by certain epidemic strains of C. difficile in humans.
Prior to 2000, trehalose use was limited by a relatively high cost of production, approximately $700 per kilogram. A production innovation that utilized a novel enzymatic method that yielded trehalose from starch brought the price of trehalose to approximately $3 per kilogram, making it a commercially viable food supplement. After being considered “generally recognized as safe” by the U.S. Food and Drug Administration in 2000 and approved for use in Europe, the trehalose concentrations in food skyrocketed from around 2% to 11.25%, and trehalose became widely used in several foods, including ice cream, pasta, and ground beef.
Dr. Collins and his associates said that there is considerable evidence that the widespread use of dietary trehalose has contributed to the spread of epidemic C. difficile ribotypes. First, strains RT027 and RT078 have always had the ability to metabolize trehalose, as evidenced by outbreaks of nonepidemic C. difficile in the 1980s. But no epidemic outbreaks were reported until after 2003, several years after trehalose was approved by the FDA. Second, RT027 and RT078 are phylogenetically distant, but independently evolved the ability to metabolize low levels of trehalose. Third, increased severity of the RT027 strain, which metabolizes trehalose in mice, is consistent with increased virulence of RT078 and RT027 in human patients. Fourth, a competitive advantage is conferred to C. difficile being able to metabolize trehalose in low concentrations in a diverse intestinal setting. Finally, the levels of trehalose in ileostomy fluid from patients who eat a normal diet are high enough to be utilized by RT027 strains.
“On the basis of these observations, we propose that the widespread adoption and use of the disaccharide trehalose in the human diet has played a significant role in the emergence of these epidemic and hypervirulent strains,” Dr. Collins and his colleagues wrote in their article in Nature.
The authors of the study had no relevant financial disclosures to report.
SOURCE: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Fecal microbiota transplantation (FMT) is a promising new treatment for recurring C. diff infections. The AGA FMT National Registry — conducted in collaboration with the Crohn’s and Colitis Foundation, the Infectious Diseases Society of America, and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition — will allow physicians and patients to report back on outcomes of the FMT procedure. This data will help answer critical questions about the longer-term health effects of FMT and guide future use. Learn more at www.gastro.org/FMTRegistry.
, a study showed.
“Out of several carbon sources identified that supported CD2015 growth [epidemic RT027 isolate], we found the disaccharide trehalose increased the growth yield of CD2015 by approximately fivefold, compared with a non-RT027 strain,” according to James Collins, PhD, of Baylor University, Houston, and his colleagues. The increased growth of the epidemic strain of C. difficile observed by Dr. Collins and his team demonstrates that trehalose is a robust carbon source for C. difficile bacterium.
In one experiment, mice with humanized microbiota were infected with two strains of RT027, either R20291 (n = 27) or R20291-delta treA (n = 28), a phosphotrehalase enzyme (TreA) deletion mutant that cannot metabolize trehalose. Mice were then given 5 mM of trehalose ad libitum in their drinking water. Researchers observed that the mice infected with R20291-delta treA had much lower mortality rates than the R20291 group (33.3% vs.78.6%). These findings were then reinforced with a second experiment using mice with humanized microbiota, in which trehalose addition increased mortality in RT027 mice, compared with RT027-infected mice that were not given dietary trehalose.
While Dr. Collins and his team demonstrated the effect of trehalose on C. difficile in mice, they also conducted a limited analysis of ileostomy effluent from three human donors. The researchers found that in two of three samples, treA was strongly induced in CD2015, but not in another ribotype, CD2048. This demonstrates that amounts of trehalose found in food are high enough to be metabolized by certain epidemic strains of C. difficile in humans.
Prior to 2000, trehalose use was limited by a relatively high cost of production, approximately $700 per kilogram. A production innovation that utilized a novel enzymatic method that yielded trehalose from starch brought the price of trehalose to approximately $3 per kilogram, making it a commercially viable food supplement. After being considered “generally recognized as safe” by the U.S. Food and Drug Administration in 2000 and approved for use in Europe, the trehalose concentrations in food skyrocketed from around 2% to 11.25%, and trehalose became widely used in several foods, including ice cream, pasta, and ground beef.
Dr. Collins and his associates said that there is considerable evidence that the widespread use of dietary trehalose has contributed to the spread of epidemic C. difficile ribotypes. First, strains RT027 and RT078 have always had the ability to metabolize trehalose, as evidenced by outbreaks of nonepidemic C. difficile in the 1980s. But no epidemic outbreaks were reported until after 2003, several years after trehalose was approved by the FDA. Second, RT027 and RT078 are phylogenetically distant, but independently evolved the ability to metabolize low levels of trehalose. Third, increased severity of the RT027 strain, which metabolizes trehalose in mice, is consistent with increased virulence of RT078 and RT027 in human patients. Fourth, a competitive advantage is conferred to C. difficile being able to metabolize trehalose in low concentrations in a diverse intestinal setting. Finally, the levels of trehalose in ileostomy fluid from patients who eat a normal diet are high enough to be utilized by RT027 strains.
“On the basis of these observations, we propose that the widespread adoption and use of the disaccharide trehalose in the human diet has played a significant role in the emergence of these epidemic and hypervirulent strains,” Dr. Collins and his colleagues wrote in their article in Nature.
The authors of the study had no relevant financial disclosures to report.
SOURCE: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Fecal microbiota transplantation (FMT) is a promising new treatment for recurring C. diff infections. The AGA FMT National Registry — conducted in collaboration with the Crohn’s and Colitis Foundation, the Infectious Diseases Society of America, and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition — will allow physicians and patients to report back on outcomes of the FMT procedure. This data will help answer critical questions about the longer-term health effects of FMT and guide future use. Learn more at www.gastro.org/FMTRegistry.
, a study showed.
“Out of several carbon sources identified that supported CD2015 growth [epidemic RT027 isolate], we found the disaccharide trehalose increased the growth yield of CD2015 by approximately fivefold, compared with a non-RT027 strain,” according to James Collins, PhD, of Baylor University, Houston, and his colleagues. The increased growth of the epidemic strain of C. difficile observed by Dr. Collins and his team demonstrates that trehalose is a robust carbon source for C. difficile bacterium.
In one experiment, mice with humanized microbiota were infected with two strains of RT027, either R20291 (n = 27) or R20291-delta treA (n = 28), a phosphotrehalase enzyme (TreA) deletion mutant that cannot metabolize trehalose. Mice were then given 5 mM of trehalose ad libitum in their drinking water. Researchers observed that the mice infected with R20291-delta treA had much lower mortality rates than the R20291 group (33.3% vs.78.6%). These findings were then reinforced with a second experiment using mice with humanized microbiota, in which trehalose addition increased mortality in RT027 mice, compared with RT027-infected mice that were not given dietary trehalose.
While Dr. Collins and his team demonstrated the effect of trehalose on C. difficile in mice, they also conducted a limited analysis of ileostomy effluent from three human donors. The researchers found that in two of three samples, treA was strongly induced in CD2015, but not in another ribotype, CD2048. This demonstrates that amounts of trehalose found in food are high enough to be metabolized by certain epidemic strains of C. difficile in humans.
Prior to 2000, trehalose use was limited by a relatively high cost of production, approximately $700 per kilogram. A production innovation that utilized a novel enzymatic method that yielded trehalose from starch brought the price of trehalose to approximately $3 per kilogram, making it a commercially viable food supplement. After being considered “generally recognized as safe” by the U.S. Food and Drug Administration in 2000 and approved for use in Europe, the trehalose concentrations in food skyrocketed from around 2% to 11.25%, and trehalose became widely used in several foods, including ice cream, pasta, and ground beef.
Dr. Collins and his associates said that there is considerable evidence that the widespread use of dietary trehalose has contributed to the spread of epidemic C. difficile ribotypes. First, strains RT027 and RT078 have always had the ability to metabolize trehalose, as evidenced by outbreaks of nonepidemic C. difficile in the 1980s. But no epidemic outbreaks were reported until after 2003, several years after trehalose was approved by the FDA. Second, RT027 and RT078 are phylogenetically distant, but independently evolved the ability to metabolize low levels of trehalose. Third, increased severity of the RT027 strain, which metabolizes trehalose in mice, is consistent with increased virulence of RT078 and RT027 in human patients. Fourth, a competitive advantage is conferred to C. difficile being able to metabolize trehalose in low concentrations in a diverse intestinal setting. Finally, the levels of trehalose in ileostomy fluid from patients who eat a normal diet are high enough to be utilized by RT027 strains.
“On the basis of these observations, we propose that the widespread adoption and use of the disaccharide trehalose in the human diet has played a significant role in the emergence of these epidemic and hypervirulent strains,” Dr. Collins and his colleagues wrote in their article in Nature.
The authors of the study had no relevant financial disclosures to report.
SOURCE: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Fecal microbiota transplantation (FMT) is a promising new treatment for recurring C. diff infections. The AGA FMT National Registry — conducted in collaboration with the Crohn’s and Colitis Foundation, the Infectious Diseases Society of America, and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition — will allow physicians and patients to report back on outcomes of the FMT procedure. This data will help answer critical questions about the longer-term health effects of FMT and guide future use. Learn more at www.gastro.org/FMTRegistry.
FROM NATURE
Key clinical point: Metabolizing trehalose increases the virulence and mortality of C. difficile ribotype 027 (RT027).
Major finding: The ability to metabolize trehalose with the phosphotrehalase enzyme (TreA) increases mortality in RT027.
Study details: Experimental mouse models and an analysis of ileostomy effluent from three anonymous donors.
Disclosures: All authors had no financial disclosures to report.
Source: Collins J et al. Nature. 2018 Jan 3. doi: 10.1038/nature25178.
Review: Common gastrointestinal conditions in people living with HIV/AIDS
The two most common gastrointestinal conditions reported by people living with HIV/AIDS are diarrhea and nausea, according to Vincent Hall, PhD.
Diarrhea has been reported in up to 60% of people living with HIV/AIDS, and is generally classified as being infectious or noninfectious. While infectious causes of diarrhea, such as bacteria, fungi, viruses, and protozoa, have declined, noninfectious causes have increased. Common causes of noninfectious diarrhea include HIV enteropathy, diarrhea associated with highly active antiretroviral therapy (HAART), autonomic neuropathy, and chronic pancreatitis.
Prior to the development of HAART, nausea in people living with HIV/AIDS was usually caused by opportunistic infections; however, this has changed. Nausea can come from medication side effects, overlapping drug interactions, and from opportunistic infections in patients with poor immune health. The most common side effect of ART is nausea, and nausea is also the most common cause of ART discontinuation.
“It has been noted that HIV infection can be considered a disease of the GI tract because it is a significant target of infection and because of the side effects HAART can have on the GI system. Therefore, it is important that clinicians have an understanding of the causes of diarrhea and nausea and vomiting in people living with HIV/AIDS and educate patients about potential side effects and treatment options,” Mr. Hall concluded.
Find the full review in Critical Care Nursing Clinics of North America (doi: 10.1016/j.cnc.2017.10.009).
The two most common gastrointestinal conditions reported by people living with HIV/AIDS are diarrhea and nausea, according to Vincent Hall, PhD.
Diarrhea has been reported in up to 60% of people living with HIV/AIDS, and is generally classified as being infectious or noninfectious. While infectious causes of diarrhea, such as bacteria, fungi, viruses, and protozoa, have declined, noninfectious causes have increased. Common causes of noninfectious diarrhea include HIV enteropathy, diarrhea associated with highly active antiretroviral therapy (HAART), autonomic neuropathy, and chronic pancreatitis.
Prior to the development of HAART, nausea in people living with HIV/AIDS was usually caused by opportunistic infections; however, this has changed. Nausea can come from medication side effects, overlapping drug interactions, and from opportunistic infections in patients with poor immune health. The most common side effect of ART is nausea, and nausea is also the most common cause of ART discontinuation.
“It has been noted that HIV infection can be considered a disease of the GI tract because it is a significant target of infection and because of the side effects HAART can have on the GI system. Therefore, it is important that clinicians have an understanding of the causes of diarrhea and nausea and vomiting in people living with HIV/AIDS and educate patients about potential side effects and treatment options,” Mr. Hall concluded.
Find the full review in Critical Care Nursing Clinics of North America (doi: 10.1016/j.cnc.2017.10.009).
The two most common gastrointestinal conditions reported by people living with HIV/AIDS are diarrhea and nausea, according to Vincent Hall, PhD.
Diarrhea has been reported in up to 60% of people living with HIV/AIDS, and is generally classified as being infectious or noninfectious. While infectious causes of diarrhea, such as bacteria, fungi, viruses, and protozoa, have declined, noninfectious causes have increased. Common causes of noninfectious diarrhea include HIV enteropathy, diarrhea associated with highly active antiretroviral therapy (HAART), autonomic neuropathy, and chronic pancreatitis.
Prior to the development of HAART, nausea in people living with HIV/AIDS was usually caused by opportunistic infections; however, this has changed. Nausea can come from medication side effects, overlapping drug interactions, and from opportunistic infections in patients with poor immune health. The most common side effect of ART is nausea, and nausea is also the most common cause of ART discontinuation.
“It has been noted that HIV infection can be considered a disease of the GI tract because it is a significant target of infection and because of the side effects HAART can have on the GI system. Therefore, it is important that clinicians have an understanding of the causes of diarrhea and nausea and vomiting in people living with HIV/AIDS and educate patients about potential side effects and treatment options,” Mr. Hall concluded.
Find the full review in Critical Care Nursing Clinics of North America (doi: 10.1016/j.cnc.2017.10.009).
FROM CRITICAL CARE NURSING CLINICS OF NORTH AMERICA