User login
Hospitalists Outline Quality of Care Initiative for Inpatients with Atrial Fibrillation
SHM asked leaders of the Hospital-Based Quality Improvement in Stroke Prevention for Patients with Atrial Fibrillation (AF) Project, Hiren Shah, MD, MBA, SFHM, and Andrew Masica, MD, SFHM, to provide an overview of the program.
“AF is a disease state that is highly prevalent, and the numbers are rising yearly. We also know that it is one of the most common inpatient diagnoses,” Dr. Shah says. “However, when you look at the quality of care provided to our AF patients, it is quite variable and has implications for other hospital performance metrics such as 30-day readmission rates. This makes AF a high-impact target for inpatient quality improvement initiatives.”
Dr. Shah is assistant professor of medicine at Northwestern University’s Feinberg School of Medicine and medical director at Northwestern Memorial Hospital in Chicago. Dr. Masica is vice president of clinical effectiveness at Baylor Health Care System in Dallas.
The implementation guide for SHM’s AF project will be available later in December at www.hospitalmedicine.org/afib.
Question: What is the scope of your project?
Dr. Masica: That is a question we wrestled with. Numerous care processes related to AF are amenable to inpatient quality improvement. We chose to focus our efforts on stroke prevention in AF and the development of a toolkit to help hospital-based practitioners to assess stroke and bleeding risk consistently and, if indicated, to initiate antithrombotic therapy.
Dr. Shah: Along those lines, we know that at least 25% of AF-related strokes are potentially preventable with adherence to evidence-based care; however, current data indicate that only 50% to 60% of patients with AF who are eligible to receive antithrombotic therapy are on active stroke prophylaxis.
Q: Why do you think there are such large gaps in stroke prophylaxis for AF patients?
Dr. Masica: The prophylaxis decision requires the clinician to do an anticoagulation net-benefit and risk assessment, and although there are validated tools to do this type of assessment, use of these tools hasn’t yet become hardwired into daily hospital practice. Empiric clinical assessments often overestimate the bleed risk and underestimate stroke risk, so the ultimate result can be underuse of antithrombotic therapy.

–Dr. Shah
Dr. Shah: Another barrier is that in many hospitals, there are not reminders in place in our workflow for this assessment to happen at all. Hospitalists may think that the anticoagulation decision is an outpatient issue, better addressed by their primary care doctor, so it is sometimes even intentionally bypassed. Another barrier is that it takes time to discuss a patient’s values and preferences in the anticoagulation decision.
Q: But isn’t stroke prevention in AF more of an outpatient issue?
Dr. Shah: We think the hospital is a great place to start this evaluation and to make the anticoagulation decision. Of course, we should discuss these issues with the primary care doctor. Ideally, we would like to start anticoagulation during the hospital stay or on discharge, if indicated, but even if we clearly communicate a patient’s stroke and bleed risk to the PCP on discharge, we can help ensure that this issue will be addressed on outpatient follow-up.
Q: What specific tools for stroke and bleed risk are you referring to?
Dr. Shah: The CHADS2 scoring system is a well-validated tool for estimating the risk of stroke in AF patients, one that most clinicians may be aware of. The CHA2DS2-VASc is a slightly more refined scoring system. When it comes to bleeding, however, fewer clinicians are aware of the HAS-BLED bleeding risk assessment method.
Dr. Masica: The scoring systems represent a consistent, reproducible approach by which to evaluate inpatients with AF. Of course, there is some discretion for other patient-specific factors (e.g. fall risk) that are not captured in the scoring systems, but they are good starting points in the decision-making process. Finally and most importantly, although it is often overlooked, shared decision-making should take place with the patients, because their values in facing the risk of stroke versus bleeding often tip the balance one way or the other.
Q: How will the project help hospitals in this process?
Dr. Shah: We have written a QI Implementation Guide for hospitals with tools intended to improve the care of patients with AF in the hospital setting. This book will be similar to SHM’s VTE Prevention Implementation Guide, published a few years ago. We also will have an upcoming AF QI resource room within the SHM website. Additionally, similar to VTE, there are likely to be future mentored implementation projects where we will be working directly with hospitals and coaching them in this initiative.
Dr. Masica: We also have given a recent SHM-sponsored webinar that outlines some content of the guide. It can be accessed on the SHM website. This webinar reviews how to start a QI project in AF, assess your current state of care, build an interdisciplinary team, use validated tools, and deploy interventions to help make the stroke risk assessment and prophylaxis decision. I would note that the intended audience for these tools is broad and includes frontline hospitalists, QI directors, CMOs, and COOs, as well as nursing leadership, NPs, PAs, pharmacists, and other care providers.
Q: Does healthcare reform impact your efforts in this area?
Dr. Shah: Value-based purchasing, preventing readmissions, accountable care organizations, and bundled payments are all aspects of reform that will involve this therapeutic area, as their scope will impact the quality of care we deliver, how our cost structures are, and how we improve fragmentation of care across care transitions.
Dr. Masica: In addition, market forces, healthcare legislation, conceptual shifts regarding the need for systematic approaches to healthcare improvement, and new rules that may impact hospital reimbursement will continue to make AF an important healthcare quality issue. Thus, we think the discussion around delivering patient-centered care in AF is really just beginning.
Brendon Shank is SHM’s associate vice president of communications.
SHM asked leaders of the Hospital-Based Quality Improvement in Stroke Prevention for Patients with Atrial Fibrillation (AF) Project, Hiren Shah, MD, MBA, SFHM, and Andrew Masica, MD, SFHM, to provide an overview of the program.
“AF is a disease state that is highly prevalent, and the numbers are rising yearly. We also know that it is one of the most common inpatient diagnoses,” Dr. Shah says. “However, when you look at the quality of care provided to our AF patients, it is quite variable and has implications for other hospital performance metrics such as 30-day readmission rates. This makes AF a high-impact target for inpatient quality improvement initiatives.”
Dr. Shah is assistant professor of medicine at Northwestern University’s Feinberg School of Medicine and medical director at Northwestern Memorial Hospital in Chicago. Dr. Masica is vice president of clinical effectiveness at Baylor Health Care System in Dallas.
The implementation guide for SHM’s AF project will be available later in December at www.hospitalmedicine.org/afib.
Question: What is the scope of your project?
Dr. Masica: That is a question we wrestled with. Numerous care processes related to AF are amenable to inpatient quality improvement. We chose to focus our efforts on stroke prevention in AF and the development of a toolkit to help hospital-based practitioners to assess stroke and bleeding risk consistently and, if indicated, to initiate antithrombotic therapy.
Dr. Shah: Along those lines, we know that at least 25% of AF-related strokes are potentially preventable with adherence to evidence-based care; however, current data indicate that only 50% to 60% of patients with AF who are eligible to receive antithrombotic therapy are on active stroke prophylaxis.
Q: Why do you think there are such large gaps in stroke prophylaxis for AF patients?
Dr. Masica: The prophylaxis decision requires the clinician to do an anticoagulation net-benefit and risk assessment, and although there are validated tools to do this type of assessment, use of these tools hasn’t yet become hardwired into daily hospital practice. Empiric clinical assessments often overestimate the bleed risk and underestimate stroke risk, so the ultimate result can be underuse of antithrombotic therapy.
–Dr. Shah
Dr. Shah: Another barrier is that in many hospitals, there are not reminders in place in our workflow for this assessment to happen at all. Hospitalists may think that the anticoagulation decision is an outpatient issue, better addressed by their primary care doctor, so it is sometimes even intentionally bypassed. Another barrier is that it takes time to discuss a patient’s values and preferences in the anticoagulation decision.
Q: But isn’t stroke prevention in AF more of an outpatient issue?
Dr. Shah: We think the hospital is a great place to start this evaluation and to make the anticoagulation decision. Of course, we should discuss these issues with the primary care doctor. Ideally, we would like to start anticoagulation during the hospital stay or on discharge, if indicated, but even if we clearly communicate a patient’s stroke and bleed risk to the PCP on discharge, we can help ensure that this issue will be addressed on outpatient follow-up.
Q: What specific tools for stroke and bleed risk are you referring to?
Dr. Shah: The CHADS2 scoring system is a well-validated tool for estimating the risk of stroke in AF patients, one that most clinicians may be aware of. The CHA2DS2-VASc is a slightly more refined scoring system. When it comes to bleeding, however, fewer clinicians are aware of the HAS-BLED bleeding risk assessment method.
Dr. Masica: The scoring systems represent a consistent, reproducible approach by which to evaluate inpatients with AF. Of course, there is some discretion for other patient-specific factors (e.g. fall risk) that are not captured in the scoring systems, but they are good starting points in the decision-making process. Finally and most importantly, although it is often overlooked, shared decision-making should take place with the patients, because their values in facing the risk of stroke versus bleeding often tip the balance one way or the other.
Q: How will the project help hospitals in this process?
Dr. Shah: We have written a QI Implementation Guide for hospitals with tools intended to improve the care of patients with AF in the hospital setting. This book will be similar to SHM’s VTE Prevention Implementation Guide, published a few years ago. We also will have an upcoming AF QI resource room within the SHM website. Additionally, similar to VTE, there are likely to be future mentored implementation projects where we will be working directly with hospitals and coaching them in this initiative.
Dr. Masica: We also have given a recent SHM-sponsored webinar that outlines some content of the guide. It can be accessed on the SHM website. This webinar reviews how to start a QI project in AF, assess your current state of care, build an interdisciplinary team, use validated tools, and deploy interventions to help make the stroke risk assessment and prophylaxis decision. I would note that the intended audience for these tools is broad and includes frontline hospitalists, QI directors, CMOs, and COOs, as well as nursing leadership, NPs, PAs, pharmacists, and other care providers.
Q: Does healthcare reform impact your efforts in this area?
Dr. Shah: Value-based purchasing, preventing readmissions, accountable care organizations, and bundled payments are all aspects of reform that will involve this therapeutic area, as their scope will impact the quality of care we deliver, how our cost structures are, and how we improve fragmentation of care across care transitions.
Dr. Masica: In addition, market forces, healthcare legislation, conceptual shifts regarding the need for systematic approaches to healthcare improvement, and new rules that may impact hospital reimbursement will continue to make AF an important healthcare quality issue. Thus, we think the discussion around delivering patient-centered care in AF is really just beginning.
Brendon Shank is SHM’s associate vice president of communications.
SHM asked leaders of the Hospital-Based Quality Improvement in Stroke Prevention for Patients with Atrial Fibrillation (AF) Project, Hiren Shah, MD, MBA, SFHM, and Andrew Masica, MD, SFHM, to provide an overview of the program.
“AF is a disease state that is highly prevalent, and the numbers are rising yearly. We also know that it is one of the most common inpatient diagnoses,” Dr. Shah says. “However, when you look at the quality of care provided to our AF patients, it is quite variable and has implications for other hospital performance metrics such as 30-day readmission rates. This makes AF a high-impact target for inpatient quality improvement initiatives.”
Dr. Shah is assistant professor of medicine at Northwestern University’s Feinberg School of Medicine and medical director at Northwestern Memorial Hospital in Chicago. Dr. Masica is vice president of clinical effectiveness at Baylor Health Care System in Dallas.
The implementation guide for SHM’s AF project will be available later in December at www.hospitalmedicine.org/afib.
Question: What is the scope of your project?
Dr. Masica: That is a question we wrestled with. Numerous care processes related to AF are amenable to inpatient quality improvement. We chose to focus our efforts on stroke prevention in AF and the development of a toolkit to help hospital-based practitioners to assess stroke and bleeding risk consistently and, if indicated, to initiate antithrombotic therapy.
Dr. Shah: Along those lines, we know that at least 25% of AF-related strokes are potentially preventable with adherence to evidence-based care; however, current data indicate that only 50% to 60% of patients with AF who are eligible to receive antithrombotic therapy are on active stroke prophylaxis.
Q: Why do you think there are such large gaps in stroke prophylaxis for AF patients?
Dr. Masica: The prophylaxis decision requires the clinician to do an anticoagulation net-benefit and risk assessment, and although there are validated tools to do this type of assessment, use of these tools hasn’t yet become hardwired into daily hospital practice. Empiric clinical assessments often overestimate the bleed risk and underestimate stroke risk, so the ultimate result can be underuse of antithrombotic therapy.
–Dr. Shah
Dr. Shah: Another barrier is that in many hospitals, there are not reminders in place in our workflow for this assessment to happen at all. Hospitalists may think that the anticoagulation decision is an outpatient issue, better addressed by their primary care doctor, so it is sometimes even intentionally bypassed. Another barrier is that it takes time to discuss a patient’s values and preferences in the anticoagulation decision.
Q: But isn’t stroke prevention in AF more of an outpatient issue?
Dr. Shah: We think the hospital is a great place to start this evaluation and to make the anticoagulation decision. Of course, we should discuss these issues with the primary care doctor. Ideally, we would like to start anticoagulation during the hospital stay or on discharge, if indicated, but even if we clearly communicate a patient’s stroke and bleed risk to the PCP on discharge, we can help ensure that this issue will be addressed on outpatient follow-up.
Q: What specific tools for stroke and bleed risk are you referring to?
Dr. Shah: The CHADS2 scoring system is a well-validated tool for estimating the risk of stroke in AF patients, one that most clinicians may be aware of. The CHA2DS2-VASc is a slightly more refined scoring system. When it comes to bleeding, however, fewer clinicians are aware of the HAS-BLED bleeding risk assessment method.
Dr. Masica: The scoring systems represent a consistent, reproducible approach by which to evaluate inpatients with AF. Of course, there is some discretion for other patient-specific factors (e.g. fall risk) that are not captured in the scoring systems, but they are good starting points in the decision-making process. Finally and most importantly, although it is often overlooked, shared decision-making should take place with the patients, because their values in facing the risk of stroke versus bleeding often tip the balance one way or the other.
Q: How will the project help hospitals in this process?
Dr. Shah: We have written a QI Implementation Guide for hospitals with tools intended to improve the care of patients with AF in the hospital setting. This book will be similar to SHM’s VTE Prevention Implementation Guide, published a few years ago. We also will have an upcoming AF QI resource room within the SHM website. Additionally, similar to VTE, there are likely to be future mentored implementation projects where we will be working directly with hospitals and coaching them in this initiative.
Dr. Masica: We also have given a recent SHM-sponsored webinar that outlines some content of the guide. It can be accessed on the SHM website. This webinar reviews how to start a QI project in AF, assess your current state of care, build an interdisciplinary team, use validated tools, and deploy interventions to help make the stroke risk assessment and prophylaxis decision. I would note that the intended audience for these tools is broad and includes frontline hospitalists, QI directors, CMOs, and COOs, as well as nursing leadership, NPs, PAs, pharmacists, and other care providers.
Q: Does healthcare reform impact your efforts in this area?
Dr. Shah: Value-based purchasing, preventing readmissions, accountable care organizations, and bundled payments are all aspects of reform that will involve this therapeutic area, as their scope will impact the quality of care we deliver, how our cost structures are, and how we improve fragmentation of care across care transitions.
Dr. Masica: In addition, market forces, healthcare legislation, conceptual shifts regarding the need for systematic approaches to healthcare improvement, and new rules that may impact hospital reimbursement will continue to make AF an important healthcare quality issue. Thus, we think the discussion around delivering patient-centered care in AF is really just beginning.
Brendon Shank is SHM’s associate vice president of communications.
Hospital Strategies for Decreasing Readmissions for Heart Failure Patients
Clinical question: What steps can hospitals take to reduce readmission rates in patients with heart failure?
Background: Evidence about various hospital strategies to decrease readmissions in patients with heart failure is limited.
Study Design: Cross-sectional study using a web-based survey.
Setting: Survey of 599 hospitals participating in quality initiatives to reduce readmissions.
Synopsis: Readmission of patients with heart failure is common and costly. Hospitals with high readmissions can lose up to 3% of their Medicare reimbursements by 2015.
This study found six strategies associated with lower risk-standardized 30-day readmission rates.
- Partnering with community physicians and physician groups (0.33%; P=0.017);
- Partnering with local hospitals (0.34%; P=0.020);
- Having nurses responsible for medication reconciliation (0.18%; P=0.002);
- Arranging follow-up visit before discharge (0.19%; P=0.037);
- Having a process in place to send all discharge summaries directly to the patient’s primary care physician (0.21%; P=0.004); and
- Assigning staff to follow up on test results after the patient is discharged (0.26%; P=0.049).
Individually, the magnitude of the effects was modest, but implementing multiple strategies was more beneficial (0.34% additional benefit for each additional strategy). Only 7% of the hospitals surveyed implemented all six strategies, highlighting substantial opportunities for improvement.
Bottom line: Implementing multiple strategies may help reduce readmission in patients with heart failure.
Citation: Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6:444-450.
Clinical question: What steps can hospitals take to reduce readmission rates in patients with heart failure?
Background: Evidence about various hospital strategies to decrease readmissions in patients with heart failure is limited.
Study Design: Cross-sectional study using a web-based survey.
Setting: Survey of 599 hospitals participating in quality initiatives to reduce readmissions.
Synopsis: Readmission of patients with heart failure is common and costly. Hospitals with high readmissions can lose up to 3% of their Medicare reimbursements by 2015.
This study found six strategies associated with lower risk-standardized 30-day readmission rates.
- Partnering with community physicians and physician groups (0.33%; P=0.017);
- Partnering with local hospitals (0.34%; P=0.020);
- Having nurses responsible for medication reconciliation (0.18%; P=0.002);
- Arranging follow-up visit before discharge (0.19%; P=0.037);
- Having a process in place to send all discharge summaries directly to the patient’s primary care physician (0.21%; P=0.004); and
- Assigning staff to follow up on test results after the patient is discharged (0.26%; P=0.049).
Individually, the magnitude of the effects was modest, but implementing multiple strategies was more beneficial (0.34% additional benefit for each additional strategy). Only 7% of the hospitals surveyed implemented all six strategies, highlighting substantial opportunities for improvement.
Bottom line: Implementing multiple strategies may help reduce readmission in patients with heart failure.
Citation: Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6:444-450.
Clinical question: What steps can hospitals take to reduce readmission rates in patients with heart failure?
Background: Evidence about various hospital strategies to decrease readmissions in patients with heart failure is limited.
Study Design: Cross-sectional study using a web-based survey.
Setting: Survey of 599 hospitals participating in quality initiatives to reduce readmissions.
Synopsis: Readmission of patients with heart failure is common and costly. Hospitals with high readmissions can lose up to 3% of their Medicare reimbursements by 2015.
This study found six strategies associated with lower risk-standardized 30-day readmission rates.
- Partnering with community physicians and physician groups (0.33%; P=0.017);
- Partnering with local hospitals (0.34%; P=0.020);
- Having nurses responsible for medication reconciliation (0.18%; P=0.002);
- Arranging follow-up visit before discharge (0.19%; P=0.037);
- Having a process in place to send all discharge summaries directly to the patient’s primary care physician (0.21%; P=0.004); and
- Assigning staff to follow up on test results after the patient is discharged (0.26%; P=0.049).
Individually, the magnitude of the effects was modest, but implementing multiple strategies was more beneficial (0.34% additional benefit for each additional strategy). Only 7% of the hospitals surveyed implemented all six strategies, highlighting substantial opportunities for improvement.
Bottom line: Implementing multiple strategies may help reduce readmission in patients with heart failure.
Citation: Bradley EH, Curry L, Horwitz LI, et al. Hospital strategies associated with 30-day readmission rates for patients with heart failure. Circ Cardiovasc Qual Outcomes. 2013;6:444-450.
Superficial and Deep/Organ-Space Surgical Site Infections Should Not Be Combined for Quality Measurement
Clinical question: What patient-risk factors predict superficial and deep/organ-space surgical site infections (SSIs) following colectomy procedures?
Background: SSIs are often targeted by policymakers for quality improvement and cost saving. Superficial and deep/organ-specific SSIs are traditionally considered a single entity for quality measurement, although they vary by anatomic location and clinical severity.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement program (ACS-NSQIP).
Synopsis: Researchers used the ACS-NSQIP registry to identify all patients who underwent colectomy procedures across 305 hospitals. Various patient variables, such as demographics, pre-operative risk factors, comorbidities, and operative information, were collected on all patients. The primary outcome was 30-day post-operative superficial SSI and deep/organ-space SSI.
Overall, 27,011 patients underwent colectomy procedures, of which 6.2% developed a superficial SSI and 4.7% developed deep/organ-space SSI. Open surgical approach (vs. laparoscopic) and current smoking were the only risk factors that predicted the occurrence of both superficial and deep/organ-space SSI. Other risk factors (e.g., post-operative diagnoses, disseminated cancer, and irradiation therapy) had a differential effect and only predicted the occurrence of deep/organ-space SSI. Elevated body mass index was strongly correlated with the occurrence of superficial SSI.
Key limitations of the study included unavailability of infection rates beyond 30 days and grouping of deep and organ-space SSIs, as the latter might vary in magnitude and significance.
Bottom Line: Risk factors that predict superficial and deep/organ-space SSI differ significantly, suggesting that future quality initiatives and reporting should evaluate different types of SSIs independently.
Citation: Lawson EH, Hall BL, Ko CY. Risk factors for superficial vs. deep/organ-space surgical site infections: implications for quality improvement initiatives [published online ahead of print July 17, 2013]. JAMA Surg.
Clinical question: What patient-risk factors predict superficial and deep/organ-space surgical site infections (SSIs) following colectomy procedures?
Background: SSIs are often targeted by policymakers for quality improvement and cost saving. Superficial and deep/organ-specific SSIs are traditionally considered a single entity for quality measurement, although they vary by anatomic location and clinical severity.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement program (ACS-NSQIP).
Synopsis: Researchers used the ACS-NSQIP registry to identify all patients who underwent colectomy procedures across 305 hospitals. Various patient variables, such as demographics, pre-operative risk factors, comorbidities, and operative information, were collected on all patients. The primary outcome was 30-day post-operative superficial SSI and deep/organ-space SSI.
Overall, 27,011 patients underwent colectomy procedures, of which 6.2% developed a superficial SSI and 4.7% developed deep/organ-space SSI. Open surgical approach (vs. laparoscopic) and current smoking were the only risk factors that predicted the occurrence of both superficial and deep/organ-space SSI. Other risk factors (e.g., post-operative diagnoses, disseminated cancer, and irradiation therapy) had a differential effect and only predicted the occurrence of deep/organ-space SSI. Elevated body mass index was strongly correlated with the occurrence of superficial SSI.
Key limitations of the study included unavailability of infection rates beyond 30 days and grouping of deep and organ-space SSIs, as the latter might vary in magnitude and significance.
Bottom Line: Risk factors that predict superficial and deep/organ-space SSI differ significantly, suggesting that future quality initiatives and reporting should evaluate different types of SSIs independently.
Citation: Lawson EH, Hall BL, Ko CY. Risk factors for superficial vs. deep/organ-space surgical site infections: implications for quality improvement initiatives [published online ahead of print July 17, 2013]. JAMA Surg.
Clinical question: What patient-risk factors predict superficial and deep/organ-space surgical site infections (SSIs) following colectomy procedures?
Background: SSIs are often targeted by policymakers for quality improvement and cost saving. Superficial and deep/organ-specific SSIs are traditionally considered a single entity for quality measurement, although they vary by anatomic location and clinical severity.
Study design: Retrospective cohort study.
Setting: American College of Surgeons National Surgical Quality Improvement program (ACS-NSQIP).
Synopsis: Researchers used the ACS-NSQIP registry to identify all patients who underwent colectomy procedures across 305 hospitals. Various patient variables, such as demographics, pre-operative risk factors, comorbidities, and operative information, were collected on all patients. The primary outcome was 30-day post-operative superficial SSI and deep/organ-space SSI.
Overall, 27,011 patients underwent colectomy procedures, of which 6.2% developed a superficial SSI and 4.7% developed deep/organ-space SSI. Open surgical approach (vs. laparoscopic) and current smoking were the only risk factors that predicted the occurrence of both superficial and deep/organ-space SSI. Other risk factors (e.g., post-operative diagnoses, disseminated cancer, and irradiation therapy) had a differential effect and only predicted the occurrence of deep/organ-space SSI. Elevated body mass index was strongly correlated with the occurrence of superficial SSI.
Key limitations of the study included unavailability of infection rates beyond 30 days and grouping of deep and organ-space SSIs, as the latter might vary in magnitude and significance.
Bottom Line: Risk factors that predict superficial and deep/organ-space SSI differ significantly, suggesting that future quality initiatives and reporting should evaluate different types of SSIs independently.
Citation: Lawson EH, Hall BL, Ko CY. Risk factors for superficial vs. deep/organ-space surgical site infections: implications for quality improvement initiatives [published online ahead of print July 17, 2013]. JAMA Surg.
MARQUIS Highlights Need for Improved Medication Reconciliation
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
![]()
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.1
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Listen to more of our interview with MARQUIS principal investigator Jeffrey Schnipper, MD, MPH, FHM.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website. TH
Larry Beresford is a freelance writer in San Francisco.
Reference
1. Schnipper JL, Mueller SK, Salanitro AH, Stein J. Got Med Wreck? Targeted Repairs from the Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS). PowerPoint presentation at Society of Hospital Medicine annual meeting, May 16-19, 2013, National Harbor, Md.
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
![]()
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.1
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Listen to more of our interview with MARQUIS principal investigator Jeffrey Schnipper, MD, MPH, FHM.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website. TH
Larry Beresford is a freelance writer in San Francisco.
Reference
1. Schnipper JL, Mueller SK, Salanitro AH, Stein J. Got Med Wreck? Targeted Repairs from the Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS). PowerPoint presentation at Society of Hospital Medicine annual meeting, May 16-19, 2013, National Harbor, Md.
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
![]()
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.1
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Listen to more of our interview with MARQUIS principal investigator Jeffrey Schnipper, MD, MPH, FHM.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website. TH
Larry Beresford is a freelance writer in San Francisco.
Reference
1. Schnipper JL, Mueller SK, Salanitro AH, Stein J. Got Med Wreck? Targeted Repairs from the Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS). PowerPoint presentation at Society of Hospital Medicine annual meeting, May 16-19, 2013, National Harbor, Md.
Society of Hospital Medicine’s MARQUIS Initiative Highlights Need For Improved Medication Reconciliation


–Jeffrey Schnipper, MD, MPH, FHM
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
The concept of the “best possible medication history” (BPMH) originated with patient-safety expert Edward Etchells, MD, MSc, at Sunnybrook Health Sciences Centre in Toronto. The concept is outlined on a pocket reminder card for MARQUIS participants, explained co-presenter and principal investigator Jeffrey Schnipper MD, MPH, FHM, a hospitalist at Brigham & Women’s Hospital in Boston.
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website at www.hospitalmedicine.org/marquis.
Larry Beresford is a freelance writer in San Francisco.
–Jeffrey Schnipper, MD, MPH, FHM
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
The concept of the “best possible medication history” (BPMH) originated with patient-safety expert Edward Etchells, MD, MSc, at Sunnybrook Health Sciences Centre in Toronto. The concept is outlined on a pocket reminder card for MARQUIS participants, explained co-presenter and principal investigator Jeffrey Schnipper MD, MPH, FHM, a hospitalist at Brigham & Women’s Hospital in Boston.
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website at www.hospitalmedicine.org/marquis.
Larry Beresford is a freelance writer in San Francisco.
–Jeffrey Schnipper, MD, MPH, FHM
What is the best possible medication history? How is it done? Who should do it? When should it be done during a patient’s journey in and out of the hospital? What medication discrepancies—and potential adverse drug events—are most likely?
Those are questions veteran hospitalist Jason Stein, MD, tried to answer during an HM13 breakout session on medication reconciliation at the Gaylord National Resort and Conference Center in National Harbor, Md.
“How do you know as the discharging provider if the medication list you’re looking at is gold or garbage?” said Dr. Stein, associate director for quality improvement (QI) at Emory University in Atlanta and a mentor for SHM’s Multi-Center Medication Reconciliation Quality Improvement Study (MARQUIS) quality-research initiative.
The concept of the “best possible medication history” (BPMH) originated with patient-safety expert Edward Etchells, MD, MSc, at Sunnybrook Health Sciences Centre in Toronto. The concept is outlined on a pocket reminder card for MARQUIS participants, explained co-presenter and principal investigator Jeffrey Schnipper MD, MPH, FHM, a hospitalist at Brigham & Women’s Hospital in Boston.
“Sometimes it’s impossible to know what the patient was or wasn’t taking, but it doesn’t mean you don’t do your best,” he said, adding that hospitalists should attempt to get at least one reliable, corroborating source of information for a patient’s medical history.
Sometimes it is necessary to speak to family members or the community pharmacy, Dr. Schnipper said, because many patients can’t remember all of the drugs they are taking. Trying to do medication reconciliation at the time of discharge when BPMH has not been done can lead to more work for the provider, medication errors, or rehospitalizations. Ideally, knowledge of what the patient was taking before admission, as well as the patient’s health literacy and adherence history, should be gathered and documented once, early, and well during the hospitalization by a trained provider, according to Dr. Schnipper.
An SHM survey, however, showed 50% to 70% percent of front-line providers have never received BPMH training, and 60% say they are not given the time.
“Not knowing means a diligent provider would need to take a BPMH at discharge, which is a waste,” Dr. Stein said. It would be nice to tell from the electronic health record whether a true BPMH had been taken for every hospitalized patient—or at least every high-risk patient—but this goal is not well-supported by current information technology, MARQUIS investigators said they have learned.
The MARQUIS program was launched in 2011 with a grant from the federal Agency for Healthcare Research and Quality. It began with a thorough review of the literature on medication reconciliation and the development of a toolkit of best practices. In 2012, six pilot sites were offered a menu of 11 MARQUIS medication-reconciliation interventions to choose from and help in implementing them from an SHM mentor, with expertise in both QI and medication safety.
Participating sites have mobilized high-level hospital leadership and utilize a local champion, usually a hospitalist, tools for assessing high-risk patients, medication-reconciliation assistants or counselors, and pharmacist involvement. Different sites have employed different professional staff to take medication histories.
Dr. Schnipper said he expects another round of MARQUIS-mentored implementation, probably in 2014, after data from the first round have been analyzed. The program is tracking such outcomes as the number of potentially harmful, unintentional medication discrepancies per patient at participating sites.
The MARQUIS toolkit is available on the SHM website at www.hospitalmedicine.org/marquis.
Larry Beresford is a freelance writer in San Francisco.
Boston Hospital Earns Quality Award
In July, four U.S. hospitals were recognized for their leadership and innovation in quality improvement (QI) and safety—as defined by the Institute of Medicine (IOM)—through the American Hospital Association’s McKesson Quest for Quality Prize.2 Beth Israel Deaconess Medical Center (BIDMC) in Boston was awarded the overall prize for its sustainable approach and hospitalwide commitment to pursuing IOM’s quality aims for safe, effective, efficient, timely, patient-centered, and equitable health care.
The award, presented since 2002, is supported by healthcare-services company McKesson Corp., based in San Francisco.
Key to BIDMC’s success is the clear message of its top leadership’s commitment to quality and a strong partnership with the medical community, says Kenneth Sands, MD, MPH, BIDMC’s senior vice president for healthcare quality. “That includes an official vote by the hospital’s board to adopt IOM’s definition of quality. And everyone here participates in the quality process,” he says.
Each year, the hospital holds a quality symposium featuring QI projects solicited from across the organization. This year’s poster contest recognized three winners, one from the finance department, one from an ICU, and a third from the hospital cafeteria (it tracked the percentage of days that fresh fish is offered as a healthy menu choice).
“To see these three winners standing together on the podium sends a powerful message,” Dr. Sands says. “These are not quality-improvement experts, but front-line staff.”
Another quality initiative involves a hospitalist leader trying to promote “conversation readiness” for a hospital staff’s ability to respond to patients’ expressed desires to complete advance directives, then make sure these documents get captured in the medical record.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
In July, four U.S. hospitals were recognized for their leadership and innovation in quality improvement (QI) and safety—as defined by the Institute of Medicine (IOM)—through the American Hospital Association’s McKesson Quest for Quality Prize.2 Beth Israel Deaconess Medical Center (BIDMC) in Boston was awarded the overall prize for its sustainable approach and hospitalwide commitment to pursuing IOM’s quality aims for safe, effective, efficient, timely, patient-centered, and equitable health care.
The award, presented since 2002, is supported by healthcare-services company McKesson Corp., based in San Francisco.
Key to BIDMC’s success is the clear message of its top leadership’s commitment to quality and a strong partnership with the medical community, says Kenneth Sands, MD, MPH, BIDMC’s senior vice president for healthcare quality. “That includes an official vote by the hospital’s board to adopt IOM’s definition of quality. And everyone here participates in the quality process,” he says.
Each year, the hospital holds a quality symposium featuring QI projects solicited from across the organization. This year’s poster contest recognized three winners, one from the finance department, one from an ICU, and a third from the hospital cafeteria (it tracked the percentage of days that fresh fish is offered as a healthy menu choice).
“To see these three winners standing together on the podium sends a powerful message,” Dr. Sands says. “These are not quality-improvement experts, but front-line staff.”
Another quality initiative involves a hospitalist leader trying to promote “conversation readiness” for a hospital staff’s ability to respond to patients’ expressed desires to complete advance directives, then make sure these documents get captured in the medical record.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
In July, four U.S. hospitals were recognized for their leadership and innovation in quality improvement (QI) and safety—as defined by the Institute of Medicine (IOM)—through the American Hospital Association’s McKesson Quest for Quality Prize.2 Beth Israel Deaconess Medical Center (BIDMC) in Boston was awarded the overall prize for its sustainable approach and hospitalwide commitment to pursuing IOM’s quality aims for safe, effective, efficient, timely, patient-centered, and equitable health care.
The award, presented since 2002, is supported by healthcare-services company McKesson Corp., based in San Francisco.
Key to BIDMC’s success is the clear message of its top leadership’s commitment to quality and a strong partnership with the medical community, says Kenneth Sands, MD, MPH, BIDMC’s senior vice president for healthcare quality. “That includes an official vote by the hospital’s board to adopt IOM’s definition of quality. And everyone here participates in the quality process,” he says.
Each year, the hospital holds a quality symposium featuring QI projects solicited from across the organization. This year’s poster contest recognized three winners, one from the finance department, one from an ICU, and a third from the hospital cafeteria (it tracked the percentage of days that fresh fish is offered as a healthy menu choice).
“To see these three winners standing together on the podium sends a powerful message,” Dr. Sands says. “These are not quality-improvement experts, but front-line staff.”
Another quality initiative involves a hospitalist leader trying to promote “conversation readiness” for a hospital staff’s ability to respond to patients’ expressed desires to complete advance directives, then make sure these documents get captured in the medical record.
Larry Beresford is a freelance writer in San Francisco.
References
- Harrison J, Quinn K, Mourad M. Is anyone home? The association between being reached for a post-discharge telephone call and 30-day hospital readmission. Harrison J, Quinn K, Mourad M. Any questions? The relationship between responses to post-discharge call questions and 30-day hospital readmissions [abstracts]. Journal of Hospital Medicine, 2013, 8 Suppl 1.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Institute of Medicine website. Available at: http://www.iom.edu/~/media/Files/Report%20Files/2001/Crossing-the-Quality-Chasm/Quality%20Chasm%202001%20%20report%20brief.pdf. Accessed Sept. 9, 2013.
- Shlaes DM, Sahm D, Opiela C, Spellberg B. Commentary: the FDA reboot of antibiotic development. Antimicrob Agents Chemother. 29 Jul 2013 [Epub ahead of print].
- Alliance for Aging Research. HAIs growing problem, group says. Alliance for Aging Research website. Available at: http://www.agingresearch.org/content/article/detail/33504. Accessed Sept. 9, 2013.
- Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. N Engl J Med. 2013;368:2255-2265.
- Hospitals in Pursuit of Excellence. Eliminating catheter-associated urinary tract infections. Hospitals in Pursuit of Excellence website. Available at: http://www.hpoe.org/Reports-HPOE/eliminating_catheter_associated_urinary_tract_infection.pdf. Accessed Sept. 9, 2013.
- Center to Advance Palliative Care. Growth of palliative care in U.S. hospitals 2013 snapshot. Center to Advance Palliative Care website. Available at: http://www.capc.org/capc-growth-analysis-snapshot-2013.pdf. Accessed Sept. 9, 2013.
New Thinking, Higher Expectations Needed to Solve Hospital Readmission Problem


As we enter a new era of health-care and payment reform, we are all keenly aware of the need to limit unnecessary readmissions. We have been given tools and tips on how to most efficiently and effectively transition patients from the hospital setting to the outpatient world in order to limit the chances that they will “bounce back” to us, resulting in penalties to our hospital or health-care system. Tools such as Project BOOST and others help us to educate patients, transfer information effectively, follow up on patients post-discharge, and reconcile medications safely across the continuum of care. But without a competent and committed provider of care to “catch” the patient on the other side, we might just be dropping the ball yet again.
It is imperative as we look to safely transition patients into the next level of care that we, as hospitalists, get outside the box and begin to engage the community of care providers outside our walls, and yes, even outside of our control. We have been down this road before with other quality initiatives, which at first glance appeared to be outside our sphere of influence—such projects as post-operative antibiotic use and hospitalwide DVT prophylaxis. Given the right hospitalist leader, with the right set of leadership tools, these quality-improvement (QI) projects have been widely successful in many environments.
I would suggest that the issue of safe transitions for our patients is no different, and maybe more important, to the health and safety of our patients.
Solving the readmission problem on a local level requires an analytical approach, much like a “root-cause analysis.” We need to begin to examine the sources of our readmitted patients, as well as the routes of our discharged patients, and we need to ask ourselves if we are continuing to feed patients into the vicious circle that results in readmissions. Are there post-acute-care facilities in your area that are responsible for more than their fair share of patients returning to your service? If so, why do we continue to discharge patients to their care? Is it because we are pressured to lower length of stay, and any bed at the next level of care is better than another day in the acute-care hospital? At some point, this reasoning fails, and given the penalties coming soon, it may be better to begin to more discriminately discharge patients to facilities that provide higher-quality care and assist us in our goals to reduce unnecessary readmissions. Leading the charge in this endeavor also necessitates that we begin to engage those providers on the other side, making them aware of the quality data related to their facility and providing education and resources to assist them in improving their performance.
Realities of the Care Continuum
Several options pertaining to hospitalist groups are available. The first, already a large movement in our current marketplace, is to extend the current hospitalist group across the chasm and begin to deliver care in those post-acute facilities. Long-term acute care (LTAC) and skilled nursing facilities (SNF) are prime examples of this movement; the obvious advantage lies in the effective control of quality and efficient transfer of information that a single group can achieve when it extends to these facilities. Obviously, manpower issues and financial support are drawbacks in a model such as this.
More realistically, a group might consider taking a less aggressive approach to this problem. Educating care providers and assisting these facilities with QI projects would require fewer resources and might provide a higher return on investment (ROI) for your group and hospital. Engaging these physicians, nonphysician providers, and facility administrators is key to our ability to impact this problem. Demanding quality care for our discharged patients in terms of timeliness of follow-up, adherence to care paths, and responsiveness to changes in condition should be non-negotiable and factored into our development of referral patterns.
As our population of patients continues to be more acutely ill, and the level of care provided at post-acute care facilities continues to rise, our current reality is that a majority of these patients, at any given time, meet hospital admissions criteria. Preventing readmissions requires that post-acute care providers have mechanisms in place to stop the “knee-jerk” transfer to the emergency department, rather than attempt to evaluate and treat the patient in the facility. Interact II (http://interact2.net/index.aspx) is a resource that provides tools for post-acute-care facilities to use in monitoring their own internal data around acute-care transfers. It also provides tracking tools, communication strategies, advanced-care-planning tools, and clinical pathways for limiting the number of acute-care transfers. The reality is, once these patients end up in the emergency department, they are likely to be referred to us for consideration of readmission. The best way to stop this is to stop the transfer before it happens.
Demand Better
We, as hospitalists, need to begin to leverage our own “buying power” as it relates to the care of our patients post-discharge. We can start by educating and assisting care providers on a local level to improve compliance with well-known standards of care that prevent unnecessary readmissions. We need to be prepared to wield our collective weight as a specialty to demand from our post-acute care colleagues what has been demanded of us over the last several years: quality and value. Make no mistake—hospitalists have to get outside the box.
Dr. Harrington is an SHM board member and chief medical officer of Locum Leaders in Alpharetta, Ga.
As we enter a new era of health-care and payment reform, we are all keenly aware of the need to limit unnecessary readmissions. We have been given tools and tips on how to most efficiently and effectively transition patients from the hospital setting to the outpatient world in order to limit the chances that they will “bounce back” to us, resulting in penalties to our hospital or health-care system. Tools such as Project BOOST and others help us to educate patients, transfer information effectively, follow up on patients post-discharge, and reconcile medications safely across the continuum of care. But without a competent and committed provider of care to “catch” the patient on the other side, we might just be dropping the ball yet again.
It is imperative as we look to safely transition patients into the next level of care that we, as hospitalists, get outside the box and begin to engage the community of care providers outside our walls, and yes, even outside of our control. We have been down this road before with other quality initiatives, which at first glance appeared to be outside our sphere of influence—such projects as post-operative antibiotic use and hospitalwide DVT prophylaxis. Given the right hospitalist leader, with the right set of leadership tools, these quality-improvement (QI) projects have been widely successful in many environments.
I would suggest that the issue of safe transitions for our patients is no different, and maybe more important, to the health and safety of our patients.
Solving the readmission problem on a local level requires an analytical approach, much like a “root-cause analysis.” We need to begin to examine the sources of our readmitted patients, as well as the routes of our discharged patients, and we need to ask ourselves if we are continuing to feed patients into the vicious circle that results in readmissions. Are there post-acute-care facilities in your area that are responsible for more than their fair share of patients returning to your service? If so, why do we continue to discharge patients to their care? Is it because we are pressured to lower length of stay, and any bed at the next level of care is better than another day in the acute-care hospital? At some point, this reasoning fails, and given the penalties coming soon, it may be better to begin to more discriminately discharge patients to facilities that provide higher-quality care and assist us in our goals to reduce unnecessary readmissions. Leading the charge in this endeavor also necessitates that we begin to engage those providers on the other side, making them aware of the quality data related to their facility and providing education and resources to assist them in improving their performance.
Realities of the Care Continuum
Several options pertaining to hospitalist groups are available. The first, already a large movement in our current marketplace, is to extend the current hospitalist group across the chasm and begin to deliver care in those post-acute facilities. Long-term acute care (LTAC) and skilled nursing facilities (SNF) are prime examples of this movement; the obvious advantage lies in the effective control of quality and efficient transfer of information that a single group can achieve when it extends to these facilities. Obviously, manpower issues and financial support are drawbacks in a model such as this.
More realistically, a group might consider taking a less aggressive approach to this problem. Educating care providers and assisting these facilities with QI projects would require fewer resources and might provide a higher return on investment (ROI) for your group and hospital. Engaging these physicians, nonphysician providers, and facility administrators is key to our ability to impact this problem. Demanding quality care for our discharged patients in terms of timeliness of follow-up, adherence to care paths, and responsiveness to changes in condition should be non-negotiable and factored into our development of referral patterns.
As our population of patients continues to be more acutely ill, and the level of care provided at post-acute care facilities continues to rise, our current reality is that a majority of these patients, at any given time, meet hospital admissions criteria. Preventing readmissions requires that post-acute care providers have mechanisms in place to stop the “knee-jerk” transfer to the emergency department, rather than attempt to evaluate and treat the patient in the facility. Interact II (http://interact2.net/index.aspx) is a resource that provides tools for post-acute-care facilities to use in monitoring their own internal data around acute-care transfers. It also provides tracking tools, communication strategies, advanced-care-planning tools, and clinical pathways for limiting the number of acute-care transfers. The reality is, once these patients end up in the emergency department, they are likely to be referred to us for consideration of readmission. The best way to stop this is to stop the transfer before it happens.
Demand Better
We, as hospitalists, need to begin to leverage our own “buying power” as it relates to the care of our patients post-discharge. We can start by educating and assisting care providers on a local level to improve compliance with well-known standards of care that prevent unnecessary readmissions. We need to be prepared to wield our collective weight as a specialty to demand from our post-acute care colleagues what has been demanded of us over the last several years: quality and value. Make no mistake—hospitalists have to get outside the box.
Dr. Harrington is an SHM board member and chief medical officer of Locum Leaders in Alpharetta, Ga.
As we enter a new era of health-care and payment reform, we are all keenly aware of the need to limit unnecessary readmissions. We have been given tools and tips on how to most efficiently and effectively transition patients from the hospital setting to the outpatient world in order to limit the chances that they will “bounce back” to us, resulting in penalties to our hospital or health-care system. Tools such as Project BOOST and others help us to educate patients, transfer information effectively, follow up on patients post-discharge, and reconcile medications safely across the continuum of care. But without a competent and committed provider of care to “catch” the patient on the other side, we might just be dropping the ball yet again.
It is imperative as we look to safely transition patients into the next level of care that we, as hospitalists, get outside the box and begin to engage the community of care providers outside our walls, and yes, even outside of our control. We have been down this road before with other quality initiatives, which at first glance appeared to be outside our sphere of influence—such projects as post-operative antibiotic use and hospitalwide DVT prophylaxis. Given the right hospitalist leader, with the right set of leadership tools, these quality-improvement (QI) projects have been widely successful in many environments.
I would suggest that the issue of safe transitions for our patients is no different, and maybe more important, to the health and safety of our patients.
Solving the readmission problem on a local level requires an analytical approach, much like a “root-cause analysis.” We need to begin to examine the sources of our readmitted patients, as well as the routes of our discharged patients, and we need to ask ourselves if we are continuing to feed patients into the vicious circle that results in readmissions. Are there post-acute-care facilities in your area that are responsible for more than their fair share of patients returning to your service? If so, why do we continue to discharge patients to their care? Is it because we are pressured to lower length of stay, and any bed at the next level of care is better than another day in the acute-care hospital? At some point, this reasoning fails, and given the penalties coming soon, it may be better to begin to more discriminately discharge patients to facilities that provide higher-quality care and assist us in our goals to reduce unnecessary readmissions. Leading the charge in this endeavor also necessitates that we begin to engage those providers on the other side, making them aware of the quality data related to their facility and providing education and resources to assist them in improving their performance.
Realities of the Care Continuum
Several options pertaining to hospitalist groups are available. The first, already a large movement in our current marketplace, is to extend the current hospitalist group across the chasm and begin to deliver care in those post-acute facilities. Long-term acute care (LTAC) and skilled nursing facilities (SNF) are prime examples of this movement; the obvious advantage lies in the effective control of quality and efficient transfer of information that a single group can achieve when it extends to these facilities. Obviously, manpower issues and financial support are drawbacks in a model such as this.
More realistically, a group might consider taking a less aggressive approach to this problem. Educating care providers and assisting these facilities with QI projects would require fewer resources and might provide a higher return on investment (ROI) for your group and hospital. Engaging these physicians, nonphysician providers, and facility administrators is key to our ability to impact this problem. Demanding quality care for our discharged patients in terms of timeliness of follow-up, adherence to care paths, and responsiveness to changes in condition should be non-negotiable and factored into our development of referral patterns.
As our population of patients continues to be more acutely ill, and the level of care provided at post-acute care facilities continues to rise, our current reality is that a majority of these patients, at any given time, meet hospital admissions criteria. Preventing readmissions requires that post-acute care providers have mechanisms in place to stop the “knee-jerk” transfer to the emergency department, rather than attempt to evaluate and treat the patient in the facility. Interact II (http://interact2.net/index.aspx) is a resource that provides tools for post-acute-care facilities to use in monitoring their own internal data around acute-care transfers. It also provides tracking tools, communication strategies, advanced-care-planning tools, and clinical pathways for limiting the number of acute-care transfers. The reality is, once these patients end up in the emergency department, they are likely to be referred to us for consideration of readmission. The best way to stop this is to stop the transfer before it happens.
Demand Better
We, as hospitalists, need to begin to leverage our own “buying power” as it relates to the care of our patients post-discharge. We can start by educating and assisting care providers on a local level to improve compliance with well-known standards of care that prevent unnecessary readmissions. We need to be prepared to wield our collective weight as a specialty to demand from our post-acute care colleagues what has been demanded of us over the last several years: quality and value. Make no mistake—hospitalists have to get outside the box.
Dr. Harrington is an SHM board member and chief medical officer of Locum Leaders in Alpharetta, Ga.
Project BOOST Study Documents Modest Impact on 30-Day Hospital Readmissions

Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Initial research on outcomes following Project BOOST (Better Outcomes for Older Adults through Safe Transitions) implementation shows modest improvement in rehospitalization rates. Moreover, some experts suggest the real problem might lie in using 30-day hospital readmissions, now a target for Medicare reimbursement penalties, as the quality metric for care transitions out of the hospital.
Study data showed a 2% absolute reduction in all-patient, 30-day readmission rates at 11 of the original 30 BOOST sites (to 12.7% from 14.7%), according to an article in the August issue of the Journal of Hospital Medicine.1
“Everybody has talked about readmissions as the quality target, but really it should be about improving transitions of care for the patient going home,” says Ashish Jha, MD, MPH, of the Harvard School of Public Health, Health Policy and Management. “If we’re going to use readmissions as our quality measure, maybe we’re set up to fail. Can we do care transitions better? Yes, we can. Can we do better quality measures? Yes. My take-home message is that we should get clearer on what we are trying to achieve.”
Project BOOST (www.hospitalmedicine.org/boost) has been a major quality initiative for SHM since 2008 and one of several national programs aimed at helping hospitals improve care-transitions processes and patient outcomes. BOOST offers participating sites an online toolkit of strategies and interventions, along with the support of an expert mentor.
“Participation in Project BOOST appeared to be associated with a decrease in readmission rates,” the authors conclude. But two accompanying editorials in the journal expressed disappointment with a lack of “robustness” to these results and lack of participation by BOOST sites.2,3 The editorials also acknowledge the challenges of multisite, voluntary research on a topic that, so far, has largely resisted validated, generalizable research outcomes demonstrating what really works in preventing readmissions.
“I think people want a silver bullet on this issue,” says lead author Luke Hansen, MD, MHS, of the division of hospital medicine at Northwestern University Feinberg School of Medicine in Chicago. “They want to be able to define an intervention to take care of all of the avoidable fraction of rehospitalizations. But I don’t think that’s possible. The disappointment may come from the fact that this is a more complicated issue than we thought.”
Dr. Hansen says data reporting was voluntary and uncompensated, and the BOOST research team is trying to facilitate better reporting from subsequent cohorts. He says one of BOOST’s unique aspects—tailoring interventions to local circumstances—could be a drawback to outcomes research. “We have to incorporate the diversity of experience into our research methods and our expectations,” he says.
Hospitalist Bradley Flansbaum, DO, MPH, FACP, SFHM, of Lenox Hill Hospital in New York City says BOOST reinforces many of things hospitalists should be doing to provide optimal discharges and transitions
.
—Ashish Jha, MD, MPH, Harvard School of Public Health, Health Policy, and Management, Boston
“Like appropriate teaching and patient education, medication reconciliation, and setting up follow-up appointments,” says Dr. Flansbaum, a member of SHM’s Public Policy Committee and regular contributor to SHM’s Practice Management blog. “But if there was one thing I’d like hospitalists to take home from this research, it’s the cognitive dissonance—the challenge of matching the evidence with what the regulatory bodies expect from us and knowing that the evidence is falling short.
“As much as we might be held accountable for outcomes like readmissions, the reality is that we can’t control them. What we’re learning is that this is really hard to do.”
Amy Boutwell, MD, MPP, a hospitalist in Newton, Mass., and founder of Collaborative Healthcare Strategies, agrees transitions of care are difficult. However, she also thinks hospitals and hospitalists cannot wait for conclusive research that proves what works in preventing readmissions.
“The BOOST results reflect my own experience working with more than a hundred STAAR [State Action on Avoidable Readmissions] hospitals. We haven’t yet been able to sufficiently extract the data about readmissions from the field—and we need to figure out how to do that,” she says. “But when you look at the issue from a patient’s perspective and their desire for a safe transition, why would you not do the things recommended by Project BOOST and similar initiatives?”
Primary-care physicians (PCPs) need to know about major changes in a discharged patient’s plan of care in a timely manner, along with any results from pending lab tests, Dr. Boutwell explains. She emphasizes that patients and their caregivers need to be given clear discharge instructions when they leave the hospital.
“We have an obligation to do what we know to be best practices and standards of care. The BOOST toolkit of recommendations is very comprehensive and gives hospitals a lot of options to improve their internal processes,” Dr. Boutwell says. “It’s hard to argue against any of them, even if it’s hard to draw clear links between them and readmissions rates. These are the self-evident, basic tasks that I would want done for myself or my child or my parent, if we were in the hospital.”
Larry Beresford is a freelance writer in San Francisco.
References
- Hansen L, Greenwald J, Budnitz T, et al. Project BOOST: Effectiveness of a multihospital effort to reduce rehospitalization. J Hosp Med. 2013;8(8):421-427. doi: 10.1002/jhm.2054. Epub 2013 Jul 22.
- Auerbach A, Fang M, Glasheen J, Brotman D, O’Leary KJ, Horwitz LJ. BOOST: Evidence needing a lift. J Hosp Med. 2013;8(8):468-469. doi: 10.1002/jhm.2065. Epub 2013 Jul 22.
- Jha A. BOOST and readmissions: Thinking beyond the walls of the hospital. J Hosp Med. 2013;8(8):470-471. doi: 10.1002/jhm.2069. Epub 2013 Jul 22.
Medicare Penalties Make Hospital-Acquired-Infection Solutions a Priority
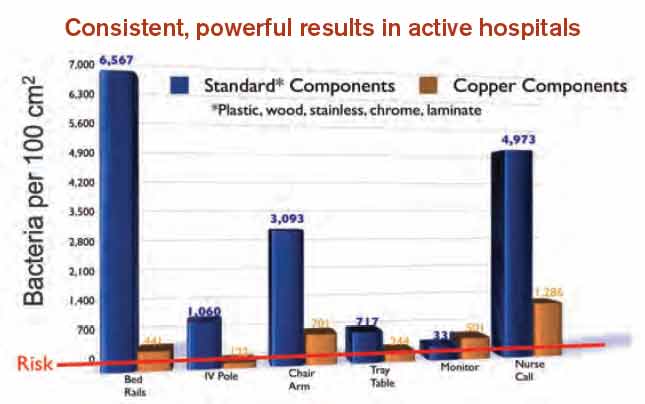
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
A shift in governmental regulations regarding reimbursement for hospital-acquired infections (HAIs) is forcing hospitals to take a closer look at how to reduce them. A recent study in Infection Control and Hospital Epidemiology shows that copper-alloy surfaces may be one such solution.3 According to the study, although only 9% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases.1
“Before these regulations, hospitals didn’t necessarily want technology to decrease HAI rates, because the more infections and complications, the longer the length of patient stay, the greater the reimbursement, and the better the bottom line,” says Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association.
Three regulations that have resulted in reimbursements to hospitals getting cut include:
- The Deficit Reduction Act of 2005, which was implemented on Oct. 1, 2008, which states that Medicare will not reimburse for certain types of HAIs;
- Section 3025 of the Affordable Care Act (signed into law in 2010), which incentivizes hospitals to decrease their readmission rates, which frequently are caused by HAIs. Beginning this fall, hospitals are getting reduced reimbursement when their readmission rates exceed a certain threshold. The maximum penalty in 2013 is 1% and will increase to 3% by 2015; and
- Section 1886 of the Affordable Care Act, which describes value-based purchasing and makes hospitals eligible to receive incentive payments for achieving better care on certain quality metrics. Funding for the program comes from withholding payment from poor-performing hospitals. The financial impact to hospitals started this year. In 2014, urinary tract infections and vascular-catheter-associated infections will be among the targeted conditions measured by CMS to calculate incentives and penalties.
“Hospitals are now feeling a direct impact from all of this,” Dr. Georgiou says. “Back in 2008, hospitals were noticing, but it was hard to get their attention since only one program was impacting their bottom line. But, pretty soon, hospitals risk losing upwards of 5% of their Medicare reimbursement for decreased quality.
“Reducing HAIs is clearly on the priority list of chief operating officers. They are very aware of the impact to their bottom line. They are looking to their vendors and suppliers to develop strategies to work with their hospitals to improve performance around these metrics.”
Karen Appold is a freelance writer in Pennsylvania.
How Copper Could Solve Problem of Hospital-Acquired Infections

—James Pile, MD, FACP, SFHM, vice chair, department of hospital medicine, Cleveland Clinic
Hospital-acquired infections (HAIs) are on the rise despite efforts to decrease them. HAIs cause an estimated 100,000 deaths annually and account for up to $45 billion in health-care costs. Adding fuel to the fire, bacteria increasingly are becoming resistant to last-resort drugs. Despite this gloomy outlook, a recent study in Infection Control and Hospital Epidemiology shows that a material known for its antimicrobial properties for more than 4,000 years—copper—might be a light at the end of this darkening tunnel.1
Ancient Indians stored water in copper pots to prevent illness, says lead study author Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, and medical director for infection prevention at the Medical University of South Carolina (MUSC) in Charleston. But copper rarely is used in that manner today because molded plastics and stainless steel are less expensive and easier to mass-produce.
Dr. Salgado explains that the antimicrobial effect of copper-alloy surfaces is a result of the metal stealing electrons from the bacteria when they come into contact with each other. “Once the bacteria donate the electrons to the copper metal, this places the organism into a state of electrical-charge deficit,” she says. “As a consequence, free radicals are generated inside the cell, which ultimately leads to the cell’s death.”
Copper-alloy surfaces kill 99.9% of bacteria in less than two hours, says Harold T. Michels, PhD, PE, senior vice president of technology and technical services for Copper Development Association Inc. in New York, who was a study author. On other surfaces, bacteria may live for multiple days or even months.
Unlike current methods used to decrease HAIs (i.e. hand-washing and sanitizing surfaces), copper components don’t require human intervention or compliance to be effective.
“It supplements what these other things can do; it’s in the background and it’s always working,” Michels says.

—Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, medical director for infection prevention, Medical University of South Carolina, Charleston
Study Specifics
To conduct the study, copper prototypes of items touched most frequently by patients, health-care providers, and visitors were made and placed in patient rooms located within ICUs. “We placed the copper around the patient [much like a defensive perimeter] to reduce the likelihood that the health-care worker or visitor would introduce the infectious agent to the patient,” says the study’s lead investigator, Michael Schmidt, PhD, a professor and vice chair of MUSC’s department of microbiology and immunology.
Then, bacterial loads were measured on each object. For every study room, there was a control room without copper objects. Researchers were most interested in methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). For a period of time, bacterial burdens were measured in both copper rooms and control rooms.
Results exceeded the researchers’ expectations. Although only 7% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases. The rate of HAI and/or MRSA or VRE colonization in ICU rooms with copper-alloy surfaces was significantly lower than that in standard ICU rooms (0.071 versus 0.123). For HAIs only, the rate was reduced to 0.034 from 0.081.3
“We were pleasantly surprised with the reductions,” Dr. Salgado says. “We consistently saw a more than 50% reduction in HAIs in all study sites.”
Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association, is an advocate for making the health-care system simpler and safer for consumers. She says copper is a “game-changer.”
“It’s a brand-new way of thinking about decreasing the number of HAIs,” she says.
Green Light?
In light of the study’s encouraging findings, hospitalist and infectious-disease specialist James Pile, MD, FACP, SFHM, vice chair of the Department of Hospital Medicine at Cleveland Clinic, says that although study results appear valid, “it didn’t provide any final answers.”

“It would be premature for a hospital to install copper based on this study,” he says, adding he didn’t find the study results surprising, because copper is known to have antimicrobial properties.
But, Dr. Pile says, the study did provide proof of concept and opens the door for larger, more definitive studies that will show if installing copper in hospital rooms is worthwhile.
“If future studies confirm earlier results, then hospitals should seriously consider copper installations,” he says.
Barriers to Implementation
Despite the promising outlook for copper in dramatically reducing HAIs, implantation of copper components is off to a slow start.
Negotiations with the Environmental Protection Agency, the federal agency with jurisdiction over public-health claims for antimicrobial surfaces, started in 2004. Testing started in 2005. Although federal registration was completed in February 2008, it wasn’t until late 2011 that all regulatory issues were resolved for manufacturers.
“The regulatory process created delays in educating hospitals and the public about copper’s effectiveness in killing certain bacteria,” Dr. Georgiou explains. “As a result, American manufacturers with the ability to make copper components weren’t developing products because they couldn’t sell them.”
Now that the regulatory issues have been resolved, U.S. manufacturers are beginning to make copper components. The first wave of commercial products came on the market in late 2011. Meanwhile, European countries have not been delayed and are well ahead of U.S. hospitals in implementing copper components.
Presently, nine U.S. hospitals have installed some form of copper components, including door hardware, cabinet pulls, sinks, stretchers, and IV poles, Michels reports.
Despite these advances, hospitals may be slow to incorporate copper components due to a variety of reasons:
Cost. Dr. Pile believes that cost will be the major barrier. “Installing copper surfaces won’t be cheap,” he says. “But, then again, HAIs are very costly. I think it will be more difficult to justify their existence if they can be prevented. If copper is effective in preventing HAIs, it would prove to be cost-effective over time.”
Dr. Salgado concurs. “A study needs to be done on the cost-effectiveness of copper surfaces,” she says. “Health economists estimate that if copper surfaces were incorporated into ICUs, after three to six months, those surfaces would pay for themselves. That is not a long time period. Hospitals need to understand that there will be upfront costs but that they will realize benefits downstream.”
The Center for Medicare & Medicaid Services (CMS) has reported that one infection adds $43,000 in patient costs.4 A typical U.S. hospital room contains $100,000 worth of goods and equipment.
“When you do the math using the amount of copper in our study, the cost would be between $1 and $10 per patient,” Dr. Schmidt says. “It’s also important to note that an infection adds 19 days to a patient’s hospital stay.”
Aesthetics. For some, appearance may be a concern. “Copper is actually an appealing material that is offered in an array of colors and surface finishes,” Dr. Michels says. Because a copper-and-brass combination is more prone to tarnishing, a copper-nickel alloy may be more desirable.
Availability. Copper components are not produced and marketed to U.S. hospitals; however, they are available. “We are hoping with our study and future studies that some medical-device companies, as well as hospital-furniture manufacturers, will jump on board to look at ways to mass-produce items,” Dr. Salgado says.
Acceptance. The study published in Infection Control and Hospital Epidemiology validated the effectiveness of copper in decreasing HAIs. This pilot study, however, was not blinded.3
“It was pretty apparent to providers where copper surfaces were located, which tends to result in some bias. Future studies will, hopefully, try to answer questions regarding healthcare providers’ behaviors with different surfaces,” says Dr. Salgado, noting researchers in California and Chile also are studying the effects of copper surfaces in hospitals.
Possible loss of efficacy. Even if a surface is effective initially, Dr. Pile points out that it’s possible for that to change. “I have a theoretical concern that, over time, bacterial pathogens may develop a tolerance to copper,” he says. “Bacterial adversaries have been able to overcome any type of treatment that we have devised for them thus far. But this remains to be seen.”
This has been an issue with other surfaces; once microbes establish a foothold, it is hard to eliminate them. But Dr. Schmidt says because bacteria are killed so quickly on copper surfaces and cleaning is only required once daily, the ability to establish a foothold is greatly reduced, if not completely eliminated.

—Harold T. Michels, PhD, PE, senior vice president of technology and technical services, Copper Development Association Inc.
Champion Proven Strategies
Dr. Pile sees antimicrobial stewardship as a great opportunity for hospitalists as a specialty. In fact, the Centers for Disease Control and Prevention is partnering with HM groups on piloting multiple antimicrobial stewardship initiatives at several sites.
Dr. Pile suggests that leaders spearhead formal quality-improvement efforts, be involved with patient-safety efforts, and serve as physician champions.
“No one is better positioned to do this than hospitalists, because we own the hospital environment,” he says. “We have an incredible stake in making sure that our inpatient environment provides safe and high-value care.”
As a result of the published study, Dr. Salgado says discussions are underway with hospital leaders at MUSC to determine if copper surfaces will be used in its ICUs and, if so, how changes will be implemented.
Karen Appold is a freelance writer in Pennsylvania.
References
- Klevens RM, Edwards JR, Richards CL, et al. Estimating healthcare-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
- Scott RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta: Centers for Disease Control and Prevention, 2009.
- Salgado CD, Sepkowitz KA, John JF, et al. Copper Surfaces Reduce the Rate of Healthcare-Acquired Infections in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
- Healthcare Cost and Utilization Project. Statistical Brief No. 94. Agency for Healthcare Research and Quality. Aug. 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb94.pdf. Accessed Aug. 6, 2013.
—James Pile, MD, FACP, SFHM, vice chair, department of hospital medicine, Cleveland Clinic
Hospital-acquired infections (HAIs) are on the rise despite efforts to decrease them. HAIs cause an estimated 100,000 deaths annually and account for up to $45 billion in health-care costs. Adding fuel to the fire, bacteria increasingly are becoming resistant to last-resort drugs. Despite this gloomy outlook, a recent study in Infection Control and Hospital Epidemiology shows that a material known for its antimicrobial properties for more than 4,000 years—copper—might be a light at the end of this darkening tunnel.1
Ancient Indians stored water in copper pots to prevent illness, says lead study author Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, and medical director for infection prevention at the Medical University of South Carolina (MUSC) in Charleston. But copper rarely is used in that manner today because molded plastics and stainless steel are less expensive and easier to mass-produce.
Dr. Salgado explains that the antimicrobial effect of copper-alloy surfaces is a result of the metal stealing electrons from the bacteria when they come into contact with each other. “Once the bacteria donate the electrons to the copper metal, this places the organism into a state of electrical-charge deficit,” she says. “As a consequence, free radicals are generated inside the cell, which ultimately leads to the cell’s death.”
Copper-alloy surfaces kill 99.9% of bacteria in less than two hours, says Harold T. Michels, PhD, PE, senior vice president of technology and technical services for Copper Development Association Inc. in New York, who was a study author. On other surfaces, bacteria may live for multiple days or even months.
Unlike current methods used to decrease HAIs (i.e. hand-washing and sanitizing surfaces), copper components don’t require human intervention or compliance to be effective.
“It supplements what these other things can do; it’s in the background and it’s always working,” Michels says.
—Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, medical director for infection prevention, Medical University of South Carolina, Charleston
Study Specifics
To conduct the study, copper prototypes of items touched most frequently by patients, health-care providers, and visitors were made and placed in patient rooms located within ICUs. “We placed the copper around the patient [much like a defensive perimeter] to reduce the likelihood that the health-care worker or visitor would introduce the infectious agent to the patient,” says the study’s lead investigator, Michael Schmidt, PhD, a professor and vice chair of MUSC’s department of microbiology and immunology.
Then, bacterial loads were measured on each object. For every study room, there was a control room without copper objects. Researchers were most interested in methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). For a period of time, bacterial burdens were measured in both copper rooms and control rooms.
Results exceeded the researchers’ expectations. Although only 7% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases. The rate of HAI and/or MRSA or VRE colonization in ICU rooms with copper-alloy surfaces was significantly lower than that in standard ICU rooms (0.071 versus 0.123). For HAIs only, the rate was reduced to 0.034 from 0.081.3
“We were pleasantly surprised with the reductions,” Dr. Salgado says. “We consistently saw a more than 50% reduction in HAIs in all study sites.”
Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association, is an advocate for making the health-care system simpler and safer for consumers. She says copper is a “game-changer.”
“It’s a brand-new way of thinking about decreasing the number of HAIs,” she says.
Green Light?
In light of the study’s encouraging findings, hospitalist and infectious-disease specialist James Pile, MD, FACP, SFHM, vice chair of the Department of Hospital Medicine at Cleveland Clinic, says that although study results appear valid, “it didn’t provide any final answers.”
“It would be premature for a hospital to install copper based on this study,” he says, adding he didn’t find the study results surprising, because copper is known to have antimicrobial properties.
But, Dr. Pile says, the study did provide proof of concept and opens the door for larger, more definitive studies that will show if installing copper in hospital rooms is worthwhile.
“If future studies confirm earlier results, then hospitals should seriously consider copper installations,” he says.
Barriers to Implementation
Despite the promising outlook for copper in dramatically reducing HAIs, implantation of copper components is off to a slow start.
Negotiations with the Environmental Protection Agency, the federal agency with jurisdiction over public-health claims for antimicrobial surfaces, started in 2004. Testing started in 2005. Although federal registration was completed in February 2008, it wasn’t until late 2011 that all regulatory issues were resolved for manufacturers.
“The regulatory process created delays in educating hospitals and the public about copper’s effectiveness in killing certain bacteria,” Dr. Georgiou explains. “As a result, American manufacturers with the ability to make copper components weren’t developing products because they couldn’t sell them.”
Now that the regulatory issues have been resolved, U.S. manufacturers are beginning to make copper components. The first wave of commercial products came on the market in late 2011. Meanwhile, European countries have not been delayed and are well ahead of U.S. hospitals in implementing copper components.
Presently, nine U.S. hospitals have installed some form of copper components, including door hardware, cabinet pulls, sinks, stretchers, and IV poles, Michels reports.
Despite these advances, hospitals may be slow to incorporate copper components due to a variety of reasons:
Cost. Dr. Pile believes that cost will be the major barrier. “Installing copper surfaces won’t be cheap,” he says. “But, then again, HAIs are very costly. I think it will be more difficult to justify their existence if they can be prevented. If copper is effective in preventing HAIs, it would prove to be cost-effective over time.”
Dr. Salgado concurs. “A study needs to be done on the cost-effectiveness of copper surfaces,” she says. “Health economists estimate that if copper surfaces were incorporated into ICUs, after three to six months, those surfaces would pay for themselves. That is not a long time period. Hospitals need to understand that there will be upfront costs but that they will realize benefits downstream.”
The Center for Medicare & Medicaid Services (CMS) has reported that one infection adds $43,000 in patient costs.4 A typical U.S. hospital room contains $100,000 worth of goods and equipment.
“When you do the math using the amount of copper in our study, the cost would be between $1 and $10 per patient,” Dr. Schmidt says. “It’s also important to note that an infection adds 19 days to a patient’s hospital stay.”
Aesthetics. For some, appearance may be a concern. “Copper is actually an appealing material that is offered in an array of colors and surface finishes,” Dr. Michels says. Because a copper-and-brass combination is more prone to tarnishing, a copper-nickel alloy may be more desirable.
Availability. Copper components are not produced and marketed to U.S. hospitals; however, they are available. “We are hoping with our study and future studies that some medical-device companies, as well as hospital-furniture manufacturers, will jump on board to look at ways to mass-produce items,” Dr. Salgado says.
Acceptance. The study published in Infection Control and Hospital Epidemiology validated the effectiveness of copper in decreasing HAIs. This pilot study, however, was not blinded.3
“It was pretty apparent to providers where copper surfaces were located, which tends to result in some bias. Future studies will, hopefully, try to answer questions regarding healthcare providers’ behaviors with different surfaces,” says Dr. Salgado, noting researchers in California and Chile also are studying the effects of copper surfaces in hospitals.
Possible loss of efficacy. Even if a surface is effective initially, Dr. Pile points out that it’s possible for that to change. “I have a theoretical concern that, over time, bacterial pathogens may develop a tolerance to copper,” he says. “Bacterial adversaries have been able to overcome any type of treatment that we have devised for them thus far. But this remains to be seen.”
This has been an issue with other surfaces; once microbes establish a foothold, it is hard to eliminate them. But Dr. Schmidt says because bacteria are killed so quickly on copper surfaces and cleaning is only required once daily, the ability to establish a foothold is greatly reduced, if not completely eliminated.
—Harold T. Michels, PhD, PE, senior vice president of technology and technical services, Copper Development Association Inc.
Champion Proven Strategies
Dr. Pile sees antimicrobial stewardship as a great opportunity for hospitalists as a specialty. In fact, the Centers for Disease Control and Prevention is partnering with HM groups on piloting multiple antimicrobial stewardship initiatives at several sites.
Dr. Pile suggests that leaders spearhead formal quality-improvement efforts, be involved with patient-safety efforts, and serve as physician champions.
“No one is better positioned to do this than hospitalists, because we own the hospital environment,” he says. “We have an incredible stake in making sure that our inpatient environment provides safe and high-value care.”
As a result of the published study, Dr. Salgado says discussions are underway with hospital leaders at MUSC to determine if copper surfaces will be used in its ICUs and, if so, how changes will be implemented.
Karen Appold is a freelance writer in Pennsylvania.
References
- Klevens RM, Edwards JR, Richards CL, et al. Estimating healthcare-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
- Scott RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta: Centers for Disease Control and Prevention, 2009.
- Salgado CD, Sepkowitz KA, John JF, et al. Copper Surfaces Reduce the Rate of Healthcare-Acquired Infections in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
- Healthcare Cost and Utilization Project. Statistical Brief No. 94. Agency for Healthcare Research and Quality. Aug. 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb94.pdf. Accessed Aug. 6, 2013.
—James Pile, MD, FACP, SFHM, vice chair, department of hospital medicine, Cleveland Clinic
Hospital-acquired infections (HAIs) are on the rise despite efforts to decrease them. HAIs cause an estimated 100,000 deaths annually and account for up to $45 billion in health-care costs. Adding fuel to the fire, bacteria increasingly are becoming resistant to last-resort drugs. Despite this gloomy outlook, a recent study in Infection Control and Hospital Epidemiology shows that a material known for its antimicrobial properties for more than 4,000 years—copper—might be a light at the end of this darkening tunnel.1
Ancient Indians stored water in copper pots to prevent illness, says lead study author Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, and medical director for infection prevention at the Medical University of South Carolina (MUSC) in Charleston. But copper rarely is used in that manner today because molded plastics and stainless steel are less expensive and easier to mass-produce.
Dr. Salgado explains that the antimicrobial effect of copper-alloy surfaces is a result of the metal stealing electrons from the bacteria when they come into contact with each other. “Once the bacteria donate the electrons to the copper metal, this places the organism into a state of electrical-charge deficit,” she says. “As a consequence, free radicals are generated inside the cell, which ultimately leads to the cell’s death.”
Copper-alloy surfaces kill 99.9% of bacteria in less than two hours, says Harold T. Michels, PhD, PE, senior vice president of technology and technical services for Copper Development Association Inc. in New York, who was a study author. On other surfaces, bacteria may live for multiple days or even months.
Unlike current methods used to decrease HAIs (i.e. hand-washing and sanitizing surfaces), copper components don’t require human intervention or compliance to be effective.
“It supplements what these other things can do; it’s in the background and it’s always working,” Michels says.
—Cassandra D. Salgado, MD, associate professor of medicine, hospital epidemiologist, medical director for infection prevention, Medical University of South Carolina, Charleston
Study Specifics
To conduct the study, copper prototypes of items touched most frequently by patients, health-care providers, and visitors were made and placed in patient rooms located within ICUs. “We placed the copper around the patient [much like a defensive perimeter] to reduce the likelihood that the health-care worker or visitor would introduce the infectious agent to the patient,” says the study’s lead investigator, Michael Schmidt, PhD, a professor and vice chair of MUSC’s department of microbiology and immunology.
Then, bacterial loads were measured on each object. For every study room, there was a control room without copper objects. Researchers were most interested in methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE). For a period of time, bacterial burdens were measured in both copper rooms and control rooms.
Results exceeded the researchers’ expectations. Although only 7% of the touch surfaces in each ICU were replaced with copper components, there were 58% fewer HAI cases. The rate of HAI and/or MRSA or VRE colonization in ICU rooms with copper-alloy surfaces was significantly lower than that in standard ICU rooms (0.071 versus 0.123). For HAIs only, the rate was reduced to 0.034 from 0.081.3
“We were pleasantly surprised with the reductions,” Dr. Salgado says. “We consistently saw a more than 50% reduction in HAIs in all study sites.”
Archelle Georgiou, MD, president of Georgiou Consulting LLC in Minneapolis and an advisor to the Copper Development Association, is an advocate for making the health-care system simpler and safer for consumers. She says copper is a “game-changer.”
“It’s a brand-new way of thinking about decreasing the number of HAIs,” she says.
Green Light?
In light of the study’s encouraging findings, hospitalist and infectious-disease specialist James Pile, MD, FACP, SFHM, vice chair of the Department of Hospital Medicine at Cleveland Clinic, says that although study results appear valid, “it didn’t provide any final answers.”
“It would be premature for a hospital to install copper based on this study,” he says, adding he didn’t find the study results surprising, because copper is known to have antimicrobial properties.
But, Dr. Pile says, the study did provide proof of concept and opens the door for larger, more definitive studies that will show if installing copper in hospital rooms is worthwhile.
“If future studies confirm earlier results, then hospitals should seriously consider copper installations,” he says.
Barriers to Implementation
Despite the promising outlook for copper in dramatically reducing HAIs, implantation of copper components is off to a slow start.
Negotiations with the Environmental Protection Agency, the federal agency with jurisdiction over public-health claims for antimicrobial surfaces, started in 2004. Testing started in 2005. Although federal registration was completed in February 2008, it wasn’t until late 2011 that all regulatory issues were resolved for manufacturers.
“The regulatory process created delays in educating hospitals and the public about copper’s effectiveness in killing certain bacteria,” Dr. Georgiou explains. “As a result, American manufacturers with the ability to make copper components weren’t developing products because they couldn’t sell them.”
Now that the regulatory issues have been resolved, U.S. manufacturers are beginning to make copper components. The first wave of commercial products came on the market in late 2011. Meanwhile, European countries have not been delayed and are well ahead of U.S. hospitals in implementing copper components.
Presently, nine U.S. hospitals have installed some form of copper components, including door hardware, cabinet pulls, sinks, stretchers, and IV poles, Michels reports.
Despite these advances, hospitals may be slow to incorporate copper components due to a variety of reasons:
Cost. Dr. Pile believes that cost will be the major barrier. “Installing copper surfaces won’t be cheap,” he says. “But, then again, HAIs are very costly. I think it will be more difficult to justify their existence if they can be prevented. If copper is effective in preventing HAIs, it would prove to be cost-effective over time.”
Dr. Salgado concurs. “A study needs to be done on the cost-effectiveness of copper surfaces,” she says. “Health economists estimate that if copper surfaces were incorporated into ICUs, after three to six months, those surfaces would pay for themselves. That is not a long time period. Hospitals need to understand that there will be upfront costs but that they will realize benefits downstream.”
The Center for Medicare & Medicaid Services (CMS) has reported that one infection adds $43,000 in patient costs.4 A typical U.S. hospital room contains $100,000 worth of goods and equipment.
“When you do the math using the amount of copper in our study, the cost would be between $1 and $10 per patient,” Dr. Schmidt says. “It’s also important to note that an infection adds 19 days to a patient’s hospital stay.”
Aesthetics. For some, appearance may be a concern. “Copper is actually an appealing material that is offered in an array of colors and surface finishes,” Dr. Michels says. Because a copper-and-brass combination is more prone to tarnishing, a copper-nickel alloy may be more desirable.
Availability. Copper components are not produced and marketed to U.S. hospitals; however, they are available. “We are hoping with our study and future studies that some medical-device companies, as well as hospital-furniture manufacturers, will jump on board to look at ways to mass-produce items,” Dr. Salgado says.
Acceptance. The study published in Infection Control and Hospital Epidemiology validated the effectiveness of copper in decreasing HAIs. This pilot study, however, was not blinded.3
“It was pretty apparent to providers where copper surfaces were located, which tends to result in some bias. Future studies will, hopefully, try to answer questions regarding healthcare providers’ behaviors with different surfaces,” says Dr. Salgado, noting researchers in California and Chile also are studying the effects of copper surfaces in hospitals.
Possible loss of efficacy. Even if a surface is effective initially, Dr. Pile points out that it’s possible for that to change. “I have a theoretical concern that, over time, bacterial pathogens may develop a tolerance to copper,” he says. “Bacterial adversaries have been able to overcome any type of treatment that we have devised for them thus far. But this remains to be seen.”
This has been an issue with other surfaces; once microbes establish a foothold, it is hard to eliminate them. But Dr. Schmidt says because bacteria are killed so quickly on copper surfaces and cleaning is only required once daily, the ability to establish a foothold is greatly reduced, if not completely eliminated.
—Harold T. Michels, PhD, PE, senior vice president of technology and technical services, Copper Development Association Inc.
Champion Proven Strategies
Dr. Pile sees antimicrobial stewardship as a great opportunity for hospitalists as a specialty. In fact, the Centers for Disease Control and Prevention is partnering with HM groups on piloting multiple antimicrobial stewardship initiatives at several sites.
Dr. Pile suggests that leaders spearhead formal quality-improvement efforts, be involved with patient-safety efforts, and serve as physician champions.
“No one is better positioned to do this than hospitalists, because we own the hospital environment,” he says. “We have an incredible stake in making sure that our inpatient environment provides safe and high-value care.”
As a result of the published study, Dr. Salgado says discussions are underway with hospital leaders at MUSC to determine if copper surfaces will be used in its ICUs and, if so, how changes will be implemented.
Karen Appold is a freelance writer in Pennsylvania.
References
- Klevens RM, Edwards JR, Richards CL, et al. Estimating healthcare-associated infections and deaths in U.S. hospitals, 2002. Public Health Rep. 2007;122:160-166.
- Scott RD. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. Atlanta: Centers for Disease Control and Prevention, 2009.
- Salgado CD, Sepkowitz KA, John JF, et al. Copper Surfaces Reduce the Rate of Healthcare-Acquired Infections in the Intensive Care Unit. Infect Control Hosp Epidemiol. 2013;34(5):479-486.
- Healthcare Cost and Utilization Project. Statistical Brief No. 94. Agency for Healthcare Research and Quality. Aug. 2010. Available at: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb94.pdf. Accessed Aug. 6, 2013.