User login
Men, women, and migraine: The role of sex, hormones, obesity, and PTSD
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
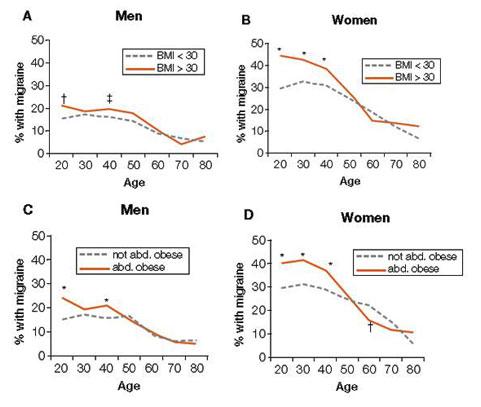
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
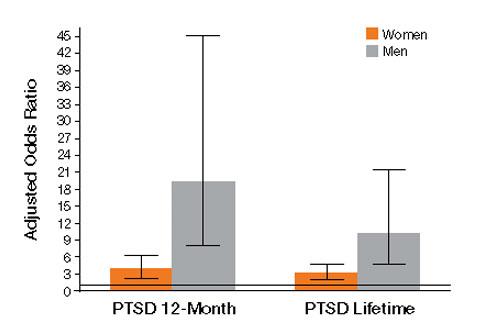
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.