User login
Yale meeting draws cadre of physician-scientists
E. Albert Reece, MD, PhD, MBA, the dean of the University of Maryland School of Medicine, Baltimore, and medical editor of Ob.Gyn. News, has spoken often in the newspaper’s pages about how the fetus has become a visible and intimate patient – one who, “like the mother, can be interrogated, monitored, and sometimes treated before birth.”
Physician-scientists have been instrumental in lifting the cloud of mystery that surrounded the fetus and fetal outcomes. Yet today, in a trend that Dr. Reece and his colleagues call deeply concerning, the number of physician-scientists is declining. “We’re missing out on a workforce that is dedicated to exploring the biologic basis of disease – knowledge that enables the development of targeted therapeutic interventions,” he said in an interview.

Notable Yale physician-scientist alumni have been honored over the years as part of the YOGS meetings, including John C. Hobbins, MD, a former division head of maternal-fetal medicine and a pioneer of ultrasound imaging in the field of obstetrics and gynecology; Roberto Romero, MD, DMedSci, chief of the Perinatology Research Branch at the National Institute of Child Health and Human Development, and editor-in-chief of the American Journal of Obstetrics and Gynecology; and Charles J. Lockwood, MD, dean of the University of South Florida’s Morsani College of Medicine, Tampa, and a former chair of Yale’s ob.gyn. department.
As this year’s honoree, Dr. Reece spoke about the importance of inspiring a new generation of physician-scientists not only within colleges and universities, but also by reaching out to younger students to spark interest in science and research. He recalled being a postdoctoral fellow in perinatology at Yale in the 1980s and being inspired by Dr. Hobbins, whom he credits as his mentor, as well as Dr. Romero, who was finishing his fellowship at Yale while Dr. Reece was beginning his fellowship.
Yale’s department of ob.gyn. and its division of maternal-fetal medicine have had a long history of “firsts” and seminal contributions, including the first ultrasound-guided fetal blood sampling and transfusions in the United States, invention of the fetal heart monitor, the first karyotype in amniotic fluid, the development of postcoital contraception and of methods for early detection of ectopic pregnancies, the discovery of endometrial stem cells and the role that endocrine-disrupting chemicals play in the developmental programming of the uterus, and discovery of the role of cytokines in premature labor and fetal injury.
According to current department chair, Hugh S. Taylor, MD, the 1980s and 1990s were a particularly “exciting time.” Under the tutelage of Dr. Hobbins, who directed both obstetrics and maternal-fetal medicine, obstetrical ultrasound was fast advancing, for instance, and fetoscopy was drawing patients and other physician-scientists from around the world.
“It was an unbelievable time – a magnetic period when many of the things we now take for granted were first being introduced,” said Dr. Reece, who went on after his fellowship to serve as an instructor in ob.gyn. (1982-4), assistant professor (1984-7), and then associate professor (1987-91) at Yale. “It was like going to the symphony and getting to choose the best seat in the house to see the rehearsals all the way through the concert.”
After leaving the Yale faculty and prior to joining the University of Maryland School of Medicine, Dr. Reece served as the chair of obstetrics and gynecology at Temple University School of Medicine, Philadelphia, and then vice chancellor and dean of the University of Arkansas College of Medicine, Little Rock. “Dr. Reece is an incredible bulldog,” said Dr. Hobbins, speaking of the honor given to Dr. Reece at the YOGS meeting. “We could see this right at the beginning at Yale. He latches into something and won’t let it go. He has a work ethic that’s remarkable ... He’s always thinking, ‘How can this be done better?’ ”
Dr. Hobbins, who went on after Yale to a tenure at the University of Colorado at Denver, Aurora, told Ob.Gyn. News that what he remembers “more than anything else, is that we would sit down in a room and just kind of spitball – just brainstorm.”
It is this intellectual curiosity and scientific drive that seems increasingly at risk of being lost, Dr. Hobbins said. “There’s not the same impetus to do a fellowship or to become a physician-scientist or pursue an MD-PhD,” he said. “There just doesn’t seem to be the same oomph to get into the nuts and bolts of how things work, to explore and understand the science. Yes, it has to do with funding. But there’s more to it: We have to somehow stimulate more fire in the belly.”
Dr. Lockwood, who served his fellowship in maternal-fetal medicine at Yale under the guidance of Dr. Hobbins, Dr. Reece, and other faculty, and who later chaired the Yale department of ob.gyn. for 9 years, said that research-rich environments that are “full of inquiry” drive better clinical care.
“The same rigor [gets] applied to the clinical enterprise. Where evidence-based medicine is applicable, it’s done ... and where there are gaps in knowledge, there’s a real spirit of research and inquiry to try to improve care,” Dr. Lockwood said in an interview. “All the great stuff in our health care system is really a direct correlate with the fact that we’ve had this extraordinary research enterprise for so long – most of it funded by the National Institutes of Health, either directly or indirectly.”
The University of Maryland requires all its medical students to take a course in research and critical thinking and to complete a research project. It also runs programs for young students such as a “mini medical school” for underprivileged children who live in nearby neighborhoods. “If you get them excited about science early, and you keep the research continuum going, we believe you’ll have a better chance of recruiting committed physician-scientists into the field,” Dr. Reece said.

The infection has “become an important issue because 10%-20% of women who receive an epidural develop a fever and many of these babies have to have a septic workup and antibiotic treatment,” he said in an e-mail after the meeting. ”Our data indicate that antibiotic administration is not indicated in 40% of cases and the antibiotics currently used do not cover frequent organisms causing infection.”
Dr. Hobbins, who has been using sophisticated imaging techniques to assess subtle changes in fetuses with growth restriction, spoke about the potential value of cardiac size as an indicator of cardiac dysfunction. In utero cardiac dysfunction “sets the tone” for later cardiovascular and neurologic function, he told Ob.Gyn. News. “We think that you can use cardiac size in small babies as a screening tool to tell you whether you need to delve a little further into cardiac function ... Let’s get away from old protocols and rethink other things that are going on in the [small] fetus. Let’s cast a wider net.”
Dr. Lockwood has long been investigating the prevention of recurrent pregnancy loss and preterm delivery, and at the meeting he presented March of Dimes–funded research aimed at identifying mechanisms for dysfunction of the progesterone receptor in premature birth.
Dr. Reece spoke about his research on diabetes in pregnancy and birth defects, and how years of research on diabetes-induced birth defects has shown that maternal hyperglycemia is a teratogen that can trigger a series of developmental fetal defects. “We now have enough information such that we truly have a biomolecular map regarding the precise steps and cascading events which lead to the induction of diabetes-induced birth defects,” said Dr. Reece, who holds a PhD in biochemistry and directs a multimillion-dollar NIH-funded research laboratory at the University of Maryland.
This research began when Dr. Reece asked a question during his fellowship at Yale. “I was struck by the number of birth defects I saw in women with diabetes. I asked Jerry Mahoney, one of the geneticists: Do we know the cause of this? Why is this happening?” he recalled in the interview. “Dr. Mahoney took me to his office, opened his file cabinet and showed me some papers of an [in-vitro rat embryo model], where the rats were made diabetic and the serum seemed to have a way of inducing these birth defects in the embryo. That intrigued me immensely and I thought: I can do this!”
Dr. Reece got his feet wet in an embryology laboratory. As he moved on after his fellowship to join the faculty at Yale, he began directing his own research team – the Diabetes-in-Pregnancy Study Unit.
Dr. Romero said this was the start of “many important contributions to optimize the care of pregnant women with diabetes.” Dr. Reece, he said, has been “able to dissect the role of oxidative stress, program cell death, and lipid metabolism in the genesis of congenital anomalies” in babies of mothers with diabetes.
In other talks at the YOGS meeting, Yale alumnus Ray Bahado-Singh, MD, of Oakwood University, Rochester, Mich., addressed the epigenetics of cardiac dysfunction and the “new frontier” of using epigenetic markers to assess fetal cardiac function. Frank A. Chervenak, MD, of Cornell University, New York, rounded out the meeting by addressing the issue of professionalism and putting the patient first, as well as the professional virtues of self-sacrifice, compassion, and integrity – themes that Dr. Reece frequently cites as integral to both practice and research in ob.gyn.
Clinical care and “the research we’re all doing to assess fetal health both directly and indirectly has to be sitting on a platform of moral, ethical, and solid principles,” said Dr. Reece, who authored a special feature for Ob.Gyn. News – “Obstetrics Moonshots: 50 Years of Discoveries,” on the recent history of obstetrics.
Mary Jane Minkin, MD, a Yale alumna of many levels (medical school through residency) and a longtime Yale faculty member and private-practice ob.gyn. in New Haven, Conn., noted that the YOGS meeting was attended by the 94-year-old Virginia Stuermer, MD, who joined Yale’s ob.gyn. department in 1954 and who is “celebrated within the department” for defying legal barriers to provide patients with contraception and services. “She wanted to come see Dr. Reece,” said Dr. Minkin, who has served as director of YOGS since its inception.
Dr. Stuermer was running the Planned Parenthood clinic in New Haven the day in 1961 when then-department chair Charles Lee Buxton, MD, and Connecticut Planned Parenthood League executive director Estelle Griswold were arrested and jailed. “Everyone knows about the Supreme Court decision, Griswold v. Connecticut [1965], that legalized contraception in the U.S.,” said Dr. Minkin. “But most don’t realize that the doctor who was actually fitting the diaphragms that day was Dr. Stuermer.”
The YOGS reunion preceded a symposium held early in June commemorating the 100-year anniversary of women at Yale Medical School.
E. Albert Reece, MD, PhD, MBA, the dean of the University of Maryland School of Medicine, Baltimore, and medical editor of Ob.Gyn. News, has spoken often in the newspaper’s pages about how the fetus has become a visible and intimate patient – one who, “like the mother, can be interrogated, monitored, and sometimes treated before birth.”
Physician-scientists have been instrumental in lifting the cloud of mystery that surrounded the fetus and fetal outcomes. Yet today, in a trend that Dr. Reece and his colleagues call deeply concerning, the number of physician-scientists is declining. “We’re missing out on a workforce that is dedicated to exploring the biologic basis of disease – knowledge that enables the development of targeted therapeutic interventions,” he said in an interview.
Notable Yale physician-scientist alumni have been honored over the years as part of the YOGS meetings, including John C. Hobbins, MD, a former division head of maternal-fetal medicine and a pioneer of ultrasound imaging in the field of obstetrics and gynecology; Roberto Romero, MD, DMedSci, chief of the Perinatology Research Branch at the National Institute of Child Health and Human Development, and editor-in-chief of the American Journal of Obstetrics and Gynecology; and Charles J. Lockwood, MD, dean of the University of South Florida’s Morsani College of Medicine, Tampa, and a former chair of Yale’s ob.gyn. department.
As this year’s honoree, Dr. Reece spoke about the importance of inspiring a new generation of physician-scientists not only within colleges and universities, but also by reaching out to younger students to spark interest in science and research. He recalled being a postdoctoral fellow in perinatology at Yale in the 1980s and being inspired by Dr. Hobbins, whom he credits as his mentor, as well as Dr. Romero, who was finishing his fellowship at Yale while Dr. Reece was beginning his fellowship.
Yale’s department of ob.gyn. and its division of maternal-fetal medicine have had a long history of “firsts” and seminal contributions, including the first ultrasound-guided fetal blood sampling and transfusions in the United States, invention of the fetal heart monitor, the first karyotype in amniotic fluid, the development of postcoital contraception and of methods for early detection of ectopic pregnancies, the discovery of endometrial stem cells and the role that endocrine-disrupting chemicals play in the developmental programming of the uterus, and discovery of the role of cytokines in premature labor and fetal injury.
According to current department chair, Hugh S. Taylor, MD, the 1980s and 1990s were a particularly “exciting time.” Under the tutelage of Dr. Hobbins, who directed both obstetrics and maternal-fetal medicine, obstetrical ultrasound was fast advancing, for instance, and fetoscopy was drawing patients and other physician-scientists from around the world.
“It was an unbelievable time – a magnetic period when many of the things we now take for granted were first being introduced,” said Dr. Reece, who went on after his fellowship to serve as an instructor in ob.gyn. (1982-4), assistant professor (1984-7), and then associate professor (1987-91) at Yale. “It was like going to the symphony and getting to choose the best seat in the house to see the rehearsals all the way through the concert.”
After leaving the Yale faculty and prior to joining the University of Maryland School of Medicine, Dr. Reece served as the chair of obstetrics and gynecology at Temple University School of Medicine, Philadelphia, and then vice chancellor and dean of the University of Arkansas College of Medicine, Little Rock. “Dr. Reece is an incredible bulldog,” said Dr. Hobbins, speaking of the honor given to Dr. Reece at the YOGS meeting. “We could see this right at the beginning at Yale. He latches into something and won’t let it go. He has a work ethic that’s remarkable ... He’s always thinking, ‘How can this be done better?’ ”
Dr. Hobbins, who went on after Yale to a tenure at the University of Colorado at Denver, Aurora, told Ob.Gyn. News that what he remembers “more than anything else, is that we would sit down in a room and just kind of spitball – just brainstorm.”
It is this intellectual curiosity and scientific drive that seems increasingly at risk of being lost, Dr. Hobbins said. “There’s not the same impetus to do a fellowship or to become a physician-scientist or pursue an MD-PhD,” he said. “There just doesn’t seem to be the same oomph to get into the nuts and bolts of how things work, to explore and understand the science. Yes, it has to do with funding. But there’s more to it: We have to somehow stimulate more fire in the belly.”
Dr. Lockwood, who served his fellowship in maternal-fetal medicine at Yale under the guidance of Dr. Hobbins, Dr. Reece, and other faculty, and who later chaired the Yale department of ob.gyn. for 9 years, said that research-rich environments that are “full of inquiry” drive better clinical care.
“The same rigor [gets] applied to the clinical enterprise. Where evidence-based medicine is applicable, it’s done ... and where there are gaps in knowledge, there’s a real spirit of research and inquiry to try to improve care,” Dr. Lockwood said in an interview. “All the great stuff in our health care system is really a direct correlate with the fact that we’ve had this extraordinary research enterprise for so long – most of it funded by the National Institutes of Health, either directly or indirectly.”
The University of Maryland requires all its medical students to take a course in research and critical thinking and to complete a research project. It also runs programs for young students such as a “mini medical school” for underprivileged children who live in nearby neighborhoods. “If you get them excited about science early, and you keep the research continuum going, we believe you’ll have a better chance of recruiting committed physician-scientists into the field,” Dr. Reece said.
The infection has “become an important issue because 10%-20% of women who receive an epidural develop a fever and many of these babies have to have a septic workup and antibiotic treatment,” he said in an e-mail after the meeting. ”Our data indicate that antibiotic administration is not indicated in 40% of cases and the antibiotics currently used do not cover frequent organisms causing infection.”
Dr. Hobbins, who has been using sophisticated imaging techniques to assess subtle changes in fetuses with growth restriction, spoke about the potential value of cardiac size as an indicator of cardiac dysfunction. In utero cardiac dysfunction “sets the tone” for later cardiovascular and neurologic function, he told Ob.Gyn. News. “We think that you can use cardiac size in small babies as a screening tool to tell you whether you need to delve a little further into cardiac function ... Let’s get away from old protocols and rethink other things that are going on in the [small] fetus. Let’s cast a wider net.”
Dr. Lockwood has long been investigating the prevention of recurrent pregnancy loss and preterm delivery, and at the meeting he presented March of Dimes–funded research aimed at identifying mechanisms for dysfunction of the progesterone receptor in premature birth.
Dr. Reece spoke about his research on diabetes in pregnancy and birth defects, and how years of research on diabetes-induced birth defects has shown that maternal hyperglycemia is a teratogen that can trigger a series of developmental fetal defects. “We now have enough information such that we truly have a biomolecular map regarding the precise steps and cascading events which lead to the induction of diabetes-induced birth defects,” said Dr. Reece, who holds a PhD in biochemistry and directs a multimillion-dollar NIH-funded research laboratory at the University of Maryland.
This research began when Dr. Reece asked a question during his fellowship at Yale. “I was struck by the number of birth defects I saw in women with diabetes. I asked Jerry Mahoney, one of the geneticists: Do we know the cause of this? Why is this happening?” he recalled in the interview. “Dr. Mahoney took me to his office, opened his file cabinet and showed me some papers of an [in-vitro rat embryo model], where the rats were made diabetic and the serum seemed to have a way of inducing these birth defects in the embryo. That intrigued me immensely and I thought: I can do this!”
Dr. Reece got his feet wet in an embryology laboratory. As he moved on after his fellowship to join the faculty at Yale, he began directing his own research team – the Diabetes-in-Pregnancy Study Unit.
Dr. Romero said this was the start of “many important contributions to optimize the care of pregnant women with diabetes.” Dr. Reece, he said, has been “able to dissect the role of oxidative stress, program cell death, and lipid metabolism in the genesis of congenital anomalies” in babies of mothers with diabetes.
In other talks at the YOGS meeting, Yale alumnus Ray Bahado-Singh, MD, of Oakwood University, Rochester, Mich., addressed the epigenetics of cardiac dysfunction and the “new frontier” of using epigenetic markers to assess fetal cardiac function. Frank A. Chervenak, MD, of Cornell University, New York, rounded out the meeting by addressing the issue of professionalism and putting the patient first, as well as the professional virtues of self-sacrifice, compassion, and integrity – themes that Dr. Reece frequently cites as integral to both practice and research in ob.gyn.
Clinical care and “the research we’re all doing to assess fetal health both directly and indirectly has to be sitting on a platform of moral, ethical, and solid principles,” said Dr. Reece, who authored a special feature for Ob.Gyn. News – “Obstetrics Moonshots: 50 Years of Discoveries,” on the recent history of obstetrics.
Mary Jane Minkin, MD, a Yale alumna of many levels (medical school through residency) and a longtime Yale faculty member and private-practice ob.gyn. in New Haven, Conn., noted that the YOGS meeting was attended by the 94-year-old Virginia Stuermer, MD, who joined Yale’s ob.gyn. department in 1954 and who is “celebrated within the department” for defying legal barriers to provide patients with contraception and services. “She wanted to come see Dr. Reece,” said Dr. Minkin, who has served as director of YOGS since its inception.
Dr. Stuermer was running the Planned Parenthood clinic in New Haven the day in 1961 when then-department chair Charles Lee Buxton, MD, and Connecticut Planned Parenthood League executive director Estelle Griswold were arrested and jailed. “Everyone knows about the Supreme Court decision, Griswold v. Connecticut [1965], that legalized contraception in the U.S.,” said Dr. Minkin. “But most don’t realize that the doctor who was actually fitting the diaphragms that day was Dr. Stuermer.”
The YOGS reunion preceded a symposium held early in June commemorating the 100-year anniversary of women at Yale Medical School.
E. Albert Reece, MD, PhD, MBA, the dean of the University of Maryland School of Medicine, Baltimore, and medical editor of Ob.Gyn. News, has spoken often in the newspaper’s pages about how the fetus has become a visible and intimate patient – one who, “like the mother, can be interrogated, monitored, and sometimes treated before birth.”
Physician-scientists have been instrumental in lifting the cloud of mystery that surrounded the fetus and fetal outcomes. Yet today, in a trend that Dr. Reece and his colleagues call deeply concerning, the number of physician-scientists is declining. “We’re missing out on a workforce that is dedicated to exploring the biologic basis of disease – knowledge that enables the development of targeted therapeutic interventions,” he said in an interview.
Notable Yale physician-scientist alumni have been honored over the years as part of the YOGS meetings, including John C. Hobbins, MD, a former division head of maternal-fetal medicine and a pioneer of ultrasound imaging in the field of obstetrics and gynecology; Roberto Romero, MD, DMedSci, chief of the Perinatology Research Branch at the National Institute of Child Health and Human Development, and editor-in-chief of the American Journal of Obstetrics and Gynecology; and Charles J. Lockwood, MD, dean of the University of South Florida’s Morsani College of Medicine, Tampa, and a former chair of Yale’s ob.gyn. department.
As this year’s honoree, Dr. Reece spoke about the importance of inspiring a new generation of physician-scientists not only within colleges and universities, but also by reaching out to younger students to spark interest in science and research. He recalled being a postdoctoral fellow in perinatology at Yale in the 1980s and being inspired by Dr. Hobbins, whom he credits as his mentor, as well as Dr. Romero, who was finishing his fellowship at Yale while Dr. Reece was beginning his fellowship.
Yale’s department of ob.gyn. and its division of maternal-fetal medicine have had a long history of “firsts” and seminal contributions, including the first ultrasound-guided fetal blood sampling and transfusions in the United States, invention of the fetal heart monitor, the first karyotype in amniotic fluid, the development of postcoital contraception and of methods for early detection of ectopic pregnancies, the discovery of endometrial stem cells and the role that endocrine-disrupting chemicals play in the developmental programming of the uterus, and discovery of the role of cytokines in premature labor and fetal injury.
According to current department chair, Hugh S. Taylor, MD, the 1980s and 1990s were a particularly “exciting time.” Under the tutelage of Dr. Hobbins, who directed both obstetrics and maternal-fetal medicine, obstetrical ultrasound was fast advancing, for instance, and fetoscopy was drawing patients and other physician-scientists from around the world.
“It was an unbelievable time – a magnetic period when many of the things we now take for granted were first being introduced,” said Dr. Reece, who went on after his fellowship to serve as an instructor in ob.gyn. (1982-4), assistant professor (1984-7), and then associate professor (1987-91) at Yale. “It was like going to the symphony and getting to choose the best seat in the house to see the rehearsals all the way through the concert.”
After leaving the Yale faculty and prior to joining the University of Maryland School of Medicine, Dr. Reece served as the chair of obstetrics and gynecology at Temple University School of Medicine, Philadelphia, and then vice chancellor and dean of the University of Arkansas College of Medicine, Little Rock. “Dr. Reece is an incredible bulldog,” said Dr. Hobbins, speaking of the honor given to Dr. Reece at the YOGS meeting. “We could see this right at the beginning at Yale. He latches into something and won’t let it go. He has a work ethic that’s remarkable ... He’s always thinking, ‘How can this be done better?’ ”
Dr. Hobbins, who went on after Yale to a tenure at the University of Colorado at Denver, Aurora, told Ob.Gyn. News that what he remembers “more than anything else, is that we would sit down in a room and just kind of spitball – just brainstorm.”
It is this intellectual curiosity and scientific drive that seems increasingly at risk of being lost, Dr. Hobbins said. “There’s not the same impetus to do a fellowship or to become a physician-scientist or pursue an MD-PhD,” he said. “There just doesn’t seem to be the same oomph to get into the nuts and bolts of how things work, to explore and understand the science. Yes, it has to do with funding. But there’s more to it: We have to somehow stimulate more fire in the belly.”
Dr. Lockwood, who served his fellowship in maternal-fetal medicine at Yale under the guidance of Dr. Hobbins, Dr. Reece, and other faculty, and who later chaired the Yale department of ob.gyn. for 9 years, said that research-rich environments that are “full of inquiry” drive better clinical care.
“The same rigor [gets] applied to the clinical enterprise. Where evidence-based medicine is applicable, it’s done ... and where there are gaps in knowledge, there’s a real spirit of research and inquiry to try to improve care,” Dr. Lockwood said in an interview. “All the great stuff in our health care system is really a direct correlate with the fact that we’ve had this extraordinary research enterprise for so long – most of it funded by the National Institutes of Health, either directly or indirectly.”
The University of Maryland requires all its medical students to take a course in research and critical thinking and to complete a research project. It also runs programs for young students such as a “mini medical school” for underprivileged children who live in nearby neighborhoods. “If you get them excited about science early, and you keep the research continuum going, we believe you’ll have a better chance of recruiting committed physician-scientists into the field,” Dr. Reece said.
The infection has “become an important issue because 10%-20% of women who receive an epidural develop a fever and many of these babies have to have a septic workup and antibiotic treatment,” he said in an e-mail after the meeting. ”Our data indicate that antibiotic administration is not indicated in 40% of cases and the antibiotics currently used do not cover frequent organisms causing infection.”
Dr. Hobbins, who has been using sophisticated imaging techniques to assess subtle changes in fetuses with growth restriction, spoke about the potential value of cardiac size as an indicator of cardiac dysfunction. In utero cardiac dysfunction “sets the tone” for later cardiovascular and neurologic function, he told Ob.Gyn. News. “We think that you can use cardiac size in small babies as a screening tool to tell you whether you need to delve a little further into cardiac function ... Let’s get away from old protocols and rethink other things that are going on in the [small] fetus. Let’s cast a wider net.”
Dr. Lockwood has long been investigating the prevention of recurrent pregnancy loss and preterm delivery, and at the meeting he presented March of Dimes–funded research aimed at identifying mechanisms for dysfunction of the progesterone receptor in premature birth.
Dr. Reece spoke about his research on diabetes in pregnancy and birth defects, and how years of research on diabetes-induced birth defects has shown that maternal hyperglycemia is a teratogen that can trigger a series of developmental fetal defects. “We now have enough information such that we truly have a biomolecular map regarding the precise steps and cascading events which lead to the induction of diabetes-induced birth defects,” said Dr. Reece, who holds a PhD in biochemistry and directs a multimillion-dollar NIH-funded research laboratory at the University of Maryland.
This research began when Dr. Reece asked a question during his fellowship at Yale. “I was struck by the number of birth defects I saw in women with diabetes. I asked Jerry Mahoney, one of the geneticists: Do we know the cause of this? Why is this happening?” he recalled in the interview. “Dr. Mahoney took me to his office, opened his file cabinet and showed me some papers of an [in-vitro rat embryo model], where the rats were made diabetic and the serum seemed to have a way of inducing these birth defects in the embryo. That intrigued me immensely and I thought: I can do this!”
Dr. Reece got his feet wet in an embryology laboratory. As he moved on after his fellowship to join the faculty at Yale, he began directing his own research team – the Diabetes-in-Pregnancy Study Unit.
Dr. Romero said this was the start of “many important contributions to optimize the care of pregnant women with diabetes.” Dr. Reece, he said, has been “able to dissect the role of oxidative stress, program cell death, and lipid metabolism in the genesis of congenital anomalies” in babies of mothers with diabetes.
In other talks at the YOGS meeting, Yale alumnus Ray Bahado-Singh, MD, of Oakwood University, Rochester, Mich., addressed the epigenetics of cardiac dysfunction and the “new frontier” of using epigenetic markers to assess fetal cardiac function. Frank A. Chervenak, MD, of Cornell University, New York, rounded out the meeting by addressing the issue of professionalism and putting the patient first, as well as the professional virtues of self-sacrifice, compassion, and integrity – themes that Dr. Reece frequently cites as integral to both practice and research in ob.gyn.
Clinical care and “the research we’re all doing to assess fetal health both directly and indirectly has to be sitting on a platform of moral, ethical, and solid principles,” said Dr. Reece, who authored a special feature for Ob.Gyn. News – “Obstetrics Moonshots: 50 Years of Discoveries,” on the recent history of obstetrics.
Mary Jane Minkin, MD, a Yale alumna of many levels (medical school through residency) and a longtime Yale faculty member and private-practice ob.gyn. in New Haven, Conn., noted that the YOGS meeting was attended by the 94-year-old Virginia Stuermer, MD, who joined Yale’s ob.gyn. department in 1954 and who is “celebrated within the department” for defying legal barriers to provide patients with contraception and services. “She wanted to come see Dr. Reece,” said Dr. Minkin, who has served as director of YOGS since its inception.
Dr. Stuermer was running the Planned Parenthood clinic in New Haven the day in 1961 when then-department chair Charles Lee Buxton, MD, and Connecticut Planned Parenthood League executive director Estelle Griswold were arrested and jailed. “Everyone knows about the Supreme Court decision, Griswold v. Connecticut [1965], that legalized contraception in the U.S.,” said Dr. Minkin. “But most don’t realize that the doctor who was actually fitting the diaphragms that day was Dr. Stuermer.”
The YOGS reunion preceded a symposium held early in June commemorating the 100-year anniversary of women at Yale Medical School.
Gyn surgeons’ EndoMarch empowers patients
Empowering women through a grassroots approach is what Camran Nezhat, MD, a gynecologic surgeon in Palo Alto, Calif., had in mind when he founded the Worldwide Endometriosis March, or EndoMarch, some years ago. In March 2018, the 5th annual international day of marches and calls to action took place across at least eight U.S. cities and dozens of locations across Europe, Africa, the Middle East, and Asia.
Dr. Nezhat founded the 501(c)(3) public charity nonprofit along with his brothers, Farr Nezhat, MD, and Ceana Nezhat, MD; his niece Azadeh Nezhat, MD; and Barbara Page, a graduate of the University of California, Berkeley, who was working in his practice at the time.
“We’d published so much on the disease [in the medical literature], we didn’t know what else to do ... to help these women. We practice in one of the most advanced cultures for medical care ... and yet women come to us who’ve been told it’s all in their heads, or that they have PID [pelvic inflammatory disease] or depression,” Dr. Camran Nezhat said. “We’d get together and talk about this ... and we thought about how not much changed [with civil rights] in this country until people marched and took matters into their own hands.”
A final catalyst was a lengthy account and reflection on the history of endometriosis that the Nezhat brothers wrote, titled “Endometriosis: Ancient disease, ancient treatments” (Fertil Steril. 2012;98[6 Suppl]:S1-62). They dedicated their research to their mother, who suffered from endometriosis during her life in Iran and who inspired them to pursue medicine and become gynecologic surgeons.
Each year’s EndoMarch events are organized by EndoMarch chapters that are run by volunteers, many of whom have used the annual events to network and fuel year-round advocacy. Chapters have played important roles, for instance, in a national, government-sponsored awareness campaign launched in 2016 in France to alert the public through ads at bus stops and on TV and other media that pain during menstruation is “not natural” and may be a sign of endometriosis.
In Australia, EndoMarch advocates also helped drive plans in December 2017 to create a federally funded “national action plan” for endometriosis. In announcing the plan, Australian health minister Greg Hunt apologized, saying that the disease should have been acknowledged and acted upon “long ago.”
Empowering women through a grassroots approach is what Camran Nezhat, MD, a gynecologic surgeon in Palo Alto, Calif., had in mind when he founded the Worldwide Endometriosis March, or EndoMarch, some years ago. In March 2018, the 5th annual international day of marches and calls to action took place across at least eight U.S. cities and dozens of locations across Europe, Africa, the Middle East, and Asia.
Dr. Nezhat founded the 501(c)(3) public charity nonprofit along with his brothers, Farr Nezhat, MD, and Ceana Nezhat, MD; his niece Azadeh Nezhat, MD; and Barbara Page, a graduate of the University of California, Berkeley, who was working in his practice at the time.
“We’d published so much on the disease [in the medical literature], we didn’t know what else to do ... to help these women. We practice in one of the most advanced cultures for medical care ... and yet women come to us who’ve been told it’s all in their heads, or that they have PID [pelvic inflammatory disease] or depression,” Dr. Camran Nezhat said. “We’d get together and talk about this ... and we thought about how not much changed [with civil rights] in this country until people marched and took matters into their own hands.”
A final catalyst was a lengthy account and reflection on the history of endometriosis that the Nezhat brothers wrote, titled “Endometriosis: Ancient disease, ancient treatments” (Fertil Steril. 2012;98[6 Suppl]:S1-62). They dedicated their research to their mother, who suffered from endometriosis during her life in Iran and who inspired them to pursue medicine and become gynecologic surgeons.
Each year’s EndoMarch events are organized by EndoMarch chapters that are run by volunteers, many of whom have used the annual events to network and fuel year-round advocacy. Chapters have played important roles, for instance, in a national, government-sponsored awareness campaign launched in 2016 in France to alert the public through ads at bus stops and on TV and other media that pain during menstruation is “not natural” and may be a sign of endometriosis.
In Australia, EndoMarch advocates also helped drive plans in December 2017 to create a federally funded “national action plan” for endometriosis. In announcing the plan, Australian health minister Greg Hunt apologized, saying that the disease should have been acknowledged and acted upon “long ago.”
Empowering women through a grassroots approach is what Camran Nezhat, MD, a gynecologic surgeon in Palo Alto, Calif., had in mind when he founded the Worldwide Endometriosis March, or EndoMarch, some years ago. In March 2018, the 5th annual international day of marches and calls to action took place across at least eight U.S. cities and dozens of locations across Europe, Africa, the Middle East, and Asia.
Dr. Nezhat founded the 501(c)(3) public charity nonprofit along with his brothers, Farr Nezhat, MD, and Ceana Nezhat, MD; his niece Azadeh Nezhat, MD; and Barbara Page, a graduate of the University of California, Berkeley, who was working in his practice at the time.
“We’d published so much on the disease [in the medical literature], we didn’t know what else to do ... to help these women. We practice in one of the most advanced cultures for medical care ... and yet women come to us who’ve been told it’s all in their heads, or that they have PID [pelvic inflammatory disease] or depression,” Dr. Camran Nezhat said. “We’d get together and talk about this ... and we thought about how not much changed [with civil rights] in this country until people marched and took matters into their own hands.”
A final catalyst was a lengthy account and reflection on the history of endometriosis that the Nezhat brothers wrote, titled “Endometriosis: Ancient disease, ancient treatments” (Fertil Steril. 2012;98[6 Suppl]:S1-62). They dedicated their research to their mother, who suffered from endometriosis during her life in Iran and who inspired them to pursue medicine and become gynecologic surgeons.
Each year’s EndoMarch events are organized by EndoMarch chapters that are run by volunteers, many of whom have used the annual events to network and fuel year-round advocacy. Chapters have played important roles, for instance, in a national, government-sponsored awareness campaign launched in 2016 in France to alert the public through ads at bus stops and on TV and other media that pain during menstruation is “not natural” and may be a sign of endometriosis.
In Australia, EndoMarch advocates also helped drive plans in December 2017 to create a federally funded “national action plan” for endometriosis. In announcing the plan, Australian health minister Greg Hunt apologized, saying that the disease should have been acknowledged and acted upon “long ago.”

The push is on to recognize endometriosis in adolescents
Meg Hayden, RN, a school nurse in Oxford, Miss., used to be a labor and delivery nurse and considers herself more attuned to women’s health issues than other school nurses are. Still, a new educational initiative on endometriosis that stresses that menstrual pain is not normal – and that teenagers are not too young to have endometriosis – has helped her “connect the dots.”
“It’s a good reminder for me to look at patterns” and advise those girls who have repeated episodes of pelvic pain and other symptoms to “keep a diary” and to seek care, Ms. Hayden said.
They are demanding that serious diagnostic delays be rectified – that disease symptoms be better recognized by gynecologists, pediatricians, and other primary care physicians – and then, that the disease be better managed.
Some of the advocacy groups have petitioned the American College of Obstetricians and Gynecologists to involve patients and endometriosis experts in creating new standards of care. And at press time, activist Shannon Cohn, who developed the School Nurse initiative after producing a documentary film titled Endo What?, was working with Sen. Orrin Hatch (R-Utah) and Sen. Elizabeth Warren (D-Mass.) on finalizing plans for a national public service announcement campaign. (Sen. Hatch wrote an opinion piece for CNN in late March describing his granddaughter’s experience with the disease and calling the widespread prevalence of the disease – and the lack of any long-term treatment options – “nothing short of a public health emergency.”)
Estimates vary, but the average interval between presentation of symptoms and definitive diagnosis of endometriosis by laparoscopy (and usually) biopsy is commonly reported as 7-10 years. The disease can cause incapacitating pain, missed days of school and work, and increasing morbidities over time, including infertility and organ damage both inside and outside the pelvic cavity. A majority of women with endometriosis – two-thirds, according to one survey of more than 4,300 women with surgically diagnosed disease (Fertil Steril. 2009;91:32-9) – report first experiencing symptoms during adolescence.
Yet, too often, adolescents believe or are told that “periods are supposed to hurt,” and other symptoms of the disease – such as gastrointestinal symptoms – are overlooked.
“If we can diagnose endometriosis in its early stages, we could prevent a lifetime of pain and suffering, and decrease rates of infertility ... hopefully stopping disease progression before it does damage,” said Marc R. Laufer, MD, chief of gynecology at Boston Children’s Hospital and professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, also in Boston. “If we don’t, we’re missing a huge opportunity because we know that endometriosis affects 10% of women.”
Atypical symptoms and presentation
Endometriosis is an enigmatic disease. It traditionally has been associated with retrograde menstruation, but today, there are more nuanced and likely overlapping theories of etiology. Identified in girls even prior to the onset of menses, the disease is generally believed to be progressive, but perhaps not all the time. Patients with significant amounts of disease may have tremendous pain or they may have very little discomfort.
While adolescents can have advanced endometriosis, most have early-stage disease, experts say. Still, adolescence offers its own complexities. Preteen and teen patients with endometriosis tend to present more often with atypical symptoms and with much more subtle and variable laparoscopic findings than do adult patients. Dr. Laufer reported more than 20 years ago that only 9.7% of 46 girls presented classically with dysmenorrhea. In 63%, pain was both acyclic and cyclic, and in 28%, pain was acyclic only (J Pediatr Adolesc Gynecol. 1997;10:199-202).
In a more recent report on adolescents treated by gynecologic surgeon Ceana Nezhat, MD, 64% had dysmenorrhea, 44% had menorrhagia, 60% had abnormal or irregular uterine bleeding, 56% had at least one gastrointestinal symptom, and 52% had at least one genitourinary symptom. The girls had seen a mean of three physicians, including psychiatrists and orthopedic surgeons, and had received diagnoses of pelvic inflammatory disease, irritable bowel syndrome, dysmenorrhea, appendicitis, ovarian cysts, and musculoskeletal pain (JSLS. 2015;19:e2015.00019). Notably, 56% had a family history of endometriosis, Dr. Nezhat, of the Atlanta Center for Minimally Invasive Surgery and Reproductive Medicine, and his colleagues found.
To address levels of pain, Dr. Laufer usually asks young women if they feel they’re at a disadvantage to other young women or to men. This opens the door to learning more about school absences, missed activities, and decreased quality of life. Pain, he emphasizes, is only part of the picture. “It’s also about fatigue and energy levels, social interaction, depression, sexual function if they’re sexually active, body image issues, and bowel and bladder functionality.”
If the new generation of school nurse programs and other educational initiatives are successful, teens will increasingly come to appointments with notes in hand. Ms. Hayden counsels students on what to discuss with the doctor. And high school students in New York who have been educated through the Endometriosis Foundation of America’s 5-year-old ENPOWR Project for endometriosis education are urged to keep a journal or use a symptom tracker app if they are experiencing pain or other symptoms associated with endometriosis.
“We tell them that, with a record, you can show that the second week of every month I’m in terrible pain, for instance, or I’ve fainted twice in the last month, or here’s when my nausea is really aggressive,” said Nina Baker, outreach coordinator for the foundation. “We’re very honest about how often this is dismissed ... and we assure them that by no means are you wrong about your pain.”
ENPOWR lessons have been taught in more than 165 schools thus far (mostly in health classes in New York schools and largely by foundation-trained educators), and a recently developed online package of educational materials for schools – the Endo EduKit – is expanding the foundation’s geographical reach to other states. Students are encouraged during the training to see a gynecologist if they’re concerned about endometriosis, Ms. Baker said.
In Mississippi, Ms. Hayden suggests that younger high-schoolers see their pediatrician, but after that, “I feel like they should go to the gynecologist.” (ACOG recommends a first visit to the gynecologist between the ages of 13 and 15 for anticipatory guidance.) The year-old School Nurse Initiative has sent toolkits, posters, and DVD copies of the “Endo What?” film to nurses in 652 schools thus far. “Our goal,” said Ms. Cohn, a lawyer, filmmaker, and an endometriosis patient, “is to educate every school nurse in middle and high schools across the country.”
Treatment dilemmas
The first-line treatment for dysmenorrhea and for suspected endometriosis in adolescents has long been empiric treatment with NSAIDs and oral contraceptive pills. Experts commonly recommend today that combined oral contraceptive pills (COCPs) be started cyclically and then changed to continuous dosing if necessary with the goal of inducing amenorrhea.
If symptoms are not well controlled within 3-6 months of compliant medication management with COCPs and NSAIDs and endometriosis is suspected, then laparoscopy by a physician who is familiar with adolescent endometriosis and can simultaneously diagnose and treat the disease should be considered, according to Dr. Laufer and several other experts in pediatric and adolescent gynecology who spoke with Ob.Gyn. News.
“If someone still has pain on one COCP, then switching to another COCP is not going to solve the problem – there is no study that shows that one pill is better than another,” Dr. Laufer said.
Yet extra months and sometimes years of pill-switching and empiric therapy with other medications – rather than surgical evaluation, diagnosis, and treatment – is not uncommon. “Usually, by the time a patient comes to me, they’ve already been on multiple birth control pills, they’ve failed NSAIDs, and they’ve often tried other medications as well,” such as progestins and gonadotropin-releasing hormone agonists, said Iris Kerin Orbuch, MD, director of the Advanced Gynecologic Laparoscopy Centers in New York and Los Angeles.
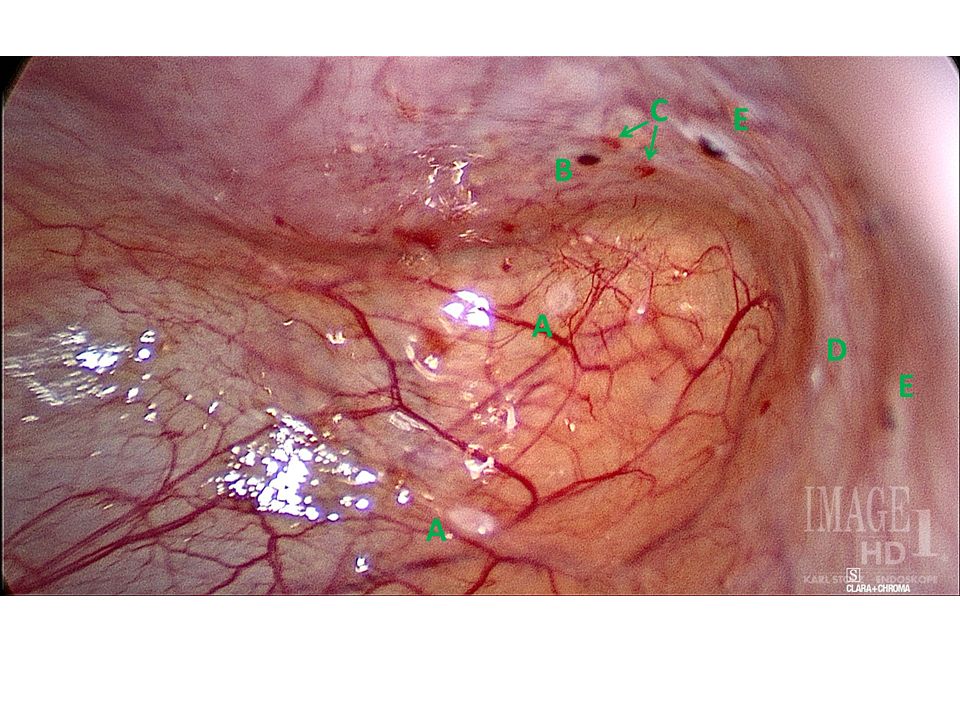
Some also have had diagnostic laparoscopies and been wrongly told that nothing is wrong. Endometriosis is “not all powder-burn lesions and chocolate cysts, which is what we’re taught in medical school,” she said. “It can have many appearances, especially in teens and adolescents. It can be clear vesicles, white, fibrotic, yellow, blue, and brown ... and quite commonly there can simply be areas of increased vascularity. I only learned this in my fellowship.”
Dr. Orbuch, who routinely treats adolescents with endometriosis, takes a holistic approach to the disease that includes working with patients – often before surgery and in partnership with other providers – to downregulate the central nervous system and to alleviate pelvic floor dysfunction that often develops secondary to the disease. When she does operate and finds endometriosis, she performs excisional surgery, in contrast with ablative techniques such as cauterization or desiccation that are used by many physicians.
Treatment of endometriosis is rife with dilemmas, controversies, and shortcomings. Medical treatments can improve pain, but as ACOG’s current Practice Bulletin (No. 114) points out, recurrence rates are high after medication is discontinued – and there is concern among some experts that hormone therapy may not keep the disease from progressing. In adolescents, there is concern about the significant side effects of gonadotropin-releasing hormone agonists, which are sometimes chosen if COCPs and NSAIDs fail to relieve symptoms. COCPs themselves may be problematic, causing premature closure of growth plates.
And when it comes to surgical treatment, there’s often sharp debate over which operative approaches are best for endometriosis. Advocates of excision – including many of the patient advocacy groups – say that ablation too often causes scar tissue and leaves behind disease, leading to recurrent symptoms and multiple surgeries. Critics of excisional surgery express concern about excision-induced adhesions and scar tissue, and about some excisional surgery being too “radical,” particularly when it is performed for earlier-stage disease in adolescents. Research is limited, comprised largely of small retrospective reports and single-institution cohort studies.
Meredith Loveless, MD, a pediatric and adolescent gynecologist who chairs ACOG’s Committee on Adolescent Health Care, is leading the development of a new ACOG committee opinion on dysmenorrhea and endometriosis in adolescents. The laparoscopic appearance of endometriosis in young patients and the need “for fertility preservation as a priority” in surgery will be among the points discussed in ACOG’s upcoming guidance, she said.
“Somebody who manages adult endometriosis and who does extremely aggressive surgical work may actually be harming an adolescent rather than helping them,” said Dr. Loveless of the Norton Children’s Hospital in Louisville, Ky. (Dr. Loveless has also worked with the American Academy of Pediatrics and notes that the academy provides education on dysmenorrhea and endometriosis as part of its national conference.)
Nicole Donnellan, MD, of the University of Pittsburgh Magee–Womens Hospital, said that fertility preservation is always a goal – and is possible – regardless of age. “A lot of us who are advanced laparoscopic surgeons are passionate about excision because (with other approaches) you’re not fully exploring the extent of the disease – what’s behind the superficial things you see,” she said. “Whether you’re 38 and wanting to preserve your fertility, or whether you’re 18, I’m still going to use the same approach. I want to make sure you have a functioning tube, ovaries, and uterus.”
Ken R. Sinervo, MD, medical director of the Center for Endometriosis Care in Atlanta, which has followed patients postsurgically for an average of 7-8 years, said adhesions can occur "whether you're ablating the disease or excising it," and that in his excisional surgeries, he successfully prevents adhesion formation with the use of various intraoperative adhesion barriers as well as bioregenerative medicine to facilitate healing. The key to avoiding repeat surgeries is to "remove all the disease that is present," he emphasized, adding that the "great majority of young patients will have peritoneal disease and very little ovarian involvement."*
ACOG under fire
Dr. Sinervo and Dr. Orbuch are among the gynecologic surgeons, other providers, and patients who have signed a petition to ACOG urging it to involve both educated patients and expert, multidisciplinary endometriosis providers in improving their guidance and policies on endometriosis to facilitate earlier diagnosis and more effective treatment.
The petition was organized by advocate Casey Berna in July and supported by more than a half-dozen endometriosis advocacy groups; in early May, it had almost 8,700 signatures. Ms. Berna also co-organized a demonstration outside ACOG headquarters on April 5-6 as leaders were reviewing practice bulletins and deciding which need revision – and a virtual protest (#WeMatterACOG) – to push for better guidelines.

Ms. Berna, Ms. Cohn, and others have also expressed concern that ob.gyns.’ management of endometriosis – and the development of guidelines – is colored by financial conflicts of interest. The petition, moreover, calls upon ACOG to help create coding specific for excision surgery; currently, because of the lack of reimbursement, many surgeons operate out of network and patients struggle with treatment costs.
In a statement issued in response to the protests, ACOG chief executive officer and executive vice president Hal Lawrence, MD, said that “ACOG is aware of the sensitivities and concerns surrounding timely and accurate diagnosis and treatment of endometriosis. We are always working diligently to review all the available literature and ensure that our guidance to members is accurate and up to date. It’s our aim that [diagnosis and care] are both evidence based and patient centered. To that end, we recognize that patient voices and advocacy are an important part of ensuring we are meeting these high standards.”
In an interview before the protests, Dr. Lawrence said the Committee on Practice Bulletins–Gynecology will revise its guidelines on the management of endometriosis, which were last revised in 2010 and reaffirmed in 2016. He said that he had spoken at length with Ms. Berna on the phone and had passed on a file of research and other materials to the Committee for their consideration.
On April 5, ACOG also joined the American Society for Reproductive Medicine and seven other organizations in sending a letter to the U.S. Senate and House calling for more research on and attention to the disease. NIH research dollars for the disease have dropped from $16 million in 2010 to $7 million in 2018, and “there are too few treatment options available to patients,” the letter says. “We urge you to [prioritize endometriosis] as an important women’s health issue.”
*This article was updated June 5, 2018. An earlier version of this article misstated Dr. Ken R. Sinervo’s name.
Meg Hayden, RN, a school nurse in Oxford, Miss., used to be a labor and delivery nurse and considers herself more attuned to women’s health issues than other school nurses are. Still, a new educational initiative on endometriosis that stresses that menstrual pain is not normal – and that teenagers are not too young to have endometriosis – has helped her “connect the dots.”
“It’s a good reminder for me to look at patterns” and advise those girls who have repeated episodes of pelvic pain and other symptoms to “keep a diary” and to seek care, Ms. Hayden said.
They are demanding that serious diagnostic delays be rectified – that disease symptoms be better recognized by gynecologists, pediatricians, and other primary care physicians – and then, that the disease be better managed.
Some of the advocacy groups have petitioned the American College of Obstetricians and Gynecologists to involve patients and endometriosis experts in creating new standards of care. And at press time, activist Shannon Cohn, who developed the School Nurse initiative after producing a documentary film titled Endo What?, was working with Sen. Orrin Hatch (R-Utah) and Sen. Elizabeth Warren (D-Mass.) on finalizing plans for a national public service announcement campaign. (Sen. Hatch wrote an opinion piece for CNN in late March describing his granddaughter’s experience with the disease and calling the widespread prevalence of the disease – and the lack of any long-term treatment options – “nothing short of a public health emergency.”)
Estimates vary, but the average interval between presentation of symptoms and definitive diagnosis of endometriosis by laparoscopy (and usually) biopsy is commonly reported as 7-10 years. The disease can cause incapacitating pain, missed days of school and work, and increasing morbidities over time, including infertility and organ damage both inside and outside the pelvic cavity. A majority of women with endometriosis – two-thirds, according to one survey of more than 4,300 women with surgically diagnosed disease (Fertil Steril. 2009;91:32-9) – report first experiencing symptoms during adolescence.
Yet, too often, adolescents believe or are told that “periods are supposed to hurt,” and other symptoms of the disease – such as gastrointestinal symptoms – are overlooked.
“If we can diagnose endometriosis in its early stages, we could prevent a lifetime of pain and suffering, and decrease rates of infertility ... hopefully stopping disease progression before it does damage,” said Marc R. Laufer, MD, chief of gynecology at Boston Children’s Hospital and professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, also in Boston. “If we don’t, we’re missing a huge opportunity because we know that endometriosis affects 10% of women.”
Atypical symptoms and presentation
Endometriosis is an enigmatic disease. It traditionally has been associated with retrograde menstruation, but today, there are more nuanced and likely overlapping theories of etiology. Identified in girls even prior to the onset of menses, the disease is generally believed to be progressive, but perhaps not all the time. Patients with significant amounts of disease may have tremendous pain or they may have very little discomfort.
While adolescents can have advanced endometriosis, most have early-stage disease, experts say. Still, adolescence offers its own complexities. Preteen and teen patients with endometriosis tend to present more often with atypical symptoms and with much more subtle and variable laparoscopic findings than do adult patients. Dr. Laufer reported more than 20 years ago that only 9.7% of 46 girls presented classically with dysmenorrhea. In 63%, pain was both acyclic and cyclic, and in 28%, pain was acyclic only (J Pediatr Adolesc Gynecol. 1997;10:199-202).
In a more recent report on adolescents treated by gynecologic surgeon Ceana Nezhat, MD, 64% had dysmenorrhea, 44% had menorrhagia, 60% had abnormal or irregular uterine bleeding, 56% had at least one gastrointestinal symptom, and 52% had at least one genitourinary symptom. The girls had seen a mean of three physicians, including psychiatrists and orthopedic surgeons, and had received diagnoses of pelvic inflammatory disease, irritable bowel syndrome, dysmenorrhea, appendicitis, ovarian cysts, and musculoskeletal pain (JSLS. 2015;19:e2015.00019). Notably, 56% had a family history of endometriosis, Dr. Nezhat, of the Atlanta Center for Minimally Invasive Surgery and Reproductive Medicine, and his colleagues found.
To address levels of pain, Dr. Laufer usually asks young women if they feel they’re at a disadvantage to other young women or to men. This opens the door to learning more about school absences, missed activities, and decreased quality of life. Pain, he emphasizes, is only part of the picture. “It’s also about fatigue and energy levels, social interaction, depression, sexual function if they’re sexually active, body image issues, and bowel and bladder functionality.”
If the new generation of school nurse programs and other educational initiatives are successful, teens will increasingly come to appointments with notes in hand. Ms. Hayden counsels students on what to discuss with the doctor. And high school students in New York who have been educated through the Endometriosis Foundation of America’s 5-year-old ENPOWR Project for endometriosis education are urged to keep a journal or use a symptom tracker app if they are experiencing pain or other symptoms associated with endometriosis.
“We tell them that, with a record, you can show that the second week of every month I’m in terrible pain, for instance, or I’ve fainted twice in the last month, or here’s when my nausea is really aggressive,” said Nina Baker, outreach coordinator for the foundation. “We’re very honest about how often this is dismissed ... and we assure them that by no means are you wrong about your pain.”
ENPOWR lessons have been taught in more than 165 schools thus far (mostly in health classes in New York schools and largely by foundation-trained educators), and a recently developed online package of educational materials for schools – the Endo EduKit – is expanding the foundation’s geographical reach to other states. Students are encouraged during the training to see a gynecologist if they’re concerned about endometriosis, Ms. Baker said.
In Mississippi, Ms. Hayden suggests that younger high-schoolers see their pediatrician, but after that, “I feel like they should go to the gynecologist.” (ACOG recommends a first visit to the gynecologist between the ages of 13 and 15 for anticipatory guidance.) The year-old School Nurse Initiative has sent toolkits, posters, and DVD copies of the “Endo What?” film to nurses in 652 schools thus far. “Our goal,” said Ms. Cohn, a lawyer, filmmaker, and an endometriosis patient, “is to educate every school nurse in middle and high schools across the country.”
Treatment dilemmas
The first-line treatment for dysmenorrhea and for suspected endometriosis in adolescents has long been empiric treatment with NSAIDs and oral contraceptive pills. Experts commonly recommend today that combined oral contraceptive pills (COCPs) be started cyclically and then changed to continuous dosing if necessary with the goal of inducing amenorrhea.
If symptoms are not well controlled within 3-6 months of compliant medication management with COCPs and NSAIDs and endometriosis is suspected, then laparoscopy by a physician who is familiar with adolescent endometriosis and can simultaneously diagnose and treat the disease should be considered, according to Dr. Laufer and several other experts in pediatric and adolescent gynecology who spoke with Ob.Gyn. News.
“If someone still has pain on one COCP, then switching to another COCP is not going to solve the problem – there is no study that shows that one pill is better than another,” Dr. Laufer said.
Yet extra months and sometimes years of pill-switching and empiric therapy with other medications – rather than surgical evaluation, diagnosis, and treatment – is not uncommon. “Usually, by the time a patient comes to me, they’ve already been on multiple birth control pills, they’ve failed NSAIDs, and they’ve often tried other medications as well,” such as progestins and gonadotropin-releasing hormone agonists, said Iris Kerin Orbuch, MD, director of the Advanced Gynecologic Laparoscopy Centers in New York and Los Angeles.
Some also have had diagnostic laparoscopies and been wrongly told that nothing is wrong. Endometriosis is “not all powder-burn lesions and chocolate cysts, which is what we’re taught in medical school,” she said. “It can have many appearances, especially in teens and adolescents. It can be clear vesicles, white, fibrotic, yellow, blue, and brown ... and quite commonly there can simply be areas of increased vascularity. I only learned this in my fellowship.”
Dr. Orbuch, who routinely treats adolescents with endometriosis, takes a holistic approach to the disease that includes working with patients – often before surgery and in partnership with other providers – to downregulate the central nervous system and to alleviate pelvic floor dysfunction that often develops secondary to the disease. When she does operate and finds endometriosis, she performs excisional surgery, in contrast with ablative techniques such as cauterization or desiccation that are used by many physicians.
Treatment of endometriosis is rife with dilemmas, controversies, and shortcomings. Medical treatments can improve pain, but as ACOG’s current Practice Bulletin (No. 114) points out, recurrence rates are high after medication is discontinued – and there is concern among some experts that hormone therapy may not keep the disease from progressing. In adolescents, there is concern about the significant side effects of gonadotropin-releasing hormone agonists, which are sometimes chosen if COCPs and NSAIDs fail to relieve symptoms. COCPs themselves may be problematic, causing premature closure of growth plates.
And when it comes to surgical treatment, there’s often sharp debate over which operative approaches are best for endometriosis. Advocates of excision – including many of the patient advocacy groups – say that ablation too often causes scar tissue and leaves behind disease, leading to recurrent symptoms and multiple surgeries. Critics of excisional surgery express concern about excision-induced adhesions and scar tissue, and about some excisional surgery being too “radical,” particularly when it is performed for earlier-stage disease in adolescents. Research is limited, comprised largely of small retrospective reports and single-institution cohort studies.
Meredith Loveless, MD, a pediatric and adolescent gynecologist who chairs ACOG’s Committee on Adolescent Health Care, is leading the development of a new ACOG committee opinion on dysmenorrhea and endometriosis in adolescents. The laparoscopic appearance of endometriosis in young patients and the need “for fertility preservation as a priority” in surgery will be among the points discussed in ACOG’s upcoming guidance, she said.
“Somebody who manages adult endometriosis and who does extremely aggressive surgical work may actually be harming an adolescent rather than helping them,” said Dr. Loveless of the Norton Children’s Hospital in Louisville, Ky. (Dr. Loveless has also worked with the American Academy of Pediatrics and notes that the academy provides education on dysmenorrhea and endometriosis as part of its national conference.)
Nicole Donnellan, MD, of the University of Pittsburgh Magee–Womens Hospital, said that fertility preservation is always a goal – and is possible – regardless of age. “A lot of us who are advanced laparoscopic surgeons are passionate about excision because (with other approaches) you’re not fully exploring the extent of the disease – what’s behind the superficial things you see,” she said. “Whether you’re 38 and wanting to preserve your fertility, or whether you’re 18, I’m still going to use the same approach. I want to make sure you have a functioning tube, ovaries, and uterus.”
Ken R. Sinervo, MD, medical director of the Center for Endometriosis Care in Atlanta, which has followed patients postsurgically for an average of 7-8 years, said adhesions can occur "whether you're ablating the disease or excising it," and that in his excisional surgeries, he successfully prevents adhesion formation with the use of various intraoperative adhesion barriers as well as bioregenerative medicine to facilitate healing. The key to avoiding repeat surgeries is to "remove all the disease that is present," he emphasized, adding that the "great majority of young patients will have peritoneal disease and very little ovarian involvement."*
ACOG under fire
Dr. Sinervo and Dr. Orbuch are among the gynecologic surgeons, other providers, and patients who have signed a petition to ACOG urging it to involve both educated patients and expert, multidisciplinary endometriosis providers in improving their guidance and policies on endometriosis to facilitate earlier diagnosis and more effective treatment.
The petition was organized by advocate Casey Berna in July and supported by more than a half-dozen endometriosis advocacy groups; in early May, it had almost 8,700 signatures. Ms. Berna also co-organized a demonstration outside ACOG headquarters on April 5-6 as leaders were reviewing practice bulletins and deciding which need revision – and a virtual protest (#WeMatterACOG) – to push for better guidelines.
Ms. Berna, Ms. Cohn, and others have also expressed concern that ob.gyns.’ management of endometriosis – and the development of guidelines – is colored by financial conflicts of interest. The petition, moreover, calls upon ACOG to help create coding specific for excision surgery; currently, because of the lack of reimbursement, many surgeons operate out of network and patients struggle with treatment costs.
In a statement issued in response to the protests, ACOG chief executive officer and executive vice president Hal Lawrence, MD, said that “ACOG is aware of the sensitivities and concerns surrounding timely and accurate diagnosis and treatment of endometriosis. We are always working diligently to review all the available literature and ensure that our guidance to members is accurate and up to date. It’s our aim that [diagnosis and care] are both evidence based and patient centered. To that end, we recognize that patient voices and advocacy are an important part of ensuring we are meeting these high standards.”
In an interview before the protests, Dr. Lawrence said the Committee on Practice Bulletins–Gynecology will revise its guidelines on the management of endometriosis, which were last revised in 2010 and reaffirmed in 2016. He said that he had spoken at length with Ms. Berna on the phone and had passed on a file of research and other materials to the Committee for their consideration.
On April 5, ACOG also joined the American Society for Reproductive Medicine and seven other organizations in sending a letter to the U.S. Senate and House calling for more research on and attention to the disease. NIH research dollars for the disease have dropped from $16 million in 2010 to $7 million in 2018, and “there are too few treatment options available to patients,” the letter says. “We urge you to [prioritize endometriosis] as an important women’s health issue.”
*This article was updated June 5, 2018. An earlier version of this article misstated Dr. Ken R. Sinervo’s name.
Meg Hayden, RN, a school nurse in Oxford, Miss., used to be a labor and delivery nurse and considers herself more attuned to women’s health issues than other school nurses are. Still, a new educational initiative on endometriosis that stresses that menstrual pain is not normal – and that teenagers are not too young to have endometriosis – has helped her “connect the dots.”
“It’s a good reminder for me to look at patterns” and advise those girls who have repeated episodes of pelvic pain and other symptoms to “keep a diary” and to seek care, Ms. Hayden said.
They are demanding that serious diagnostic delays be rectified – that disease symptoms be better recognized by gynecologists, pediatricians, and other primary care physicians – and then, that the disease be better managed.
Some of the advocacy groups have petitioned the American College of Obstetricians and Gynecologists to involve patients and endometriosis experts in creating new standards of care. And at press time, activist Shannon Cohn, who developed the School Nurse initiative after producing a documentary film titled Endo What?, was working with Sen. Orrin Hatch (R-Utah) and Sen. Elizabeth Warren (D-Mass.) on finalizing plans for a national public service announcement campaign. (Sen. Hatch wrote an opinion piece for CNN in late March describing his granddaughter’s experience with the disease and calling the widespread prevalence of the disease – and the lack of any long-term treatment options – “nothing short of a public health emergency.”)
Estimates vary, but the average interval between presentation of symptoms and definitive diagnosis of endometriosis by laparoscopy (and usually) biopsy is commonly reported as 7-10 years. The disease can cause incapacitating pain, missed days of school and work, and increasing morbidities over time, including infertility and organ damage both inside and outside the pelvic cavity. A majority of women with endometriosis – two-thirds, according to one survey of more than 4,300 women with surgically diagnosed disease (Fertil Steril. 2009;91:32-9) – report first experiencing symptoms during adolescence.
Yet, too often, adolescents believe or are told that “periods are supposed to hurt,” and other symptoms of the disease – such as gastrointestinal symptoms – are overlooked.
“If we can diagnose endometriosis in its early stages, we could prevent a lifetime of pain and suffering, and decrease rates of infertility ... hopefully stopping disease progression before it does damage,” said Marc R. Laufer, MD, chief of gynecology at Boston Children’s Hospital and professor of obstetrics, gynecology, and reproductive biology at Harvard Medical School, also in Boston. “If we don’t, we’re missing a huge opportunity because we know that endometriosis affects 10% of women.”
Atypical symptoms and presentation
Endometriosis is an enigmatic disease. It traditionally has been associated with retrograde menstruation, but today, there are more nuanced and likely overlapping theories of etiology. Identified in girls even prior to the onset of menses, the disease is generally believed to be progressive, but perhaps not all the time. Patients with significant amounts of disease may have tremendous pain or they may have very little discomfort.
While adolescents can have advanced endometriosis, most have early-stage disease, experts say. Still, adolescence offers its own complexities. Preteen and teen patients with endometriosis tend to present more often with atypical symptoms and with much more subtle and variable laparoscopic findings than do adult patients. Dr. Laufer reported more than 20 years ago that only 9.7% of 46 girls presented classically with dysmenorrhea. In 63%, pain was both acyclic and cyclic, and in 28%, pain was acyclic only (J Pediatr Adolesc Gynecol. 1997;10:199-202).
In a more recent report on adolescents treated by gynecologic surgeon Ceana Nezhat, MD, 64% had dysmenorrhea, 44% had menorrhagia, 60% had abnormal or irregular uterine bleeding, 56% had at least one gastrointestinal symptom, and 52% had at least one genitourinary symptom. The girls had seen a mean of three physicians, including psychiatrists and orthopedic surgeons, and had received diagnoses of pelvic inflammatory disease, irritable bowel syndrome, dysmenorrhea, appendicitis, ovarian cysts, and musculoskeletal pain (JSLS. 2015;19:e2015.00019). Notably, 56% had a family history of endometriosis, Dr. Nezhat, of the Atlanta Center for Minimally Invasive Surgery and Reproductive Medicine, and his colleagues found.
To address levels of pain, Dr. Laufer usually asks young women if they feel they’re at a disadvantage to other young women or to men. This opens the door to learning more about school absences, missed activities, and decreased quality of life. Pain, he emphasizes, is only part of the picture. “It’s also about fatigue and energy levels, social interaction, depression, sexual function if they’re sexually active, body image issues, and bowel and bladder functionality.”
If the new generation of school nurse programs and other educational initiatives are successful, teens will increasingly come to appointments with notes in hand. Ms. Hayden counsels students on what to discuss with the doctor. And high school students in New York who have been educated through the Endometriosis Foundation of America’s 5-year-old ENPOWR Project for endometriosis education are urged to keep a journal or use a symptom tracker app if they are experiencing pain or other symptoms associated with endometriosis.
“We tell them that, with a record, you can show that the second week of every month I’m in terrible pain, for instance, or I’ve fainted twice in the last month, or here’s when my nausea is really aggressive,” said Nina Baker, outreach coordinator for the foundation. “We’re very honest about how often this is dismissed ... and we assure them that by no means are you wrong about your pain.”
ENPOWR lessons have been taught in more than 165 schools thus far (mostly in health classes in New York schools and largely by foundation-trained educators), and a recently developed online package of educational materials for schools – the Endo EduKit – is expanding the foundation’s geographical reach to other states. Students are encouraged during the training to see a gynecologist if they’re concerned about endometriosis, Ms. Baker said.
In Mississippi, Ms. Hayden suggests that younger high-schoolers see their pediatrician, but after that, “I feel like they should go to the gynecologist.” (ACOG recommends a first visit to the gynecologist between the ages of 13 and 15 for anticipatory guidance.) The year-old School Nurse Initiative has sent toolkits, posters, and DVD copies of the “Endo What?” film to nurses in 652 schools thus far. “Our goal,” said Ms. Cohn, a lawyer, filmmaker, and an endometriosis patient, “is to educate every school nurse in middle and high schools across the country.”
Treatment dilemmas
The first-line treatment for dysmenorrhea and for suspected endometriosis in adolescents has long been empiric treatment with NSAIDs and oral contraceptive pills. Experts commonly recommend today that combined oral contraceptive pills (COCPs) be started cyclically and then changed to continuous dosing if necessary with the goal of inducing amenorrhea.
If symptoms are not well controlled within 3-6 months of compliant medication management with COCPs and NSAIDs and endometriosis is suspected, then laparoscopy by a physician who is familiar with adolescent endometriosis and can simultaneously diagnose and treat the disease should be considered, according to Dr. Laufer and several other experts in pediatric and adolescent gynecology who spoke with Ob.Gyn. News.
“If someone still has pain on one COCP, then switching to another COCP is not going to solve the problem – there is no study that shows that one pill is better than another,” Dr. Laufer said.
Yet extra months and sometimes years of pill-switching and empiric therapy with other medications – rather than surgical evaluation, diagnosis, and treatment – is not uncommon. “Usually, by the time a patient comes to me, they’ve already been on multiple birth control pills, they’ve failed NSAIDs, and they’ve often tried other medications as well,” such as progestins and gonadotropin-releasing hormone agonists, said Iris Kerin Orbuch, MD, director of the Advanced Gynecologic Laparoscopy Centers in New York and Los Angeles.
Some also have had diagnostic laparoscopies and been wrongly told that nothing is wrong. Endometriosis is “not all powder-burn lesions and chocolate cysts, which is what we’re taught in medical school,” she said. “It can have many appearances, especially in teens and adolescents. It can be clear vesicles, white, fibrotic, yellow, blue, and brown ... and quite commonly there can simply be areas of increased vascularity. I only learned this in my fellowship.”
Dr. Orbuch, who routinely treats adolescents with endometriosis, takes a holistic approach to the disease that includes working with patients – often before surgery and in partnership with other providers – to downregulate the central nervous system and to alleviate pelvic floor dysfunction that often develops secondary to the disease. When she does operate and finds endometriosis, she performs excisional surgery, in contrast with ablative techniques such as cauterization or desiccation that are used by many physicians.
Treatment of endometriosis is rife with dilemmas, controversies, and shortcomings. Medical treatments can improve pain, but as ACOG’s current Practice Bulletin (No. 114) points out, recurrence rates are high after medication is discontinued – and there is concern among some experts that hormone therapy may not keep the disease from progressing. In adolescents, there is concern about the significant side effects of gonadotropin-releasing hormone agonists, which are sometimes chosen if COCPs and NSAIDs fail to relieve symptoms. COCPs themselves may be problematic, causing premature closure of growth plates.
And when it comes to surgical treatment, there’s often sharp debate over which operative approaches are best for endometriosis. Advocates of excision – including many of the patient advocacy groups – say that ablation too often causes scar tissue and leaves behind disease, leading to recurrent symptoms and multiple surgeries. Critics of excisional surgery express concern about excision-induced adhesions and scar tissue, and about some excisional surgery being too “radical,” particularly when it is performed for earlier-stage disease in adolescents. Research is limited, comprised largely of small retrospective reports and single-institution cohort studies.
Meredith Loveless, MD, a pediatric and adolescent gynecologist who chairs ACOG’s Committee on Adolescent Health Care, is leading the development of a new ACOG committee opinion on dysmenorrhea and endometriosis in adolescents. The laparoscopic appearance of endometriosis in young patients and the need “for fertility preservation as a priority” in surgery will be among the points discussed in ACOG’s upcoming guidance, she said.
“Somebody who manages adult endometriosis and who does extremely aggressive surgical work may actually be harming an adolescent rather than helping them,” said Dr. Loveless of the Norton Children’s Hospital in Louisville, Ky. (Dr. Loveless has also worked with the American Academy of Pediatrics and notes that the academy provides education on dysmenorrhea and endometriosis as part of its national conference.)
Nicole Donnellan, MD, of the University of Pittsburgh Magee–Womens Hospital, said that fertility preservation is always a goal – and is possible – regardless of age. “A lot of us who are advanced laparoscopic surgeons are passionate about excision because (with other approaches) you’re not fully exploring the extent of the disease – what’s behind the superficial things you see,” she said. “Whether you’re 38 and wanting to preserve your fertility, or whether you’re 18, I’m still going to use the same approach. I want to make sure you have a functioning tube, ovaries, and uterus.”
Ken R. Sinervo, MD, medical director of the Center for Endometriosis Care in Atlanta, which has followed patients postsurgically for an average of 7-8 years, said adhesions can occur "whether you're ablating the disease or excising it," and that in his excisional surgeries, he successfully prevents adhesion formation with the use of various intraoperative adhesion barriers as well as bioregenerative medicine to facilitate healing. The key to avoiding repeat surgeries is to "remove all the disease that is present," he emphasized, adding that the "great majority of young patients will have peritoneal disease and very little ovarian involvement."*
ACOG under fire
Dr. Sinervo and Dr. Orbuch are among the gynecologic surgeons, other providers, and patients who have signed a petition to ACOG urging it to involve both educated patients and expert, multidisciplinary endometriosis providers in improving their guidance and policies on endometriosis to facilitate earlier diagnosis and more effective treatment.
The petition was organized by advocate Casey Berna in July and supported by more than a half-dozen endometriosis advocacy groups; in early May, it had almost 8,700 signatures. Ms. Berna also co-organized a demonstration outside ACOG headquarters on April 5-6 as leaders were reviewing practice bulletins and deciding which need revision – and a virtual protest (#WeMatterACOG) – to push for better guidelines.
Ms. Berna, Ms. Cohn, and others have also expressed concern that ob.gyns.’ management of endometriosis – and the development of guidelines – is colored by financial conflicts of interest. The petition, moreover, calls upon ACOG to help create coding specific for excision surgery; currently, because of the lack of reimbursement, many surgeons operate out of network and patients struggle with treatment costs.
In a statement issued in response to the protests, ACOG chief executive officer and executive vice president Hal Lawrence, MD, said that “ACOG is aware of the sensitivities and concerns surrounding timely and accurate diagnosis and treatment of endometriosis. We are always working diligently to review all the available literature and ensure that our guidance to members is accurate and up to date. It’s our aim that [diagnosis and care] are both evidence based and patient centered. To that end, we recognize that patient voices and advocacy are an important part of ensuring we are meeting these high standards.”
In an interview before the protests, Dr. Lawrence said the Committee on Practice Bulletins–Gynecology will revise its guidelines on the management of endometriosis, which were last revised in 2010 and reaffirmed in 2016. He said that he had spoken at length with Ms. Berna on the phone and had passed on a file of research and other materials to the Committee for their consideration.
On April 5, ACOG also joined the American Society for Reproductive Medicine and seven other organizations in sending a letter to the U.S. Senate and House calling for more research on and attention to the disease. NIH research dollars for the disease have dropped from $16 million in 2010 to $7 million in 2018, and “there are too few treatment options available to patients,” the letter says. “We urge you to [prioritize endometriosis] as an important women’s health issue.”
*This article was updated June 5, 2018. An earlier version of this article misstated Dr. Ken R. Sinervo’s name.
Shift to long-term ‘maternal care’ needs boost
WASHINGTON – George R. Saade, MD, wants to see a Time magazine cover story like the 2010 feature titled, “How the first 9 months shape the rest of your life” – except this new story would read “How the first 9 months shape the rest of the mother’s life.”
It’s time, he says, that pregnancy truly be appreciated as a “window to future health” for the mother as well as for the baby, and that the term “maternal care” replaces prenatal care. “How many of your [primary care] providers have asked you if you’ve had any pregnancies and if any of your pregnancies were complicated by hypertension, preterm delivery, growth restriction, or gestational diabetes?” Dr. Saade asked at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“It’s better than before, but not good enough ... Checking with patients 6 weeks postpartum is not enough” to prevent long-term metabolic and cardiovascular disorders, he said. “We need regular screening of women.”
The relationship between gestational diabetes (GDM) and subsequent type 2 diabetes, demonstrated several decades ago, offered the “first evidence that pregnancy is a window to future health,” and evidence of the relationship continues to grow. “We know today that there is no other predictive marker of type 2 diabetes that is better and stronger than gestational diabetes,” said Dr. Saade, chief of obstetrics and maternal-fetal medicine at the University of Texas Medical Branch, Galveston.
GDM has also recently been shown to elevate cardiovascular risk independent of its association with type 2 diabetes and metabolic disease.
And similarly, there is now an incontrovertible body of evidence that women who have had preeclampsia are at significantly higher risk of developing hypertension, stroke, and ischemic heart disease later in life than are women who have not have preeclampsia, Dr. Saade said.
Layered evidence
The study that first caught Dr. Saade’s attention was a large Norwegian population-based study published in 2001 that looked at maternal mortality up to 25 years after pregnancy. Women who had preeclampsia had a 1.2-fold higher long-term risk of death from cardiovascular diseases, cancer, and stroke – and women with a history of both preeclampsia and a preterm delivery had a 2.71-fold higher risk – than that of women without such history.
Looking at cardiovascular causes of death specifically, the risk among women with both preeclampsia and preterm delivery was 8.12-fold higher than in women who did not have preeclampsia.
Since then, studies and reviews conducted in the United States and Europe have shown that a history of preeclampsia doubles the risk of developing cardiovascular disease, more than triples the risk of later hypertension, and also increases the risk of stroke, though more moderately.
Recently, Dr. Saade said, researchers have also begun reporting subclinical cardiac abnormalities in women with a history of preeclampsia. A study of 107 women with preeclampsia and 41 women with uneventful pregnancies found that the prevalence of subclinical heart failure (heart failure Stage B) was approximately 3.5% higher in the short term in the preeclampsia group. The women underwent regular cardiac ultrasound and other cardiovascular risk assessment tests 4-10 years postpartum (Ultrasound Obstet Gynecol. 2017;49[1]:143-9).
Preterm delivery and small for gestational age have also been associated with increased risk of ischemic heart disease and other cardiovascular events later in life. And gestational hypertension, research has shown, is a clear risk factor for later hypertension. “We always think of preeclampsia as a different disease, but as far as long-term health is concerned, it doesn’t matter if a woman had preeclampsia or gestational hypertension; she’s still at [greater] risk for hypertension later,” Dr. Saade said.
“And we don’t have to wait 30 years to see evidence” of the association between pregnancy complications and adverse cardiovascular outcomes, he emphasized. A recent retrospective cohort study of more than 300,000 women in Florida showed that women who experienced a maternal placental syndrome during their first pregnancy were at higher risk of subsequent cardiovascular disease during just 5 years of follow-up (Am J Obstet Gynecol. 2016;215[4]:484.e1-14).
Into practice
Regular screening of women whose pregnancies were complicated by conditions associated with long-term health risks “need not be that sophisticated,” Dr. Saade said. Measurement of blood pressure, waist circumference, fasting lipid profile, and fasting glucose is often enough for basic maternal health surveillance, he said.
Dr. Saade said he and some other experts in the field are recommending yearly follow-up for patients who’ve had preeclampsia and other complications. Among the other experts urging early heart disease risk screening is Graeme N. Smith, MD, PhD, an ob.gyn in Ontario who has developed surveillance protocols, follow-up forms, and risk prediction tools for use in a maternal health clinic he established at Kingston General Hospital, Queens University. At the meeting, Dr. Saade encouraged the audience to access Dr. Smith’s resources.
The American Heart Association, in its 2011 guidelines for cardiovascular disease prevention in women, includes pregnancy risks factors (specifically a history of preeclampsia, gestational diabetes, or pregnancy-induced hypertension) as part of its list of major factors for use in risk assessment (Circulation. 2011;123:1243-62).
But as Erica P. Gunderson, PhD, MPH, of Kaiser Permanente Northern California’s division of research, pointed out during another presentation at the meeting, there is more work to be done. Reproductive history is not included in existing disease prediction or risk stratification models for atherosclerotic cardiovascular disease, making it hard at this point to devise specific screening protocols and schedules, especially when it comes to a history of GDM, she said.
“We need more coordinated systems, surveillance in younger women, and some prediction models so that we can know who is at highest risk and needs more surveillance,” she said.
The AHA’s inclusion of GDM history is based on its strong link to overt diabetes, but recent evidence has shown that a history of GDM can independently elevate cardiovascular risk, she noted. Research from the Nurses Health Study II cohort, for instance, found a 30% higher relative risk of cardiovascular events (myocardial infarction and stroke) in women with a history of GDM without progression to diabetes, compared with women who did not have GDM or diabetes (JAMA Intern Med. 2017;177[12]:1735-42).
Dr. Gunderson has also found through analyses of the Coronary Artery Risk Development in Young Adults study data that women who had GDM but did not go on to develop overt diabetes or impaired glycemia had greater carotid intima media thickness many years post delivery than did women without a history of gestational diabetes (J Am Heart Assoc. 2014;3[2]:e000490).
In some models, she has written, this difference in carotid intima media thickness could represent 3-5 years of greater vascular aging for women with previous gestational diabetes and no apparent metabolic dysfunction outside of pregnancy (JAMA Intern Med. 2017;177[12]:1742-4).
There’s a question, she and Dr. Saade both noted, of whether pregnancies unmask previous dispositions to cardiovascular disease or whether pregnancy complications more directly drive adverse long-term outcomes. There is evidence that disorders such as GDM, Dr. Gunderson said, are superimposed on already altered metabolism. But at this time, Dr. Saade said, it appears that “the answer is both.”
According to Dr. Saade, at least three studies are currently following women prospectively to learn more about pregnancy as a window to future cardiovascular health. One of them is the National Institute of Child Health and Human Development’s Nulliparous Pregnancy Outcomes Study–Monitoring Mothers-to-Be Heart Health Study; some data from this study will be presented soon, he said.
Both Dr. Saade and Dr. Gunderson reported in their presentations that they had no disclosures.
WASHINGTON – George R. Saade, MD, wants to see a Time magazine cover story like the 2010 feature titled, “How the first 9 months shape the rest of your life” – except this new story would read “How the first 9 months shape the rest of the mother’s life.”
It’s time, he says, that pregnancy truly be appreciated as a “window to future health” for the mother as well as for the baby, and that the term “maternal care” replaces prenatal care. “How many of your [primary care] providers have asked you if you’ve had any pregnancies and if any of your pregnancies were complicated by hypertension, preterm delivery, growth restriction, or gestational diabetes?” Dr. Saade asked at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“It’s better than before, but not good enough ... Checking with patients 6 weeks postpartum is not enough” to prevent long-term metabolic and cardiovascular disorders, he said. “We need regular screening of women.”
The relationship between gestational diabetes (GDM) and subsequent type 2 diabetes, demonstrated several decades ago, offered the “first evidence that pregnancy is a window to future health,” and evidence of the relationship continues to grow. “We know today that there is no other predictive marker of type 2 diabetes that is better and stronger than gestational diabetes,” said Dr. Saade, chief of obstetrics and maternal-fetal medicine at the University of Texas Medical Branch, Galveston.
GDM has also recently been shown to elevate cardiovascular risk independent of its association with type 2 diabetes and metabolic disease.
And similarly, there is now an incontrovertible body of evidence that women who have had preeclampsia are at significantly higher risk of developing hypertension, stroke, and ischemic heart disease later in life than are women who have not have preeclampsia, Dr. Saade said.
Layered evidence
The study that first caught Dr. Saade’s attention was a large Norwegian population-based study published in 2001 that looked at maternal mortality up to 25 years after pregnancy. Women who had preeclampsia had a 1.2-fold higher long-term risk of death from cardiovascular diseases, cancer, and stroke – and women with a history of both preeclampsia and a preterm delivery had a 2.71-fold higher risk – than that of women without such history.
Looking at cardiovascular causes of death specifically, the risk among women with both preeclampsia and preterm delivery was 8.12-fold higher than in women who did not have preeclampsia.
Since then, studies and reviews conducted in the United States and Europe have shown that a history of preeclampsia doubles the risk of developing cardiovascular disease, more than triples the risk of later hypertension, and also increases the risk of stroke, though more moderately.
Recently, Dr. Saade said, researchers have also begun reporting subclinical cardiac abnormalities in women with a history of preeclampsia. A study of 107 women with preeclampsia and 41 women with uneventful pregnancies found that the prevalence of subclinical heart failure (heart failure Stage B) was approximately 3.5% higher in the short term in the preeclampsia group. The women underwent regular cardiac ultrasound and other cardiovascular risk assessment tests 4-10 years postpartum (Ultrasound Obstet Gynecol. 2017;49[1]:143-9).
Preterm delivery and small for gestational age have also been associated with increased risk of ischemic heart disease and other cardiovascular events later in life. And gestational hypertension, research has shown, is a clear risk factor for later hypertension. “We always think of preeclampsia as a different disease, but as far as long-term health is concerned, it doesn’t matter if a woman had preeclampsia or gestational hypertension; she’s still at [greater] risk for hypertension later,” Dr. Saade said.
“And we don’t have to wait 30 years to see evidence” of the association between pregnancy complications and adverse cardiovascular outcomes, he emphasized. A recent retrospective cohort study of more than 300,000 women in Florida showed that women who experienced a maternal placental syndrome during their first pregnancy were at higher risk of subsequent cardiovascular disease during just 5 years of follow-up (Am J Obstet Gynecol. 2016;215[4]:484.e1-14).
Into practice
Regular screening of women whose pregnancies were complicated by conditions associated with long-term health risks “need not be that sophisticated,” Dr. Saade said. Measurement of blood pressure, waist circumference, fasting lipid profile, and fasting glucose is often enough for basic maternal health surveillance, he said.
Dr. Saade said he and some other experts in the field are recommending yearly follow-up for patients who’ve had preeclampsia and other complications. Among the other experts urging early heart disease risk screening is Graeme N. Smith, MD, PhD, an ob.gyn in Ontario who has developed surveillance protocols, follow-up forms, and risk prediction tools for use in a maternal health clinic he established at Kingston General Hospital, Queens University. At the meeting, Dr. Saade encouraged the audience to access Dr. Smith’s resources.
The American Heart Association, in its 2011 guidelines for cardiovascular disease prevention in women, includes pregnancy risks factors (specifically a history of preeclampsia, gestational diabetes, or pregnancy-induced hypertension) as part of its list of major factors for use in risk assessment (Circulation. 2011;123:1243-62).
But as Erica P. Gunderson, PhD, MPH, of Kaiser Permanente Northern California’s division of research, pointed out during another presentation at the meeting, there is more work to be done. Reproductive history is not included in existing disease prediction or risk stratification models for atherosclerotic cardiovascular disease, making it hard at this point to devise specific screening protocols and schedules, especially when it comes to a history of GDM, she said.
“We need more coordinated systems, surveillance in younger women, and some prediction models so that we can know who is at highest risk and needs more surveillance,” she said.
The AHA’s inclusion of GDM history is based on its strong link to overt diabetes, but recent evidence has shown that a history of GDM can independently elevate cardiovascular risk, she noted. Research from the Nurses Health Study II cohort, for instance, found a 30% higher relative risk of cardiovascular events (myocardial infarction and stroke) in women with a history of GDM without progression to diabetes, compared with women who did not have GDM or diabetes (JAMA Intern Med. 2017;177[12]:1735-42).
Dr. Gunderson has also found through analyses of the Coronary Artery Risk Development in Young Adults study data that women who had GDM but did not go on to develop overt diabetes or impaired glycemia had greater carotid intima media thickness many years post delivery than did women without a history of gestational diabetes (J Am Heart Assoc. 2014;3[2]:e000490).
In some models, she has written, this difference in carotid intima media thickness could represent 3-5 years of greater vascular aging for women with previous gestational diabetes and no apparent metabolic dysfunction outside of pregnancy (JAMA Intern Med. 2017;177[12]:1742-4).
There’s a question, she and Dr. Saade both noted, of whether pregnancies unmask previous dispositions to cardiovascular disease or whether pregnancy complications more directly drive adverse long-term outcomes. There is evidence that disorders such as GDM, Dr. Gunderson said, are superimposed on already altered metabolism. But at this time, Dr. Saade said, it appears that “the answer is both.”
According to Dr. Saade, at least three studies are currently following women prospectively to learn more about pregnancy as a window to future cardiovascular health. One of them is the National Institute of Child Health and Human Development’s Nulliparous Pregnancy Outcomes Study–Monitoring Mothers-to-Be Heart Health Study; some data from this study will be presented soon, he said.
Both Dr. Saade and Dr. Gunderson reported in their presentations that they had no disclosures.
WASHINGTON – George R. Saade, MD, wants to see a Time magazine cover story like the 2010 feature titled, “How the first 9 months shape the rest of your life” – except this new story would read “How the first 9 months shape the rest of the mother’s life.”
It’s time, he says, that pregnancy truly be appreciated as a “window to future health” for the mother as well as for the baby, and that the term “maternal care” replaces prenatal care. “How many of your [primary care] providers have asked you if you’ve had any pregnancies and if any of your pregnancies were complicated by hypertension, preterm delivery, growth restriction, or gestational diabetes?” Dr. Saade asked at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“It’s better than before, but not good enough ... Checking with patients 6 weeks postpartum is not enough” to prevent long-term metabolic and cardiovascular disorders, he said. “We need regular screening of women.”
The relationship between gestational diabetes (GDM) and subsequent type 2 diabetes, demonstrated several decades ago, offered the “first evidence that pregnancy is a window to future health,” and evidence of the relationship continues to grow. “We know today that there is no other predictive marker of type 2 diabetes that is better and stronger than gestational diabetes,” said Dr. Saade, chief of obstetrics and maternal-fetal medicine at the University of Texas Medical Branch, Galveston.
GDM has also recently been shown to elevate cardiovascular risk independent of its association with type 2 diabetes and metabolic disease.
And similarly, there is now an incontrovertible body of evidence that women who have had preeclampsia are at significantly higher risk of developing hypertension, stroke, and ischemic heart disease later in life than are women who have not have preeclampsia, Dr. Saade said.
Layered evidence
The study that first caught Dr. Saade’s attention was a large Norwegian population-based study published in 2001 that looked at maternal mortality up to 25 years after pregnancy. Women who had preeclampsia had a 1.2-fold higher long-term risk of death from cardiovascular diseases, cancer, and stroke – and women with a history of both preeclampsia and a preterm delivery had a 2.71-fold higher risk – than that of women without such history.
Looking at cardiovascular causes of death specifically, the risk among women with both preeclampsia and preterm delivery was 8.12-fold higher than in women who did not have preeclampsia.
Since then, studies and reviews conducted in the United States and Europe have shown that a history of preeclampsia doubles the risk of developing cardiovascular disease, more than triples the risk of later hypertension, and also increases the risk of stroke, though more moderately.
Recently, Dr. Saade said, researchers have also begun reporting subclinical cardiac abnormalities in women with a history of preeclampsia. A study of 107 women with preeclampsia and 41 women with uneventful pregnancies found that the prevalence of subclinical heart failure (heart failure Stage B) was approximately 3.5% higher in the short term in the preeclampsia group. The women underwent regular cardiac ultrasound and other cardiovascular risk assessment tests 4-10 years postpartum (Ultrasound Obstet Gynecol. 2017;49[1]:143-9).
Preterm delivery and small for gestational age have also been associated with increased risk of ischemic heart disease and other cardiovascular events later in life. And gestational hypertension, research has shown, is a clear risk factor for later hypertension. “We always think of preeclampsia as a different disease, but as far as long-term health is concerned, it doesn’t matter if a woman had preeclampsia or gestational hypertension; she’s still at [greater] risk for hypertension later,” Dr. Saade said.
“And we don’t have to wait 30 years to see evidence” of the association between pregnancy complications and adverse cardiovascular outcomes, he emphasized. A recent retrospective cohort study of more than 300,000 women in Florida showed that women who experienced a maternal placental syndrome during their first pregnancy were at higher risk of subsequent cardiovascular disease during just 5 years of follow-up (Am J Obstet Gynecol. 2016;215[4]:484.e1-14).
Into practice
Regular screening of women whose pregnancies were complicated by conditions associated with long-term health risks “need not be that sophisticated,” Dr. Saade said. Measurement of blood pressure, waist circumference, fasting lipid profile, and fasting glucose is often enough for basic maternal health surveillance, he said.
Dr. Saade said he and some other experts in the field are recommending yearly follow-up for patients who’ve had preeclampsia and other complications. Among the other experts urging early heart disease risk screening is Graeme N. Smith, MD, PhD, an ob.gyn in Ontario who has developed surveillance protocols, follow-up forms, and risk prediction tools for use in a maternal health clinic he established at Kingston General Hospital, Queens University. At the meeting, Dr. Saade encouraged the audience to access Dr. Smith’s resources.
The American Heart Association, in its 2011 guidelines for cardiovascular disease prevention in women, includes pregnancy risks factors (specifically a history of preeclampsia, gestational diabetes, or pregnancy-induced hypertension) as part of its list of major factors for use in risk assessment (Circulation. 2011;123:1243-62).
But as Erica P. Gunderson, PhD, MPH, of Kaiser Permanente Northern California’s division of research, pointed out during another presentation at the meeting, there is more work to be done. Reproductive history is not included in existing disease prediction or risk stratification models for atherosclerotic cardiovascular disease, making it hard at this point to devise specific screening protocols and schedules, especially when it comes to a history of GDM, she said.
“We need more coordinated systems, surveillance in younger women, and some prediction models so that we can know who is at highest risk and needs more surveillance,” she said.
The AHA’s inclusion of GDM history is based on its strong link to overt diabetes, but recent evidence has shown that a history of GDM can independently elevate cardiovascular risk, she noted. Research from the Nurses Health Study II cohort, for instance, found a 30% higher relative risk of cardiovascular events (myocardial infarction and stroke) in women with a history of GDM without progression to diabetes, compared with women who did not have GDM or diabetes (JAMA Intern Med. 2017;177[12]:1735-42).
Dr. Gunderson has also found through analyses of the Coronary Artery Risk Development in Young Adults study data that women who had GDM but did not go on to develop overt diabetes or impaired glycemia had greater carotid intima media thickness many years post delivery than did women without a history of gestational diabetes (J Am Heart Assoc. 2014;3[2]:e000490).
In some models, she has written, this difference in carotid intima media thickness could represent 3-5 years of greater vascular aging for women with previous gestational diabetes and no apparent metabolic dysfunction outside of pregnancy (JAMA Intern Med. 2017;177[12]:1742-4).
There’s a question, she and Dr. Saade both noted, of whether pregnancies unmask previous dispositions to cardiovascular disease or whether pregnancy complications more directly drive adverse long-term outcomes. There is evidence that disorders such as GDM, Dr. Gunderson said, are superimposed on already altered metabolism. But at this time, Dr. Saade said, it appears that “the answer is both.”
According to Dr. Saade, at least three studies are currently following women prospectively to learn more about pregnancy as a window to future cardiovascular health. One of them is the National Institute of Child Health and Human Development’s Nulliparous Pregnancy Outcomes Study–Monitoring Mothers-to-Be Heart Health Study; some data from this study will be presented soon, he said.
Both Dr. Saade and Dr. Gunderson reported in their presentations that they had no disclosures.
EXPERT ANALYSIS FROM DPSG-NA 2017
NIH goes straight to pregnant women in new research project
Research on pregnancy is now being crowdsourced, with pregnant women being asked in a new federal research project to “tell researchers and health care providers what pregnancy is really like.”
The project, PregSource, was launched in November by the National Institute of Child Health and Human Development (NICHD). Women who join PregSource (https://pregsource.nih.gov) are asked to chart changes to their weight, sleep, mood, morning sickness, and physical activity and to answer monthly online surveys about their pregnancy experiences, symptoms, and complications. It is hoped that resulting de-identified data will help inform future studies and improve maternal care, NICHD officials said.
“We had come to the recognition that we – the scientific community – lack a comprehensive database about how pregnancy affects women in the modern world,” said Caroline Signore, MD, MPH, deputy director of NICHD’s division of extramural research and principal investigator of PregSource.
“We spend a lot of time talking about the complications of pregnancy, but we don’t know a whole lot about the baseline experiences. . .the experiential trends of pregnancy” such as how many women experience morning sickness and for how long, and how pregnancy affects sleep patterns, she said.
By crowdsourcing to pregnant women themselves – by asking them to voluntarily offer data and make observations, “we’re researching on a large scale and doing so relatively cost effectively,” said Dr. Signore, an ob.gyn. “Women who are interested in contributing to science can [do so] on their own terms. They can visit PregSource on their own time and enter as much data as they want.”
Hal E. Lawrence III, MD, executive vice president and chief executive officer of the American College of Obstetricians and Gynecologists, called the project “groundbreaking” and said that NICHD should have “no problem” meeting its initial target of 100,000 pregnant women. “This is different from the other pregnancy apps,” he said. “This is more of a reporting and an informative [site], which the others aren’t.”
ACOG is one of about a dozen partnering organizations – along with the American Academy of Pediatrics and the American College of Nurse-Midwives – that have worked with NICHD on shaping the project and contributing content for a resource library that PregSource participants will have access to.
The project is currently in a “soft-launch phase,” Dr. Signore said, and will step up its outreach to women and providers in January.
Along with the current series of “trackers” and monthly questionnaires (in addition to questionnaires about prepregnancy health), women who indicate that they have physical disabilities or certain complications or conditions such as diabetes will be asked to participate in additional information-gathering modules. And once the project has amassed enough data, women will be able to compare specific experiences with those of other participants.
“A woman who’s 5 months’ pregnant and completes questions on nausea and vomiting, say, can click a button and see how everyone else who’s been in PregSource at this time has answered that question,” Dr. Signore said. “Or a woman who indicates she’s having a lot of heartburn at 27 weeks can learn about how many other women are having heartburn. We think this will be valuable for women, because [they’re] always wondering, ‘Is my experience unique?’ ”
NICHD officials said they hope women will share with their ob.gyns. or other providers the charts from their PregSource trackers, such as those plotting the individual’s weight gain against Institute of Medicine-recommended weight gain ranges. “We like to think that PregSource will promote conversations and shared decision making. . .and hopefully that it will improve that individual woman’s outcomes,” Dr. Signore said.
Indeed, said Uma M. Reddy, MD, MPH, project scientist for the NICHD’s Maternal-Fetal Medicine Units (MFMU) Network, women who use PregSource’s trackers should be “more in tune with their pregnancies” and with staying healthy. She and other experts touted PregSource at the recent biennial meeting of the Diabetes in Pregnancy Study Group.
The NICHD also plans to gently nudge women toward any relevant clinical studies underway in their locales “by simply notifying the women and making the information available to them,” Dr. Signore said. In addition, the project will invite women to track their experiences for several years after childbirth so more data can be generated on associations between pregnancy and child and maternal health. “Just as with the whole project, we’re trying to take into account the benefit-burden ratio and hope that women will continue to see value,” she said.
The NICHD-sponsored project will not sell or share any personal information to a third party, and participants will not receive any ads or product announcements. Data from the project – all of it de-identified – will be shared with approved researchers for their own analyses.
“We see it being already equipped to answer [existing] questions and to probe relationships” between pregnancy characteristics and complications, for instance, Dr. Signore said. “But it also could be a hypothesis-generating resource.”
A Spanish version will come “once we know we’ve optimized functionality and syntax,” she said. And overall, the NICHD is ready for growth, both in numbers of participants and in content.
ACOG is rooting for its success, Dr. Lawrence said. “We’ll have to wait and see how the results help us, but I’ll tell you one thing, having no data will never help us.”
Research on pregnancy is now being crowdsourced, with pregnant women being asked in a new federal research project to “tell researchers and health care providers what pregnancy is really like.”
The project, PregSource, was launched in November by the National Institute of Child Health and Human Development (NICHD). Women who join PregSource (https://pregsource.nih.gov) are asked to chart changes to their weight, sleep, mood, morning sickness, and physical activity and to answer monthly online surveys about their pregnancy experiences, symptoms, and complications. It is hoped that resulting de-identified data will help inform future studies and improve maternal care, NICHD officials said.
“We had come to the recognition that we – the scientific community – lack a comprehensive database about how pregnancy affects women in the modern world,” said Caroline Signore, MD, MPH, deputy director of NICHD’s division of extramural research and principal investigator of PregSource.
“We spend a lot of time talking about the complications of pregnancy, but we don’t know a whole lot about the baseline experiences. . .the experiential trends of pregnancy” such as how many women experience morning sickness and for how long, and how pregnancy affects sleep patterns, she said.
By crowdsourcing to pregnant women themselves – by asking them to voluntarily offer data and make observations, “we’re researching on a large scale and doing so relatively cost effectively,” said Dr. Signore, an ob.gyn. “Women who are interested in contributing to science can [do so] on their own terms. They can visit PregSource on their own time and enter as much data as they want.”
Hal E. Lawrence III, MD, executive vice president and chief executive officer of the American College of Obstetricians and Gynecologists, called the project “groundbreaking” and said that NICHD should have “no problem” meeting its initial target of 100,000 pregnant women. “This is different from the other pregnancy apps,” he said. “This is more of a reporting and an informative [site], which the others aren’t.”
ACOG is one of about a dozen partnering organizations – along with the American Academy of Pediatrics and the American College of Nurse-Midwives – that have worked with NICHD on shaping the project and contributing content for a resource library that PregSource participants will have access to.
The project is currently in a “soft-launch phase,” Dr. Signore said, and will step up its outreach to women and providers in January.
Along with the current series of “trackers” and monthly questionnaires (in addition to questionnaires about prepregnancy health), women who indicate that they have physical disabilities or certain complications or conditions such as diabetes will be asked to participate in additional information-gathering modules. And once the project has amassed enough data, women will be able to compare specific experiences with those of other participants.
“A woman who’s 5 months’ pregnant and completes questions on nausea and vomiting, say, can click a button and see how everyone else who’s been in PregSource at this time has answered that question,” Dr. Signore said. “Or a woman who indicates she’s having a lot of heartburn at 27 weeks can learn about how many other women are having heartburn. We think this will be valuable for women, because [they’re] always wondering, ‘Is my experience unique?’ ”
NICHD officials said they hope women will share with their ob.gyns. or other providers the charts from their PregSource trackers, such as those plotting the individual’s weight gain against Institute of Medicine-recommended weight gain ranges. “We like to think that PregSource will promote conversations and shared decision making. . .and hopefully that it will improve that individual woman’s outcomes,” Dr. Signore said.
Indeed, said Uma M. Reddy, MD, MPH, project scientist for the NICHD’s Maternal-Fetal Medicine Units (MFMU) Network, women who use PregSource’s trackers should be “more in tune with their pregnancies” and with staying healthy. She and other experts touted PregSource at the recent biennial meeting of the Diabetes in Pregnancy Study Group.
The NICHD also plans to gently nudge women toward any relevant clinical studies underway in their locales “by simply notifying the women and making the information available to them,” Dr. Signore said. In addition, the project will invite women to track their experiences for several years after childbirth so more data can be generated on associations between pregnancy and child and maternal health. “Just as with the whole project, we’re trying to take into account the benefit-burden ratio and hope that women will continue to see value,” she said.
The NICHD-sponsored project will not sell or share any personal information to a third party, and participants will not receive any ads or product announcements. Data from the project – all of it de-identified – will be shared with approved researchers for their own analyses.
“We see it being already equipped to answer [existing] questions and to probe relationships” between pregnancy characteristics and complications, for instance, Dr. Signore said. “But it also could be a hypothesis-generating resource.”
A Spanish version will come “once we know we’ve optimized functionality and syntax,” she said. And overall, the NICHD is ready for growth, both in numbers of participants and in content.
ACOG is rooting for its success, Dr. Lawrence said. “We’ll have to wait and see how the results help us, but I’ll tell you one thing, having no data will never help us.”
Research on pregnancy is now being crowdsourced, with pregnant women being asked in a new federal research project to “tell researchers and health care providers what pregnancy is really like.”
The project, PregSource, was launched in November by the National Institute of Child Health and Human Development (NICHD). Women who join PregSource (https://pregsource.nih.gov) are asked to chart changes to their weight, sleep, mood, morning sickness, and physical activity and to answer monthly online surveys about their pregnancy experiences, symptoms, and complications. It is hoped that resulting de-identified data will help inform future studies and improve maternal care, NICHD officials said.
“We had come to the recognition that we – the scientific community – lack a comprehensive database about how pregnancy affects women in the modern world,” said Caroline Signore, MD, MPH, deputy director of NICHD’s division of extramural research and principal investigator of PregSource.
“We spend a lot of time talking about the complications of pregnancy, but we don’t know a whole lot about the baseline experiences. . .the experiential trends of pregnancy” such as how many women experience morning sickness and for how long, and how pregnancy affects sleep patterns, she said.
By crowdsourcing to pregnant women themselves – by asking them to voluntarily offer data and make observations, “we’re researching on a large scale and doing so relatively cost effectively,” said Dr. Signore, an ob.gyn. “Women who are interested in contributing to science can [do so] on their own terms. They can visit PregSource on their own time and enter as much data as they want.”
Hal E. Lawrence III, MD, executive vice president and chief executive officer of the American College of Obstetricians and Gynecologists, called the project “groundbreaking” and said that NICHD should have “no problem” meeting its initial target of 100,000 pregnant women. “This is different from the other pregnancy apps,” he said. “This is more of a reporting and an informative [site], which the others aren’t.”
ACOG is one of about a dozen partnering organizations – along with the American Academy of Pediatrics and the American College of Nurse-Midwives – that have worked with NICHD on shaping the project and contributing content for a resource library that PregSource participants will have access to.
The project is currently in a “soft-launch phase,” Dr. Signore said, and will step up its outreach to women and providers in January.
Along with the current series of “trackers” and monthly questionnaires (in addition to questionnaires about prepregnancy health), women who indicate that they have physical disabilities or certain complications or conditions such as diabetes will be asked to participate in additional information-gathering modules. And once the project has amassed enough data, women will be able to compare specific experiences with those of other participants.
“A woman who’s 5 months’ pregnant and completes questions on nausea and vomiting, say, can click a button and see how everyone else who’s been in PregSource at this time has answered that question,” Dr. Signore said. “Or a woman who indicates she’s having a lot of heartburn at 27 weeks can learn about how many other women are having heartburn. We think this will be valuable for women, because [they’re] always wondering, ‘Is my experience unique?’ ”
NICHD officials said they hope women will share with their ob.gyns. or other providers the charts from their PregSource trackers, such as those plotting the individual’s weight gain against Institute of Medicine-recommended weight gain ranges. “We like to think that PregSource will promote conversations and shared decision making. . .and hopefully that it will improve that individual woman’s outcomes,” Dr. Signore said.
Indeed, said Uma M. Reddy, MD, MPH, project scientist for the NICHD’s Maternal-Fetal Medicine Units (MFMU) Network, women who use PregSource’s trackers should be “more in tune with their pregnancies” and with staying healthy. She and other experts touted PregSource at the recent biennial meeting of the Diabetes in Pregnancy Study Group.
The NICHD also plans to gently nudge women toward any relevant clinical studies underway in their locales “by simply notifying the women and making the information available to them,” Dr. Signore said. In addition, the project will invite women to track their experiences for several years after childbirth so more data can be generated on associations between pregnancy and child and maternal health. “Just as with the whole project, we’re trying to take into account the benefit-burden ratio and hope that women will continue to see value,” she said.
The NICHD-sponsored project will not sell or share any personal information to a third party, and participants will not receive any ads or product announcements. Data from the project – all of it de-identified – will be shared with approved researchers for their own analyses.
“We see it being already equipped to answer [existing] questions and to probe relationships” between pregnancy characteristics and complications, for instance, Dr. Signore said. “But it also could be a hypothesis-generating resource.”
A Spanish version will come “once we know we’ve optimized functionality and syntax,” she said. And overall, the NICHD is ready for growth, both in numbers of participants and in content.
ACOG is rooting for its success, Dr. Lawrence said. “We’ll have to wait and see how the results help us, but I’ll tell you one thing, having no data will never help us.”

To predict macrosomia, focus on the abdomen
WASHINGTON – , John C. Hobbins, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“Everything that the estimated fetal weight [EFW] can do, the abdominal circumference can do better,” especially in diabetic mothers, said Dr. Hobbins, who is widely regarded as one of the early pioneers in the development and use of obstetric ultrasound as a diagnostic tool.
Because it reflects liver size and incorporates subcutaneous fat, the abdominal circumference (AC) “concentrates on where the action is,” he said. It also “roughly correlates” with the size of the fetal shoulders and is not affected by genetic factors.
Moreover, “it focuses on one task rather than putting into play four variables, each with its own standard error of the method,” said Dr. Hobbins, referring to the four fetal biometric parameters incorporated into the Hadlock formula for EFW that is provided “upon fire-up of virtually every ultrasound machine.”
These four parameters (biparietal diameter, head circumference, femur length, and AC) each contribute to fetal weight but the AC has been shown to correlate better with weight at birth than the other variables, and it is the only measure that reflects how corpulent the fetus is, he noted.
The “general rule of thumb is that the EFW [as calculated by ultrasound machine–based equations] has a standard error of the method of plus or minus 10%. … which means that an EFW of 4,000 g is associated with a splay of plus or minus 1.2 pounds,” said Dr. Hobbins, professor of obstetrics and gynecology at the University of Colorado at Denver, Aurora.
“But the problem for us is not the failure of the ultrasound – it’s the way we use it,” he said.
An assortment of customized formulas have been developed for macrosomia, including one designed for use in diabetes that incorporates AC, head circumference, femur length, and 3D volumes of the thigh and abdomen. “If one used this and set a cut-off at 4,300 g, you’d pick up 93%. … but at false positive rate of 38%,” he said.
While not perfect, the AC alone is as accurate as more complicated formulas to detect macrosomic fetuses, he emphasized. “It’s a tough [measurement] to get just before the baby is born, but you can do it a little bit earlier,” he said. Research has shown that screening at 30-34 weeks can capture a majority of the fetuses destined to be greater than 4,000 g at birth, with a lower false-positive rate.
He pointed to one “very interesting” recent study in which AC was measured with a handheld ultrasound device at 24-40 weeks’ gestation, prior to formal ultrasound estimation of EFW. Early AC was a better predictor of large-for-gestational age babies at birth than EFW or early fundal height measurement, with sensitivities of 67%, 25%, and 50%, respectively (Am J Obstet Gynecol. 2015 Jun;212[6]:820.e1-8).
“And AC had a false-positive rate of only 10%,” Dr. Hobbins said.
Macrosomia occurs in 20% of cases of gestational diabetes and 25% of pregestational diabetes, he said. “And even if there is adequate glucose control, 17% will be macrosomic.”
The condition correlates with childhood and adulthood metabolic dysfunction and is associated with significantly increased risk of birth injury to the infant and to the mother. The alternative – cesarean delivery – is “not innocuous,” and “[we have] a very low threshold for cesarean if macrosomia is suspected,” Dr. Hobbins said.
Dr. Hobbins reported having no financial disclosures.
WASHINGTON – , John C. Hobbins, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“Everything that the estimated fetal weight [EFW] can do, the abdominal circumference can do better,” especially in diabetic mothers, said Dr. Hobbins, who is widely regarded as one of the early pioneers in the development and use of obstetric ultrasound as a diagnostic tool.
Because it reflects liver size and incorporates subcutaneous fat, the abdominal circumference (AC) “concentrates on where the action is,” he said. It also “roughly correlates” with the size of the fetal shoulders and is not affected by genetic factors.
Moreover, “it focuses on one task rather than putting into play four variables, each with its own standard error of the method,” said Dr. Hobbins, referring to the four fetal biometric parameters incorporated into the Hadlock formula for EFW that is provided “upon fire-up of virtually every ultrasound machine.”
These four parameters (biparietal diameter, head circumference, femur length, and AC) each contribute to fetal weight but the AC has been shown to correlate better with weight at birth than the other variables, and it is the only measure that reflects how corpulent the fetus is, he noted.
The “general rule of thumb is that the EFW [as calculated by ultrasound machine–based equations] has a standard error of the method of plus or minus 10%. … which means that an EFW of 4,000 g is associated with a splay of plus or minus 1.2 pounds,” said Dr. Hobbins, professor of obstetrics and gynecology at the University of Colorado at Denver, Aurora.
“But the problem for us is not the failure of the ultrasound – it’s the way we use it,” he said.
An assortment of customized formulas have been developed for macrosomia, including one designed for use in diabetes that incorporates AC, head circumference, femur length, and 3D volumes of the thigh and abdomen. “If one used this and set a cut-off at 4,300 g, you’d pick up 93%. … but at false positive rate of 38%,” he said.
While not perfect, the AC alone is as accurate as more complicated formulas to detect macrosomic fetuses, he emphasized. “It’s a tough [measurement] to get just before the baby is born, but you can do it a little bit earlier,” he said. Research has shown that screening at 30-34 weeks can capture a majority of the fetuses destined to be greater than 4,000 g at birth, with a lower false-positive rate.
He pointed to one “very interesting” recent study in which AC was measured with a handheld ultrasound device at 24-40 weeks’ gestation, prior to formal ultrasound estimation of EFW. Early AC was a better predictor of large-for-gestational age babies at birth than EFW or early fundal height measurement, with sensitivities of 67%, 25%, and 50%, respectively (Am J Obstet Gynecol. 2015 Jun;212[6]:820.e1-8).
“And AC had a false-positive rate of only 10%,” Dr. Hobbins said.
Macrosomia occurs in 20% of cases of gestational diabetes and 25% of pregestational diabetes, he said. “And even if there is adequate glucose control, 17% will be macrosomic.”
The condition correlates with childhood and adulthood metabolic dysfunction and is associated with significantly increased risk of birth injury to the infant and to the mother. The alternative – cesarean delivery – is “not innocuous,” and “[we have] a very low threshold for cesarean if macrosomia is suspected,” Dr. Hobbins said.
Dr. Hobbins reported having no financial disclosures.
WASHINGTON – , John C. Hobbins, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“Everything that the estimated fetal weight [EFW] can do, the abdominal circumference can do better,” especially in diabetic mothers, said Dr. Hobbins, who is widely regarded as one of the early pioneers in the development and use of obstetric ultrasound as a diagnostic tool.
Because it reflects liver size and incorporates subcutaneous fat, the abdominal circumference (AC) “concentrates on where the action is,” he said. It also “roughly correlates” with the size of the fetal shoulders and is not affected by genetic factors.
Moreover, “it focuses on one task rather than putting into play four variables, each with its own standard error of the method,” said Dr. Hobbins, referring to the four fetal biometric parameters incorporated into the Hadlock formula for EFW that is provided “upon fire-up of virtually every ultrasound machine.”
These four parameters (biparietal diameter, head circumference, femur length, and AC) each contribute to fetal weight but the AC has been shown to correlate better with weight at birth than the other variables, and it is the only measure that reflects how corpulent the fetus is, he noted.
The “general rule of thumb is that the EFW [as calculated by ultrasound machine–based equations] has a standard error of the method of plus or minus 10%. … which means that an EFW of 4,000 g is associated with a splay of plus or minus 1.2 pounds,” said Dr. Hobbins, professor of obstetrics and gynecology at the University of Colorado at Denver, Aurora.
“But the problem for us is not the failure of the ultrasound – it’s the way we use it,” he said.
An assortment of customized formulas have been developed for macrosomia, including one designed for use in diabetes that incorporates AC, head circumference, femur length, and 3D volumes of the thigh and abdomen. “If one used this and set a cut-off at 4,300 g, you’d pick up 93%. … but at false positive rate of 38%,” he said.
While not perfect, the AC alone is as accurate as more complicated formulas to detect macrosomic fetuses, he emphasized. “It’s a tough [measurement] to get just before the baby is born, but you can do it a little bit earlier,” he said. Research has shown that screening at 30-34 weeks can capture a majority of the fetuses destined to be greater than 4,000 g at birth, with a lower false-positive rate.
He pointed to one “very interesting” recent study in which AC was measured with a handheld ultrasound device at 24-40 weeks’ gestation, prior to formal ultrasound estimation of EFW. Early AC was a better predictor of large-for-gestational age babies at birth than EFW or early fundal height measurement, with sensitivities of 67%, 25%, and 50%, respectively (Am J Obstet Gynecol. 2015 Jun;212[6]:820.e1-8).
“And AC had a false-positive rate of only 10%,” Dr. Hobbins said.
Macrosomia occurs in 20% of cases of gestational diabetes and 25% of pregestational diabetes, he said. “And even if there is adequate glucose control, 17% will be macrosomic.”
The condition correlates with childhood and adulthood metabolic dysfunction and is associated with significantly increased risk of birth injury to the infant and to the mother. The alternative – cesarean delivery – is “not innocuous,” and “[we have] a very low threshold for cesarean if macrosomia is suspected,” Dr. Hobbins said.
Dr. Hobbins reported having no financial disclosures.
EXPERT ANALYSIS FROM DPSG-NA 2017
Experts question insulin as top choice in GDM
WASHINGTON – The American College of Obstetricians and Gynecologists’ conclusion that insulin should be considered the first-line pharmacologic treatment for gestational diabetes came under fire at a recent meeting on diabetes in pregnancy, indicating the extent to which controversy persists over the use of oral antidiabetic medications in pregnancy.
“Like many others, I’m perplexed by the strong endorsement,” Mark Landon, MD, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus, said during an open discussion of oral hypoglycemic agents held at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
Dr. Landon and several other researchers and experts in diabetes in pregnancy expressed discontent with any firm prioritization of the drugs most commonly used for gestational diabetes, saying that there are not yet enough data to do so.

The endorsement of insulin as the first-line option when pharmacologic treatment is needed is a level A conclusion/recommendation in ACOG’s updated practice bulletin on gestational diabetes mellitus, released in July 2017 (Obstet Gynecol. 2017;130[1]:e17-37). In accompanying level B recommendations, ACOG stated that in women who decline insulin therapy or who are believed to be “unable to safely administer insulin,” metformin is a “reasonable second-line choice.” Glyburide “should not be recommended as a first-line pharmacologic treatment because, in most studies, it does not yield equivalent outcomes to insulin.”
Level A recommendations are defined as “based on good and consistent scientific evidence,” while the evidence for level B recommendations is “limited or inconsistent.”
Asked to comment on the concerns voiced at the meeting, an ACOG spokeswoman said that the recommendations were developed after a thorough literature review, but that the evidence was being reexamined with the option of updating the practice bulletin.
Current recommendations
In its practice bulletin, ACOG noted that oral antidiabetic medications, such as glyburide and metformin, are increasingly used among women with GDM, despite not being approved by the Food and Drug Administration for this indication and even though insulin continues to be the recommended as first-line therapy by the American Diabetes Association (ADA).
The ADA, in a summary of its 2017 guideline on the management of diabetes in pregnancy, stated that insulin is the “preferred medication for treating hyperglycemia in gestational diabetes mellitus, as it does not cross the placenta to a measurable extent.” Metformin and glyburide are options, “but both cross the placenta to the fetus, with metformin likely crossing to a greater extent than glyburide” (Diabetes Care. 2017 Jan;40[Suppl 1]:S114- 9).Regarding metformin, the ACOG bulletin cited two trials that randomized women to metformin or insulin – one in which both groups experienced similar rates of a composite outcome of perinatal morbidity, and another in which women receiving metformin had lower mean glucose levels, less gestational weight gain, and neonates with lower rates of hypoglycemia.
ACOG also cited a meta-analysis, that found “minimal differences” between neonates of women randomized to metformin versus insulin, but also noted that “interestingly, women randomized to metformin experienced a higher rate of preterm birth” and a lower rate of gestational hypertension (BMJ. 2015;350:h102).
With respect to glyburide, the ACOG bulletin said that two recent meta-analyses had demonstrated worse neonatal outcomes with glyburide, compared with insulin, and that observational studies have shown higher rates of preeclampsia, hyperbilirubinemia, and stillbirth with the use of glyburide, compared with insulin. However, many other outcomes have not been statistically significantly different, according to the practice bulletin.
Additionally, at least 4%-16% of women eventually require the addition of insulin when glyburide is used as initial treatment, as do 26%-46% of women who take metformin, according to ACOG.
Regarding placental transfer, ACOG’s bulletin said that while one study that analyzed umbilical cord blood revealed no detectable glyburide in exposed pregnancies, another study demonstrated that glyburide does cross the placenta. Metformin has also been found to cross the placenta, with the fetus exposed to concentrations similar to maternal levels, the bulletin noted.
“Although current data demonstrate no adverse short-term effects on maternal or neonatal health from oral diabetic therapy during pregnancy, long-term outcomes are not yet available,” ACOG wrote in the practice bulletin.
Concerns about research
As Thomas Moore, MD, sees it, the quality of available data is insufficient to recommend insulin over oral agents, or one oral agent over another. “We really need to focus [the National Institutes of Health] on putting together proper studies,” he said at the meeting.
In a later interview, Dr. Moore referred to two recent Cochrane reviews. One review, published in January 2017, analyzed eight studies of oral antidiabetic therapies for GDM and concluded there was “insufficient high-quality evidence to be able to draw any meaningful conclusions as to the benefits of one oral antidiabetic pharmacological therapy over another” (Cochrane Database Syst Rev. 2017 Jan 25;1:CD011967).
The other Cochrane review, published in November 2017, concluded that insulin and oral antidiabetic agents have similar effects on key health outcomes, and that each one has minimal harms. The quality of evidence, the authors said, ranged from “very low to moderate, with downgrading decisions due to imprecision, risk of bias, and inconsistency” (Cochrane Database Syst Rev. 2017 Nov 5;11:CD012037).
Dr. Moore, professor of maternal-fetal medicine at the University of California, San Diego, cautioned against presuming that placental transfer of an antidiabetic drug is “ipso facto dangerous or terrible.” Moreover, he said that it’s not yet clear whether glyburide crosses the placenta in the first place.
Dr. Moore, Dr. Landon, and others at the meeting said they are eagerly awaiting long-term follow-up data from the Metformin in Gestational Diabetes (MiG) trial underway in Australia. The prospective randomized trial is designed to compare metformin with insulin and finished recruiting women in 2006. A recently published analysis found similar neurodevelopmental outcomes in offspring at 2 years, but it’s the longer-term data looking into early puberty that experts now want to see (Arch Dis Child Fetal Neonatal Ed. 2016 Feb 24. doi: 10.1136/archdischild-2015-309602).
In the meantime, Dr. Landon said the “short-term safety record for oral antidiabetic medications is actually pretty good.” There are studies “suggesting an increased risk for large babies with glyburide, but these are very small RCTs [randomized controlled trials],” he said in an interview.
Data from population-based studies, moreover, are “flawed in as much as we don’t know the thresholds for initiating glyburide treatment, nor do we know whether the women were really good candidates for this therapy,” Dr. Landon said. “It’s conceivable, and it’s been my experience, that glyburide has been overprescribed and inappropriately prescribed in certain women with GDM who really should receive insulin therapy.”
Whether glyburide and metformin are being prescribed for GDM in optimal doses is another growing question – one that interests Steve N. Caritis, MD. The drugs are typically prescribed to be taken twice a day every 12 hours, but he said he is finding that some patients may need more frequent, individually tailored dosing.
“We may have come to conclusions in [the studies published thus far] that may not be the correct conclusions,” Dr. Caritis, who coleads obstetric pharmacology research at the Magee-Womens Research Institute in Pittsburgh, said at the DPSG meeting. “The question is, If the dosing were appropriate, would we have the same outcomes?”
“We were asked, Are people using [oral antidiabetic medications] properly? Could the fact that glyburide may not have had the efficacy we’d hoped for [in published studies] be due to it not being used properly?” Dr. Catalano said.
Individualizing drug choice
Dosing aside, there may be populations of women who respond poorly to a medication because of the underlying pathophysiology of their GDM, said Maisa N. Feghali, MD, assistant professor of obstetrics, gynecology, and reproductive sciences at the University of Pittsburgh.
A study published in 2016 demonstrated the heterogeneity of the physiologic processes underlying hyperglycemia in 67 women with GDM. Almost one-third of women with GDM had predominant insulin secretion deficit, one-half had predominant insulin resistance, and the remaining 20% had a mixed “metabolic profile” (Diabetes Care. 2016 Jun;39[6]:1052-5).
This study prompted Dr. Feghali and her colleagues to design a pilot study aimed at testing an individualized approach that matches treatment to GDM mechanism. “We [currently] have the expectation that all glucose-lowering agents will be similarly effective despite significant variation in underlying GDM pathophysiology,” she said during a presentation at the DPSG meeting. “But I think we have a mismatch between variations in GDM and the uniformity of treatment.”
In her pilot study, women diagnosed with GDM who fail dietary control will be randomized into usual treatment or matched treatment (metformin for predominant insulin resistance, glyburide or insulin for predominant insulin secretion defects, and one of the three for combined insulin resistance and insulin secretion defects).
The MATCh-GDM study (Metabolic Analysis for Treatment Choice of GDM) is just getting underway. Patients will be monitored for consistency of GDM mechanism and glucose control, and routine clinical variables (hypertensive diseases, cesarean delivery, and birth weight) will be studied, as well as neonatal body composition, cord blood glucose, and cord blood C-peptide.
WASHINGTON – The American College of Obstetricians and Gynecologists’ conclusion that insulin should be considered the first-line pharmacologic treatment for gestational diabetes came under fire at a recent meeting on diabetes in pregnancy, indicating the extent to which controversy persists over the use of oral antidiabetic medications in pregnancy.
“Like many others, I’m perplexed by the strong endorsement,” Mark Landon, MD, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus, said during an open discussion of oral hypoglycemic agents held at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
Dr. Landon and several other researchers and experts in diabetes in pregnancy expressed discontent with any firm prioritization of the drugs most commonly used for gestational diabetes, saying that there are not yet enough data to do so.
The endorsement of insulin as the first-line option when pharmacologic treatment is needed is a level A conclusion/recommendation in ACOG’s updated practice bulletin on gestational diabetes mellitus, released in July 2017 (Obstet Gynecol. 2017;130[1]:e17-37). In accompanying level B recommendations, ACOG stated that in women who decline insulin therapy or who are believed to be “unable to safely administer insulin,” metformin is a “reasonable second-line choice.” Glyburide “should not be recommended as a first-line pharmacologic treatment because, in most studies, it does not yield equivalent outcomes to insulin.”
Level A recommendations are defined as “based on good and consistent scientific evidence,” while the evidence for level B recommendations is “limited or inconsistent.”
Asked to comment on the concerns voiced at the meeting, an ACOG spokeswoman said that the recommendations were developed after a thorough literature review, but that the evidence was being reexamined with the option of updating the practice bulletin.
Current recommendations
In its practice bulletin, ACOG noted that oral antidiabetic medications, such as glyburide and metformin, are increasingly used among women with GDM, despite not being approved by the Food and Drug Administration for this indication and even though insulin continues to be the recommended as first-line therapy by the American Diabetes Association (ADA).
The ADA, in a summary of its 2017 guideline on the management of diabetes in pregnancy, stated that insulin is the “preferred medication for treating hyperglycemia in gestational diabetes mellitus, as it does not cross the placenta to a measurable extent.” Metformin and glyburide are options, “but both cross the placenta to the fetus, with metformin likely crossing to a greater extent than glyburide” (Diabetes Care. 2017 Jan;40[Suppl 1]:S114- 9).Regarding metformin, the ACOG bulletin cited two trials that randomized women to metformin or insulin – one in which both groups experienced similar rates of a composite outcome of perinatal morbidity, and another in which women receiving metformin had lower mean glucose levels, less gestational weight gain, and neonates with lower rates of hypoglycemia.
ACOG also cited a meta-analysis, that found “minimal differences” between neonates of women randomized to metformin versus insulin, but also noted that “interestingly, women randomized to metformin experienced a higher rate of preterm birth” and a lower rate of gestational hypertension (BMJ. 2015;350:h102).
With respect to glyburide, the ACOG bulletin said that two recent meta-analyses had demonstrated worse neonatal outcomes with glyburide, compared with insulin, and that observational studies have shown higher rates of preeclampsia, hyperbilirubinemia, and stillbirth with the use of glyburide, compared with insulin. However, many other outcomes have not been statistically significantly different, according to the practice bulletin.
Additionally, at least 4%-16% of women eventually require the addition of insulin when glyburide is used as initial treatment, as do 26%-46% of women who take metformin, according to ACOG.
Regarding placental transfer, ACOG’s bulletin said that while one study that analyzed umbilical cord blood revealed no detectable glyburide in exposed pregnancies, another study demonstrated that glyburide does cross the placenta. Metformin has also been found to cross the placenta, with the fetus exposed to concentrations similar to maternal levels, the bulletin noted.
“Although current data demonstrate no adverse short-term effects on maternal or neonatal health from oral diabetic therapy during pregnancy, long-term outcomes are not yet available,” ACOG wrote in the practice bulletin.
Concerns about research
As Thomas Moore, MD, sees it, the quality of available data is insufficient to recommend insulin over oral agents, or one oral agent over another. “We really need to focus [the National Institutes of Health] on putting together proper studies,” he said at the meeting.
In a later interview, Dr. Moore referred to two recent Cochrane reviews. One review, published in January 2017, analyzed eight studies of oral antidiabetic therapies for GDM and concluded there was “insufficient high-quality evidence to be able to draw any meaningful conclusions as to the benefits of one oral antidiabetic pharmacological therapy over another” (Cochrane Database Syst Rev. 2017 Jan 25;1:CD011967).
The other Cochrane review, published in November 2017, concluded that insulin and oral antidiabetic agents have similar effects on key health outcomes, and that each one has minimal harms. The quality of evidence, the authors said, ranged from “very low to moderate, with downgrading decisions due to imprecision, risk of bias, and inconsistency” (Cochrane Database Syst Rev. 2017 Nov 5;11:CD012037).
Dr. Moore, professor of maternal-fetal medicine at the University of California, San Diego, cautioned against presuming that placental transfer of an antidiabetic drug is “ipso facto dangerous or terrible.” Moreover, he said that it’s not yet clear whether glyburide crosses the placenta in the first place.
Dr. Moore, Dr. Landon, and others at the meeting said they are eagerly awaiting long-term follow-up data from the Metformin in Gestational Diabetes (MiG) trial underway in Australia. The prospective randomized trial is designed to compare metformin with insulin and finished recruiting women in 2006. A recently published analysis found similar neurodevelopmental outcomes in offspring at 2 years, but it’s the longer-term data looking into early puberty that experts now want to see (Arch Dis Child Fetal Neonatal Ed. 2016 Feb 24. doi: 10.1136/archdischild-2015-309602).
In the meantime, Dr. Landon said the “short-term safety record for oral antidiabetic medications is actually pretty good.” There are studies “suggesting an increased risk for large babies with glyburide, but these are very small RCTs [randomized controlled trials],” he said in an interview.
Data from population-based studies, moreover, are “flawed in as much as we don’t know the thresholds for initiating glyburide treatment, nor do we know whether the women were really good candidates for this therapy,” Dr. Landon said. “It’s conceivable, and it’s been my experience, that glyburide has been overprescribed and inappropriately prescribed in certain women with GDM who really should receive insulin therapy.”
Whether glyburide and metformin are being prescribed for GDM in optimal doses is another growing question – one that interests Steve N. Caritis, MD. The drugs are typically prescribed to be taken twice a day every 12 hours, but he said he is finding that some patients may need more frequent, individually tailored dosing.
“We may have come to conclusions in [the studies published thus far] that may not be the correct conclusions,” Dr. Caritis, who coleads obstetric pharmacology research at the Magee-Womens Research Institute in Pittsburgh, said at the DPSG meeting. “The question is, If the dosing were appropriate, would we have the same outcomes?”
“We were asked, Are people using [oral antidiabetic medications] properly? Could the fact that glyburide may not have had the efficacy we’d hoped for [in published studies] be due to it not being used properly?” Dr. Catalano said.
Individualizing drug choice
Dosing aside, there may be populations of women who respond poorly to a medication because of the underlying pathophysiology of their GDM, said Maisa N. Feghali, MD, assistant professor of obstetrics, gynecology, and reproductive sciences at the University of Pittsburgh.
A study published in 2016 demonstrated the heterogeneity of the physiologic processes underlying hyperglycemia in 67 women with GDM. Almost one-third of women with GDM had predominant insulin secretion deficit, one-half had predominant insulin resistance, and the remaining 20% had a mixed “metabolic profile” (Diabetes Care. 2016 Jun;39[6]:1052-5).
This study prompted Dr. Feghali and her colleagues to design a pilot study aimed at testing an individualized approach that matches treatment to GDM mechanism. “We [currently] have the expectation that all glucose-lowering agents will be similarly effective despite significant variation in underlying GDM pathophysiology,” she said during a presentation at the DPSG meeting. “But I think we have a mismatch between variations in GDM and the uniformity of treatment.”
In her pilot study, women diagnosed with GDM who fail dietary control will be randomized into usual treatment or matched treatment (metformin for predominant insulin resistance, glyburide or insulin for predominant insulin secretion defects, and one of the three for combined insulin resistance and insulin secretion defects).
The MATCh-GDM study (Metabolic Analysis for Treatment Choice of GDM) is just getting underway. Patients will be monitored for consistency of GDM mechanism and glucose control, and routine clinical variables (hypertensive diseases, cesarean delivery, and birth weight) will be studied, as well as neonatal body composition, cord blood glucose, and cord blood C-peptide.
WASHINGTON – The American College of Obstetricians and Gynecologists’ conclusion that insulin should be considered the first-line pharmacologic treatment for gestational diabetes came under fire at a recent meeting on diabetes in pregnancy, indicating the extent to which controversy persists over the use of oral antidiabetic medications in pregnancy.
“Like many others, I’m perplexed by the strong endorsement,” Mark Landon, MD, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus, said during an open discussion of oral hypoglycemic agents held at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
Dr. Landon and several other researchers and experts in diabetes in pregnancy expressed discontent with any firm prioritization of the drugs most commonly used for gestational diabetes, saying that there are not yet enough data to do so.
The endorsement of insulin as the first-line option when pharmacologic treatment is needed is a level A conclusion/recommendation in ACOG’s updated practice bulletin on gestational diabetes mellitus, released in July 2017 (Obstet Gynecol. 2017;130[1]:e17-37). In accompanying level B recommendations, ACOG stated that in women who decline insulin therapy or who are believed to be “unable to safely administer insulin,” metformin is a “reasonable second-line choice.” Glyburide “should not be recommended as a first-line pharmacologic treatment because, in most studies, it does not yield equivalent outcomes to insulin.”
Level A recommendations are defined as “based on good and consistent scientific evidence,” while the evidence for level B recommendations is “limited or inconsistent.”
Asked to comment on the concerns voiced at the meeting, an ACOG spokeswoman said that the recommendations were developed after a thorough literature review, but that the evidence was being reexamined with the option of updating the practice bulletin.
Current recommendations
In its practice bulletin, ACOG noted that oral antidiabetic medications, such as glyburide and metformin, are increasingly used among women with GDM, despite not being approved by the Food and Drug Administration for this indication and even though insulin continues to be the recommended as first-line therapy by the American Diabetes Association (ADA).
The ADA, in a summary of its 2017 guideline on the management of diabetes in pregnancy, stated that insulin is the “preferred medication for treating hyperglycemia in gestational diabetes mellitus, as it does not cross the placenta to a measurable extent.” Metformin and glyburide are options, “but both cross the placenta to the fetus, with metformin likely crossing to a greater extent than glyburide” (Diabetes Care. 2017 Jan;40[Suppl 1]:S114- 9).Regarding metformin, the ACOG bulletin cited two trials that randomized women to metformin or insulin – one in which both groups experienced similar rates of a composite outcome of perinatal morbidity, and another in which women receiving metformin had lower mean glucose levels, less gestational weight gain, and neonates with lower rates of hypoglycemia.
ACOG also cited a meta-analysis, that found “minimal differences” between neonates of women randomized to metformin versus insulin, but also noted that “interestingly, women randomized to metformin experienced a higher rate of preterm birth” and a lower rate of gestational hypertension (BMJ. 2015;350:h102).
With respect to glyburide, the ACOG bulletin said that two recent meta-analyses had demonstrated worse neonatal outcomes with glyburide, compared with insulin, and that observational studies have shown higher rates of preeclampsia, hyperbilirubinemia, and stillbirth with the use of glyburide, compared with insulin. However, many other outcomes have not been statistically significantly different, according to the practice bulletin.
Additionally, at least 4%-16% of women eventually require the addition of insulin when glyburide is used as initial treatment, as do 26%-46% of women who take metformin, according to ACOG.
Regarding placental transfer, ACOG’s bulletin said that while one study that analyzed umbilical cord blood revealed no detectable glyburide in exposed pregnancies, another study demonstrated that glyburide does cross the placenta. Metformin has also been found to cross the placenta, with the fetus exposed to concentrations similar to maternal levels, the bulletin noted.
“Although current data demonstrate no adverse short-term effects on maternal or neonatal health from oral diabetic therapy during pregnancy, long-term outcomes are not yet available,” ACOG wrote in the practice bulletin.
Concerns about research
As Thomas Moore, MD, sees it, the quality of available data is insufficient to recommend insulin over oral agents, or one oral agent over another. “We really need to focus [the National Institutes of Health] on putting together proper studies,” he said at the meeting.
In a later interview, Dr. Moore referred to two recent Cochrane reviews. One review, published in January 2017, analyzed eight studies of oral antidiabetic therapies for GDM and concluded there was “insufficient high-quality evidence to be able to draw any meaningful conclusions as to the benefits of one oral antidiabetic pharmacological therapy over another” (Cochrane Database Syst Rev. 2017 Jan 25;1:CD011967).
The other Cochrane review, published in November 2017, concluded that insulin and oral antidiabetic agents have similar effects on key health outcomes, and that each one has minimal harms. The quality of evidence, the authors said, ranged from “very low to moderate, with downgrading decisions due to imprecision, risk of bias, and inconsistency” (Cochrane Database Syst Rev. 2017 Nov 5;11:CD012037).
Dr. Moore, professor of maternal-fetal medicine at the University of California, San Diego, cautioned against presuming that placental transfer of an antidiabetic drug is “ipso facto dangerous or terrible.” Moreover, he said that it’s not yet clear whether glyburide crosses the placenta in the first place.
Dr. Moore, Dr. Landon, and others at the meeting said they are eagerly awaiting long-term follow-up data from the Metformin in Gestational Diabetes (MiG) trial underway in Australia. The prospective randomized trial is designed to compare metformin with insulin and finished recruiting women in 2006. A recently published analysis found similar neurodevelopmental outcomes in offspring at 2 years, but it’s the longer-term data looking into early puberty that experts now want to see (Arch Dis Child Fetal Neonatal Ed. 2016 Feb 24. doi: 10.1136/archdischild-2015-309602).
In the meantime, Dr. Landon said the “short-term safety record for oral antidiabetic medications is actually pretty good.” There are studies “suggesting an increased risk for large babies with glyburide, but these are very small RCTs [randomized controlled trials],” he said in an interview.
Data from population-based studies, moreover, are “flawed in as much as we don’t know the thresholds for initiating glyburide treatment, nor do we know whether the women were really good candidates for this therapy,” Dr. Landon said. “It’s conceivable, and it’s been my experience, that glyburide has been overprescribed and inappropriately prescribed in certain women with GDM who really should receive insulin therapy.”
Whether glyburide and metformin are being prescribed for GDM in optimal doses is another growing question – one that interests Steve N. Caritis, MD. The drugs are typically prescribed to be taken twice a day every 12 hours, but he said he is finding that some patients may need more frequent, individually tailored dosing.
“We may have come to conclusions in [the studies published thus far] that may not be the correct conclusions,” Dr. Caritis, who coleads obstetric pharmacology research at the Magee-Womens Research Institute in Pittsburgh, said at the DPSG meeting. “The question is, If the dosing were appropriate, would we have the same outcomes?”
“We were asked, Are people using [oral antidiabetic medications] properly? Could the fact that glyburide may not have had the efficacy we’d hoped for [in published studies] be due to it not being used properly?” Dr. Catalano said.
Individualizing drug choice
Dosing aside, there may be populations of women who respond poorly to a medication because of the underlying pathophysiology of their GDM, said Maisa N. Feghali, MD, assistant professor of obstetrics, gynecology, and reproductive sciences at the University of Pittsburgh.
A study published in 2016 demonstrated the heterogeneity of the physiologic processes underlying hyperglycemia in 67 women with GDM. Almost one-third of women with GDM had predominant insulin secretion deficit, one-half had predominant insulin resistance, and the remaining 20% had a mixed “metabolic profile” (Diabetes Care. 2016 Jun;39[6]:1052-5).
This study prompted Dr. Feghali and her colleagues to design a pilot study aimed at testing an individualized approach that matches treatment to GDM mechanism. “We [currently] have the expectation that all glucose-lowering agents will be similarly effective despite significant variation in underlying GDM pathophysiology,” she said during a presentation at the DPSG meeting. “But I think we have a mismatch between variations in GDM and the uniformity of treatment.”
In her pilot study, women diagnosed with GDM who fail dietary control will be randomized into usual treatment or matched treatment (metformin for predominant insulin resistance, glyburide or insulin for predominant insulin secretion defects, and one of the three for combined insulin resistance and insulin secretion defects).
The MATCh-GDM study (Metabolic Analysis for Treatment Choice of GDM) is just getting underway. Patients will be monitored for consistency of GDM mechanism and glucose control, and routine clinical variables (hypertensive diseases, cesarean delivery, and birth weight) will be studied, as well as neonatal body composition, cord blood glucose, and cord blood C-peptide.
EXPERT ANALYSIS FROM DPSG-NA 2017
Don’t let GDM history limit contraception choices
WASHINGTON – Women with a history of gestational diabetes can use any contraceptive method safely, and those with uncomplicated pregestational diabetes can also consider all methods, said Anne Burke, MD, director of the family planning division at Johns Hopkins University, Baltimore.
“The real cautions, and some red lights,” apply to those with vascular sequelae, diabetes of 20 years’ duration or more, and patients with other vascular disease in addition to diabetes, she said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“The contraception options for women with diabetes aren’t necessarily terribly limited compared to the options for other women,” Dr. Burke said. “And the big take home is that, across the board, .”
The U.S. Medical Eligibility Criteria for Contraceptive Use issued by the Centers for Disease Control and Prevention assign a 1-4 rating for each method for women with certain characteristics or medical conditions. Category 1 indicates no restrictions, and category 2 means that the advantages generally outweigh theoretical or proven risks. Category 3 indicates that such risks usually outweigh the advantages, and category 4 means there is an unacceptable risk.
The assignment to category 2 instead of category 1 can reflect either limitations in the overall amount of data available or the lack of strong randomized studies “whereas the data [otherwise] seem to support safety,” Dr. Burke said. “And sometimes, it relates to most studies saying one thing and another being a little inconsistent.”
Uncomplicated pregestational diabetes
This is important to understand because all the methods for women with uncomplicated pregestational diabetes (no evidence of vascular disease or end-organ damage) are classified as category 2, except for the copper IUD and emergency contraception, which are in category 1. The document distinguishes between insulin-dependent and non–insulin-dependent diabetes, but the recommendations do not differ between the two categories, she said.
Progestin-only contraceptives appear to have little effect on short- or long-term diabetes control, hemostatic markers, or the lipid profile in women with uncomplicated diabetes. Combined hormonal contraception appears to have no effect on long-term diabetes control or progression to retinopathy; there may be changes in the lipid profile and hemostatic markers, but “mostly within normal values, and in some cases, in a favorable direction,” said Dr. Burke of the department of gynecology and obstetrics at the university.
GDM history
In women who have had gestational diabetes, all methods are in category 1 of the Medical Eligibility Criteria (MEC). While “there have been a couple of question marks” with progestin-only contraceptives and the later development of diabetes, “it seems that there’s really not an increased risk,” she said. Nor does there seem to be an increased risk of developing later diabetes with combined hormonal contraception.
In general, the data backing the MEC come from a limited number of studies, and “few that are rigorously done,” she said. “So the recommendations reflect consensus [that is] based on the best available information.”
Severe or long-standing disease
Data are especially limited for women with more severe and/or long-standing disease, as these women have been excluded from studies. There is enough knowledge, however, to make the hypoestrogenic effects of the depot medroxyprogesterone acetate (DMPA) injectable (Depo-Provera) concerning. “It has a pretty hefty dose of a particular type of progestin that significantly suppresses the hypothalamic-pituitary-ovarian axis – more than other progestin-only methods,” she said. “And we may see some unfavorable lipid changes and changes in carbohydrate metabolism.”
The effects of the DMPA injectable, which is in category 3 for these women, may persist for several months – or longer – after discontinuation, Dr. Burke said. The levonorgestrel IUD, on the other hand, has little effect on diabetes control, hemostatic markers, or lipids; it is in category 2 for these women.
A recently published database analysis found that diabetic users of the DMPA injectable had a hazard ratio for venous thromboembolism of 4.6, compared with IUD users, Dr. Burke said. The study included patients with type 1 and type 2 diabetes (Diabetes Care 2017;40:233-8).
Combined hormonal contraception is assigned to categories 3 and 4 for women with complicated or long-standing diabetes, in part because of thrombosis risk, which “as we know, is slightly elevated even for healthy women,” Dr. Burke said. “There are still quite a few methods that are safe to use without reservation, so here is where we start to move away from combined hormonal methods.”
In addition to the Medical Eligibility Criteria, the CDC has another document, the U.S. Selected Practice Recommendations for Contraceptive Use, also last updated in 2016, which offers “helpful” advice on precontraception tests to perform, timing after pregnancy for starting contraceptive methods, and other issues, Dr. Burke said.
Dr. Burke reported receiving research funding from Bayer, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Ibis Reproductive Health.
WASHINGTON – Women with a history of gestational diabetes can use any contraceptive method safely, and those with uncomplicated pregestational diabetes can also consider all methods, said Anne Burke, MD, director of the family planning division at Johns Hopkins University, Baltimore.
“The real cautions, and some red lights,” apply to those with vascular sequelae, diabetes of 20 years’ duration or more, and patients with other vascular disease in addition to diabetes, she said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“The contraception options for women with diabetes aren’t necessarily terribly limited compared to the options for other women,” Dr. Burke said. “And the big take home is that, across the board, .”
The U.S. Medical Eligibility Criteria for Contraceptive Use issued by the Centers for Disease Control and Prevention assign a 1-4 rating for each method for women with certain characteristics or medical conditions. Category 1 indicates no restrictions, and category 2 means that the advantages generally outweigh theoretical or proven risks. Category 3 indicates that such risks usually outweigh the advantages, and category 4 means there is an unacceptable risk.
The assignment to category 2 instead of category 1 can reflect either limitations in the overall amount of data available or the lack of strong randomized studies “whereas the data [otherwise] seem to support safety,” Dr. Burke said. “And sometimes, it relates to most studies saying one thing and another being a little inconsistent.”
Uncomplicated pregestational diabetes
This is important to understand because all the methods for women with uncomplicated pregestational diabetes (no evidence of vascular disease or end-organ damage) are classified as category 2, except for the copper IUD and emergency contraception, which are in category 1. The document distinguishes between insulin-dependent and non–insulin-dependent diabetes, but the recommendations do not differ between the two categories, she said.
Progestin-only contraceptives appear to have little effect on short- or long-term diabetes control, hemostatic markers, or the lipid profile in women with uncomplicated diabetes. Combined hormonal contraception appears to have no effect on long-term diabetes control or progression to retinopathy; there may be changes in the lipid profile and hemostatic markers, but “mostly within normal values, and in some cases, in a favorable direction,” said Dr. Burke of the department of gynecology and obstetrics at the university.
GDM history
In women who have had gestational diabetes, all methods are in category 1 of the Medical Eligibility Criteria (MEC). While “there have been a couple of question marks” with progestin-only contraceptives and the later development of diabetes, “it seems that there’s really not an increased risk,” she said. Nor does there seem to be an increased risk of developing later diabetes with combined hormonal contraception.
In general, the data backing the MEC come from a limited number of studies, and “few that are rigorously done,” she said. “So the recommendations reflect consensus [that is] based on the best available information.”
Severe or long-standing disease
Data are especially limited for women with more severe and/or long-standing disease, as these women have been excluded from studies. There is enough knowledge, however, to make the hypoestrogenic effects of the depot medroxyprogesterone acetate (DMPA) injectable (Depo-Provera) concerning. “It has a pretty hefty dose of a particular type of progestin that significantly suppresses the hypothalamic-pituitary-ovarian axis – more than other progestin-only methods,” she said. “And we may see some unfavorable lipid changes and changes in carbohydrate metabolism.”
The effects of the DMPA injectable, which is in category 3 for these women, may persist for several months – or longer – after discontinuation, Dr. Burke said. The levonorgestrel IUD, on the other hand, has little effect on diabetes control, hemostatic markers, or lipids; it is in category 2 for these women.
A recently published database analysis found that diabetic users of the DMPA injectable had a hazard ratio for venous thromboembolism of 4.6, compared with IUD users, Dr. Burke said. The study included patients with type 1 and type 2 diabetes (Diabetes Care 2017;40:233-8).
Combined hormonal contraception is assigned to categories 3 and 4 for women with complicated or long-standing diabetes, in part because of thrombosis risk, which “as we know, is slightly elevated even for healthy women,” Dr. Burke said. “There are still quite a few methods that are safe to use without reservation, so here is where we start to move away from combined hormonal methods.”
In addition to the Medical Eligibility Criteria, the CDC has another document, the U.S. Selected Practice Recommendations for Contraceptive Use, also last updated in 2016, which offers “helpful” advice on precontraception tests to perform, timing after pregnancy for starting contraceptive methods, and other issues, Dr. Burke said.
Dr. Burke reported receiving research funding from Bayer, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Ibis Reproductive Health.
WASHINGTON – Women with a history of gestational diabetes can use any contraceptive method safely, and those with uncomplicated pregestational diabetes can also consider all methods, said Anne Burke, MD, director of the family planning division at Johns Hopkins University, Baltimore.
“The real cautions, and some red lights,” apply to those with vascular sequelae, diabetes of 20 years’ duration or more, and patients with other vascular disease in addition to diabetes, she said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“The contraception options for women with diabetes aren’t necessarily terribly limited compared to the options for other women,” Dr. Burke said. “And the big take home is that, across the board, .”
The U.S. Medical Eligibility Criteria for Contraceptive Use issued by the Centers for Disease Control and Prevention assign a 1-4 rating for each method for women with certain characteristics or medical conditions. Category 1 indicates no restrictions, and category 2 means that the advantages generally outweigh theoretical or proven risks. Category 3 indicates that such risks usually outweigh the advantages, and category 4 means there is an unacceptable risk.
The assignment to category 2 instead of category 1 can reflect either limitations in the overall amount of data available or the lack of strong randomized studies “whereas the data [otherwise] seem to support safety,” Dr. Burke said. “And sometimes, it relates to most studies saying one thing and another being a little inconsistent.”
Uncomplicated pregestational diabetes
This is important to understand because all the methods for women with uncomplicated pregestational diabetes (no evidence of vascular disease or end-organ damage) are classified as category 2, except for the copper IUD and emergency contraception, which are in category 1. The document distinguishes between insulin-dependent and non–insulin-dependent diabetes, but the recommendations do not differ between the two categories, she said.
Progestin-only contraceptives appear to have little effect on short- or long-term diabetes control, hemostatic markers, or the lipid profile in women with uncomplicated diabetes. Combined hormonal contraception appears to have no effect on long-term diabetes control or progression to retinopathy; there may be changes in the lipid profile and hemostatic markers, but “mostly within normal values, and in some cases, in a favorable direction,” said Dr. Burke of the department of gynecology and obstetrics at the university.
GDM history
In women who have had gestational diabetes, all methods are in category 1 of the Medical Eligibility Criteria (MEC). While “there have been a couple of question marks” with progestin-only contraceptives and the later development of diabetes, “it seems that there’s really not an increased risk,” she said. Nor does there seem to be an increased risk of developing later diabetes with combined hormonal contraception.
In general, the data backing the MEC come from a limited number of studies, and “few that are rigorously done,” she said. “So the recommendations reflect consensus [that is] based on the best available information.”
Severe or long-standing disease
Data are especially limited for women with more severe and/or long-standing disease, as these women have been excluded from studies. There is enough knowledge, however, to make the hypoestrogenic effects of the depot medroxyprogesterone acetate (DMPA) injectable (Depo-Provera) concerning. “It has a pretty hefty dose of a particular type of progestin that significantly suppresses the hypothalamic-pituitary-ovarian axis – more than other progestin-only methods,” she said. “And we may see some unfavorable lipid changes and changes in carbohydrate metabolism.”
The effects of the DMPA injectable, which is in category 3 for these women, may persist for several months – or longer – after discontinuation, Dr. Burke said. The levonorgestrel IUD, on the other hand, has little effect on diabetes control, hemostatic markers, or lipids; it is in category 2 for these women.
A recently published database analysis found that diabetic users of the DMPA injectable had a hazard ratio for venous thromboembolism of 4.6, compared with IUD users, Dr. Burke said. The study included patients with type 1 and type 2 diabetes (Diabetes Care 2017;40:233-8).
Combined hormonal contraception is assigned to categories 3 and 4 for women with complicated or long-standing diabetes, in part because of thrombosis risk, which “as we know, is slightly elevated even for healthy women,” Dr. Burke said. “There are still quite a few methods that are safe to use without reservation, so here is where we start to move away from combined hormonal methods.”
In addition to the Medical Eligibility Criteria, the CDC has another document, the U.S. Selected Practice Recommendations for Contraceptive Use, also last updated in 2016, which offers “helpful” advice on precontraception tests to perform, timing after pregnancy for starting contraceptive methods, and other issues, Dr. Burke said.
Dr. Burke reported receiving research funding from Bayer, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and Ibis Reproductive Health.
EXPERT ANALYSIS FROM DPSG-NA 2017
One-step GDM diagnosis: Research moves closer
WASHINGTON – in the United States.
The American College of Obstetricians and Gynecologists now acknowledges this approach as an option, yet “tremendous controversy persists,” according to Mark Landon, MD.
“In the U.S., we continue to be the principal purveyors of a two-step method with a 100-g [oral glucose tolerance test] diagnostic approach, which is in contrast to much of the rest of the world,” he said the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“At this time, if we’re going to [turn nationally] to the one-step approach, we have to lower the cost of diagnosis and treatment, and we may need some upwards adjustments in the [International Association of Diabetes and Pregnancy Study Groups] criteria in order to achieve consensus,” said Dr. Landon, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus.
The International Association of Diabetes in Pregnancy Study Groups (IADPSG) created a stir in the American obstetrics community when it recommended in 2010 that a universal 75-g, 2-hour oral glucose tolerance test (OGTT) be performed during pregnancy and that gestational diabetes mellitus (GDM) be diagnosed when any single measurement threshold – a fasting value of 92 mg/dL, a 1-hour value of 180 mg/dL, or a 2-hour value of 153 mg/dL – is met or exceeded (Diabetes Care 2010 Mar; 33[3]:676-82).
The consensus group made its recommendation based largely on published associations of maternal glycemia with perinatal and long-term outcomes in offspring. Chief among the studies was the landmark Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, which found continuous linear relationships between maternal glucose levels – including levels that had been viewed as normal – and adverse fetal outcomes such as high fetal birth weight, cord-blood serum C-peptide level (an index of fetal beta-cell function and fetal hyperinsulinemia), and clinical neonatal hypoglycemia. Maternal glucose tolerance was measured in the study with the 75-g 2-hour OGTT.
The IADPSG chose its cut-off points to convey an odds ratio for adverse outcomes of 1.75. But use of the criteria meant that 16%-18% of pregnant women in the United States would be identified as having GDM – a doubling, at least.
In 2013, a National Institute of Child Health and Human Development Consensus Development Conference recommended against adoption of the new criteria, citing uncertainties regarding the benefits of treating so many additional cases of GDM, as well as the costs and additional burden on patients, providers, and the health care system.
In an updated Practice Bulletin on GDM, ACOG recommends that the suggested changes be studied “before they are proposed at a national level.” But ACOG noted that “individual practices and institutions may choose to use the IADPSG’s recommendation, if appropriate, for the population they serve” (Obstet Gynecol. 2017;130[1]:e17-37).
Since the IADPSG proposal came out, Dr. Landon said, at least a half-dozen published studies have attempted to clarify the additional benefit of their proposed criteria, analyzing the risk of adverse maternal and fetal outcomes in women who are diagnosed using IADPSG criteria and not treated, versus those with a normal glucose tolerance test. In these analyses, researchers have excluded women who would also meet usual diagnostic criteria, such as the Carpenter-Coustan criteria, in order to hone in on those with the mildest levels of GDM – the new diagnoses.
Research published “in the last 5-6 years has almost exclusively shown that, in using the IADPSG criteria, and excluding other usual criteria, you see graded, increased frequencies in large babies, preeclampsia, [neonatal] hypoglycemia” and other adverse outcomes, Dr. Landon said. “I know of only one study that refutes these associations.”
A secondary analysis of HAPO study data, for instance, grouped women into three categories: those with no GDM, GDM based on traditional Carpenter-Coustan criteria, and GDM based on IADPSG criteria but not the Carpenter-Coustan thresholds. A 3-hour OGTT result was not used in this analysis since the HAPO study did not collect this.
Compared with cases with no GDM, those with GDM based on IADPSG criteria (but not the Carpenter-Coustan criteria) were nearly twice as likely to have birth weights above the 90th percentile, newborn percentage fat over the 90th percentile, and preeclampsia, for instance (Diabetes Care 2016;39[12];2204-10).
Other researchers are trying to tease apart risk levels according to thresholds that differ slightly from traditional criteria. A retrospective cohort study from Kaiser Permanente Southern California, for instance, chose two strata of women whose GDM was in the lower levels of the IADPSG-defined spectrum for glucose intolerance and found that, in those with the lesser degree of hyperglycemia, only birth weight and large-for-gestational-age was significantly greater than in women with no GDM (Obstet Gynecol. 2015;126[1]:67-73).
“This study is interesting because it raises the question of whether there might be differential treatment effects based on the level of hyperglycemia within the IADPSG category,” Dr. Landon said.
Dr. Landon served as the principal investigator of a large national, randomized controlled trial that showed a reduction in the risk of fetal overgrowth, shoulder dystocia, cesarean delivery, and hypertensive disorders in women who were treated for mild gestational diabetes (N Engl J Med. 2009;361:1339-48). But this study defined mild gestational diabetes according to the Carpenter-Coustan criteria.
“What about the women who meet the [even lower thresholds] of the IADPSG criteria? One would expect that the treatment benefit would not be as great, but will they still benefit from treatment? To date, this is simply unknown,” he said in an interview.
Research in the last 5 years has also begun to look at the financial implications of the IADPSG criteria and strategies for reducing the cost of implementation. Dr. Landon noted that investigators in Brazil, for instance, have determined that an alternative strategy of using a fasting plasma glucose value of 92 mg/gL or greater to rule in GDM, and a fasting value of 80 mg/dL or less to rule out GDM, eliminates the need for 61% of oral glucose challenges and has 96.9% sensitivity for diagnosing GDM (Diabetes Res Clin Pract. 2015 May;108[2]:288-95).
Dr. Landon reported having no relevant financial disclosures.
WASHINGTON – in the United States.
The American College of Obstetricians and Gynecologists now acknowledges this approach as an option, yet “tremendous controversy persists,” according to Mark Landon, MD.
“In the U.S., we continue to be the principal purveyors of a two-step method with a 100-g [oral glucose tolerance test] diagnostic approach, which is in contrast to much of the rest of the world,” he said the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“At this time, if we’re going to [turn nationally] to the one-step approach, we have to lower the cost of diagnosis and treatment, and we may need some upwards adjustments in the [International Association of Diabetes and Pregnancy Study Groups] criteria in order to achieve consensus,” said Dr. Landon, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus.
The International Association of Diabetes in Pregnancy Study Groups (IADPSG) created a stir in the American obstetrics community when it recommended in 2010 that a universal 75-g, 2-hour oral glucose tolerance test (OGTT) be performed during pregnancy and that gestational diabetes mellitus (GDM) be diagnosed when any single measurement threshold – a fasting value of 92 mg/dL, a 1-hour value of 180 mg/dL, or a 2-hour value of 153 mg/dL – is met or exceeded (Diabetes Care 2010 Mar; 33[3]:676-82).
The consensus group made its recommendation based largely on published associations of maternal glycemia with perinatal and long-term outcomes in offspring. Chief among the studies was the landmark Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, which found continuous linear relationships between maternal glucose levels – including levels that had been viewed as normal – and adverse fetal outcomes such as high fetal birth weight, cord-blood serum C-peptide level (an index of fetal beta-cell function and fetal hyperinsulinemia), and clinical neonatal hypoglycemia. Maternal glucose tolerance was measured in the study with the 75-g 2-hour OGTT.
The IADPSG chose its cut-off points to convey an odds ratio for adverse outcomes of 1.75. But use of the criteria meant that 16%-18% of pregnant women in the United States would be identified as having GDM – a doubling, at least.
In 2013, a National Institute of Child Health and Human Development Consensus Development Conference recommended against adoption of the new criteria, citing uncertainties regarding the benefits of treating so many additional cases of GDM, as well as the costs and additional burden on patients, providers, and the health care system.
In an updated Practice Bulletin on GDM, ACOG recommends that the suggested changes be studied “before they are proposed at a national level.” But ACOG noted that “individual practices and institutions may choose to use the IADPSG’s recommendation, if appropriate, for the population they serve” (Obstet Gynecol. 2017;130[1]:e17-37).
Since the IADPSG proposal came out, Dr. Landon said, at least a half-dozen published studies have attempted to clarify the additional benefit of their proposed criteria, analyzing the risk of adverse maternal and fetal outcomes in women who are diagnosed using IADPSG criteria and not treated, versus those with a normal glucose tolerance test. In these analyses, researchers have excluded women who would also meet usual diagnostic criteria, such as the Carpenter-Coustan criteria, in order to hone in on those with the mildest levels of GDM – the new diagnoses.
Research published “in the last 5-6 years has almost exclusively shown that, in using the IADPSG criteria, and excluding other usual criteria, you see graded, increased frequencies in large babies, preeclampsia, [neonatal] hypoglycemia” and other adverse outcomes, Dr. Landon said. “I know of only one study that refutes these associations.”
A secondary analysis of HAPO study data, for instance, grouped women into three categories: those with no GDM, GDM based on traditional Carpenter-Coustan criteria, and GDM based on IADPSG criteria but not the Carpenter-Coustan thresholds. A 3-hour OGTT result was not used in this analysis since the HAPO study did not collect this.
Compared with cases with no GDM, those with GDM based on IADPSG criteria (but not the Carpenter-Coustan criteria) were nearly twice as likely to have birth weights above the 90th percentile, newborn percentage fat over the 90th percentile, and preeclampsia, for instance (Diabetes Care 2016;39[12];2204-10).
Other researchers are trying to tease apart risk levels according to thresholds that differ slightly from traditional criteria. A retrospective cohort study from Kaiser Permanente Southern California, for instance, chose two strata of women whose GDM was in the lower levels of the IADPSG-defined spectrum for glucose intolerance and found that, in those with the lesser degree of hyperglycemia, only birth weight and large-for-gestational-age was significantly greater than in women with no GDM (Obstet Gynecol. 2015;126[1]:67-73).
“This study is interesting because it raises the question of whether there might be differential treatment effects based on the level of hyperglycemia within the IADPSG category,” Dr. Landon said.
Dr. Landon served as the principal investigator of a large national, randomized controlled trial that showed a reduction in the risk of fetal overgrowth, shoulder dystocia, cesarean delivery, and hypertensive disorders in women who were treated for mild gestational diabetes (N Engl J Med. 2009;361:1339-48). But this study defined mild gestational diabetes according to the Carpenter-Coustan criteria.
“What about the women who meet the [even lower thresholds] of the IADPSG criteria? One would expect that the treatment benefit would not be as great, but will they still benefit from treatment? To date, this is simply unknown,” he said in an interview.
Research in the last 5 years has also begun to look at the financial implications of the IADPSG criteria and strategies for reducing the cost of implementation. Dr. Landon noted that investigators in Brazil, for instance, have determined that an alternative strategy of using a fasting plasma glucose value of 92 mg/gL or greater to rule in GDM, and a fasting value of 80 mg/dL or less to rule out GDM, eliminates the need for 61% of oral glucose challenges and has 96.9% sensitivity for diagnosing GDM (Diabetes Res Clin Pract. 2015 May;108[2]:288-95).
Dr. Landon reported having no relevant financial disclosures.
WASHINGTON – in the United States.
The American College of Obstetricians and Gynecologists now acknowledges this approach as an option, yet “tremendous controversy persists,” according to Mark Landon, MD.
“In the U.S., we continue to be the principal purveyors of a two-step method with a 100-g [oral glucose tolerance test] diagnostic approach, which is in contrast to much of the rest of the world,” he said the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“At this time, if we’re going to [turn nationally] to the one-step approach, we have to lower the cost of diagnosis and treatment, and we may need some upwards adjustments in the [International Association of Diabetes and Pregnancy Study Groups] criteria in order to achieve consensus,” said Dr. Landon, professor and chair of the department of obstetrics and gynecology at Ohio State University, Columbus.
The International Association of Diabetes in Pregnancy Study Groups (IADPSG) created a stir in the American obstetrics community when it recommended in 2010 that a universal 75-g, 2-hour oral glucose tolerance test (OGTT) be performed during pregnancy and that gestational diabetes mellitus (GDM) be diagnosed when any single measurement threshold – a fasting value of 92 mg/dL, a 1-hour value of 180 mg/dL, or a 2-hour value of 153 mg/dL – is met or exceeded (Diabetes Care 2010 Mar; 33[3]:676-82).
The consensus group made its recommendation based largely on published associations of maternal glycemia with perinatal and long-term outcomes in offspring. Chief among the studies was the landmark Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study, which found continuous linear relationships between maternal glucose levels – including levels that had been viewed as normal – and adverse fetal outcomes such as high fetal birth weight, cord-blood serum C-peptide level (an index of fetal beta-cell function and fetal hyperinsulinemia), and clinical neonatal hypoglycemia. Maternal glucose tolerance was measured in the study with the 75-g 2-hour OGTT.
The IADPSG chose its cut-off points to convey an odds ratio for adverse outcomes of 1.75. But use of the criteria meant that 16%-18% of pregnant women in the United States would be identified as having GDM – a doubling, at least.
In 2013, a National Institute of Child Health and Human Development Consensus Development Conference recommended against adoption of the new criteria, citing uncertainties regarding the benefits of treating so many additional cases of GDM, as well as the costs and additional burden on patients, providers, and the health care system.
In an updated Practice Bulletin on GDM, ACOG recommends that the suggested changes be studied “before they are proposed at a national level.” But ACOG noted that “individual practices and institutions may choose to use the IADPSG’s recommendation, if appropriate, for the population they serve” (Obstet Gynecol. 2017;130[1]:e17-37).
Since the IADPSG proposal came out, Dr. Landon said, at least a half-dozen published studies have attempted to clarify the additional benefit of their proposed criteria, analyzing the risk of adverse maternal and fetal outcomes in women who are diagnosed using IADPSG criteria and not treated, versus those with a normal glucose tolerance test. In these analyses, researchers have excluded women who would also meet usual diagnostic criteria, such as the Carpenter-Coustan criteria, in order to hone in on those with the mildest levels of GDM – the new diagnoses.
Research published “in the last 5-6 years has almost exclusively shown that, in using the IADPSG criteria, and excluding other usual criteria, you see graded, increased frequencies in large babies, preeclampsia, [neonatal] hypoglycemia” and other adverse outcomes, Dr. Landon said. “I know of only one study that refutes these associations.”
A secondary analysis of HAPO study data, for instance, grouped women into three categories: those with no GDM, GDM based on traditional Carpenter-Coustan criteria, and GDM based on IADPSG criteria but not the Carpenter-Coustan thresholds. A 3-hour OGTT result was not used in this analysis since the HAPO study did not collect this.
Compared with cases with no GDM, those with GDM based on IADPSG criteria (but not the Carpenter-Coustan criteria) were nearly twice as likely to have birth weights above the 90th percentile, newborn percentage fat over the 90th percentile, and preeclampsia, for instance (Diabetes Care 2016;39[12];2204-10).
Other researchers are trying to tease apart risk levels according to thresholds that differ slightly from traditional criteria. A retrospective cohort study from Kaiser Permanente Southern California, for instance, chose two strata of women whose GDM was in the lower levels of the IADPSG-defined spectrum for glucose intolerance and found that, in those with the lesser degree of hyperglycemia, only birth weight and large-for-gestational-age was significantly greater than in women with no GDM (Obstet Gynecol. 2015;126[1]:67-73).
“This study is interesting because it raises the question of whether there might be differential treatment effects based on the level of hyperglycemia within the IADPSG category,” Dr. Landon said.
Dr. Landon served as the principal investigator of a large national, randomized controlled trial that showed a reduction in the risk of fetal overgrowth, shoulder dystocia, cesarean delivery, and hypertensive disorders in women who were treated for mild gestational diabetes (N Engl J Med. 2009;361:1339-48). But this study defined mild gestational diabetes according to the Carpenter-Coustan criteria.
“What about the women who meet the [even lower thresholds] of the IADPSG criteria? One would expect that the treatment benefit would not be as great, but will they still benefit from treatment? To date, this is simply unknown,” he said in an interview.
Research in the last 5 years has also begun to look at the financial implications of the IADPSG criteria and strategies for reducing the cost of implementation. Dr. Landon noted that investigators in Brazil, for instance, have determined that an alternative strategy of using a fasting plasma glucose value of 92 mg/gL or greater to rule in GDM, and a fasting value of 80 mg/dL or less to rule out GDM, eliminates the need for 61% of oral glucose challenges and has 96.9% sensitivity for diagnosing GDM (Diabetes Res Clin Pract. 2015 May;108[2]:288-95).
Dr. Landon reported having no relevant financial disclosures.
EXPERT ANALYSIS FROM DPSG-NA 2017
The race is on for a Zika vaccine
WASHINGTON – A DNA vaccine developed at the National Institute of Allergy and Infectious Diseases Vaccine Research Center – one of five National Institutes of Health Zika vaccine candidates – has entered phase 2 testing in a trial underway in Brazil, Peru, Ecuador, Mexico, and Texas.
“The DNA vaccine is a simple 21st century way of developing vaccines that I think will become one of the major [methods of the future] for emerging infections, as opposed to growing a virus and inactivating or attenuating it,” Anthony S. Fauci, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America. With Zika “this is the vaccine that is ahead of all the others.”

Will it be possible to test efficacy, given the declining prevalence of Zika across the Americas, and will it be too late to prevent more disease? Dr. Fauci, director of NIAID, said that’s a concern, and that an accelerated approval based on a bridging of animal efficacy data with human safety and immunogenicity data might be possible.
The Southern hemisphere is “entering their summer, so it’s conceivable there will be an uptick in Zika. … We’ll just need to wait and see,” he said.
Sexual transmission
The Zika virus is part of a “long line of arboviruses that have threatened us in the Americas,” but infection with the organism is “the first – and may be the only – arthropod-borne or mosquito-borne infection that is also sexually transmitted,” Dr. Fauci said.
Sexual contact as an important mode of viral transmission “has been documented very clearly through a number of studies in which individuals clearly had no exposure to mosquitoes but were in fact a sexual partner of someone who got infected,” he said. And recent research suggests that the “female reproductive tract is a preferentially permissive site for Zika replication, which adds to the concern about sexual transmission.”
He cited a study published in July 2017 in PLOS Pathogens in which the Zika virus was found to preferentially replicate in the reproductive tract of female rhesus macaques who received vaginal inoculations of the virus.
Zika virus was “detected in the reproductive tract before it was detected in plasma, and replication levels in the reproductive tract did not reflect viral levels in other parts of the body,” according to the author summary. The kinetics of virus replication and dissemination after intravaginal inoculation were markedly different from what was previously seen in macaques infected with the Zika virus by subcutaneous infection, the report noted (PLOS Pathogens 13[7]:e1006537).
Dr. Fauci briefly described this and several other studies and findings that he said exemplify growing knowledge of the infection. He pointed to a prospective observational study that documents episodes of oligospermia in 15 men who presented with infection in 2016 in the French Caribbean (Lancet Infect Dis. 2017;17:1200-08).
Sperm counts fell in some of the study participants by about 50% between days 7 and 60 post infection, and the counts “recovered somewhat” by day 120. “We’re still following patients in prospective studies to determine if there’s a long-term effect in men,” he said.
In the meantime, he said, research in mice has shown that “without a doubt, Zika infection damages the testes,” Dr. Fauci said, noting that the mouse model is proving to be a good model for studying Zika’s effects. “They become oligospermic and have testicular atrophy.”
Maternal-fetal transmission
Regarding maternal-fetal transmission, there’s evidence that placental trophoblasts “are exquisitely permissive for Zika virus replication,” he said.
In another recent study, primary human placental trophoblasts from nonexposed donors were found to be infected by the Zika virus ex-vivo and permissive for viral RNA replication, compared with dengue virus, a fellow flavivirus (Sci Rep. 2017;7:41389. doi: 10.1038/srep41389).
However, Yoel Sadovsky, MD, who also presented at the meeting, explained that his lab’s ex-vivo studies show that primary human trophoblasts have inherent resistance to a number of viruses – and that trophoblasts are refractory to direct infection with the Zika virus. “We don’t think the trophoblasts are very permissive at all,” he said.
Moreover, trophoblasts appear to confer their antiviral effects to other nontrophoblast cells by releasing a particular type of interferon – type III interferon IFN1 – and by delivering certain micro-RNAs (C19MC miRNAs) that are packaged within trophoblast-derived nanovesicles called exosomes, said Dr. Sadovsky, scientific director of the Magee-Womens Research Institute and professor of ob.gyn., reproductive sciences, microbiology, and molecular genetics at the University of Pittsburgh.
WASHINGTON – A DNA vaccine developed at the National Institute of Allergy and Infectious Diseases Vaccine Research Center – one of five National Institutes of Health Zika vaccine candidates – has entered phase 2 testing in a trial underway in Brazil, Peru, Ecuador, Mexico, and Texas.
“The DNA vaccine is a simple 21st century way of developing vaccines that I think will become one of the major [methods of the future] for emerging infections, as opposed to growing a virus and inactivating or attenuating it,” Anthony S. Fauci, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America. With Zika “this is the vaccine that is ahead of all the others.”
Will it be possible to test efficacy, given the declining prevalence of Zika across the Americas, and will it be too late to prevent more disease? Dr. Fauci, director of NIAID, said that’s a concern, and that an accelerated approval based on a bridging of animal efficacy data with human safety and immunogenicity data might be possible.
The Southern hemisphere is “entering their summer, so it’s conceivable there will be an uptick in Zika. … We’ll just need to wait and see,” he said.
Sexual transmission
The Zika virus is part of a “long line of arboviruses that have threatened us in the Americas,” but infection with the organism is “the first – and may be the only – arthropod-borne or mosquito-borne infection that is also sexually transmitted,” Dr. Fauci said.
Sexual contact as an important mode of viral transmission “has been documented very clearly through a number of studies in which individuals clearly had no exposure to mosquitoes but were in fact a sexual partner of someone who got infected,” he said. And recent research suggests that the “female reproductive tract is a preferentially permissive site for Zika replication, which adds to the concern about sexual transmission.”
He cited a study published in July 2017 in PLOS Pathogens in which the Zika virus was found to preferentially replicate in the reproductive tract of female rhesus macaques who received vaginal inoculations of the virus.
Zika virus was “detected in the reproductive tract before it was detected in plasma, and replication levels in the reproductive tract did not reflect viral levels in other parts of the body,” according to the author summary. The kinetics of virus replication and dissemination after intravaginal inoculation were markedly different from what was previously seen in macaques infected with the Zika virus by subcutaneous infection, the report noted (PLOS Pathogens 13[7]:e1006537).
Dr. Fauci briefly described this and several other studies and findings that he said exemplify growing knowledge of the infection. He pointed to a prospective observational study that documents episodes of oligospermia in 15 men who presented with infection in 2016 in the French Caribbean (Lancet Infect Dis. 2017;17:1200-08).
Sperm counts fell in some of the study participants by about 50% between days 7 and 60 post infection, and the counts “recovered somewhat” by day 120. “We’re still following patients in prospective studies to determine if there’s a long-term effect in men,” he said.
In the meantime, he said, research in mice has shown that “without a doubt, Zika infection damages the testes,” Dr. Fauci said, noting that the mouse model is proving to be a good model for studying Zika’s effects. “They become oligospermic and have testicular atrophy.”
Maternal-fetal transmission
Regarding maternal-fetal transmission, there’s evidence that placental trophoblasts “are exquisitely permissive for Zika virus replication,” he said.
In another recent study, primary human placental trophoblasts from nonexposed donors were found to be infected by the Zika virus ex-vivo and permissive for viral RNA replication, compared with dengue virus, a fellow flavivirus (Sci Rep. 2017;7:41389. doi: 10.1038/srep41389).
However, Yoel Sadovsky, MD, who also presented at the meeting, explained that his lab’s ex-vivo studies show that primary human trophoblasts have inherent resistance to a number of viruses – and that trophoblasts are refractory to direct infection with the Zika virus. “We don’t think the trophoblasts are very permissive at all,” he said.
Moreover, trophoblasts appear to confer their antiviral effects to other nontrophoblast cells by releasing a particular type of interferon – type III interferon IFN1 – and by delivering certain micro-RNAs (C19MC miRNAs) that are packaged within trophoblast-derived nanovesicles called exosomes, said Dr. Sadovsky, scientific director of the Magee-Womens Research Institute and professor of ob.gyn., reproductive sciences, microbiology, and molecular genetics at the University of Pittsburgh.
WASHINGTON – A DNA vaccine developed at the National Institute of Allergy and Infectious Diseases Vaccine Research Center – one of five National Institutes of Health Zika vaccine candidates – has entered phase 2 testing in a trial underway in Brazil, Peru, Ecuador, Mexico, and Texas.
“The DNA vaccine is a simple 21st century way of developing vaccines that I think will become one of the major [methods of the future] for emerging infections, as opposed to growing a virus and inactivating or attenuating it,” Anthony S. Fauci, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America. With Zika “this is the vaccine that is ahead of all the others.”
Will it be possible to test efficacy, given the declining prevalence of Zika across the Americas, and will it be too late to prevent more disease? Dr. Fauci, director of NIAID, said that’s a concern, and that an accelerated approval based on a bridging of animal efficacy data with human safety and immunogenicity data might be possible.
The Southern hemisphere is “entering their summer, so it’s conceivable there will be an uptick in Zika. … We’ll just need to wait and see,” he said.
Sexual transmission
The Zika virus is part of a “long line of arboviruses that have threatened us in the Americas,” but infection with the organism is “the first – and may be the only – arthropod-borne or mosquito-borne infection that is also sexually transmitted,” Dr. Fauci said.
Sexual contact as an important mode of viral transmission “has been documented very clearly through a number of studies in which individuals clearly had no exposure to mosquitoes but were in fact a sexual partner of someone who got infected,” he said. And recent research suggests that the “female reproductive tract is a preferentially permissive site for Zika replication, which adds to the concern about sexual transmission.”
He cited a study published in July 2017 in PLOS Pathogens in which the Zika virus was found to preferentially replicate in the reproductive tract of female rhesus macaques who received vaginal inoculations of the virus.
Zika virus was “detected in the reproductive tract before it was detected in plasma, and replication levels in the reproductive tract did not reflect viral levels in other parts of the body,” according to the author summary. The kinetics of virus replication and dissemination after intravaginal inoculation were markedly different from what was previously seen in macaques infected with the Zika virus by subcutaneous infection, the report noted (PLOS Pathogens 13[7]:e1006537).
Dr. Fauci briefly described this and several other studies and findings that he said exemplify growing knowledge of the infection. He pointed to a prospective observational study that documents episodes of oligospermia in 15 men who presented with infection in 2016 in the French Caribbean (Lancet Infect Dis. 2017;17:1200-08).
Sperm counts fell in some of the study participants by about 50% between days 7 and 60 post infection, and the counts “recovered somewhat” by day 120. “We’re still following patients in prospective studies to determine if there’s a long-term effect in men,” he said.
In the meantime, he said, research in mice has shown that “without a doubt, Zika infection damages the testes,” Dr. Fauci said, noting that the mouse model is proving to be a good model for studying Zika’s effects. “They become oligospermic and have testicular atrophy.”
Maternal-fetal transmission
Regarding maternal-fetal transmission, there’s evidence that placental trophoblasts “are exquisitely permissive for Zika virus replication,” he said.
In another recent study, primary human placental trophoblasts from nonexposed donors were found to be infected by the Zika virus ex-vivo and permissive for viral RNA replication, compared with dengue virus, a fellow flavivirus (Sci Rep. 2017;7:41389. doi: 10.1038/srep41389).
However, Yoel Sadovsky, MD, who also presented at the meeting, explained that his lab’s ex-vivo studies show that primary human trophoblasts have inherent resistance to a number of viruses – and that trophoblasts are refractory to direct infection with the Zika virus. “We don’t think the trophoblasts are very permissive at all,” he said.
Moreover, trophoblasts appear to confer their antiviral effects to other nontrophoblast cells by releasing a particular type of interferon – type III interferon IFN1 – and by delivering certain micro-RNAs (C19MC miRNAs) that are packaged within trophoblast-derived nanovesicles called exosomes, said Dr. Sadovsky, scientific director of the Magee-Womens Research Institute and professor of ob.gyn., reproductive sciences, microbiology, and molecular genetics at the University of Pittsburgh.
AT DPSG-NA 2017