User login
An unconventional approach to chest wall pain
THE CASE
A 45-year-old airman presented to our medical group with acute onset of sharp, positional left lateral chest wall pain that he’d had for 2 days. The pain began after an extreme core body workout. Treatment with ibuprofen 800 mg and local electrical stimulation one day prior provided no benefit. The patient reported the pain to be a 6 out of 10 when still and a 9 to 10 when sitting for more than a few minutes, turning, or taking a medium to deep breath. The patient felt “dangerously distracted by the pain” while driving in for his appointment.
We noted focal left lower lateral intercostal muscle tenderness without trigger point-like thickness or spasm. The patient also had restricted inspiration, secondary to the severe pain, and decreased left lower field breath sounds. His vital signs were normal, as was his cardiac exam.
THE DIAGNOSIS
While awaiting a chest x-ray, the patient was offered and opted to try acupuncture for pain relief. (We have medical acupuncturists on staff.) Analgesics had already been used, but had provided little relief.
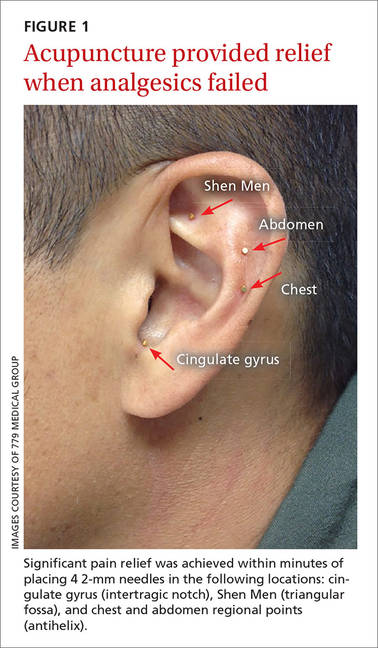
We identified 4 acupuncture sites in the ear: 2 were battlefield acupuncture (BFA) points (more on this in a bit) and 2 points were deemed active by a skin conductance point finder (a handheld device that assesses changes in electrical skin resistance at auricular acupuncture points). The left ear points that were treated included the cingulate gyrus (intertragic notch), Shen Men (triangular fossa), and chest and abdomen regional points (antihelix) (FIGURE 1).
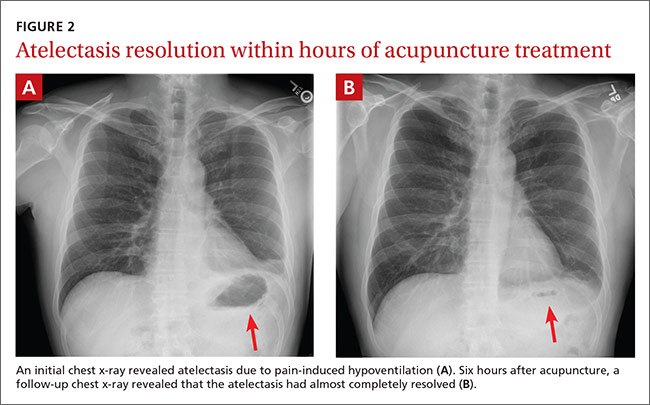
Within 15 minutes, the patient reported significant pain relief and was able to inspire deeply without pain. The patient also underwent a chest x-ray, which revealed atelectasis of the left lower lobe (FIGURE 2A) caused by pain-induced hypoventilation.
Because the patient’s pain was so well controlled, he returned to work immediately after the appointment. At the end of his shift 6 hours later he returned, unscheduled, to report pain at a level of one out of 10 and said he was able to breathe normally. In addition, lung auscultation was normal and a repeat chest x-ray revealed that the atelectasis had almost completely resolved (FIGURE 2B). This occurred without medication or other therapy. The pain did not return.
DISCUSSION
Although acupuncture is over 2000 years old, it has been largely disregarded in the United States due to a lack of mainstream evidence supporting its efficacy. Research is hindered by significant variation in approach between providers, the difficulties inherent to blinding patients and providers to treatment vs placebo, and poor insurance coverage and reimbursement.
Acupuncture research is burgeoning. A 2012 meta-analysis concluded that patients receiving acupuncture had less pain than those receiving sham or no acupuncture for several pain conditions. Specifically, scores for back and neck pain, osteoarthritis, and chronic headache were 0.23, 0.16, and 0.15 standard deviations (SDs), respectively, lower for patients receiving acupuncture than for those who got sham acupuncture. The effect sizes for acupuncture patients compared to no acupuncture controls were 0.55, 0.57, and 0.42 respectively (all P<.001).1
Several theories explain how auricular acupuncture may work. Paul Nogier, MD, noted that the ear is composed of ectodermal, mesodermal, and endodermal tissues, and mapped the “inverted fetus” homunculus in the ear, which corresponds to specific body points.2 Functional magnetic resonance imaging has demonstrated increased brain activity in the cingulate gyrus and thalamic regions in response to a painful stimulus, as well as attenuation of this activity after the placement of needles in corresponding auricular cingulate gyrus and thalamus points.3 In addition, research has confirmed that acupuncture raises serum and cerebrospinal levels of endorphins and enkephalins.4
Battlefield acupuncture (BFA) was developed by Richard Niemtzow, MD, and has been used for acute injuries in the front lines of battle as well as for many health conditions. BFA treats pain using a sequence of 5 predetermined auricular acupuncture points.5 Onset and duration of pain relief vary depending on the location and nature of the pathology. We’ve noted that BFA for chronic pain has a shorter duration of benefit and is more likely to need to be repeated.
One randomized pilot study involving 87 patients presenting to the emergency room blinded emergency health care providers to the inclusion of the first 2 BFA points in their otherwise usual care of acute pain patients. Participants in the acupuncture group experienced a 23% reduction in pain before discharge compared to no change in the standard care group (P<.0005).6
Our patient. We inserted semi-permanent needles with a needle length of 2 mm into 4 locations on the ear. (These needles can remain in the ear for several days and fall out on their own or they may be removed by pulling the stud ends.) As noted earlier, our patient reported pain relief within 15 minutes and was pain free by the next day.
THE TAKEAWAY
Auricular acupuncture can treat acute and chronic pain. As proof, the BFA technique is widely used by health care providers throughout the US military and Department of Veterans Affairs. In this case, the immediate pain relief and x-ray documentation of atelectasis resolution within 6 hours of treatment provide support that auricular acupuncture was beneficial in reversing the cause of this atelectasis, which was pain-induced hypoventilation.
While the acute pain control observed with this patient is not unusual in our experience, what is unusual is the rare visual confirmation of the striking degree of pain reduction possible with auricular acupuncture.
1. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
2. Oleson T. Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture. 4th ed. Los Angeles: Churchill Livingstone; 2014.
3. Sjölund B, Eriksson M. Electro-acupunture and endogenous morphines. Lancet. 1976;2:1085.
4. Cho ZH, Chung SC, Jones JP, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Natl Acad Sci U S A. 1998;95:2670-2673.
5. Niemtzow RC. Battlefield acupuncture: Update. Medical Acupuncture. 2007;19:225-228.
6.Goertz CM, Niemtzow R, Burns SM, et al. Auricular acupuncture in the treatment of acute pain syndromes: A pilot study. Mil Med. 2006;171:1010-1014.
THE CASE
A 45-year-old airman presented to our medical group with acute onset of sharp, positional left lateral chest wall pain that he’d had for 2 days. The pain began after an extreme core body workout. Treatment with ibuprofen 800 mg and local electrical stimulation one day prior provided no benefit. The patient reported the pain to be a 6 out of 10 when still and a 9 to 10 when sitting for more than a few minutes, turning, or taking a medium to deep breath. The patient felt “dangerously distracted by the pain” while driving in for his appointment.
We noted focal left lower lateral intercostal muscle tenderness without trigger point-like thickness or spasm. The patient also had restricted inspiration, secondary to the severe pain, and decreased left lower field breath sounds. His vital signs were normal, as was his cardiac exam.
THE DIAGNOSIS
While awaiting a chest x-ray, the patient was offered and opted to try acupuncture for pain relief. (We have medical acupuncturists on staff.) Analgesics had already been used, but had provided little relief.
We identified 4 acupuncture sites in the ear: 2 were battlefield acupuncture (BFA) points (more on this in a bit) and 2 points were deemed active by a skin conductance point finder (a handheld device that assesses changes in electrical skin resistance at auricular acupuncture points). The left ear points that were treated included the cingulate gyrus (intertragic notch), Shen Men (triangular fossa), and chest and abdomen regional points (antihelix) (FIGURE 1).
Within 15 minutes, the patient reported significant pain relief and was able to inspire deeply without pain. The patient also underwent a chest x-ray, which revealed atelectasis of the left lower lobe (FIGURE 2A) caused by pain-induced hypoventilation.
Because the patient’s pain was so well controlled, he returned to work immediately after the appointment. At the end of his shift 6 hours later he returned, unscheduled, to report pain at a level of one out of 10 and said he was able to breathe normally. In addition, lung auscultation was normal and a repeat chest x-ray revealed that the atelectasis had almost completely resolved (FIGURE 2B). This occurred without medication or other therapy. The pain did not return.
DISCUSSION
Although acupuncture is over 2000 years old, it has been largely disregarded in the United States due to a lack of mainstream evidence supporting its efficacy. Research is hindered by significant variation in approach between providers, the difficulties inherent to blinding patients and providers to treatment vs placebo, and poor insurance coverage and reimbursement.
Acupuncture research is burgeoning. A 2012 meta-analysis concluded that patients receiving acupuncture had less pain than those receiving sham or no acupuncture for several pain conditions. Specifically, scores for back and neck pain, osteoarthritis, and chronic headache were 0.23, 0.16, and 0.15 standard deviations (SDs), respectively, lower for patients receiving acupuncture than for those who got sham acupuncture. The effect sizes for acupuncture patients compared to no acupuncture controls were 0.55, 0.57, and 0.42 respectively (all P<.001).1
Several theories explain how auricular acupuncture may work. Paul Nogier, MD, noted that the ear is composed of ectodermal, mesodermal, and endodermal tissues, and mapped the “inverted fetus” homunculus in the ear, which corresponds to specific body points.2 Functional magnetic resonance imaging has demonstrated increased brain activity in the cingulate gyrus and thalamic regions in response to a painful stimulus, as well as attenuation of this activity after the placement of needles in corresponding auricular cingulate gyrus and thalamus points.3 In addition, research has confirmed that acupuncture raises serum and cerebrospinal levels of endorphins and enkephalins.4
Battlefield acupuncture (BFA) was developed by Richard Niemtzow, MD, and has been used for acute injuries in the front lines of battle as well as for many health conditions. BFA treats pain using a sequence of 5 predetermined auricular acupuncture points.5 Onset and duration of pain relief vary depending on the location and nature of the pathology. We’ve noted that BFA for chronic pain has a shorter duration of benefit and is more likely to need to be repeated.
One randomized pilot study involving 87 patients presenting to the emergency room blinded emergency health care providers to the inclusion of the first 2 BFA points in their otherwise usual care of acute pain patients. Participants in the acupuncture group experienced a 23% reduction in pain before discharge compared to no change in the standard care group (P<.0005).6
Our patient. We inserted semi-permanent needles with a needle length of 2 mm into 4 locations on the ear. (These needles can remain in the ear for several days and fall out on their own or they may be removed by pulling the stud ends.) As noted earlier, our patient reported pain relief within 15 minutes and was pain free by the next day.
THE TAKEAWAY
Auricular acupuncture can treat acute and chronic pain. As proof, the BFA technique is widely used by health care providers throughout the US military and Department of Veterans Affairs. In this case, the immediate pain relief and x-ray documentation of atelectasis resolution within 6 hours of treatment provide support that auricular acupuncture was beneficial in reversing the cause of this atelectasis, which was pain-induced hypoventilation.
While the acute pain control observed with this patient is not unusual in our experience, what is unusual is the rare visual confirmation of the striking degree of pain reduction possible with auricular acupuncture.
THE CASE
A 45-year-old airman presented to our medical group with acute onset of sharp, positional left lateral chest wall pain that he’d had for 2 days. The pain began after an extreme core body workout. Treatment with ibuprofen 800 mg and local electrical stimulation one day prior provided no benefit. The patient reported the pain to be a 6 out of 10 when still and a 9 to 10 when sitting for more than a few minutes, turning, or taking a medium to deep breath. The patient felt “dangerously distracted by the pain” while driving in for his appointment.
We noted focal left lower lateral intercostal muscle tenderness without trigger point-like thickness or spasm. The patient also had restricted inspiration, secondary to the severe pain, and decreased left lower field breath sounds. His vital signs were normal, as was his cardiac exam.
THE DIAGNOSIS
While awaiting a chest x-ray, the patient was offered and opted to try acupuncture for pain relief. (We have medical acupuncturists on staff.) Analgesics had already been used, but had provided little relief.
We identified 4 acupuncture sites in the ear: 2 were battlefield acupuncture (BFA) points (more on this in a bit) and 2 points were deemed active by a skin conductance point finder (a handheld device that assesses changes in electrical skin resistance at auricular acupuncture points). The left ear points that were treated included the cingulate gyrus (intertragic notch), Shen Men (triangular fossa), and chest and abdomen regional points (antihelix) (FIGURE 1).
Within 15 minutes, the patient reported significant pain relief and was able to inspire deeply without pain. The patient also underwent a chest x-ray, which revealed atelectasis of the left lower lobe (FIGURE 2A) caused by pain-induced hypoventilation.
Because the patient’s pain was so well controlled, he returned to work immediately after the appointment. At the end of his shift 6 hours later he returned, unscheduled, to report pain at a level of one out of 10 and said he was able to breathe normally. In addition, lung auscultation was normal and a repeat chest x-ray revealed that the atelectasis had almost completely resolved (FIGURE 2B). This occurred without medication or other therapy. The pain did not return.
DISCUSSION
Although acupuncture is over 2000 years old, it has been largely disregarded in the United States due to a lack of mainstream evidence supporting its efficacy. Research is hindered by significant variation in approach between providers, the difficulties inherent to blinding patients and providers to treatment vs placebo, and poor insurance coverage and reimbursement.
Acupuncture research is burgeoning. A 2012 meta-analysis concluded that patients receiving acupuncture had less pain than those receiving sham or no acupuncture for several pain conditions. Specifically, scores for back and neck pain, osteoarthritis, and chronic headache were 0.23, 0.16, and 0.15 standard deviations (SDs), respectively, lower for patients receiving acupuncture than for those who got sham acupuncture. The effect sizes for acupuncture patients compared to no acupuncture controls were 0.55, 0.57, and 0.42 respectively (all P<.001).1
Several theories explain how auricular acupuncture may work. Paul Nogier, MD, noted that the ear is composed of ectodermal, mesodermal, and endodermal tissues, and mapped the “inverted fetus” homunculus in the ear, which corresponds to specific body points.2 Functional magnetic resonance imaging has demonstrated increased brain activity in the cingulate gyrus and thalamic regions in response to a painful stimulus, as well as attenuation of this activity after the placement of needles in corresponding auricular cingulate gyrus and thalamus points.3 In addition, research has confirmed that acupuncture raises serum and cerebrospinal levels of endorphins and enkephalins.4
Battlefield acupuncture (BFA) was developed by Richard Niemtzow, MD, and has been used for acute injuries in the front lines of battle as well as for many health conditions. BFA treats pain using a sequence of 5 predetermined auricular acupuncture points.5 Onset and duration of pain relief vary depending on the location and nature of the pathology. We’ve noted that BFA for chronic pain has a shorter duration of benefit and is more likely to need to be repeated.
One randomized pilot study involving 87 patients presenting to the emergency room blinded emergency health care providers to the inclusion of the first 2 BFA points in their otherwise usual care of acute pain patients. Participants in the acupuncture group experienced a 23% reduction in pain before discharge compared to no change in the standard care group (P<.0005).6
Our patient. We inserted semi-permanent needles with a needle length of 2 mm into 4 locations on the ear. (These needles can remain in the ear for several days and fall out on their own or they may be removed by pulling the stud ends.) As noted earlier, our patient reported pain relief within 15 minutes and was pain free by the next day.
THE TAKEAWAY
Auricular acupuncture can treat acute and chronic pain. As proof, the BFA technique is widely used by health care providers throughout the US military and Department of Veterans Affairs. In this case, the immediate pain relief and x-ray documentation of atelectasis resolution within 6 hours of treatment provide support that auricular acupuncture was beneficial in reversing the cause of this atelectasis, which was pain-induced hypoventilation.
While the acute pain control observed with this patient is not unusual in our experience, what is unusual is the rare visual confirmation of the striking degree of pain reduction possible with auricular acupuncture.
1. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
2. Oleson T. Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture. 4th ed. Los Angeles: Churchill Livingstone; 2014.
3. Sjölund B, Eriksson M. Electro-acupunture and endogenous morphines. Lancet. 1976;2:1085.
4. Cho ZH, Chung SC, Jones JP, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Natl Acad Sci U S A. 1998;95:2670-2673.
5. Niemtzow RC. Battlefield acupuncture: Update. Medical Acupuncture. 2007;19:225-228.
6.Goertz CM, Niemtzow R, Burns SM, et al. Auricular acupuncture in the treatment of acute pain syndromes: A pilot study. Mil Med. 2006;171:1010-1014.
1. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
2. Oleson T. Auriculotherapy Manual: Chinese and Western Systems of Ear Acupuncture. 4th ed. Los Angeles: Churchill Livingstone; 2014.
3. Sjölund B, Eriksson M. Electro-acupunture and endogenous morphines. Lancet. 1976;2:1085.
4. Cho ZH, Chung SC, Jones JP, et al. New findings of the correlation between acupoints and corresponding brain cortices using functional MRI. Proc Natl Acad Sci U S A. 1998;95:2670-2673.
5. Niemtzow RC. Battlefield acupuncture: Update. Medical Acupuncture. 2007;19:225-228.
6.Goertz CM, Niemtzow R, Burns SM, et al. Auricular acupuncture in the treatment of acute pain syndromes: A pilot study. Mil Med. 2006;171:1010-1014.