User login
2011: Measles Cases, Outbreaks in U.S. Hit 15-Year High
The number of cases of measles reported in the United States last year was higher than any year since 1996 – an increase the Centers for Disease Control and Prevention attributes primarily to an increase in the importation of the disease from other countries and the vulnerability of susceptible, unimmunized people in the community.
A total of 222 measles cases and 17 measles outbreaks from 31 states were reported to the CDC in 2011, compared with a median of 60 cases and 4 outbreaks reported annually during 2001-2010, Dr. Anne Schuchat, director of the National Center for Immunization and Respiratory Disease’s Office of Infectious Diseases reported in a telebriefing April 19. Of the 222 cases, 200 (90%) were associated with importations from other countries, including 52 (26%) cases in U.S. residents who had recently traveled abroad and 20 (10%) in foreign visitors, she said, presenting data from the April 20 Morbidity and Mortality Weekly Report (MMWR Morb. Mortal. Wkly. Rep. 2012;61:253-7).
Of the patients who contracted the disease in 2011, 86% were either unvaccinated or had unknown vaccination status, underscoring the ongoing risk for measles among unvaccinated individuals and the importance of vaccination, despite the fact that the disease was declared to be eliminated – defined as the interruption of year-round endemic transmission – in the United States in 2000, Dr. Schuchat said.
For the purposes of the CDC report, measles outbreaks were defined as three or more cases linked in time or place, and U.S residents were classified as eligible or ineligible for measles, mumps, and rubella (MMR) vaccination according to the recommendations of the Advisory Committee on Immunization Practices, whereby vaccine-eligible patients were those who were unvaccinated or had unknown vaccination status; did not have vaccination contraindications; and were either born after 1957 and at least 12 months old without documented evidence of measles immunity or 6-11 months with a recent history of international travel, according to the report.
The median age of the infected patients was 14 years (3 months to 84 years). Of the 222, 196 were U.S. residents; of those, 166 were unvaccinated or had unknown vaccination status, 141 of whom were eligible for vaccination, 18 who were too young for vaccination, 6 who were born before 1957 and thus had presumptive immunity, and 1 with previous evidence of presumptive immunity.
Nine of the 141 unvaccinated, but vaccination-eligible patients were infants 6 to 11 months old with recent history of international travel; 14 were 12-15 months, the recommended age of the first MMR vaccine dose; and 66 were aged 16 months to 19 years, 50 of whom had not been vaccinated because of a philosophic, religious, or personal objection.
In all, 72 of the 200 importation-associated measles cases were imported from other countries, 67 were linked epidemiologically to importations, 39 had virologic evidence that suggested recent importation, and 22 were linked to cases with virologic evidence of recent importation, according to the report. Importantly, nearly half of the 72 importations occurred among individuals who contracted the disease in the European region, Dr. Schuchat said. "We don’t usually think of Europe being associated with measles, but in reality there has been a lot of measles in that region. In 2011, more than 30,000 cases were recorded in Europe, including 8 measles-related deaths. The hardest hit regions were places Americans tend to travel to, including France, Italy, and Spain."
Unvaccinated U.S. residents traveling to regions where measles are endemic put themselves and others in their communities at risk for measles and its complications, she said.
Physicians need to keep measles in mind when they encounter persons with a fever and rash, along with symptoms such as cough, coryza, or conjunctivitis, especially in persons who recently have traveled abroad or have had contact with travelers.
Despite the relatively small number of measles cases in the United States, vigilance on behalf of the public and health care providers is critical to avoid a drop in MMR vaccination coverage, which increases the risk for large, sustained measles outbreaks, according to Dr. Schuchat.
Such vigilance includes rapid public health response and high two-dose MMR vaccine coverage, she said, noting that one dose of the vaccine is recommended for all children ages 12-15 months and a second dose at 4-6 years. Further, adults without evidence of immunity should receive one vaccine dose, and unvaccinated health care personnel, international travelers, and college students should receive two doses, according to the report.
Dr. Schuchat said she had no financial conflicts of interest.
The number of cases of measles reported in the United States last year was higher than any year since 1996 – an increase the Centers for Disease Control and Prevention attributes primarily to an increase in the importation of the disease from other countries and the vulnerability of susceptible, unimmunized people in the community.
A total of 222 measles cases and 17 measles outbreaks from 31 states were reported to the CDC in 2011, compared with a median of 60 cases and 4 outbreaks reported annually during 2001-2010, Dr. Anne Schuchat, director of the National Center for Immunization and Respiratory Disease’s Office of Infectious Diseases reported in a telebriefing April 19. Of the 222 cases, 200 (90%) were associated with importations from other countries, including 52 (26%) cases in U.S. residents who had recently traveled abroad and 20 (10%) in foreign visitors, she said, presenting data from the April 20 Morbidity and Mortality Weekly Report (MMWR Morb. Mortal. Wkly. Rep. 2012;61:253-7).
Of the patients who contracted the disease in 2011, 86% were either unvaccinated or had unknown vaccination status, underscoring the ongoing risk for measles among unvaccinated individuals and the importance of vaccination, despite the fact that the disease was declared to be eliminated – defined as the interruption of year-round endemic transmission – in the United States in 2000, Dr. Schuchat said.
For the purposes of the CDC report, measles outbreaks were defined as three or more cases linked in time or place, and U.S residents were classified as eligible or ineligible for measles, mumps, and rubella (MMR) vaccination according to the recommendations of the Advisory Committee on Immunization Practices, whereby vaccine-eligible patients were those who were unvaccinated or had unknown vaccination status; did not have vaccination contraindications; and were either born after 1957 and at least 12 months old without documented evidence of measles immunity or 6-11 months with a recent history of international travel, according to the report.
The median age of the infected patients was 14 years (3 months to 84 years). Of the 222, 196 were U.S. residents; of those, 166 were unvaccinated or had unknown vaccination status, 141 of whom were eligible for vaccination, 18 who were too young for vaccination, 6 who were born before 1957 and thus had presumptive immunity, and 1 with previous evidence of presumptive immunity.
Nine of the 141 unvaccinated, but vaccination-eligible patients were infants 6 to 11 months old with recent history of international travel; 14 were 12-15 months, the recommended age of the first MMR vaccine dose; and 66 were aged 16 months to 19 years, 50 of whom had not been vaccinated because of a philosophic, religious, or personal objection.
In all, 72 of the 200 importation-associated measles cases were imported from other countries, 67 were linked epidemiologically to importations, 39 had virologic evidence that suggested recent importation, and 22 were linked to cases with virologic evidence of recent importation, according to the report. Importantly, nearly half of the 72 importations occurred among individuals who contracted the disease in the European region, Dr. Schuchat said. "We don’t usually think of Europe being associated with measles, but in reality there has been a lot of measles in that region. In 2011, more than 30,000 cases were recorded in Europe, including 8 measles-related deaths. The hardest hit regions were places Americans tend to travel to, including France, Italy, and Spain."
Unvaccinated U.S. residents traveling to regions where measles are endemic put themselves and others in their communities at risk for measles and its complications, she said.
Physicians need to keep measles in mind when they encounter persons with a fever and rash, along with symptoms such as cough, coryza, or conjunctivitis, especially in persons who recently have traveled abroad or have had contact with travelers.
Despite the relatively small number of measles cases in the United States, vigilance on behalf of the public and health care providers is critical to avoid a drop in MMR vaccination coverage, which increases the risk for large, sustained measles outbreaks, according to Dr. Schuchat.
Such vigilance includes rapid public health response and high two-dose MMR vaccine coverage, she said, noting that one dose of the vaccine is recommended for all children ages 12-15 months and a second dose at 4-6 years. Further, adults without evidence of immunity should receive one vaccine dose, and unvaccinated health care personnel, international travelers, and college students should receive two doses, according to the report.
Dr. Schuchat said she had no financial conflicts of interest.
The number of cases of measles reported in the United States last year was higher than any year since 1996 – an increase the Centers for Disease Control and Prevention attributes primarily to an increase in the importation of the disease from other countries and the vulnerability of susceptible, unimmunized people in the community.
A total of 222 measles cases and 17 measles outbreaks from 31 states were reported to the CDC in 2011, compared with a median of 60 cases and 4 outbreaks reported annually during 2001-2010, Dr. Anne Schuchat, director of the National Center for Immunization and Respiratory Disease’s Office of Infectious Diseases reported in a telebriefing April 19. Of the 222 cases, 200 (90%) were associated with importations from other countries, including 52 (26%) cases in U.S. residents who had recently traveled abroad and 20 (10%) in foreign visitors, she said, presenting data from the April 20 Morbidity and Mortality Weekly Report (MMWR Morb. Mortal. Wkly. Rep. 2012;61:253-7).
Of the patients who contracted the disease in 2011, 86% were either unvaccinated or had unknown vaccination status, underscoring the ongoing risk for measles among unvaccinated individuals and the importance of vaccination, despite the fact that the disease was declared to be eliminated – defined as the interruption of year-round endemic transmission – in the United States in 2000, Dr. Schuchat said.
For the purposes of the CDC report, measles outbreaks were defined as three or more cases linked in time or place, and U.S residents were classified as eligible or ineligible for measles, mumps, and rubella (MMR) vaccination according to the recommendations of the Advisory Committee on Immunization Practices, whereby vaccine-eligible patients were those who were unvaccinated or had unknown vaccination status; did not have vaccination contraindications; and were either born after 1957 and at least 12 months old without documented evidence of measles immunity or 6-11 months with a recent history of international travel, according to the report.
The median age of the infected patients was 14 years (3 months to 84 years). Of the 222, 196 were U.S. residents; of those, 166 were unvaccinated or had unknown vaccination status, 141 of whom were eligible for vaccination, 18 who were too young for vaccination, 6 who were born before 1957 and thus had presumptive immunity, and 1 with previous evidence of presumptive immunity.
Nine of the 141 unvaccinated, but vaccination-eligible patients were infants 6 to 11 months old with recent history of international travel; 14 were 12-15 months, the recommended age of the first MMR vaccine dose; and 66 were aged 16 months to 19 years, 50 of whom had not been vaccinated because of a philosophic, religious, or personal objection.
In all, 72 of the 200 importation-associated measles cases were imported from other countries, 67 were linked epidemiologically to importations, 39 had virologic evidence that suggested recent importation, and 22 were linked to cases with virologic evidence of recent importation, according to the report. Importantly, nearly half of the 72 importations occurred among individuals who contracted the disease in the European region, Dr. Schuchat said. "We don’t usually think of Europe being associated with measles, but in reality there has been a lot of measles in that region. In 2011, more than 30,000 cases were recorded in Europe, including 8 measles-related deaths. The hardest hit regions were places Americans tend to travel to, including France, Italy, and Spain."
Unvaccinated U.S. residents traveling to regions where measles are endemic put themselves and others in their communities at risk for measles and its complications, she said.
Physicians need to keep measles in mind when they encounter persons with a fever and rash, along with symptoms such as cough, coryza, or conjunctivitis, especially in persons who recently have traveled abroad or have had contact with travelers.
Despite the relatively small number of measles cases in the United States, vigilance on behalf of the public and health care providers is critical to avoid a drop in MMR vaccination coverage, which increases the risk for large, sustained measles outbreaks, according to Dr. Schuchat.
Such vigilance includes rapid public health response and high two-dose MMR vaccine coverage, she said, noting that one dose of the vaccine is recommended for all children ages 12-15 months and a second dose at 4-6 years. Further, adults without evidence of immunity should receive one vaccine dose, and unvaccinated health care personnel, international travelers, and college students should receive two doses, according to the report.
Dr. Schuchat said she had no financial conflicts of interest.
FROM THE CDC MORBIDITY AND MORTALITY WEEKLY REPORT
Major Finding: In 2001, 222 cases of measles and 17 outbreaks in 31 states were reported in the United States.
Data Source: Findings came from reports to the Centers for Disease Control and Prevention.
Disclosures: Dr. Schuchat said she had no financial conflicts of interest to disclose.
Cixutumumab With Temsirolimus Slows Ewing's Sarcoma
CHICAGO – Two targeted therapies may be better than one for the treatment of refractory Ewing’s sarcoma, according to findings of an early clinical trial reported at the annual meeting of the American Association for Cancer Research.
Combining the investigational agent cixutumumab with temsirolimus (Torisel) resulted in 2 complete responses and 3 partial responses in 17 adolescent and young adult patients with heavily pretreated disease in the phase I clinical trial.

Cixutumumab, a novel monoclonal antibody targeting the insulin-like growth factor 1-receptor (IGF-1R), is under investigation for various cancers. Temsirolimus, a mammalian target of rapamycin (mTOR) inhibitor, is approved for the treatment of advanced renal cell carcinomas.
The two drugs have previously been used as single treatment agents, producing mixed results, according to Dr. Aung Naing of the department of investigational cancer therapeutics at the University of Texas M.D. Anderson Cancer Center in Houston.
Based on data from preclinical studies, "we hypothesized that combining the two could help prevent drug-resistance, which is a common problem in Ewing’s sarcoma," he said in an interview. The two agents target molecular pathways associated with cell proliferation and survival, abnormal blood vessel growth, and resistance to both chemotherapy and radiation therapy, Dr. Naing explained.
To test their hypothesis, the investigators enrolled 20 patients, median age 20 years, with Ewing’s sarcoma (17) or desmoplastic small-round-cell tumors (3) in the trial. The median number of prior therapies per patient was 6. Two patients previously received temsirolimus and six previously received an IGF-1R inhibitor, he said.
All of the patients received 6 mg/kg of intravenous cixutumumab and 25-37.5mg of intravenous temsirolimus weekly for 4-week cycles, with restaging after 8 weeks, Dr. Naing reported.
At a median follow-up of 8.9 months, 7 of the 20 patients (35%) had achieved a complete or partial response or stable disease lasting more than 5 months.
In Ewing’s sarcoma patients specifically, 29% had evidence of tumor regression greater than 20%, Dr. Naing said, noting, "Two patients achieved complete responses, one of which lasted 27 months."
The most frequent, possibly drug-related toxicities included thrombocytopenia (85%), mucositis (80%), hypercholesterolemia (75%), hypertriglyceridemia (70%), and hyperglycemia (65%).
"Most were grade 1-2 [toxicities], but four of the seven best responders developed grade 3 mucositis, myelosuppression, or hyperglycemia, which were managed while maintaining drug dose," Dr. Naing stated.
"Typically, patients who develop these types of grade 3 toxicities would be removed from the study, but we were able to continue with treatment after receiving approval from the sponsor and notification from our institutional review board," he said. Because the toxicities were able to be controlled using supportive measures, "the drug dose did not have to be compromised."
One of the Ewing’s sarcoma patients had achieved a partial response with prior IGF-1R treatment. After initiating the combination therapy, this patient had a mixed response with "remarkable" regression in three lung nodules but progression in a fourth. Morphoproteomic analysis of biopsy samples from this patient demonstrated upregulation of mTOR and ERK/MEK signals, suggesting the possibility that a combination of IGFR/mTOR and MAPK/ERK kinase (MEK) inhibitors might warrant investigation in order to reverse resistance, according to Dr. Naing.
Based on the evidence of activity for the drug combination, the investigators are planning further studies in larger numbers of patients with tumors in the Ewing’s sarcoma family, as well as additional studies into the underlying mechanisms of resistance in individual patients, Dr. Naing said during a press conference.
The results of this study were published simultaneously in Clinical Cancer Research (2012 [doi:10.1158/1078-0432.CCR-12-0061]).
Dr. Naing reported having no relevant financial relationships to disclose.
CHICAGO – Two targeted therapies may be better than one for the treatment of refractory Ewing’s sarcoma, according to findings of an early clinical trial reported at the annual meeting of the American Association for Cancer Research.
Combining the investigational agent cixutumumab with temsirolimus (Torisel) resulted in 2 complete responses and 3 partial responses in 17 adolescent and young adult patients with heavily pretreated disease in the phase I clinical trial.
Cixutumumab, a novel monoclonal antibody targeting the insulin-like growth factor 1-receptor (IGF-1R), is under investigation for various cancers. Temsirolimus, a mammalian target of rapamycin (mTOR) inhibitor, is approved for the treatment of advanced renal cell carcinomas.
The two drugs have previously been used as single treatment agents, producing mixed results, according to Dr. Aung Naing of the department of investigational cancer therapeutics at the University of Texas M.D. Anderson Cancer Center in Houston.
Based on data from preclinical studies, "we hypothesized that combining the two could help prevent drug-resistance, which is a common problem in Ewing’s sarcoma," he said in an interview. The two agents target molecular pathways associated with cell proliferation and survival, abnormal blood vessel growth, and resistance to both chemotherapy and radiation therapy, Dr. Naing explained.
To test their hypothesis, the investigators enrolled 20 patients, median age 20 years, with Ewing’s sarcoma (17) or desmoplastic small-round-cell tumors (3) in the trial. The median number of prior therapies per patient was 6. Two patients previously received temsirolimus and six previously received an IGF-1R inhibitor, he said.
All of the patients received 6 mg/kg of intravenous cixutumumab and 25-37.5mg of intravenous temsirolimus weekly for 4-week cycles, with restaging after 8 weeks, Dr. Naing reported.
At a median follow-up of 8.9 months, 7 of the 20 patients (35%) had achieved a complete or partial response or stable disease lasting more than 5 months.
In Ewing’s sarcoma patients specifically, 29% had evidence of tumor regression greater than 20%, Dr. Naing said, noting, "Two patients achieved complete responses, one of which lasted 27 months."
The most frequent, possibly drug-related toxicities included thrombocytopenia (85%), mucositis (80%), hypercholesterolemia (75%), hypertriglyceridemia (70%), and hyperglycemia (65%).
"Most were grade 1-2 [toxicities], but four of the seven best responders developed grade 3 mucositis, myelosuppression, or hyperglycemia, which were managed while maintaining drug dose," Dr. Naing stated.
"Typically, patients who develop these types of grade 3 toxicities would be removed from the study, but we were able to continue with treatment after receiving approval from the sponsor and notification from our institutional review board," he said. Because the toxicities were able to be controlled using supportive measures, "the drug dose did not have to be compromised."
One of the Ewing’s sarcoma patients had achieved a partial response with prior IGF-1R treatment. After initiating the combination therapy, this patient had a mixed response with "remarkable" regression in three lung nodules but progression in a fourth. Morphoproteomic analysis of biopsy samples from this patient demonstrated upregulation of mTOR and ERK/MEK signals, suggesting the possibility that a combination of IGFR/mTOR and MAPK/ERK kinase (MEK) inhibitors might warrant investigation in order to reverse resistance, according to Dr. Naing.
Based on the evidence of activity for the drug combination, the investigators are planning further studies in larger numbers of patients with tumors in the Ewing’s sarcoma family, as well as additional studies into the underlying mechanisms of resistance in individual patients, Dr. Naing said during a press conference.
The results of this study were published simultaneously in Clinical Cancer Research (2012 [doi:10.1158/1078-0432.CCR-12-0061]).
Dr. Naing reported having no relevant financial relationships to disclose.
CHICAGO – Two targeted therapies may be better than one for the treatment of refractory Ewing’s sarcoma, according to findings of an early clinical trial reported at the annual meeting of the American Association for Cancer Research.
Combining the investigational agent cixutumumab with temsirolimus (Torisel) resulted in 2 complete responses and 3 partial responses in 17 adolescent and young adult patients with heavily pretreated disease in the phase I clinical trial.
Cixutumumab, a novel monoclonal antibody targeting the insulin-like growth factor 1-receptor (IGF-1R), is under investigation for various cancers. Temsirolimus, a mammalian target of rapamycin (mTOR) inhibitor, is approved for the treatment of advanced renal cell carcinomas.
The two drugs have previously been used as single treatment agents, producing mixed results, according to Dr. Aung Naing of the department of investigational cancer therapeutics at the University of Texas M.D. Anderson Cancer Center in Houston.
Based on data from preclinical studies, "we hypothesized that combining the two could help prevent drug-resistance, which is a common problem in Ewing’s sarcoma," he said in an interview. The two agents target molecular pathways associated with cell proliferation and survival, abnormal blood vessel growth, and resistance to both chemotherapy and radiation therapy, Dr. Naing explained.
To test their hypothesis, the investigators enrolled 20 patients, median age 20 years, with Ewing’s sarcoma (17) or desmoplastic small-round-cell tumors (3) in the trial. The median number of prior therapies per patient was 6. Two patients previously received temsirolimus and six previously received an IGF-1R inhibitor, he said.
All of the patients received 6 mg/kg of intravenous cixutumumab and 25-37.5mg of intravenous temsirolimus weekly for 4-week cycles, with restaging after 8 weeks, Dr. Naing reported.
At a median follow-up of 8.9 months, 7 of the 20 patients (35%) had achieved a complete or partial response or stable disease lasting more than 5 months.
In Ewing’s sarcoma patients specifically, 29% had evidence of tumor regression greater than 20%, Dr. Naing said, noting, "Two patients achieved complete responses, one of which lasted 27 months."
The most frequent, possibly drug-related toxicities included thrombocytopenia (85%), mucositis (80%), hypercholesterolemia (75%), hypertriglyceridemia (70%), and hyperglycemia (65%).
"Most were grade 1-2 [toxicities], but four of the seven best responders developed grade 3 mucositis, myelosuppression, or hyperglycemia, which were managed while maintaining drug dose," Dr. Naing stated.
"Typically, patients who develop these types of grade 3 toxicities would be removed from the study, but we were able to continue with treatment after receiving approval from the sponsor and notification from our institutional review board," he said. Because the toxicities were able to be controlled using supportive measures, "the drug dose did not have to be compromised."
One of the Ewing’s sarcoma patients had achieved a partial response with prior IGF-1R treatment. After initiating the combination therapy, this patient had a mixed response with "remarkable" regression in three lung nodules but progression in a fourth. Morphoproteomic analysis of biopsy samples from this patient demonstrated upregulation of mTOR and ERK/MEK signals, suggesting the possibility that a combination of IGFR/mTOR and MAPK/ERK kinase (MEK) inhibitors might warrant investigation in order to reverse resistance, according to Dr. Naing.
Based on the evidence of activity for the drug combination, the investigators are planning further studies in larger numbers of patients with tumors in the Ewing’s sarcoma family, as well as additional studies into the underlying mechanisms of resistance in individual patients, Dr. Naing said during a press conference.
The results of this study were published simultaneously in Clinical Cancer Research (2012 [doi:10.1158/1078-0432.CCR-12-0061]).
Dr. Naing reported having no relevant financial relationships to disclose.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION OF CANCER RESEARCH
Major Finding: Five of 17 patients with refractory Ewing’s sarcoma demonstrated partial or complete response to combination therapy with cixutumumab and temsirolimus.
Data Source: Data were taken from a phase I clinical trial of cixutumumab and temsirolimus in 20 heavily pretreated patients with Ewing’s sarcoma family of tumors.
Disclosures: Dr. Naing reported having no relevant financial relationships to disclose.
Galeterone Lowers PSA in Castration-Resistant Prostate Cancer
CHICAGO – About half of men with castration-resistant prostate cancer demonstrated considerable declines in prostate-specific antigen levels when treated with the investigational agent galeterone in a phase I dose-escalation trial, investigators reported.
Galeterone (TOK-001), an orally available, semisynthetic steroid analogue, mounts a three-pronged attack on prostate cancer, according to Dr. R. Bruce Montgomery of the University of Washington in Seattle. It inhibits CYP17 lyase (a key enzyme in the androgen production pathway in the disease), inhibits androgen-receptor binding, and disrupts internal androgen-receptor production in prostate cancer cells.

This novel triple-target mechanism, which was identified in preclinical studies, "could help prevent drug resistance," Dr. Montgomery said during a press briefing at the annual meeting of the American Association for Cancer Research, where the data were presented.
To evaluate the safety and efficacy of the drug, Dr. Montgomery and his colleagues enrolled 49 men with metastatic and nonmetastatic, chemotherapy-naive, castration-resistant prostate cancer (CRPC) in the ARMOR1 trial sponsored by Tokai Pharmaceuticals.
All of the men, who ranged in age from 48-93 years, had an ECOG (Eastern Cooperative Oncology Group) performance status of 0 or 1, as well as disease progression during androgen ablation therapy. Exclusion criteria included prior treatment with ketoconazole, MDV3100, abiraterone (Zytiga), sipuleucel-T (Provenge), TAK-700, mitoxantrone (Novantrone), or chemotherapy based on either docetaxel (Taxotere) or cabazitaxel (Jevtana).
The study participants were randomized to eight dose-escalation cohorts that received single or split daily doses of galeterone ranging from 650 mg to 2,600 mg per day for 12 weeks, followed by optional continuation in an extension phase, Dr. Montgomery explained.
Efficacy was a secondary outcome measure, which was assessed based on change in PSA level, changes from baseline in CT/MRI and bone scans, RECIST (Response Evaluation Criteria in Solid Tumors) data, and laboratory measures.
A majority of patients had PSA reductions; among them, 11 patients had PSA reductions of at least 50% and an additional 13 patients had PSA reductions of 30%-49%, reported Dr. Montgomery, noting that the magnitude of the reductions were dose related. In addition, some patients had evidence of a reduction in tumor size on CT scans.
"The improved PSA response indicates that the drug is getting to the target, because PSA expression is controlled by the androgen receptor," he said in an interview. "The fact that so many patients had a PSA reduction of 30% or more is exceptional in a phase I dose-finding trial."
The primary outcome measures were tolerability and safety, as measured by the incidence of adverse events and the change from baseline in clinical laboratory assessments, physical examination, vital signs, and electrocardiograms, he said.
Grade 1 and 2 adverse events were reported in 58% and 30% of the patients, respectively. These included fatigue (36.7%), abnormal AST tests (32.7%), abnormal ALT tests (30.6%), nausea (28.6%), diarrhea (26.5%), and pruritis (24.5%), Dr. Montgomery reported.
In all, "15 patients had transient grade 2/3 liver-enzyme elevations, including 11 who required dose interruptions," he said.
Of the 11 patients with dose interruptions, 7 resumed galeterone treatment, and 6 completed the treatment without recurrent grade 3 elevations in liver enzymes, he added, noting that "the transaminitis was not dose-related and was very transient."
The finding does suggest, however, that regular monitoring of liver function enzymes may be warranted in men taking the drug, he said.
Of nine serious adverse events reported in the study, only one was linked to galeterone. "The single, related grade 4 adverse event was rhabdomyolysis in a patient with renal insufficiency who was on simvastatin therapy," Dr. Montgomery said. "No cases of adrenal mineralocorticoid excess were observed."
The study did not reveal dose proportionality, but "the maximum tolerated dose was identified at the doses evaluated in the trial," Dr. Montgomery said. Therefore, Tokai Pharmaceuticals is currently reformulating the drug "to optimize pharmacokinetics and pharmacodynamics."
The new formulation will be evaluated later this year in a phase II clinical trial, he said.
Tokai Pharmaceuticals sponsored the trial. Dr. Montgomery disclosed no relevant financial conflicts of interest.
CHICAGO – About half of men with castration-resistant prostate cancer demonstrated considerable declines in prostate-specific antigen levels when treated with the investigational agent galeterone in a phase I dose-escalation trial, investigators reported.
Galeterone (TOK-001), an orally available, semisynthetic steroid analogue, mounts a three-pronged attack on prostate cancer, according to Dr. R. Bruce Montgomery of the University of Washington in Seattle. It inhibits CYP17 lyase (a key enzyme in the androgen production pathway in the disease), inhibits androgen-receptor binding, and disrupts internal androgen-receptor production in prostate cancer cells.
This novel triple-target mechanism, which was identified in preclinical studies, "could help prevent drug resistance," Dr. Montgomery said during a press briefing at the annual meeting of the American Association for Cancer Research, where the data were presented.
To evaluate the safety and efficacy of the drug, Dr. Montgomery and his colleagues enrolled 49 men with metastatic and nonmetastatic, chemotherapy-naive, castration-resistant prostate cancer (CRPC) in the ARMOR1 trial sponsored by Tokai Pharmaceuticals.
All of the men, who ranged in age from 48-93 years, had an ECOG (Eastern Cooperative Oncology Group) performance status of 0 or 1, as well as disease progression during androgen ablation therapy. Exclusion criteria included prior treatment with ketoconazole, MDV3100, abiraterone (Zytiga), sipuleucel-T (Provenge), TAK-700, mitoxantrone (Novantrone), or chemotherapy based on either docetaxel (Taxotere) or cabazitaxel (Jevtana).
The study participants were randomized to eight dose-escalation cohorts that received single or split daily doses of galeterone ranging from 650 mg to 2,600 mg per day for 12 weeks, followed by optional continuation in an extension phase, Dr. Montgomery explained.
Efficacy was a secondary outcome measure, which was assessed based on change in PSA level, changes from baseline in CT/MRI and bone scans, RECIST (Response Evaluation Criteria in Solid Tumors) data, and laboratory measures.
A majority of patients had PSA reductions; among them, 11 patients had PSA reductions of at least 50% and an additional 13 patients had PSA reductions of 30%-49%, reported Dr. Montgomery, noting that the magnitude of the reductions were dose related. In addition, some patients had evidence of a reduction in tumor size on CT scans.
"The improved PSA response indicates that the drug is getting to the target, because PSA expression is controlled by the androgen receptor," he said in an interview. "The fact that so many patients had a PSA reduction of 30% or more is exceptional in a phase I dose-finding trial."
The primary outcome measures were tolerability and safety, as measured by the incidence of adverse events and the change from baseline in clinical laboratory assessments, physical examination, vital signs, and electrocardiograms, he said.
Grade 1 and 2 adverse events were reported in 58% and 30% of the patients, respectively. These included fatigue (36.7%), abnormal AST tests (32.7%), abnormal ALT tests (30.6%), nausea (28.6%), diarrhea (26.5%), and pruritis (24.5%), Dr. Montgomery reported.
In all, "15 patients had transient grade 2/3 liver-enzyme elevations, including 11 who required dose interruptions," he said.
Of the 11 patients with dose interruptions, 7 resumed galeterone treatment, and 6 completed the treatment without recurrent grade 3 elevations in liver enzymes, he added, noting that "the transaminitis was not dose-related and was very transient."
The finding does suggest, however, that regular monitoring of liver function enzymes may be warranted in men taking the drug, he said.
Of nine serious adverse events reported in the study, only one was linked to galeterone. "The single, related grade 4 adverse event was rhabdomyolysis in a patient with renal insufficiency who was on simvastatin therapy," Dr. Montgomery said. "No cases of adrenal mineralocorticoid excess were observed."
The study did not reveal dose proportionality, but "the maximum tolerated dose was identified at the doses evaluated in the trial," Dr. Montgomery said. Therefore, Tokai Pharmaceuticals is currently reformulating the drug "to optimize pharmacokinetics and pharmacodynamics."
The new formulation will be evaluated later this year in a phase II clinical trial, he said.
Tokai Pharmaceuticals sponsored the trial. Dr. Montgomery disclosed no relevant financial conflicts of interest.
CHICAGO – About half of men with castration-resistant prostate cancer demonstrated considerable declines in prostate-specific antigen levels when treated with the investigational agent galeterone in a phase I dose-escalation trial, investigators reported.
Galeterone (TOK-001), an orally available, semisynthetic steroid analogue, mounts a three-pronged attack on prostate cancer, according to Dr. R. Bruce Montgomery of the University of Washington in Seattle. It inhibits CYP17 lyase (a key enzyme in the androgen production pathway in the disease), inhibits androgen-receptor binding, and disrupts internal androgen-receptor production in prostate cancer cells.
This novel triple-target mechanism, which was identified in preclinical studies, "could help prevent drug resistance," Dr. Montgomery said during a press briefing at the annual meeting of the American Association for Cancer Research, where the data were presented.
To evaluate the safety and efficacy of the drug, Dr. Montgomery and his colleagues enrolled 49 men with metastatic and nonmetastatic, chemotherapy-naive, castration-resistant prostate cancer (CRPC) in the ARMOR1 trial sponsored by Tokai Pharmaceuticals.
All of the men, who ranged in age from 48-93 years, had an ECOG (Eastern Cooperative Oncology Group) performance status of 0 or 1, as well as disease progression during androgen ablation therapy. Exclusion criteria included prior treatment with ketoconazole, MDV3100, abiraterone (Zytiga), sipuleucel-T (Provenge), TAK-700, mitoxantrone (Novantrone), or chemotherapy based on either docetaxel (Taxotere) or cabazitaxel (Jevtana).
The study participants were randomized to eight dose-escalation cohorts that received single or split daily doses of galeterone ranging from 650 mg to 2,600 mg per day for 12 weeks, followed by optional continuation in an extension phase, Dr. Montgomery explained.
Efficacy was a secondary outcome measure, which was assessed based on change in PSA level, changes from baseline in CT/MRI and bone scans, RECIST (Response Evaluation Criteria in Solid Tumors) data, and laboratory measures.
A majority of patients had PSA reductions; among them, 11 patients had PSA reductions of at least 50% and an additional 13 patients had PSA reductions of 30%-49%, reported Dr. Montgomery, noting that the magnitude of the reductions were dose related. In addition, some patients had evidence of a reduction in tumor size on CT scans.
"The improved PSA response indicates that the drug is getting to the target, because PSA expression is controlled by the androgen receptor," he said in an interview. "The fact that so many patients had a PSA reduction of 30% or more is exceptional in a phase I dose-finding trial."
The primary outcome measures were tolerability and safety, as measured by the incidence of adverse events and the change from baseline in clinical laboratory assessments, physical examination, vital signs, and electrocardiograms, he said.
Grade 1 and 2 adverse events were reported in 58% and 30% of the patients, respectively. These included fatigue (36.7%), abnormal AST tests (32.7%), abnormal ALT tests (30.6%), nausea (28.6%), diarrhea (26.5%), and pruritis (24.5%), Dr. Montgomery reported.
In all, "15 patients had transient grade 2/3 liver-enzyme elevations, including 11 who required dose interruptions," he said.
Of the 11 patients with dose interruptions, 7 resumed galeterone treatment, and 6 completed the treatment without recurrent grade 3 elevations in liver enzymes, he added, noting that "the transaminitis was not dose-related and was very transient."
The finding does suggest, however, that regular monitoring of liver function enzymes may be warranted in men taking the drug, he said.
Of nine serious adverse events reported in the study, only one was linked to galeterone. "The single, related grade 4 adverse event was rhabdomyolysis in a patient with renal insufficiency who was on simvastatin therapy," Dr. Montgomery said. "No cases of adrenal mineralocorticoid excess were observed."
The study did not reveal dose proportionality, but "the maximum tolerated dose was identified at the doses evaluated in the trial," Dr. Montgomery said. Therefore, Tokai Pharmaceuticals is currently reformulating the drug "to optimize pharmacokinetics and pharmacodynamics."
The new formulation will be evaluated later this year in a phase II clinical trial, he said.
Tokai Pharmaceuticals sponsored the trial. Dr. Montgomery disclosed no relevant financial conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR CANCER RESEARCH
Major Finding: In all, 24 of 49 men with castration-resistant prostate cancer achieved reductions in PSA levels of at least 30% when treated with the investigational agent galeterone.
Data Source: Investigators conducted a phase I dose-finding trial in 49 chemotherapy-naive men with metastatic and nonmetastatic castrate-resistant prostate cancer.
Disclosures: Tokai Pharmaceuticals sponsored the trial. Dr. Montgomery reported having no relevant financial conflicts of interest.
NCCN: Skip ALND in Some Early Breast Cancer
Axillary lymph node dissection can be skipped in some early-stage breast cancer patients with minimal sentinel node involvement, as well as in those with negative findings on sentinel node biopsy, according to revised clinical practice guidelines issued by the National Comprehensive Cancer Network.
The recommendation that no further axial surgery be considered for certain patients with only one or two involved sentinel lymph nodes reflects an upgrade of the National Comprehensive Cancer Network (NCCN) guideline on sentinel node biopsy to a category 1 recommendation.
The change is based on the findings of recent prospective studies. In particular, the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial, found no survival difference between early-stage breast cancer patients who underwent axillary lymph node dissection [ALND] and those who did not after one or two sentinel nodes were determined to be positive on biopsy (JAMA 2011;305:569-75).
The revised recommendation extends only to those patients with early-stage disease (tumor grades 1 or 2) who undergo breast-conserving surgery and whole-breast radiation and who have not received neoadjuvant chemotherapy, according to the guidelines. A primary objective is to reduce the risk of lymphedema associated with axillary lymph node dissection.
"In the absence of definitive data demonstrating superior survival from the performance of axillary lymph node dissection, patients who have particularly favorable tumors, patients for whom the selection of adjuvant systemic therapy is unlikely to be affected, for the elderly or those with serious comorbid conditions, the performance of axillary lymph node dissection may be considered optional," the guidelines advise.
The update was presented at the NCCN annual meeting in Hollywood, Fla. The Breast Cancer Panel lists potential conflict of interest disclosures on the NCCN website.
Axillary lymph node dissection can be skipped in some early-stage breast cancer patients with minimal sentinel node involvement, as well as in those with negative findings on sentinel node biopsy, according to revised clinical practice guidelines issued by the National Comprehensive Cancer Network.
The recommendation that no further axial surgery be considered for certain patients with only one or two involved sentinel lymph nodes reflects an upgrade of the National Comprehensive Cancer Network (NCCN) guideline on sentinel node biopsy to a category 1 recommendation.
The change is based on the findings of recent prospective studies. In particular, the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial, found no survival difference between early-stage breast cancer patients who underwent axillary lymph node dissection [ALND] and those who did not after one or two sentinel nodes were determined to be positive on biopsy (JAMA 2011;305:569-75).
The revised recommendation extends only to those patients with early-stage disease (tumor grades 1 or 2) who undergo breast-conserving surgery and whole-breast radiation and who have not received neoadjuvant chemotherapy, according to the guidelines. A primary objective is to reduce the risk of lymphedema associated with axillary lymph node dissection.
"In the absence of definitive data demonstrating superior survival from the performance of axillary lymph node dissection, patients who have particularly favorable tumors, patients for whom the selection of adjuvant systemic therapy is unlikely to be affected, for the elderly or those with serious comorbid conditions, the performance of axillary lymph node dissection may be considered optional," the guidelines advise.
The update was presented at the NCCN annual meeting in Hollywood, Fla. The Breast Cancer Panel lists potential conflict of interest disclosures on the NCCN website.
Axillary lymph node dissection can be skipped in some early-stage breast cancer patients with minimal sentinel node involvement, as well as in those with negative findings on sentinel node biopsy, according to revised clinical practice guidelines issued by the National Comprehensive Cancer Network.
The recommendation that no further axial surgery be considered for certain patients with only one or two involved sentinel lymph nodes reflects an upgrade of the National Comprehensive Cancer Network (NCCN) guideline on sentinel node biopsy to a category 1 recommendation.
The change is based on the findings of recent prospective studies. In particular, the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial, found no survival difference between early-stage breast cancer patients who underwent axillary lymph node dissection [ALND] and those who did not after one or two sentinel nodes were determined to be positive on biopsy (JAMA 2011;305:569-75).
The revised recommendation extends only to those patients with early-stage disease (tumor grades 1 or 2) who undergo breast-conserving surgery and whole-breast radiation and who have not received neoadjuvant chemotherapy, according to the guidelines. A primary objective is to reduce the risk of lymphedema associated with axillary lymph node dissection.
"In the absence of definitive data demonstrating superior survival from the performance of axillary lymph node dissection, patients who have particularly favorable tumors, patients for whom the selection of adjuvant systemic therapy is unlikely to be affected, for the elderly or those with serious comorbid conditions, the performance of axillary lymph node dissection may be considered optional," the guidelines advise.
The update was presented at the NCCN annual meeting in Hollywood, Fla. The Breast Cancer Panel lists potential conflict of interest disclosures on the NCCN website.
FROM THE NATIONAL COMPREHENSIVE CANCER NETWORK
At-Risk Lung Cancer Patients Respond to Nab-Paclitaxel Regimen
CHICAGO – Combination therapy with nanoparticle albumin bound–paclitaxel and carboplatin may be an option for the subset of advanced non–small cell lung cancer patients who are ineligible for bevacizumab treatment because of bleeding risk.
The combined treatment produced an objective response rate of more than 40% among non–small cell lung cancer (NSCLC) patients with squamous histology or other hemorrhagic risk factors in a single-arm, single institution, phase II trial presented at the annual meeting of the American Association for Cancer Research.
The preliminary results, which include evidence of "tolerable toxicity," are especially encouraging because of the limited treatment options available to this patient population, according to the senior investigator Dr. Gregory Otterson of the Ohio State University Comprehensive Cancer Center in Columbus.
Much attention has been focused on the addition of bevacizumab (Avastin) to platinum-based chemotherapy in the treatment of advanced NSCLC because the combination has been shown to improve objective response rates, progression-free survival, and overall survival in this population, Dr. Otterson explained. However, bevacizumab’s association with hemorrhagic complications precludes its indication for patients already at increased risk of bleeding, including those with squamous cell carcinoma or a history of hemoptysis, as well as those taking anticoagulant medication,
For these patients, paclitaxel – a compound that stabilizes microtubules to induce cell death – plus the DNA-targeting platinum compound carboplatin is a common therapeutic option, but it is frequently associated with hypersensitivity reactions to the toxic solvent Cremophor through which paclitaxel is delivered. In contrast, nab-paclitaxel (Abraxane) is a solvent-free formulation delivered by a nanoparticle technology that binds to the natural protein albumin.
"It is thought that delivering paclitaxel with this technology causes fewer hypersensitivity reactions and may lead to greater drug uptake in tumors," Dr. Otterson said, noting that "higher doses can be administered over a shorter infusion time without the need for special infusion sets or premedications."
A previous randomized controlled trial comparing the nab-paclitaxel plus carboplatin combination with the conventional paclitaxel plus carboplatin combination in advanced NSCLC patients demonstrated superior overall response rates with the former combination, especially in patients with squamous cell histology, Dr. Otterson said. Based on this finding, the current study is focusing specifically on squamous cell patients and others whose bleeding risk precludes bevacizumab treatment, he said.
The investigators enrolled 63 chemotherapy-naive NSCLC patients (21 female and 42 male) in the trial, including 48 with squamous cell carcinoma, 9 with adenocarcinomas, 4 with NSCLC not otherwise specified, and 2 with adenosquamous carcinoma, Dr. Otterson said. Of the patients with nonsquamous disease, 11 had a history of hemoptysis and 2 had a history of thrombosis, while one patient was undergoing therapeutic anticoagulation. The average tobacco use history for all of the patients, median age 63 years, was 50-pack years, he said.
At baseline, microRNA profiles were generated from blood/serum samples acquired from all of the patients. Treatment was administered every 21 days, initially at 300 mg per m2/AUC=6, then adjusted to 260 mg per m2/AUC=6 because of excess neuropathy, Dr. Otterson said. The study’s primary end point is overall response rate: safety and toxicities as well as overall survival and progression-free survival are secondary end points.
Preliminary findings for 53 patients evaluable to date indicate that 22 patients experienced a partial response to the therapy, while none experienced a complete response, for an ORR of 41.5%. The investigators observed stable disease in 21 patients, and progressive disease in 10 patients, Dr. Otterson said.
With respect to tolerability, "more than 10% of the patients experienced grade 3/4 toxicities," including hematologic toxicity in 36 patients febrile neutropenia in 9, infection in 15, sensory neuropathy in 17, dyspnea in 10, and dehydration in 8. Additionally, there were four deaths, reported as grade 5 toxicities, including sudden death in one patient and respiratory failure in another, he said.
Although median overall survival and progression-free survival, at 9.7 months and 5 months, respectively, "were not as high as we would have liked to see," the apparent durability of the treatment – some of the patients did not require additional treatment for at least 6 months – is "surprising and promising," Dr. Otterson said: "Based on the findings, additional investigation in the squamous cell population, in particular, is warranted."
The study was supported by Abraxis Biosciences. Dr. Otterson reported having no relevant conflicts of interest.
CHICAGO – Combination therapy with nanoparticle albumin bound–paclitaxel and carboplatin may be an option for the subset of advanced non–small cell lung cancer patients who are ineligible for bevacizumab treatment because of bleeding risk.
The combined treatment produced an objective response rate of more than 40% among non–small cell lung cancer (NSCLC) patients with squamous histology or other hemorrhagic risk factors in a single-arm, single institution, phase II trial presented at the annual meeting of the American Association for Cancer Research.
The preliminary results, which include evidence of "tolerable toxicity," are especially encouraging because of the limited treatment options available to this patient population, according to the senior investigator Dr. Gregory Otterson of the Ohio State University Comprehensive Cancer Center in Columbus.
Much attention has been focused on the addition of bevacizumab (Avastin) to platinum-based chemotherapy in the treatment of advanced NSCLC because the combination has been shown to improve objective response rates, progression-free survival, and overall survival in this population, Dr. Otterson explained. However, bevacizumab’s association with hemorrhagic complications precludes its indication for patients already at increased risk of bleeding, including those with squamous cell carcinoma or a history of hemoptysis, as well as those taking anticoagulant medication,
For these patients, paclitaxel – a compound that stabilizes microtubules to induce cell death – plus the DNA-targeting platinum compound carboplatin is a common therapeutic option, but it is frequently associated with hypersensitivity reactions to the toxic solvent Cremophor through which paclitaxel is delivered. In contrast, nab-paclitaxel (Abraxane) is a solvent-free formulation delivered by a nanoparticle technology that binds to the natural protein albumin.
"It is thought that delivering paclitaxel with this technology causes fewer hypersensitivity reactions and may lead to greater drug uptake in tumors," Dr. Otterson said, noting that "higher doses can be administered over a shorter infusion time without the need for special infusion sets or premedications."
A previous randomized controlled trial comparing the nab-paclitaxel plus carboplatin combination with the conventional paclitaxel plus carboplatin combination in advanced NSCLC patients demonstrated superior overall response rates with the former combination, especially in patients with squamous cell histology, Dr. Otterson said. Based on this finding, the current study is focusing specifically on squamous cell patients and others whose bleeding risk precludes bevacizumab treatment, he said.
The investigators enrolled 63 chemotherapy-naive NSCLC patients (21 female and 42 male) in the trial, including 48 with squamous cell carcinoma, 9 with adenocarcinomas, 4 with NSCLC not otherwise specified, and 2 with adenosquamous carcinoma, Dr. Otterson said. Of the patients with nonsquamous disease, 11 had a history of hemoptysis and 2 had a history of thrombosis, while one patient was undergoing therapeutic anticoagulation. The average tobacco use history for all of the patients, median age 63 years, was 50-pack years, he said.
At baseline, microRNA profiles were generated from blood/serum samples acquired from all of the patients. Treatment was administered every 21 days, initially at 300 mg per m2/AUC=6, then adjusted to 260 mg per m2/AUC=6 because of excess neuropathy, Dr. Otterson said. The study’s primary end point is overall response rate: safety and toxicities as well as overall survival and progression-free survival are secondary end points.
Preliminary findings for 53 patients evaluable to date indicate that 22 patients experienced a partial response to the therapy, while none experienced a complete response, for an ORR of 41.5%. The investigators observed stable disease in 21 patients, and progressive disease in 10 patients, Dr. Otterson said.
With respect to tolerability, "more than 10% of the patients experienced grade 3/4 toxicities," including hematologic toxicity in 36 patients febrile neutropenia in 9, infection in 15, sensory neuropathy in 17, dyspnea in 10, and dehydration in 8. Additionally, there were four deaths, reported as grade 5 toxicities, including sudden death in one patient and respiratory failure in another, he said.
Although median overall survival and progression-free survival, at 9.7 months and 5 months, respectively, "were not as high as we would have liked to see," the apparent durability of the treatment – some of the patients did not require additional treatment for at least 6 months – is "surprising and promising," Dr. Otterson said: "Based on the findings, additional investigation in the squamous cell population, in particular, is warranted."
The study was supported by Abraxis Biosciences. Dr. Otterson reported having no relevant conflicts of interest.
CHICAGO – Combination therapy with nanoparticle albumin bound–paclitaxel and carboplatin may be an option for the subset of advanced non–small cell lung cancer patients who are ineligible for bevacizumab treatment because of bleeding risk.
The combined treatment produced an objective response rate of more than 40% among non–small cell lung cancer (NSCLC) patients with squamous histology or other hemorrhagic risk factors in a single-arm, single institution, phase II trial presented at the annual meeting of the American Association for Cancer Research.
The preliminary results, which include evidence of "tolerable toxicity," are especially encouraging because of the limited treatment options available to this patient population, according to the senior investigator Dr. Gregory Otterson of the Ohio State University Comprehensive Cancer Center in Columbus.
Much attention has been focused on the addition of bevacizumab (Avastin) to platinum-based chemotherapy in the treatment of advanced NSCLC because the combination has been shown to improve objective response rates, progression-free survival, and overall survival in this population, Dr. Otterson explained. However, bevacizumab’s association with hemorrhagic complications precludes its indication for patients already at increased risk of bleeding, including those with squamous cell carcinoma or a history of hemoptysis, as well as those taking anticoagulant medication,
For these patients, paclitaxel – a compound that stabilizes microtubules to induce cell death – plus the DNA-targeting platinum compound carboplatin is a common therapeutic option, but it is frequently associated with hypersensitivity reactions to the toxic solvent Cremophor through which paclitaxel is delivered. In contrast, nab-paclitaxel (Abraxane) is a solvent-free formulation delivered by a nanoparticle technology that binds to the natural protein albumin.
"It is thought that delivering paclitaxel with this technology causes fewer hypersensitivity reactions and may lead to greater drug uptake in tumors," Dr. Otterson said, noting that "higher doses can be administered over a shorter infusion time without the need for special infusion sets or premedications."
A previous randomized controlled trial comparing the nab-paclitaxel plus carboplatin combination with the conventional paclitaxel plus carboplatin combination in advanced NSCLC patients demonstrated superior overall response rates with the former combination, especially in patients with squamous cell histology, Dr. Otterson said. Based on this finding, the current study is focusing specifically on squamous cell patients and others whose bleeding risk precludes bevacizumab treatment, he said.
The investigators enrolled 63 chemotherapy-naive NSCLC patients (21 female and 42 male) in the trial, including 48 with squamous cell carcinoma, 9 with adenocarcinomas, 4 with NSCLC not otherwise specified, and 2 with adenosquamous carcinoma, Dr. Otterson said. Of the patients with nonsquamous disease, 11 had a history of hemoptysis and 2 had a history of thrombosis, while one patient was undergoing therapeutic anticoagulation. The average tobacco use history for all of the patients, median age 63 years, was 50-pack years, he said.
At baseline, microRNA profiles were generated from blood/serum samples acquired from all of the patients. Treatment was administered every 21 days, initially at 300 mg per m2/AUC=6, then adjusted to 260 mg per m2/AUC=6 because of excess neuropathy, Dr. Otterson said. The study’s primary end point is overall response rate: safety and toxicities as well as overall survival and progression-free survival are secondary end points.
Preliminary findings for 53 patients evaluable to date indicate that 22 patients experienced a partial response to the therapy, while none experienced a complete response, for an ORR of 41.5%. The investigators observed stable disease in 21 patients, and progressive disease in 10 patients, Dr. Otterson said.
With respect to tolerability, "more than 10% of the patients experienced grade 3/4 toxicities," including hematologic toxicity in 36 patients febrile neutropenia in 9, infection in 15, sensory neuropathy in 17, dyspnea in 10, and dehydration in 8. Additionally, there were four deaths, reported as grade 5 toxicities, including sudden death in one patient and respiratory failure in another, he said.
Although median overall survival and progression-free survival, at 9.7 months and 5 months, respectively, "were not as high as we would have liked to see," the apparent durability of the treatment – some of the patients did not require additional treatment for at least 6 months – is "surprising and promising," Dr. Otterson said: "Based on the findings, additional investigation in the squamous cell population, in particular, is warranted."
The study was supported by Abraxis Biosciences. Dr. Otterson reported having no relevant conflicts of interest.
NEWS FROM THE AMERICAN ASSOCIATION FOR CANCER RESEARCH
Major Finding: The combination of nanoparticle albumin bound–paclitaxel and carboplatin produced an objective response rate of 41% in a cohort of advanced non–small cell lung cancer patients with bleeding risks.
Data Source: Investigators conducted a single-arm, single institution phase II trial in 63 patients ineligible for bevacizumab therapy because of bleeding risk
Disclosures: The study was supported by Abraxis Biosciences. Dr. Otterson reported having no relevant conflicts of interest.
In the Pipeline: Immunotherapy Slows Childhood Gliomas
CHICAGO – Immunotherapy with peptide vaccines may offer a much-needed therapeutic option for gliomas in children, which carry a poor prognosis despite current treatments.
In a pilot trial of subcutaneous vaccinations with peptides for glioma-associated antigen (GAA) epitopes in children who have been newly diagnosed with brain stem gliomas, cerebral high-grade gliomas, or recurrent gliomas, the immunotherapy was well tolerated and demonstrated immunologic and clinical activity, Dr. Ian F. Pollack reported April 2 at the annual meeting of the American Association for Cancer Research.

Based on significant experience with immunotherapy for adult gliomas, "we extended these insights to childhood gliomas – malignant astrocytomas of the brain stem and cerebral hemispheres and recurrent low-grade gliomas – based on our observations of their glioma-associated antigen expression profiles," Dr. Pollack explained during a press conference.
For the pilot study, Dr. Pollack, chief of pediatric neurosurgery at Children’s Hospital of Pittsburgh Brain Care Institute, and his colleagues have enrolled 27 human leukocyte antigen (HLA) A2–positive children to date, including 16 who are newly diagnosed with brain stem gliomas, 5 with newly diagnosed high-grade gliomas, and 6 with recurrent gliomas. The GAAs were EphA2, interleukin-13 receptor alpha 2 (IL-13RA2), and survivin, he said.
All of the children received eight courses of subcutaneous vaccinations with peptides for GAA epitopes emulsified in Montanide-ISA-51 every 3 weeks, along with intramuscular injections of the immunoadjuvant poly-ICLC, which promotes the infiltration of effector T cells into intracranial gliomas.
"Our primary end points were safety and T-cell response against vaccine-targeted [GAAs]," he said, noting that treatment response was assessed clinically and by MRI.
The preliminary results reported at the meeting are based on an interim analysis of 22 evaluable patients. To date, no non–central nervous system toxicities have limited the vaccine dosages, Dr. Pollack said. Of the 22 children, 4 showed signs of rapidly progressive disease, 14 had stable disease for more than 3 months, 3 had sustained partial responses, and 1 had prolonged disease-free status after surgery, he reported.
Symptomatic "pseudoprogression" – consisting of transient neurologic deterioration and tumor enlargement, followed by tumor regression and stabilization on decreasing steroid doses with sustained partial response – was observed in four of the children with brain stem glioma, said Dr. Pollack, who is also codirector of the University of Pittsburgh Cancer Institute’s brain tumor program.
Results of the ELISPOT (enzyme-linked immunosorbent spot) assay, which was completed in seven of the children, showed responses in six of them. Specifically, the investigators observed responses to IL-13RA2 in five cases, EphA2 in three cases, and survivin in three cases, Dr. Pollack said.
"Based on what we’ve seen so far, it seems that these kids are able to mount immune responses to the vaccine at high rates, possibly higher than we’ve seen in adult studies," likely because of their robust immune systems, he said in an interview.
The observation of immunologic and clinical response – particularly the evidence of tumor shrinkage in children with very high-risk tumors – "has been extremely encouraging and somewhat surprising," Dr. Pollack reported. "This is the first study of its type that examined peptide vaccine therapy for children with brain tumors like this."
The findings are especially notable because children with these tumors generally do not respond well to standard chemotherapy, he said, stressing that if further study validates the early findings, "immunotherapy may be a promising strategy to control tumor growth."
The study was funded by the National Institutes of Health. Dr. Pollack disclosed having no potential conflicts of interest.
CHICAGO – Immunotherapy with peptide vaccines may offer a much-needed therapeutic option for gliomas in children, which carry a poor prognosis despite current treatments.
In a pilot trial of subcutaneous vaccinations with peptides for glioma-associated antigen (GAA) epitopes in children who have been newly diagnosed with brain stem gliomas, cerebral high-grade gliomas, or recurrent gliomas, the immunotherapy was well tolerated and demonstrated immunologic and clinical activity, Dr. Ian F. Pollack reported April 2 at the annual meeting of the American Association for Cancer Research.
Based on significant experience with immunotherapy for adult gliomas, "we extended these insights to childhood gliomas – malignant astrocytomas of the brain stem and cerebral hemispheres and recurrent low-grade gliomas – based on our observations of their glioma-associated antigen expression profiles," Dr. Pollack explained during a press conference.
For the pilot study, Dr. Pollack, chief of pediatric neurosurgery at Children’s Hospital of Pittsburgh Brain Care Institute, and his colleagues have enrolled 27 human leukocyte antigen (HLA) A2–positive children to date, including 16 who are newly diagnosed with brain stem gliomas, 5 with newly diagnosed high-grade gliomas, and 6 with recurrent gliomas. The GAAs were EphA2, interleukin-13 receptor alpha 2 (IL-13RA2), and survivin, he said.
All of the children received eight courses of subcutaneous vaccinations with peptides for GAA epitopes emulsified in Montanide-ISA-51 every 3 weeks, along with intramuscular injections of the immunoadjuvant poly-ICLC, which promotes the infiltration of effector T cells into intracranial gliomas.
"Our primary end points were safety and T-cell response against vaccine-targeted [GAAs]," he said, noting that treatment response was assessed clinically and by MRI.
The preliminary results reported at the meeting are based on an interim analysis of 22 evaluable patients. To date, no non–central nervous system toxicities have limited the vaccine dosages, Dr. Pollack said. Of the 22 children, 4 showed signs of rapidly progressive disease, 14 had stable disease for more than 3 months, 3 had sustained partial responses, and 1 had prolonged disease-free status after surgery, he reported.
Symptomatic "pseudoprogression" – consisting of transient neurologic deterioration and tumor enlargement, followed by tumor regression and stabilization on decreasing steroid doses with sustained partial response – was observed in four of the children with brain stem glioma, said Dr. Pollack, who is also codirector of the University of Pittsburgh Cancer Institute’s brain tumor program.
Results of the ELISPOT (enzyme-linked immunosorbent spot) assay, which was completed in seven of the children, showed responses in six of them. Specifically, the investigators observed responses to IL-13RA2 in five cases, EphA2 in three cases, and survivin in three cases, Dr. Pollack said.
"Based on what we’ve seen so far, it seems that these kids are able to mount immune responses to the vaccine at high rates, possibly higher than we’ve seen in adult studies," likely because of their robust immune systems, he said in an interview.
The observation of immunologic and clinical response – particularly the evidence of tumor shrinkage in children with very high-risk tumors – "has been extremely encouraging and somewhat surprising," Dr. Pollack reported. "This is the first study of its type that examined peptide vaccine therapy for children with brain tumors like this."
The findings are especially notable because children with these tumors generally do not respond well to standard chemotherapy, he said, stressing that if further study validates the early findings, "immunotherapy may be a promising strategy to control tumor growth."
The study was funded by the National Institutes of Health. Dr. Pollack disclosed having no potential conflicts of interest.
CHICAGO – Immunotherapy with peptide vaccines may offer a much-needed therapeutic option for gliomas in children, which carry a poor prognosis despite current treatments.
In a pilot trial of subcutaneous vaccinations with peptides for glioma-associated antigen (GAA) epitopes in children who have been newly diagnosed with brain stem gliomas, cerebral high-grade gliomas, or recurrent gliomas, the immunotherapy was well tolerated and demonstrated immunologic and clinical activity, Dr. Ian F. Pollack reported April 2 at the annual meeting of the American Association for Cancer Research.
Based on significant experience with immunotherapy for adult gliomas, "we extended these insights to childhood gliomas – malignant astrocytomas of the brain stem and cerebral hemispheres and recurrent low-grade gliomas – based on our observations of their glioma-associated antigen expression profiles," Dr. Pollack explained during a press conference.
For the pilot study, Dr. Pollack, chief of pediatric neurosurgery at Children’s Hospital of Pittsburgh Brain Care Institute, and his colleagues have enrolled 27 human leukocyte antigen (HLA) A2–positive children to date, including 16 who are newly diagnosed with brain stem gliomas, 5 with newly diagnosed high-grade gliomas, and 6 with recurrent gliomas. The GAAs were EphA2, interleukin-13 receptor alpha 2 (IL-13RA2), and survivin, he said.
All of the children received eight courses of subcutaneous vaccinations with peptides for GAA epitopes emulsified in Montanide-ISA-51 every 3 weeks, along with intramuscular injections of the immunoadjuvant poly-ICLC, which promotes the infiltration of effector T cells into intracranial gliomas.
"Our primary end points were safety and T-cell response against vaccine-targeted [GAAs]," he said, noting that treatment response was assessed clinically and by MRI.
The preliminary results reported at the meeting are based on an interim analysis of 22 evaluable patients. To date, no non–central nervous system toxicities have limited the vaccine dosages, Dr. Pollack said. Of the 22 children, 4 showed signs of rapidly progressive disease, 14 had stable disease for more than 3 months, 3 had sustained partial responses, and 1 had prolonged disease-free status after surgery, he reported.
Symptomatic "pseudoprogression" – consisting of transient neurologic deterioration and tumor enlargement, followed by tumor regression and stabilization on decreasing steroid doses with sustained partial response – was observed in four of the children with brain stem glioma, said Dr. Pollack, who is also codirector of the University of Pittsburgh Cancer Institute’s brain tumor program.
Results of the ELISPOT (enzyme-linked immunosorbent spot) assay, which was completed in seven of the children, showed responses in six of them. Specifically, the investigators observed responses to IL-13RA2 in five cases, EphA2 in three cases, and survivin in three cases, Dr. Pollack said.
"Based on what we’ve seen so far, it seems that these kids are able to mount immune responses to the vaccine at high rates, possibly higher than we’ve seen in adult studies," likely because of their robust immune systems, he said in an interview.
The observation of immunologic and clinical response – particularly the evidence of tumor shrinkage in children with very high-risk tumors – "has been extremely encouraging and somewhat surprising," Dr. Pollack reported. "This is the first study of its type that examined peptide vaccine therapy for children with brain tumors like this."
The findings are especially notable because children with these tumors generally do not respond well to standard chemotherapy, he said, stressing that if further study validates the early findings, "immunotherapy may be a promising strategy to control tumor growth."
The study was funded by the National Institutes of Health. Dr. Pollack disclosed having no potential conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR CANCER RESEARCH
Major Finding: Of 22 children with HLA A2–positive gliomas receiving eight courses of subcutaneous peptide vaccination, 4 showed signs of rapidly progressive disease, 14 had stable disease for more than 3 months, 3 had sustained partial responses, and 1 had prolonged disease-free status.
Data Source: The interim results are from a pilot trial of subcutaneous peptide vaccine in children with newly diagnosed gliomas.
Disclosures: Dr. Pollack disclosed no conflicts of interest.
Older Women May Not Need Radiation for Luminal A Breast Tumors
CHICAGO – Older breast cancer patients with the luminal A tumor subtype may be able to forgo whole breast radiation therapy if they are taking tamoxifen or other breast cancer hormone therapy.
Preliminary results from a randomized clinical trial of tamoxifen with and without radiation therapy showed that radiation therapy had minimal impact on the risk of developing ipsilateral breast tumor recurrence in patients aged 50 years and older with T1 and T2 node-negative breast cancer identified with luminal A disease based on 6-marker immunohistochemistry testing.

In contrast, radiation therapy appeared to decrease the risk of breast cancer relapse in patients with luminal B, human epidermal growth factor receptor 2 (HER2)–enriched, and basal tumor subtypes, according to radiation oncologist Dr. Fei-Fei Liu of Princess Margaret Hospital, the Ontario Cancer Institute, and the University of Toronto, all in Toronto. She discussed the findings in a press conference April 1 at the annual meeting of the American Association for Cancer Research.
Luminal A tumors – estrogen receptor (ER) or progesterone receptor (PR) positive, HER2-negative, and low Ki-67 (a nuclear marker for cell proliferation) – are associated with a relatively good prognosis compared with the other subtypes, she noted.
To determine the predictive value of tumor subtype for ipsilateral recurrence in this population, Dr. Liu and her colleagues performed molecular subtyping for ER, PR, Ki-67, HER2, EGFR, and cytokeratine 5/6 on 304 available tumor specimens from 769 women in a clinical trial. All had been randomized to treatment with tamoxifen and whole breast radiation or tamoxifen alone between December 1992 and June 2000.
Based on the subtyping results, the patients were classified as luminal A, luminal B, luminal HER2, HER2-enriched, basal-like, or triple-negative phenotype–non-basal and followed for a median of 10 years, she said.
In the overall group of 769 women, the recurrence rate at a median of 10 years was 13.8% in the tamoxifen-only group and 5.0% in the combination group, Dr. Liu reported, noting that, in a multivariate analysis, "patient age, tumor size, estrogen-receptor positive status, and combination tamoxifen/whole breast radiation therapy were all significant factors."
Of the 304 tissue microarrays, 145 came from patients treated with tamoxifen only and 159 from patients treated with tamoxifen plus radiotherapy. In this population, the best outcomes were observed in 133 patients with luminal A tumors; their rate of ipsilateral recurrence was statistically similar at 8% among those in the tamoxifen-only group and 4.6% in the tamoxifen plus radiation group, Dr. Liu reported.
The 103 women older than 60 years with luminal A tumors fared particularly well, with rates of 4.3% with tamoxifen alone and 6.0% with tamoxifen and radiotherapy. The respective rates for the 114 women with grade I-II luminal A tumors also were similar at 4.9% and 5.5%, she said.
In contrast, the ipsilateral recurrence rates for the tamoxifen only and tamoxifen plus radiation groups were, respectively, 16.1% and 3.9% in 82 patients with luminal B tumors (differentiated from luminal A tumors by Ki-67 expression greater than 14%), said Dr. Liu.
Further, although the number of HER2 (11), HER2-enriched (11), and basal-like tumors (16) were small, "we saw higher relapse rates in patients who did not undergo radiation therapy," she said.
Luminal A lymph-node negative breast cancer represents approximately 25% of all cases of newly diagnosed breast cancer in North America, according to Dr. Liu. In addition to sparing a large number of women unnecessary radiation exposures, unwanted side effects, and inconvenience, bypassing radiation therapy in early cases would save millions of health care dollars each year.
"We estimated a savings of $20 million annually in Ontario if radiation therapy were avoided in early luminal A [breast cancer]," she said. "Extrapolating the figures to the [United States] resulted in a savings of about $400 million per year."
Dr. Liu stressed that the data presented at the meeting are preliminary but noted that, if the findings are validated through the analysis of a larger number of tumor samples, "we would recommend adding Ki-67 to the current standard immunohistochemistry panel, and discussing the possibility of avoiding radiation with lymph node–negative patients in whom the luminal A subtype is identified, if they are taking tamoxifen or an equivalent medication, especially patients who are 60 years old or older."
Dr. Liu disclosed no conflicts of interest.
CHICAGO – Older breast cancer patients with the luminal A tumor subtype may be able to forgo whole breast radiation therapy if they are taking tamoxifen or other breast cancer hormone therapy.
Preliminary results from a randomized clinical trial of tamoxifen with and without radiation therapy showed that radiation therapy had minimal impact on the risk of developing ipsilateral breast tumor recurrence in patients aged 50 years and older with T1 and T2 node-negative breast cancer identified with luminal A disease based on 6-marker immunohistochemistry testing.
In contrast, radiation therapy appeared to decrease the risk of breast cancer relapse in patients with luminal B, human epidermal growth factor receptor 2 (HER2)–enriched, and basal tumor subtypes, according to radiation oncologist Dr. Fei-Fei Liu of Princess Margaret Hospital, the Ontario Cancer Institute, and the University of Toronto, all in Toronto. She discussed the findings in a press conference April 1 at the annual meeting of the American Association for Cancer Research.
Luminal A tumors – estrogen receptor (ER) or progesterone receptor (PR) positive, HER2-negative, and low Ki-67 (a nuclear marker for cell proliferation) – are associated with a relatively good prognosis compared with the other subtypes, she noted.
To determine the predictive value of tumor subtype for ipsilateral recurrence in this population, Dr. Liu and her colleagues performed molecular subtyping for ER, PR, Ki-67, HER2, EGFR, and cytokeratine 5/6 on 304 available tumor specimens from 769 women in a clinical trial. All had been randomized to treatment with tamoxifen and whole breast radiation or tamoxifen alone between December 1992 and June 2000.
Based on the subtyping results, the patients were classified as luminal A, luminal B, luminal HER2, HER2-enriched, basal-like, or triple-negative phenotype–non-basal and followed for a median of 10 years, she said.
In the overall group of 769 women, the recurrence rate at a median of 10 years was 13.8% in the tamoxifen-only group and 5.0% in the combination group, Dr. Liu reported, noting that, in a multivariate analysis, "patient age, tumor size, estrogen-receptor positive status, and combination tamoxifen/whole breast radiation therapy were all significant factors."
Of the 304 tissue microarrays, 145 came from patients treated with tamoxifen only and 159 from patients treated with tamoxifen plus radiotherapy. In this population, the best outcomes were observed in 133 patients with luminal A tumors; their rate of ipsilateral recurrence was statistically similar at 8% among those in the tamoxifen-only group and 4.6% in the tamoxifen plus radiation group, Dr. Liu reported.
The 103 women older than 60 years with luminal A tumors fared particularly well, with rates of 4.3% with tamoxifen alone and 6.0% with tamoxifen and radiotherapy. The respective rates for the 114 women with grade I-II luminal A tumors also were similar at 4.9% and 5.5%, she said.
In contrast, the ipsilateral recurrence rates for the tamoxifen only and tamoxifen plus radiation groups were, respectively, 16.1% and 3.9% in 82 patients with luminal B tumors (differentiated from luminal A tumors by Ki-67 expression greater than 14%), said Dr. Liu.
Further, although the number of HER2 (11), HER2-enriched (11), and basal-like tumors (16) were small, "we saw higher relapse rates in patients who did not undergo radiation therapy," she said.
Luminal A lymph-node negative breast cancer represents approximately 25% of all cases of newly diagnosed breast cancer in North America, according to Dr. Liu. In addition to sparing a large number of women unnecessary radiation exposures, unwanted side effects, and inconvenience, bypassing radiation therapy in early cases would save millions of health care dollars each year.
"We estimated a savings of $20 million annually in Ontario if radiation therapy were avoided in early luminal A [breast cancer]," she said. "Extrapolating the figures to the [United States] resulted in a savings of about $400 million per year."
Dr. Liu stressed that the data presented at the meeting are preliminary but noted that, if the findings are validated through the analysis of a larger number of tumor samples, "we would recommend adding Ki-67 to the current standard immunohistochemistry panel, and discussing the possibility of avoiding radiation with lymph node–negative patients in whom the luminal A subtype is identified, if they are taking tamoxifen or an equivalent medication, especially patients who are 60 years old or older."
Dr. Liu disclosed no conflicts of interest.
CHICAGO – Older breast cancer patients with the luminal A tumor subtype may be able to forgo whole breast radiation therapy if they are taking tamoxifen or other breast cancer hormone therapy.
Preliminary results from a randomized clinical trial of tamoxifen with and without radiation therapy showed that radiation therapy had minimal impact on the risk of developing ipsilateral breast tumor recurrence in patients aged 50 years and older with T1 and T2 node-negative breast cancer identified with luminal A disease based on 6-marker immunohistochemistry testing.
In contrast, radiation therapy appeared to decrease the risk of breast cancer relapse in patients with luminal B, human epidermal growth factor receptor 2 (HER2)–enriched, and basal tumor subtypes, according to radiation oncologist Dr. Fei-Fei Liu of Princess Margaret Hospital, the Ontario Cancer Institute, and the University of Toronto, all in Toronto. She discussed the findings in a press conference April 1 at the annual meeting of the American Association for Cancer Research.
Luminal A tumors – estrogen receptor (ER) or progesterone receptor (PR) positive, HER2-negative, and low Ki-67 (a nuclear marker for cell proliferation) – are associated with a relatively good prognosis compared with the other subtypes, she noted.
To determine the predictive value of tumor subtype for ipsilateral recurrence in this population, Dr. Liu and her colleagues performed molecular subtyping for ER, PR, Ki-67, HER2, EGFR, and cytokeratine 5/6 on 304 available tumor specimens from 769 women in a clinical trial. All had been randomized to treatment with tamoxifen and whole breast radiation or tamoxifen alone between December 1992 and June 2000.
Based on the subtyping results, the patients were classified as luminal A, luminal B, luminal HER2, HER2-enriched, basal-like, or triple-negative phenotype–non-basal and followed for a median of 10 years, she said.
In the overall group of 769 women, the recurrence rate at a median of 10 years was 13.8% in the tamoxifen-only group and 5.0% in the combination group, Dr. Liu reported, noting that, in a multivariate analysis, "patient age, tumor size, estrogen-receptor positive status, and combination tamoxifen/whole breast radiation therapy were all significant factors."
Of the 304 tissue microarrays, 145 came from patients treated with tamoxifen only and 159 from patients treated with tamoxifen plus radiotherapy. In this population, the best outcomes were observed in 133 patients with luminal A tumors; their rate of ipsilateral recurrence was statistically similar at 8% among those in the tamoxifen-only group and 4.6% in the tamoxifen plus radiation group, Dr. Liu reported.
The 103 women older than 60 years with luminal A tumors fared particularly well, with rates of 4.3% with tamoxifen alone and 6.0% with tamoxifen and radiotherapy. The respective rates for the 114 women with grade I-II luminal A tumors also were similar at 4.9% and 5.5%, she said.
In contrast, the ipsilateral recurrence rates for the tamoxifen only and tamoxifen plus radiation groups were, respectively, 16.1% and 3.9% in 82 patients with luminal B tumors (differentiated from luminal A tumors by Ki-67 expression greater than 14%), said Dr. Liu.
Further, although the number of HER2 (11), HER2-enriched (11), and basal-like tumors (16) were small, "we saw higher relapse rates in patients who did not undergo radiation therapy," she said.
Luminal A lymph-node negative breast cancer represents approximately 25% of all cases of newly diagnosed breast cancer in North America, according to Dr. Liu. In addition to sparing a large number of women unnecessary radiation exposures, unwanted side effects, and inconvenience, bypassing radiation therapy in early cases would save millions of health care dollars each year.
"We estimated a savings of $20 million annually in Ontario if radiation therapy were avoided in early luminal A [breast cancer]," she said. "Extrapolating the figures to the [United States] resulted in a savings of about $400 million per year."
Dr. Liu stressed that the data presented at the meeting are preliminary but noted that, if the findings are validated through the analysis of a larger number of tumor samples, "we would recommend adding Ki-67 to the current standard immunohistochemistry panel, and discussing the possibility of avoiding radiation with lymph node–negative patients in whom the luminal A subtype is identified, if they are taking tamoxifen or an equivalent medication, especially patients who are 60 years old or older."
Dr. Liu disclosed no conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR CANCER RESEARCH
Major Finding: The rate of ipsilateral breast tumor recurrence in women older than 60 years with luminal A tumor subtypes was 4.3% among those taking tamoxifen only and 6.0% among those undergoing whole breast radiation therapy in addition to tamoxifen.
Data Source: Investigators presented preliminary results from microarray analyses of 304 patients in a randomized clinical trial of tamoxifen with and without radiation therapy.
Disclosures: Dr. Liu disclosed no conflicts of interest.
Estrogen-Only HT Also Increases Breast Cancer Risk
CHICAGO – Long-term use of estrogen-only therapy increases the risk of postmenopausal women developing breast cancer, according to new data from the Nurses’ Health Study.
The finding, reported April 1 by Dr. Wendy Chen at the annual meeting of the American Association for Cancer Research, suggests that opting for progesterone-free hormone therapy for the treatment of menopause symptoms should not be considered the risk-free alternative to combination progesterone plus estrogen formulations.
Still, the absolute risks were small. During the study’s 1.57 million person-years of follow-up from 1980 through 2008, 5,631 incident invasive breast cancers were diagnosed and 884 of the women died of breast cancer.
To evaluate the breast cancer risk associated with long-term use of both combined and estrogen-only hormone therapy, Dr. Chen of Brigham and Women’s Hospital in Boston and her colleagues evaluated data collected over 28 years through the Nurses’ Health Study. Of the 121,700 study participants who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those women not on hormone therapy (HT).
"Our data also confirmed the previously reported increased risk associated with combined hormone therapy," Dr. Chen stated, noting that women in the study who used progesterone plus estrogen for 10-14.9 years had an 88% increased risk of developing breast cancer relative to those not on HT and the risk increased to more than twofold in women using it for up to 20 years. Further, the risk of developing breast cancer does not appear to plateau over time, but rather continues to increase. "The longer women use [HT]. The higher their risk," she said.
In a separate analysis, the investigators restricted the study population to healthy, active postmenopausal women 50-79 years with an intact uterus – the same population observed in the Women’s Health Initiative. "What we saw was a decline in breast cancer risk among women using estrogen-only therapy for less than 10 years, but an increased risk among those women using estrogen for 15-20 years," Dr. Chen said.
Importantly, although breast cancer incidence was increased in the HT groups, "there was no increase in the risk of fatal breast cancer, either with combined or estrogen-only therapy," Dr. Chen stressed. "This is something we are continuing to investigate."
The findings have the potential to increase the confusion regarding HT and to perhaps reignite the hormone therapy debate, Dr. Chen acknowledged in an interview. However, they should be considered in their proper context. "While the relative risk of developing breast cancer in increased, the absolute risk associated with [HT] are low," she said.
The observed effects associated with HT were stronger for estrogen receptor–positive tumors and among thinner women, Dr. Chen noted, adding that the results were similar when limited to women who underwent regular breast cancer screening.
The study was funded by the National Cancer Institute. Dr. Chen disclosed no financial conflicts of interest.
CHICAGO – Long-term use of estrogen-only therapy increases the risk of postmenopausal women developing breast cancer, according to new data from the Nurses’ Health Study.
The finding, reported April 1 by Dr. Wendy Chen at the annual meeting of the American Association for Cancer Research, suggests that opting for progesterone-free hormone therapy for the treatment of menopause symptoms should not be considered the risk-free alternative to combination progesterone plus estrogen formulations.
Still, the absolute risks were small. During the study’s 1.57 million person-years of follow-up from 1980 through 2008, 5,631 incident invasive breast cancers were diagnosed and 884 of the women died of breast cancer.
To evaluate the breast cancer risk associated with long-term use of both combined and estrogen-only hormone therapy, Dr. Chen of Brigham and Women’s Hospital in Boston and her colleagues evaluated data collected over 28 years through the Nurses’ Health Study. Of the 121,700 study participants who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those women not on hormone therapy (HT).
"Our data also confirmed the previously reported increased risk associated with combined hormone therapy," Dr. Chen stated, noting that women in the study who used progesterone plus estrogen for 10-14.9 years had an 88% increased risk of developing breast cancer relative to those not on HT and the risk increased to more than twofold in women using it for up to 20 years. Further, the risk of developing breast cancer does not appear to plateau over time, but rather continues to increase. "The longer women use [HT]. The higher their risk," she said.
In a separate analysis, the investigators restricted the study population to healthy, active postmenopausal women 50-79 years with an intact uterus – the same population observed in the Women’s Health Initiative. "What we saw was a decline in breast cancer risk among women using estrogen-only therapy for less than 10 years, but an increased risk among those women using estrogen for 15-20 years," Dr. Chen said.
Importantly, although breast cancer incidence was increased in the HT groups, "there was no increase in the risk of fatal breast cancer, either with combined or estrogen-only therapy," Dr. Chen stressed. "This is something we are continuing to investigate."
The findings have the potential to increase the confusion regarding HT and to perhaps reignite the hormone therapy debate, Dr. Chen acknowledged in an interview. However, they should be considered in their proper context. "While the relative risk of developing breast cancer in increased, the absolute risk associated with [HT] are low," she said.
The observed effects associated with HT were stronger for estrogen receptor–positive tumors and among thinner women, Dr. Chen noted, adding that the results were similar when limited to women who underwent regular breast cancer screening.
The study was funded by the National Cancer Institute. Dr. Chen disclosed no financial conflicts of interest.
CHICAGO – Long-term use of estrogen-only therapy increases the risk of postmenopausal women developing breast cancer, according to new data from the Nurses’ Health Study.
The finding, reported April 1 by Dr. Wendy Chen at the annual meeting of the American Association for Cancer Research, suggests that opting for progesterone-free hormone therapy for the treatment of menopause symptoms should not be considered the risk-free alternative to combination progesterone plus estrogen formulations.
Still, the absolute risks were small. During the study’s 1.57 million person-years of follow-up from 1980 through 2008, 5,631 incident invasive breast cancers were diagnosed and 884 of the women died of breast cancer.
To evaluate the breast cancer risk associated with long-term use of both combined and estrogen-only hormone therapy, Dr. Chen of Brigham and Women’s Hospital in Boston and her colleagues evaluated data collected over 28 years through the Nurses’ Health Study. Of the 121,700 study participants who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those women not on hormone therapy (HT).
"Our data also confirmed the previously reported increased risk associated with combined hormone therapy," Dr. Chen stated, noting that women in the study who used progesterone plus estrogen for 10-14.9 years had an 88% increased risk of developing breast cancer relative to those not on HT and the risk increased to more than twofold in women using it for up to 20 years. Further, the risk of developing breast cancer does not appear to plateau over time, but rather continues to increase. "The longer women use [HT]. The higher their risk," she said.
In a separate analysis, the investigators restricted the study population to healthy, active postmenopausal women 50-79 years with an intact uterus – the same population observed in the Women’s Health Initiative. "What we saw was a decline in breast cancer risk among women using estrogen-only therapy for less than 10 years, but an increased risk among those women using estrogen for 15-20 years," Dr. Chen said.
Importantly, although breast cancer incidence was increased in the HT groups, "there was no increase in the risk of fatal breast cancer, either with combined or estrogen-only therapy," Dr. Chen stressed. "This is something we are continuing to investigate."
The findings have the potential to increase the confusion regarding HT and to perhaps reignite the hormone therapy debate, Dr. Chen acknowledged in an interview. However, they should be considered in their proper context. "While the relative risk of developing breast cancer in increased, the absolute risk associated with [HT] are low," she said.
The observed effects associated with HT were stronger for estrogen receptor–positive tumors and among thinner women, Dr. Chen noted, adding that the results were similar when limited to women who underwent regular breast cancer screening.
The study was funded by the National Cancer Institute. Dr. Chen disclosed no financial conflicts of interest.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION OF CANCER RESEARCH
Major Finding: Of the 121,700 study participants in the Nurses’ Health Study who were aged 30-55 years in 1976, women who used estrogen-only therapy for 10.0-14.9 years and for 15.0-19.9 years had, respectively, a 22% and 43% increased risk of developing breast cancer relative to those not on hormone therapy.
Data Source: The Nurses’ Health Study of data collected during 1980-2008 from 121,700 postmenopausal women aged 30-55 years in 1976.
Disclosures: Dr. Chen disclosed no financial conflicts of interest.
Cancer Incidence, Deaths Decline Overall; Obesity Threatens Setback
Fewer people are being diagnosed with and dying from cancer in the United States, thanks to advances in prevention, diagnosis, and treatment, but the growing obesity problem may slow the downward trend, according to an annual report to the nation.
Between 1999 and 2008, the rates of death from cancer decreased by an average of 1.7% per year for men, 1.3% per year for women, and 1.5% per year for children, investigators reported online ahead of print on March 29 in Cancer. All four of the most common cancers – lung, colorectal, breast, and prostate – had declines in their death rates.
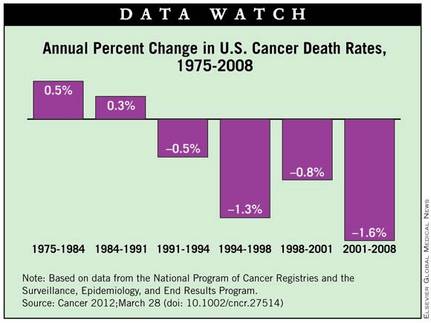
The incidence rates for several cancers associated with excess weight and lack of sufficient physical activity increased during the period of study, however. These included pancreatic cancer, kidney cancer, and adenocarcinomas of the esophagus.
Tobacco prevention and control contributed to the falling death rates, but more needs to be done on multiple levels to promote healthy weight and physical activity, concluded Christie Eheman, Ph.D., of the Centers for Disease Control and coauthors of the Annual Report to the Nation on the Status of Cancer, 1975-2008.
The report represents a collaboration of the CDC, the American Cancer Society, the National Cancer Institute, and the North American Association of Central Cancer Registries.
Cancer Incidence Declined in Adults but Rose in Children
Overall cancer incidence decreased by an average 0.6% among men from 1994 to 2008 and by an average of 0.5% among women from 1998 to 2006, remaining stable in 2006-2008.
In children, however, overall cancer incidence increased annually in 1998-2008 by 0.5% among children 0-14 years and by 0.6% among those 0-19 years, the authors wrote (Cancer 2012, March 29 [doi: 10.1002/cncr.27514]).
By individual cancer site, the incidence of colorectal and prostate cancers, as well as lung cancer in men, decreased during the 10-year and most recent 5-year (2004-2008) periods included in the report. The incidence of lung cancer in women also declined from 2004 to 2008.
During the same 5- and 10-year periods, "death rates increased for pancreatic cancer among both men and women, for liver cancer and melanoma of the skin among men, and for corpus uterus [uterine] cancer among women." Cervical cancer death rates saw little change, according to the authors.
Kidney cancer incidence increased across racial and ethnic groups in 1999-2008 by approximately 2.9% among men and 3.3% among women.
The incidence of pancreatic cancer increased by approximately 1.2% over the 10 years in white men and women; the incidence of uterine cancer increased significantly among black, Asian and Pacific Islander, and Hispanic women during that time.
Adenocarcinoma of the esophagus increased 2.6% annually among white and Hispanic men and 3.3% among white women.
Among racial and ethnic groups, in 2004-2008, black men and white women had the highest rates of cancer incidence, and black men and black women had the highest cancer mortality rates. These discrepancies could reflect differences in risk factors as well as access to and use of screening and treatment, the authors stated.
Progress Noted but With a Cautionary Note
The continued declines in overall cancer death rates since the 1990s among men and women overall and in nearly all racial and ethnic groups "indicate progress in cancer prevention and control," the authors wrote. "These decreases are largely a result of tobacco prevention and control efforts, screening and early detection of some cancers, and improvements in treatment for many cancers."
Despite improvements in the overall cancer burden, however, "excess weight and lack of sufficient physical activity contribute to the increased incidence of many cancers, adversely affect quality of life for cancer survivors, and may worsen prognosis for several cancers," they said.
As such, efforts to promote healthy weight and sufficient physical activity must be undertaken at multiple levels, rather than solely at the level of the individual, they stressed:
"Supporting recommended healthy lifestyle behaviors will require concerted actions from individuals; communities; the media; federal, state, and local governments; food industries; international agencies; and sectors beyond what is usually considered public health, such as transportation and agriculture."
Importantly, the authors concluded, "quality, population-based risk factor and cancer surveillance data can be used to identify areas and populations with unhealthy behaviors and high cancer rates that could benefit from targeted, effective strategies and interventions to improve health behaviors and support healthy environments."
Data on cancer incidence came from the CDC, NCI, and NAACCR, and data on cancer mortality from the CDC National Center for Health Statistics.
The authors disclosed no conflicts of interest.
Fewer people are being diagnosed with and dying from cancer in the United States, thanks to advances in prevention, diagnosis, and treatment, but the growing obesity problem may slow the downward trend, according to an annual report to the nation.
Between 1999 and 2008, the rates of death from cancer decreased by an average of 1.7% per year for men, 1.3% per year for women, and 1.5% per year for children, investigators reported online ahead of print on March 29 in Cancer. All four of the most common cancers – lung, colorectal, breast, and prostate – had declines in their death rates.
The incidence rates for several cancers associated with excess weight and lack of sufficient physical activity increased during the period of study, however. These included pancreatic cancer, kidney cancer, and adenocarcinomas of the esophagus.
Tobacco prevention and control contributed to the falling death rates, but more needs to be done on multiple levels to promote healthy weight and physical activity, concluded Christie Eheman, Ph.D., of the Centers for Disease Control and coauthors of the Annual Report to the Nation on the Status of Cancer, 1975-2008.
The report represents a collaboration of the CDC, the American Cancer Society, the National Cancer Institute, and the North American Association of Central Cancer Registries.
Cancer Incidence Declined in Adults but Rose in Children
Overall cancer incidence decreased by an average 0.6% among men from 1994 to 2008 and by an average of 0.5% among women from 1998 to 2006, remaining stable in 2006-2008.
In children, however, overall cancer incidence increased annually in 1998-2008 by 0.5% among children 0-14 years and by 0.6% among those 0-19 years, the authors wrote (Cancer 2012, March 29 [doi: 10.1002/cncr.27514]).
By individual cancer site, the incidence of colorectal and prostate cancers, as well as lung cancer in men, decreased during the 10-year and most recent 5-year (2004-2008) periods included in the report. The incidence of lung cancer in women also declined from 2004 to 2008.
During the same 5- and 10-year periods, "death rates increased for pancreatic cancer among both men and women, for liver cancer and melanoma of the skin among men, and for corpus uterus [uterine] cancer among women." Cervical cancer death rates saw little change, according to the authors.
Kidney cancer incidence increased across racial and ethnic groups in 1999-2008 by approximately 2.9% among men and 3.3% among women.
The incidence of pancreatic cancer increased by approximately 1.2% over the 10 years in white men and women; the incidence of uterine cancer increased significantly among black, Asian and Pacific Islander, and Hispanic women during that time.
Adenocarcinoma of the esophagus increased 2.6% annually among white and Hispanic men and 3.3% among white women.
Among racial and ethnic groups, in 2004-2008, black men and white women had the highest rates of cancer incidence, and black men and black women had the highest cancer mortality rates. These discrepancies could reflect differences in risk factors as well as access to and use of screening and treatment, the authors stated.
Progress Noted but With a Cautionary Note
The continued declines in overall cancer death rates since the 1990s among men and women overall and in nearly all racial and ethnic groups "indicate progress in cancer prevention and control," the authors wrote. "These decreases are largely a result of tobacco prevention and control efforts, screening and early detection of some cancers, and improvements in treatment for many cancers."
Despite improvements in the overall cancer burden, however, "excess weight and lack of sufficient physical activity contribute to the increased incidence of many cancers, adversely affect quality of life for cancer survivors, and may worsen prognosis for several cancers," they said.
As such, efforts to promote healthy weight and sufficient physical activity must be undertaken at multiple levels, rather than solely at the level of the individual, they stressed:
"Supporting recommended healthy lifestyle behaviors will require concerted actions from individuals; communities; the media; federal, state, and local governments; food industries; international agencies; and sectors beyond what is usually considered public health, such as transportation and agriculture."
Importantly, the authors concluded, "quality, population-based risk factor and cancer surveillance data can be used to identify areas and populations with unhealthy behaviors and high cancer rates that could benefit from targeted, effective strategies and interventions to improve health behaviors and support healthy environments."
Data on cancer incidence came from the CDC, NCI, and NAACCR, and data on cancer mortality from the CDC National Center for Health Statistics.
The authors disclosed no conflicts of interest.
Fewer people are being diagnosed with and dying from cancer in the United States, thanks to advances in prevention, diagnosis, and treatment, but the growing obesity problem may slow the downward trend, according to an annual report to the nation.
Between 1999 and 2008, the rates of death from cancer decreased by an average of 1.7% per year for men, 1.3% per year for women, and 1.5% per year for children, investigators reported online ahead of print on March 29 in Cancer. All four of the most common cancers – lung, colorectal, breast, and prostate – had declines in their death rates.
The incidence rates for several cancers associated with excess weight and lack of sufficient physical activity increased during the period of study, however. These included pancreatic cancer, kidney cancer, and adenocarcinomas of the esophagus.
Tobacco prevention and control contributed to the falling death rates, but more needs to be done on multiple levels to promote healthy weight and physical activity, concluded Christie Eheman, Ph.D., of the Centers for Disease Control and coauthors of the Annual Report to the Nation on the Status of Cancer, 1975-2008.
The report represents a collaboration of the CDC, the American Cancer Society, the National Cancer Institute, and the North American Association of Central Cancer Registries.
Cancer Incidence Declined in Adults but Rose in Children
Overall cancer incidence decreased by an average 0.6% among men from 1994 to 2008 and by an average of 0.5% among women from 1998 to 2006, remaining stable in 2006-2008.
In children, however, overall cancer incidence increased annually in 1998-2008 by 0.5% among children 0-14 years and by 0.6% among those 0-19 years, the authors wrote (Cancer 2012, March 29 [doi: 10.1002/cncr.27514]).
By individual cancer site, the incidence of colorectal and prostate cancers, as well as lung cancer in men, decreased during the 10-year and most recent 5-year (2004-2008) periods included in the report. The incidence of lung cancer in women also declined from 2004 to 2008.
During the same 5- and 10-year periods, "death rates increased for pancreatic cancer among both men and women, for liver cancer and melanoma of the skin among men, and for corpus uterus [uterine] cancer among women." Cervical cancer death rates saw little change, according to the authors.
Kidney cancer incidence increased across racial and ethnic groups in 1999-2008 by approximately 2.9% among men and 3.3% among women.
The incidence of pancreatic cancer increased by approximately 1.2% over the 10 years in white men and women; the incidence of uterine cancer increased significantly among black, Asian and Pacific Islander, and Hispanic women during that time.
Adenocarcinoma of the esophagus increased 2.6% annually among white and Hispanic men and 3.3% among white women.
Among racial and ethnic groups, in 2004-2008, black men and white women had the highest rates of cancer incidence, and black men and black women had the highest cancer mortality rates. These discrepancies could reflect differences in risk factors as well as access to and use of screening and treatment, the authors stated.
Progress Noted but With a Cautionary Note
The continued declines in overall cancer death rates since the 1990s among men and women overall and in nearly all racial and ethnic groups "indicate progress in cancer prevention and control," the authors wrote. "These decreases are largely a result of tobacco prevention and control efforts, screening and early detection of some cancers, and improvements in treatment for many cancers."
Despite improvements in the overall cancer burden, however, "excess weight and lack of sufficient physical activity contribute to the increased incidence of many cancers, adversely affect quality of life for cancer survivors, and may worsen prognosis for several cancers," they said.
As such, efforts to promote healthy weight and sufficient physical activity must be undertaken at multiple levels, rather than solely at the level of the individual, they stressed:
"Supporting recommended healthy lifestyle behaviors will require concerted actions from individuals; communities; the media; federal, state, and local governments; food industries; international agencies; and sectors beyond what is usually considered public health, such as transportation and agriculture."
Importantly, the authors concluded, "quality, population-based risk factor and cancer surveillance data can be used to identify areas and populations with unhealthy behaviors and high cancer rates that could benefit from targeted, effective strategies and interventions to improve health behaviors and support healthy environments."
Data on cancer incidence came from the CDC, NCI, and NAACCR, and data on cancer mortality from the CDC National Center for Health Statistics.
The authors disclosed no conflicts of interest.
FROM CANCER
Major Finding: The overall rates of death from cancer declined by an average of 1.7% among men, 1.3% among women, and 1.5% among children from 1999 to 2008.
Data Source: Data were taken from the Annual Report to the Nation on the Status of Cancer, 1975-2008.
Disclosures: The authors disclosed no conflicts of interest.
NCCN: Stratify Acute Lymphoblastic Leukemia Patients by Age
Management of acute lymphoblastic leukemia should be driven in large part by patient age, according to new clinical practice guidelines issued by the National Comprehensive Cancer Network.
Adolescents and young adults between the ages of 15 and 39 years benefit from the intensive therapies used to treat children, while older adults are thought to be less tolerant of the high-dose pediatric regimens, explained Dr. Patrick A. Brown.
"At this point, multiple studies have indicated that young adults with acute lymphoblastic leukemia [ALL] benefit significantly from pediatric-inspired treatments, and the new guidelines reflect this," said Dr. Brown, cochair of the NCCN panel that wrote the guidelines.
The treatment of older adults, on the other hand, is compromised relative to their younger counterparts, not only by their diminished tolerance of high-dose therapies but also by the presence in many adults of cytogenic abnormalities, including the translocation that results in the Philadelphia (Ph) chromosome, said Dr. Brown, director of the Pediatric Leukemia Program at the Kimmel Comprehensive Cancer Canter, Johns Hopkins University, Baltimore.
The Ph chromosome, a common feature in adult ALL patients but rare in children, leads to formation of the BCR-ABL fusion gene that is associated with a poor prognosis independent of age, he noted in an interview.
The new guidelines were presented March 17 at the conference in Hollywood, Fla.
They call for initial patient stratification based on Ph status and treatment of Ph-positive ALL patients with regimens that incorporate BCR-ABL-targeting tyrosine kinase inhibitors, such as imatinib (Gleevec). Imatinib is FDA approved for the treatment of adult patients with relapsed or refractory Ph-positive ALL.
Regarding treatment decisions, the guidelines recommend risk stratification by age, with adolescent and young adult patients aged 15-39 years being considered separately from the adult population 40 years and older. The guidelines also advocate that those 65 years and older be considered separately as well, but caution that "chronological age alone is a poor surrogate for determining patient fitness for therapy."
Consideration of allogeneic stem cell transplantation as a consolidation option following induction therapy in ALL patients should be based on Ph status and age, Dr. Brown said, noting that the guidelines recommend it for Ph-positive patients as well as PH-negative patients younger than 65 years who have high-risk features. These include elevated white blood cell count, hypodiploidy, or rearrangements of the mixed-lineage leukemia gene, not including those adult patients with preclusive comorbidities, such as organ dysfunction.
The guidelines also recommend:
• Central nervous system prophylaxis and treatment, including cranial irradiation, intrathecal chemotherapy, or high-dose systemic chemotherapy, throughout the course of therapy, from induction through maintenance, to clear leukemic cells from CNS sites that cannot be accessed by systemic chemotherapy because of the blood-brain barrier.
• Postinduction consolidation comprising drug combinations similar to those used during the induction phase, such as high-dose methotrexate, cytarabine, mercaptopurine, and l-asparaginase.
• Extended maintenance therapy for all patients (except those with mature B-cell ALL in whom relapses rarely occur beyond 12 months), typically comprising daily mercaptopurine and weekly methotrexate, often with periodic vincristine and corticosteroids, for 2 years in adults and 2-3 years in children.
• The possible inclusion of novel, immune-based agents that target specific genetic abnormalities, such as the BCR-ABL selective tyrosine kinase inhibitors for Ph-positive ALL, the anti-CD20 monoclonal antibody rituximab (Rituxan) for CD20-expression B-cell lineage ALL, and the adenosine deaminase substrate nelarabine (Arranon) for T-cell lineage ALL.
The NCCN guidelines also incorporate recommendations for minimal residual disease evaluation, provision of supportive care, and management of treatment-associated toxicities.
While the survival outcomes associated with ALL have improved dramatically among children in recent years – the cure rate with current treatment regimens is approximately 80% – the long-term prognosis for adults with the disease is poor, with cure rates of 30-40%, according to NCCN ALL guidelines panel member Dr. Daniel J. DeAngelo.
"ALL is the rarest form of adult leukemia, and we still have a lot of unanswered questions," said Dr. DeAngelo of the Dana-Farber Cancer Institute, Boston. "For this reason, adult patients with the disease should be referred to specialized cancer treatment centers and should be enrolled in clinical trials whenever possible."
Dr. Brown disclosed no relevant conflicts of interest. Dr. DeAngelo disclosed relationships with Bristol-Myers Squibb, Novartis, and Sigma-Tau Pharmaceuticals. The full list of disclosures for the NCCN ALL Guidelines Panel members can be found at http://www.nccn.org.
Management of acute lymphoblastic leukemia should be driven in large part by patient age, according to new clinical practice guidelines issued by the National Comprehensive Cancer Network.
Adolescents and young adults between the ages of 15 and 39 years benefit from the intensive therapies used to treat children, while older adults are thought to be less tolerant of the high-dose pediatric regimens, explained Dr. Patrick A. Brown.
"At this point, multiple studies have indicated that young adults with acute lymphoblastic leukemia [ALL] benefit significantly from pediatric-inspired treatments, and the new guidelines reflect this," said Dr. Brown, cochair of the NCCN panel that wrote the guidelines.
The treatment of older adults, on the other hand, is compromised relative to their younger counterparts, not only by their diminished tolerance of high-dose therapies but also by the presence in many adults of cytogenic abnormalities, including the translocation that results in the Philadelphia (Ph) chromosome, said Dr. Brown, director of the Pediatric Leukemia Program at the Kimmel Comprehensive Cancer Canter, Johns Hopkins University, Baltimore.
The Ph chromosome, a common feature in adult ALL patients but rare in children, leads to formation of the BCR-ABL fusion gene that is associated with a poor prognosis independent of age, he noted in an interview.
The new guidelines were presented March 17 at the conference in Hollywood, Fla.
They call for initial patient stratification based on Ph status and treatment of Ph-positive ALL patients with regimens that incorporate BCR-ABL-targeting tyrosine kinase inhibitors, such as imatinib (Gleevec). Imatinib is FDA approved for the treatment of adult patients with relapsed or refractory Ph-positive ALL.
Regarding treatment decisions, the guidelines recommend risk stratification by age, with adolescent and young adult patients aged 15-39 years being considered separately from the adult population 40 years and older. The guidelines also advocate that those 65 years and older be considered separately as well, but caution that "chronological age alone is a poor surrogate for determining patient fitness for therapy."
Consideration of allogeneic stem cell transplantation as a consolidation option following induction therapy in ALL patients should be based on Ph status and age, Dr. Brown said, noting that the guidelines recommend it for Ph-positive patients as well as PH-negative patients younger than 65 years who have high-risk features. These include elevated white blood cell count, hypodiploidy, or rearrangements of the mixed-lineage leukemia gene, not including those adult patients with preclusive comorbidities, such as organ dysfunction.
The guidelines also recommend:
• Central nervous system prophylaxis and treatment, including cranial irradiation, intrathecal chemotherapy, or high-dose systemic chemotherapy, throughout the course of therapy, from induction through maintenance, to clear leukemic cells from CNS sites that cannot be accessed by systemic chemotherapy because of the blood-brain barrier.
• Postinduction consolidation comprising drug combinations similar to those used during the induction phase, such as high-dose methotrexate, cytarabine, mercaptopurine, and l-asparaginase.
• Extended maintenance therapy for all patients (except those with mature B-cell ALL in whom relapses rarely occur beyond 12 months), typically comprising daily mercaptopurine and weekly methotrexate, often with periodic vincristine and corticosteroids, for 2 years in adults and 2-3 years in children.
• The possible inclusion of novel, immune-based agents that target specific genetic abnormalities, such as the BCR-ABL selective tyrosine kinase inhibitors for Ph-positive ALL, the anti-CD20 monoclonal antibody rituximab (Rituxan) for CD20-expression B-cell lineage ALL, and the adenosine deaminase substrate nelarabine (Arranon) for T-cell lineage ALL.
The NCCN guidelines also incorporate recommendations for minimal residual disease evaluation, provision of supportive care, and management of treatment-associated toxicities.
While the survival outcomes associated with ALL have improved dramatically among children in recent years – the cure rate with current treatment regimens is approximately 80% – the long-term prognosis for adults with the disease is poor, with cure rates of 30-40%, according to NCCN ALL guidelines panel member Dr. Daniel J. DeAngelo.
"ALL is the rarest form of adult leukemia, and we still have a lot of unanswered questions," said Dr. DeAngelo of the Dana-Farber Cancer Institute, Boston. "For this reason, adult patients with the disease should be referred to specialized cancer treatment centers and should be enrolled in clinical trials whenever possible."
Dr. Brown disclosed no relevant conflicts of interest. Dr. DeAngelo disclosed relationships with Bristol-Myers Squibb, Novartis, and Sigma-Tau Pharmaceuticals. The full list of disclosures for the NCCN ALL Guidelines Panel members can be found at http://www.nccn.org.
Management of acute lymphoblastic leukemia should be driven in large part by patient age, according to new clinical practice guidelines issued by the National Comprehensive Cancer Network.
Adolescents and young adults between the ages of 15 and 39 years benefit from the intensive therapies used to treat children, while older adults are thought to be less tolerant of the high-dose pediatric regimens, explained Dr. Patrick A. Brown.
"At this point, multiple studies have indicated that young adults with acute lymphoblastic leukemia [ALL] benefit significantly from pediatric-inspired treatments, and the new guidelines reflect this," said Dr. Brown, cochair of the NCCN panel that wrote the guidelines.
The treatment of older adults, on the other hand, is compromised relative to their younger counterparts, not only by their diminished tolerance of high-dose therapies but also by the presence in many adults of cytogenic abnormalities, including the translocation that results in the Philadelphia (Ph) chromosome, said Dr. Brown, director of the Pediatric Leukemia Program at the Kimmel Comprehensive Cancer Canter, Johns Hopkins University, Baltimore.
The Ph chromosome, a common feature in adult ALL patients but rare in children, leads to formation of the BCR-ABL fusion gene that is associated with a poor prognosis independent of age, he noted in an interview.
The new guidelines were presented March 17 at the conference in Hollywood, Fla.
They call for initial patient stratification based on Ph status and treatment of Ph-positive ALL patients with regimens that incorporate BCR-ABL-targeting tyrosine kinase inhibitors, such as imatinib (Gleevec). Imatinib is FDA approved for the treatment of adult patients with relapsed or refractory Ph-positive ALL.
Regarding treatment decisions, the guidelines recommend risk stratification by age, with adolescent and young adult patients aged 15-39 years being considered separately from the adult population 40 years and older. The guidelines also advocate that those 65 years and older be considered separately as well, but caution that "chronological age alone is a poor surrogate for determining patient fitness for therapy."
Consideration of allogeneic stem cell transplantation as a consolidation option following induction therapy in ALL patients should be based on Ph status and age, Dr. Brown said, noting that the guidelines recommend it for Ph-positive patients as well as PH-negative patients younger than 65 years who have high-risk features. These include elevated white blood cell count, hypodiploidy, or rearrangements of the mixed-lineage leukemia gene, not including those adult patients with preclusive comorbidities, such as organ dysfunction.
The guidelines also recommend:
• Central nervous system prophylaxis and treatment, including cranial irradiation, intrathecal chemotherapy, or high-dose systemic chemotherapy, throughout the course of therapy, from induction through maintenance, to clear leukemic cells from CNS sites that cannot be accessed by systemic chemotherapy because of the blood-brain barrier.
• Postinduction consolidation comprising drug combinations similar to those used during the induction phase, such as high-dose methotrexate, cytarabine, mercaptopurine, and l-asparaginase.
• Extended maintenance therapy for all patients (except those with mature B-cell ALL in whom relapses rarely occur beyond 12 months), typically comprising daily mercaptopurine and weekly methotrexate, often with periodic vincristine and corticosteroids, for 2 years in adults and 2-3 years in children.
• The possible inclusion of novel, immune-based agents that target specific genetic abnormalities, such as the BCR-ABL selective tyrosine kinase inhibitors for Ph-positive ALL, the anti-CD20 monoclonal antibody rituximab (Rituxan) for CD20-expression B-cell lineage ALL, and the adenosine deaminase substrate nelarabine (Arranon) for T-cell lineage ALL.
The NCCN guidelines also incorporate recommendations for minimal residual disease evaluation, provision of supportive care, and management of treatment-associated toxicities.
While the survival outcomes associated with ALL have improved dramatically among children in recent years – the cure rate with current treatment regimens is approximately 80% – the long-term prognosis for adults with the disease is poor, with cure rates of 30-40%, according to NCCN ALL guidelines panel member Dr. Daniel J. DeAngelo.
"ALL is the rarest form of adult leukemia, and we still have a lot of unanswered questions," said Dr. DeAngelo of the Dana-Farber Cancer Institute, Boston. "For this reason, adult patients with the disease should be referred to specialized cancer treatment centers and should be enrolled in clinical trials whenever possible."
Dr. Brown disclosed no relevant conflicts of interest. Dr. DeAngelo disclosed relationships with Bristol-Myers Squibb, Novartis, and Sigma-Tau Pharmaceuticals. The full list of disclosures for the NCCN ALL Guidelines Panel members can be found at http://www.nccn.org.
FROM THE ANNUAL CONFERENCE OF THE NATIONAL COMPREHENSIVE CANCER NETWORK