User login
Screen for Depression in Sleep Apnea Patients
ORLANDO — Obstructive sleep apnea patients with symptoms of excessive sleepiness have the greatest risk of depression, based on data from a prospective study of 107 adults.
Data from previous studies have shown that self-reported depression is more common among women with obstructive sleep apnea (OSA) compared with men with OSA, but data on the relationship among depression, severity of OSA, and sleepiness are limited, said Dr. Stacey Ishman of Johns Hopkins University, Baltimore.
Dr. Ishman and her colleagues evaluated 56 consecutive OSA patients aged 27-74 years who presented to an otolaryngology clinic and compared them with 51 controls. The average age of patients and controls alike was 47 years. A total of 61% of the OSA patients were male.
Overall, significantly more OSA patients met the criteria for depression, compared with controls (29% vs. 8%). The severity of OSA (measured using the Respiratory Disturbance Index) was a significant predictor of Beck Depression Inventory (BDI) scores, but BDI scores were not correlated with the severity of OSA.
These findings suggest that “depression may be significant even in patients with mild OSA,” Dr. Ishman said at the meeting jointly sponsored by the Triological Society and the American College of Surgeons. BDI scores were significantly correlated with higher Epworth Sleepiness Scale (ESS) scores, but the ESS did not correlate with sleep apnea severity.
Disclosures: Dr. Ishman had no financial conflicts to disclose.
ORLANDO — Obstructive sleep apnea patients with symptoms of excessive sleepiness have the greatest risk of depression, based on data from a prospective study of 107 adults.
Data from previous studies have shown that self-reported depression is more common among women with obstructive sleep apnea (OSA) compared with men with OSA, but data on the relationship among depression, severity of OSA, and sleepiness are limited, said Dr. Stacey Ishman of Johns Hopkins University, Baltimore.
Dr. Ishman and her colleagues evaluated 56 consecutive OSA patients aged 27-74 years who presented to an otolaryngology clinic and compared them with 51 controls. The average age of patients and controls alike was 47 years. A total of 61% of the OSA patients were male.
Overall, significantly more OSA patients met the criteria for depression, compared with controls (29% vs. 8%). The severity of OSA (measured using the Respiratory Disturbance Index) was a significant predictor of Beck Depression Inventory (BDI) scores, but BDI scores were not correlated with the severity of OSA.
These findings suggest that “depression may be significant even in patients with mild OSA,” Dr. Ishman said at the meeting jointly sponsored by the Triological Society and the American College of Surgeons. BDI scores were significantly correlated with higher Epworth Sleepiness Scale (ESS) scores, but the ESS did not correlate with sleep apnea severity.
Disclosures: Dr. Ishman had no financial conflicts to disclose.
ORLANDO — Obstructive sleep apnea patients with symptoms of excessive sleepiness have the greatest risk of depression, based on data from a prospective study of 107 adults.
Data from previous studies have shown that self-reported depression is more common among women with obstructive sleep apnea (OSA) compared with men with OSA, but data on the relationship among depression, severity of OSA, and sleepiness are limited, said Dr. Stacey Ishman of Johns Hopkins University, Baltimore.
Dr. Ishman and her colleagues evaluated 56 consecutive OSA patients aged 27-74 years who presented to an otolaryngology clinic and compared them with 51 controls. The average age of patients and controls alike was 47 years. A total of 61% of the OSA patients were male.
Overall, significantly more OSA patients met the criteria for depression, compared with controls (29% vs. 8%). The severity of OSA (measured using the Respiratory Disturbance Index) was a significant predictor of Beck Depression Inventory (BDI) scores, but BDI scores were not correlated with the severity of OSA.
These findings suggest that “depression may be significant even in patients with mild OSA,” Dr. Ishman said at the meeting jointly sponsored by the Triological Society and the American College of Surgeons. BDI scores were significantly correlated with higher Epworth Sleepiness Scale (ESS) scores, but the ESS did not correlate with sleep apnea severity.
Disclosures: Dr. Ishman had no financial conflicts to disclose.
Screen for Depression in Obstructive Sleep Apnea Patients
Major Finding: 29% of patients with OSA met criteria for depression, compared with 8% of controls.
Data Source: Prospective study of 56 obstructive sleep apnea patients at an otolaryngology clinic.
Disclosures: Dr. Ishman had no financial conflicts.
ORLANDO — Obstructive sleep apnea patients with symptoms of excessive sleepiness have the greatest risk of depression, based on data from a prospective study of 107 adults.
Data from previous studies have shown that self-reported depression is more common among women with obstructive sleep apnea (OSA) compared with men with OSA, but data on the relationship among depression, severity of OSA, and sleepiness are limited, said Dr. Stacey Ishman of Johns Hopkins University, Baltimore.
Dr. Ishman and her colleagues evaluated 56 consecutive OSA patients aged 27-74 years who presented to an otolaryngology clinic and compared them with 51 controls. The average age of patients and controls was 47 years; 61% of the OSA patients were male.
Overall, significantly more OSA patients met the criteria for depression, compared with controls (29% vs. 8%). The severity of OSA (measured using the Respiratory Disturbance Index) was a significant predictor of Beck Depression Inventory (BDI) scores, but BDI scores were not correlated with the severity of OSA.
These findings suggest that “depression may be significant even in patients with mild OSA,” Dr. Ishman said at the meeting jointly sponsored by the Triological Society and the American College of Surgeons.
BDI scores were significantly correlated with higher scores on the Epworth Sleepiness Scale (ESS), but the ESS did not correlate with the severity of sleep apnea. However, findings from previous studies have shown that more than 50% of individuals with severe OSA (an apnea-hypopnea index of at least 30 events/hour) do not report subjective sleepiness, she noted.
The relationship between BDI and ESS suggests that OSA patients with excessive sleepiness in particular might benefit from depression screening, she said.
Major Finding: 29% of patients with OSA met criteria for depression, compared with 8% of controls.
Data Source: Prospective study of 56 obstructive sleep apnea patients at an otolaryngology clinic.
Disclosures: Dr. Ishman had no financial conflicts.
ORLANDO — Obstructive sleep apnea patients with symptoms of excessive sleepiness have the greatest risk of depression, based on data from a prospective study of 107 adults.
Data from previous studies have shown that self-reported depression is more common among women with obstructive sleep apnea (OSA) compared with men with OSA, but data on the relationship among depression, severity of OSA, and sleepiness are limited, said Dr. Stacey Ishman of Johns Hopkins University, Baltimore.
Dr. Ishman and her colleagues evaluated 56 consecutive OSA patients aged 27-74 years who presented to an otolaryngology clinic and compared them with 51 controls. The average age of patients and controls was 47 years; 61% of the OSA patients were male.
Overall, significantly more OSA patients met the criteria for depression, compared with controls (29% vs. 8%). The severity of OSA (measured using the Respiratory Disturbance Index) was a significant predictor of Beck Depression Inventory (BDI) scores, but BDI scores were not correlated with the severity of OSA.
These findings suggest that “depression may be significant even in patients with mild OSA,” Dr. Ishman said at the meeting jointly sponsored by the Triological Society and the American College of Surgeons.
BDI scores were significantly correlated with higher scores on the Epworth Sleepiness Scale (ESS), but the ESS did not correlate with the severity of sleep apnea. However, findings from previous studies have shown that more than 50% of individuals with severe OSA (an apnea-hypopnea index of at least 30 events/hour) do not report subjective sleepiness, she noted.
The relationship between BDI and ESS suggests that OSA patients with excessive sleepiness in particular might benefit from depression screening, she said.
Major Finding: 29% of patients with OSA met criteria for depression, compared with 8% of controls.
Data Source: Prospective study of 56 obstructive sleep apnea patients at an otolaryngology clinic.
Disclosures: Dr. Ishman had no financial conflicts.
ORLANDO — Obstructive sleep apnea patients with symptoms of excessive sleepiness have the greatest risk of depression, based on data from a prospective study of 107 adults.
Data from previous studies have shown that self-reported depression is more common among women with obstructive sleep apnea (OSA) compared with men with OSA, but data on the relationship among depression, severity of OSA, and sleepiness are limited, said Dr. Stacey Ishman of Johns Hopkins University, Baltimore.
Dr. Ishman and her colleagues evaluated 56 consecutive OSA patients aged 27-74 years who presented to an otolaryngology clinic and compared them with 51 controls. The average age of patients and controls was 47 years; 61% of the OSA patients were male.
Overall, significantly more OSA patients met the criteria for depression, compared with controls (29% vs. 8%). The severity of OSA (measured using the Respiratory Disturbance Index) was a significant predictor of Beck Depression Inventory (BDI) scores, but BDI scores were not correlated with the severity of OSA.
These findings suggest that “depression may be significant even in patients with mild OSA,” Dr. Ishman said at the meeting jointly sponsored by the Triological Society and the American College of Surgeons.
BDI scores were significantly correlated with higher scores on the Epworth Sleepiness Scale (ESS), but the ESS did not correlate with the severity of sleep apnea. However, findings from previous studies have shown that more than 50% of individuals with severe OSA (an apnea-hypopnea index of at least 30 events/hour) do not report subjective sleepiness, she noted.
The relationship between BDI and ESS suggests that OSA patients with excessive sleepiness in particular might benefit from depression screening, she said.
New MS Agent Reduces Relapse Rate, Disability
Major Finding: The annualized relapse rate was reduced by 54% in multiple sclerosis patients who took 0.5 mg of fingolimod and by 60% in those who took 1.25 mg of fingolimod. After 24 months, around 70% of patients given fingolimod were relapse free, compared with 46% of the placebo group.
Data Source: A randomized, double-blind, placebo-controlled phase III study of 1,272 adults with MS.
Disclosures: The study was supported by Novartis Pharma AG. Dr. Kappos has received research support from multiple pharmaceutical companies, including Novartis. Dr. O'Connor has served as a consultant and received research support for multiple pharmaceutical companies, including Novartis.
TORONTO — The investigational drug fingolimod at doses of 0.5 mg and 1.25 mg appears to be a safe and effective treatment for adults with multiple sclerosis, based on data from more than 1,000 patients.
In previous studies, fingolimod had “a clear cut effect on inflammatory outcomes” in relapsing-remitting multiple sclerosis patients, said Dr. Ludwig Kappos of University Hospital in Basel, Switzerland.
The current phase III study addressed whether the effects of fingolimod (FTY720) persisted over time, and whether a 0.5-mg dose is as effective as the previously studied 1.25-mg dose. The main outcome was relapse rate per year over a 2-year follow-up period.
The Food and Drug Administration is scheduled to review the safety and efficacy data for fingolimod this month.
The Fingolimod (FTY720) vs. Placebo in Relapsing-Remitting Multiple Sclerosis (FREEDOMS) study included 1,272 patients aged 18-55 years.
The average age of the patients was 37 years, and the average duration of MS was 8 years.
Patients with systemic or immune system disease were excluded, and 1,033 patients completed the study.
Patients were randomized to receive a daily dose of 1.25 mg fingolimod, 0.5 mg fingolimod, or a placebo.
The annualized relapse rate was reduced by 54% in patients who took 0.5 mg of fingolimod and by 60% in those who took 1.25 mg of fingolimod.
There was no significant difference in effectiveness between the doses, and both doses were significantly more effective than the placebo.
After 24 months, significantly more patients in either fingolimod group (70%-75%) were relapse free, compared with 46% of the placebo group.
In addition, both the 1.25-mg and 0.5-mg doses of fingolimod were associated with of 32% and 30%, reductions, respectively, in the risk of 3-month confirmed disability progression. Both reductions were significant, compared with placebo.
Similarly, both the 1.25-mg and 0.5-mg doses were associated with reductions in risk of 6-month confirmed disability progression of 40% and 37%, also significant compared with placebo.
Safety and tolerability data for the study population were presented separately in a poster by Dr. Paul O'Connor of St. Michael's Hospital, Toronto, and his colleagues.
In the safety analysis, the researchers evaluated all patients at baseline screening, week 2, and months 1, 2, 3, 6, 9, 12, 15, 18, 21, and 24.
Overall, the incidence of any adverse event was 94% in both of the fingolimod groups and 93% in the placebo group. The incidence of an adverse event that caused a patient to stop treatment was 14% in the 1.25-mg group, and 8% in both the 0.5-mg and placebo groups.
Serious adverse events were reported in 51 patients (12%) in the 1.25-mg group, 42 patients (10%) in the 0.5-mg group, and 56 patients (13%) in the placebo group. Serious adverse events included cardiovascular disorders, neoplasms, nervous system disorders, macular edema, and abnormal liver function test results.
Sinus bradycardia, the most common ECG finding, occurred in 47 patients (11%) in the 1.25-mg group, 20 patients (5%) in the 0.5-mg group, and 6 patients (2%) in the placebo group.
In addition, first- and second-degree atrioventricular blocks were reported in 20 patients (5%) and 1 patient (0.2%), respectively, in the 0.5-mg group, compared with 37 patients (9%) and 4 patients (1%), respectively, in the 1.25-mg group.
Malignant neoplasms were reported in 4 patients in each of the fingolimod groups and in 10 patients in the placebo group.
All 11 cases of skin cancer reported in the study were successfully treated with excision.
Abnormal liver function tests were reported more than twice as frequently in the fingolimod 1.25-mg and 0.5-mg groups, compared with placebo (19%, 16%, and 5%, respectively).
But “liver enzyme elevations were asymptomatic and improved once therapy was discontinued; no patient developed liver failure,” the investigators wrote.
In the 1.25-mg group, one case of ischemic stroke occurred during the study period, and a transient ischemic attack occurred 8 months after the discontinuation of treatment.
No clinically relevant pulmonary function changes were observed in any of the groups.
All seven reported cases of macular edema occurred in the group that took 1.25 mg of fingolimod, and all cases resolved after treatment was discontinued.
The overall incidence of infections was similar (69%-72%) for all three groups, and included herpesvirus infections, lower respiratory tract infections, and urinary tract infections.
The results support safety data from previous studies and suggest that most patients with MS tolerate oral fingolimod, the researchers said.
Also consistent with previous studies, “the overall safety profile of fingolimod 0.5 mg appears to be more favorable than that of the 1.25-mg dose,” they added.
Major Finding: The annualized relapse rate was reduced by 54% in multiple sclerosis patients who took 0.5 mg of fingolimod and by 60% in those who took 1.25 mg of fingolimod. After 24 months, around 70% of patients given fingolimod were relapse free, compared with 46% of the placebo group.
Data Source: A randomized, double-blind, placebo-controlled phase III study of 1,272 adults with MS.
Disclosures: The study was supported by Novartis Pharma AG. Dr. Kappos has received research support from multiple pharmaceutical companies, including Novartis. Dr. O'Connor has served as a consultant and received research support for multiple pharmaceutical companies, including Novartis.
TORONTO — The investigational drug fingolimod at doses of 0.5 mg and 1.25 mg appears to be a safe and effective treatment for adults with multiple sclerosis, based on data from more than 1,000 patients.
In previous studies, fingolimod had “a clear cut effect on inflammatory outcomes” in relapsing-remitting multiple sclerosis patients, said Dr. Ludwig Kappos of University Hospital in Basel, Switzerland.
The current phase III study addressed whether the effects of fingolimod (FTY720) persisted over time, and whether a 0.5-mg dose is as effective as the previously studied 1.25-mg dose. The main outcome was relapse rate per year over a 2-year follow-up period.
The Food and Drug Administration is scheduled to review the safety and efficacy data for fingolimod this month.
The Fingolimod (FTY720) vs. Placebo in Relapsing-Remitting Multiple Sclerosis (FREEDOMS) study included 1,272 patients aged 18-55 years.
The average age of the patients was 37 years, and the average duration of MS was 8 years.
Patients with systemic or immune system disease were excluded, and 1,033 patients completed the study.
Patients were randomized to receive a daily dose of 1.25 mg fingolimod, 0.5 mg fingolimod, or a placebo.
The annualized relapse rate was reduced by 54% in patients who took 0.5 mg of fingolimod and by 60% in those who took 1.25 mg of fingolimod.
There was no significant difference in effectiveness between the doses, and both doses were significantly more effective than the placebo.
After 24 months, significantly more patients in either fingolimod group (70%-75%) were relapse free, compared with 46% of the placebo group.
In addition, both the 1.25-mg and 0.5-mg doses of fingolimod were associated with of 32% and 30%, reductions, respectively, in the risk of 3-month confirmed disability progression. Both reductions were significant, compared with placebo.
Similarly, both the 1.25-mg and 0.5-mg doses were associated with reductions in risk of 6-month confirmed disability progression of 40% and 37%, also significant compared with placebo.
Safety and tolerability data for the study population were presented separately in a poster by Dr. Paul O'Connor of St. Michael's Hospital, Toronto, and his colleagues.
In the safety analysis, the researchers evaluated all patients at baseline screening, week 2, and months 1, 2, 3, 6, 9, 12, 15, 18, 21, and 24.
Overall, the incidence of any adverse event was 94% in both of the fingolimod groups and 93% in the placebo group. The incidence of an adverse event that caused a patient to stop treatment was 14% in the 1.25-mg group, and 8% in both the 0.5-mg and placebo groups.
Serious adverse events were reported in 51 patients (12%) in the 1.25-mg group, 42 patients (10%) in the 0.5-mg group, and 56 patients (13%) in the placebo group. Serious adverse events included cardiovascular disorders, neoplasms, nervous system disorders, macular edema, and abnormal liver function test results.
Sinus bradycardia, the most common ECG finding, occurred in 47 patients (11%) in the 1.25-mg group, 20 patients (5%) in the 0.5-mg group, and 6 patients (2%) in the placebo group.
In addition, first- and second-degree atrioventricular blocks were reported in 20 patients (5%) and 1 patient (0.2%), respectively, in the 0.5-mg group, compared with 37 patients (9%) and 4 patients (1%), respectively, in the 1.25-mg group.
Malignant neoplasms were reported in 4 patients in each of the fingolimod groups and in 10 patients in the placebo group.
All 11 cases of skin cancer reported in the study were successfully treated with excision.
Abnormal liver function tests were reported more than twice as frequently in the fingolimod 1.25-mg and 0.5-mg groups, compared with placebo (19%, 16%, and 5%, respectively).
But “liver enzyme elevations were asymptomatic and improved once therapy was discontinued; no patient developed liver failure,” the investigators wrote.
In the 1.25-mg group, one case of ischemic stroke occurred during the study period, and a transient ischemic attack occurred 8 months after the discontinuation of treatment.
No clinically relevant pulmonary function changes were observed in any of the groups.
All seven reported cases of macular edema occurred in the group that took 1.25 mg of fingolimod, and all cases resolved after treatment was discontinued.
The overall incidence of infections was similar (69%-72%) for all three groups, and included herpesvirus infections, lower respiratory tract infections, and urinary tract infections.
The results support safety data from previous studies and suggest that most patients with MS tolerate oral fingolimod, the researchers said.
Also consistent with previous studies, “the overall safety profile of fingolimod 0.5 mg appears to be more favorable than that of the 1.25-mg dose,” they added.
Major Finding: The annualized relapse rate was reduced by 54% in multiple sclerosis patients who took 0.5 mg of fingolimod and by 60% in those who took 1.25 mg of fingolimod. After 24 months, around 70% of patients given fingolimod were relapse free, compared with 46% of the placebo group.
Data Source: A randomized, double-blind, placebo-controlled phase III study of 1,272 adults with MS.
Disclosures: The study was supported by Novartis Pharma AG. Dr. Kappos has received research support from multiple pharmaceutical companies, including Novartis. Dr. O'Connor has served as a consultant and received research support for multiple pharmaceutical companies, including Novartis.
TORONTO — The investigational drug fingolimod at doses of 0.5 mg and 1.25 mg appears to be a safe and effective treatment for adults with multiple sclerosis, based on data from more than 1,000 patients.
In previous studies, fingolimod had “a clear cut effect on inflammatory outcomes” in relapsing-remitting multiple sclerosis patients, said Dr. Ludwig Kappos of University Hospital in Basel, Switzerland.
The current phase III study addressed whether the effects of fingolimod (FTY720) persisted over time, and whether a 0.5-mg dose is as effective as the previously studied 1.25-mg dose. The main outcome was relapse rate per year over a 2-year follow-up period.
The Food and Drug Administration is scheduled to review the safety and efficacy data for fingolimod this month.
The Fingolimod (FTY720) vs. Placebo in Relapsing-Remitting Multiple Sclerosis (FREEDOMS) study included 1,272 patients aged 18-55 years.
The average age of the patients was 37 years, and the average duration of MS was 8 years.
Patients with systemic or immune system disease were excluded, and 1,033 patients completed the study.
Patients were randomized to receive a daily dose of 1.25 mg fingolimod, 0.5 mg fingolimod, or a placebo.
The annualized relapse rate was reduced by 54% in patients who took 0.5 mg of fingolimod and by 60% in those who took 1.25 mg of fingolimod.
There was no significant difference in effectiveness between the doses, and both doses were significantly more effective than the placebo.
After 24 months, significantly more patients in either fingolimod group (70%-75%) were relapse free, compared with 46% of the placebo group.
In addition, both the 1.25-mg and 0.5-mg doses of fingolimod were associated with of 32% and 30%, reductions, respectively, in the risk of 3-month confirmed disability progression. Both reductions were significant, compared with placebo.
Similarly, both the 1.25-mg and 0.5-mg doses were associated with reductions in risk of 6-month confirmed disability progression of 40% and 37%, also significant compared with placebo.
Safety and tolerability data for the study population were presented separately in a poster by Dr. Paul O'Connor of St. Michael's Hospital, Toronto, and his colleagues.
In the safety analysis, the researchers evaluated all patients at baseline screening, week 2, and months 1, 2, 3, 6, 9, 12, 15, 18, 21, and 24.
Overall, the incidence of any adverse event was 94% in both of the fingolimod groups and 93% in the placebo group. The incidence of an adverse event that caused a patient to stop treatment was 14% in the 1.25-mg group, and 8% in both the 0.5-mg and placebo groups.
Serious adverse events were reported in 51 patients (12%) in the 1.25-mg group, 42 patients (10%) in the 0.5-mg group, and 56 patients (13%) in the placebo group. Serious adverse events included cardiovascular disorders, neoplasms, nervous system disorders, macular edema, and abnormal liver function test results.
Sinus bradycardia, the most common ECG finding, occurred in 47 patients (11%) in the 1.25-mg group, 20 patients (5%) in the 0.5-mg group, and 6 patients (2%) in the placebo group.
In addition, first- and second-degree atrioventricular blocks were reported in 20 patients (5%) and 1 patient (0.2%), respectively, in the 0.5-mg group, compared with 37 patients (9%) and 4 patients (1%), respectively, in the 1.25-mg group.
Malignant neoplasms were reported in 4 patients in each of the fingolimod groups and in 10 patients in the placebo group.
All 11 cases of skin cancer reported in the study were successfully treated with excision.
Abnormal liver function tests were reported more than twice as frequently in the fingolimod 1.25-mg and 0.5-mg groups, compared with placebo (19%, 16%, and 5%, respectively).
But “liver enzyme elevations were asymptomatic and improved once therapy was discontinued; no patient developed liver failure,” the investigators wrote.
In the 1.25-mg group, one case of ischemic stroke occurred during the study period, and a transient ischemic attack occurred 8 months after the discontinuation of treatment.
No clinically relevant pulmonary function changes were observed in any of the groups.
All seven reported cases of macular edema occurred in the group that took 1.25 mg of fingolimod, and all cases resolved after treatment was discontinued.
The overall incidence of infections was similar (69%-72%) for all three groups, and included herpesvirus infections, lower respiratory tract infections, and urinary tract infections.
The results support safety data from previous studies and suggest that most patients with MS tolerate oral fingolimod, the researchers said.
Also consistent with previous studies, “the overall safety profile of fingolimod 0.5 mg appears to be more favorable than that of the 1.25-mg dose,” they added.
Antiepileptic Side Effects a Problem for 40% of Patients
TORONTO — About 40% of epilepsy patients are bothered by side effects of their antiepileptic drugs, based on data from a survey of adults with epilepsy.
Information on the tolerability of antiepileptic drugs (AEDs) and the reasons for discontinuing treatment are limited, George J. Wan, Ph.D., said in a poster.
To examine drug tolerability and treatment satisfaction, Dr. Wan and his colleagues reviewed data from the National Survey of Epilepsy, Comorbidities, and Health Outcomes (EPIC), a large U.S. survey conducted in 2009 that included 7,500 epilepsy patients and 2,500 controls.
A total of 2,395 respondents reported being formally diagnosed with epilepsy or a seizure disorder; of those, 1,415 (59%) were taking antiepilepsy drugs at the time of the survey. About 60% of the respondents reported taking one AED, 35% reported taking two or three, and 5% reported taking four or more.
A total of 772 respondents said that they were “not at all” bothered by side effects from AEDs. But 519 respondents reported some degree of bother: 22% were mildly bothered; 12%, moderately bothered; 5%, markedly bothered; and 1%, extremely bothered. The researchers did not identify specific side effects.
Overall, 72% of the respondents said they were either “somewhat satisfied” or “very satisfied” with their current AED regimens. But 304 respondents said that they had discontinued their medications. Of those, 50% discontinued on their doctor's advice; 45% because of side effects; 30% because of improvement in seizures; and 21% because of inadequate seizure control. Some respondents indicated more than one reason for discontinuing their AEDs.
Patients taking two or more AEDs were significantly more likely to be bothered by side effects, compared with those taking one, the researchers reported.
Disclosures: Dr. Wan is an employee of Ortho-McNeil Janssen Scientific Affairs, which supported the study.
TORONTO — About 40% of epilepsy patients are bothered by side effects of their antiepileptic drugs, based on data from a survey of adults with epilepsy.
Information on the tolerability of antiepileptic drugs (AEDs) and the reasons for discontinuing treatment are limited, George J. Wan, Ph.D., said in a poster.
To examine drug tolerability and treatment satisfaction, Dr. Wan and his colleagues reviewed data from the National Survey of Epilepsy, Comorbidities, and Health Outcomes (EPIC), a large U.S. survey conducted in 2009 that included 7,500 epilepsy patients and 2,500 controls.
A total of 2,395 respondents reported being formally diagnosed with epilepsy or a seizure disorder; of those, 1,415 (59%) were taking antiepilepsy drugs at the time of the survey. About 60% of the respondents reported taking one AED, 35% reported taking two or three, and 5% reported taking four or more.
A total of 772 respondents said that they were “not at all” bothered by side effects from AEDs. But 519 respondents reported some degree of bother: 22% were mildly bothered; 12%, moderately bothered; 5%, markedly bothered; and 1%, extremely bothered. The researchers did not identify specific side effects.
Overall, 72% of the respondents said they were either “somewhat satisfied” or “very satisfied” with their current AED regimens. But 304 respondents said that they had discontinued their medications. Of those, 50% discontinued on their doctor's advice; 45% because of side effects; 30% because of improvement in seizures; and 21% because of inadequate seizure control. Some respondents indicated more than one reason for discontinuing their AEDs.
Patients taking two or more AEDs were significantly more likely to be bothered by side effects, compared with those taking one, the researchers reported.
Disclosures: Dr. Wan is an employee of Ortho-McNeil Janssen Scientific Affairs, which supported the study.
TORONTO — About 40% of epilepsy patients are bothered by side effects of their antiepileptic drugs, based on data from a survey of adults with epilepsy.
Information on the tolerability of antiepileptic drugs (AEDs) and the reasons for discontinuing treatment are limited, George J. Wan, Ph.D., said in a poster.
To examine drug tolerability and treatment satisfaction, Dr. Wan and his colleagues reviewed data from the National Survey of Epilepsy, Comorbidities, and Health Outcomes (EPIC), a large U.S. survey conducted in 2009 that included 7,500 epilepsy patients and 2,500 controls.
A total of 2,395 respondents reported being formally diagnosed with epilepsy or a seizure disorder; of those, 1,415 (59%) were taking antiepilepsy drugs at the time of the survey. About 60% of the respondents reported taking one AED, 35% reported taking two or three, and 5% reported taking four or more.
A total of 772 respondents said that they were “not at all” bothered by side effects from AEDs. But 519 respondents reported some degree of bother: 22% were mildly bothered; 12%, moderately bothered; 5%, markedly bothered; and 1%, extremely bothered. The researchers did not identify specific side effects.
Overall, 72% of the respondents said they were either “somewhat satisfied” or “very satisfied” with their current AED regimens. But 304 respondents said that they had discontinued their medications. Of those, 50% discontinued on their doctor's advice; 45% because of side effects; 30% because of improvement in seizures; and 21% because of inadequate seizure control. Some respondents indicated more than one reason for discontinuing their AEDs.
Patients taking two or more AEDs were significantly more likely to be bothered by side effects, compared with those taking one, the researchers reported.
Disclosures: Dr. Wan is an employee of Ortho-McNeil Janssen Scientific Affairs, which supported the study.
Indoor Tanning Raises Risk of Melanoma, New Study Finds
Indoor tanning is associated with a fourfold increased risk of melanoma, according to findings published online May 27 in Cancer Epidemiology, Biomarkers & Prevention.
The findings were based on data from the Skin Health Study, a population-based, case-control study of 1,167 cases and 1,101 controls.

Melanoma was 2.9 times more likely to occur in users of high-speed/high-intensity (UVB-enhanced) tanning devices and 4.4 times more likely in users of high-pressure (primarily UVA-emitting) devices, compared with individuals who had never used the devices.
In addition, melanoma was 1.8 and 1.9 times more likely in users of conventional indoor tanning devices and sunlamps, respectively, compared with never users.
The study population included individuals aged 25-59 years who were diagnosed with invasive cutaneous melanoma between July 2004 and December 2007 in Minnesota and who were enrolled in a state cancer registry. Controls were selected at random from the Minnesota state driver’s license list. Study participants completed a self-administered questionnaire and a detailed 1-hour phone interview (Cancer Epidemiol. Biomarkers Prev. 2010 [doi: 10.1158/1055-9965.EPI-09-1249]).
DeAnn Lazovich, Ph.D., of the University of Minnesota, Minneapolis, and colleagues began the Skin Health Study in 2004 in Minnesota, a state with a documented high rate of indoor tanning. The data collected by the researchers included skin, hair, and eye color; presence of moles and freckles; lifetime routine sun exposure; age at which tanning beds were first used; duration and frequency of indoor tanning; and type of tanning device used.
Overall, 63% of individuals with melanoma and 51% of controls reported any indoor tanning. Melanoma risk increased significantly as the frequency of indoor tanning increased. Individuals with melanoma were more than twice as likely as controls to report painful burns resulting from indoor tanning, and they reported significantly more of these painful burns than controls.
The researchers also noted that a dose-response relationship between the number of tanning sessions and the number of melanoma lesions on the trunk was identified in both men and women.
“We did not find lifetime routine sun exposure or sun exposure via recreational outdoor activities or occupations to be associated with melanoma risk,” Dr. Lazovich and associates wrote. “To the extent that sunburns are a marker of intermittent sun exposure, then our results adequately represent the independent effect of indoor tanning use on the risk of melanoma.”
“As dermatologists, we see the horrible price paid for using these devices,” Dr. Allan C. Halpern, chief of dermatology at Memorial Sloan-Kettering Cancer Center, New York, said during a teleconference on May 27 to discuss the study findings. Dr. Halpern was not involved in the study.

“We now know that the total amount of UV exposure in tanning beds over time is important,” Dr. Halpern said. “I’m hopeful that this study is going to be very helpful in the hands of the FDA to further regulate the industry.”
Dr. Halpern said that dermatologists have long understood the importance of educating patients about the dangers of indoor tanning devices, but that misinformation about the risks and benefits of indoor tanning persist.
“I think this study very much strengthens our hand,” he said. Dr. Halpern added that he was encouraged to see the consumer video posted by the FDA earlier this week, which states than any UV indoor tanning device should be avoided.
In 2009, the International Agency for Research on Cancer classified tanning beds as carcinogenic to humans. In 2010, a Food and Drug Administration advisory panel recommended tighter restrictions on the use of indoor tanning devices, but the FDA has yet to issue any guidelines based on these recommendations.
The findings address several limitations of previous studies on this topic, including the ability to control for confounding variables such as sun exposure, the investigators noted.
None of the study authors stated that they had any conflicts of interest to disclose. The study was supported in part by a grant from the American Cancer Society and the National Cancer Institute.
Indoor tanning is associated with a fourfold increased risk of melanoma, according to findings published online May 27 in Cancer Epidemiology, Biomarkers & Prevention.
The findings were based on data from the Skin Health Study, a population-based, case-control study of 1,167 cases and 1,101 controls.
Melanoma was 2.9 times more likely to occur in users of high-speed/high-intensity (UVB-enhanced) tanning devices and 4.4 times more likely in users of high-pressure (primarily UVA-emitting) devices, compared with individuals who had never used the devices.
In addition, melanoma was 1.8 and 1.9 times more likely in users of conventional indoor tanning devices and sunlamps, respectively, compared with never users.
The study population included individuals aged 25-59 years who were diagnosed with invasive cutaneous melanoma between July 2004 and December 2007 in Minnesota and who were enrolled in a state cancer registry. Controls were selected at random from the Minnesota state driver’s license list. Study participants completed a self-administered questionnaire and a detailed 1-hour phone interview (Cancer Epidemiol. Biomarkers Prev. 2010 [doi: 10.1158/1055-9965.EPI-09-1249]).
DeAnn Lazovich, Ph.D., of the University of Minnesota, Minneapolis, and colleagues began the Skin Health Study in 2004 in Minnesota, a state with a documented high rate of indoor tanning. The data collected by the researchers included skin, hair, and eye color; presence of moles and freckles; lifetime routine sun exposure; age at which tanning beds were first used; duration and frequency of indoor tanning; and type of tanning device used.
Overall, 63% of individuals with melanoma and 51% of controls reported any indoor tanning. Melanoma risk increased significantly as the frequency of indoor tanning increased. Individuals with melanoma were more than twice as likely as controls to report painful burns resulting from indoor tanning, and they reported significantly more of these painful burns than controls.
The researchers also noted that a dose-response relationship between the number of tanning sessions and the number of melanoma lesions on the trunk was identified in both men and women.
“We did not find lifetime routine sun exposure or sun exposure via recreational outdoor activities or occupations to be associated with melanoma risk,” Dr. Lazovich and associates wrote. “To the extent that sunburns are a marker of intermittent sun exposure, then our results adequately represent the independent effect of indoor tanning use on the risk of melanoma.”
“As dermatologists, we see the horrible price paid for using these devices,” Dr. Allan C. Halpern, chief of dermatology at Memorial Sloan-Kettering Cancer Center, New York, said during a teleconference on May 27 to discuss the study findings. Dr. Halpern was not involved in the study.
“We now know that the total amount of UV exposure in tanning beds over time is important,” Dr. Halpern said. “I’m hopeful that this study is going to be very helpful in the hands of the FDA to further regulate the industry.”
Dr. Halpern said that dermatologists have long understood the importance of educating patients about the dangers of indoor tanning devices, but that misinformation about the risks and benefits of indoor tanning persist.
“I think this study very much strengthens our hand,” he said. Dr. Halpern added that he was encouraged to see the consumer video posted by the FDA earlier this week, which states than any UV indoor tanning device should be avoided.
In 2009, the International Agency for Research on Cancer classified tanning beds as carcinogenic to humans. In 2010, a Food and Drug Administration advisory panel recommended tighter restrictions on the use of indoor tanning devices, but the FDA has yet to issue any guidelines based on these recommendations.
The findings address several limitations of previous studies on this topic, including the ability to control for confounding variables such as sun exposure, the investigators noted.
None of the study authors stated that they had any conflicts of interest to disclose. The study was supported in part by a grant from the American Cancer Society and the National Cancer Institute.
Indoor tanning is associated with a fourfold increased risk of melanoma, according to findings published online May 27 in Cancer Epidemiology, Biomarkers & Prevention.
The findings were based on data from the Skin Health Study, a population-based, case-control study of 1,167 cases and 1,101 controls.
Melanoma was 2.9 times more likely to occur in users of high-speed/high-intensity (UVB-enhanced) tanning devices and 4.4 times more likely in users of high-pressure (primarily UVA-emitting) devices, compared with individuals who had never used the devices.
In addition, melanoma was 1.8 and 1.9 times more likely in users of conventional indoor tanning devices and sunlamps, respectively, compared with never users.
The study population included individuals aged 25-59 years who were diagnosed with invasive cutaneous melanoma between July 2004 and December 2007 in Minnesota and who were enrolled in a state cancer registry. Controls were selected at random from the Minnesota state driver’s license list. Study participants completed a self-administered questionnaire and a detailed 1-hour phone interview (Cancer Epidemiol. Biomarkers Prev. 2010 [doi: 10.1158/1055-9965.EPI-09-1249]).
DeAnn Lazovich, Ph.D., of the University of Minnesota, Minneapolis, and colleagues began the Skin Health Study in 2004 in Minnesota, a state with a documented high rate of indoor tanning. The data collected by the researchers included skin, hair, and eye color; presence of moles and freckles; lifetime routine sun exposure; age at which tanning beds were first used; duration and frequency of indoor tanning; and type of tanning device used.
Overall, 63% of individuals with melanoma and 51% of controls reported any indoor tanning. Melanoma risk increased significantly as the frequency of indoor tanning increased. Individuals with melanoma were more than twice as likely as controls to report painful burns resulting from indoor tanning, and they reported significantly more of these painful burns than controls.
The researchers also noted that a dose-response relationship between the number of tanning sessions and the number of melanoma lesions on the trunk was identified in both men and women.
“We did not find lifetime routine sun exposure or sun exposure via recreational outdoor activities or occupations to be associated with melanoma risk,” Dr. Lazovich and associates wrote. “To the extent that sunburns are a marker of intermittent sun exposure, then our results adequately represent the independent effect of indoor tanning use on the risk of melanoma.”
“As dermatologists, we see the horrible price paid for using these devices,” Dr. Allan C. Halpern, chief of dermatology at Memorial Sloan-Kettering Cancer Center, New York, said during a teleconference on May 27 to discuss the study findings. Dr. Halpern was not involved in the study.
“We now know that the total amount of UV exposure in tanning beds over time is important,” Dr. Halpern said. “I’m hopeful that this study is going to be very helpful in the hands of the FDA to further regulate the industry.”
Dr. Halpern said that dermatologists have long understood the importance of educating patients about the dangers of indoor tanning devices, but that misinformation about the risks and benefits of indoor tanning persist.
“I think this study very much strengthens our hand,” he said. Dr. Halpern added that he was encouraged to see the consumer video posted by the FDA earlier this week, which states than any UV indoor tanning device should be avoided.
In 2009, the International Agency for Research on Cancer classified tanning beds as carcinogenic to humans. In 2010, a Food and Drug Administration advisory panel recommended tighter restrictions on the use of indoor tanning devices, but the FDA has yet to issue any guidelines based on these recommendations.
The findings address several limitations of previous studies on this topic, including the ability to control for confounding variables such as sun exposure, the investigators noted.
None of the study authors stated that they had any conflicts of interest to disclose. The study was supported in part by a grant from the American Cancer Society and the National Cancer Institute.
High Intake of Animal Protein Tied to IBD Risk
Major Finding: The relative risk for developing IBD was 3.31 for high total protein intake and 3.03 for high animal protein intake, when comparing the highest tertile of intake with the lowest tertile of intake.
Data Source: A prospective study of 60,000 women aged 40–65 years, 77 of whom developed IBD.
Disclosures: Dr. Jantchou said that he had no financial conflicts to disclose.
A high intake of animal protein was significantly associated with increased risk of developing inflammatory bowel disease in a prospective study of 60,000 women aged 40–65 years, 77 of whom developed IBD.
The results of the study were presented at a teleconference in advance of the annual Digestive Disease Week.
Although doctors have long suspected an association between diet and inflammatory bowel disease (IBD), most previous studies on this topic have been retrospective, said Dr. Prévost Jantchou of the Centre for Research in Epidemiology and Population Health in Villejuif, France.
In this prospective study, onset of IBD occurred after the first dietary questionnaire was completed by each participant, so it was not necessary for the women to try to recall what they had eaten in the past.
The 77 patients with confirmed IBD were part of the E3N study, a cohort of more than 60,000 women that was established in France in 1990 to assess risk factors for female cancers. The controls were all the women in the cohort of 60,000 who did not state that they had developed IBD by 2005, the final follow-up. A Cox survival model analysis was performed.
The participants completed questionnaires about diet, disease incidence, and lifestyle every 2 years until 2005. The average follow-up period for the women in this study was 10 years.
Dr. Jantchou and colleagues examined the participants' intake of protein, carbohydrate, and fat. Then the study participants were divided into three groups based on protein intake. The average intake of the low, middle, and high tertiles was 1.08 g/kg, 1.52 g/kg, and 2.07 g/kg, respectively. The Food and Drug Administration recommends an average daily protein intake of 0.8 g/kg of body weight, he said.
More than two-thirds of the 77 participants who developed IBD had an elevated protein intake, Dr. Jantchou noted. Mean total protein intake was 102.4 g/day for IBD cases vs. 92.1 g/day for controls, Dr. Jantchou said in an interview. Animal protein intake also was higher for the women who developed IBD during the study: 70.1 g/day vs. 61.9 g/day for the controls, he said.
Overall, a high intake of animal protein was associated with a significantly increased risk of IBD. The relative risks for the highest tertile of intake vs. the lowest tertile were 3.31 for total protein intake and 3.03 for animal protein intake specifically. The associations remained significant after researchers controlled for smoking and hormone therapy, both of which can increase the risk for IBD.
When the investigators looked at specific animal protein sources consumed, they found that higher than average consumption of meat or fish was associated with a significantly increased risk of IBD, but high consumption of dairy products or eggs was not linked to increased risk, Dr. Jantchou said.
When IBD was broken down into Crohn's disease and ulcerative colitis, similar trends were seen between high intake of animal protein and an increased risk of each disease, he noted.
The researchers found no association between either carbohydrate intake or fat intake and risk of IBD.
This study is the first to prospectively show an association between a high intake of animal protein and an increased risk of IBD, Dr. Jantchou said. “The next step we want to take is to look at animal protein in patients already diagnosed with IBD and to give them dietary advice,” Dr. Jantchou added.
Major Finding: The relative risk for developing IBD was 3.31 for high total protein intake and 3.03 for high animal protein intake, when comparing the highest tertile of intake with the lowest tertile of intake.
Data Source: A prospective study of 60,000 women aged 40–65 years, 77 of whom developed IBD.
Disclosures: Dr. Jantchou said that he had no financial conflicts to disclose.
A high intake of animal protein was significantly associated with increased risk of developing inflammatory bowel disease in a prospective study of 60,000 women aged 40–65 years, 77 of whom developed IBD.
The results of the study were presented at a teleconference in advance of the annual Digestive Disease Week.
Although doctors have long suspected an association between diet and inflammatory bowel disease (IBD), most previous studies on this topic have been retrospective, said Dr. Prévost Jantchou of the Centre for Research in Epidemiology and Population Health in Villejuif, France.
In this prospective study, onset of IBD occurred after the first dietary questionnaire was completed by each participant, so it was not necessary for the women to try to recall what they had eaten in the past.
The 77 patients with confirmed IBD were part of the E3N study, a cohort of more than 60,000 women that was established in France in 1990 to assess risk factors for female cancers. The controls were all the women in the cohort of 60,000 who did not state that they had developed IBD by 2005, the final follow-up. A Cox survival model analysis was performed.
The participants completed questionnaires about diet, disease incidence, and lifestyle every 2 years until 2005. The average follow-up period for the women in this study was 10 years.
Dr. Jantchou and colleagues examined the participants' intake of protein, carbohydrate, and fat. Then the study participants were divided into three groups based on protein intake. The average intake of the low, middle, and high tertiles was 1.08 g/kg, 1.52 g/kg, and 2.07 g/kg, respectively. The Food and Drug Administration recommends an average daily protein intake of 0.8 g/kg of body weight, he said.
More than two-thirds of the 77 participants who developed IBD had an elevated protein intake, Dr. Jantchou noted. Mean total protein intake was 102.4 g/day for IBD cases vs. 92.1 g/day for controls, Dr. Jantchou said in an interview. Animal protein intake also was higher for the women who developed IBD during the study: 70.1 g/day vs. 61.9 g/day for the controls, he said.
Overall, a high intake of animal protein was associated with a significantly increased risk of IBD. The relative risks for the highest tertile of intake vs. the lowest tertile were 3.31 for total protein intake and 3.03 for animal protein intake specifically. The associations remained significant after researchers controlled for smoking and hormone therapy, both of which can increase the risk for IBD.
When the investigators looked at specific animal protein sources consumed, they found that higher than average consumption of meat or fish was associated with a significantly increased risk of IBD, but high consumption of dairy products or eggs was not linked to increased risk, Dr. Jantchou said.
When IBD was broken down into Crohn's disease and ulcerative colitis, similar trends were seen between high intake of animal protein and an increased risk of each disease, he noted.
The researchers found no association between either carbohydrate intake or fat intake and risk of IBD.
This study is the first to prospectively show an association between a high intake of animal protein and an increased risk of IBD, Dr. Jantchou said. “The next step we want to take is to look at animal protein in patients already diagnosed with IBD and to give them dietary advice,” Dr. Jantchou added.
Major Finding: The relative risk for developing IBD was 3.31 for high total protein intake and 3.03 for high animal protein intake, when comparing the highest tertile of intake with the lowest tertile of intake.
Data Source: A prospective study of 60,000 women aged 40–65 years, 77 of whom developed IBD.
Disclosures: Dr. Jantchou said that he had no financial conflicts to disclose.
A high intake of animal protein was significantly associated with increased risk of developing inflammatory bowel disease in a prospective study of 60,000 women aged 40–65 years, 77 of whom developed IBD.
The results of the study were presented at a teleconference in advance of the annual Digestive Disease Week.
Although doctors have long suspected an association between diet and inflammatory bowel disease (IBD), most previous studies on this topic have been retrospective, said Dr. Prévost Jantchou of the Centre for Research in Epidemiology and Population Health in Villejuif, France.
In this prospective study, onset of IBD occurred after the first dietary questionnaire was completed by each participant, so it was not necessary for the women to try to recall what they had eaten in the past.
The 77 patients with confirmed IBD were part of the E3N study, a cohort of more than 60,000 women that was established in France in 1990 to assess risk factors for female cancers. The controls were all the women in the cohort of 60,000 who did not state that they had developed IBD by 2005, the final follow-up. A Cox survival model analysis was performed.
The participants completed questionnaires about diet, disease incidence, and lifestyle every 2 years until 2005. The average follow-up period for the women in this study was 10 years.
Dr. Jantchou and colleagues examined the participants' intake of protein, carbohydrate, and fat. Then the study participants were divided into three groups based on protein intake. The average intake of the low, middle, and high tertiles was 1.08 g/kg, 1.52 g/kg, and 2.07 g/kg, respectively. The Food and Drug Administration recommends an average daily protein intake of 0.8 g/kg of body weight, he said.
More than two-thirds of the 77 participants who developed IBD had an elevated protein intake, Dr. Jantchou noted. Mean total protein intake was 102.4 g/day for IBD cases vs. 92.1 g/day for controls, Dr. Jantchou said in an interview. Animal protein intake also was higher for the women who developed IBD during the study: 70.1 g/day vs. 61.9 g/day for the controls, he said.
Overall, a high intake of animal protein was associated with a significantly increased risk of IBD. The relative risks for the highest tertile of intake vs. the lowest tertile were 3.31 for total protein intake and 3.03 for animal protein intake specifically. The associations remained significant after researchers controlled for smoking and hormone therapy, both of which can increase the risk for IBD.
When the investigators looked at specific animal protein sources consumed, they found that higher than average consumption of meat or fish was associated with a significantly increased risk of IBD, but high consumption of dairy products or eggs was not linked to increased risk, Dr. Jantchou said.
When IBD was broken down into Crohn's disease and ulcerative colitis, similar trends were seen between high intake of animal protein and an increased risk of each disease, he noted.
The researchers found no association between either carbohydrate intake or fat intake and risk of IBD.
This study is the first to prospectively show an association between a high intake of animal protein and an increased risk of IBD, Dr. Jantchou said. “The next step we want to take is to look at animal protein in patients already diagnosed with IBD and to give them dietary advice,” Dr. Jantchou added.
Two Lasers May Be Better Than One for Hair Removal
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
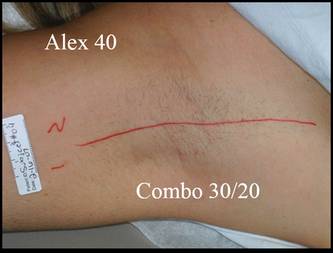
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Age May Alter Bisphosphonate Effect on Stenosis
Major Finding: The prevalence of aortic valve ring stenosis was 38% in women aged 65 years and older who took nitrogen-containing bisphosphonates, vs. 59% in women who didn't take bisphosphonates.
Data Source: A cross-sectional study of 3,710 women aged 45–84 years.
Disclosures: Dr. Elmariah has received grant support from the New York Academy of Medicine; the National Heart, Lung, and Blood Institute; and GlaxoSmithKline.
WASHINGTON — Nitrogen-containing bisphosphonates were associated with a significantly decreased prevalence of cardiovascular calcification in women older than 65 years, based on data from 3,710 women who are part of a large, ongoing study.
“Early on in the analysis, we came across a very unexpected finding,” said Dr. Sammy Elmariah of Mount Sinai School of Medicine in New York. “The association with bisphosphonate use was dependent on the patient's age.”
The data were taken from the Multi-Ethnic Study of Atherosclerosis (MESA), a longitudinal cohort study of 6,814 asymptomatic men and women aged 45–84 years.
Overall, the bisphosphonate users were more likely to be older and white. In the current study, Dr. Elmariah and his colleagues examined the impact of bisphosphonates on cardiovascular calcification in women.
Clinical studies have shown that bisphosphonates have an effect on serum lipids, Dr. Elmariah said. Some experimental data, including data from animal models and dialysis patients, suggest that nitrogen-containing bisphosphonates (NCBPs) may limit cardiovascular calcification. In addition, the results of one recent study showed that patients on bisphosphonates for osteoporosis had a slower progression of aortic stenosis, he noted.
The prevalence of aortic valve ring stenosis was 38% in women aged 65 years and older who used NCBPs, which was significantly lower than in non-NCBP users of the same age (59%). Aortic valve ring stenosis prevalence also was 38% in women younger than 65 years who used NCBPs; it was significantly lower at 17% among similarly aged non-NCBP users.
Significant patterns also were seen for stenosis of the thoracic aorta and mitral annulus. The relationship between bisphosphonate use and the decrease in cardiovascular calcification in the 65-years-and-older group did not reach statistical significance for the prevalence of aortic valve stenosis and coronary artery stenosis, but the trends were similar.
This study is the first evaluation of the relationship between bisphosphonate use and the prevalence of cardiovascular calcification in a healthy patient population, Dr. Elmariah said.
Cardiovascular calcification was measured using cardiac CT. Bisphosphate use was defined as use of either oral or intravenous bisphosphonates at the time of the cardiac CT. The average age of the NCBP users was 67 years, and the average age of the nonusers was 62 years. Approximately 60% of the women were white.
After adjustment for variables including age, body mass index, diabetes, hypertension, smoking, race, insurance status, education, and income level, the significance remained, Dr. Elmariah said.
“We get a fairly dramatic reduction in the prevalence of cardiovascular calcification in bisphosphonate users over the age of 65,” he added.
When the researchers divided the study population into 10-year age groups, they saw a gradual reduction in cardiovascular calcification with increasing age, he noted.
The study was limited by its cross-sectional design and by the lack of data on the duration of bisphosphonate use. “It's unclear whether this finding is due to true age-related differences in the pathogenesis of cardiovascular calcification or in the effect of bisphosphonates,” said Dr. Elmariah. But the results merit additional studies to tease out the reason for the age-related impact of bisphosphonates on cardiovascular calcification in women, he said.
{kind=link}
NCBPs significantly cut cardiovascular calcification in women over 65, said Dr. Sammy Elmariah.
Source Courtesy Dr. Sammy Elmariah
Major Finding: The prevalence of aortic valve ring stenosis was 38% in women aged 65 years and older who took nitrogen-containing bisphosphonates, vs. 59% in women who didn't take bisphosphonates.
Data Source: A cross-sectional study of 3,710 women aged 45–84 years.
Disclosures: Dr. Elmariah has received grant support from the New York Academy of Medicine; the National Heart, Lung, and Blood Institute; and GlaxoSmithKline.
WASHINGTON — Nitrogen-containing bisphosphonates were associated with a significantly decreased prevalence of cardiovascular calcification in women older than 65 years, based on data from 3,710 women who are part of a large, ongoing study.
“Early on in the analysis, we came across a very unexpected finding,” said Dr. Sammy Elmariah of Mount Sinai School of Medicine in New York. “The association with bisphosphonate use was dependent on the patient's age.”
The data were taken from the Multi-Ethnic Study of Atherosclerosis (MESA), a longitudinal cohort study of 6,814 asymptomatic men and women aged 45–84 years.
Overall, the bisphosphonate users were more likely to be older and white. In the current study, Dr. Elmariah and his colleagues examined the impact of bisphosphonates on cardiovascular calcification in women.
Clinical studies have shown that bisphosphonates have an effect on serum lipids, Dr. Elmariah said. Some experimental data, including data from animal models and dialysis patients, suggest that nitrogen-containing bisphosphonates (NCBPs) may limit cardiovascular calcification. In addition, the results of one recent study showed that patients on bisphosphonates for osteoporosis had a slower progression of aortic stenosis, he noted.
The prevalence of aortic valve ring stenosis was 38% in women aged 65 years and older who used NCBPs, which was significantly lower than in non-NCBP users of the same age (59%). Aortic valve ring stenosis prevalence also was 38% in women younger than 65 years who used NCBPs; it was significantly lower at 17% among similarly aged non-NCBP users.
Significant patterns also were seen for stenosis of the thoracic aorta and mitral annulus. The relationship between bisphosphonate use and the decrease in cardiovascular calcification in the 65-years-and-older group did not reach statistical significance for the prevalence of aortic valve stenosis and coronary artery stenosis, but the trends were similar.
This study is the first evaluation of the relationship between bisphosphonate use and the prevalence of cardiovascular calcification in a healthy patient population, Dr. Elmariah said.
Cardiovascular calcification was measured using cardiac CT. Bisphosphate use was defined as use of either oral or intravenous bisphosphonates at the time of the cardiac CT. The average age of the NCBP users was 67 years, and the average age of the nonusers was 62 years. Approximately 60% of the women were white.
After adjustment for variables including age, body mass index, diabetes, hypertension, smoking, race, insurance status, education, and income level, the significance remained, Dr. Elmariah said.
“We get a fairly dramatic reduction in the prevalence of cardiovascular calcification in bisphosphonate users over the age of 65,” he added.
When the researchers divided the study population into 10-year age groups, they saw a gradual reduction in cardiovascular calcification with increasing age, he noted.
The study was limited by its cross-sectional design and by the lack of data on the duration of bisphosphonate use. “It's unclear whether this finding is due to true age-related differences in the pathogenesis of cardiovascular calcification or in the effect of bisphosphonates,” said Dr. Elmariah. But the results merit additional studies to tease out the reason for the age-related impact of bisphosphonates on cardiovascular calcification in women, he said.
NCBPs significantly cut cardiovascular calcification in women over 65, said Dr. Sammy Elmariah.
Source Courtesy Dr. Sammy Elmariah
Major Finding: The prevalence of aortic valve ring stenosis was 38% in women aged 65 years and older who took nitrogen-containing bisphosphonates, vs. 59% in women who didn't take bisphosphonates.
Data Source: A cross-sectional study of 3,710 women aged 45–84 years.
Disclosures: Dr. Elmariah has received grant support from the New York Academy of Medicine; the National Heart, Lung, and Blood Institute; and GlaxoSmithKline.
WASHINGTON — Nitrogen-containing bisphosphonates were associated with a significantly decreased prevalence of cardiovascular calcification in women older than 65 years, based on data from 3,710 women who are part of a large, ongoing study.
“Early on in the analysis, we came across a very unexpected finding,” said Dr. Sammy Elmariah of Mount Sinai School of Medicine in New York. “The association with bisphosphonate use was dependent on the patient's age.”
The data were taken from the Multi-Ethnic Study of Atherosclerosis (MESA), a longitudinal cohort study of 6,814 asymptomatic men and women aged 45–84 years.
Overall, the bisphosphonate users were more likely to be older and white. In the current study, Dr. Elmariah and his colleagues examined the impact of bisphosphonates on cardiovascular calcification in women.
Clinical studies have shown that bisphosphonates have an effect on serum lipids, Dr. Elmariah said. Some experimental data, including data from animal models and dialysis patients, suggest that nitrogen-containing bisphosphonates (NCBPs) may limit cardiovascular calcification. In addition, the results of one recent study showed that patients on bisphosphonates for osteoporosis had a slower progression of aortic stenosis, he noted.
The prevalence of aortic valve ring stenosis was 38% in women aged 65 years and older who used NCBPs, which was significantly lower than in non-NCBP users of the same age (59%). Aortic valve ring stenosis prevalence also was 38% in women younger than 65 years who used NCBPs; it was significantly lower at 17% among similarly aged non-NCBP users.
Significant patterns also were seen for stenosis of the thoracic aorta and mitral annulus. The relationship between bisphosphonate use and the decrease in cardiovascular calcification in the 65-years-and-older group did not reach statistical significance for the prevalence of aortic valve stenosis and coronary artery stenosis, but the trends were similar.
This study is the first evaluation of the relationship between bisphosphonate use and the prevalence of cardiovascular calcification in a healthy patient population, Dr. Elmariah said.
Cardiovascular calcification was measured using cardiac CT. Bisphosphate use was defined as use of either oral or intravenous bisphosphonates at the time of the cardiac CT. The average age of the NCBP users was 67 years, and the average age of the nonusers was 62 years. Approximately 60% of the women were white.
After adjustment for variables including age, body mass index, diabetes, hypertension, smoking, race, insurance status, education, and income level, the significance remained, Dr. Elmariah said.
“We get a fairly dramatic reduction in the prevalence of cardiovascular calcification in bisphosphonate users over the age of 65,” he added.
When the researchers divided the study population into 10-year age groups, they saw a gradual reduction in cardiovascular calcification with increasing age, he noted.
The study was limited by its cross-sectional design and by the lack of data on the duration of bisphosphonate use. “It's unclear whether this finding is due to true age-related differences in the pathogenesis of cardiovascular calcification or in the effect of bisphosphonates,” said Dr. Elmariah. But the results merit additional studies to tease out the reason for the age-related impact of bisphosphonates on cardiovascular calcification in women, he said.
NCBPs significantly cut cardiovascular calcification in women over 65, said Dr. Sammy Elmariah.
Source Courtesy Dr. Sammy Elmariah
Maternal Asthma Tied to Risk of Preeclampsia, Prematurity
NEW ORLEANS — Maternal asthma has a significant effect on several adverse pregnancy outcomes including preeclampsia, preterm delivery, and low birth weight, based on a meta-analysis of 30 studies.
Pregnant asthmatic women have been reported to have an overall increased risk of adverse perinatal outcomes, but study results are conflicting, Dr. Jennifer Namazy said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“Our meta-analysis was conducted to see whether the risks were real,” said Dr. Namazy of Scripps Health in San Diego.
Dr. Namazy and her colleagues' review included prospective cohort studies and retrospective studies conducted between 1975 and 2009, in which pregnancy outcomes were compared between women with asthma and nonasthmatic controls. The 30 studies included 8 studies involving asthma management.
Compared with control women without asthma, asthmatic women had a significantly increased risk of preeclampsia (relative risk, 1.54). Low birth weight (defined as 2,500 g or less) was significantly more likely in babies of women with asthma (RR, 1.46). Babies born prematurely (birth after less than 37 weeks' gestation) or small for gestational age were significantly more likely among women with asthma compared with controls (RR, 1.41 and 1.22). Neonatal death was significantly more likely in babies of women with asthma (RR, 1.49). Perinatal mortality (stillbirth plus neonatal death) was significantly more likely in babies of women with asthma (RR, 1.25). No significant associations were seen between maternal asthma and an increased risk of congenital anomalies (RR, 1.08).
“The data suggest that active management may reduce some, but not other perinatal complications,” she said. But active management may not ensure adequate asthma control, and more research is needed to specifically assess the effect of asthma control on perinatal outcomes.
Disclosures: Dr. Namazy has served as a consultant for Genentech.
NEW ORLEANS — Maternal asthma has a significant effect on several adverse pregnancy outcomes including preeclampsia, preterm delivery, and low birth weight, based on a meta-analysis of 30 studies.
Pregnant asthmatic women have been reported to have an overall increased risk of adverse perinatal outcomes, but study results are conflicting, Dr. Jennifer Namazy said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“Our meta-analysis was conducted to see whether the risks were real,” said Dr. Namazy of Scripps Health in San Diego.
Dr. Namazy and her colleagues' review included prospective cohort studies and retrospective studies conducted between 1975 and 2009, in which pregnancy outcomes were compared between women with asthma and nonasthmatic controls. The 30 studies included 8 studies involving asthma management.
Compared with control women without asthma, asthmatic women had a significantly increased risk of preeclampsia (relative risk, 1.54). Low birth weight (defined as 2,500 g or less) was significantly more likely in babies of women with asthma (RR, 1.46). Babies born prematurely (birth after less than 37 weeks' gestation) or small for gestational age were significantly more likely among women with asthma compared with controls (RR, 1.41 and 1.22). Neonatal death was significantly more likely in babies of women with asthma (RR, 1.49). Perinatal mortality (stillbirth plus neonatal death) was significantly more likely in babies of women with asthma (RR, 1.25). No significant associations were seen between maternal asthma and an increased risk of congenital anomalies (RR, 1.08).
“The data suggest that active management may reduce some, but not other perinatal complications,” she said. But active management may not ensure adequate asthma control, and more research is needed to specifically assess the effect of asthma control on perinatal outcomes.
Disclosures: Dr. Namazy has served as a consultant for Genentech.
NEW ORLEANS — Maternal asthma has a significant effect on several adverse pregnancy outcomes including preeclampsia, preterm delivery, and low birth weight, based on a meta-analysis of 30 studies.
Pregnant asthmatic women have been reported to have an overall increased risk of adverse perinatal outcomes, but study results are conflicting, Dr. Jennifer Namazy said at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
“Our meta-analysis was conducted to see whether the risks were real,” said Dr. Namazy of Scripps Health in San Diego.
Dr. Namazy and her colleagues' review included prospective cohort studies and retrospective studies conducted between 1975 and 2009, in which pregnancy outcomes were compared between women with asthma and nonasthmatic controls. The 30 studies included 8 studies involving asthma management.
Compared with control women without asthma, asthmatic women had a significantly increased risk of preeclampsia (relative risk, 1.54). Low birth weight (defined as 2,500 g or less) was significantly more likely in babies of women with asthma (RR, 1.46). Babies born prematurely (birth after less than 37 weeks' gestation) or small for gestational age were significantly more likely among women with asthma compared with controls (RR, 1.41 and 1.22). Neonatal death was significantly more likely in babies of women with asthma (RR, 1.49). Perinatal mortality (stillbirth plus neonatal death) was significantly more likely in babies of women with asthma (RR, 1.25). No significant associations were seen between maternal asthma and an increased risk of congenital anomalies (RR, 1.08).
“The data suggest that active management may reduce some, but not other perinatal complications,” she said. But active management may not ensure adequate asthma control, and more research is needed to specifically assess the effect of asthma control on perinatal outcomes.
Disclosures: Dr. Namazy has served as a consultant for Genentech.
QOL a Factor in Combo vs. Sequential Tx for Ovarian Ca
Major Finding: Median progression-free survival reached 13.7 months for women treated with combination docetaxel and carboplatin therapy, vs. 8.4 months for those treated with sequential therapy.
Data Source: A randomized trial of 150 women with recurrent platinum-sensitive ovarian cancer.
Disclosures: Dr. Alvarez-Secord has received grants and research support from or served as a consultant to several pharmaceutical companies and device manufacturers, including GlaxoSmithKline, Eli Lilly & Co., Sanofi-Aventis, Precision Therapeutics Inc., and Intuitive Surgical Inc.
SAN FRANCISCO — Combination docetaxel and carboplatin therapy significantly improved progression-free survival among women with recurrent platinum-sensitive ovarian cancer, compared with sequential therapy, in a randomized trial of 150 patients.
The improvement was associated with higher neurotoxicity, however, and quality of life studies are ongoing, Dr. Angeles Alvarez-Secord of Duke University in Durham, N.C., said at the annual meeting of the Society of Gynecologic Oncologists.
Combination therapy with docetaxel and carboplatin has been shown to improve survival in platinum-sensitive ovarian cancer patients, but it had not been compared with sequential therapy regarding efficacy and adverse events, Dr. Alvarez-Secord said.
In this multicenter, phase II study, median progression-free survival (the primary end point) reached 13.7 months for women who were treated with combination therapy, vs. 8.4 months for those who received the same drugs in sequence.
Median overall survival was similar at 33 months and 30 months.
After clinical variables were controlled for, women who were treated with sequential therapy had a 62% increased risk of disease progression, compared with those who received combination therapy.
The study population included women with platinum-sensitive peritoneal, ovarian, or tubal cancer who were enrolled between January 2004 and March 2009.
Their average age was 64 years; demographic characteristics were similar between the two groups.
One group of 75 women received 30 mg/m
The overall response rates for the combination and sequential therapies were 55% and 43%.
The incidence of grade 2 or 3 neurotoxicity was higher in the combination therapy group (11.7% vs. 8.5%), as was the incidence of grade 3 or 4 neutropenia (36.8% vs. 11.3%).
“I was very surprised to see that the quality of life was superior for those patients that were treated with sequential monotherapy, compared with combination therapy,” Dr. Alvarez-Secord said in an interview.
The clinical implication of the study is that combination therapy, although yielding a survival benefit, was associated with a worse quality of life, she said.
“It becomes a counseling issue,” she continued.
The results contribute to the larger goal of being able to customize cancer care to a patient's preferences and priorities, rather than taking a one-size-fits-all approach, Dr. Alvarez-Secord said.
Major Finding: Median progression-free survival reached 13.7 months for women treated with combination docetaxel and carboplatin therapy, vs. 8.4 months for those treated with sequential therapy.
Data Source: A randomized trial of 150 women with recurrent platinum-sensitive ovarian cancer.
Disclosures: Dr. Alvarez-Secord has received grants and research support from or served as a consultant to several pharmaceutical companies and device manufacturers, including GlaxoSmithKline, Eli Lilly & Co., Sanofi-Aventis, Precision Therapeutics Inc., and Intuitive Surgical Inc.
SAN FRANCISCO — Combination docetaxel and carboplatin therapy significantly improved progression-free survival among women with recurrent platinum-sensitive ovarian cancer, compared with sequential therapy, in a randomized trial of 150 patients.
The improvement was associated with higher neurotoxicity, however, and quality of life studies are ongoing, Dr. Angeles Alvarez-Secord of Duke University in Durham, N.C., said at the annual meeting of the Society of Gynecologic Oncologists.
Combination therapy with docetaxel and carboplatin has been shown to improve survival in platinum-sensitive ovarian cancer patients, but it had not been compared with sequential therapy regarding efficacy and adverse events, Dr. Alvarez-Secord said.
In this multicenter, phase II study, median progression-free survival (the primary end point) reached 13.7 months for women who were treated with combination therapy, vs. 8.4 months for those who received the same drugs in sequence.
Median overall survival was similar at 33 months and 30 months.
After clinical variables were controlled for, women who were treated with sequential therapy had a 62% increased risk of disease progression, compared with those who received combination therapy.
The study population included women with platinum-sensitive peritoneal, ovarian, or tubal cancer who were enrolled between January 2004 and March 2009.
Their average age was 64 years; demographic characteristics were similar between the two groups.
One group of 75 women received 30 mg/m
The overall response rates for the combination and sequential therapies were 55% and 43%.
The incidence of grade 2 or 3 neurotoxicity was higher in the combination therapy group (11.7% vs. 8.5%), as was the incidence of grade 3 or 4 neutropenia (36.8% vs. 11.3%).
“I was very surprised to see that the quality of life was superior for those patients that were treated with sequential monotherapy, compared with combination therapy,” Dr. Alvarez-Secord said in an interview.
The clinical implication of the study is that combination therapy, although yielding a survival benefit, was associated with a worse quality of life, she said.
“It becomes a counseling issue,” she continued.
The results contribute to the larger goal of being able to customize cancer care to a patient's preferences and priorities, rather than taking a one-size-fits-all approach, Dr. Alvarez-Secord said.
Major Finding: Median progression-free survival reached 13.7 months for women treated with combination docetaxel and carboplatin therapy, vs. 8.4 months for those treated with sequential therapy.
Data Source: A randomized trial of 150 women with recurrent platinum-sensitive ovarian cancer.
Disclosures: Dr. Alvarez-Secord has received grants and research support from or served as a consultant to several pharmaceutical companies and device manufacturers, including GlaxoSmithKline, Eli Lilly & Co., Sanofi-Aventis, Precision Therapeutics Inc., and Intuitive Surgical Inc.
SAN FRANCISCO — Combination docetaxel and carboplatin therapy significantly improved progression-free survival among women with recurrent platinum-sensitive ovarian cancer, compared with sequential therapy, in a randomized trial of 150 patients.
The improvement was associated with higher neurotoxicity, however, and quality of life studies are ongoing, Dr. Angeles Alvarez-Secord of Duke University in Durham, N.C., said at the annual meeting of the Society of Gynecologic Oncologists.
Combination therapy with docetaxel and carboplatin has been shown to improve survival in platinum-sensitive ovarian cancer patients, but it had not been compared with sequential therapy regarding efficacy and adverse events, Dr. Alvarez-Secord said.
In this multicenter, phase II study, median progression-free survival (the primary end point) reached 13.7 months for women who were treated with combination therapy, vs. 8.4 months for those who received the same drugs in sequence.
Median overall survival was similar at 33 months and 30 months.
After clinical variables were controlled for, women who were treated with sequential therapy had a 62% increased risk of disease progression, compared with those who received combination therapy.
The study population included women with platinum-sensitive peritoneal, ovarian, or tubal cancer who were enrolled between January 2004 and March 2009.
Their average age was 64 years; demographic characteristics were similar between the two groups.
One group of 75 women received 30 mg/m
The overall response rates for the combination and sequential therapies were 55% and 43%.
The incidence of grade 2 or 3 neurotoxicity was higher in the combination therapy group (11.7% vs. 8.5%), as was the incidence of grade 3 or 4 neutropenia (36.8% vs. 11.3%).
“I was very surprised to see that the quality of life was superior for those patients that were treated with sequential monotherapy, compared with combination therapy,” Dr. Alvarez-Secord said in an interview.
The clinical implication of the study is that combination therapy, although yielding a survival benefit, was associated with a worse quality of life, she said.
“It becomes a counseling issue,” she continued.
The results contribute to the larger goal of being able to customize cancer care to a patient's preferences and priorities, rather than taking a one-size-fits-all approach, Dr. Alvarez-Secord said.